Submitted:
11 March 2024
Posted:
12 March 2024
You are already at the latest version
Abstract
The aging populations observed across numerous countries worldwide necessitate a thorough exploration of interventions aimed at promoting healthy aging. As individuals age, they undergo significant physiological changes that impact their functional capacity and often necessitate increased reliance on external support systems. Enhancing the autonomy and well-being of elderly individuals emerges as a critical imperative, serving not only individual interests but also broader societal goals. This review investigates various interventions designed to optimize the health and independence of aging populations, offering insights into effective strategies for promoting healthy aging and mitigating the societal burdens associated with an aging demographic.
Keywords:
aging populations
; healthy aging interventions
; physiological changes
; autonomy
; well-being
1. Introduction
Populations in the developed world are more skewed towards older individuals than at any previous time in history. Extrapolating the current population trends, the over-50 population in the US will increase by 61% between 2020 and 2050 [1]. The number of people in that age range with at least one chronic disease is expected to double in that same time period, and the population of those with two or more chronic conditions is expected to increase by 91% [1].
With significant disease burden in the older population, it falls on the proportionately smaller working age population to sustain economic functions and to care for the elderly people. The ratio of the number of working age people to the number of retirees will increase by approximately 35%, from 23 retirees per 100 working people in 2010 to 31 retirees per 100 working people in 2030 [2]. Put another way, for each retired person in 2010, there were four people working, whereas in 2030, there will be only three.
Healthcare expenditures also vary significantly by age. For a 25-year-old in the US in 2011, healthcare consumption is roughly 8% of GDP per capita, for those 85 and above, healthcare consumption is almost 70% of GDP per capita [3]. A projection of healthcare expenditures up to 2045 in Switzerland predicts that healthcare expenditures as a proportion of GDP in 2045 will increase between 30% and 45% from 2013 levels [4]. These models assume GDP growth in line with current projections, and it should be noted that unless GDP per capita is increasing greater than this rate, then the relative burden per working individual will increase.
In the overall global population, approximately one third of people experience multiple chronic conditions [5]. Developed countries have a higher rate of multimorbidity (38%) compared to low or middle income countries (30%) [1]. Multimorbidity increases by roughly 78% for every decade increase in age, and women have rates of multimorbidity 23% higher than males of the same age category. Those living in lower income neighborhoods also had higher rates of multimorbidity [5].
Figure 1.
Prevalence of (multi)-morbidity in the UK by age group. Source: reproduced from [5].
Figure 1.
Prevalence of (multi)-morbidity in the UK by age group. Source: reproduced from [5].
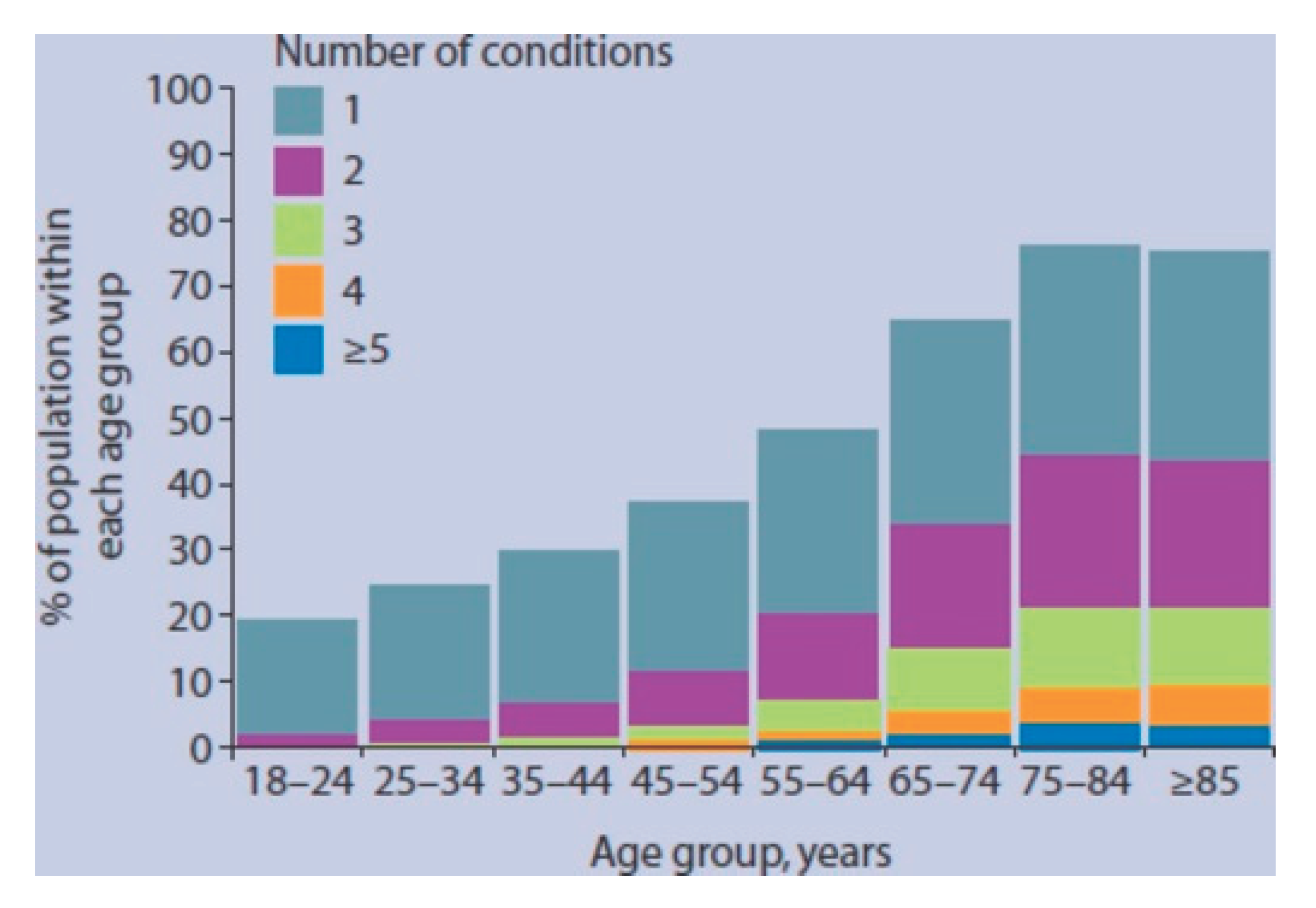

Table 1.
Trends in morbidity in the US adult population between 2020 and 2050 (projected). Table is adapted from [1].
Table 1.
Trends in morbidity in the US adult population between 2020 and 2050 (projected). Table is adapted from [1].
| Age cohort | 2020 | 2035 | 2050 | Relative change between 2020 and 2050(%) |
| Population (million) | ||||
| Total adult population | 137 | 180 | 221 | 61% |
| 50–59 years | 48 | 56 | 69 | 42% |
| 60–79 years | 72 | 95 | 112 | 56% |
| 80 and older | 17 | 30 | 40 | 137% |
| ≥1 chronic condition (million) | ||||
| Adult population | 72 | 114 | 143 | 100% |
| 50–59 years | 16 | 18 | 22 | 40% |
| 60–79 years | 45 | 71 | 84 | 86% |
| 80 and older | 11 | 26 | 37 | 244% |
| Multimorbidity (million) | ||||
| Adult population | 8 | 12 | 15 | 91% |
| 50–59 years | 2 | 2 | 2 | 40% |
| 60–79 years | 5 | 7 | 9 | 79% |
| 80 and older | 1 | 3 | 4 | 203% |
| Prevalence of ≥1 chronic condition (%) | 22% | 35% | 48% | 120% |
| Prevalence of multimorbidity (%) | 2% | 4% | 5% | 111% |
Resulting from this, there is a potential tsunami of chronic health conditions associated with age, and a subsequent increase in health care expenditures, already accounting for 17.3 percent of Gross Domestic Product (GDP) [6]. Disease chronicity increases with age in the general population. In 2013, 80% of the US population over the age of 65 had at least one chronic condition [7].
Fortunately, implementing healthy aging strategies can drastically reduce disease burden. Dementia for example, manifests over decades [8], giving the individual power to alter their expected course. A previous estimate for the increase in healthcare expenditures per capita was 30 to 45% between 2013 and 2045 [4]. The authors also proposed a ‘Healthy Ageing’ scenario wherein the increase was only 21%, which is still a considerable challenge, but attainable with increases in worker productivity.
The presence of ‘Blue Zones’ or pockets of high life expectancy, demonstrates that it is possible to successfully create a culture of longevity and health [9]. While popular authors have emphasized aspects of the diet of the people in Blue Zones, particularly them being highly plant-based, what remains similar to them is the primacy of whole foods which are traditional to the region and population [10]. In Okinawa one of the identified Blue Zones, 0.8% of people born during the 1900 birth cohort reached the age of 100 [11], compared to 0.3% in the USA, or 0.1% in the UK [9].
These long-lived populations point to a way of healthy aging, as their elderly population retains a high degree of autonomy and independence in their everyday lives, many still keeping up leisurely activities, reading and sports [12].
2. Metabolism
Poor metabolic function can contribute to a wide variety of illnesses. Those who are metabolically unwell (having metabolic multimorbidity) spend 52% more time as an inpatient in hospitals, have a 36% increased likelihood of not being able to perform activities of daily living (ADL) [13]. Metabolic dysregulation is comorbid with mental health disorders [14], cancer [15,16], neurodegenerative diseases [17,18].
Importantly, metabolic health can be readily changed through a shift in food consumption patterns. Any policy decision to tackle chronic disease must have food policy and agriculture at its core. Ultra processed foods (UPFs) comprise a larger proportion of people’s diet now than before, often for reasons of convenience. These UPFs with an often-poor nutritional profile crowd out whole foods in the diet [19], and consumption is associated with an increased risk of all-cause mortality, cardiovascular disease, hypertension, metabolic syndrome, obesity, depression, cancer, gastrointestinal disorders [20] and frailty among others [21]. Factors positively associated with UPF consumption are male sex, young age, smoking (only significant for females) and living alone [20,22]. UPFs have significant and wide-ranging deleterious impacts on health [23].
Aging decreases resting metabolic rate (RMR), which is partially attributable to losses in fat-free mass (FFM, i.e., muscle and bone), though there is a decline independent of FFM [24]. Additionally central adiposity increases as one ages [25], and metabolic changes occur regularly, leading experts to classify metabolic dysregulation as hallmarks of aging [26]. Excess body fat can also alter hormone balance, as adipose tissue can promote estrogen production [27].
There is also significant crosstalk between metabolic health and brain health, where metabolically unhealthy individuals have lower brain volumes into old age than their metabolically fit counterparts [28]. When it comes to healthy aging, it is important to avoid insulin resistance, as this is a significant predictor of age-related disease [29]. Those who live to ages past 100 (centenarians) have better insulin sensitivity than their counterparts who die at younger ages [30].
Endurance exercise can reduce age-related declines in mitochondrial oxidative capacity in individuals [31]. Overall, it is important to maintain metabolic health throughout one’s lifespan.
As one’s general fitness can be broken down into components of strength, speed, agility, balance, flexibility and more, one’s metabolic health can be operationalized through meaningful metrics.
First, examining function, we would want a metabolic system to extract energy from food, enough to perform all Activities of Daily Living (ADL), as well as be able to perform athletically when required. The food that people eat should grow and repair their bodies and be sufficient to power all of the necessary functions that contribute to the basal metabolic rate (BMR).
2.1. Fatigue
Endurance exercise, as opposed to punctuated, vigorous exercise, involves exerting power over a longer duration of time at a lower intensity than acute bursts. While this would appear to have limited applicability outside of endurance sports, one major desire of people is to have sustained energy throughout the day. Typically, energy levels are high in the morning, low in the early afternoon, and then increase again before dropping again at night. Higher Body mass index and waist circumference are associated with higher levels of fatigue [32].
Most studies of energy levels of people look at those which suffer from fatigue due to an illness, and not quotidian fatigue. Several dietary conditions have been investigated for their effect on fatigue in disease contexts, and some literature exists on the impact of diet on fatigue in the context of physical training.
In chronic fatigue syndrome (CFS), adoptees of a low sugar and low yeast diet decreased their fatigue significantly (p=0.002, difference measured by the Chalder fatigue score) from their baseline measured before the dietary intervention [33].
A study of breast cancer survivors found that fatigue was associated with fat consumption, and negatively associated with carbohydrate and fiber consumption [34]. A meta-analysis on Multiple Sclerosis (MS) related fatigue came to similar conclusions, finding diets high in greens and low in fat [35], such as a modified paleo diet, may improve MS-related fatigue [36]. The meta-analysis also demonstrated low-quality evidence supporting folate and magnesium for decreasing fatigue [37]. Carbohydrate intake is positively associated with physical capacity, while fat consumption is negatively associated with physical performance in a six-minute walk test and VO2max tests [38]. Omega 3 improved VO2 max, and vitamin D was associated with a nonsignificant improvement in VO2max. Paleolithic diets and Mediterranean diets improved fatigue in MS patients [39], as well as anti-inflammatory diets [40].
Chronic fatigue syndrome (CFS) is another condition where people have difficulty with energy levels. A 2017 meta-analysis showed improvements in fatigue for nicotinamide adenine dinucleotide hydride (NADH), probiotics, high cocoa polyphenol rich chocolate, and a combination of NADH and coenzyme Q10[41]. Omega 3, D-ribose, polyphenols and a multivitamin supplement also have support for their therapeutic use in CFS [42,43].
In the case of cancer related fatigue, adoption of the Mediterranean diet was associated with a small-moderate decrease in fatigue levels [44]. High protein [45], carnitine [46,47], Omega-3 [48], American Ginseng [49], Wisconsin Ginseng [50] and Astralagus membranacus [51] reduced fatigue [52]. Guarana had mixed positive effects [53] and nonsignificant effects [54,55].
3. Cognition
One of the most feared outcomes of aging is a loss of cognition. Many elderly people do suffer from dementia, whether in mild or severe forms. This can be attributed to several mechanisms, some of which can be mediated through diet and lifestyle. First, mitochondrial function often degrades, and aggregates can form in the cases of full-blown Alzheimer’s disease. Other factors include decreased circulation, which can also precipitate hair loss.
As people age, they often become more set in their ways and are less likely to actively learn new things, despite, in retirement, having more leisure time than during their working life. In fact, retirement can have very negative mental health consequences for seniors, as inactivity and seclusion can harm neural pathways.
Furthermore, one commonality in old age is a reduction of one’s social circle, as this often decreases as one increasingly becomes home bound. Old age homes may precipitate some social interaction in the common areas, but this is typically inadequate. Additionally, one social trend acting against senior cognitive health is that parents and children are decreasingly co-located in the same region, making visits more difficult.
The importance of regular social engagement for senior mental health has been studied, showing a significant impact of loneliness on senior health.
This impact often stretches back many years, where those with a more robust friend circle decades earlier also maintain a robust friend circle into old age. Therefore, the social circle is another ‘biomarker’ albeit unconventional, associated with successful aging. Here, relationships should be considered as a vital part of aging, as they present a vital support.
Heart rate variability [58] and vagal nerve tone [59] are important biomarkers for stress tolerance.
Hobbies, including engagement with music [60], are associated with lower rates of cognitive decline and dementia [61,62,63]. Endurance exercise also prevents cognitive decline in older adults [64].
Table 2.
Body systems, associated biomarkers and means of training.
| Training Type | Trend (absent training) | System | Associated tests and biomarkers | Training | Adaptations |
|---|---|---|---|---|---|
| Strength Training | Sarcopenia, muscle loss, bone loss | Musculoskeltal | Grip Strength [65] | Weightlifting | Increase in muscle mass and bone density |
| Endurance training | Lower VO2 max | Metabolic, cardiopulmonary | Resting Metabolic Rate, Creatine phosphokinase [66] | Running, swimming, walking, cycling, cross-country skiing, hiking, etc. | Increased mitochondrial size, greater ability to metabolize fat, increased (heart) stroke volume |
| Balance training | Poorer coordination | Musculoskeletal, nervous | Self-selected gait velocity [67], Chair rise test (timed 5 chair rises), Tandem standing and walking, timed up and go test, clinical gait analysis with special focus on regularity, mechanography [68] | Yoga | Neuromuscular control [69] |
| Flexibility | Decrease in joint flexion [70,71] | Musculoskeletal, tendons, fascia | Flexibility tests: Flexindex [71] | Yoga, Pilates | Improved flexibility and stability |
| Preservation of genomic integrity | Accumulation of mutations [72], accumulation of methylation, higher cancer rates [73] | Genomic Integrity |
Telomere Length [74], Methylation level [75] | Low inflammation practices, avoiding carcinogenic exposures, possibly fasting [76] | Low inflammation practices, avoiding carcinogenic exposures, possibly fasting [76] |
| Cognition | Impairment on task switching [78], working and long-term memory [78] | Nervous | Cognitive tests [79]: Mini-Mental State Examination, Isaacs Set Test, Benton Visual Retention Test, Digit Symbol Substitution Test [80], Combined panel [81] |
Equivocal evidence for transfer effects of cognitive training [82], Combined program (exercise, brain training and lecture) [83], Reading [84], Hobbies [85], Multilingualism [86], Dance [87], Social Activity [88], meditation [89] |
Increased BDNF and neurogenesis [90] preservation of white matter |
4. Cardiovascular and Pulmonary Health
Heart stroke volume from the heart increases with age, while heart rate decreases [91]. Maximum heart rate also decreases with age [92].
While total lung volume remains constant [93], respiratory strength decreases with age [94]. Aging causes a change in deep breathing where deep breathing is less able to increase the size of peripheral airways [95]
In addition, breath volume decreases with age, unless it is countervailed by physical activity.
Endurance exercise is excellent for aging people, as endurance exercise improves mitochondrial density [96] by enlargement of existing mitochondria [97,98].
Can keep increasing, even as one grows older. The impacts of endurance exercise are cumulative, and people with histories of endurance exercise retain their endurance into advanced age.
Cardiopulmonary health can be assessed by the VO2 max test, which involves finding the maximal level of exertion and measuring the flow of oxygen at this level. VO2 max typically decreases with age, dropping more modestly in exercising individuals [99,100].
Given the trend of decreases in heart stroke volume and heart rate with increasing chronological age, VO2 max also declines with age, as it measures the combination of these factors along with respiratory capacity. It is important to retain VO2 max as one ages, and VO2 max helps with capacity to perform daily actions, such as walking up stairs. Additionally, endurance exercise also provides the metabolic benefits of increased mitochondrial density.
Another means by which older adults can improve their metabolic parameters is by cold exposure, which can facilitate the conversion of white adipose tissue to more metabolically active brown adipose tissue (BAT). This increases one’s basal metabolic rate and the practice can also improve one’s tolerance to cold. Older people, especially women, often feel cold at higher temperatures than their younger and male counterparts, so intentional cold exposure can help to alleviate this.
In addition to the cognitive benefits espoused above, periodic fasting can be important for metabolic parameters as well as improving cognitive function. Regular fasting can help to reduce blood sugar variation, which is a contributor to neurodegenerative diseases.
One common intervention that elderly people use is oxygen support. Approximately 1 in 5 people over the age of 70 have some form of chronic obstructive pulmonary disease [101]. Breathing pattern can impact the rates of respiratory illness, with mouth breathing contributing to the development of respiratory disorders [102,103]. One simple means of improving breathing performance is the practice of mouth taping, which involves taping one’s mouth shut during sleep, preferably using a tape that does not leave a residue. Participants in a study experienced significant improvements in rates of snoring and decreases in rates of apnoea events [104].
Ideally, in healthy aging we would prevent the need for supplementary oxygen. Being on cannula oxygen is often bulky and cumbersome, though newer models have reduced the mass to <10lbs (~3kg) [105].
5. Musculoskeletal (Strength and Stability)
Musculoskeletal fitness and stability are very important for older individuals to maintain their independence and sovereignty as they age. Without their own mobility, they are dependent on a caregiver, either paid, a family or friend, for their transportation needs. Paid caregivers can be financially taxing, and the relational caregivers may strain the relationship if one asks too often, creating resentment.
Hip fractures are a major reason for senior death, the one-year mortality after a hip fracture is 24% [106]. Additionally, the sense of autonomy ties into many other positive health circuits. If one is mobile, they can reap the benefits of exercise and the outdoors. If people are left indoors without social interaction, an extreme case being solitary confinement, mental health degrades quickly, and physical deterioration is fast.
Generally, after a certain age, muscle mass declines by a few percentage points per year [107,108]. This can be combatted through resistance training to increase muscle mass and improve both stability (to prevent falls) and strength (to resist injury in the case of falls). Vitamin D is associated with musculoskeletal strength [109] and may be an important intervention for maintaining strength in old age.
6. Emotional Health for Aging
Maintaining a positive life outlook throughout times of stress is associated with decreases in inflammation and future depressive symptom onset [110], additionally, an optimistic spirit is associated with healthier behaviours [111,112,113]. Optimism is a significant predictor of positive health outcomes [114], and improved quality of life in individuals experiencing disease [115]. Optimism can also have a positive impact on people close to the optimistic individual, as a spouse’s optimism is associated with the health of the other spouse [116]
Holding onto regret is a factor in lowered psychological well-being in the aged [117,118], thought the emotional salience of missed opportunities is lesser in older people as opposed to young [119]. Forgiveness is also associated with increased well-being [120,121], including forgiveness of self- [122].
The ‘Big Five’ personality traits include openness, agreeableness, extraversion, conscientiousness, and neuroticism. Of these traits, extraversion [126,127], conscientiousness [128] and openness [129] have been positively associated with life satisfaction. The impact of agreeableness is more heterogenous, and it may have a negative impact on life satisfaction [130]. Neuroticism is associated with lower levels of subjective well-being [127].
Table 3.
Psychological factors for fulfillment in later life.
| Factor | Interventions |
|---|---|
| Regret | Reflect and change behaviour going forward [131] Create positive life experiences |
| Gratitude | Express, journal [132] |
| Forgiveness | Reflecting on events, moving from resentment to compassion [133] |
| Openness | Explore, try new things [134] |
| Meaning/Purpose Intrinsic Motivation | Life crafting [135] |
| Conscientiousness | Adhere to a program [136] |
| Belongingness | Connect [137] |
| Self-transcendence | Experience flow [138] |
One significant cause of reduced quality of life in older people is a lack oof emotional health, sense of purpose and connection. Emotional, spiritual, and relational health are important aspects that are often neglected in favor of more salient and quantifiable changes in the body. Aging often marks the point at which people retire, and so no longer have their daily work to provide them meaning. Often, if people do not find a sense of meaning in what they do day to day, their health suffers and deteriorates quite rapidly after retirement.
It is important to occupy oneself with hobbies which are engaging. Ideally, one could develop these before retirement, and allow them to take up a larger portion of one’s focus and energy. However, the concept of retirement, is a modern invention, which only really existed from about the 1950s to today, as older people, while they may not be working if their younger counterparts, still engaged themselves in mentorship and community activities well into their later years.
The ubiquitous reliance on old age care homes has also been a modern invention, with relative overlap with the development of retirement as a social phenomenon. Within care homes, conditions vary, though these are almost universally seen as less preferable to independent living, and often undermine the autonomy of older individuals through rules and restrictions on movement, for example.
Most residents of care homes have some form of cognitive impairment [139,140], and cognitive decline accelerates in nursing homes as opposed to more independent living [141,142]. This trend was worsened during the pandemic restrictions [143]. Elderly people in residential care or assisted living facilities have lower rates of depression and higher social functioning than their counterparts in nursing homes with less independence [144]
Often in aging, when one’s capabilities begin to decline, this causes psychological pain; this can also be exacerbated by the attitudes of caregivers which may reinforce the supposed helplessness of those advanced in age [145]. Caregivers employed by old age care homes are paid poor wages and often lack the motivation to enable autonomy of those in their care [146], cultural misunderstandings may occur between residents and care home employees [147].
7. Resiliency in Aging
In prior eras, the care of the elderly would have come to the family, lacking that, the elderly lacking cognitive ability would have been destitute or been in the care of the community institutions, which could mean the church or poorhouses, the forerunners to current public old age homes [148]. Life would have been difficult for the aged lacking physical capability, though lifespans were significantly shorter, and there was often a shorter gap between health span (length of healthy life) and lifespan (length of life) [149]. This can partly be attributed to medical care, which allowed people to survive despite chronic illnesses, and economic prosperity, which allowed elderly people to exist as non-productive members of society.
The experience of older people in care homes is generally more negative than that in independent living, provided the elder retains autonomy in the latter case [150]. Examining the social determinants of health, it is also very important that older adults consider their financial health, to enable themselves to live independently well into their later years. Poor financial earnings are associated with higher rates of dementia [151], and dementia can further aggravate one’s financial issues [152]. Furthermore, those with limited financial resources have fewer options for treatment and long-term care, and this negatively impacts their prognosis.
Within the framework of permaculture, it is presented the 8 forms of capital, which include [153]:
- (1)
- Financial
- (2)
- Living
- (3)
- Material
- (4)
- Knowledge
- (5)
- Emotional and Spiritual
- (6)
- Social
- (7)
- Cultural
- (8)
- Time.
Table 4.
Types of Capital and their relationship with healthy aging.
| Type of Capital | Explanation | Relationship with healthy aging | Interventions |
| Financial | One’s financial resources | Financial health associated with lower rates of dementia, and better outcomes in case of dementia [152] | Saving, Investing, Increasing Earning Potential |
| Living | One’s natural surroundings | Surrounding green space associated with lower dementia risk [154,155] | Gardening, planting trees, regenerative agriculture/silviculture |
| Knowledge | One’s knowledge base and skillset | Lifelong learning associated with lower risk of dementia [156] | Learning, Hobbies |
| Emotional and Spiritual | One’s personal faith | Religious attendance associated with lower dementia risk [157,158] | Religious and spiritual practice, prayer, meditation |
| Social | One’s connections with other people | Loneliness associated with dementia [159] | Social activity |
| Cultural | Values and traditions | Frequent family visits associated with decrease in dementia symptoms [160] | Story Telling |
| Time Capital | One’s time remaining | Age associated with dementia [161] | Maximize health span, leave unfulfilling time obligations, optimize practices, delegate |
8. Conclusions
Addressing the challenges posed by aging populations requires a holistic approach encompassing various facets of health and well-being. The review underscores the importance of enhancing autonomy and well-being among the elderly to achieve individual and societal goals. Interventions targeting metabolic health, endurance exercise, dietary patterns, and cognitive engagement emerge as crucial strategies for promoting healthy aging. The interconnectedness of factors such as cardiovascular health, musculoskeletal fitness, and emotional well-being is highlighted, emphasizing the need for a comprehensive perspective. Beyond biomedical markers, the paper recognizes the significance of emotional health, social connections, and a sense of purpose in determining overall well-being. Exploring different forms of capital further underscores the diverse aspects influencing the aging process, including financial, living, knowledge, emotional and spiritual, social, cultural, and time capital. The paper advocates for proactive measures, family support, and community engagement to foster resilience in aging, ultimately contributing to healthier and more fulfilling lives for the elderly.
Author Contributions
Conceptualization, M.T.J.H. and P.E.M.; writing—original draft preparation, M.T.J.H.; writing—review and editing, P.E.M and M.T.J.H.
Funding
This research is funded by donations to the Frontline Covid-19 Critical Care Alliance (FLCCC).
Acknowledgments
We thank donors to the FLCCC Alliance.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ansah, J.P.; Chiu, C.-T. Projecting the Chronic Disease Burden among the Adult Population in the United States Using a Multi-State Population Model. Front Public Health 2023, 10, 1082183. [Google Scholar] [CrossRef]
- Lau, S.-H.P.; Tsui, A.K. ECONOMIC-DEMOGRAPHIC DEPENDENCY RATIO IN A LIFE-CYCLE MODEL. Macroeconomic Dynamics 2020, 24, 1635–1673. [Google Scholar] [CrossRef]
- Mason, C.N.; Miller, T. International Projections of Age Specific Healthcare Consumption: 2015–2060. The Journal of the Economics of Ageing 2018, 12, 202–217. [Google Scholar] [CrossRef]
- Braendle, T.; Colombier, C. Healthcare Expenditure Projections up to 2045. Available online: https://mpra.ub.uni-muenchen.de/104737/ (accessed on 7 March 2024).
- Salisbury, C.; Johnson, L.; Purdy, S.; Valderas, J.M.; Montgomery, A.A. Epidemiology and Impact of Multimorbidity in Primary Care: A Retrospective Cohort Study. Br J Gen Pract 2011, 61, e12–e21. [Google Scholar] [CrossRef] [PubMed]
- Hartman, M.; Martin, A.B.; Whittle, L.; Catlin, A. The National Health Expenditure Accounts Team National Health Care Spending In 2022: Growth Similar To Prepandemic Rates: National Health Care Spending Growth in 2022 Similar to Prepandemic Rates. Health Affairs 2024, 43, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Sung, B.; Aggarwal, B.B. Age-Associated Chronic Diseases Require Age-Old Medicine: Role of Chronic Inflammation. Prev Med 2012, 54, S29–S37. [Google Scholar] [CrossRef]
- Davies, L.; Wolska, B.; Hilbich, C.; Multhaup, G.; Martins, R.; Simms, G.; Beyreuther, K.; Masters, C.L. A4 Amyloid Protein Deposition and the Diagnosis of Alzheimer’s Disease: Prevalence in Aged Brains Determined by Immunocytochemistry Compared with Conventional Neuropathologic Techniques. Neurology 1988, 38, 1688. [Google Scholar] [CrossRef] [PubMed]
- Poulain, M.; Herm, A.; Pes, G. The Blue Zones: Areas of Exceptional Longevity around the World. Vienna Yearbook of Population Research 2013, 11, 87–108. [Google Scholar] [CrossRef]
- Pes, G.M.; Dore, M.P.; Tsofliou, F.; Poulain, M. Diet and Longevity in the Blue Zones: A Set-and-Forget Issue? Maturitas 2022, 164, 31–37. [Google Scholar] [CrossRef]
- Poulain, M.; Pes, G.M.; Grasland, C.; Carru, C.; Ferrucci, L.; Baggio, G.; Franceschi, C.; Deiana, L. Identification of a Geographic Area Characterized by Extreme Longevity in the Sardinia Island: The AKEA Study. Experimental Gerontology 2004, 39, 1423–1429. [Google Scholar] [CrossRef]
- Fastame, M.C.; Hitchcott, P.K.; Penna, M.P. The Impact of Leisure on Mental Health of Sardinian Elderly from the ‘Blue Zone’: Evidence for Ageing Well. Aging Clin Exp Res 2018, 30, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhang, P.; Lee, J.T.; Oldenburg, B.; van Heusden, A.; Haregu, T.N.; Wang, H. The Prevalence of Metabolic Disease Multimorbidity and Its Associations With Spending and Health Outcomes in Middle-Aged and Elderly Chinese Adults. Frontiers in Public Health 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, J.A.; Reddy, P.; Davis-Lameloise, N.; Philpot, B.; Laatikainen, T.; Kilkkinen, A.; Bunker, S.J.; Best, J.D.; Vartiainen, E.; Kai Lo, S.; et al. Depression: An Important Comorbidity With Metabolic Syndrome in a General Population. Diabetes Care 2008, 31, 2368–2373. [Google Scholar] [CrossRef]
- Yang, Y.; Mauldin, P.D.; Ebeling, M.; Hulsey, T.C.; Liu, B.; Thomas, M.B.; Camp, E.R.; Esnaola, N.F. Effect of Metabolic Syndrome and Its Components on Recurrence and Survival in Colon Cancer Patients. Cancer 2013, 119, 1512–1520. [Google Scholar] [CrossRef]
- Braun, S.; Bitton-Worms, K.; LeRoith, D. The Link between the Metabolic Syndrome and Cancer. International journal of biological sciences 2011, 7, 1003. [Google Scholar] [CrossRef] [PubMed]
- Pal, K.; Mukadam, N.; Petersen, I.; Cooper, C. Mild Cognitive Impairment and Progression to Dementia in People with Diabetes, Prediabetes and Metabolic Syndrome: A Systematic Review and Meta-Analysis. Soc Psychiatry Psychiatr Epidemiol 2018, 53, 1149–1160. [Google Scholar] [CrossRef]
- Marseglia, A.; Darin-Mattsson, A.; Skoog, J.; Rydén, L.; Hadarsson-Bodin, T.; Kern, S.; Rydberg Sterner, T.; Shang, Y.; Zettergren, A.; Westman, E. Metabolic Syndrome Is Associated with Poor Cognition: A Population-Based Study of 70-Year-Old Adults without Dementia. The Journals of Gerontology: Series A 2021, 76, 2275–2283. [Google Scholar] [CrossRef]
- Martini, D.; Godos, J.; Bonaccio, M.; Vitaglione, P.; Grosso, G. Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples. Nutrients 2021, 13, 3390. [Google Scholar] [CrossRef]
- Schnabel, L.; Buscail, C.; Sabate, J.-M.; Bouchoucha, M.; Kesse-Guyot, E.; Allès, B.; Touvier, M.; Monteiro, C.A.; Hercberg, S.; Benamouzig, R.; et al. Association Between Ultra-Processed Food Consumption and Functional Gastrointestinal Disorders: Results From the French NutriNet-Santé Cohort. Official journal of the American College of Gastroenterology | ACG 2018, 113, 1217. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, Z.; Yang, H.; Qiu, P.; Wang, H.; Wang, F.; Zhao, Q.; Fang, J.; Nie, J. Consumption of Ultra-Processed Foods and Health Outcomes: A Systematic Review of Epidemiological Studies. Nutrition Journal 2020, 19, 86. [Google Scholar] [CrossRef]
- Magalhães, V.; Severo, M.; Correia, D.; Torres, D.; de Miranda, R.C.; Rauber, F.; Levy, R.; Rodrigues, S.; Lopes, C. Associated Factors to the Consumption of Ultra-Processed Foods and Its Relation with Dietary Sources in Portugal. Journal of Nutritional Science 2021, 10, e89. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, M.A.; Baker, P.I. Ultra-Processed Food and Adverse Health Outcomes. BMJ 2019, 365, l2289. [Google Scholar] [CrossRef] [PubMed]
- Poehlman, E.T.; Arciero, P.J.; Goran, M.I. Endurance Exercise in Aging Humans: Effects on Energy Metabolism. Exercise and Sport Sciences Reviews 1994, 22, 251. [Google Scholar] [CrossRef]
- Palmer, A.K.; Jensen, M.D. Metabolic Changes in Aging Humans: Current Evidence and Therapeutic Strategies. J Clin Invest 2022, 132. [Google Scholar] [CrossRef] [PubMed]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The Hallmarks of Aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef]
- Nelson, L.R.; Bulun, S.E. Estrogen Production and Action. Journal of the American Academy of Dermatology 2001, 45, S116–S124. [Google Scholar] [CrossRef]
- Angoff, R.; Himali, J.J.; Maillard, P.; Aparicio, H.J.; Vasan, R.S.; Seshadri, S.; Beiser, A.S.; Tsao, C.W. Relations of Metabolic Health and Obesity to Brain Aging in Young to Middle-Aged Adults. Journal of the American Heart Association 2022, 11, e022107. [Google Scholar] [CrossRef]
- Facchini, F.S.; Hua, N.; Abbasi, F.; Reaven, G.M. Insulin Resistance as a Predictor of Age-Related Diseases. The Journal of Clinical Endocrinology & Metabolism 2001, 86, 3574–3578. [Google Scholar] [CrossRef]
- Paolisso, G.; Gambardella, A.; Ammendola, S.; D’Amore, A.; Balbi, V.; Varricchio, M.; D’Onofrio, F. Glucose Tolerance and Insulin Action in Healthy Centenarians. Am J Physiol 1996, 270, E890–E894. [Google Scholar] [CrossRef]
- Lanza, I.R.; Short, D.K.; Short, K.R.; Raghavakaimal, S.; Basu, R.; Joyner, M.J.; McConnell, J.P.; Nair, K.S. Endurance Exercise as a Countermeasure for Aging. Diabetes 2008, 57, 2933–2942. [Google Scholar] [CrossRef]
- Resnick, H.E.; Carter, E.A.; Aloia, M.; Phillips, B. Cross-Sectional Relationship of Reported Fatigue to Obesity, Diet, and Physical Activity: Results From the Third National Health and Nutrition Examination Survey. Journal of Clinical Sleep Medicine 2006, 02, 163–169. [Google Scholar] [CrossRef]
- Hobday, R.A.; Thomas, S.; O’Donovan, A.; Murphy, M.; Pinching, A.J. Dietary Intervention in Chronic Fatigue Syndrome. Journal of Human Nutrition and Dietetics 2008, 21, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Guest, D.D.; Evans, E.M.; Rogers, L.Q. Diet Components Associated with Perceived Fatigue in Breast Cancer Survivors: Diet, Fatigue and Breast Cancer. European Journal of Cancer Care 2013, 22, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Chase, E.; Chen, V.; Martin, K.; Lane, M.; Wooliscroft, L.; Adams, C.; Rice, J.; Silbermann, E.; Hollen, C.; Fryman, A.; et al. A Low-Fat Diet Improves Fatigue in Multiple Sclerosis: Results from a Randomized Controlled Trial. Mult Scler 2023, 29, 1659–1675. [Google Scholar] [CrossRef]
- Pommerich, U.M.; Brincks, J.; Christensen, M.E. Is There an Effect of Dietary Intake on MS-Related Fatigue? – A Systematic Literature Review. Multiple Sclerosis and Related Disorders 2018, 25, 282–291. [Google Scholar] [CrossRef]
- Bitarafan, S.; Harirchian, M.-H.; Nafissi, S.; Sahraian, M.-A.; Togha, M.; Siassi, F.; Saedisomeolia, A.; Alipour, E.; Mohammadpour, N.; Chamary, M.; et al. Dietary Intake of Nutrients and Its Correlation with Fatigue in Multiple Sclerosis Patients. Iran J Neurol 2014, 13, 28–32. [Google Scholar] [PubMed]
- Albrechtsen, M.T.; Langeskov-Christensen, M.; Jørgensen, M.L.K.; Dalgas, U.; Hansen, M. Is Diet Associated with Physical Capacity and Fatigue in Persons with Multiple Sclerosis? – Results from a Pilot Study. Multiple Sclerosis and Related Disorders 2020, 40, 101921. [Google Scholar] [CrossRef]
- Snetselaar, L.G.; Cheek, J.J.; Fox, S.S.; Healy, H.S.; Schweizer, M.L.; Bao, W.; Kamholz, J.; Titcomb, T.J. Efficacy of Diet on Fatigue and Quality of Life in Multiple Sclerosis. Neurology 2023, 100, e357–e366. [Google Scholar] [CrossRef]
- Mousavi-Shirazi-Fard, Z.; Mazloom, Z.; Izadi, S.; Fararouei, M. The Effects of Modified Anti-Inflammatory Diet on Fatigue, Quality of Life, and Inflammatory Biomarkers in Relapsing-Remitting Multiple Sclerosis Patients: A Randomized Clinical Trial. International Journal of Neuroscience 2021, 131, 657–665. [Google Scholar] [CrossRef]
- Campagnolo, N.; Johnston, S.; Collatz, A.; Staines, D.; Marshall-Gradisnik, S. Dietary and Nutrition Interventions for the Therapeutic Treatment of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: A Systematic Review. Journal of Human Nutrition and Dietetics 2017, 30, 247–259. [Google Scholar] [CrossRef]
- Maric, D.; Brkic, S.; Mikic, A.N.; Tomic, S.; Cebovic, T.; Turkulov, V. Multivitamin Mineral Supplementation in Patients with Chronic Fatigue Syndrome. Medical science monitor: International medical journal of experimental and clinical research 2014, 20, 47. [Google Scholar]
- Bo, S.; Pisu, E. Role of Dietary Magnesium in Cardiovascular Disease Prevention, Insulin Sensitivity and Diabetes. Current Opinion in Lipidology 2008, 19, 50. [Google Scholar] [CrossRef]
- Kleckner, A.S.; Reschke, J.E.; Kleckner, I.R.; Magnuson, A.; Amitrano, A.M.; Culakova, E.; Shayne, M.; Netherby-Winslow, C.S.; Czap, S.; Janelsins, M.C.; et al. The Effects of a Mediterranean Diet Intervention on Cancer-Related Fatigue for Patients Undergoing Chemotherapy: A Pilot Randomized Controlled Trial. Cancers 2022, 14, 4202. [Google Scholar] [CrossRef]
- Stobäus, N.; Müller, M.J.; Küpferling, S.; Schulzke, J.-D.; Norman, K. Low Recent Protein Intake Predicts Cancer-Related Fatigue and Increased Mortality in Patients with Advanced Tumor Disease Undergoing Chemotherapy. Nutrition and Cancer 2015, 67, 818–824. [Google Scholar] [CrossRef]
- Gramignano, G.; Lusso, M.R.; Madeddu, C.; Massa, E.; Serpe, R.; Deiana, L.; Lamonica, G.; Dessì, M.; Spiga, C.; Astara, G.; et al. Efficacy of L-Carnitine Administration on Fatigue, Nutritional Status, Oxidative Stress, and Related Quality of Life in 12 Advanced Cancer Patients Undergoing Anticancer Therapy. Nutrition 2006, 22, 136–145. [Google Scholar] [CrossRef]
- Marx, W.; Teleni, L.; Opie, R.S.; Kelly, J.; Marshall, S.; Itsiopoulos, C.; Isenring, E. Efficacy and Effectiveness of Carnitine Supplementation for Cancer-Related Fatigue: A Systematic Literature Review and Meta-Analysis. Nutrients 2017, 9, 1224. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.M.; Imayama, I.; Neuhouser, M.L.; Kiecolt-Glaser, J.K.; Smith, A.W.; Meeske, K.; McTiernan, A.; Bernstein, L.; Baumgartner, K.B.; Ulrich, C.M.; et al. Fatigue, Inflammation, and ω-3 and ω-6 Fatty Acid Intake Among Breast Cancer Survivors. JCO 2012, 30, 1280–1287. [Google Scholar] [CrossRef]
- Barton, D.L.; Soori, G.S.; Bauer, B.A.; Sloan, J.A.; Johnson, P.A.; Figueras, C.; Duane, S.; Mattar, B.; Liu, H.; Atherton, P.J.; et al. Pilot Study of Panax Quinquefolius (American Ginseng) to Improve Cancer-Related Fatigue: A Randomized, Double-Blind, Dose-Finding Evaluation: NCCTG Trial N03CA. Support Care Cancer 2010, 18, 179–187. [Google Scholar] [CrossRef]
- Barton, D.L.; Liu, H.; Dakhil, S.R.; Linquist, B.; Sloan, J.A.; Nichols, C.R.; McGinn, T.W.; Stella, P.J.; Seeger, G.R.; Sood, A.; et al. Wisconsin Ginseng (Panax Quinquefolius) to Improve Cancer-Related Fatigue: A Randomized, Double-Blind Trial, N07C2. JNCI: Journal of the National Cancer Institute 2013, 105, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-H.; Tsai, C.-H.; Li, T.-C.; Yang, Y.-W.; Huang, W.-S.; Lu, M.-K.; Tseng, C.-H.; Huang, H.-C.; Chen, K.-F.; Hsu, T.-S.; et al. Effects of the Traditional Chinese Herb Astragalus Membranaceus in Patients with Poststroke Fatigue: A Double-Blind, Randomized, Controlled Preliminary Study. Journal of Ethnopharmacology 2016, 194, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Inglis, J.E.; Lin, P.-J.; Kerns, S.L.; Kleckner, I.R.; Kleckner, A.S.; Castillo, D.A.; Mustian, K.M.; Peppone, L.J. Nutritional Interventions for Treating Cancer-Related Fatigue: A Qualitative Review. Nutrition and Cancer 2019, 71, 21–40. [Google Scholar] [CrossRef]
- de Oliveira Campos, M.P.; Riechelmann, R.; Martins, L.C.; Hassan, B.J.; Casa, F.B.A.; Giglio, A.D. Guarana (Paullinia Cupana) Improves Fatigue in Breast Cancer Patients Undergoing Systemic Chemotherapy. The Journal of Alternative and Complementary Medicine 2011, 17, 505–512. [Google Scholar] [CrossRef] [PubMed]
- da Costa Miranda, V.; Trufelli, D.C.; Santos, J.; Campos, M.P.; Nobuo, M.; da Costa Miranda, M.; Schlinder, F.; Riechelmann, R.; del Giglio, A. Effectiveness of Guaraná (Paullinia Cupana) for Postradiation Fatigue and Depression: Results of a Pilot Double-Blind Randomized Study. The Journal of Alternative and Complementary Medicine 2009, 15, 431–433. [Google Scholar] [CrossRef] [PubMed]
- de Sette, C.V.M.; Ribas de Alcântara, B.B.; Schoueri, J.H.M.; Cruz, F.M.; de Cubero, D.I.G.; Pianowski, L.F.; Peppone, L.J.; Fonseca, F.; del Giglio, A. Purified Dry Paullinia Cupana (PC-18) Extract for Chemotherapy-Induced Fatigue: Results of Two Double-Blind Randomized Clinical Trials. Journal of Dietary Supplements 2018, 15, 673–683. [Google Scholar] [CrossRef]
- Helms, E.R.; Zinn, C.; Rowlands, D.S.; Naidoo, R.; Cronin, J. High-Protein, Low-Fat, Short-Term Diet Results in Less Stress and Fatigue Than Moderate-Protein, Moderate-Fat Diet During Weight Loss in Male Weightlifters: A Pilot Study. International Journal of Sport Nutrition and Exercise Metabolism 2015, 25, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Kaya Kaçar, H.; Avery, A.; Bennett, S.; McCullough, F. Dietary Patterns and Fatigue in Female Slimmers. Nutrition & Food Science 2020, 50, 1213–1227. [Google Scholar] [CrossRef]
- Kim, H.-G.; Cheon, E.-J.; Bai, D.-S.; Lee, Y.H.; Koo, B.-H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig 2018, 15, 235–245. [Google Scholar] [CrossRef]
- Porges, S.W. Vagal Tone: A Physiologic Marker of Stress Vulnerability. Pediatrics 1992, 90, 498–504. [Google Scholar] [CrossRef]
- Fang, R.; Ye, S.; Huangfu, J.; Calimag, D.P. Music Therapy Is a Potential Intervention for Cognition of Alzheimer’s Disease: A Mini-Review. Transl Neurodegener 2017, 6, 2. [Google Scholar] [CrossRef]
- Matsumura, T.; Muraki, I.; Ikeda, A.; Yamagishi, K.; Shirai, K.; Yasuda, N.; Sawada, N.; Inoue, M.; Iso, H.; Brunner, E.J.; et al. Hobby Engagement and Risk of Disabling Dementia. J Epidemiol 2023, 33, 456–463. [Google Scholar] [CrossRef]
- Sommerlad, A.; Sabia, S.; Livingston, G.; Kivimäki, M.; Lewis, G.; Singh-Manoux, A. Leisure Activity Participation and Risk of Dementia. Neurology 2020, 95, e2803–e2815. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Tsutsumimoto, K.; Doi, T.; Nakakubo, S.; Kurita, S.; Makizako, H.; Shimada, H. Relationships between Cognitive Leisure Activities and Cognitive Function in Older Adults with Depressive Symptoms: A Cross-Sectional Study. BMJ Open 2020, 10, e032679. [Google Scholar] [CrossRef] [PubMed]
- Muscari, A.; Giannoni, C.; Pierpaoli, L.; Berzigotti, A.; Maietta, P.; Foschi, E.; Ravaioli, C.; Poggiopollini, G.; Bianchi, G.; Magalotti, D.; et al. Chronic Endurance Exercise Training Prevents Aging-Related Cognitive Decline in Healthy Older Adults: A Randomized Controlled Trial. International Journal of Geriatric Psychiatry 2010, 25, 1055–1064. [Google Scholar] [CrossRef]
- Cui, M.; Zhang, S.; Liu, Y.; Gang, X.; Wang, G. Grip Strength and the Risk of Cognitive Decline and Dementia: A Systematic Review and Meta-Analysis of Longitudinal Cohort Studies. Frontiers in Aging Neuroscience 2021, 13. [Google Scholar] [CrossRef]
- Kim, S.; Jazwinski, S.M. Quantitative Measures of Healthy Aging and Biological Age. Healthy Aging Res 2015, 4, 26. [Google Scholar] [CrossRef]
- Hirase, T.; Okubo, Y.; Delbaere, K.; Menant, J.C.; Lord, S.R.; Sturnieks, D.L. Risk Factors for Falls and Fall-Related Fractures in Community-Living Older People with Pain: A Prospective Cohort Study. International Journal of Environmental Research and Public Health 2023, 20, 6040. [Google Scholar] [CrossRef] [PubMed]
- Runge, M.; Hunter, G. Determinants of Musculoskeletal Frailty and the Risk of Falls in Old Age. J Musculoskelet Neuronal Interact 2006, 6, 167–173. [Google Scholar]
- Zech, A.; Hübscher, M.; Vogt, L.; Banzer, W.; Hänsel, F.; Pfeifer, K. Balance Training for Neuromuscular Control and Performance Enhancement: A Systematic Review. Journal of Athletic Training 2010, 45, 392–403. [Google Scholar] [CrossRef]
- Stathokostas, L.; McDonald, M.W.; Little, R.M.D.; Paterson, D.H. Flexibility of Older Adults Aged 55–86 Years and the Influence of Physical Activity. Journal of Aging Research 2013, 2013, e743843. [Google Scholar] [CrossRef]
- Araújo, C.G.S. de Flexibility Assessment: Normative Values for Flexitest from 5 to 91 Years of Age. Arq. Bras. Cardiol. 2008, 90, 280–287. [Google Scholar] [CrossRef]
- Wolters, S.; Schumacher, B. Genome Maintenance and Transcription Integrity in Aging and Disease. Frontiers in Genetics 2013, 4. [Google Scholar] [CrossRef] [PubMed]
- Hoeijmakers, J.H.J. DNA Damage, Aging, and Cancer. New England Journal of Medicine 2009, 361, 1475–1485. [Google Scholar] [CrossRef]
- Sanders, J.L.; Newman, A.B. Telomere Length in Epidemiology: A Biomarker of Aging, Age-Related Disease, Both, or Neither? Epidemiologic Reviews 2013, 35, 112–131. [Google Scholar] [CrossRef] [PubMed]
- Horvath, S.; Raj, K. DNA Methylation-Based Biomarkers and the Epigenetic Clock Theory of Ageing. Nat Rev Genet 2018, 19, 371–384. [Google Scholar] [CrossRef]
- Brandhorst, S.; Longo, V.D. Fasting and Caloric Restriction in Cancer Prevention and Treatment. In Metabolism in Cancer; Cramer, T., A. Schmitt, C., Eds.; Recent Results in Cancer Research; Springer International Publishing: Cham, Switzerland, 2016; ISBN 978-3-319-42118-6. [Google Scholar]
- Chow, M.T.; Möller, A.; Smyth, M.J. Inflammation and Immune Surveillance in Cancer. Seminars in Cancer Biology 2012, 22, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Riddle, D.R. Brain Aging: Models, Methods, and Mechanisms; CRC Press, 2007; ISBN 978-1-00-061155-7.
- Wild, K.; Howieson, D.; Webbe, F.; Seelye, A.; Kaye, J. Status of Computerized Cognitive Testing in Aging: A Systematic Review. Alzheimer’s & Dementia 2008, 4, 428–437. [Google Scholar] [CrossRef]
- Proust-Lima, C.; Amieva, H.; Dartigues, J.-F.; Jacqmin-Gadda, H. Sensitivity of Four Psychometric Tests to Measure Cognitive Changes in Brain Aging-Population–Based Studies. American Journal of Epidemiology 2007, 165, 344–350. [Google Scholar] [CrossRef]
- Belleville, S.; Fouquet, C.; Hudon, C.; Zomahoun, H.T.V.; Croteau, J. Consortium for the Early Identification of Alzheimer’s disease-Quebec Neuropsychological Measures That Predict Progression from Mild Cognitive Impairment to Alzheimer’s Type Dementia in Older Adults: A Systematic Review and Meta-Analysis. Neuropsychol Rev 2017, 27, 328–353. [Google Scholar] [CrossRef]
- Butler, M.; McCreedy, E.; Nelson, V.A.; Desai, P.; Ratner, E.; Fink, H.A.; Hemmy, L.S.; McCarten, J.R.; Barclay, T.R.; Brasure, M.; et al. Does Cognitive Training Prevent Cognitive Decline? Ann Intern Med 2018, 168, 63–68. [Google Scholar] [CrossRef]
- Kouzuki, M.; Kato, T.; Wada-Isoe, K.; Takeda, S.; Tamura, A.; Takanashi, Y.; Azumi, S.; Kojima, Y.; Maruyama, C.; Hayashi, M.; et al. A Program of Exercise, Brain Training, and Lecture to Prevent Cognitive Decline. Annals of Clinical and Translational Neurology 2020, 7, 318–328. [Google Scholar] [CrossRef]
- Chang, Y.-H.; Wu, I.-C.; Hsiung, C.A. Reading Activity Prevents Long-Term Decline in Cognitive Function in Older People: Evidence from a 14-Year Longitudinal Study. International Psychogeriatrics 2021, 33, 63–74. [Google Scholar] [CrossRef]
- Fallahpour, M.; Borell, L.; Luborsky, M.; Nygård, L. Leisure-Activity Participation to Prevent Later-Life Cognitive Decline: A Systematic Review. Scandinavian Journal of Occupational Therapy 2016, 23, 162–197. [Google Scholar] [CrossRef] [PubMed]
- Van den Noort, M.; Vermeire, K.; Bosch, P.; Staudte, H.; Krajenbrink, T.; Jaswetz, L.; Struys, E.; Yeo, S.; Barisch, P.; Perriard, B.; et al. A Systematic Review on the Possible Relationship Between Bilingualism, Cognitive Decline, and the Onset of Dementia. Behavioral Sciences 2019, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Muiños, M.; Ballesteros, S. Does Dance Counteract Age-Related Cognitive and Brain Declines in Middle-Aged and Older Adults? A Systematic Review. Neuroscience & Biobehavioral Reviews 2021, 121, 259–276. [Google Scholar] [CrossRef]
- Marioni, R.E.; Proust-Lima, C.; Amieva, H.; Brayne, C.; Matthews, F.E.; Dartigues, J.-F.; Jacqmin-Gadda, H. Social Activity, Cognitive Decline and Dementia Risk: A 20-Year Prospective Cohort Study. BMC Public Health 2015, 15, 1089. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, L.; Hutt, R.; Yi Tsui, C.K.; Zorokong, K.; Marfeo, E. Meditation-Based Interventions for Adults With Dementia: A Scoping Review. The American Journal of Occupational Therapy 2020, 74, 7403205010p1–7403205010p14. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Zhu, L.; Zhu, L.; Chen, D.; Cai, K.; Liu, Z.; Chen, A. Moderate Exercise Combined with Enriched Environment Enhances Learning and Memory through BDNF/TrkB Signaling Pathway in Rats. International Journal of Environmental Research and Public Health 2021, 18, 8283. [Google Scholar] [CrossRef] [PubMed]
- Houghton, D.; Jones, T.W.; Cassidy, S.; Siervo, M.; MacGowan, G.A.; Trenell, M.I.; Jakovljevic, D.G. The Effect of Age on the Relationship between Cardiac and Vascular Function. Mech Ageing Dev 2016, 153, 1–6. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-Predicted Maximal Heart Rate Revisited. J Am Coll Cardiol 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Sharma, G.; Goodwin, J. Effect of Aging on Respiratory System Physiology and Immunology. Clin Interv Aging 2006, 1, 253–260. [Google Scholar] [CrossRef]
- Tolep, K.; Higgins, N.; Muza, S.; Criner, G.; Kelsen, S.G. Comparison of Diaphragm Strength between Healthy Adult Elderly and Young Men. Am J Respir Crit Care Med 1995, 152, 677–682. [Google Scholar] [CrossRef]
- Berry, R.B.; Pai, U.P.; Fairshter, R.D. Effect of Age on Changes in Flow Rates and Airway Conductance after a Deep Breath. Journal of Applied Physiology 1990, 68, 635–643. [Google Scholar] [CrossRef]
- Booth, F.W.; Ruegsegger, G.N.; Toedebusch, R.G.; Yan, Z. Chapter Six - Endurance Exercise and the Regulation of Skeletal Muscle Metabolism. In Progress in Molecular Biology and Translational Science; Bouchard, C., Ed.; Molecular and Cellular Regulation of Adaptation to Exercise; Academic Press, 2015; Vol. 135, pp. 129–151.
- Meinild Lundby, A.-K.; Jacobs, R.A.; Gehrig, S.; de Leur, J.; Hauser, M.; Bonne, T.C.; Flück, D.; Dandanell, S.; Kirk, N.; Kaech, A.; et al. Exercise Training Increases Skeletal Muscle Mitochondrial Volume Density by Enlargement of Existing Mitochondria and Not de Novo Biogenesis. Acta Physiologica 2018, 222, e12905. [Google Scholar] [CrossRef]
- Lundby, C.; Jacobs, R.A. Adaptations of Skeletal Muscle Mitochondria to Exercise Training. Experimental Physiology 2016, 101, 17–22. [Google Scholar] [CrossRef]
- Kasch, F.W.; Boyer, J.L.; Camp, S.V.; Nettl, F.; Verity, L.S.; Wallace, J.P. Cardiovascular Changes with Age and Exercise. Scandinavian Journal of Medicine & Science in Sports 1995, 5, 147–151. [Google Scholar] [CrossRef]
- Skinner, J.S.; Gaskill, S.E.; Rankinen, T.; Leon, A.S.; Rao, D.C.; Wilmore, J.H.; Bouchard, C. Heart Rate versus %VO2max: Age, Sex, Race, Initial Fitness, and Training Response--HERITAGE. Med Sci Sports Exerc 2003, 35, 1908–1913. [Google Scholar] [CrossRef]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.; Sullivan, S.D.; Lee, T.A.; Weiss, K.B.; et al. International Variation in the Prevalence of COPD (The BOLD Study): A Population-Based Prevalence Study. The Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Izuhara, Y.; Matsumoto, H.; Nagasaki, T.; Kanemitsu, Y.; Murase, K.; Ito, I.; Oguma, T.; Muro, S.; Asai, K.; Tabara, Y.; et al. Mouth Breathing, Another Risk Factor for Asthma: The Nagahama Study. Allergy 2016, 71, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Triana, B.E.G.; Ali, A.H.; León, I.B.G. Mouth Breathing and Its Relationship to Some Oral and Medical Conditions: Physiopathological Mechanisms Involved. Revista Habanera de Ciencias Médicas 2016, 15, 200–212. [Google Scholar]
- Lee, Y.-C.; Lu, C.-T.; Cheng, W.-N.; Li, H.-Y. The Impact of Mouth-Taping in Mouth-Breathers with Mild Obstructive Sleep Apnea: A Preliminary Study. Healthcare 2022, 10, 1755. [Google Scholar] [CrossRef] [PubMed]
- Home Oxygen Therapy. Available online: https://www.nhs.uk/conditions/home-oxygen-treatment/ (accessed on 27 October 2023).
- Pioli, G.; Barone, A.; Giusti, A.; Oliveri, M.; Pizzonia, M.; Razzano, M.; Palummeri, E. Predictors of Mortality after Hip Fracture: Results from 1-Year Follow-Up. Aging Clin Exp Res 2006, 18, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.A.; Evans, W.J. Changes in Skeletal Muscle with Aging: Effects of Exercise Training. Exerc Sport Sci Rev 1993, 21, 65–102. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.; Engelhardt, M. Strength and Muscle Mass Loss with Aging Process. Age and Strength Loss. Muscles Ligaments Tendons J 2014, 3, 346–350. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Duque, G. Vitamin D in the Aging Musculoskeletal System: An Authentic Strength Preserving Hormone. Molecular Aspects of Medicine 2005, 26, 203–219. [Google Scholar] [CrossRef]
- Aschbacher, K.; Epel, E.; Wolkowitz, O.M.; Prather, A.A.; Puterman, E.; Dhabhar, F.S. Maintenance of a Positive Outlook during Acute Stress Protects against Pro-Inflammatory Reactivity and Future Depressive Symptoms. Brain, Behavior, and Immunity 2012, 26, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Lipowski, M. Level of Optimism and Health Behavior in Athletes. Med Sci Monit 2012, 18, CR39–CR43. [Google Scholar] [CrossRef] [PubMed]
- Ingledew, D.K.; Brunning, S. Personality, Preventive Health Behaviour and Comparative Optimism about Health Problems. J Health Psychol 1999, 4, 193–208. [Google Scholar] [CrossRef]
- Mulkana, S.S.; Hailey, B.J. The Role of Optimism in Health-Enhancing Behavior. American Journal of Health Behavior 2001, 25, 388–395. [Google Scholar] [CrossRef]
- Rasmussen, H.N.; Scheier, M.F.; Greenhouse, J.B. Optimism and Physical Health: A Meta-Analytic Review. Annals of Behavioral Medicine 2009, 37, 239–256. [Google Scholar] [CrossRef]
- Mannix, M.M.; Feldman, J.M.; Moody, K. Optimism and Health-Related Quality of Life in Adolescents with Cancer. Child: Care, Health and Development 2009, 35, 482–488. [Google Scholar] [CrossRef]
- Kim, E.S.; Chopik, W.J.; Smith, J. Are People Healthier If Their Partners Are More Optimistic? The Dyadic Effect of Optimism on Health among Older Adults. Journal of Psychosomatic Research 2014, 76, 447–453. [Google Scholar] [CrossRef]
- Isenberg, C. An Examination of Regret as Expressed in the Life Reflections of Older Adults: Predictors of Regret Intensity and Frequency, and Association with Well-Being. phd, Concordia University, 2007.
- Jokisaari, M. Regrets and Subjective Well-Being: A Life Course Approach. Journal of Adult Development 2004, 11, 281–288. [Google Scholar] [CrossRef]
- Brassen, S.; Gamer, M.; Peters, J.; Gluth, S.; Büchel, C. Don’t Look Back in Anger! Responsiveness to Missed Chances in Successful and Nonsuccessful Aging. Science 2012, 336, 612–614. [Google Scholar] [CrossRef] [PubMed]
- Bono, G.; McCullough, M.E.; Root, L.M. Forgiveness, Feeling Connected to Others, and Well-Being: Two Longitudinal Studies. Pers Soc Psychol Bull 2008, 34, 182–195. [Google Scholar] [CrossRef] [PubMed]
- Allemand, M.; Hill, P.L.; Ghaemmaghami, P.; Martin, M. Forgivingness and Subjective Well-Being in Adulthood: The Moderating Role of Future Time Perspective. Journal of Research in Personality 2012, 46, 32–39. [Google Scholar] [CrossRef]
- Macaskill, A. Differentiating Dispositional Self-Forgiveness from Other-Forgiveness: Associations with Mental Health and Life Satisfaction. Journal of Social and Clinical Psychology 2012, 31, 28–50. [Google Scholar] [CrossRef]
- Robustelli, B.L.; Whisman, M.A. Gratitude and Life Satisfaction in the United States and Japan. J Happiness Stud 2018, 19, 41–55. [Google Scholar] [CrossRef]
- Kong, F.; Ding, K.; Zhao, J. The Relationships Among Gratitude, Self-Esteem, Social Support and Life Satisfaction Among Undergraduate Students. J Happiness Stud 2015, 16, 477–489. [Google Scholar] [CrossRef]
- Unanue, W.; Gomez Mella, M.E.; Cortez, D.A.; Bravo, D.; Araya-Véliz, C.; Unanue, J.; Van Den Broeck, A. The Reciprocal Relationship Between Gratitude and Life Satisfaction: Evidence From Two Longitudinal Field Studies. Frontiers in Psychology 2019, 10. [Google Scholar] [CrossRef]
- Mayungbo, O. AGREEABLENESS, CONSCIENTIOUSNESS AND SUBJECTIVE WELLBEING. PEOPLE: International Journal of Social Sciences 2016, 2, 68–87. [Google Scholar] [CrossRef]
- Gale, C.R.; Booth, T.; Mõttus, R.; Kuh, D.; Deary, I.J. Neuroticism and Extraversion in Youth Predict Mental Wellbeing and Life Satisfaction 40 Years Later. Journal of Research in Personality 2013, 47, 687–697. [Google Scholar] [CrossRef]
- Duckworth, A.; Weir, D.; Tsukayama, E.; Kwok, D. Who Does Well in Life? Conscientious Adults Excel in Both Objective and Subjective Success. Frontiers in Psychology 2012, 3. [Google Scholar]
- Stephan, Y. Openness to Experience and Active Older Adults’ Life Satisfaction: A Trait and Facet-Level Analysis. Personality and Individual Differences 2009, 47, 637–641. [Google Scholar] [CrossRef]
- Fors Connolly, F.; Johansson Sevä, I. Agreeableness, Extraversion and Life Satisfaction: Investigating the Mediating Roles of Social Inclusion and Status. Scandinavian Journal of Psychology 2021, 62, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Ph.D, N.R. If Only: How to Turn Regret Into Opportunity; Clarkson Potter/Ten Speed/Harmony, 2005; ISBN 978-0-7679-2023-0.
- Davis, D.E.; Choe, E.; Meyers, J.; Wade, N.; Varjas, K.; Gifford, A.; Quinn, A.; Hook, J.N.; Van Tongeren, D.R.; Griffin, B.J.; et al. Thankful for the Little Things: A Meta-Analysis of Gratitude Interventions. Journal of Counseling Psychology 2016, 63, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Smallen, D. Practicing Forgiveness: A Framework for a Routine Forgiveness Practice. Spirituality in Clinical Practice 2019, 6, 219–228. [Google Scholar] [CrossRef]
- Jackson, J.J.; Hill, P.L.; Payne, B.R.; Roberts, B.W.; Stine-Morrow, E.A.L. Can an Old Dog Learn (and Want to Experience) New Tricks? Cognitive Training Increases Openness to Experience in Older Adults. Psychol Aging 2012, 27, 286–292. [Google Scholar] [CrossRef]
- Schippers, M.C.; Ziegler, N. Life Crafting as a Way to Find Purpose and Meaning in Life. Frontiers in Psychology 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Javaras, K.N.; Williams, M.; Baskin-Sommers, A.R. Psychological Interventions Potentially Useful for Increasing Conscientiousness. Personality Disorders: Theory, Research, and Treatment 2019, 10, 13–24. [Google Scholar] [CrossRef]
- Suragarn, U.; Hain, D.; Pfaff, G. Approaches to Enhance Social Connection in Older Adults: An Integrative Review of Literature. Aging and Health Research 2021, 1, 100029. [Google Scholar] [CrossRef]
- Csikszentmihalyi, M. Flow. The Psychology of Optimal Experience. New York (HarperPerennial) 1990. 1990.
- Magsi, H.; Malloy, T. Underrecognition of Cognitive Impairment in Assisted Living Facilities. Journal of the American Geriatrics Society 2005, 53, 295–298. [Google Scholar] [CrossRef]
- Hayajneh, A.A.; Rababa, M.; Alghwiri, A.A.; Masha’al, D. Factors Influencing the Deterioration from Cognitive Decline of Normal Aging to Dementia among Nursing Home Residents. BMC Geriatrics 2020, 20, 479. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; McCann, J.J.; Li, Y.; Aggarwal, N.T.; Gilley, D.W.; Evans, D.A. Nursing Home Placement, Day Care Use, and Cognitive Decline in Alzheimer’s Disease. Am J Psychiatry 2007, 164, 910–915. [Google Scholar] [CrossRef]
- González-Colaço Harmand, M.; Meillon, C.; Rullier, L.; Avila-Funes, J.-A.; Bergua, V.; Dartigues, J.-F.; Amieva, H. Cognitive Decline After Entering a Nursing Home: A 22-Year Follow-Up Study of Institutionalized and Noninstitutionalized Elderly People. Journal of the American Medical Directors Association 2014, 15, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodríguez, P.; Díaz de Bustamante, M.; Aparicio Mollá, S.; Arenas, M.C.; Jiménez-Armero, S.; Lacosta Esclapez, P.; González-Espinoza, L.; Bermejo Boixareu, C. Functional, Cognitive, and Nutritional Decline in 435 Elderly Nursing Home Residents after the First Wave of the COVID-19 Pandemic. Eur Geriatr Med 2021, 12, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Sefton, N.; Craig, K.; Meadows, S.; Neher, J.O. Quality of Life in Older Persons with Dementia Living in Nursing Homes. afp 2008, 77, 1011–1012. [Google Scholar]
- Brandriet, L.M. Changing Nurse Aide Behavior to Decrease Learned Helplessness in Nursing Home Elders. Gerontology & Geriatrics Education 1996, 16, 3–19. [Google Scholar] [CrossRef]
- Powers, E.T.; Powers, N.J. Should Government Subsidize Caregiver Wages? Some Evidence on Worker Turnover and the Cost of Long-Term Care in Group Homes for Persons With Developmental Disabilities. Journal of Disability Policy Studies 2011, 21, 195–209. [Google Scholar] [CrossRef]
- Janevic, M.R.; M Connell, C. Racial, Ethnic, and Cultural Differences in the Dementia Caregiving Experience: Recent Findings. The Gerontologist 2001, 41, 334–347. [Google Scholar] [CrossRef]
- Katz, M.B. Poorhouses and the Origins of the Public Old Age Home. Milbank Mem Fund Q Health Soc 1984, 62, 110–140. [Google Scholar] [CrossRef]
- A History of Elder Care. Bayview Healthcare St. Augustine 2015.
- Karakaya, M.G.; Bilgin, S.Ç.; Ekici, G.; Köse, N.; Otman, A.S. Functional Mobility, Depressive Symptoms, Level of Independence, and Quality of Life of the Elderly Living at Home and in the Nursing Home. Journal of the American Medical Directors Association 2009, 10, 662–666. [Google Scholar] [CrossRef]
- Samuel, L.J.; Szanton, S.L.; Wolff, J.L.; Ornstein, K.A.; Parker, L.J.; Gitlin, L.N. Socioeconomic Disparities in Six-Year Incident Dementia in a Nationally Representative Cohort of U.S. Older Adults: An Examination of Financial Resources. BMC Geriatrics 2020, 20, 156. [Google Scholar] [CrossRef]
- Nicholas, L.H.; Langa, K.M.; Bynum, J.P.W.; Hsu, J.W. Financial Presentation of Alzheimer Disease and Related Dementias. JAMA Internal Medicine 2021, 181, 220–227. [Google Scholar] [CrossRef]
- Martenson, C.; Taggart, A. Prosper!: How to Prepare for the Future and Create a World Worth Inheriting; RDA Press, LLC, 2015; ISBN 1-937832-77-5.
- Paul, L.A.; Hystad, P.; Burnett, R.T.; Kwong, J.C.; Crouse, D.L.; van Donkelaar, A.; Tu, K.; Lavigne, E.; Copes, R.; Martin, R.V.; et al. Urban Green Space and the Risks of Dementia and Stroke. Environmental Research 2020, 186, 109520. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Navakatikyan, M.A.; Feng, X. Urban Green Space, Tree Canopy and 11-Year Risk of Dementia in a Cohort of 109,688 Australians. Environment International 2020, 145, 106102. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, M.; Snyder, H.M.; Carrillo, M.C.; Fazio, S.; Kim, H.; Johns, H. Summary of the Evidence on Modifiable Risk Factors for Cognitive Decline and Dementia: A Population-Based Perspective. Alzheimer’s & Dementia 2015, 11, 718–726. [Google Scholar] [CrossRef]
- Britt, K.C.; Richards, K.C.; Acton, G.; Hamilton, J.; Radhakrishnan, K. Association of Religious Service Attendance and Neuropsychiatric Symptoms, Cognitive Function, and Sleep Disturbances in All-Cause Dementia. Int J Environ Res Public Health 2023, 20, 4300. [Google Scholar] [CrossRef]
- Upenieks, L.; Zhu, X. Life Course Religious Attendance and Cognitive Health at Midlife: Exploring Gendered Contingencies. Research on aging 2023, 1640275231188998. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Rolls, E.T.; Cheng, W.; Kang, J.; Dong, G.; Xie, C.; Zhao, X.-M.; Sahakian, B.J.; Feng, J. Associations of Social Isolation and Loneliness With Later Dementia. Neurology 2022, 99, e164–e175. [Google Scholar] [CrossRef]
- Minematsu, A. The Frequency of Family Visits Influences the Behavioral and Psychological Symptoms of Dementia (BPSD) of Aged People with Dementia in a Nursing Home. Journal of Physical Therapy Science - J PHYS THER SCI 2006, 18, 123–126. [Google Scholar] [CrossRef]
- Sahathevan, R. Chapter 18 - Dementia: An Overview of Risk Factors. In Diet and Nutrition in Dementia and Cognitive Decline; Martin, C.R., Preedy, V.R., Eds.; Academic Press: San Diego, CA, USA, 2015; ISBN 978-0-12-407824-6. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



