
Submitted:
12 March 2024
Posted:
12 March 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Feline infectious peritonitis (FIP) is a fatal feline disease classified as either effusive (‘wet’), non-effusive (‘dry’), or a mixture of both forms (‘mixed’). The anti-FIP therapeutic effect of Mutian and molnupiravir, two drugs whose active ingredient is a nucleic acid analog, has been confirmed recently. Methods: Of the cats with FIP, we observed a total of 122 and 56 cases achieved remission after administration of Mutian and molnupiravir as routine treatments, respectively. Changes in clinical indicators suggested to be correlated with FIP remission (weight, hematocrit, and albumin to globulin ratio) before and after the administration of each drug and during follow-up observation were statistically compared for each FIP type. Results: In all three FIP types, administration of either Mutian or molnupiravir resulted in statistically significant increases in these indicators. Furthermore, the effect of Mutian on improving the albumin to globulin ratio was not observed at all in wet FIP, as compared with that of molnupiravir, but statistically significant in mixed and dry (P<0.02 and P<0.003, respectively). These clinical features were all due to differences in fluctuations of circulating globulin levels. Conclusions: These results indicate slight inflammatory responses might be elicited continuously by residual feline coronavirus non-disappeared through molnupiravir treatments.
Keywords:
cat
; feline infectious peritonitis
; non-effusive
; nucleic acid analog
; albumin to globulin ratio
; feline coronavirus
; routine treatment
1. Introduction
Feline infectious peritonitis (FIP) is a fatal feline disease caused by an exaggerated pro-inflammatory response to feline coronavirus (FCoV), and the cats infected with FCoV exhibit nonspecific clinical symptoms, such as recurrent fever, vomiting, and diarrhea, during the early stages of disease [1,2,3]. FIP is classified as effusive (wet), non-effusive (dry), or a mixture (mixed) of effusive and non-effusive forms [1,2]. The mixed type is a transitional state from one of the wet and dry types to the other and shows symptoms of both types at the same time [1,3,4]. The wet type is characterized by fibrotic pleura-peritonitis with vasculitis and exudation of body cavity fluid into adjacent areas, followed by accumulation of exudate in the body cavities, including the abdomen, thorax, pericardium, and scrotum. The dry type is characterized by granulomatous lesions in several organs, including the central nervous system, and clinical signs in the eyes, whereas in the mixed type, features of both types are observed simultaneously [1,4]. Currently, ante-mortem diagnosis of FIP is difficult, and there is no definitive noninvasive diagnostic test method for cats without body cavity fluid collection, which is diagnosed comprehensively based on the veterinarian’s examination of physical signs, the results of various clinical tests, and viral RNA detection in routine veterinary care [3,5,6].
There are no treatments for FIP that have been legalized for clinical use outside countries such as the UK, and supportive care aimed solely at prolonging survival has been widely used for many years [7,8]. Additionally, several previous studies have suggested the possibility of treating FIP with immune-stimulants or other related drugs; however, no clinical benefit has been demonstrated [9,10]. In 2018, the nucleic acid analog GS-441524 was found to inhibit the replication of FCoV [11]. The prodrug GS-441524 (GS-5734, remdesivir) inhibits the replication of several taxonomically diverse RNA viruses [12,13]. Subsequently, the administration of GS-441524 to cats with spontaneous FIP and its therapeutic effects were confirmed; however, the initial method of administration was limited to subcutaneous injection [14,15]. An oral formulation of GS-441524 (designated as “Mutian X” in the later section) was developed by the Chinese company, making it available for both oral administration and subcutaneous injection routes [16,17]. Recently, with informed consent from owners, we administered this drug to cats with FIP in our routine practice and investigated its effectiveness [18,19]. It was observed in these studies the remission rates were 82.3% (116 of 141 cases), 93.9% (153 of 163 cases), and 85.1% (137 of 161 cases) in the wet type, dry type, and mixed type FIP groups, respectively [18,19].
Additionally, molnupiravir (MPV), an orally administrable prodrug (EIDD2801) of N4-hydroxycytidine (EIDD1931) developed as an anti-COVID-19 drug, has been confirmed to exhibit antiviral activity against FCoV [20,21]. This drug has been approved in various countries as a treatment for human COVID-19 patients, and is now being used in veterinary care as a treatment for FIP in Japan. However, there has never been any comparative analysis to characterize the therapeutic effect on FIP disease between GS-442534-containing formulation, which has been used to treat many FIP cases, and the MPV for which there are few reports.
In this study, we compared the changes in the clinical indicators via several laboratory tests for each case when each drug was used as a single agent for FIP treatment under routine veterinary care and analyzed the effects of both drugs on the remission of FIP and quality of life of the cats according to the three disease types (wet, dry, and mixed). Furthermore, since both drugs routinely induce FIP remission, we investigated the differences in changes of clinical laboratory indicators, resultantly elucidating slight differences in their therapeutic efficacy, which may lead to contribute potential benefits to the cat’s owners. Therefore, to clarify statistical analysis, this study only included cases in which remission had been induced, and the cats for whom both drugs were used together were excluded even if administered temporarily.
2. Materials and Methods
2.1. Drugs and Administration
Orally administered Xraphconn (Mutian X) was purchased from Mutian Life Sciences (Nantong, China). The main active ingredient of Mutian X is demonstrated to be GS-441524 [22], and the manufacturer provides the information that the content of the main active ingredient in a 100 mg formulation is 5 mg [23]. Furthermore, the active ingredients in the subcutaneously administrative formulation (designated as “Mutian II”) are estimated to be the same as those in the orally administrative one, possible to be used interchangeably with Mutian X [19,24], and the both were collectively designated as “Mutian” in the following section. These preparations were administered to cats with FIP, which was carried out according to our previous reports [18,19]. Briefly, Mutian was administered q24 h orally or subcutaneously for 12 weeks, and the dosages were increased or decreased in the range of 100 to 200 mg/kg, depending on each FIP type and the disease stage. Oral administration was performed by the cat owners. Temporary administration of the injectable form (Mutian II) required hospitalization at our facility; however, long-term administration was performed under the supervision of a veterinarian near the owner’s home.
Commercially available MPV powder capsules (200 mg/capsule) were purchased from Healing Pharma (Mumbai, India), Azista Industries (Hyderabad, India) or Mankind Pharma (New Delhi, India). The MPV capsule powder was completely dissolved in a simple syrup and orally administered to the cats. The veterinarian prescribed a dosage within the range of 10 to 20 mg/kg, considering the disease types or severity stages of FIP, based on twice-daily administration for 12 consecutive weeks, according to published reports using MPV as the first-line therapy for FIP [25].
2.2. Patients and Diagnostic Procedures
We enrolled 178 cats presented to our hospitals, which were diagnosed with FIP, received treatment with Mutian or MPV, were followed up, and ultimately achieved remission between December 2021 and December 2023. Notably, most of the fatal cases had already become seriously ill and died during the early stages of treatment, before the apparent therapeutic effects were observed. These cases were excluded since the study focused on the long-term effectiveness of the treatment drugs, and the essential requirement for all test values at four time points for approximately ≥100 days survival time and onset of remission after treatments for statistical analysis.
The cats were diagnosed based on the same criteria as previously reported [18,19]. Clinical specimens (whole blood with EDTA or plasma samples isolated by centrifugation of heparinized whole blood) were collected at four time points: at the first dose, 1 month after starting the medication, after completion of each drug administration (84 days after the first dose), and 1–3 months after the completion of each medication. Body cavity effusions were collected from most cats with wet and mixed FIP. Total bilirubin (TB) and albumin to globulin ratio (A/G) (DRI-CHEM4000V system, FUJIFILM Corporation, Tokyo, Japan), serum amyloid-A (SAA) (DRI-CHEM IMMUNO AU10V system, FUJIFILM Corporation), EDTA-treated whole blood hematocrit (HCT) (MEK-6550 Celltac-α, NIHON KOHDEN Corporation, Tokyo, Japan), and α1-acid glycoprotein concentrations in plasma using the latex agglutination method (FUJIFILM VET Systems Co., Ltd., Tokyo, Japan) were also analyzed. Reverse transcriptase-PCR (RT-PCR) tests were performed by the Canine Lab Co., Ltd (Tokyo, Japan) as previously described [18,19]. The circulating levels for total globulin were determined by subtracting those for the albumin from those for total protein according to the general biochemical calculation formula. The parameters of appetite (volume, frequency, and speed of feed intake) and activity (movement, walking speed, and agility) were assessed during the initial interviews with the owners according to predetermined criteria and five interview items (classified into six stages 0–5), respectively. Each parameter was then converted to an arbitrary value as an appetite or activity score on a scale of 1–6; the scores were then analyzed statistically to assess the owner’s perception of the cat’s physical condition, along with the results of the routine physical examination at the clinic (body temperature, weight, ultrasonography, auscultation, and palpation). Ultrasonography was performed to determine the presence of ascites, pleural effusions, or swollen lymph nodes in the cats using the Aplio a CUS-AA000V ultrasound system (Canon Medtech Supply Co., Kanagawa, Japan).
The disease characteristics were confirmed through a comprehensive examination of the apparent clinical signs (anorexia, underactivity, vomiting, diarrhea, seizures, tremors, ataxia, etc), qualitative PCR-based detection of FCoV in the blood, ascites, pleural effusions, and laboratory tests (HCT, whole cell count, total protein, TB, A/G, SAA, α1-acid glycoprotein, and activity of hepatic enzymes). The age, body temperature, and weight of all cats were recorded during the initial consultation with the veterinarian. Etiological ante-mortem diagnosis of FIP may be difficult, if not impossible, due to the invasiveness of biopsy collection from a sick cat, since, there is currently no non-invasive confirmatory test available for cats without effusion [7]. Under such a circumstances, FIP diagnosis was made by a comprehensive analysis of the above indicators. Diagnostic and treatment histories from other institutions, breeding status, birth and adoption records, and the medical history of their previously cohabiting parents and siblings were also recorded. In order to prevent subjective biases that might have favored the author's theory construction, a nurse was required to help input information to the owner's questionnaire and care was taken exclude the veterinarian's subjectivity. The cases used in our previous study were excluded from this study. Cases in which both Mutian and MPV were used in combination were excluded from this study. Furthermore, cases whose survival was not achieved between the start of medication and completion of the follow-up period were also excluded from this study.
Cats with FIP were classified as wet, mixed, or dry at initial examination. The subsequent transition from wet to dry or from dry to wet conditions was not considered in this study. All cat owners were provided with detailed information regarding FIP treatment with Mutian and MPV, including the potential risks and benefits, estimated costs, and treatment duration. Written informed consent were obtained in advance from all owners regarding the selected treatment after mutual agreement between the veterinarians and owners. Additionally, both parties confirmed that Mutian or MPV were administered under optimal conditions to all cats as a standard of care and not as an experimental therapy. All data were obtained within the scope of normal veterinary practice and were appropriately anonymized. The studies were conducted in accordance with the local legislation and institutional requirements. The need for ethical review and approval was waived for these reasons.
2.3. Statistical Analysis
Age in months, appetite score, activity score, body temperature, and TB levels between the Mutian and MPV groups were compared statistically using the Mann–Whitney nonparametric U test. Kolmogorov–Smirnov test was used to assess the normality of distribution for the measured variables. Statistical analysis of body temperature and circulating SAA levels between them were performed by unpaired t-test as each of their data were judged to be normally distributed. Repeated measures ANOVA was used to determine any significant changes in the tested variables (body weight, HCT, and A/G) at four time points: at the time of the first dose, 1 month after starting the medication, after the completion of each drug administration (84 days after the first dose), and 1–3 months after the completion of each therapy. Repeated-measures ANOVA, accounting for the measurement of physical or clinical parameters (body weight, HCT, and A/G), treatment group (Mutian and MPV), and interaction of measurement and group, was used to determine and compare significant changes in the tested variables at the four time points in the groups. Differences were considered significant at P < 0.05. StatView 5.0 (SAS Institute, Cary, NC) was used for statistical analysis.
3. Results
3.1. Baseline Characteristics of Observed Participants
The 178 cats with FIP in this study were classified into wet (57 cases), mixed (61 cases), and dry types (60 cases) according to the initial diagnosis by veterinarians (Table 1 and Table 2). All cats received the standard treatment with Mutian or MPV for 84 days. After completion of the therapy, stable clinical signs with no obvious decline in quality of life were confirmed continuously by the end of the 3-month observation period, and the cats were determined to be in remission.
Of the 57 cases with wet type FIP in this study, 43 were administered Mutian and 14 were administered MPV after receiving prior veterinarian consultation. Similarly, among the 61 cases of mixed type FIP disease, 37 were treated with Mutian and 24 were treated with MPV. Furthermore, among all 60 cases of mixed type FIP, 42 received Mutian treatment and 18 received MPV treatment (Table 1 and Table 2). For each type of FIP (wet, mixed, or dry), there was no statistically significant difference between the Mutian-administered and MPV-administered case groups in terms of age in months, appetite score, activity score, body temperature, TB, or SAA value confirmed at the time of starting medication (Table 1). Based on the parametric statistical analysis (unpaired t-test), there were no significant difference in body temperature or SAA levels between the two groups, which were normally distributed parameters.
3.2. Changes of Clinical Parameters Over Times
Next, we examined the changes in the three parameters of body weight, HCT, and A/G values between four time points: the time of dosing each drug, 1 month later, the end of the standard dosing period, and their follow-up time point. In all disease type groups, statistical significance was confirmed in the variation patterns of each index between the four time points due to Mutian administration and MPV administration in body weight, HCT, and A/G values. The results of the repeated measures ANOVA showed that treatment with both drugs effectively changed all three indicators for all wet, mixed, and dry types (P < 0.0001).
Table 2 showed that no interaction was observed between the case groups treated with these two drugs in terms of increase in body weight and HCT for any disease type, and there was no statistically significant difference in the effects of the two drugs. Furthermore, regarding the course of the increase in A/G, the effects of both Mutian and MPV were not significantly different for the wet FIP (Figure 1A). However, an interaction between the two drugs was observed in either of the mixed or the dry FIP, and a statistically significant difference was detected between the two drugs in terms of their effects on the increasing trend of A/G as shown in Figure 1B or Figure 1C (P < 0.02 or P < 0.003, respectively). In addition, their increasing trends in the A/G appeared to be different throughout from initiation to the end of the administration period (Figure 1B and Figure 1C).
3.3. Changes of Albumin and Globulin Levels in Circulation Over Times
In order to investigate a key factor which has induced the phenomenon that the improvement trend of A/G ratio in dry and mixed type FIP cases was statistically different between two treatments, we tried to analyze the fluctuations of their albumin and globulin levels separately.
Regarding the course of the increase in albumin concentrations, the effects of both Mutian and MPV were not significantly different for the mixed FIP (Figure 2A). However, an interaction between the two drugs was observed for globulin levels in the mixed FIP, and a statistically significant difference was detected between the two drugs in terms of their effects on the increasing trend of globulin concentrations as shown in Figure 2B (P < 0.02). In dry type FIP, almost no changes in albumin concentrations along with the course of both treatments has been detected (Figure 3A). As comparable with those in the mixed type, however, a statistically significant difference was detected between the two drugs in terms of their effects on the increasing trend of globulin concentrations (Figure 3B, P < 0.02).
4. Discussion
Regarding the changes in the three parameters of body weight, HCT, and A/G values between the two time points of dosing each drug and the end of the standard treatment process, at least the changes in each parameter due to the Mutian formulation, we observed a significant increase in body weight, HCT, and A/G levels (Table 2 and Figure 1), similar to our previous reports [18,19]. Additionally, it was confirmed that both Mutian and MPV had statistically significant effects on the changes in each parameter between the four time points, including the follow-up time after the end of medication. Although our current study was conducted under conditions of general practice and with an extremely limited number of cases, this is the first study in which a comparative analysis of the time series was conducted using two different types of anti-FCoV nucleic acid analogs to evaluate their pharmacological effects in parallel.
Notably, this study might have entailed some biases, particularly regarding case selection for comparing the clinical effects of two distinct therapeutic drugs. However, since the purpose of the study was to compare their efficacy within the scope of routine medical treatment, we comparatively analyzed physical characteristics including disease severity. It was also necessary to ensure that the treatment groups did not differ significantly regarding physical and clinical conditions, including disease severity, to minimize the influence of these biases.
FIP is recognized as a disease that primarily affects cats aged between 6 months and 2 years of age [26]. It is also recognized that the initial diagnosis of this disease is based first and foremost on signalments, including the cat's age, place of birth, clinical signs, physical examination, and breeding status for cats between 4 and 36 months of age in group housing. In this study, we investigated the ages of all cats with FIP and analyzed whether there were any differences between the case groups. In addition, a persistent and undulating tendency to fever that is unresponsive to certain antibiotics strongly suggests FIP, as it is unlikely that there are any other diseases that produce these symptoms [5]. We referred to existing information obtained from the initial diagnosis of FIP and have shown that the measured body temperature may be a useful numerical index for predicting the effect of Mutian treatment on subsequent FIP disease, in addition to the appetite and activity scores calculated based on the results of interviews with owners at the time of the first diagnosis in the previous studies [18,19].
Hyperbilirubinemia and hyperbilirubinuria commonly occur in FIP, and both have no correlation with the blood concentrations of liver dysfunction indicators and are known to occur particularly at high frequencies in effusive FIP [7]. The previous studies demonstrated that the TB concentration at the time of initial diagnosis is a useful clinical index for predicting the subsequent therapeutic effect of Mutian and that this phenomenon is limited to effusive FIP [18,19]. Furthermore, as an acute phase protein, SAA is known to be normally almost undetectable and increase with viral infections that cause acute systemic inflammation. Elevated SAA levels may facilitate early and effective detection of many viral infections such as FIP, since it strongly mirrors clinical condition [27]. Although these six clinical or physical numerical indicators, including age, may be correlated with the prognosis of the therapeutic effect of the nucleic acid analog preparation, no statistically significant differences were detected between the parameters of the two treatment groups, and no significant differences were observed for each FIP type in the present study (Table 1). Considering the above results, we consequently judged that there was no noteworthy difference in FIP severity or physical condition at their first visit to our hospital, which may affect the effectiveness of subsequent drug treatment, between cats whose owners selected the administration of Mutian and MPV.
In the present study, although not observed in wet type FIP, a different effect of the two drugs on the A/G increase was observed in each of mixed and dry type, and the difference was confirmed to be apparently significant (Figure 1B and Figure 1C, respectively). In the four-time series period of the Mutian and MPV treatment groups for dry type disease, the tendency for an increase in A/G after the end of the treatment period was clearly different between the two drugs, and a significant difference was observed in the period from the end of treatment to follow-up observation (Figure 1C). One retrospective study in China previously indicated critical value of the A/G could be considered as 0.5, FIP was negligibly detected when the A/G > 0.8 and its possibility remained within those ranges [28]. In our present study, even if observed in the mixed and the dry FIP cases, their A/G reached around 0.8 only at Mutian administration, suggesting the disease remission might be more evident (Figure 1B and Figure 1C). These data led to some possible assumptions as follows: either the therapeutic effect of Mutian on dry type FIP is superior to that of MPV, MPV has any independent negative effects (including unknown adverse effects or irregular pharmacokinetics) of its own, or both occur simultaneously.
Because MPV has been confirmed to have medicinal efficacy in treating coronavirus infections other than FCoV, some owners have used commercially available MPV to treat cats with FIP at home. However, there have been extremely limited reports that scientifically verified the clinical effects of MPV on FIP [29]. One previous report suggested that it is desirable to use MPV as an emergency treatment when disease symptoms persist or recur after a cat with suspected FIP is treated as the first-line therapy using drugs with proven track records, such as GS-441524 [25]. In the other study, several cases were confirmed that exhibited nausea symptoms even with the standard dose of MPV (10 mg/kg, twice a day); when the dose was further increased (23 mg/kg, twice a day), various side effects (ear breakage, hair loss, and severe leukopenia) have been observed with multiple administrations of MPV [25,30]. Furthermore, unlike the wet type, the dry and mixed types of FIP are characterized by granulomatous lesions in various organs of the body, ocular symptoms, and neurological symptoms [1,5,6,7]. It has been confirmed that the anti-FCoV agent GS-441524, MPV, and its activated form N4-hydroxycytidine (EIDD1931) can cross the blood–brain barrier and migrate into the brain after administration into the blood. However, because the transfer efficiency from circulation to intraocular tissues and cranial nerves is not sufficient, it is necessary to increase the dosage to obtain a sufficient amount of the drug [11,31,32]. In our study, we included cases in which the dosage of MPV was increased to a maximum of 20 mg/kg twice a day, depending on the symptoms of each type of FIP; however, higher dosages were not always observed in non-effusive FIP (data not presented). The relationship between the phenomenon observed here and the abovementioned issues reported with MPV requires further research on the following hypothesis; individual differences in the pharmacokinetics of MPV administered to cats may potentially lead to low efficiency in the active ingredient leach to granulomatous tissues characteristic of mixed or dry FIP, resultantly causing virus persistence possibly in some cases.
Three disease types of FIP (wet, mixed and dry types) are presumed to occur because of the status of the host defense immunity against FCoV [1]. Macrophages infected with FCoV acquire the ability to destroy viruses; however, infected macrophages can be recognized as foreign substances by the host immune system and are further destroyed. If cell-mediated immunity is well developed early in the infection process, clinical signs of FIP will not occur and viral replication will be inhibited; however, if humoral immunity occurs but cell-mediated immunity does not develop; wet type FIP develops resultantly. However, an intermediate stage of immunity involving strong humoral and weak cellular immunity may also occur simultaneously, resulting in the development of a mixed type. If the equilibrium between humoral and cell-mediated immunity persists, a dry type FIP develops [1]. In all disease types, an increase in the concentration of γ-globulin, which is mainly composed of antibodies in serum proteins, accompanying enhancement of humoral immunity is a clinical chemical feature commonly observed in all of the FIP cats [26,33]. Most cats with FIP present with abnormalities in serum biochemistry, primarily hyperproteinemia, hyperglobulinemia (even in the absence of increased serum total protein), and hypoalbuminemia. Furthermore, among these biochemical abnormalities, hyperglobulinemia has the highest frequency at 89% [26,33]. Our present study has revealed that the discrepant fluctuation of A/G levels between Mutian– and MPV–administered FIP cases is due to the differences in reducing tendency of circulating globulin concentrations in them (Figure 2 and 3). We can reasonably understand, therefore, insufficiently-reduced levels of circulating globulin (mainly defined as immunoglobulin) indicate any residual infective agents such as FCoV retained in the MPV-administered cats. Although MPV has been the first oral antiviral authorized for COVID-19, however, it has recently reported to be associated with poor clinical efficacy, the risk of creating novel coronavirus variants of concern, and long-term risk for mutagenicity in humans [34]. The former two are severe concerns, especially in the FIP treatments considered in the current study. From the above perspective, alternative antivirals such as Mutian formulation should be preferred over MPV.
The first limitation of our present study was that this study appears to be insufficient as a formal test for evaluating the clinical effectiveness of a new therapeutic agent. In the initial step of evaluating the clinical efficacy of a new drug, it is desirable to conduct a clinical trial based on case selection using a random sampling method, such as a randomized placebo-controlled clinical trial. First, there are no officially approved drugs or treatments for FIP, and it is difficult to establish a comparative therapy or positive control drug. A blinded non-inferiority study to compare the clinical effects of GS-441524 and remdesivir on FIP has recently been conducted, and the authors have also reported that the initiation of medication was delayed because of allocation and long-distance transport of the cats, resulting in lower remission rates for both therapies compared to other previous reports [35]. Unfortunately, setting up such a controlled clinical trial seems difficult because our top priority in routine clinical practice is to save each cat's life. The results of this non-inferiority trial indicate that it may be important to ensure the success rate of prospective treatment to gain owners’ attendance.
The second limitation of this study was that the population of the cat FIP group used for comparison was slightly small; in particular, the number of cases in which MPV was administered as a first-line drug was extremely small (14 to 24 cases). Furthermore, in this study, we compared physical signs and disease severity before treatment between the Mutian and MPV administration groups to maximize our ability to confirm the equivalence between these two groups, but it is difficult to deny that there may be any bias in the selection of cases in either of these groups with respect to determining the effectiveness of the drugs. For example, because MPV is limited to oral administration, cases in which oral administration is difficult due to gastrointestinal disorders must be automatically excluded. In contrast, Mutian can be administered both subcutaneously and orally; therefore, cats with possible gastrointestinal disorders are not usually excluded, resulting in the fact that this type of bias does not occur because Mutian can be administered subcutaneously to cats that are unable to swallow. In future, the manufacturers and distributors of each drug should take the lead in taking these points into account and set appropriate conditions, especially in case selection, planning, and execution of clinical trials, leading to their formal approval from the authorities.
The third limitation involved potential ethical and legal issues. First, uncontrolled expansion of utilization of antiviral agents may accelerate FCoV mutation itself, which in turn may lead to the generation of new infectious viruses potentially harmful to humans. We previously stated that the widespread use of antiviral drugs as preemptive therapy does not benefit the public as it increases the risk of multi-drug resistance and epidemic infections [18]. We cannot recommend the widespread use of such anti-FIP drugs without veterinary supervision, or that the cat’s owners without medicinal knowledge voluntarily obtain these drugs through the online shopping and dose them to their cats at home. We also strongly discourage the owner-driven, autonomous practice of administering any medicines to pets, and instruct owners who visit our hospital to always administer medication under veterinarian’s consultation and supervision. Of course, we only administered anti-FIP drugs to the cases suspected as FIP through our diagnosis, and ensured that benefits to the cases and their owners outweigh the risks. In this study, only qualitative detection of residual virus in body fluids and feces was performed using PCR. Unfortunately, PCR tests are currently outsourced to external organizations and are only qualitative tests unable to detect all virus mutations. We recognize that molecular biology-based verification may be very important in detecting FCoV mutations, and look forward to future scientific progress by specialists for detecting resistant viral mutations caused by antiviral drugs. Regarding legal issues, under the current legal framework in Japan, the use of any unauthorized veterinary drugs as therapeutics is recognized within the judgment and discretion of individual veterinarians with prior consent of pet owners. Furthermore, we consulted a lawyer in Japan regarding this issue and confirmed that there were no legal issues.
Recently, a long-term prognostic follow-up study for 1 year after confirmation of remission after treatment of FIP with Mutian X (orally administered GS-441524) was conducted, demonstrating its effectiveness against FIP in both the short and long term, with no significant relapse [36]. Considering the results of our study and those of previous reports, oral GS-441524 may still be preferable as a first-line drug for FIP therapy. MPV should be considered for use in cats if Mutian’s efficacy is not expected, but veterinarians should be careful when increasing the MPV dosage.
5. Conclusions
In this study, we confirmed significant improvements in the physical and clinical laboratory indicators for each type of FIP by administering Mutian or MPV, which have already been reported as drugs for the treatment of FIP, and confirmed clear therapeutic effects. Statistical analysis of transitional changes in the clinical parameters (body weight, HCT, and A/G levels) suggested to be correlated with FIP remission before and after each drug administration, and at subsequent follow-up observations for each type of FIP group revealed a significant difference in the effects of both drugs on A/G transition fluctuations, especially in cats with mixed or dry type FIP. The clinical features observed in these cases were all due to differences in fluctuations of circulating globulin levels, indicating host immuno-responses might be induced by residual FCoV after MPV treatments. This phenomenon confirmed this time may help us elucidate the relationship between the granulomatous inflammation in several organs of non-effusive FIP, tissue distribution of antiviral therapeutics and A/G fluctuations, as well as the future directions in developing new nucleic acid analogs effective for FCoV.
Author Contributions
Conceptualization, M.K.; methodology, M.K.; software, M.K.; validation, M.K., Y.U. and D.K.; formal analysis, M.K.; investigation, M.K.; resources, M.K.; data curation, Y.U.; writing—original draft preparation, M.K.; writing—review and editing, Y.U and D.K.; visualization, M.K.; supervision, M.K.; project administration, M.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The studies were conducted in accordance with the local legislation and institutional requirements. Ethical review and approval were waived for the present study because all data were obtained within the scope of usual veterinary care and were anonymized.
Informed Consent Statement
Written informed consent was obtained from the owners for the participation of their animals in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Data Availability Statement
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to express sincere gratitude to the staff in Bloom Animal Hospital and Katori Animal Hospital for their support during clinical specimen processing and interviewing the owners.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Pedersen, N.C. A review of feline infectious peritonitis virus infection: 1963-2008. J. Feline Med. Surg. 2009, 11, 225–258. [Google Scholar] [CrossRef]
- Tekes, G.; Thiel, H.J. Feline coronaviruses: pathogenesis of feline infectious peritonitis. Adv. Virus Res. 2016, 96, 193–218. [Google Scholar]
- Thayer, V.; Gogolski, S.; Felten, S.; Hartmann, K.; Kennedy, M.; Olah, G.A. 2022 AAFP/everycat feline infectious peritonitis diagnosis guidelines. J. Feline Med. Surg. 2022, 24, 905–933. [Google Scholar] [CrossRef]
- Kipar, A.; Meli, M.L. Feline infectious peritonitis: still an enigma? Vet. Pathol. 2014, 51, 505–526. [Google Scholar] [CrossRef]
- Pedersen, N.C. An update on feline infectious peritonitis: diagnostics and therapeutics. Vet. J. 2014, 201, 133–141. [Google Scholar] [CrossRef]
- Felten, S.; Hartmann, K. Diagnosis of feline infectious peritonitis: a review of the current literature. Viruses. 2019, 11, 1068. [Google Scholar] [CrossRef]
- Addie, D.; Belák, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Hosie, M.J.; Lloret, A.; Lutz, H.; et al. Feline infectious peritonitis. ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Gunn-Moore, D.; Barker, E.; Taylor, S.; Tasker, S.; Sorrell, S. An update on treatment of FIP in the UK. Vet. Times. 2024, 51, 8–11. Available online: https://www.vettimes.co.uk/article/an-update-on-treatment-of-fip-in-the-uk-cpdfip/ [Accessed February 9, 2024].
- Ritz, S.; Egberink, H.; Hartmann, K. Effect of feline interferon-omega on the survival time and quality of life of cats with feline infectious peritonitis. J. Vet. Intern. Med. 2007, 21, 1193–1197. [Google Scholar] [PubMed]
- Tanaka, Y.; Sato, Y.; Osawa, S.; Inoue, M.; Tanaka, S.; Sasaki, T. Suppression of feline coronavirus replication in vitro by cyclosporin A. Vet. Res. 2012, 43, 41. [Google Scholar] [CrossRef]
- Murphy, B.G.; Perron, M.; Murakami, E.; Bauer, K.; Park, Y.; Eckstrand, C.; Liepnieks, M.; Pedersen, N.C. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet. Microbiol. 2018, 219, 226–233. [Google Scholar] [CrossRef]
- Brown, A.J.; Won, J.J.; Graham, R.L.; Dinnon, K.H., 3rd.; Sims, A.C.; Feng, J.Y.; Cihlar, T.; Denison, M.R.; Baric, R.S.; Sheahan, T.P. Broad spectrum antiviral remdesivir inhibits human endemic and zoonotic deltacoronaviruses with a highly divergent RNA dependent RNA polymerase. Antiviral Res. 2019, 169, 104541. [Google Scholar] [CrossRef]
- Amirian, E.S.; Levy, J.K. Current knowledge about the antivirals remdesivir (GS-5734) and GS-441524 as therapeutic options for coronaviruses. One Health. 2020, 9, 100128. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Perron, M.; Bannasch, M.; Montgomery, E.; Murakami, E.; Liepnieks, M.; Lie, H. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, P.J.; Bannasch, M.; Thomasy, S.M.; Murthy, V.D.; Vernau, K.M.; Liepnieks, M.; Montgomery, E.; Knickelbein, K.E.; Murphy, B.; Pedersen, N.C. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. J. Vet. Intern. Med. 2020, 34, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Addie, D.D.; Covell-Ritchie, J.; Jarrett, O.; Fosbery, M. Rapid resolution of non-effusive feline infectious peritonitis uveitis with an oral adenosine nucleoside analogue and feline interferon omega. Viruses. 2020, 12, 1216. [Google Scholar] [CrossRef] [PubMed]
- Addie, D.D.; Curran, S.; Bellini, F.; Crowe, B.; Sheehan, E.; Ukrainchuk, L.; Decaro, N. Oral Mutian®X stopped faecal feline coronavirus shedding by naturally infected cats. Res. Vet. Sci. 2020, 130, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Katayama, M.; Uemura, Y. Therapeutic effects of Mutian® Xraphconn on 141 client-owned cats with feline infectious peritonitis predicted by total bilirubin levels. Vet. Sci. 2021, 8, 328. [Google Scholar] [CrossRef] [PubMed]
- Katayama, M.; Uemura, Y. Prognostic prediction for therapeutic effects of Mutian on 324 client-owned cats with feline infectious peritonitis based on clinical laboratory indicators and physical signs. Vet. Sci. 2023, 10, 136. [Google Scholar] [CrossRef]
- Wahl, A.; Gralinski, L.E.; Johnson, C.E.; Yao, W.; Kovarova, M.; Dinnon, K.H., 3rd; Liu, H.; Madden, V.J.; Krzystek, H.M.; De, C.; et al. SARS-CoV-2 infection is effectively treated and prevented by EIDD-2801. Nature. 2021, 591, 451–457. [Google Scholar] [CrossRef]
- Cook, S.E.; Vogel, H.; Castillo, D.; Olsen, M.; Pedersen, N.; Murphy, B.G. Investigation of monotherapy and combined anticoronaviral therapies against feline coronavirus serotype II in vitro. J. Feline Med. Surg. 2022, 24, 943–953. [Google Scholar] [CrossRef]
- Krentz, D.; Zenger, K.; Alberer, M.; Felten, S.; Bergmann, M.; Dorsch, R.; Matiasek, K.; Kolberg, L.; Hofmann-Lehmann, R.; Meli, M.L.; et al. Curing cats with feline infectious peritonitis with an oral multi-component drug containing GS-441524. Viruses. 2021, 13, 2228. [Google Scholar] [CrossRef] [PubMed]
- Homepage of Mutian Life Sciences Co., Ltd. Available online: https://www.mutian.com/en/ [Accessed February 9, 2024].
- Addie, D.D.; Silveira, C.; Aston, C.; Brauckmann, P.; Covell-Ritchie, J.; Felstead, C.; Fosbery, M.; Gibbins, C.; Macaulay, K.; McMurrough, J.; et al. Alpha-1 acid glycoprotein reduction differentiated recovery from remission in a small cohort of cats treated for feline infectious peritonitis. Viruses. 2022, 14, 744. [Google Scholar] [CrossRef]
- Roy, M.; Jacque, N.; Novicoff, W.; Li, E.; Negash, R.; Evans, S.J.M. Unlicensed molnupiravir is an effective rescue treatment following failure of unlicensed GS-441524-like therapy for cats with suspected feline infectious peritonitis. Pathogens. 2022, 11, 1209. [Google Scholar] [CrossRef]
- Riemer, F.; Kuehner, K.A.; Ritz, S.; Sauter-Louis, C.; Hartmann, K. Clinical and laboratory features of cats with feline infectious peritonitis--a retrospective study of 231 confirmed cases (2000-2010). J. Feline Med, Surg. 2016, 18, 348–356. [Google Scholar] [CrossRef]
- Rossi, G. Acute phase proteins in cats: Diagnostic and prognostic role, future directions, and analytical challenges. Vet. Clin. Pathol. 2023, 52 (Suppl. 1), 37–49. [Google Scholar] [CrossRef]
- Yin, Y.; Li, T.; Wang, C.; Liu, X.; Ouyang, H.; Ji, W.; Liu, J.; Liao, X.; Li, J.; Hu, C. A retrospective study of clinical and laboratory features and treatment on cats highly suspected of feline infectious peritonitis in Wuhan, China. Sci. Rep. 2021, 11, 5208. [Google Scholar] [CrossRef] [PubMed]
- Sase, O. Molnupiravir treatment of 18 cats with feline infectious peritonitis: A case series. J. Vet. Intern. Med. 2023, 37, 1876–1880. [Google Scholar] [CrossRef]
- Cook, S.; Wittenburg, L.; Yan, V.C.; Theil, J.H.; Castillo, D.; Reagan, K.L.; Williams, S.; Pham, C.D.; Li, C.; Muller, F.L.; et al. An optimized bioassay for screening combined anticoronaviral compounds for efficacy against feline infectious peritonitis virus with pharmacokinetic analyses of GS-441524, remdesivir, and molnupiravir in cats. Viruses. 2022, 14, 2429. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, P.J. Coronavirus infection of the central nervous system: animal models in the time of COVID-19. Front. Vet. Sci. 2020, 7, 584673. [Google Scholar] [CrossRef]
- Chang, C.H.; Peng, W.Y.; Lee, W.H.; Lin, T.Y.; Yang, M.H.; Dalley, J.W.; Tsai, T.H. Biotransformation and brain distribution of the anti-COVID-19 drug molnupiravir and herb-drug pharmacokinetic interactions between the herbal extract Scutellaria formula-NRICM101. J. Pharm. Biomed. Anal. 2023, 234, 115499. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.Y.; Wang, Q.; Liang, X.Y.; Zhang, S.; Bao, D.; Zhao, H.; Li, S.B.; Wang, K.; Hu, G.X.; Gao, F.S. An updated review of feline coronavirus: mind the two biotypes. Virus Res. 2023, 326, 199059. [Google Scholar] [CrossRef] [PubMed]
- Focosi, D. Molnupiravir: From Hope to Epic Fail? Viruses 2022, 14, 2560. [Google Scholar] [CrossRef] [PubMed]
- Cosaro, E.; Pires, J.; Castillo, D.; Murphy, B.G.; Reagan, K.L. Efficacy of oral remdesivir compared to GS-441524 for treatment of cats with naturally occurring effusive feline infectious peritonitis: a blinded, non-inferiority study. Viruses 2023, 15, 1680. [Google Scholar] [CrossRef]
- Zwicklbauer, K.; Krentz, D.; Bergmann, M.; Felten, S.; Dorsch, R.; Fischer, A.; Hofmann-Lehmann, R.; Meli, M.L.; Spiri, A.M.; Alberer, M.; et al. Long-term follow-up of cats in complete remission after treatment of feline infectious peritonitis with oral GS-441524. J. Feline Med. Surg. 2023, 25, 1098612X231183250. [Google Scholar] [CrossRef]
Figure 1.
Changes of A/G in Mutian and MPV administration groups in the cat with wet type (A), mixed type (B) and dry type FIP (C). Statistically significant differences between treatments (Mutian and MPV) for the effects on each parameter were determined using repeated-measures ANOVA. Of the 57 cases with wet type FIP, 43 were administered Mutian and 14 were administered MPV. Among the 61 cases of mixed type, 37 were treated with Mutian and 24 were treated with MPV, and among the 60 cases of dry type, 42 received Mutian and 18 received MPV treatment. The cats were tested at four time points: at the first dose (Pre), 1 month after starting the medication (Interim), after completion of each drug administration (Post), and 1–3 months after completion of each medication (Follow-up). Symbols and vertical lines in the graph indicate mean values and standard errors, respectively. Abbreviations: A/G: albumin to globulin ratio, MPV: molnupiravir; FIP: feline infectious peritonitis; NS: not significant.
Figure 1.
Changes of A/G in Mutian and MPV administration groups in the cat with wet type (A), mixed type (B) and dry type FIP (C). Statistically significant differences between treatments (Mutian and MPV) for the effects on each parameter were determined using repeated-measures ANOVA. Of the 57 cases with wet type FIP, 43 were administered Mutian and 14 were administered MPV. Among the 61 cases of mixed type, 37 were treated with Mutian and 24 were treated with MPV, and among the 60 cases of dry type, 42 received Mutian and 18 received MPV treatment. The cats were tested at four time points: at the first dose (Pre), 1 month after starting the medication (Interim), after completion of each drug administration (Post), and 1–3 months after completion of each medication (Follow-up). Symbols and vertical lines in the graph indicate mean values and standard errors, respectively. Abbreviations: A/G: albumin to globulin ratio, MPV: molnupiravir; FIP: feline infectious peritonitis; NS: not significant.
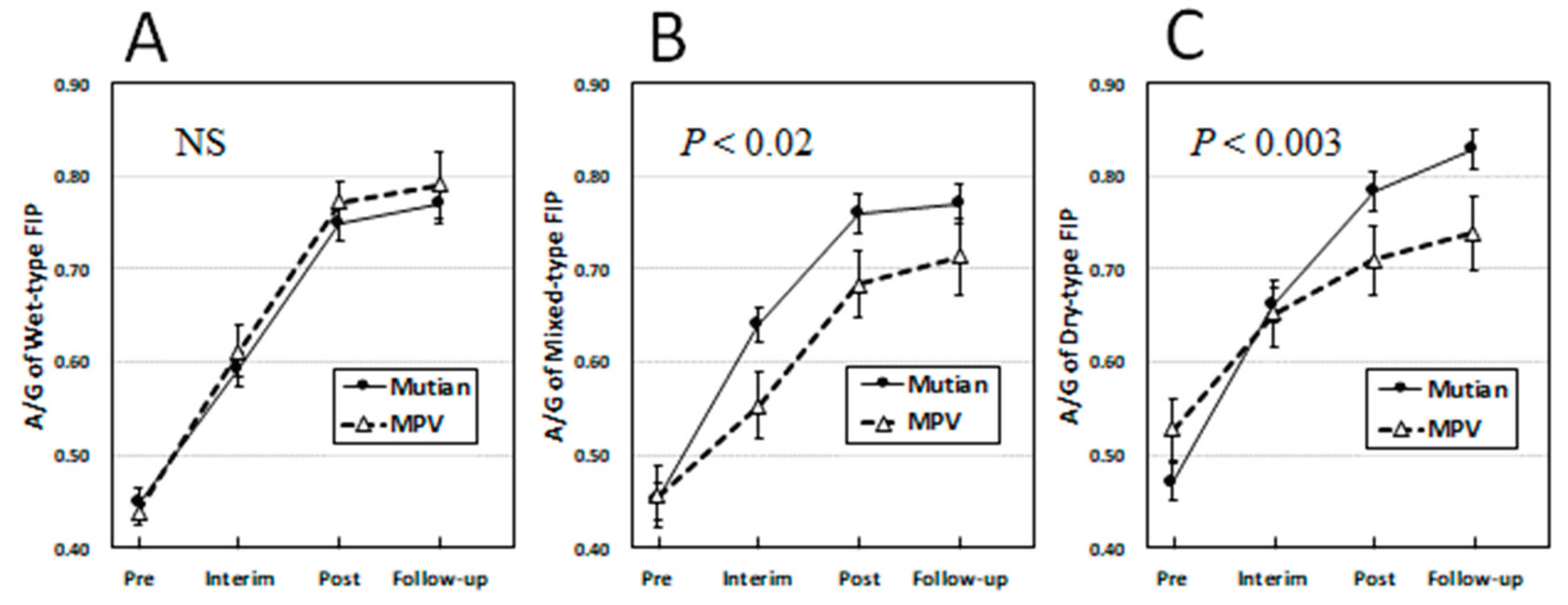
Figure 2.
Changes of albumin (A) and globulin concentration (B) in Mutian and MPV administration groups in the cat with mixed type FIP. Statistically significant differences between treatments (Mutian and MPV) for the effects on each parameter were determined using repeated-measures ANOVA. Among the 61 cases of mixed type, 37 were treated with Mutian and 24 were treated with MPV. The cats were tested at four time points: at the first dose (Pre), 1 month after starting the medication (Interim), after completion of each drug administration (Post), and 1–3 months after completion of each medication (Follow-up). Symbols and vertical lines in the graph indicate mean values and standard errors, respectively. Abbreviations: MPV: molnupiravir; FIP: feline infectious peritonitis; NS: not significant.
Figure 2.
Changes of albumin (A) and globulin concentration (B) in Mutian and MPV administration groups in the cat with mixed type FIP. Statistically significant differences between treatments (Mutian and MPV) for the effects on each parameter were determined using repeated-measures ANOVA. Among the 61 cases of mixed type, 37 were treated with Mutian and 24 were treated with MPV. The cats were tested at four time points: at the first dose (Pre), 1 month after starting the medication (Interim), after completion of each drug administration (Post), and 1–3 months after completion of each medication (Follow-up). Symbols and vertical lines in the graph indicate mean values and standard errors, respectively. Abbreviations: MPV: molnupiravir; FIP: feline infectious peritonitis; NS: not significant.
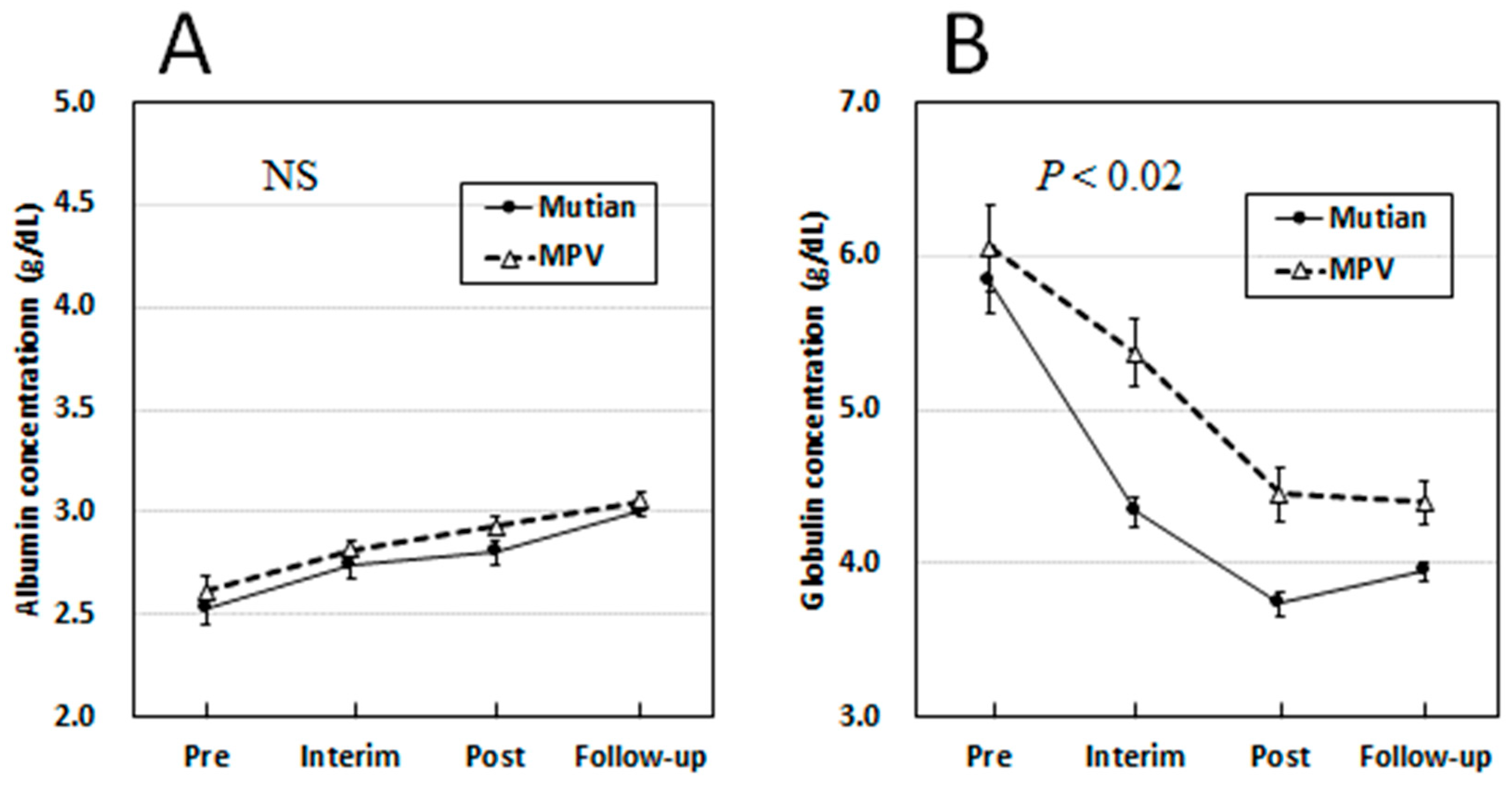
Figure 3.
Changes of albumin (A) and globulin concentration (B) in Mutian and MPV administration groups in the cat with dry type FIP. Statistically significant differences between treatments (Mutian and MPV) for the effects on each parameter were determined using repeated-measures ANOVA. Among the 60 cases of mixed type, 42 were treated with Mutian and 18 were treated with MPV. The cats were tested at four time points: at the first dose (Pre), 1 month after starting the medication (Interim), after completion of each drug administration (Post), and 1–3 months after completion of each medication (Follow-up). Symbols and vertical lines in the graph indicate mean values and standard errors, respectively. Abbreviations: MPV: molnupiravir; FIP: feline infectious peritonitis; NS: not significant.
Figure 3.
Changes of albumin (A) and globulin concentration (B) in Mutian and MPV administration groups in the cat with dry type FIP. Statistically significant differences between treatments (Mutian and MPV) for the effects on each parameter were determined using repeated-measures ANOVA. Among the 60 cases of mixed type, 42 were treated with Mutian and 18 were treated with MPV. The cats were tested at four time points: at the first dose (Pre), 1 month after starting the medication (Interim), after completion of each drug administration (Post), and 1–3 months after completion of each medication (Follow-up). Symbols and vertical lines in the graph indicate mean values and standard errors, respectively. Abbreviations: MPV: molnupiravir; FIP: feline infectious peritonitis; NS: not significant.
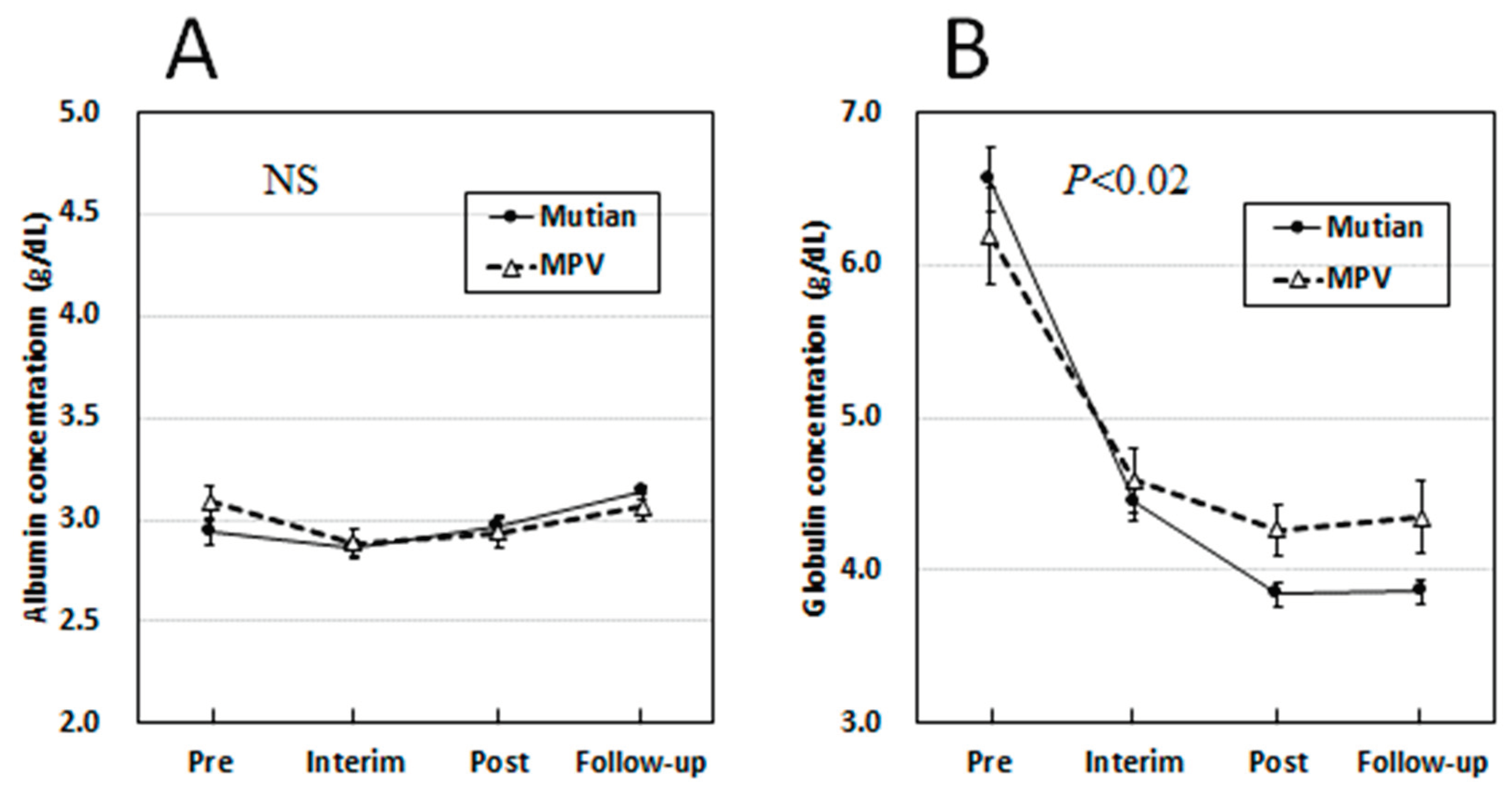

Table 1.
Statistical comparison of parameters between Mutian and MPV treatment groups for each disease type of FIP.
Table 1.
Statistical comparison of parameters between Mutian and MPV treatment groups for each disease type of FIP.
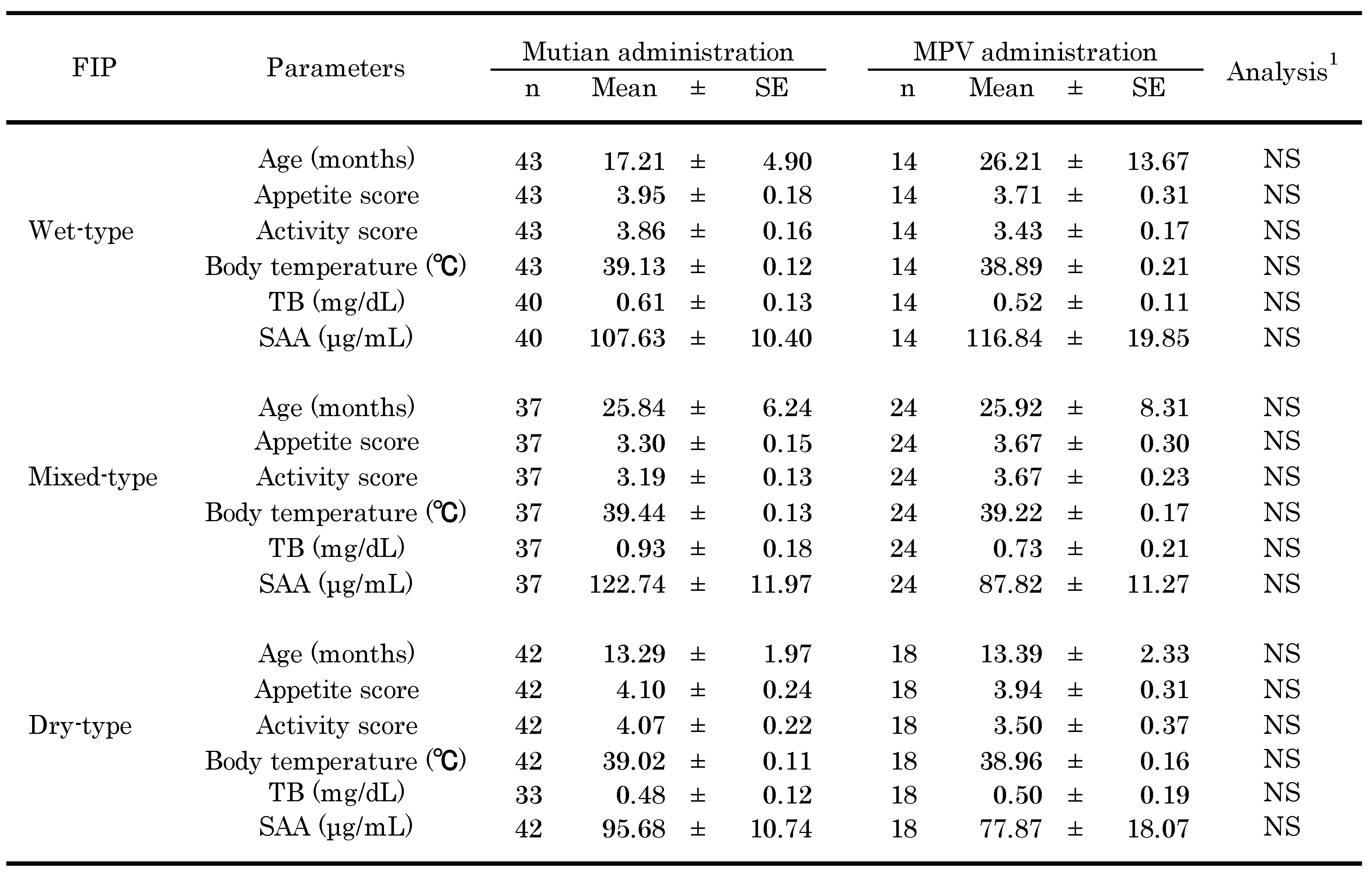
1 Statistically differences between each of some parameters (age, appetite score, activity score and TB levels) in both drug administration groups were determined by the Mann-Whitney nonparametric method, and those between each of the others (body temperature and SAA levels) were determined by unpaired t-test as each of their data were assessed to be normally distributed by Kolmogorov-Smirnov test method. Abbreviations: MPV: molnupiravir; TB: total bilirubin; SAA: serum amyloid-A; FIP: feline infectious peritonitis; NS: not significant; SE: standard error of the mean.
Table 2.
Repeated measures ANOVA of the effects of Mutian and MPV administration on changes of physical and clinical parameters by FIP types.
Table 2.
Repeated measures ANOVA of the effects of Mutian and MPV administration on changes of physical and clinical parameters by FIP types.
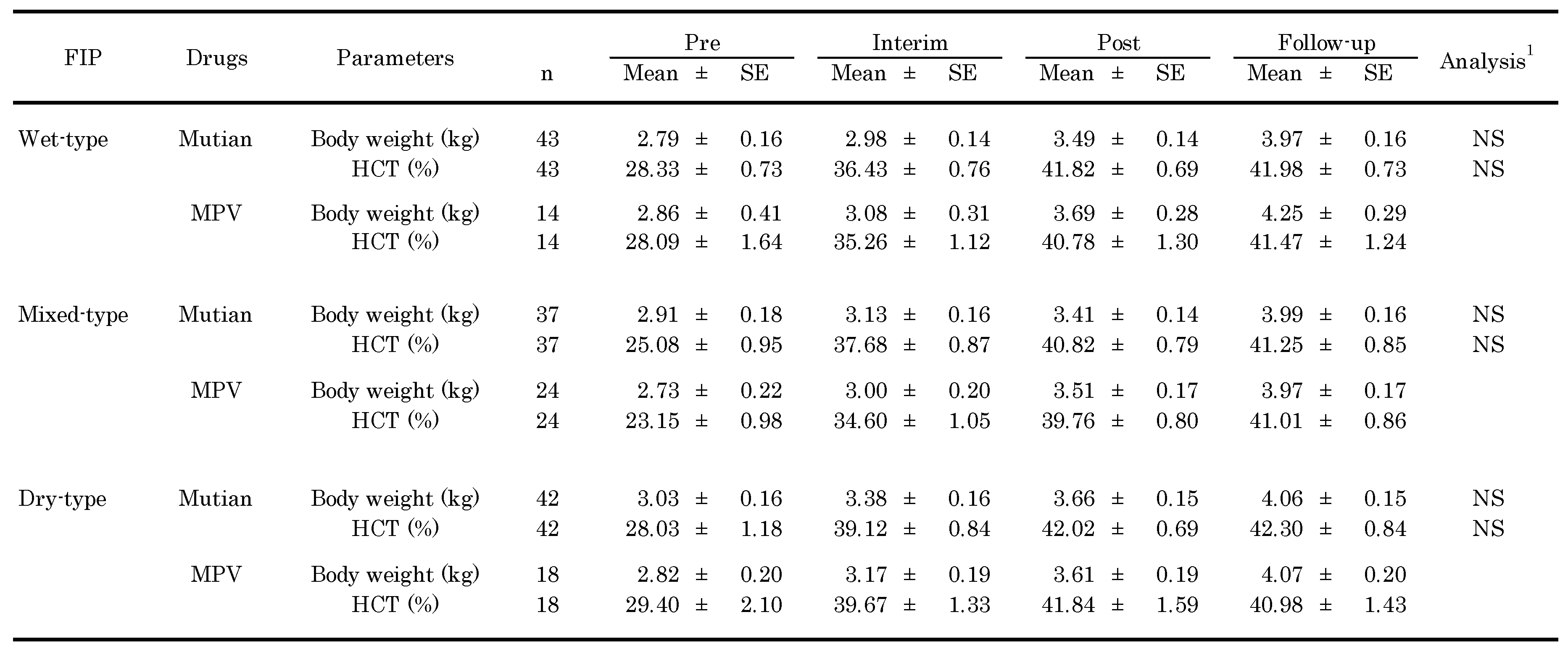
1 Statistically differences between Mutian and MPV for effects on each parameter were determined to by the repeated measures ANOVA. Abbreviations: MPV: molnupiravir; FIP: feline infectious peritonitis; NS: not significant; SE: standard error of the mean.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



