
Submitted:
09 March 2024
Posted:
11 March 2024
You are already at the latest version
Abstract
Musculoskeletal injuries such as equine osteoarthritis, osteoarticular defects, tendonitis/desmitis, and muscular disorders are prevalent among sport horses, with a fair prognosis for returning to exercise or previous performance levels. The field of equine medicine has witnessed rapid and fruitful development, resulting in a diverse range of therapeutic options for musculoskeletal problems. Staying abreast of these advancements can be challenging, prompting the need for a comprehensive review of commonly used and recent treatments. The aim is to compile current therapeutic options for managing these injuries, spanning from simple to complex physiotherapy techniques, conservative treatments including steroidal and non-steroidal anti-inflammatory drugs, hyaluronic acid, and polyacrylamides, to the promising regenerative therapies such as hemoderivatives and stem cell-based therapies. Each therapeutic modality is scrutinized for its benefits, limitations, and potential synergistic actions to facilitate their most effective application for intended healing/regeneration of the injured tissue/organ and subsequent patient recovery. While stem cell-based therapies emerge as particularly promising for equine musculoskeletal injuries, a multidisciplinary approach is underscored throughout the discussion, emphasizing the importance of considering various therapeutic modalities in tandem.
Keywords:
Conservative therapies
; equine
; hemoderivatives
; musculoskeletal
; osteoarthritis
; physiotherapy
; regenerative therapies
; sports medicine
; stem cell
; tendinitis
1. Introduction
In equine sports medicine, musculoskeletal lesions, such as, tendonitis, desmitis, osteoarticular lesions/defects, and muscular strains stand as significant challenges. These conditions often result in a partial or complete loss of performance, jeopardizing the athlete’s sporting career. Beyond the immediate impact on performance, these injuries can have far-reaching consequences, affecting the overall well-being of the horse [1,2]. The repercussions extend to individual health, sporting activity, and carry social and economic implications, making the management and prevention of such musculoskeletal issues crucial in the field of equine sports[3,4,5]—Figure 1.
Each of these injuries presents unique challenges in terms of diagnosis, treatment, and rehabilitation. Understanding and addressing these issues is vital for maintaining the health and longevity of equine athletes.
The present work provides an overview of prevalent musculoskeletal pathologies, explores complementary diagnostic exams, and reviews existing therapeutic options for managing pain, inflammation, and the healing or regeneration of affected musculoskeletal structures. The current prospect offers a diverse range of therapeutic options, each varying in ease of use, availability, economic considerations, mode of action, effectiveness, and clinical outcomes.
Initial treatment protocols emphasize conservative interventions aimed at alleviating clinical signs, slowing progression, and potentially facilitating tissue repair through fibrosis or scar formation [6]. These interventions span both non-pharmacological and pharmacological approaches, encompassing a spectrum of exercises and physical modalities (e.g., laser therapy, ultrasound, electrotherapy, and shock waves) as well as pharmacological options including anti-inflammatories, viscosupplementation, and bisphosphonates. Surgical techniques, such as tendon splitting, are also employed for conditions as tendonitis to provide relief of clinical signs and induce tissue repair.
More recently, the focus has shifted towards achieving tissue regeneration rather than mere repair. Several pro-regenerative therapeutic options have emerged, and others are currently in development. Termed orthobiologics, a subdivision of regenerative medicine, with a specific emphasis on addressing musculoskeletal conditions, these therapies are based on biological substances to promote regeneration in tendons, muscles, and joints [7]. Two major categories within orthobiologics are hemoderivatives and stem cell-based therapies. The composition, distinctions, beneficial contributions, advantages offered by each, and the appropriate scenarios for their application will be elucidated through the document. The overarching objective of these regenerative therapies is to preserve organ function and facilitate the restoration of native physiological capacity in musculoskeletal diseases.
2. Epidemiology
Equine sportive modalities influence the musculoskeletal injury location, as well as its type, prevalence and predisposition [8,9].
Equine orthopaedic conditions are more frequently described in race horses, perhaps because horseracing is strongly present worldwide, being a very representative part of equine industry. Race horses are predominantly young horses, from 2-5 years old [10]. The most representative types of injuries are stress fractures, tendonitis and suspensory ligament (SL) desmitis of the forelimbs (FL), metacarpophalangeal and carpal joints pathologies [8,11,12,13]. In race horses, muscular injuries by fatigue are also common [8].
In showjumping horses, the higher percentage of lesions are at the FL. The highest incidence of lesions appears as following: FL tendon/ligament, metacarpophalangeal and metatarsophalangeal joints and in the FL hoof [8]. This is promptly understood as showjumping horses are required to jump obstacles accurately and at high speed, with tight turns, doing landings of extreme impact with an associated ground reaction that overloads the FL. Comparing with horses practising other modalities, FL tendonitis are more frequent in showjumping horses [8,9].
Dressage horses perform a type of exercises that overload hindlimbs (HL), being more prone to injuries at the HL tendons/ligaments—the most frequent type of lesion—followed by stifle joint, metacarpophalangeal joint, FL tendon/ligament, tarsus, hip and metatarsophalangeal joints [8]. SL desmitis is very common in dressage and race horses, being more common at FL in dressage horses and HL in race horses [9].
Working horses are more predisposed to injuries at FL tendons/ligaments, metacarpophalangeal joint, scapulohumeral and tarsal joints and FL hoofs [8].
Training conditions might also interfere with musculoskeletal pathology. Variables such as indoor arenas, horse-walkers, back problems, arenas that sink and become irregular with wet conditions and sand-based arenas—are factors associated with increased risk of injury. On the other hand, lunging appears to have a protective effect [14,15]. It was also demonstrated that there was a decreased risk of lameness in larger stables than in smaller ones, and an increased risk of lameness in active horses [16].
3. Most Common Musculoskeletal Pathologies
The most common musculoskeletal pathologies involve those affecting the tendon, cartilage, muscle and bone. In younger animals, soft tissue injuries are more frequent and, degenerative diseases are more prevalent in mature horses [8,9,15].
Age-related degenerative diseases, such as joint disease are more common among horses whose physical activities require longer training and in those who have longer athletic careers, such as jumping, dressage, polo pony and working [8,15]. Degenerative joint diseases, such as osteoarthritis (OA), adversely impact the health of the equine athlete, being considered one of the most common causes of lameness and consequent loss of performance, thus causing important sportive, social and economic constraints in equine industry [17].
OA arises consequent to articular damage and is defined as a progressive and permanent destruction of articular cartilage and subchondral bone exposure, resulting in loss of function and associated changes in the bones and soft tissues of the joint (ligaments, synovial membrane and menisci) such as osteophytes formation, subchondral sclerosis, desmitis, and synovial hyperplasia [18]. The articular cartilage is a highly differentiated structure with a limited healing potential due to lack of organization, innervation and lymphatic vessels which result in reduced inflow of blood progenitor cells, thus remaining a big challenge to repair [17]. The lack of cartilage innervation means that only when the subchondral bone is affected, the animal begins to manifest pain more intensely. Several factors, including trauma to the joint, immobilization, conformation, shoeing, and ageing, have been related with OA [19]. It is a disease characterized by pain, joint deformity and instability, reduction of function and motion. Once initiated, it is very difficult to control the progress of OA as conventional treatments only attenuate its clinical signs and do not alter disease progression [20,21].
In equine lameness, joint injury represents 60% of the causes. OA affects over 80% of horses with more than 15 years [22]. OA can also develop in younger horses depending on their age, body weight and exercise program [23]. In horseraces, the metacarpophalangeal and the carpal joints are the most common affected joints with spontaneous OA [24]. Among joint disease it is also included full and partial thickness articular defects whose prognosis is very fair regarding return to function. Partial thickness defects affect only articular cartilage; full-thickness defects also reach subchondral bone and may occur in young horses and in mature sport horses, secondarily to stress-related trauma [25]. Invariably, these types of joint defects result in secondary OA.
Tendinopathy is also one of the most common musculoskeletal disorders. Tendons and ligaments are important structures in the musculoskeletal system of distal limbs, transmitting large forces between muscles and bones. While this is the predominant function of all tendons, some also serve as energy stores, reducing the cost of locomotion. Energy storing tendons experience extremely high strains and need to be able to recoil efficiently for maximum energy storage and return. In the equine forelimb, the energy storing superficial digital flexor tendon (SDFT) has much higher failure strains than the positional common digital extensor tendon (CDET), being therefore more commonly injured [26]. Tendon injuries are common in athletic horses, requiring a long rehabilitation process characterized by slow and incomplete repair mechanisms. Instead of native elastic tissue, fibrotic tissue forms, often leading to re-injury. This can significantly impact the horse’s athletic performance and career [27]. Poor vascularization is one of the reasons for limited tendon tissue healing ability as adequate blood supply is necessary for the transport of nutrients, inflammatory mediators, and proteolytic enzymes in and out of a tendon [28]. The most common cause of tendonitis and desmitis is external trauma, nevertheless, athleticism and ageing are also common causes. Tendonitis and desmitis may occur in different anatomical locations (e.g. enthesis, mid body, distal part) and the clinical presentation may also be variable going from acute sprains, to ruptures and chronic tendinopathy, with a range of clinical signs. This spectrum of the disease concomitantly with tendon characteristics results into a considerable therapeutic defiance, with no clear single approach and often poor and long-term outcomes [1].
Traumatic muscular lesions also represent a significant threat in sports medicine, as the healing process often leads to excessive fibrosis or fatty degeneration. These outcomes frequently occur after severe traumatic injury and contribute to muscle degeneration and dysfunction [29]. Muscular lacerations may be partial or complete and are accompanied by lameness [30,31]. Mild lacerations may cause severe volumetric skeletal muscle loss and injury [32]. Showjumpers and eventers are both prone to gluteal and lumbar muscular strains, presenting mild to moderate lameness. Also, muscular fatigue is responsible for soreness and consequent lameness.
When lesion occur, the main source for muscle regeneration and growth is a population of muscle stem cells called satellite cells. This population becomes depleted when there is muscle wastage or atrophy, or when a continuous injury is exerted in the muscle, thus decreasing its regenerative capacity [32].
4. Clinical Examination
A complete history and a comprehensive clinical and orthopaedic examination holds paramount importance in the field of orthopaedic medicine, to accurately diagnose musculoskeletal conditions [33]. The findings from a clinical and orthopaedic examination guide the formulation of an appropriate plan of complementary diagnostic exams and tailored treatment strategy. Also, the examination aids in identifying any underlying issue contributing to musculoskeletal problems. Orthopaedic examination must include inspection, palpation, percussion, hoof testers and dynamic analysis of the horse. This holistic approach ensures that all relevant factors are considered for comprehensive care [34]. Regular clinical examinations can help identify risk factors or early signs of musculoskeletal issues. This allows for the implementation of preventive measures to mitigate the progression of conditions or prevent future injuries. Follow-up examinations are essential for monitoring the progress of treatment and adjusting interventions as needed. This constant process ensures that the patient’s musculoskeletal health is continually assessed and managed effectively. In summary, equine clinical examinations are essential for maintaining the health, well-being, and performance of horses [35].
5. Complementary Diagnostic Exams
To accurately diagnose musculoskeletal pathologies, a comprehensive physical and orthopaedic examinations, along with detailed complementary diagnostic (CD) tests, is imperative. CD tools encompass a broad spectrum, including flexion tests, perineural nerve blocks, and various imaging techniques. The selection of these tools depends on factors such as accuracy, accessibility, cost, and the ability of individuals or professionals to interpret the images. For the diagnosis of musculoskeletal injuries, available imaging techniques comprise radiographs (X-ray), ultrasound (U/S) images, arthroscopy, magnetic resonance imaging (MRI), computed tomography (CT), and scintigraphy. Each of these methods offers unique advantages and considerations in the diagnostic process.
Perineural nerve blocks aid in the determination of pain localization area [36].Radiography stands as a non-invasive and primary diagnostic tool, offering crucial insights into several aspects. It enables the identification of significant information, encompassing the diagnosis of evident bone fractures, defects in articular cartilage, and indications of OA. In radiological OA diagnosis, three primary findings are prominent: the presence of osteophytes, increased subchondral density, and the eventual narrowing of the joint space in its advanced stages [17].
Nevertheless, during the early stages of a lesion, the observation of radiological evidence becomes challenging, potentially leading to inappropriate exclusion or insufficient information regarding the actual extent of the lesions. Moreover, when assessing complex joints, radiography faces limitations as it provides a two-dimensional (2D) representation of three-dimensional (3D) structures. This limitation arises because multiple soft tissues and bony structures are superimposed, making it difficult to evaluate them individually. Consequently, radiography may not be the most favourable method for the assessment of soft tissues [37,38]. Nonetheless, when dealing with cases involving joint or limb distension, radiography is recommended as an initial diagnostic procedure. In instances of acute tendinopathy, desmopathy, or enthesopathy without fragmentation of the insertional surface, radiography may primarily indicate the presence of soft tissue swelling [39].
Ultrasonography emerges as the preferred technique for diagnosing, assessing, and documenting tendon and ligament lesions, offering valuable insights into therapeutic and healing progresses. The ultrasonographic method for evaluating the pastern region, specifically for palmar/plantar tendon/ligament assessment, is roughly documented in the existing literature [40,41,42]. A thorough ultrasound assessment of soft tissue injuries is very important to accurate diagnosis of these lesions [7]. However, in conditions of intra-articular soft tissue lesions, it does not allow visualization of structures located deep to bone [38,43,44]. Since 1990, ultrasonography started to be a complement to radiograph in cartilage defects diagnosis [45]. Ultrasound has become an essential diagnostic tool as it gives precise information on the synovial membrane and fluid, articular cartilage, subchondral bone, joint margins, ligaments and menisci, as well as on the periarticular structures [45]. It requires good ultrasound devices and a strict standardization of the approach technique to every joint. A substantial anatomical knowledge of the equine locomotor system is crucial to warrant sensitivity and specificity of diagnostic ultrasonography of joint structures [45,46].
In cases of joint lesions, arthroscopy proves to be a valuable diagnostic tool with dual functionality for both diagnosis and treatment. This invasive technique enables intra-articular visualization of the cartilage surface, synovia, and ligaments, offering information on the characteristics of cartilage defects and allowing for grading. Arthroscopy is particularly adept at assessing early, subtle cartilage lesions. However, it should be noted that it has limitations, as it may underestimate the extent of certain lesions and overestimate others. This is attributed to its inability to provide a representative image of the entire articular surface [47,48]. At the same time, it also grants the treatment of some lesions such as removal of cartilage fragments and joint/synovial debris, osteochondral curettage, as well as samples collection.
Currently, MRI is the optimal method for the evaluation and monitoring of tendon/ligament and articular cartilage health, providing cross sectional images. While it is a non-invasive assessment technique, it can detect soft tissue changes and can assess cartilage morphology. It also provides volumetric and whole joint assessment without ionizing radiation. This technique is able to non-invasively detect biochemical changes in tendons, ligaments and cartilage that precede structural damage and may offer a great advance in the diagnosis and treatment of this debilitating conditions[49,50,51]. For soft tissue injuries of the palmar aspect of the metacarpal/tarsal regions, MRI is considered more accurate that U/S due to the risk of underdiagnosing injuries [52]. For diagnostic of distal structure lesions, it might be done in a standing manner, with an open U-shaped MRI, that is designed to enable imaging up to the level of carpus and tarsus excluding the need of general anaesthesia [53]. However, its high cost prevents widespread use in initial clinical assessments or during subsequent follow-up examinations to characterize the progression of healing, and the technique requires the availability of professionals trained in interpreting the images obtained.
CT scan is also a non-invasive procedure that involves the use of radiation enabling visualization of bones and soft tissues, producing a 3D image reconstruction [54]. It usually implies general anaesthesia but nowadays there are also standing CTs. CT arthrography is a very useful diagnostic tool for assessing cartilage defects in metacarpo/tarso-phalangeal joints due to its short acquisition time, its specificity and sensitivity, and it might also be more accurate than MRI. However, MRI allows a better assessment of soft tissues and subchondral bone, being a useful technique for joint evaluation [56]. A study was performed comparing CT arthrography (CTA) and MRI sensitivity and specificity in articular cartilage defects in equine metacarpophalangeal joints. CTA scan sensitivity and specificity were 0.82 and 0.96, respectively, and were significantly higher than those of MRI (0.41 and 0.93, respectively) in detecting overall cartilage defects (no defect vs. defect). CTA was considered a valuable tool in the diagnostic of articular cartilage defects. CTA specificity is greater than MRI, and their sensitivity is very similar, thus concluding that CTA may be preferred, in this cases, over MRI due to higher availability and easier image acquisition [50].
Nuclear scintigraphy involves the intravenous administration of a radioisotope that binds to bone structures, reflecting osteoblast activity and organ function rather than providing detailed anatomical information. This approach enables the diagnosis of skeletal activity and injuries. Nuclear scintigraphy is particularly employed in the evaluation of lameness and poor performance, offering high sensitivity in detecting osseous remodelling associated with stress fractures and stress-related bone injuries [55]. The radioisotope uptake (IRU) by bone might not reflect the pain focus, only bone activity, and can also be associated with other musculoskeletal injuries rather than osseous [56]. Therefore, an in-depth investigation must be done, it is advisable to use this technique together with regional nerve blocks and other diagnostic imaging techniques, to better identify the injuries and the focus of lameness. Scintigraphy has the potential to provide valuable information, but interpretation is not always straightforward, requiring careful correlation with other clinical and imaging findings [56].
6. Treatment Options
A diverse array of therapeutic modalities is available for addressing musculoskeletal injuries, ranging from straightforward pain management and inflammation medications to the use of physiotherapy with the shared goal of enhancing biomechanics and restoring function to affected tissues [57]. A relatively recent entrant into the musculoskeletal therapeutic panorama is regenerative therapies, also known as orthobiologics, which assert the ability to regenerate injured tissues or structures. The knowledge and development in this field are progressing rapidly. Both conservative and regenerative therapies play crucial roles in managing musculoskeletal injuries, offering a spectrum of options for horse owners, trainers, and veterinarians to tailor treatments based on the nature and severity of the condition. The choice between these approaches often depends on factors like the specific injury, the horse’s individual characteristics, and the desired outcome for the athlete’s performance and well-being. Subsequently, this discussion will delve into the conservative and regenerative therapeutic options available for treating the aforementioned musculoskeletal pathologies—Table 1.
6.1. Conservative Therapies
Conservative therapies have the primary objective of alleviating pain, reducing inflammation, and restoring function. These approaches resort to the use of physical rehabilitation and therapeutic exercises, as well as the administration of pharmacological agents. These interventions aim to manage symptoms and promote the gradual recovery of musculoskeletal health without resorting to more invasive procedures[6,39,58].
6.1.1. Physiotherapeutic Modalities
Physical treatment and rehabilitation exercises play a crucial role in promoting the sound musculoskeletal recovery of horses, offering solutions in both preventive and therapeutic scenarios for athletes [57]. In equine sports, physiotherapy primarily targets the soft tissues involved and is deemed essential to the overall recovery process [57]. Interestingly, during a “Federation Equestre Internationale” (FEI) competition, physiotherapy may be the sole type of therapy permitted for horses, as many of physiotherapeutic modalities are not considered doping and must be administered by “Permitted Equine Therapists”.
Physical therapies encompass a broad spectrum of modalities, ranging from manual therapies to more intricate procedures involving various tools and appliances. Manual therapies often include passive stretching, tissue mobilization, and joint mobilization. Physical and mechanical agents consist of thermal therapy, kinesiotape and/or bandages, and electrotherapy. Within the electrotherapy scenario, options such as magnetic field therapy, electrostimulation, therapeutic ultrasound, laser therapy, extracorporeal shockwave therapy, and vibration plates are used.
The overarching objective of physiotherapy is to reduce or improve the management of biomechanical constraints that generate and sustain pain and/or lesions. Physiotherapy interventions aim to address inflammation and pain, promote healing, and prevent or manage secondary lesions or complications [57]. This comprehensive approach to physical therapy contributes significantly to the overall well-being and performance of equine athletes.
Physical and Mechanical Agents
Manual Therapy
Manual therapy consists of applying the therapist’s hands to the patient’s body for diagnostic or therapeutic purposes. Passive stretching, a modality within manual therapy, is used to improve range of motion, prevent injury and decrease pain. It is recommended that each stretch be performed for 3–5 min, once daily, over 3–7 days per week to provide an adequate stimulus [59]. Tissue mobilization implies a deeper mobilization of tissues, including massage, myofascial release, tissue mobilization to break down myofascial adhesions such as scar tissue, to decrease blood or tissue fluids and to relax muscle tension to optimize fascia, muscle and tendon’s function. Joint mobilization implies active or passive mobilization of joints to increase range of motion, reduce stiffness and pain. This technique implies small oscillating and gliding movements perpendicular or parallel to joint axis.
Thermal Therapy
Thermal therapy is perhaps the most used type of physical therapy and the easiest to apply. It varies from cold to heat therapy. Their use is determined by the time elapsed after injury and by the desired objective. The range of thermal modalities is so wide that it may vary from the application of cold water, to cryotherapy applied with compression boots, to hot pads, or even therapeutic ultrasound [60].
Cold Therapy
Cold therapy should be applied in the first 24-48 hours after injury. After this it can be performed in alternance with hot therapy until 72h. The main benefits of cold therapy are decrease of local circulation, tissue swelling and pain. Reduced blood flow will decrease haemorrhage, and extravasation of inflammatory cells. It will also reduce tissue metabolism and enzymatic activity, inhibiting some of the effects of inflammatory mediators, reduce cellular oxygen demands, and decrease subsequent hypoxic injury. Cold therapy also provides an analgesic effect by decreasing nerve conduction velocity. These benefits are more effective immediately after injury or surgery. After a minimum of 15 minutes of cold/ice therapy, tissue temperature decreases 10-15ºC, average time of cold therapy is 20-30 minutes [61,62]. Treatments shall be repeated every 2-4h during the first 48h. There are different methods of applying cold therapy—ice water immersion, ice packs, ice bandages, and cryotherapy. Cryotherapy decreases skin temperature to 4ºC and is a prohibitive treatment at FEI events in and five days prior to the event due to its analgesics and anti-inflammatory effects. Cold therapy can be administered by directing a cold-water hose onto the specific target site. While this approach is practical, it may not be as effective in reducing tissue temperatures compared to immersion in ice water. However, the physical pressure exerted can still be beneficial in addressing oedema and promoting the debridement of wounds [60].
The main advantages of this technique include its simplicity of use and ready availability, relatively low cost (except for spas and baths), effectiveness in acute cases, and multiple effects such as analgesia, restricted blood flow, and reduced tissue metabolism and activity of inflammatory enzymes.
Heat Therapy
Heat therapy is used from 72h after injury as it increases the metabolic activity in cells, which leads to induced capillary dilation. This increased blood supply leads to increased supplementation of oxygen and nutrition into the area, and enhances removal of cellular waste products, such as prostaglandins, decreasing nerve fibre sensitization and pain.
Heating prior to exercise is a good procedure as it improves the flexibility of structures such as soft tissue contractures, fibrosis or scarring around joints, making physical work more comfortable. Heating of dense connective tissues increases extensibility and flexibility, due to effects on collagen molecular bonding. Heating and stretching of tissues around joints over a period of time can increase the range of joint movement. Heat also has effects in muscle spasms as it will relax muscles and decrease spasms. In wounds it will also increase the healing response and improves oedema resorption. An increment of 2–4°C is required to produce these effects [63]. It is contraindicated in cases with infection or neoplasia, where there is haemorrhage, altered skin sensitivity, burns, circulatory problems, or acute inflammation.
Kynesiotape and Bandage
Kynesiotape is an adhesive tape made of cotton with an elasticity of 130%–140% of its neutral state [64]. Kynesiotaping (KT) is a technique consisting of the application of an elastic tape to the skin, capable of acting on its mechanoreceptors to generate analgesic, muscular and circulatory effects. These effects depend on the way the tape is attached to the skin. The elevation of the tissue triggered by the taping (convolutions) decreases the pressure on the nociceptors and increases blood circulation, providing analgesia [65].
The goal is to enhance the activity of mechanoreceptors and proprioceptive receptors within the skin, fascia, ligaments, and joints. The equine skin boasts a significant presence of sensory nerves and receptors intricately linked to hair follicles, characterized by a thinner epidermis compared to human skin. The application of tape is intended to coordinate the interplay between neural and muscular activity, ultimately achieving the modulation or alteration of locomotion and/or range of motion. There is lack of studies in literature confirming the efficacy of kynesiotape in horses. Nevertheless, in one study it did not show any significant effect of kynesiotape in range of motion in extension-flexion or stabilization of the back of the trotting horse [64]. Another one demonstrated that the use of therapeutic bandages resulted in a significant reduction in postoperative swelling of tibio-patellofemoral arthroscopy in horses compared with control group [66]. And another one demonstrated KT led to short term analgesia [65].
Therapeutic Exercise
Controlled exercise stands as a fundamental and crucial component of every rehabilitation program, complementing and enhancing the regenerative process. To implement an optimal exercise regimen, an accurate diagnosis of the injury type, severity, and periodic reassessments of the lesion and lameness grade are essential [67]. Occasionally, horses may contend with multiple injuries simultaneously; for example, a diagnosed sesamoid fracture might coincide with desmitis of a collateral branch of the SL. Both injuries necessitate precise diagnosis to inform the design of an effective controlled exercise program. The program typically initiates with complete rest, followed by stall rest, and involves a gradual and systematic escalation in exercise intensity [68].
Regarding soft tissue injuries, hand walking should start very soon after injury to promote optimal fibre alignment and prevent restrictive adhesions. Exercise is started hand walking 5-10 minutes once or twice a day, depending on lesion gravity. Ultrasound and lameness evaluation should be made periodically, every 4-6 weeks and exercise level may be increased as improvement is achieved—Table 1 [60]. If ultrasound image deteriorates or lameness grade increases, the exercise plan shall be reevaluated. Controlled exercise alone resulted in successful outcomes for 67% to 71% of horses with soft tissue injuries [69].
Maturation of tendon and ligament fibres depends on mechanical loading. After the inflammatory phase of healing, controlled stretching is recommended in order to increase collagen synthesis and improve fibre alignment, resulting in higher tensile strength [70]. These effects are explained by an increase of content of collagen and extracellular matrix (ECM) produced by tenocytes [22]. The promotion of appropriate orientation and remodelling of collagen into mature, strong, and optimized tissue is ensured by mechanical stress. Controlled exercise during the chronic remodelling phase provides this conversion and improves the mechanical properties of the healed tendon. The quality of the longitudinal fibre pattern has been linked to prognosis for return to work. Collagen that remains unstressed during the proliferative and remodelling phases remains randomly organized and is weaker than stressed collagen. A prolonged immobilization leads to a tendon with reduced content on water and proteoglycan, as well as, to weaker and random organized collagen fibres with lower tensile strength and failure at lower strains [71]. It also results in tendon atrophy due to lower vascularization and metabolic rate.
Clinical studies have shown the benefit of early mobilization following tendon repair and the fact that training has improved tensile strength, elastic stiffness, weight and cross-sectional area of tendons [22,24].
Concerning articular cartilage, slowly progressive physical exercise causes significant adaptive changes, there is enlargement of the cells and nuclei of chondrocytes and increasement of proteoglycan content and cartilage thickness. Nevertheless, if the exercise is strenuous or misconducted it may lead to a cartilage degeneration process. The same happens with bone, as bone tissue adapts to weight-bearing and muscular workout by increasing bone mass and density, through osteoblast stimulation. This remodelling cycle is slow, taking several months to occur and the achieved bone mass also depends on genetic, nutritional and hormonal factors. Immobilization causes the reverse effect on bone tissue, leading, ultimately, to osteoporosis [70]. Table 2 presents a suggestion for controlled exercise program for bone injuries. An ideal program is based on individual patient and lesion specificities and requires periodic controlled veterinary check-ups [68].
Water Exercise—Hydrotherapy
The most renowned modalities of exercise in water for horses are swimming pools (complete flotation), and water treadmills (WT) (semi flotation) [72].
Marked locomotor differences exist between swimming and exercise on a WT. Usually, when swimming, horses stop forelimbs movement presenting only hindlimbs movements. From the rehabilitation point of view, it is interesting and important. They use their forelimbs to maintain balance and hindlimbs for propulsion. Extreme range of motion (ROM) though the hip, stifle, and hock joints are observed in horses during swimming. Moreover, horses adopt a lordotic posture with cervical thoracolumbar and pelvic extension, so caution is recommended when using swimming in horses with thoracolumbar, sacroiliac, hip, stifle, or hock injuries [72]. On WT, as water depth increases, buoyancy increases, impact shock reduces, hydrostatic pressure on the limbs increases, all of which have potential benefits for the rehabilitation of certain conditions [73]. Additionally, drag increases which has the potential to limit limb protraction, alter muscle use and change stride pattern [73]. A WT exercise session is equivalent to a challenging ground schooling session [73].
Water exercise presents a wide range of advantages: increases joint mobility and its ROM, promotes normal motor patterns, prevents muscle atrophy, increases muscle activation and strength, increases of soft tissue flexibility, reduces oedema and joint effusion, reduces comorbidities caused secondarily to primary joint pathology, as well, as stress applied to the limb, increases joint range of motion and decreases pain and inflammation [74,75,76]. Limitations of these techniques concern with the fact of non-diagnosed injuries that may be worsted with their overstimulation, presence of skin disease or wounds and with water mistreatment that may lead to cross-infections [77,78]. A good evaluation of each pathology should be done before recommending water exercises to understand if the benefit is real [57]. Regular monitoring of the gait pattern throughout rehabilitation either by therapist/vet or both is recommended.
Electrotherapy
Therapeutic Ultrasound
Therapeutic ultrasound (U/S) is a electric device whose action is based on thermal effects, that may be used for superficial and/or deep heating of tissues. Ultrasound selectively heats tissue with high protein/collagen content. The most intense heating occurs at tissue interfaces such as skin, tendon, and fluid [63,79]. To achieve therapeutic effects, there must be a temperature increase of at least 2°C in tendons [63]. In equine epaxial muscles mean temperature rise after 20 minutes of treatment at 3.3 MHz at 1.5 W/cm2 was 1.3°C at a depth of 1.0 cm, 0.7°C at 4.0 cm, and 0.7°C at 8 cm. However, temperatures in tendons were significantly elevated following 10 minutes of treatment at 3.3 MHz: mean temperature rise was 3.5°C in the SDFT and 2.5°C in the DDFT at the end of the 1.0 W/cm treatment and 5.2°C in the SDFT and 3.0°C in the DDFT at the end of the 1.5-W/cm treatment [79]. The other benefit of therapeutic U/S is that sound waves cause a deep massage of tissues known as cavitation. This massage is caused by expansion and compression of tissues and fluids that enhance tissue healing. For example, fibrous connective tissue scars may be effectively stretched using this technique [63].
This technique is advantageous in articular and tendon disabilities. It addresses joint mobility limitations with the objective of elevating the temperature of connective tissues before engaging in stretching or ROM exercises. Previous observations indicate that warming deep tissue either before or during stretching yields a more pronounced impact on tissue length and reduces the risk of injury compared to stretching in isolation. The joint capsule, rich in collagen, frequently contributes to restricting joint motion. Ultrasound energy is efficiently absorbed by collagenous tissue, augmenting its elastic properties [80].
A study found differences among rates of tissue heating between different tissues. The explanation concerns with the thermal and acoustical properties of the tissue through which the continuous sound waves travelled. The difference in the rate of tissue heating among species is likely the result of the distinct acoustical properties of the tissues based on anatomic location and variation of tissue composition between species [63].
Laser
Laser therapy has been widely used for over 50 years and in equine medicine rehabilitation it is gaining much more attention.
The term LASER is an acronym for Light Amplification by Stimulated Emission of Radiation. It is a device that produces coherent, collimated and monochromatic light through a process of optical amplification. Laser devices have different classifications—I, II, III and IV but only class 3B and IV have therapeutic abilities. Class 3B are therapeutic lasers that have a power output from 5 to 500 mW, and are called low level laser therapy (LLLT). Class IV lasers are therapeutic lasers with a much higher power, above 500mW and are called high intensity laser therapy (HILT) [81]. The use of class IV lasers in FEI competitions is not allowed.
Low-level light therapy generally employs light at red and near-infrared spectral band (390—1100 nm) to modulate biological activity, without generation of heat [82,83]. The therapeutic treatments are based upon three principles; to minimize tissues inflammation, oedema, and chronic disorders of joints by targeting joint [46], to promote healing of superficial and deeper tissues, tendons and ligaments due to stimulation of fibroblastic activity and proliferation [47,48,49], and to treat neurological disorders and pain reduction [84]. On the other hand, the class IV laser differs from the class 3B due to the formation of heat. The temperature rising increases the intensity of metabolic processes in cells [27].
Nowadays, many studies reflect the therapeutic benefits of class LLLT and HILT in tendonitis/desmitis treatment and OA amelioration.
Several studies showed that high power laser therapy alone can effectively be applied to treat various musculoskeletal disorders [85,86,87,88,89]. LLLT facilitates tendon healing through various histological, physiological, and biomechanical effects in animal models [90]. It was demonstrated that LLLT has a significant effect on tendon repair by activating cytochrome C oxidase, by acting in all the three phases of tendon repair, and finally improving tendon recovery. The repair mechanisms of LLLT are different in the three phases of tendon repair. In the inflammatory phase, LLLT mainly activates vascular endothelial growth factor (VEGF) and promotes angiogenesis under hypoxia. During the proliferation phase, LLLT increases the amount of collagen type III by promoting the proliferation of fibroblasts. Throughout the remodelling phase, LLLT mainly activates M2 macrophages and downregulates inflammatory factors, thus reducing inflammatory responses. However, it should also be noted that in the final phase of tendon repair, the use of LLLT causes excessive upregulation of some growth factors, which might lead to tendon fibrosis [87].
LLLT therapeutic efficacy has also been evidenced in joints and articular cartilage being demonstrated that it presents anti-inflammatory effects and promotes a fast recuperation and regeneration of the articular cartilage [91]. Multiple studies conducted both in vivo and in vitro, have shown that the effect of laser treatment increased the bone regeneration process only in the first weeks after the fracture (2/4 weeks), while after about 60 days there was no advantage observed over controls, indicating that LLLT is effective only in the early stages of the process [89]. LLLT is a safe and non-invasive method which has recently attracted the attention of many researchers interested in modalities for treatment of knee OA being recommended as a physical agent to be used concomitantly at rehabilitation programs [88,92].
Regarding on HILT effects, it presents the same as LLLT and presents photothermal effects on soft tissues, increasing a mean of 3ºC skin surface, increasing vascularization, when applied in horses [28]. On tendon and ligament injuries it was demonstrated it reduced pain, swelling, lameness and promoted healing, being recognized as a non-invasive and nonpharmacological way to initially treat clinical signs of tendon and ligament injuries. In ultrasound assessment HILT significantly reduced injury percentage, being therefore useful as a supportive therapy for healing of tendon and ligament injuries in horses[27]. Also, HILT seems to be efficient in reducing pain and providing functional improvements in patients with knee OA [93,94,95].
Patient preparation before applying this therapy is essential to ensure that the skin is clean and free from any materials that could absorb light. Dirt, sand, and dust shall be removed, although washing may be necessary if the animal is particularly dirty or if leg paints, poultices, or ointments have been applied. Ideally, the animal should be dry when applying PBMT, but damp skin has minimal impact on the penetration of photons. Wounds should be cleaned and debrided before Laser application to prevent them from inadvertently absorbing the energy [96].
Safety precautions are paramount when using any laser system. Therapists, handlers, and patients should wear appropriate eye protection before activating the laser. Patient eye protection is simple and effective: a thick black towel or folded piece of black felt can be used [96].
Extracorporeal Shockwave
Extracorporeal shock wave therapy (ESWT) is a well investigated and widely used non-invasive treatment modality for many equine musculoskeletal disorders. Acoustic waves are applied to an injury region and trigger a mechano-transduction cascade. Mechanical energy causes biological effects that lead to an enzymatic response and to up-regulation of angiogenic growth factors (GF), responsible for neovascularization, improvement in blood supply and tissue regeneration, thus improving the healing process [97].
The application of ESWT in chronic tendinopathies stimulates neovascularization, alleviating pain and initiating repair of the chronically inflamed tissues [98]. Its therapeutical value in calcified tendonitis is also largely described [99]. Additionally, ESWT has been shown to improve lameness, decrease time of healing and improves ultrasonographic appearance of tendon and ligament injuries. Optimization of collagen synthesis, maturation, and strength progressively increases tendon tensile strength and hence recovery. These findings account for the gradual and long-term benefits of shock wave therapy in tendinopathy [100].
In knee OA, ESWT demonstrated clinical benefits for pain and physical function improvement. In acute fractures, ESWT treatments enhanced callus formation and induced cortical bone formation. In this cases, the effect of shockwave therapy appeared to be time-dependent [101,102].
Limitations of ESWT are the potential pain and minor haematomas. To overcome these limitations, pretreatment with laser therapy is described, being the results a faster and/or better treatment outcome than ESWT without laser pretreatment. Combining ESWT with laser pretreatment leads to synergistic effects and, thus, is superior to either treatment modality alone [103].
Electromagnetic field
Electromagnetic field therapy operates on the principle of electrical generation of magnetic waves. This therapeutic action can be achieved through high-frequency electromagnetic waves, also known as pulsed diathermy, which induce heat production, increasing temperature in 3-4oC; or by lower-frequency electromagnetic waves, referred as pulsed electromagnetic frequency (PEMF) therapy produces magnetic fields within the tissues without causing heating. For equines there are several devices of PEMF, including blankets, and wraps with coils and energy-generating battery units built into them [104]. There are small and large coil systems that produce magnetic field in different strengths and sizes. Usually, treatment protocols are stablished by the devices manufacturers and are based on frequency of the pulses and the treatment time. It is indicated for bone fractures, non-union fractures and to decrease pain and muscle tension and spasm [104].
Electrostimulation
Electrical current is applied to surface electrodes to produce controlled movement of the skin, muscle, tendon, and associated ligaments. Some of the important advantages of electrotherapy are improved quality of healing and shortened rehabilitation time. Electrotherapy devices can be placed into two categories of sensory nerve or motor nerve stimulators [105].
Transcutaneous electrical nerve stimulation (TENS)
TENS provides pain relief through electrical stimulation in the low-frequency range (<250 Hz) using appropriate pulse durations and intensities to activate the desired nerves. It acts primarily via segmental inhibition through pain gating mechanisms [104]. These rely on activation of larger diameter fibres in peripheral nerves, which in turn helps block nociceptive activity in smaller afferent ones. Secondarily, this stimulation of peripheral nerves can induce a central release of endogenous opiate-like substances, which can have a descending inhibitory effect on pain. Large diameter sensory nerves are firstly activated due to their skin proximity and then motor nerves are activated. Limitations concern with skin irritation. The main indications are pain control in acute and chronic musculoskeletal disorders, oedema and wound healing control [104]. In equines it is mostly described for superficial flexor tendon injuries in order to decrease pain and oedema and epaxial muscle pain [106].
Neural Electrical Muscle Stimulation (NEMS)
Neural electrical muscle devices stimulate motor nerves, producing controlled and visible muscle contractions generated by electrical high intensity impulses, which are directed toward the target muscle through a surface electrode [107]. The main indications are muscle stimulation through α-motor nerve activation and stimulation of de-enervated muscles [104]. Effects, such as, changes in fibre types and physiological factors of equine muscles, muscle strength and hypertrophy, muscle spasm and hypertonicity were described [106].
Vibration plates
The use of vibration platforms in equine rehabilitation is gaining more supporters. The main indication is to be used prior to exercise to mimic a warm-up effect caused by vibration, reducing injuries at exercise [108]. It is theorized, although not substantiated, that vibration platforms cause longer stride lengths, lower lameness scores, and higher heart rates after treatment [109]. However, it appears to have an acute relaxation effect in stalled, healthy horses [109,110]. Further studies need to be performed.
6.1.2. Pharmacologic Conservative Therapies
Anti-Inflammatories
In musculoskeletal disease, anti-inflammatories—NSAIDs and SAIDs—are the most prescribed and used drugs either administered orally (PO) (both), endovenous (IV) (both), intramuscular (IM) (SAIDs) or injected intra-articularly (IA) (SAIDs). They can relieve pain and reduce inflammation through inhibition of proinflammatory prostaglandins production by cyclooxygenase enzymes.
Despite this, as soon as tendonitis or OA are triggered, their histopathology clearly reveals they have a degenerative course instead of inflammatory one [111], therefore anti-inflammatories do not alter the course of the disease, they only relieve symptoms inherent to the pathology [58]. Additionally, these drugs can impair healing by down regulation of cycloxigenase-2 (COX-2) pathway for tendon and bone injuries. This entails a profound understanding of the early inflammatory cascade and how it might affect the treatment [112]. Some evidence suggests that NSAIDs may impair the tenogenic differentiation of the mesenchymal stem cells drawing differentiation toward adipogenic differentiation, negatively influencing the healing process leading to scar tissue formation and impair functional outcomes [58]. Moreover, it must be considered the risk of renal, cardiovascular and gastrointestinal side effects.
Corticosteroids local injections in tendons are not advisable as they may induce tendon fibrosis. Evidence suggests that they are not effective and do not represent any advantage in tendon repair [58,113,114,115].
Regarding the use of intra-articular (IA) SAIDs with OA, they may be associated with moderate improvement in pain and function but with low duration [116]. The beneficial effects of IA SAIDs are rapid in onset, but may be relatively short lived (approximately one to three weeks) [117].
The use of anti-inflammatories must be very well balanced because if in one hand aberrant cellular activity in the inflammatory phase often results in impaired tissue healing and defective host responses, with over-fibrosis and scarring, on the other hand, inflammation is part of the regenerative process and recruits a number of immune cell subtypes that impact on tissue healing processes [118]. Thus, in acute stages of inflammation they might be considered in a short-term use (3-5 days) but their long-term use is not recommended as inflammation is critical for normal tissue repair, aiding debris clearance and signalling tissue repair [119].
Hyaluronic Acid (HyA)
HyA is a non-sulphated glycosaminoglycan (GAGs) and is clinically used for the treatment of equine acute tendonitis and OA [120,121,122,123,124]. There are several commercial products licensed for injectable use in equine medicine such as Legend® (Boehringer Ingelheim Animal Health USA Inc), Adequan® (American Regent, Inc., animal health, USA), Zycosan® (Dechra, USA), Hyalovet® 20 (Boehringer Ingelheim, Italia) HY-50® (Dechra, EU), Hyonate 10mg/mL (Boehringer Ingelheim, Germany), Gel-50® (Equimed, USA).
HyA presents anti-inflammatory and lubricative effects, improving organ function [125,126]. Effects of HyA on pain have been already specifically analysed in intra-articular injections in OA [127] and confirmed to be effective on functional improvement even in subjects suffering from tendinopathies [126]. HyA permits tendon gliding, reduces adhesions, creates better tendon architectural organisation and limits inflammation [124].
Wound healing and immunosuppressive properties have also been reported in in vitro and in vivo studies [120,125]. Its beneficial action to the repair process is stronger after acute tendonitis and should be used soon after injury.
HyA has been used as an alternative treatment for equine OA for more than 50 years and is still considered a safe, cost-effective therapeutic for helping lower the side effects of OA and is frequently used in clinical routine. HyA provides lubrication to the joints, increasing its chondroprotective effects secondary to an inhibition of the production of nitric oxide, a mediator that enhances cartilage degeneration and chondrocyte death. HyA treatment also limits the progression of OA lesions by stabilizing proteoglycan structure, limiting the enzymatic breakdown associated with degenerative arthritis [128]. HyA improves the viscosity of synovial fluid, helping its physiological function acting as a buffer and stabilizer of lubrication, acting as an anti-inflammatory and analgesic due to increased joint lubrication, resulting in decreased pain in unstable joints [129]. Treatment can be done IA, IV or PO, being the IA more effective. A rest period (12h-24h) is advised after IA treatment [123,130]. The higher the molecular-weight hyaluronic acid, the more efficacious the treatment of OA [121]. Higher molecular weight HyA may provide superior chondroprotective, proteoglycan/glycosaminoglycan synthesis, anti-inflammatory, mechanical and analgesic effects [131].
The first experimental study using HyA in horses with osteoarthritis was conducted in the seventies, and it was concluded that IA injection of HyA and SAIDs improved performance of race horses with traumatic arthritis [132]. Since then, this association has been done until the present. Studies revealed that there is no scientific evidence that hyaluronic acid combined or not with anti-inflammatory drugs is effective in the long run and that the association with SAIDs is more effective reducing lameness than HyA itself [129].
Lately, the development of alternative treatments to the classic “HyA and Corticoids”, such as platelet rich plasma (PRPs), created the need of comparing treatment effectiveness of these treatment options. Comparing the effectiveness of HyA with PRPs is consensual assuming PRPs are more effective reducing long-term pain and lameness in OA’s treatment and improving joint function. Several studies demonstrated that PRPs in combination with HyA are more effective reducing pain than PRPs or HyA alone [133,134,135,136].
New products that alter the composition of the HyA molecule are continuously being developed, as well as combinations with other drugs to enhance their effects. HyA holds significant potential both as a therapeutic agent on its own and as a scaffold when combined with other therapeutic molecules, and it remains the focus of ongoing research. Nowadays the association of HyA with mesenchymal stem/stromal cells (MSCs) is being largely studied for the treatment of cartilage repair using HyA as scaffolds for MSCs implantation [122,137,138,139,140,141].
Polyacrylamide Hydrogel
Polyacrylamide hydrogel (PHyd) is licensed to equine medicine under the brands of Arthramid® Vet (Polyacrylamide hydrogel 2.5%, Revatis Europe) and Noltrex® vet (Polyacrilamide hydrogel 4%, Bioform, USA).
PHyd appeared more recently than HyA and is a 100% synthetic product, non-soluble and acts essentially as a substitute for synovial fluid, increasing joint lubrication and consequently joint pain/inflammation, improving joint function. In an in vivo study with rabbits it was possible to detect the presence of hydrogel in joint cartilage space at day 60 after one single dose treatment [142]. The efficacy of PHyd can be explained possibly because its molecular weight is three times greater than HyA, thus preventing the degenerative process caused by the inflammatory cytokines present in the synovial fluid of the joints [143].
Intra-articular administration route is more efficient than IV or PO, is effective reducing lameness caused by OA in horses and has a long period of action enabling their physical activities and increasing horses’ welfare [129].
In a recent study it was demonstrated that intra-articular 2.5% PHyd is highly effective (82.5% free of lameness horses at 2-year follow-up), lasting and safe for the treatment of equine OA. No other medical treatment had proven such prolonged efficacy. These studies enhanced the belief that hydrogel exerts its effects through the integration in synovial membrane, increasing joint elasticity and viscosupplementation, protecting articular surfaces and preventing pro-inflammatory cytokines to exert their effects potentiating OA [143,144]. These studies also suggest absence of intra-articular neurotoxic effects or fibrosis [144].
All these studies support the application of polyacrylamide hydrogel in reducing lameness caused by OA in horses due to its long-lasting viscoelastic supplementation. Its association with other therapies such as PRPs or stem cells could be beneficial.
Bisphosphonates: Tiludronate and Clodronate
Bisphosphonates are widely used in both human and equine medicine due to its ability of reducing bone resorption, inhibiting osteoclastic activity. In equine medicine, tiludronate was the first bisphosphonate being approved. It acts mainly as an antiresorptive drug, reducing the ability of the osteoclasts to degrade bone matrix, although anti-inflammatory and analgesic properties mediated by other mechanisms are also recognized [145,146]. Tiludronate disodium (Tildren®, Ceva Animal Health LLC, Lenexa, KS, USA) and clodronate disodium (Osphos®, Dechra, Ltd., Staffordshire, UK) are the bisphosphonates drugs that are licensed for use in horses. These two are non-nitrogen containing bisphosphonates that reduce osteoclastic bone resorption by causing osteoclast apoptosis [147].
At the beginning it was mainly used in navicular syndrome and bone spavin. Nowadays it is also used in thoracolumbar spine OA as well as to prevent osteopenia in long term immobilizations [148]. Tiludronate had efficacy in the treatment of horses with signs of pain induced by osteoarticular lesions of the thoracolumbar vertebral column, causing a significant improvement in dorsal flexibility, thus becoming a treatment option for the management of horses with intervertebral lesions and the associated pain [9 [149].
In navicular syndrome, horses treated with 1mg/Kg administered via IV injections, daily over 10 days for the treatment of navicular disease. showed optimal improvement of lameness and return to normal level of activity 2–6 months post treatment [150]. Several studies have proven bisphosphonates effectivity in improving lameness associated with navicular syndrome [151,152,153].
Tiludronate has proven to be effective in bone spavin medical treatment, in association with a controlled exercise programme, by reducing lameness score and improving radiological images [154,155,156].
A study conducted in race horses with fetlock traumatic osteoarticular lesions, compared the therapeutical effects of IA treatment with triamcinolone acetonide and hyaluronic acid, polysulfated glycosaminoglycan (PSAG), interleukin-1 receptor antagonist protein (IRAP) and IV treatment of tiludronate diluted in 500mL of saline solution. Despite both decreased inflammatory process and cartilage degeneration after treatment, tiludronate patients presented a decrease in radiographic score, meaning it inhibited the radiographic progression of OA in fetlocks at 6 months after treatment by inhibiting subchondral bone remodelling [157]. The radiographic scoring systems adopted in equine clinical and experimental studies are mainly based on the number and size of osteophytes and periarticular enthesophytes at the capsular insertion of the joint, as an index of local inflammation. It was also highlighted the advantage of using tiludronate in young horses to control subchondral bone pain in the initial stages of OA, because it causes an acidic environment near the osteoclasts, inhibiting free nerve endings activation [157]. It is consensual, bisphosphonates have analgesic effects [148,149,151,157,158,159,160,161,162,163] and are considered a “controlled medication” by FEI Equine anti-doping and controlled medication rules. “Controlled substances” are substances that are deemed by the FEI to have therapeutic value and/or be commonly used in equine medicine but have the potential to affect performance and/or be a welfare risk to the horse horses cannot compete under its action. It has a detection time on blood or urine of 28 days (vid “FEI List of detection time”). A detection time is an approximate period of time for which a drug (or its metabolite) remains in a horse’s system, such that it can be detected by the laboratory and is provided only as a guide.
Despite limited data available on its secondary effects, current literature suggests good tolerance of tiludronate, being discomfort or colic [148,164,165] and renal damage [162] the most frequent side effects.
Although bisphosphonates label use is on horses older than 4 years old, in race horses it’s off label use in younger horses, generates concerns regarding impairment of normal physiological functions (growth, bone repair, and bone remodelling) [159], that might cause detrimental, even catastrophic, musculoskeletal injuries [166]. Additional research must focus on identifying the short-term and long-term effects of bisphosphonates in young and exercising animals to ensure the efficacious and judicious use of this powerful, long-lasting group of drugs [158].
The perspective of the use of bisphosphonates in horses, seems bright and growing as its advantages in osteoclast activity are consolidated. Nevertheless, its usage must be controlled and properly performed.
6.1.3. Conservative Surgical Techniques
Tendon Splitting
Tendon splitting is a surgical technique performed in acute and chronic tendonitis that has been described for equine tendonitis treatment since the early 70′s.
In acute tendonitis, there is collagen fibre damage and an increase in the cross-section area of the tendon due to intratendinous haemorrhage and inflammatory fluid accumulation within the lesion. In this type of lesion, the objective of this technique is to alleviate pressure from the core lesion, as fluid accumulation within the epitendon and paratendon produce “compartment syndrome”, increasing pressure in the lesion and therefore reducing perfusion capacity, causing a slow resolution of inflammation and healing. This decompression of the core lesion, allows evacuation of accumulated inflammatory fluid and promotes vascular ingrowth within the lesion.
In chronic lesions the procedure is similar but the objective is to increase vascularization of the scar lesion, to promote healing and increase tissue elasticity through the same technique.
Tendon splitting can be done blindly but ultrasound guided is recommended to avoid damage of healthy tendon fibres and other structures other than the injured ones. Briefly, after trichotomy of the area and aseptically preparation of the limb, patient sedation and a high four-point regional nerve block are performed. Ultrasound probe is covered with sterile lubricant and a sterile sleeve and allows tendon visualization.
The stab incision or splitting begins at the most distal aspect of the core lesion to avoid blood contamination of the next stab incision. A #11 scalpel blade is inserted into the medial or lateral surface of the tendon, perpendicular to the ultrasound probe, being its entry and location observed by U/S. The blade is advanced until the lesion, avoiding normal fibres and then is rotated in upward and downward movements, parallel to the long axis of the tendon. The blade is removed and subsequent stab incisions are made as needed to split the entire length of the core lesion [26].
Although this technique was more described in the 70′s, 80’s and 90′s [27], nowadays it is still used and was referenced in a recent studies describing the treatment of SL branches with stem cells in race horses, were percutaneous splitting of the ligament was performed in lesions with cross-sectional area (CSA) grade III and IV in order to evacuate the inflammatory fluid within the core lesion, to reduce oedema and enhance revascularization as the reduction in intra-tendinous swelling through the creation of a communication between the core lesion and peritendinous/ligamentar tissue, improves circulation, reducing repair size and enhancing tissue repair organization [27,28]. Splitting the ligament in the higher CSA grades—III and IV—was correlated with a beneficial input treating these lesions but more studies need to be performed.
Classification of CSA in percentage estimates lesion area, meaning grade 0: 0%; grade 1, lesion is inferior to 25%; grade 2, lesion represents 25 to 50%; grade 3 lesion represents 50 to 75% and grade 4, lesion is superior to 75% of the cross-sectional area [29].
6.2. Regenerative Therapies
Regenerative medicine’s main goal is to replace or regenerate cells and tissues, in order to restore normal structure and function of the injured tissue or organ [167,168].
In contemporary equine orthopaedic medicine, there is a growing interest in various regenerative therapeutic approaches, with a notable focus on hemoderivative therapies and stem cell-based therapies. These treatments have gained prominence due to their demonstrated anti-inflammatory effects, immunomodulatory/paracrine properties, regenerative potential, and high tolerability [169].
Hemoderivative therapeutics include PRP [135,170,171,172,173], ACS [174,175,176,177,178], APS [179,180] and α2M [181,182].
Mesenchymal Stromal/Stem cell-based therapies include cell-based and cell-free therapies. Cell-based therapies resort to use of stem cells themselves, these are multipotent cells that can be harvested from various tissues. MSCs have the potential to differentiate into different cell types and exert immunomodulatory effects, making them valuable for tissue regeneration. Cell-free therapies rely on cells secreted factors such as cytokines, chemokines, GF, extracellular vesicles (EVs) and exosomes which present many biological activities as well as therapeutic potential in several organ system and disease contexts. Currently, for equine, it is only commercially available MSCs cell-based therapies under the name of Arti-cell® forte (Boehringer Ingelheim Vetmedica GmbH, Germany), Horstem® (Equicord, Spain), and Vet-stem is a laboratory that prepares stem cells from adipose tissue and sells the autologous stem cell product.
The interest in these regenerative approaches stems from their ability to address musculoskeletal injuries at a cellular level, providing a more integrated and potentially more effective treatment strategy. As research in equine regenerative medicine continues to advance, these therapies hold promise for enhancing the overall well-being and performance of horses in diverse disciplines.
6.2.1. Hemoderivatives
Hemoderivatives present anti-inflammatory and healing effects, being used in muscle, tendon, ligament and joint injuries such as strain injuries, tendonitis, desmitis, osteoarthritis, cartilage injury and synovitis [182]. They also enable healing and restoration of function in acute and chronic injuries.
In cases of OA treatment, they represent an advantage when compared with traditional intra-articular treatments (HyA + SAIDs), that are only palliative for pain and inflammation control [183], as they improve clinical signs and appear to be chondrogenic and promote chondrocyte homeostasis [183,184,185]. In cases of tendonitis/desmitis they also present therapeutic effects, enhancing healing and leading to the formation of a functional tissue without scar formation [186,187].
The common principle across hemoderivatives, including PRP, ACS, and APS, lies in harnessing the regenerative potential of platelets and their associated bioactive substances to modulate inflammation, support tissue repair, and facilitate healing processes. Each of these approaches offers a personalized autologous solution, utilizing the horse’s own blood components to enhance musculoskeletal health. It is advisable that no NSAIDs treatments have been done 1-5 days prior to these hemoderivatives preparation [182].
PRP
PRP primarily leverages the therapeutic properties of platelets, which play a crucial role in the natural healing response to injury. When tissue damage occurs, platelets become activated and initiate the clotting process, leading to the release of various bioactive substances. The key components released by α granules of the activated platelets include cytokines, growth factors (GF), chemokines such as platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), and insulin-like growth factor (IGF). These substances are instrumental in modulating the inflammatory response, attracting immune cells to the site of injury. Platelets also contribute to angiogenesis, the formation of new blood vessels, by releasing factors that stimulate the growth and migration of endothelial cells. This process is crucial for supplying oxygen and nutrients to the healing tissue. PRP has garnered significant attention in both equine and human medicine owing to its remarkable ability to stimulate the proliferation and migration of fibroblasts, facilitate collagen synthesis, and induce chemotaxis of macrophages. These cellular processes are crucial for promoting cellular proliferation, tissue healing, and regeneration. PRP finds extensive application in treating musculoskeletal tissue lesions, particularly osteoarthritis (OA) and tendonitis/desmitis, due to its well-established anti-inflammatory and anabolic effects. The proven beneficial effects of PRP underscore its role as a valuable therapeutic tool in promoting tissue repair and regeneration in conditions involving the musculoskeletal system [188,189].
PRP is produced through a centrifugation process of whole blood, during which red blood cells and buffy coat are separated from plasma. Platelets are then aspirated, and a subsequent centrifugation concentrates the platelets in plasma. Platelets release the bioactive factors after degranulation of alpha granules in the platelet cytoplasm, which occur upon activation with citrate [190]. Most GFs are released within 1 hour of platelet activation and their half-life usually ranges from minutes to hours. This is a simple process that takes approximately 15 minutes to prepare, being a portable centrifuge the main device to be used, being easy to do in ambulatory clinic.
PRP can be obtained through commercial kits for horses: Restigen PRP® (Zoetis, United States); ACP® (Arthrex, USA) ACP MAX® (Arthrex, USA) and Angel PRP® (Arthrex, USA) or through manual procedures. Although it is described three different manual protocols, in equine practice the most used protocol involves two centrifugations to concentrate platelets in a small volume of plasma (e.g., 2–5 mL) for injection in tendons or intra-articular treatment [191]. PRP can be stored for up to 7 days in a cooled storage, however 24 hours is the ideal time of storing at 5oC because it was demonstrated platelet counting and viability did not change in this conditions [192]. When using a commercial kit, PRP can be aseptically and stably prepared with a consistent platelet content, however, the total platelet count is slightly lower than when using double-centrifugation methods [170].
The platelet content of PRP is affected by several factors, such as the breed and age of the horse, AI’s administration, anticoagulants, blood sampling, and the technical skills of the clinician [193,194]. Depending on the PRP preparation protocol, the cellular and cytokine compositions can vary, being such variability a main clinical concern once it can potentially influence on PRPs therapeutic effects [195,196]. Nevertheless, all of them present higher levels of TGF-β1, VEGF and PDGF [170,197].
To sum up, PRP provides a growth factor concentrate that enhances cellular repair of musculoskeletal lesions [189,196]. Other advantages of PRP as a regenerative therapy are its autologous nature, rapid preparation, and non-invasive collection process.
ACS
ACS presents its therapeutic effect based on the increase of Interleukin -1 receptor antagonist (IL-1ra) concentration, being therefore known as interleukin receptor antagonist protein (IRAP). It also presents high concentrations of anti-inflammatory interleukins 4, 10 and 1 (IL-4, IL-10, and IL-1), and growth factors including IGF-1, PDGF, and TGF-β in autologous serum [108,109].
In equine medicine, there are commercial kits for the preparation of ACS: Orthokine® vet IRAP (Dechra, USA) and IRAP Pro EAS® (Arthrex, USA)- which is a natural anti-inflammatory product used for treatment of OA. They have different preparation protocols but basically it consists of whole blood incubation in a syringe containing borosilicate medical glass beads. The blood is then centrifuged to obtain an IL-1ra—enhanced serum product which can then be injected intra-articularly or intra-lesionally. This product may be applied in joint, muscle and tendons/ligaments injuries.
The role of IRAP is very important in OA control as research in molecular biology discovered the major inducer of OA was the general inflammatory cytokine interleukin-1β (IL-1), which plays a key role in accelerating tissue destruction and the repair mechanisms, being one of the major mediators responsible for the pathogenesis of OA as it activates an inflammatory response leading to cartilage degradation and bone resorption. The proposed mechanism of ACS action is through the blockade of IL-1 receptors, inhibiting IL-1 action, preventing detrimental effects of IL-1β on articular tissues in OA pathophysiology [198,199].
Recent studies also refer the important contribution of other cytokines such as TGF-β, VEGF and IGF-1 that would positively influence treatment response as potent anti-inflammatories and cartilage catabolics [174,184]. IGF-1 is responsible for the stimulation of the production of cartilage matrix components—matrix aggrecan and collagen synthesis—being this profile, another major benefit to add to higher levels of IL-1Ra [200,201].
In tendons, it is demonstrated that ACS treatment causes early significant reduction of lameness and leads to temporary improvement of ultrasonographic parameters of repair tissue, as well as, a positive effect on the histopathological and biomechanical healing [175,202].
APS
APS is an orthobiologic that resorts its action through a combination of cytokines, growth factors and anti-inflammatory agents, being also its main characteristic, the high concentration of IL-1ra. APS is prepared through an available commercial kit—Prostride (Zoetis, USA) and the process involves the collection of the horse’s own blood which is processed with the commercial kit intended to stimulate white blood cells (WBC) to produce anti-inflammatory cytokines concentrating its content in a smaller volume of plasma. This product concentrates IL-1ra 5,8 times more than in plasma, creating a positive ratio of IL1Ra:IL-1β [184,203]. It is reported to include significantly greater concentrations of IL-1RA, IGF-1, TGF-β, IL-10, and growth factors such as epidermal growth factor and PDGF, compared with PRP alone [182].
Its preparation takes 20 minutes and then, the prepared solution is injected directly into the affected joint or tissue. APS can be prepared using a portable centrifugation equipment and is a very simple, quick and non-invasive technique. The intra-lesional injections can be performed in a single treatment in an ambulatory-based practice [184,203].
APS contains a higher concentration of platelets and therefore has its associated benefits previously described, being particularly valued for its elevated levels of growth factors, such as platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), and others.
It is designed to reduce inflammation, relieve pain, regenerate tissue, promote angiogenesis, and cell proliferation capitalizing the horse’s own biological resources to enhance the healing processes, making it a personalized and potentially effective treatment.
In horses with naturally occurring OA, APS significantly improved lameness, pain-in-flexion, gait analysis and range of motion up to 14 days after treatment compared with baseline and controls. In equine joint fluid, there was a significant decrease in protein concentration in treated horses compared to untreated controls [203].
In tendons, it has beneficial effects as an anti-inflammatory and promotes tendon healing [204].
Essentially, the effects of ACS and APS are very similar because they are characterized by higher concentrations of IL-1ra. Nevertheless, literature presents some dissimilarities regarding other cytokines, GF and anti-inflammatory profiles, directing some effectiveness variations to these differences [184]. At this point, there is insufficient evidence-based research to support superiority of APS compared with ACS [184]. However, in the treatment of articular injuries, equine clinicians use more IRAP® and Prostride® although there is nothing that proves they are more efficacious than PRP in this type of pathologies [205,206].
α2M
α2M is a broad-spectrum proteinase inhibitor, present in vertebrate’s plasma, as it binds to proteinases that induce chronic inflammation, especially proteinases released by granulocytes and other inflammatory cells. It was demonstrated that it can inhibit many cartilage catabolic factors, attenuating post traumatic OA degeneration. Up regulation of cartilage catabolic factors seems to be a key mechanism for cartilage damage. Thus, inhibition of these molecules will prevent disease progression [207].
α2M is naturally present in high levels in plasma and in low levels synovial fluid (SF). It is produced by the liver—being released to plasma—and by chondrocytes and sinoviocytes—being released in SF. In inflammatory events, such as OA, α2M synovial levels do not significantly increase due to its high molecular weight, it does not pass from plasma to SF, being unable to inhibit severe intra-articular inflammation. Having this in mind, several therapies have been developed to administer α2M intra-articularly. It has been proved that this treatment could inhibit inflammation, delay articular cartilage degeneration and bone resorption mediated by the inhibition of catabolic enzymes [207,208,209]. It was also demonstrated that α2M enhanced cartilage matrix, ie, collagen type II and aggrecan synthesis. This fact suggests that α2M may have cartilage repair functions or facilitate the synthesis of cartilage matrix [209]. It was also suggested that early administration of α2M may provide cartilage protection by reducing the presence of local catabolic enzymes [209]. In chondrocyte culture, concentrated α2M serum was found to promote chondrocyte proliferation and reduce apoptosis and catabolic gene expression [145].
Nowadays, to create α2M therapeutic levels within the joint, it was created a process that isolates and concentrates α2M from a blood sample. This process was developed and is commercialized as a system—Alpha2EQ® (Astaria Global, USA). Alfa2EQ® isolates A2M from the horse’s own blood through an alpha active filtration technology allowing its use as a potent biological anti-inflammatory molecule—α2M—to address equine lameness, joint inflammation, and soft tissue injury.
To sum up, hemoderivatives represent a new class of regenerative autologous medicinal therapeutics that are evolving rapidly due to their demonstrated efficacy and reduced adverse reactions compared to traditional therapies [210,211]. The production of PRP, ACS and APS involves the collection of the horse’s own blood, followed by centrifugation and serum collection. In ACS and APS process, a step of incubation before centrifugation is also present. They all exert their actions based on bioactive factors released by platelets, with anti-inflammatory, modulation and regenerative actions and present different concentration of specific bioactive factors. A2M presents a different production mode and is a multifunctional protein with diverse roles in inflammation, protease inhibition, and immune modulation.
Since they are autologous, they have a personalized nature and avoidance of compatibility issues, thus minimizing the risks of adverse reactions.
However, they also present some limitations. Although safe, promising and appealing, its use should always require a good evaluation of the patient and should be done in a thoughtful way, considering that this is an autologous product, encompassing a considerable inter-individual variability of cytokine and growth factor content, being difficult to assure its constancy and homogeneity [174,194,195,212]. Current literature has failed to identify a preparation method where such variability is limited or negligible [177,211,213,214]. Efficacy differences between the various hemoderivatives it’s not possible yet [184,204,211].
6.2.2. Mesenchymal Stromal/Stem Cell Based Therapies
Stem cells are undifferentiated cells that can self-renew and differentiate into cells and tissues with specialized functions. Therefore, nowadays they are on focus for the development of regenerative medicinal therapeutics used to overcome body’s inability to regenerate damaged tissues after acute or chronic insults. They are classified by their source as embryonic (ESC), adult and induced pluripotent stem cells (IPSC) and by their development and differentiation capacity as totipotent, pluripotent and multipotent cells. Totipotent stem cells are present only in a very early embryo during the morula stage and can develop into all embryonic and extra-embryonic tissues. During early embryonic development, ESC develops and may give rise to all tissue cells in the body, except for extra-embryonic tissues and germ cells. With further development, they gradually lose their pluripotency and become multipotent which are characterized by the ability to differentiate into limited types of specific cells, often depending on their germ layer origin [215]. Multipotent stem cells might be hematopoietic stem cells (HSC) or MSC depending on their origin. HSCs can differentiate into different cells of the immune system, erythrocytes, and platelets, and MSCs into cells of bone, cartilage, ligaments, tendons, fat, skin, muscle, neural and connective tissue. Nowadays there are proposals to change the acronym MSC to “Mesenchymal stromal cells” as these critical advocates that they do not represent true stem cells as there is a lack of some stemness markers [216]. More recently, another nomenclature change was proposed to “Medicinal Signalling Cells” as these cells home in into sites of injury or disease due to the profile of secreted cytokines by these tissues being therefore signalling cells with medicinal intents [217]. However, recent studies have demonstrated that MSCs can release prostaglandin E2 (PGE2). The autocrine effect of PGE2 displays a major role in MSCs self-renewal ability and immunomodulation thus generating a cascade of events on MSCs proliferation, a major characteristic of stem cells, demonstrating MSC stemness. [218,219].
The International Society for Cellular Therapy proposed a set of standards to define multipotent mesenchymal stromal cells. First, MSC must be plastic-adherent when maintained in standard culture conditions using tissue culture flasks. Second, ≥95% of the MSC population must express the clusters of differentiation (CD)105, CD73 and CD90, as measured by flow cytometry. Additionally, these cells must lack expression (≤2% positive) of CD45, CD34, CD14 or CD11b, CD79α or CD19 and human leucocyte antigen (HLA) class II. Third, the cells must be able to follow a tridifferentiation into osteoblasts, adipocytes and chondroblasts under standard in vitro differentiating conditions [220].
MSCs exert their function through different paths: homing, that is, migration to the site of injury; differentiation into various cell types that can engraft to the damaged tissue for repair; and secretion of bioactive factors [221]. Initially it was thought that MSCs migrated to injured tissues, got differentiated and replaced the local cells. It is currently known that the immunomodulatory capacity of MSC is its main characteristic. This ability is due to the paracrine effect of MSC, secretion of extracellular vesicles, immunomodulation of apoptosis and mitochondrial transfer [221].
MSC treatments can be categorized as either autologous or allogeneic, each with its own set of advantages and disadvantages. Opting for autologous treatment offers the advantage of reducing the likelihood of immune reactions, given that the MSCs are derived from the same individual receiving the treatment. However, this approach involves a more time-consuming preparation process, including harvesting, processing, and culturing cells from the patient, leading to a delayed treatment onset. Additionally, the individualized production of doses can make autologous treatments more expensive. Furthermore, the patient’s specific characteristics, such as sex, age, and health, may impact the quality and potency of the MSC treatment. On the other hand, allogeneic treatments, while carrying the risk of possible immune reactions, present the benefit of utilizing cells from a young and healthy donor. This allows for large-scale production and storage in a cell bank, making them readily available for the treatment of acute lesions [222].
No significant differences in efficacy have been established between allogeneic and autologous MSCs for the treatment of musculoskeletal injuries in horses. Therefore, it is suggested that allogeneic MSCs may serve as a safe alternative to autologous MSCs [223]. While autologous MSCs are more commonly used in clinical trials for OA in horses, attributed to their perceived low immunogenicity and lower risk of adverse reactions, recent studies in horses and humans have demonstrated the absence of severe adverse events associated with allogeneic MSCs. This evidence supports the safety of administering allogeneic MSCs [222,224,225,226].
Mesenchymal stromal/stem cell therapies
As previously stated, the use of MSC therapy is one of the potential treatments of orthopaedic injuries [3,227,228]. Nowadays there is proof of concept that a variety of tissues have been identified as MSCs sources for tissue regeneration and engineering. Bone marrow-MSCs (BM-MSCs) [229,230,231,232], adipose tissue-MSCs (AT-MSCs) [227,229,233,234], synovial membrane-MSCs (SM-MSCs) [222,224,235,236,237,238], amniotic fluid-derived MSCs (AFS-MSCs) [239,240], umbilical cord Wharton jelly’s -MSCs (UC- MCS) [241,242,243,244], periosteum-MSCs (Po-MSCs) [245,246], dental pulp-MSCs (DP-MSCs) [247,248] and muscle tissue-MSCs (MT-MSCs) [249,250,251] are some of them.
Currently, BM-MSCs, AT-MSCs, SM-MSCs, and UC- MSCs are four of the most widely used types of MSCs in the treatment of musculoskeletal lesions.
Literature refers to tendon/ligament injuries with MSCs as very efficacious, suggesting that SCs can contribute to accelerate and improve the quality of tendon healing [222,224,252,253]. MSC treatment of tendon/ligament injuries improve tissue strength, provides a more favourable type I collagen composition, indicating a beneficial therapeutic response to these cells [254]. There are several clinical studies using BM-MSCs as the therapeutic option for tendon repair, perhaps because it is the most studied tissue source of MSCs [255,256]. Still, a recent study compared them with UC-MSC, in vitro, and concluded UC-MSC surpasses other MSCs in its ability to differentiate into tendon-like lineage cells and establish a well-organized tendon-like matrix. In terms of histological properties, UC-MSC promotes superior regeneration of full-thickness defects when compared to BM- and UCB-MSC [257]. Notwithstanding, studies with AT-MSC advocate this source might be superior regarding their potential to positively influence tendon matrix reorganization and because it’s easier to harvest [258,259].
In equine patients, good results have been achieved resorting to the use of SM-MSCs which improved clinical signs, lesion ultrasonographic image and led to no lesion relapse [222,224]. Regarding cartilage defects, BM-MSCs and AT-MSCs have been widely used for the treatment of OA. However, as synovium and cartilage have the same origin during the development of synovial joints, synovial membrane-derived SM-MSCs are especially suitable for cartilage [260,261]. The implantation of MSCs into these defects have shown great promise in both cartilage and subchondral bone repair [225,262,263,264,265,266]. MSCs can migrate to cartilage defects and promote repair and regeneration [267,268,269,270,271,272].
Each MSCs tissue origin has its own advantages in cartilage regeneration as they have heterogeneous potential concerning with their accessibility, invasion during harvest, immunogenicity, proliferative, chondrogenic and immunomodulatory abilities [262]. However, synovial MSCs have shown a greater chondrogenic ability among other MSCs, suggesting superiority in cartilage repair [273,274,275,276]. They also present greater proliferation and chondrogenic potential than do those from bone marrow, periosteum, fat, and muscle [231,235,268,269,270,275,277]. The fact that synovium cells have a close contact with cartilage suggest they have a close bias toward the production of cartilage, becoming a good candidate to cartilage tissue-engineering [269]. Comparatively with BM-MSCs, SM-MSCs possess a greater colony-forming potential, have a low-density expansion which allows retention of multilineage differentiation capacity and their gene profile matches the chondrocyte and meniscal cell gene profile closer than BM-MSCs [278].
UC-MSC present higher proliferation potential, differentiation and immunogenic abilities from the four most used tissues, previously referred[279]. They also can release trophic factors that make them an excellent candidate for use in the clinical setting to provide cell-based restoration of hyaline-like cartilage. Even in allogeneic administrations, these cells stimulate little or no host immune response and can be stored for long periods while maintaining viability [280]. UC-MSCs also have shown the ability of in vitro induction of the production of glycosaminoglycans and collagen type II [281].
A recent review evidence significant improvement of pain and function as main advantages of MSC-based therapy in the treatment of cartilage repair in knees with OA. MSCs and the derived exosomes have various functions in the treatment of this pathology, such as increase of chondrogenesis, proliferation of chondrocyte, reduction of apoptosis, maintenance of autophagy, regulation of synthesis and catabolism of the ECM, regulation of immune response, inhibition of inflammation, monitoring the mitochondrial dysfunction as MSCs were able to do mitochondrial transfer to senescent chondrocytes, improving activity of mitochondrial respiratory chain enzymes and the content of adenosine triphosphates , as well as the overall paracrine effect [282].
To sum up, MSCs can delay the progression of cartilage degeneration in OA, relieve pain, improve joint function, and prevent chondrocyte apoptosis through a paracrine effect.
In skeletal muscle injuries, treatment with AT-MSCs was pointed out to be the best choice due to their efficient contribution to myoregeneration. The following characteristics were pointed out as differentiating and advantageous points: their high ex vivo expansion potential, and less demanding harvesting than that of BM- or SM-MSCs [283]. Nevertheless, this study refers to autologous treatments.
Overall, the clinical use of MSCs is safe, is an “easy to do” procedure and the treatment administration is not very invasive [226].
Autologous chondrocyte implantation (ACI)
ACI is a novel surgical and regenerative treatment that aims regeneration of full-thickness cartilage defects. Chondrocytes are collected from a less loaded area of the joint, digested and expanded, seeded in a scaffold and then injected in the defect region. At the moment, there are several commercial products available, e.g., Cartilife® (Biosolution, Co., Ltd, Seoul, Korea), MACI® (Vericel Corporation, Sidney, Australia), ChondroCelect® (TiGenix N.V., Belgium), Spherox® (CO.DON AG, Germany), Chondron™ (CELLONTECH Co.,Ltd., Korea), Chondrocytes-T-Ortho-ACI® (Orthocell, Ltd., Australia) and JACC® (Japan Tissue Engineering Co.,Ltd., Japan) [284]. Different tissue sources have been used: cartilage, bone marrow, adipose and umbilical cord tissues to produce chondrocytes. However, the mainly used are autologous bone marrow and cartilage tissues. Recently, there has been a trend shift, a biggest bet has been done in allogeneic and adipose tissues [285]. Although these methods can solve the problem of cartilage regeneration to a certain extent, most of the regenerated tissues are fibrous cartilaginous which is inferior to hyaline cartilage for the intended purposes of load bearing and joint movement. thus, it is difficult to achieve the composition and mechanical properties of natural articular cartilage, and long-term efficacy is not guaranteed [45]. They are relatively successful in relieving pain for the patients, but do not result in regeneration of native tissue [285]. Comparatively with other techniques such as microfracture or osteochondral autograft/mosaicplasty, ACI seems to be an effective tool for cartilage restoration that may be more efficacious and durable than the other cartilage restoration techniques [286]. Thus, new cell-based and tissue engineering approaches are necessary and continue to be evaluated and optimized with the aim of promoting and inducing cartilage regeneration [285].
Mesenchymal stromal/stem cell-free therapies
As previously discussed, the application of MSCs as cell therapy is grounded in their ability to regulate the inflammatory response and promote tissue repair and regeneration. The therapeutic efficacy of MSCs primarily arises from their immunomodulatory function. When exposed to inflammatory stimuli, MSCs secrete a variety of bioactive molecules collectively known as the secretome. The secretome is the collective term for the soluble factors produced by stem cells and employed for their intra and inter-cell communications [287]. These factors are secreted to the extracellular space, which include soluble factors (cytokines, chemokines and GFs) as well as non-soluble factors, extracellular vesicles (EVs) that transport lipids, proteins, ribonucleic acid (RNA) and desoxyribonucleic acid (DNA) subtypes [221,288]—Figure 2.
EVs can be subdivided in apoptotic bodies, microvesicles and exosomes. This commixture activates the resident stem cells and hence mediate the endogenous regeneration. However, the secretome of individual cells and tissues is specific, and changes in response to fluctuations in physiological states or pathological conditions [221].
In laboratory settings where MSCs are cultured under specific and adapted conditions, this secretome contributes to the generation of conditioned medium (CM) [289].
Studies have demonstrated that the application of MSC-conditioned medium (MSC-CM) yields promising results. This specialized medium, enriched with bioactive factors derived from MSC secretion, has shown efficacy in promoting tissue healing and modulating inflammatory processes due to proangiogenic, antiapoptotic, antifibrotic, anti-inflammatory, and immunomodulatory effects [288]. Previous literature reviews have consistently reported positive outcomes associated with the use of MSC-CM, highlighting its potential as a therapeutic intervention [224,225,289,290]. These findings underscore the importance of exploring MSC-derived secretome and conditioned medium as viable treatment options for various inflammatory and tissue injury conditions.
Furthermore, the preservation of the therapeutic action of the parent MSCs stands as an additional advantage as each cell type secrets a specific type of bioactive factors [291]. Beyond the biological benefits and addressing safety concerns associated with the direct application of cells, cell-free therapies offer the potential avoid of immune compatibility, tumorigenicity and transmission of infectious diseases potentially related with stem cell therapy, as well as several logistical advantages for clinical implementation [287]. These include scalability, ensuring a sufficient supply, and longer shelf-lives [288]. This shift towards cell-free therapies not only enhances safety considerations but also streamlines the practical aspects of treatment, making it more accessible, scalable, and feasible for clinical applications.
Certain limitations associated with these treatments pertain to the standardization of MSC. These include factors such as the age and tissue source of the MSC donor, the duration of MSC preconditioning, the choice of nutritional medium for preculture, the oxygen tension within the culture environment, and the specific preconditioning factors applied [289]. The variability in these factors can influence the characteristics and effectiveness of MSC-derived therapies, emphasizing the need for standardized protocols to enhance consistency and reliability across different treatment approaches. Addressing these considerations will contribute to advancing the field of regenerative medicine and optimizing the therapeutic potential of MSC-based treatments.
A new trend of regenerative investigation of cell-free therapies is the use of EV. They have various subtypes and are important mediators in cell-to-cell communication, as they carry certain proteins, glycoproteins, lipids, and ribonucleic acids that transmit biological information to support healing in injured tissues [292]. MSC-derived EVs have low-immunogenicity and strong potential for therapeutic applications, to treat tissue fibrosis and promote tissue regeneration, being therefore proposed as a novel therapeutic agent to mediate immunomodulation and promote regeneration [293]. Current investigations support the basis for clinical translation of MSCs exosomes as a cell-free therapy for tissue repair. Recent studies also enhanced some EVs characteristics such as their maintenance in systemic circulation and passage through physiological barriers to ultimately exert their effects on recipient cells. Having this in mind, they are being studied for different purposes such as regeneration, drug delivery, activity control strategies for pathological EVs and targeting technologies [294]. However, it is unclear whether using isolated EVs or exosomes excludes an important component of cell-based therapy associated therapeutic effects [295].
Cell-free products can be used naturally or engineered in order to provide superior biocompatibility and biostability, representing a big therapeutical promise in regenerative medicine, as they are considered useful for stimulating regeneration with comparable effectiveness to MSCs themselves [190]. These cell-free systems also have the advantage of low immunogenicity, non-cytotoxicity, and non-mutagenicity. In this way, they are becoming a centre of interest and researched as the best candidates to replace cellular systems in regenerative and immunomodulating medicine field [294].
Literature refers to exosomes as joint protectors against the OA damage by promoting cartilage repair, attenuating inflammation, balancing cartilage matrix formation inhibiting synovitis, and mediating subchondral bone remodelling [296,297]. In tendonitis it also attenuated the inflammatory phase, increased the proliferation and differentiation of tenocytes, had effects balancing tendon extracellular matrix, promoting the tenogenesis of tendon stem cells, and improved enthesis [298,299,300]. In muscular strain and ischemic injuries, exosomes also modulate inflammation, fibrosis, and myogenesis [301,302].
Nevertheless, the use of exosomes is still in its infancy and approaches for selectively harvesting the exosomes with regenerative potential and screening the regenerative contents have not been achieved yet [298].
7. Prognosis
Conservative treatments for OA typically focus on managing joint inflammation and pain, aiming to provide temporary functional improvement. However, they do not halt the progression of the disease, allowing a continuous degenerative process to unfold.
In the case of tendon and ligament injuries, conservative treatments include NSAIDs, local cooling, and controlled exercise programs. Unfortunately, these approaches frequently result in prolonged and unsuccessful outcomes. Healing in these cases occurs through fibrosis, restricting the return to function and resulting in loss of tissue elasticity, making the affected area more susceptible to reinjury.
Muscular injuries are commonly addressed with conservative treatments such as NSAIDs, massage, swimming and other physiotherapeutic modalities. Despite these efforts, the prognosis is often fair, as fibrosis may develop, leading to mechanical lameness and a potential recurrence of the lesion [30].
The overall prognosis for musculoskeletal injuries treated conservatively is typically moderate to fair, with clinical signs being alleviated and when healing occurs is through fibrosis. In joint injuries, degeneration continues unabated, and as a result, the affected organ fails to fully recover function, preventing a return to the same performance level.
However, recent advancements in medical therapies have introduced regenerative treatments designed to impede disease progression, reduce inflammation, and promote tissue regeneration. These innovative therapies mark a significant shift in the clinical paradigm of sports medicine, offering a robust and promising contribution. This transformative approach has the potential to improve the prognosis for musculoskeletal injuries, turning it from moderate to fair to a more optimistic outlook [27].
8. Discussion
As emphasized in this work, there is a wide array of therapeutic options for addressing musculoskeletal injuries, with the choice depending on various factors. It’s crucial to note that the selection of a specific therapy depends on the type and severity of the musculoskeletal issue, as well as the horse’s overall health and intended use.
It is indisputable that the most effective approach to handling musculoskeletal injuries is through prevention, which requires a comprehensive investment in the education and training of the entire equine community. This includes breeders, grooms, farriers, trainers, riders, nutritionists, and veterinarians, who collectively form the backbone of the horse population [303]. Recognizing the multidisciplinary nature of equine health, it is increasingly apparent that a collaborative effort is essential to achieve optimal sporting and therapeutic outcomes. Factors such as age, weight, shoeing, exercise protocols, and ground conditions significantly influence the equine athlete’s well-being [304].
Early foal management is critical, with proper exercise dosage vital for optimizing musculoskeletal development and minimizing future injuries. Research indicates that the musculoskeletal system benefits from early activity and loading, underscoring the importance of commencing exercise promptly but in appropriate quantities. Achieving a balance is key to fostering optimal musculoskeletal development and preventing future lesions, highlighting the need for further research to refine early life foal exercise protocols [2,9,15].
When prevention measures prove insufficient and injuries occur, there are various conservative and regenerative therapeutic options currently available for managing equine injuries. These treatments aim to promote healing, alleviate pain, and restore functionality.
Conservative treatments are considered the first line of intervention and aim to alleviate clinical signs promote healing and improve overall well-being without resorting to surgery or other measures. They play a crucial role in managing both acute and chronic pain in horses [305]. The suitability of conservative treatments depends on the specific condition, its severity, and the individual needs of the horse. However, their results are usually unsatisfactory and recovery is slow [58].
When these treatments prove ineffective in halting clinical signs and pathological traits, regenerative treatments emerge as the most effective means, offering both anti-inflammatory and regenerative effects [169,198,199,200]. Nowadays they represent the most promising class of therapeutics and continue in constant development. They are biologic and therefore “drug-free”, having no concerns with clearance, making it very appealing to be used in high-level sports.
Within this class, stem cell-based therapies, exhibit clinical efficacy, inducing favourable outcomes [215,282,299]. The ability to manufacture or engineer MSCs and their products according to specific pathologies enhances therapeutic responses based on tissue source, secretome, or cytokine manipulation [221,288,306].
Concerns regarding the immunogenicity and tumorigenicity of stem cell therapies have been mitigated, as no severe adverse reactions have been reported in clinical experiments [219,222,224,225,307]. The use of allogeneic bank cells from healthy donors facilitates prompt treatment in the acute phase, circumventing constraints associated with autologous treatments, such as individual variability (sex, age and health status of the animal), as well as heterogenic and time-consuming processes of harvest and production that may lead to variations on product’s cell and cytokine composition [308]. All of these factors that potentially affect product variability are a main clinical concern once they can negatively influence therapeutic effects [309].
Lack of qualitative and quantitative evidence-based data supporting regenerative therapies clinical use persists, despite of the numerous studies intended to accomplish this purpose [195]. The high heterogeneity of the reviewed studies does not allow a meta-analysis to compare results between treatments, however, results have been unanimous, concluding there is achievement of tissue regeneration using this type of therapies [222,224,306,310,311]. Part of this great heterogeneity concerns with the fact that most of the equine clinical experiments are observational being therefore dissimilar from each other [4,5,22,152,157,203,225,312,313,314,315,316].
Significant strides are yet to be taken in the pursuit of standardized protocols for the therapeutic production, storage, and application of regenerative treatments. Additionally, comprehensive studies under controlled conditions are imperative to unravel the true benefits and limitations of each class of regenerative products, including hemoderivatives and stem cell-based therapies. Establishing accurate therapeutic protocols, identifying optimal hemoderivative or MSC-tissue sources for specific diseases, determining suitable dosages, and establishing the ideal intervals between applications for various pathologies are critical areas that warrant further exploration [195,317].
It is an undeniable fact that conservative treatments are extensively and commonly used in comparison to regenerative treatments [206]. Conservative approaches, including physical therapy, medication, and non-invasive interventions, tend to be more cost-effective when contrasted with certain biologic therapies. The latter often involve advanced technologies, making them more expensive, however they are becoming more widely used [206]. Cost considerations become particularly significant for horse owners and veterinarians working within budget constraints [305].
Furthermore, conservative treatments are generally more widely available and accessible compared to some advanced biologic therapies. Concerns may arise about the perceived effectiveness of conservative treatments when compared to newer or less-studied biologic therapies [305]. Conservative treatments often benefit from a long history of use and are supported by a substantial body of empirical evidence. In contrast, biologic therapies may lack extensive research in the context of equine musculoskeletal injuries, however clinical results demonstrate their effectiveness and different abilities such as tissue regeneration [222,224,311].
The effectiveness of any treatment, whether conservative or biologic, ideally should be substantiated by scientific research and evidence. Horses exhibit significant variability in their responses to treatments, underlining the importance of considering individual characteristics, health status, and the specific condition of each horse when tailoring an appropriate treatment plan [305]. When considering the choice between conservative and biologic treatments, a balanced assessment of cost, accessibility, perceived effectiveness, expected outcome and available scientific evidence is essential [206,305]. Ongoing research in equine medicine remains imperative for expanding our understanding of various therapies and their applications in managing musculoskeletal injuries in horses.
Additionally, in-depth research is needed to delineate the most effective physiotherapeutic protocols during rehabilitation period and in routine exercise plans [57,60]. A profound understanding of each physiotherapeutic technique is essential, considering this is a crucial aspect of any musculoskeletal treatment and must be used synergistically with other therapies in order to offer a more favourable return to function and improved clinical outcomes [57].
Recognizing the evolving understanding of a multidisciplinary approach is pivotal for achieving optimal therapeutic results. Ensuring a well-balanced environment is decisive for the health and performance of equine. A collective effort of the horse-environment is compelling in preventing injuries effectively, fostering a holistic and informed approach from the earliest stages of horse production.
9. Conclusion and Future Research Directions
Currently, a diverse array of musculoskeletal treatments is available. While conservative treatments have their merits, they also come with several limitations. This has propelled regenerative treatments into a position of high importance and hope within the field. The regenerative approach holds promise for addressing musculoskeletal issues in novel and potentially more effective ways, as they have anti-inflammatory ability and enable return to function due to its regenerative competence, providing a beacon of optimism for both practitioners and horse community. However, the strength of the evidence is currently hampered by the absence of controlled clinical trials. Additionally, there is a recognized need for medium- and long-term evaluations to assess the durability and sustained efficacy of regenerative therapies. To gain a comprehensive understanding of the advantages and limitations of each regenerative therapy, more studies are warranted as these therapies hold significant potential for the future of sports medicine and rehabilitation, prompting the necessity for further research. The outlook in this therapeutic area is promising, generating high expectations and capturing extensive attention in both equine and human medicine. Consequently, the field is evolving rapidly, propelled by auspicious results that are currently emerging. It’s important to bear in mind that the synergistic integration of physiotherapeutic techniques and regenerative approaches holds the promise of delivering superior outcomes.
Currently, the primary hurdle facing regenerative medicine within the domain of sports medicine is the attainment of consistent clinical outcomes. The challenge also lies in identifying the most effective orthobiologic, one that is readily accessible, easy to administer, carries minimal risk, and is financially feasible. Promising results in the realm of tissue repair and regeneration, particularly due to the advantageous properties of MSCs, are evident in experimental studies with horses. However, further research is imperative to validate efficacy and establish precise guidelines for clinical implementation. Despite the ongoing quest for answers in regenerative therapies, it seems that they presently emerge as the most effective approach to address musculoskeletal injuries.
Author Contributions
Conceptualization, A.C.M, J.M.S., I.L.R., CM.M., L.M.A and A.R.C.; methodology, A.C.M, R.D.A., J.M.S., I.L.R., B.L., A.C.S., P.S., and A.R.C.; software, A.C.S., I.L.R., B.L., and P.S.; validation, A.C.M, R.D.A., J.M.S., I.L.R. CM.M., L.M.A and A.R.C.; formal analysis, A.C.M, R.D.A., J.M.S., I.L.R., CM.M., and L.M.A; investigation, A.C.M, R.D.A., J.M.S., I.L.R. CM.M., L.M.A and A.R.C.; formal analysis, A.C.M, R.D.A., J.M.S., I.L.R., CM.M., and L.M.A; resources, A.C.M., J.M.S., C.M.M., R.D.A., and L.M.A.; data curation, , I.L.R., R.D.A., A.C.M., and L.M.A.; writing—original draft preparation, I.L.R., R.D.A., A.C.M., J.M.S., and L.M.A.; writing—review and editing, I.L.R.; R.D.A.; P.S.; A.C.M.; J.M.S., and L.M.A.; visualization, A.C.S., I.L.R., B.L., and P.S.; supervision, A.C.M., R.D.A., L.M.A., C.M.M., L.L., and J.M.S.; project administration, A.C.M., R.D.A., L.M.A., C.M.M., and J.M.S.; funding acquisition, A.C.M., R.D.A., L.M.A., C.M.M., and J.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
Funding: This work was supported by Prémios Santa Casa Neurociências–Prize Melo e Castro for Spinal Cord Injury Research (MC-04/17; MC-18-2021). The author Rui D. Alvites acknowledges the Centro de Estudos de Ciência Animal (CECA), Instituto de Ciências, Tecnologias e Agroambiente (ICETA), Porto University (UP), and Fundação para a Ciência e Tecnologia (FCT) for the funding and availability of all technical, structural, and human resources necessary for the development of this work. The work was supported through the project UIDB/00211/2020 funded by FCT/MCTES through national funds. The authors acknowledge FCT for funding the project 2022.04501.PTDC (Olfabionerve-Olfactory Mucosa Mesenchymal Stem Cells and Biomaterials Promoting Peripheral Nerve Regeneration) and the PhD Scholarships Ana Catarina Sousa (SFRH/BD/146689/2019), Bruna Lopes (2021.05265.BD), and Patrícia Sousa (2023.00246.BD).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| 2D | two-dimensional |
| 3D | three-dimensional |
| ACI | autologous chondrocyte implantation |
| ACS | autologous conditioned serum |
| AFS-MSC | amniotic fluid mesenchymal stromal/stem cell |
| AINEs | non-steroidal anti-inflammatories |
| APS | autologous protein serum |
| AT-MSC | adipose tissue mesenchymal stromal/stem cell |
| BM-MSC | bone marrow mesenchymal stromal/stem cell |
| CD | cluster differentiation |
| CD | complementary diagnostic exams |
| CDET | common digital extensor tendon |
| cm | centimeter |
| CM | conditioned medium |
| cm2 | square centimeter |
| COX | cycloxigenase |
| CSA | cross sectional area |
| CT | Computed Tomography |
| CTA | Computed Tomography Arthrography |
| DDFT | deep digital flexor tendon |
| DNA | desoxyribonucleic acid |
| DP-MSC | dental pulp mesenchymal stromal/stem cell |
| ECM | extracellular matrix |
| ESC | embryonic stem cell |
| ESWT | extracorporeal shock wave therapy |
| EV | extracellular vesicles |
| FEI | Federation Equestre Internationale |
| FGF | fibroblast growth factor |
| FL | forelimbs |
| GAG | glycosaminoglicans |
| GF | growth factor |
| h | hour |
| HILT | high intensity laser therapy |
| HL | hindlimbs |
| HLA | human leucocyte antigen |
| HSC | hematopoietic stem cell |
| HyA | hyaluronic acid |
| Hz | Hertz |
| IA | intra-articular |
| IGF | insulin growth factor |
| IL | Interleukyn |
| IM | intramuscular |
| IPSC | induced pluripotent stem cell |
| IRAP | interleukin-1 receptor antagonist protein |
| IRU | radioisotope uptake |
| IV | endovenous |
| Kg | kilogram |
| KT | Kynesiotaping |
| LLLT | low level laser therapy |
| mg | milligram |
| MHz | megahertz |
| min | minute |
| ml | milliliter |
| MRI | Magnetic Resonance image |
| MSC | mesenchymal stem/stromal cells |
| MT-MSC | muscle tissue mesenchymal stromal/stem cell |
| mW | milliwatts |
| NEMS | Neural electrical muscle stimulation |
| nm | nanometres |
| OA | osteoarthritis |
| oC | Celsius degree |
| PDEGF | platelet derived epidermal growth factor |
| PDGF | platelet derived growth factor |
| PEMF | pulsed electromagnetic frequency |
| PGE2 | Prostaglandin E2 |
| PHyd | Polyacrylamide hydrogel |
| Po -MSC | periosteum mesenchymal stromal/stem cell |
| PO | Per os |
| PSAG | Polysulfated glycosaminoglycan |
| RNA | ribonucleic acid |
| ROM | range of motion |
| SAIDs | steroidal anti-inflammatories |
| SDFT | superficial digital flexor tendon |
| SL | suspensory ligament |
| SM-MSC | synovial membrane mesenchymal stromal/stem cell |
| TENS | transcutaneous electrical nerve stimulation |
| TGF | Transforming growth factor |
| U/S | Ultrasound |
| UC-MSC | umbilical cord derived Whartons jelly mesenchymal stromal/stem cell |
| VEGF | vascular endothelial growth factor |
| VEGF | vascular endothelial growth factor |
| W | Watts |
| WT | water treadmill |
| X-ray | Radiograph |
| α2M | Alfa-2 macroglobulin |
References
- Smith, R.K.W.; McIlwraith, C.W. “One Health” in tendinopathy research: Current concepts. J. Orthop. Res. 2021, 39, 1596–1602. [Google Scholar] [CrossRef]
- Rogers, C.W.; Bolwell, C.F.; Gee, E.K.; Rosanowski, S.M. Equine musculoskeletal development and performance: impact of the production system and early training. Anim. Prod. Sci. 2020, 60, 2069–2079. [Google Scholar] [CrossRef]
- Smith, R.; Webbon, P. Harnessing the stem cell for the treatment of tendon injuries: heralding a new dawn? British journal of sports medicine 2005, 39, 582–584. [Google Scholar] [CrossRef]
- Shokry, M.; Mostafa, A.; Tohamy, A.; El-Sharkawi, M. Autologous mesenchymal stem cells for treatment of acute superficial digital flexor tendonitis in athletic horses: clinical study of 15 cases. Pferdeheilkunde Equine Med. 2020, 36, 43–48. [Google Scholar] [CrossRef]
- Salz, R.O.; Elliott, C.R.B.; Zuffa, T.; Bennet, E.D.; Ahern, B.J. Treatment of racehorse superficial digital flexor tendonitis: A comparison of stem cell treatments to controlled exercise rehabilitation in 213 cases. Equine Veter- J. 2023, 55, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.B.; Al-Dadah, O. Conservative treatment of knee osteoarthritis: A review of the literature. World J. Orthop. 2022, 13, 212–229. [Google Scholar] [CrossRef]
- Sutton, J.S.; Muran, A.; Zaslav, K.; Grande, D. Orthobiologics: An Updated Definition. Open Journal of Regenerative Medicine 2023, 12, 36–48. [Google Scholar] [CrossRef]
- De Sousa, N.R.; Luna, S.P.L.; Pizzigatti, D.; Martins, M.T.A.; Possebon, F.S.; Aguiar, A.C.S. Relation between type and local of orthopedic injuries with physical activity in horses. Ciência Rural 2016, 47. [Google Scholar] [CrossRef]
- Lönnell, C. Yard differences in training, management and orthopedic injury in showjumping, riding school, and thoroughbred race horses; Department of Clinical Sciences, Swedish University of Agricultural Sciences: 2012.
- Gramm, M.; Marksteiner, R. The Effect of Age on Thoroughbred Racing Performance. J. Equine Sci. 2010, 21, 73–78. [Google Scholar] [CrossRef]
- Cruz, A.M.; Poljak, Z.; Filejski, C.; Lowerison, M.L.; Goldie, K.; Martin, S.W.; Hurtig, M.B. Epidemiologic characteristics of catastrophic musculoskeletal injuries in Thoroughbred racehorses. Am. J. Veter- Res. 2007, 68, 1370–1375. [Google Scholar] [CrossRef]
- Bertuglia, A.; Bullone, M.; Rossotto, F.; Gasparini, M. Epidemiology of musculoskeletal injuries in a population of harness Standardbred racehorses in training. BMC Veter- Res. 2014, 10, 1–10. [Google Scholar] [CrossRef]
- Bolwell, C.; Rogers, C.; Gee, E.; McIlwraith, W. Epidemiology of Musculoskeletal Injury during Racing on New Zealand Racetracks 2005–2011. Animals 2017, 7, 62. [Google Scholar] [CrossRef] [PubMed]
- Walters, J.M.; Parkin, T.; A Snart, H.; Murray, R.C. Current management and training practices for UK dressage horses. Comp. Exerc. Physiol. 2008, 5, 73–83. [Google Scholar] [CrossRef]
- Murray, R.C.; Dyson, S.J.; Tranquille, C.; Adams, V. Association of type of sport and performance level with anatomical site of orthopaedic injury diagnosis. Equine Veter- J. 2006, 38, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Kaneene, J.B.; Ross, W.A.; Miller, R. The Michigan equine monitoring system. II. Frequencies and impact of selected health problems. Prev. Veter- Med. 1997, 29, 277–292. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, E.; Hassaneen, A.S.A.; Noby, M.A.; Mawas, A.; Abdel-Hady, A.-N.A. Equine osteoarthritis: An overview of different treatment strategies. SVU-International J. Veter- Sci. 2021, 4, 85–96. [Google Scholar] [CrossRef]
- Chen, D.; Shen, J.; Zhao, W.; Wang, T.; Han, L.; Hamilton, J.L.; Im, H.-J. Osteoarthritis: toward a comprehensive understanding of pathological mechanism. Bone Res. 2017, 5, 1–13. [Google Scholar] [CrossRef]
- E Schlueter, A.; Orth, M.W. Equine osteoarthritis: a brief review of the disease and its causes. Equine Comp. Exerc. Physiol. 2004, 1, 221–231. [Google Scholar] [CrossRef]
- Grässel, S.; Zaucke, F.; Madry, H. Osteoarthritis: Novel Molecular Mechanisms Increase Our Understanding of the Disease Pathology. J. Clin. Med. 2021, 10, 1938. [Google Scholar] [CrossRef]
- Grässel, S.; Muschter, D. Recent advances in the treatment of osteoarthritis. F1000Research 2020, 9, 325. [Google Scholar] [CrossRef]
- Ireland, J.L.; Clegg, P.D.; McGOWAN, C.M.; McKANE, S.A.; Chandler, K.J.; Pinchbeck, G.L. Comparison of owner-reported health problems with veterinary assessment of geriatric horses in the United Kingdom. Equine Veter- J. 2012, 44, 94–100. [Google Scholar] [CrossRef]
- Di Filippo, P.A.; Meireles, M.A.D.; Ribeiro, L.M.F.; de Lannes, S.T.; Meireles, N.F.T.; Viana, I.S.; Hokamura, H.K. Influence of Exercise, Age, Body weight, and Growth on the Development of Tarsal Osteoarthritis in Young Mangalarga Marchador Horses. J. Equine Veter- Sci. 2019, 80, 36–39. [Google Scholar] [CrossRef]
- Neundorf, R.H.; Lowerison, M.B.; Cruz, A.M.; Thomason, J.J.; McEwen, B.J.; Hurtig, M.B. Determination of the prevalence and severity of metacarpophalangeal joint osteoarthritis in Thoroughbred racehorses via quantitative macroscopic evaluation. Am. J. Vet. Res. 2010, 71, 1284–1293. [Google Scholar] [CrossRef]
- INVALID CITATION !!!
- Thorpe, C.T.; Godinho, M.S.; Riley, G.P.; Birch, H.L.; Clegg, P.D.; Screen, H.R. The interfascicular matrix enables fascicle sliding and recovery in tendon, and behaves more elastically in energy storing tendons. J. Mech. Behav. Biomed. Mater. 2015, 52, 85–94. [Google Scholar] [CrossRef]
- Zielińska, P.; Nicpoń, J.; Kiełbowicz, Z.; Soroko, M.; Dudek, K.; Zaborski, D. Effects of High Intensity Laser Therapy in the Treatment of Tendon and Ligament Injuries in Performance Horses. Animals 2020, 10, 1327. [Google Scholar] [CrossRef]
- Zielińska, P.; Soroko, M.; Godlewska, M.; Śniegucka, K.; Dudek, K.; Howell, K. Photothermal Effects of High-Intensity Laser Therapy on the Superficial Digital Flexor Tendon Area in Clinically Healthy Racehorses. Animals 2022, 12, 1253. [Google Scholar] [CrossRef] [PubMed]
- Qazi, T.H.; Duda, G.N.; Ort, M.J.; Perka, C.; Geissler, S.; Winkler, T. Cell therapy to improve regeneration of skeletal muscle injuries. J. Cachexia Sarcopenia Muscle 2019, 10, 501–516. [Google Scholar] [CrossRef] [PubMed]
- Piercy, R.J.; Rivero, J. Muscle disorders of equine athletes. Equine Sports Medicine and Surgery E-Book: Basic and clinical sciences of the equine athlete 2013, 109.
- Walmsley, E.; Steel, C.; Richardson, J.; Whitton, R. Muscle strain injuries of the hindlimb in eight horses: diagnostic imaging, management and outcomes. Aust. Veter- J. 2010, 88, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.-Y.; Lee, E.-J.; Park, J.-K.; Park, S.-I.; Cho, S.-G.; Kim, H.K.; Kim, S.-Y.; Jeong, K.-S. Generation of Equine-Induced Pluripotent Stem Cells and Analysis of Their Therapeutic Potential for Muscle Injuries. Cell Transplant. 2016, 25, 2003–2016. [Google Scholar] [CrossRef]
- Redden, R.F. Clinical and radiographic examination of the equine foot. 2003.
- Hinchcliff, K.W.; Kaneps, A.J.; Geor, R.J.; Van Erck-Westergen, E. Equine Sports Medicine and Surgery: Equine Sports Medicine and Surgery-E-Book; Elsevier Health Sciences: 2023.
- Hinchcliff, K.W. Clinical Epidemiology and Evidence-Based Medicine. Equine Internal Medicine-E-Book 2017, 1, 218.
- Schumacher, J.; Taylor, D.R.; Schramme, M.C.; Schumacher, J. Localization of pain in the equine foot emphasizing the physical examination and analgesic techniques. 2012.
- Park, R.D.; Nelson, T.R.; Hoopes, P.J. Magnetic resonance imaging of the normal equine digit and metacarpophalangeal joint. Veter- Radiol. 1987, 28, 105–116. [Google Scholar] [CrossRef]
- Kraft, S.L.; Gavin, P. Physical Principles and Technical Considerations for Equine Computed Tomography and Magnetic Resonance Imaging. Veter- Clin. North Am. Equine Pr. 2001, 17, 115–130. [Google Scholar] [CrossRef]
- Fraschetto, C.; Dancot, M.; Vandersmissen, M.; Denoix, J.-M.; Coudry, V. Conservative management of equine tarsal collateral ligament injuries may allow return to normal performance. J. Am. Veter- Med Assoc. 2023, 261, 995–1003. [Google Scholar] [CrossRef]
- Coudry, V.; Denoix, J. Ultrasonographic examination of the palmar aspect of the pastern of the horse: Digital flexor tendons and digital sheath. Equine Veter- Educ. 2013, 25, 196–203. [Google Scholar] [CrossRef]
- Denoix, J.-M. Diagnostic Techniques for Identification and Documentation of Tendon and Ligament Injuries. Veter- Clin. North Am. Equine Pr. 1994, 10, 365–407. [Google Scholar] [CrossRef]
- Werpy, N.M.; Denoix, J.-M. Imaging of the Equine Proximal Suspensory Ligament. Veter- Clin. North Am. Equine Pr. 2012, 28, 507–525. [Google Scholar] [CrossRef]
- Garrett, K.S. Ultrasonography of the hock. Atlas of equine ultrasonography 2022, 173-188.
- Dik, K.J. Ultrasonography of the equine tarsus. Veterinary Radiology & Ultrasound 1993, 34, 36–43. [Google Scholar] [CrossRef]
- Denoix, J.-M. Ultrasonographic examination of joints, a revolution in equine locomotor pathology. Bulletin de l’Académie vétérinaire de France 2009, 162, 313–325. [Google Scholar] [CrossRef]
- De Bastiani, G.; de La Côrte, F.D.; Brass, K.E.; Kommers, G.D.; Denoix, J.M. Association of Ultrasound and Anatomopathologic Findings of Equine Metacarpophalangeal Lesions. J. Equine Veter- Sci. 2014, 34, 1218–1225. [Google Scholar] [CrossRef]
- Brommer, H.; Rijkenhuizen, A.B.M.; Brama, P.A.J.; Barneveld, A.; van Weeren, P.R. Accuracy of diagnostic arthroscopy for the assessment of cartilage damage in the equine metacarpophalangeal joint. Equine Veter- J. 2004, 36, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Merkely, G.; Ackermann, J.; Lattermann, C. Articular cartilage defects: incidence, diagnosis, and natural history. Operative techniques in sports medicine 2018, 26, 156–161. [Google Scholar] [CrossRef]
- Ehrle, A.; Lilge, S.; Clegg, P.D.; Maddox, T.W. Equine flexor tendon imaging part 2: Current status and future directions in advanced diagnostic imaging, with focus on the deep digital flexor tendon. Veter- J. 2021, 278, 105763. [Google Scholar] [CrossRef]
- Palmer, A.J.R.; Brown, C.P.; McNally, E.G.; Price, A.J.; Tracey, I.; Jezzard, P.; Carr, A.J.; Glyn-Jones, S.; Ayyar-Gupta, V.; Dutton, S.J.; et al. Non-invasive imaging of cartilage in early osteoarthritis. Bone Jt. J. 2013, 95, 738–746. [Google Scholar] [CrossRef]
- Doll, C.U.; Bohner, M.; Berner, D.; Buettner, K.; Horstmeier, C.; Winter, K.; Burk, J. Approaches to standardising the magnetic resonance image analysis of equine tendon lesions. Veter- Rec. Open 2023, 10, e257. [Google Scholar] [CrossRef] [PubMed]
- Barrett, M.F.; Goorchenko, G.E.; Frisbie, D.D. Comparison of Ultrasound and Magnetic Resonance Imaging for Identifying Soft Tissue Abnormalities in the Palmar Aspect of the Equine Digit. Animals 2023, 13, 2328. [Google Scholar] [CrossRef] [PubMed]
- Mair, T.S.; Kinns, J.; Jones, R.D.; Bolas, N.M. Magnetic resonance imaging of the distal limb of the standing horse. Equine Veter- Educ. 2005, 17, 74–78. [Google Scholar] [CrossRef]
- Vanderperren, K.; Raes, E.; Hoegaerts, M.; Saunders, J.H. Diagnostic imaging of the equine tarsal region using radiography and ultrasonography. Part 1: The soft tissues. Veter- J. 2009, 179, 179–187. [Google Scholar] [CrossRef]
- Biggi, M. Equine scintigraphy: basic principles and interpretation. UK-Vet Equine 2020, 4, 84–86. [Google Scholar] [CrossRef]
- Dyson, S. Musculoskeletal Scintigraphy of the Equine Athlete. Semin. Nucl. Med. 2014, 44, 4–14. [Google Scholar] [CrossRef]
- Denoix, J.-M. Physical Therapy and Massage for the Horse: Biomechanics-Excercise-Treatment; CRC Press: 2021.
- Yang, S.-M.; Chen, W.-S. Conservative treatment of tendon injuries. American Journal of Physical Medicine & Rehabilitation 2020, 99, 550–557. [Google Scholar] [CrossRef]
- Frick, A. Stretching exercises for horses: are they effective? Journal of equine veterinary science 2010, 30, 50–59. [Google Scholar] [CrossRef]
- Kaneps, A.J. Practical Rehabilitation and Physical Therapy for the General Equine Practitioner. Veter- Clin. North Am. Equine Pr. 2016, 32, 167–180. [Google Scholar] [CrossRef]
- van Eps, A.W.; Orsini, J.A. A comparison of seven methods for continuous therapeutic cooling of the equine digit. Equine Veter- J. 2016, 48, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Marlin, D. Evaluation of the cooling efficacy of different equine leg cooling methods. Comp. Exerc. Physiol. 2019, 15, 113–122. [Google Scholar] [CrossRef]
- Montgomery, L.; Elliott, S.B.; Adair, H.S. Muscle and Tendon Heating Rates with Therapeutic Ultrasound in Horses. Veter- Surg. 2013, 42, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Ericson, C.; Stenfeldt, P.; Hardeman, A.; Jacobson, I. The Effect of Kinesiotape on Flexion-Extension of the Thoracolumbar Back in Horses at Trot. Animals 2020, 10, 301. [Google Scholar] [CrossRef] [PubMed]
- GARCIA PIQUERES, M.; FORÉS JACKSON, P. Evaluation of kinesio taping applied to the equine thoracolumbar spine: clinical response and mechanical nociceptive threshold. Journal of Veterinary Medical Research 2021, 28, 1–11. [Google Scholar] [CrossRef]
- de Mattos, L.H.L.; Yamada, A.L.M.; dos Santos, V.H.; Hussni, C.A.; Rodrigues, C.A.; Watanabe, M.J.; Alves, A.L.G. Treatment With Therapeutic Bandages to Control Equine Postarthroscopic Tibio-Patellofemoral Swelling. J. Equine Veter- Sci. 2017, 54, 87–92. [Google Scholar] [CrossRef]
- Practitioners, A.A.o.E. Guide for veterinary service and judging of equestrian events. 1991.
- Davidson, E.J. Controlled Exercise in Equine Rehabilitation. Veter- Clin. North Am. Equine Pr. 2016, 32, 159–165. [Google Scholar] [CrossRef]
- Gillis, C.L. Rehabilitation of tendon and ligament injuries. In Proceedings of the Proc Am Assoc Equine Pract; 1997; pp. 306–309. [Google Scholar]
- Kannus, P.; Jozsa, L.; Natri, A.; Järvinen, M. Effects of training, immobilization and remobilization on tendons. Scandinavian journal of medicine & science in sports 1997, 7, 67–71. [Google Scholar] [CrossRef]
- Sharma, P.; Maffulli, N. Tendon injury and tendinopathy: healing and repair. JBJS 2005, 87, 187–202. [Google Scholar] [CrossRef]
- Muñoz, A.; Saitua, A.; Becero, M.; Riber, C.; Satué, K.; de Medina, A.S.; Argüelles, D.; Castejón-Riber, C. The use of the water treadmill for the rehabilitation of musculoskeletal injuries in the sport horse. J. Veter- Res. 2019, 63, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Nankervis, K.; Tranquille, C.; McCrae, P.; York, J.; Lashley, M.; Baumann, M.; King, M.; Sykes, E.; Lambourn, J.; Miskimmin, K.-A.; et al. Consensus for the General Use of Equine Water Treadmills for Healthy Horses. Animals 2021, 11, 305. [Google Scholar] [CrossRef]
- King, M.R. Principles and Application of Hydrotherapy for Equine Athletes. Veter- Clin. North Am. Equine Pr. 2016, 32, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Kamioka, H.; Tsutani, K.; Okuizumi, H.; Mutoh, Y.; Ohta, M.; Handa, S.; Okada, S.; Kitayuguchi, J.; Kamada, M.; Shiozawa, N.; et al. Effectiveness of Aquatic Exercise and Balneotherapy: A Summary of Systematic Reviews Based on Randomized Controlled Trials of Water Immersion Therapies. J. Epidemiology 2010, 20, 2–12. [Google Scholar] [CrossRef]
- .
- Nankervis, K.J.; Launder, E.J.; Murray, R.C. The Use of Treadmills Within the Rehabilitation of Horses. J. Equine Veter- Sci. 2017, 53, 108–115. [Google Scholar] [CrossRef]
- Tranquille, C.A.; Tacey, J.B.; Walker, V.A.; Nankervis, K.J.; Murray, R.C. International survey of equine water treadmills—Why, when, and how? Journal of Equine Veterinary Science 2018, 69, 34–42. [Google Scholar] [CrossRef]
- Kaneps, A.J.; Beverly, M. THERAPEUTIC ULTRASOUND.
- Porter, M. Equine Rehabilitation Therapy for Joint Disease. Veter- Clin. North Am. Equine Pr. 2005, 21, 599–607. [Google Scholar] [CrossRef]
- Riegel, R.J.; Godbold Jr, J.C. Laser therapy in veterinary medicine: photobiomodulation; John Wiley & Sons: 2017.
- Riegel, R.J.; Godbold Jr, J.C. Fundamental information. Laser Therapy in Veterinary Medicine: Photobiomodulation 2017, 7-18.
- Heiskanen, V.; Hamblin, M.R. Photobiomodulation: lasers vs. light emitting diodes? Photochemical & Photobiological Sciences 2018, 17, 1003–1017. [Google Scholar] [CrossRef]
- Leotty, C.L.R.; Lima, M.M.C.; Araújo, F.X.d. Effect of low-level laser therapy on pain and function of patients with shoulder tendinopathy: A systematic review. Fisioterapia e Pesquisa 2020, 27, 210–217. [Google Scholar] [CrossRef]
- Kaub, L.; Schmitz, C. More than Ninety Percent of the Light Energy Emitted by Near-Infrared Laser Therapy Devices Used to Treat Musculoskeletal Disorders Is Absorbed within the First Ten Millimeters of Biological Tissue. Biomedicines 2022, 10, 3204. [Google Scholar] [CrossRef]
- Jadah, N.A.; Shamkhi, I.A. A comparative study of low-level laser efficacy on autologous activity of PRP injected in knee arthritis, in vivo study. Lasers Med Sci. 2021, 36, 357–363. [Google Scholar] [CrossRef]
- Lyu, K.; Liu, X.; Jiang, L.; Chen, Y.; Lu, J.; Zhu, B.; Liu, X.; Li, Y.; Wang, D.; Li, S. The Functions and Mechanisms of Low-Level Laser Therapy in Tendon Repair (Review). Front. Physiol. 2022, 13, 808374. [Google Scholar] [CrossRef]
- Wu, M.; Luan, L.; Pranata, A.; Witchalls, J.; Adams, R.; Bousie, J.; Han, J. Is high intensity laser therapy more effective than other physical therapy modalities for treating knee osteoarthritis? A systematic review and network meta-analysis. Front. Med. 2022, 9, 956188. [Google Scholar] [CrossRef] [PubMed]
- Berni, M.; Brancato, A.M.; Torriani, C.; Bina, V.; Annunziata, S.; Cornella, E.; Trucchi, M.; Jannelli, E.; Mosconi, M.; Gastaldi, G.; et al. The Role of Low-Level Laser Therapy in Bone Healing: Systematic Review. Int. J. Mol. Sci. 2023, 24, 7094. [Google Scholar] [CrossRef]
- He, K.; Zhou, X.; Zheng, F.; Ju, X.; Fu, S.-N.; Wong, A.Y.L. Histological, Physiological and Biomechanical Effects of Low-Level Laser Therapy on Tendon Healing in Animals and Humans: A Systematic Review. Ann. Biomed. Eng. 2023, 1–49. [Google Scholar] [CrossRef] [PubMed]
- Calatrava, I.R.; Valenzuela, J.M.S.; Gómez-Villamandos, R.J.; Redondo, J.I.; Gómez-Villamandos, J.C.; Jurado, I.A. Histological and clinical responses of articular cartilage to low-level laser therapy: Experimental study. Lasers Med Sci. 1997, 12, 117–121. [Google Scholar] [CrossRef]
- Jankaew, A.; You, Y.-L.; Yang, T.-H.; Chang, Y.-W.; Lin, C.-F. The effects of low-level laser therapy on muscle strength and functional outcomes in individuals with knee osteoarthritis: a double-blinded randomized controlled trial. Sci. Rep. 2023, 13, 165. [Google Scholar] [CrossRef] [PubMed]
- Wyszyńska, J.; Bal-Bocheńska, M. Efficacy of High-Intensity Laser Therapy in Treating Knee Osteoarthritis: A First Systematic Review. Photomed. Laser Surg. 2018, 36, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Angelova, A.; Ilieva, E.M. Effectiveness of High Intensity Laser Therapy for Reduction of Pain in Knee Osteoarthritis. Pain Res. Manag. 2016, 2016, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Stiglić-Rogoznica, N.; Stamenković, D.; Frlan-Vrgoc, L.; Avancini-Dobrović, V.; Vrbanić, T.S.-L. Analgesic effect of high intensity laser therapy in knee osteoarthritis. Coll. Antropol. 2011, 183–185. [Google Scholar]
- Riegel, R.J. Fundamentals of Equine Laser Therapy. Laser Therapy in Veterinary Medicine: Photobiomodulation 2017, 335-343.
- Auersperg, V.; Trieb, K. Extracorporeal shock wave therapy: an update. EFORT Open Rev. 2020, 5, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-J. Extracorporeal shockwave therapy in musculoskeletal disorders. J. Orthop. Surg. Res. 2012, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, A.N.; Tenforde, A.S.; Jelsing, E.J. Extracorporeal Shockwave Therapy in the Management of Sports Medicine Injuries. Optom. Vis. Sci. 2021, 20, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Stania, M.; Juras, G.; Chmielewska, D.; Polak, A.; Kucio, C.; Król, P. Extracorporeal Shock Wave Therapy for Achilles Tendinopathy. BioMed Res. Int. 2019, 2019, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.-D.; Yang, C.-L.; Lo, H.-Y.; Yeh, H.-J. Extracorporeal shockwave therapy with a modified technique on tendon and ligament for knee osteoarthritis: a randomized controlled trial. American Journal of Physical Medicine & Rehabilitation 2022, 101, 11–17. [Google Scholar] [CrossRef]
- Yocom, A.F.; Bass, L.D. Review of the application and efficacy of extracorporeal shockwave therapy in equine tendon and ligament injuries. Equine Veter- Educ. 2019, 31, 271–277. [Google Scholar] [CrossRef]
- Schmitz, C. Improving extracorporeal shock wave therapy with 904 or 905 nm pulsed, high power laser pretreatment. 2021.
- Schlachter, C.; Lewis, C. Electrophysical Therapies for the Equine Athlete. Veter- Clin. North Am. Equine Pr. 2016, 32, 127–147. [Google Scholar] [CrossRef]
- Schils, S.J. Review of electrotherapy devices for use in veterinary medicine. In Proceedings of the Proceedings of the 55th Annual Convention of the American Association of Equine Practitioners, Las Vegas, NV, 2009; pp. 68–73.
- Hyytiäinen, H.K.; Boström, A.; Asplund, K.; Bergh, A. A Systematic Review of Complementary and Alternative Veterinary Medicine in Sport and Companion Animals: Electrotherapy. Animals 2022, 13, 64. [Google Scholar] [CrossRef]
- Lucas, R.G.; Rodríguez-Hurtado, I.; Álvarez, C.T.; Ortiz, G. Effectiveness of Neuromuscular Electrical Stimulation and Dynamic Mobilization Exercises on Equine Multifidus Muscle Cross-Sectional Area. J. Equine Veter- Sci. 2022, 113, 103934. [Google Scholar] [CrossRef]
- Buchner, H.H.F.; Zimmer, L.; Haase, L.; Perrier, J.; Peham, C. Effects of Whole Body Vibration on the Horse: Actual Vibration, Muscle Activity, and Warm-up Effect. J. Equine Veter- Sci. 2017, 51, 54–60. [Google Scholar] [CrossRef]
- Nowlin, C.; Nielsen, B.; Mills, J.; Robison, C.; Schott, H.; Peters, D. Acute and Prolonged Effects of Vibrating Platform Treatment on Horses: A Pilot Study. J. Equine Veter- Sci. 2018, 62, 116–122. [Google Scholar] [CrossRef]
- Sugg, S.J. Effects of Whole Body Vibration on Lameness, Stride Length, Cortisol, and Other Parameters in Healthy Horses. Middle Tennessee State University, 2018.
- Khan, K.M.; Cook, J.L.; Bonar, F.; Harcourt, P.; Åstrom, M. Histopathology of common tendinopathies: update and implications for clinical management. Sports medicine 1999, 27, 393–408. [Google Scholar] [CrossRef]
- Sass, F.A.; Fuchs, M.; Pumberger, M.; Geissler, S.; Duda, G.N.; Perka, C.; Schmidt-Bleek, K. Immunology guides skeletal muscle regeneration. International journal of molecular sciences 2018, 19, 835. [Google Scholar] [CrossRef]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. Lancet 2010, 376, 1751–1767. [Google Scholar] [CrossRef]
- Lin, M.-T.; Chiang, C.-F.; Wu, C.-H.; Huang, Y.-T.; Tu, Y.-K.; Wang, T.-G. Comparative Effectiveness of Injection Therapies in Rotator Cuff Tendinopathy: A Systematic Review, Pairwise and Network Meta-analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabilitation 2018, 100, 336–349. [Google Scholar] [CrossRef]
- Everhart, J.S.; Cole, D.; Sojka, J.H.; Higgins, J.D.; Magnussen, R.A.; Schmitt, L.C.; Flanigan, D.C. Treatment Options for Patellar Tendinopathy: A Systematic Review. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 861–872. [Google Scholar] [CrossRef]
- da Costa, B.R.; Hari, R.; Jüni, P. Intra-articular Corticosteroids for Osteoarthritis of the Knee. JAMA 2016, 316, 2671–2672. [Google Scholar] [CrossRef]
- Bellamy, N.; Campbell, J.; Welch, V.; Gee, T.L.; Bourne, R.; Wells, G.A. Intraarticular corticosteroid for treatment of osteoarthritis of the knee. Cochrane Database of Systematic Reviews 2006. [CrossRef]
- Shanley, L.C.; Mahon, O.R.; Kelly, D.J.; Dunne, A. Harnessing the innate and adaptive immune system for tissue repair and regeneration: Considering more than macrophages. Acta Biomater. 2021, 133, 208–221. [Google Scholar] [CrossRef]
- Arvind, V.; Huang, A.H. Reparative and Maladaptive Inflammation in Tendon Healing. Front. Bioeng. Biotechnol. 2021, 9. [Google Scholar] [CrossRef]
- Oliva, F.; Marsilio, E.; Asparago, G.; Frizziero, A.; Berardi, A.C.; Maffulli, N. The Impact of Hyaluronic Acid on Tendon Physiology and Its Clinical Application in Tendinopathies. Cells 2021, 10, 3081. [Google Scholar] [CrossRef]
- Lo, G.H.; LaValley, M.; McAlindon, T.; Felson, D.T. Intra-articular hyaluronic acid in treatment of knee osteoarthritis: a meta-analysis. Jama 2003, 290, 3115–3121. [Google Scholar] [CrossRef]
- Han, S.-B.; Seo, I.-W.; Shin, Y.-S. Intra-Articular Injections of Hyaluronic Acid or Steroids Associated With Better Outcomes Than Platelet-Rich Plasma, Adipose Mesenchymal Stromal Cells, or Placebo in Knee Osteoarthritis: A Network Meta-analysis. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 292–306. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.; Awad, M.E.; Hamrick, M.W.; Hunter, M.; Fulzele, S. Recent advances in hyaluronic acid based therapy for osteoarthritis. Clin. Transl. Med. 2018, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kaux, J.-F.; Samson, A.; Crielaard, J.-M. Hyaluronic acid and tendon lesions. Muscles, ligaments and tendons journal 2015, 5, 264. [Google Scholar] [CrossRef] [PubMed]
- Agostini, F.; de Sire, A.; Paoloni, M.; Finamore, N.; Ammendolia, A.; Mangone, M.; Bernetti, A. Effects of hyaluronic acid injections on pain and functioning in patients affected by tendinopathies: A narrative review. J. Back Musculoskelet. Rehabilitation 2022, 35, 949–961. [Google Scholar] [CrossRef]
- Ning, C.; Li, P.; Gao, C.; Fu, L.; Liao, Z.; Tian, G.; Yin, H.; Li, M.; Sui, X.; Yuan, Z.; et al. Recent advances in tendon tissue engineering strategy. Front. Bioeng. Biotechnol. 2023, 11, 1115312. [Google Scholar] [CrossRef]
- Bannuru, R.; Natov, N.; Dasi, U.; Schmid, C.; McAlindon, T. Therapeutic trajectory following intra-articular hyaluronic acid injection in knee osteoarthritis – meta-analysis. Osteoarthr. Cartil. 2011, 19, 611–619. [Google Scholar] [CrossRef]
- Strauss, E.J.; Hart, J.A.; Miller, M.D.; Altman, R.D.; Rosen, J.E. Hyaluronic acid viscosupplementation and osteoarthritis: current uses and future directions. The American journal of sports medicine 2009, 37, 1636–1644. [Google Scholar] [CrossRef]
- Xavier, A.A.d.S.; da Rosa, P.P.; Mackmill, L.d.B.; Roll, V.F.B. An assessment of the effectiveness of hyaluronic acid and polyacrylamide hydrogel in horses with osteoarthritis: Systematic review and network meta-analysis. Res. Veter- Sci. 2021, 134, 42–50. [Google Scholar] [CrossRef]
- Henrotin, Y.; Raman, R.; Richette, P.; Bard, H.; Jerosch, J.; Conrozier, T.; Chevalier, X.; Migliore, A. Consensus statement on viscosupplementation with hyaluronic acid for the management of osteoarthritis. Semin. Arthritis Rheum. 2015, 45, 140–149. [Google Scholar] [CrossRef]
- Cooper, C.; Rannou, F.; Richette, P.; Bruyère, O.; Al-Daghri, N.; Altman, R.D.; Brandi, M.L.; Basset, S.C.; Herrero-Beaumont, G.; Migliore, A.; et al. Use of Intraarticular Hyaluronic Acid in the Management of Knee Osteoarthritis in Clinical Practice. Arthritis Care Res. 2017, 69, 1287–1296. [Google Scholar] [CrossRef]
- Rydell, N.W.; Butler, J.; Balazs, E.A. yaluronic acid in synovial fluid: VI. Effect of intra-articular injection of hyaluronic acid on the clinical symptoms of arthritis in track horses. Acta Veterinaria Scandinavica 1970, 11, 139. [Google Scholar] [CrossRef]
- Chen, Z.; Wang, C.; You, D.; Zhao, S.; Zhu, Z.; Xu, M. Platelet-rich plasma versus hyaluronic acid in the treatment of knee osteoarthritis: A meta-analysis. Medicine 2020, 99. [Google Scholar] [CrossRef]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Mechanisms of Action and Efficacy of Hyaluronic Acid, Corticosteroids and Platelet-Rich Plasma in the Treatment of Temporomandibular Joint Osteoarthritis—A Systematic Review. Int. J. Mol. Sci. 2021, 22, 7405. [Google Scholar] [CrossRef]
- Zhao, J.; Huang, H.; Liang, G.; Zeng, L.-F.; Yang, W.; Liu, J. Effects and safety of the combination of platelet-rich plasma (PRP) and hyaluronic acid (HA) in the treatment of knee osteoarthritis: a systematic review and meta-analysis. BMC Musculoskelet. Disord. 2020, 21, 1–12. [Google Scholar] [CrossRef]
- Xu, Z.; He, Z.; Shu, L.; Li, X.; Ma, M.; Ye, C. Intra-Articular Platelet-Rich Plasma Combined With Hyaluronic Acid Injection for Knee Osteoarthritis Is Superior to Platelet-Rich Plasma or Hyaluronic Acid Alone in Inhibiting Inflammation and Improving Pain and Function. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 903–915. [Google Scholar] [CrossRef]
- Dovedytis, M.; Liu, Z.J.; Bartlett, S. Hyaluronic acid and its biomedical applications: A review. Eng. Regen. 2020, 1, 102–113. [Google Scholar] [CrossRef]
- Galarraga, J.H.; Locke, R.C.; E Witherel, C.; Stoeckl, B.D.; Castilho, M.; Mauck, R.L.; Malda, J.; Levato, R.; A Burdick, J. Fabrication of MSC-laden composites of hyaluronic acid hydrogels reinforced with MEW scaffolds for cartilage repair. Biofabrication 2021, 14, 014106. [Google Scholar] [CrossRef] [PubMed]
- Matas, J.; Orrego, M.; Amenabar, D.; Infante, C.; Tapia-Limonchi, R.; Cadiz, M.I.; Alcayaga-Miranda, F.; González, P.L.; Muse, E.; Khoury, M.; et al. Umbilical Cord-Derived Mesenchymal Stromal Cells (MSCs) for Knee Osteoarthritis: Repeated MSC Dosing Is Superior to a Single MSC Dose and to Hyaluronic Acid in a Controlled Randomized Phase I/II Trial. Stem Cells Transl. Med. 2019, 8, 215–224. [Google Scholar] [CrossRef]
- Yang, Y.; Zhu, Z.; Gao, R.; Yuan, J.; Zhang, J.; Li, H.; Xie, Z.; Wang, Y. Controlled release of MSC-derived small extracellular vesicles by an injectable Diels-Alder crosslinked hyaluronic acid/PEG hydrogel for osteoarthritis improvement. Acta Biomater. 2021, 128, 163–174. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, X.; Xu, H.; Xing, Y.; Wu, T.; Sun, X.; Kuang, M.; Ma, X.; Liu, W.; Yang, Q. Wharton's jelly MSC-derived extracellular vehicles—loaded hyaluronic acid-alginate adhesives for treatment of osteoarthritis. J. Mater. Sci. Technol. 2023, 142, 240–252. [Google Scholar] [CrossRef]
- Shekhter, A.B.; Zar, V.V.; Voloshin, V.P.; Lopatin, V.V. issue and cell reaction of the synovial media to intraarticular injection of polymer viscoprosthesis “Noltrex” in experimental conditions. Alm. Clin. Med. 2016, 20–24. [Google Scholar] [CrossRef]
- Christensen, L.; Camitz, L.; Illigen, K.; Hansen, M.; Sarvaa, R.; Conaghan, P. Synovial incorporation of polyacrylamide hydrogel after injection into normal and osteoarthritic animal joints. Osteoarthr. Cartil. 2016, 24, 1999–2002. [Google Scholar] [CrossRef]
- Tnibar, A.; Persson, A.; Jensen, H. Mechanisms of action of an intraarticular 2.5% polyacrylamide hydrogel (Arthramid Vet) in a goat model of osteoarthritis: preliminary observations. SM Journal of Biomedical Engineering 2017, 3, 1022. [Google Scholar]
- Moreau, M.; Rialland, P.; Pelletier, J.-P.; Martel-Pelletier, J.; Lajeunesse, D.; Boileau, C.; Caron, J.; Frank, D.; Lussier, B.; del Castillo, J.R.; et al. Tiludronate treatment improves structural changes and symptoms of osteoarthritis in the canine anterior cruciate ligament model. Arthritis Res. Ther. 2011, 13, R98. [Google Scholar] [CrossRef]
- Fan, T.M.; de Lorimier, L.P.; Charney, S.C.; Hintermeister, J.G. Evaluation of intravenous pamidronate administration in 33 cancer-bearing dogs with primary or secondary bone involvement. Journal of veterinary internal medicine 2005, 19, 74–80. [Google Scholar]
- Richbourg, H.A.; Mitchell, C.F.; Gillett, A.N.; McNulty, M.A. Tiludronate and clodronate do not affect bone structure or remodeling kinetics over a 60 day randomized trial. BMC Veter- Res. 2018, 14, 1–11. [Google Scholar] [CrossRef]
- Tischmacher, A.; Wilford, S.; Allen, K.; Mitchell, R.D.; Parkin, T.; Denoix, J.-M. Retrospective Analysis of the Use of Tiludronate in Equine Practice: Safety on 1804 Horses, Efficacy on 343 Horses. J. Equine Veter- Sci. 2022, 115, 104007. [Google Scholar] [CrossRef]
- Story, M.R.; Haussler, K.K.; Nout-Lomas, Y.S.; Aboellail, T.A.; Kawcak, C.E.; Barrett, M.F.; Frisbie, D.D.; McIlwraith, C.W. Equine Cervical Pain and Dysfunction: Pathology, Diagnosis and Treatment. Animals 2021, 11, 422. [Google Scholar] [CrossRef]
- Denoix, J. .; Thibaud, D.; Riccio, B. Tiludronate as a new therapeutic agent in the treatment of navicular disease: a double-blind placebo-controlled clinical trial. Equine Veter- J. 2003, 35, 407–413. [Google Scholar] [CrossRef]
- Yocom, A.; Contino, E.; Kawcak, C. Review of the Mechanism of Action and Use of Bisphosphonates in Horses. J. Equine Veter- Sci. 2023, 127, 104503. [Google Scholar] [CrossRef]
- Argüelles, D.; Saitua, A.; de Medina, A.S.; Muñoz, J.A.; Muñoz, A. Clinical efficacy of clodronic acid in horses diagnosed with navicular syndrome: A field study using objective and subjective lameness evaluation. Res. Veter- Sci. 2019, 125, 298–304. [Google Scholar] [CrossRef]
- Osborn, M.L.; Cornille, J.L.; Blas-Machado, U.; Uhl, E.W. The equine navicular apparatus as a premier enthesis organ: Functional implications. Veter- Surg. 2021, 50, 713–728. [Google Scholar] [CrossRef]
- Gough, M.R.; Thibaud, D.; Smith, R.K.W. Tiludronate infusion in the treatment of bone spavin: A double blind placebo-controlled trial. Equine Veter- J. 2010, 42, 381–387. [Google Scholar] [CrossRef]
- Dubuc, J. Distal tarsal joints osteoarthritis: Evidence behind bisphosphonates and NSAIDs to improve lameness. Veter- Évid. 2020, 5. [Google Scholar] [CrossRef]
- Soto, S.A.; Barbará, A.C. Bisphosphonates: Pharmacology and Clinical Approach to Their Use in Equine Osteoarticular Diseases. J. Equine Veter- Sci. 2014, 34, 727–737. [Google Scholar] [CrossRef]
- Bertuglia, A.; Basano, I.; Pagliara, E.; Bottegaro, N.B.; Spinella, G.; Bullone, M. Effect of intravenous tiludronate disodium administration on the radiographic progression of osteoarthritis of the fetlock joint in Standardbred racehorses. J. Am. Veter- Med Assoc. 2021, 259, 651–661. [Google Scholar] [CrossRef] [PubMed]
- Vergara-Hernandez, F.B.; Nielsen, B.D.; Colbath, A.C. Is the Use of Bisphosphonates Putting Horses at Risk? An Osteoclast Perspective. Animals 2022, 12, 1722. [Google Scholar] [CrossRef] [PubMed]
- Suva, L.J.; Cooper, A.; Watts, A.E.; Ebetino, F.H.; Price, J.; Gaddy, D. Bisphosphonates in veterinary medicine: The new horizon for use. Bone 2020, 142, 115711. [Google Scholar] [CrossRef]
- Mitchell, A.; Watts, A.E.; Ebetino, F.H.; Suva, L.J. Bisphosphonate use in the horse: what is good and what is not? BMC veterinary research 2019, 15, 1–7. [Google Scholar] [CrossRef]
- Knych, H.K.; Finno, C.J.; Katzman, S.; Ryan, D.; McKemie, D.S.; Kass, P.H.; Arthur, R.M. Clodronate detection and effects on markers of bone resorption are prolonged following a single administration to horses. Equine Veter- J. 2023, 55, 696–706. [Google Scholar] [CrossRef]
- Mama, K.R.; Hector, R.C. Therapeutic developments in equine pain management. Veter- J. 2019, 247, 50–56. [Google Scholar] [CrossRef]
- Krueger, C.R.; Mitchell, C.F.; Leise, B.S.; Knych, H.K. Pharmacokinetics and pharmacodynamics of clodronate disodium evaluated in plasma, synovial fluid and urine. Equine Veter- J. 2020, 52, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Delguste, C.; Amory, H.; Doucet, M.; Piccot-Crézollet, C.; Thibaud, D.; Garnero, P.; Detilleux, J.; Lepage, O. Pharmacological effects of tiludronate in horses after long-term immobilization. Bone 2007, 41, 414–421. [Google Scholar] [CrossRef]
- Kamm, L.; McIlwraith, W.; Kawcak, C. A Review of the Efficacy of Tiludronate in the Horse. J. Equine Veter- Sci. 2008, 28, 209–214. [Google Scholar] [CrossRef]
- Knych, H.K.; Janes, J.; Kennedy, L.; McKemie, D.S.; Arthur, R.M.; Samol, M.A.; Uzal, F.A.; Scollay, M. Detection and residence time of bisphosphonates in bone of horses. J. Veter- Diagn. Investig. 2022, 34, 23–27. [Google Scholar] [CrossRef]
- Ortved, K.F. Regenerative Medicine and Rehabilitation for Tendinous and Ligamentous Injuries in Sport Horses. Veter- Clin. North Am. Equine Pr. 2018, 34, 359–373. [Google Scholar] [CrossRef]
- Fortier, L.A.; Smith, R.K. Regenerative Medicine for Tendinous and Ligamentous Injuries of Sport Horses. Veter- Clin. North Am. Equine Pr. 2008, 24, 191–201. [Google Scholar] [CrossRef]
- Godek, P. Regenerative Medicine and Cell Biology. Regen Med 2022, 1, 1. [Google Scholar]
- Fukuda, K.; Kuwano, A.; Kuroda, T.; Tamura, N.; Mita, H.; Okada, Y.; Kasashima, Y. Optimal double-spin method for maximizing the concentration of platelets in equine platelet-rich plasma. J. Equine Sci. 2020, 31, 105–111. [Google Scholar] [CrossRef]
- Garbin, L.C.; Olver, C.S. Platelet-Rich Products and Their Application to Osteoarthritis. J. Equine Veter- Sci. 2020, 86, 102820. [Google Scholar] [CrossRef]
- Garbin, L.C.; Contino, E.K.; Olver, C.S.; Frisbie, D.D. A safety evaluation of allogeneic freeze-dried platelet-rich plasma or conditioned serum compared to autologous frozen products equivalents in equine healthy joints. BMC Veter- Res. 2022, 18, 141. [Google Scholar] [CrossRef]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef]
- Marques-Smith, P.; Kallerud, A.S.; Johansen, G.M.; Boysen, P.; Jacobsen, A.M.; Reitan, K.M.; Henriksen, M.M.; Löfgren, M.; Fjordbakk, C.T. Is clinical effect of autologous conditioned serum in spontaneously occurring equine articular lameness related to ACS cytokine profile? BMC veterinary research 2020, 16, 1–9. [Google Scholar] [CrossRef]
- Geburek, F.; Lietzau, M.; Beineke, A.; Rohn, K.; Stadler, P.M. Effect of a single injection of autologous conditioned serum (ACS) on tendon healing in equine naturally occurring tendinopathies. Stem Cell Res. Ther. 2015, 6, 1–14. [Google Scholar] [CrossRef]
- Genc, E.; Yuksel, S.; Caglar, A.; Beytemur, O.; Gulec, M.A. Comparison on effects of platelet-rich plasma versus autologous conditioned serum on Achilles tendon healing in a rat model. Acta Orthop. et Traumatol. Turc. 2020, 54, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Fjordbakk, C.T.; Johansen, G.M.; Løvås, A.C.; Oppegård, K.L.; Storset, A.K. Surgical stress influences cytokine content in autologous conditioned serum. Equine Veter- J. 2015, 47, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Stashak, T.S. Adams’ lameness in horses; Verlag M. & H. Schaper: 2008.
- Clegg, P. Differential diagnosis of a swollen hock in the horse. Pr. 2003, 25, 328–341. [Google Scholar] [CrossRef]
- Kümmerle, J.M.; Kummer, M.R. Arthroscopically Accessible Anatomy of the Tarsal Collateral Ligaments in the Horse. Veter- Surg. 2013, 42, 267–274. [Google Scholar] [CrossRef]
- Jindal, K.; Patel, S.; Dhillon, M. The future of injectable orthobiologic substances for knee osteoarthritis: Options beyond platelet-rich plasma. J. Musculoskelet. Surg. Res. 2020, 4, 173. [Google Scholar] [CrossRef]
- Kaneps, A.J. A one-health perspective: use of hemoderivative regenerative therapies in canine and equine patients. J. Am. Veter- Med Assoc. 2023, 261, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Linardi, R.L.; Dodson, M.E.; Moss, K.L.; King, W.J.; Ortved, K.F. The Effect of Autologous Protein Solution on the Inflammatory Cascade in Stimulated Equine Chondrocytes. Front. Veter- Sci. 2019, 6, 64. [Google Scholar] [CrossRef]
- Garbin, L.C.; Morris, M.J. A Comparative Review of Autologous Conditioned Serum and Autologous Protein Solution for Treatment of Osteoarthritis in Horses. Front. Veter- Sci. 2021, 8. [Google Scholar] [CrossRef]
- Soontararak, S.; Ardaum, P.; Senarat, N.; Yangtara, S.; Lekcharoensuk, C.; Putchong, I.; Kashemsant, N.; Vijarnsorn, M.; Chow, L.; Dow, S.; et al. In Vitro Anti-Inflammatory and Regenerative Effects of Autologous Conditioned Serum from Dogs with Osteoarthritis. Animals 2022, 12, 2717. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, E.; Ruggeri, M.; Rossi, S.; Vigani, B.; Miele, D.; Bonferoni, M.C.; Sandri, G.; Ferrari, F. Innovative Strategies in Tendon Tissue Engineering. Pharmaceutics 2021, 13, 89. [Google Scholar] [CrossRef] [PubMed]
- Gaesser, A.M.; Underwood, C.; Linardi, R.L.; Even, K.M.; Reef, V.B.; Shetye, S.S.; Mauck, R.L.; King, W.J.; Engiles, J.B.; Ortved, K.F. Evaluation of Autologous Protein Solution Injection for Treatment of Superficial Digital Flexor Tendonitis in an Equine Model. Front. Veter- Sci. 2021, 8. [Google Scholar] [CrossRef]
- Geburek, F.; Gaus, M.; van Schie, H.T.M.; Rohn, K.; Stadler, P.M. Effect of intralesional platelet-rich plasma (PRP) treatment on clinical and ultrasonographic parameters in equine naturally occurring superficial digital flexor tendinopathies – a randomized prospective controlled clinical trial. BMC Veter- Res. 2016, 12, 1–16. [Google Scholar] [CrossRef]
- Peng, C.; Yang, L.; Labens, R.; Gao, Y.; Zhu, Y.; Li, J. A systematic review and meta-analysis of the efficacy of platelet-rich plasma products for treatment of equine joint disease. Equine Veter- J. 2024. [Google Scholar] [CrossRef]
- Abu-Seida, A.M. Regenerative Therapy for Equine Osteoarthritis: A Concise Review. Asian J. Anim. Veter- Adv. 2015, 10, 500–508. [Google Scholar] [CrossRef]
- Pereira, R.C.d.F.; De La Côrte, F.D.; Brass, K.E.; Azevedo, M.d.S.; Gallio, M.; Cantarelli, C.; Dau, S.L.; Cezar, A.S.; Inkelmann, M.A. Evaluation of Three Methods of Platelet-Rich Plasma for Treatment of Equine Distal Limb Skin Wounds. J. Equine Veter- Sci. 2019, 72, 1–7. [Google Scholar] [CrossRef]
- Gottschall, J.; Johnston, V.L.; Rzad, L.; Anderson, A.J.; Aster, R. Importance of white blood cells in platelet storage. Vox sanguinis 1984, 47, 101–107. [Google Scholar] [CrossRef]
- E Giraldo, C.; López, C.; E Álvarez, M.; Samudio, I.J.; Prades, M.; Carmona, J.U. Effects of the breed, sex and age on cellular content and growth factor release from equine pure-platelet rich plasma and pure-platelet rich gel. BMC Veter- Res. 2013, 9, 1–10. [Google Scholar] [CrossRef]
- McCarrel, T.M. Equine Platelet-Rich Plasma. Veterinary Clinics: Equine Practice 2023, 39, 429–442. [Google Scholar] [CrossRef]
- Garbin, L.C.; Lopez, C.; Carmona, J.U. A Critical Overview of the Use of Platelet-Rich Plasma in Equine Medicine Over the Last Decade. Front. Veter- Sci. 2021, 8. [Google Scholar] [CrossRef]
- Bosch, G.; van Schie, H.T.; de Groot, M.W.; Cadby, J.A.; van de Lest, C.H.; Barneveld, A.; van Weeren, P.R. Effects of platelet-rich plasma on the quality of repair of mechanically induced core lesions in equine superficial digital flexor tendons: a placebo-controlled experimental study. Journal of orthopaedic research 2010, 28, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Bosch, G.; Moleman, M.; Barneveld, A.; van Weeren, P.R.; van Schie, H.T.M. The effect of platelet-rich plasma on the neovascularization of surgically created equine superficial digital flexor tendon lesions. Scand. J. Med. Sci. Sports 2011, 21, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, K.; Nuovo, G.; Bertone, A. In vivo reduction or blockade of interleukin-1β in primary osteoarthritis influences expression of mediators implicated in pathogenesis. Osteoarthr. Cartil. 2012, 20, 1610–1618. [Google Scholar] [CrossRef] [PubMed]
- Hopper, S.A. Regenerative Medicine–Under-standing IRAP, PRP and stem cell Therapies. Rood and Riddle 2015.
- Crawford, D.C.; Miller, L.E.; Block, J.E. Conservative management of symptomatic knee osteoarthritis: a flawed strategy? Orthopedic reviews 2013, 5. [Google Scholar]
- Rönn, K.; Reischl, N.; Gautier, E.; Jacobi, M. Current Surgical Treatment of Knee Osteoarthritis. Arthritis 2011, 2011, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Genç, E.; Beytemur, O.; Yuksel, S.; Eren, Y.; Çağlar, A.; Küçükyıldırım, B.O.; Güleç, M.A. Investigation of the biomechanical and histopathological effects of autologous conditioned serum on healing of Achilles tendon. Acta Orthop. et Traumatol. Turc. 2018, 52, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Bertone, A.L.; Ishihara, A.; Zekas, L.J.; Wellman, M.L.; Lewis, K.B.; Schwarze, R.A.; Barnaba, A.R.; Schmall, M.L.; Kanter, P.M.; Genovese, R.L. Evaluation of a single intra-articular injection of autologous protein solution for treatment of osteoarthritis in horses. Am. J. Vet. Res. 2014, 75, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Ortved, K.F. Equine Autologous Conditioned Serum and Autologous Protein Solution. Veter- Clin. North Am. Equine Pr. 2023, 39, 443–451. [Google Scholar] [CrossRef]
- Knott, L.E.; Fonseca-Martinez, B.A.; O'Connor, A.M.; Goodrich, L.R.; McIlwraith, C.W.; Colbath, A.C. Current use of biologic therapies for musculoskeletal disease: A survey of board-certified equine specialists. Veter- Surg. 2022, 51, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, A.V.; Boone, L.H.; Braim, A.P.; Taintor, J.S.; Caldwell, F.; Wright, J.C.; Wooldridge, A.A. A Survey of Clinical Usage of Non-steroidal Intra-Articular Therapeutics by Equine Practitioners. Front. Veter- Sci. 2020, 7, 579967. [Google Scholar] [CrossRef]
- Wang, S.; Wei, X.; Zhou, J.; Zhang, J.; Li, K.; Chen, Q.; Terek, R.; Fleming, B.C.; Goldring, M.B.; Ehrlich, M.G. Identification of α2-macroglobulin as a master inhibitor of cartilage-degrading factors that attenuates the progression of posttraumatic osteoarthritis. Arthritis & rheumatology 2014, 66, 1843–1853. [Google Scholar] [CrossRef]
- Zhu, M.; Zhao, B.; Wei, L.; Wang, S. alpha-2-Macroglobulin, a Native and Powerful Proteinase Inhibitor, Prevents Cartilage Degeneration Disease by Inhibiting Majority of Catabolic Enzymes and Cytokines. Curr. Mol. Biol. Rep. 2021, 7, 1–7. [Google Scholar] [CrossRef]
- Li, S.; Xiang, C.; Wei, X.; Sun, X.; Li, R.; Li, P.; Sun, J.; Wei, D.; Chen, Y.; Zhang, Y.; et al. Early supplemental α2-macroglobulin attenuates cartilage and bone damage by inhibiting inflammation in collagen II-induced arthritis model. Int. J. Rheum. Dis. 2019, 22, 654–665. [Google Scholar] [CrossRef]
- Szponder, T.; Latalski, M.; Danielewicz, A.; Krać, K.; Kozera, A.; Drzewiecka, B.; Nguyen Ngoc, D.; Dobko, D.; Wessely-Szponder, J. Osteoarthritis: pathogenesis, animal models, and new regenerative therapies. Journal of Clinical Medicine 2022, 12, 5. [Google Scholar] [CrossRef]
- Velloso Alvarez, A.; Boone, L.H.; Pondugula, S.R.; Caldwell, F.; Wooldridge, A.A. Effects of autologous conditioned serum, autologous protein solution, and triamcinolone on inflammatory and catabolic gene expression in equine cartilage and synovial explants treated with IL-1β in co-culture. Frontiers in veterinary science 2020, 7, 323. [Google Scholar] [CrossRef]
- Tokawa, P.K.A.; Brossi, P.M.; Baccarin, R.Y.A. Autologous conditioned serum in equine and human orthopedic therapy: A systematic review. Res. Veter- Sci. 2022, 146, 34–52. [Google Scholar] [CrossRef] [PubMed]
- Hraha, T.H.; Doremus, K.M.; McILWRAITH, C.W.; Frisbie, D.D. Autologous conditioned serum: The comparative cytokine profiles of two commercial methods (IRAP and IRAP II) using equine blood. Equine Veter- J. 2011, 43, 516–521. [Google Scholar] [CrossRef]
- Lasarzik, J.; Bondzio, A.; Rettig, M.; Estrada, R.; Klaus, C.; Ehrle, A.; Einspanier, R.; Lischer, C.J. Evaluation of Two Protocols Using Autologous Conditioned Serum for Intra-articular Therapy of Equine Osteoarthritis—A Pilot Study Monitoring Cytokines and Cartilage-Specific Biomarkers. J. Equine Veter- Sci. 2018, 60, 35–42. [Google Scholar] [CrossRef]
- Voga, M.; Adamic, N.; Vengust, M.; Majdic, G. Stem Cells in Veterinary Medicine—Current State and Treatment Options. Front. Veter- Sci. 2020, 7, 278. [Google Scholar] [CrossRef]
- Prockop, D.J.; Oh, J.Y. Medical therapies with adult stem/progenitor cells (MSCs): A backward journey from dramatic results in vivo to the cellular and molecular explanations. J. Cell. Biochem. 2012, 113, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.I. Mesenchymal stem cells: time to change the name! Stem cells translational medicine 2017, 6, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.-C.; Kim, H.-S.; Shin, T.-H.; Kang, I.; Lee, J.Y.; Kim, J.-J.; Kang, H.K.; Seo, Y.; Lee, S.; Yu, K.-R.; et al. PGE2 maintains self-renewal of human adult stem cells via EP2-mediated autocrine signaling and its production is regulated by cell-to-cell contact. Sci. Rep. 2016, 6, 26298. [Google Scholar] [CrossRef]
- Margiana, R.; Markov, A.; Zekiy, A.O.; Hamza, M.U.; Al-Dabbagh, K.A.; Al-Zubaidi, S.H.; Hameed, N.M.; Ahmad, I.; Sivaraman, R.; Kzar, H.H.; et al. Clinical application of mesenchymal stem cell in regenerative medicine: a narrative review. Stem Cell Res. Ther. 2022, 13, 1–22. [Google Scholar] [CrossRef]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.C.; Krause, D.S.; Deans, R.J.; Keating, A.; Prockop, D.J.; Horwitz, E.M. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Vizoso, F.J.; Eiro, N.; Cid, S.; Schneider, J.; Perez-Fernandez, R. Mesenchymal Stem Cell Secretome: Toward Cell-Free Therapeutic Strategies in Regenerative Medicine. Int. J. Mol. Sci. 2017, 18, 1852. [Google Scholar] [CrossRef]
- Reis, I.L.; Lopes, B.; Sousa, P.; Sousa, A.C.; Branquinho, M.; Caseiro, A.R.; Pedrosa, S.S.; Rêma, A.; Oliveira, C.; Porto, B.; et al. Allogenic Synovia-Derived Mesenchymal Stem Cells for Treatment of Equine Tendinopathies and Desmopathies—Proof of Concept. Animals 2023, 13, 1312. [Google Scholar] [CrossRef]
- Colbath, A.C.; Dow, S.W.; Phillips, J.N.; McIlwraith, C.W.; Goodrich, L.R. Autologous and Allogeneic Equine Mesenchymal Stem Cells Exhibit Equivalent Immunomodulatory Properties In Vitro. Stem Cells Dev. 2017, 26, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Reis, I.L.; Lopes, B.; Sousa, P.; Sousa, A.C.; Branquinho, M.V.; Caseiro, A.R.; Rêma, A.; Briote, I.; Mendonça, C.M.; Santos, J.M.; et al. Treatment of Equine Tarsus Long Medial Collateral Ligament Desmitis with Allogenic Synovial Membrane Mesenchymal Stem/Stromal Cells Enhanced by Umbilical Cord Mesenchymal Stem/Stromal Cell-Derived Conditioned Medium: Proof of Concept. Animals 2024, 14, 370. [Google Scholar] [CrossRef] [PubMed]
- Reis, I.; Lopes, B.; Sousa, P.; Sousa, A.; Caseiro, A.R.; Briote, I.; Rocha, A.M.; Pereira, J.; Mendonça, C.; Santos, J. Equine Metacarpophalangeal Joint Partial and Full Thickness Defects Treated with Allogenic Equine Synovial Membrane Mesenchymal Stem/Stromal Cell and Umbilical Cord Mesenchymal Stem/Stromal Cell Conditioned Medium: The Proof-of-Concept. 2024.
- Iijima, H.; Isho, T.; Kuroki, H.; Takahashi, M.; Aoyama, T. Effectiveness of mesenchymal stem cells for treating patients with knee osteoarthritis: a meta-analysis toward the establishment of effective regenerative rehabilitation. npj Regen. Med. 2018, 3, 15. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.M.; Kalamegam, G.; Pushparaj, P.N.; Matta, C.; Memic, A.; Khademhosseini, A.; Mobasheri, R.; Poletti, F.L.; Hoyland, J.A.; Mobasheri, A. Mesenchymal stem cells in regenerative medicine: Focus on articular cartilage and intervertebral disc regeneration. Methods 2016, 99, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Ouyang, H.; Dass, C.R.; Xu, J. Current research on pharmacologic and regenerative therapies for osteoarthritis. Bone Res. 2016, 4, 15040. [Google Scholar] [CrossRef] [PubMed]
- Im, G.-I.; Shin, Y.-W.; Lee, K.-B. Do adipose tissue-derived mesenchymal stem cells have the same osteogenic and chondrogenic potential as bone marrow-derived cells? Osteoarthritis and cartilage 2005, 13, 845–853. [Google Scholar] [CrossRef]
- Huang, Y.-Z.; Xie, H.-Q.; Silini, A.; Parolini, O.; Zhang, Y.; Deng, L.; Huang, Y.-C. Mesenchymal Stem/Progenitor Cells Derived from Articular Cartilage, Synovial Membrane and Synovial Fluid for Cartilage Regeneration: Current Status and Future Perspectives. Stem Cell Rev. Rep. 2017, 13, 575–586. [Google Scholar] [CrossRef]
- Song, Y.; Du, H.; Dai, C.; Zhang, L.; Li, S.; Hunter, D.J.; Lu, L.; Bao, C. Human adipose-derived mesenchymal stem cells for osteoarthritis: a pilot study with long-term follow-up and repeated injections. Regen. Med. 2018, 13, 295–307. [Google Scholar] [CrossRef]
- Terada, N.; Hamazaki, T.; Oka, M.; Hoki, M.; Mastalerz, D.M.; Nakano, Y.; Meyer, E.M.; Morel, L.; Petersen, B.E.; Scott, E.W. Bone marrow cells adopt the phenotype of other cells by spontaneous cell fusion. Nature 2002, 416, 542–545. [Google Scholar] [CrossRef]
- Konno, M.; Hamabe, A.; Hasegawa, S.; Ogawa, H.; Fukusumi, T.; Nishikawa, S.; Ohta, K.; Kano, Y.; Ozaki, M.; Noguchi, Y.; et al. Adipose-derived mesenchymal stem cells and regenerative medicine. Dev. Growth Differ. 2013, 55, 309–318. [Google Scholar] [CrossRef]
- Lee, W.-S.; Kim, H.J.; Kim, K.-I.; Kim, G.B.; Jin, W. Intra-Articular Injection of Autologous Adipose Tissue-Derived Mesenchymal Stem Cells for the Treatment of Knee Osteoarthritis: A Phase IIb, Randomized, Placebo-Controlled Clinical Trial. Stem Cells Transl. Med. 2019, 8, 504–511. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Sekiya, I.; Yagishita, K.; Muneta, T. Comparison of human stem cells derived from various mesenchymal tissues: Superiority of synovium as a cell source. Arthritis Rheum. 2005, 52, 2521–2529. [Google Scholar] [CrossRef] [PubMed]
- To, K.; Zhang, B.; Romain, K.; Mak, C.; Khan, W. Synovium-Derived Mesenchymal Stem Cell Transplantation in Cartilage Regeneration: A PRISMA Review of in vivo Studies. Front. Bioeng. Biotechnol. 2019, 7, 314. [Google Scholar] [CrossRef] [PubMed]
- Zupan, J.; Drobnič, M.; Stražar, K. Synovium-derived mesenchymal stem/stromal cells and their promise for cartilage regeneration. Cell Biology and Translational Medicine, Volume 6: Stem Cells: Their Heterogeneity, Niche and Regenerative Potential 2020, 87-106.
- Kondo, S.; Muneta, T.; Nakagawa, Y.; Koga, H.; Watanabe, T.; Tsuji, K.; Sotome, S.; Okawa, A.; Kiuchi, S.; Ono, H.; et al. Transplantation of autologous synovial mesenchymal stem cells promotes meniscus regeneration in aged primates. J. Orthop. Res. 2017, 35, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, Y.; Kim, H.; Hwang, K.J.; Kwon, H.C.; Kim, S.K.; Cho, D.J.; Kang, S.G.; You, J. Human amniotic fluid-derived stem cells have characteristics of multipotent stem cells. Cell Prolif. 2007, 40, 75–90. [Google Scholar] [CrossRef]
- De Coppi, P.; Bartsch Jr, G.; Siddiqui, M.M.; Xu, T.; Santos, C.C.; Perin, L.; Mostoslavsky, G.; Serre, A.C.; Snyder, E.Y.; Yoo, J.J. Isolation of amniotic stem cell lines with potential for therapy. Nature biotechnology 2007, 25, 100–106. [Google Scholar] [CrossRef]
- Davies, J.E.; Walker, J.T.; Keating, A. Concise review: Wharton’s jelly: the rich, but enigmatic, source of mesenchymal stromal cells. Stem cells translational medicine 2017, 6, 1620–1630. [Google Scholar] [CrossRef]
- Anzalone, R.; Iacono, M.L.; Corrao, S.; Magno, F.; Loria, T.; Cappello, F.; Zummo, G.; Farina, F.; La Rocca, G. New Emerging Potentials for Human Wharton’s Jelly Mesenchymal Stem Cells: Immunological Features and Hepatocyte-Like Differentiative Capacity. Stem Cells Dev. 2010, 19, 423–438. [Google Scholar] [CrossRef]
- Jiang, S.; Tian, G.; Yang, Z.; Gao, X.; Wang, F.; Li, J.; Tian, Z.; Huang, B.; Wei, F.; Sang, X.; et al. Enhancement of acellular cartilage matrix scaffold by Wharton's jelly mesenchymal stem cell-derived exosomes to promote osteochondral regeneration. Bioact. Mater. 2021, 6, 2711–2728. [Google Scholar] [CrossRef]
- Abbaszadeh, H.; Ghorbani, F.; Derakhshani, M.; Movassaghpour, A.A.; Yousefi, M.; Talebi, M.; Shamsasenjan, K. Regenerative potential of Wharton's jelly-derived mesenchymal stem cells: A new horizon of stem cell therapy. J. Cell. Physiol. 2020, 235, 9230–9240. [Google Scholar] [CrossRef]
- Thitiset, T.; Damrongsakkul, S.; Yodmuang, S.; Leeanansaksiri, W.; Apinun, J.; Honsawek, S. A novel gelatin/chitooligosaccharide/demineralized bone matrix composite scaffold and periosteum-derived mesenchymal stem cells for bone tissue engineering. Biomater. Res. 2021, 25, 19. [Google Scholar] [CrossRef]
- Moon, D.K.; Kim, B.G.; Lee, A.R.; Choe, Y.I.; Khan, I.; Moon, K.M.; Jeon, R.-H.; Byun, J.-H.; Hwang, S.-C.; Woo, D.K. Resveratrol can enhance osteogenic differentiation and mitochondrial biogenesis from human periosteum-derived mesenchymal stem cells. J. Orthop. Surg. Res. 2020, 15, 1–10. [Google Scholar] [CrossRef]
- Masuda, K.; Han, X.; Kato, H.; Sato, H.; Zhang, Y.; Sun, X.; Hirofuji, Y.; Yamaza, H.; Yamada, A.; Fukumoto, S. Dental Pulp-Derived Mesenchymal Stem Cells for Modeling Genetic Disorders. Int. J. Mol. Sci. 2021, 22, 2269. [Google Scholar] [CrossRef]
- Caseiro, A.R.; Pedrosa, S.S.; Ivanova, G.; Branquinho, M.V.; Almeida, A.; Faria, F.; Amorim, I.; Pereira, T.; Maurício, A.C. Mesenchymal Stem/ Stromal Cells metabolomic and bioactive factors profiles: A comparative analysis on the umbilical cord and dental pulp derived Stem/ Stromal Cells secretome. PLOS ONE 2019, 14, e0221378. [Google Scholar] [CrossRef]
- Kern, S.; Eichler, H.; Stoeve, J.; Klüter, H.; Bieback, K. Comparative Analysis of Mesenchymal Stem Cells from Bone Marrow, Umbilical Cord Blood, or Adipose Tissue. Stem Cells 2006, 24, 1294–1301. [Google Scholar] [CrossRef]
- Jin, H.J.; Bae, Y.K.; Kim, M.; Kwon, S.-J.; Jeon, H.B.; Choi, S.J.; Kim, S.W.; Yang, Y.S.; Oh, W.; Chang, J.W. Comparative Analysis of Human Mesenchymal Stem Cells from Bone Marrow, Adipose Tissue, and Umbilical Cord Blood as Sources of Cell Therapy. Int. J. Mol. Sci. 2013, 14, 17986–18001. [Google Scholar] [CrossRef] [PubMed]
- Čamernik, K.; Mihelič, A.; Mihalič, R.; Presen, D.M.; Janež, A.; Trebše, R.; Marc, J.; Zupan, J. Skeletal-muscle-derived mesenchymal stem/stromal cells from patients with osteoarthritis show superior biological properties compared to bone-derived cells. Stem Cell Res. 2019, 38, 101465. [Google Scholar] [CrossRef] [PubMed]
- Godwin, E.E.; Young, N.J.; Dudhia, J.; Beamish, I.C.; Smith, R.K.W. Implantation of bone marrow-derived mesenchymal stem cells demonstrates improved outcome in horses with overstrain injury of the superficial digital flexor tendon. Equine Veter- J. 2012, 44, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Costa-Almeida, R.; Calejo, I.; Gomes, M.E. Mesenchymal Stem Cells Empowering Tendon Regenerative Therapies. Int. J. Mol. Sci. 2019, 20, 3002. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, C.S.; E Saether, E.; Vanderby, R.; Aktas, E. Mesenchymal Stem Cell Therapy on Tendon/Ligament Healing. J. Cytokine Biol. 2017, 2, 1–3. [Google Scholar] [CrossRef]
- Lee, J.Y.; Zhou, Z.; Taub, P.J.; Ramcharan, M.; Li, Y.; Akinbiyi, T.; Maharam, E.R.; Leong, D.J.; Laudier, D.M.; Ruike, T.; et al. BMP-12 Treatment of Adult Mesenchymal Stem Cells In Vitro Augments Tendon-Like Tissue Formation and Defect Repair In Vivo. PLOS ONE 2011, 6, e17531. [Google Scholar] [CrossRef] [PubMed]
- Docheva, D.; Müller, S.A.; Majewski, M.; Evans, C.H. Biologics for tendon repair. Advanced drug delivery reviews 2015, 84, 222–239. [Google Scholar] [CrossRef]
- Yea, J.-H.; Kim, Y.; Jo, C.H. Comparison of mesenchymal stem cells from bone marrow, umbilical cord blood, and umbilical cord tissue in regeneration of a full-thickness tendon defect in vitro and in vivo. Biochem. Biophys. Rep. 2023, 34, 101486. [Google Scholar] [CrossRef]
- Burk, J.; Gittel, C.; Heller, S.; Pfeiffer, B.; Paebst, F.; Ahrberg, A.B.; Brehm, W. Gene expression of tendon markers in mesenchymal stromal cells derived from different sources. BMC Res. Notes 2014, 7, 1–6. [Google Scholar] [CrossRef]
- Conze, P.; van Schie, H.T.; van Weeren, R.; Staszyk, C.; Conrad, S.; Skutella, T.; Hopster, K.; Rohn, K.; Stadler, P.; Geburek, F. Effect of autologous adipose tissue-derived mesenchymal stem cells on neovascularization of artificial equine tendon lesions. Regen. Med. 2014, 9, 743–757. [Google Scholar] [CrossRef]
- Archer, C.W.; Dowthwaite, G.P.; Francis-West, P. Development of synovial joints. Birth Defects Research Part C: Embryo Today: Reviews 2003, 69, 144–155. [Google Scholar] [CrossRef]
- Koyama, E.; Shibukawa, Y.; Nagayama, M.; Sugito, H.; Young, B.; Yuasa, T.; Okabe, T.; Ochiai, T.; Kamiya, N.; Rountree, R.B.; et al. A distinct cohort of progenitor cells participates in synovial joint and articular cartilage formation during mouse limb skeletogenesis. Dev. Biol. 2008, 316, 62–73. [Google Scholar] [CrossRef]
- Zha, K.; Li, X.; Yang, Z.; Tian, G.; Sun, Z.; Sui, X.; Dai, Y.; Liu, S.; Guo, Q. Heterogeneity of mesenchymal stem cells in cartilage regeneration: from characterization to application. npj Regen. Med. 2021, 6, 14. [Google Scholar] [CrossRef]
- Lam, A.T.; Reuveny, S.; Oh, S.K.-W. Human mesenchymal stem cell therapy for cartilage repair: Review on isolation, expansion, and constructs. Stem Cell Res. 2020, 44, 101738. [Google Scholar] [CrossRef]
- Richter, W. Mesenchymal stem cells and cartilage in situ regeneration. J. Intern. Med. 2009, 266, 390–405. [Google Scholar] [CrossRef]
- Grande, D.A.; Southerland, S.S.; Manji, R.; Pate, D.W.; Schwartz, R.E.; Lucas, P.A. Repair of Articular Cartilage Defects Using Mesenchymal Stem Cells. Tissue Eng. 1995, 1, 345–353. [Google Scholar] [CrossRef]
- Otto, W.R.; Rao, J. Tomorrow's skeleton staff: mesenchymal stem cells and the repair of bone and cartilage. Cell Prolif. 2004, 37, 97–110. [Google Scholar] [CrossRef]
- Koga, H.; Muneta, T.; Nagase, T.; Nimura, A.; Ju, Y.-J.; Mochizuki, T.; Sekiya, I. Comparison of mesenchymal tissues-derived stem cells for in vivo chondrogenesis: suitable conditions for cell therapy of cartilage defects in rabbit. Cell Tissue Res. 2008, 333, 207–215. [Google Scholar] [CrossRef]
- Yoshimura, H.; Muneta, T.; Nimura, A.; Yokoyama, A.; Koga, H.; Sekiya, I. Comparison of rat mesenchymal stem cells derived from bone marrow, synovium, periosteum, adipose tissue, and muscle. Cell Tissue Res. 2007, 327, 449–462. [Google Scholar] [CrossRef]
- Jones, B.A.; Pei, M. Synovium-Derived Stem Cells: A Tissue-Specific Stem Cell for Cartilage Engineering and Regeneration. Tissue Eng. Part B: Rev. 2012, 18, 301–311. [Google Scholar] [CrossRef]
- Hassanzadeh, A.; Vousooghi, N.; Rahimnia, R.; Razeghian, E.; Rajaeian, S.; Seyhoun, I.; Sharif, S.; Verdi, J. Recent advances in mesenchymal stem/stromal cells (MSCs)-based approaches for osteoarthritis (OA) therapy. Cell Biol. Int. 2023, 47, 1033–1048. [Google Scholar] [CrossRef] [PubMed]
- Granero-Molto, F.; A Weis, J.; Longobardi, L.; Spagnoli, A.; D, P. ; Bs; Md Role of mesenchymal stem cells in regenerative medicine: application to bone and cartilage repair. Expert Opin. Biol. Ther. 2008, 8, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Stanford, W.L.; Kandel, R.A. Mesenchymal stem and progenitor cells for cartilage repair. Skelet. Radiol. 2007, 36, 909–912. [Google Scholar] [CrossRef] [PubMed]
- Kubosch, E.J.; Lang, G.; Furst, D.; Kubosch, D.; Izadpanah, K.; Rolauffs, B.; Sudkamp, N.P.; Schmal, H. The Potential for Synovium-derived Stem Cells in Cartilage Repair. Curr. Stem Cell Res. Ther. 2018, 13, 174–184. [Google Scholar] [CrossRef]
- Mochizuki, T.; Muneta, T.; Sakaguchi, Y.; Nimura, A.; Yokoyama, A.; Koga, H.; Sekiya, I. Higher chondrogenic potential of fibrous synovium– and adipose synovium–derived cells compared with subcutaneous fat–derived cells: Distinguishing properties of mesenchymal stem cells in humans. Arthritis Rheum. 2006, 54, 843–853. [Google Scholar] [CrossRef]
- Koga, H.; Muneta, T.; Ju, Y.-J.; Nagase, T.; Nimura, A.; Mochizuki, T.; Ichinose, S.; von der Mark, K.; Sekiya, I. Synovial Stem Cells Are Regionally Specified According to Local Microenvironments After Implantation for Cartilage Regeneration. Stem Cells 2006, 25, 689–696. [Google Scholar] [CrossRef]
- De Bari, C.; Dell’Accio, F.; Tylzanowski, P.; Luyten, F.P. Multipotent mesenchymal stem cells from adult human synovial membrane. Arthritis Rheum. 2001, 44, 1928–1942. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Tuan, R.S. Transdifferentiation potential of human mesenchymal stem cells derived from bone marrow. FASEB J. 2004, 18, 980–982. [Google Scholar] [CrossRef]
- Prockop, D.J.; Gregory, C.A.; Spees, J.L. One strategy for cell and gene therapy: Harnessing the power of adult stem cells to repair tissues. Proc. Natl. Acad. Sci. 2003, 100, 11917–11923. [Google Scholar] [CrossRef]
- Zha, K.; Sun, Z.; Yang, Y.; Chen, M.; Gao, C.; Fu, L.; Li, H.; Sui, X.; Guo, Q.; Liu, S. Recent Developed Strategies for Enhancing Chondrogenic Differentiation of MSC: Impact on MSC-Based Therapy for Cartilage Regeneration. Stem Cells Int. 2021, 2021, 1–15. [Google Scholar] [CrossRef]
- Sadlik, B.; Jaroslawski, G.; Puszkarz, M.; Blasiak, A.; Oldak, T.; Gladysz, D.; Whyte, G.P. Cartilage Repair in the Knee Using Umbilical Cord Wharton's Jelly–Derived Mesenchymal Stem Cells Embedded Onto Collagen Scaffolding and Implanted Under Dry Arthroscopy. Arthrosc. Tech. 2018, 7, e57–e63. [Google Scholar] [CrossRef]
- Liu, T.P.; Ha, P.; Xiao, C.Y.; Kim, S.Y.; Jensen, A.R.; Easley, J.; Yao, Q.; Zhang, X. Updates on mesenchymal stem cell therapies for articular cartilage regeneration in large animal models. Front. Cell Dev. Biol. 2022, 10, 982199. [Google Scholar] [CrossRef]
- Xiang, X.-N.; Zhu, S.-Y.; He, H.-C.; Yu, X.; Xu, Y.; He, C.-Q. Mesenchymal stromal cell-based therapy for cartilage regeneration in knee osteoarthritis. Stem Cell Res. Ther. 2022, 13, 1–20. [Google Scholar] [CrossRef] [PubMed]
- De La Garza-Rodea, A.S.; Van Der Velde-Van Dijke, I.; Boersma, H.; Gonçalves, M.A.; Van Bekkum, D.W.; De Vries, A.A.; Knaän-Shanzer, S. Myogenic properties of human mesenchymal stem cells derived from three different sources. Cell transplantation 2012, 21, 153–173. [Google Scholar] [CrossRef]
- Kim, J.; Park, J.; Song, S.-Y.; Kim, E. Advanced Therapy medicinal products for autologous chondrocytes and comparison of regulatory systems in target countries. Regen. Ther. 2022, 20, 126–137. [Google Scholar] [CrossRef]
- Carballo, C.B.; Nakagawa, Y.; Sekiya, I.; Rodeo, S.A. Basic Science of Articular Cartilage. Clin. Sports Med. 2017, 36, 413–425. [Google Scholar] [CrossRef]
- Welch, T.; Mandelbaum, B.; Tom, M. Autologous chondrocyte implantation: past, present, and future. Sports medicine and arthroscopy review 2016, 24, 85–91. [Google Scholar] [CrossRef]
- Xia, J.; Minamino, S.; Kuwabara, K.; Arai, S. Stem cell secretome as a new booster for regenerative medicine. Biosci. Trends 2019, 13, 299–307. [Google Scholar] [CrossRef]
- Daneshmandi, L.; Shah, S.; Jafari, T.; Bhattacharjee, M.; Momah, D.; Saveh-Shemshaki, N.; Lo, K.W.-H.; Laurencin, C.T. Emergence of the Stem Cell Secretome in Regenerative Engineering. Trends Biotechnol. 2020, 38, 1373–1384. [Google Scholar] [CrossRef]
- Djatche, W.H.B.; Zhu, H.; Ma, W.; Li, Y.; Li, Z.; Zhao, H.; Liu, Z.; Qiao, H. Potential of mesenchymal stem cell-derived conditioned medium/secretome as a therapeutic option for ocular diseases. Regen. Med. 2023, 18, 795–807. [Google Scholar] [CrossRef]
- Pawitan, J.A. Prospect of Stem Cell Conditioned Medium in Regenerative Medicine. BioMed Res. Int. 2014, 2014, 965849. [Google Scholar] [CrossRef] [PubMed]
- Jafarinia, M.; Alsahebfosoul, F.; Salehi, H.; Eskandari, N.; Ganjalikhani-Hakemi, M. Mesenchymal Stem Cell-Derived Extracellular Vesicles: A Novel Cell-Free Therapy. Immunol. Investig. 2020, 49, 758–780. [Google Scholar] [CrossRef]
- Yu, H.; Cheng, J.; Shi, W.; Ren, B.; Zhao, F.; Shi, Y.; Yang, P.; Duan, X.; Zhang, J.; Fu, X.; et al. Bone marrow mesenchymal stem cell-derived exosomes promote tendon regeneration by facilitating the proliferation and migration of endogenous tendon stem/progenitor cells. Acta Biomater. 2020, 106, 328–341. [Google Scholar] [CrossRef]
- Kou, M.; Huang, L.; Yang, J.; Chiang, Z.; Chen, S.; Liu, J.; Guo, L.; Zhang, X.; Zhou, X.; Xu, X. Mesenchymal stem cell-derived extracellular vesicles for immunomodulation and regeneration: a next generation therapeutic tool? Cell Death & Disease 2022, 13, 580. [Google Scholar]
- Kwon, S.; Shin, S.; Do, M.; Oh, B.H.; Song, Y.; Bui, V.D.; Lee, E.S.; Jo, D.-G.; Cho, Y.W.; Kim, D.-H.; et al. Engineering approaches for effective therapeutic applications based on extracellular vesicles. J. Control. Release 2021, 330, 15–30. [Google Scholar] [CrossRef]
- Mebarki, M.; Abadie, C.; Larghero, J.; Cras, A. Human umbilical cord-derived mesenchymal stem/stromal cells: a promising candidate for the development of advanced therapy medicinal products. Stem Cell Res. Ther. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Ni, Z.; Zhou, S.; Li, S.; Kuang, L.; Chen, H.; Luo, X.; Ouyang, J.; He, M.; Du, X.; Chen, L. Exosomes: Roles and therapeutic potential in osteoarthritis. Bone Res. 2020, 8, 25. [Google Scholar] [CrossRef]
- Fan, W.-J.; Liu, D.; Pan, L.-Y.; Wang, W.-Y.; Ding, Y.-L.; Zhang, Y.-Y.; Ye, R.-X.; Zhou, Y.; An, S.-B.; Xiao, W.-F. Exosomes in osteoarthritis: Updated insights on pathogenesis, diagnosis, and treatment. Front. Cell Dev. Biol. 2022, 10, 949690. [Google Scholar] [CrossRef]
- Fang, W.H.; Agrawal, D.K.; Thankam, F.G. “Smart exosomes”: a smart approach for tendon regeneration. Tissue Engineering Part B: Reviews 2022, 28, 613–625. [Google Scholar] [CrossRef]
- Wang, Y.; He, G.; Guo, Y.; Tang, H.; Shi, Y.; Bian, X.; Zhu, M.; Kang, X.; Zhou, M.; Lyu, J.; et al. Exosomes from tendon stem cells promote injury tendon healing through balancing synthesis and degradation of the tendon extracellular matrix. J. Cell. Mol. Med. 2019, 23, 5475–5485. [Google Scholar] [CrossRef]
- Lyu, K.; Liu, T.; Chen, Y.; Lu, J.; Jiang, L.; Liu, X.; Liu, X.; Li, Y.; Li, S. A “cell-free treatment” for tendon injuries: adipose stem cell-derived exosomes. European Journal of Medical Research 2022, 27, 75. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.R.; Scheiber, A.L.; Yarowsky, P.; Henn III, R.F.; Otsuru, S.; Lovering, R.M. Exosomes isolated from platelet-rich plasma and mesenchymal stem cells promote recovery of function after muscle injury. The American Journal of Sports Medicine 2020, 48, 2277–2286. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Song, W.; Chen, B.; Liu, X.; He, Y. Exosomes Isolated From Adipose-Derived Stem Cells: A New Cell-Free Approach to Prevent the Muscle Degeneration Associated With Torn Rotator Cuffs. Am. J. Sports Med. 2019, 47, 3247–3255. [Google Scholar] [CrossRef]
- Holmes, T.Q.; Brown, A.F. Champing at the Bit for Improvements: A Review of Equine Welfare in Equestrian Sports in the United Kingdom. Animals 2022, 12, 1186. [Google Scholar] [CrossRef]
- Mactaggart, G.; Waran, N.; Phillips, C.J.C. Identification of Thoroughbred Racehorse Welfare Issues by Industry Stakeholders. Animals 2021, 11, 1358. [Google Scholar] [CrossRef]
- Marshall-Gibson, M.E.; Durham, M.G.; Seabaugh, K.A.; Moorman, V.J.; Ferris, D.J. Survey of equine veterinarians regarding primary equine back pain in the United States. Front. Veter- Sci. 2023, 10, 1224605. [Google Scholar] [CrossRef]
- Rhatomy, S.; Prasetyo, T.E.; Setyawan, R.; Soekarno, N.R.; Romaniyanto, F.; Sedjati, A.P.; Sumarwoto, T.; Utomo, D.N.; Suroto, H.; Mahyudin, F.; et al. Prospect of stem cells conditioned medium (secretome) in ligament and tendon healing: A systematic review. Stem Cells Transl. Med. 2020, 9, 895–902. [Google Scholar] [CrossRef]
- Rodríguez-Fuentes, D.E.; Fernández-Garza, L.E.; Samia-Meza, J.A.; Barrera-Barrera, S.A.; Caplan, A.I.; Barrera-Saldaña, H.A. Mesenchymal Stem Cells Current Clinical Applications: A Systematic Review. Arch. Med Res. 2021, 52, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Carter-Arnold, J.; Neilsen, N.; Amelse, L.; Odoi, A.; Dhar, M. In vitro analysis of equine, bone marrow-derived mesenchymal stem cells demonstrates differences within age-and gender-matched horses. Equine veterinary journal 2014, 46, 589–595. [Google Scholar] [CrossRef]
- Colbath, A.C.; Dow, S.W.; McIlwraith, C.W.; Goodrich, L.R. Mesenchymal stem cells for treatment of musculoskeletal disease in horses: Relative merits of allogeneic versus autologous stem cells. Equine Veter- J. 2020, 52, 654–663. [Google Scholar] [CrossRef]
- Jammes, M.; Contentin, R.; Audigié, F.; Cassé, F.; Galéra, P. Effect of pro-inflammatory cytokine priming and storage temperature of the mesenchymal stromal cell (MSC) secretome on equine articular chondrocytes. Front. Bioeng. Biotechnol. 2023, 11, 1204737. [Google Scholar] [CrossRef]
- Broeckx, S.Y.; Seys, B.; Suls, M.; Vandenberghe, A.; Mariën, T.; Adriaensen, E.; Declercq, J.; Van Hecke, L.; Braun, G.; Hellmann, K.; et al. Equine Allogeneic Chondrogenic Induced Mesenchymal Stem Cells Are an Effective Treatment for Degenerative Joint Disease in Horses. Stem Cells Dev. 2019, 28, 410–422. [Google Scholar] [CrossRef]
- Taylor, C.J.; Peter, V.G.; Coleridge, M.O.D.; Bathe, A.P. Immediate pre-operative computed tomography for surgical planning of equine fracture repair: A retrospective review of 55 cases. PLOS ONE 2022, 17, e0278748. [Google Scholar] [CrossRef]
- Sherlock, C.E.; Eggleston, R.B.; Peroni, J.F.; Parks, A.H. Desmitis of the medial tarsal collateral ligament in 7 horses. Equine Veter- Educ. 2011, 24, 72–80. [Google Scholar] [CrossRef]
- Santos, V.H.; Pfeifer, J.P.H.; Rosa, G.S. Synovial-Derived Mesenchymal Stem Cells Encapsulated in Alginate Beads Provide Better Outcomes for Equine Tarsus Chondral Lesions. J. Orthop. Sports Med. 2023, 5, 265–279. [Google Scholar] [CrossRef]
- Rose, P.L.; Moore, I. Imaging diagnosis--avulsion of the medial collateral ligament of the tarsus in a horse. Veterinary Radiology & Ultrasound: The Official Journal of the American College of Veterinary Radiology and the International Veterinary Radiology Association 2003, 44, 657–659. [Google Scholar] [CrossRef]
- Mitchell, R.; DaSilva, D.; Rosenbaum, C.; Blikslager, A.; Edwards III, R. Ultrasound findings in tendons and ligaments of lame sport horses competing or training in South Florida venues during the winter seasons of 2007 through 2016. Equine Veterinary Education 2021, 33, 306–309. [Google Scholar] [CrossRef]
- Roessingh, A.S.d.B.; Laurent, A.; E Darwiche, S.; Hirt-Burri, N.; Scaletta, C.; Michetti, M.; Laurent, P.; Raffoul, W.; Applegate, L.A. Banking Progenitor Cells for Hippiatric Regenerative Medicine: Optimized Establishment of Safe and Consistent Cell Sources for Standardized Veterinary Therapeutic Protocols. Am. J. Biomed. Sci. Res. 2020, 8, 252–271. [Google Scholar] [CrossRef]
Figure 1.
Most common equine musculoskeletal injuries.
Figure 2.
Secretome constitution. The secretome encompasses a varied collection of soluble and non-soluble factors. Soluble factors include cytokines, chemokines and growth factors. Non-soluble factors include extracellular vesicles (exosomes, apoptotic bodies and microvesicles) [223].
Figure 2.
Secretome constitution. The secretome encompasses a varied collection of soluble and non-soluble factors. Soluble factors include cytokines, chemokines and growth factors. Non-soluble factors include extracellular vesicles (exosomes, apoptotic bodies and microvesicles) [223].
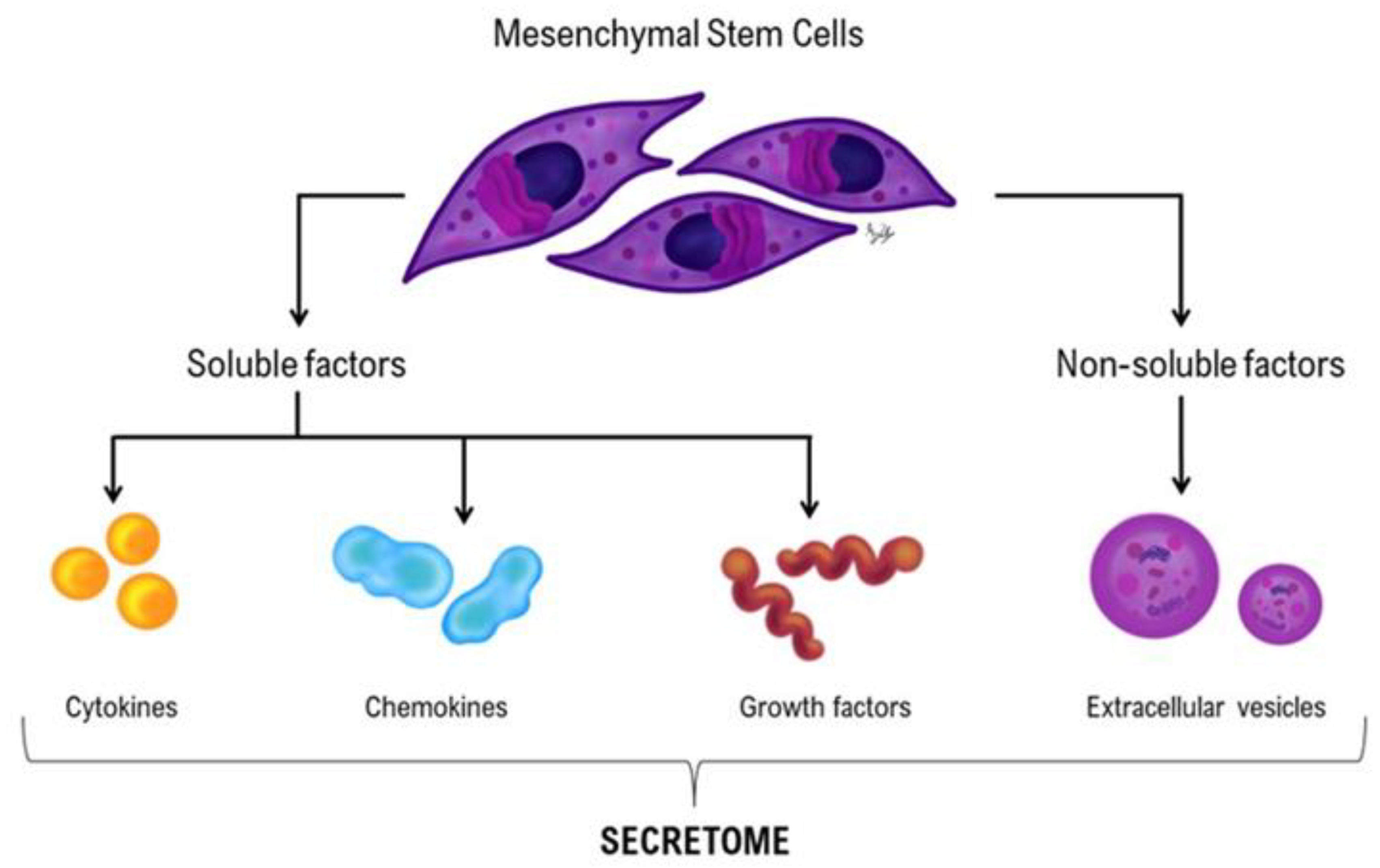

Table 1.
Therapeutical options for musculoskeletal injuries. Conservative therapies include physiotherapeutic, pharmacologic and surgical methods. Physiotherapeutic techniques: manual therapies, passive stretching, tissue and joint mobilization, thermal therapy, kinesiotape/bandage, electrotherapy (magnetic field, electrostimulation, therapeutic ultrasound (U/S), laser, extracorporeal shockwave, vibration plates). Pharmacological methods: anti-inflammatories (AI’s) (nonsteroidal anti-inflammatories (NSAIDs), corticosteroids (SAIDs)), hyaluronic acid (HyA), polyacrylamide gel, and bisphosphonates to manage pain and inflammation. Surgical approach: tendon splitting for tendonitis. Regenerative Therapies: hemoderivatives, stem cell-based therapies and autologous chondrocyte implantation (ACI). Hemoderivatives: platelet-rich plasma (PRP), autologous conditioned serum (ACS); autologous protein solution (APS) and alfa-2-macroglobulin (α2M). Stem Cell-Based Therapies: mesenchymal stromal/stem cells (MSCs) or MSC-derived products. ACI is a surgical regenerative approach.
Table 1.
Therapeutical options for musculoskeletal injuries. Conservative therapies include physiotherapeutic, pharmacologic and surgical methods. Physiotherapeutic techniques: manual therapies, passive stretching, tissue and joint mobilization, thermal therapy, kinesiotape/bandage, electrotherapy (magnetic field, electrostimulation, therapeutic ultrasound (U/S), laser, extracorporeal shockwave, vibration plates). Pharmacological methods: anti-inflammatories (AI’s) (nonsteroidal anti-inflammatories (NSAIDs), corticosteroids (SAIDs)), hyaluronic acid (HyA), polyacrylamide gel, and bisphosphonates to manage pain and inflammation. Surgical approach: tendon splitting for tendonitis. Regenerative Therapies: hemoderivatives, stem cell-based therapies and autologous chondrocyte implantation (ACI). Hemoderivatives: platelet-rich plasma (PRP), autologous conditioned serum (ACS); autologous protein solution (APS) and alfa-2-macroglobulin (α2M). Stem Cell-Based Therapies: mesenchymal stromal/stem cells (MSCs) or MSC-derived products. ACI is a surgical regenerative approach.
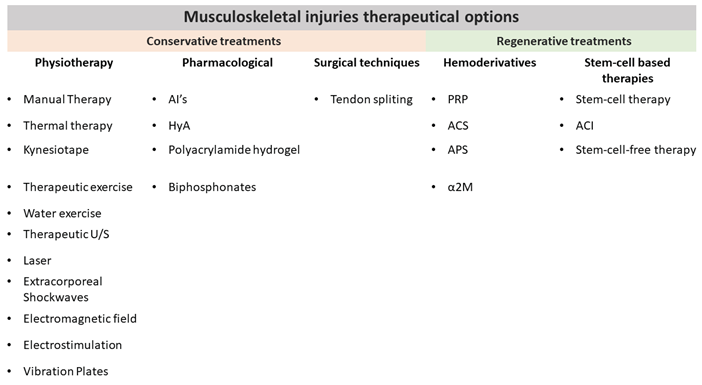 |
Table 2.
Controlled exercise protocol for tendon/ligament injury. The horse is confined to a stall or equivalent size paddock. Adapted from [60].
Table 2.
Controlled exercise protocol for tendon/ligament injury. The horse is confined to a stall or equivalent size paddock. Adapted from [60].
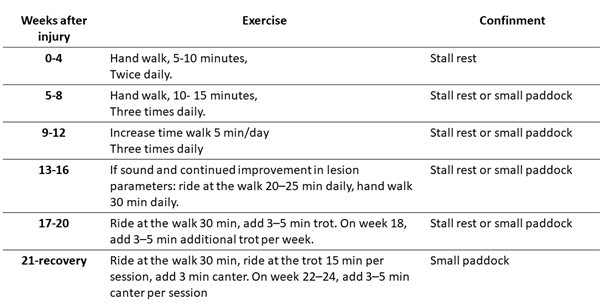 |
Table 3.
Controlled exercise protocol for bone injury. In the first month, horse must be confined to stall rest and then start gradual and increasing of exercise. Adapted from [68].
Table 3.
Controlled exercise protocol for bone injury. In the first month, horse must be confined to stall rest and then start gradual and increasing of exercise. Adapted from [68].
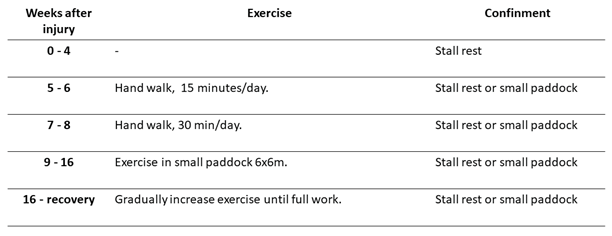 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



