
Submitted:
08 March 2024
Posted:
12 March 2024
You are already at the latest version
Abstract
Abstract: The VSI represents a significant advancement in the assessment of gastrointestinal-specific anxiety among patients with Irritable Bowel Syndrome (IBS) and other Chronic Inflammatory Bowel Diseases (IBD). However, an Italian version of the instrument is not yet available for the reference population. This study utilized a national sample of 500 individuals, including healthy controls and patients with Ulcerative Colitis and Crohn's Disease, to test the validity and reliability of the Italian VSI. Using back-translation methodology to ensure translation fidelity, the research applied a questionnaire and the VSI through an online format to 500 participants. Data analysis revealed that the Italian VSI had excellent psychometric properties, demonstrating high internal consistency (Cronbach’s α = 0.95) and construct validity. The scale proved sensitive in detecting significant differences in visceral sensitivity among groups, highlighting its utility as a clinical and research assessment tool. Specifically, the Italian VSI exhibited a unidimensional factorial structure and maintained a strong correlation with other measures of anxiety and the severity of gastrointestinal symptoms, confirming its role in enhancing the understanding and management of IBS and IBD in Italy.
Keywords:
VSI
; IBD
; IBS
; Crohn's disease
; Ulcerative Colitis
; Visceral Sensitivity
; Visceral Anxiety
1. Introduction
The VSI is a psychometric assessment tool developed to specifically measure visceral sensitivity and anxiety related to gastrointestinal disorders, particularly within the context of Irritable Bowel Syndrome (IBS). This index is designed to better understand how patients with IBS perceive and react to gastrointestinal symptoms, which often include abdominal pain, bloating, and alterations in bowel habits. The VSI specifically focuses on symptom-related anxiety known as Gastrointestinal-Specific Anxiety (GSA). This type of anxiety is characterized by fear and apprehension regarding visceral sensations and symptoms, which can significantly impact the patients’ quality of life.
Through 15 items the VSI assesses the frequency and intensity of these concerns and how they influence the patient’s daily behavior. The validity and reliability of the VSI have been confirmed through various studies, showing a strong correlation with other measures of anxiety and sensitivity, as well as the severity of gastrointestinal symptoms [1,2]. This makes the VSI a useful tool for clinicians and researchers in identifying and addressing the psychological aspects of IBS, contributing to a more holistic and personalized approach to managing this complex condition [3].
The VSI was originally developed in Englis, but, over time, it has been translated and validated in various other languages to adapt to different cultural and linguistic contexts. These translations enable healthcare professionals to use the VSI in a variety of populations, enhancing the understanding and treatment of IBS globally.
The initial version of the VSI was developed by Labus and colleagues in 2004 [1]. The research focused on creating a valid and reliable psychometric tool to measure symptom-specific anxiety related to gastrointestinal symptoms—an aspect considered significant in the pathophysiology and health outcomes of patients with IBS. In the process of developing the VSI, researchers engaged both external and internal experts, as well as a group of patients, to evaluate a broad set of potential items gathered from psychological and gastrointestinal literature.
After administering these potential scale elements to 96 patients diagnosed with IBS along with a set of validation questionnaires, a final item selection was made based on rigorous empirical criteria. The result was a unidimensional scale of 15 items, the Visceral Sensitivity Index, which demonstrated excellent reliability and good content, convergent, divergent, and predictive validity.
Subsequently, the validity study of the Norwegian version [4] investigated whether psychological factors such as general and symptom-specific anxiety and depression could predict the severity of symptoms in patients with unexplained subjective food hypersensitivity. To do so, they translated and validated the Norwegian version of the VSI. Seventy consecutive patients completed questionnaires on the Hospital Anxiety and Depression Scale, VSI, Irritable Bowel Syndrome Symptom Questionnaire, and Subjective Health Complaints Inventory. Multiple regression analyses were used to study the relationship between psychological factor scores and the severity of somatic symptoms. The results showed that most patients reported non-gastrointestinal symptoms in addition to the typical complaints of irritable bowel syndrome, but general and symptom-specific anxiety, and depression did not explain a significant portion of the variance in somatic complaints. Symptom-specific anxiety for gastrointestinal symptoms was a significant predictor of gastrointestinal complaints, and age was the only significant predictor of non-gastrointestinal complaints. About 90% of the total variance in symptom severity remained unexplained by psychological factors. The Norwegian version of the VSI demonstrated satisfactory validity with a Cronbach’s alpha of 0.93, and there was a significant correlation between symptom-specific anxiety and general anxiety.
Subsequently, the Japanese version of the Visceral Sensitivity Index (VSI-J) was validated in a study conducted by Tatsuo Saigo and colleagues in 2014 [5]. This study translated the VSI into Japanese and assessed its reliability and validity. The primary objective was to introduce a Japanese version of the VSI to measure symptom-specific anxiety related to gastrointestinal symptoms (GSA) in patients with IBS, considering the importance of GSA as an endpoint for therapeutic interventions. The participant group consisted of 349 university students aged 18 and 19. The study used the VSI-J along with other instruments such as the Anxiety Sensitivity Index (ASI), the Hospital Anxiety and Depression Scale (HAD), and the IBS Severity Index (IBS-SI) to analyze the internal consistency, stability, and factorial structure of the VSI-J, along with its associations with anxiety, depression, and measures of intestinal pathology severity. The factorial structure of the VSI-J was found to be unidimensional and similar to that of the original VSI, with high internal consistency (Cronbach’s α = 0.93). Construct validity was demonstrated by significant correlations with ASI, HAD-ANX, and IBS-SI scores. Additionally, the VSI-J proved to be a significant predictor of severity scores on the IBS-SI and showed good discriminant and incremental validity.
More recently, the validation of the Ukrainian version of the Visceral Sensitivity Index (VSI-UA) has represented a significant development in the field of gastroenterology, particularly for Ukrainian-speaking patients with IBS. The study conducted by Neverovskyi, Shypulin & Mikhnova [6] translated and validated the VSI to adapt it to the linguistic and cultural needs of the Ukrainian population, demonstrating the effectiveness of the tool in assessing specific anxiety related to the gastrointestinal tract. The results of the study show that the VSI-UA possesses good psychometric properties, with high internal reliability indicated by a Cronbach’s alpha value of 0.84, and test-retest consistency confirmed by an Intra-Class Correlation (ICC) coefficient of 0.92. Furthermore, the VSI-UA demonstrated excellent content validity, with a Content Validity Index (CVI) of 0.94 and a Content Validity Ratio (CVR) exceeding the critical value for each item. Construct validity was also confirmed through moderate and positive correlations with validated instruments such as the Patient Health Questionnaire-9 (PHQ-9), Beck Depression Inventory (BDI), and the Hospital Anxiety and Depression Scale (HADS).
Currently, there is no Italian version of the VSI, a crucial tool for assessing gastrointestinal-specific anxiety in IBS patients [8,9] The need for an Italian adaptation arises from the importance of culturally and linguistically specific instruments in medical research and practice. Such an adaptation would enable more accurate assessment and management of IBS in Italian-speaking populations, facilitating a better understanding of the disorder’s impact on patients’ lives and improving treatment outcomes in a culturally relevant manner.
Considering these premises, the objectives of the present study can be summarized as follows:
RQ1. Investigate the reliability and validity of the VSI-IT (Visceral Sensitivity Index-Italian).
RQ2. Explore the sensitivity and discriminant validity of the VSI-IT.
RQ3. Examine the concurrent validity of the VSI-IT.
2. Materials and Methods
2.1. Procedure
After obtaining approval from the Ethics Committee at the IRB of the Polish Society of Disaster Medicine (Approval date: January 3. 2023. Approval no. 15.01.2023.IRB) subjects were recruited online through social network groups created by ambassadors and patients who are members of AMICI-ONLUS. Additionally, recruitment took place in person at the University of Messina. Prior to administration, all participants provided informed consent. Data collection occurred from February 13 to March 23. 2023.
The back translation process for the Italian version of the Visceral Sensitivity Index involved the initial translation of the text from English to Italian by an experienced translator, followed by a review by a professional in the field of gastroenterology to ensure that all terms and concepts were accurately interpreted. Subsequently, a second translator, a native English speaker, converted the Italian text back into English without seeing the original document. The two English versions were then compared to identify discrepancies, which were discussed and resolved with the help of bilingual experts. After necessary adjustments to refine the accuracy of the translation, the Italian version was pretested on a small sample to ensure its clarity and relevance. Finally, it was validated through comparison with the original version to confirm its conceptual and linguistic fidelity.
Through the informed consent form (containing information regarding data confidentiality and the option to discontinue participation at any time), each participant provided their consent before proceeding with the survey.
2.2. Participants
The study involved 500 Italian-speaking participants, including 108 males, 391 female, and 1 non-binary individual, with an age range from 18 to 85 years (M = 35.04; SD = 13.29). Two groups were formed, including a control group with healthy subjects (164 participants) and an experimental group consisting of patients with Chronic Inflammatory Bowel Diseases (180 UC; 111 CD; 34 IBS; 11 awaiting diagnosis) in either an active state of the disease or remission. The first criterion for questionnaire participation was reporting an age of at least 18 years.
The majority of participants reside in the South of Italy (39.9%), followed by residents in the North (28.1%), the Islands (18.0%), and a smaller number in the Central region (13.6%). There is a predominant response from a female sample (78.0%) and a partial response from a male audience (21.4%), with a minority identifying as non-binary (0.2%). Most participants reported being single (40.3%), followed by married (36.5%), cohabiting (17.8%), divorced (2.8%), separated (1.8%), and widowed (0.4%). The majority of participants have a higher education level (51.1%), followed by a bachelor’s degree (22.0%), postgraduate studies (15.0%); a minority reported completing only middle school (7.6%), specialized diploma (1.6%), and Ph.D. (1.6%), with a few participants having a three-year qualification (0.2%), a first-level university master’s degree (0.2%), and professional training courses in healthcare assistance (0.2%). Most participants identified as students (34.3%), followed by employees (28.1%), freelancers (10.0%), homemakers (10.0%), workers (7.6%), unemployed (3.6%), self-employed (2.2%), retirees (1.8%), interns/trainees (0.8%), doctoral candidates/university researchers (0.8%), and volunteers (0.4%).
2.3. Instruments
2.3.1. VSI
The Visceral Sensitivity Index (VSI) was developed by Labus et al. in 2004 [1], to evaluate specific anxiety related to the gastrointestinal tract (GSA). The questionnaire consists of 15 items and assesses concern, fear, vigilance, sensitivity, avoidance, as well as cognitions and behaviors related to gastrointestinal aspects, often accompanying misperceptions and misjudgements of bodily sensations. Items are rated on a six-point Likert scale, ranging from 1 (strongly agree) to 6 (strongly disagree). Subsequently, the numbers indicated by the patient for each item are evaluated by assigning a score from 0 to 5. The overall VSI score ranges from 0 to 75, with higher scores indicating more severe GSA. Given the total score, a value greater than 37.5 has been chosen to indicate an increased VSI in individuals [10].
2.3.2. MAIA
The Multidimensional Assessment of Interoceptive Awareness (MAIA), developed by Mehling et al. in 2012 [10], is a self-report questionnaire comprising 32 items. It provides a multidimensional profile of interoceptive sensitivity, including the following eight subscales:
- Noticing: Awareness of uncomfortable, comfortable, and neutral bodily sensations.
- Not-Distracting: Tendency to ignore or distract oneself from sensations of pain or discomfort.
- Not-Worrying: Emotional distress or worry associated with sensations of pain or discomfort.
- Attention Regulation: The ability to sustain and control attention to bodily sensations.
- Emotional Awareness: Awareness of the connection between bodily sensations and emotional states.
- Self-Regulation: The ability to regulate psychological discomfort through attention to bodily sensations.
- Body Listening: Active listening to the body for understanding.
- Trusting: Experiencing one’s own body as safe and reliable (subscales range: 0-5).
Higher scores on the MAIA indicate greater interoceptive sensitivity.
Statistical Analysis
The data were analyzed using SPSS 27.0 software (SPSS Inc., Chicago, IL, USA). Continuous variables were reported using mean (M) and standard deviation (SD), while categorical variables were presented as frequencies and percentages. Correlations between continuous variables were assessed using the Pearson correlation coefficient. For group comparisons, ANOVA and the Kruskall-Wallis Test for independent samples were employed.
3. Results
3.1. Validity and Reliability of VSI-IT
The Cronbach’s Alpha value, which measures the internal reliability of the scale is 0.949 for 15 items. This value indicates that the items in the Italian version of the VSI are consistent with each other, suggesting that they reliably measure the same psychological construct, namely, specific anxiety related to gastrointestinal symptoms. In terms of validity, the Kaiser-Meyer-Olkin Measure of Sampling Adequacy (KMO) provides another indicator of adequacy. With a value of 0.961, it far exceeds the acceptable minimum of 0.5, indicating that the data sampling for factor analysis is more than adequate. This high KMO value suggests that the partial correlations between items are sufficiently low, making the items well-suited for factor analysis. Bartlett’s test of sphericity, with an approximate chi-square value of 5339.394 and p < .001, further confirms the validity of the scale. This test verifies the hypothesis that variables in the correlation matrix are not correlated in the entire population, indicating that there is a sufficient correlation between items to proceed with a factor analysis.
The principal component matrix for the VSI provides an insightful overview of how each item contributes to specific anxiety related to gastrointestinal symptoms. Principal component analysis reveals a strong unidimensionality in the construct measured by the VSI, with all 15 items showing factor loadings higher than 0.5 (Table 1). This indicates that each question within the index is closely linked to anxiety related to gastrointestinal symptoms, a central aspect of IBS. In particular, items with higher factor loadings (exceeding 0.8), such as Item __"I often worry about belly problems" and Item __"I have difficulty enjoying myself because I can’t take my mind off belly discomfort." reflect deep and persistent concerns regarding abdominal discomfort and its impact on daily life. At the same time, even items with slightly lower factor loadings, like Item __"I am constantly aware of the sensations I have in my belly." represent relevant aspects of specific anxiety for gastrointestinal symptoms, indicating high awareness and concern for bodily sensations. Furthermore, the percentage of variance explained by the single extracted component, which is significantly high (approximately 59%), confirms that the VSI is effective in capturing the majority of anxiety related to gastrointestinal symptoms in a single construct.
3.2. Sensitivity and Discriminant Validity of the VSI-IT
3.2.1. The Ability of the VSI-IT to Discriminate between Various Pathological Conditions
The analysis of differences between patient groups with various gastrointestinal conditions and healthy controls shows significant results (Table 2 and Table 3). Healthy controls markedly differ from patients with irritable bowel syndrome, Crohn’s disease, and ulcerative colitis, with the latter exhibiting significantly higher levels of visceral sensitivity, indicating a stronger impact of these conditions on anxiety-related visceral symptoms. This difference remains statistically significant even after applying the Bonferroni correction, known for its strict control of Type I errors in multiple analyses (ANOVA Between groups sum of squares= 65044.587; df=4; F=66.291; p<.001).
Comparison between patients with irritable bowel syndrome and other patient groups did not reveal statistically significant differences before applying the Bonferroni correction, suggesting a similar level of visceral sensitivity among these groups (See Figure 1). This changes when irritable bowel syndrome is compared with ulcerative colitis, where the difference becomes significant but loses significance after adjustment. When comparing groups awaiting diagnosis ("other") with those affected by Crohn’s disease or ulcerative colitis, visceral sensitivity differences are not statistically significant, indicating that visceral sensitivity among these conditions may not vary substantially. Similarly, the direct comparison between Crohn’s disease and ulcerative colitis shows no significance, suggesting that these two disorders share similar aspects in terms of how patients perceive and react to gastrointestinal symptoms (See Figure 2).
3.2.2. The Ability of the VSI-IT to Discriminate Based on the Severity of Symptoms
The graph (Figure 3) displays the results of the non-parametric Kruskal-Wallis test, used to assess whether there are significant differences in visceral sensitivity among patient groups with different symptom severity levels: absent, mild, moderate, and severe. In terms of discriminant validity, which refers to the ability of an instrument to distinguish between groups that should differ based on the construct the instrument intends to measure, the graph suggests that the VSI has a certain ability to discriminate between groups based on symptom severity (Kruskall-Wallis test statistics = 39.443; p<.001). However, the presence of outliers, especially in the group with severe symptoms, might also indicate that factors other than symptom severity could influence visceral sensitivity, such as anxiety or other psychological factors. In conclusion, the VSI appears to have a certain degree of discriminant validity concerning symptom severity, but the degree of overlap between groups suggests that further research may be needed to explore the complexity of this construct and to better understand the interactions between visceral sensitivity and other psychological or physical factors.
3.3. Concurrent Validity of VSI-IT
The correlation table (Table 5) shown in the image provides Pearson correlation coefficients between visceral sensitivity and various psychological constructs such as attentional ability, emotional regulation, and bodily awareness (MAIA). The concurrent validity of a measurement instrument refers to its ability to significantly correlate with other tests that are theoretically connected to the same construct. Specifically, "Noticing" has a moderate positive correlation with visceral sensitivity (r = 0.277. p < 0.001), suggesting that increased attention or awareness of GI symptoms is associated with higher visceral sensitivity. "Not-worrying" shows a moderate negative correlation (r = -0.414. p < 0.001), suggesting that the ability not to excessively worry is associated with lower visceral sensitivity. "Attention regulation" has a negative correlation (r = -0.142. p = 0.001), which may indicate that increased attention regulation reduces visceral sensitivity. "Emotional awareness" is positively correlated (r = 0.235. p < 0.001), meaning that greater awareness of one’s emotions is associated with higher visceral sensitivity. "Self-regulation" shows a weak negative correlation (r = -0.135. p = 0.003), suggesting that the ability to self-regulation might have a moderating effect on visceral sensitivity. Finally, the component "Trusting" exhibits a negative correlation with VSI (r = -0.302. p < 0.001), implying that greater trust in one’s bodily sensations is associated with lower visceral sensitivity.
| Variable | Visceral Sensitivity Index |
| Noticing | 0.277 ** |
| Not-distracting | -0.044 |
| Not-worrying | -0.414 ** |
| Attention regulation | -0.142 ** |
| Emotional awareness | 0.235 ** |
| Self-regulation | -0.135 * |
| Body Listening | 0.056 |
| Trusting | -0.302 ** |
4. Discussion
This study aimed to examine the psychometric characteristics of the VSI-IT in patients with IBS and IBD (Inflammatory Bowel Disease). The validity of the Italian version of the VSI was demonstrated through a series of positive statistical outcomes. The correlations found between VSI scores and gastroenterological conditions, coupled with the statistical significance and clinical relevance of these correlations, affirm the reliability and convergent validity of the instrument. Therefore, the VSI proves to be a valid and sensitive tool, suitable for assessing specific anxiety related to gastrointestinal symptoms, applicable in both clinical practice and research to enhance the understanding and management of IBS and other related conditions.
Furthermore, from a clinical perspective, these results suggest that aspects of emotional and bodily awareness [11], as well as the ability to manage concerns and attention, are correlated with visceral sensitivity, in line with Atanasova’s studies [12]. This supports the concurrent validity of the VSI as a tool for assessing visceral sensitivity in the context of various psychological experiences and strategies. Specifically, the statistical significance of correlations with constructs such as not worrying, emotional regulation, and trust in bodily sensations confirms the relevance and validity of the VSI in evaluating how individuals perceive and respond to gastrointestinal symptoms.
On the other hand, the differences observed in mean scores between healthy controls and various patient groups indicate that the instrument is valid in distinguishing levels of visceral anxiety between healthy individuals and those with specific gastroenterological conditions, in line with Trieschmann [2]. The consistency of these differences across different comparisons, and their persistence even after correction for multiple tests, suggests that the VSI could also be a sensitive indicator of variations in anxiety related to gastrointestinal symptoms [13].
According to Trieschmann [2], the VSI is a useful measure in IBD. Patients with IBD exhibit GSA associated with a decrease in HRQOL, which can negatively impact treatment compliance and other long-term disease outcomes. It is believed that IBS symptoms are influenced by both external stressors. such as major life events, and internal stressors, such as excessive conditioned reactivity [14,15].
The discriminant validity of the VSI (Visceral Sensitivity Index) partly succeeds in distinguishing between patient groups based on the severity of their symptoms, as evidenced by the significant value of the statistics. However, the existence of some outliers, especially among patients with more severe symptoms, suggests that there are other factors, such as anxiety or psychological aspects, that may influence visceral sensitivity beyond the sole severity of symptoms.
As noted by Labus [16], patients with non-functional gastrointestinal disorders (chronic inflammatory bowel disease, cancer) might achieve a relatively low score on the VSI despite the significant severity of symptoms, while patients with other functional gastrointestinal disorders (such as functional dyspepsia or non-cardiac chest pain, and especially those with multiple disorders) might obtain a high score due to generalized anxiety about gastrointestinal sensations.
Limitations
There are several limitations to this study that need to be emphasized. The analyzed groups are not homogeneous, and the IBS patient group consists of a small number of subjects. Additional studies with a more balanced sample size and a broader distribution of various pathologies within IBD would be necessary to draw meaningful conclusions about VSI differences concerning IBD disease types. Additionally, subjects awaiting diagnosis were excluded; however, it would be interesting to explore the diagnostic capabilities of the VSI in patients awaiting diagnosis. Furthermore, comparisons with other studies are only partially possible, as in this study, the assessment of interoceptive awareness was preferred over clinical scales assessing anxiety and depression.
5. Conclusions
These results indicate that the Italian version of the VSI is a highly reliable and valid tool for measuring specific anxiety related to gastrointestinal symptoms. Internal consistency is appropriate, and the sample adequacy and item correlation are ideal for factor analysis, confirming the robustness of the Italian VSI’s structure. This makes the instrument particularly useful for research and clinical practice in the context of IBS in Italy [17,18,19]. The VSI (Visceral Sensitivity Index) represents a fundamental tool for patients as it provides a specific and personalized assessment of their gastrointestinal sensitivity. Additionally, the VSI helps identify the potential influence of non-clinical factors such as stress and anxiety, which may exacerbate symptoms or alter their perception.
The use of the VSI can not only provide clinicians with a clear picture of the patient’s symptoms but also serve as a guide in selecting the most appropriate treatments. This means that a patient with high visceral sensitivity and severe symptoms may receive a more comprehensive therapeutic approach, which could include psychological therapies alongside physical treatments. Understanding and managing visceral sensitivity through the VSI can lead to a significant improvement in the quality of life for patients [20]. This tool can be crucial for optimal management of gastrointestinal conditions, providing patients and their physicians with a valuable resource to address the complexities and challenges associated with such disorders.
Author Contributions
Conceptualization, A.R, A.M. and A.S.; methodology, A.R., L.T., F.C.; software, A.R., M.Y., validation, L.Z., M.P. and G.N.; formal analysis, A.R., A.M.; investigation, A.M.; resources, H.K., L.Z.; data curation, A.R., A.M., A.S., L.T.; writing—original draft preparation, A.R., A.M., A.S., L.T; writing—review and editing, L.Z., M.P., H.K., D.A.A., K.O.; visualization, all the authors; supervision, F.C., M.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. and approved by the Ethics Committee at the IRB of the Polish Society of Disaster Medicine (Approval date: January 3. 2023. Approval no. 15.01.2023.IRB).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data will be made available by the corresponding author under reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Visceral Sensitivity Index – Italian Version (VSI-IT)
© Rizzo, Mautone et al., (2024)
| Pienamente d’accordo | D’accordo | Parzialmente d’accordo | Parzialmente in disaccordo | In disaccordo | Fortemente in disaccordo | |
| 1. Temo che ogni volta che mangio durante il giorno, il gonfiore e la distensione della pancia peggioreranno. | □ | □ | □ | □ | □ | □ |
| 2. Divento ansioso quando vado in un nuovo ristorante. | □ | □ | □ | □ | □ | □ |
| 3. Mi preoccupo spesso per problemi alla pancia. | □ | □ | □ | □ | □ | □ |
| 4. Ho difficoltà a divertirmi perché non riesco a distogliere la mente dal disagio della pancia. | □ | □ | □ | □ | □ | □ |
| 5. Spesso temo di non riuscire ad avere un normale movimento intestinale. | □ | □ | □ | □ | □ | □ |
| 6. A causa della paura di sviluppare disturbi addominali, raramente provo cibi nuovi. | □ | □ | □ | □ | □ | □ |
| 7. Qualunque cosa mangi, probabilmente mi sentirò a disagio. | □ | □ | □ | □ | □ | □ |
| 8. Non appena sento fastidio addominale comincio a preoccuparmi e a sentirmi ansioso. | □ | □ | □ | □ | □ | □ |
| 9. Quando entro in un posto dove non sono mai stato, una delle prime cose che faccio è cercare un bagno. | □ | □ | □ | □ | □ | □ |
| 10. Sono costantemente consapevole delle sensazioni che ho nella mia pancia. | □ | □ | □ | □ | □ | □ |
| 11. Sento spesso che il fastidio alla pancia potrebbe essere segno di una grave malattia. | □ | □ | □ | □ | □ | □ |
| 12. Non appena mi sveglio, temo che avrò fastidio alla pancia durante il giorno. | □ | □ | □ | □ | □ | □ |
| 13. Quando sento disagio nel mio ventre, mi spavento. | □ | □ | □ | □ | □ | □ |
| 14. In situazioni stressanti, la mia pancia mi dà molto fastidio. | □ | □ | □ | □ | □ | □ |
| 15. Penso costantemente a ciò che sta accadendo nella mia pancia. | □ | □ | □ | □ | □ | □ |
References
- Labus, J. S., Bolus, R., Chang, L., Wiklund, I., Naesdal, J., Mayer, E. A., & Naliboff, B. D. (2004). The Visceral Sensitivity Index: development and validation of a gastrointestinal symptom-specific anxiety scale. Alimentary pharmacology & therapeutics, 20(1), 89–97. [CrossRef]
- Trieschmann, K., Chang, L., Park, S., Naliboff, B., Joshi, S., Labus, J. S., Sauk, J. S., Limketkai, B. N., & Mayer, E. A. (2022). The visceral sensitivity index: A novel tool for measuring GI-symptom-specific anxiety in inflammatory bowel disease. Neurogastroenterology and motility, 34(9), e14384. [CrossRef]
- Caballero-Mateos, A.M. Gut Feelings: The Psychological Impact of Inflammatory Bowel Disease. J. Clin. Med. 2023, 12, 3867. [Google Scholar] [CrossRef] [PubMed]
- Lind R, Lied GA, Lillestøl K, Valeur J, Berstad A: Do psychological factors predict symptom severity in patients with subjective food hypersensitivity? Scand J Gastroenterol 2010, 45:835–843.
- Saigo, T., Tayama, J., Hamaguchi, T., Nakaya, N., Tomiie, T., Bernick, P. J., Kanazawa, M., Labus, J. S., Naliboff, B. D., Shirabe, S., & Fukudo, S. (2014). Gastrointestinal specific anxiety in irritable bowel syndrome: validation of the Japanese version of the visceral sensitivity index for university students. BioPsychoSocial medicine, 8(1), 10. [CrossRef]
- Neverovskyi, A., Shypulin, V., & Mikhnova, N. (2023). Translation and validation of the Ukrainian version of the visceral sensitivity index for patients with irritable bowel syndrome. Przeglad gastroenterologiczny, 18(3), 313–319. 3. [CrossRef]
- Brown, T. A., Reilly, E. E., Murray, H. B., Perry, T. R., Kaye, W. H., & Wierenga, C. E. (2021). Validating the visceral sensitivity index in an eating disorder sample. The International journal of eating disorders, 54(6), 986–994. [CrossRef]
- Hayes, B., Burgell, R., Apputhurai, P., Garg, M., & Knowles, S. R. (2022). Extending the Common Sense Model to Explore the Impact of Visceral Sensitivity on Quality of Life in Inflammatory Bowel Disease. The Turkish journal of gastroenterology: the official journal of Turkish Society of Gastroenterology, 33(2), 103–110. [CrossRef]
- Larussa T, Abenavoli L, Corea A, Procopio AC, Giubilei L, Vallelunga R, Polimeni N, Suraci E, Marasco R, Imeneo M, Boccuto L, Luzza F. Trends and characteristics associated with dietary triggers and psychological distress in patients with irritable bowel syndrome: a cross-sectional study. Eur Rev Med Pharmacol Sci. 2021 May;25(10):3752-3761. [CrossRef]
- Mehling WE, Price C, Daubenmier JJ, Acree M, Bartmess E, Stewart A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS One. 2012;7(11):e48230. [CrossRef]
- Schiller, D., Alessandra, N. C., Alia-Klein, N., Becker, S., Cromwell, H.C., Dolcos, F., …& Soreq, H. (2023). The human affectome. Neuroscience & Biobehavioral Reviews, 158:105450. [CrossRef]
- Atanasova, K., Lotter, T., Reindl W., Lis S., Multidimensional Assessment of Interoceptive Abilities, Emotion Processing and the Role of Early Life Stress in Inflammatory Bowel Diseases. Front Psychiatry. 2021 Jun 24; 12:680878. [CrossRef]
- Gîlcă-Blanariu, G. E., Șchiopu, C. G., Ștefănescu, G., Mihai, C., Diaconescu, S., Afrăsânie, V. A., ... & Ștefănescu, C. (2023). The intertwining roads between psychological distress and gut microbiota in inflammatory bowel disease. Microorganisms, 11(9), 2268. 9.
- Bruno, A., Rizzo, A., Muscatello, M. R. A., Celebre, L., Silvestri, M.C., Zoccali, R.A., & Mento, C. (2020). Hyperarousal scale: Italian cultural validation, age and gender differences, in a nonclinical population. International Journal of Environmental Research and Public Health, 17(4), 1176.
- Fracas, E.; Constantino, A.; Vecchi, M.; Buoli, M. Depressive and Anxiety Disorders in Patients with Inflammatory Bowel Diseases: Are There Any Gender Differences? Int. J. Environ. Res. Public Health 2023, 20, 6255. [Google Scholar] [CrossRef] [PubMed]
- Labus, J. S., Mayer, E. A., Chang, L., Bolus, R., & Naliboff, B. D. (2007). The central role of gastrointestinal-specific anxiety in irritable bowel syndrome: further validation of the visceral sensitivity index. Psychosomatic medicine, 69(1), 89–98. [CrossRef]
- Macaluso, F. S., Ventimiglia, M., Fries, W., Viola, A., Sitibondo, A., Cappello, M., ... & Sicilian Network for Inflammatory Bowel Disease (SN-IBD). (2021). A propensity score weighted comparison of vedolizumab and adalimumab in Crohn’s disease. Journal of Gastroenterology and Hepatology, 36(1), 105-111.
- Belvedere, A., Scoglio, R., Viola, A., Costantino, G., Sitibondo, A., Muscianisi, M., ... & Fries, W. (2021). A real world investigation on prevalence, clinical features, and therapy of inflammatory bowel disease in the city of Messina, Italy. Acta Bio Medica: Atenei Parmensis, 92(2).
- Viola, A., Fontana, A., Belvedere, A., Scoglio, R., Costantino, G., Sitibondo, A., ... & Fries, W. (2020). Diagnostic accuracy of faecal calprotectin in a symptom-based algorithm for early diagnosis of inflammatory bowel disease adjusting for differential verification bias using a Bayesian approach. Scandinavian Journal of Gastroenterology, 55(10), 1176-1184.
- Yildrim, M., Turan, M. E., Albeladi, N.S., Crescenzo, P., Rizzo, A., Nucera, G., …& Chirico F. (2023). Resilience and perceived social support as predictors of emotional well-being. J Health Soc Sci, 8(1), 59-75.
Figure 1.
– Boxplot VSI-IT between subjects.
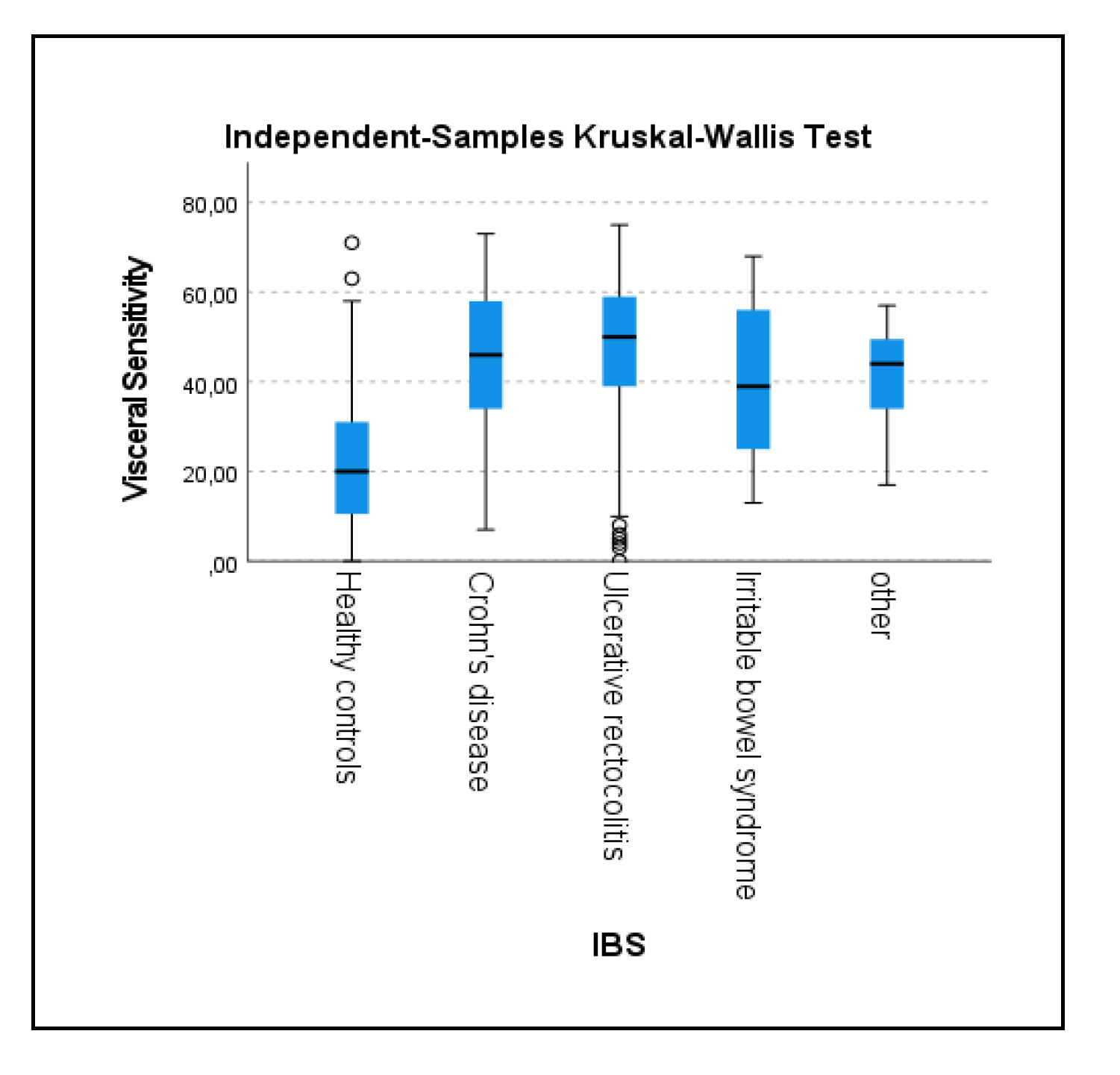
Figure 2.
- Comparisons between patient groups.
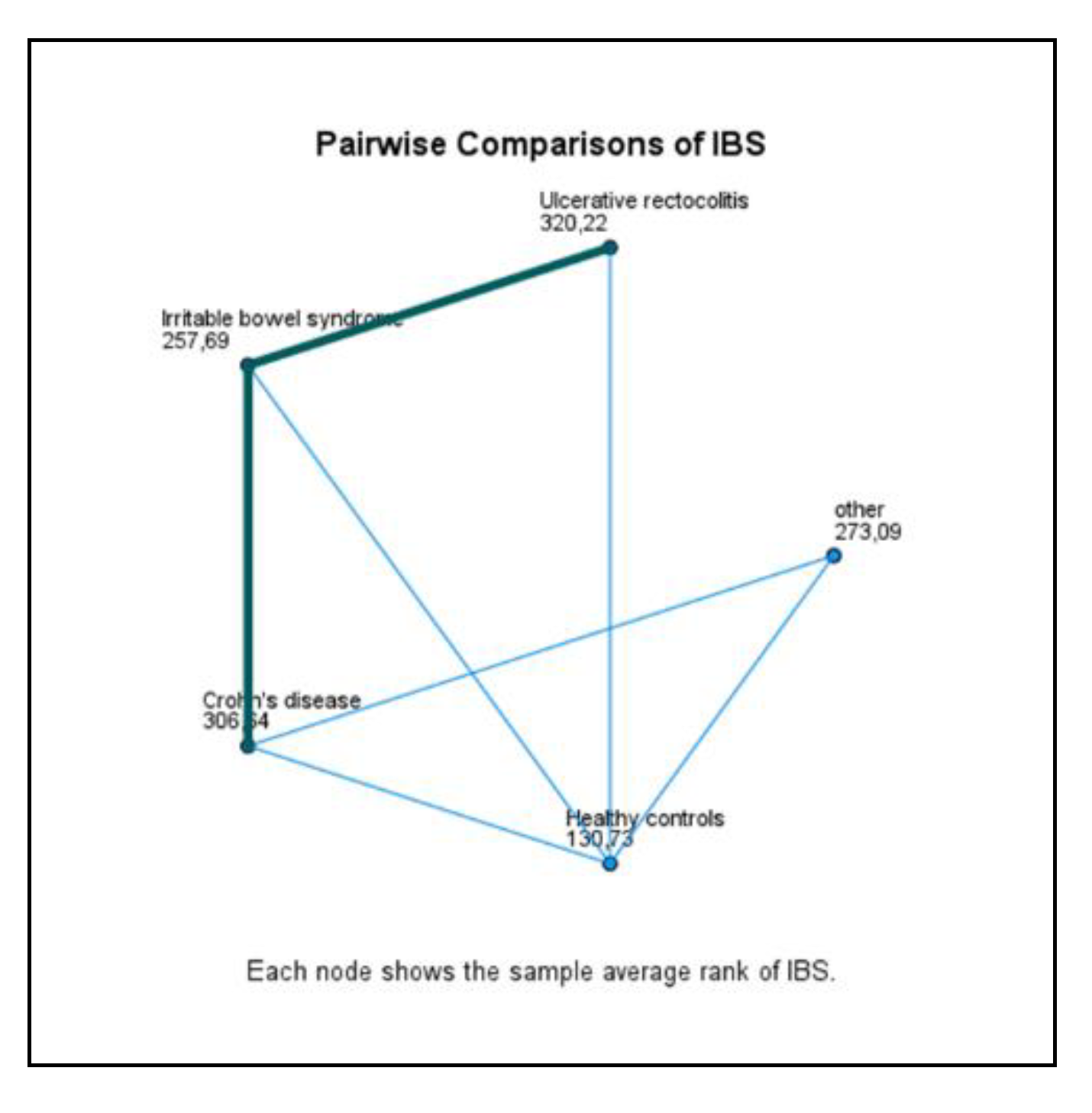
Figure 3.
– Boxplot of VSI-IT according to symptom severity.
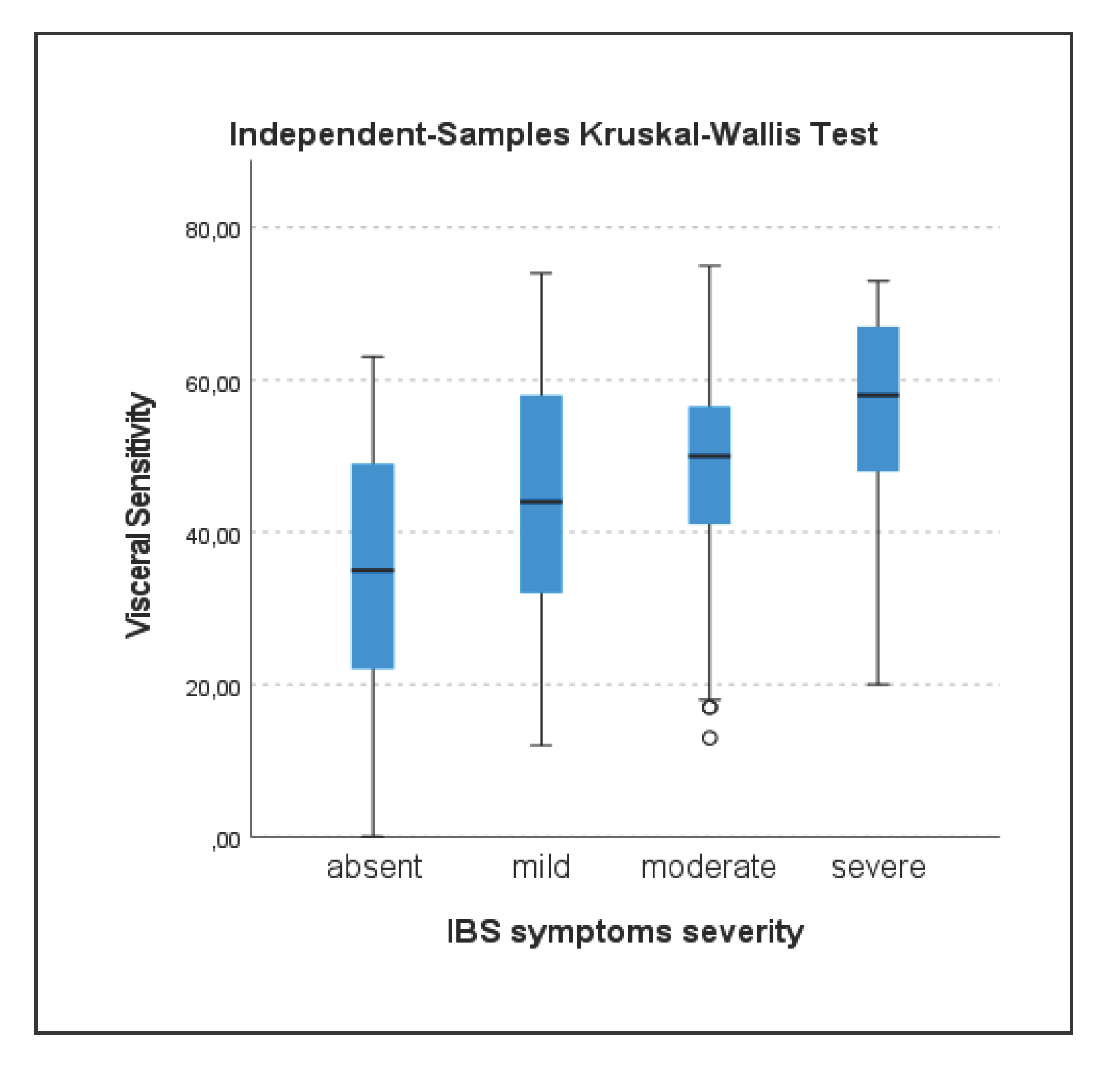

Table 1.
Factor loadings of the scale.
| VSI-IT Item | Item factor loading |
|---|---|
| Item 1 | 0.67 |
| Item 2 | 0.74 |
| Item 3 | 0.83 |
| Item 4 | 0.83 |
| Item 5 | 0.82 |
| Item 6 | 0.78 |
| Item 7 | 0.80 |
| Item 8 | 0.83 |
| Item 9 | 0.71 |
| Item 10 | 0.58 |
| Item 11 | 0.76 |
| Item 12 | 0.83 |
| Item 13 | 0.76 |
| Item 14 | 0.72 |
| Item 15 | 0.84 |
1 Legend: Extraction Method: Principal Component Analysis. 1 component extracted. Total of Variance explained= 58.964%.
Table 2.
Sensitivity and validity of VSI-IT in discriminating between various pathological conditions.
Table 2.
Sensitivity and validity of VSI-IT in discriminating between various pathological conditions.
| Healthy controls (N=164) | Crohn’s Disease (N=111) | Ulcerative Rectocolitis (N=180) | IBS (N=34) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| VSI-IT | M | SD | M | SD | M | SD | M | SD | |
| Item 1 | 2.31 | 1.668 | 3.26 | 1.367 | 3.19 | 1.468 | 2.94 | 1.455 | |
| Item 2 | 1.20 | 1.431 | 2.66 | 1.735 | 2.53 | 1.676 | 2.32 | 1.701 | |
| Item 3 | 1.96 | 1.543 | 3.77 | 1.270 | 3.75 | 1.303 | 3.12 | 1.647 | |
| Item 4 | 1.20 | 1.504 | 2.65 | 1.570 | 2.76 | 1.558 | 2.24 | 1.707 | |
| Item 5 | 1.45 | 1.560 | 3.37 | 1.414 | 3.44 | 1.503 | 3.44 | 1.397 | |
| Item 6 | 0.82 | 1.207 | 2.78 | 1.665 | 2.82 | 1.665 | 2.41 | 1.893 | |
| Item 7 | 0.89 | 1.324 | 2.22 | 1.603 | 2.29 | 1.629 | 2.03 | 1.547 | |
| Item 8 | 1.66 | 1.480 | 3.36 | 1.380 | 3.48 | 1.432 | 3.03 | 1.487 | |
| Item 9 | 0.94 | 1.313 | 3.00 | 1.868 | 3.22 | 1.802 | 1.53 | 1.482 | |
| Item 10 | 2.40 | 1.530 | 3.77 | 1.084 | 3.73 | 1.235 | 3.03 | 1.446 | |
| Item 11 | 1.10 | 1.373 | 2.71 | 1.410 | 2.95 | 1.503 | 1.88 | 1.533 | |
| Item 12 | 0.85 | 1.275 | 2.24 | 1.674 | 2.72 | 1.741 | 1.97 | 1.642 | |
| Item 13 | 1.65 | 1.497 | 3.09 | 1.462 | 3.31 | 1.454 | 2.74 | 1.729 | |
| Item 14 | 2.26 | 1.647 | 4.00 | 1.228 | 3.96 | 1.274 | 3.85 | 1.258 | |
| Item 15 | 0.92 | 1.242 | 2.64 | 1.565 | 2.91 | 1.520 | 2.41 | 1.725 | |
Table 3.
- Kruskall Wallis Test for independent samples.
| Sample 1-Sample 2 | Test Statistic | Std. Error | Std. Test Statistic | Sig. |
|---|---|---|---|---|
| Healthy controls-Irritable bowel syndrome | -126.96 | 27.18 | -4.67 | 0.00 |
| Healthy controls-waiting for diagnosis | -142.36 | 44.91 | -3.17 | 0.00 |
| Healthy controls-Crohn’s disease | -175.91 | 17.74 | -9.92 | 0.00 |
| Healthy controls-Ulcerative rectocolitis | -189.49 | 15.59 | -12.16 | 0.00 |
| Irritable bowel syndrome-waiting for diagnosis | -15.40 | 50.01 | -0.31 | 0.76 |
| Irritable bowel syndrome-Crohn’s disease | 48.95 | 28.26 | 1.73 | 0.08 |
| Irritable bowel syndrome-Ulcerative rectocolitis | 62.53 | 26.96 | 2.32 | 0.02 |
| Waiting for diagnosis-Crohn’s disease | 33.55 | 45.57 | 0.74 | 0.46 |
| Waiting for diagnosis-Ulcerative rectocolitis | 47.13 | 44.78 | 1.05 | 0.29 |
| Crohn’s disease-Ulcerative rectocolitis | -13.58 | 17.40 | -0.78 | 0.44 |
Table 4.
Pairwise Comparisons of symptoms severity.
| Sample 1-Sample 2 | Test Statistic | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. a |
|---|---|---|---|---|---|
| Absent-mild | -44.18 | 16.44 | -2.69 | 0.01 | 0.04 |
| Absent-moderate | -66.93 | 15.36 | -4.36 | 0.00 | 0.00 |
| Absent-severe | -119.58 | 19.94 | -6.00 | 0.00 | 0.00 |
| Mild-moderate | -22.75 | 12.76 | -1.78 | 0.08 | 0.45 |
| Mild-severe | -75.40 | 18.01 | -4.19 | 0.00 | 0.00 |
| Moderate-severe | -52.64 | 17.04 | -3.09 | 0.00 | 0.01 |
Legend: Each row tests the null hypothesis that the Sample 1 and Sample 2 distributions are the same. Asymptotic significances (2-sided tests) are displayed. The significance level is.050. Significance values have been adjusted by the Bonferroni correction for multiple tests.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



