
Submitted:
13 March 2024
Posted:
13 March 2024
You are already at the latest version
Abstract
(1) Background: The aim of this study was to compare the survival benefit of radical ante-grade-modular pancreato-splenectomy (RAMPS) with conventional distal pancreato-splenectomy (cDPS) in left-sided pancreatic cancer. (2) Methods: A retrospective propensity score matching (PSM) analysis was conducted on 333 patients who underwent RAMPS or cDPS for left-sided pancreatic cancer at four tertiary cancer centers. The study assessed prognostic factors and com-pared survival and operative outcomes. (3) Results: After PSM, 99 patients were matched in each group. RAMPS resulted in a higher retrieved lymph node count than cDPS (15.0 vs. 10.0, p < 0.001). No significant differences were observed between the two groups in terms of R0 resection rate, blood loss, hospital stay, or morbidity. The 5-year overall survival rate was similar in both groups (cDPS vs. RAMPS, 44.4% vs. 45.2%, p = 0.853), and disease-free survival was also comparable. Multivariate analysis revealed that ASA score, preoperative CA19-9, histologic differentiation, R1 resection, adjuvant treatment, and lymphovascular invasion were significant prognostic factors for overall survival. Preoperative CA19-9, histologic differentiation, T-stage, adjuvant treatment, and lymphovascular invasion were independent significant prognostic factors for disease-free survival. (4) Conclusions: Although RAMPS resulted in a higher retrieved lymph node count, survival outcomes were not different between two groups. RAMPS was a surgical option to achieve R0 resection rather than a standard procedure. Adjuvant treatment was an independent prognostic factor for both overall and disease-free survival.
Keywords:
pancreatic neoplasm
; pancreatectomy
; survival
; prognosis
1. Introduction
Pancreatic ductal adenocarcinoma (PDAC) has a poor prognosis, with margin status and lymph node metastasis being recognized as unfavorable prognostic factors [1,2,3,4,5,6]. To address this issue, Strasberg et al. developed the concept of radical antegrade modular pancreatosplenectomy (RAMPS) [7]. RAMPS is a modified type of distal pancreatectomy to facilitate complete dissection of the N1 and N2 lymph nodes and obtaining negative posterior margins. RAMPS has been shown to be effective in achieving a higher lymph node yield and a negative posterior tangential margin in advanced left-sided PDAC when the tumor involves the peripancreatic soft tissue or peripancreatic lymph node metastases are suspected. However, it remains unclear whether RAMPS should be considered a standard operation for all left-sided PDACs, including non-advanced cases, or if it should be reserved as one of the surgical options only for advanced PDACs. Reports have shown that RAMPS has a 91% success rate in achieving negative tangential margins in patients [8]. However, the benefits of RAMPS over conventional distal pancreatosplenectomy (cDPS) in terms of survival outcomes have not been clearly established in previous studies [3,9,10,11]. This study aims to compare the operative and survival outcomes of RAMPS and cDPS to evaluate the value of RAMPS as a standard procedure in let-sided PDACs, as well as identify prognostic factors for left-sided pancreatic cancer.
2. Materials and Methods
2.1. Data Collection
We conducted a retrospective study of patients with PDAC who RAMPS or cDPS at four tertiary hospitals between January 2010 and December 2020. RAMPS was defined according to the method described by Strasberg et al. The resection level at pancreatic neck was reviewed from a postoperative CT scan and the extent of retropancreatic dissection and lymph node dissection was confirmed from the operation record. cDPS was defined as a distal pancreatectomy that does not fulfil the criteria of RAMPS (neck level transection, N1 and N2 lymph node dissection, and posterior dissection plane including the Gerota’s fascia). Cases which the pancreatic resection was performed lateral to the pancreatic neck depending on location of the tumor or a reduced lymph node dissection was performed according to surgeon’s decision, or the posterior dissection plane did not follow the RAMPS plane were classified as cDPS. Patients with metastatic lesions, non-curative resection were excluded. Patients who underwent extended surgery such as combined organ resection or celiac axis resection which cannot be classified in routne RAMPS nor cDPS were also excluded. We collected demographic and operative data, including age, sex, American Society of Anesthesiologist (ASA) score, body mass index (BMI), preoperative carcinoembryonic antigen (CEA), preoperative carbohydrate antigen 19-9 (CA19-9), neoadjuvant treatment, adjuvant treatment, operation type (RAMPS vs. cDPS), operation time, estimated blood loss, and hospital stay. Pathological data included tumor size, histologic differentiation, retrieved lymph node count, metastatic lymph node count, perineural invasion (PNI), lymphovascular invasion (LVI), and margin status. R1 resection was defined as the safety margin from the tumor to the resection margin was less than 1mm. All postoperative morbidities were recorded and graded according to the Clavien–Dindo classification, and postoperative pancreatic fistula (POPF), post-pancreatectomy hemorrhage (PPH), and delayed gastric emptying (DGE) were graded according to the International Study Group of Pancreatic Surgery.
2.2. Statistical Analysis
A retrospective 1:1 propensity score matching analysis was conducted to compare the clinical and pathological outcomes of patients who underwent RAMPS or cDPS for PDAC. Six preoperative covariates, including age, sex, ASA score, tumor location, tumor size, and preoperative serum CA19-9 level, were used for propensity score matching. Because the tumor location influenced the decision regarding the pancreatic resection level and extent of lymph node dissection, tumor location was included in the propensity score matching. The matching was performed using a nearest neighborhood method with 0.01 of caliper. Continuous variables were compared using either the independent samples t-test or Mann-Whitney U test based on the normality test results, and categorical variables were compared using the chi-square test or Fisher's exact test. The Kaplan-Meier method was used to estimate overall survival (OS) and disease-free survival (DFS), and the log-rank test was used to identify risk factors. Multivariate analysis was conducted using a Cox regression hazard model. Statistical significance was set at P < 0.05, and all statistical analyses were performed using SPSS version 26.0 (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY).
3. Results
3.1. Baseline Characteristics before and after Propensity Score Matching
In this study, 333 patients with pancreatic ductal adenocarcinoma were initially enrolled. To balance the baseline characteristics between the two groups, 1:1 propensity score matching was performed, resulting in 99 patients included in both the RAMPS and cDPS groups. Table 1 demonstrates the baseline characteristics of the patients before and after PSM. After matching, both groups were found to be well-balanced in terms of their preoperative characteristics.
3.2. Operative Outcomes
The results revealed a significantly higher retrieved lymph node count in the RAMPS group than in the cDPS group. However, the R0 resection rate was comparable between the two groups. Moreover, no significant differences were observed in the length of hospital stay, operation time, estimated blood loss, transfusion rate, and morbidity between the two groups. There was no mortality within 30 and 90 days. The recurrence rate and recurrence pattern were also found to be comparable between both groups. The detailed operative outcomes are presented in Table 2.
3.2. Comparison of Pathologic Results
No significant differences were found in terms of histologic differentiation, T-stage, perineural invasion, and lymphovascular invasion between the two groups. However, there was a significant difference in the number of positive lymph nodes and N-stage, with higher counts observed in the RAMPS group compared to the cDPS group. This observation raises the possibility of under-staging in the cDPS group. The detailed pathologic results can be found in Table 3.
3.3. Comparison of Survival Outcomes
The study included a mean and median follow-up time of 30.84 and 22.5 months (range, 3-133 months) for all matched patients, with no significant differences in the mean and median follow-up times between the cDPS and RAMPS groups (32.81 vs. 28.88 months, P = 0.281, 26.0 vs. 20.0 months, P = 0.576, respectively). The 2-year and 5-year overall survival rates for all matched cohorts were 68.5% and 44.8%, respectively, with a median survival time of 48.0 months. Although the median survival time was slightly longer in the cDPS group than in the RAMPS group, the difference was not significant (50.0 vs. 41.0 months, P = 0.853). The 2-year and 5-year overall survival rates were comparable between the cDPS and RAMPS groups (71.9% and 44.4% vs. 64.5% and 45.2%, respectively) (Figure 1a). The overall recurrence rate was 73.2%, with no significant difference between both groups (cDPS vs. RAMPS, 75.8% vs. 70.7%, P = 0.422). The 2-year and 5-year disease-free survival rates for all matched cohorts were 35.1% and 21.9%, respectively, with no significant difference between the cDPS and RAMPS groups (34.5% and 21.2% vs. 35.4% and 22.3%, respectively). The median DFS time was also similar between the groups (RAMPS: 14.0 months; cDPS: 10.0 months, P = 0.929) (Figure 1b).
3.4. Prognostic Factor Analysis
In the univariate analysis, several prognostic factors for overall survival (OS) were found significant, including age, ASA score, preoperative serum CA19-9, histologic differentiation, lymph node ratio, margin status, adjuvant treatment, PNI, and LVI. However, in the multivariate analysis, only ASA score, preoperative CA19-9, histologic differentiation, margin status, adjuvant treatment, and lymphovascular invasion were identified as independent significant prognostic factors for OS, as shown in Table 4.
Regarding disease-free survival (DFS), in the univariate analysis, preoperative CA19-9, histologic differentiation, T-stage, N-stage, lymph node ratio, adjuvant treatment, PNI, and LVI were identified as significant prognostic factors. However, in the multivariate analysis, only preoperative CA19-9, histologic differentiation, T-stage, adjuvant treatment, and LVI were found to be independent significant prognostic factors for DFS (Table 5).
4. Discussion
The RAMPS involves resection of the pancreatic body and tail, as well as an extensive lymph node dissection. Several studies have reported that RAMPS does not increase morbidity and mortality rates [2,9,10,11,12,13]. In our study, the operative outcomes in terms of EBL, transfusion, hospital stay, and the incidence of morbidity, including POPF, PPH, and DGE, were comparable between the groups. In our study, we found that the short-term operative outcomes, including estimated blood loss, transfusion requirements, hospital stay, and the incidence of complications such as postoperative pancreatic fistula, post-pancreatectomy hemorrhage, and delayed gastric emptying, were similar between the RAMPS and cDPS groups. However, the removal of a significant portion of the pancreas during RAMPS can increase the risk of developing diabetes or pancreatic exocrine insufficiency, which may require lifelong enzyme replacement therapy [14,15,16]. The operative time was not significantly different after PSM. (Table 2)
Previous studies have demonstrated that RAMPS is associated with a higher number of retrieved lymph nodes and R0 resection rate compared to cDPS [2,3,4,9,11,12,13,17,18]. In contrast, Sham et al. reported lower rates for these parameters in the RAMPS group compared to the cDPS group [10]. In our study, we also observed a significantly higher median number of retrieved lymph nodes in the RAMPS group compared to the cDPS group (15.0 vs. 10.0, P = 0.001), but no significant difference in R0 resection rates between the two groups (94.9% in RAMPS vs. 93.9% in cDPS, P = 0.756). Although the retrieved LN count was significantly higher in the RAMPS group, there was no evidence that extensive LN dissection can improve survival in patients with pancreatic ductal adenocarcinoma [19]. Several researchers suggested a tailored lymph node dissection extent according to the location of the tumor, based on the results of their research about lymph node metastasis pattern according to the tumor location [20,21].
Although RAMPS has been shown to improve retrieved lymph node counts and R0 resection rates, the evidence for its survival benefit remains unclear. Dai et al. reported that the RAMPS group had a higher number of retrieved lymph nodes, longer OS time, and longer DFS time compared to cDPS [3]. However, other studies, including Kim et al., Park et al., and Sham et al., found no significant differences in OS and DFS rates between the RAMPS and cDPS groups [4,10,11]. The meta-analysis also showed mixed results, with some authors reporting no significant survival benefit [12,17,18,22], while others reported higher 1-year survival rates in the RAMPS group. In our study, we found no significant difference in OS and DFS between the two groups. By contrast, Dragomir et al. and Zhou et al. reported that the 1-yr survival rate was significantly higher in the RAMPS group than in the cDPS group [9,13]. In our study, There was also no significant difference in OS and DFS between the two groups.
Previous studies have demonstrated that margin status, histological grade, lymph node involvement, tumor size, LNR, and CEA were independent prognostic factors in pancreatic ductal adenocarcinoma [1,2,6,23,24,25,26,27]. In the present study, higher ASA score, preoperative CA19-9 > 37 U/ml, poorly/undifferentiated carcinoma, R1 resection, no adjuvant treatment, and lymphovascular invasion were independent poor prognostic factors for OS, and preoperative serum CA19-9 > 37 U/ml, poorly/undifferentiated carcinoma, T3 stage, no adjuvant treatment, and lymphovascular invasion were independent poor prognostic factors for DFS. OS and DFS were not affected by the operation type. Old age and higher ASA scores did not affect DFS. However, they were significant prognostic factors in univariate analysis for OS, because the patients with old age or poor physical status often could not receive adjuvant chemotherapy.
Our study has limitations, including potential selection bias in this retrospective analysis. To evaluate the value of RAMPS as a standard procedure, the tumor size was included in the covariates for PSM. Therefore large, advanced cases requiring RAMPS to achieve R0 resection could be excluded. R0 resection rate was not significantly different between both groups. A larger prospective study with longer follow-up is necessary to accurately assess the survival benefit of RAMPS.
5. Conclusions
In conclusion, our study demonstrates that RAMPS is a safe and feasible procedure that increases the number of retrieved lymph nodes however a significant survival benefit was not observed. Margin status was a significant prognostic factor. Therefore, RAMPS is a treatment option for advanced cases to achieve negative tangential margin rather than a standard procedure for all left-sided pancreatic cancer. Adjuvant treatment remains a significant independent prognostic factor for OS and DFS.
Author Contributions
Conceptualization, H.J.K and S.H.S; methodology, J.K. and H.L.; validation, H.K. and S.H.K.; formal analysis, J.D.Y. and W.H.L.; investigation, J.S.L.; data curation, H.J.K., S.H.S., J.K., and H.L.; writing—original draft preparation, J.K. and H.L.; writing—review and editing, H.J.K. and S.H.H.; visualization, J.D.Y.; supervision, H.J.K.; project administration, H.J.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Chonnam National University Hospital (Gwangju, Republic of Korea, IRB No. CNUH-2022-298, date of approval: 16th August 2022).
Informed Consent Statement
Our Institutional Review Board of Chonnam National University Hospital waived the need for written informed consent from the participants since the research involved no more than minimal risk to subjects, and there was no reason to assume rejection of agreement.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to individual privacy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fujita, T.; Nakagohri, T.; Gotohda, N.; Takahashi, S.; Konishi, M.; Kojima, M.; Kinoshita, T. Evaluation of the prognostic factors and significance of lymph node status in invasive ductal carcinoma of the body or tail of the pancreas. Pancreas 2010, 39, e48–e54. [Google Scholar] [CrossRef]
- Abe, T.; Ohuchida, K.; Miyasaka, Y.; Ohtsuka, T.; Oda, Y.; Nakamura, M. Comparison of Surgical Outcomes Between Radical Antegrade Modular Pancreatosplenectomy (RAMPS) and Standard Retrograde Pancreatosplenectomy (SPRS) for Left-Sided Pancreatic Cancer. World J Surg 2016, 40, 2267–2275. [Google Scholar] [CrossRef]
- Dai, M.; Zhang, H.; Li, Y.; Xing, C.; Ding, C.; Liao, Q.; Zhang, T.; Guo, J.; Xu, Q.; Han, X.; et al. Radical antegrade modular pancreatosplenectomy (RAMPS) versus conventional distal pancreatosplenectomy (CDPS) for left-sided pancreatic ductal adenocarcinoma. Surgery today 2021. [Google Scholar] [CrossRef]
- Park, H.J.; You, D.D.; Choi, D.W.; Heo, J.S.; Choi, S.H. Role of radical antegrade modular pancreatosplenectomy for adenocarcinoma of the body and tail of the pancreas. World J Surg 2014, 38, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, J.; Saiura, A.; Koga, R.; Seki, M.; Katori, M.; Kato, Y.; Sakamoto, Y.; Kokudo, N.; Yamaguchi, T. Improved Survival of Left-sided Pancreas Cancer after Surgery. Japanese Journal of Clinical Oncology 2010, 40, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Sakamoto, Y.; Sano, T.; Kosuge, T. Prognostic factors after distal pancreatectomy with extended lymphadenectomy for invasive pancreatic adenocarcinoma of the body and tail. Surgery 2006, 139, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Strasberg, S.M.; Drebin, J.A.; Linehan, D. Radical antegrade modular pancreatosplenectomy. Surgery 2003, 133, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Strasberg, S.M.; Linehan, D.C.; Hawkins, W.G. Radical antegrade modular pancreatosplenectomy procedure for adenocarcinoma of the body and tail of the pancreas: ability to obtain negative tangential margins. J Am Coll Surg 2007, 204, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Fengwei, G.; Gong, J.; Xie, Q.; Liu, Y.; Wang, Q.; Lei, Z. Assessement of postoperative long-term survival quality and complications associated with radical antegrade modular pancreatosplenectomy and distal pancreatectomy: a meta-analysis and systematic review. BMC Surg 2019, 19. [Google Scholar] [CrossRef]
- Sham, J.G.; Guo, S.; Ding, D.; Shao, Z.; Wright, M.; Jing, W.; Yin, L.D.; Zhang, Y.; Gage, M.M.; Zhou, Y.; et al. Radical antegrade modular pancreatosplenectomy versus standard distal pancreatosplenectomy for pancreatic cancer, a dual-institutional analysis. Chin Clin Oncol 2020, 9. [Google Scholar] [CrossRef]
- Kim, E.Y.; You, Y.K.; Kim, D.G.; Hong, T.H. Initial experience with radical antegrade modular pancreatosplenectomy in a single institution. Ann Surg Treat Res 2016, 91, 29–36. [Google Scholar] [CrossRef]
- Zhou, Y.; Shi, B.; Wu, L.; Si, X. A systematic review of radical antegrade modular pancreatosplenectomy for adenocarcinoma of the body and tail of the pancreas. HPB : the official journal of the International Hepato Pancreato Biliary Association 2017, 19, 10–15. [Google Scholar] [CrossRef]
- Dragomir, M.; Eftimie, M.A. Is Radical Antegrade Modular Pancreatosplenectomy the Solution? A Systematic Literature Review and Meta-Analysis. Chirurgia (Bucur) 2017, 112, 653–663. [Google Scholar] [CrossRef]
- Shirakawa, S.; Matsumoto, I.; Toyama, H.; Shinzeki, M.; Ajiki, T.; Fukumoto, T.; Ku, Y. Pancreatic Volumetric Assessment as a Predictor of New-Onset Diabetes Following Distal Pancreatectomy. Journal of Gastrointestinal Surgery 2012, 16, 2212–2219. [Google Scholar] [CrossRef]
- Thomas, A.S.; Huang, Y.; Kwon, W.; Schrope, B.A.; Sugahara, K.; Chabot, J.A.; Wright, J.D.; Kluger, M.D. Prevalence and Risk Factors for Pancreatic Insufficiency After Partial Pancreatectomy. Journal of Gastrointestinal Surgery 2022. [Google Scholar] [CrossRef]
- Kwon, J.H.; Kim, S.C.; Shim, I.K.; Song, K.B.; Lee, J.H.; Hwang, D.W.; Park, K.M.; Lee, Y.J. Factors Affecting the Development of Diabetes Mellitus After Pancreatic Resection. Pancreas 2015, 44, 1296–1303. [Google Scholar] [CrossRef] [PubMed]
- Chun, Y.S. Role of Radical Antegrade Modular Pancreatosplenectomy (RAMPS) and Pancreatic Cancer. Ann Surg Oncol 2018, 25, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Cao, F.; Li, J.; Li, A.; Li, F. Radical antegrade modular pancreatosplenectomy versus standard procedure in the treatment of left-sided pancreatic cancer: A systemic review and meta-analysis. BMC Surg 2017, 17. [Google Scholar] [CrossRef]
- Jang, J.Y.; Kang, M.J.; Heo, J.S.; Choi, S.H.; Choi, D.W.; Park, S.J.; Han, S.S.; Yoon, D.S.; Yu, H.C.; Kang, K.J.; et al. A prospective randomized controlled study comparing outcomes of standard resection and extended resection, including dissection of the nerve plexus and various lymph nodes, in patients with pancreatic head cancer. Ann Surg 2014, 259, 656–664. [Google Scholar] [CrossRef]
- Imamura, T.; Yamamoto, Y.; Sugiura, T.; Okamura, Y.; Ito, T.; Ashida, R.; Ohgi, K.; Uesaka, K. Reconsidering the Optimal Regional Lymph Node Station According to Tumor Location for Pancreatic Cancer. Annals of Surgical Oncology 2021, 28, 1602–1611. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Nakamura, T.; Asano, T.; Nakanishi, Y.; Noji, T.; Tsuchikawa, T.; Okamura, K.; Shichinohe, T.; Hirano, S. Pancreatic body and tail cancer and favorable metastatic lymph node behavior on the left edge of the aorta. Pancreatology 2020, 20, 1451–1457. [Google Scholar] [CrossRef]
- Huo, Z.; Zhai, S.; Wang, Y.; Qian, H.; Tang, X.; Shi, Y.; Weng, Y.; Zhao, S.; Deng, X.; Shen, B. Comparison of Radical Antegrade Modular Pancreatosplenectomy with Standard Retrograde Pancreatosplenectomy for Left-Sided Pancreatic Cancer: A Meta-Analysis and Experience of a Single Center. Med Sci Monit 2019, 25, 4590–4601. [Google Scholar] [CrossRef]
- Korrel, M.; Lof, S.; Van Hilst, J.; Alseidi, A.; Boggi, U.; Busch, O.R.; Van Dieren, S.; Edwin, B.; Fuks, D.; Hackert, T.; et al. Predictors for Survival in an International Cohort of Patients Undergoing Distal Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Annals of Surgical Oncology 2021, 28, 1079–1087. [Google Scholar] [CrossRef]
- Latorre, M.; Ziparo, V.; Nigri, G.; Balducci, G.; Cavallini, M.; Ramacciato, G. Standard retrograde pancreatosplenectomy versus radical antegrade modular pancreatosplenectomy for body and tail pancreatic adenocarcinoma. Am Surg 2013, 79, 1154–1158. [Google Scholar] [CrossRef]
- Li, H.J.; Chen, Y.T.; Yuan, S.Q. Proposal of a modified American Joint Committee on Cancer staging scheme for resectable pancreatic ductal adenocarcinoma with a lymph node ratio-based N classification: A retrospective cohort study. Medicine (Baltimore) 2018, 97. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.M.; Rahman, A.; Haugk, B.; French, J.J.; Manas, D.M.; Jaques, B.C.; Charnley, R.M.; White, S.A. Metastatic lymph node ratio as an important prognostic factor in pancreatic ductal adenocarcinoma. European Journal of Surgical Oncology (EJSO) 2012, 38, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Sivasanker, M.; Desouza, A.; Bhandare, M.; Chaudhari, V.; Goel, M.; Shrikhande, S.V. Radical antegrade modular pancreatosplenectomy for all pancreatic body and tail tumors: rationale and results. Langenbecks Arch Surg 2019, 404, 183–190. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A. Overall survival curve according to the operation type. B. Disease-free survival curve according to the operation type. There were no differences in overall survival or disease-free survival between the conventional DPS and the RAMPS groups..
Figure 1.
A. Overall survival curve according to the operation type. B. Disease-free survival curve according to the operation type. There were no differences in overall survival or disease-free survival between the conventional DPS and the RAMPS groups..
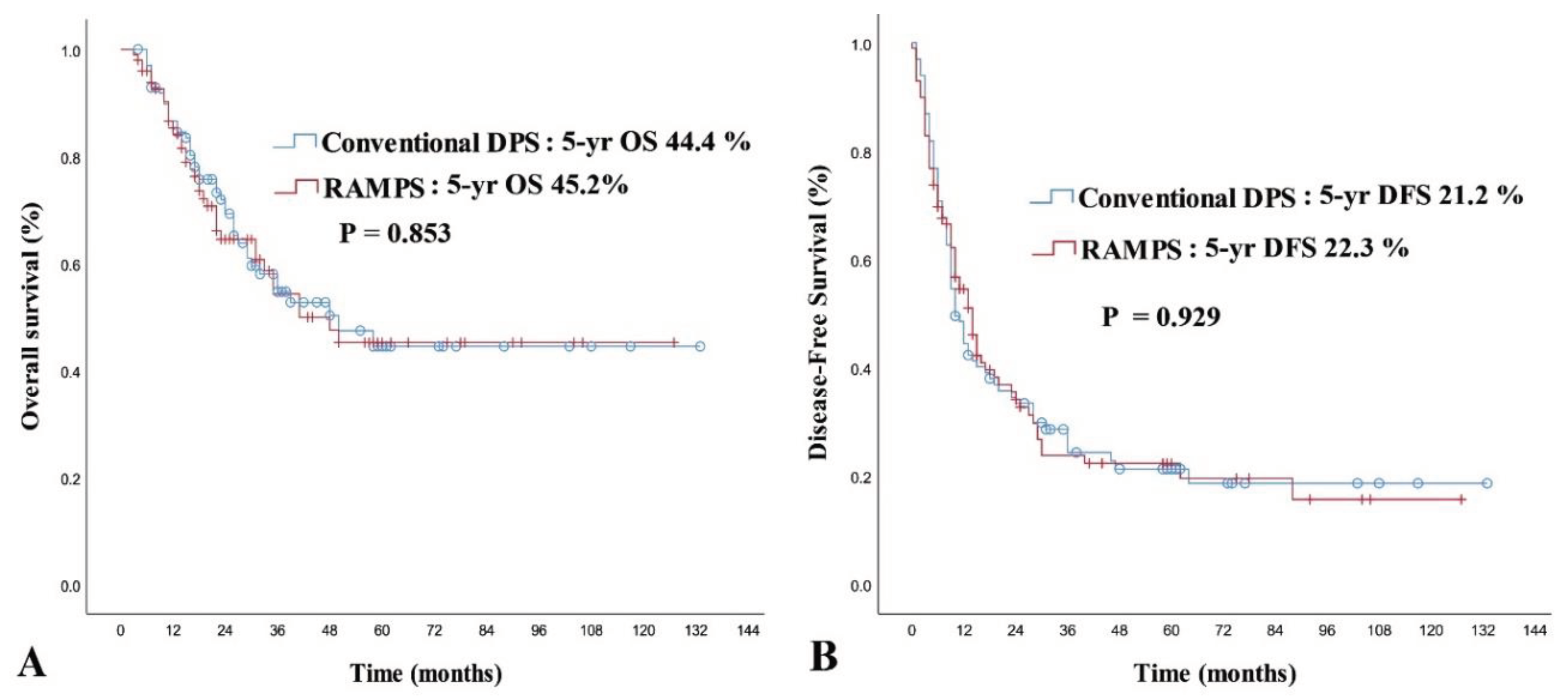

Table 1.
Basal characteristics of total and matched cohort.
| Pre-PSM | Post-PSM | |||||
| cDPS (n = 130) |
RAMPS (n = 203) |
p-value | cDPS (n = 99) |
RAMPS (n = 99) |
p-value | |
| Age [median (range)] (y) | 66.0 (39-86) | 64.0 (41-84) | 0.503* | 65.0 (39-80) | 66.0 (43-81) | 0.301* |
| Sex [n (%)] | 0.262 | 1.000 | ||||
| Male | 72 (55.4 ) | 125 (61.6) | 53 (53.5) | 53 (53.5) | ||
| Female | 58 (44.6) | 78 (38.4) | 46 (46.5) | 46 (46.5) | ||
| Approach [n (%)] | 0.031† | 0.747† | ||||
| Open | 120 (92.3) | 198 (97.5) | 93 (93.9) | 95 (96.0) | ||
| Lap | 10 (7.7) | 5 (2.5) | 6 (6.1) | 4 (4.0) | ||
| Tumor location [n (%)] | <0.001 | 1.000 | ||||
| confined to neck/body | 58 (44.6) | 159 (78.3) | 56 (56.6) | 56 (56.6) | ||
| body to tail | 19 (14.6) | 11 (5.4) | 10 (10.1) | 10 (10.1) | ||
| confined to tail | 53 (40.8) | 33 (16.3) | 33 (33.3) | 33 (33.3) | ||
| BMI (mean ± SD) | 23.70 ± 3.288 | 23.29 ± 2.937 | 0.234 | 23.71 ± 3.459 | 23.41 ± 2.781 | 0.513 |
| ASA score [n (%)] | 0.503 | 0.571 | ||||
| I | 14 (10.8) | 31 (15.3) | 12 (12.1) | 14 (14.1) | ||
| II | 102 (78.5) | 151 (74.4) | 78 (78.8) | 72 (72.7) | ||
| III | 14 (10.8) | 21 (10.3) | 9 (9.1) | 13 (13.1) | ||
| CEA, ng/ml [median (range)] | 2.52 (0.20-165.10) | 2.20 (0.44-56.92) | 0.126* | 2.49 (0.20-165.10) | 2.51 (0.44-56.92) | 0.734* |
| CA 19-9, U/ml [median (range)] | 59.93 (1.00-11387.00) |
75.01 (1.20-10028.49) |
0.436* | 168.13 (1.80-11387.00) |
244.32 (2.00-6808.37) |
0.101* |
| Tumor size, cm [median (range)] |
3.0 (0.5-9.5) |
2.5 (0.3-10.0) |
0.282* | 3.0 (1.0-8.0) |
3.2 (1.2-8.5) |
0.132* |
| Neoadjuvant treatment [n (%)] | 0.606† | 0.246† | ||||
| No | 125 (96.2) | 192 (94.6) | 96 (97.0) | 99 (100) | ||
| Yes | 5 (3.8) | 11 (5.4) | 3 (3.0) | 0 (0.0) | ||
| Adjuvant treatment [n (%)] | 0.164 | 0.66 | ||||
| No | 54 (41.5) | 69 (34.0) | 36 (36.4) | 39 (39.4) | ||
| Yes | 76 (58.5) | 134 (66.0) | 63 (63.6) | 60 (60.6) | ||
PSM, propensity score matching; DPS, distal pancreato-splenectomy; RAMPS, radical antegrade-modular pancreato-spelenctomy; BMI, body mass index; SD, standard deviation; ASA, American Society of Anesthesiologists; CEA, carcinoembryonic antigen; CA, carbohydrate antigen; * Mann-Whitney U test. † Fisher’s exact test.
Table 2.
Comparison of operative outcomes.
| Pre-PSM | Post-PSM | |||||
| cDPS (n = 130) |
RAMPS (n = 203) |
p-value | cDPS (n = 99) |
RAMPS (n = 99) |
p-value | |
| LOS [median (range)](days) | 10.0 (5–52) | 9.0 (6–152) | 0.065* | 10.0 (5–52) | 10.0 (7–35) | 0.806* |
| Approach [n (%)] | 0.031 | 0.747 | ||||
| Open | 120 (92.3) | 198 (97.5) | 93 (93.9) | 95 (96.0) | ||
| Laparoscopic | 10 (7.7) | 5 (2.5) | 6 (6.1) | 4 (4.0) | ||
| Op. time [median (range)] (minutes) | 195 (93–420) | 204 (117–494) | 0.045* | 195 (98–420) | 210 (118–458) | 0.305* |
| EBL [median (range)] (ml) | 250 (30–1600) | 300 (50–3000) | 0.488* | 250 (50–1600) | 250 (50–3000) | 0.934* |
| Retrieved LN count [median (range)] | 10 (0–39) | 15 (4–51) | <0.001* | 10.0 (0–36) | 15.0 (5–51) | 0.001* |
| R0 resection [n (%)] | 120/130 (92.3) | 198/203 (97.5) | 0.031 | 93/99 (93.9) | 94/99 (94.9) | 0.756 |
| Transfusion [n (%)] | 0.692 | >0.99 | ||||
| No | 123 (94.6) | 194 (95.6) | 94 (94.9) | 94 (94.9) | ||
| YES | 7 (5.4) | 9 (4.4) | 5 (5.1) | 5 (5.1) | ||
| POPF [n (%)] | 0.045† | 0.165† | ||||
| No or BCL | 110 (84.6) | 187 (92.1) | 85 (85.9) | 92 (92.9) | ||
| CR-POPF | 20 (15.4) | 16 (7.9) | 14 (14.1) | 7 (7.1) | ||
| DGE [n (%)] | 0.262 | 0.261 | ||||
| No | 127 (97.7) | 199 (98.0) | 96 (97.0) | 96 (97.0) | ||
| Grade A | 0 (0.0) | 3 (1.5) | 0 (0.0) | 2 (2.0) | ||
| Grade B | 1 (0.8) | 1 (0.5) | 1 (1.0) | 1 (1.0) | ||
| Grade C | 2 (1.5) | 0 (0.0) | 2 (2.0) | 0 (0.0) | ||
| PPH [n (%)] | 0.22 | 0.384 | ||||
| No | 125 (96.2) | 201 (99.0) | 95 (96.0) | 98 (99.0) | ||
| Grade A | 1 (0.8) | 0 (0.0) | 1 (1.0) | 0 (0.0) | ||
| Grade B | 3 (2.3) | 0 (0.0) | 2 (2.0) | 0 (0.0) | ||
| Grade C | 1 (0.8) | 2 (1.0) | 1 (1.0) | 1 (1.05) | ||
| Chyle leak [n (%)] | 0.300 | 0.251 | ||||
| No | 126 (96.9) | 191 (94.1) | 95 (96.0) | 90 (90.9) | ||
| Yes | 4 (3.1) | 12 (5.9) | 4 (4.0) | 9 (9.1) | ||
| SSI [n (%)] | 0.966 | 0.884 | ||||
| No | 128 (98.5) | 199 (98.0) | 97 (98.0) | 96 (97.0) | ||
| Superficial | 1 (0.8) | 3 (1.5) | 1 (1.0) | 2 (2.0) | ||
| Organ/space | 1 (0.8) | 1 (0.5) | 1 (1.0) | 1 (1.0) | ||
| Severe complication [n (%)] | 0.998 | 0.663 | ||||
| No | 114 (87.7) | 178 (87.7) | 86 (86.9) | 88 (88.9) | ||
| Yes | 16 (12.3) | 25 (12.3) | 13 (13.1) | 11 (11.1) | ||
| Recurrence [n (%)] | 0.251 | >0.99 | ||||
| No | 37 (28.5) | 70 (34.5) | 24 (24.2) | 24 (24.2) | ||
| Yes | 93 (71.5) | 133 (65.5) | 75 (75.8) | 75 (75.8) | ||
| Recurrence pattern [n (%)] | 0.177 | 0.507 | ||||
| No | 37 (28.5) | 70 (34.5) | 24 (24.2) | 24 (24.2) | ||
| Locoregional | 20 (15.4) | 17 (8.4) | 16 (16.2) | 11 (11.1) | ||
| Systemic | 61 (46.9) | 92 (45.3) | 49 (49.5) | 51 (51.5) | ||
| Both | 12 (9.2) | 24 (11.8) | 10 (10.1) | 13 (13.1) | ||
PSM, propensity score match; DPS, distal pancreatosplenectomy; RAMPS, radical antegrade modular pancreatosplenectomy; LOS, length of stay; Op, operation; EBL, estimated blood loss; LN, lymph node; POPF, postoperative pancreatic fistula; BCL, biochemical leak; CR-POPF, clinically relevant POPF; DGE, delayed gastric emptying; PPH, post-pancreatectomy hemorrhage; SSI, surgical site infection. * Mann-Whitney U test. † Fisher’s exact test.
Table 3.
Histopathologic results before and after propensity score matching.
| Pre-PSM | Post-PSM | |||||
| cDPS (n = 130) |
RAMPS (n = 203) |
p-value | cDPS (n = 99) |
RAMPS (n = 99) |
p-value | |
| Differentiation [n (%)] | 0.472 | 0.677 | ||||
| Well | 18 (13.8) | 20 (9.9) | 13 (13.4) | 12 (12.1) | ||
| Moderate | 82 (63.1) | 129 (63.5) | 61 (62.9) | 68 (68.7) | ||
| Poorly/undifferentiated | 30 (23.1) | 54 (26.6) | 23 (23.7) | 19 (19.2) | ||
| T-stage [n (%)] | 0.208 | 0.216 | ||||
| T1 | 30 (23.1) | 65 (32.0) | 23 (23.2) | 19 (45.2) | ||
| T2 | 72 (55.4) | 98 (48.3) | 54 (54.5) | 47 (47.5) | ||
| T3 | 28 (21.5) | 40 (19.7) | 22 (22.2) | 33 (33.3) | ||
| Involved LN count [median (range)] | 0.0 (0-15) | 1.0 (0–22) | 0.028 | 1.0 (0–15) | 1.0 (0–17) | 0.006 |
| LNR [median (range)] | 0.048 (0.0-1.00) | 0.057 (0–0.71) | 0.383 | 0.042(0–1.0) | 0.090 (0–0.71) | 0.059 |
| N-stage [n (%)] | 0.083* | 0.024 | ||||
| N0 | 62 (47.7) | 83 (40.9) | 44 (44.4) | 31 (41.3) | ||
| N1 | 48 (36.9) | 84 (41.4) | 38 (38.4) | 42 (42.4) | ||
| N2 | 12 (9.2) | 36 (17.7) | 12 (12.1) | 26 (26.3) | ||
| Nx | 8 (6.2) | 0 (0.0) | 5 (5.1) | 0 (0.0) | ||
| Perineural invasion [n (%)] | 0.360 | 0.290 | ||||
| PNI- | 17 (13.1) | 21 (10.3) | 13 (13.5) | 8 (8.2) | ||
| PNI+ | 106 (81.5) | 180 (88.7) | 83 (86.5) | 90 (91.8) | ||
| Unknown | 7 (5.4) | 2 (1.0) | 3 (3.0) | 1 (1.0) | ||
| Lymphovascular invasion [n (%)] | 0.376 | 0.281 | ||||
| LVI- | 64 (49.2) | 95 (46.8) | 44 (44.4) | 37 (37.4) | ||
| LVI+ | 46 (35.4) | 85 (41.9) | 39 (39.4) | 50 (50.5) | ||
| unknown | 20 (15.4) | 23 (11.3) | 16 (16.2) | 12 (42.9) | ||
PSM, propensity score matching; cDPS, conventional distal pancreatosplenectomy; RAMPS, radical antegrade modular pancreatospelenectomy; LN, lymph node; LNR, lymph node ratio; PNI, perineural invasion; LVI, lymphovascular invasion.
Table 4.
Risk factor analysis for overall survival after propensity score matching.
| Univariate | Multivariate | ||||||
| n | 2YSR (%) | 5YSR (%) | MST(months) | p-value | HR (95% CI) | p-value | |
| Age (years) | 0.008 | ||||||
| <65 | 95 | 75.5 | 56.1 | 85.62 | 1 (Reference) | ||
| 65–75 | 75 | 66.1 | 34.3 | 51.77 | 1.663 (0.899–3.079) | 0.105 | |
| >75 | 28 | 47.5 | 34.6 | 46.71 | 1.328 (0.511–3.453) | 0.561 | |
| Sex | 0.060 | ||||||
| Male | 106 | 64.2 | 33.7 | 61.72 | |||
| Female | 92 | 73.4 | 55.5 | 80.35 | |||
| Operation type | 0.853 | ||||||
| Conventional DPS | 99 | 71.9 | 44.4 | 72.90 | 1 (Reference) | ||
| RAMPS | 99 | 64.5 | 45.2 | 69.82 | 1.014 (0.568–1.811) | 0.962 | |
| ASA physical status | 0.047 | ||||||
| 1 | 26 | 87.6 | 74.9 | 105.04 | 1 (Reference) | ||
| 2 | 150 | 66.0 | 41.9 | 66.87 | 4.553 (1.081–19.172) | 0.039 | |
| 3 | 22 | 63.6 | 31.9 | 51.69 | 5.494 (1.148–26.298) | 0.033 | |
| CEA | 0.079 | ||||||
| ≤6 ng/ml | 147 | 69.0 | 45.9 | 74.40 | |||
| >6 ng/ml | 24 | 65.4 | 29.3 | 36.86 | |||
| CA 19-9 | 0.039 | ||||||
| ≤37 U/ml | 49 | 75.9 | 57.9 | 84.98 | 1 (Reference) | ||
| >37 U/ml | 149 | 65.9 | 39.6 | 66.59 | 2.155 (1.112–4.174) | 0.023 | |
| Differentiation | <0.001 | ||||||
| Well/moderate | 25 | 74.0 | 49.8 | 79.24 | 1 (Reference) | ||
| Poorly/undifferentiated | 42 | 46.8 | 25.3 | 40.58 | 2.299(1.290–4.096) | 0.005 | |
| T-stage | 0.143 | ||||||
| T1 | 42 | 74.4 | 58.8 | 79.15 | |||
| T2 | 101 | 68.0 | 37.0 | 64.39 | |||
| T3 | 55 | 64.7 | 42.9 | 59.61 | |||
| N-stage (Nx exluded) | 0.254 | ||||||
| N0 | 75 | 74.4 | 53.0 | 72.89 | |||
| N1 | 80 | 65.0 | 37.6 | 65.97 | |||
| N2 | 38 | 58.9 | 26.9 | 45.57 | |||
| Nx | 5 | 80.0 | 80.0 | 45.40 | |||
| Lymph node ratio | 0.016 | ||||||
| <0.2 | 143 | 72.1 | 49.6 | 78.24 | 1 (Reference) | ||
| ≥0.2 | 50 | 55.8 | 26.0 | 44.81 | 1.758 (0.718–4.305) | 0.217 | |
| Margin status | <0.001 | ||||||
| R0 | 187 | 70.9 | 47.5 | 75.93 | 1 (Reference) | ||
| R1 | 11 | 31.8 | 0.0 | 21.06 | 4.583 (2.034–10.325) | <0.001 | |
| Adjuvant treatment | 0.005 | ||||||
| Yes | 118 | 74.8 | 50.2 | 79.90 | 1 (Reference) | ||
| No | 80 | 56.6 | 35.3 | 54.20 | 1.915 (1.112–3.298) | 0.019 | |
| Perineural invasion | 0.032 | ||||||
| No | 21 | 80.7 | 74.9 | 99.32 | 1 (Reference) | ||
| Yes | 173 | 65.9 | 39.4 | 67.08 | 3.423 (0.813–14.415) | 0.093 | |
| Lymphovascular invasion | 0.003 | ||||||
| No | 81 | 80.5 | 55.8 | 83.83 | 1 (Reference) | ||
| Yes | 89 | 63.6 | 31.7 | 50.78 | 2.054 (1.196–3.528) | 0.009 | |
YSR, year survival rate; MST, mean survival time; HR, hazard ratio; CI, confidence interval; DPS, distal pancreatosplenectomy; RAMPS, radical antegrade modular pancreatosplenectomy; ASA, American society of anesthesiologists; CEA, carcinoembryonic antigen; CA19-9, cancer antigen 19-9.
Table 5.
Risk factor analysis for disease-free survival after propensity score matching.
| Univariate | Multivariate | ||||||
| n | 2YSR (%) | 5YSR (%) | MST(months) | p-value | HR (95% CI) | p-value | |
| Age (years) | 0.290 | ||||||
| <65 | 95 | 38.5 | 28.1 | 40.71 | |||
| 65–75 | 75 | 32.1 | 14.5 | 26.58 | |||
| >75 | 28 | 29.7 | 14.8 | 25.32 | |||
| Sex | 0.341 | ||||||
| Male | 106 | 32.7 | 17.1 | 33.14 | |||
| Female | 92 | 37.7 | 26.7 | 38.46 | |||
| Operation type | 0.929 | ||||||
| Conventional DPS | 99 | 34.5 | 21.2 | 36.25 | |||
| RAMPS | 99 | 35.4 | 22.3 | 34.19 | |||
| ASA physical status | 0.665 | ||||||
| 1 | 26 | 38.1 | 29.6 | 43.63 | |||
| 2 | 150 | 34.8 | 20.4 | 33.09 | |||
| 3 | 22 | 33.8 | 21.1 | 32.15 | |||
| CEA | 0.580 | ||||||
| ≤6 ng/ml | 147 | 37.0 | 22.3 | 37.56 | |||
| >6 ng/ml | 24 | 32.5 | 17.3 | 23.77 | |||
| CA 19-9 | 0.003 | ||||||
| ≤37 U/ml | 49 | 48.8 | 28.4 | 49.56 | 1 (Reference) | ||
| >37 U/ml | 149 | 30.6 | 20.0 | 30.65 | 1.808 (1.182–2.767) | 0.006 | |
| Differentiation | 0.002 | ||||||
| Well/moderate | 25 | 39.9 | 25.0 | 39.62 | 1 (Reference) | ||
| Poorly/undifferentiated | 42 | 16.0 | 0.0 | 18.48 | 1.729 (1.122–2.664) | 0.013 | |
| T-stage | <0.001 | ||||||
| T1 | 42 | 57.9 | 36.5 | 48.88 | 1 (Reference) | ||
| T2 | 101 | 34.9 | 20.6 | 35.52 | 1.627 (0.975–2.718) | 0.063 | |
| T3 | 55 | 18.0 | 12.8 | 20.52 | 2.611 (1.504–4.532) | 0.001 | |
| N-stage (Nx exluded) | 0.039 | ||||||
| N0 | 75 | 41.8 | 29.2 | 41.74 | 1 (Reference) | ||
| N1 | 80 | 33.1 | 16.6 | 30.07 | 1.030 (0.621–1.630) | 0.899 | |
| N2 | 38 | 21.3 | 15.9 | 21.59 | 1.255 (0.599–2.627) | 0.548 | |
| Nx | 5 | 60.0 | 0.0 | 24.40 | 1.905 (0.565–6.420) | 0.299 | |
| Lymph node ratio | 0.012 | ||||||
| <0.2 | 143 | 38.4 | 23.9 | 40.35 | 1 (Reference) | ||
| ≥0.2 | 50 | 24.9 | 15.6 | 21.18 | 0.963 (0.629–1.474) | 0.864 | |
| Margin status | 0.642 | ||||||
| R0 | 187 | 34.9 | 22.1 | 35.88 | |||
| R1 | 11 | 36.4 | 18.2 | 21.18 | |||
| Adjuvant treatment | 0.018 | ||||||
| Yes | 114 | 36.7 | 23.1 | 37.20 | 1 (Reference) | ||
| No | 75 | 27.9 | 17.6 | 28.40 | 1.848 (1.257–2.717) | 0.002 | |
| Perineural invasion | 0.013 | ||||||
| No | 21 | 52.4 | 46.6 | 58.40 | 1 (Reference) | ||
| Yes | 173 | 31.8 | 17.0 | 30.80 | 1.740 (0.831–3.647) | 0.142 | |
| Lymphovascular invasion | 0.001 | ||||||
| No | 81 | 46.2 | 26.8 | 42.50 | 1(Reference) | ||
| Yes | 89 | 22.6 | 13.4 | 22.20 | 1.846 (1.256–2.714) | 0.002 | |
YSR, year survival rate; MST, mean survival time; HR, hazard ratio; CI, confidence interval; DPS, distal pancreato-splenectomy; RAMPS, radical antegrade modular pancreato-splenectomy; ASA, American society of anesthesiologists; CEA, carcinoembryonic antigen; CA19-9, cancer antigen 19-9.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



