
Submitted:
04 March 2024
Posted:
04 March 2024
You are already at the latest version
Abstract
Depression is the commonest mental disorder worldwide. Both antidepressants and psychotherapy are effective in treating depression, but response to these treatments is often incomplete. Yoga-based interventions (YBIs) have emerged as a promising adjunctive treatment for depression. Recent research has attempted to identify the biological mechanisms associated with the antidepressant actions of YBIs. In this scoping review, conducted according to the PRISMA-ScR guidelines, the PubMed and Scopus databases were searched to retrieve research on biomarkers of response to YBIs in patients with depression. Eleven studies were included in the review. Based on these studies, YBIs may improve depression through beneficial effects on systemic inflammation, stress axis regulation, cardiac autonomic functioning, and possibly reductions in oxidative stress-related cellular damage. Increases in brain-derived neurotrophic factor (BDNF) may represent a final common pathway upon which these processes converge. Though these results are theoretically plausible, they should be interpreted with caution due to certain methodological limitations in the existing research. Replication of these results and improvements in study methodology, and the evaluation of other biomarkers relevant to the pathophysiology of depression, could further elucidate the mechanism of action of YBIs in this disorder, and identify which patients would benefit most from this treatment approach.
Keywords:
major depressive disorder
; yoga
; adjunctive treatment
; hypothalamic-pituitary-adrenal axis
; heart rate variability
; interleukin-6
; brain-derived neurotrophic factor
1. Introduction
Depressive disorders are one of the leading causes of morbidity and disability worldwide [1]. This group of disorders is characterized by persistent low mood with associated changes in cognition, behavior, and biological functions. It includes major depressive disorder (MDD), characterized by discrete episodes of a greater severity, and dysthymia, characterized by chronic, “low-grade” depressive symptoms [2]. It is estimated that at least 300 million people suffer from depressive disorders globally; in the year 2017 alone, it was estimated that there were around 250 million new cases or episodes of depression [3].
The treatment of depressive disorders usually involves pharmacological treatment with antidepressant medications and psychotherapies such as interpersonal therapy (IPT) and cognitive-behavioral therapy (CBT) [4]. Though these treatments are effective, there is a significant number of patients who do not respond to them. It is estimated that at least 30-40% of patients will not respond to initial treatment with antidepressants, and the likelihood of response to subsequent treatments is of a similar order [5,6,7,8]. Moreover, some patients who respond initially to medication may relapse despite continued treatment [9]. Psychotherapies have advantages over medication in terms of effectiveness, safety, and sustained response [10], but may not be readily available in low-resource settings [11]. There is significant heterogeneity within the group of depressive disorders, and patients with different symptom profiles may respond better to specific types of treatment or combinations of treatments [12].
The limitations of conventional monotherapies for depression were highlighted by a recent meta-analysis, which showed that combined therapies were superior both in terms of efficacy and of sustained improvement in symptoms of depression [13]. However, providing combined pharmacotherapy and psychotherapy poses its own challenges in terms of requirements in time, personnel, and infrastructure.
The increasing awareness of the limits of “conventional” treatment for depression has led to a renewed interest in complementary and alternative therapies. This term “complementary and alternative medicine” (CAM) or “integrative medicine” encompasses a wide range of interventions that fall outside the umbrella of “allopathic” medicine [14]. A wide range of CAM-based treatments have been tested in depression, but only a few have shown replicated evidence of efficacy [15,16]. Most of these treatments have been used as adjuncts to standard treatments, though some have been tried as monotherapies for milder forms of depression [17].
1.1. Yoga as a Treatment for Depression
Yoga is an ancient spiritual discipline originating from India. The word yoga is derived from a Sanskrit root meaning “union”, which refers to the aim of this discipline – to achieve union between individual and universal (divine) consciousness, and between mind and body [18]. Yoga is sometimes classed together with CAM or integrative therapies. Experts in the field emphasize that it is not primarily a “treatment” or an “intervention” for physical or mental illnesses; rather, it is a set of practices aimed at mind-body “oneness” or “integration” [19,20]. Nevertheless, some researchers have investigated the potential of yoga as a treatment for mental disorders, including depressive disorders. The first clinical trials in this field, conducted over two decades ago, found that yoga was effective in the treatment of both major depression and dysthymia, with an efficacy comparable to that of antidepressant monotherapy [21,22].
Subsequent studies have tended to confirm this result, with some caveats. A systematic review of yoga for depression, published in 2017, concluded that it did have positive effects that exceeded those of placebo. This review also identified significant methodological concerns in existing research, pertaining to study power, differences between monotherapy and combined therapy trials, and a lack of medium- or long-term results [23]. Based on these results, yoga has been recommended as a “first- or second-line CAM intervention” for depression in the Canadian Network for Mood and Anxiety Treatment’s guideline [24]. In contrast, the Indian Psychiatric Society’s guideline on depression has taken a more conservative position, highlighting the limitations of the existing data [25]. A more recent meta-analysis, published in 2023, found that yoga had a moderate effect on the reduction of depressive symptoms (effect size 0.6), and was well-tolerated by patients [26].
Results from the most recent published reports suggest that yoga, when used as an adjunct or “add-on” to treatment as usual (TAU), is both effective and cost-effective in the management of depressive episodes. Similar results have been observed in controlled trials from India [27,28] and from high-income European countries [29,30]. This suggests that yoga is an effective form of combination therapy for depression regardless of patients’ cultural backgrounds or beliefs.
1.2. The Therapeutic Potential of Biomarkers in Yoga Research for Depression
In spite of these promising results, the integration of yoga-based interventions (YBI) into depression care has been slow. In a review addressing this issue, published in 2019, Nauphal et al. concluded that this was due to methodological limitations [31]. They identified five questions that needed to be addressed by researchers before firm recommendations regarding yoga could be incorporated into standard practice. These questions can be briefly summarized as follows:
- Are specific types of YBI better than others in the treatment of depression?
- How often / for how long should YBI be used to achieve a meaningful response?
- Are there any adverse effects associated with the use of YBIs in depression?
- How do YBIs synergize with “standard” treatments for depression?
- What are the barriers and challenges in accessing YBIs for patients in diverse settings?
To some extent, these questions are being answered by recent research. For example, there is now more evidence on the combination of YBIs with standard therapy than there was in 2019 [27,28,29,30,32,33], and we know that a wide range of YBIs show comparable efficacy in depression, including hatha yoga, Sudharshan Kriya Yoga (SKY), body-oriented yoga, mindful yoga, and even yoga packages developed specifically for depression [32,33,34].
Despite these advances, there is an unanswered, sixth question that remains to be addressed in this field: what are the molecular and cellular processes associated with response to yoga in depression? Depression is a complex syndrome associated with alterations in central nervous, autonomic, neuroendocrine, immune-inflammatory, and gut-brain axis functioning [35]. The disciplines that constitute yoga can be broadly divided into four components: physical movements (asana), relaxation (savasana), breathing techniques (pranayama), and meditative techniques (dhyana) [36]. All these techniques can potentially exert beneficial effects on pathways implicated in the pathogenesis of depression. For example, relaxation and breathing techniques may ameliorate the autonomic dysfunction or neuroendocrine dysregulation seen in depression, while meditation may have positive effects on higher brain regions, such as the dorsolateral prefrontal cortices. There is a need to understand and characterize these mechanisms, so that improvements in symptoms can be correlated with underlying physiological and biochemical changes [37]. Understanding these changes at the molecular, cellular and organ level would have three key benefits: [38]
- A better understanding of the biological correlates of symptom improvement in depression
- A more evidence-based approach to YBI, facilitating a rapprochement between yoga practitioners and practitioners of modern medicine, thereby avoiding the extremes of skepticism and unrealistic claims [25]
- A personalized approach to the use of YBI in depression, through the identification of those patients who would respond best to them
In other words, what is required is a careful study of biomarkers associated with response to yoga-based interventions in depression. A biomarker has been defined by the United States Food and Drug Administration (FDA) and National Institutes of Health (NIH) Biomarker Working Group as “A defined characteristic that is measured as an indicator of normal biological processes, pathogenic processes or responses to an exposure or intervention” [39]. Biomarkers are measures based on “molecular, histologic, radiographic or physiologic characteristics,” and are distinct from measures of an individual’s emotions, behavior, or performance on a given test [40]. They are objective measures of cellular, organ or system function that can be correlated with changes in self- or clinician-rated (subjective) status. In the past decade, several promising leads have emerged regarding biomarkers of response to yoga-based treatments for depression. The purpose of this review is to summarize this work, critically analyze it and examine its implications for the treatment of depression.
2. Review Process
The objective of the current paper is to review existing studies of potential biomarkers associated with response to adjunctive YBI in patients with depression. Due to the heterogeneity of the available research, a scoping review methodology was adopted based on the PRISMA-ScR guidelines [41].
For this review, the PubMed and Scopus databases were searched for relevant papers using the following search terms: (“major depression” OR “depressive episode” OR “major depressive episode” OR “depressive disorder” OR “major depressive disorder” OR “recurrent depressive disorder” OR “dysthymia”) AND (“yoga” OR “hatha yoga” OR “yoga-based intervention” OR “yoga-based therapy” OR “yoga therapy”). One further study was identified through the reference lists of the retrieved citations. Out of a total of 495 citations screened, eleven relevant studies were included in the review. Studies were selected if they fulfilled the following criteria:
- Clinical trials in patients with depression, defined as major depressive disorder or dysthymia
- No primary medical comorbidity, such as diabetes mellitus, cancer, or cardiovascular disease
- Use of a yoga-based intervention as an adjunct or add-on to standard treatment or “treatment as usual”
- Measurement of one or more biomarkers at baseline and/or during treatment
- Papers published in English
Biomarkers were identified based on the FDA-NIH criteria [39]. The decision to focus on adjunctive YBI was made because yoga-based therapies are generally used, and recommended in certain guidelines, as adjuncts and not as monotherapy. Moreover, the number of biomarker studies of yoga monotherapy in depression was too small (n = 6) for a meaningful review. These studies will be discussed in the analysis of the review findings (Section 4.4). A PRISMA-ScR flow diagram depicting the review process is provided below (Figure 1):
Data from the eleven papers was extracted and tabulated under the following headings
- Study sample characteristics: country of origin, setting, sample size
- Clinical diagnosis, including any comorbidities if documented
- Treatment(s) received in addition to YBI, if specified
- YBI characteristics: type of YBI, number of sessions
- Biomarkers measures
- Study results, both positive and negative, in terms of changes in biomarkers and/or associations between biomarkers and treatment response.
3. Review Findings
3.1. Characteristics of the Included Studies
Eleven studies of adjunctive yoga-based interventions were included in this review [44,45,46,47,48,49,50,51,52,53,54]. Details of each study are provided in Table 1. All these reports involved patients with major depression; there were no biomarker studies pertaining to adjunctive yoga in dysthymia. Of these studies, three involved secondary analyses of data from earlier trials [45,48,52]. Thus, effectively, the available data was based on eight clinical trials involving a total of 326 patients.
Ten of the eleven studies involved patients with a confirmed diagnosis of major depressive disorder (MDD) as per the American Psychiatric Association’s Diagnostic and Statistical Manual for Mental Disorders, fourth edition (DSM-IV), based on structured clinical interviews. The remaining study involved patients with either anxiety or depressive disorders as per DSM-IV criteria, but was included in the review as all participants had significant depressive symptoms [49]. Eight of the studies originated from India, and seven of these eight reports were from a single center. The remaining three studies were from Germany [47], Italy [49] and the United States of America [53] respectively.
3.2. Methodological Concerns
The mean BIOCROSS score for the papers included in this study was 14.7 ± 2.7, indicating a generally acceptable methodological quality. The lowest score obtained was 11 (out of a maximum of 20) [44] and the highest was 19 [47]. Studies obtained high mean scores on assessments of study hypothesis (1.7 of a maximum of 2), sample selection and reporting of participant characteristics (1.6), and description of the biomarkers measured (1.6). The lowest scores were obtained for limitations (1.2) and statistical modeling of biomarker changes in relation to clinical response (1.2).
Another way of evaluating the latter number is that 6 of the 11 studies did not directly model the clinical-biomarker relationship, and one reported only a temporal correlation but no statistical association. In other words, most studies described their rationale in clear and logical terms, and included clear-cut “cases” of depression representative of those seen in out-patient clinic settings. However, they had deficiencies in terms of statistical analysis and of emphasizing study strengths and positive findings without fully acknowledging limitations.
Study sample sizes were low (mean 40.5 ± 16.9 participants, range 22-84), and none of the reports included a formal sample size estimation, raising the possibility that some of this research may have been statistically underpowered.
3.3. Biomarker and Treatment Characteristics
A wide range of biomarkers were studied in relation to adjunctive yoga in the existing literature. The most frequently assessed parameters were immune-inflammatory markers [50,53,54] and measures of autonomic function [45,49,52]. Other markers that were assessed included brain-derived neurotrophic factor (BDNF) [46,50], measures of hypothalamic-pituitary-adrenal (HPA) axis functioning [47,48], measures of cellular aging, oxidative stress and DNA damage [50], and electroencephalographic (EEG) alpha activity [44]. Two studies examined the relationship between multiple biomarkers [48,50]. In all studies, these parameters were estimated longitudinally, both at baseline and following treatment.
The type and duration of yoga-based interventions varied significantly across studies. Techniques used included Sahaj yoga meditation [44,45], Hatha yoga [47,53], a depression-specific yoga module developed by experts [46,48,51,52,54], Sudarshan Kriya yoga [49] and a yoga- and meditation-based lifestyle intervention [50]. The duration of treatment ranged from 2 to 12 weeks, though most studies provided yoga-based interventions for 8-12 weeks.
Concurrent treatments are an important confounder in studies of adjunctive treatment. Ten of the eleven studies included patients with antidepressants “as usual”, meaning that they were allowed to continue stable doses of antidepressant treatment in a naturalistic manner. One study attempted to standardize pharmacological treatment by randomizing participants to receive either the antidepressant escitalopram (10 mg/day) or the atypical antipsychotic quetiapine (300 mg/day) [47]. In ten of the studies, adjunctive yoga was compared to pharmacotherapy alone, which served as the control group. In a single report from the United States, the control group received an educational intervention on lifestyle modification in addition to medication [53].
3.3. Changes in Biomarkers related to Yoga-Based Intervention
The body of research included in this review yielded mixed results in terms of changes in specific biomarkers related to yoga-based interventions. Six studies reported unequivocal positive findings that were specific to the yoga arm [48,49,50,51,53,54], four reported no significant differences between yoga and control groups [44,45,46,47], and one reported a trend towards a significant difference in favor of yoga [52]. There was an apparent time trend in the reporting of positive results; studies published in 2007-2014 yielded negative results, while those published in 2016-2021 tended to report positive findings.
3.3.1. Immune-Inflammatory Markers
All three studies examining immune-inflammatory markers reported at least one significant change in patients receiving adjunctive yoga. Two studies reported significant decreases in the pro-inflammatory cytokine interleukin-6 (IL-6) after 10-12 weeks of yoga-based intervention, compared to either treatment as usual [50] or a lifestyle modification intervention [53]. The third found significant reduction in three components of the complement pathway (C1q, Factor H and properdin) after 12 weeks of yoga-based intervention [54]. On the other hand, yoga-based intervention did not significantly reduce levels of tumor necrosis factor alpha (TNF-α) or the inflammatory marker C-reactive protein (CRP) after 10 weeks of treatment [53].
3.3.2. Autonomic Markers
A single study evaluated general autonomic markers (pulse rate, respiratory rate and galvanic skin response) in patients with depression receiving adjunctive Sahaj yoga, but did not find any significant changes post-treatment [45]. A study of Sudarshan Kriya yoga given for 2 weeks found beneficial effects on cardiac autonomic parameters, suggestive of improved parasympathetic modulation of cardiac functioning [49]. However, a longer study of a depression-specific yoga module found only a trend in favour of improved cardiac autonomic function (improved low- to high-frequency ratio) after 12 weeks of treatment [52].
3.3.3. Other Biomarkers
Two studies evaluated changes in BDNF following adjunctive yoga-based treatment. Both found significant changes post-yoga [46,50], but one also found a significant change in the control group [46]. Two studies examined measures of HPA axis functioning. In the first, there was no effect of adjunctive yoga on cortisol responsiveness to dexamethasone (DEX) and corticotropin-releasing hormone (CRH) [47]; in the second, yoga was associated with a significant reduction in serum cortisol post-treatment [48]. In the latter report, a significant negative correlation was observed between changes in serum BDNF, as reported earlier in [46], and serum cortisol.
Other biomarkers found to be significantly associated with yoga-based interventions in single studies include a measure of cortical inhibition - the cortical silent period, as measured by transcranial magnetic stimulation [51], and serum markers of oxidative stress, DNA damage and cellular aging [50]. In a sole report, adjunctive yoga was not associated with changes in EEG alpha activity despite symptomatic improvement [44].
3.4. Relationship between Changes in Biomarkers and Clinical Improvement
As noted in section 3.2, only four studies formally modelled associations between changes in putative biomarkers of response to adjunctive yoga and clinical improvement, defined as reduction in scores on a standardized rating scale for depressive symptoms [46,47,50,54]. Changes in serum BDNF were correlated with symptomatic improvement in the yoga group, but not the control group, in two studies [46,50]; it should be noted that in the first of these studies, BDNF increased in both the study and the control groups. Changes in cortisol responses to DEX/CRH were associated with improvement in depressive symptoms regardless of treatment received [47]. Changes in complement components were not correlated with improvements in depressive symptoms after 12 weeks of a yoga-based module [54]. Apart from these results, a fifth study reported a temporal association between improvements in cardiac parasympathetic modulation and depressive symptoms in patients receiving yoga, but did not formally analyze this association [49].
4. Critical Analysis of the Review Findings
Yoga-based interventions (YBI) are an emerging option for the treatment of depression. There has been a significant growth of research in this field, with most published studies showing that adjunctive YBI outperforms patients receiving treatment as usual, and is well-tolerated. However, the mechanisms through which YBIs exert their beneficial effects on depression are being elucidated only now. The purpose of the current review was to provide an overview of biomarker research in patients receiving adjunctive YBI for depression.
4.1. Pathophysiological Significance of Biomarker Results in Studies of YBI for Depression
Based on the available data, it can be tentatively stated that adjunctive YBIs produce significant reductions in specific immune-inflammatory markers (IL-6 and the complement components C1q, factor H and properdin), and are tentatively associated with increases in serum BDNF and improvements in cardiac autonomic parameters. YBIs may also be associated with an increase in the cortical silent period, with a decrease in markers of oxidative stress, DNA damage, and cellular aging, and with reduced serum cortisol.
Though all these results require replication, they are significant because they align in a coherent manner with our existing knowledge of the pathophysiology of depression. Depression is increasingly being viewed as a disorder linked to both peripheral and central nervous system inflammation. Patients with MDD have elevated serum levels of pro-inflammatory molecules such as CRP and IL-6 [55,56]. These peripheral inflammatory changes are linked to stress-related dysregulation of the HPA axis, which manifests as alterations in cortisol responsiveness [57,58]. Peripheral inflammation is in turn associated with, neuroinflammation and reduced neuroplasticity, which is associated with reduced levels of BDNF [59,60]. There is a bidirectional relationship between inflammation and measures of oxidative stress, which are elevated in patients with MDD [61]. More recent research has also established an association between MDD and elevated levels of complement C1q and factor H [62,63]. Brain imaging studies have also found evidence of reduced central gamma-amino butyric acid (GABA) levels in depression, resulting in reduced GABAB receptor activation; this would result in a shorter cortical silent period on magnetic stimulation [64,65]. There is also a substantial body of literature linking depression to reduced heart rate variability, which is though to reflect cardiac autonomic dysfunction arising from an imbalance between sympathetic and parasympathetic nervous activity [66].
There is evidence in human subjects without depression – both healthy volunteers and those with medical illnesses – that yoga does exert beneficial effects on the aforementioned processes [67,68,69,70,71]. Thus, it is – at the very least – biologically plausible to consider that YBIs may ameliorate not only depression, but the medical conditions often comorbid with it, through its moderating effects on multiple physiological and biochemical pathways. More remains to be learned about the relationships between depression and novel biomarkers such as sirtuin-1, which appear to be sensitive to YBI and have been implicated in translational models of depression [72].
4.2. Correlation or Causation?
The key question to be considered when appraising the results of biomarker studies is whether changes in biomarkers are meaningfully associated with changes in the patient’s symptomatic status. Stated in simple terms, it is necessary not just to show that yoga changes levels of certain well-defined markers, but that these changes correlate with reductions in depressive symptoms. The majority (7 of 11) of the papers included in this review reported significant changes in one or more biomarkers. Yet, only a minority (4 of 11) of papers sought to establish a causal connection between changes in biomarkers and symptomatic improvement. The results of these studies suggest that the response to adjunctive YBI is correlated with increases in serum BDNF, while changes in complement components are not correlated with symptom improvement.
BDNF is a neurotrophic factor that plays a key role in hippocampal neurogenesis and neural plasticity in the adult brain. Neuroinflammation can result in reduced BDNF and impaired plasticity, leading some experts to consider BDNF a “bridge” between immune-inflammatory processes and neural plasticity [73]. Increases in serum BDNF have been associated with response to several forms of effective treatment in depression, including antidepressants, ketamine, combined medication and psychotherapy, and electroconvulsive therapy [74,75,76,77]. Thus, changes in BDNF may represent a “final common pathway” through which various anti-depressive treatments work, though their proximal mechanisms of action may differ. In the case of YBIs, one of these proximal mechanisms may involve reductions in serum cortisol, which were negatively correlated with changes in BDNF in one study [48]. This is consistent with what is known about the inverse relationship between stress-induced increases in cortisol and BDNF levels [57,59].
The existing evidence cannot confirm a causal link between changes in cardiac autonomic activity or cytokine levels and response to depression in patients receiving adjunctive YBI. Yet, the temporal associations observed in the existing research, as well as their biological plausibility (see section 4.1), suggest that such mechanisms may well play a role in the effects of YBI on depression. This possibility can be confirmed through better statistical modeling, such as comparison of biomarker changes in responders and non-responders to YBI.
4.3. Specificity of Biomarkers of Response to YBI in Depression
A question that flows naturally from the preceding discussion is whether the changes in biomarkers observed in response to YBI are specific to it, or whether they accompany response to other forms of treatment for depression. In some of the included studies, changes in biomarkers appear to be non-specific: for example, changes in cortisol responsiveness were linked to improvements in depression regardless of whether patients received YBI or not [47]. In others, there were hints of yoga-specific effects: for example, yoga, but not lifestyle modification, was associated with reductions in IL-6 [53]. Likewise, though BDNF was found to be increased both in the YBI and control groups, a correlation between changes in BDNF and depressive symptoms was seen only in the YBI group [46]. A study of complement components found that there were distinct changes in the plasma levels of specific components in the YBI and control groups, though their significance remains unclear [54]. Given that “conventional” antidepressants may also reduce levels of pro-inflammatory cytokines, a firm conclusion cannot be reached at this point [78]. Nevertheless, it is possible that YBIs may exert additional or synergistic effects on these pathways in patients not responding to treatment as usual; they may be “adjunctive” not just clinically but biologically. It is also possible that YBIs may have beneficial effects on specific symptom domains in depression, such as cognitive impairments or anxiety, which correlate with changes in these pathways [49,79].
4.4. Comparison with Studies of Yoga Monotherapy for Depression
It is instructive, at this point, to compare the research on adjunctive YBIs with the few available studies that have measured biomarkers of response to YBI monotherapy in depression [80,81,82,83,84,85]. This research was retrieved using the same process described in Section 2, and is summarized in Table 2 below.
The results of these studies reveal a certain overlap with those involving adjunctive YBIs. More specifically, YBI monotherapy has also been associated with significant increases in BDNF [85], and baseline cardiac autonomic function appeared to predict a good response to this type of treatment [82]. The positive findings related to P300 amplitude and changes in brain GABA levels [80,84] appear to align with the findings of improved GABAB activity in patients receiving adjunctive YBI, as evidenced by an increased cortical silent period [51]. These similarities suggest that these particular pathways warrant further attention in future biomarker research involving patients receiving YBIs for depression.
A summary of the possible mechanisms through which YBIs may act in depression, based on existing biomarker research, is provided in Figure 2.
4.5. Methodological Concerns and Limitations
Certain limitations of the existing evidence should be kept in mind when appraising these results. First, most significant findings have been reported in only one or two studies, and all these results require replication. Second, most of the results are derived from secondary analyses of clinical trial data. This has several inherent limitations, the most important of which is the likelihood of false-positive findings [86,87]. Third, most studies did not adequately evaluate the association between biomarker changes and clinical outcomes. Fourth, most of the relevant data was reported from a single center and country, which may lead to limitations in generalizability. Fifth, as most studies used different YBI modules or packages, it is not certain if specific yoga techniques are particularly associated with changes in specific biomarkers (e.g., pranayama with autonomic parameters, or meditation with changes in cortical functioning). Sixth, certain biomarkers that are strongly associated with depression, such as alterations in regional brain functioning and measures of gut-brain axis dysfunction, have not yet been studied in relation to YBIs. Finally, some of the published reports may have been underpowered, leading to a risk of false-negative results.
The limitations of this review should also be acknowledged. First, due to the heterogeneity of methods and outcomes, a formal systematic review or meta-analysis could not be carried out. Second, as only papers written in English were included, it is possible that relevant trials of YBIs written in other languages may have been omitted. Third, the study relied on citations retrieved from databases of biomedical research, in which studies of yoga may have been under-represented. Finally, it is possible that YBIs may improve depression through as yet unidentified biological mechanisms that were not considered in this review.
5. Conclusions
The available evidence implicates several biological pathways, particularly immune-inflammatory networks, cardiac autonomic regulation, and oxidative stress, in the beneficial effects of adjunctive yoga-based interventions for patients with depression. Though much of this evidence is provisional, it is biologically plausible and consistent with current models of the neurobiology of depressive disorder. Further research involving larger samples and more rigorous statistical methods could deepen our understanding of the processes involved in the therapeutic benefits of yoga, and identify subsets of patients with depression – for example, those with prominent symptoms of anxiety and evidence of autonomic dysfunction – who would respond best to this form of treatment. The findings of this review could also provide leads to researchers seeking to isolate the biological changes associated with specific yoga techniques in patients with depression. Ultimately, this would lead to personalized and optimized treatment options for patients with this chronic and disabling disorder.
Author Contributions
Conceptualization, methodology, formal analysis, investigation, data curation, writing and editing – R.P.R.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No original data was generated for the purpose of this review.
Conflicts of Interest
The author declares no conflict of interest.
References
- Kessler, R. C. The costs of depression. Psychiatr Clin North Am 2012, 35, 1–14. [Google Scholar] [CrossRef]
- Uher, R.; Payne, J. L.; Pavlova, B.; Perlis, R. H. (2014). Major depressive disorder in DSM-5: implications for clinical practice and research of changes from DSM-IV. Depress Anxiety 2014, 31, 459–471. [Google Scholar] [CrossRef]
- Liu, Q.; He, H.; Yang, J.; Feng, X.; Zhao, F.; Lyu, J. Changes in the global burden of depression from 1990 to 2017: Findings from the Global Burden of Disease study. J Psychiatr Res 2020, 126, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, S.; McLean, L.; Fritz, K.; Lampe, L.; Malhi, G. S. Getting depression clinical practice guidelines right: time for change?. Acta Psychiatr Scand Suppl 2013, 444, 24–30. [Google Scholar] [CrossRef] [PubMed]
- de Silva, V. A.; Hanwella, R. Efficacy and tolerability of venlafaxine versus specific serotonin reuptake inhibitors in treatment of major depressive disorder: a meta-analysis of published studies. Int Clin Psychopharmacol 2012, 27, 8–16. [Google Scholar] [CrossRef]
- Rush, A. J., Trivedi, M., Fava, M., Thase, M., Wisniewski, S. The STAR*D Data Remain Strong: Reply to Pigott et al. Am J Psychiatry 2023, 180, 919–920. [CrossRef]
- Sakurai, H.; Noma, H.; Watanabe, K.; Uchida, H.; Furukawa, T. A. Cumulative remission rate after sequential treatments in depression: reappraisal of the STAR*D trial data. World Psychiatry 2024, 23, 156–157. [Google Scholar] [CrossRef]
- Pigott, H. E.; Kim, T.; Xu, C.; Kirsch, I.; Amsterdam, J. What are the treatment remission, response and extent of improvement rates after up to four trials of antidepressant therapies in real-world depressed patients? A reanalysis of the STAR*D study's patient-level data with fidelity to the original research protocol. BMJ open 2023, 13, e063095. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, S. N. Why antidepressants are not antidepressants: STEP-BD, STAR*D, and the return of neurotic depression. Bipolar Disord 2008, 10, 957–968. [Google Scholar] [CrossRef]
- Chen, C.; Shan, W. Pharmacological and non-pharmacological treatments for major depressive disorder in adults: A systematic review and network meta-analysis. Psychiatry Res 2019, 281, 112595. [Google Scholar] [CrossRef]
- Levy, L. B..; O'Hara, M. W. Psychotherapeutic interventions for depressed, low-income women: a review of the literature. Clin Psychol Rev 2010, 30, 934–950. [Google Scholar] [CrossRef]
- Ghaemi, S. N.; Vöhringer, P. A.; Vergne, D. E. (2012). The varieties of depressive experience: diagnosing mood disorders. The Psychiatr Clin North Am, 35, 73–86. [CrossRef]
- Furukawa, T. A.; Shinohara, K.; Sahker, E.; Karyotaki, E.; Miguel, C.; Ciharova, M.; Bockting, C. L. H.; Breedvelt, J. J. F.; Tajika, A.; Imai, H.; Ostinelli, E. G.; Sakata, M.; Toyomoto, R.;…; Cuijpers, P. Initial treatment choices to achieve sustained response in major depression: a systematic review and network meta-analysis. World Psychiatry 2021, 20, 387–396. [CrossRef]
- Warnick, S. J.; Mehdi, L.; Kowalkowski, J. Wait-there's evidence for that? Integrative medicine treatments for major depressive disorder. Int J Psychiatry Med 2021, 56, 334–343. [Google Scholar] [CrossRef]
- Asher, G. N.; Gartlehner, G.; Gaynes, B. N.; Amick, H. R.; Forneris, C.; Morgan, L. C.; Coker-Schwimmer, E; Boland, E.; Lux, L. J.; Gaylord, S.; Bann, C.; Pierl, C. B.; Lohr, K. N. Comparative Benefits and Harms of Complementary and Alternative Medicine Therapies for Initial Treatment of Major Depressive Disorder: Systematic Review and Meta-Analysis. J Altern Complement Med 2017, 23, 907–919. [Google Scholar] [CrossRef] [PubMed]
- Ng, J. Y.; Nazir, Z.; Nault, H. Complementary and alternative medicine recommendations for depression: a systematic review and assessment of clinical practice guidelines. BMC Complement Med Ther 2020, 20, 299. [Google Scholar] [CrossRef] [PubMed]
- Cutler, J. B. R.; Pane, O.; Panesar, S. K.; Updike, W.; Moore, T. R. Treatment of Mood and Depressive Disorders With Complementary and Alternative Medicine: Efficacy Review. J Midwifery Womens Health 2023, 68, 421–429. [Google Scholar] [CrossRef]
- Introduction to Yoga – Vikaspedia. Available online: https://vikaspedia.in/health/ayush/yoga-1/introduction-to-yoga (accessed on 28 February 2024).
- Srinivasan, T. Is yoga an intervention? Int J Yoga 2012, 5, 1–2. [Google Scholar] [CrossRef]
- Bhavanani, A. B. Yoga is not an intervention but may be yogopathy is. Int J Yoga 2012, 5, 157–158. [Google Scholar] [CrossRef]
- Naga Venkatesha Murthy, P. J.; Janakiramaiah, N.; Gangadhar, B. N.; Subbakrishna, D. K. P300 amplitude and antidepressant response to Sudarshan Kriya Yoga (SKY). J Affect Disord 1998, 50, 45–48. [Google Scholar] [CrossRef]
- Janakiramaiah, N.; Gangadhar, B. N.; Naga Venkatesha Murthy, P. J.; Harish, M. G.; Subbakrishna, D. K.; Vedamurthachar, A. Antidepressant efficacy of Sudarshan Kriya Yoga (SKY) in melancholia: a randomized comparison with electroconvulsive therapy (ECT) and imipramine. J Affect Disord 2000, 57, 255–259. [Google Scholar] [CrossRef]
- Cramer, H.; Anheyer, D.; Lauche, R.; Dobos, G. A systematic review of yoga for major depressive disorder. J Affect Disord 2017, 213, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, A. V.; Balneaves, L. G.; Faulkner, G.; Ortiz, A.; McIntosh, D.; Morehouse, R. L.; Ravindran, L.; Yatham, L. N.; Kennedy, S. H.; Lam, R. W.; MacQueen, G. M.; Milev, R. V.; Parikh, S. V.; CANMAT Depression Work Group. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 5. Complementary and Alternative Medicine Treatments. Can J Psychiatry 2016, 61, 576–587. [Google Scholar] [CrossRef]
- Gautam, S.; Jain, A.; Gautam, M.; Vahia, V. N.; Grover, S. Clinical Practice Guidelines for the management of Depression. Indian J Psychiatry 2017, 59, S34–S50. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yan, D.; Yang, J. Effectiveness of yoga for major depressive disorder: A systematic review and meta-analysis. Front Psychiatry 2023, 14, 1138205. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Subramaniam, E.; Bhavanani, A. B.; Sarkar, S.; Balasundaram, S. Effect of adjunct yoga therapy in depressive disorders: Findings from a randomized controlled study. Indian J Psychiatry 2019, 61, 592–597. [Google Scholar] [CrossRef]
- Srivastava, A.; Kuppili, P. P.; Gupta, T.; Nebhinani, N.; Chandani, A. Kriya Yoga in Patients with Depressive Disorders: A Pilot Study. J Neurosci Rural Pract 2021, 12, 362–367. [Google Scholar] [CrossRef]
- Bieber, M.; Görgülü, E.; Schmidt, D.; Zabel, K.; Etyemez, S.; Friedrichs, B.; Prvulovic, D.; Reif, A.; Oertel, V. Effects of body-oriented yoga: a RCT study for patients with major depressive disorder. Eur Arch Psychiatry Clin Neurosci 2021, 271, 1217–1229. [Google Scholar] [CrossRef]
- Vollbehr, N. K.; Stant, A. D.; Hoenders, H. J. R.; Bartels-Velthuis, A. A.; Nauta, M. H.; Castelein, S.; Schroevers, M. J.; de Jong, P. J.; Ostafin, B. D. Cost-effectiveness of a mindful yoga intervention added to treatment as usual for young women with major depressive disorder versus treatment as usual only: Cost-effectiveness of yoga for young women with depression. Psychiatry Res 2024, 333, 115692. [Google Scholar] [CrossRef]
- Nauphal, M.; Mischoulon, D.; Uebelacker, L.; Streeter, C.; Nyer, M. Yoga for the treatment of depression: Five questions to move the evidence-base forward. Complement Ther Med 2019, 46, 153–157. [Google Scholar] [CrossRef]
- Bressington, D.; Mui, J.; Yu, C.; Leung, S. F.; Cheung, K.; Wu, C. S. T.; Bollard, M.; Chien, W. T. Feasibility of a group-based laughter yoga intervention as an adjunctive treatment for residual symptoms of depression, anxiety and stress in people with depression. J Affect Disord 2019, 248, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Vollbehr, N. K.; Hoenders, H. J. R.; Bartels-Velthuis, A. A.; Nauta, M. H.; Castelein, S.; Schroevers, M. J.; Stant, A. D.; Albers, C. J.; de Jong, P. J.; Ostafin, B. D. Mindful yoga intervention as add-on to treatment as usual for young women with major depressive disorder: Results from a randomized controlled trial. J Consult Clin Psychol 2022, 90, 925–941. [Google Scholar] [CrossRef] [PubMed]
- Naveen, G.H.; Rao, M.G.; Vishal, V.; Thirthalli, J.; Varambally, S.; Gangadhar, B.N. Development and feasibility of yoga therapy module for out-patients with depression in India. Indian J Psychiatry 2013, 55, S350–S356. [Google Scholar] [CrossRef] [PubMed]
- Ivanets, N. N.; Svistunov, A. A.; Chubarev, V. N.; Kinkulkina, M. A.; Tikhonova, Y. G.; Syzrantsev, N. S.; Sologova, S. S.; Ignatyeva, N. V.; Mutig, K.; Tarasov, V. V. Can Molecular Biology Propose Reliable Biomarkers for Diagnosing Major Depression?. Curr Pharm Des 2021, 27, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Douglass, L. How did we get here? A history of yoga in America, 1800-1970. Int J Yoga Ther 2007, 17, 35–42. [Google Scholar] [CrossRef]
- Kinser, P. A.; Goehler, L. E.; Taylor, A. G. How might yoga help depression? A neurobiological perspective. Explore 2012, 8, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Tolahunase, M. R.; Gautam, S.; Sagar, R.; Kumar, M.; Dada, R. Yoga in major depressive disorder: molecular mechanisms and clinical utility. Front Biosci 2021, 13, 56–81. [Google Scholar] [CrossRef]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and other Tools) Resource. Silver Spring (MD): Food and Drug Administration (US); Bethesda (MD): National Institutes of Health (US); 2016. Available online at: https://www.ncbi.nlm.nih. 3267.
- Califf, R.M. Biomarker definitions and their applications. Exp Biol Med 2018, 243, 213–221. [Google Scholar] [CrossRef]
- Tricco, A. C.; Lillie, E.; Zarin, W.; O'Brien, K. K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M. D. J.; Horsley, T.; Weeks, L.; Hempel, S.; Akl, E. A.; Chang, C.; McGowan, J.; Stewart, L.; Hartling, L.; Aldcroft, A.; Wilson, M. G.; Garritty, C.; Lewin, S.; … Straus, S. E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Wirsching, J.; Graßmann, S.; Eichelmann, F.; Harms, L. M.; Schenk, M.; Barth, E.; Berndzen, A.; Olalekan, M.; Sarmini, L.; Zuberer, H.; Aleksandrova, K. Development and reliability assessment of a new quality appraisal tool for cross-sectional studies using biomarker data (BIOCROSS). BMC Med Res Methodol 2018, 18, 122. [Google Scholar] [CrossRef]
- Rajkumar, R. P. Immune-inflammatory markers of response to repetitive transcranial magnetic stimulation in depression: A scoping review. Asian J Psychiatry 2024, 91, 103852. [Google Scholar] [CrossRef]
- Sharma, V.K.; Das, S.; Mondal, S.; Goswami, U. Comparative effect of Sahaj Yoga on EEG in patients of major depression and healthy subjects. Biomedicine 2007, 27, 95–99. [Google Scholar]
- Sharma, V.K.; Das, S.; Mondal, S.; Goswami, U. Effect of Sahaj Yoga on autonomic functions in healthy subjects and patients of major depression. Biomedicine 2008, 28, 139–141. [Google Scholar]
- Naveen, G.H.; Thirthalli, J.; Rao, M.G.; Varambally, S.; Christopher, R.; Gangadhar, B.N. Positive therapeutic and neurotropic effects of yoga in depression: a comparative study. Indian J Psychiatry 2013, 55, 400–404. [Google Scholar] [CrossRef]
- Sarubin, N.; Nothdurfter, C.; Schule, C.; Lieb, M.; Uhr, M.; Born, C.; Zimmermann, R.; Buhner, M.; Konopka, K.; Ruppercht, R.; Baghai, T.C. The influence of Hatha yoga as add-on treatment in major depression on hypothalamic-pituitary-adrenal axis activity: a randomized trial. J Psychiatr Res 2014, 53, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Naveen, G.H.; Varambally, S.; Thirthalli, J.; Rao, M.; Christopher, R.; Gangadhar, B.N. Serum cortisol and BDNF in patients with major depression – effect of yoga. Int Rev Psychiatry 2016, 28, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Toschi-Dias, E.; Tobaldini, E.; Solbiati, M.; Costantino, G.; Sanlorenzo, R.; Doria, S.; Irtelli, F.; Mencacci, C.; Montano, N. Sudarshan Kriya Yoga improves cardiac autonomic control in patients with anxiety-depression disorders. J Affect Disord 2017, 214, 74–80. [Google Scholar] [CrossRef]
- Tolahunase, M.R.; Sagar, R.; Faiq, M.; Dada, R. Yoga- and meditation-based lifestyle intervention increases neuroplasticity and reduces severity of major depressive disorder: a randomized controlled trial. Restor Neurol Neurosci 2018, 36, 423–442. [Google Scholar] [CrossRef]
- Bhargav, P.H.; Reddy, P.V.; Govindaraj, R.; Gulati, K.; Ravindran, A.; Gayathri, D.; Karmani, S.J.; Udupa, K.; Venkatasubramanian, G.; Philip, M.; Debnath, M.; Bharath, R.D.; Sathyaprabha, T.N.; Gangadhar, B.N.; Muralidharan, K. Impact of a course of add-on supervised yoga on cortical inhibition in major depressive disorder: a randomized controlled trial. Can J Psychiatry 2021, 66, 179–181. [Google Scholar] [CrossRef]
- Gulati, K.; Bhargav, P.H.; Reddy, P.V.; Govindaraj, R.; Ravindran, A.; Gayathri, D.; Karmani, S.J.; Udupa, K.; Philip, M.; Debnath, M.; Bharath, R.D.; Sathyaprabha, T.N.; Venkatasubramanian, G.; Muralidharan, K. Adjunct yoga therapy: influence on heart rate variability in major depressive disorder – a randomized controlled trial. Asian J Psychiatry 2021, 65, 102832. [Google Scholar] [CrossRef]
- Nugent, N.R.; Brick, L.; Armey, M.F.; Tyrka, A.R.; Ridout, K.K.; Uebelacker, L.A. Benefits of yoga on IL-6: findings from a randomized controlled trial of yoga for depression. Behav Med 2021, 47, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Subbanna, M.; Talukdar, P.M.; Abdul, F.; Debnath, M.; Reddy, P.V.; Arasappa, R.; Venkatasubramanian, G.; Muralidharan, K.; Gangadhar, B.N.; Bhargav, P.H.; Karmani, S. Long-term add-on Yoga therapy offers clinical benefits in major depressive disorder by modulating the complement pathway: a randomized controlled trial. Asian J Psychiatry 2021, 66, 102876. [Google Scholar] [CrossRef]
- Haapakoski, R.; Mathieu, J.; Ebmeier, K.P.; Alenius, H.; Kivimaki, M. Cumulative meta-analysis of interleukins 6 and 1β, tumor necrosis factor α and C-reactive protein in patients with major depressive disorder. Brain Behav Immun 2015, 49, 206–215. [Google Scholar] [CrossRef]
- Osimo, E.F.; Baxter, L.J.; Lewis, G.; Jones, P.B.; Khandaker, G.M. Prevalence of low-grade inflammation in depression: a systematic review and meta-analysis of CRP levels. Psychol Med 2019, 49, 1958–1970. [Google Scholar] [CrossRef]
- Hassamal, S. Chronic stress, neuroinflammation, and depression: an overview of pathophysiological mechanisms and emerging anti-inflammatories. Front Psychiatry 2023, 14, 1130989. [Google Scholar] [CrossRef] [PubMed]
- Zajkowska, Z.; Gullett, N.; Walsh, A.; Zonca, V.; Pedersen, G.A.; Souza, L.; Kieling, C.; Fisher, H.L.; Kohrt, B.A.; Mondelli, V. Cortisol and development of depression in adolescence and young adulthood – a systematic review and meta-analysis. Psychoneuroendocrinology 2022, 136, 105625. [Google Scholar] [CrossRef]
- Jeon, S.W.; Kim, Y.K. Neuroinflammation and cytokine abnormality in major depression: cause or consequence in that illness? World J Psychiatry 2016, 6, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Bocchio-Chiavetto, L.; Bagnardi, V.; Zanardini, R.; Molteni, R.; Nielsen, M.G.; Placentino, A.; Giovannini, C.; Rillosi, L.; Ventriglia, M.; Riva, M.A.; Gennarelli, M. Serum and plasma BDNF levels in major depression: a replication study and meta-analyses. World J Biol Psychiatry 2010, 11, 763–773. [Google Scholar] [CrossRef]
- Liu, T.; Zhong, S.; Liao, X.; Chen, J.; He, T.; Lai, S.; Jia, Y. A meta-analysis of oxidative stress markers in depression. PloS One 2015, 10, e0138904. [Google Scholar] [CrossRef]
- Yang, J.; Li, R.; Shi, Y.; Jiang, S.; Liu, J. Is serum complement C1q related to major depressive disorder? Indian J Psychiatry 2020, 62, 659–663. [Google Scholar] [CrossRef]
- Tang, W.; Liu, H.; Chen, L.; Zhao, K.; Zhang, Y.; Zheng, K.; Zhu, C.; Zheng, T.; Liu, J.; Wang, D.; Yu, L.; Fang, X.; Zhang, C.; Su, K.P. Inflammatory cytokines, complement factor H and anhedonia in drug-naïve major depressive disorder. Brain Behav Immun 2021, 95, 238–244. [Google Scholar] [CrossRef]
- Romeo, B.; Choucha, W.; Fossati, P.; Rotge, J.Y. Meta-analysis of central and peripheral γ-aminobutyric acid levels in patients with unipolar and bipolar depression. J Psychiatr Neurosci 2018, 43, 58–66. [Google Scholar] [CrossRef]
- Kinjo, M.; Wada, M.; Nakajima, S.; Tsugawa, S.; Nakahara, T.; Blumberger, D.M.; Mimura, M.; Noda, Y. Transcranial magnetic stimulation neurophysiology of patients with major depressive disorder: a systematic review and meta-analysis. Psychol Med 2021, 51, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Luo, Y.; Zhang, Y.; Chen, L.; Zou, Y.; Xiao, J.; Min, W.; Yuan, C.; Ye, Y.; Li, M.; Tu, M.; Hu, J.; Zou, Z. Heart rate variability in generalized anxiety disorder, major depressive disorder and panic disorder: a network meta-analysis and systematic review. J Affect Disord 2023, 330, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Estevao, C. The role of yoga in inflammatory markers. Brain Behav Immun Health 2022, 20, 100421. [Google Scholar] [CrossRef]
- Shobana, R.; Maheshkumar, K.; Venkateswaran, S.T.; Geetha, M.B.; Padmavathi, R. Effects of long-term yoga training on autonomic function among the healthy adults. J Family Med Prim Care 2023, 11, 3471–3475. [Google Scholar] [CrossRef]
- Pascoe, M.C.; Bauer, I.E. A systematic review of randomized control trials on the effects of yoga on stress measures and mood. J Psychiatr Res 2015, 68, 270–2872. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Bhardwaj, S.; Gupta, A.; Katoch, V.M.; Sharma, K.K.; Gupta, R. Influence of 24-week yoga intervention on cardiovascular risk factors and inflammatory markers in type 2 diabetes. Int J Yoga 2023, 16, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Tolahunase, M.; Sagar, R.; Dada, R. Impact of yoga and meditation on cellular aging in apparently healthy individuals: a prospective, open-label single-arm exploratory study. Oxid Med Cell Longev 2017, 2017, 7928981. [Google Scholar] [CrossRef]
- Yu, H.; Zhang, F.; Guan, X. Baicalin reverse depressive-like behaviors through regulation SIRT1-NF-κB signaling pathway in olfactory bulbectomized rats. Phytother Res 2019, 33, 1480–1489. [Google Scholar] [CrossRef]
- Calabrese, F., Rossetti, A.C.; Racagni, G.; Gass, P.; Riva, M.A.; Molteni, R. Brain-derived neurotrophic factor: a bridge between inflammation and neuroplasticity. Front Cell Neurosci 2014, 8, 430. [CrossRef] [PubMed]
- Shi, Y.; Luan, D.; Song, R.; Zhang, Z. Value of peripheral neurotrophin levels for the diagnosis of depression and response to treatment: a systematic review and meta-analysis. Eur Neuropsychopharmacol 2020, 41, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, G.C.; Gould, T.D.; Prueitt, W.L.; Nanavati, J.; Grunebaum, M.F.; Farber, N.B.; Singh, B.; Selvaraj, S.; Machado-Vieira, R.; Achtyes, E.D.; Parikh, S.V.; Frye, M.A.; Zarate, C.A.; Goes, F.S. Blood-based biomarkers of antidepressant response to ketamine and esketamine: a systematic review and meta-analysis. Mol Psychiatry 2022, 27, 3658–3669. [Google Scholar] [CrossRef] [PubMed]
- Claudino, F.C.A.; Goncalves, L.; Schuch, F.B.; Martins, H.R.S.; da Rocha, N.S. The effects of individual psychotherapy in BDNF levels of patients with mental disorders: a systematic review. Front Psychiatry 2020, 11, 445. [Google Scholar] [CrossRef]
- Pelosof, R.; Dos Santos, L.A.; Farhat, L.C.; Gattaz, W.F.; Talib, L.; Brunoni, A.R. BDNF blood levels after electroconvulsive therapy in patients with mood disorders: an updated systematic review and meta-analysis. World J Biol Psychiatry 2023, 43, 24–33. [Google Scholar] [CrossRef]
- Cakici, N.; Sutterland, A.L.; Penninx, B.W.J.H.; de Haan, L.; van Beveren, N.J.M. Changes in peripheral blood compounds following psychopharmacological treatment in drug-naïve first-episode patients with either schizophrenia or major depressive disorder: a meta-analysis. Psychol Med 2021, 51, 538–549. [Google Scholar] [CrossRef]
- Halappa, N.G.; Thirthalli, J.; Varambally, S.; Rao, M.; Christopher, R.; Nanjundaiah, G.B. Improvement in neurocognitive functions and serum brain-derived neurotrophic factor levels in patients with depression treated with antidepressants and yoga. Indian J Psychiatry 2018, 60, 32–37. [Google Scholar] [CrossRef]
- Murthy, P.J.; Gangadhar, B.N.; Janakiramaiah, N.; Subbakrishna, D.K. Normalization of P300 amplitude following treatment in dysthymia. Biol Psychiatry 1997, 42, 740–743. [Google Scholar] [CrossRef]
- Naga Venkatesha Murthy, P.J.; Janakiramaiah, N.; Gangadhar, B.N.; Subbakrishna, D.K. P300 amplitude and antidepressant response to Sudarshan Kriya Yoga (SKY). J Affect Disord 1998, 50, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Jain, F.A.; Cook, I.A.; Leuchter, A.F.; Hunter, A.M.; Davydov, D.M.; Ottaviani, C.; Tartter, M.; Crump, C.; Shapiro, D. Heart rate variability and treatment outcome in major depression: a pilot study. Int J Psychophysiol 2014, 93, 204–210. [Google Scholar] [CrossRef]
- Tolahunase, M.R.; Sagar, R.; Dada, R. 5-HTTLPR and MTHFR 677C>T polymorphisms and response to yoga-based lifestyle intervention in major depressive disorder: a randomized active-controlled trial. Indian J Psychiatry 2018, 60, 410–426. [Google Scholar] [CrossRef]
- Streeter, C.C.; Gerbarg, P.L.; Brown, R.P.; Scott, T.M.; Nielsen, G.H.; Owen, L.; Sakai, O.; Sneider, J.T.; Nyer, M.B.; Silveri, M.M. Thalamic gamma aminobutyric acid level changes in major depressive disorder after a 12-week Iyengar yoga and coherent breathing intervention. J Altern Complement Med 2020, 26, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Aditi Devi, N.; Philip, M.; Varambally, S.; Christopher, R.; Gangadhar, B.N. Yoga as a monotherapy alters proBDNF – mature BDNF ratio in patients with major depressive disorder. Asian J Psychiatry 2023, 81, 103429. [Google Scholar] [CrossRef] [PubMed]
- Heneghan, C.; Goldacre, B.; Mahtani, K.R. Why clinical trial outcomes fail to translate into benefits for patients. Trials 2017, 18, 122. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Taljaard, M.; Van den Heuvel, E.R.; Levine, M.A.H.; Cook, D.J.; Wells, G.A.; Devereaux, P.J.; Thabane, L. An introduction to multiplicity issues in clinical trials: the what, why, when and how. Int J Epidemiol 2017, 46, 746–755. [Google Scholar] [CrossRef]
Figure 1.
PRISMA-ScR 2020 flow diagram for the current review.
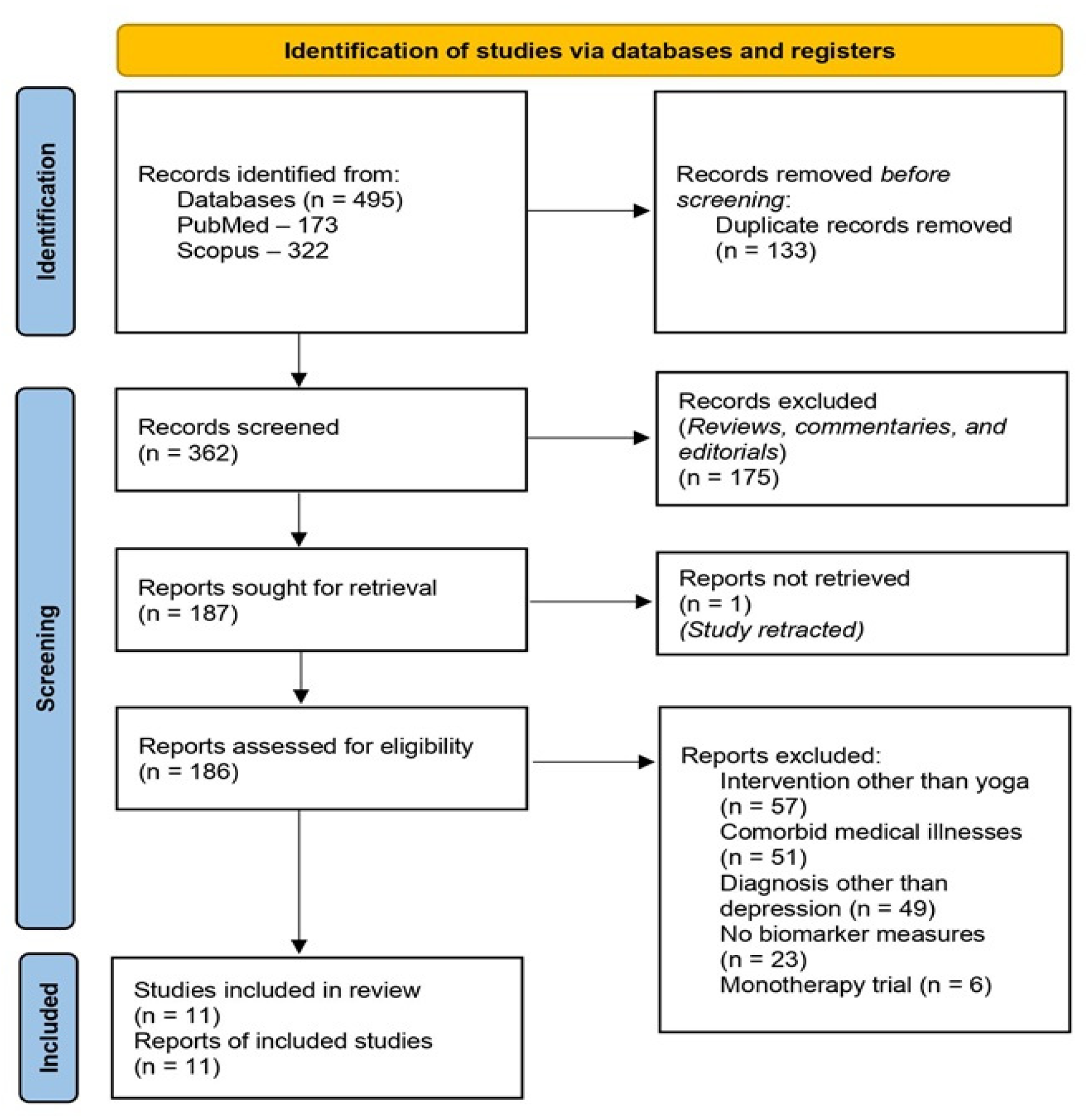
Figure 2.
Mechanisms through which yoga-based interventions may influence biological processes involved in recovery from depression.
Figure 2.
Mechanisms through which yoga-based interventions may influence biological processes involved in recovery from depression.
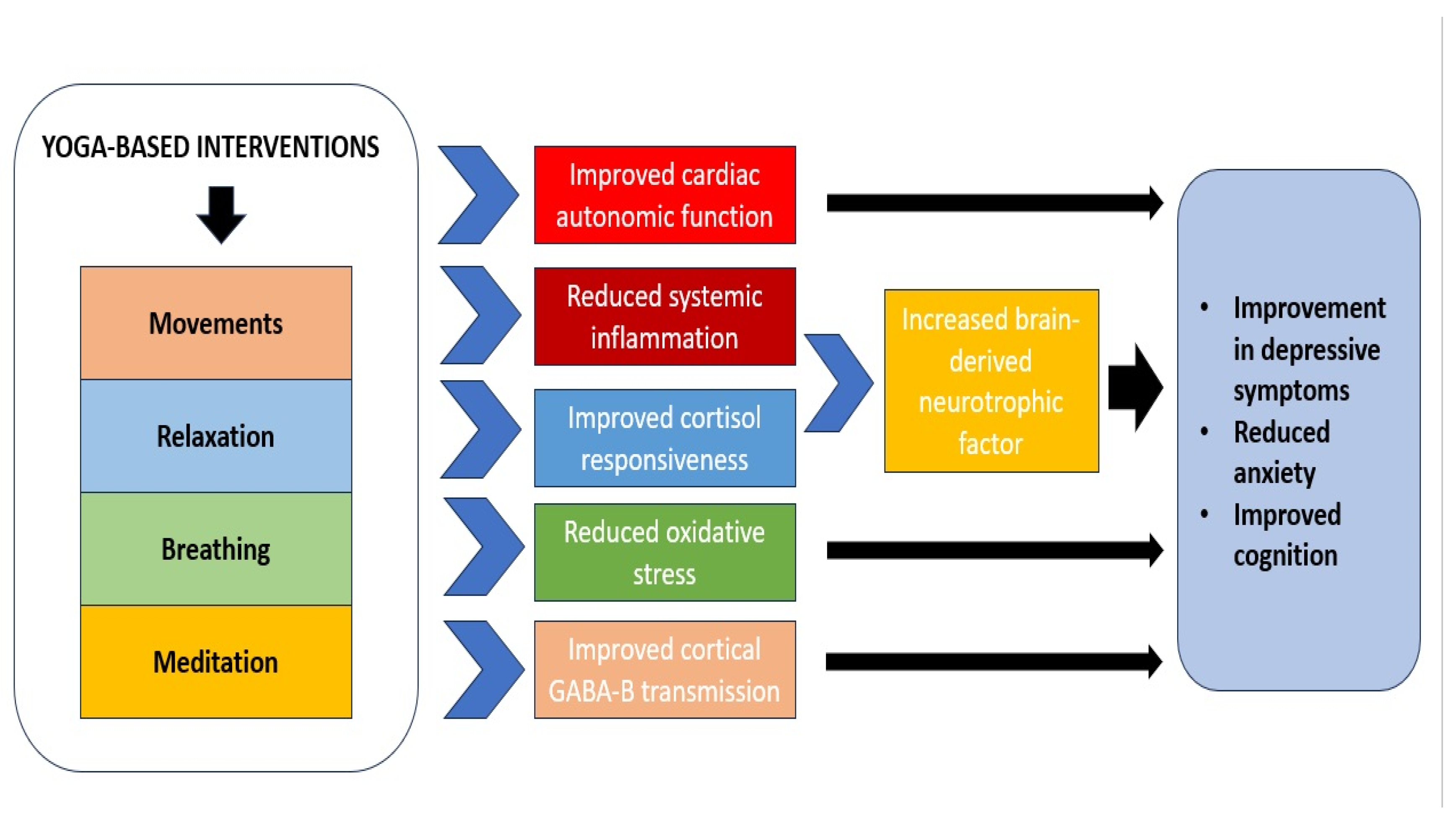

Table 1.
Characteristics of studies examining biomarkers of response to adjunctive yoga in patients with depression.
Table 1.
Characteristics of studies examining biomarkers of response to adjunctive yoga in patients with depression.
| Study | Country of origin | Sample size and diagnosis | Yoga intervention | Concurrent treatment(s) | Biomarkers estimated | Results | BIO-CROSS score |
|---|---|---|---|---|---|---|---|
| Sharma et al., 2007 [44] | India | n = 30, MDD (DSM-IV criteria) | Sahaj yoga meditation (8 weeks) | Antidepressants as usual | EEG alpha activity | No significant effect of yoga on alpha activity. Correlation with clinical improvement not reported. | 11 |
| Sharma et al., 2008 [45] | India | n = 30, MDD (DSM-IV criteria) | Sahaj yoga meditation (8 weeks) | Antidepressants as usual | Autonomic parameters – PR, RR, GSR | No significant effect of yoga on autonomic parameters. Correlation with clinical improvement not reported. | 12 |
| Naveen et al., 2013 [46] | India | n = 35, MDD (DSM-IV criteria) | Depression-specific yoga module (12 weeks) |
Antidepressants as usual | Serum BDNF | Significant increase in BDNF both in yoga and control groups; increased BDNF correlated with reduced depressive symptoms only in yoga group | 17 |
| Sarubin et al., 2014 [47] | Germany | n = 60, MDD (DSM-IV criteria) | Hatha yoga (1 hour/week for 5 weeks) | Escitalopram (10 mg/day) or quetiapine (300 mg/day) | Cortisol response to serial DEX/CRH tests | No significant effect of yoga on cortisol responses. Changes in cortisol correlated with reduced depressive symptoms regardless of treatment. | 19 |
| Naveen et al., 2016 [48] | India | n = 35, MDD (DSM-IV criteria) | Depression-specific yoga module (12 weeks) |
Antidepressants as usual | Serum cortisol | Significant reduction in serum cortisol in yoga group. Correlation with clinical improvement not reported. | 15 |
| Toschi-Dias et al., 2017 [49] | Italy | n = 46, “depression or anxiety disorders” (DSM-IV criteria) | Sudarshan Kriya Yoga (10 sessions over 2 weeks) | Antidepressants as usual | Cardiac autonomic parameters recorded through ECG | Reduced sympathetic modulation and improved parasympathetic modulation and cardiorespiratory coupling in yoga group. Temporal but not direct correlation with improvement in depressive symptoms. | 13 |
| Tolahunase et al., 2018 [50] | India | n = 58, MDD (DSM-IV criteria) | Yoga and meditation lifestyle intervention (12 weeks) | Antidepressants as usual | Serum 8OH2dG, BDNF, cortisol, DHEAS, IL-6, oxidative stress markers (ROS, TAC), sirtuin-1, telomerase | Significant increase in BDNF, DHEAS, sirtuin-1 and telomerase and decrease in cortisol, IL-6, ROS, TAC and 8OH2dG in yoga group. Changes in BDNF correlated with reduction in depressive symptoms. | 14 |
| Bhargav et al., 2021 [51] | India | n = 70, MDD (DSM-IV criteria) | Depression-specific yoga module (12 weeks) |
Antidepressants as usual | TMS measures of cortical inhibition (CI, CSP, RMT, LICI, SICI) | Significant increase in CSP in yoga group. Correlation with clinical improvement not reported. | 13 |
| Gulati et al., 2021 [52] | India | n = 68, MDD (DSM-IV criteria) | Depression-specific yoga module (12 weeks) |
Antidepressants as usual | HRV parameters recorded through ECG | Trend towards greater decrease in HRF low-frequency/high-frequency ratio in yoga group; no significant group differences. Correlation with clinical improvement not reported. |
18 |
| Nugent et al., 2021 [53] | United States | n = 84, MDD (DSM-IV criteria) | Hatha yoga vs Healthy Living Workshop (10 weeks) |
Antidepressants as usual | Serum CRP, IL-6, TNF-α | Significant reduction in IL-6 in yoga group. Correlation with clinical improvement not reported. | 17 |
| Subbanna et al., 2021 [54] | India | n = 22, MDD (DSM-IV criteria) | Depression-specific yoga module (12 weeks) |
Antidepressants as usual | Plasma complement components C1q, C3, C3b/iC3b, C4, Factor B, Factor H, properdin | Significant reduction in C1q, Factor H and properdin in yoga group; not correlated with improvement in depression. Significant reduction in C4 in control group | 13 |
Abbreviations: 8OH2dG, 8-hyrdoxy 2-deoxyguanosine; BDNF, brain-derived neurotrophic factor; CRH, corticotropin-releasing hormone; CRP, C-reactive protein; CSP, cortical silent period; DHEAS, dehydroepiandrosterone sulfate; DSM, Diagnostic and Statistical Manual for Mental Disorders; DEX, dexamethasone; ECG, electrocardiography; EEG, electroencephalography; GSR, galvanic skin response; HRV, heart rate variability; IL-6, interleukin-6; LICI, long interval cortical inhibition; MDD, major depressive disorder; PR, pulse rate; RMT, resting motor threshold; ROS, reactive oxygen species; RR, respiratory rate; SICI, short interval cortical inhibition; TAC, total antioxidant capacity; TMS, transcranial magnetic stimulation; TNF-α, tumor necrosis factor alpha.
Table 2.
Biomarkers of response to yoga monotherapy in depression.
| Study | Sample Characteristics | Yoga-Based Intervention Characteristics | Biomarkers Assessed | Results |
|---|---|---|---|---|
| Murthy et al., 1997 [80] | Dysthymia, n = 15, India | Sudarshan Kriya yoga (12 weeks) |
Auditory P300 event-related potential | Significant increase in P300 amplitude after yoga; temporal correlation with symptomatic improvement |
| Naga Venkatesha Murthy et al., 1998 [81] | Depression, n = 30 (MDD, n = 15; dysthymia, n = 15), India | Sudarshan Kriya yoga (12 weeks) |
Baseline auditory P300 event-related potential | No association between baseline P300 amplitude and response to yoga |
| Jain et al., 2014 [82] | MDD, n = 16, United States | Iyengar yoga (20 sessions over 8 weeks) | Baseline HRV parameters measured using ECG | Lower HRV rVLF predicted response to yoga |
| Tolahunase et al., 2018 [83] | MDD, n = 89, India | Yoga-based lifestyle intervention (5 sessions/week over 12 weeks) | 5-HTTLPR and MTHFR functional polymorphisms | No significant association between either polymorphism and response to yoga |
| Streeter et al., 2020 [84] | MDD, n = 28, United States | Iyengar yoga (12 weeks, randomized to high- or low-dose) | Thalamic GABA measured using MRS | Increased thalamic GABA low-dose yoga group; negative correlation between thalamic GABA and depression severity in high-dose group |
| Aditi Devi et al., 2023 [85] | MDD, n = 13, India | Brief yoga module (10 sessions over 2 weeks) |
Serum BDNF, pro-BDNF, mature BDNF | Significant increase in total and mature BDNF; reduced pro-BDNF / mature BDNF ratio; temporal correlation with symptomatic improvement |
Abbreviations: 5-HTTLPR, serotonin transporter gene promoter functional polymorphism; BDNF, brain-derived neurotrophic factor; GABA, gamma-amino butyric acid; HRV, heart rate variability; MDD, major depressive disorder; MRS, magnetic resonance spectroscopy; MTHFR, methyl-tetrahydrofolate reductase gene; VLF, very low frequency band.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



