
Submitted:
04 March 2024
Posted:
06 March 2024
You are already at the latest version
Abstract
BackgroundThe use of antimicrobials to treat food animals may result in antimicrobial residues in foodstuffs of animal origin. The European Medicines Association (EMA) and World Health Organization (WHO) define safe antimicrobial concentrations in food based on acceptable daily intakes (ADIs). It is unknown if ADI doses of antimicrobials in food could influence the antimicrobial susceptibility of human-associated bacteria. ObjectivesThis aim of this study was to evaluate if the consumption of ADI doses of erythromycin could select for erythromycin resistance in a Galleria mellonella model of Streptococcus pneumoniae infection. Methods A chronic model of S. pneumoniae infection in G. mellonella larvae was used for the experiment. Inoculation of larvae with S. pneumoniae was followed by injections of EMA (0.0875 μg/ml) and WHO (0.012 μg/ml) ADI doses of erythromycin proceeded by isolation of S. pneumoniae colonies on selective agar plates. Minimum inhibitory concentrations (MICs) of resistant colonies were measured, and whole genome sequencing (WGS) was performed followed by variant calling to determine the genetic modifications. Results Exposure to single doses of both EMA and WHO ADI doses of erythromycin resulted in the emergence of erythromycin resistance in S. pneumoniae. Emergent resistance to erythromycin was associated with a mutation in rplA. Conclusion In our in vivo model, even single dose of erythromycin that are classified as acceptable by the WHO and EMA induced significant increases in erythromycin MICs in S. pneumoniae. These results suggest the need to include the induction of antimicrobial resistance (AMR) as a significant criterion for determining ADIs.
Keywords:
S. pneumoniae
; erythromycin
; AMR
; MSC (minimal selective concentration)
; G. mellonella
; ADI (acceptable daily intake)
; MRL (maximum residue limit)
; HGT (horizontal gene transfer)
Introduction
There is increasing evidence that low concentrations of antimicrobials can select for antimicrobial resistance (AMR). Studies have found that antimicrobial concentrations over 200-fold lower than the minimum inhibitory concentration (MIC) select for resistant versus susceptible strains of Escherichia coli and Salmonella enterica spp. [1,2]. These studies have defined the minimal selective concentration (MSC) as the minimum concentration of an antimicrobial that selects for antimicrobial resistance [1,3]. Two types of MSC have been defined. The MSCdenovo is defined as the minimum concentration of an antimicrobial at which one can induce de novo resistance. The MSCselect is the lowest antimicrobial concentration that selects for a resistant compared to a susceptible strain [4]. Gullberg et al. found the E. coli ciprofloxacin MSCselect to be 230-fold lower than MIC, and the MSCdenovo to be at least tenfold lower than the MIC [3].
Much remains unknown about the MSCs for macrolides. The E. coli erythromycin MSCselect has been found to be less than 0.200 µg/mL, which is less than 1/60th of the MIC [1]. Stanton et al. determined the erythromycin MSCselect for the ermF gene in a complex microbial community to be a similar concentration - 0.514 µg/mL [2]. Theoretical MSCs for the most susceptible species can be calculated by applying the ratio between the MIC and MSC from a species where this has been measured, such as E. coli, to the species with the lowest MIC for the antimicrobial in the EUCAST dataset [5,6]. This predicted MSC value (PMSC) has been calculated to be 0.13 µg/mL for erythromycin [6]. Macrolide MSCs have not been evaluated for other bacterial species and have never been assessed in vivo. Testing MSCs in vivo is particularly important since previous studies have found that MSCs are typically higher in complex polymicrobial environments [2]. A crucial hypothesis to test is if the concentrations of antimicrobials allowed in food can induce AMR in pathobionts colonizing humans. This hypothesis has been raised by authors who have found evidence that the consumption of antimicrobials such as macrolides by food-producing animals is independently correlated with AMR in humans [7,8,9]. For example, an integrated analysis of the consumption of antimicrobials revealed positive association between macrolide use in animal farming and macrolide resistance in Campylobacter spp. in humans [10]. Another study has found that antibiotic consumption in animals was linked to resistance in some priority human pathogens [11]. A related investigation found that reducing the use of macrolides in food-producing animals was associated with a decrease in bacterial macrolide resistance in both animals and humans [12]. Another ecological study found a positive association between the intensity of macrolides used for food-producing animals and the prevalence of macrolide resistance in Streptococcus pneumoniae [9].
These findings provided the rationale for the central hypothesis tested in this paper: can the amount of erythromycin allowed in food induce erythromycin resistance in S. pneumoniae? More specifically, we use an in vivo model to test if the acceptable daily intake (ADI) of erythromycin, according to the European Medicines Agency (EMA) and World Health Organization (WHO)/Food and Agriculture Organization (FAO) is able to induce resistance to erythromycin. The ADI is defined by the FAO/WHO as “an estimate of the amount of a food additive in food or beverages expressed on a body weight (bw) basis that can be ingested daily over a lifetime without appreciable health risk to the consumer” [13]. The ADI of a medicinal compound is based on studies evaluating thresholds for different types of toxicity [14,15]. For the macrolides, EMA ADIs are determined based on microbiological toxicity [16,17,18]. These are established by evaluating the MICs for human bacterial commensal species and calculating estimated dose exposures in the human colon [19,20]. EMA and WHO/FAO use the ADIs and other information such as dietary exposure to the relevant foodstuff to set maximum residue limits (MRLs). The WHO/FAO define the MRL as “the maximum concentration of residue resulting from the use of a veterinary drug (expressed in mg/kg or μg/kg on a fresh weight basis) that is recommended by the CAC to be legally permitted or recognized as acceptable in or on a food” [21]. The MRL is set at a level that ensures that the residues in food do not exceed the ADI [13,19,21]. In their assessments of ADIs and MRLs of antimicrobials in food products, the EMA and WHO/FAO guidelines do not include induction of resistance [21,22].
The most recent EMA reports concluded that the ADI of erythromycin is 5 μg/kg/body weight (bw) [17,23]. The Joint FAO/WHO Expert Committee on Food Additives (JECFA) set a lower erythromycin ADI of 0.7 μg/kg/bw [22]. We hypothesized that both these doses could induce erythromycin resistance in vivo. We tested this hypothesis in a Galleria mellonella model of chronic S. pneumoniae infection treated with ADI equivalent concentrations of erythromycin. Several studies have established that G. mellonella offers a useful model of human-microbial interactions [24,25].
Materials and Methods
Bacterial strain and live microbial inoculum preparation
Streptococcus pneumoniae strain (ATCC 49619) with a low erythromycin MIC (0.064 mg/L) was selected for the experiment. The selected strain of S. pneumoniae was cultured from the frozen stock onto Mueller Hinton Agar (MHA) + 5% horse blood (bioMérieux) at 37°C overnight. Single colonies were selected from this culture and spread onto fresh agar plates, which were incubated at 37°C with 5% (v/v) CO2 overnight. The S. pneumoniae was then inoculated into the haemocoel of the G. mellonella larva (10 μL of PBS containing 550 x 103 CFU of S. pneumoniae). This dose of S. pneumoniae was determined based on experiments that established a dose that enabled recovery of the bacteria up to 6 days post- inoculation without an excessive mortality rate of the G. mellonella (data not shown).
Injection of G. mellonella larvae
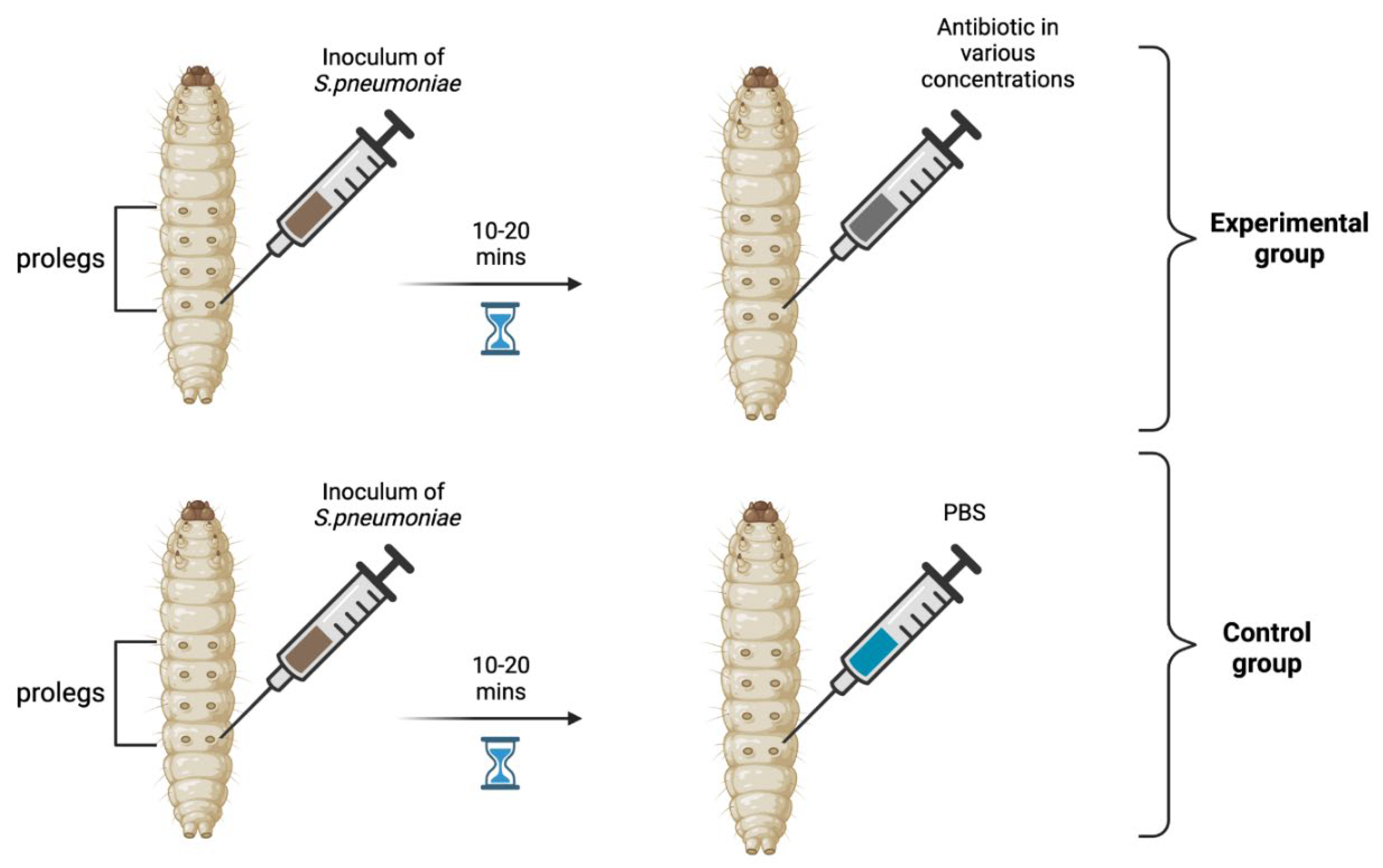
The last larval stage G. mellonella (Terramania, Arnhem, NL) was used for the experiments. Only macroscopically healthy, non-discolored larvae 300 to 400 mg were selected (Table S1). The larvae were placed into individual Petri dishes in groups of 10 per dish. The larvae were kept in an incubator at 37°C with a 5% (v/v) CO2 atmosphere for the duration of the experiments. Each control and experimental group consisted of 20 larvae (1ADI EMA erythromycin, 10ADI EMA erythromycin, 1ADI WHO erythromycin, 0.1ADI WHO erythromycin). The larvae were injected in the last pro-leg with 10 μL of bacterial suspension followed 10-20 minutes later by various doses (see below) of erythromycin (Erythromycin lactobionate, Amdipharm, Basildon, UK) using 0.3mL U-100 insulin syringes BD Micro-Fine (Figure 1). One syringe and needle were used for 10 larvae in each Petri dish.
Figure 1.
Visual scheme illustrating injection of G. mellonella larvae in the last pro-leg with bacterial suspension of S. pneumoniae followed 10-20 minutes later by various doses of erythromycin (experimental group) or PBS (control group).
Figure 1.
Visual scheme illustrating injection of G. mellonella larvae in the last pro-leg with bacterial suspension of S. pneumoniae followed 10-20 minutes later by various doses of erythromycin (experimental group) or PBS (control group).
Concentration of erythromycin for injection
EMA acceptable daily intake (ADI) of erythromycin (5 μg/kg/body weight) [17,23] translates into a dose of 1.75 ng for 350 mg G. mellonella – the average weight of the larvae used in our experiment (Table S1). In contrast, JECFA/WHO ADI of erythromycin is 0.7 μg/kg/bw [22]. This translates into a dose of 0.25 ng for 350 mg G. mellonella. We assessed the effects of four doses of erythromycin on AMR – 0.025 ng (0.1ADI WHO), 0.25 ng (1ADI WHO), 1.75 ng (1ADI EMA) and 17.5 ng (10ADI EMA). For all experiments, a control group was included that received the same protocol – bacterial inoculation followed by 10 μL/larva of PBS.
Retrieval of S. pneumoniae from G. mellonella
24 hours after the injection of the bacteria and at 24 hourly intervals thereafter, the mortality of each group of larvae were assessed and 1-2 larvae from each group of 10 larvae were randomly selected for extraction of hemolymph. This was continued for the duration of the experiments – 6 days. The larvae were considered dead when there were no signs of movement in response to external prodding [26].
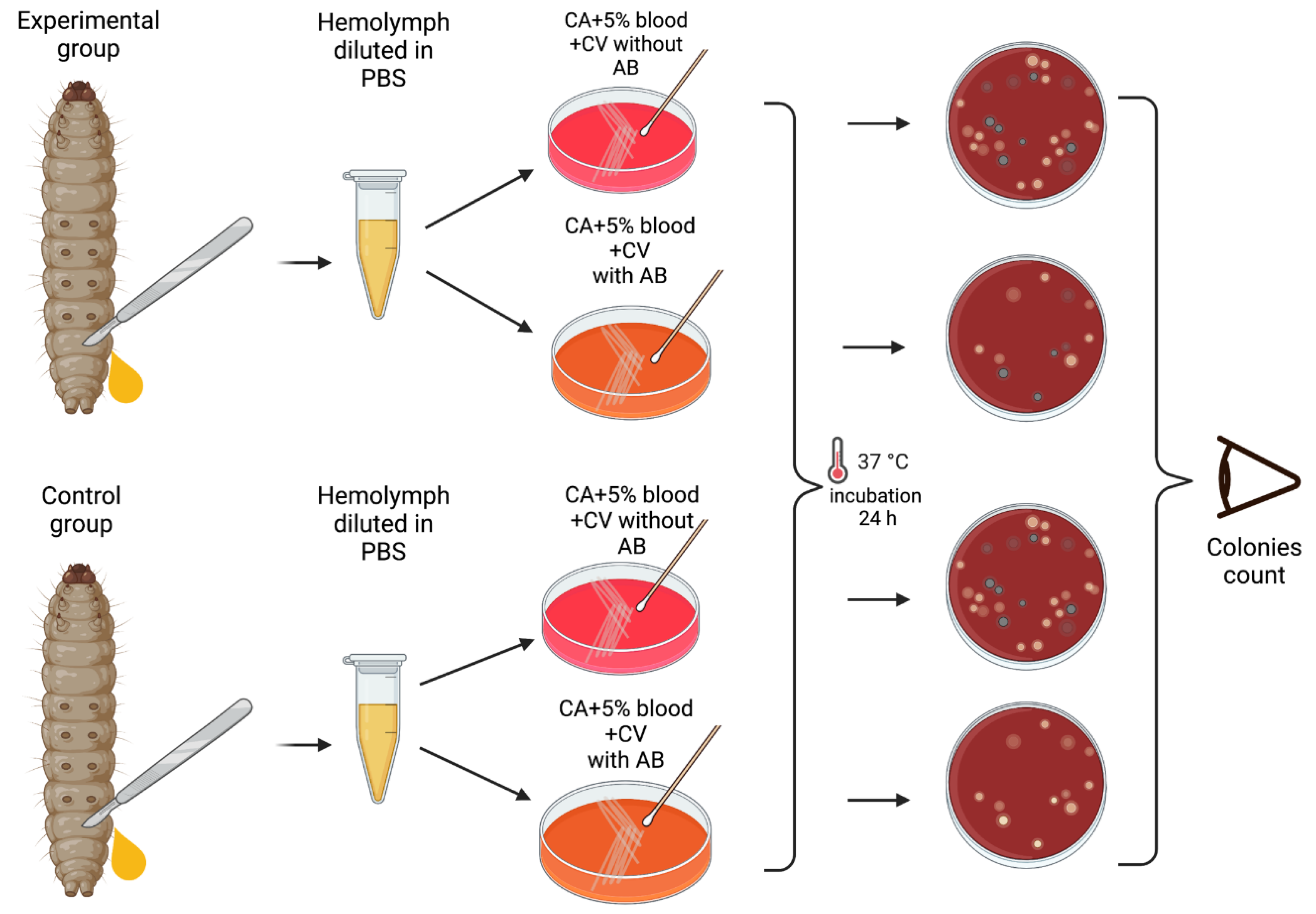
The larvae were placed at -70°C for 60 seconds until no movements were observable. Afterwards, they were placed on a Petri dish, and an incision was made between two segments closest to the tail of the larva. Hemolymph was then extracted by squeezing it into 1.8mL centrifuge tubes containing 100 μL PBS. The hemolymph from each larva was vortexed and plated into plates with and without erythromycin. Modified CNA agar +5% horse blood + 0,0032 g/L Crystal Violet with or without 3 x MIC (0.192 mg/L) of erythromycin were used for these experiments.
Plates were then incubated at 37°C in a 5% (v/v) CO2 for 24 hours, and the grey alpha-hemolytic colonies were counted manually (Figure 2). All the grey colonies with greenish alpha-hemolysis zone growing on the erythromycin plates and a random selection of up to two single colonies from the non-antibiotic plates were selected for identification via Matrix-Assisted Laser Desorption/Ionization-Time-of-Flight mass spectrometry (MALDI-TOF MS). Following EUCAST guidelines, erythromycin resistance was defined as erythromycin MIC >0.25 mg/L [27].
Figure 2.
Visual scheme illustrating hemolymph extraction of1-2 randomly selected G. mellonella larvae from each group of 10 at 24 hourly intervals after injection during 6 days of experiment and retrieval of S. pneumoniae on selective agar plates with or without erythromycin. Colonies count was performed manually.
Figure 2.
Visual scheme illustrating hemolymph extraction of1-2 randomly selected G. mellonella larvae from each group of 10 at 24 hourly intervals after injection during 6 days of experiment and retrieval of S. pneumoniae on selective agar plates with or without erythromycin. Colonies count was performed manually.
When each experiment was completed, the surviving and dead G. mellonella were kept at −70°C overnight to sedate and kill them. They were then autoclaved at 121°C for 15 min and discarded.
MALDI-TOF MS species identification and E-Test
Each bacterial isolate was spread on a steel target plate and covered with 1 μL of α-cyano-4-hydroxycinnamic acid (CHCA) matrix solution. After drying the target plate was loaded and read. The spectra were acquired in linear mode in a mass range of 2–20 kDa and then compared to the library. Results were classified as reliable or unreliable according to recommended cut-off values of 1.7 and 2 for validated results for the genus and species levels, respectively [28].
The E-tests (AB bioMerieux, Solna, Sweden) to determine erythromycin MICs were performed on MHA (Becton Dickinson) + 5% horse blood plates incubated for 18–20 h at 37°C in a 5% (v/v) CO2, following EUCAST guidelines [27]. E-tests strips were placed on a freshly inoculated plate using an inoculum of 0.5-1 McFarland of S. pneumoniae. The strips with an ellipse inhibition shape were read at 80% inhibition of bacterial growth.
Data Analysis
Statistical analyses and data visualization, such as graphs and boxplots, were performed using GraphPad Prism® version 9.5.1 with Mann-Whitney or ANOVA tests that were used to compare groups, depending on Gaussian distribution. The Kaplan-Meier statistical method was used for survival analysis. P-value <0.05 was considered statistically significant. Visual schemes of materials and methods were created with BioRender.com.
Whole Genome Sequencing
Whole genome sequencing (WGS) of the following samples was carried out – ATCC 49619, 1EMA ADI-2802b, 1EMA ADI-0303c, 1WHO ADI-1403b, 1WHO ADI-1403c, Ctrl-B2, Ctrl-B4. The whole genome sequencing was outsourced to Eurofins, where the samples were processed as follows. In brief, genomic DNA was extracted using the QIAGEN extraction Kit (DNeasy® Blood &Tissue Kit (50)) and suspended in nuclease-free water (Sigma-Aldrich). Paired-end 150-bp indexed reads using Nextera XT DNA library prep kit were generated using Illumina technology according to the manufacturer’s instructions (Eurofins, Konstanz, Germany).
After the initial quality control by FastQC (https://github.com/s-andrews/FastQC) and trimming using trimmomatic [29], the processed Illumina reads were de novo assembled with Shovill v1.0.4 (https://github.com/tseemann/shovill), which uses SPAdes v3.14.0 (https://github.com/ablab/spades), with the following parameters: --trim --depth 150 --opts –isolate. Annotation was performed with Prokka, v1.14.6 [30]. PfaSTer, a machine learning-based method was used to identify the serotypes from the assembled S. pneumoniae genomes [31].
Abricate v1.01(https://github.com/tseemann/abricate) was used to search for virulence and antibiotic resistance (AMR) genes from the genome assemblies (.fna files) using the vfdb [32] and card [33] databases, respectively (updated 2021 March 27), the results are reported where they achieved >99% coverage and identity with no gaps. Additionally, the genomes with evidence of horizontal gene transfer (HGT), BLASTN was carried out against nr database. Furthermore, the quality-controlled reads were mapped to the ATCC 49619 reference genome. The different single nucleotide polymorphisms (SNPs) were determined with a minimum coverage of 10X and minimum frequency of 35% using the variant detection tool implemented in CLC genomics Workbench V22. The raw reads are deposited under the BioProject ID PRJNA1011801.
Results
Colonization
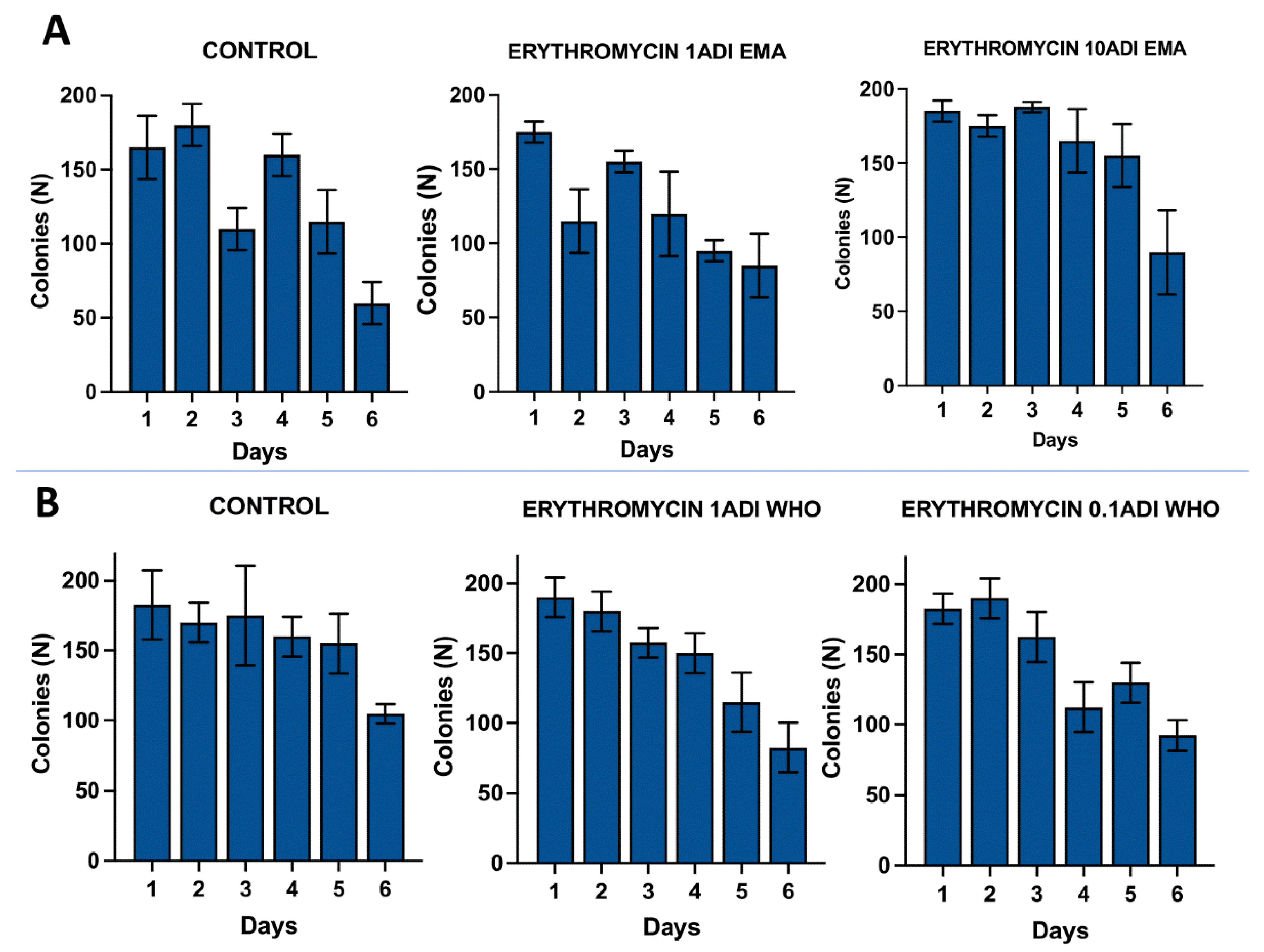
The G. mellonella larvae were successfully colonized for 5 to 6 days with the S. pneumoniae strain (Figure 3). S. pneumoniae species could be recovered from the hemolymph upon culturing on a selective agar plate without erythromycin for 5 to 6 days after inoculation. The species identity of 1-2 colonies per agar plate were confirmed with MALDI-TOF MS (Table S2).
Figure 3.
Colonization of G. mellonella larvae with S. pneumoniae on 1-6 days after injections of S. pneumoniae followed by administration of various concentrations of erythromycin or PBS (control). (A). Colony count of S. pneumoniae growth done manually on non-antibiotic plates after injection of erythromycin ADI doses defined by EMA: 1.75 ng (1ADI EMA) and 17.5 ng (10ADI EMA) (B). Colony count of S. pneumoniae growth done manually on non-antibiotic plates after injection of erythromycin ADI WHO doses: 0.025 ng (0.1ADI WHO) and 0.25 ng (1ADI WHO). The bars display the standard error of the mean.
Figure 3.
Colonization of G. mellonella larvae with S. pneumoniae on 1-6 days after injections of S. pneumoniae followed by administration of various concentrations of erythromycin or PBS (control). (A). Colony count of S. pneumoniae growth done manually on non-antibiotic plates after injection of erythromycin ADI doses defined by EMA: 1.75 ng (1ADI EMA) and 17.5 ng (10ADI EMA) (B). Colony count of S. pneumoniae growth done manually on non-antibiotic plates after injection of erythromycin ADI WHO doses: 0.025 ng (0.1ADI WHO) and 0.25 ng (1ADI WHO). The bars display the standard error of the mean.
Mortality
There was no significant difference in the mortality rates of the larvae between the antibiotic- treated and control groups (Figure S1). The cumulative number of dead larvae per group of ten gradually increased from 1-2 on the first day after injection to 7-8 on the sixth day.
Serotyping, virulence and antimicrobial resistance genes
All the S. pneumoniae isolates belonged to the 19F serotype. The following virulence genes were identified in all the isolates: cbpD, cbpG, cps4A, cps4B, cps4C, cps4D, hysA, lytA, lytB, lytC, nanB, pavA, pce,pfbA, ply, psaA (Table S3a). RlmA(II), patA, patB, pmrA AMR genes were identified in all the isolates (Table S3b). Additionally, vanRC gene was identified in one isolate - 1EMA ADI-2802b (Table 2). Further BLASTN of the flanking region of the vanC cluster from 1 EMA ADI-2802b isolate showed 100% identity to Enterococcus innesii (accession no: AP025635.1) and Enterococcus casseliflavus (accession no: LR607377.1).

Table 2.
Mutations detected in S. pneumoniae exposed to low dose erythromycin but not in unexposed controls.
Table 2.
Mutations detected in S. pneumoniae exposed to low dose erythromycin but not in unexposed controls.
| Gene Product | CDS/Gene | Strain | ||||||
|---|---|---|---|---|---|---|---|---|
| 2802b | 1403b | 1403c | 0303c | Ctrl_B2 | Ctrl_B4 | ATCC | ||
| Hypothetical Protein | OPMNIGBM_00355 | - | - | - | c.888A>C | - | - | - |
| Hypothetical Protein | OPMNIGBM_00536 | - | - | - | p.Arg77Trp | - | - | - |
| Tyrosine recombinase | xerS | - | - | - | p.Val324Leu | - | - | - |
| Hypothetical Protein | OPMNIGBM_00800 | - | - | - | p.Ser121Gly | - | - | - |
| Putative TrmH family tRNA/rRNA methyltransferase | OPMNIGBM_00823 | - | - | - | p.Ser203Arg | - | - | - |
| Hypothetical Protein | OPMNIGBM_00925 | - | - | - | p.Trp47Leu | - | - | - |
| Hypothetical Protein | OPMNIGBM_01263 | - | - | - | p.Leu8Ser | - | - | - |
| Hypothetical Protein | OPMNIGBM_00216 | - | p.Glu159* | - | NA | - | - | - |
| Hypothetical Protein | OPMNIGBM_00913 | - | p.His44Asn | - | NA | - | - | - |
| Arylsulfatase | OPMNIGBM_00351 | c.750T>C | - | c.750T>C | NA | - | - | - |
| Heat-inducible transcription repressor | hrcA | c.954C>A | - | c.954C>A | NA | - | - | - |
| 50S ribosomal protein L1 | rplA | p.Asn34Lys | - | p.Asn34Lys | NA | - | - | - |
| Hyothetical protein | OPMNIGBM_00258 | p.Cys102Arg | - | - | NA | - | - | - |
| ATP dependant DNA helicase | recG | c.837A>G | - | - | NA | - | - | - |
| Hypothetical Protein | OPMNIGBM_00430 | p.Asp27Asn | - | - | NA | - | - | - |
| Autolysin | lytA_2 | c.108C>T | - | - | NA | - | - | - |
Emergence of AMR
The emergence of erythromycin resistance was assessed via manually counting colonies of S. pneumoniae on the selective agar plates with erythromycin. No S. pneumoniae colonies were seen on the control plates with erythromycin, 0.1ADI WHO erythromycin or10ADI EMA erythromycin plates (Figure 4). Resistant colonies emerged on 1ADI EMA erythromycin plates at days 1 and 4 (Table 1; Figure 4). Resistant colonies also emerged on 1ADI WHO plates at day 1 only (Table 1; Figure 4).
Figure 4.
Emergence of colonies of S. pneumoniae with elevated erythromycin MICs on antibiotic plates, 1-4 days after injection of S. pneumoniae followed by administration of various concentrations of erythromycin or PBS (control). (A). Manual count of S. pneumoniae colonies on antibiotic plates after injection of erythromycin ADI doses defined by EMA: 1.75 ng (1ADI EMA) and 17.5 ng (10ADI EMA) (B). Manual colony count of S. pneumoniae on antibiotic plates after injection of erythromycin ADI doses defined by WHO: 0.025 ng (0.1ADI WHO) and 0.25 ng (1ADI WHO). The bars display standard error of the mean.
Figure 4.
Emergence of colonies of S. pneumoniae with elevated erythromycin MICs on antibiotic plates, 1-4 days after injection of S. pneumoniae followed by administration of various concentrations of erythromycin or PBS (control). (A). Manual count of S. pneumoniae colonies on antibiotic plates after injection of erythromycin ADI doses defined by EMA: 1.75 ng (1ADI EMA) and 17.5 ng (10ADI EMA) (B). Manual colony count of S. pneumoniae on antibiotic plates after injection of erythromycin ADI doses defined by WHO: 0.025 ng (0.1ADI WHO) and 0.25 ng (1ADI WHO). The bars display standard error of the mean.
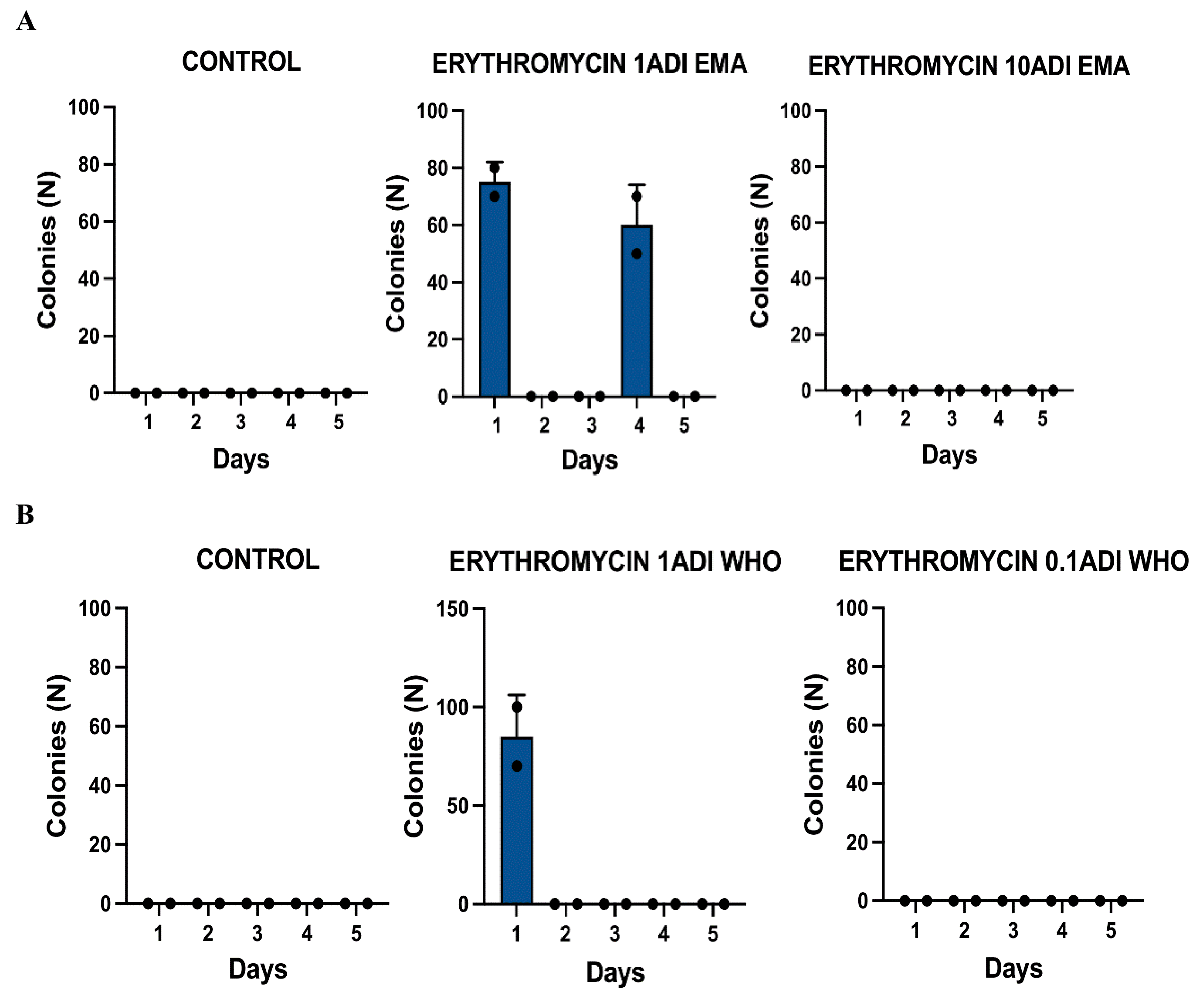
Table 1.
S. pneumoniae isolates with elevated erythromycin MICs with available whole genomes and ribosomal protein mutations detected.
Table 1.
S. pneumoniae isolates with elevated erythromycin MICs with available whole genomes and ribosomal protein mutations detected.
| Dose | Strain ID | Groups | Erythromycin injected | MIC | Day of experiment | Ribosomal protein mutations |
|---|---|---|---|---|---|---|
| ng | mg/L | rplA | ||||
| 1EMA ADI | 2802b | Test | 1.75 | 0.25 | 1 | Asn34Lys |
| 1EMA ADI | 0303c | Test | 1.75 | 0.190 | 4 | |
| 1WHO ADI | 1403b | Test | 0.25 | 0.25 | 1 | |
| 1WHO ADI | 1403c | Test | 0.25 | 0.38 | 1 | Asn34Lys |
| No dose | ATCC 49619 | Reference | 0.064 | |||
| No dose | Ctrl-B2 | Control | 0.125 | |||
| No dose | Ctrl-B4 | Control | 0.094 |
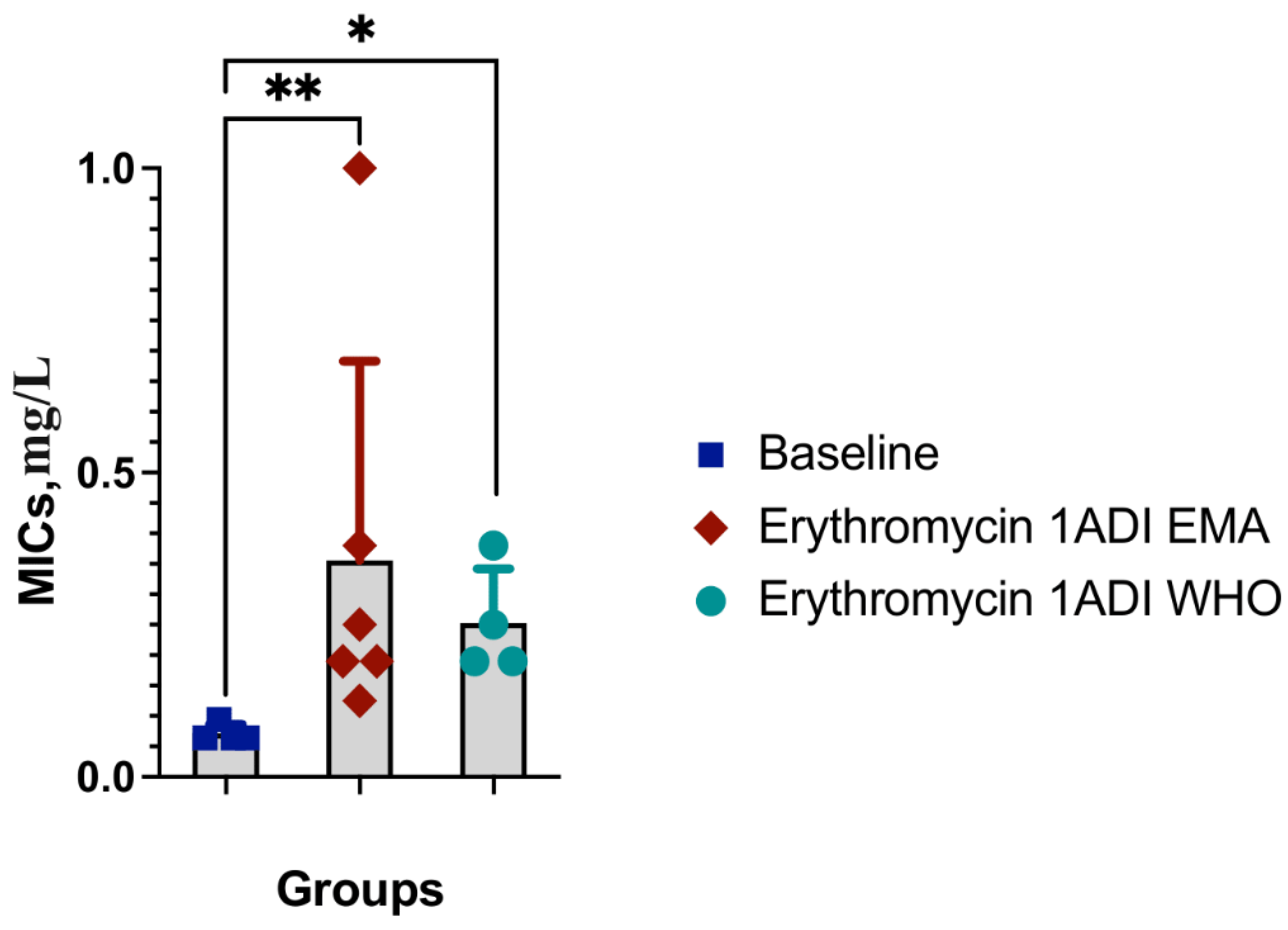
The median erythromycin MIC of the 1 ADI EMA colonies was 0.36 mg/L (IQR 0.125 - 1 mg/L; Table 1). These MICs were 2 to 15 times higher than the baseline MIC – 0.064 mg/L (P-value 0.0048; Figure 5). The median erythromycin MIC of the 1ADI WHO colonies was 0.25 mg/L (0.190 – 0.38 mg/L; Table 1). These MICs were 3 to 6 times higher than the baseline MIC – 0.064 mg/L (P-value 0.0286; Figure 5).
WGS revealed mutations in relevant ribosomal proteins in two of the isolates exposed to erythromycin that were not detected in the control groups: 102C>G (Asn34Lys) in rplA gene encoding the 50S ribosomal protein L1 (Table 1). In addition, non-synonymous mutations were detected in 6 hypothetical proteins, as well as Val324Leu in xerS and Ser203Arg in Putative TrmH family tRNA/rRNA methyltransferase (Table 2). A number of synonymous mutations were also detected in lytA_2, recG, hrcA, arylsulfatase and two hypothetical proteins. The list of relevant mutations found in all the strains can be found in supplementary materials (Table S4).
Discussion
The lowest single dose of erythromycin at which we could induce de novo resistance of S. pneumoniae (Serotype 19F) in a G. mellonella model was 0.7 μg/kg/bw. This concentration (0.012 μg/ml) was calculated based on the determined WHO ADI injected dose of erythromycin per larva (0.25 ng) and the injected volume per larva (20 μl). It is 5.3-fold lower than the erythromycin MIC for this strain. According to the FAO/WHO, this dose of erythromycin can safely be ingested by humans on a daily basis. The EMA classifies doses 7-fold higher than this as safe for daily consumption. We did not assess if lower doses could induce resistance and thus cannot exclude the possibility that the in vivo S. pneumoniae MSCdenovo for erythromycin is lower than this value. Because the MSCselect is typically lower than the MSCdenovo [1,3], future studies are required to assess the MSCselect in vivo.
To the best of our knowledge, these data represent the first in vivo assessment of MSCs. As already noted, several ecological level studies have found a link between macrolide consumption in food animals and AMR in human-associated bacteria [8,9]. Our findings could therefor help explain the high prevalence of macrolide resistance in S. pneumoniae and other bacteria in some East Asian countries, that report high macrolide consumption in food animals but moderate macrolide consumption in humans [7,9,34].
The S. pneumoniae isolate used for this experiment had the following virulence genes: cbpD, cbpG, cps4A, cps4B, cps4C, cps4D, hysA, lytA, lytB, lytC, nanB, pavA, pce, pfbA, ply, psaA that encode products important for adherence, colonization, invasion, and survival [35,36,37,38,39,40,41,42,43,44]. Both intrinsic and acquired mechanisms affect susceptibility to a large variety of antibiotics [45]. The following intrinsic AMR genes were present: rlmA(II), patA, patB and pmrA. RlmA(II) encodes a methyltransferase gene and pmrA, a MFS-type efflux pump that confers resistance to tylosin, mycinamicin and ciprofloxacin [46,47,48]. PatA and patB encode half-ABC transporters that have been shown to be involved in fluoroquinolone resistance [49,50].
The vanA resistance locus in Enterococcus, consists of a cluster of seven genes: vanS, vanR, vanH, vanA, vanX, vanY, and vanZ [51,52] that confers resistance to vancomycin and teicoplanin. The vanR along with vanS are involved in response regulation and the expression of proteins accountable for detecting the extracellular presence of antimicrobial drugs and intracellular signalling [53,54,55]. Interestingly one isolate 1EMA ADI-2802b (Day 1) had the vanRC, a vanA gene found in the vanC cluster that could have been acquired from Enterococcus innesiii. Previously, Enterococcus innesiii sp. nov., was isolated from Galleria mellonella and found to encode atypical vancomycin resistance genes [56]. Enterococcal species are the dominant bacteria in G. mellonella microbiome [57]. Our findings could therefore be explained by the S. pneumoniae acquiring this vanRC gene from one of the enterococcal species in the G. mellonella microbiome. To the best of our knowledge, this vanRC gene has never been detected in S. pneumoniae before.
Macrolide resistance in S. pneumoniae typically emerges via either active efflux or target modification. Active efflux is mediated via the acquisition of the mef(A), mef(E), or mef(I) efflux pumps [58,59]. None of the genes coding these proteins were present in our strain of S. pneumoniae. Some of the resistant strains acquired mutations in rplA and rplD that code for the L1 and L4 ribosomal proteins. Target modification in the genes encoding riboproteins L4 and L22 has been shown to result in macrolide resistance in S. pneumoniae and other bacteria [60,61,62]. Mutations in L1 have not, as yet, been found to be causally associated with macrolide resistance in S. pneumoniae. L1 serves as a ribosomal protein to bind rRNA and as a translational repressor binding its mRNA [63]. Studies in Mycoplasma bovis and Stenotrophomonas maltophilia have found that mutations in both L1 and L4 proteins were independently associated with elevated macrolide MICs [64,65]. For example, a genome wide association study in Mycoplasma bovis identified nucleotide variants in L1 and L4 as independently associated with macrolide MICs [65]. Two of the strains with erythromycin resistance had acquired a 102C>G mutation in rplA that coded for a Asn34Lys change in L1. We could not find any evidence that this mutation is associated with macrolide resistance. It is however possible that this mutation, possibly in conjunction with other two synonymous mutations (arylsulfatase -750T>C, and hrcA 954C>A) found in both isolates may play a role. Further experiments are required to test this hypothesis. Because macrolides act by binding to the 23s rRNA, and ribosomal proteins do not directly interact with macrolides, mutations in ribosomal proteins frequently cause resistance via inducing conformational changes in the 23S rRNA [66,67,68]. It is therefore possible that some combination of these mutations is responsible for the observed increases in erythromycin MICs.
Two previous studies of sub-MIC exposure to ciprofloxacin and ceftriaxone in E. coli have found that low dose antimicrobials selected for resistant isolates, but that in only a minority of isolates could the elevated MICs be explained by known resistance mechanisms [69,70]. Both studies found novel mutations that could explain the increased MICs. These findings suggest that low dose antimicrobials may select for AMR via different pathways to high dose exposure. These mutations may act as stepping-stones to the future emergence of higher levels of resistance. For example, studies have found that transient mutations in ribosomal proteins including in L4, L22 and L34 can act as stepping-stones to higher level macrolide and fluoroquinolone resistance [71,72]. Another common form of target modification is acquisition of a methylase enzyme, erm(A) or erm(B) that methylate key residues of the 23S rRNA [58,73]. These methylases were not detected in any of our isolates.
There were a number of other limitations to our study. We only assessed the effect of a single dose of 4 concentrations of a single antimicrobial on a single strain of S. pneumoniae. The infection model used was a chronic hemolymph infection in G. mellonella. It would be more relevant to determine if these low doses could induce resistance after oral ingestion in different mammalian models or humans. Our experiment only considered a single dose of erythromycin, whereas this dose of the antimicrobial could be ingested daily in everyday life. Furthermore, we did not include low doses of other antimicrobials, biocides or antidepressants, all of which have been shown to act synergistically in inducing AMR at low concentrations [74,75]. We only assessed the MSCdenovo and not the MSCselect, which is typically the lower of the two [1,8]. One of the studies that evaluated the effects of exposure to residual levels of erythromycin on human intestinal epithelium found that this erythromycin resulted in increased intestinal permeability [76]. We did not assess these effects. The dose of erythromycin given was based on a larva of 350mg. The larvae weighed between 300mg and 400mg, meaning that the 300mg larvae received up to 14,3% higher erythromycin concentration than that prescribed (Table S1). No resistant colonies emerged in the S. pneumoniae exposed to the highest concentration of erythromycin (10 ADI EMA). If this is not a stochastic event, we are unable to explain this finding. We did not perform transcriptomic or proteomic analyses. Finally, we did not conduct the complementation experiments necessary to assess if the novel mutations are causally associated with elevations in erythromycin MIC.
Macrolides are frequently used for food producing animals [77,78]. In the United States, 9% of all macrolides consumed are used for this purpose [78]. In some countries, this usage is increasing. In the United States, for example, the consumption of macrolides for food animals increased by 21% between 2020 through 2021 [78]. Thus, if our results are replicated in mammalians, then it may be prudent to include the induction of AMR in the criteria used to define ADIs and MRLs. Finally, if our findings are validated in a mammalian gut model, then the G. mellonella model of chronic infections could be used as a high throughput tool to test safe ADIs for other bug-drug combinations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
YB, CK, ZG and SB conceptualized the study. YB, CK and ZG conducted the MSC experiments. YB was responsible for the statistical analyses. SB and BX were responsible for bioinformatic analyses. All authors read and approved the final draft.
Funding
The study was funded by SOFI 2021 grant— ‘PReventing the Emergence of untreatable STIs via radical Prevention’ (PRESTIP).
Acknowledgements
Yuliia Baranchyk was registered in the EMJMD LIVE (Erasmus+ Mundus Joint Master Degree Leading International Vaccinology Education), co-funded by the EACEA (Education, Audiovisual and Culture Executive Agency, award 2018-1484) of the European Commission, and received a scholarship from the EACEA.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
References
- Gullberg E, Albrecht LM, Karlsson C, et al. Selection of a Multidrug Resistance Plasmid by Sublethal Levels of Antibiotics and Heavy Metals Baquero F, ed. mBio 2014; 5. [CrossRef]
- Stanton IC, Murray AK, Zhang L, et al. Evolution of antibiotic resistance at low antibiotic concentrations including selection below the minimal selective concentration. Commun Biol 2020; 3. [CrossRef]
- Gullberg E, Cao S, Berg OG, et al. Selection of Resistant Bacteria at Very Low Antibiotic Concentrations Lipsitch M, ed. PLoS Pathog 2011; 7: e1002158. [CrossRef]
- Kraupner N, Ebmeyer S, Hutinel M, et al. Selective concentrations for trimethoprim resistance in aquatic environments. Environ Int 2020; 144: 106083. [CrossRef]
- Bengtsson-Palme J, Larsson DGJ. Concentrations of antibiotics predicted to select for resistant bacteria: Proposed limits for environmental regulation. Environ Int 2016; 86: 140–9. [CrossRef]
- EFSA Panel on Biological Hazards (BIOHAZ), Koutsoumanis K, Allende A, et al. Maximum levels of cross-contamination for 24 antimicrobial active substances in non-target feed. Part 1: Methodology, general data gaps and uncertainties. EFS2 2021; 19.
- Mitchell JM, Griffiths MW, Mcewen SA, et al. Antimicrobial Drug Residues in Milk and Meat: Causes, Concerns, Prevalence, Regulations, Tests, and Test Performance. J Food Prot 1998; 61: 742–56. [CrossRef]
- González N, Abdellati S, De Baetselier I, et al. Ciprofloxacin Concentrations 1/1000th the MIC Can Select for Antimicrobial Resistance in N. gonorrhoeae—Important Implications for Maximum Residue Limits in Food. Antibiotics 2022; 11: 1430. [CrossRef]
- Kenyon, C. Positive association between the use of macrolides in food-producing animals and pneumococcal macrolide resistance: a global ecological analysis. Int J Infect Dis 2022; 116: 344–7. [CrossRef]
- European Centre for Disease Prevention and Control (ECDC), European Food Safety Authority (EFSA), European Medicines Agency (EMA). ECDC/EFSA/EMA second joint report on the integrated analysis of the consumption of antimicrobial agents and occurrence of antimicrobial resistance in bacteria from humans and food-producing animals. EFS2 2017; 15.
- Allel K, Day L, Hamilton A, et al. Global antimicrobial-resistance drivers: an ecological country-level study at the human–animal interface. Lancet Planet Health 2023; 7: e291–303. [CrossRef]
- Tang KL, Caffrey NP, Nóbrega DB, et al. Restricting the use of antibiotics in food-producing animals and its associations with antibiotic resistance in food-producing animals and human beings: a systematic review and meta-analysis. Lancet Planet Health 2017; 1: e316–27. [CrossRef]
- FAO/WHO. Codex Alimentarius: Guidelines for the simple evaluation of dietary exposure to food additives. CAC/GL 3-1989 Adopted 1989. Revision 2014. https://www.fao.org/input/download/standards/6/cxg_003e.pdf.
- Murray AK, Stanton I, Gaze WH, Snape J. Dawning of a new ERA: Environmental Risk Assessment of antibiotics and their potential to select for antimicrobial resistance. Water Res 2021; 200: 117233. [CrossRef]
- Subirats J, Domingues A, Topp E. Does Dietary Consumption of Antibiotics by Humans Promote Antibiotic Resistance in the Gut Microbiome? J Food Prot 2019; 82: 1636–42. [CrossRef]
- EMEA. The European Agency for the Evaluation of Medicinal Products. Committee for veterinary medicinal products: enrofloxacin summary report (2).1998. https://www.ema.europa.eu/en/documents/mrl-report/enrofloxacin-modification-bovine-porcine-poultry-summary-report-2-committee-veterinary-medicinal_en.pdf.
- EMEA. The European Agency for the Evaluation of Medicinal Products. Committee for veterinary medicinal products: erythromycin summary report (1).2000. https://www.ema.europa.eu/en/documents/mrl-report/erythromycin-erythromycin-thiocyante-erythromycin-stearate-summary-report-1-committee-veterinary_en.pdf.
- EMEA. The European Agency for the Evaluation of Medicinal Products. Committee for medicinal products for veterinary use. European public MRL assessment report (EPMAR).Tylvalosin.2007. https://www.ema.europa.eu/en/documents/mrl-report/tylvalosin-acetylisovaleryltylosin-modification-acceptable-daily-intake-adi-european-public-mrl_en.pdf.
- EMA. European Medicines Agency. Committee for Medicinal Products for Veterinary Use: VICH GL36(R2): Studies to evaluate the safety of residues of veterinary drugs in human food: general approach to establish a microbiological ADI.2019. https://www.ema.europa.eu/en/documents/scientific-guideline/vich-gl36r2-studies-evaluate-safety-residues-veterinary-drugs-human-food-general-approach-establish_en.pdf.
- FAO/WHO. Codex Alimentarius Commission (CAC): Maximum Residue Limits.2021. http://www.fao.org/fao-who-codexalimentarius/codex-texts/maximum-residue-limits/en/.
- FAO/WHO. Codex Alimentarius Commission Procedural Manual. Twenty-eighth edition, revised, 2023. Rome. [CrossRef]
- WHO. Evaluations of the Joint FAO/WHO Expert Committee on Food Additives (JECFA). Erythromycin. 2006. https://apps.who.int/food-additives-contaminants-jecfa-database/Home/Chemical/3938. 3938.
- EMEA. The European Agency for the Evaluation of Medicinal Products. Committee for veterinary medicinal products: erythromycin summary report (3).2002. https://www.ema.europa.eu/en/documents/mrl-report/erythromycin-extension-all-food-producing-species-summary-report-3-committee-veterinary-medicinal_en.pdf.
- Andrea A, Krogfelt K, Jenssen H. Methods and Challenges of Using the Greater Wax Moth (Galleria mellonella) as a Model Organism in Antimicrobial Compound Discovery. Microorganisms 2019; 7: 85. [CrossRef]
- Cutuli MA, Petronio Petronio G, Vergalito F, et al. Galleria mellonella as a consolidated in vivo model hosts: New developments in antibacterial strategies and novel drug testing. Virulence 2019; 10: 527–41. [CrossRef]
- Cools F, Torfs E, Aizawa J, et al. Optimization and Characterization of a Galleria mellonella Larval Infection Model for Virulence Studies and the Evaluation of Therapeutics Against Streptococcus pneumoniae. Front Microbiol 2019; 10.
- EUCAST. The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 13.0., 2023. http://www.eucast.org.
- Laumen JGE, Van Dijck C, Abdellati S, et al. Antimicrobial susceptibility of commensal Neisseria in a general population and men who have sex with men in Belgium. Sci Rep 2022; 12. [CrossRef]
- Bolger AM, Lohse M, Usadel B. Trimmomatic: a flexible trimmer for Illumina sequence data. Bioinformatics 2014; 30: 2114–20. [CrossRef]
- Seemann T. Prokka: rapid prokaryotic genome annotation. Bioinformatics 2014; 30: 2068–9. [CrossRef]
- Lee JT, Li X, Hyde C, et al. PfaSTer: a machine learning-powered serotype caller for Streptococcus pneumoniae genomes. Microb Genom 2023; 9. [CrossRef]
- Chen L, Zheng D, Liu B, et al. VFDB 2016: hierarchical and refined dataset for big data analysis—10 years on. Nucleic Acids Res 2015; 44: D694–7. [CrossRef]
- ia B, Raphenya AR, Alcock B, et al. CARD 2017: expansion and model-centric curation of the comprehensive antibiotic resistance database. Nucleic Acids Res 2016; 45: D566–73. [CrossRef]
- Felmingham D, Cantón R, Jenkins SG. Regional trends in β-lactam, macrolide, fluoroquinolone and telithromycin resistance among Streptococcus pneumoniae isolates 2001–2004. J Infect 2007; 55: 111–8. [CrossRef]
- Huang L-D, Yang M-J, Huang Y-Y, et al. Molecular Characterization of Predominant Serotypes, Drug Resistance, and Virulence Genes of Streptococcus pneumoniae Isolates From East China. Front Microbiol 2022; 13. [CrossRef]
- 36. Holmes AR, McNab R, Millsap KW, et al. The pavA gene of Streptococcus pneumoniae encodes a fibronectin-binding protein that is essential for virulence. Mol Microbiol 2001; 41: 1395–408. [CrossRef]
- Romero-Steiner S, Pilishvili T, Sampson JS, et al. Inhibition of Pneumococcal Adherence to Human Nasopharyngeal Epithelial Cells by Anti-PsaA Antibodies. Clin Vaccine Immunol 2003; 10: 246–51. [CrossRef]
- Marion C, Stewart JM, Tazi MF, et al. Streptococcus pneumoniae Can Utilize Multiple Sources of Hyaluronic Acid for Growth Camilli A, ed. Infect Immun 2012; 80: 1390–8. [CrossRef]
- Croney CM, Nahm MH, Juhn SK, et al. Invasive and Noninvasive Streptococcus pneumoniae Capsule and Surface Protein Diversity following the Use of a Conjugate Vaccine. Clin Vaccine Immunol 2013; 20: 1711–8. [CrossRef]
- Mellroth P, Sandalova T, Kikhney A, et al. Structural and Functional Insights into Peptidoglycan Access for the Lytic Amidase LytA of Streptococcus pneumoniae Rappuoli R, ed. mBio 2014; 5. [CrossRef]
- Rai P, He F, Kwang J, et al. Pneumococcal Pneumolysin Induces DNA Damage and Cell Cycle Arrest. Sci Rep 2016; 6. [CrossRef]
- Wren JT, Blevins LK, Pang B, et al. Pneumococcal Neuraminidase A (NanA) Promotes Biofilm Formation and Synergizes with Influenza A Virus in Nasal Colonization and Middle Ear Infection Pirofski L, ed. Infect Immun 2017; 85. [CrossRef]
- Subramanian, K.; Henriques-Normark, B.; Normark, S. Emerging concepts in the pathogenesis of theStreptococcus pneumoniae: From nasopharyngeal colonizer to intracellular pathogen. Cell Microbiol 2019; 21. [CrossRef]
- Zhao W, Pan F, Wang B, et al. Epidemiology Characteristics of Streptococcus pneumoniae From Children With Pneumonia in Shanghai: A Retrospective Study. Front Cell Infect Microbiol 2019; 9. [CrossRef]
- El Moujaber G, Osman M, Rafei R, et al. Molecular mechanisms and epidemiology of resistance in Streptococcus pneumoniae in the Middle East region. J Med Microbiol 2017; 66: 847–58. [CrossRef]
- Gill, M.J.; Brenwald, N.P.; Wise, R. Identification of an Efflux Pump Gene, pmrA, Associated with Fluoroquinolone Resistance in Streptococcus pneumoniae. Antimicrob Agents Chemother 1999; 43: 187–9. [CrossRef]
- Piddock, L.J.V.; Johnson, M.M.; Simjee, S.; Pumbwe, L. Expression of Efflux Pump Gene pmrA in Fluoroquinolone-Resistant and -Susceptible Clinical Isolates of Streptococcus pneumoniae. Antimicrob Agents Chemother 2002; 46: 808–12. [CrossRef]
- Lee, H.; Hsu, F.-F.; Turk, J.; Groisman, E.A. The PmrA-Regulated pmrC Gene Mediates Phosphoethanolamine Modification of Lipid A and Polymyxin Resistance in Salmonella enterica. J Bacteriol 2004; 186: 4124–33. [CrossRef]
- El Garch F, Lismond A, Piddock LJV, et al. Fluoroquinolones induce the expression of patA and patB, which encode ABC efflux pumps in Streptococcus pneumoniae. J Antimicrob Chemother 2010; 65: 2076–82. [CrossRef]
- Garvey, M.I.; Baylay, A.J.; Wong, R.L.; Piddock, L.J.V. Overexpression of patA and patB, Which Encode ABC Transporters, Is Associated with Fluoroquinolone Resistance in Clinical Isolates of Streptococcus pneumoniae. Antimicrob Agents Chemother 2011; 55: 190–6. [CrossRef]
- Arthur, M.; Courvalin, P. Genetics and mechanisms of glycopeptide resistance in enterococci. Antimicrob Agents Chemother 1993; 37: 1563–71. [CrossRef]
- Arthur, M.; Molinas, C.; Depardieu, F.; Courvalin, P. Characterization of Tn1546, a Tn3-related transposon conferring glycopeptide resistance by synthesis of depsipeptide peptidoglycan precursors in Enterococcus faecium BM4147. J Bacteriol 1993; 175: 117–27. [CrossRef]
- Monteiro da Silva BN, Faria AR, Souza S da SR, et al. Expression of VanA-type vancomycin resistance in a clinical isolate of Enterococcus faecium showing insertion of IS19 in the vanS gene. Int J Antimicrob Agents 2020; 55: 105897. [CrossRef]
- Clewell DB, Weaver KE, Dunny GM, et al. Extrachromosomal and Mobile Elements in Enterococci: Transmission, Maintenance, and Epidemiology. Enterococci: From Commensals to Leading Causes of Drug Resistant Infection [Internet]. Boston: Massachusetts Eye and Ear Infirmary, 2014.
- Hong, H.-J.; Hutchings, M.I.; Buttner, M.J. Vancomycin Resistance VanS/VanR Two-Component Systems. Adv Exp Med Biol 2008; 631: 200–13. [CrossRef]
- Gooch HCC, Kiu R, Rudder S, et al. Enterococcus innesii sp. nov., isolated from the wax moth Galleria mellonella. Int J Syst Evol Microbiol 2021; 71. [CrossRef]
- Allonsius CN, Van Beeck W, De Boeck I, et al. The microbiome of the invertebrate model host Galleria mellonella is dominated by Enterococcus. Anim microbiome 2019; 1. [CrossRef]
- Ambrose, K.D.; Nisbet, R.; Stephens, D.S. Macrolide Efflux in Streptococcus pneumoniae Is Mediated by a Dual Efflux Pump (mel and mef) and Is Erythromycin Inducible. Antimicrob Agents Chemother 2005; 49: 4203–9. [CrossRef]
- Schroeder, M.R.; Stephens, D.S. Macrolide Resistance in Streptococcus pneumoniae. Front Cell Infect Microbiol 2016; 6. [CrossRef]
- Tait-Kamradt A, Davies T, Appelbaum PC, et al. Two New Mechanisms of Macrolide Resistance in Clinical Strains of Streptococcus pneumoniae from Eastern Europe and North America. Antimicrob Agents Chemother 2000; 44: 3395–401. [CrossRef]
- Tait-Kamradt A, Davies T, Cronan M, et al. Mutations in 23S rRNA and Ribosomal Protein L4 Account for Resistance in Pneumococcal Strains Selected In Vitro by Macrolide Passage. Antimicrob Agents Chemother 2000; 44: 2118–25. [CrossRef]
- Canu A, Malbruny B, Coquemont M, et al. Diversity of Ribosomal Mutations Conferring Resistance to Macrolides, Clindamycin, Streptogramin, and Telithromycin in Streptococcus pneumoniae. Antimicrob Agents Chemother 2002; 46: 125–31. [CrossRef]
- Nevskaya, N. Ribosomal protein L1 recognizes the same specific structural motif in its target sites on the autoregulatory mRNA and 23S rRNA. Nucleic Acids Res 2005; 33: 478–85. [CrossRef]
- Calvopiña, K.; Dulyayangkul, P.; Avison, M.B. Mutations in Ribosomal Protein RplA or Treatment with Ribosomal Acting Antibiotics Activates Production of Aminoglycoside Efflux Pump SmeYZ in Stenotrophomonas maltophilia. Antimicrob Agents Chemother 2020; 64. [CrossRef]
- Waldner M, Kinnear A, Yacoub E, et al. Genome-Wide Association Study of Nucleotide Variants Associated with Resistance to Nine Antimicrobials in Mycoplasma bovis. Microorganisms 2022; 10: 1366. [CrossRef]
- Schlünzen F, Zarivach R, Harms J, et al. Structural basis for the interaction of antibiotics with the peptidyl transferase centre in eubacteria. Nature 2001; 413: 814–21. [CrossRef]
- Tu D, Blaha G, Moore PB, Steitz TA. Structures of MLSBK Antibiotics Bound to Mutated Large Ribosomal Subunits Provide a Structural Explanation for Resistance. Cell 2005; 121: 257–70. [CrossRef]
- Wilson, D.N. Ribosome-targeting antibiotics and mechanisms of bacterial resistance. Nat Rev Microbiol 2013; 12: 35–48. [CrossRef]
- Ching, C.; Zaman, M.H. Development and selection of low-level multi-drug resistance over an extended range of sub-inhibitory ciprofloxacin concentrations in Escherichia coli. Sci Rep 2020; 10. [CrossRef]
- Ching, C.; Zaman, M.H. Identification of Multiple Low-Level Resistance Determinants and Coselection of Motility Impairment upon Sub-MIC Ceftriaxone Exposure in Escherichia coli Gales AC, ed. mSphere 2021; 6. [CrossRef]
- Gomez JE, Kaufmann-Malaga BB, Wivagg CN, et al. Ribosomal mutations promote the evolution of antibiotic resistance in a multidrug environment. eLife 2017; 6. [CrossRef]
- Laumen JGE, Manoharan-Basil SS, Verhoeven E, et al. Molecular pathways to high-level azithromycin resistance in Neisseria gonorrhoeae. J Antimicrob Chemother 2021; 76: 1752–8. [CrossRef]
- Fyfe, C.; Grossman, T.H.; Kerstein, K.; Sutcliffe, J. Resistance to Macrolide Antibiotics in Public Health Pathogens. Cold Spring Harb Perspect Med 2016; 6: a025395. [CrossRef]
- Seiler, C.; Berendonk, T.U. Heavy metal driven co-selection of antibiotic resistance in soil and water bodies impacted by agriculture and aquaculture. Front Microbio 2012; 3. [CrossRef]
- Jin M, Lu J, Chen Z, et al. Antidepressant fluoxetine induces multiple antibiotics resistance in Escherichia coli via ROS-mediated mutagenesis. Environ Int 2018; 120: 421–30. [CrossRef]
- Hao H, Gokulan K, Piñeiro SA, et al. Effects of Acute and Chronic Exposure to Residual Level Erythromycin on Human Intestinal Epithelium Cell Permeability and Cytotoxicity. Microorganisms 2019; 7: 325. [CrossRef]
- Van Boeckel TP, Glennon EE, Chen D, et al. Reducing antimicrobial use in food animals. Science 2017; 357: 1350–2. [CrossRef]
- FDA, Center For Veterinary Medicine. 2021 Summary Report On Antimicrobials Sold or Distributed for Use in Food-Producing animals. 2022. https://www.fda.gov/media/163739/download.
Figure 5.
Erythromycin MICs distribution for S. pneumoniae baseline (ATCC 49619) colonies and resistant colonies (1ADI EMA and 1ADI WHO). Mean values with SD. Mann-Whitney test used to assess for statistically significant differences (*P < 0.05, **P< 0.01): *P = 0.0048; **P = 0.0286.
Figure 5.
Erythromycin MICs distribution for S. pneumoniae baseline (ATCC 49619) colonies and resistant colonies (1ADI EMA and 1ADI WHO). Mean values with SD. Mann-Whitney test used to assess for statistically significant differences (*P < 0.05, **P< 0.01): *P = 0.0048; **P = 0.0286.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



