
Submitted:
28 February 2024
Posted:
28 February 2024
You are already at the latest version
Abstract
Introduction: The repertoire of microRNAs (miRNAs) in thyroid carcinomas starts to be elucidated. Among differentiated thyroid carcinomas (DTC), papillary thyroid carcinoma (PTC) is the most common. The assessment of miRNAs expression may contribute to refine the pre-surgical diagnosis, in order to obtain a personalized and more effective treatment of patients.
Aims: This study aims to evaluated 1) miRNAs expression in a series of DTC, and the association with the presence of selected genetic mutations, in order to improve diagnosis and predict biologic behavior of DTC/PTC. 2) the reliability of molecular tests in Ultrasound-guided Fine Needle Aspiration Cytology (US-FNAC) for a more precise preoperative diagnosis.
Material and methods: This series includes 176 samples (98 cytology samples and 78 formalin-fixed paraffin embedded (FFPE) tissues) obtained from 106 patients submitted to surgery, being 13 benign lesions (controls) and 93 DTCs (cases). The microRNA expression was assessed for miR-146b, miR-221, miR-222, and miR-15a by quantitative reverse transcriptase-polymerase chain reaction (qRT-PCR) and the results were analyzed using the 2- ΔΔCT method, using miR16 as an endogenous control. The discriminative ability of miRNAs expression regarding PTC diagnosis was evaluated using the area under the Receiver Operating Characteristic Curve (AUC). The association of miRNAs expression, clinicopatological features and genetic alterations (BRAF, RAS and TERTp) was evaluated in PTCs.
Results/Discussion: All the analyzed miRNAs showed a tendency to be over expressed in DTCs/PTCs when compared with benign lesions, both in cytology and histology samples. In cytology, miRNAs expression levels were higher in malignant than in benign tumors. In histology, corresponding discriminative abilities regarding PTC diagnosis were: miR-146b (AUC0.94, 95%CI 0.87-1), miR-221 (AUC0.79, 95%CI 0.68-0.9), miR-222 (AUC0.76, 95%CI 0.63-0.89) and miR-15a (AUC0.85, 95%CI 0.74-0.97). miR-146b showed 89% sensitivity (se) and 87% specificity (sp); mi-R221 se=68.4, sp=90; miR222 se=73, sp=70, and mi-R15a se=72, sp=80. MicroRNAs were associated with aggressive clinicopathological features and tumor progression in PTCs (p < 0.05), particularly for miR-222. Our data reveals a significant association between higher expression levels of miR-146b, miR-221 and miR-222, with the presence of BRAF mutation (p<0.001), and miR-146b (p=0.016) and miR-221 (p=0.010) with the presence of RAS mutation, suggesting an interplay of these mutations with miRNAs expression. Although this study has a relatively small sample size, over expression of miRNAs in cytology may contribute to a more precise preoperative diagnosis. The miRNAs showed a good discriminative ability in PTC diagnosis. The association between the miRNAs expression profile and genetic alterations results could be useful for an accurate diagnosis of DTCs/PTCs in FNAC.
Keywords:
microRNAs
; miR-146b
; miR-221
; miR-222
; miR-15a
; differentiated thyroid carcinoma
; papillary thyroid carcinoma
; genetic mutations
; TERTp
; BRAF
; RAS
1. Introduction
The incidence of DTC, with over 95% of them diagnosed as papillary thyroid carcinoma (PTC) [1,2], has increased in the last years, mainly attributed to enhanced sensitivity of complementary diagnostic techniques and the influence of environmental factors, but not accompanied by a corresponding change in mortality rate [3,4]. Despite the favorable prognosis of PTCs, it was advanced that some clinicopathological features and the presence of some genetic alterations can influence their progression [5]. An accurate diagnosis in a pre-surgical phase is crucial to optimize medical or surgical treatment, and to avoid unnecessary surgeries and complications [6].
Ultrasound-guided fine needle aspiration cytology (US-FNAC) is the gold standard method in the diagnosis of nodular thyroid disease, but up to 30% of nodules remain without a definitive diagnosis [7]. Bethesda II and VI cytological results have excellent performance to assess the benign or malignant nature of a thyroid nodule, respectively. Diagnostic limitations are particularly significant in indeterminate Bethesda categories: III – atypia of undeterminate significance (AUS), and IV – follicular neoplasm. Each category harbors a different risk of malignancy (ROM) and a different option for treatment and follow-up [8,9].
Although the American and European Thyroid Association [10,11] consider the inclusion of molecular tests in US-FNAC, no consensus is yet achieved on the best molecular biomarkers panel to use in pre-surgical diagnosis and prognosis of thyroid cancer [12,13].
A promising area of study in thyroid cancer (TC) is the assessment of microRNAs (miRNAs) expression and its contribution for diagnosis and prognosis of thyroid nodules [14,15,16]. They are stable molecules that can be detected in cytology and histology samples [17,18], in small amounts of fresh or stored material, and can also be studied in the blood [19,20].
MiRNAs are an important class and numerous, of small (with a length of approximately 22 nucleotides) non-coding RNAs. MiRNAs are supposed to modulate 30% of the human genome and play an important role as global regulators of gene expression [21,22]. They have a key role in posttranscriptional gene expression, by reducing the stability of the target messenger RNA (mRNA) and/or repressing its translation. These events may have influence in intracellular regulatory processes implicated in carcinogenesis, including differentiation, proliferation, and apoptosis [23,24].
Studies of the miRNA expression profile in human tumors allowed the identification of specific "signatures" associated with diagnosis, staging, prognosis, and response to treatment [25,26]. Unraveling their potential poses a substantial scientific challenge, underscoring the depth and importance of this tool.
When TC grows due to the action of oncogenes, a series of alterations on miRNAs biogenesis is revealed. Altered expression of miRNAs occurs, contributing to a constitutive activation of MAPK pathway [27]. MiRNAs can act as tumor promoters (oncomiRs) which downregulates tumor suppressor genes or act as tumor suppressors leading to upregulation of oncogenes with consequences in tumor progression and growth [28].
In 2008 Nikiforova et al. [29] described the biological importance and diagnostic value of miRNAs analysis in thyroid tumors, estimating that in thyroid tumors 32% of miRNAs are upregulated while 38% are downregulated. When compared with thyroid normal tissue, specific up and downregulated miRNAs arose as involved in the progression of PTC such as miR-146b, miR-221, miR-222 (upregulated) and miR-15a (downregulated) (29). The miRNA expression is tissue specific, varying among the different types of TC. Upregulated miR-146b, miR-221 and miR-222, are shown to downregulate proto-oncogene receptor tyrosine kinase (KIT), which is involved in cell differentiation and growth, while miR-15a downregulates B-cell lymphoma 2 (BCL-2) and controls the proliferation and apoptosis of PTC through AKT pathway [29].
Castagna, et al. [30] have shown, in a series of fine-needle aspiration samples, that miR-146b, miR-221 and miR-222 are overexpressed in malignant or suspicious for malignancy nodules confirming the utility of these miRNAs in the classification of thyroid nodules. The overexpression of these miRNA was correlated with tumor aggressiveness, extra thyroidal extension, recurrence and metastases, representing a signature of PTC [31]. Therefore, the study of miRNA expression can be useful in the early and accurate diagnosis, as well as in the evaluation of biological behavior of PTC [32,33,34].
Although the identification of miRNAs expression profiles in thyroid cancer is being revealed, more studies are needed to establish its diagnostic, prognostic and predictive role in clinical practice. The identification of miRNAs and their target genes can allows us to envisage new and more personalized therapies [35,36].
This study aims to evaluate the expression of selected miRNAs (miR146b, miR221, miR222 and miR15a) in thyroid nodules, their association with the presence of clinicopathologic features and genetic alterations (TERTp, BRAF and RAS mutations). As an ultimate goal we want to evaluate the reliability of molecular tests on US-FNAC as a pre-surgical diagnostic tool in the improvement of DTC diagnosis.
2. Materials and Methods
2.1. Study Design
This retrospective study was conducted in a series of patients with thyroid nodular disease suspicious of malignancy, which underwent surgery, in a single non-oncologic hospital, between 2013 and 2020. Criteria for suspicion of malignancy in thyroid nodules were based in clinical evaluation, image features and Bethesda classification for cytology [7], in accordance with 2015 ATA [10] and 2017 ETA guidelines [37]. Surgical protocols and recommendations for the extent of surgical treatment followed the same guidelines [10,37]. A series of 13 histological benign lesions were also included for comparative purposes.
Study inclusion criteria: patients diagnosed, after surgery, with differentiated thyroid carcinoma (cases) or benign thyroid nodules (controls), of both genders, over 18 years old, with available representative histological and cytological samples.
Study exclusion criteria: patients with toxic goiter, papillary carcinoma smaller than 1 cm, and patients with other than thyroid neoplasm at the time of thyroid surgery.
This series includes 176 samples (98 cytology samples and 78 formalin-fixed paraffin embedded (FFPE) tissues) obtained from 106 patients-submitted to surgery. In 70 patients, paired cytology and histology samples were analyzed. Epidemiological and clinicopathological features of patients and tumors were gathered based on the information available in the clinical and histopathological reports from the reference hospital.
All the samples were reviewed by two independent pathologists based on the 4th edition of the World Health Organization (WHO) classification of tumors of endocrine organs [38].
2.2. MicroRNAs Expression Profile Analysis
2.2.1. MicroRNA Extraction from FFPE Tissues and FNAC Samples
The initial step is different for FFPE tissues and FNAC samples. For FFPE tissues, a slide with a 10 μm cut was deparaffinized and the tumor area was manually micro dissected. For FNAC samples, the entire smears were manually scraped. MicroRNA extraction was performed with the miRNeasy Mini kit (1038703 Qiagen, Germany) following the manufacturer’s instructions.
RNA concentration was determined using the NanoDrop (ND-1000, Thermo Fisher Scientific, Lithuania) spectrophotometer. RNA handling was always performed on ice.
2.2.2. Reverse Transcription and Quantitative Real Time PCR (RT-qPCR)
Complementary deoxyribonucleic acid (cDNA) synthesis was achieved with TaqMan® Advanced miRNA cDNA Synthesis Kit (refª A28007 Applied biosystems, USA) following the manufacturer’s instructions.
RT-qPCR was performed to evaluate the relative expression levels of miR-146b, miR-221, miR-222 and miR-15a (refª A25576, ThermoScientific, USA) [39]. MiR-16 (refªA25576, ThermoScientific, USA) was used as an endogenous control for normalization of the expression values [40]. The relative quantification of gene expression was attained using the 2-ΔΔCT method [41].
RT-qPCR was performed using TaqMan® Fast Advanced (refª 4444557, ThermoScientific, USA) system according to the manufacturer´s instruction on a QuantStudio 5 Real-Time PCR System (ThermoScientific, USA). Duplicates were done for all samples.
2.3. Genetic Analysis
2.3.1. DNA Extraction
Genomic DNA was extracted using the GRS Genomic DNA BroadRange Kit (refª GK06.0100 GRiSP Research Solutions, Portugal) or the QIAmp® DNA Investigator Kit (refª 56504 Qiagen, Germany), for FFPE and US-FNACs, respectively, according to the manufacturer’s instructions. NanoDropTM One UV185 Vis Spectrophotometer (Thermo Fisher Scientific Inc) was used for quantification of isolated DNA.
2.3.2. Mutational Screening
For genetic characterization of the lesions PCR (SimpliAmp TM Thermalcycler, Applied Biosystems, USA) and Sanger sequencing (Applied Biosystems 3130/3130XL Genetic Analyzer, USA) were used. Mutations in TERTp, BRAF and RAS (NRAS, HRAS and KRAS), were evaluate by PCR/sequencing with primers for the most frequent regions mutated on thyroid carcinoma, as previously described [42,43]. All detected mutations were validated by performing a new independent analysis.
2.4. Clinicopathological Features
Only PTCs were considered in the statistical analysis of the miRNAs expression and clinicopathological features of the nodules. The tumor’s clinicopathological features analyzed were: tumor size, extra thyroidal invasion, capsule invasion, vascular and lymphatic invasion, presence of fibrosis, inflammatory infiltrate, tall cell, oncocytic component, psammoma bodies, calcification, necrosis, and presence of lymph node metastases, focality, and laterality.
2.5. Statistical Analysis
An exploratory analysis was performed with categorical variables presented with frequencies (percentages), and quantitative variables with mean, and standard deviation (SD) or median, and percentiles (25-75) and/or range (minimum-maximum), as appropriate. Regarding quantitative variables, Student’s t and non-parametric Mann Whitney tests were used to compare groups, as appropriate. In the case of categorical variables, the Chi-square or Fisher’s exact tests were used, as required.
The discriminative ability of biomarkers regarding malignancy was performed by estimating sensitivity, specificity, positive and negative predictive values, with corresponding 95% confidence intervals. A level of significance α=0.05 was considered. Data analysis was performed using the SPSS software version 27.0 (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp).
3. Results
3.1. Series Description
3.1.1. Epidemiologic Data
From the 106 patients, 89 (84%) were female, with mean age at diagnosis of 52.2 (16.4) years (range 18-84), and 17 (16%) were male, with mean age of 55.2 (13.5) years (range 35-79). The distribution of age was the same across categories of gender (p =0.564), and across categories of histological diagnosis (p=0.503).
Mean tumor size was 33.1 mm (11.94) for benign lesions and 28.3 mm (14.76) for malignant lesions; the distribution of tumor size was the same across categories of histological diagnosis (p=0.152).
The histology samples were composed by 13 (12.3%) benign lesions, and 93 (87.7%) malignant lesions (DTC). PTC represented the larger group in malignant histology, with 81 (87.1%) cases.
Cytology samples were distributed according to the Bethesda classification, as follows: I. non diagnostic (ND), 3 samples (2.8%); II. benign (B), 23 samples (21.7%); III. atypia of undetermined significance (AUS), 23 samples (21.7%); IV. Follicular Neoplasm (FN), 29 samples (27.4%); V. suspicious for malignancy (SM), 14 samples (13.2%); VI. malignant 14 samples (13.2%).
The 49.1% (n=52) of nodules whose cytological result was indeterminate (Bethesda III and IV) corresponded in histology to one (1.9%) benign and to 51 malignant lesions (98.1%).
The distribution of cytology samples within histological subtypes in all series is presented in Table 1.
3.1.2. MiRNAS Profile in Cytology Samples
The miRNAs expression levels of miR-146b, miR-221, miR-222 and miR-15a in cytology samples by Bethesda categories is summarized in Supplementary Table S1. The levels of miRNAs expression observed across Bethesda categories exhibit elevated values, characterized by high median values, progressing from category I to category VI. Expressive variations in maximum values were noted among all miRNAs for each category, with the exception of miR-15a, which precludes statistically significant differences.
Indeterminate nodules (Bethesda III and IV) and nodules suspicious or malignancy (Bethesda V and VI) with higher miRNAs expression levels, proved to be malignant in histology, except in one benign case (Bethesda IV) as seen also in Table 1.
The miRNA expression levels of miR-146b, miR-221, miR-222 and miR-15a in cytology samples by histology diagnosis, in all series, is summarized in Figure 1. and Supplementary Table S2. The miRNAs profile observed in cytology samples showed a tendency to be overexpressed in malignant tumors when compared with benign lesions, with higher median for miRNAs 146b and 222 and wider amplitude of expression for all miRNAs in malignant tumors, although without statistical significance.
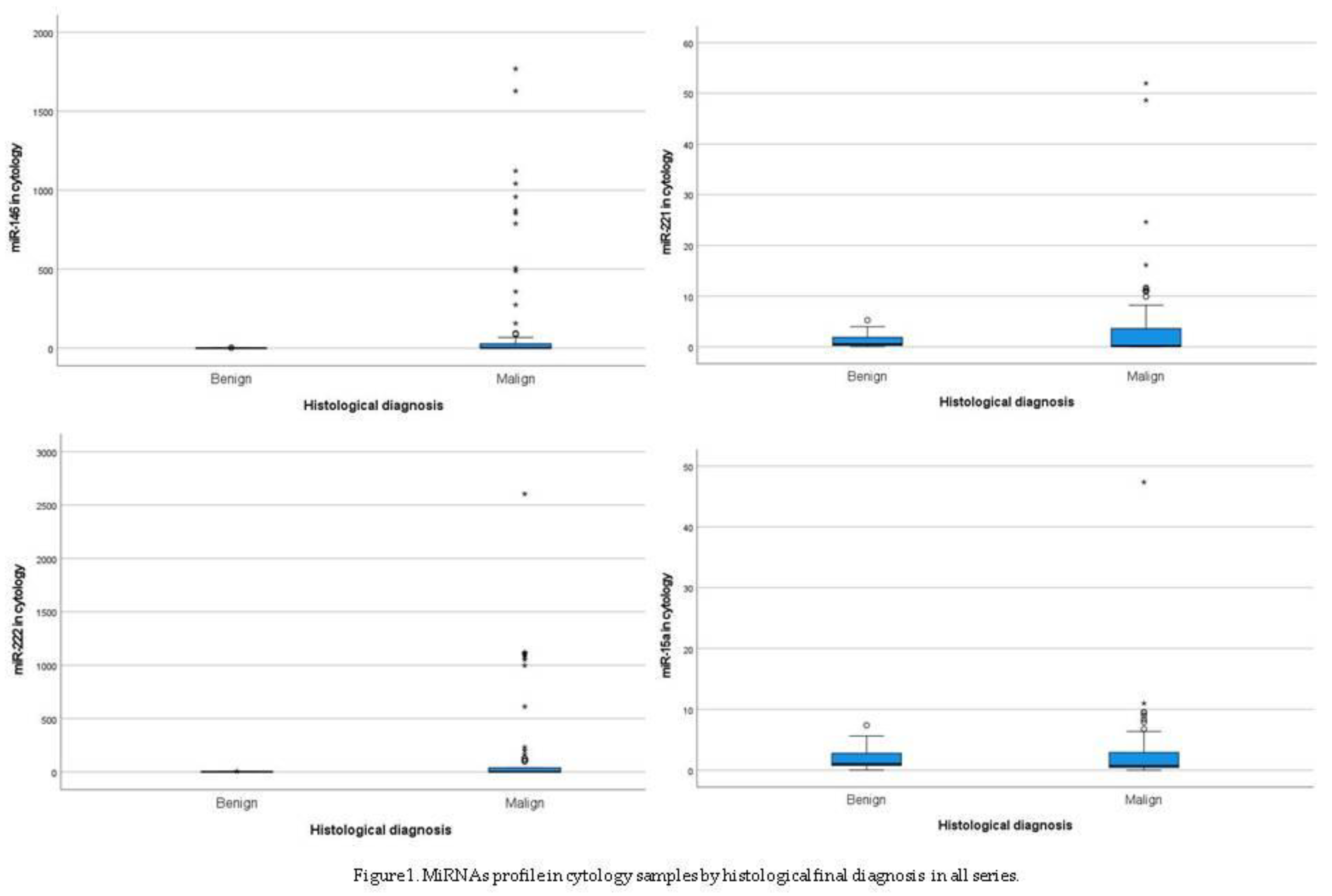
When we analyzed miRNA values obtained in cytology samples, according to the final diagnosis of malignancy, we noted that the malignant cases presented miRNA expression values above those obtained in benign cases. The number of malignant cases that presented (in the cytology sample) value of miRNAs expression above the maximum levels obtained for benign tumors, were 34.1% (n= 29) cases for miRNA-146b, 17.4% (n= 16) for miRNA-221, 35.4% (n=29) for miRNA-222, and 10.3% (n=9) for miRNA-15a, as showed in Table 2.
Malignant tumors presented, in cytology, higher values of miRNAs expression when compared with benign tumors. The five highest extreme values for miRNAs expression in cytology by histological diagnosis were shown in Supplementary Table S3.
3.1.3. MiRNAs Profile in Histology Samples
The miRNAs expression levels of miR-146b, miR-221, miR-222 and miR-15a in histology samples in all series is showed in Figure 2. and Table 3.
The miRNAs profile observed in histologies presented a statistical significant difference between benign and malignant tumors for all miRNAs (Table 3), showing higher median values and wider amplitude of expression in malignant tumors.
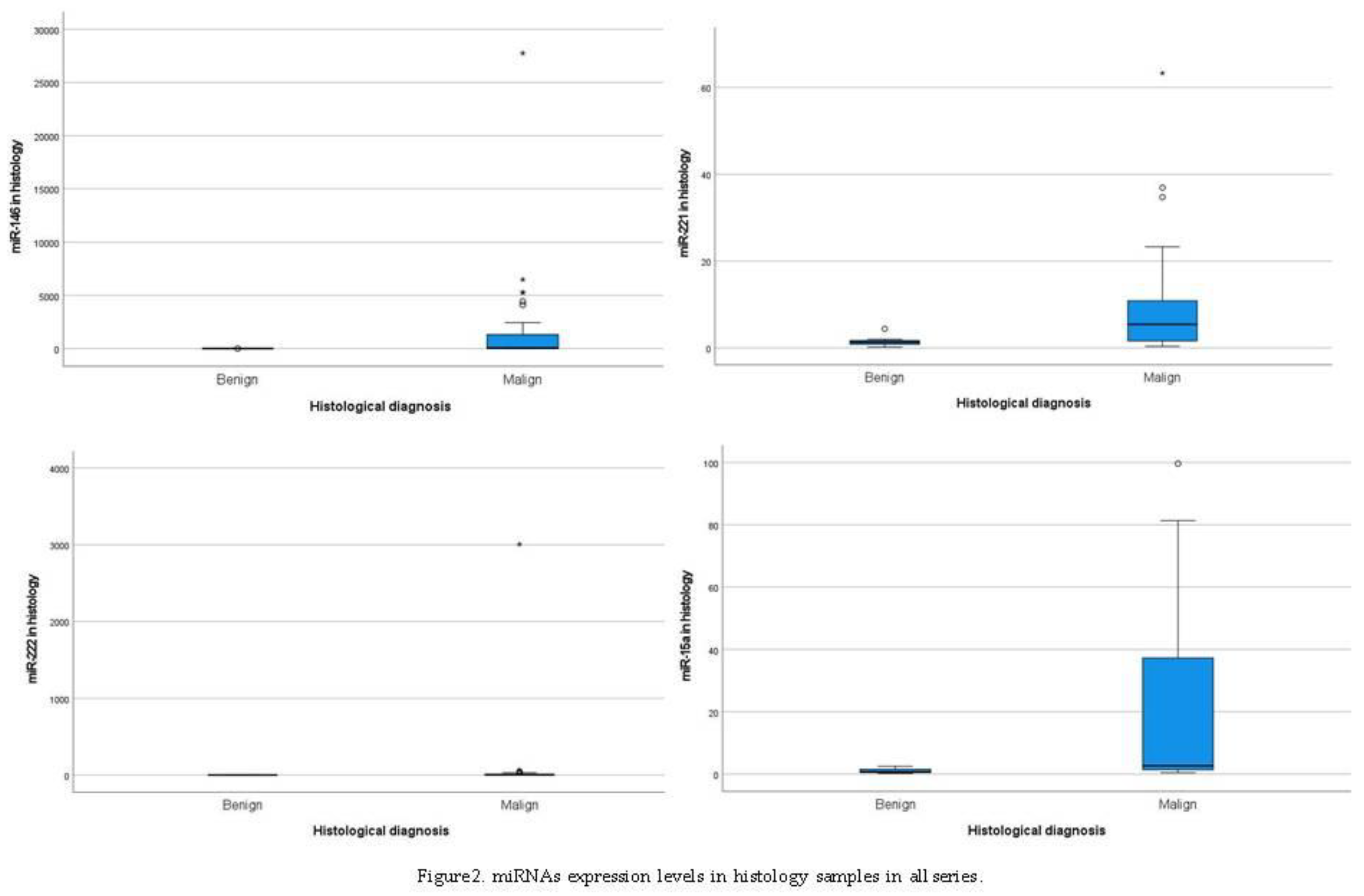
The miRNAs expression levels of miR-146b, miR-221, miR-222 and miR-15a in histology samples within histological subtypes is summarized in Supplementary Table S4.
Most histological subtypes of DTCs were PTCs (81/93), and presented higher median values and wider amplitude of expression for all miRNAs. Twelve cases were non-PTCs, from which two cases of HCC presented higher median values and wider amplitude of expression for miRNAs 221 and 222.
3.2. MiRNA Expression and Mutations in Cytology and Histology Samples in PTCs
For the analysis of the association between miRNAs expression levels and the presence of genetic mutations in cytology and histology samples, only PTCs were considered due to the limited number of the other subtypes of DTC.
In cytology samples, miRNAs profile revealed a higher median expression value in the presence of genetic mutations, as showed by miRNA-146b in the presence of TERTp and BRAF mutations, miRNA-221 and miRNA-222 associated with BRAF mutations, and miRNA-15a with TERTp and RAS mutations, although no statistically significant association was observed Supplementary Table S5.
In histology samples, miRNAs expression revealed a higher median value in the presence of almost all genetic mutations, and statistically significant associations between miRNAs expression levels and the presence of genetic mutations were obtained. MiRNA-146 and miRNA-221 expression levels were significantly associated with the presence of BRAF and RAS mutations, miRNA-222 with the presence of BRAF mutations, and miRNA-15a with the presence of TERTp and RAS mutations (Table 4).
3.3. MiRNA Expression and Clinicopatological Features in PTCs
The association between microRNAs expression and clinicopathological features of the tumors was evaluated in PTCs, being the results presented in Supplementary Table S6. A,B,C,D.
No statistically significant differences were achieved for gender or age. The distribution of tumor size was the same across microRNAs expression at diagnosis.
MiR-146b expression showed an association with capsular invasion, psammoma bodies (p=0.019) and calcification (p=0.010). Overexpressed miR-221 was associated with capsule invasion and vascular invasion (p< 0.001), oncocytic component (p=0.002) and calcification (p=0.031). miR-222 expression presented associations with the presence of extra thyroidal invasion, capsule invasion, vascular invasion, lymphatic invasion, oncocytic component, psammoma bodies, inflammatory infiltrate, tall cell component, calcification, and focality (p<0.05 for all parameters). miR-15a expression was significantly associated with capsular invasion and focality (p=0.41).
3.4. The Discriminative Ability of miRNAs in Histology for the Diagnosis of Malignancy
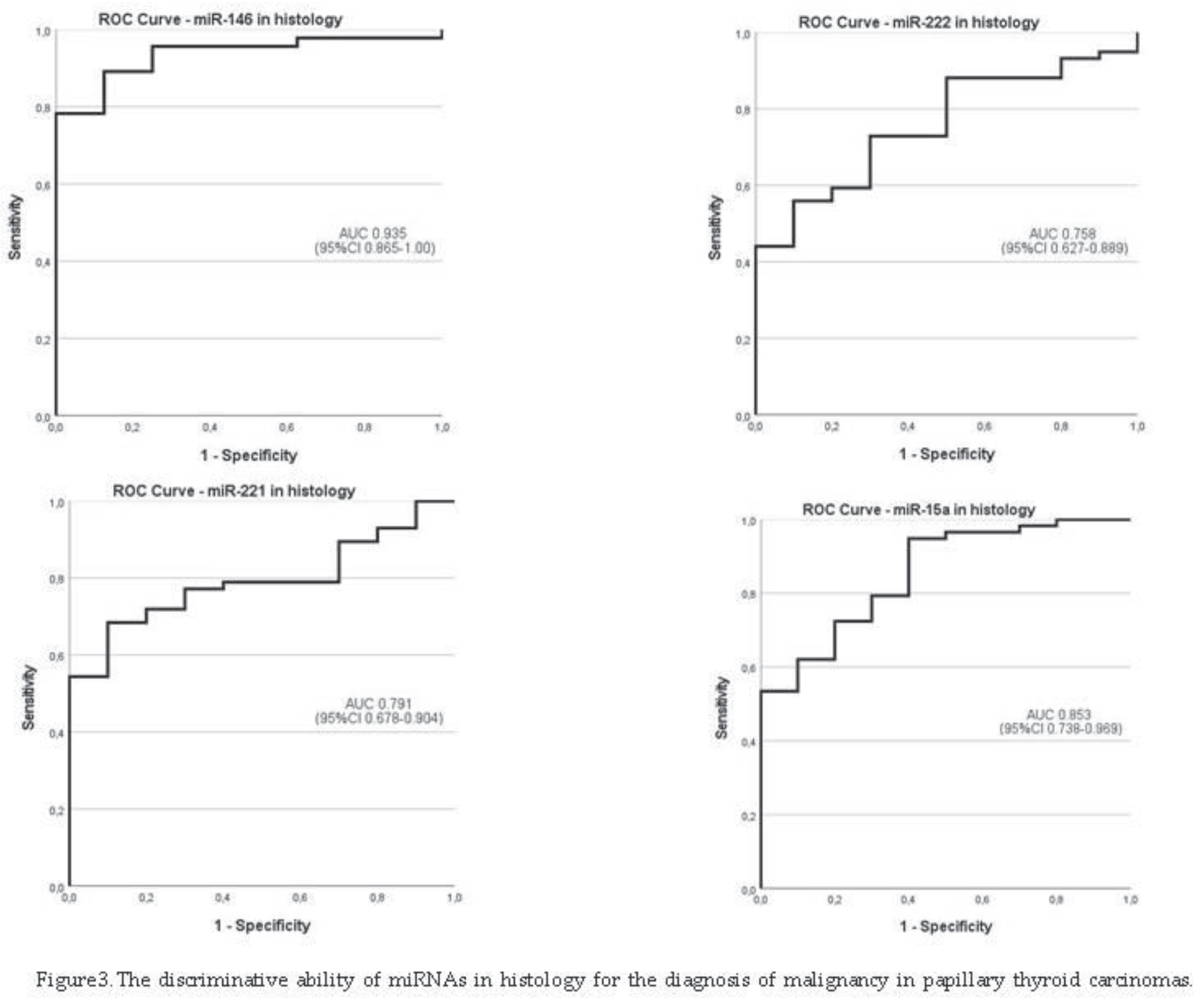
The discriminative ability of miRNAs profile for the diagnosis of malignancy in our series was analyzed only for PTCs, due to the limited number of the other malignant subtypes of DTC, as shown in Figure 3. and Table 5.
Area under the curve (AUC) for all miRNAs showed acceptable to exceptional discriminative ability regarding histological diagnosis, with estimates from 75.8% (95%CI: 62.7-88.9) for miR-222 to 93.5% (95%CI: 86.5-100) for miR-146b.
Regarding PTCs diagnosis and considering the cutoff values obtained by maximizing sensitivity and specificity, all miRNAs exhibited sensitivity (se) and specificity (sp) over 70%, with higher estimates for miR-146b (89.1% se and 87.5% sp). The positive predictive value (PPV) was over 93.5 % for all miRNAs, and attained a maximum of 97.6% for miR-146b.
The statistical analysis of combined miRNAs did not improve the discriminative ability of miRNAs for PTC diagnosis in our study. The analysis of miRNAs expression in 70 paired cyto-histology samples did not showed statistical significances.
4. Discussion
The expression of miRNAs is deregulated in many types of human cancers, including thyroid cancer, leading to alterations of different cellular processes, namely in cell differentiation, proliferation, migration and invasion [26]. Allied to genetic alterations, microRNAs have been described as new biomarkers in TC and are pointed as possible therapeutic targets [43,44,45].
In 2022, the 5th WHO classification of thyroid neoplasms [46] and in 2023, the 3rd Bethesda Classification [8], included genetic and molecular biomarkers for pre-surgical diagnosis to refine the diagnostic categories and their risk of malignancy. However, in addition to the lack of consensus on which panels of molecular biomarkers to use, their implementation in clinical practice is not yet possible in the vast majority of countries worldwide for technique and economic reasons.
This study aimed to determinate the expression levels of four microRNAs in cytology via US-FNAC, and in histology samples of patients with thyroid nodular disease that underwent surgery, based in clinical evaluation, imageology features and cytological criteria for suspicion of malignancy. We selected three miRNAs previously described as upregulated in TC (miR-146b, miR-221 and miR-222), and one categorized as downregulated (miR-15a), for expression profile analyses [47].
We observed a broad spectrum of variation in miRNAs expression levels, evident in both cytology and histology analyses. The study reveals a significant overexpression for miRNAs in malignant tumors when compared with benign lesions, in histology samples. Alterations of these specific miRNAs in TC have been already described in the literature, being associated with thyroid cell transformation [31,48].
In cytology samples, miRNAs showed a consistent trend for overexpression in malignant tumors compared with benign lesions, displaying higher median values across Bethesda categories I to VI. Notably, there were considerable differences in maximum values within each Bethesda category for all miRNAs, except miR-15a, despite no statistical significance have been achieved. In histology samples, all four miRNAs were overexpressed with a statistical significance between malignant tumors and benign lesions. The microRNA expression profile in cytology and in histology presented different levels with high amplitudes, which can reflect tumor heterogeneity, multifocality and/or low cellular representativity, particularly marked on cytology samples, with a lower percentage of cells (neoplastic) causing an increase of false negative results.
When we considered the values of miRNAs expression in cytology for malignant tumors under maximum levels for benign tumors (Table 2), the cytological information taken together with clinical evaluation, and imageology, could improved the diagnosis in one third of cases for miRNAs 146b and 222, almost 20% for miR-221, and even 10% for miR-15a. Those nodules could be diagnosed as malignant in a pre-surgical phase, without performing more FNACs and allowing better surgical options and health cost reduction.
In indeterminate nodules, miRNAs showed a tendency for overexpression in cytology, and with statistical significance in histology, reflecting their malignity in our series. Indeterminate nodules represented a high number of malignant cases in our series, because case selection was done based in a histology diagnosis of malignancy (or benignity in the 13 control cases), and these patients underwent surgery due to clinical reasons besides FNACs results (e.g. US features).
We found a tendency for upregulation in miR-146b, in cytology and statistically significant in histology, being in line with other studies [49,50]. MiR-146b is described to target SMADA and IRAK1, causing downregulation and increasing cells proliferation and migration in PTCs. [51].
The expression levels of miR-221 and miR-222 in cytology were higher in malignant tumors than in benign lesions, and reached statistical significance in histology, in accordance with Visone R. et al. [53]. Both miR-221 and miR-222 are described to target CDKN1B (p27Kip1 protein) and KIT. CDKN1B is an important regulator of the cell cycle, and KIT is involved in cell differentiation and growth. The overexpression of miR-221 and miR-222 induced the papillary thyroid carcinoma cell line (TPC-1) to progress into the S phase of the cell cycle. Moreover, miR-221 and miR-222 also play a role in vivo since there is an inverse correlation between their expression levels and down regulation of p27Kip1. On the contrary, the inhibition of miR-221 and miR-222 expression increases p27Kip1 protein levels. These results support the influence of these miRNAs in the control of the cell cycle through the regulation of the p27Kip1 protein levels.
The miR-15a has been described as downregulated in thyroid cancer. However, in our series, we observed an upregulation, suggesting a gain of function of this specific miRNA in PTCs. Jin J et al. [25] have reported an association between miR-15a low expression levels and human PTCs suggesting a possible influence of this miRNA in TC development by promoting proliferation, survival, and invasion. However, Lu Z et al. [35], showed that the upregulation of miR15a suppresses BCL-2 expression. In an in vivo study, it was found inhibition of cell proliferation and invasion, promoting apoptosis, when miR15a was upregulated, concluding that the overexpression of miR-15a inhibit tumor progression via regulation of AKT pathway. These discrepant results indicate that further studies are necessary to establish the role of miR-15a in thyroid cancer.
Several statistically significant associations between clinicopathological and molecular features of the PTCs were already described for BRAF mutations [54] and TERTp mutations [55], both associated with features of worse prognosis, whereas RAS mutations associated with benign or low-risk tumors [56,57]. Our data revealed a significant association between the expression levels of miR-146b, miR-221 and miR-222 and the presence of BRAF mutations in PTCs. Our findings are in accordance with Yang S. I. et al. [58] showing that the expression of miR-146b was significantly associated with the presence of BRAF mutations. Sun Y. et al. [59] showed that miR-146b, miR-221 and miR-222 together with miR-181 were upregulated in PTCs patients with BRAF mutations. These findings suggest a connection or influence of the presence of BRAF mutations with miRNAs expression in the development of TC. Our results showed a significant association between the expression levels of miR-146b, miR-221and miR15a, and the presence of RAS mutations in PTCs. The presence of RAS mutations confirms a neoplastic process but does not differentiate between benign, malignant, and low-risk neoplasm, whose analysis was beyond the scope of our study, as done by others [60]. Curiously, only miR-15a was significant associated with the presence of TERTp mutations in PTCs, suggesting that TERTp mutated PTCs can have a different repertoire of microRNA expression.
The (over)expression of the four microRNAs was significantly associated with several clinicopatological features in PTCs, namely for capsular invasion, vascular and lymphatic invasion, which were related with and an aggressive tumor behavior in accordance with others [30,34]. For example, upregulation of miR-146b was previously associated with tumor aggressiveness and poor clinicopathological features, such as extra thyroidal and capsule invasion, presence of lymph nodes or distant metastasis [52].
Our miRNAs expression analysis presents some limitations, namely the retrospective nature of the study and the small size of the series, both in cytology (lower representatives neoplastic cells), and in histology, due to the small number of non-PTCs subtypes. Both mentioned limitations plus the great variability of miRNAs expression level in cytology and histology, did not allowed the comparison in paired cyto-histological cases. Another limitation was the bias in the selection of indeterminate nodules in our series, making their study unfeasible, as done by others [61]. However, our results suggest that cytologies with overexpression levels of miRNAs have a higher risk to be malignant lesions, and miRNA evaluation may contribute to a pre-surgical diagnosis, changing the clinical and therapeutic decision.
Our results of miRNA expression profile in thyroid nodules reinforce the potential clinical utility of molecular testing in cytological assessments by US-FNAC, contributing to anticipate a diagnosis of malignancy and to predict tumor behavior. By integrating molecular information, clinicians achieve better informed decisions, and optimize treatment strategies.
5. Conclusions
Our results confirm that in TC there is a dysregulation of the expression levels of miRNAs, potentially influencing their target genes on the promotion of cell differentiation, proliferation and survival. While the miRNA profile´s ability to exclude malignancy is limited, we may suspect for malignancy in cytology samples with high expression levels of miRNAs, contributing to reduce repeated US-FNAC, and to a optimize the pre-surgical diagnosis . Moreover, the associations identified between miRNAs expression and clinicopathological features, in one hand, and genetic profile of PTCs, in the other hand, suggest that molecular analysis in US-FNAC can provide early insights into tumor genetic profile and behavior.
Current results suggest that US-FNAC molecular analysis will be useful in the early and accurate diagnosis of DTCs and, therefore, is likely to contribute to a more efficient treatment of TC. Yet, confirmation is pending from the analysis of a larger series.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
ML.M. and P.S. conceived the study and wrote the paper. M.P. and A.G. performed experiments and analyzed the data. S.C. reviewed the cytology and histology samples. ML.M, M.A. and AL.P. performed statistical analyses. AL.P, MJ.B, and P.S. supervised the work, regarding the conception, analyses, and review of the paper. All authors have read and agreed to the published version of the manuscript.
Funding
This research received funding for SC, in the framework of a Ph.D. grant (SFRH/BD/147650/2019) supported by Portuguese funds through Fundação para a Ciência e a Tecnologia (FCT). This study is part of the project “Institute for Research and Innovation in Health Sciences” (UID/BIM/04293/2019) and the project “The Porto Comprehensive Cancer Center” ref. NORTE-01-0145-FEDER-072678—Consórcio PORTO.CCC—Porto. Comprehensive Cancer Center Raquel Seruca.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Centro Hospitalar Universitário Lisboa Central (CES586, 19 July 2018) and Nova Medical School (nº 58/2018/CEFCM, 5 September 2018) and adheres to national and institutional ethical standards (Law n°12/2005).
Informed Consent Statement
Written informed consent has been obtained from each patient involved in the study, after full explanation of the purpose and nature of all procedures used, whenever possible, and we guaranteed data confidentiality and patient privacy through data anonymization.
Data Availability Statement
Data are contained within the article and Supplementary Materials.
Acknowledgments
The authors thank Isabel Dinis from the Department of Pathology, and Paula Tavares and José Coutinho from the Department of Surgery, Hospital de Curry Cabral, Unidade Local de Saúde São José, for their collaboration in this study.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Schlumberger, M.; Pacini, F.; Tuttle, R.M. Thyroid Tumors, 4th ed.; Institut Médico-Educatif: Paris, France, 2015. [Google Scholar]
- Grussendorf, M.; Ruschenburg, I.; Brabant, G. Malignancy rates in thyroid nodules: A long-term cohort study of 17,592 patients. Eur. Thyroid J. 2022, 11, e220027. [Google Scholar] [CrossRef]
- Li, M.; Brito, J.P.; Vaccarella, S. Long-Term Declines of Thyroid Cancer Mortality: An International Age-Period-Cohort Analysis. Thyroid 2020, 30, 838–846. [Google Scholar] [CrossRef]
- Miranda-Filho, A.; Lortet-Tieulent, J.; Bray, F.; Cao, B.; Franceschi, S.; Vaccarella, S.; Dal Maso, L. Thyroid Cancer Incidence Trends by Histology in 25 Countries: A Population-Based Study. Lancet Diabetes Endocrinol. 2021, 9, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Ren, H.; et al. Co-existence of BRAF (V600E) and TERT promoter mutations in papillary thyroid carcinoma is associated with tumor aggressiveness, but not with lymph node metastasis. Cancer Manag Res 2018, 10, 1005–1013. [Google Scholar] [CrossRef]
- Hlozek, J.; Pekova, B.; Rotnágl, J.; Holý, R.; Astl, J. Genetic Changes in Thyroid Cancers and the Importance of Their Preoperative Detection in Relation to the General Treatment and Determination of the Extent of Surgical Intervention—A Review. Biomedicines 2022, 10, 1515. [Google Scholar] [CrossRef]
- Ali, S.Z.; Cibas, E.S. The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria, and Explanatory Notes, 2nd ed.; Springer International Publishing: Cham, Switzerland, 2018. [Google Scholar]
- Syed Z Ali 1, Zubair W Baloch 2, Beatrix Cochand-Priollet 3, Fernando C Schmitt 4, Philippe Vielh 5, Paul A VanderLaan 6. The 2023 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2023, 33, 1039–1044. [CrossRef]
- Fulvio Basolo, Elisabetta Macerola, Anello Marcello Poma, and Liborio Torregrossa. The 5th edition of WHO classification of tumors of endocrine organs: changes in the diagnosis of follicular-derived thyroid carcinoma. Endocrine 2023, 80, 470–476. [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; et al. American Thyroid Association: Management Guidelines for Adult Patients with Thyroid Nodules and differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Cosimo Durante, Laszlo Hegedüs, Agnieszka Czarniecka, Ralf Paschke, Gilles Russ, Fernando Schmitt, Paula Soares, Tamas Solymosi, and Enrico Papini. 2023 European Thyroid Association Clinical Practice Guidelines for thyroid nodule management. Eur Thyroid J. 2023, 12, e230067. [CrossRef]
- Oczko-Wojciechowska, M.; Kotecka-Blicharz, A.; Krajewska, J.; Rusinek, D.; Barczynski, M.; Jarzab, B.; Czarniecka, A. European perspective on the use of molecular tests in the diagnosis and therapy of thyroid neoplasms. Gland. Surg. 2020, 9 (Suppl. S2), S69–S76. [Google Scholar] [CrossRef]
- Moore, A.; Bar, Y.; Maurice-Dror, C.; Finkel, I.; Goldvaser, H.; Dudnik, E.; Goldstein, D.A.; Gordon, N.; Billan, S.; Gutfeld, O.; et al. Next-generation sequencing in thyroid cancers: Do targetable alterations lead to a therapeutic advantage: A multicenter experience. Medicine 2021, 100, e26388. [Google Scholar] [CrossRef]
- Cristina Alina Silaghi 1, Vera Lozovanu 1, Carmen Emanuela Georgescu 1, Raluca Diana Georgescu 2, Sergiu Susman 3 4, Bogdana Adriana Năsui 5, Anca Dobrean 2 6, Horatiu Silaghi 7. Thyroseq v3, Afirma GSC, and microRNA Panels Versus Previous Molecular Tests in the Preoperative Diagnosis of Indeterminate Thyroid Nodules: A Systematic Review and Meta-Analysis. Front Endocrinol 2021, 12, 649522. [CrossRef]
- Sergei Titov 1 2, Pavel S Demenkov 3 4, Sergei A Lukyanov 5, Sergei V Sergiyko 5, Gevork A Katanyan 6, Yulia A Veryaskina 7 3, Mikhail K Ivanov 7 2 Preoperative detection of malignancy in fine-needle aspiration cytology (FNAC) smears with indeterminate cytology (Bethesda III, IV) by a combined molecular classifier. J Clin Pathol. 2020, 73, 722–727. [CrossRef]
- Shipra Agarwal 1, Andrey Bychkov 2, Chan-Kwon Jung 3 4. Emerging Biomarkers in Thyroid Practice and Research. Cancers 2021, 14, 204. [CrossRef] [PubMed] [PubMed Central]
- Marcos Tadeu Santos 1, Bruna Moretto Rodrigues 2, Satye Shizukuda 2, Andrei Félix Oliveira 2, Miriane Oliveira 2, David Livingstone Alves Figueiredo 3, Giulianno Molina Melo 4, Rubens Adão Silva 5, Claudio Fainstein 6, Gerson Felisbino Dos Reis 7, Rossana Corbo 8, Helton Estrela Ramos 9, Cléber Pinto Camacho 10, Fernanda Vaisman 11, Mário Vaisman 12. Clinical decision support analysis of a microRNA-based thyroid molecular classifier: A real-world, prospective and multicentre validation studies. EBioMedicine 2022, 82, 104137. [CrossRef]
- Lithwick-Yanai G1, Dromi N1, Shtabsky A2,3, Morgenstern S3,4, Strenov Y3,4, Feinmesser M3,4, Kravtsov V3,5, Leon ME6, Hajdúch M7, Ali SZ8, VandenBussche CJ8, Zhang X9,10, Leider-Trejo L2,3, Zubkov A2, Vorobyov S11, Kushnir M1, Goren Y1,12, Tabak S1, Kadosh E1, Benjamin H13, Schnitzer-Perlman T1, Marmor H1, Motin M1, Lebanony D1, Kredo-Russo S1, Mitchell H13, Noller M13, Smith A13, Dattner O13, Ashkenazi K13, Sanden M13, Berlin KA13, Bar D1, Meiri E1. Multicentre validation of a microRNA-based assay for diagnosing indeterminate thyroid nodules utilising fine needle aspirate smears. J Clin Pathol. 2017, 70, 500–507. [CrossRef]
- Yuping Chen 1, Bingtian Dong 2, Lichun Huang 1, Huibin Huang 1 Serum microRNAs as biomarkers for the diagnosis of papillary thyroid carcinoma: a meta-analysis. Bosn J Basic Med Sci. 2022, 22, 862–871. [CrossRef] [PubMed] [PubMed Central]
- Shi-Lin Xu 1, Yu-Yang Tian 2 3, Ying Zhou 3, Li-Qiao Liu 1 .Diagnostic value of circulating microRNAs in thyroid carcinoma: A systematic review and meta-analysis. Clin Endocrinol 2020, 93, 489–498. [CrossRef]
- Nikiforova MN1, Chiosea SI, Nikiforov YE. MicroRNA expression profiles in thyroid tumors. Endocr Pathol. 2009, 20, 85–91. [CrossRef]
- Wójcicka, A.; Kolanowska, M.; Jażdżewski, K. MECHANISMS IN ENDOCRINOLOGY: MicroRNA in diagnostics and therapy of thyroid cancer. Eur J Endocrinol. 2016, 174, R89–R98. [Google Scholar] [CrossRef]
- Ludvíková, M.; Kalfeřt, D.; Kholová, I. Pathobiology of MicroRNAs and Their Emerging Role in Thyroid Fine-Needle Aspiration. Acta Cytol. 2015, 59, 435–444. [Google Scholar] [CrossRef]
- Abdullah, M.I.; Junit, S.M.; Leong Ng, K.; Jayapalan, J.J.; Karikalan, B.; Hashim, O.H. Papillary Thyroid Cancer: Genetic Alterations and Molecular Biomarker Investigations. International Journal of Medical Sciences 2019, 16, 450–460. [Google Scholar] [CrossRef]
- Jin, J.; Zhang, J.; Xue, Y.; et al. miRNA-15a regulates the proliferation and apoptosis of papillary thyroid carcinoma via regulating AKT pathway. OncoTargets and Therapy 2019, 12, 6217–6226. [Google Scholar] [CrossRef]
- Marini, F.; Luzi, E.; Brandi, M.L. MicroRNA Role in Thyroid Cancer Development. Journal of Thyroid Research, 2011, 1-12. [CrossRef]
- Luzón-Toro, B.; Fernández, R.M.; Villalba-Benito, L.; et al. Influencers on Thyroid Cancer Onset: Molecular Genetic Basis. Genes 2019, 10, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Nikiforova, M.N.; Chiosea, S.I.; Nikiforov, Y.E. MicroRNA Expression Profiles in Thyroid Tumors. Endocr Pathol 2009, 20, 85–91. [Google Scholar] [CrossRef]
- Nikiforova, M.N.; Tseng, G.C.; Steward, D.; Diorio, D.; Nikiforov, Y.E. MicroRNA Expression Profiling of Thyroid Tumors: Biological Significance and Diagnostic Utility. J Clin Endocrinol Metab 2008, 93, 1600–1608. [Google Scholar] [CrossRef] [PubMed]
- Castagna, M.G.; Marzocchi, C.; Pilli, T.; et al. MicroRNA expression profile of thyroid nodules in fine-needle aspiration cytology: a confirmatory series. Journal of Endocrinological Investigation 2019, 42, 97–100. [Google Scholar] [CrossRef]
- Wei, Z.; Gao, AB.; Wang, Q.; et al. MicroRNA-221 promotes papillary thyroid carcinoma cell migration and invasion via targeting RECK and regulating epithelial–mesenchymal transition. OncoTargets and Therapy 2019, 12, 2323–2333. [Google Scholar] [CrossRef]
- Francesca Napoli 1, Ida Rapa 2, Umberto Mortara 3, Federica Massa 2, Stefania Izzo 2, Angelica Rigutto 1 4, Vanessa Zambelli 1, Claudio Bellevicine 5, Giancarlo Troncone 5, Mauro Papotti 1, Marco Volante 1. MicroRNA profiling predicts positive nodal status in papillary thyroid carcinoma in the preoperative setting. Cancer Cytopathol. 2022, 130, 695–704. [CrossRef]
- Jong-Lyul Park 1 2, Seon-Kyu Kim 2 3, Sora Jeon 4, Chan-Kwon Jung 4 5, Yong-Sung Kim 1,6. MicroRNA Profile for Diagnostic and Prognostic Biomarkers in Thyroid Cancer. Cancers 2021, 13, 632. [CrossRef]
- Viviana A Ruiz-Pozo 1, Santiago Cadena-Ullauri 1, Patricia Guevara-Ramírez 1, Elius Paz-Cruz 1, Rafael Tamayo-Trujillo 1, Ana Karina Zambrano 1 Differential microRNA expression for diagnosis and prognosis of papillary thyroid cancer. Review Front Med 2023, 10, 1139362. [CrossRef]
- Lu, Z.; Wu, Z.; Hu, J.; Wei, W.; Ma, B.; Wen, D. MicroRNA-15 regulates the proliferation, migration and invasion of thyroid cancer cells by targeting Bcl-2. JBUON 2019, 24, 2114–2119. [Google Scholar]
- Laetitia Lebrun, Isabelle Salmon. Pathology and new insights in thyroid neoplasms in the 2022 WHO classification. Review Curr Opin Oncol. 2024, 36, 13–21. [CrossRef]
- Paschke, R.; Cantara, S.; Crescenzi, A.; Jarzab, B.; Musholt, T.J.; Sobrinho Simões, M. European Thyroid Association Guidelines regarding Thyroid Nodule Molecular Fine-Needle Aspiration Cytology Diagnostics. Eur. Thyroid J. 2017, 6, 115–129. [Google Scholar] [CrossRef]
- Cameselle-Teijeiro, J.M.; Sobrinho-Simões, M. New WHO classification of thyroid tumors: a pragmatic categorization of thyroid gland neoplasms. Endocrinol Diabetes Nutr. 2018, 65, 133–135. [Google Scholar] [CrossRef]
- Wang, J.; et al. Identification of key miRNAs in papillary thyroid carcinoma based on data mining and bioinformatics methods. Biomed Rep 2020, 12, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; et al. Dynamic monitoring of circulating microRNAs as a predictive biomarker for the diagnosis and recurrence of papillary thyroid carcinoma. Oncol Lett 2017, 13, 4252–4266. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of Relative Gene Expression Data Using Real-Time Quantitative PCR and the 2-ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Melo, M.; da Rocha, A.G.; Batista, R.; Vinagre, J.; Martins, M.J.; Costa, G.; Ribeiro, C.; Carrilho, F.; Leite, V.; Lobo, C.; et al. TERT, BRAF, and NRAS in Primary Thyroid Cancer and Metastatic Disease. J Clin Endocrinol Metab. 2017, 102, 1898–1907. [Google Scholar] [CrossRef]
- Celano, M.; Rosignolo, F.; Maggisano, V.;et al. MicroRNAs as Biomarkers in Thyroid Carcinoma. International Journal of Genomics, 2017, 1-11. [CrossRef]
- Elisabetta Macerola, 1 Anello Marcello Poma, 1 Paola Vignali, 1 Agnese Proietti, 1 Clara Ugolini, 1 Liborio Torregrossa, 1 Alessio Basolo, 2 Rossella Elisei, 2 Ferruccio Santini, 2 and Fulvio Basolo. Predictive Biomarkers in Thyroid Cancer. Front Oncol. 2022, 12, 901004. [CrossRef]
- Maria Papaioannou 1, Angeliki G Chorti 2, Anthoula Chatzikyriakidou 3, Kleanthis Giannoulis 2, Sohail Bakkar 4, Theodosios S Papavramidis 2. MicroRNAs in Papillary Thyroid Cancer: What Is New in Diagnosis and Treatment. Review Front Oncol. 2022, 11, 755097. [CrossRef]
- Zubair W Baloch 1, Sylvia L Asa 2, Justine A Barletta 3, Ronald A Ghossein 4, C Christofer Juhlin 5 6, Chan Kwon Jung 7, Virginia A LiVolsi 8, Mauro G Papotti 9, Manuel Sobrinho-Simões 10, Giovanni Tallini 11 12, Ozgur Mete 13 .Overview of the 2022 WHO Classification of Thyroid Neoplasms. Review Endocr Pathol. 2022, 33, 27–63. [CrossRef]
- Pallante, P.; Visone, R.; Ferracin, M.; et al. MicroRNA deregulation in human thyroid papillary carcinomas. Endocrine-Related Cancer 2006, 13, 497–508. [Google Scholar] [CrossRef]
- Panebianco, F.; Mazzanti, C.; Tomei, S.; Aretini, P.; Franceschi, S.; Lessi, F.; Di Coscio, G.; Bevilacqua, G.; Marchetti, I. The combination of four molecular markers improves thyroid cancer cytologic diagnosis and patient management. BMC Cancer. 2015, 15, 918. [Google Scholar] [CrossRef] [PubMed]
- Sheikholeslami, S.; et al. Overexpression of mir-129-1, miR-146b, mir-183, and mir-197 in follicular thyroid carcinoma and adenoma tissues. Mol Cell Probes 2020, 51, 1–6. [Google Scholar] [CrossRef]
- Qiu, Z.; et al. miR-146a and miR-146b in the diagnosis and prognosis of papillary thyroid carcinoma. Oncol Rep 2017, 38, 2735–2740. [Google Scholar] [CrossRef]
- Daina Pamedytyte 1, Vaida Simanaviciene 1, Dalia Dauksiene 2, Enrika Leipute 1, Aurelija Zvirbliene 1, Valdas Sarauskas 3, Albertas Dauksa 4, Rasa Verkauskiene 2, Birute Zilaitiene 2. Association of MicroRNA Expression and BRAFV600E Mutation with Recurrence of Thyroid Cancer Biomolecules. 2020, 10, 625. [CrossRef]
- John Woody Sistrunk 1, Alexander Shifrin 2, Marc Frager 3, Ricardo H Bardales 4, Johnson Thomas 5, Norman Fishman 6, Philip Goldberg 7, Richard Guttler 8, Edward Grant 9. Clinical impact of testing for mutations and microRNAs in thyroid nodules. Diagn Cytopathol. 2019, 47, 758–764. [CrossRef]
- Visone, R.; Russo, L.; Pallante, P.; De Martino, I.; Ferraro, A.;et al. MicroRNAs (miR)-221 and miR-222, both overexpressed in human thyroid papillary carcinomas, regulate p27Kip1. [CrossRef]
- Liu, X.; Zhang, S.; Gang, Q.; Shen, S.; Zhang, J.; Lun, Y.; Xu, D.; Duan, Z.; Xin, S. Interstitial fibrosis in papillary thyroid microcarcinoma and its association with biological behavior. Oncology Letters 2018, 15, 4937–4943. [Google Scholar] [CrossRef]
- Bournaud, C.; Descotes, F.; Decaussin-Petrucci, M.; et al. TERT promoter mutations identify a high-risk group in metastasis-free advanced thyroid carcinoma. European Journal of Cancer 2019, 108, 41–49. [Google Scholar] [CrossRef]
- Gilani, S.M.; Abi-Raad, R.; Garritano, J.; Cai, G.; Prasad, M.L.; Adeniran, A.J. RAS mutation and associated risk of malignancy in the thyroid gland: An FNA study with cytology-histology correlation. Cancer Cytopathol. 2022, 130, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Matos, M.d.L.; Pinto, M.; Alves, M.; Canberk, S.; Gonçalves, A.; Bugalho, M.J.; Papoila, A.L.; Soares, P. Comparative CytoHistological Genetic Profile in a Series of Differentiated Thyroid Carcinomas. Diagnostics 2024, 14, 278. [Google Scholar] [CrossRef]
- Yang, S.I.; Choi, Y.S. Expressions of miRNAs in Papillary Thyroid Carcinoma and Their Associations with the BRAFV600EMutation and Clinicopathological Features. Kosin Medical Journal 2020, 35, 1–14. [Google Scholar] [CrossRef]
- Sun, Y.; et al. Expression of miRNAs in Papillary Thyroid Carcinomas Is Associated with BRAF Mutation and Clinicopathological Features in Chinese Patients. Int J Endocrinol. 2013, 128735. [Google Scholar] [CrossRef]
- Nicole A Cipriani 1, Daniel N Johnson 2, David H Sarne 3, Peter Angelos 4, Ward Reeves 5, Tatjana Antic 5. The Significance of RAS-Like Mutations and MicroRNA Profiling in Predicting Malignancy in Thyroid Biopsy Specimens. Endocr Pathol. 2022, 33, 446–456. 2022. [CrossRef] [PubMed]
- Anna B Banizs 1, Jan F Silverman 1. The utility of combined mutation analysis and microRNA classification in reclassifying cancer risk of cytologically indeterminate thyroid nodules. Diagn Cytopathol. 2019, 47, 268–274. 201. [CrossRef]

Table 1.
Distribution of the cytology samples within histological subtypes in all series.
| Cytology diagnosis n=106 |
Histology diagnosis n=106 |
|||||||
|---|---|---|---|---|---|---|---|---|
| Benign | WDT-UMP | NIFT | PTC | FTC | HCC | Total | ||
| 1.ND 2.Benign 3.AUS 4.FN 5.SM 6.Malignant |
||||||||
| 0 (0%) 12 (11.3%) 0 (0%) 1 (0.9%) 0 (0%) 0 (0%) |
0 (0%) 0 (0%) 0 (0%) 2 (1.9%) 0 (0%) 0 (0%) |
1 (0.9%) 2 (1.9%) 0 (0%) 1 (0.9%) 0 (0%) 0 (0%) |
2 (1.9%) 7 (6.6%) 23 (21.7%) 23 (21.7%) 12 (11.3%) 14 (13.2%) |
0 (0%) 1 (0.9%) 0 (0%) 1(0.9%) 2 (1.9%) 0 (0%) |
0 (0%) 1(0.9%) 0 (0%) 1 (0.9%) 0 (0%) 0 (0%) |
3 (2.8%) 23 (21.7%) 23 (21.7%) 29 (27.4%) 14 (13.2%) 14 (13.2%) |
||
| Total | 13 (12.3%) | 2 (1.9%) | 4 (3.8%) | 81 (76.4%) | 4 (3.8%) | 2 (1.9%) | 106 (100%) | |
Legend: ND: Non-diagnostic, B: Benign, AUS: Atypia of Undetermined Significance, FN: Follicular Neoplasm, SM: Suspicious for malignancy and M: Malignant. WDT-UMP: Well differentiated thyroid tumor of uncertain malignant potential; NIFT: noninvasive follicular thyroid neoplasm with papillary-like nuclear features; PTC: papillary thyroid carcinoma; FTC: follicular thyroid carcinoma; HCC: Hürthle cell carcinoma.
Table 2.
Frequencies of miRNAs expression in cytology by histology diagnosis in all series.
| miRNAs in cytology | Frequencies of miRNAs expression by histology diagnosis |
||||
|---|---|---|---|---|---|
| Final diagnosis |
Median | Under max-value n= (%) |
Over max-value n= (%) |
Total n= (%) |
|
| miRNA146 |
Benign Malignant |
0.308 0.489 |
≤ 4.394 11 (100) 55 (64.7) |
> 4.394 - 30 (35.3) |
96 (100) 11 (11.5) 85 (88.5) |
| miRNA221 | Benign Malignant |
0.535 0.172 |
≤ 5.242 11 (100) 70 (81.4) |
> 5.242 - 16 (18.6) |
97 (100) 11 (11.3) 86 (88.7) |
| miRNA222 | Benign Malignant |
0.914 1.460 |
≤ 6.358 11 (100) 56 (65.1) |
> 6.358 - 30 (34.9) |
97 (100) 11 (11.3) 86 (88.7) |
| miRNA15a | Benign Malignant |
1.053 0.686 |
≤ 7.39 11 (100) 77 (88.5) |
> 7.39 - 10 (11.5) |
98 (100) 11 (11.2) 87 (88.8) |
Table 3.
miRNAs expression in histology samples by histology diagnosis in all series.
| miRNAs in histology | By histology diagnosis | |||||||||
| n | histology | Median* | P25 - P75 | min - max value | p-value** | |||||
| miRNA146 | 60 08 52 |
Benign Malignant |
0.660 44.529 |
0.392 –2.455 3.215 – 907.373 |
0.322 – 5.341 0.016 – 27755.76 |
0.002 | ||||
| miRNA221 | 76 10 66 |
Benign Malignant |
1.312 4.297 |
0.781 –1.798 1.475 – 9.695 |
0.192 –4.395 0.012 – 63.304 |
0.008 | ||||
| miRNA222 | 78 10 68 |
Benign Malignant |
1.067 3.409 |
0.645 – 2.544 1.075 – 13.027 |
0.328 – 4.347 0.114 – 3006.772 |
0.017 | ||||
| miRNA15a | 77 10 67 |
Benign Malignant |
0.683 2.111 |
0.510 – 1.619 1.204 – 37.237 |
0.282 – 2.513 0.230 – 99.640 |
0.002 | ||||
Table 4.
Association between miRNAs expression levels and the presence of genetic mutations in histology samples in PTCs.
Table 4.
Association between miRNAs expression levels and the presence of genetic mutations in histology samples in PTCs.
| miRNAs in histology | ||||||||
|
Genetic mutations in histology | ||||||||
| miRNA-146 | miRNA-221 | miRNA-222 | miRNA15a | |||||
| n | Median | n | Median | n | Median | n | Median | |
|
TERTp Absent Present p-value |
54 48 06 |
29.856 60.203 0.563 |
67 59 08 |
2.990 6.310 0.451 |
69 61 08 |
3.076 3.958 0.708 |
68 60 08 |
1.981 37.494 0.033 |
|
BRAF Absent Present p-value |
54 39 15 |
9.900 133.574 0.020 |
67 49 18 |
1.820 8.625 0.001 |
69 50 19 |
1.548 14.006 <0.001 |
68 50 18 |
2.087 2.257 0.792 |
|
RAS Absent Present p-value |
54 41 13 |
26.511 716.144 0.016 |
67 53 14 |
2.464 10.900 0.010 |
69 55 14 |
2.325 5.284 0.144 |
68 54 14 |
1.713 24.767 0.026 |
Table 5.
The discriminative ability of miRNAs for PTC diagnosis.
| miRNAs in Histology | Papillary thyroid carcinomas | |||||
| (n) | cutoff | AUC (95%CI) | Se % (95%CI) | Sp % (95%CI) | PPV % (95%CI) | NPV % (95%CI) |
| miRNA-146b | 3. 070 | 93.5 (86.5-100) | 89.1 (76.4-96.3) | 87.5 (84-99.2) | 97.6 (84-99.2) | 58.3 (35.6-98.4) |
| miRNA-221 | 1.762 | 79.1 (67.8-90.4) | 71.9 (58.5-83) | 80 (44.4-97.5) | 95.3 (80.4-97.5) | 33.3 ( 21.5-82.9) |
| miRNA-222 | 1.392 | 75.8 (62.7-88.9 | 72.9 (59.7-83.6) | 70 ( 34.8-93.3) | 93.5 ( 76.6-96.5) | 30.4 ( 19.5-72.4) |
| miRNA-15a | 1.537 | 85.3 (73.8-96.9) | 72.4 (59.1-83.3) | 80 (44.4-97.5) | 95.5 (80.7-97.6) | 33.3 (21.6-82.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



