
Submitted:
04 April 2024
Posted:
05 April 2024
You are already at the latest version
Abstract
Infant mortality remains a major global concern. Sudden unexpected death in infancy (SUDI) is reported globally and in the Western Cape of South Africa it accounted for 40% of all infant deaths between 2012 and 2016. Research highlighting molecular typing of respiratory viruses in SUDI cases is lacking. A total of 116 PCR-positive human rhinovirus (HRV) and respiratory syncytial virus (RSV) swab samples collected from the lungs and trachea of SUDI cases admitted to Tygerberg Medico-legal Mortuary in Cape Town between 2015 and 2019 were included and underwent sequencing and phylogenetic analysis. Three distinct HRV species were identified; HRV-A (n=28), HRV-C (n=11), and HRV-B (n=4), including eight HRV-A, seven HRV-C and one HRV-B genotypes. For RSV, both RSV-A (n=5) and -B (n=5) were detected, but no RSV-A. After amino acid alignment indicating 20 amino acid duplication and nine substitutions, two BA9 genotypes were confirmed. This study describes the first molecular and phylogenetic characterisation of respiratory viruses in SUDI cases in South Africa. The rapid decline in viral viability in post-mortem samples and the retrospective study design employed for the current study did not allow for any correlations between viral genotypes and cause of death and future prospective studies should investigate temporality and specific viral strains associated with clinical disease severity.
Keywords:
respiratory infection
; human rhinovirus
; respiratory syncytial virus
; genotypes
; SUDI / SIDS
; infant death
; Sanger sequencing
; phylogenetic analysis
1. Introduction
Lower respiratory tract infection (LRTI) is a major barrier to the United Nations Millennium Development Goal to reduce global under-five child mortality [1]. Human rhinovirus (HRV) and respiratory syncytial virus (RSV) are among the common causes of LRTIs in infants and are associated with wheezing and childhood asthma [2,3,4,5,6,7,8,9,10,11].
HRV was first discovered in the 1950s as a causative agent for the common cold (12,13], and is still regarded as a leading cause of infant hospitalisation [5,14,15]. Primary infection occurs through inhalation of aerosolised droplets or physical inoculation after contact with fomites, followed by a 2-day incubation period [16]. Viral replication and infection occur in the epithelial cells of the upper and lower respiratory tracts [4,17]. Children serves as the main reservoir and infection is four times more common in children than in adults [5,12,14,18]. HRV is a member of the family Picornaviridae and the genus Enterovirus. These viruses are positive sense (ps), single-stranded (ss) RNA viruses with a 7 200 base pair (bp) genome, consisting of structural and non-structural regions, flanked by 5' and 3' untranslated regions (UTR). HRV is classified by genotype into HRV-A (80 serotypes), HRV-B (32 serotypes), and HRV-C (57 serotypes), and by cell surface receptor differences into Major and Minor groups. Over 160 genotypes exist [16,19]. Genotype differentiation of HRV is commonly achieved by reverse transcriptase polymerase chain reaction (RT-PCR) targeting the 5’UTR and VP4/2 followed by sequence analysis [20,21,22,23,24,25,26,27].
RSV was first identified in 1956 in a chimpanzee during an outbreak of coryza. The virus was later detected in humans which remain the only host [9,28]. Similar to HRV, RSV is also regarded as a leading global cause of LRTI and hospitalisations in infants [8,29,30,31,32,33,34]. Mortality may be lower in infants in developed countries; however, regardless of the socioeconomic status, infants under the age of six months have the same high risk of childhood asthma and recurrent wheeze when infection occurs during peak RSV season [9,35]. RSV used to be a subfamily within the Paramyxoviridae family [36], but in 2016 it was reclassified into the family of Pneumoviridae, genus Orthopneumovirus. The virus is a non-segmented, negative sense (ns) enveloped ssRNA virus with an approximate genome length of 15 000 bp [28]. Subtypes are based on sequence variations of the second hypervariable region (HVR), or HRV2, of the RSV G-gene [37]. Immune pressure, inherent lack of proof-reading capabilities, and duplication events in the RSV G-gene ectodomain enabled the detection of the Buenos Aires (BA) and the Ontario genotypes (ON) in 1999 and 2010 respectively [31,38,39]. The ON1 and BA strains within RSV-A and -B respectively, are differentiated by nucleotide duplications in the genome [31]. The relationship between genotype variation and clinical severity is still unclear. RSV-A and -B co-circulate with one predominating subtype each, with ON and BA genotypes rapidly becoming the predominant subtypes across the globe [28].
All three HRV species circulate within South Africa, commonly infecting young children. Similar to Jordan, Hong Kong, and Taiwan, HRV-A and -C predominate circulation in South Africa [4,6,16,40]. A previous South African study of 220 children presenting with wheeze at Red Cross War Memorial Children’s Hospital, Cape Town, showed that all three HRV genotypes were detected, with HRV-C (52%) predominating, followed by HRV-A (37%), and -B (11%). More than 70% of these children were under the age of 2 years [4]. Another South African study [42] confirmed this HRV-species distribution, but neither studies investigated any relationship between HRV genotype and disease severity [4,42]. More recently a study conducted in Mali, South Africa, and Zambia, found a higher prevalence of HRV-A in infants than HRV-B and HRV-C [25]. Clinical and molecular epidemiology data in low- and middle-income countries in Africa are limited and the specific role of HRV in childhood respiratory disease needs elucidation [4,25].
Both RSV-A and -B subtypes circulate in South Africa and are associated with LRTI [44,45] and infants comprise the majority of hospitalisation as a result of RSV [46]. The Drakenstein Child Health Study is an ongoing birth cohort longitudinal study on 1 143 infants in the Western Cape, South Africa. Of these, only 13% developed RSV-associated LRTI, while 60% did not develop any LRTI. Infants with RSV-associated LTRI had a ten-fold higher incidence of recurrent wheezing (43%) than those with no prior infection (3%). The results of this study further showed that LRTI and hospitalisation as a result of RSV were most common in winter and infants younger than 6 months of age, becoming less common with increasing age [11].
Globally, respiratory viral infections is a major burden in infants [15,32,47,48,49]. HRV, RSV, human CoV, and human adenovirus are commonly detected in infants with respiratory illness. Sudden unexpected death in infancy (SUDI) cases, defined as sudden and unexpected death in an infant with no clinical signs suggesting possible illness up to two days prior to death, show the same viral patterns than live infants [50,51,52,53,54,55]. All SUDI cases in South Africa must undergo a full medico-legal investigation at the respective Medico-legal Mortuaries and if no cause of death can be confirmed after an extensive autopsy, review of medical history, and death scene investigation, such cases are classified as sudden infant death syndrome (SIDS) [56,57,58]. Thus, SIDS is a subset of SUDI [59,60]. Both are regarded as leading causes of infant mortality [60,61].
2. Materials and Methods
2.1. Ethical Considerations
This study was approved by the Health Research Ethics Committee (HREC) of Stellenbosch University, Cape Town, South Africa (HREC Registration number: N12/02/007).
2.2. Sample Collection and Analysis
During autopsy, flocculated FLOQSwabs™ (Copan Flock technologies, Italy) samples were collected from the trachea and left lower lobes of the lungs of SUDI cases between 2015 and 2019 and screened with the Seegene AllplexTM RV Essential multiplex real-time RT-PCR assay (Seegene, South Korea) as per manufacturer’s instructions for a panel of respiratory viruses. All samples positive for HRV or RSV were included in this study.
Samples underwent automated RNA extraction using Microlab STAR Hamilton (Hamilton Company, USA) with the NucleoMag Pathogen Kit (Macherey-Nagel, Germany) as per the manufacturer’s guidelines. A one-step, nested RT-PCR assay was optimised for specific gene amplification of HRV and RSV.
2.3. Sequencing and Phylogenetic Analysis
Primers for genotyping and sequencing were selected from the literature for HRV [22,62,63] and manufactured by Integrated DNA Technologies (USA). Detailed methodolocy is attached as Supplementary Data.
Phylogenetic analysis was performed by assembling patient consensus sequences with De Novo Assemble tool of forward and reverse sequences in Geneious Prime® 2021.1.1. The Basic Local Alignment Search Tool (BLAST) within Geneious Prime was used to identify reference sequences for each nucleotide sequence. For HRV, Coxsackie virus (M16560) and Poliovirus 1 (V01149), and for RSV, Bovine orthopneumovirus (AF092942), listed by the International Committee on Taxonomy of Viruses website, were selected as outgroups for phylogenetic analysis. All files were uploaded to Multiple Alignment using Fast Fourier Transformation version 7 software for multiple sequence alignment.
The HRV phylogenetic tree was constructed using the Maximum Likelihood Method in Randomised Axelerated Maximum Likelihood (RAxML) program with 1000 bootstrap replicates with values over 70% shown. The General Time Reversible substitution model with gamma distributed rate variation and invariant sites (GTR + G + I). The tree was rooted with Coxsackievirus B1 (M16560) and Poliovirus 1 (V01149), and represent the outgroups in this phylogenetic analysis, as both viruses are closely related to the in-group (HRV) as per the ICTV website. Blue shading indicates HRV-A species, purple shading indicated HRV-B species, and pink shading indicates HRV-C species. The Samples successfully genotyped of each species are shaded in darker colour and are labelled with the respective genotype following the tip label, where appropriate.
The RSV phylogenetic tree was constructed using the Maximum Likelihood Method in Randomised Axelerated Maximum Likelihood program with 1000 bootstrap replicates with values over 70% shown. The Hasegawa-Kishino-Yano model with gamma distributed rates (HKY + G) was used. The tree was rooted with Bovine orthopneumovirus (AF092942), and represents the outgroup selected for phylogenetic analysis. Blue shading indicates RSA-A genotype and purple shading indicated RSV-B genotype. The Samples successfully subtyped of each genotype are shaded in darker colour and are labelled with the respective subtyped following the tip label, where appropriate.
3. Results
Previous prospective viral screening during 2015/2016 and 2018/2019 produced 106 positive HRV and 56 postive RSV samples. Since different PRC kits were utilised during previous studies and in order to obtain Ct values, all positive samples were retrieved and retested with the Seegene AllplexTM RV Essential multiplex real-time RT-PCR assay. Samples with Ct values below 40 for HRV and 30 for RSV were included in manual PCR.
Of these, 64/106 (60%) and 15/56 (27%) were positive for HRV and RSV respectively. Ct values were below 40 for 60 HRV-positive samples and below 30 for 10 RSV-positive samples. The remaining four HRV-positive and five RSV-positive samples were not included in the manual PCR, because the Ct values were outside the RSV manual PCR amplification limits. Two of the selected RSV-positive samples produced Ct values of 29.30 and 27.99, which were higher than the detection limit previously determined by the RSV manual PCR assay, but these samples were included, and amplification was successful.
PCR products were obtained from a total of 60 HRV and 10 RSV positive samples which successfully amplified, of which 43 HRV and all 10 RSV samples were successfully sequenced.
HRV samples produced three distinct species , HRV-A (n=28), followed by -C (n=11), and -B (n=4). In total, eight HRV-A (A28, A80, A10, A82, A43, A56, A11, and A56), one -B (B84), and seven -C (C22, C19, C24, C35, C29, C38, and C2) genotypes were identified. HRV-A was detected in all seasons, while -C was detected in the cooler seasons (autumn and winter), and -B was only detected in winter.
RSV-A and RSV-B were confirmed in five samples each. None of the RSV-A sequences were assigned as ON1, and three samples were assigned BA9 after phylogenetic analysis. RSV-A was detected in samples from all seasons, except summer, while RSV-B was detected throughout the year. Some samples from the same SUDI case clustered together and had a bootstrap value of 100 (HRV samples 4A and 10B and 1 and 7, and RSV samples 5 and 9).
All RSV-A deduced amino acid sequences were aligned and compared to prototype ON1 strain (Accession number: JN257693; ON67-1210A), which is characterised by a nucleotide insertion of a 72-nucleotide duplication in the second hypervariable region of the RSV G-gene, otherwise a 23 amino acid duplication (QEETLHSTTSEGYLSPSQVYTTS) beginning at amino acid 261 to 283 and 285 to 307. None of the RSV-A samples presented with this duplication or matching N-glycosylation sites.
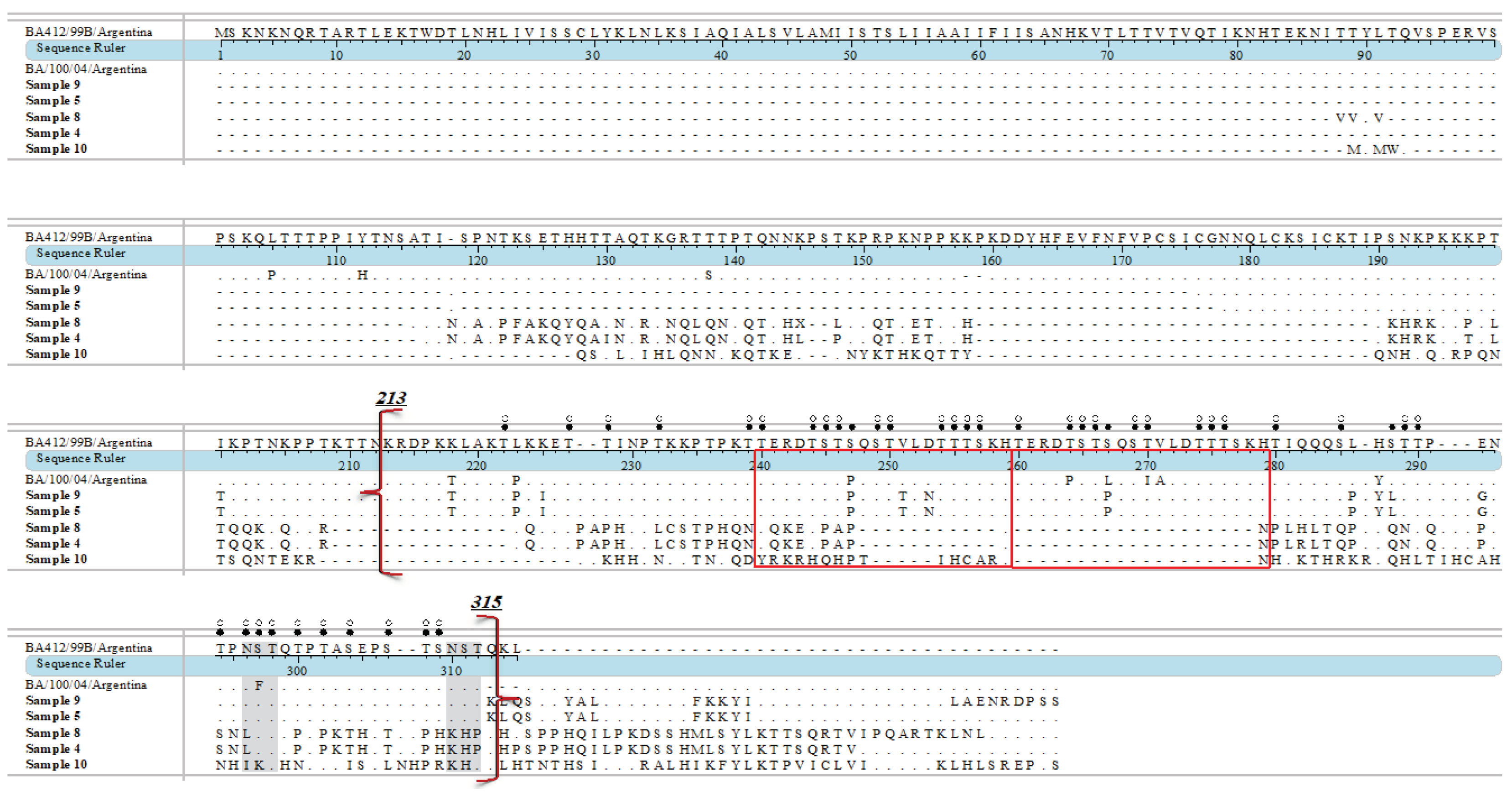
BA9 genotypes display a characteristic 60 nucleotide duplication, otherwise a duplication of 20 amino acids (TERDTSTSQSTVLDTTTSKH) beginning at position 240 to 259 and 260 to 279 of the RSV G-gene. Though sample 8 was closely related to LR699741—genotype BA9—and Samples 5 and 9 diverge from KY249662—also genotype BA9—as depicted in phylogenetic analysis following amino acid alignment of all RSV-B sequences obtained in this study to sequences of prototype BA1 (Accession number: AY333364; BA/4128/99B) and the inclusion of a BA9 subtype (Accession number: DQ227395; BA/100/04), only samples 9, and 5 displayed the insertion of 20 amino acid duplication, and amino acid substitutions K218T, L223P, K225I, V251T, D253N, S267P, H287Y, S288L, and E292G. All samples showed S247P, and four showed L286P substitutions. Additionally, outside of the second hypervariable region, all samples had I200T substitution. Two NST N-Glycosylation sites are reported within the RSV-B second hypervariable region of the G- gene, at codons 296 to 298 and 310 to 312. N-Glycosylation sites were determined by scores over 0.5. Sample 9 retained both N-Glycosylation sites, at codon 296 (0.52) and 310 (N-Glyc: 0.57). Sample 5 also retained both N-Glycosylation sites at codons 296 (0.51) and 310 (0.56). Sample 8 matched the first glycosylation site (N-Glyc: 0.59) with N296L substitution.
Deduced amino acid alignment of RSV G-gene of RSV-A and RSV-B samples are presented as Figure 3 and Figure 4. RSV-A sample sequences were aligned and are shown relative to the sequence of RSV ON1 (Accession number: JN257693; ON67-1210A), while RSV-B samples sequences were aligned and are shown relative to sequence of prototype RSV-BA1 (Accession number: AY333364; BA/4128/99B) and BA9 (Accession number: DQ227395; BA/100/04).
4. Discussion
This study used Sanger sequencing to describe the different HRV and RSV genotypes in retrospective respiratory tract samples collected from SUDI cases admitted to the Tygerberg Medico-legal Mortuary in Cape Town between 2015 and 2019. The literature describes genotypic characterisation of HRV-A, -B, and -C, as well as RSV-A and -B in infants and children admitted for hospital care in South Africa [4,44,64]; however, this is the first study to genotype respiratory viruses in SUDI cases at Tygerberg Medico-legal Mortuary, and South Africa.
4.1. Human Rhinovirus
HRV genotypes HRV-A10, -A11, A28, -A43, -A56, -A63 and -A80 and -A82 were all confirmed in SUDI samples from this study. HRV-B84, -C2, -C19,- C22, -C24, -C29, -C35 and -C38 were also detected.
The results agree with the literature that describes HRV-A10, HRV-A11 and HRV-A28 in infants with acute respiratory illness [65]. Although HRV-A10 is less frequently reported than HRV-A28, HRV-A56, and HRV-A80, it is commonly detected in infants presenting with respiratory disease in other sub-Saharan Africa countries [25,66,67]. Furthermore HRV-A80 was also detected in Tunisia and in China in hospitalised infants presenting with severe and acute respiratory tract infection during the same time period as the current study [68,69]. Certain HRV genotypes, such as HRV-A82 and HRV-A43, are not exclusively detected in infants, but also in adolescents and adults, who may transmit the virus to infants when in close contact [70], such as bed-sharing. Since most infants in this study had reported a history of bed-sharing where the infant is in close contact with other individuals for prolonged periods of time. If such individuals present with HRV or any other viral infection, it may increase the risk of viral transmission.
The samples from this study were collected before the COVID-19 pandemic and were not tested for severe acute respiratory syndome-2 (SARS-CoV-2), but HRV-A82 was commonly reported in children and adolescents presenting with respiratory disease during the COVID-19 pandemic [71,72]. Genotype HRV-A43 has also been described to reinfect children, adults and the elderly with acute respiratory infections and subsequent prolonged viral shedding [73,74,75]. It is therefore postulated that HRV may either play a contributory role in infant death, or the detection during post-mortem analysis may not infer causation of SUDI, but rather transmission from close-contact with other infected individuals. This hypothesis is supported by a study from the Salt River Mortuary, Cape Town, that has identified the consequences of overcrowded living conditions and infection-related causes of death in SUDI cases [76]. Finally, genotypes HRV-A28, -A56 and -A80 were among the most frequently reported in clinical studies reporting on HRV diversity Asia and Africa between 2013 and 2021 [16]. Only Genotype HRV-A63 has been detected in another SUDI case in the literature [77]. This may be attributed to the lack of SUDI investigations assessing viral genotypes in forensic settings in South Africa and globally.
Only one HRV-B genotype (-B84) was detected in this study, which agrees with the reported trend by molecular epidemiology research in Tanzania, Nigeria, Kenya, Mozambique and South Africa [25,67,78,79,80]. HRV-B84 was one of the top 25 genotypes reported by seven studies from Africa [16]. This species is not associated with severe disease and parents might therefore not seek medical attention and laboratory testing, suggesting that the true burden may be underrepresented [78]. The low detection of HRV-B in this study might therefore also not be a true representation of its diversity in SUDI cases in this population.
HRV-C is commonly detected in children with respiratory disease [4]. HRV-C2 and -C38 were among the top three identified in Kenya from 2007 to 2018 in children presenting with severe acute respiratory infection, and -C2 was previously detected in Amsterdam between 2007 and 2012 [16,81]. Genotype -C22 was also detected in children in Nigeria and Tanzania suspected of respiratory illness, and hospitalised children in Sweden [16,67,78].
The burden of HRV infection in infants living in Africa and hospitalised in the Cape Town Metropole has previously been well described [4,42,67]. The findings of this study suggest that certain HRV genotypes were present in the SUDI cases at the time of death, but the studies to date were not designed to assess a causal relationship between PCR-results and infant death. Since quantification of viral loads in post-mortem samples proves to be challenging and unreliable due to decrased viral viability post-mortem, the mechanisms by which infection may lead to death, especially in infants, may be supplemented by biomarkers of infection and sepsis, and genotype identification in the presence of clinical features of respiratory disease to further elucidate the role of HRV genotypes in infant death [15,82,83].
4.2. Respiratory Syncytial Virus
RSV-A remains the most common and diverse group in South Africa, China and Saudi Arabia [64,84,85,86,87]. Despite a high prevalence of ON1 in South Africa between 2015 and 2017, none of the RSV-A samples from this study closely related to ON1.
RSV-B has been reported to predominate in eight other countries between 2017 and 2018, possibly due to virulence and circulation of specific strains at the time [84] and was first detected in South Africa in 2006 during a nosocomial outbreak [37,85,88,89]. RSV-BA9 was first identified in Japan during the 2006 and 2007 epidemic season and is commonly detected in infants presenting with LRTI [84,90,91,92,93].
In 2021, RSV-BA9 was detected in an outbreak in China in hospitalised neonates presenting with respiratory failure [94]. One study sample closely related to RSV-BA9 first isolated from a male infant in Spain as per the GenBank record. RSV-BA9 has previously been detected in infants and other regions of South Africa, however recently published amino acid substitutions are limited [37,44,64,87,95]. The amino acid substitutions noted in RSV-BA9 this study were characteristics of RSV-BA9 strains reported in the literature [92,96,97]. However, substitutions I281T and P291L differentiating between sub-genotypes RSV-BA9a and RSV-BA9b were not noted in this study [93], although two samples had commonly reported RSV-BA9 K218T, L233P, and H287Y substitutions [98,99,100]. S247P, also a common substitution of RSV-BA9 strains, was present in all samples, while L223P was only noted in two sampels. S247P substitution has been reported from Taiwan, Panama, Thailand, and other countries [92,100,101,102,103]. Furthermore, 247P with L223P and H287Y substitutions detected in these two samples were noted in strains identified in Central African Republic between 2015 and 2018 [104].
In the RSV-B duplication site, D253N amino acid substitution was reported in RSV seasonal epidemics in Shanghai, China and multiple studies in India from children presenting with respiratory disease from children presenting with LRTI [91,105,106]. Additionally, the substitution may lead to a possible third N-glycosylation site [107], but this was not present in the current study. Interestingly, E292G substitution in the above-mentioned two samples were reported in RSV-BA10 detected in children admitted for acute respiratory infection in Vietnam and is confirmed by other publications in RSV-BA10 genotypes [108,109]. One additional sample did not have any amino acid duplication insertion, but it had T254I substitution, which was reported as a characteristic of RSV-BA9 [92]. The literature suggsts that this substitution in combination with mutation K314R, might have been involved in the BA9 predominance in 2015/2016 in Taiwan [100]. When RSV-B sequences from this study were compared to DQ227395 (BA/100/04), the A269V substitution was confirmed, which is in agreement with reported RSV strains in children in China during the COVID-19 pandemic [110].
4.3. Strengths and Limitations
This was the first study in South Africa to investigate specific viral genotypes of the most common respiratory viruses in SUDI cases and this forms the foundation for continued research to further identify and describe distribution patterns, viral diversity, severity of disease, and possible associations between the identified risk factors and genotypes for the most prevalent respiratory viruses in infants and children.
The main limitations of this study were varying success in retrieval, and amplification of previously identified PCR-positive HRV and/or RSV samples, confirmatory PCR retesting and successful sequencing of amplified PCR products.
Limited resources and research capacity at the Tygerberg Medico-legal Mortuary resulted in intermittend sample collection periods, challenging assessment of the distribution and true seasonality patterns of the viruses commonly found in SUDI cases. Financial constraints also only allowed for Sanger sequencing to be used, but future studies should employ more second- or third-generation sequencing platforms, such as Illumina or Oxford Nanopore Technology.
The most important limitation is the fact that viral viability decreases significantly with increasing post-mortem interval, which is typically between 3 and 10 days at the Tygerberg Medico-legal Mortuary and this does not allow for quantification of viruses or assessing temporality in formulating the cause of death.
5. Conclusions
This study described specific viral genotypes in post-mortem samples collected from SUDI cases in Cape Town, South Africa and was able to confirm the presence of specific HRV and RSV genotypes with known morbidity in infants and children from the literature during the same time period than the current study. Due to ethical constraints and the invasive nature of sample collection, it is not possible to include a post-mortem infant control group and results were compared to published data of infants and children with respiratory disease where HRV and/or RSV were confirmed. Rapidly decreasing viral viability after death makes quantification difficult and the direct association between viruses and active infection cannot be assessed. Other aspects, such as macro- and microscopic investigation of tissue, need to be included and considered in the formulation of the cause of death of these infants.
Future studies should therefore include prospective investigation of other markers of infection or sepsis, such as cytokines and acute phase proteins. Known sociodemographic risk factors should also be assessed and considered in the formulation of the cause of death in SUDI cases.
Author Contributions
Conceptualization, Protocol and Methodology, Institutional Review Application and Approval, Funding acquisition, Resources, Provided training and supervision, Project administration, Visualisation, Overseeing laboratory work, results, data analysis and interpretation, Writing – review, editing and submission of manuscript – C.D.B.; Methodology, Data analysis and interpretation, writing—original draft preparation, H.D.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the South African Medical Research Council [MRC] (Self-initiated research), Poliomyelitis Research Foundation [PRF] (Grant numbers 22/03, 17/05, 15/07, 12/06, 09/29 and Student Bursaries 21/47, 18/53, 18/33, 16/35, 15/53, 14/31, 12/42, 11/37,09/33); National Health Laboratory Service [NHLS] Research Grants (Grant numbers 94795, 94603, 94380, 94172, KNC 151).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Stellenbosch University Health Research Ethics Committee [HREC] (Registration Number N12/02/007, first registration 07/03/2012, with annual renewal).
Informed Consent Statement
HREC approved a waiver of consent under Protocol N12/02/007. Consent is provided for by Section 3(a) of the Inquests Act (58 of 1959) and the Criminal Procedure Act (1977) as all SUDI cases must be subjected to a full post-mortem investigation according to the Act (58 of 1959), as it is regarded as unnatural deaths, and samples are collected to ascertain the cause(s) of death.
Data Availability Statement
No publicly archived datasets were analyzed or generated during the study. Datasets are available on request from the authors.
Acknowledgments
Johan Dempers (deceased) for his involvement in earlier SUDI studies, Mathilda Claassen for training and assistance with sequencing and analysis.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Geoghegan, S. Erviti, A., Caballero, M.T., Vallone, F., Zanone, S.M., Losada, J.V., Bianchi, A., Acosta, P.L., Talarico, L.B., Ferretti, A., Grimaldi, L.A., Sancilio, A., Dueñas, K., Sastre, G., Rodriguez, A., Ferrero, F., Barboza, E., Gago, G.., Nocito, C., Flamenco, E., … Polack, F. P. Mortality due to Respiratory Syncytial Virus. Burden and Risk Factors. Am J Respir Crit Care Med 2017, 195, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Kotaniemi-Syrjänen, A. Vainionpää, R., Reijonen, T.M., Waris, M., Korhonen, K., Korppi, M. Rhinovirus-induced wheezing in infancy--the first sign of childhood asthma? J Allergy Clin Immunol 2003, 111, 66–71. [Google Scholar] [CrossRef]
- Linsuwanon, P. Payungporn, S., Suwannakarn, K., Chieochansin, T., Theamboonlers, A., Poovorawan, Y. Complete coding sequence characterization and comparative analysis of the putative novel human rhinovirus (HRV) species C and B. Virology J, 2003; 8, 5. [Google Scholar] [CrossRef]
- Smuts, H.E. Workman, L.J., Zar, H.J. Human rhinovirus infection in young African children with acute wheezing. BMC Infect Dis 2011, 11, 65. [Google Scholar] [CrossRef] [PubMed]
- Drysdale, S.B. Alcazar, M., Wilson, T., Smith, M., Zuckerman, M., Lauinger, I.L., Tong, C.Y., Broughton, S., Rafferty, G.F., Johnston, S.L., Greenough, A. Respiratory outcome of prematurely born infants following human rhinovirus A and C infections. Eur J Pediatr 2014, 173, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Stone, C.A. Jr, Miller, E.K. Understanding the Association of Human Rhinovirus with Asthma. Clin Vaccine Immunol 2015, 23, 23–10. [Google Scholar] [CrossRef]
- Jartti, T. Gern, J.E. Role of viral infections in the development and exacerbation of asthma in children. J Allergy Clinical Immunol 2017, 140, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Shi, T. McAllister, D.A., O'Brien, K.L., Simoes, E.A.F., Madhi, S.A., Gessner, B.D., Polack, F.P., Balsells, E., Acacio, S., Aguayo, C., Alassani, I., Ali, A., Antonio, M., Awasthi, S., Awori, J.O., Azziz-Baumgartner, E., Baggett, H.C., Baillie, V.L., Balmaseda, A., Barahona, A., … RSV Global Epidemiology Network. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet (London, England) 2017, 390, 946–958. [Google Scholar] [CrossRef]
- Borchers, A.T. Chang, C., Gershwin, M.E., Gershwin, L.J. Respiratory syncytial virus--a comprehensive review. Clin Rev Allergy Immunol 2013, 45, 331–379. [Google Scholar] [CrossRef] [PubMed]
- Laudanno, S.L. Sánchez Yanotti, C.I., Polack, F.P. RSV Lower Respiratory Tract Illness in Infants of Low- and Middle-income Countries. Acta Med Acad 2020, 49, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Zar, H.J. Nduru, P. , Stadler, J.A.M., Gray, D., Barnett, W., Lesosky, M., Myer, L., Nicol, M.P. Early-life respiratory syncytial virus lower respiratory tract infection in a South African birth cohort: epidemiology and effect on lung health. Lancet Glob Health 2020, 8, e1316–e1325. [Google Scholar] [CrossRef]
- Jacobs, S.E. Lamson, D.M., St George, K., Walsh, T.J. Human rhinoviruses. Clin Microbiol Rev 2013, 26, 135–162. [Google Scholar] [CrossRef]
- Nakauchi, M. Nagata, N., Takayama, I., Saito, S., Kubo, H., Kaida, A., Oba, K., Odagiri, T., Kageyama, T. Propagation of Rhinovirus C in Differentiated Immortalized Human Airway HBEC3-KT Epithelial Cells. Viruses 2019, 11, 216. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, S. Brockman-Schneider, R., Bochkov, Y.A., Pasic, T.R., Gern, J.E. Biological characteristics and propagation of human rhinovirus-C in differentiated sinus epithelial cells. Virology 2013, 436, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Perosanz, M. Sanchez-Trincado, J.L., Fernandez-Arquero, M., Sidney, J., Sette, A., Lafuente, E.M., Reche, P.A. Human rhinovirus-specific CD8 T cell responses target conserved and unusual epitopes. FASEB J 2021, 35, e21208. [Google Scholar] [CrossRef] [PubMed]
- Esneau, C. Duff, A.C., Bartlett, N.W. Understanding Rhinovirus Circulation and Impact on Illness. Viruses 2022, 14, 141. [Google Scholar] [CrossRef] [PubMed]
- Clementi, N. Ghosh, S., De Santis, M., Castelli, M., Criscuolo, E., Zanoni, I., Clementi, M., Mancini, N. Viral Respiratory Pathogens and Lung Injury. Clin Microbiol Rev 2021, 34, e00103–20. [Google Scholar] [CrossRef]
- Han, M. Rajput, C., Hershenson, M.B. Rhinovirus Attributes that Contribute to Asthma Development. Immunol Allergy Clin North Am 2019, 39, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Makris, S. Johnston, S. Recent advances in understanding rhinovirus immunity. F1000Res, 2018; 7, F1000 Faculty Rev-1537. [Google Scholar] [CrossRef]
- Santti, J. Hyypiä, T., Kinnunen, L., Salminen, M. Evidence of recombination among enteroviruses. J Virol 1999, 73, 8741–8749. [Google Scholar] [CrossRef] [PubMed]
- Savolainen, C. Laine, P., Mulders, M.N., Hovi, T. Sequence analysis of human rhinoviruses in the RNA-dependent RNA polymerase coding region reveals large within-species variation. J Gen Virol, 2004; 85, Pt 8, 2271–2277. [Google Scholar] [CrossRef]
- Arden, K.E. McErlean, P., Nissen, M.D., Sloots, T.P., Mackay, I.M. Frequent detection of human rhinoviruses, paramyxoviruses, coronaviruses, and bocavirus during acute respiratory tract infections. J Med Virol 2006, 78, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Ren, L. Yang, D., Ren, X., Li, M., Mu, X., Wang, Q., Cao, J., Hu, K., Yan, C., Fan, H., Li, X., Chen, Y., Wang, R., An, F., An, S., Luo, M., Wang, Y., Xiao, Y., … Wang, J. Genotyping of human rhinovirus in adult patients with acute respiratory infections identified predominant infections of genotype A21. Sci Rep 2017, 7, 41601. [Google Scholar] [CrossRef]
- Zhao, Y. Shen, J., Wu, B., Liu, G., Lu, R., Tan, W. Genotypic Diversity and Epidemiology of Human Rhinovirus Among Children With Severe Acute Respiratory Tract Infection in Shanghai, 2013-2015. Front Microbiol 2018, 9, 1836. [Google Scholar] [CrossRef] [PubMed]
- Baillie, V.L. Moore, D.P., Mathunjwa, A., Morailane, P., Simões, E.A.F., Madhi, S.A. Molecular Subtyping of Human Rhinovirus in Children from Three Sub-Saharan African Countries. J Clin Microbiol 2019, 57, e00723–19. [Google Scholar] [CrossRef] [PubMed]
- Luka, M.M. Kamau, E., Adema, I., Munywoki, P.K., Otieno, G.P., Gicheru, E., Gichuki, A., Kibinge, N., Agoti, C.N., Nokes, D.J. Molecular Epidemiology of Human Rhinovirus From 1-Year Surveillance Within a School Setting in Rural Coastal Kenya. Open Forum Infect Dis, 2020; 7, ofaa385. [Google Scholar] [CrossRef]
- da Costa Souza, L. Bello, E.J.M., Dos Santos, E.M., Nagata, T. Molecular and clinical characteristics related to rhinovirus infection in Brasília, Brazil. Braz J Microbiol 2021, 52, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Pandya, M.C. Callahan, S.M., Savchenko, K.G., Stobart, C.C. A Contemporary View of Respiratory Syncytial Virus (RSV) Biology and Strain-Specific Differences. Pathogens 2019, 8, 67. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, M.L. Calvo Rey, C., Del Rosal Rabes, T. Pediatric Asthma and Viral Infection. Asma y virus en el niño. Arch Bronconeumol, 2016; 52, 269–273. [Google Scholar] [CrossRef]
- Karron, R.A. Zar, H.J. Determining the outcomes of interventions to prevent respiratory syncytial virus disease in children: what to measure? Lancet Respir Med 2018, 6, 65–74. [Google Scholar] [CrossRef]
- Battles, M.B. McLellan, J.S. Respiratory syncytial virus entry and how to block it. Nat Rev Microbiol 2019, 17, 233–245. [Google Scholar] [CrossRef]
- Ruckwardt, T.J. Morabito, K.M., Graham, B.S. Immunological Lessons from Respiratory Syncytial Virus Vaccine Development. Immunity 2019, 51, 429–442. [Google Scholar] [CrossRef]
- Driscoll, A.J. Arshad, S.H., Bont, L., Brunwasser, S.M., Cherian, T., Englund, J.A., Fell, D.B., Hammitt, L.L., Hartert, T.V., Innis, B.L., Karron, R.A., Langley, G.E., Mulholland, E.K., Munywoki, P.K., Nair, H., Ortiz, J.R., Savitz, D.A., Scheltema, N.M., Simões, E.A.F., Smith, P.G., … Feikin, D.R. Does respiratory syncytial virus lower respiratory illness in early life cause recurrent wheeze of early childhood and asthma? Critical review of the evidence and guidance for future studies from a World Health Organization-sponsored meeting. Vaccine, 2020; 38, 2435–2448. [Google Scholar] [CrossRef]
- Bergeron, H.C. Tripp, R.A. Immunopathology of RSV: An Updated Review. Viruses, 2478. [Google Scholar] [CrossRef]
- Malinczak, C.A. Lukacs, N.W., Fonseca, W. Early-Life Respiratory Syncytial Virus Infection, Trained Immunity and Subsequent Pulmonary Diseases. Viruses 2020, 12, 505. [Google Scholar] [CrossRef]
- Nam, H.H. Ison, M.G. Respiratory syncytial virus infection in adults. Br Med J 2019, 366, l5021. [Google Scholar] [CrossRef]
- Liu, H. Lu, B., Tabor, D.E., Tovchigrechko, A., Wilkins, D., Jin, H., Madhi, S.A., Soofie, N., Esser, M.T., Nunes, M.C. Characterization of human respiratory syncytial virus (RSV) isolated from HIV-exposed-uninfected and HIV-unexposed infants in South Africa during 2015-2017. Influenza Other Respir Viruses, 2020; 14, 403–411. [Google Scholar] [CrossRef]
- 38. Bin Lu, Liu, H., Tabor, D.E., Tovchigrechko, A., Qi, Y., Ruzin, A., Esser, M.T., Jin, H. Emergence of new antigenic epitopes in the glycoproteins of human respiratory syncytial virus collected from a US surveillance study, 2015-17. Sci Rep, 2019; 9, 3898. [CrossRef]
- Yun, K.W. Choi, E.H., Lee, H.J. Molecular epidemiology of respiratory syncytial virus for 28 consecutive seasons (1990-2018) and genetic variability of the duplication region in the G gene of genotypes ON1 and BA in South Korea. Arch Virol, 2020; 165, 1069–1077. [Google Scholar] [CrossRef]
- Lau, S.K. Yip, C.C., Lin, A.W., Lee, R.A., So, L.Y., Lau, Y.L., Chan, K.H., Woo, P.C., Yuen, K.Y. Clinical and molecular epidemiology of human rhinovirus C in children and adults in Hong Kong reveals a possible distinct human rhinovirus C subgroup. J Infect Dis 2009, 200, 1096–1103. [Google Scholar] [CrossRef]
- Miller, E.K. Khuri-Bulos, N., Williams, J.V., Shehabi, A.A., Faouri, S., Al Jundi, I., Chen, Q., Heil, L., Mohamed, Y., Morin, L.L., Ali, A., Halasa, N.B. Human rhinovirus C associated with wheezing in hospitalised children in the Middle East. J Clin Virol 2009, 46, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, M.A. Tempia, S., Treurnicht, F.K., Walaza, S., Cohen, A.L., Moyes, J., Hellferscee, O., Variava, E., Dawood, H., Chhagan, M., Haffjee, S., Madhi, S.A., Cohen, C., Venter, M. Genetic diversity and molecular epidemiology of human rhinoviruses in South Africa. Influenza Other Respir Viruses 2014, 8, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Hung, H.M. Yang, S.L., Chen, C.J., Chiu, C.H., Kuo, C.Y., Huang, K.A., Lin, T.Y., Hsieh, Y.C., Gong, Y. N., Tsao, K.C., Huang, Y.C. Molecular epidemiology and clinical features of rhinovirus infections among hospitalized patients in a medical center in Taiwan. J Microbiol Immunol Infect 2019, 52, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Venter, M. Madhi, S.A., Tiemessen, C.T., Schoub, B.D. Genetic diversity and molecular epidemiology of respiratory syncytial virus over four consecutive seasons in South Africa: identification of new subgroup A and B genotypes. J Gen Virol 2001, 82 Pt 9, 2117–2124. [Google Scholar] [CrossRef] [PubMed]
- Robertson, S.E. Roca, A., Alonso, P., Simoes, E.A., Kartasasmita, C.B., Olaleye, D.O., Odaibo, G.N., Collinson, M., Venter, M., Zhu, Y., Wright, P.F. Respiratory syncytial virus infection: denominator-based studies in Indonesia, Mozambique, Nigeria and South Africa. Bull World Health Organ 2004, 82, 914–922. [Google Scholar]
- McMorrow, M.L. Tempia, S., Walaza, S., Treurnicht, F.K., Moyes, J., Cohen, A.L., Pretorius, M., Hellferscee, O., Wolter, N., von Gottberg, A., Nguweneza, A., McAnerney, J.M., Naby, F., Mekgoe, O., Venter, M., Madhi, S.A., Cohen, C. The Role of Human Immunodeficiency Virus in Influenza- and Respiratory Syncytial Virus-associated Hospitalizations in South African Children, 2011-2016. Clin Infect Dis 2019, 68, 773–780. [Google Scholar] [CrossRef]
- Xu, L. Gao, H., Zeng, J., Liu, J., Lu, C., Guan, X., Qian, S., Xie, Z. A fatal case associated with respiratory syncytial virus infection in a young child. BMC Infect Dis 2018, 18, 217. [Google Scholar] [CrossRef]
- Kubale, J. Kuan, G., Gresh, L., Ojeda, S., Azziz-Baumgartner, E., Sanchez, N., Lopez, R., Harris, E., Balmaseda, A., Gordon, A. Assessing the Incidence of Symptomatic Respiratory Syncytial Virus Illness Within a Prospective Birth Cohort in Managua, Nicaragua. Clin Infect Dis 2020, 70, 2029–2035. [Google Scholar] [CrossRef] [PubMed]
- Winterbach M, Hattingh C, Heathfield, LJ. Retrospective study of sudden unexpected death of infants in the Garden Route and Central Karoo districts of South Africa: Causes of death and epidemiological factors. S Afr J Child Health 2021, 15, 74–82. [Google Scholar] [CrossRef]
- la Grange, H. Respiratory Pathogens in Cases of Sudden Unexpected Death in Infancy (SUDI) at Tygerberg Forensic Pathology Service Mortuary. 2013. [Google Scholar]
- Luoto, R. Jartti, T., Ruuskanen, O., Waris, M., Lehtonen, L., Heikkinen, T. Review of the clinical significance of respiratory virus infections in newborn infants. Acta Paediatr 2016, 105, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Toizumi, M. Suzuki, M., Nguyen, H.A.T., Le, M.N., Ariyoshi, K., Moriuchi, H., Hashizume, M., Dang, D.A., Yoshida, L.M. Viral Acute Respiratory Illnesses in Young Infants Increase the Risk of Respiratory Readmission. Pediatr Infect Dis 2018, 37, 1217–1222. [Google Scholar] [CrossRef] [PubMed]
- Boonyaratanakornkit, J. Englund, J.A., Magaret, A.S., Bu, Y., Tielsch, J.M., Khatry, S.K., Katz, J., Kuypers, J., Shrestha, L., LeClerq, S.C., Steinhoff, M.C., Chu, H.Y. Primary and Repeated Respiratory Viral Infections Among Infants in Rural Nepal. J Pediatr Infect Dis Soc 2020, 9, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Dempers, J.J. Burger, E.H., Toit-Prinsloo, L.D., Verster, J. A South African Perspective. In: SIDS Sudden Infant and Early Childhood Death: The Past, the Present and the Future. Duncan, J.R., Byard, R.W., Eds. University of Adelaide Press: Adelaide, Australia, 2018. Chapter 17. [PubMed]
- Garstang, J. Watson, D., Pease, A., Ellis, C., Blair, P.S., Fleming, P. Improving engagement with services to prevent Sudden Unexpected Death in Infancy (SUDI) in families with children at risk of significant harm: A systematic review of evidence. Child Care Health Dev 2021, 47, 713–731. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.A. Ashworth, M.T., Risdon, R.A., Hartley, J.C., Malone, M., Sebire, N.J. The role of post-mortem investigations in determining the cause of sudden unexpected death in infancy. Arch Dis Child 2008, 93, 1048–1053. [Google Scholar] [CrossRef] [PubMed]
- la Grange, H. Verster, J., Dempers, J.J., de Beer, C. Review of immunological and virological aspects as contributory factors in Sudden Unexpected Death in Infancy (SUDI). For Sci Int 2014, 245, 12–16. [Google Scholar] [CrossRef]
- Dempers, J.J. Coldrey, J., Burger, E.H., Thompson, V., Wadee, S.A., Odendaal, H.J., Sens, M.A., Randall, B.B., Folkerth, R.D., Kinney, H.C., PASS Network. The Institution of a Standardized Investigation Protocol for Sudden Infant Death in the Eastern Metropole, Cape Town, South Africa. J Forensic Sci 2016, 61, 1508–1514. [Google Scholar] [CrossRef] [PubMed]
- du Toit-Prinsloo, L. Dempers, J., Verster, J., Hattingh, C., Nel, H., Brandt, V.D., Jordaan, J., Saayman, G. Toward a standardized investigation protocol in sudden unexpected deaths in infancy in South Africa: a multicenter study of medico-legal investigation procedures and outcomes. Forensic Sci Med Pathol 2013, 9, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Osei-Poku, G.K. Thomas, S., Mwananyanda, L., Lapidot, R., Elliott, P.A., Macleod, W.B., Somwe, S.W., Gill, C.J. A systematic review of the burden and risk factors of sudden infant death syndrome (SIDS) in Africa. J Glob Health 2021, 11, 04075. [Google Scholar] [CrossRef]
- Shipstone, R.A. Young, J., Kearney, L., Thompson, J.M.D. Applying a Social Exclusion Framework to Explore the Relationship Between Sudden Unexpected Deaths in Infancy (SUDI) and Social Vulnerability. Front Public Health, 5635. [Google Scholar] [CrossRef]
- Coiras, M.T. Aguilar, J.C., García, M.L., Casas, I., Pérez-Breña, P. Simultaneous detection of fourteen respiratory viruses in clinical specimens by two multiplex reverse transcription nested-PCR assays. J Med Virol 2004, 72, 484–495. [Google Scholar] [CrossRef]
- Slovic, A. Ivancic-Jelecki, J., Ljubin-Sternak, S., Galinović, G.M., Forcic, D. A molecular epidemiological study of human respiratory syncytial virus in Croatia, 2011-2014. Infect Genet Evol 2016, 44, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Venter, M. Collinson, M., Schoub, B.D. Molecular epidemiological analysis of community circulating respiratory syncytial virus in rural South Africa: Comparison of viruses and genotypes responsible for different disease manifestations. J Med Virol 2002, 68, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Fawkner-Corbett, D.W. Khoo, S.K., Duarte, C.M., Bezerra, P.G., Bochkov, Y.A., Gern, J.E., Le Souef, P.N., McNamara, P.S. Rhinovirus-C detection in children presenting with acute respiratory infection to hospital in Brazil. J Med Virol 2016, 88, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Daleno, C. Piralla, A., Scala, A., Senatore, L., Principi, N., Esposito, S. Phylogenetic analysis of human rhinovirus isolates collected from otherwise healthy children with community-acquired pneumonia during five successive years. PloS One 2013, 8, e80614. [Google Scholar] [CrossRef]
- Oluwasemowo, O.O. Nejo, Y.T., Abokede, J.O., Lawson, M., Motayo, B.O. Genotypes of rhinovirus detected among children in two communities of South-West Nigeria. Virus genes 2021, 57, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Haddad-Boubaker, S. Mefteh, K., Mejri, C., Bouaffsoun, A., El Moussi, A., Boutiba, I., Mnif, K., Slim, A., Kechrid, A., Smaoui, H. High genotypic diversity of Rhinoviruses obtained from Tunisian children with severe acute respiratory infection. J Infect Dev Ctries 2021, 15, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Li, W. Yu, B., Zhou, J., Wang, Y., Xue, B., Pan, J., Ran, Y., Yang, X., Wang, X., Yang, F., Li, H. Genetic diversity and epidemiology of human rhinovirus among children with severe acute respiratory tract infection in Guangzhou, China. Virol J 2021, 18, 174. [Google Scholar] [CrossRef] [PubMed]
- Panda, S. Mohakud, N.K., Panda, S., Kumar, S. Epidemiology and phylogenetic analysis of human rhinovirus/Enterovirus in Odisha, Eastern India. Indian J Med Microbiol 2019, 37, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Peltola, V. Waris, M., Osterback, R., Susi, P., Ruuskanen, O., Hyypiä, T. Rhinovirus transmission within families with children: incidence of symptomatic and asymptomatic infections. J Infect Dis 2008, 197, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Jia, R. Lu, L., Li, S., Liu, P., Xu, M., Cao, L., Su, L., Xu, J. Human rhinoviruses prevailed among children in the setting of wearing face masks in Shanghai, 2020. BMC Infect Dis 2022, 22, 253. [Google Scholar] [CrossRef] [PubMed]
- Zlateva, K.T. de Vries, J.J., Coenjaerts, F.E., van Loon, A.M., Verheij, T., Little, P., Butler, C.C., Goossens, H., Ieven, M., Claas, E.C., GRACE Study Group. Prolonged shedding of rhinovirus and re-infection in adults with respiratory tract illness. Eur Respir J 2014, 44, 169–177. [Google Scholar] [CrossRef]
- Prasetyo, A.A. Desyardi, M.N., Tanamas, J., Suradi, Reviono, Harsini, Kageyama, S., Chikumi, H., Shimizu, E. Respiratory viruses and torque teno virus in adults with acute respiratory infections. Intervirology 2015, 58, 57–68. [Google Scholar] [CrossRef]
- Kamau, E. Onyango, C.O., Otieno, G.P., Kiyuka, P.K., Agoti, C.N., Medley, G.F., Cane, P.A., Nokes, D.J., Munywoki, P.K. An Intensive, Active Surveillance Reveals Continuous Invasion and High Diversity of Rhinovirus in Households. J Infect Dis 2019, 219, 1049–1057. [Google Scholar] [CrossRef]
- Heathfield, L. Martin, L., Ramesar, R. A 5-year retrospective analysis of infant death at Salt River Mortuary, Cape Town. S Afr J Child Health 2020, 14, 148–154. [Google Scholar] [CrossRef]
- Baker, T. Schandl, C., Presnell, S.E., Madory, J., Nolte, F.S., Batalis, N. Use of an Automated Nested Multiplex Respiratory Pathogen PCR Panel Postmortem in the Pediatric Forensic Setting. J For Sci 2017, 62, 1223–1228. [Google Scholar] [CrossRef]
- L'Huillier, A.G. Kaiser, L., Petty, T.J., Kilowoko, M., Kyungu, E., Hongoa, P., Vieille, G., Turin, L., Genton, B., D'Acremont, V., Tapparel, C. Molecular Epidemiology of Human Rhinoviruses and Enteroviruses Highlights Their Diversity in Sub-Saharan Africa. Viruses 2015, 7, 6412–6423. [Google Scholar] [CrossRef]
- Annamalay, A.A. Lanaspa, M., Khoo, S.K., Madrid, L., Acácio, S., Zhang, G., Laing, I.A., Gern, J., Goldblatt, J., Bizzintino, J., Lehmann, D., Le Souëf, P.N., Bassat, Q. Rhinovirus species and clinical features in children hospitalised with pneumonia from Mozambique. Trop Med Int Health 2016, 21, 1171–1180. [Google Scholar] [CrossRef]
- Milanoi, S. Ongus, J.R., Gachara, G., Coldren, R., Bulimo, W. Serotype and genetic diversity of human rhinovirus strains that circulated in Kenya in 2008. Influenza Other Respir Viruses 2016, 10, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Morobe, J.M. Nyiro, J.U., Brand, S., Kamau, E., Gicheru, E., Eyase, F., Otieno, G.P., Munywoki, P.K., Agoti, C.N., Nokes, D.J. Human rhinovirus spatial-temporal epidemiology in rural coastal Kenya, 2015-2016, observed through outpatient surveillance. Wellcome Open Res 2019, 3, 128. [Google Scholar] [CrossRef]
- Basnet, S. Palmenberg, A.C., Gern, J.E. Rhinoviruses and Their Receptors. Chest 2019, 155, 1018–1025. [Google Scholar] [CrossRef]
- Lamborn, I.T. Su, H.C. Genetic determinants of host immunity against human rhinovirus infections. Hum Genet 2020, 139, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Tabor, D.E. Fernandes, F., Langedijk, A.C., Wilkins, D., Lebbink, R.J., Tovchigrechko, A., Ruzin, A., Kragten-Tabatabaie, L., Jin, H., Esser, M.T., Bont, L.J., Abram, M.E., INFORM-RSV Study Group. Global Molecular Epidemiology of Respiratory Syncytial Virus from the 2017-2018 INFORM-RSV Study. J Clin Microbiol 2020, 59, e01828–20. [Google Scholar] [CrossRef]
- A Al-Sharif, H. El-Kafrawy, S.A., Yousef, J.M., Kumosani, T.A., Kamal, M.A., Khathlan, N.A., Kaki, R.M., Alnajjar, A.A., Azhar, E.I. Dominance of the ON1 Genotype of RSV-A and BA9 Genotype of RSV-B in Respiratory Cases from Jeddah, Saudi Arabia. Genes 2020, 11, 1323. [Google Scholar] [CrossRef] [PubMed]
- Song, J. Wang, H., Shi, J., Cui, A., Huang, Y., Sun, L., Xiang, X., Ma, C., Yu, P., Yang, Z., Li, Q., Ng, T.I., Zhang, Y., Zhang, R., Xu, W. Emergence of BA9 genotype of human respiratory syncytial virus subgroup B in China from 2006 to 2014. Sci Rep 2017, 7, 16765. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A. Venter, M., Alexandra, R., Lewis, H., Kara, Y., Karshagen, W.F., Greef, M., Lassen, C. Respiratory syncytial virus associated illness in high-risk children and national characterisation of the circulating virus genotype in South Africa. J Clin Virol 2003, 27, 180–189. [Google Scholar] [CrossRef]
- van Niekerk, S. Venter, M. Replacement of previously circulating respiratory syncytial virus subtype B strains with the BA genotype in South Africa. J Virol 2011, 85, 8789–8797. [Google Scholar] [CrossRef]
- Ihling, C.M. Schnitzler, P., Heinrich, N., Mangu, C., Sudi, L., Souares, A., Gies, S., Sié, A., Coulibaly, B., Ouédraogo, A.T., Mordmüller, B., Held, J., Adegnika, A.A., Fernandes, J.F., Eckerle, I., May, J., Hogan, B., Eibach, D., Tabatabai, J. Molecular epidemiology of respiratory syncytial virus in children in sub-Saharan Africa. Trop Med Int Health 2021, 26, 810–822. [Google Scholar] [CrossRef] [PubMed]
- Pangesti, K.N.A. Abd El Ghany, M., Walsh, M.G., Kesson, A.M., Hill-Cawthorne, G.A. Molecular epidemiology of respiratory syncytial virus. Rev Med Virol 2018, 28, 10–1002. [Google Scholar] [CrossRef]
- Kang, H.M. Park, K.C., Park, J., Kil, H.R., Yang, E.A. Circulating Respiratory Syncytial Virus Genotypes and Genetic Variability of the G Gene during 2017 and 2018/2019 Seasonal Epidemics Isolated from Children with Lower Respiratory Tract Infections in Daejeon, Korea. Journal of Korean medical science 2020, 35, e422. [Google Scholar] [CrossRef]
- Korsun, N. Angelova, S., Trifonova, I., Voleva, S., Grigorova, I., Tzotcheva, I., Mileva, S., Alexiev, I., Perenovska, P. Predominance of ON1 and BA9 genotypes of respiratory syncytial virus (RSV) in Bulgaria, 2016-2018. J Med Virol 2021, 93, 3401–3411. [Google Scholar] [CrossRef] [PubMed]
- Razanajatovo Rahombanjanahary, N.H. Rybkina, K., Randriambolamanantsoa, T.H., Razafimanjato, H., Heraud, J.M. Genetic diversity and molecular epidemiology of respiratory syncytial virus circulated in Antananarivo, Madagascar, from 2011 to 2017: Predominance of ON1 and BA9 genotypes. J Clin Virol 2020, 129, 104506. [Google Scholar] [CrossRef]
- Wang, B. Song, J., Song, J., Mao, N., Liang, J., Chen, Y., Qi, Y., Bai, L., Xie, Z., Zhang, Y. An Outbreak of Severe Neonatal Pneumonia Caused by Human Respiratory Syncytial Virus BA9 in a Postpartum Care Centre in Shenyang, China. Microbiol Spectr 2022, 10, e0097422. [Google Scholar] [CrossRef]
- Valley-Omar, Z. Muloiwa, R., Hu, N.C., Eley, B., Hsiao, N.Y. Novel respiratory syncytial virus subtype ON1 among children, Cape Town, South Africa, 2012. Emerg Infect Dis 2013, 19, 668–670. [Google Scholar] [CrossRef]
- Tabatabai, J. Prifert, C., Pfeil, J., Grulich-Henn, J., Schnitzler, P. Novel respiratory syncytial virus (RSV) genotype ON1 predominates in Germany during winter season 2012-13. PloS One 2014, 9, e109191. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, F. Izadi, A., Yavarian, J., Sharifi-Zarchi, A., Salimi, V., Mokhtari-Azad, T. Determination of genetic characterization and circulation pattern of Respiratory Syncytial Virus (RSV) in children with a respiratory infection, Tehran, Iran, during 2018-2019. Virus Res 2021, 305, 198564. [Google Scholar] [CrossRef]
- Kenmoe, S. Vernet, M.A., Miszczak, F., Dina, J., Schoenhals, M., Beng, V.P., Vabret, A., Njouom, R. Genetic diversity of human respiratory syncytial virus isolated among children with acute respiratory infections in Southern Cameroon during three consecutive epidemic seasons, 2011-2013. Trop Med Health 2018, 46, 7. [Google Scholar] [CrossRef]
- Luo, H.J. Huang, X.B., Zhong, H.L., Ye, C.X., Tan, X., Zhou, K., Yuan, L., Zhang, S.F., Zhu, X., Lin, C.J., Wang, W.J., Xu, L., Cao, K.Y. Epidemiological characteristics and phylogenic analysis of human respiratory syncytial virus in patients with respiratory infections during 2011-2016 in southern China. Int J Infect Dis 2020, 90, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.Y. Fang, Y.P., Wang, L.C., Chou, T.Y., Liu, H.F. Genetic Diversity and Molecular Epidemiology of Circulating Respiratory Syncytial Virus in Central Taiwan, 2008-2017. Viruses 2021, 14, 32. [Google Scholar] [CrossRef] [PubMed]
- Auksornkitti, V. Kamprasert, N., Thongkomplew, S., Suwannakarn, K., Theamboonlers, A., Samransamruajkij, R., Poovorawan, Y. Molecular characterization of human respiratory syncytial virus, 2010-2011: identification of genotype ON1 and a new subgroup B genotype in Thailand. Arch Virol 2014, 159, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Etemadi, M.R. Sekawi, Z., Othman, N., Lye, M.S., Moghaddam, F.Y. Circulation of human respiratory syncytial virus strains among hospitalized children with acute lower respiratory infection in malaysia. Evol Bioinform Online 2013, 9, 151–161. [Google Scholar] [CrossRef]
- Ábrego, L.E. Delfraro, A., Franco, D., Castillo, J., Castillo, M., Moreno, B., López-Vergès, S., Pascale, J. M., Arbiza, J. Genetic variability of human respiratory syncytial virus group B in Panama reveals a novel genotype BA14. J Med Virol 2017, 89, 1734–1742. [Google Scholar] [CrossRef] [PubMed]
- Komoyo, G.F. Yambiyo, B.M., Manirakiza, A., Gody, J.C., Muller, C.P., Hübschen, J.M., Nakoune, E., Snoeck, C.J. Epidemiology and genetic characterization of respiratory syncytial virus in children with acute respiratory infections: Findings from the influenza sentinel surveillance network in Central African Republic, 2015 to 2018. Health Sci Rep 2021, 4, e298. [Google Scholar] [CrossRef]
- Raghuram S,V. Khan, W.H., Deeba, F., Sullender, W., Broor, S., Parveen, S. Retrospective phylogenetic analysis of circulating BA genotype of human respiratory syncytial virus with 60 bp duplication from New Delhi, India during 2007-2010. Virusdisease 2015, 26, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Bandla, S.S. Devadiga, S., Bhatt, R., Dsa, O.C., Govindakarnavar, A. Molecular epidemiology of respiratory syncytial virus among children and adults in India 2016 to 2018. Virus Genes 2021, 57, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Hindupur, A. Menon, T., Dhandapani, P. Genetic diversity of human respiratory syncytial virus in children with acute respiratory infections in Chennai, South India. Ind J Med Microbiol 2019, 37, 248–254. [Google Scholar] [CrossRef]
- Do, L.A.H. Wilm, A., van Doorn, H.R., Lam, H.M., Sim, S., Sukumaran, R., Tran, A.T., Nguyen, B.H., Tran, T.T.L., Tran, Q.H., Vo, Q.B., Dac, N.A.T., Trinh, H.N., Nguyen, T.T.H., Binh, B.T.L., Le, K., Nguyen, M.T., Thai, Q.T., Vo, T.V., Ngo, N.Q.M., … Hibberd, M.L. Direct whole-genome deep-sequencing of human respiratory syncytial virus A and B from Vietnamese children identifies distinct patterns of inter- and intra-host evolution. J Gen Virol 2015, 96, 3470–3483. [Google Scholar] [CrossRef]
- Thongpan, I. Mauleekoonphairoj, J., Vichiwattana, P., Korkong, S., Wasitthankasem, R., Vongpunsawad, S., Poovorawan, Y. Respiratory syncytial virus genotypes NA1, ON1, and BA9 are prevalent in Thailand, 2012-2015. PeerJ 2017, 5, e3970. [Google Scholar] [CrossRef]
- Jia, R. Lu, L., Su, L., Lin, Z., Gao, D., Lv, H., Xu, M., Liu, P., Cao, L., Xu, J. Resurgence of Respiratory Syncytial Virus Infection During COVID-19 Pandemic Among Children in Shanghai, China. Front Microbiol 2022, 13, 938372. [Google Scholar] [CrossRef]
Figure 1.
Phylogeny of HRV 5’UTR and capsid coding region sequences of samples from SUDI cases and reference sequences obtained from NCBI BLAST.
Figure 1.
Phylogeny of HRV 5’UTR and capsid coding region sequences of samples from SUDI cases and reference sequences obtained from NCBI BLAST.
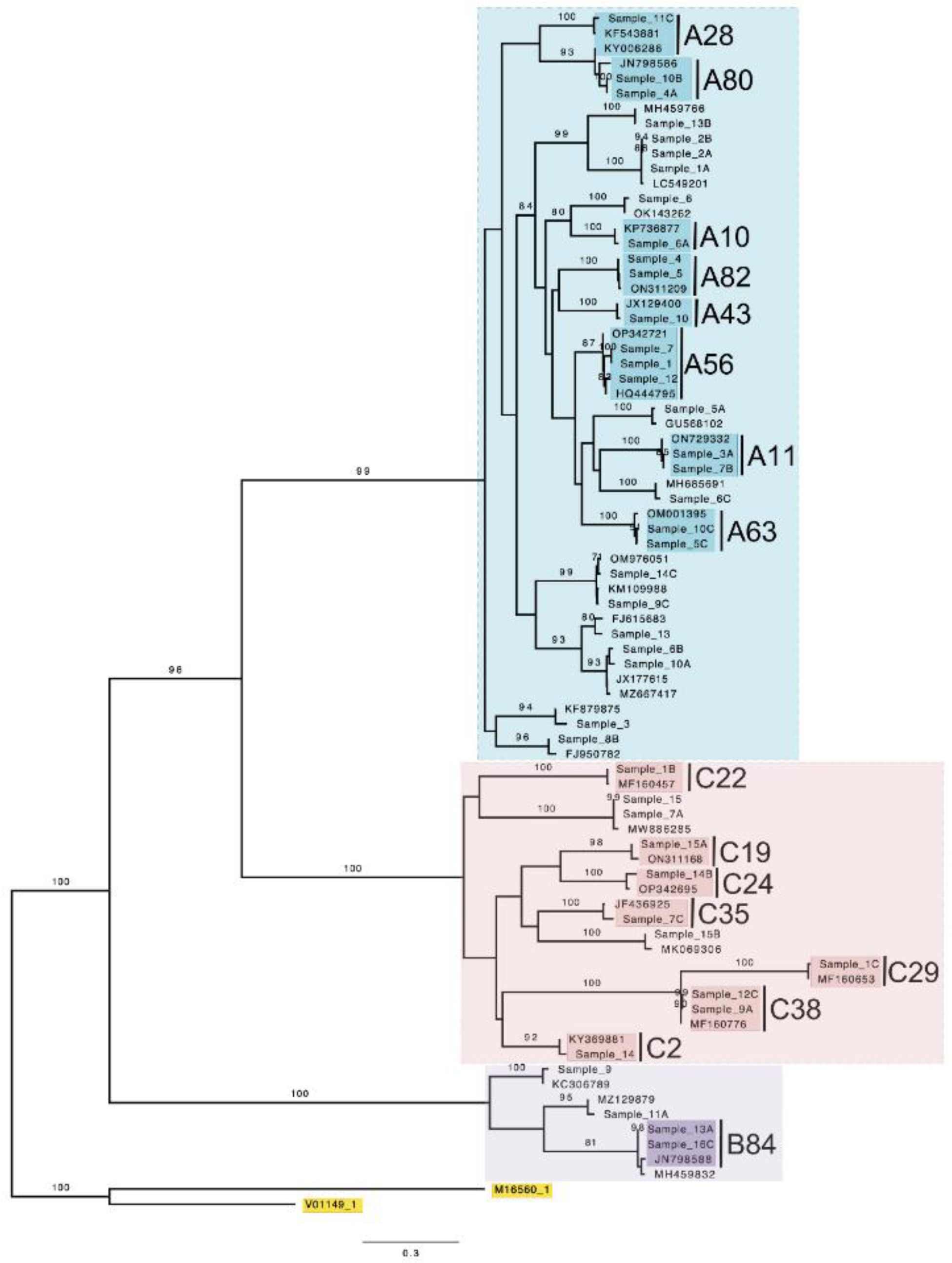
Figure 2.
Phylogeny of RSV G-gene sequences of samples from SUDI cases and reference sequences obtained from NCBI BLAST.
Figure 2.
Phylogeny of RSV G-gene sequences of samples from SUDI cases and reference sequences obtained from NCBI BLAST.
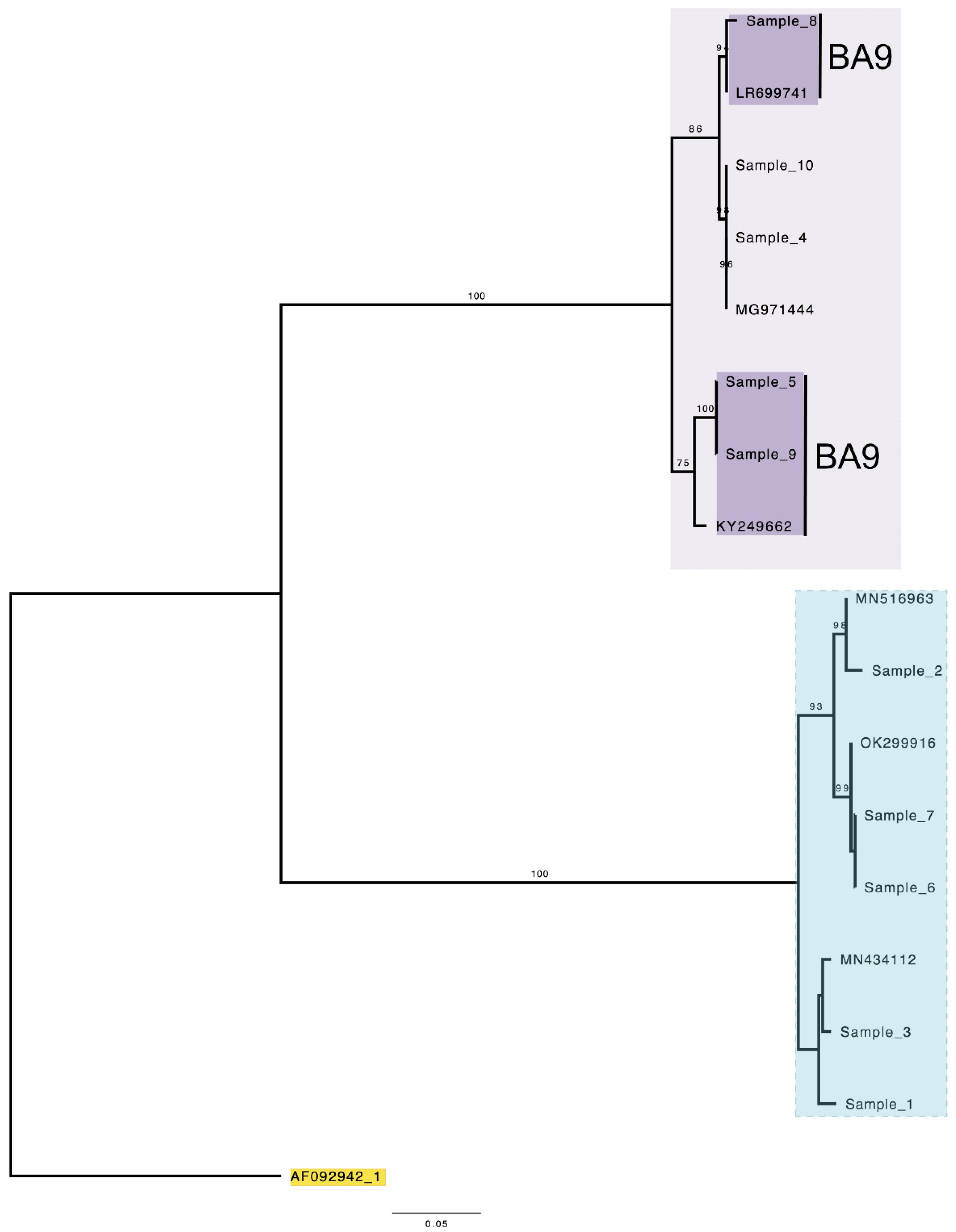
Figure 3.
Deduced amino acid alignment of RSV G-gene of RSV-A samples. Sample sequences were aligned and are shown relative to the sequence of RSV ON1 (Accession number: JN257693; ON67-1210A). The amino acid numbers of the sequence ruler (in blue) within the orange braces correspond to the positions of 212 and 321 of the second hypervariable region of the G-gene of the RSV ON1 sequence. The red outlined rectangular boxes depict the 23 amino acid duplication (QEETLHSTTSEGYLSPSQVYTTS) of the 24 amino acid insertion, characteristic to RSV ON1. Dots represent matching amino acid to reference sequence (RSV ON1). Dashes represent missing amino acid. Grey shading depicts predicted N-glycosylation sites.
Figure 3.
Deduced amino acid alignment of RSV G-gene of RSV-A samples. Sample sequences were aligned and are shown relative to the sequence of RSV ON1 (Accession number: JN257693; ON67-1210A). The amino acid numbers of the sequence ruler (in blue) within the orange braces correspond to the positions of 212 and 321 of the second hypervariable region of the G-gene of the RSV ON1 sequence. The red outlined rectangular boxes depict the 23 amino acid duplication (QEETLHSTTSEGYLSPSQVYTTS) of the 24 amino acid insertion, characteristic to RSV ON1. Dots represent matching amino acid to reference sequence (RSV ON1). Dashes represent missing amino acid. Grey shading depicts predicted N-glycosylation sites.
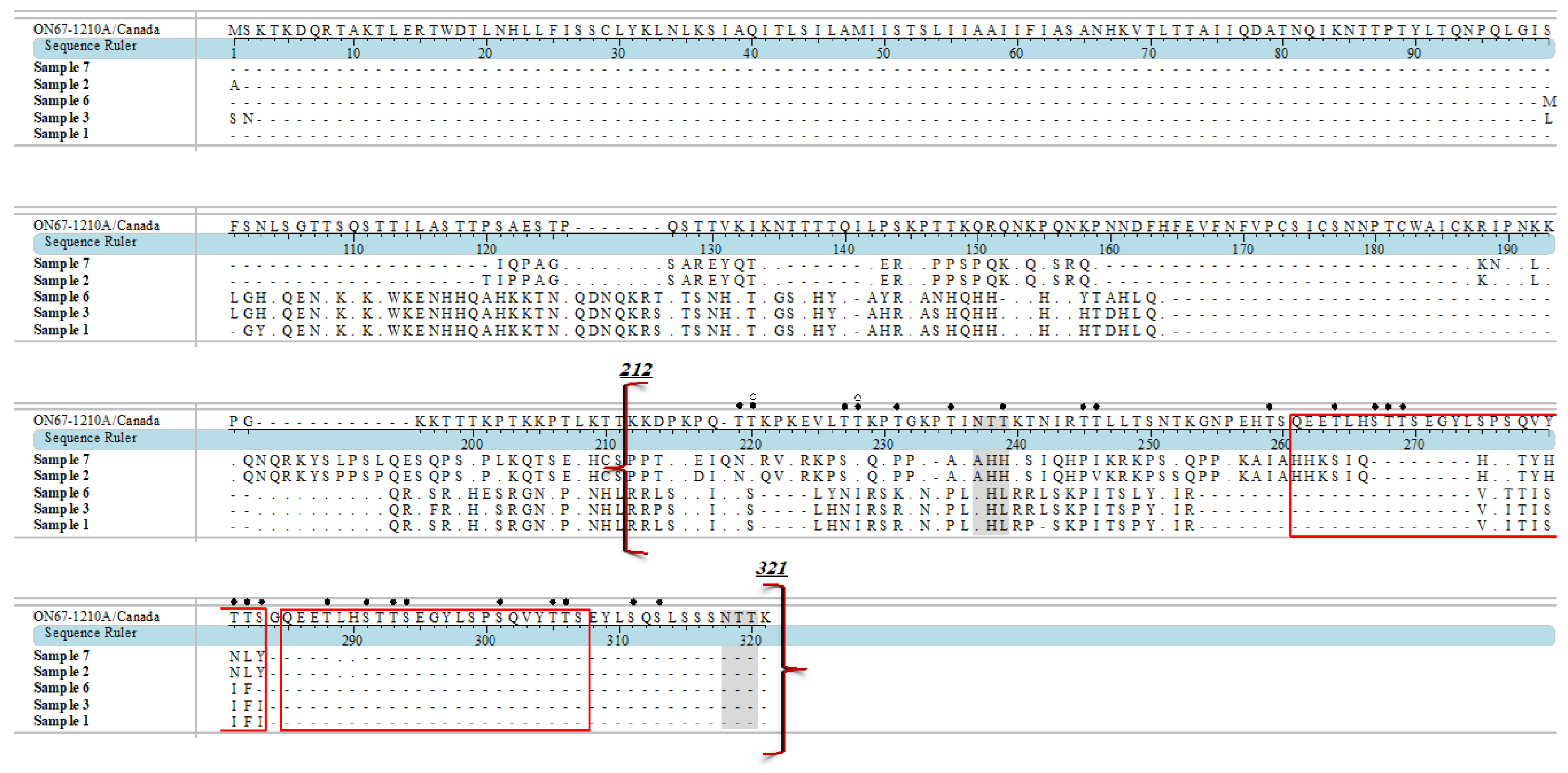
Figure 4.
Deduced amino acid alignments of RSV G-gene sequences of RSV-B sample. Samples sequences were aligned and are shown relative to sequence of prototype RSV-BA1 (Accession number: AY333364; BA/4128/99B) and BA9 (Accession number: DQ227395; BA/100/04). The amino acid numbers of the sequence ruler (in blue) within the orange braces correspond to the positions of 213 and 315 of the second hypervariable region of the G-gene of the RSV-BA1 sequence. The red outlined rectangular boxes depict the 20 amino acid duplication (TERDTSTSQSTVLDTTTSKH) insertion, characteristic to RSV-BA. Dots represent matching amino acid to reference sequence (RSV-BA1). Dashes represent missing amino acid. Grey shading depicts predicted N-glycosylation sites.
Figure 4.
Deduced amino acid alignments of RSV G-gene sequences of RSV-B sample. Samples sequences were aligned and are shown relative to sequence of prototype RSV-BA1 (Accession number: AY333364; BA/4128/99B) and BA9 (Accession number: DQ227395; BA/100/04). The amino acid numbers of the sequence ruler (in blue) within the orange braces correspond to the positions of 213 and 315 of the second hypervariable region of the G-gene of the RSV-BA1 sequence. The red outlined rectangular boxes depict the 20 amino acid duplication (TERDTSTSQSTVLDTTTSKH) insertion, characteristic to RSV-BA. Dots represent matching amino acid to reference sequence (RSV-BA1). Dashes represent missing amino acid. Grey shading depicts predicted N-glycosylation sites.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



