
Submitted:
28 February 2024
Posted:
29 February 2024
You are already at the latest version
Abstract
Background: Peripheral Ossifying Fibroma (POF) is a benign gingival tumor generally presenting as a slow-growing mass, usually not ulcerated, and without bleeding. Histopathological exam shows fibrous connective tissue with spots or extensive areas of intralesional calcifications, which can also be detectable on radiograms. Methods and case presentation: We present the case of a 4-year-old male with a retro-incisive swelling of the hard palate, associated with speaking and feeding difficulties. On CT scans, a small intralesional calcification was detected. After conscious sedation, the patient was subjected to diode laser excision (910 nm, 2W, CW, 300 m fiber) with-out post-operative complications. A review was conducted by searching the words “peripheral ossifying fibroma” AND “children” OR “infant” and including manuscripts of the last 15 years. Results: POF is an uncommon lesion of the oral mucosa and may sporadically affect the palatal mucosa in children. Considering its epidemiology and conventional clinical presentation as epu-lis, the pre-operative diagnosis may be relatively difficult. Risk factors could be represented by plaque, calculus, or trauma, all supporting a possible reactive pathogenesis, but a certain etiology is still missing. The main problem of POF is the recurrence rate, which is particularly high (8-20%), thus suggesting that a deep excision is recommended with full extension to the hard tis-sue of bone and to the adjacent periodontal ligament. Diode laser surgery may be recommended for such treatments, especially in pediatric patients, associated with intraoperative conscious se-dation. Data emerging from the relevant literature on POF management in children have been collected and discussed. Conclusions: The authors suggest the use of diode laser for the complete excision of POF, especially in less-compliant patients as children, with a low grade of comorbidi-ties and good outcomes, giving the surgeon a viable alternative to conventional surgery.
Keywords:
peripheral ossifying fibroma
; POF
; pediatric
; laser
; gingival tumor
1. Introduction
Intraoral peripheral ossifying fibroma (POF) was first described in 1844 by Shepherd et al., then named also as peripheral cementifying fibroma, peripheral odontogenic fibroma, calcifying or ossifying fibrous epulis, peripheral fibroma with calcification [1]. It is considered the gingival counterpart of the central ossifying fibroma, a fibro-osseous lesion presenting as a radiolucent area with radiopaque spots, frequently associated with vital teeth [2]. POF is an uncommon occurrence and is mainly located in the anterior maxilla of young patients between the 2nd and 3rd decades [3]. Clinically, it is generally described as a well-circumscribed gingival lesion with slow and progressive growth, rarely associated with pain, tooth displacement, ulcerations, and usually lacking radiographic alterations. However, calcification spots may occasionally be found on radiograms [4]. Although the true etiopathogenesis remains unclear, two different theories have been proposed over the years. The first theory considers POF as an evolved calcified pyogenic granuloma, while the second one suggests that POF may arise from inflammatory hyperplasia of the gingival tissues, the periosteum, or the superficial periodontal ligament [5]. Moreover, the POF lacks GNAS mutation, a characteristic feature of fibrous dysplasia, leaning toward a reactive origin [6]. Several local irritative factors have been related to POF, such as traumas, microorganisms, plaque, calculus, irregular restorations, and dental appliances, mainly supporting the reactive nature of POF. However, a general consensus is still missing [7]. Histologically, POF is characterized by fibrous connective tissue with many fibroblasts, mesenchymal cells, collagen, endothelial proliferation, and the presence of calcified material (such as mature or immature bone, cementum, and dystrophic calcification), while inflammatory tissue may be occasionally found at the periphery of the lesion. The histopathologic features are consistent with the theory that the POF originates from the superficial periodontal ligament cells [8]. Usually, the surgical excision (with periosteum debridement) is generally resolutive for POF, although the recurrence rate is particularly high (8-20%) [9], mainly related to incomplete removal of the lesion due to the impossibility or difficulty of eliminating local irritative agents during surgery. Moreover, conventional surgical treatment with scalpel is frequently characterized by intraoperative bleeding (related to gingival inflammation and poor dental hygiene), post-operative bleeding (related to frequent impossibility of suture), post-operative edema, and discomfort. POF management by laser has been reported as an alternative and resolutive surgical method. Generally, lasers such as diode, KTP, Neodymium: YAG, have proven surgical advantages for oral surgery procedures because they are associated with rarer intra-operative complications, low to absent intra-operative bleeding, faster mucosal healing, reduced post-operative pain and edema, and higher patient acceptance [10]. We report the rare case of a POF involving the palatal mucosa in a child, which was removed by using the diode laser. In this study we emphasize the benefits of laser excision as a viable surgical alternative in POF management, particularly in patients with special needs, reviewing the last 15 years international literature on such topic, as regards diagnosis, treatment and recurrence rate.
2. Case Presentation
A 4-year-old healthy male patient was referred to the Complex Unit of Odontostomatology of the University Hospital “Policlinico of Bari”, Italy, for a palatal swelling in the upper retro-incisive region. Their parents reported no relevant medical history. The lesion occurred two months earlier with a slow and progressive growth that caused discomfort and difficulties in speech and feeding, but without pain or bleeding. At the intraoral examination, a solitary nodular swelling on the palate, measuring approximately 0,5 x 0.5 cm in size and covered by normally colored mucosa, was observable (Figure 1a). A pre-operative maxillary CT, which required general anesthesia, was performed, showing an intra-lesional calcification. Bone involvement was absent (Figure 1b,c).
3. Results
On the basis of the clinical and radiological features, and with the parent’s agreement, it was decided to perform a diode laser surgical excision under conscious sedation. After a minimal local anesthesia, excision was performed by diode laser (Lasotronix, 910nm, 2W, CW, 300-micron fiber), the marginal gingiva of the 5.1 was preserved, and the lesion was removed with extensive lateral and deep margins, without intra-operative bleeding. Suture was not necessary (Figure 2).
Paracetamol (500 mg twice a day) was suggested for pain management during the 3-4 days following surgery. The specimen was fixed in 10% formalin and sent for the histological examination at the Unit of Pathological Anatomy. On Hematoxylin and Eosin stain, the lesion was composed of fibroblasts immersed in a dense fibrous connective tissue with many collagen fibers; inside the stroma, low endothelial proliferation and calcified material, along with deposition of immature bone and cementum, were also observable. On the basis of typical histopathological features, the final diagnosis was POF with calcifications (Figure 3).
No adjunctive immunohistochemical investigation was necessary to confirm the diagnosis. No artifacts or alterations related to the diode laser were reported by the pathologist, confirming the absence of morpho-structural or cytological changes induced by the thermal effect, as a result of tissue-laser light interaction.
No post-operative complication was observed, and no recurrence was detected after 8 months of follow-up (Figure 4).
4. Literature Review
In order to compare the management we proposed in the current case of POF occurring in a 4 y.o. child to the guidelines available in the recent literature, we searched in Google Scholar, PubMed, Scopus, and SciELO, using the following keywords: “peripheral ossifying fibroma” AND “pediatric” OR “infant”. Only case reports or case series of specific POF of the last 15 years were included, which provided the case description with age, sex, localization, clinical description, treatment, histological diagnosis and eventual recurrence. A synoptic table was set up with all included studies, reporting every described aspect.
5. Discussion
Herein, after having reported the rare occurrence of POF involving the palatal mucosa in a pediatric patient, as well as its management from diagnosis to follow-up, we compare our case with data emerging from the most recent and pertinent literature.
5.1. Epidemiology
POF represents the 3% of all oral benign tumors [11], which are subdivided into epithelial tumors (e.g., squamous papilloma), connective tissue tumors (e.g., lipoma, fibroma, lymphangioma, and hemangioma), and odontogenic tumors (e.g., ameloblastic fibroma, ameloblastoma odontoma, and odontogenic fibroma) [12]. Since it was described by Eversole and Rovin in 1972, it is considered a rare tumor, mostly affecting females in the second/third decades [1]. The female predilection may be related to hormone influence, such as high levels of estrogen and progesterone during puberty or pregnancy, which might explain the incidence peak in the second decade [13]. According to literature, POF localization may be quite different: Franco-Barrera et al. reported a preference for the anterior maxilla [14]. In contrast, other authors reported a preference for the posterior mandible [15,16]. In our review of POF exclusively occurring in pediatric and adolescent patients, we noted a preference for the anterior maxilla (55%), followed by the anterior mandible (18%) and generalized (18%).
5.2. Etiopathological Theories
Despite the latest immunohistochemical techniques, which allow for an understanding of the etiology of most diseases, the real etiopathogenesis of POF is still unknown. Even if not confirmed, the most widely accepted theory is a reactive origin [17]. Several irritative local factors may be related to the connective tissue metaplasia derived from periosteal and periodontal ligament cells, thus generating a proliferation of fibroblasts with consequent production of collagen, deposition of immature cementum and bone matrix by cementoblasts and osteoblasts, respectively. Local irritative factors are identified as bacterial deposits such as plaque or calculus, over-contoured restorations, and mobile prosthesis wearing. Overall, the histopathologic features, the exclusive gingival localization, and the common presence of irritative factors support the reactive origin of POF [8]. In contrast, the aforementioned hypothesis of POF derivation from Pyogenic Granuloma is based on the same irritative local factors and the role of osteopontin, a non-collagenous protein with high calcium binding potential, which may lead to mineralization of extracellular matrix [18]. Osteopontin is always present in POF and frequently present in Pyogenic Granuloma, suggesting a possible histopathological evolution of a single entity [19].
5.3. Clinico-Radiological Features and Differential Diagnosis
Considering the clinico-pathological features, as a localized slow-growth of keratinized gingival tissue with nodular aspect, covered by normally colored mucosa, asymptomatic, which may be ulcerated due to secondary trauma [9], the differential diagnosis includes a large spectrum of benign gingival lesions involving teeth (e.g., pyogenic granulomas, peripheral fibro-osseous lesions, peripheral odontogenic tumors and peripheral giant cell granuloma or fibromas), malignancies (e.g., osseous, salivary glands, epithelial malignancy) and hereditary diseases (e.g., hereditary gingival fibromatosis, plasminogen deficiency, mucopolysaccharidosis II and Gardner syndrome) [20]. Their dimension is usually a few centimeters, possibly involving the interdental papilla. This review confirms this aspect as the mean dimension is 2 x 1.5 cm. Radiological images could provide the first hint: intralesional calcifications without findings of osteolysis could guide the surgeon and pathologist toward a benign lesion such as a fibro-osseous or odontogenic tumor [21]. The most prescribed first-level exam, the orthopantomography, is generally not helpful in showing and defining little calcifications because of the possible overlapping with hard tissues (teeth or bone). Periapical radiograms may occasionally be adequate. The second-level exams as CT and CT-Cone Beam undoubtedly represent the more fit radiological exams for diagnosis because they allow to study each aspect with the possibility of switching different axes of visualization to identify the proper dimension, the possible involvement of adjacent anatomical structures and the small spots of calcification, due to high sensitivity [22]. Also, MRI could be helpful, but it is considered a more expensive and invasive exam with a lower definition than CT [23].
As for the herein reported case, an adjunctive challenge was the low grade of compliance due to the age, which made mandatory the general anesthesia to perform the CT at the time of pre-operative investigations; as such, the radiograph demonstrated the real extent of the lesion, the absence of bone involvement and a little intralesional calcification [23], thus orienting to a pre-operative diagnosis of a benign lesion.
5.4. POF in Pediatric Patients: Analysis of the Recent Literature
Considering that 95% of POF cases occur in 10-19 years old pediatric patients, only few studies report of POF cases in children under 10 years [24]; for this reason, we decided to carry out a brief review of the relevant literature about POF in pediatric patients, and the results are presented as follows. Tomáz Ferraresso [25] described an interesting case of POF of the anterior mandible in a 6-year-old patient, affected by Ellis-van Creveld (EVC) syndrome, an autosomal recessive disease consisting in skeletal and ectodermal dysplasia, characterized by short stature, postaxial polydactyly, ectodermal dysplasia, and congenital heart disease. The patient showed a small nodular neoformation on the edentulous alveolar ridge in the mandible, without radiological investigations, treated by conventional surgical excision, hemostasis and suture, without recurrence. Botazzo Delbem [15] described a case of the lateral maxillary region in a 5-year-old girl presenting as a non-ulcerated painless swelling, with radiological signs of osteolysis in correspondence of 1.2. The tumor was completely removed, without recurrence, by scalpel excision followed by curettage and periodontal scaling, diagnosed as “Peripheral Cemento-Ossifying Fibroma (PCOF)”. Lima et al. [20] reported a rare case of generalized POF in a 4 years old child, presenting as extensive exophytic lesion covering several teeth and interfering with the chewing, treated by a partial debulking to improve the masticatory function, but characterized by more than 30 recurrences in 9 years. Moreover, two authors described POF in newborns of 2 and 5 months. Singh et al. [26] presented a case report of POF manifesting as two distinct swellings localized in the mandibular edentulous ridge that did not allow a correct feeding. Interestingly, these two swellings began to grow after the exfoliations of two neonatal teeth. Both were removed by conventional surgery and showed no recurrence. Soares Tavares [27] reported a POF in a 2-month-old infant, localized on the mandibular alveolar ridge during the eruption of 8.1, impairing the patient’s feeding. In contrast with the previous study, the authors decided to perform an excisional biopsy using laser, providing a valuable sample for the pathologists and a better post-operative course without bleeding, pain, and suture. No recurrence was shown in this case. Rallan et al. [8] described a retro-incisive POF in a 12-year-old child. The clinical presentation was like our case but in an older patient. Only an intraoral Rx was performed, which showed no radiolucency and lamina dura integrity. The treatment consisted of a cold blade excision and bone debridement to exclude further recurrences. Choubey [28] reported a POF localized in the mandibular canine region in a 13-year-old girl. She was treated with pre-operative scaling and root planing to reduce the local irritative factor as much as possible. Scalpel excision was carried out, and an aesthetic gingival recontouring was performed. Histopathologic examination reported “Peripheral Cementifying Fibroma (PCF)”, quite similar to POF, but basophilic concentric calcifications consisting of “cementicles” were encountered at the center of the lesion. Franco-Barrera [14] conducted an interesting narrative review and reported a maxillary POF in an 11 years old girl, manifesting as an exophytic, painless and not ulcerated lesion of the maxillary right canine area, approximately measuring 4 × 3 × 1.5 cm, undergoing first to an incisional biopsy to exclude malignancy, then followed by scalpel excision and deep extension to the bone, with no recurrence. Yu [11] reported a case, very similar to the one reported by Lima et al., of a diffuse POF in a 13 years old girl, localized on the maxilla, mandible, and palate, presenting with difficulties in speech, feeding, and oral hygiene; after a first debulking, the patient received a more aggressive excision in the following year that allowed complete healing without recurrence. Hasanuddin [29] reported a maxillary POF in a 15 years old female that impeded lip competence because of its dimension of 2.4 x 2 cm, without radiolucency on the orthopantomography; the patient was subjected to an excisional biopsy with a scalpel following a bone debridement, and no recurrence was detected after 2 years. Nair and Tewari [30,31] described two similar cases of POF located in the anterior mandible, respectively in 3 and 2 months patients, with medical history of neonatal teeth; in both cases, lesions did not allow correct breastfeeding, so their surgical excision was necessary. All data mentioned above are summarized in Table 1 (Table 1).
Considering the most relevant literature on this topic, we found 12 case reports in the last 15 years, confirming a relatively rare occurrence in children or a low publication rate; 5 were between the range of 10 and 20 (42%), 3 between the 1-10 years (25%), 4 in newborn (< 1 year, 33%). Of particular interest are data about sex distribution: 7 cases (58%) occurred in females and 5 (42%) in males, confirming the female predilection of POF. Besides the age range, all cases show common histopathologic features: para-keratinized epithelium with a chronic inflammatory infiltrate, which delimitates a spindle fibroblast stroma, and calcification spots without areas of cellular atypia. Considering that POF occurrence in pediatric patients is very rare, the sample of this narrative review is too small to carry out any statistical analysis, but several considerations might be deduced. First of all, the distribution of sex and localization is consistent with previous studies, with a slight predominance in females [14,26]. In half of the cases, POF was localized in the mandible, then maxilla (33%) or generalized (17%), thus confirming that the epidemiological data of POF in infants are different from POF in adults, which predilects the maxillary region [12]. It is relevant to highlight that 4/6 of the cases presented in the anterior mandibula (inferior incisor region) belongs to newborn with neonatal teeth history; however, such association is persistent but not statistically demonstrated [30,33]. The case we presented was in contrast with the literature we found, as the maxillary POF mainly occurred in the vestibular region of the maxilla and only one case in the upper retroincisal area; in fact, as reported by Rallan et al. [8], the palatal occurrence further expands the differential diagnosis including reactive lesions as well neoplastic lesions both odontogenic and salivary. As often happens in such cases, in our patient the challenge was to predict the lesion’s nature without a pre-operative biopsy. In this, we were helped only by a CT scan that, although performed under general anesthesia, showed no cortical bone erosion and no tooth displacement, leading to exclude malignancy. In addition, CT was very useful in evaluating a little calcification spot in the lesion center, directing us toward an ossifying/cementifying lesion.
As found in literature, the pre-operative assessment of similar lesions, especially in children, lacks consensus. In the studies considered in this review, the most used radiogram was the periapical radiogram, followed by OPT. Both are first-level exams that must be executed if the patient is compliant, they are very useful for central lesions (lesions with exclusive bony involvement) but useless for peripheral lesions because of the overlapping of healthy hard tissues such as teeth and bone [34]. The radiological exam suggestable for this type of lesion is the CT or CT Cone Beam [35]. In previous studies, CT was executed only once, precisely by Franco-Barrera [14], as a pre-operative assessment of a large POF removed under general anesthesia.
The operative regime must be deepened: 11/12 cases were treated exclusively under local anesthesia. Local anesthesia is the safest and most practiced regimen but requires entire patient’s compliance. It is interesting to report that all newborns were treated in local anesthesia because the cost-effectiveness ratio was unfavorable for general anesthesia. In our case, thanks to the anesthesiologist, the patient was treated under conscious sedation and local anesthesia, avoiding an intra-operative general anesthesia. The advantages of conscious sedation in dental procedures are well established in the literature [36], so it should be preferred when compliance is reduced and general anesthesia is not suggested, especially in pediatric patients.
5.5. Therapeutic Strategies
As regards therapy, data from the literature confirm that surgery represents the eligible treatment for POF [37]. Surgical removal should permit the complete excision, often involving the periosteum. The removal of local irritative factors is mandatory, hence surgery is frequently associated with adjacent teeth scaling and root planning, when involved or substituting over contoured restorations. The main problem in POF treatment is the relatively high recurrence rate [23], usually related to partial excision due to the presence of teeth. In fact, the recurrence rate is estimated to be in a range from 8% to 20% [9]. In addition, surgery is usually performed without a preliminary incisional biopsy, especially in small lesions, and as a consequence without a pre-operative diagnosis. The possibility to obatain a pre-operative diagnosis is hugely relevant in order to plan a more or less invasive surgical procedure; therefore, in such cases, clinicians face the challenge of being resolutive in removing a lesion only clinically diagnosed as POF but anyway falling in a wide panel of possible differential diagnosis and, at the same time, to be as conservative as possible. Resective surgery is generally not indicated for such lesions. The most reported and performed surgery consists of scalpel, followed by bone debridement, tooth scaling and root planning, with an approach that is as conservative as possible [39]. Of the 12 studies conducted on pediatric patients that we considered in this review, 9 authors have preferred this conventional treatment strategy because of its well-established reliability [8,11,14,20,25,26,28,29,32]. The remaining 3 authors reported the surgical excision of POF in newborns using diode laser [27,30,31].
An alternative surgical approach is represented by the diode laser thanks to the possibility of reduced comorbidity, no suture needed, reduced rate of superinfections, and reduced drug intake for post-operative pain management [40]. Diode laser use in dentistry and oral surgery is widely supported by literature, mainly for soft tissue surgery (both for benign and malignant lesions) [41,42,43], providing a fast and not-bleeding lesion removal with (usually) second intention healing of the covering mucosa, as well as the transmucosal or intralesional photocoagulation of vascular malformations (thus avoiding invasive and unpredictable surgical procedures as in the past years) or lesions with high risk of intraoperative bleeding before the surgical removal [44]. It is relevant to underline that the use of diode laser was debated due to the risk of thermal alterations at the histologic examination, but it is fully demonstrated that the thermal effect is usually very low and doesn’t affect the histological diagnosis [45]. Therefore, diode laser excision is highly suggestable for patients with reduced compliance, including children, and with similar lesions reported herein [27,31]. In our case, the patient was a 4 year old child, thus with very low compliance, so the use of diode laser was very useful because the suture was unnecessary, the post-operative course was out of complications, and the palatal mucosa fully recovered in 10 days through second intention. This therapeutical choice is also strictly in accordance with the suggestions of the American Academy of Pediatric Dentistry regarding the policy on the use of lasers from 2013 [46] to the latest version of 2022 [47], precisely recognizing “Lasers as an alternative and complementary method of providing soft and hard tissue dental procedures for infants, children, adolescents, and persons with special health care needs”.
5.6. Limitations and Future Directions
Some limitations are present in this narrative review: the lack of data in the literature regarding POF in pediatric patients is very prominent. It did not allow us to perform any statistical analysis nor to draw definitive conclusions. The lack of articles differing from case reports or short case series is due to the rarity of POF, especially in children. Our intention was to report the diagnostic-therapeutic pathway that we followed with good outcomes, comparing it with the past literature, finally suggesting the possible best option in such a delicate situation. Based on the case description, and supported by the latest literature, authors would further encourage the use of diode laser to induce rapid and complete healing with reduced comorbidities, especially in pediatric patients. Moreover, this approach is also supported by the use of the pre-operative conscious sedation, providing the opportunity to carry out the adequate surgical procedure, which is often complicated by the proximity of teeth and/or periodontal tissues. Lastly, the use of diode laser for such interventions, when performed by an expert surgeon with the most adequate laser setting, is helpful in collecting a surgical specimen for the following histological examination, without any morphological alterations limiting the final diagnosis.
Author Contributions
Conceptualization, G.B. and S.C.; methodology, S.C., A.M.; validation, M.F; formal analysis, M.F..; investigation, G.B. G.I.; resources, S.C.; data curation, G.B.; writing—original draft preparation, A.D.; writing—review and editing, S.C.; visualization, A.D.; supervision, M.C. and G.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
not applicable.
Informed Consent Statement
All the detailed information about benefits and possible adverse effects of surgery, predicted outcome and treatment alternatives were reported to parents of little patient and written informed consent has been obtained from them.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Eversole, L.R.; Rovin, S. Reactive Lesions of the Gingiva. J. Oral Pathol. 1972, 1, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Nilesh, K.; Punde, P.; Patil, N.S.; Gautam, A. Central Ossifying Fibroma of Mandible. BMJ Case Rep. 2020, 13, e239286. [Google Scholar] [CrossRef]
- Bawazir, M.; Islam, M.N.; Cohen, D.M.; Fitzpatrick, S.; Bhattacharyya, I. Gingival Fibroma: An Emerging Distinct Gingival Lesion with Well-Defined Histopathology. Head. Neck Pathol. 2021, 15, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Lázare, H.; Peteiro, A.; Pérez Sayáns, M.; Gándara-Vila, P.; Caneiro, J.; García-García, A.; Antón, I.; Gándara-Rey, J.M.; Suárez-Peñaranda, J.M. Clinicopathological Features of Peripheral Ossifying Fibroma in a Series of 41 Patients. Br. J. Oral Maxillofac. Surg. 2019, 57, 1081–1085. [Google Scholar] [CrossRef]
- Shahrabi-Farahani, S.; Pencarinha, D.M.; Anderson, M. SATB2 Immunoexpression in Peripheral Ossifying Fibroma and Peripheral Odontogenic Fibroma. Head. Neck Pathol. 2022, 16, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.-R.; Li, X.-F.; Zhang, R.; Chen, Y.; Li, T.-J. GNAS Mutational Analysis in Differentiating Fibrous Dysplasia and Ossifying Fibroma of the Jaw. Mod. Pathol. 2013, 26, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Dutra, K.L.; Longo, L.; Grando, L.J.; Rivero, E.R.C. Incidence of Reactive Hyperplastic Lesions in the Oral Cavity: A 10 Year Retrospective Study in Santa Catarina, Brazil. Braz. J. Otorhinolaryngol. 2019, 85, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Rallan, M.; Pathivada, L.; Rallan, N.S.; Grover, N. Peripheral Ossifying Fibroma. Case Reports 2013, 2013, bcr2013009010–bcr2013009010. [Google Scholar] [CrossRef]
- Mortazavi, H.; Safi, Y.; Baharvand, M.; Rahmani, S.; Jafari, S. Peripheral Exophytic Oral Lesions: A Clinical Decision Tree. Int. J. Dent. 2017, 2017, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Anuradha, B.R.; Penumarty, S.; Charan, C.R.; Swati, M. Application of 810-Nm Diode Laser in the Management of Peripheral Ossifying Fibroma. J. Indian. Soc. Periodontol. 2015, 19, 224–226. [Google Scholar] [CrossRef]
- Yu, J.L.; Kapur, R.P.; Susarla, S.M. Recurrent Gingival Lesions in a Pediatric Patient. Plast. Reconstr. Surg. - Glob. Open 2022, 10, e4382. [Google Scholar] [CrossRef] [PubMed]
- Maymone, M.B.C.; Greer, R.O.; Burdine, L.K.; Dao-Cheng, A.; Venkatesh, S.; Sahitya, P.C.; Maymone, A.C.; Kesecker, J.; Vashi, N.A. Benign Oral Mucosal Lesions: Clinical and Pathological Findings. J. Am. Acad. Dermatol. 2019, 81, 43–56. [Google Scholar] [CrossRef] [PubMed]
- S, S.; Gujjari, S.K.; Sreeshyla, H.S. Peripheral Ossifying Fibroma in Pregnancy: A Multifactorial Consequence. IJMDS 2014, 518–523. [Google Scholar] [CrossRef]
- Franco-Barrera, M.J.; Zavala-Cerna, M.G.; Fernández-Tamayo, R.; Vivanco-Pérez, I.; Fernández-Tamayo, N.M.; Torres-Bugarín, O. An Update on Peripheral Ossifying Fibroma: Case Report and Literature Review. Oral Maxillofac. Surg. 2016, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hsien-Yen Hung; Chia-Chuan Chang; Julia Yu-Fong Chang; Chuan-Hang Yu; Yi-Ping Wang; Bu-Yuan Liu; Chun-Pin Chiang Peripheral Ossifying Fibroma: A Clinicopathological Study of 27 Cases. J. Dent. Sci. 2007, 2. [CrossRef]
- Ojo, M.A.; Omoregie, O.F.; Altini, M.; Coleman, H. A Clinico-Pathologic Review of 56 Cases of Ossifying Fibroma of the Jaws with Emphasis on the Histomorphologic Variations. Niger. J. Clin. Pract. 2014, 17, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Childers, E.L.B.; Morton, I.; Fryer, C.E.; Shokrani, B. Giant Peripheral Ossifying Fibroma: A Case Report and Clinicopathologic Review of 10 Cases from the Literature. Head. Neck Pathol. 2013, 7, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Godinho, G.V.; Silva, C.A.; Noronha, B.R.; Silva, E.J.; Volpato, L.E. Peripheral Ossifying Fibroma Evolved From Pyogenic Granuloma. Cureus 2022, 14, e20904. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Chandra, S.; Gupta, S.; Srivastava, S. Heterogeneous Conceptualization of Etiopathogenesis: Oral Pyogenic Granuloma. Natl. J. Maxillofac. Surg. 2019, 10, 3. [Google Scholar] [CrossRef]
- Lima, M.D.M.; Teixeira, R.G.; Bonecker, M.; De Camargo Moraes, P.; Mantesso, A. Recurrent Multicentric Peripheral Ossifying Fibroma-like Lesion in a Child: A Case Report. BMC Res. Notes 2014, 7, 673. [Google Scholar] [CrossRef]
- Agarwal, P.; Chug, A.; Kumar, S.; Jain, K. Palatal Peripheral Ossifying Fibroma: A Rare Occurrence. Int. J. Health Sci. (Qassim) 2019, 13, 63–66. [Google Scholar] [PubMed]
- Popli, H.; Singh, H.; Gupta, A.; Kamboj, M. Peripheral Ossifying Fibroma Veiling a Nasopalatine Duct Cyst: An Unusual Concurrence. Indian. J. Otolaryngol. Head. Neck Surg. 2022, 74, 1459–1461. [Google Scholar] [CrossRef] [PubMed]
- Moon, W.-J.; Choi, S.Y.; Chung, E.C.; Kwon, K.H.; Chae, S.W. Peripheral Ossifying Fibroma in the Oral Cavity: CT and MR Findings. Dentomaxillofac Radiol. 2007, 36, 180–182. [Google Scholar] [CrossRef] [PubMed]
- Buchner, A.; Shnaiderman, A.; Vared, M. Pediatric Localized Reactive Gingival Lesions: A Retrospective Study from Israel. Pediatr. Dent. 2010, 32, 486–492. [Google Scholar] [PubMed]
- Ferraresso, L.F.O.T.; Fagundes, F.A.U.; Padovese, M.; Singi, P.; Paiva, M.F.; Inagaki-Nomura, L.T.; Dezan-Garbelini, C.C.; Boer, F.A.C. Peripheral Odontogenic Fibroma in a Child with Ellis-van Creveld Syndrome: Case Report. Spec. Care Dent. 2023, scd.12855. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Gupta, S.; Hussain, I.; Augustine, J.; Ghosh, S.; Gupta, S. A Rare Case of Peripheral Ossifying Fibroma in an Infant. Contemp. Clin. Dent. 2021, 12, 81. [Google Scholar] [CrossRef] [PubMed]
- Tavares, T.S.; Da Costa, A.A.S.; Freire-Maia, F.B.; Souza, L.N.; Zarzar, P.M.; Martins-Júnior, P.A.; Aguiar, M.C.F.; Mesquita, R.A.; Caldeira, P.C. Unusual Exophytic Gingival Lesion in a Newborn Treated with Diode Laser. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, e74–e79. [Google Scholar] [CrossRef] [PubMed]
- Choubey, S.; Banda, N.R.; Banda, V.R.; Vyawahare, S. Peripheral Cementifying Fibroma: A Clinical Diagnostic Dilemma. Case Reports 2013, 2013, bcr2013009472–bcr2013009472. [Google Scholar] [CrossRef] [PubMed]
- Hasanuddin, S.; Malleshwar, Y. Idiopathic Peripheral Ossifying Fibroma in a Young Adolescent Girl: A Very Rare Clinical Presentation. J. Indian. Soc. Periodontol. 2017, 21, 329–332. [Google Scholar] [CrossRef]
- Nair, K.K.; Nausheen, E.; Chaudhuri, K.; Hariharan, M.; Ramesh, S. Laser-Assisted Management of a Rare Presentation of Peripheral Ossifying Fibroma in an Infant. Cureus 2021, 13, e20417. [Google Scholar] [CrossRef]
- Tewari, N.; Mathur, V.P.; Mridha, A.; Bansal, K.; Sardana, D. 940 Nm Diode Laser Assisted Excision of Peripheral Ossifying Fibroma in a Neonate. Laser Ther. 2017, 26, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Delbem, A.C.B.; Cunha, R.F.; Silva, J.Z.; Soubhia, A.M.P. Peripheral Cemento-Ossifying Fibroma in Child. A Follow-up of 4 Years. Report of a Case. Eur. J. Dent. 2008, 2, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Kumar, Rm.; Bavle, R.; Umashankar, D.; Sharma, R. Congenital Epulis of the Newborn. J. Oral Maxillofac. Pathol. 2015, 19, 407. [Google Scholar] [CrossRef]
- Crusoé-Rebello, I.; Torres, M.; Burgos, V.; Oliveira, C.; Santos, J. dos; Azevedo, R.; Campos, P. Hybrid Lesion: Central Giant Cell Granuloma and Benign Fibro-Osseous Lesion. Dentomaxillofacial Radiol. 2009, 38, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Missias, E.M.; Nascimento, E.; Pontual, M.; Pontual, A.A.; Freitas, D.Q.; Perez, D.; Ramos-Perez, F. Prevalence of Soft Tissue Calcifications in the Maxillofacial Region Detected by Cone Beam CT. Oral Dis. 2018, 24, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Galeotti, A.; Garret Bernardin, A.; D’Antò, V.; Ferrazzano, G.F.; Gentile, T.; Viarani, V.; Cassabgi, G.; Cantile, T. Inhalation Conscious Sedation with Nitrous Oxide and Oxygen as Alternative to General Anesthesia in Precooperative, Fearful, and Disabled Pediatric Dental Patients: A Large Survey on 688 Working Sessions. Biomed. Res. Int. 2016, 2016, 7289310. [Google Scholar] [CrossRef] [PubMed]
- Katanec, T.; Budak, L.; Brajdić, D.; Gabrić, D. Atypical Peripheral Ossifying Fibroma of the Mandible. Dent. J. (Basel) 2022, 10, 9. [Google Scholar] [CrossRef]
- Cavalcante, I.-L.; Barros, C.-C.; Cruz, V.-M.; Cunha, J.-L.; Leão, L.-C.; Ribeiro, R.-R.; Turatti, E.; Andrade, B.-A.; Cavalcante, R.-B. Peripheral Ossifying Fibroma: A 20-Year Retrospective Study with Focus on Clinical and Morphological Features. Med. Oral Patol. Oral Cir. Bucal 2022, 27, e460–e467. [Google Scholar] [CrossRef] [PubMed]
- Verma, E.; Chakki, A.B.; Nagaral, S.C.; Ganji, K.K. Peripheral Cemento-Ossifying Fibroma: Case Series Literature Review. Case Rep. Dent. 2013, 2013, 930870. [Google Scholar] [CrossRef]
- Ortega-Concepción, D.; Cano-Durán, J.A.; Peña-Cardelles, J.-F.; Paredes-Rodríguez, V.-M.; González-Serrano, J.; López-Quiles, J. The Application of Diode Laser in the Treatment of Oral Soft Tissues Lesions. A Literature Review. J. Clin. Exp. Dent. 2017, 9, e925–e928. [Google Scholar] [CrossRef]
- Capodiferro, S.; Loiudice, A.M.; Pilolli, G.; Lajolo, C.; Giuliani, M.; Maiorano, E.; Favia, G. Diode Laser Excision of Chondroid Lipoma of the Tongue with Microscopic (Conventional and Confocal Laser Scanning) Analysis. Photomed. Laser Surg. 2009, 27, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Capodiferro, S.; Kazakova, R. Laser-Assisted Gingivectomy to Treat Gummy Smile. Dent. Clin. North. Am. 2022, 66, 399–417. [Google Scholar] [CrossRef] [PubMed]
- Limongelli, L.; Capodiferro, S.; Tempesta, A.; Sportelli, P.; Dell’Olio, F.; Angelelli, G.; Maiorano, E.; Favia, G. Early Tongue Carcinomas (Clinical Stage I and II): Echo-Guided Three-Dimensional Diode Laser Mini-Invasive Surgery with Evaluation of Histological Prognostic Parameters. A Study of 85 Cases with Prolonged Follow-Up. Lasers Med. Sci. 2020, 35, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Capodiferro, S.; Limongelli, L.; Tempesta, A.; Maiorano, E.; Favia, G. Diode Laser Treatment of Venous Lake of the Lip. Clin. Case Rep. 2018, 6, 1923–1924. [Google Scholar] [CrossRef] [PubMed]
- Tenore, G.; Mohsen, A.; Nuvoli, A.; Palaia, G.; Rocchetti, F.; Di Gioia, C.R.T.; Cicconetti, A.; Romeo, U.; Del Vecchio, A. The Impact of Laser Thermal Effect on Histological Evaluation of Oral Soft Tissue Biopsy: Systematic Review. Dent. J. 2023, 11, 28. [Google Scholar] [CrossRef]
- AAPD. Policy on use of Lasers for pediatric dental patients. AAPD Reference Manual 2013, 36, 75–77.
- American Academy of Pediatric Dentistry. Policy on the use of lasers for pediatric dental patients. The Reference Manual of Pediatric Dentistry. Chicago, Ill.: American Academy of Pediatric Dentistry; 2022, 131–134.
Figure 1.
a) clinical presentation of POF occurring in the retroincisal palatal mucosa, covered by normally colored mucosa without ulceration; b) coronal CT scan; c) axial CT scan. Both CT scans showed a small intra-lesion calcification.
Figure 1.
a) clinical presentation of POF occurring in the retroincisal palatal mucosa, covered by normally colored mucosa without ulceration; b) coronal CT scan; c) axial CT scan. Both CT scans showed a small intra-lesion calcification.
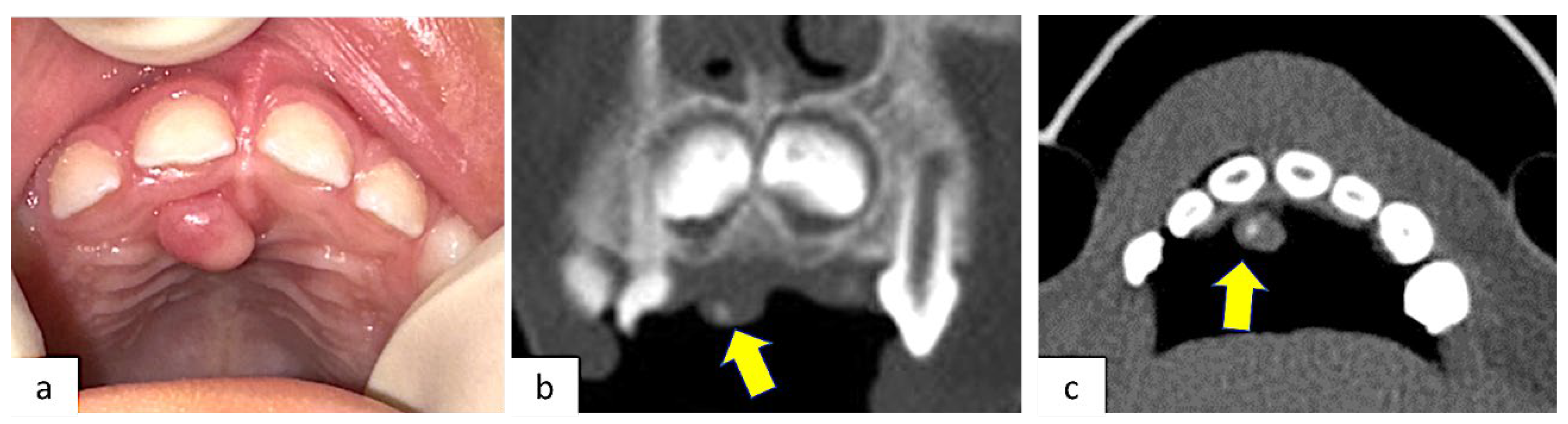
Figure 2.
Immediate post-operative appearance after diode laser removal. Surgical excision showed no bleeding or need for suture.
Figure 2.
Immediate post-operative appearance after diode laser removal. Surgical excision showed no bleeding or need for suture.

Figure 3.
a) A well-demarcated mucosal lesion characterized by an overlying reactive hyperkeratotic epithelium and a fibroblastic proliferation in a collagenous background (a). Centrally, deposition of immature bone and cementum is observable, which are essential criteria for the histological diagnosis (b).
Figure 3.
a) A well-demarcated mucosal lesion characterized by an overlying reactive hyperkeratotic epithelium and a fibroblastic proliferation in a collagenous background (a). Centrally, deposition of immature bone and cementum is observable, which are essential criteria for the histological diagnosis (b).
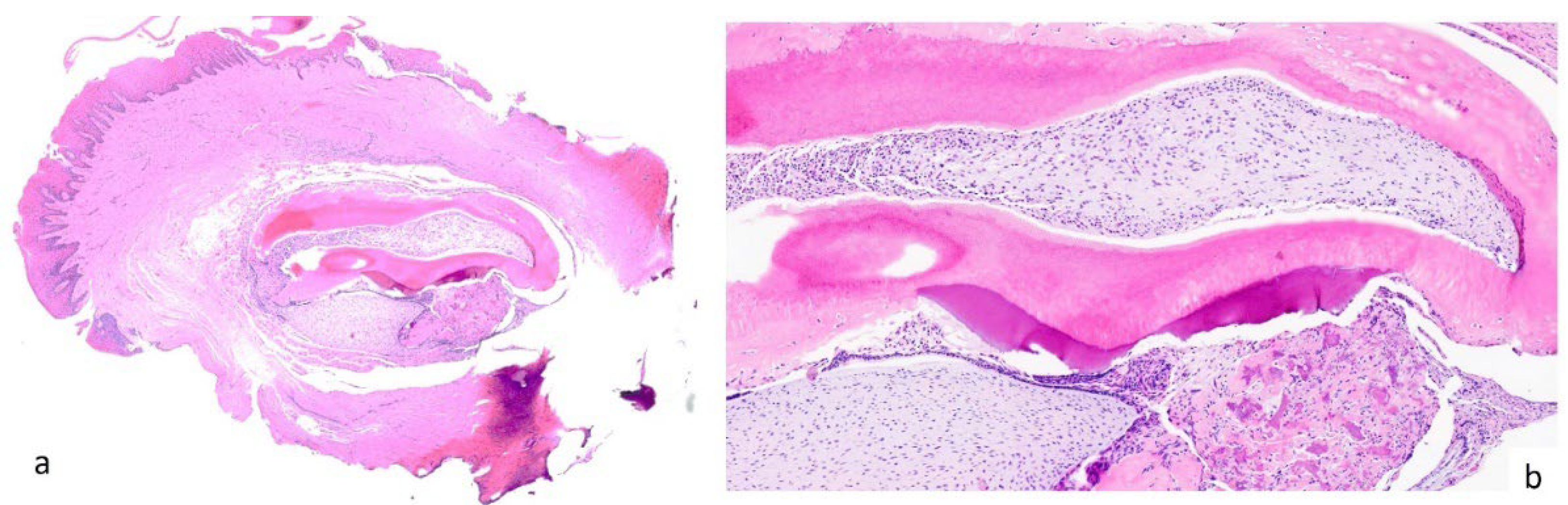
Figure 4.
Clinical appearance 8 months later showing no sign of recurrence.


Table 1.
Data from the relevant literature of the last 15 years about POF in pediatric patients.
| AUTHOR | YEAR | PATIENTS | AGE | SEX | LOCALIZATION | DIMENSIONS | CLINICAL PRESENTATION | RADIOLOGICAL EXAMS |
ANESTHESIOLOGICAL REGIMEN | DIAGNOSIS | RECURRENCE |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Deus Moura Lima [20] |
2014 | 1 | 9 | M | Generalized | Diffuse | Extensive exophytic, sessile, firm lesion with areas of ulcerated surface and a pink-to-red coloration that covered almost all the upper and lower teeth | OPT Periapical radiogram |
Local anesthesia | POF | 30 times |
|
Botazzo Delbem [32] |
2008 | 1 | 5 | F | Anterior maxilla Alveolar ridge |
1,5 cm | “lump” in the right upper alveolar margin between teeth 52 and 53 | Periapical radiogram | Local anesthesia | PCOF | No |
|
Rallan [8] |
2013 | 1 | 12 | M | Anterior maxilla Retroincisal (palate) |
2 × 2 cm | well-circumscribed, sessile, and erythematous upper retroincisal swelling, firm on palpation | Periapical radiogram | Local anesthesia | POF | No |
|
Choubey [28] |
2013 | 1 | 13 | F | Anterior mandibula | 3 × 1.5 cm | Large gingival overgrowth | Periapical radiogram | Local anesthesia | PCF | No |
|
Singh [26] |
2020 | 1 | 5 months | M | Anterior mandibula | 1.5 × 1 cm | Two distinct, firm, soft pedunculated growths; normal-appearing overlying mucosa | Periapical radiogram | Local anesthesia | POF | No |
|
Franco-Barrera [14] |
2015 | 1 | 11 | F | Anterior maxilla Right canine region |
4 × 3 cm | sessile exophytic lesion without changes in color, indurations, or ulceration. | OPT CT |
General anesthesia | POF | No |
|
Yu [11] |
2022 | 1 | 13 | F | Generalized | Diffuse | Diffuse hyperplastic gingival tissue across the maxillary and mandibular alveolar segments | OPT | Local anesthesia | POF | 1 time |
|
Hasanuddin [29] |
2017 | 1 | 15 | F | Anterior maxilla Vestibular middle-line |
2.4 × 2 cm | Elevated, oval-shaped mass with a smooth, shiny surface without bleeding or ulceration. | OPT | Local anesthesia | POF | No |
|
Tomáz Ferraresso [25] |
2022 | 1 | 6 | M | Anterior mandibula | 0.5 × 1 cm | Sessile, firm, whitish nodule located on the alveolar ridge | OPT | Local anesthesia | POF | No |
|
Soares Tavares [27] |
2020 | 1 | 2 months | F | Anterior mandibula | 1 x 0.5 cm | Nodular, firm, pedunculated lesion and covered by pink, flat, smooth mucosa | Occlusal radiogram | Local anesthesia | POF | No |
|
Nair [30] |
2021 | 1 | 3 months | F | Anterior mandibula | 0.5 x 1 cm | Solitary pedunculated nodular swelling | No radiograph | Local anesthesia | POF | No |
|
Tewari [31] |
2017 | 1 | 2 months | M | Anterior mandibula | 2.5 x 1 cm | Pink, nodular, pedunculated growth with smooth, intact surface | No radiograph | Local anesthesia | POF | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



