
Submitted:
04 March 2024
Posted:
05 March 2024
You are already at the latest version
Abstract
Background: The Liver Imaging Reporting and Data System (LI-RADS) combines standardized terminology with a classification system for imaging findings in patients with HCC, therefore rendering diagnostic biopsy unnecessary in many cases. This retrospective study included 23 patients with a biopsy diagnosis of HCC, performed either before or after local interventional procedures, in order to evaluate the histopathologic changes induced by previous procedures and their potential influence on the response to immune therapy. Material and Methods: The study encompassed a cohort of patients diagnosed with Hepatocellular Carcinoma (HCC). Diagnosis was established through contrast-enhanced computer tomography or magnetic resonance imaging that identified LI-RADS-5 nodules in conjunction with historical liver disease and elevated alpha-fetoprotein (AFP) levels, or through histological examination confirming positivity for glypican3, heat shock protein70, and glutamine synthetase. The study detailed the liver disease etiology, LI-RADS scores, characteristics and dimensions of HCC nodules, serum AFP concentrations, Edmondson-Steiner grading, and the expression of programmed cell death ligand 1 (PD-L1) in the tumor cells. Results: Among the study's cohort of Hepatocellular Carcinoma (HCC) patients, a portion had not received any prior treatments, while the remainder experienced local HCC recurrence following trans-arterial chemoembolization or radiofrequency ablation. Observations indicated elevated alpha-fetoprotein (AFP) levels in those who had not undergone any previous interventions, showing statistical significance. The Edmondson-Steiner classification predominantly identified grade III differentiation across patients, irrespective of their treatment history. Furthermore, an increase in intra-tumoral programmed cell death ligand 1 (PD-L1) expression was noted in patients who had not been subjected to previous therapies. Conclusion: Liver biopsy offers valuable insights for patients with Hepatocellular Carcinoma (HCC), assisting in the tailoring of immune therapy strategies, particularly in cases of recurrence following prior local interventions.
Keywords:
cancer
; hepatocellular
; biopsy
; alpha-fetoprotein
; immune checkpoint inhibitor
Background
Hepatocellular carcinoma (HCC) remains a public health challenge, despite the numerous diagnostic and therapeutic means currently available [1]. In 2018, an estimated 841,000 HCC cases were diagnosed and 782,000 HCC associated deaths were recorded [2]. An estimate using GLOBOCAN database found over 900,000 new HCC cases in 2020 and predicted an incidence increase by 55%, to about 1.4 million patients diagnosed in 2040 [3]. Some authors estimate that the incidence of HCC will rise to approximatively 1 million patients per year by 2025 [4]. Increasing awareness for chronic viral hepatitis as well as the high rates of sustained virologic response obtained by direct-acting antiviral therapy for hepatitis C were expected to lower the incidence of HCC [5]. However, the rising prevalence of obesity and metabolic syndrome leads to an increase in non-alcoholic fatty liver disease and its complications (cirrhosis and HCC) overcoming the benefits of virologic advances [6].
Current guidelines recommend a personalized approach regarding screening, diagnosis and management of HCC [5,7]. The European Association for the Study of the Liver (EASL) recommends periodic surveillance for HCC in high-risk patients such as patients with advanced liver disease (cirrhotic patients) or patients with advanced fibrosis (F3) and hepatitis B infection [5]. The American Association for the Study of Liver Diseases (AASLD) also refers to cirrhosis as the main risk factor for HCC, particularly with underlying viral etiology, but raises awareness towards the increasing incidence of metabolic syndrome-associated HCC [7]. According to the AASLD guidelines, HCC screening should be performed in patients with Child Pugh class A or B cirrhosis (as it is not cost-efficient for Class C cirrhosis) and in non-cirrhotic hepatitis B patients [7].
The diagnosis of HCC requires evaluation of risk factors (chronic liver disease), tumoral markers (alpha-fetoprotein (AFP) being the most commonly used) and imaging patterns based on the enhancement after intravenous contrast [5]. EASL guidelines recommend non-invasive tests for HCC diagnosis in cirrhotic patients, comprised of serum markers and imaging, while strongly recommending a histological diagnosis in non-cirrhotic patients [5]. Non-invasive criteria should only be applied to cirrhotic patients, with nodules larger than 1cm. Imagining techniques include multiphasic computer tomography (CT) or dynamic contrast-enhanced magnetic resonance imaging (MRI); contrast enhanced ultrasonography (CEUS) shows similar specificity and sensitivity but currently has insufficient evidence for a strong recommendation [5,8]. The imagistic hallmark of HCC consists of arterial hyperenhancement with delayed washout, attributable to the vascular abnormalities associated with HCC [9]. Typical MRI aspects include hyperintensity in the arterial phase, hypo-intensity in the portal phase and hypo-intensity in the transitional phase [10].
Imaging features of liver nodules may be classified according to LI-RADS score, to predict the possibility of malignancy depending mainly on nodule dimensions and enhancement pattern. [11]. Importantly, this score also aids in establishing the need for liver biopsy, for atypical nodules or nodules with malignancy characteristics and low HCC risk. This classification defines 8 categories of liver nodules, according to the CT or MRI aspect, according to the probability of malignancy of a liver nodule [12]:
- -
- LR-NC, non-categorizable, due to degraded images
- -
- LR-1, definitely benign,
- -
- LR-2, probably benign, referring to nodules less than 2cm, without any imagistic criteria of malignancy
- -
- LR-3, intermediate probability of malignancy, referring to nodules less than 2 cm with nonrim arterial hyperenhancement or nodules larger than 2cm with arterial iso or hypo-enhancement.
- -
- LR-4, high HCC probability, referring to nodules less than 10mm, with arterial hyperenhancement and one other typical feature or nodules over 20mm with arterial hyperenhancement and no other suggestive features
- -
- LR-5, definite diagnosis of HCC, nodules over 10mm with arterial hyperenhancement and portal washout, or with a 50% size increase in less than 6 months.
- -
- LR-TIV, malignant venous thrombus, with arterial hyperenhancement regardless of the presence of a liver nodule
- -
- LR-M, high malignancy probability, but not HCC, referring to nodules with rim arterial enhancement, peripheral washout, targetoid aspect or infiltrative appearance.
LI-RADS criteria have been validated in cirrhotic patients or patients with severe fibrosis and hepatitis B (HBV) infection, therefore in all other situations histology analysis is required for a definite HCC diagnosis [7]. Pathologic diagnosis is based on criteria established by the World Health Organization and the International Consensus Group for Hepatocellular Neoplasia, and takes into consideration stromal invasion, increased cell density, intratumoral portal tracts, excessive arteries, a pseudoglandular pattern and diffuse fatty changes. A panel of 3 immunohistological markers (heat shock protein 70, glypican 3 and glutamine synthetase) has shown good specificity and sensitivity in HCC diagnosis, in cases where histology is controversial [13]. Edmondson Steiner grade is a histologic predictor for HCC recurrence, classifying HCC as: well differentiated, moderately differentiated, poorly differentiated and pleiomorphism [14]. A retrospective trial found that high Edmondson Steiner degrees correlate to high AFP levels, large or infiltrative tumors and advanced HCC, but did not correlate with outcome after local procedures (chemoembolization, ablation, yttrium-radioembolization) [14].
Therapeutic decision is based on the Barcelona Clinic Liver Cancer (BCLC) classification, which stratifies patients according to tumor burden, clinical status and baseline liver function [15]. For patients with very early stage and early stage HCC, curative procedures are recommended (surgical resection or radiofrequency ablation (RFA), liver transplantation) [7]. Patients with intermediate stage HCC are also candidates for liver transplant, but may undergo transarterial chemoembolization (TACE) or systemic therapies, while patients with advanced stage should receive systemic therapies alone [7]. The 2018 EASL guideline and the 2023 AASLD guidelines have different recommendations for first line systemic therapies: EASL recommends sorafenib or Lenvatinib, while AASLD recommends atezolizumab/bevacizumab or durvalumab/tremelimumab [5,7]
As mentioned before, systemic therapies are currently reserved for patients with advanced disease, disease progression or patients with nodules amendable to local therapies which are unavailable or technically impossible [16]. These therapies include tyrosine kinase inhibitors (sorafenib, lenvatinib, regorafenib and cabozatinib), an inhibitor of the vascular endothelial growth factor receptor 2 (ramucirumab) and immune checkpoint inhibitors (ICI) (atezolizumab associated with bevacizumab, ipilimumab associated with nivolumab, nivolumab and pembrolizumab as monotherapies) [16].
Recent data suggest that intra-tumoral biomarkers may predict the response to immunotherapy, especially to immune check-point inhibitors, currently the first line of systemic therapy [17]. For instance, programmed cell death ligand 1 (PD-L1) expression in tumor cells (associated with poor differentiation and macrovascular invasion) correlates with a better response to immune therapy [18]. As new markers and treatments emerge, it is important to personalize the management of the patients to achieve the best prognosis, in the setting of limited curative interventions [17]. As such, tumor biopsy regains importance in HCC management, even in patients with a definite imaging diagnosis. A recent review summarizes predictive biomarkers for HCC prognosis and response to immune therapy, including PD-L1 expression in tumor cells, DNA Damage Repair pathways expression, tumor mutational burden, tumor infiltrating lymphocytes [19]. There is controversial evidence regarding PD-L1 as prognosis marker. Overexpression of PD-L1 in HCC histology has been associated with poor prognosis in a series of 217 HCC patients but the IMBrave150 trial revealed thatPD-L1 expression predicted a good outcome in patient treated vit atezolizumab/bevacizumab compared with patients treated with sorafenib [20;21]
According to the National Guidelines, atezolizumab/bevacizumab therapy is reserved for patients with Class A cirrhosis, with progression after local therapies or sorafenib therapy with a positive HCC diagnosis established by contrast-enhanced imaging in cirrhotic patients and by histology in non-cirrhotic patients [22]. In this setting, we performed liver biopsy on eligible HCC patients for therapy approval.
This retrospective study included 23 patients with a biopsy diagnosis of HCC to evaluate whether histological differences before and after local procedures may help predict the response to systemic therapy.
Materials and Methods:
Ethical Statement
All the participants signed inform consent forms for the medical procedures and for participation in medical studies. The study is approved by the Local Ethics Committee (1718/2021).
Patient Selection
Our study entailed a retrospective analysis of 76 liver tumor biopsies conducted at our facility from January 2021 to January 2022. These liver biopsies were executed percutaneously, guided by computer tomography (CT) scans, and carried out by an experienced interventional radiologist. A senior pathologist then evaluated the biopsies for size and histopathological characteristics.
We excluded patients from the study if their imaging indicated liver metastases (classified as LR-M according to LI-RADS criteria), if they had a known history of solid malignancies, or if the biopsy results confirmed liver metastases (total exclusions: 53). In cases where histological findings were ambiguous, we employed an immunochemistry panel to definitively diagnose Hepatocellular Carcinoma (HCC). This process resulted in a subset of 33 biopsies being selected for further examination of PD-L1 expression.
For each participant, we documented the etiology of the underlying liver disease. We categorized HCC patients based on their treatment history: those who had not undergone any previous local therapies, those who experienced recurrence following Transarterial Chemoembolization (TACE), and those with recurrence after Radiofrequency Ablation (RFA). Additionally, we compiled data on serum alpha-fetoprotein (AFP) levels for each patient.
Imaging Techniques
Patients underwent contrast enhanced abdominal CT scan or MRI before liver biopsy. We collected data regarding size and number of nodules, portal vein invasion and LI-RADS degree (LR-4 or LR-5 in LI-RADS criteria). All nodules had a diameter of over 10mm and presented nonrim arterial hyperenhancement (Figure 1)
Histology Analysis
Following the collection of samples, the tissue underwent histological examination. The identification of Hepatocellular Carcinoma (HCC) relied on specific characteristics, including polygonal cells exhibiting nuclear irregularities, an elevated nucleus-to-cytoplasm ratio, pronounced nuclei, uneven nuclear contours, and the presence of multiple nuclei. Additionally, the analysis included the observation of a trabecular pattern (refer to Figure 2).
In patients without a clear histology diagnosis, we performed a panel of immunohistochemical testing consisting of glypican3, heat shock protein70 and glutamine synthetase. After a definitive HCC diagnosis, we determined the expression of PD-L1 in tumor cells by immunohistochemistry on formalin-fixed paraffin-embedded sections.
Statistical Analysis
Statistical analysis was performed using SPSS (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp). Numerical data such as AFP levels and PD-L1 expression are described as means. Qualitative variables are described as percentages. Correlations between AFP levels or PD-L1 expression and previous interventional therapies were determined using chi-square test.
Results:
Descriptive Data
This research encompassed 23 participants, comprising 12 men and 11 women, with an average age of 51.04 years, plus or minus 13.2 years. The classification of patients was based on prior treatments administered to the same region as the biopsied nodule, categorizing them into groups of no prior intervention, those who underwent Radiofrequency Ablation (RFA), or those treated with Transarterial Chemoembolization (TACE). Individuals whose biopsies were taken from newly identified nodules were categorized as having received no previous interventions. Detailed demographic information and patient data are summarized in Table 1.
Consistent with expectations, a predominant number of lesions were identified in patients with chronic viral hepatitis. Specifically, an analysis revealed that 8 of the 9 patients infected with Hepatitis C Virus (HCV) had received antiviral therapy resulting in a sustained virologic response. In the cohort of patients with Hepatitis B Virus (HBV) infection, 3 out of 8 were being treated with nucleoside analogues. Furthermore, a significant difference in alpha-fetoprotein (AFP) levels was observed, with higher AFP levels noted in patients who had not received any prior interventions on the lesion of interest in comparison to those who had undergone prior interventions (p= 0.02, 95% Confidence Interval).
Liver Biopsy Outcomes
For 3 patients who had undergone Transarterial Chemoembolization (TACE) and one patient previously treated with Radiofrequency Ablation (RFA), liver biopsies were repeated due to initial inconclusive outcomes. It is noteworthy that none of the patients experienced complications post-biopsy.
The dimensions of the biopsy samples were approximately 1.2 cm (ranging from 0.7 to 1.5 cm) in patients without prior treatments, 1.1 cm (ranging from 0.6 to 1.3 cm) in those previously subjected to TACE, and 1.2 cm (ranging from 0.8 to 1.4 cm) in the cohort with prior RFA treatments. Histopathological examination of all biopsy specimens confirmed the diagnosis of hepatocellular carcinoma, predominantly demonstrating moderate differentiation as per the Edmondson-Steiner grading system (refer to Table 2).
TACE transarterial chemoembolization; RFA radiofrequency ablation, PD-L1 programmed cell death ligand 1
Additionally, the examination of programmed death-ligand 1 (PD-L1) expression indicated elevated levels in patients who had not undergone any previous treatments, although this difference did not reach statistical significance (p= 0.6, 95% Confidence Interval).
Top of Form
Discussion
Our study revealed that nodule biopsy performed even after a local interventional procedure may bring new information that could impact patient prognosis and establish therapeutic approaches. The patients in our study had moderately differentiated/ poorly differentiated HCC, which translates into a poor prognosis [14], proven by recurrence in patients after TACE or RFA. Increased PD-L1 expression may indicate an increased susceptibility to ICI therapies (atezolizumab/bevacizumab) which may prove a valuable option for tumor reduction and as a neoadjuvant technique for further local interventional procedures [23].
In the setting of advanced imaging techniques, liver biopsy is no longer required for the diagnosis of HCC [24]. Considering the fact that HCC occurs more frequently in cirrhotic patients, with decompensated disease and coagulopathy, the risks of complications increase significantly [25]. These include severe bleeding, abscesses or portal vein thrombosis. A recent meta-analysis revealed that bleeding of any kind occurred in 10.9% of image-guided liver biopsies [26]. In HCC biopsies, a particular complication is seeding of tumor cells along the needle trajectory, which may occur in 1.5% to 5.8% of cases [27]. However, a more recent retrospective study revealed a risk of 0.13% of abdominal wall seeding in liver biopsy alone, and a risk of 1.82% in patients with ablation following biopsy [28].
There is a strong point to be made in favor of avoiding liver biopsy for HCC diagnosis. Imaging techniques such as contrast-enhanced ultrasonography (CEUS) and CT scan have high sensitivity and specificity for HCC (64.1% sensitivity, 97.4% specificity and 73.6% accuracy for CEUS, 62.35% sensitivity, 73.85% specificity and 67.33% accuracy for CT scan) [29,30]. In addition to this, magnetic resonance imaging, particularly using contrast, is more specific for the detection of small HCC lesions [31,32]. Combining the imaging aspects with serum biomarkers such as AFP in a patient with a diagnosed liver disease increases the diagnostic accuracy. Histology diagnosis may be required in the setting of non-cirrhotic patients [5]. Liver biopsy has a varied sensitivity in several studies (ranging from 66% to 93%, depending on tumor and needle size as well as operator experience), with a 100% specificity and positive predictive value [33]. On the other hand, even the LIRADS classification of liver nodules reserves certain cases to be diagnosed by biopsy [11]. This is the case of LR-4 nodules (with a 74% risk of HCC and an 80% risk of malignancy) and LR-TIV (the presence of malignant portal vein thrombus with or without liver nodule). In our study, all LR-4 cases were histologically proven, confirming the imaging diagnosis.
The main advantage of liver biopsy is providing useful markers for prognosis and therapeutic schemes, in the current setting of interventional and systemic options. To this end, one of the most studied markers was the expression of PD-L1 in tumor cells, explored in validation studies for ICI. PD-L1 positive tumors have better response to nivolumab or pembrolizumab compared to sorafenib [34,35]. However, the overall response rates were lower than expected, regardless of PD-L1 expression. It appears that PD-L1 expression in immune cells infiltrating the tumor better correlates to the response to ICI in several solid neoplasia [36]. A recent review argues in favor of using PD-L1 expression on immune cells rather than tumor cells as a prognosis marker for the response to anti PD-1/PD-L1 response [37].
In our study we found an expression of PD-L1 on tumor cells varying between 8.7% and 11.6%, similar to literature data [38]. We did not evaluate the expression of PD-1/PD-L1 in immune cells. This particular line of research is under development, as there are uncertainties regarding the histochemical methods of evaluating this expression, cut-off values and what parameter better associates with patient prognosis. These uncertainties arise from the different methods and antibodies used to determine PD-L1 expression, as this is not yet standardized [39]. Also, PD-L1 expression in tumor cells changes over time and this has not yet been evaluated as a prognostic factor [40]. In addition to this, there are two possible methods of defining PD-L1 positive expression, the proportion of PD-L1 positive tumor cells and the ratio of PD-L1 positive tumor cells and immune cells. The latter appears to be a more reliable marker for prognosis [35].
As an expression of ongoing research in HCC therapies is the high number of clinical trials studying the efficacy of neoadjuvant immune therapy [41]. For example, the use of camrelizumab (PD-1 inhibitor) and apatinib (tyrosine kinase inhibitor) in treatment naïve patients with resectable HCCs led to a major pathologic response in nearly a third of patients [42].
Little data exists on performing tumor biopsy after a local interventional procedure as these patients should be monitored by multimodal imaging according to the international consensus [43]. Histology data in these cases are mostly obtained by analyzing the explanted liver after transplantation. An interesting comparison between non-treated HCCs and post-TACE HCCs revealed that TACE induces morphological changes in the tumor cells (producing a hepatocholangiocellular phenotype) as well as in the tumoral microenvironment (active endothelial proliferation adjacent to the necrotic area [44]. These changes are associated with chemoresistance and a worse outcome. Therefore, the emerging systemic therapies bring into attention the importance of tumor histology for the prognosis of the patients even in the setting of a clear imaging diagnosis [45,46].
Our study has several limitations. First, the number of patients is small and statistical associations lack in strength. In addition to this, the small number of patients made it impossible to corelate pathology findings with the underlying etiology of HCC. Second, since this is a retrospective study, we could not perform liver biopsy before and after local interventional procedures in the same patients, which might have given more valuable information regarding prognostic histology markers. Third, the study did not have as aim to evaluate patient outcomes according to immune therapy response, as there is limited availability for these therapies in our country.
However, we argue that in the setting of limited resources for liver transplantation (a curative therapeutic option for HCC) tumor biopsy and immune histochemical analysis should be performed at any time during patient management, in order to optimize and customize the therapeutic approach. For example, a single center trial showed increased median survival over 3 years in patients with advanced HCC on sequential systemic therapies alone [47].
Conclusion
In conclusion, the practice of conducting biopsies on Hepatocellular Carcinoma (HCC) lesions, even subsequent to local interventional treatments, can be instrumental in unveiling critical data that significantly influences the determination of the most effective treatment strategies for patients. This approach not only has the potential to reveal the HCC phenotype with greater clarity but also to provide insights into the tumor's behavior and response to previous treatments. Such information is invaluable in tailoring personalized therapeutic plans that are more likely to result in successful outcomes.
As the landscape of HCC management evolves with the introduction and integration of new systemic therapies, there is a pressing need to revisit and refine existing protocols for sequencing these treatments. Biopsies, particularly those performed in high-caliber tertiary care centers, are pivotal in this process. They not only contribute to a deeper understanding of the disease at the molecular and cellular levels but also ensure that the data collected can support ongoing clinical trials and systematic reviews. This collaborative and systematic approach to data collection and analysis is essential for advancing the field of HCC treatment.
Moreover, the role of biopsies in identifying the phenotypic characteristics of HCC after local procedures cannot be overstated. By providing a window into the tumor's morphological and molecular changes post-treatment, biopsies can guide the selection of subsequent interventions, including the possibility of incorporating emerging systemic therapies that may be more effective against specific tumor phenotypes or in the context of the tumor's altered microenvironment.
In light of these considerations, it is imperative that the medical community, particularly those specializing in oncology and hepatology, recognize the value of biopsies not just as a diagnostic tool but as a cornerstone of comprehensive patient care in HCC. This entails not only the execution of biopsies with precision and safety but also the integration of biopsy findings into a broader, multidisciplinary discussion on patient management. By doing so, clinicians can ensure that each patient's treatment plan is as informed, nuanced, and effective as possible, ultimately leading to better prognostic outcomes and enhanced quality of life for individuals afflicted with this challenging and complex disease.
References
- Lee HM, Lidofsky SD, Taddei TH, Townshend-Bulson LJ. Attacking the public health crisis of hepatocellular carcinoma at its roots. Hepatology. 2023 Apr 1;77(4):1456-1459. https://doi.org/10.1002/hep.32741. Epub 2022 Oct 11. PMID: 35989555; PMCID: PMC10026951. [CrossRef]
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 Nov;68(6):394-424. https://doi.org/10.3322/caac.21492. Epub 2018 Sep 12. Erratum in: CA Cancer J Clin. 2020 Jul;70(4):313. PMID: 30207593. [CrossRef] [PubMed]
- Rumgay H, Arnold M, Ferlay J, Lesi O, Cabasag CJ, Vignat J, Laversanne M, McGlynn KA, Soerjomataram I. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022 Dec;77(6):1598-1606. https://doi.org/10.1016/j.jhep.2022.08.021. Epub 2022 Oct 5. PMID: 36208844; PMCID: PMC9670241. [CrossRef]
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018 Mar 31;391(10127):1301-1314. https://doi.org/10.1016/S0140-6736(18)30010-2. Epub 2018 Jan 5. PMID: 29307467. [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018 Jul;69(1):182-236. https://doi.org/10.1016/j.jhep.2018.03.019. Epub 2018 Apr 5. Erratum in: J Hepatol. 2019 Apr;70(4):817. PMID: 29628281. [CrossRef]
- Valery PC, Laversanne M, Clark PJ, Petrick JL, McGlynn KA, Bray F. Projections of primary liver cancer to 2030 in 30 countries worldwide. Hepatology. 2018 Feb;67(2):600-611. https://doi.org/10.1002/hep.29498. Epub 2017 Dec 23. PMID: 28859220; PMCID: PMC5832532. [CrossRef]
- Singal AG, Llovet JM, Yarchoan M, Mehta N, Heimbach JK, Dawson LA, Jou JH, Kulik LM, Agopian VG, Marrero JA, Mendiratta-Lala M, Brown DB, Rilling WS, Goyal L, Wei AC, Taddei TH. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023 May 22. https://doi.org/10.1097/HEP.0000000000000466. Epub ahead of print. Erratum in: Hepatology. 2023 Oct 16;: PMID: 37199193. [CrossRef] [PubMed]
- Eisenbrey JR, Gabriel H, Savsani E, Lyshchik A. Contrast-enhanced ultrasound (CEUS) in HCC diagnosis and assessment of tumor response to locoregional therapies. Abdom Radiol (NY). 2021 Aug;46(8):3579-3595. https://doi.org/10.1007/s00261-021-03059-y. Epub 2021 Apr 7. PMID: 33825927; PMCID: PMC8569604. [CrossRef]
- Matsui O, Kobayashi S, Sanada J, Kouda W, Ryu Y, Kozaka K, Kitao A, Nakamura K, Gabata T. Hepatocelluar nodules in liver cirrhosis: hemodynamic evaluation (angiography-assisted CT) with special reference to multi-step hepatocarcinogenesis. Abdom Imaging. 2011 Jun;36(3):264-72. https://doi.org/10.1007/s00261-011-9685-1. PMID: 21267562; PMCID: PMC3102849. [CrossRef]
- Huang P, Wu F, Hou K, Zhou C, Xiao Y, Wang C, Miao G, Yang C, Zeng M. Diagnostic algorithm for subcentimeter hepatocellular carcinoma using alpha-fetoprotein and imaging features on gadoxetic acid-enhanced MRI. Eur Radiol. 2023 Oct 4. https://doi.org/10.1007/s00330-023-10214-0. Epub ahead of print. PMID: 37792079. [CrossRef]
- Lee YT, Wang JJ, Zhu Y, Agopian VG, Tseng HR, Yang JD. Diagnostic Criteria and LI-RADS for Hepatocellular Carcinoma. Clin Liver Dis (Hoboken). 2021 Aug 5;17(6):409-413. https://doi.org/10.1002/cld.1075. PMID: 34386205; PMCID: PMC8340355. [CrossRef]
- Chernyak V, Fowler KJ, Kamaya A, Kielar AZ, Elsayes KM, Bashir MR, Kono Y, Do RK, Mitchell DG, Singal AG, Tang A, Sirlin CB. Liver Imaging Reporting and Data System (LI-RADS) Version 2018: Imaging of Hepatocellular Carcinoma in At-Risk Patients. Radiology. 2018 Dec;289(3):816-830. https://doi.org/10.1148/radiol.2018181494. Epub 2018 Sep 25. PMID: 30251931; PMCID: PMC6677371. [CrossRef]
- Tremosini S, Forner A, Boix L, Vilana R, Bianchi L, Reig M, Rimola J, Rodríguez-Lope C, Ayuso C, Solé M, Bruix J. Prospective validation of an immunohistochemical panel (glypican 3, heat shock protein 70 and glutamine synthetase) in liver biopsies for diagnosis of very early hepatocellular carcinoma. Gut. 2012 Oct;61(10):1481-7. https://doi.org/10.1136/gutjnl-2011-301862. Epub 2012 Jan 27. PMID: 22287594. [CrossRef]
- Park BV, Gaba RC, Huang YH, Chen YF, Guzman G, Lokken RP. Histology of Hepatocellular Carcinoma: Association with Clinical Features, Radiological Findings, and Locoregional Therapy Outcomes. J Clin Imaging Sci. 2019 Nov 18;9:52. https://doi.org/10.25259/JCIS_111_2019. PMID: 31819829; PMCID: PMC6884980. [CrossRef]
- Reig M, Forner A, Rimola J, Ferrer-Fàbrega J, Burrel M, Garcia-Criado Á, Kelley RK, Galle PR, Mazzaferro V, Salem R, Sangro B, Singal AG, Vogel A, Fuster J, Ayuso C, Bruix J. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. 2022 Mar;76(3):681-693. https://doi.org/10.1016/j.jhep.2021.11.018. Epub 2021 Nov 19. PMID: 34801630; PMCID: PMC8866082. [CrossRef]
- Bruix J, Chan SL, Galle PR, Rimassa L, Sangro B. Systemic treatment of hepatocellular carcinoma: An EASL position paper. J Hepatol. 2021 Oct;75(4):960-974. https://doi.org/10.1016/j.jhep.2021.07.004. Epub 2021 Jul 10. PMID: 34256065. [CrossRef] [PubMed]
- He Y, Lu M, Che J, Chu Q, Zhang P, Chen Y. Biomarkers and Future Perspectives for Hepatocellular Carcinoma Immunotherapy. Front Oncol. 2021 Sep 6;11:716844. https://doi.org/10.3389/fonc.2021.716844. PMID: 34552872; PMCID: PMC8450565. [CrossRef]
- Yau T, Park JW, Finn RS, Cheng AL, Mathurin P, Edeline J, Kudo M, Harding JJ, Merle P, Rosmorduc O, Wyrwicz L, Schott E, Choo SP, Kelley RK, Sieghart W, Assenat E, Zaucha R, Furuse J, Abou-Alfa GK, El-Khoueiry AB, Melero I, Begic D, Chen G, Neely J, Wisniewski T, Tschaika M, Sangro B. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022 Jan;23(1):77-90. https://doi.org/10.1016/S1470-2045(21)00604-5. Epub 2021 Dec 13. PMID: 34914889. [CrossRef] [PubMed]
- Ji JH, Ha SY, Lee D, Sankar K, Koltsova EK, Abou-Alfa GK, Yang JD. Predictive Biomarkers for Immune-Checkpoint Inhibitor Treatment Response in Patients with Hepatocellular Carcinoma. Int J Mol Sci. 2023 Apr 21;24(8):7640. https://doi.org/10.3390/ijms24087640. PMID: 37108802; PMCID: PMC10144688. [CrossRef]
- Calderaro J, Rousseau B, Amaddeo G, Mercey M, Charpy C, Costentin C, Luciani A, Zafrani ES, Laurent A, Azoulay D, Lafdil F, Pawlotsky JM. Programmed death ligand 1 expression in hepatocellular carcinoma: Relationship With clinical and pathological features. Hepatology. 2016 Dec;64(6):2038-2046. https://doi.org/10.1002/hep.28710. Epub 2016 Aug 9. PMID: 27359084. [CrossRef]
- Cheng AL, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, Lim HY, Kudo M, Breder V, Merle P, Kaseb AO, Li D, Verret W, Ma N, Nicholas A, Wang Y, Li L, Zhu AX, Finn RS. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022 Apr;76(4):862-873. https://doi.org/10.1016/j.jhep.2021.11.030. Epub 2021 Dec 11. PMID: 34902530. [CrossRef]
- http://www.casan.ro/casbz/media/pageFiles/201)%20L01XC32.5-ATEZOLIZUMAB%20carcinom%20hepatocelular.pdf.
- Chiang CL, Chan ACY, Chiu KWH, Kong FS. Combined Stereotactic Body Radiotherapy and Checkpoint Inhibition in Unresectable Hepatocellular Carcinoma: A Potential Synergistic Treatment Strategy. Front Oncol. 2019 Nov 12;9:1157. https://doi.org/10.3389/fonc.2019.01157. PMID: 31799176; PMCID: PMC6874138. [CrossRef]
- Finn RS. The Role of Liver Biopsy in Hepatocellular Carcinoma. Gastroenterol Hepatol (N Y). 2016 Oct;12(10):628-630. PMID: 27917077; PMCID: PMC5114505.
- Seeff LB, Everson GT, Morgan TR, Curto TM, Lee WM, Ghany MG, Shiffman ML, Fontana RJ, Di Bisceglie AM, Bonkovsky HL, Dienstag JL; HALT–C Trial Group. Complication rate of percutaneous liver biopsies among persons with advanced chronic liver disease in the HALT-C trial. Clin Gastroenterol Hepatol. 2010 Oct;8(10):877-83. https://doi.org/10.1016/j.cgh.2010.03.025. Epub 2010 Apr 1. PMID: 20362695; PMCID: PMC3771318. [CrossRef]
- Midia M, Odedra D, Shuster A, Midia R, Muir J. Predictors of bleeding complications following percutaneous image-guided liver biopsy: a scoping review. Diagn Interv Radiol. 2019 Jan;25(1):71-80. https://doi.org/10.5152/dir.2018.17525. PMID: 30644369; PMCID: PMC6339629. [CrossRef]
- Silva MA, Hegab B, Hyde C, Guo B, Buckels JA, Mirza DF. Needle track seeding following biopsy of liver lesions in the diagnosis of hepatocellular cancer: a systematic review and meta-analysis. Gut. 2008 Nov;57(11):1592-6. https://doi.org/10.1136/gut.2008.149062. Epub 2008 Jul 31. PMID: 18669577. [CrossRef] [PubMed]
- Szpakowski JL, Drasin TE, Lyon LL. Rate of seeding with biopsies and ablations of hepatocellular carcinoma: A retrospective cohort study. Hepatol Commun. 2017 Sep 29;1(9):841-851. https://doi.org/10.1002/hep4.1089. PMID: 29404497; PMCID: PMC5721456. [CrossRef]
- Liu GJ, Wang W, Lu MD, Xie XY, Xu HX, Xu ZF, Chen LD, Wang Z, Liang JY, Huang Y, Li W, Liu JY. Contrast-Enhanced Ultrasound for the Characterization of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Liver Cancer. 2015 Dec;4(4):241-52. https://doi.org/10.1159/000367738. Epub 2015 Oct 21. PMID: 26779444; PMCID: PMC4702012. [CrossRef]
- Wang G, Zhu S, Li X. Comparison of values of CT and MRI imaging in the diagnosis of hepatocellular carcinoma and analysis of prognostic factors. Oncol Lett. 2019 Jan;17(1):1184-1188. https://doi.org/10.3892/ol.2018.9690. Epub 2018 Nov 12. PMID: 30655882; PMCID: PMC6312947. [CrossRef]
- Semaan S, Vietti Violi N, Lewis S, Chatterji M, Song C, Besa C, Babb JS, Fiel MI, Schwartz M, Thung S, Sirlin CB, Taouli B. Hepatocellular carcinoma detection in liver cirrhosis: diagnostic performance of contrast-enhanced CT vs. MRI with extracellular contrast vs. gadoxetic acid. Eur Radiol. 2020 Feb;30(2):1020-1030. https://doi.org/10.1007/s00330-019-06458-4. Epub 2019 Oct 31. PMID: 31673837. [CrossRef] [PubMed]
- Peng J, Zheng J, Yang C, Wang R, Zhou Y, Tao YY, Gong XQ, Wang WC, Zhang XM, Yang L. Intravoxel incoherent motion diffusion-weighted imaging to differentiate hepatocellular carcinoma from intrahepatic cholangiocarcinoma. Sci Rep. 2020 May 7;10(1):7717. https://doi.org/10.1038/s41598-020-64804-9. PMID: 32382050; PMCID: PMC7206040. [CrossRef]
- Di Tommaso L, Spadaccini M, Donadon M, Personeni N, Elamin A, Aghemo A, Lleo A. Role of liver biopsy in hepatocellular carcinoma. World J Gastroenterol. 2019 Oct 28;25(40):6041-6052. https://doi.org/10.3748/wjg.v25.i40.6041. PMID: 31686761; PMCID: PMC6824282. [CrossRef]
- Yau T, Park JW, Finn RS, Cheng AL, Mathurin P, Edeline J, Kudo M, Harding JJ, Merle P, Rosmorduc O, Wyrwicz L, Schott E, Choo SP, Kelley RK, Sieghart W, Assenat E, Zaucha R, Furuse J, Abou-Alfa GK, El-Khoueiry AB, Melero I, Begic D, Chen G, Neely J, Wisniewski T, Tschaika M, Sangro B. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022 Jan;23(1):77-90. https://doi.org/10.1016/S1470-2045(21)00604-5. Epub 2021 Dec 13. PMID: 34914889. [CrossRef] [PubMed]
- Zhu AX, Finn RS, Edeline J, Cattan S, Ogasawara S, Palmer D, Verslype C, Zagonel V, Fartoux L, Vogel A, Sarker D, Verset G, Chan SL, Knox J, Daniele B, Webber AL, Ebbinghaus SW, Ma J, Siegel AB, Cheng AL, Kudo M; KEYNOTE-224 investigators. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018 Jul;19(7):940-952. https://doi.org/10.1016/S1470-2045(18)30351-6. Epub 2018 Jun 3. Erratum in: Lancet Oncol. 2018 Sep;19(9):e440. PMID: 29875066. [CrossRef] [PubMed]
- Powles T, Eder JP, Fine GD, Braiteh FS, Loriot Y, Cruz C, Bellmunt J, Burris HA, Petrylak DP, Teng SL, Shen X, Boyd Z, Hegde PS, Chen DS, Vogelzang NJ. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. 2014 Nov 27;515(7528):558-62. https://doi.org/10.1038/nature13904. PMID: 25428503. [CrossRef] [PubMed]
- Kleinovink JW, van Hall T, Ossendorp F, Fransen MF. PD-L1 immune suppression in cancer: Tumor cells or host cells? Oncoimmunology. 2017 May 12;6(7):e1325982. https://doi.org/10.1080/2162402X.2017.1325982. PMID: 28811961; PMCID: PMC5543902. [CrossRef]
- Pinato DJ, Mauri FA, Spina P, Cain O, Siddique A, Goldin R, Victor S, Pizio C, Akarca AU, Boldorini RL, Mazzucchelli L, Black JRM, Shetty S, Marafioti T, Sharma R. Clinical implications of heterogeneity in PD-L1 immunohistochemical detection in hepatocellular carcinoma: the Blueprint-HCC study. Br J Cancer. 2019 May;120(11):1033-1036. https://doi.org/10.1038/s41416-019-0466-x. Epub 2019 May 7. PMID: 31061454; PMCID: PMC6738063. [CrossRef]
- Yi M, Jiao D, Xu H, Liu Q, Zhao W, Han X, Wu K. Biomarkers for predicting efficacy of PD-1/PD-L1 inhibitors. Mol Cancer. 2018 Aug 23;17(1):129. https://doi.org/10.1186/s12943-018-0864-3. PMID: 30139382; PMCID: PMC6107958. [CrossRef]
- Vilain RE, Menzies AM, Wilmott JS, Kakavand H, Madore J, Guminski A, Liniker E, Kong BY, Cooper AJ, Howle JR, Saw RPM, Jakrot V, Lo S, Thompson JF, Carlino MS, Kefford RF, Long GV, Scolyer RA. Dynamic Changes in PD-L1 Expression and Immune Infiltrates Early During Treatment Predict Response to PD-1 Blockade in Melanoma. Clin Cancer Res. 2017 Sep 1;23(17):5024-5033. https://doi.org/10.1158/1078-0432.CCR-16-0698. Epub 2017 May 16. PMID: 28512174. [CrossRef] [PubMed]
- Rallis KS, Makrakis D, Ziogas IA, Tsoulfas G. Immunotherapy for advanced hepatocellular carcinoma: From clinical trials to real-world data and future advances. World J Clin Oncol. 2022 Jun 24;13(6):448-472. https://doi.org/10.5306/wjco.v13.i6.448. PMID: 35949435; PMCID: PMC9244967. [CrossRef]
- Xia Y, Tang W, Qian X, Li X, Cheng F, Wang K, Zhang F, Zhang C, Li D, Song J, Zhang H, Zhao J, Yao A, Wu X, Wu C, Ji G, Liu X, Zhu F, Qin L, Xiao X, Deng Z, Kong X, Li S, Yu Y, Xi W, Deng W, Qi C, Liu H, Pu L, Wang P, Wang X. Efficacy and safety of camrelizumab plus apatinib during the perioperative period in resectable hepatocellular carcinoma: a single-arm, open label, phase II clinical trial. J Immunother Cancer. 2022 Apr;10(4):e004656. https://doi.org/10.1136/jitc-2022-004656. PMID: 35379737; PMCID: PMC8981365. [CrossRef]
- Maas M, Beets-Tan R, Gaubert JY, Gomez Munoz F, Habert P, Klompenhouwer LG, Vilares Morgado P, Schaefer N, Cornelis FH, Solomon SB, van der Reijd D, Bilbao JI. Follow-up after radiological intervention in oncology: ECIO-ESOI evidence and consensus-based recommendations for clinical practice. Insights Imaging. 2020 Jul 16;11(1):83. https://doi.org/10.1186/s13244-020-00884-5. PMID: 32676924; PMCID: PMC7366866. [CrossRef]
- Zen C, Zen Y, Mitry RR, Corbeil D, Karbanová J, O'Grady J, Karani J, Kane P, Heaton N, Portmann BC, Quaglia A. Mixed phenotype hepatocellular carcinoma after transarterial chemoembolization and liver transplantation. Liver Transpl. 2011 Aug;17(8):943-54. https://doi.org/10.1002/lt.22314. PMID: 21491582. [CrossRef] [PubMed]
- Russo FP, Imondi A, Lynch EN, Farinati F. When and how should we perform a biopsy for HCC in patients with liver cirrhosis in 2018? A review. Dig Liver Dis. 2018 Jul;50(7):640-646. https://doi.org/10.1016/j.dld.2018.03.014. Epub 2018 Mar 20. PMID: 29636240. [CrossRef] [PubMed]
- Ciuhu AN, Rahnea-Nita G, Popescu M, Rahnea-Nita RA. Abstract P5-15-22: Evaluation of quality of life in patients with advanced and metastatic breast cancer proposed for palliative chemotherapy and best supportive care versus best supportive care. Cancer Res. 2015, 75, P5-15-22. https://doi.org/10.1158/1538-7445.SABCS14-P5-15-22. [CrossRef]
- von Felden J, Karkmann K, Ittrich H, Gil-Ibanez I, Fründt T, Krause J, Lohse AW, Wege H, Schulze K. Sequential Systemic Treatment in Advanced Hepatocellular Carcinoma Is Able to Prolong Median Survival to More than 3 Years in a Selected Real-World Cohort. Visc Med. 2021 Mar;37(2):87-93. https://doi.org/10.1159/000507381. Epub 2020 May 7. PMID: 33981749; PMCID: PMC8077524. [CrossRef]
Figure 1.
CT imaging of HCC in an 84 years old patient before and after interventional therapy. Initial contrast enhanced CT showing a 45/50mm tumor in the 7th segment, with arterial hyperenhancement (a) and portal wash-out (b). CT imaging after TACE and RFA showing no hyperenhancement in the arterial phase (c) and no wash-out in the portal phase (d).
Figure 1.
CT imaging of HCC in an 84 years old patient before and after interventional therapy. Initial contrast enhanced CT showing a 45/50mm tumor in the 7th segment, with arterial hyperenhancement (a) and portal wash-out (b). CT imaging after TACE and RFA showing no hyperenhancement in the arterial phase (c) and no wash-out in the portal phase (d).
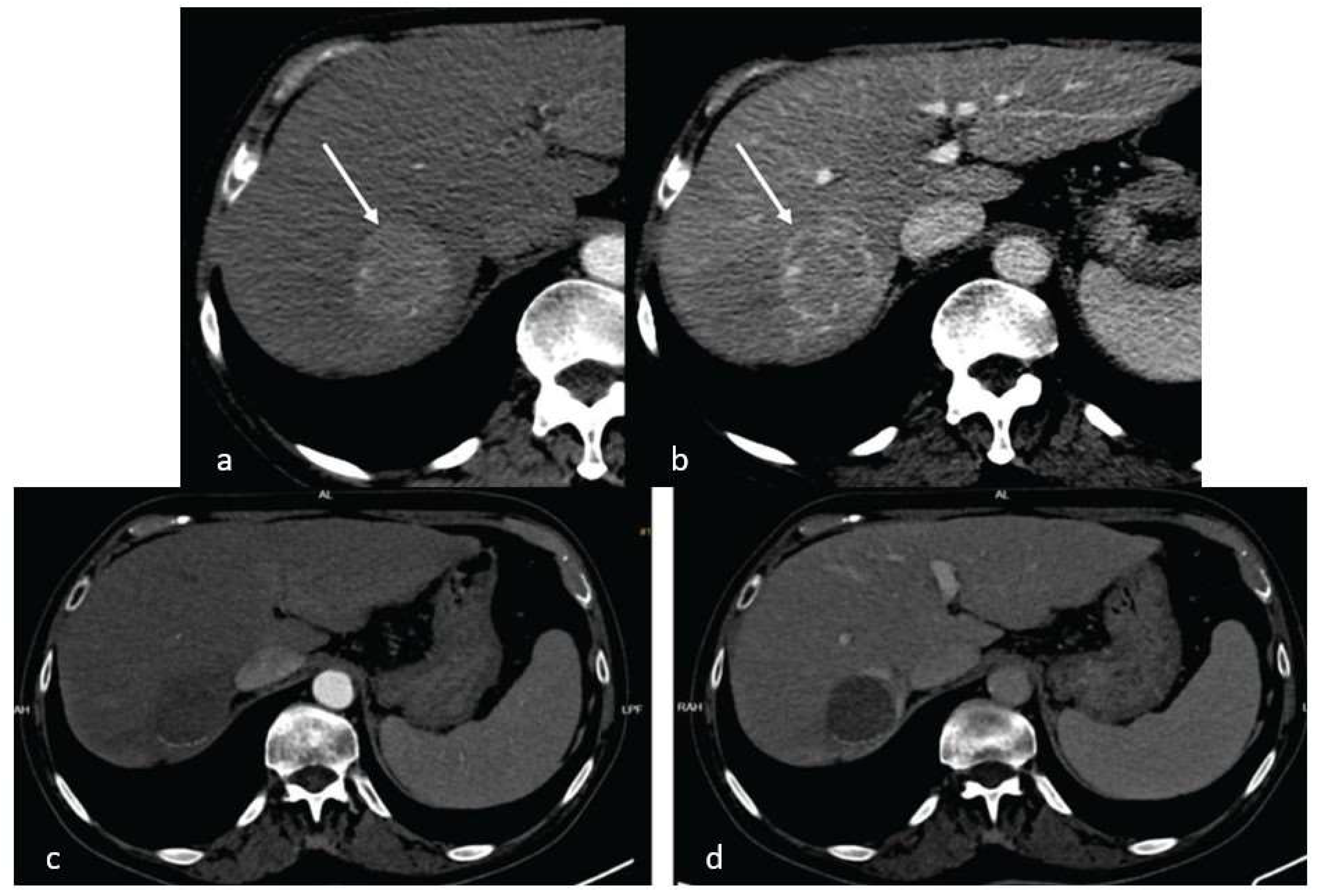
Figure 2.
Histology aspects of HCC. A). increased N/C ratio, macronucleoli, hyaline globules (hematoxylin eosin stain x400). B) Cellular monomorphism suggestive for malignancy (hematoxylin eosin stain x400). C) Trabecular pattern (hematoxylin eosin stain x20). D). PD-L1 overexpression in HCC cells.
Figure 2.
Histology aspects of HCC. A). increased N/C ratio, macronucleoli, hyaline globules (hematoxylin eosin stain x400). B) Cellular monomorphism suggestive for malignancy (hematoxylin eosin stain x400). C) Trabecular pattern (hematoxylin eosin stain x20). D). PD-L1 overexpression in HCC cells.
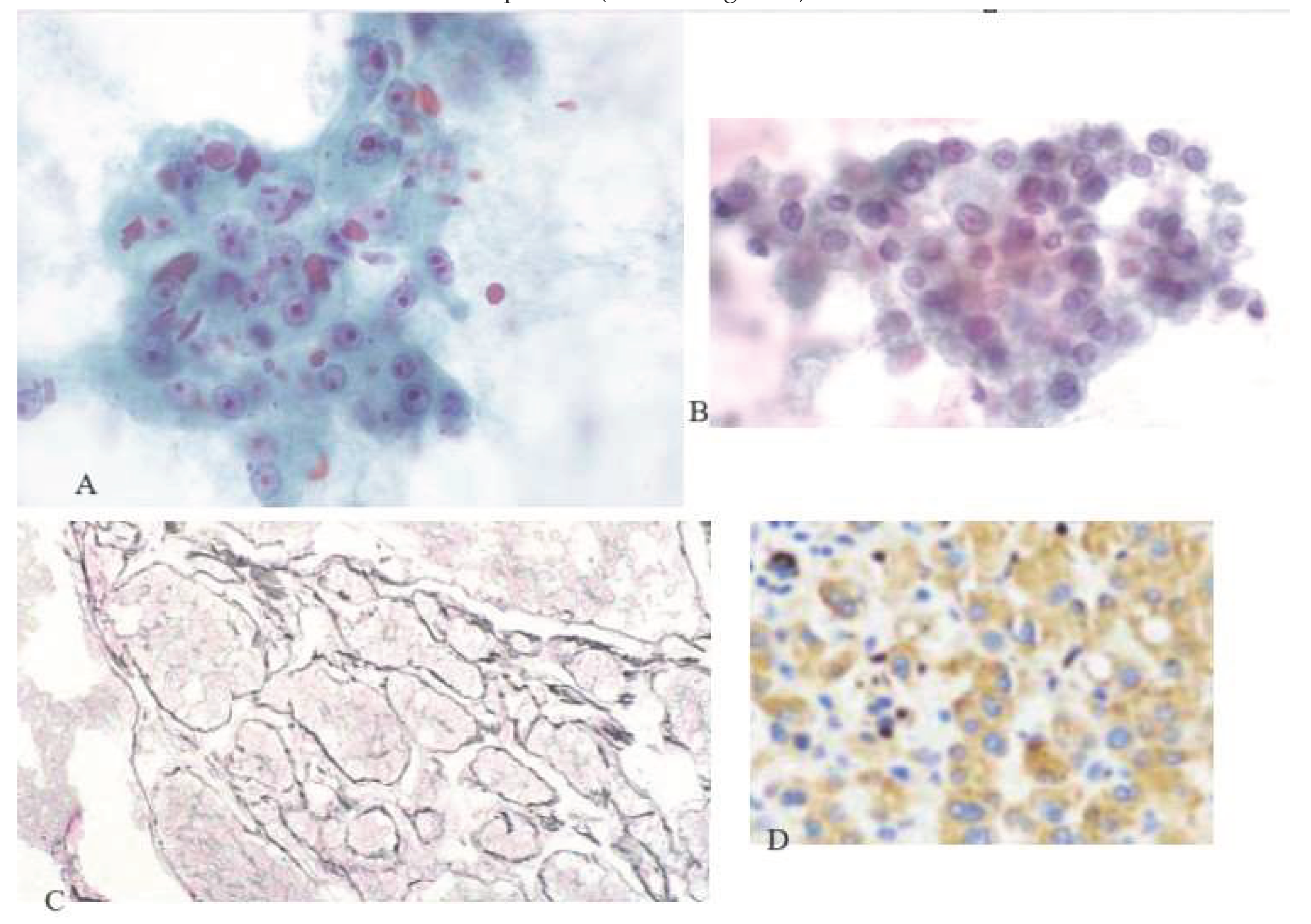

Table 1.
Demographic and imaging data.
| No previous interventions (N= 10 patients) |
Previous TACE (N= 9 patients) |
Previous RFA (N= 4 patients) |
|
| Etiology of liver disease | HCV cirrhosis: 2 patients (20%) HBV cirrhosis: 5 patients (50%) NASH cirrhosis: 1 patient (10%) HBV +HDV hepatitis: 2 patients (20%) |
HCV cirrhosis: 5 patients (55.5%) HBV hepatitis: 1 patient (11.1%) HBV + HDV hepatitis: 2 patients (22.2%) NASH cirrhosis: 1 patient (11.1%) |
HCV cirrhosis: 2 patients (50%) HBV hepatitis: 1 patient (25%) HBV cirrhosis: 1 patient (25%) |
| AFP (N: 0 - 8.1 ng/ml) |
380.52 +/- 134.83 | 112.56 +/- 45.24 | 135 +/- 46.13 |
| LI-RADS score | LR- 4: 2 patients (20%) LR- 5: 8 patients (80%) |
LR- 4: 2 patients (22.2%) LR-5: 7 patients (77.7%) |
LR- 4: 1 patient (25%) LR- 5: 3 patients (75%) |
| Number of nodules | 1-3: 8 patients (80%) >3: 2 patients (20%) |
1-3: 6 patients (66.6%) >3: 3 patients (33.3%) |
1-3: 3 patients (75%) >3: 1 patient (25%) |
| Size of nodule of interest | Median 3.5 cm Range 1.6-5.2 cm |
Median 2.4 cm Range 1.8- 3.7 |
Median 2.2 cm Range 2.1-2.5 cm |
| Portal vein invasion | Yes – 4 patients (40%) | Yes- 2 patients (22.2%) | Yes- 0 patients (0%) |
Table 2.
Histology and immunohistochemistry analysis of biopsies.
| No previous interventions (N= 10 patients) |
Previous TACE (N= 9 patients) |
Previous RFA (N= 4 patients) |
|
| Edmondson – Steiner | Grade II: 4 patients (40%) Grade III: 5 patients (50%) Grade IV: 1 patient (1%) |
Grade II: 3 patients (33.3%) Grade III: 6 patients (66.6%) |
Grade II: 1 patient (25%) Grade III: 3 patients (75%) |
| PD-L1 expression | 11.6% | 8.7% | 9.4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



