
Submitted:
04 March 2024
Posted:
06 March 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
After the global challenges posed by COVID-19, researchers strived to identify risk factors for severe cases, which lead to various complications - including death. Lifestyle modifications, such as implementing a healthy diet and recommended physical activity, have shown to be protective against severe COVID-19 cases. Despite an association of a plant-based diet with reduced COVID-19 severity, specific dietary characteristics have not been identified. Also, the methodology for measuring physical activity is variable, with studies overlooking the intensity or the habit components of physical activity. To bridge this gap, our study designed, validated, and applied a retrospective questionnaire with aims of exploring the relationship between lifestyle factors, specifically diet and physical activity, and severe COVID-19. We considered the intensity and years of physical activity habit, which is a limitation of other questionnaires. Results reveal associations of age and BMI with severe COVID-19. An excessive sugar diet was found to be associated with severe COVID-19 and increased symptom duration. We also observed an inverse relationship pattern of moderate and vigorous intensity physical activity across case severity, which is absent in walking PA. This study lays a foundation for research aiming to identify lifestyle factors that prevent severe COVID-19 cases.
Keywords:
COVID-19
; physical activity
; diet
; lifestyle
; questionnaire
1. Introduction
The emergence of the coronavirus disease 2019 (COVID-19), driven by the SARS-CoV-2 virus, had a significant adverse impact on societies worldwide. The rapid spread of this disease caused unprecedented challenges to global public health systems. As of current date, COVID-19 has reached about 800 million cases and caused 7 million deaths globally, indicating a prevalence rate of 9.7% and a case-fatality rate of 0.9% [1]. Severe cases of COVID-19 are associated with complications such as pneumonia, acute respiratory distress syndrome, organ failure, and mortality [2]. Identified high risk factors for severe COVID-19 include age, obesity, type 2 diabetes, chronic kidney disease, chronic obstructive pulmonary disease, and coronary atherosclerosis [3,4,5]. Consequently, understanding and managing factors contributing to the severity of COVID-19 cases would allow for the prevention of its related complications.
Lifestyle modifications, including a healthy diet and recommended levels of physical activity (PA) [6], have proven to be effective tools for improving outcomes of chronic conditions associated with severe forms of COVID-19 - such as type 2 diabetes and cardiovascular diseases [7,8]. Also, a plant-based diet has been associated with reduced COVID-19 severity [9]. But further research is needed to identify specific dietary characteristics influencing the severity of COVID-19. Furthermore, PA has been related to a reduction in severe COVID-19 outcomes such as hospitalization, ICU admission, and mortality [5,10,11,12,13,14,15]. However, there is a high variability in the methodology for measuring PA [10,11,12], limiting the quality of a quantitative synthesis of results (meta-analysis). Several studies use the International Physical Activity Questionnaire (IPAQ) [11,13,15] as a PA measuring tool. The IPAQ is limited to the assessment of the PA pattern of the week preceding the questionnaire application [16], overlooking the PA habit of the individual. Other studies focus on the frequency and duration of PA, ignoring the intensity component of PA [12].
In this context, our study designed, validated, and applied a retrospective questionnaire with aims of exploring the relationship between lifestyle factors, specifically diet and PA, and the severity of COVID-19. We examined the association between specific dietary characteristics and COVID-19 severity. We also considered the intensity component of PA beyond its frequency and duration, and integrated items to account for the temporal limitation of the IPAQ (focus on the most recent week of PA) [16]. This article serves as a hypothesis-generating piece for more comprehensive research aiming to assess the association between lifestyle and severe COVID-19.
2. Materials and Methods
2.1. Questionnaire Design
The questionnaire was designed to identify PA and eating patterns in subjects who developed severe COVID-19. A retrospective questionnaire was applied in a cross-sectional fashion. The questionnaire was divided into the following six sections: 1) Demographic information without revealing identity (age, sex, nationality, occupation, and education); 2) COVID-19 diagnosis and disease severity (diagnostic method, symptoms, hospitalization, number of days with symptoms, oxygen support); 3) Medical history (particularly chronic medical conditions); 4) Diet and social history (type of diet, food cooking habits, eating schedule, water consumption, tobacco smoking, alcohol consumption, and sleep habits); 5) PA activity (based on the IPAQ short version questionnaire plus additional items addressing the type, frequency, intensity, session duration, and years of PA habit); and 6) Vaccination (type of vaccine and received doses). The questionnaire comprised 56 items, but some questions could be skipped if the previous answer was negative. The questions were kept as short and simple as possible, and technical terms were avoided.
2.2. Questionnaire Validation
The questionnaire was validated in the following order: content validity, face validity, and test reproducibility. A Spanish native speaker expert panel assessed the validity of the content. The panel consisted of 11 health sciences professionals involved in research, including sports scientists, physicians, and nutritionists. The panel evaluated the relevance, clarity, writing, terminology, and format of each item using a numerical scale from 1 (unacceptable) to 5 (excellent) [17]. A content validity coefficient (CVC) was employed to determine the concordance of the answers among experts [17]. An item was accepted if it achieved a CVC ≥ 0.80. Items with a score below this threshold were excluded from the questionnaire.
A cohort of healthy Spanish native speakers from the northwest of Mexico assessed the face validity. Participants evaluated the clarity and comprehension of each questionnaire item. To assess clarity, a three-point ordinal scale was utilized: 1 (incomprehensible), 2 (difficult to understand), and 3 (clear and comprehensible) [18]. Comprehension was evaluated using a numerical scale ranging from 0 (very difficult to understand) to 10 (very easy to understand) [18]. Furthermore, a comment section was included, allowing participants to suggest improvements for each item. The agreement among participants’ responses was analyzed using Kendall’s W coefficient of concordance. Items were considered clear and comprehensible if they achieved both a clarity score of ≥2 and a comprehension score of ≥7, coupled with Kendall’s W coefficient of ≥0.70. These items were not subject to further rewording. Additionally, the readability of each questionnaire item was evaluated by the Flesch-Szigriszt test [19]. The INFLESZ scale was employed to interpret the results [20]. The readability test was carried out using the INFLESZ software (Granada, Granada, Spain). A score of ≥60 was established as the benchmark for considering the questionnaire items as readable.
The reproducibility of the questionnaire was evaluated through a test-retest analysis conducted on a cohort of individuals who had recovered from COVID-19. The participants were instructed to complete the questionnaire on two different occasions, with a minimum interval of two weeks between the first and second administrations. Cohen’s kappa coefficient test was employed to analyze the consistency of the answers between the first and second administrations of the questionnaire. The time to answer the questionnaire was also recorded.
2.3. Questionnaire Application
The questionnaire was digitized, and data were collected using the Survey-Monkey platform. Participants were recruited through a hyperlink disseminated on social media, targeting the general population residing in Culiacan, Mexico. Data were collected from November 2022 to January 2023. Individuals aged 18 years or older that self-identified as having a history of COVID-19 disease, completed the questionnaire. Only participants who concluded the entire questionnaire were included in the study. All participants provided informed consent for their involvement in this study.
2.4. Participants
The questionnaire was administered to 296 subjects, of whom 197 met the inclusion criteria, having either received a clinical diagnosis of COVID-19 by a physician or undergone a laboratory positive for COVID-19. Consequently, the final sample comprised 197 participants. COVID-19 severity was classified based on the question “How do you consider the severity of your illness?” Subjects requiring supplemental oxygen were categorized as having severe COVID-19 [21], even if they reported a different perception of their severity.
2.5. Measuring Lifetime Physical Activity and Sedentary Patterns
Lifetime PA patterns were obtained from the product of the following variables: Metabolic equivalent task (MET) according to PA intensity; duration (minutes); frequency (days per week); and PA habit (years of PA pattern). PA intensities were categorized as walking (3.3 METs), moderate PA (4.0 METs), and vigorous PA (8.0 METs). The sedentary lifetime pattern was obtained from the product of sedentary time (hours/day) and sedentary habit (years of sedentary pattern). PA intensities, frequencies, and duration values were derived from the PA section of our questionnaire. MET intensity values align with recommended ranges from the Physical Activity Guidelines for Americans 2nd Ed. and the Compendium of Physical Activity [6,22,23].
2.6. Ethical Considerations
The design, validation, and application of the retrospective questionnaire was performed from February 2022 to January 2023. This study was approved by the ethics committee of the Faculty of Nutrition and Gastronomy of the “Universidad Autónoma de Sinaloa” (Registration number CE-FCNYG-2022-FEB-002). This study was carried out according to the Declaration of Helsinki, and does not represent any physical, emotional, or occupational risk. All the participants accepted and voluntarily answered the questionnaire, however, signed informed consent was not required. The questions were designed to avoid revealing the identity of the participants and information about researchers in charge of the study was provided.
2.7. Statistical Analysis
A Shapiro-Wilk test was used to evaluate data normality and a Levene’s test to verify the homogeneity of variables. Quantitative variables are expressed as mean ± standard deviation (SD) or standard error of the mean (SEM) when the analysis was adjusted for co-variables. Pearson coefficients were used to analyze the correlation of quantitative variables. Statistical differences between groups were analyzed using a one-way ANOVA test, and post hoc tests were performed according to the homogeneity of variance. Qualitative variables are expressed as frequencies (n) and percentages (%). Associations between qualitative variables were analyzed by the application of a chi-square test. A p value < 0.05 was considered statistically significant. All statistical analyses were performed using the software SPSS v.29.0 (IBM, Chicago, IL) and GraphPad software was used to create figures.
3. Results
3.1. Questionnaire Validation
A total of 11 health professionals assessed the relevance, clarity, writing, terminology, and format of each questionnaire item. All the evaluated parameters had scores higher than 4 (Table 1), meaning that the items are clear, relevant, and have an adequate terminology and format for the target population. We included items with a CVC ≥ 0.80. The average CVC for the whole questionnaire was 0.90 (CVCt, table 1), indicating an adequate validity and agreement among health professionals’ scores for each parameter.
Fifty-three participants (37 females, 16 males; 18–54 years old) assessed the clarity and comprehension of each questionnaire item. The average clarity score was 2.94 ± 0.04, classifying the questionnaire as clear. A strong concordance among participants for clarity scores was obtained (Kendall’s W value: 0.929), suggesting a high agreement among participants’ responses. For comprehension assessment, a continuous numerical scale ranging from 0 (very difficult to understand) to 10 (very easy to understand) was employed. We obtained a comprehension score of 9.81 ± 0.20 with a strong agreement among participants’ scores (Kendall’s W value: 0.716). No further rewording was suggested for any items evaluated. The Flesch-Szigriszt readability score was 64.88, which is considered as normal readability.
The consistency between the responses from the first and second questionnaire application was assessed by the Cohen’s k coefficient. A total of 25 participants (18 females, 7 males; 18–69 years old) answered the questionnaire twice at different times. Cohen’s k coefficient was 0.755, which is interpreted as substantial agreement. Overall, the questionnaire was classified as clear and comprehensible by participants and generates consistent responses across time.
3.2. Description of the Study Sample
3.2.1. Social and Demographic Characteristics
Our study sample (n = 197) was composed of Mexican mestizos with a mean age of 30.30 ± 12.05 years and BMI of 25.50 ± 4.21 kg/m2 (Table 2). Sex was distributed as 66.0% females and 34.0% males, most of them being single (62.4%). Education wise, 38.1% were students, 32.5% employees, and the majority (69.5%) were coursing or having finished a bachelor’s degree. The rest of the sociodemographic characteristics of the sample are illustrated in Table 2.
Regarding the COVID-19 profile (Table 3), 85.30% of the subjects were diagnosed using a laboratory test (PCR, Antigen, Antibody), and the rest were diagnosed solely by clinical evaluation (14.70%). Most of the individuals were diagnosed from 2020 to 2022 (98%). COVID-19 severity was classified as mild (n = 91, 46.2%), moderate (n = 89, 45.2%), and severe (n = 17, 8.6%). The participants had COVID-19 symptoms for a mean of 8.57 ± 5.72 days and lost 1.48 ± 3.7 Kg during their COVID-19 infection. The rest of the COVID-19 profile including the distribution of symptoms, comorbidities and vaccinations are illustrated in Table 3.
3.3. Significant Correlations among Study Participants
3.3.1. Social and Demographic Characteristics
We found Significant correlations among the following quantitative variables: Age, BMI, days with symptoms, and post-COVID-19 weight loss. Table 4 illustrates their Pearson correlation coefficient (r), and their level of significance.
3.4. Differences per COVID-19 Severity
Conducted one-way ANOVAs to assess differences in COVID severity levels according to the following variables: Age, BMI, days with symptoms, and post-COVID-19 weight loss (Figure 1). ANOVAs revealed a statistically significant difference in the subject’s age (p = 0.020), BMI (p = 0.048), days with symptoms (p < 0.001), and post-COVID-19 weight loss (p < 0.001) across COVID-19 severity levels. Post Hoc tests were conducted to assess between groups differences (Figure 1).
3.4.2. Dietary Patterns
An excessive sugar diet was found to be associated with severe COVID-19. Figure 2 illustrates how individuals with severe COVID-19 (35%) were more likely to report adherence to an excessive sugar diet when compared with moderate (15%) and mild (11%) COVID-19 cases. A statistically significant difference across COVID-19 severity levels (p = 0.034) was found.
We also found an association between an excessive sugar diet and an increased symptom duration. Figure 3 illustrates adjusted means for days with COVID-19 symptoms according to the presence or absence of an excessive sugar diet. We adjusted for the following variables: Age, BMI, and post-COVID-19 weight loss. A significant difference (p = 0.016) was found between the presence of an excessive sugar diet (x̄ = 10.9 ± 1.0 days) and an absence of an excessive sugar diet (x̄ = 8.12 ± 0.4 days).
3.4.3. Physical Activity Patterns
An ANOVA test was conducted for each independent variable in Figure 4, revealing overall non-significant differences (p > 0.05). We observed a potential inverse relationship pattern between Total Lifetime PA and COVID-19 severity levels (Figure 4-A; Mild (mean: 20448, SE: 9834); Moderate (mean: 10731, SE: 3636); Severe (mean: 2593, SE: 1105). Walking lifetime PA demonstrated an unclear relationship with COVID-19 severity [Figure 4-B: Mild (mean: 2750, SE: 1205); Moderate (mean:1093, SE: 367); Severe (mean:1528, SE: 947)]. Moderate Lifetime PA [Figure 4-C; Mild (mean: 2890, SE: 1328); Moderate (mean:1407, SE: 573); Severe (mean: 299, SE: 164)] and Vigorous Lifetime PA [Figure 4-D; Mild (mean: 6336, SE: 3437); Moderate (mean: 3220, SE: 1311); Severe (mean: 252, SE: 258)] seem to have an inverse relationship pattern with COVID-19 severity levels. Finally, the Sedentary Lifetime Pattern might have a proportional relationship with COVID-19 severity [Figure 4-E; Mild (mean: 19.6, SE: 5.1); Moderate (mean: 21.6, SE: 7.9); Severe (mean: 23.7, SE: 11.3)].
4. Discussion
This study presents the strong validation scores of the questionnaire we designed and then applied (Table 1). We found associations between severe COVID-19 and age, BMI, days with symptoms, and post-COVID-19 weight loss (Figure 1). Individuals with a high sugar diet were linked to severe COVID-19 (Figure 2) and reported an increased symptom duration (Figure 3). We also observed an inverse relationship pattern between COVID-19 severity levels and total, moderate, and vigorous lifetime PA, which is absent in walking lifetime PA (Figure 4).
Lifestyle modifications, particularly maintaining a healthy diet and engaging in PA, have shown to improve outcomes related to chronic conditions associated with severe forms of COVID-19, such as type 2 diabetes and cardiovascular diseases [7,8]. Despite evidence suggesting an association of a plant-based diet with milder COVID-19 outcomes [9], we have limited understanding of specific dietary characteristics influencing COVID-19 severity. Moreover, PA has been associated with a decrease in severe COVID-19 outcomes such as hospitalization, ICU admission, and mortality [10,11,12], even when controlling for other known risk factors such as age and chronic diseases [4,5,13,14,15]. The lack of recommended PA has been suggested as the most important modifiable risk factor for severe COVID-19 [5]. However, the methodology for measuring PA is heterogeneous, [10,11,12], limiting the synthesis of results (meta-analysis). The IPAQ is widely used for measuring PA [11,13,15], but is limited to the assessment of the PA pattern of the week preceding the questionnaire application [16] - overlooking the PA habit of the individual. Also, some studies focus on the frequency and duration of PA, ignoring the pivotal intensity component of PA [12], as emphasized in the most recent PA guideline for Americans [6].
In this context, we designed, validated, and applied a questionnaire to explore the relationship between lifestyle factors, specifically diet and PA, and the severity of COVID-19 cases. We aimed to identify specific dietary characteristics associated with COVID-19 severity. Regarding PA, our questionnaire considers the frequency, duration, and intensity of PA. We also acknowledged the temporal limitation of the IPAQ [16], which assesses the most recent week of PA assessment, by integrating an item that explores the years of PA habit.
Our study illustrates the interplay between age, BMI, days with symptoms, and post-COVID-19 weight loss, revealing positive correlations among these factors (Table 4). We also found an association between severe COVID-19 and age; BMI; days with symptoms; and post-COVID-19 weight loss (Figure 1), confirming previous findings of age and obesity as risk factors for severe COVID-19 [4-5}.
In line with previous evidence associated with a healthy diet, such as a plant-based diet with milder COVID-19 outcomes [9], we identified an association between an excessive sugar diet and COVID-19 severity (Figure 2) and symptoms duration (Figure 3). The link between a high sugar diet and severe COVID-19 has been hypothesized in literature [24] and is supported by our results (Figure 2 and Figure 3). A high sugar diet has been related to elevated inflammatory markers [25], and chronic systemic inflammation has been linked to the development of chronic diseases associated with severe COVID-19 [3,4,5,26]. Therefore, this may explain the association of a high sugar diet with severe COVID-19.
Concerning PA, our results seem to demonstrate an inverse relationship pattern between severe COVID-19 and Total, Moderate, and Vigorous Lifetime PA (Figure 4-A, C, and D). Notably, no inverse relationship pattern is observed in Walking Lifetime PA (Figure 4-B). These difference in patterns may explain the potential additive benefits of moderate to high-intensity PA on COVID-19 severity when compared to the benefits of walking or low intensity PA. The intensity of the PA seems to be a factor to consider in assessing PA protective effects against severe COVID-19, as it has been suggested for general health benefits [6]. Additionally, a slight proportional relationship pattern was observed between Sedentary Lifetime PA and COVID-19 severity levels (Figure 4-E), in line with evidence that increased sedentary behavior increases all-cause mortality [6]. Although the relationships of Lifetime PA and COVID-19 severity are not statistically significant (Figure 4), they highlight the need for further research into the role of both intensity and PA habits on the severity of COVID-19. The need for specific recommendations on the duration, frequency, habit, and intensity of PA for protection against infectious diseases has been expressed before [27]. There is no consensus on whether high intensity PA is better than moderate intensity PA for protecting against severe COVID-19. Some authors have observed a linearity in PA doses and reduced COVID-19 severity [4], but others have shown a flattening in the dose response curve [12], even when considering cardiorespiratory fitness [14]. With recent studies concluding that vigorous PA does not increase the risk of infections [28], as it was once proposed [29], more research is needed to assess the differences between moderate and vigorous intensity PA regarding their protection against severe COVID-19.
Despite these valuable insights, it is crucial to acknowledge our study limitations. A self-reported retrospective questionnaire introduces misreporting and recall biases. Additionally, the cross-sectional design of our study and a sample size limited to a pilot study constrain causal inferences. Nonetheless, our study contributes valuable insights into the relationship between lifestyle factors and the severity of COVID-19.
In conclusion, our study introduces a validated questionnaire overcoming PA assessment of temporal limitations; it reveals associations of severe COVID-19 with age, BMI, and a high sugar diet; and it hints for a potential additional protection against severe COVID-19 from performing moderate to vigorous intensity PA compared with walking PA. While preliminary, our findings lay the groundwork for further research to inform public health strategies, aiming to prevent severe cases of future COVID-19 outbreaks and enhance overall population health.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Questionnaire S1: Lifestyle in Times of COVID-19 Questionnaire (Spanish).
Author Contributions
Conceptualization: E.B.-C.; Methodology: M.J.V.-J, O.G.F.-S., J.G.A.-G., F.I.C.-T., N.O., E.B.-C; Software: F.V.-A., O.G.F.-S., J.G.A.-G., F.I.C.-T., N.O.; Formal Analysis: F.V.-A., O.G.F.-S., J.G.A.-G., E.B.-C.; Investigation: M.J.V.-J, E.M.-L., E.B.-C.; Data Curation: F.V.-A., O.G.F.-S., J.G.A.-G.; Writing—Original Draft Preparation: F.V.-A., M.J.V.-J, O.G.F.-S., J.G.A.-G., F.I.C.-T., N.O., E.M.-L., E.B.-C; Writing—Review and Editing: F.V.-A., E.B.-C.; Visualization: M.J.V.-J, E.M.-L., E.B.-C; supervision: M.J.V.-J, E.M.-L., E.B.-C; Project Administration: E.B.-C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Faculty of Nutrition and Gastronomy of the “Universidad Autónoma de Sinaloa” (Registration number CE-FCNYG-2022-FEB-002).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy reasons.
Acknowledgments
We would like to express our gratitude to the expert panel responsible for validating the questionnaire and to the individuals who participated in responding to the questionnaire.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 28 February 2024).
- Woods, J. A.; Hutchinson, N. T.; Powers, S. K.; Roberts, W. O.; Gomez-Cabrera, M. C.; Radak, Z.; Berkes, I.; Boros, A.; Boldogh, I.; Leeuwenburgh, C.; Coelho-Júnior, H. J.; Marzetti, E.; Cheng, Y.; Liu, J.; Durstine, J. L.; Sun, J.; Ji, L. L. The COVID-19 Pandemic and Physical Activity. Sports Med. Health Sci. 2020, 2 (2), 55–64. [CrossRef]
- CDC. COVID-19. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html (Accessed on 28 January 2024).
- Steenkamp, L.; Saggers, R. T.; Bandini, R.; Stranges, S.; Choi, Y.-H.; Thornton, J. S.; Hendrie, S.; Patel, D.; Rabinowitz, S.; Patricios, J. Small Steps, Strong Shield: Directly Measured, Moderate Physical Activity in 65 361 Adults Is Associated with Significant Protective Effects from Severe COVID-19 Outcomes. Br. J. Sports Med. 2022, 56 (10), 568–577. [CrossRef]
- Sallis, R.; Young, D. R.; Tartof, S. Y.; Sallis, J. F.; Sall, J.; Li, Q.; Smith, G. N.; Cohen, D. A. Physical Inactivity Is Associated with a Higher Risk for Severe COVID-19 Outcomes: A Study in 48 440 Adult Patients. Br. J. Sports Med. 2021, 55 (19), 1099–1105. [CrossRef]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd Edition., 2018. Available online: https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf (accessed on 12 January 2024).
- Bennett, D. A.; Du, H.; Clarke, R.; Guo, Y.; Yang, L.; Bian, Z.; Chen, Y.; Millwood, I.; Yu, C.; He, P.; Zheng, X.; Collins, R.; Chen, J.; Peto, R.; Li, L.; Chen, Z.; for the China Kadoorie Biobank Study Collaborative Group. Association of Physical Activity with Risk of Major Cardiovascular Diseases in Chinese Men and Women. JAMA Cardiol. 2017, 2 (12), 1349. [CrossRef]
- Uusitupa, M.; Khan, T. A.; Viguiliouk, E.; Kahleova, H.; Rivellese, A. A.; Hermansen, K.; Pfeiffer, A.; Thanopoulou, A.; Salas-Salvadó, J.; Schwab, U.; Sievenpiper, J. L. Prevention of Type 2 Diabetes by Lifestyle Changes: A Systematic Review and Meta-Analysis. Nutrients 2019, 11 (11), 2611. [CrossRef]
- Merino, J.; Joshi, A. D.; Nguyen, L. H.; Leeming, E. R.; Mazidi, M.; Drew, D. A.; Gibson, R.; Graham, M. S.; Lo, C.-H.; Capdevila, J.; Murray, B.; Hu, C.; Selvachandran, S.; Hammers, A.; Bhupathiraju, S. N.; Sharma, S. V.; Sudre, C.; Astley, C. M.; Chavarro, J. E.; Kwon, S.; Ma, W.; Menni, C.; Willett, W. C.; Ourselin, S.; Steves, C. J.; Wolf, J.; Franks, P. W.; Spector, T. D.; Berry, S.; Chan, A. T. Diet Quality and Risk and Severity of COVID-19: A Prospective Cohort Study. Gut 2021, 70 (11), 2096–2104. [CrossRef]
- Gomide, E. B. G.; Abdalla, P. P.; Pisa, M. F.; Schneider, G.; Vieira, L. G.; Mazzonetto, L. F.; De Sousa Oliveira, A.; Sebastião, E.; Dos Santos, A. P. The Role of Physical Activity in the Clinical Outcomes of People Diagnosed with Covid-19: A Systematic Review. JSAMS Plus 2022, 1, 100007. [CrossRef]
- Rahmati, M.; Shamsi, M. M.; Khoramipour, K.; Malakoutinia, F.; Woo, W.; Park, S.; Yon, D. K.; Lee, S. W.; Shin, J. I.; Smith, L. Baseline Physical Activity Is Associated with Reduced Mortality and Disease Outcomes in COVID-19: A Systematic Review and Meta-analysis. Rev. Med. Virol. 2022, 32 (5), e2349. [CrossRef]
- Ezzatvar, Y.; Ramírez-Vélez, R.; Izquierdo, M.; Garcia-Hermoso, A. Physical Activity and Risk of Infection, Severity and Mortality of COVID-19: A Systematic Review and Non-Linear Dose–Response Meta-Analysis of Data from 1 853 610 Adults. Br. J. Sports Med. 2022, 56 (20), 1188–1193. [CrossRef]
- Hamer, M.; Kivimäki, M.; Gale, C. R.; Batty, G. D. Lifestyle Risk Factors, Inflammatory Mechanisms, and COVID-19 Hospitalization: A Community-Based Cohort Study of 387,109 Adults in UK. Brain. Behav. Immun. 2020, 87, 184–187. [CrossRef]
- Brandenburg, J. P.; Lesser, I. A.; Thomson, C. J.; Giles, L. V. Does Higher Self-Reported Cardiorespiratory Fitness Reduce the Odds of Hospitalization From COVID-19? J. Phys. Act. Health 2021, 18 (7), 782–788. [CrossRef]
- Lee, S. W.; Lee, J.; Moon, S. Y.; Jin, H. Y.; Yang, J. M.; Ogino, S.; Song, M.; Hong, S. H.; Ghayda, R. A.; Kronbichler, A.; Koyanagi, A.; Jacob, L.; Dragioti, E.; Smith, L.; Giovannucci, E.; Lee, I.-M.; Lee, D. H.; Lee, K. H.; Shin, Y. H.; Kim, S. Y.; Kim, M. S.; Won, H.-H.; Ekelund, U.; Shin, J. I.; Yon, D. K. Physical Activity and the Risk of SARS-CoV-2 Infection, Severe COVID-19 Illness and COVID-19 Related Mortality in South Korea: A Nationwide Cohort Study. Br. J. Sports Med. 2022, 56 (16), 901–912. [CrossRef]
- Craig, C. L.; Marshall, A. L.; Sj??Str??M, M.; Bauman, A. E.; Booth, M. L.; Ainsworth, B. E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J. F.; Oja, P. International Physical Activity Questionnaire: 12-Country Reliability and Validity: Med. Sci. Sports Exerc. 2003, 35 (8), 1381–1395. [CrossRef]
- Hernadnez-Nieto, R. A. Contributions to Statistical Analysis. 1992.
- Arámburo-Gálvez, J.; Carvalho Gomes, I.; André, T.; Beltrán-Cárdenas, C.; Macêdo-Callou, M.; Braga Rocha, É.; Mye-Takamatu-Watanabe, E.; Rahmeier-Fietz, V.; Figueroa-Salcido, O.; Cárdenas-Torres, F.; Ontiveros, N.; Cabrera-Chávez, F. Translation, Cultural Adaptation, and Evaluation of a Brazilian Portuguese Questionnaire to Estimate the Self-Reported Prevalence of Gluten-Related Disorders and Adherence to Gluten-Free Diet. Medicina (Mex.) 2019, 55 (9), 593. [CrossRef]
- Szigriszt-Pazos, F. Sistemas Predictivos de Legilibilidad Del Mensaje Escrito: Fórmula de Perspicuidad (PhD tesis). Universidad Complutense, Madrid. 2001.
- Barrio-Cantalejo, I. M.; Simón-Lorda, P.; Melguizo, M.; Escalona, I.; Marijuán, M. I.; Hernando, P. Validation of the INFLESZ Scale to Evaluate Readability of Texts Aimed at the Patient. An. Sist. Sanit. Navar. 2008, 31 (2), 132–152.
- Wu, Z.; McGoogan, J. M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323 (13), 1239. https://doi.org/10.1001/jama.2020.2648. (22) Ashok, P.; Kharche, J.; Raju, R.; Godbole, G. Metabolic Equivalent Task Assessment for Physical Activity in Medical Students. Natl. J. Physiol. Pharm. Pharmacol. 2017, 7 (2), 1. [CrossRef]
- Ashok, P.; Kharche, J.; Raju, R.; Godbole, G. Metabolic Equivalent Task Assessment for Physical Activity in Medical Students. Natl. J. Physiol. Pharm. Pharmacol. 2017, 7 (2), 1. [CrossRef]
- Herrmann, S. D.; Willis, E. A.; Ainsworth, B. E.; Barreira, T. V.; Hastert, M.; Kracht, C. L.; Schuna, J. M.; Cai, Z.; Quan, M.; Tudor-Locke, C.; Whitt-Glover, M. C.; Jacobs, D. R. 2024 Adult Compendium of Physical Activities: A Third Update of the Energy Costs of Human Activities. J. Sport Health Sci. 2024, 13 (1), 6–12. [CrossRef]
- Chesnut, W. M.; MacDonald, S.; Wambier, C. G. Could Diet and Exercise Reduce Risk of COVID-19 Syndemic? Med. Hypotheses 2021, 148, 110502. [CrossRef]
- O’Connor, L.; Imamura, F.; Brage, S.; Griffin, S. J.; Wareham, N. J.; Forouhi, N. G. Intakes and Sources of Dietary Sugars and Their Association with Metabolic and Inflammatory Markers. Clin. Nutr. 2018, 37 (4), 1313–1322. [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D. W.; Fasano, A.; Miller, G. W.; Miller, A. H.; Mantovani, A.; Weyand, C. M.; Barzilai, N.; Goronzy, J. J.; Rando, T. A.; Effros, R. B.; Lucia, A.; Kleinstreuer, N.; Slavich, G. M. Chronic Inflammation in the Etiology of Disease across the Life Span. Nat. Med. 2019, 25 (12), 1822–1832. [CrossRef]
- Chastin, S. F. M.; Abaraogu, U.; Bourgois, J. G.; Dall, P. M.; Darnborough, J.; Duncan, E.; Dumortier, J.; Pavón, D. J.; McParland, J.; Roberts, N. J.; Hamer, M. Effects of Regular Physical Activity on the Immune System, Vaccination and Risk of Community-Acquired Infectious Disease in the General Population: Systematic Review and Meta-Analysis. Sports Med. 2021, 51 (8), 1673–1686. [CrossRef]
- Campbell, J. P.; Turner, J. E. Debunking the Myth of Exercise-Induced Immune Suppression: Redefining the Impact of Exercise on Immunological Health Across the Lifespan. Front. Immunol. 2018, 9, 648. [CrossRef]
- Nieman, D. Exercise, Infection, and Immunity. Int. J. Sports Med. 1994, 15 (S 3), S131–S141. [CrossRef]
Figure 1.
Line graphs illustrating mean and standard error of (A) Age, (B) BMI, (C) Days with symptoms, and (D) Post-COVID-19 weight loss across COVID-19 severity levels. ANOVAs were conducted and yielded overall significant differences across COVID-19 severity levels. Post Hoc p < 0.05 = *. Exact Pot Hoc p values demonstrating trends are included.
Figure 1.
Line graphs illustrating mean and standard error of (A) Age, (B) BMI, (C) Days with symptoms, and (D) Post-COVID-19 weight loss across COVID-19 severity levels. ANOVAs were conducted and yielded overall significant differences across COVID-19 severity levels. Post Hoc p < 0.05 = *. Exact Pot Hoc p values demonstrating trends are included.
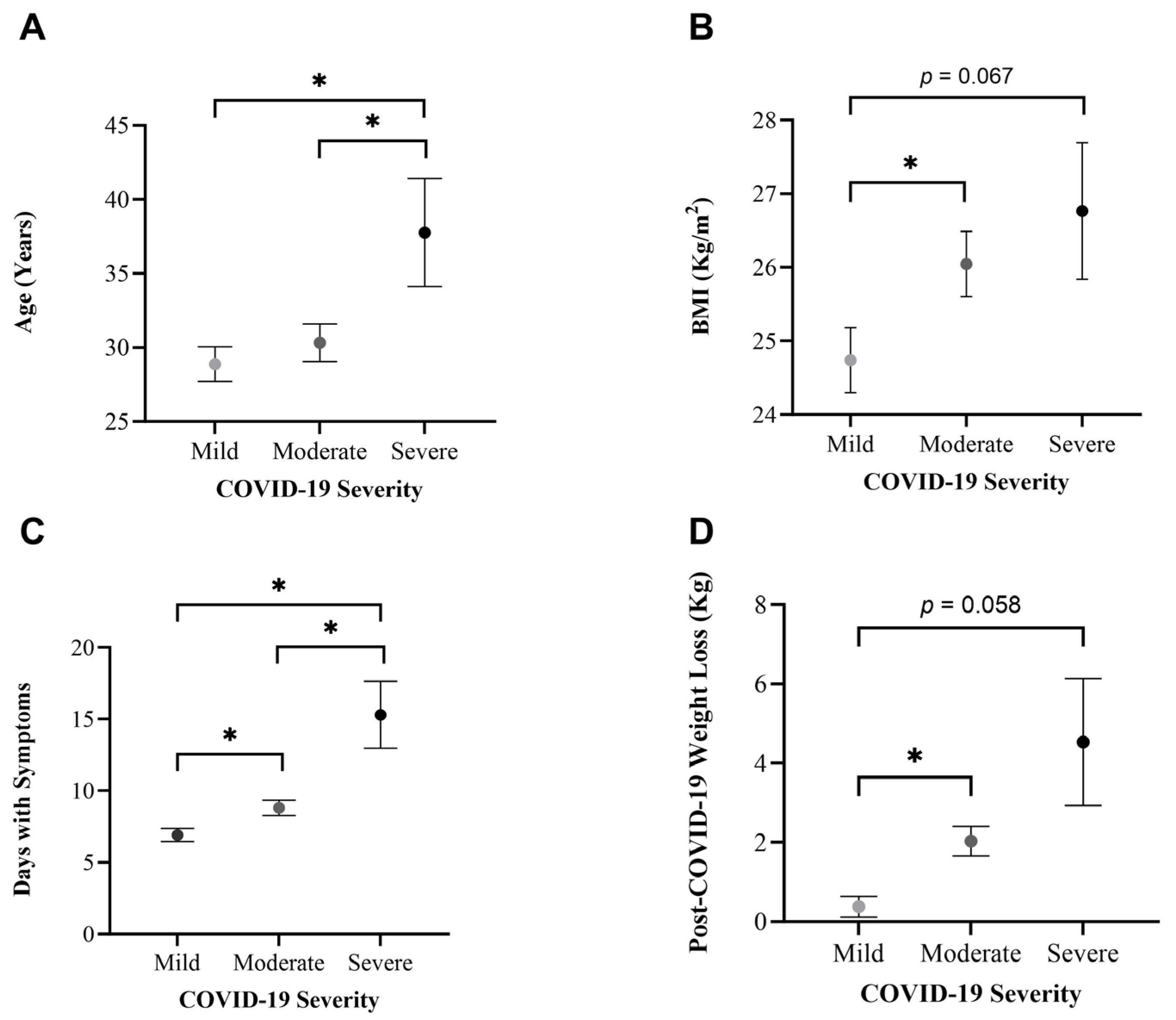
Figure 2.
Bar graph demonstrating the percentage of subjects referring to an excessive sugar diet across COVID-19 severity levels. A Chi-squared test was performed (p = 0.034). * = Highest difference between observed and expected frequencies.
Figure 2.
Bar graph demonstrating the percentage of subjects referring to an excessive sugar diet across COVID-19 severity levels. A Chi-squared test was performed (p = 0.034). * = Highest difference between observed and expected frequencies.
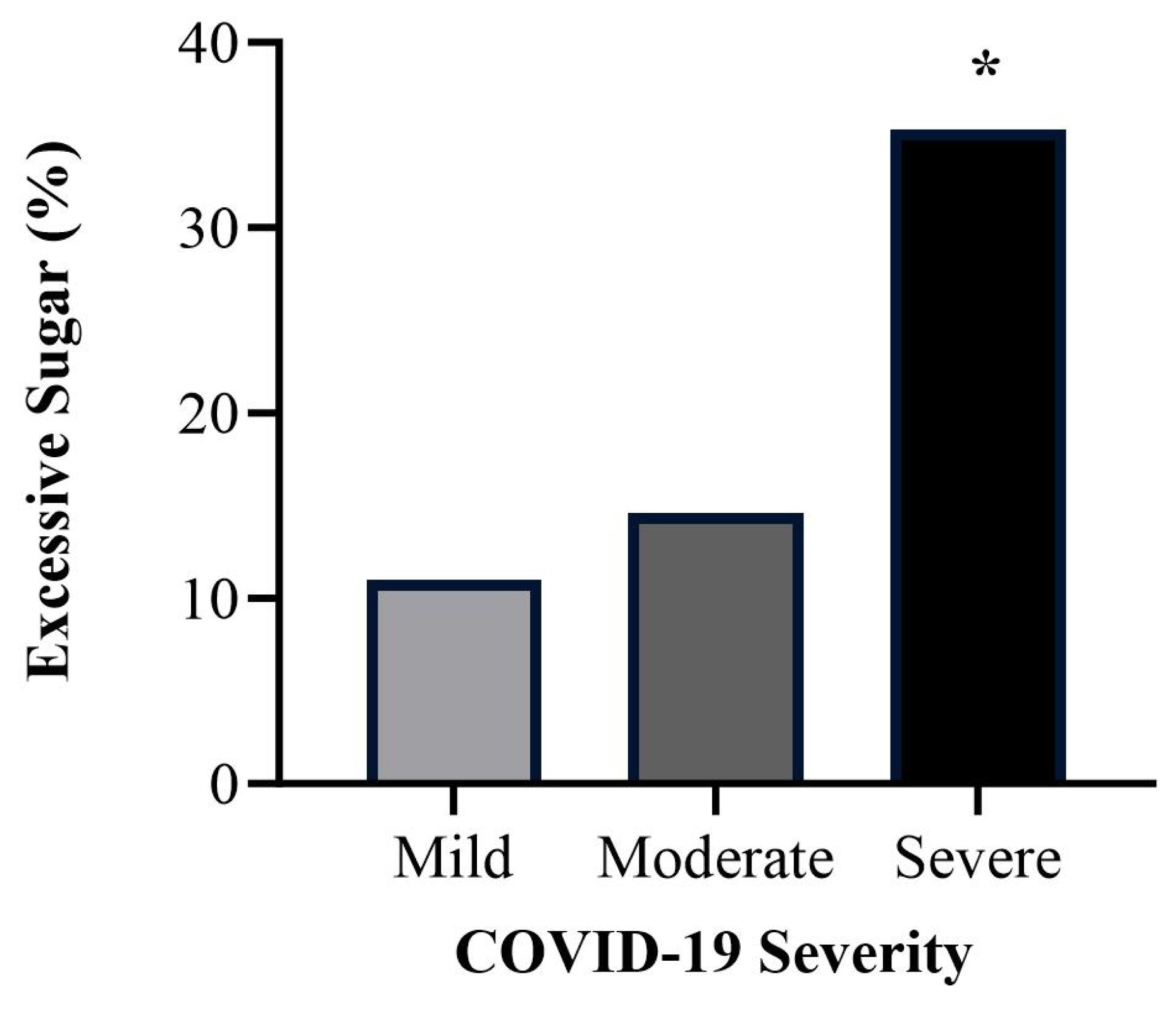
Figure 3.
Adjusted means for days with COVID-19 symptoms according to an excessive sugar diet. A significant difference was found between adjusted means (p = 0.016). Adjusted by age, BMI, and post COVID-19 weight Loss.
Figure 3.
Adjusted means for days with COVID-19 symptoms according to an excessive sugar diet. A significant difference was found between adjusted means (p = 0.016). Adjusted by age, BMI, and post COVID-19 weight Loss.
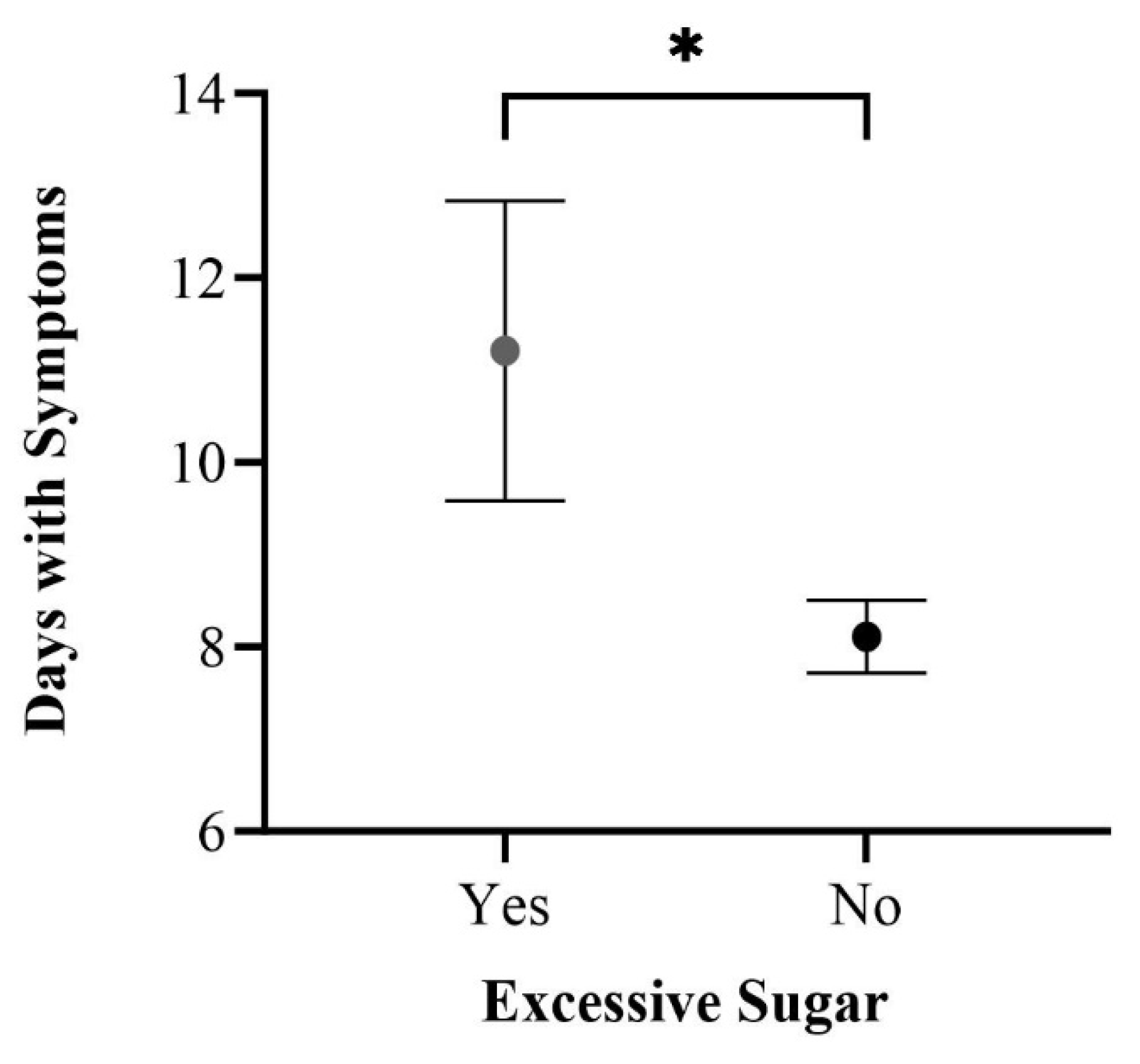
Figure 4.
Line graphs of (A) Total Lifetime PA, (B) Walking Lifetime PA, (C) Moderate Lifetime PA, (D) Vigorous Lifetime PA, and (E) Sedentary Lifetime Pattern across COVID-19 severity levels: Comparing mean and standard error. An ANOVA test was conducted, revealing overall non-significant differences (p < 0.05).
Figure 4.
Line graphs of (A) Total Lifetime PA, (B) Walking Lifetime PA, (C) Moderate Lifetime PA, (D) Vigorous Lifetime PA, and (E) Sedentary Lifetime Pattern across COVID-19 severity levels: Comparing mean and standard error. An ANOVA test was conducted, revealing overall non-significant differences (p < 0.05).
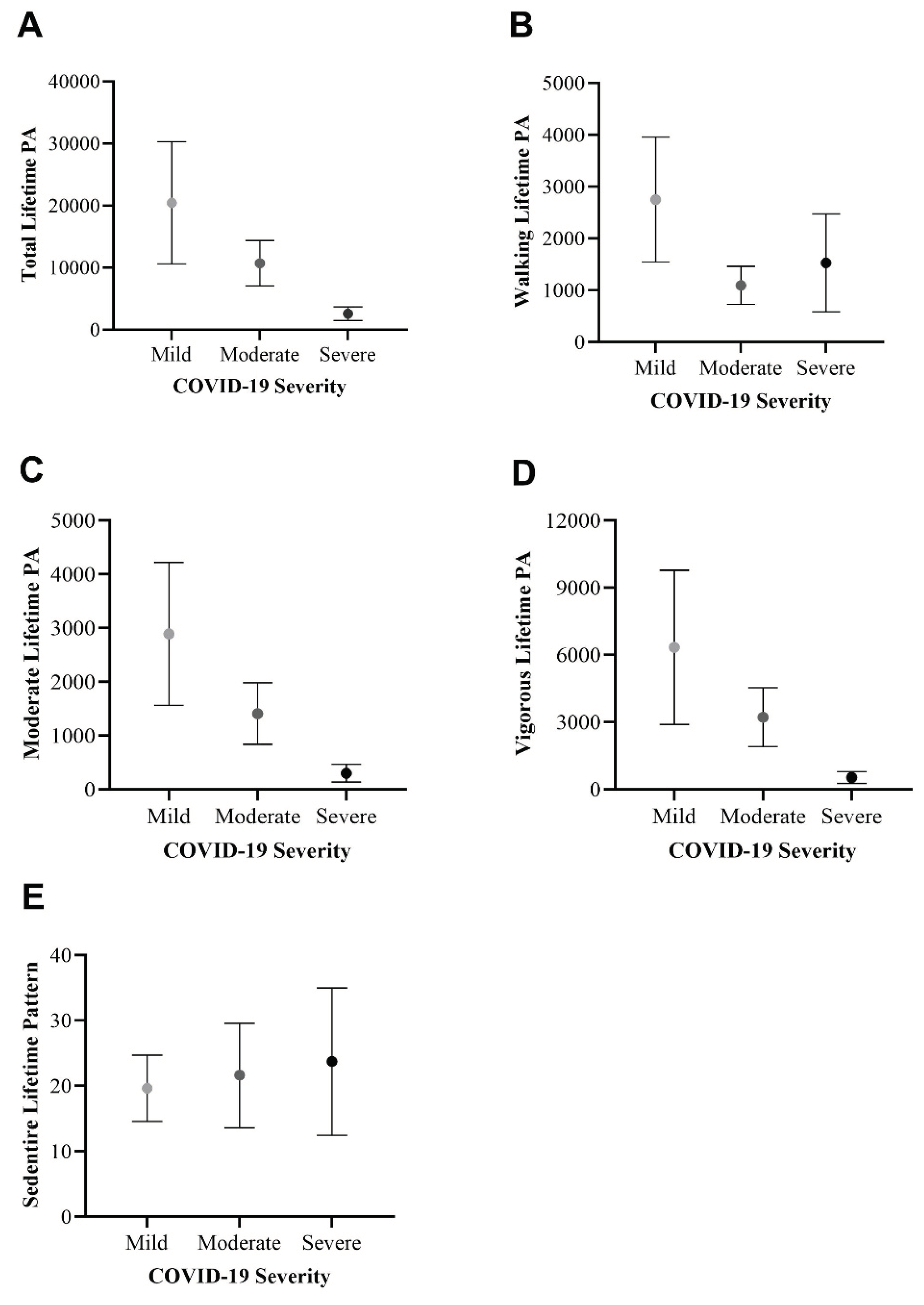

Table 1.
Questionnaire validation scores given by health professionals.
| Number of Experts | Relevance Mean ± SD | Clarity Mean ± SD | Writing and terminology Mean ± SD | Format Mean ± SD | CVCt |
|---|---|---|---|---|---|
| 11 | 4.53 ± 0.67 | 4.47 ± 0.77 | 4.44 ± 0.78 | 4.45 ± 0.82 | 0.90 |
Data are presented as mean and standard deviation. Validation scores range from 1 to 5. CVCt: Total content validity coefficient.
Table 2.
Social and Demographic Characteristics of the Study Sample.
| Variable | |
|---|---|
| Age (mean ± SD) | 30.30 ± 12.05 |
| Sex n (%) | |
| Female | 130 (66.0) |
| Male | 67 (34.0) |
| BMI kg/m2 (mean ± SD) | 25.50 ± 4.21 |
| Ethnicity n (%) | |
| Mexican Mestizo | 197 (100) |
| Marital Status n (%) | |
| Single | 123 (62.4) |
| Married | 63 (32.0) |
| Consensual Union | 7 (3.6) |
| Other | 4 (2.0) |
| Education n (%) | |
| Postsecondary Education | 137 (69.5) |
| Elementary and Secondary Education | 60 (30.5) |
| Occupation n (%) | |
| Student | 75 (38.1) |
| Employee | 64 (32.5) |
| Self-Employed | 43 (21.8) |
| Unemployed | 5 (2.5) |
| Other | 10 (5.1) |
| Total sample = 197. Quantitative variables are represented as “Mean (± SD)” and qualitative variables as “n (%)”. | |
Table 3.
COVID-19 General Profile of the Individuals.
| Variable | Variable | ||
|---|---|---|---|
| Diagnostic Tool n (%) | Days with Symptoms (mean ± SD) | 8.57 ± 5.72 | |
| PCR | 76 (38.6) | Hospitalized n (%) | |
| Antigen Test | 59 (29.9) | No | 185 (98.4) |
| Antibody Test | 22 (11.2) | Yes | 3 (1.6) |
| Antigen Test + Clinical | 4 (2.0) | ICU | 1 (33.3) |
| Antibody Test + Clinical | 7 (3.6) | Oxygen Need n (%) | |
| Clinical | 29 (14.7) | No | 181 (96.3) |
| Year of Diagnosis n (%) | Yes | 7 (3.7) | |
| 2022 | 56 (28.6) | Severity n (%) | |
| 2021 | 81 (41.3) | Mild | 91 (46.2) |
| 2020 | 55 (28.1) | Moderate | 89 (45.2) |
| 2019 | 4 (2.0) | Severe | 17 (8.6) |
| Symptoms n (%) | Post COVID-19 Weight Loss (Kg) (mean ± SD) | 1.48 ± 3.67 | |
| Present | 188 (95.4) | Comorbidities n (%) | |
| Headache | 149 (75.6) | No | 162 (82.2) |
| Fatigue | 137 (69.5) | Yes | 35 (17.8) |
| Fever | 119 (60.4) | Vaccination n (%) | |
| Sore Throat | 111 (56.3) | Yes | 187 (96.4) |
| Anosmia | 107 (54.3) | No | 7 (3.6) |
| Cough | 91 (46.2) | Initial Vaccine Type | |
| Joint Pain | 89 (45.2) | AstraZeneca | 70 (37.4) |
| Eye Pain | 73 (37.1) | Sinovac | 69 (37.0) |
| Nasal Congestion | 69 (35.0) | Pfizer | 23 (12.3) |
| Runny Nose | 66 (33.5) | CanSino | 15 (8.0) |
| Shortness of Breath | 60 (30.5) | Other | 10 (5.3) |
| Diarrhea | 26 (13.2) | COVID-19 Post Vaccine n (%) | |
| Vomit | 11 (5.6) | Yes | 62 (35.0) |
| Absent | 9 (4.6) | No | 115 (65.0) |
| Items totaling less than 197 (total sample) are attributed to instances where participants left items in blank. Quantitative variables are represented as “Mean (± SD)” and qualitative variables as “n (%)”. | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



