
Submitted:
27 February 2024
Posted:
28 February 2024
You are already at the latest version
Abstract
Background: One challenge in implant dentistry is to reduce marginal bone resorption to avoid long-term esthetic and biological complications. Sub-gingival implant placement has been suggested as a suitable strategy.
Methods: 38 healthy patients were enrolled to receive bone level (BL – Control group) or 2 mm sub-crestal (SC - Test group) conical connection, platform-switched implants. An immediate tissue level abutment was used in the Test group by following a One Time Abutment (OTA) restorative procedure. Marginal Bone Modification (MBM) was calcu-latied on standardized radiographs at surgery (T0), loading (T1), and 6 months (T2) and 12 months after loading (T3), and cathegorised in Bone Loss (BL) if the resorption occurred below the implant neck and Bone Remodeling (BR) if above. Pocket probing depth (PPD), Bleeding on probing (BoP) and Plaque Index (PI) were also collected.
Results: The mean MBM in the test group after 12 months was 0.61mm, compared to 0.52mm in the control group. However, no BL was observed in the test group, as the MBM completely occurred above the implant neck as BR, whilst in the control group MBM corresponded in total to BL. The average PPD was 2.38mm in the test group and 3.04mm in the control group after 12 months, BoP 50% and 43%, PI 33% and 19.44% respectively.
Conclusions: Sub-crestal conical connection, platform-switched implants could be a suitable clinical choice to avoid BL with exposure of the treated implants surfaces.
Keywords:
Sub-crestal implants
; bone loss
; one time abutment
; conical connection
; mucosal tunnel depth
1. Introduction
Dental implants are a widespread and reliable treatment for the replacement single and multiple missing teeth. Whilst short term clinical success is commonly achieved, the real challenge is to maintain peri-implant hard and soft tissue stability in the long-term, which is crucial for functional and esthetic outcomes, as well as for the prevention of biological complications and, ultimately, implant success [1,2,3,4,5,6,7].
Early implant bone loss, defined as the loss of marginal bone occurring during the first year of the implant prosthetic function, is a multifactorial process which has traditionally been linked to factors such as the surgical procedure, the establishment of a peri-implant biological width, the restorative protocol and the presence of microgaps between the various components [8,9,10]. Whilst historically an early bone loss up to 1.5mm in the first year and 0.2mm for every subsequent year has been deemed acceptable [11,12], recent evidence suggests that an early bone loss exceeding 0.5 mm represents a risk factor for future peri-implantitis development and implant failure [7]. Therefore, several strategies and protocols have been tested with the aim of limiting implant bone loss.
Sub-crestal implant placement has been introduced with the rationale that anticipating the expected early bone loss by adjusting the apico-coronal position of the implant could prevent the exposure of the treated and threaded area of the fixture, lowering the risk of biological and esthetic complications [2,13,14,15]. Sub-crestal placement seems to be particularly important for patients with thin soft tissues at the time of implant placement: a thin biotypes seems to lead to more bone loss, possibly due to the space required for the establishment of a biological width of appropriate dimension [2,9,13,16].
The benefits of sub-crestal implant placement are still controversial, as recent publications found no significant difference in the bone loss around sub-crestal and equi-crestal implants [2,17,18]. However, some authors have recently started arguing that not all bone loss bear the same clinical weight: bone resorption occurring below the implant neck increases the risk of thread exposure and complications, whilst bone resorption above the implant neck leaves the fixture safely covered. Therefore, Linkevicious et al. [19] and Spinato et al. [15] introduced the distinction between bone remodeling observed above the implant collar (smooth or machined titanium surface), and bone loss which instead exposes the implant neck. It is worth mentioning that only implants placed sub-crestal present bone above the collar which could buffer the initial bone modification as bone remodeling, whilst equi-crestal implants inevitably fall into the bone loss category. With this distinction in mind, it seems that sub-crestal implant placement might not prevent bone modification, but it mostly occurs as bone remodeling, with minimal observed bone loss [19].
Sub-crestal implant placement is often used in conjunction with a One Time Abutment (OTA). An OTA consists of an immediate abutment placement at time of implant placement, which will be left in situ for all the restorative procedures, avoiding the multiple disconnection and reconnection of regular abutments during traditional workflows [20,21,22]. The use of an OTA may reduce the risk to damage the supra-crestal soft tissues complex and the implant to abutment connection wear and tear [20,23,24,25].
Other factors that seem to positively influence the initial bone modification relate to the implant design, in specific the choice of an internal conical connection and the platform switching. An internal conical connection between the fixture and the abutment seems to be less prone to bacterial infiltration and more stable under static and dynamic loads, when compared to flat-to flat connection systems [4,26,27,28,29,30] Platform switching of the abutment diameter is thought to provide an horizontal space for soft tissue attachment during the formation of the biological width therefore reducing bone modification [5,31,32]. Finally, the choice of a screw-retained restoration over a cemented one [33,34,35] and the careful positioning of the restorative margin through the correct prosthetic abutment height [36,37,38] are important considerations for the peri-implant tissues stability.
The aim of the present study was to compare the early bone changes around conical connection, platform-switched implants placed at bone level or 2mm sub-crestal. These changes were measured as Marginal Bone Modification (MBM), a term describing the apical repositioning of the peri-implant marginal bone, within which a distinction was made between Bone Remodeling (BR) above the implant neck and Bone Loss (BL) below it. Secondary outcome was the evaluation of peri-implant tissue health through Probing Depth (PD), Bleeding on Probing (Bop) and Plaque Index (PI).
2. Materials and Methods
2.1. Patient Selection
The present study is a single blind, parallel randomized controlled prospective clinical trial, which protocol was reviewed and approved by the local University/Hospital ethical committee (N4078) and recorded in public registry of clinical trials (www.clinicaltrials.gov - NCT06182670). The study was conducted according to the principles of Helsinki Declaration (as revised in Fortaleza 2013), following CONSORT (Consolidated Standards of Reporting Trials) guidelines. Patients were recruited and treated by one experienced operator from April 2021 to May 2023; the study flow-chart is reported in Figure 1.
Patients needing a single tooth replacement in the upper and lower posterior areas (premolar and molar) by means of an implant fixed rehabilitation were included in the present study. The implant site was assessed for bone volume and space based on the following requirements: 1,5 millimeter of residual buccal and lingual bone around the selected implant diameter, a minimum bone height of 10.5mm, in order to place an implant with a minimum length of 7.5mm, and at least 1.5 millimeters of bone between the fixture and the adjacent tooth. Patients with systemic diseases, history of radiation therapy in the head and neck region, current treatment with steroids, neurological or psychiatric impairments that could interfere with good oral hygiene, immuno-compromised status, including infection with human immunodeficiency virus, severe clenching or bruxism, smokers (more than 10 cigarettes per day), drug or alcohol abuse and inadequate compliance were excluded. All included patients gave their written consent after being informed in detail about the objectives of the study.
Before treatment, patients were clinically and radiographically evaluated. An orthopantomography and peri-apical radiographs were used as a first level exam to evaluate the bone quantity before implant placement. A cone beam TC was also performed to plan for a prosthetically guided implant placement..
2.2. Surgical Procedures
All surgical and prosthetic procedures were performed by a single operator (ES), and All cases have been treated with the same implant system (Advan GTB-Tzero, Advan S.r.l. Via Linussio, 1 33020 – Amaro, Italy) provided with platform switching and conical hybrid connection. Under local anesthesia, an incision along the center of the ridge was performed. After elevating a mucoperiosteal buccal envelope flap, supra-crestal soft tissue height (STH) of the undetached lingual flap was measured using a periodontal probe (PC-PUNC 15 HU-Friedy, Milan, Italy). An independent investigator then opened the randomization envelope and communicated patient’s group allocation to the surgeon. Control group received a bone level implant placement (BL) whilst Test group received a 2 millimeters sub-crestal implant placement (SC). (Figure 2, Figure 3 and Figure 4)
Implant site preparation was performed by following manufacturer's instructions. Insufficient implant primary stability (< 35 Ncm) and therefore the necessity to bury the implant was considered an exclusion criteria for the present study.
Trans-mucosal healing abutments were inserted on the BL implants, whilst a Gingival Former Abutment (GFA) for the One Time Abutment technique was connected to the implants belonging to the SC group. The flaps were repositioned and sutured, and post-operatory instructions provided. Ibuprofen 600 mg every 4-6 hours was prescribed for pain relief.
2.3. Prosthetic Protocol
Three months after surgery, implant-level and abutment-level impressions were taken to provide for single crown screw-retained restorations for the Control and Test group respectively (Figure 5 and Figure 6).
The final crowns were inserted two weeks after impressions.
2.4. Radiographic Evaluations
All peri-apical radiographs for the measurement of the Marginal Bone Modification (MBM) were taken with a standardized parallel technique (FONA™ Dental Image Plates). Images were then analyzed with a computer software (Image J, National Institute of Health, Bethesda, Rockville, MA, USA). Before measurement, each radiograph was calibrated by using the implant diameter as a reference to correct any distortion. Measurements were repeated twice by a single operator (MZ). MBM measurements were taken at both mesial and distal crest.
For each implant, radiographs performed at the time of surgical implant placement (T0), restoration delivery (T1), and after 6 (T2) and 12 (T3) months of prosthetic function were analyzed. The most coronal extension of the crestal bone at the time of the surgical placement was identified as Marginal Bone Level (MBL). MBL in the BL group corresponds to the level of the implant neck, whilst it is positioned coronal to it in the SC group. In the assessment of the MBM, Bone Remodeling (BR) and Bone Loss (BL) were distinguished. Bone loss was measured as the distance between the initial MBL and first radiographically visible bone-to-implant contact apical to the implant neck, whilst Bone Remodeling as the distance from the initial MBL to first point of contact coronal to the implant neck. The mean value of the mesial and distal MBM measurements was pooled for each implant. Any apical MBM was expressed as negative number. (Figure 12)
2.5. Clinical Evaluations
Peri-implant soft tissues parameters were collected using a calibrated probe (Vivacare TPS probe Vivadent, Scahaan, Liechtenstein) (Figure 15).
Probing depth (PD) was measured at four aspects (mesial, distal, buccal, palatal) following the Mombelli and Lang (1994) classification [39]. Bleeding on probing (BOP) and Plaque Index (PI) were measured at implant site by following Trombelli et al. (2018) [40] and O’Leary (1972) classifications [41]. PD, BoP and PI indexes were measured at different at each follow-up visits: 6 and 12 months after restoration delivery (Figure 1).
2.6. Sample Size and Randomization
Sample size was computed assuming a two parallel groups design with balanced groups and an independent sample t-test. We assumed a single implant and a single measurement for patient, a standard deviation of 0.5 mm and an average difference of at least 0.5mm. A total sample size of 34 patients provides a power of at least 80% at a 5% significance level. Assuming a 15% drop-out, the total sample size is N=40 patients.
2.7. Statistical Analysis
Data is described using standard statistics such as, mean, median standard deviation and IQR for quantitative variable, and counts and percentages for qualitative variables.Variation in MBL is modelled using both a simple t-test for independent samples (after averaging values within patients) as well as a multilevel model using GEE (Generalised Estimating Equations) on individual site measurements and accounting for within subject correlation.
Secondary continuous outcomes are modelled using GEE with ad hoc error distribution according to outcome (Gaussian for PPD, CAL, REC, binomial for BOP).Results are expressed as estimates and relative 95% confidence intervals. A significance level of 5% is used for all the comparisons and all analysis are performed using R (version 3.6.3 or higher).
3. Results
Thirty-eight patients (15 males and 23 females, respectively) aged from 23 to 72 years (mean age 49.4±32.4 years) were recruited in the present study, and 36 completed the study: two implants were considered as drop-outs due to insufficient implant primary stability (< 35 Ncm) during the implant placement. Patients demographic characteristics are reported in Table 1.
The implant and surgical site characteristics are reported in Table 2: 12 (33,3%) implants were positioned in the upper jaw. 21 implants (58,3%) were in molar region. 23 implants (63,9%) were 3,6x 9 mm and 13 (36,1%) 4,3x 7,5 mm. Observed STH was 3 mm in 21 patients (58,4%) and 2 mm in 12 (33,3%). No patient had STH equal to 1 mm and only 3 patients (8,3%) had 4 mm.
MBM for both groups from the baseline (T0) to the prosthetic loading (T1), six months follow-up visit (T2) and 1 year follow-up visit (T3) were statically significant (p<0.01) as shown in Table 3. Particularly, after 1-year of loading, the mean MBM in the Control group was -0,52 mm compared to the baseline (T0), and -0.60 mm in Test group. However, no significant difference was observed when the MBM values in two study groups were compared (p>0.05) (Table 3). The Control Group showed a mean Bone Loss (BL) equivalent to the MBM values, whilst no MBM below the implant neck was noted for the Test Group, therefore the Bone Loss for this group equals to zero at all time points.
Clinical peri-implant parameters modification over time are reported in Table 4. In the control group, a mean PD of 3.04 mm was observed after 1 year (T3), while mean PD was 2.38 mm in test group, with a statistically significant difference (p<0.05). The mean BoP at 1 year (T3), was 43.06% in the control group and 50% in the test group, with no statistically significant intergroup difference (p>0.05). Comparably, control and test group PI indexes after 1 year were 19.44% and 33.33%, respectively (p>0.05).
4. Discussion
The present study evaluate the Marginal Bone Modification around one stage, platform-switched, internal conical connection implants positioned 2 mm sub-crestally or equi-crestal. The results show that the mean MBM or the Test and Control group was comparable with values of 0.61mm and 0.52mm respectively at 12 months of prosthetic function. However, following the distinction made by Linkevicious et al. [19] and Spinato et al. [15], all the MBM in the Control group equi-crestal implants developed as Bone Loss below the implant neck level, whilst the MBM in the Test group was limited to the area above the implant neck, due to the 2mm of sub-crestal depth of the planned fixture position. Therefore, MBM in the Test group resulted in zero bone loss. This leaves on average 1.5mm of coronal marginal bone that protects the treated and threaded portion of the fixture, helping to prevent future biological and esthetic complications [2,13,14,15]. In fact, in a recent 10-years prospective study, Windael and colleagues [7] demonstrated that implants with Early BL >0,5mm during the first year of function showed 5.43 times higher odds of future peri-implantitis development than implants with Early BL <0,5mm.
Bone loss seems to have mostly occurred in the first 3 months after surgery for both groups, in agreement with other histological studies on animals and humans conducted [42,43,44]. In those studies, they also demonstrated that implant supra crestal soft tissues around implants then tend to stabilize after 8-12 weeks, achieving an average height of 3.6mm height on average, which constitutes the new biological width. MBM seems to be a necessary step for the re-establishment of such dimension [19]. As a consequence, mucosal thickness at the time of implant placement is a significant influencing factor on peri-implant marginal bone stability, and the soft tissue height seems to be inversely proportional to the early bone resorption. This is likely due to the necessary space for the formation of the 3.6mm of tissue height aforementioned, which occurs at the expense of the bone [7,9,13,16,45,46]. In the present study a soft tissue thickness ranged between 1 to 4 mm, with 2 and 3 mm being the most frequent values. Linkevicious et al. [45] analyzed the bone loss around bone-level implants in patient with thin (<2mm) and thick (>2mm) soft tissue and found a mean bone loss of 1.17mm in the first group at 12 months after restoration. Despite one third of the patients in our control group showing a STH of 2mm, none of the implants exceeded 0.75mm of bone loss. This difference might be due to other factors such as implant type and design.
Our bone loss results are in line with the one obtained by Vervake et al. [16] and Linkevicious et al. [19], who measured 0.04mm and 0.11mm of bone loss respectively around sub-crestally placed platform-switched implants. Linkevicious et al. [19] also observed 0.33mm of bone loss around equi-crestal implants, more than in the current study. However, they also performed a soft tissue augmentation procedure which could have provided the extra space for the biological width re-establishment.
When assessing the soft tissues, the mean PD value in the test group was 2.38 mm at 12 months after loading and 3.04 mm in the control group, respectively. That difference was both statistically and clinically significant considering the confidence interval of 2.13-2.62 for the test group and 2.64-3.45 in the control group. It means that in the test group more than 2.62mm of PD could not be found, while in the control group values even up to 3.45mm could be observed. The recent literature highlighted that the depth of the mucosal tunnel modifies can be a crucial factor in the treatment peri-implant mucositis, should it occur [25]. Chan et al. [25] showed that deeper mucosal tunnel depth (>= 3mm) is associated to a chronic inflammation. Crown removal and professional hygiene were needed to revert such mucositis. Differently, in the shallow tunnel depth <= 1mm just the oral hygiene practice was sufficient to revert the mucositis. Accessibility for biofilm removal around implant prosthesis is crucial for preventing and managing peri-implant diseases [47].
An additional observation was made in the test group: one year after loading, in 18% of cases BoP without presence of plaque was observed. The authors’ assumption is that the bleeding was due to compression of the soft tissues by the crown contour. In those cases, the crowns were unscrewed from the GFA, therefore without interfering with the integrity of the mucosal barrier, remodeled and polished to reduce the soft tissues compression. It was also possible to check the health of the free gingival sulcus around the GFA. The mean PD was 1.22 mm (IC 1.07-1.37mm), and juxtagingival position of the restoration margin was confirmed. This aspect may be important in patients with a history of periodontitis and high risk of implant diseases [48] in the posterior sectors where home hygiene procedures are difficult, and aesthetics is less important. Heitz-Mayfield and colleagues, in a recent randomized controlled clinical trial [36] on the management of peri-implant mucositis, showed that implants with supra-mucosal restoration margins yelded significantly greater reductions in probing depth following treatment compared to those with submucosal margins.
A limitation of the current study is that the BL control group was restored with crowns directly screwed to the implant with Ti-base abutment while in the test group a definitive GFA was used, following a One Time Abutment (OTA) prosthetic workflow. The rationale behind an OTA is to limit the disconnection and reconnection of the abutment from the fixture, which is shown to possibly negatively affect marginal bone levels [49]. However, the topic is still controversial: in fact, some papers seem to associate OTA technique to improved marginal bone stability when compared to traditional restorative procedures [20,21,22,49,50,51], whilst others failed to find significant advantages [23,52,53].
Linkevicious et al. [54] found that immediate abutments significantly reduce the amount of early bone loss at 1 month after prothesis delivery on sub-crestal implants, however no difference is found with traditional abutments at 12 months. It also appears that bone gain was obtained around traditional implant-level restorations. Conversely, a slight bone gain was observed in the test group of the present study, where the average Bone Remodeling at 6 months was -0.72mm, but becase -0.60mm at 12months.
On the other hand, Molina et al. [50] found the OTA significantly reduced the early bone loss around equi-crestal implants. Therefore, it appears that minimal disturbance of soft tissues might be of greater importance for equi-crestal implants. The bone loss observed by Molina et al. [50] around implants with traditional prosthetic workflow was 1.21mm on average, higher than the one observed in the present group. This again, could be due to differences in implant design. The choice to use the definitive GFA in the present study was due to the manufacturing company recommendations, and to facilitate the impression on deep transmucosal tunnel. However it would be interesting to replicate in a future trial both protocols of Molina et al. and Linkevicious et al. [50,54].
Nevertheless, the authors believe it would be misleading to consider separately every single factor associated to implant failure or success. A more global comprehension of different clinical parameters interacting together with the peri-implant hard and soft tissues would be more effective way to understand the crucial balance between patient biology and the implant [9,36,45].
5. Conclusions
The use of internal conical connection, platform switching implants placed 2mm sub-crestal and restored though a One Time Abutment workflow with screw-retained crowns, could result in marginal bone modifications with zero bone loss. Further clinical studies will be necessary to better understand the role of the OTA and the relationship between the STH and bone modification. Only long-term follow ups will be able to demonstrate the theoretical reduction in risk of biological complications.
Author Contributions
Conceptualization, methodology and founding acquisition MM; investigation ES; software analysis MZ, validation SS; SC formal analysis and data curation, writing DL, MM, ES, MZ, SC, medical writer and English reviewer AS. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by ADVAN SRL.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee of ASST Spedali Civili di Brescia (Prot. N. 4078).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy policies.
Acknowledgments
The authors are grateful to Matteo Dalè DDS and Sivia Marchetti DDS for the support during the clinical procedure and to Nicolò Cea DDS for the Image-J software calibration and Annamaria Sordillo DDS for English review.
Conflicts of Interest
Magda Mensi reports honorarium for lectures from ADVAN SRL. The other authors declare no conflicts of interest.
References
- Buser, D.; Mericske-Stern, R.; Dula, K.; Lang, N.P. Clinical Experience with One-Stage, Non-Submerged Dental Implants. Adv Dent Res 1999, 13, 153–161. [Google Scholar] [CrossRef]
- Palacios-Garzón, N.; Velasco-Ortega, E.; López-López, J. Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis. Materials 2019, 12. [Google Scholar] [CrossRef]
- Liu, M.; He, L.; Wang, H. Clinical and Radiographic Performance of One-Piece and Two-Piece Implant: A Systematic Review and Meta-Analysis. J Prosthodont Res 2021, 65, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Candotto, V.; Gabrione, F.; Oberti, L.; Lento, D.; Severino, M. The Role of Implant-Abutment Connection in preventing Bacterial Leakage: A Review. J Biol Regul Homeost Agents. 2019, 3, 129–134. [Google Scholar]
- Annibali, S.; Bignozzi, I.; Cristalli, M.P.; Graziani, F.; La Monaca, G.; Polimeni, A. Peri-Implant Marginal Bone Level: A Systematic Review and Meta-Analysis of Studies Comparing Platform Switching versus Conventionally Restored Implants. J Clin Periodontol 2012, 39, 1097–1113. [Google Scholar] [CrossRef]
- Cochran, D.L.; Mau, L.P.; Higginbottom, F.L.; Wilson, T.G.; Bosshardt, D.D.; Schoolfield, J.; Jones, A.A. Soft and Hard Tissue Histologic Dimensions Around Dental Implants in the Canine Restored with Smaller-Diameter Abutments: A Paradigm Shift in Peri-Implant Biology. Int J Oral Maxillofac Implants 2013, 28, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Windael, S.; Collaert, B.; De Buyser, S.; De Bruyn, H.; Vervaeke, S. Early Peri-Implant Bone Loss as a Predictor for Peri-Implantitis: A 10-Year Prospective Cohort Study. Clin Implant Dent Relat Res 2021, 23, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Hermann, J.S.; Buser, D.; Schenk, R.K.; Cochran, D.L. Crestal Bone Changes Around Titanium Implants. A Histometric Evaluation of Unloaded Non-Submerged and Submerged Implants in the Canine Mandible. 2000, 71. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.; Yoon, J.; Misch, C.E.; Wang, H. The Causes of Early Implant Bone Loss: Myth or Science? J Periodontol 2002, 73, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Tatarakis, N.; Bashutski, J.; Wang, H.L.; Oh, T.J. Early Implant Bone Loss: Preventable or Inevitable? Implant Dent 2012, 21, 379–386. [Google Scholar] [CrossRef]
- Smith, D.E.; Zarb, G.A. Criteria for Success of Osseointegrated Endosseous Implants. J Prosthet Dent 1989, 62, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.O.; Sennerby, L. Initial and Long-Term Crestal Bone Responses to Modern Dental Implants. Periodontol 2000 2017, 73, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Vervaeke, S.; Matthys, C.; Nassar, R.; Christiaens, V.; Cosyn, J.; De Bruyn, H. Adapting the Vertical Position of Implants with a Conical Connection in Relation to Soft Tissue Thickness Prevents Early Implant Surface Exposure: A 2-Year Prospective Intra-Subject Comparison. J Clin Periodontol 2018, 45, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Lamazza, L.; Rapani, A.; Troiano, G.; Messina, M.; Antonelli, A.; Giudice, A.; Lombardi, T. Marginal Bone Changes around Platform-Switched Conical Connection Implants Placed 1 or 2 Mm Subcrestally: A Multicenter Crossover Randomized Controlled Trial. Clin Implant Dent Relat Res 2023, 25, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Spinato, S.; Bernardello, F.; Lombardi, T.; Soardi, C.M.; Messina, M.; Zaffe, D.; Stacchi, C. Influence of Apico-Coronal Positioning of Tissue-Level Implants on Marginal Bone Stability during Supracrestal Tissue Height Establishment: A Multi-Center Prospective Study. Clin Implant Dent Relat Res 2022, 24, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Vervaeke, S.; Dierens, M.; Besseler, J.; De Bruyn, H. The Influence of Initial Soft Tissue Thickness on Peri-Implant Bone Remodeling. Clin Implant Dent Relat Res 2014, 16, 238–247. [Google Scholar] [CrossRef]
- Al Amri, M.D. Crestal Bone Loss around Submerged and Nonsubmerged Dental Implants: A Systematic Review. [CrossRef]
- Romanos, G.E.; Aydin, E.; Gaertner, K.; Nentwig, G.H. Long-Term Results after Subcrestal or Crestal Placement of Delayed Loaded Implants. Clin Implant Dent Relat Res 2015, 17, 133–141. [Google Scholar] [CrossRef]
- Linkevicius, T.; Puisys, A.; Linkevicius, R.; Alkimavicius, J.; Gineviciute, E.; Linkeviciene, L. The Influence of Submerged Healing Abutment or Subcrestal Implant Placement on Soft Tissue Thickness and Crestal Bone Stability. A 2-Year Randomized Clinical Trial. Clin Implant Dent Relat Res 2020, 22, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q. qing; Dai, R.; Cao, C.Y.; Fang, H.; Han, M.; Li, Q.L. One-Time versus Repeated Abutment Connection for Platform-Switched Implant: A Systematic Review and Meta-Analysis. PLoS One 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Vatėnas, I.; Linkevičius, T. One Abutment One Time vs. Repeatable Abutment Disconnections in Implants, Restored with Cemented/Screw Retained Fi Xed Partial Dentures: Marginal Bone Level Changes. A Systematic Review and Meta-Analysis. 2021, 23. [Google Scholar]
- Grandi, T.; Guazzi, P.; Samarani, R.; Garuti, G. Immediate Positioning of Definitive Abutments versus Repeated Abutment Replacements in Immediately Loaded Implants: Effects on Bone Healing at the 1-Year Follow-up of a Multicentre Controlled Trial. Eur J Oral Implantol 2012, 5, 9–16. [Google Scholar] [PubMed]
- Ríos-Santos, J.V.; Tello-González, G.; Lázaro-Calvo, P.; Mur, F.J.G.; Ríos-Carrasco, B.; Fernández-Palacín, A.; Herrero-Climent, M. One Abutment One Time: A Multicenter, Prospective, Controlled, Randomized Study. Int J Environ Res Public Health 2020, 17, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, R.; Di Girolamo, M.; Mirisola, C.; Baggi, L. Effects of Repeated Screw Tightening on Implant Abutment Interfaces in Terms of Bacterial and Yeast Leakage in Vitro: One-Time Abutment Versus the Multiscrewing Technique. Int J Periodontics Restorative Dent 2016, 36, 275–280. [Google Scholar] [CrossRef]
- Chan, D.; Pelekos, G.; Ho, D.; Cortellini, P.; Tonetti, M.S. The Depth of the Implant Mucosal Tunnel Modifies the Development and Resolution of Experimental Peri-Implant Mucositis: A Case–Control Study. J Clin Periodontol 2019, 46, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Penarrocha-Oltra, D.; Soldini, C.; Mazzocco, F.; Penarrocha, M.; Covani, U. Microbiological Assessment of the Implant-Abutment Interface in Different Connections: Cross-Sectional Study after 5 Years of Functional Loading. Clin Oral Implants Res 2015, 26, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.M.; Nogueira-Filho, G.; Tenenbaum, H.C.; Lai, J.Y.; Brito, C.; Döring, H.; Nonhoff, J. Performance of Conical Abutment (Morse Taper) Connection Implants: A Systematic Review. J Biomed Mater Res A 2014, 102, 552–574. [Google Scholar] [CrossRef]
- Vetromilla, B.M.; Brondani, L.P.; Pereira-Cenci, T.; Bergoli, C.D. Influence of Different Implant-Abutment Connection Designs on the Mechanical and Biological Behavior of Single-Tooth Implants in the Maxillary Esthetic Zone: A Systematic Review. [CrossRef]
- Weng, D.; Nagata, M.J.H.; Bosco, A.F.; de Melo, L.G.N. Influence of Microgap Location and Configuration on Radiographic Bone Loss Around Submerged Implants: An Experimental Study in Dogs. Int J Oral Maxillofac Implants 2011, 26, 941–946. [Google Scholar]
- Weng, D.; Nagata, M.J.H.; Leite, C.M.; de Melo, L.G.N.; Bosco, A.F. Influence of Microgap Location and Configuration on Radiographic Bone Loss in Nonsubmerged Implants: An Experimental Study in Dogs. Int J Prosthodont 2011, 24, 445–452. [Google Scholar]
- Lazzara, R.J.; Porter, S.S. Platform Switching: A New Concept in Implant for Controlling Postrestorative Crestal Bone. Int J Periodontics Restorative Dent 2006, 26, 9–17. [Google Scholar] [CrossRef]
- Hermann, J.S.; Schenk, R.K.; Schoolfield, J.D. Biologic Width around One- and Two-Piece Titanium Implants A Histometric Evaluation of Unloaded Nonsubmerged and Submerged Implants in Tbe. Clin Oral Implants Res 2001, Dec;12, 559–71. [Google Scholar] [CrossRef]
- Sailer, I.; Mühlemann, S.; Zwahlen, M.; Hämmerle, C.H.F.; Schneider, D. Cemented and Screw-Retained Implant Reconstructions: A Systematic Review of the Survival and Complication Rates. Clin Oral Implants Res 2012, 23, 163–201. [Google Scholar] [CrossRef]
- Wilson Jr., T. G. The Positive Relationship Between Excess Cement and Peri-Implant Disease: A Prospective Clinical Endoscopic Study. J Periodontol 2009, 80, 1388–1392. [Google Scholar] [CrossRef]
- Linkevicius, T.; Vindasiute, E.; Puisys, A.; Peciuliene, V. The Influence of Margin Location on the Amount of Undetected Cement Excess after Delivery of Cement-Retained Implant Restorations. Clin Oral Implants Res 2011, 22, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Salvi, G.E.; Botticelli, D.; Mombelli, A.; Faddy, M.; Lang, N.P. Anti-Infective Treatment of Peri-Implant Mucositis: A Randomised Controlled Clinical Trial. Clin Oral Implants Res 2011, 22, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Schätzle, M.; Lang, N.P.; Ånerud, Å.; Boysen, H.; Bürgin, W.; Löe, H. The Influence of Margins of Restorations on the Periodontal Tissues over 26 Years. J Clin Periodontol 2001, 28, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; León-Cano, A.; Ortega-Oller, I.; Monje, A.; Suárez, F.; O’Valle, F.; Spinato, S.; Catena, A. Prosthetic Abutment Height Is a Key Factor in Peri-Implant Marginal Bone Loss. J Dent Res 2014, 93, 80S–85S. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Lang, N.P. Clinical Parameters for the Evaluation of Dental Implants. Periodontol 2000 1994, 4, 81–86. [Google Scholar] [CrossRef]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-Induced Gingivitis: Case Definition and Diagnostic Considerations. J Clin Periodontol 2018, 45, S44–S67. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The Plaque Control Record. J Periodontol 1972, 43, 38–38. [Google Scholar] [CrossRef]
- Bolle, C.; Gustin, M.P.; Fau, D.; Exbrayat, P.; Boivin, G.; Grosgogeat, B. Early Periimplant Tissue Healing on 1-Piece Implants with a Concave Transmucosal Design: A Histomorphometric Study in Dogs. In Proceedings of the Implant Dentistry; Lippincott Williams and Wilkins, 1 October 2015; Volume 24, pp. 598–606. [Google Scholar]
- Tomasi, C.; Tessarolo, F.; Caola, I.; Wennström, J.; Nollo, G.; Berglundh, T. Morphogenesis of Peri-Implant Mucosa Revisited: An Experimental Study in Humans. Clin Oral Implants Res 2014, 25, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Nevins, M.; Kim, D.M.; Jun, S.-H.; Guze, K.; Schupbach, P.; Nevins, M.L. Histologic Evidence of a Connective Tissue Attachment to Laser Microgrooved Abutments: A Canine Study. Int J Periodontics Restorative Dent 2012, 30, 245–255. [Google Scholar] [CrossRef]
- Linkevicius, T.; Puisys, A.; Steigmann, M.; Vindasiute, E.; Linkeviciene, L. Influence of Vertical Soft Tissue Thickness on Crestal Bone Changes Around Implants with Platform Switching: A Comparative Clinical Study. Clin Implant Dent Relat Res 2015, 17, 1228–1236. [Google Scholar] [CrossRef]
- Linkevicius, T.; Apse, P.; Grybauskas, S.; Puisys, A. Reaction of Crestal Bone around Implants Depending on Mucosal Tissue Thickness. A 1-Year Prospective Clinical Study. 2009, Vol. 11. [Google Scholar]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-Implant Mucositis. J Clin Periodontol 2018, 45, S237–S245. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Heitz, F.; Lang, N.P. Implant Disease Risk Assessment IDRA–a Tool for Preventing Peri-Implant Disease. Clin Oral Implants Res 2020, 31, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Koutouzis, T.; Gholami, F.; Reynolds, J.; Lundgren, T.; Kotsakis, G. Abutment Disconnection/Reconnection Affects Peri-Implant Marginal Bone Levels: A Meta-Analysis. Int J Oral Maxillofac Implants 2017, 32, 575–581. [Google Scholar] [CrossRef]
- Molina, A.; Sanz-Sánchez, I.; Martín, C.; Blanco, J.; Sanz, M. The Effect of One-Time Abutment Placement on Interproximal Bone Levels and Peri-Implant Soft Tissues: A Prospective Randomized Clinical Trial. Clin Oral Implants Res 2017, 28, 443–452. [Google Scholar] [CrossRef]
- Gabriel De Carvalho Barbara, J.; Luz, D.; Vianna, K.; Porto Barboza, E. The Influence of Abutment Disconnections on Peri-Implant Marginal Bone: A Systematic Review. 2019, Vol. 12. [Google Scholar]
- Praça, L. de F.G.; Teixeira, R.C.; Rego, R.O. Influence of Abutment Disconnection on Peri-Implant Marginal Bone Loss: A Randomized Clinical Trial. Clin Oral Implants Res 2020, 31, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Koutouzis, T.; Koutouzis, G.; Gadella, H.; Neiva, R. The Effect of Healing Abutment Reconnection and Disconnection on Soft and Hard Peri-Implant Tissues: A Short-Term Randomized Controlled Clinical Trial. Int J Oral Maxillofac Implants 2013, 28, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Linkevicius, R.; Gineviciute, E.; Alkimavicius, J.; Mazeikiene, A.; Linkeviciene, L. The Influence of New Immediate Tissue Level Abutment on Crestal Bone Stability of Subcrestally Placed Implants: A 1-Year Randomized Controlled Clinical Trial. Clin Implant Dent Relat Res 2021, 23, 259–269. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study flowchart and Timeline.
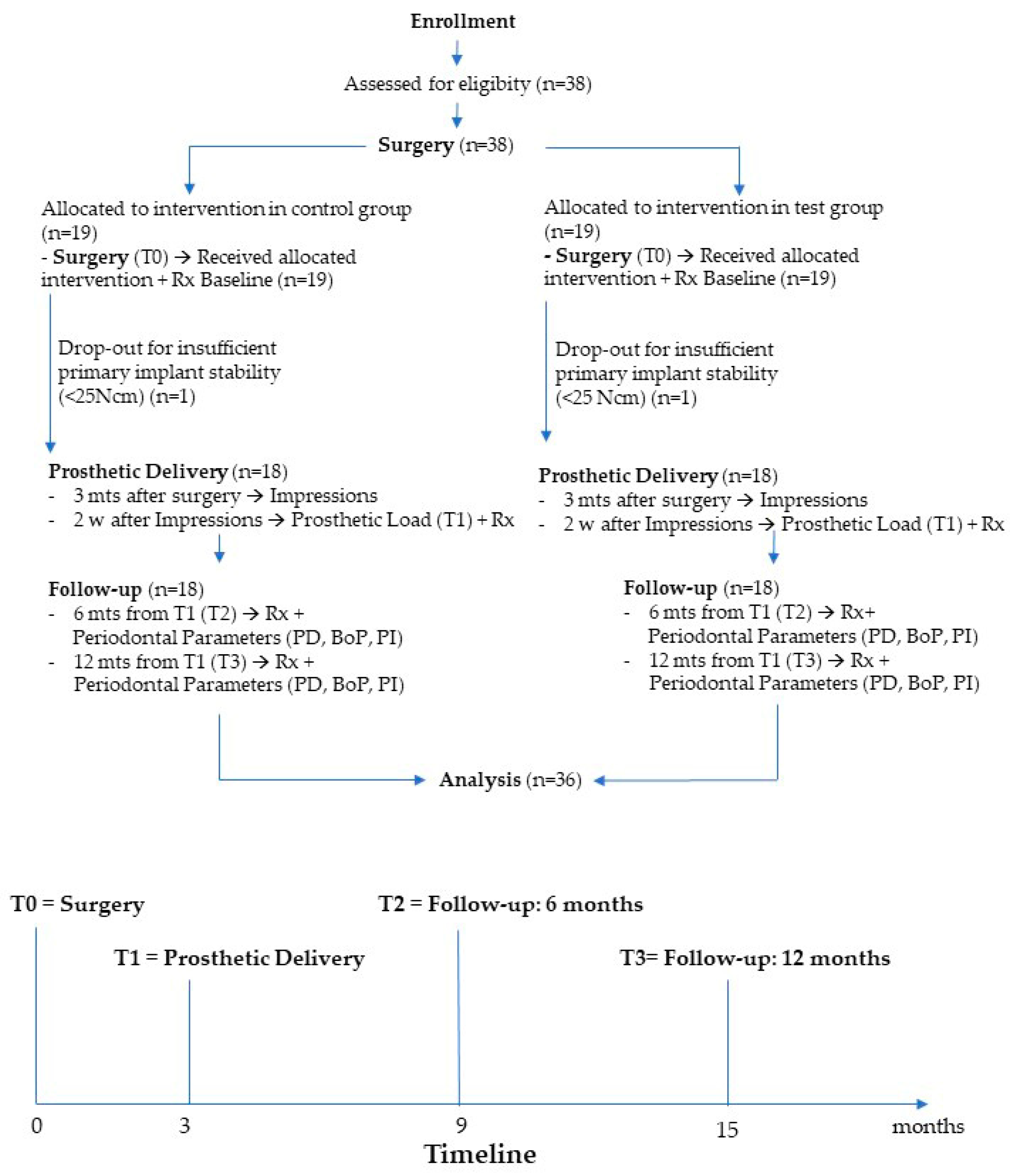
Figure 2.
Bone level implant (BL - Control Group) and sub-crestal level implant (SC - Test Group) surgical placement protocol.
Figure 2.
Bone level implant (BL - Control Group) and sub-crestal level implant (SC - Test Group) surgical placement protocol.
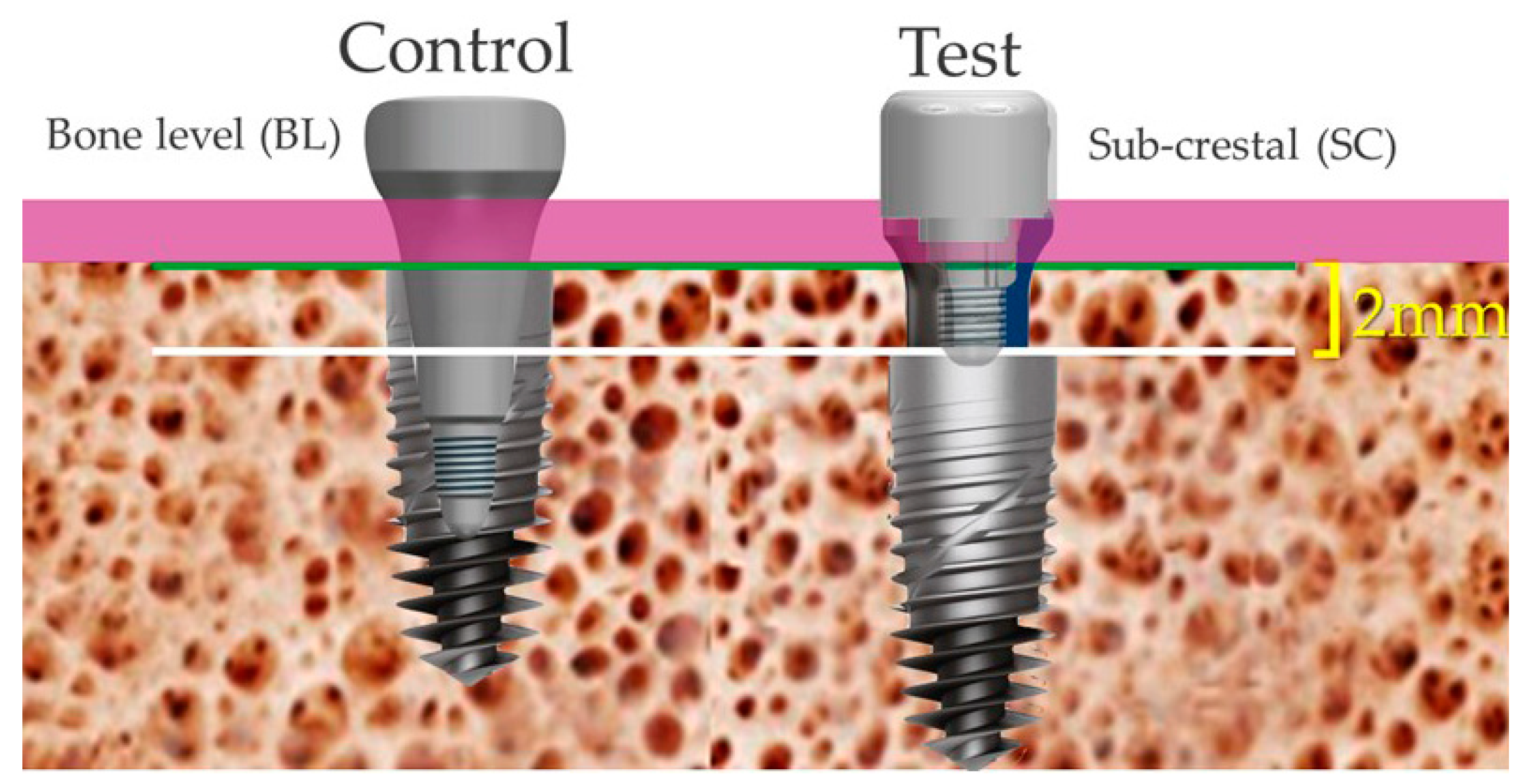
Figure 3.
Bone level implant (BL - Control Group). Occlusal view.
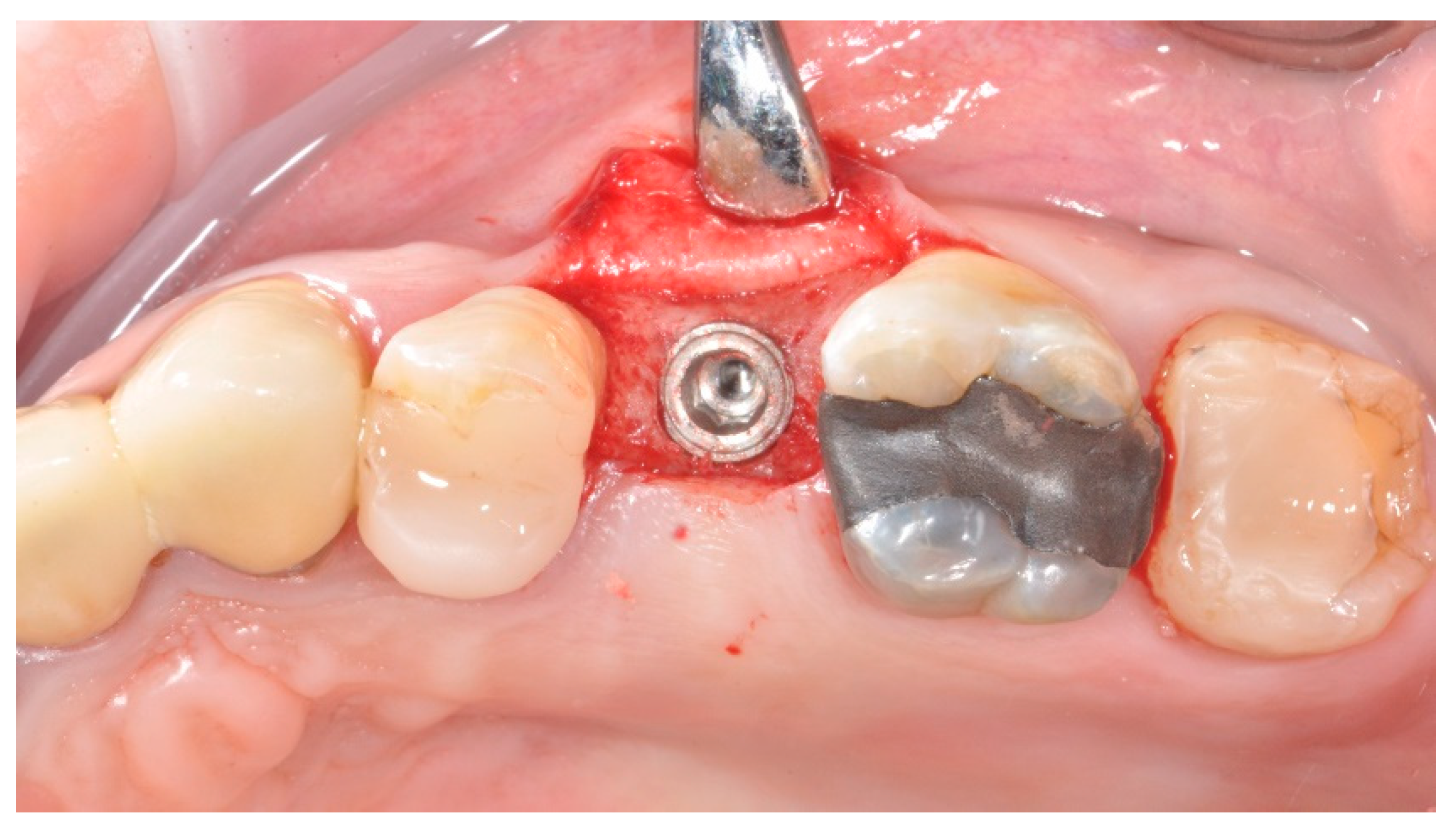
Figure 4.
Sub-crestal implant (SC - Test Group). Occlusal view.
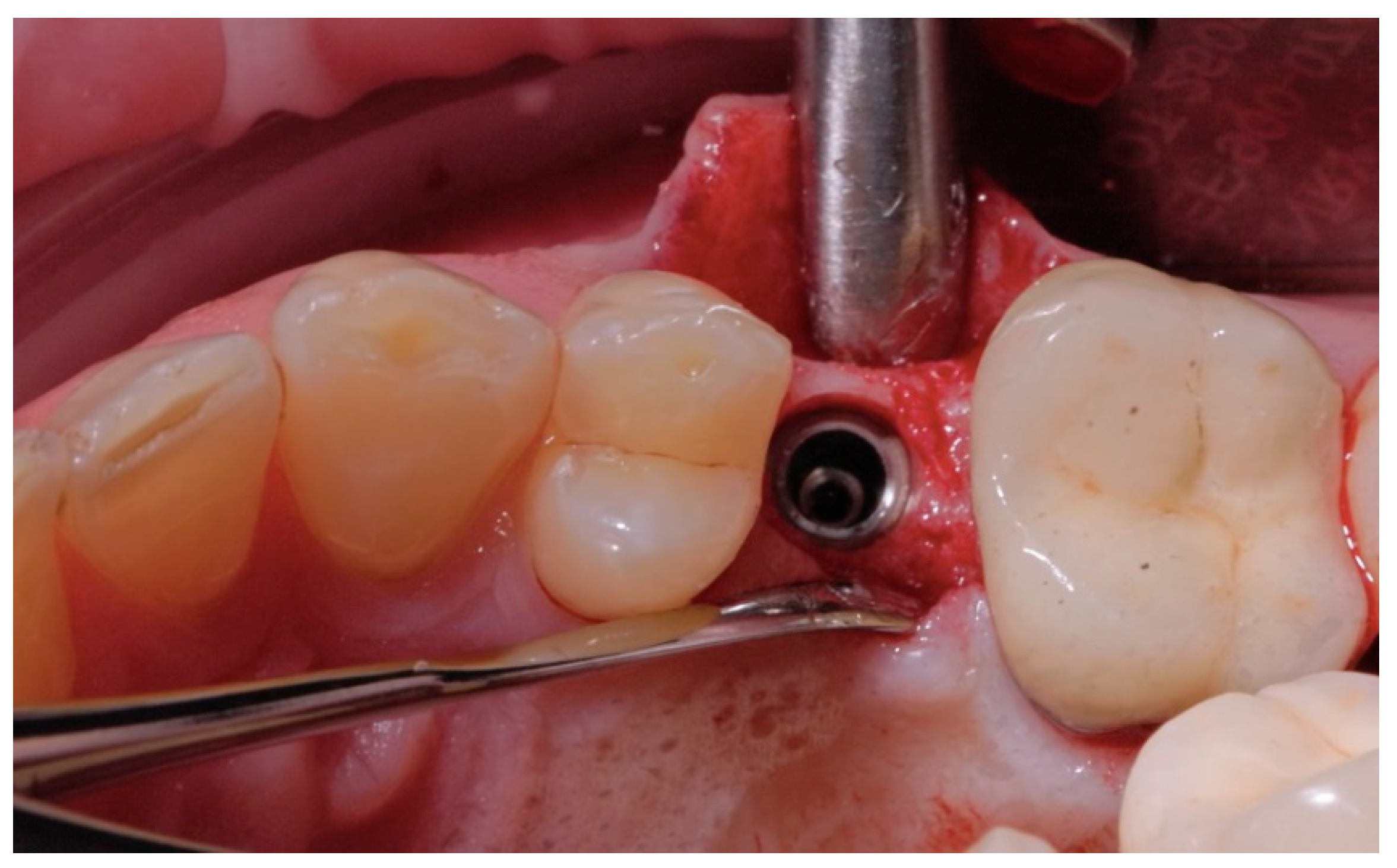
Figure 5.
Peri-implant soft tissues at time of impression: BL - Control Group.

Figure 6.
Peri-implant soft tissues at time of impression: SC - Test group.

Figure 7.
Screw-retained fixed prosthesis secured to the implant (BL - Control Group): buccal to lingual emergence profiles.
Figure 7.
Screw-retained fixed prosthesis secured to the implant (BL - Control Group): buccal to lingual emergence profiles.

Figure 8.
Screw-retained fixed prosthesis secured to the GFA (SC - Test group): buccal to lingual emergence profiles.
Figure 8.
Screw-retained fixed prosthesis secured to the GFA (SC - Test group): buccal to lingual emergence profiles.

Figure 9.
Ti-Base titanium Grade V (left) used for one-piece restoration directly connected to the fixture. GFA (right) screwed to the implants and used for two-pieces restoration connected to the GFA abutment.
Figure 9.
Ti-Base titanium Grade V (left) used for one-piece restoration directly connected to the fixture. GFA (right) screwed to the implants and used for two-pieces restoration connected to the GFA abutment.

Figure 10.
Screw-retained fixed prosthesis secured to the implant (BL - Control Group) into position: occlusal view.
Figure 10.
Screw-retained fixed prosthesis secured to the implant (BL - Control Group) into position: occlusal view.

Figure 11.
Screw-retained fixed prosthesis secured to the GFA (SC - Test Group) into position: occlusal view.
Figure 11.
Screw-retained fixed prosthesis secured to the GFA (SC - Test Group) into position: occlusal view.

Figure 12.
Example of Marginal Bone Level (MBL), Marginal Bone Modification (MBM), Bone Loss (BL) and, Bone Remodeling (BR) in bone level and sub-crestal implants.
Figure 12.
Example of Marginal Bone Level (MBL), Marginal Bone Modification (MBM), Bone Loss (BL) and, Bone Remodeling (BR) in bone level and sub-crestal implants.
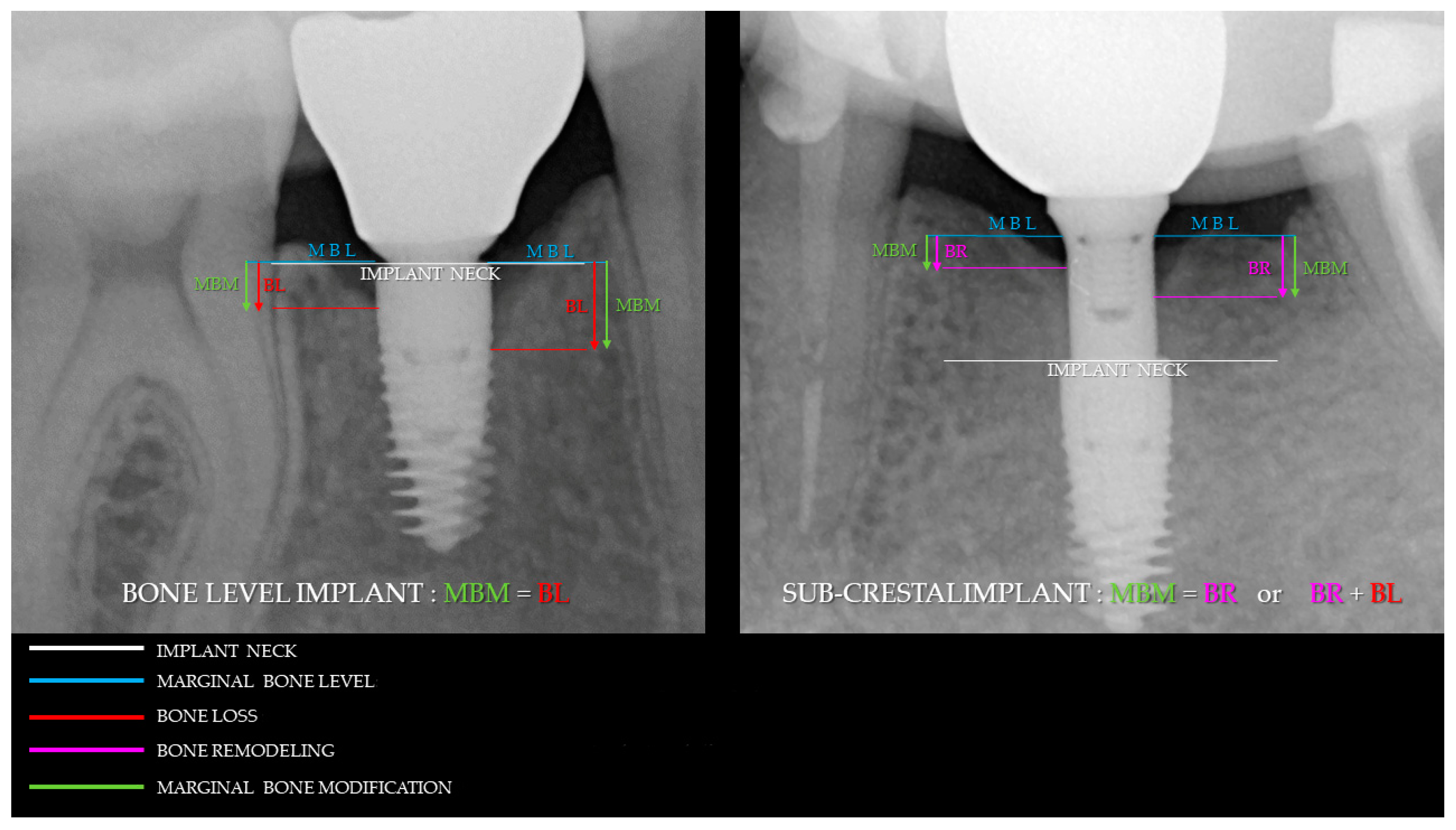
Figure 13.
Radiographic control at (T0), (T1), (T2) (T3) months, respectively. Control (BL) Group.
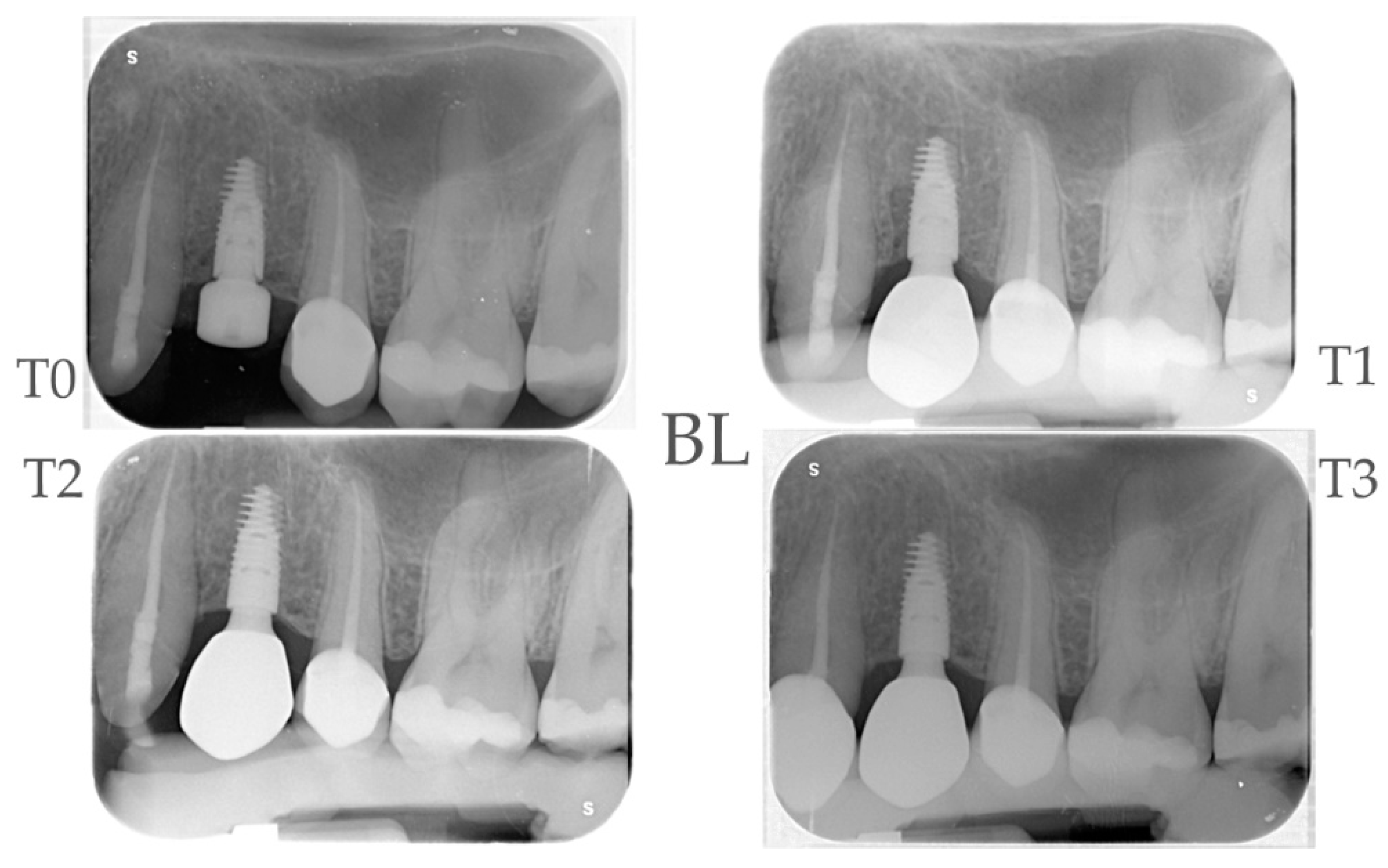
Figure 14.
Radiographic control at (T0), (T1), (T2) (T3) months, respectively. Test (SC) Group.
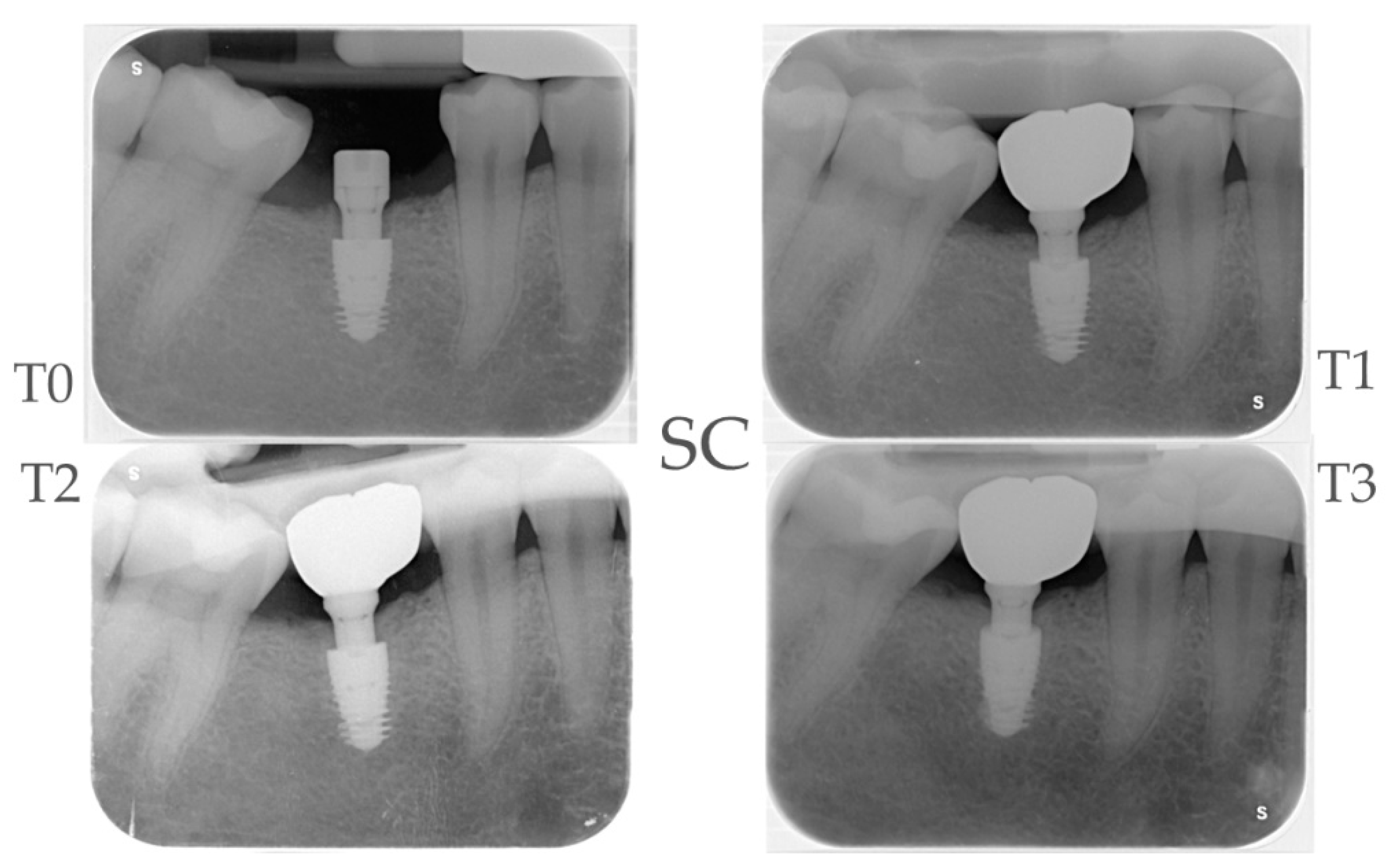
Figure 15.
Calibrated probe used to assess peri-implant soft tissues parameters.


Table 1.
Patient demographic characteristics (* - Subcrestal Implants, ** - Bone Level Implants).
| Demographic characteristics |
Total N (%) |
Control Group BL N (%)** |
Test Group SC N (%)* |
|---|---|---|---|
| Subjects enrolled | 38 (100%) | 19 (50%) | 19 (50%) |
| Drop Out | 2 (5,3%) | 1 (50%) | 1 (50%) |
| Age (mean) | 49,4 (23-72) | 47,3 (23-69) | 51,5 (33-72) |
| Sex | F: 22 (62%) M: 14 (38,9%) |
F: 13 (72,2%) M: 5 (27,8%) |
F: 9 (50%) M: 9 (50%) |
| Smokers | 6 (16,7%) | 4 ( 22,2%) | 2 (11,1%) |
* Subcrestal Implant. ** Bone Level Implant.
Table 2.
Implant site clinical features.
| Sites | Total N (%) |
Control Group BL N (%)** |
Test Group SC N (%)* |
|---|---|---|---|
| Dental arch | Upper: 12 (33,3%) Lower: 24 (66,7%) |
Upper: 7 (38,9%) Lower: 11 (61%) |
Upper: 5 (33,3%) Lower: 13 (66,7%) |
| Site | Premolar: 15 (41,7%) Molar: 21 (53,8%) |
Premolar: 9 (50%) Molar: 9 (50%) |
Premolar: 15 (41,7%) Molar: 21 (53,8%) |
| STH§ (mm) | 1: 0 (0%) 2: 12 (33,3%) 3: 21 (58,4%) 4: 3 (8,3%) |
1: 0 (0%) 2: 4 (22,2%) 3: 13 (72,2%) 4: 1 (5,6%)) |
1: 0 (0%) 2: 8 (44,4%) 3: 8 (44,4%) 4: 2 (11,2%) |
| Implant (Diametre x Length) |
3,6x 9: 23 (63,9%) 4,3x 7,5: 13 (36,1%) |
3,6x 9: 15 (83,3%) 4,3x 7,5: 3 (16,7%) |
3,6x 9: 8 (44,4%) 4,3x 7,5: 10 (55,6%) |
| Bone Density (Misch Classification) |
D1: 0 (0%) D2: 4 (11%) D3: 25 (69,4%) D4: 7 (19,4%) |
D1: 0 (0%) D2: 3 (16,7%) D3: 14 (77,8%) D4: 1 (5,6%) |
D1: 0 (0%) D2: 1 (5,6%) D3: 11 (61,1%) D4: 6 (33,3%) |
| Healing Abutment (mm) Control Group |
3,5: 6 (33,3%) 4,5: 12 (66,7%) |
||
| GFA§§ (mm) Test Group |
3,5: 7 (38,9%) 4,5: 9 (50%) 5,5 2 (11,1%) |
* Subcrestal Implant. ** Bone Level Implant. § Negative values referred to apical MBM.
Table 3.
Marginal Bone Modification (MBM), Bone Loss (BL) and Bone Remodeling at different time intervals.
Table 3.
Marginal Bone Modification (MBM), Bone Loss (BL) and Bone Remodeling at different time intervals.
| Time Points | MBM Control Group Δ (CI 95%)** |
P-value | Bone Loss Control Group Δ (CI 95%)** | MBM Test Group Δ (CI 95%)* |
P-value | Bone Loss Test Group Δ (CI 95%)** | MBM Test VS Control Δ (CI 95%) |
P-value |
|---|---|---|---|---|---|---|---|---|
| T1 – T0 | -0.44 (-0.67; -0.21) |
<0.01 | -0.44 (-0.67; -0.21) |
-0.65 (-0.89; -0.42) |
<0.01 | 0 | -0.21 (-0.54; 0.11) |
0.195 |
| T2 – T0 | -0.49 (-0.72; -0.26) |
<0.01 | -0.49 (-0.72; -0.26) |
-0.72 (-0.95; -0.49) |
<0.01 | 0 | -0,23 (-0,55; 0,10) |
0.168 |
| T3 – T0 | -0.52 (-0.75; -0.29) |
<0.01 | -0.52 (-0.75; -0.29) |
-0.60 (-0.83; -0.36) |
<0.01 | 0 | -0.07 (-0.40; 0.25) |
0.657 |
* Subcrestal Implant. ** Bone Level Implant. § Negative values referred to apical MBM.
Table 4.
Clinical perimplant parameters modification at different times intervals.
| Clinical Parameter |
Control Group** | Test Group* | TEST VS Control | |||||
|---|---|---|---|---|---|---|---|---|
| 6 months | 1 year | 1 year VS 6 months |
6 months | 1 year | 1 year VS 6 months |
6 months | 1 year | |
| PPD (mm) (CI 95%) |
3.18 (2.76; 3.60) |
3.04 (2.64; 3.45) |
0.04 (-0.72; 0.45) p=0.641 |
2.33 (2.03; 2.63) |
2.38 (2.13; 2.62) |
0.04 (-0.35; 0.43) p=0.834 |
-0.85 (-1.36; -0.33) p=0.001 |
-0.67 (-1.14; -0.19) p=0.006 |
| BOP (%) (CI 95%) |
55.56 (43.90; 70.31) |
43.06 (33.54; 55.27) |
0.78 (0.56; 1.08) [p=0.134] |
36.11 (24.51; 53.21) |
50.00 (36.40; 68.68) |
1.38 (0.86; 2.23) [p=0.180] |
0.65 (0.41; 1.02) [p=0.0627] |
1.16 (0.78; 1.74) [p=0.4681] |
| PI(%) (CI 95%) |
12.50 (4.90; 31.89) |
19.44 ( 10.54; 35.86) |
1.56 (0.49; 4.89) [p=0.44979] |
11.11 (5.03; 24.53) |
33.33 (21.00; 52.91) |
3.00 (1.33; 6.79) [p=0.00837] |
0.89 (0.26; 3.03) [p=0.851] |
1.71 (0.80; 3.69) [p=0.168] |
* Subcrestal Implant. ** Bone Level Implant. § p = p.value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



