
Submitted:
14 March 2024
Posted:
15 March 2024
You are already at the latest version
Abstract
C. auris is a newly emerging yeast, raising public health concerns due to its outbreak potential, lack of protocols for decontamination and isolation of patients or contacts, increased resistance to common antifungals and associated high mortality.
This research aimed to describe the challenges related to identifying the outbreak, limiting further contamination, and treating affected individuals.
We retrospectively analysed all cases of C. auris detected between October 2022 and August 2023, but our investigation focused on a three-month-long outbreak in the department of cardio-vascular surgery and the related intensive care unit.
Along with isolated cases in different wards, we identified 13 patients who became infected or colonized in the same area and time, even though the epidemiological link could be traced only in 10 patients, according to the epidemiological investigation.
In conclusion, our study emphasizes the substantial challenge encountered in clinical practice when attempting to diagnose and limit the spread of an outbreak. Therefore, it is crucial to promptly apply contact precaution measures and appropriate environmental cleaning, from the first case detected positive.
Keywords:
Candida auris hospital outbreak
; emerging infections
; antimicrobial resistance
; healthcare-associated infections
; post-pandemic era.
1. Introduction
In recent decades, multidrug-resistant fungal infections have attracted the attention of the international medical staff [1]. Of all Candida species, Candida auris, having a similar level of virulence with Candida albicans, but more difficult to treat [2], became a concern for healthcare workers, due to its capacity of causing outbreaks all over the world [3,4,5,6]. C. auris, a yeast difficult to identify, can rapidly develop resistance to current antifungal drugs. [4,6,7]. Its high level of contagion, the persistence in hospital environment and risk of complications in immunocompromised patients make this fungus a public health challenge. In intensive care units it is often associated with mechanical ventilation, invasive procedures, and the presence of invasive medical devices [8].
Since the first identification of C. auris in 2009 [9], along with the development of laboratory identification methods, several countries have started to report infections and colonization [10]. In the last decade, microbiological research, based on genetical and molecular biology, has shown the typical features of C. auris, highlighting its virulence and epidemiological traces [6].
A small number of samples, retrospectively analyzed, showed that the fungal pathogen was detected before 2009, but it was initially misidentified by conventional methods as Candida haemulonii, Candida famata, Rhodotorula glutinis or Saccharomyces cerevisiae [11]. The SENTRY Antifungal Surveillance Program, conducted between 1997 and 2016, found that of 20,788 Candida isolates analyzed retrospectively, consisting of 37 different species, only six were found to be C. auris [12]. Since 2009, hospital outbreaks have been reported in the US, UK, Spain, Italy, Greece, Turkey, Algeria, Kenya, Kuwait, Lebanon, Oman, Pakistan, Venezuela, Colombia, Brazil, Qatar, Saudi Arabia, India, as well as South Africa [13]. There are five genetically distant clades of C. auris identified to date: South Asian clade (I) detected in India and Pakistan, East Asian clade (II) detected in Japan, South African clade (III) identified in South Africa, the South American clade (IV) detected in Venezuela and the Iranian clade (V) recently discovered in Iran, respectively [4]. Except for the new Iranian and East Asian clade, the other C. auris clades have demonstrated the ability to generate outbreaks with invasive infections [14]. However, there is no reported difference in pathogenicity of clades in humans.[15].
Studies have found that underlying respiratory diseases and mechanical ventilation in intensive care units are risk factors for C. auris infections. Therefore, it has been suggested that the COVID-19 pandemic may have contributed to the appearance of the new outbreaks [16,17]. An epidemiological alert was released by the Pan American Health Organization (PAHO) for the outbreaks during the COVID-19 pandemic, including countries where it had not previously been identified [18,19,20]. In Italy, in February 2020, C. auris was identified in a COVID-19 intensive care unit (ICU), with a progressive increase in the number of cases throughout 2020 and 2021. In February 2022, 277 cases were reported in more than 8 hospitals in Liguria, with another 11 cases in the Emilia-Romagna region [15]. In Romania, the first cases of C. auris infections or colonization were reported at the beginning of 2022 and a study conducted on 40 specimens revealed the belonging to the South Asian clade (I) [21].
2. Materials and Methods
We present a retrospective epidemiological analysis on 21 nonduplicate clinical specimens of C. auris isolated from individual patients admitted to different wards of the “Agrippa Ionescu” Clinical Emergency Hospital, Bucharest, Romania, between October 2022 and July 2023. Patients were diagnosed with C. auris bloodstream infections (n=5), respiratory tract infections (n=3) and colonization or asymptomatic infection in different sites such as skin, urine, wounds, catheters (n=13).
All isolates were cultivated using Sabouraud Gentamicin Chloramphenicol 2 Agar and CHROMID® Candida Agar (BioMérieux, Marcy-l’Étoile, France) and grown for 48 h at 30˚C. The species-level identification was carried out using fluorescent-based technology (Advance Colorimetry ™ - VITEK 2® COMPACT system; BioMérieux, Marcy-l’Étoile, France) and VITEK 2® PC Software v9. The growth of microorganisms in blood cultures was screened by the BacT/Alert Microbial Detection System (Organon Teknika). This is an automated test system capable of incubating, agitating and continuously monitoring aerobic and anaerobic media inoculated with specimens from patients suspected of having bacteremia.
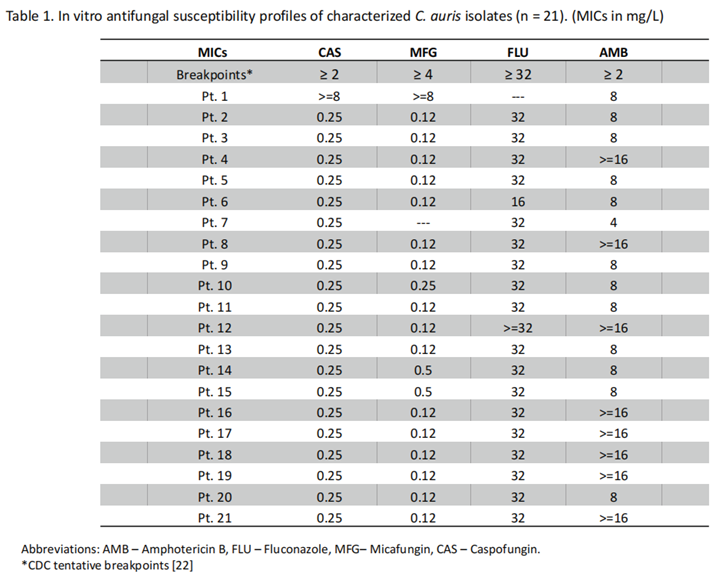
Antifungal susceptibility testing of four antifungal agents (i.e. caspofungin, micafungin, fluconazole, amphotericin B) was performed according to the CLSI M27-A3 guidelines, using broth microdilution minimum inhibitory concentrating (MIC) technique (VITEK 2® COMPACT system; BioMérieux, Marcy-l’Étoile, France). As C. auris specific susceptibility breakpoints have not yet been established, tentative breakpoints proposed by the CDC or previously adopted by other studies were used [22]. Thus, resistance breakpoints were defined as follows: caspofungin at ≥ 2 pg/ml, micafungin at ≥ 4 pg/ml, fluconazole at ≥ 32 pg/ml, amphotericin B at ≥ 2 pg/ml.
3. Results
3.1. Case Series Description
We present a series of cases of C. auris infections and/or colonization, reported from October 2022 to July 2023 in a public university hospital in Bucharest, mainly in the cardiovascular surgery (CVS) associated intensive care unit (ICU). Patients who underwent surgical procedures were screened for Methicillin-resistant Staphylococcus aureus and received perioperative antibiotic prophylaxis accordingly [23]. Of the 21 reported cases with C. auris during this period, some were isolated cases – in different departments, and others met the case definition for an outbreak diagnosed during the hospitalization (Figure 1 and Figure 2). According to national regulations [24] only 13 cases were identified as part of the outbreak, sharing the same hospital area. Among these cases, only 10 patients had an evident epidemiological link by sharing the same room, mostly in ICU department (Figure 3).
3.2. Outbreak Description
Positive patients were labeled based on the chronological order of their detection, from P1 to P13 (Figure 2). Once a link between cases was found, we further categorized them by filiation, keeping the index case number followed by new case number (Figure 3).
Patient number one (P1) admitted to the cardiovascular surgery department (CvSD), an unlikely index case, had a strain of C. auris isolated from the postoperative wound without indication for treatment, being considered a colonization. Subsequently, the index case of the declared outbreak, with no known contact with P1, but difficult to rule out, was a 75-year-old patient (P2), admitted in CvSD. He underwent cardiac surgery on the 7th day of hospitalization and rested in CVS-ICU with respiratory sepsis, mechanical ventilation, and underlying cardiovascular disease. C. auris was isolated from his tracheal aspirate on day 52 after surgery. Of the 4 contacts of patient P2 that were followed over time, two were subsequently diagnosed with C. auris infection. The first (P2.1) was detected with C. auris urinary tract infection (UTI) after 32 days of sharing the same room, and the second (P2.2) was diagnosed with C. auris systemic infection after 20 days, respectively. Of 5 contacts of patient P2.2, 3 became positive for C. auris in the days following exposure: UTIs after 20 days (P2.2.1), systemic infection after 10 days (P2.2.2) and superficial surgical site infection after 14 days (P2.2.3). The contact of patient P2.2.1 became positive after 8 days (P2.2.1.1) and subsequently his contact after 12 days (P2.2.1.1.1), both cases having skin colonization with a favorable outcome. In the same scenario was the contact of patient P2.2.3 who became positive after 6 days (P2.2.3.1) and subsequently his contact after 7 days (P2.2.3.1.1), both cases having skin colonization with different outcomes, depending on the underlying comorbidities (Figure 3).
The patient P11 was not in contact with any other C. auris positive patients. However, detection of C. auris on the skin after 21 days of hospitalization in the same department reflects the high risk of transmission, despite the prevention and control measures imposed at the detection of the outbreak.
The patient P12, transferred from another hospital, in a critical condition requiring mechanical ventilation from admission, became positive for C. auris in tracheal aspirate specimen collected on the 3rd day after the admission. It is not clear whether the respiratory detection of C. auris in this patient was secondary to the infection acquired in our hospital.
3.3. Antifungal Susceptibility Profile
Using the CDC tentative MIC breakpoints for the sus ceptibility interpretation [22], we found that all isolates were resistant to amphotericin B with a MIC ranging between 4 μg/mL and more than 16 μg/mL. A single isolate was susceptible to fluconazole, and a different isolate was pandrug-resistant (Table 1).
3.4. Epidemiological Measures for Outbreak Control and Limitation
Appropriate procedures for cleaning, environmental disinfection, and sterilization of medical devices, along with standard precautions and those addressed to the transmission pathway, are the basis for preventing and limiting the transmission of any pathogen in the healthcare facility. According to international and national guidelines, once a strain of C. auris was detected, the identified patients were isolated or grouped in a single room [15,25]. Dedicated nursing staff and medical equipment were established for colonized or infected patients. All infected materials were collected before leaving the room to minimize further transmission.
Instructions on hand hygiene protocol, contact precautions, and monitoring the appropriate implementation of environmental cleaning for all healthcare workers have been resumed. Family members and visitors were also notified and advised to wear gloves and gowns.
Periodic cleaning of surfaces and medical equipment, as well as terminal cleaning and disinfection of rooms with chlorine-based disinfectants and hydrogen peroxide, were monitored.
Close contacts were screened by swabbing axilla and groin, throat, (surgical site) wounds, catheter exit sites, urine and four were identified as carriers (Figure 3). Healthcare personnel screening or environmental monitoring is not advised on a regular basis [15].
All cases were reported to the National Institute of Public Health. At discharge, the status of infection or colonization with C. auris was mentioned in the medical documents for all patients.
4. Discussions
4.1. C. auris Epidemiological Features
A positive culture for C. auris may reflect either colonization or infection affecting one or more sites and has the potential to lead to severe, life-threatening invasive infections, depending on underlying medical conditions [26]. C. auris colonizes the skin, usually in the inguinal region, axilla, nostrils, urinary and respiratory tracts, and uncommon the intestinal mucosa [27,28]. In 2021, Rossow et al. conducted a study that demonstrated a 10-fold increased risk of colonization for patients on mechanical respiratory support or those who had received treatment with carbapenems or fluconazole within the previous 90 days [29].
In addition to candidemia, C. auris is also involved in complicated pleural effusions, pericarditis and ventriculitis, intra-abdominal infections, osteomyelitis, meningitis, and mastoiditis [13,28,30].
Until 2021 there were no Candida auris strain reported from Romania to ECDC [10]. The first published study refers to 40 strains obtained from 3 hospitals in Bucharest between January and August 2022 [21]. The comparatively low number of documented cases for Romania contrasting with Italy or Greece, most likely indicates the underdiagnosing and the lack of screening for this pathogen in patients with evident risk factors.
In our study, 6 patients out of 21 had cutaneous colonization of C auris. In 6 other cases, C. auris was isolated from the urinary tract - asymptomatic bacteriuria (n=3) or from skin wounds (n=4). Three of 4 patients with systemic infections diagnosed with positive blood cultures survived, while all patients with respiratory tract infections (n=3) died (Figure 2).
In the ICU, mortality might be more a consequence of the underlying disease and its complications than C auris infection per se [31,32,33]. The true correlation between mortality risk and C auris infection is difficult to determine due to the severe medical condition of the patients [34,35]. Some studies have ranked mortality according to the clades to which the isolated strains belong, the highest being for South America clades (96%), followed by Asian clades (80%), South African clades (45%) and East Asian clades (44%) [36]. In our study, regardless of detection site, 9 of 21 patients died (42.8%). Epidemiological data suggest that candidemia is usually associated with the South American and South Asian clade, while the East Asian clade is frequently associated with otitis externa, and the South African clade is responsible for the most colonization or urinary tract infections [37]. Our subjects were almost equally colonized and/or infected.
As an opportunistic pathogen, C. auris infections correlate with some common risk factors shared with the rest of the Candida family. It is also able to colonize the patient without infecting, thus being a major risk factor for fungal outbreaks due to its persistence and easy transmission [38,39]. Immunosuppression induced by immunosuppressive treatments, including corticosteroids, or acquired after specific medical conditions such as organ transplantation [39], bone marrow transplantation, prolonged administration of broad-spectrum antibiotics or antifungals, and neutropenia are important risk factors [36]. Underlying diseases such as diabetes, malignancies, HIV infection, chronic kidney and respiratory diseases, hemodialysis are also risk factors for colonization and infection with C. auris [40,41,42,43,44]. Invasive procedures such as mechanical ventilation or minimally invasive techniques such as insertion of central venous catheters, urinary catheters, peripheral intravascular lines, drain tubes, may predispose to colonization and infection with C auris, with a greater risk of invasive infection [17,42,45,46]. Most of these risk factors are present in patients with immunosuppressive conditions and in case of prolonged ICU hospitalization [43,47]. The more invasive the C auris infection, the higher the risk of mortality [14]. All our subjects were intensive care patients from both medical and surgical wards with a long length of hospital stay. However, not all could be epidemiologically involved in the reported outbreak, due to a known lack of close contact (e.g, P1 and P11) or possible HAI from another medical facility in case P12. This may support the high capacity of C. auris to spread and survive on surfaces for long periods of time [15,19,46]. Further molecular investigations could help in confirming clade I inclusion, or cluster filiation, as we epidemiologically showed. Also, these may shed light on the correlations, whether they are, between the genotype and virulence or outbreak potential.
C. auris has an unexpected ability to resist surface disinfection procedures compared to the rest of Candida species [48,49]. Widespread contamination of objects and surfaces around a patient colonized with C. auris has been demonstrated. It was observed that 75% of the samples collected from the living room surfaces of a colonized or infected patient were positive in molecular biology tests, respectively 25% were positive in culture [50]. C. auris has a high potential for transmission, which occurs through direct contact or through colonized surfaces and objects that have been in contact with an infected patient [46]. The most incriminated object responsible for transmission were blood pressure cuffs, thermometers, bells and textile cord [51,52,53], and the most frequently colonized sites were the axilla, although, for how long the patient may remain colonized has not yet been investigated [13].
Screening is performed by swabbing the patient's axilla and groin bilaterally, followed by inoculation of the samples in Sabouraud broth, which contains dulcitol and 10% salt [54]. A characteristic of this fungus is its good growth at temperatures between 40-42°C [55]. Detection of C. auris is complicated because other closely related fungi have similar patterns of assimilation and fermentation properties. Many of the earliest isolates of Candida auris were misidentified as Rhodotorula glutinis, Saccharomyces cerevisiae, Candida sake by the API 20C AUX, AP ID 32C systems or as Candida haemulonii by the Vitek 2 system [56,57,58]. For several decades, chromogenic methods of Candida species identification have played a major role in diagnosis [59]. However, to differentiate C. auris from the other Candida species, additional techniques are needed. Given that C. auris does not possess pseudohyphae or germ tubes [55], after chromogenic identification it is necessary to confirm either by using DNA sequencing or matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) [60].
4.2. Present Therapies and New Directions
The most commonly used antifungal agents for the treatment of Candida infections include the azoles and echinocandins. However, C. auris isolates frequently show resistance to fluconazole, while resistance to other antifungal agents shows greater variability.
Therapeutic guidelines for the management of C. auris recommend initiation of echinocandin monotherapy as empiric treatment before the results of susceptibility testing are available. This approach relies on the known prevalence of the resistance profile [61,62,63]. Despite emerging reports of echinocandin and pan-resistant isolates, in regions where the majority of strains remain susceptible, the use of echinocandin as primary treatment is considered reasonable [62]. However, patients should be closely monitored for clinical and microbiological response by performing cultures and susceptibility testing, as the organism can develop resistance rapidly even during treatment [64].
There is little evidence regarding the most appropriate therapy for pan-resistant strains, which express resistance to all three major classes of antifungal drugs, such as echinocandins, amphotericin B, and the azoles [7]. In vivo studies have shown inhibition of pan-resistant strains by combinations of two antifungal drugs at fixed concentrations. Favorable responses have been achieved from combinations of flucytosine with amphotericin B, azoles, or echinocandins [65]. Additionally, in vitro evidence supports echinocandin combination therapy, such as caspofungin in combination with posaconazole [66] or anidulafungin in combination with manogepix or flucytosine [67]. A new echinocandin, rezafungin, in phase 3 trials [68,69] also shows promise based on in vitro investigations against echinocandin-resistant C. auris subgroups. Fosmanogepix, a pioneering antifungal with a unique mechanism of action available in intravenous and oral forms, has shown potential activity in both in vitro and phase 2 studies [70,71]. For persistent and recurrent C. auris bloodstream infections, micafungin combination therapies appear promising based on animal studies and in vitro evaluations [62,63,64,65,66,67,68,69,70,71,72,73]
CDC recommends screening of patients with recent overnight stays in healthcare facilities outside the United States and of those who have infections or colonization with carbapenemase-producing Gram-negative bacteria. Screening should include the axilla and groin and additional sites as clinically indicated or where previous infections have been detected. Reassessment should occur at 1-to-3-month intervals. At least 2 evaluations at 1-week intervals are required for deisolation, with negative results after discontinuation of antifungal treatment [74]. For the same purpose, the CDC recommends using standard single room contact precautions with a gown and gloves. Practice hand hygiene with alcohol- or water-based hand sanitizer and soap if hands are visibly soiled and consider retraining staff. Screening of roommates with whom the index patient has stayed in the past month, or in contact for at least 3 days, those with mechanical ventilation or other higher levels of care required, and bilateral screening for axillary and inguinal colonization is required [74]. Treatment of colonized patients without evidence of infection is not recommended, and decolonization protocols do not yet exist [75]. Prophylactic measures remain the main tool for avoiding or stopping C. auris outbreaks. For final room decontamination, ECDC recommends the use of chlorine-based disinfectants, hydrogen peroxide or other documented fungicidal agents. Avoiding quaternary ammonium compounds is recommended. Preferably, the use of disposable equipment or equipment dedicated to patients with C. auris is recommended [75].
4.3. Unanswered Questions
More studies are necessary for better understanding the transmission dynamics of this fungus. We know little about the contact characteristics associated with cross-transmission such as type of contact, duration of the contact, and the minimum threshold in case of the contact at which there is no significant risk of transmission. In addition, there is still no consensus regarding the duration of surveillance after contact, how frequently should we test the contacts and for how many negative tests is safe to discontinue the isolation. Should we report negative tested contacts? Could topical skin decolonisation be efficient in lowering the risk of transmission? Is screening for C. auris indicated as recommended for other pathogens such as extended-spectrum beta-lactamase or carbapenem-producing Gram-negative bacteria or methicillin-resistant Staphylococcus aureus?
5. Conclusions
Because C. auris is highly transmissible and difficult to treat, our study emphasizes the substantial challenge encountered in clinical practise when attempting to diagnose and limit the spread of an outbreak. Therefore, it is crucial to promptly apply contact precaution measures and appropriate environmental cleaning, from the first case detected positive.
The use of general containment methods is still the only epidemiological strategy that can lower the morbidity and fatality rates associated with a C. auris outbreak, lacking a standard of care protocol. This research reveals a potentially uncontrolled spread of C. auris in hospital settings, which raises the question of implementing specific screening in vulnerable patients.
More studies are necessary for better understanding the transmission dynamics of this fungus, for better outcomes with respect to an efficient containing of the outbreaks and more effective antifungal therapies.
References
- Arastehfar, A.; Lass-Flörl, C.; Garcia-Rubio, R.; Daneshnia, F.F.; Ilkit, M.; Boekhout, T.; Gabaldon, T.; Perlin, D.S. The Quiet and Underappreciated Rise of Drug-Resistant Invasive Fungal Pathogens. J. Fungi 2020, 6, 138. [Google Scholar] [CrossRef]
- Ruiz-Gaitán, A.C.; Fernández-Pereira, J.; Valentin, E.; Tormo-Mas, M.A.; Eraso, E.; Pemán, J.; de Groot, P.W. Molecular identification of Candida auris by PCR amplification of species-specific GPI protein-encoding genes. Int. J. Med Microbiol. 2018, 308, 812–818. [Google Scholar] [CrossRef]
- Lone, S.A.; Ahmad, A. Candida auris—the growing menace to global health. Mycoses 2019, 62, 620–637. [Google Scholar] [CrossRef] [PubMed]
- Chybowska, A.D.; Childers, D.S.; Farrer, R.A. Nine Things Genomics Can Tell Us About Candida auris. Front. Genet. 2020, 11, 351. [Google Scholar] [CrossRef]
- Rhodes, J.; Fisher, M.C. Global epidemiology of emerging Candida auris. Curr. Opin. Microbiol. 2019, 52, 84–89. [Google Scholar] [CrossRef]
- Sabino, R.; Veríssimo, C.; Pereira. A.; Antunes, F. Candida Auris, An Agent of Hospital-Associated Outbreaks: Which Challenging Issues Do We Need to Have in Mind?. Microorganisms 2020, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, S.R. Candida auris and multidrug resistance: Defining the new normal. Fungal Genet. Biol. 2019, 131, 103243. [Google Scholar] [CrossRef] [PubMed]
- Sekyere, J.O. Candida auris: A systematic review and meta-analysis of current updates on an emerging multidrug-resistant pathogen. Microbiologyopen 2019, 8, e00901. [Google Scholar] [CrossRef]
- Satoh, K.; Makimura, K.; Hasumi, Y.; Nishiyama, Y.; Uchida, K.; Yamaguchi, H. Candida aurissp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol. Immunol. 2009, 53, 41–44. [Google Scholar] [CrossRef]
- Kohlenberg, A.; Monnet, D.L.; Plachouras, D. ; Candida auris survey collaborative group Increasing number of cases and outbreaks caused by Candida auris in the EU/EEA, 2020 to 2021. Eurosurveillance 2022, 27, 2200846. [Google Scholar] [CrossRef]
- Lamoth, F.; Kontoyiannis, D.P. The Candida auris Alert: Facts and Perspectives. J. Infect. Dis. 2017, 217, 516–520. [Google Scholar] [CrossRef] [PubMed]
- A Pfaller, M.; Diekema, D.J.; Turnidge, J.D.; Castanheira, M.; Jones, R.N. Twenty Years of the SENTRY Antifungal Surveillance Program: Results for Candida Species From 1997–2016. Open Forum Infect. Dis. 2019, 6, S79–S94. [Google Scholar] [CrossRef] [PubMed]
- Candida auris: a review of recent literature. GOV.UK. Available online: https://www.gov.uk/government/consultations/candida-auris-update-to-management-guidance/candida-auris-a-review-of-recent-literature. (accessed on 10 September 2023).
- Hardeep, K.; Khushbu, W.; Kusum, J.; Anamika, Y. Multidrug-resistant Candida auris: A global challenge. J. Appl. Biol. Biotechnol. 2021. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. (2022) Rapid risk assessment: Candida auris outbreak in healthcare facilities in northern Italy, 2019-2021; Available online: https://www.ecdc.europa.eu/en/publications-data/rapid-risk-assessment-candida-auris-outbreak-healthcare-facilities-northern-italy ; accessed on 10 September 2023.
- Borman, A.M.; Johnson, E.M. Candida auris in the UK: Introduction, dissemination, and control. PLOS Pathog. 2020, 16, e1008563. [Google Scholar] [CrossRef] [PubMed]
- Rudramurthy, S.M.; Chakrabarti, A.; Paul, R.A.; Sood, P.; Kaur, H.; Capoor, M.R.; Kindo, A.J.; Marak, R.S.K.; Arora, A.; Sardana, R.; et al. Candida auris candidaemia in Indian ICUs: analysis of risk factors. J. Antimicrob. Chemother. 2017, 72, 1794–1801. [Google Scholar] [CrossRef] [PubMed]
- PAHO/WHO | Pan American Health Organization.; Epidemiological Alert: Candida auris outbreaks in health care services in the context of the COVID-19 pandemic; 2021. Available online: https://www.paho.org/en/documents/epidemiological-alert-candida-auris-outbreaks-health-care-services-context-covid-19 (accessed on 10 September 2023).
- Prestel, C.; Anderson, E.; Forsberg, K.; Lyman, M.; de Perio, M.A.; Kuhar, D.; Edwards, K.; Rivera, M.; Shugart, A.; Walters, M.; et al. Candida auris Outbreak in a COVID-19 Specialty Care Unit — Florida, July–August 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 56–57. [Google Scholar] [CrossRef] [PubMed]
- CDC; Fungal Diseases and COVID-19; Available online: https://www.cdc.gov/fungal/covid-fungal.html accessed on 10 September 2023.
- Stanciu, A.M.; Florea, D.; Surleac, M.; Paraschiv, S.; Oțelea, D.; Tălăpan, D.; Popescu, G.A. First report of Candida auris in Romania: clinical and molecular aspects. Antimicrob. Resist. Infect. Control. 2023, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- CDC; Antifungal Susceptibility Testing and Interpretation. | Candida auris | Fungal Diseases |2022; Available online: https:// www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html ; (accessed on 1 September 2023).
- Troeman, D. P. R., Hazard, D., Timbermont, L., Malhotra-Kumar, S., van Werkhoven, C. H., Wolkewitz, M., Ruzin, A., Goossens, H., Bonten, M. J. M., Harbarth, S., Sifakis, F., Kluytmans, J. A. J. W., ASPIRE-SSI Study Team, Vlaeminck, J., Vilken, T., Xavier, B. B., Lammens, C., van Esschoten, M., Paling, F. P., Recanatini, C., … Van den Abeele, A. M. (2023). Postoperative Staphylococcus aureus Infections in Patients With and Without Preoperative Colonization. JAMA network open, 6(10), e2339793. https://doi.org/10.1001/jamanetworkopen.2023.39793 Erratum in: JAMA Netw Open. 2024 Mar 4;7(3):e244564. PMID: 37906196; PMCID: PMC10618839.
- ORDIN 1738 29/06/2022 - Portal Legislativ. Available online: https://legislatie.just.ro/Public/DetaliiDocumentAfis/257428 (accessed on 7 March 2024).
- National Institute of Public Health; Information and recommendation regarding the risk induced by colonization/ infection with Candida auris and measures to be applied in medical facilities; 2022. Available online: https://insp.gov.ro/download/informare-unitati-sanitare-privind-candida-auris/ ; (accessed on 29 February 2024).
- Chowdhary, A.; Sharma, C.; Meis, J.F. Candida auris: A rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLOS Pathog. 2017, 13, e1006290. [Google Scholar] [CrossRef]
- Piatti, G.; Sartini, M.; Cusato, C.; Schito, A.M. Colonization by Candida auris in critically ill patients: role of cutaneous and rectal localization during an outbreak. J. Hosp. Infect. 2021, 120, 85–89. [Google Scholar] [CrossRef]
- Schwartz, I.; Smith, S.; Dingle, T. Something wicked this way comes: What health care providers need to know about Candida auris. Can. Commun. Dis. Rep. 2018, 44, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Rossow, J.; Ostrowsky, B.; Adams, E.; Greenko, J.; McDonald, R.; Vallabhaneni, S.; Forsberg, K.; Perez, S.; Lucas, T.; A Alroy, K.; et al. Factors Associated With Candida auris Colonization and Transmission in Skilled Nursing Facilities With Ventilator Units, New York, 2016–2018. Clin. Infect. Dis. 2020, 72, e753–e760. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Gaitán, A.; Moret, A.M.; Tasias-Pitarch, M.; Aleixandre-López, A.I.; Martínez-Morel, H.; Calabuig, E.; Salavert-Lletí, M.; Ramírez, P.; López-Hontangas, J.L.; Hagen, F.; et al. An outbreak due to Candida auris with prolonged colonisation and candidaemia in a tertiary care European hospital. Mycoses 2018, 61, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Schelenz, S.; Hagen, F.; Rhodes, J.L.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackleton, J.; Trimlett, R.; Meis, J.F.; et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob. Resist. Infect. Control. 2016, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; Duggal, S.; Agarwal, K.; Prakash, A.; Singh, P.K.; Jain, S.; Kathuria, S.; Randhawa, H.S.; Hagen, F.; et al. New Clonal Strain ofCandida auris, Delhi, India. Emerg. Infect. Dis. 2013, 19, 1670–1673. [Google Scholar] [CrossRef]
- Jeffery-Smith, A.; Taori, S.K.; Schelenz, S.; Jeffery, K.; Johnson, E.M.; Borman, A.; Manuel, R.; Brown, C.S. Candida auris: A review of the literature. Clin. Microbiol. Rev. 2017, 31, e00029-17. [Google Scholar] [CrossRef] [PubMed]
- Al Maani, A.; Paul, H.; Al-Rashdi, A.; Wahaibi, A.A.; Al-Jardani, A.; Al Abri, A.M.A.; AlBalushi, M.A.H.; Al-Abri, S.; Al Reesi, M.; Al Maqbali, A.; et al. Ongoing challenges with healthcare-associated Candida auris outbreaks in Oman. J. Fungi 2019, 5, 101. [Google Scholar] [CrossRef]
- Araúz, A.B.; Caceres, D.H.; Santiago, E.; Armstrong, P.; Arosemena, S.; Ramos, C.; Espinosa-Bode, A.; Borace, J.; Hayer, L.; Cedeño, I.; et al. Isolation of Candida auris from 9 patients in Central America: Importance of accurate diagnosis and susceptibility testing. Mycoses 2017, 61, 44–47. [Google Scholar] [CrossRef]
- Forgács, L.; Borman, A.M.; Prépost, E.; Tóth, Z.; Kardos, G.; Kovács, R.; Szekely, A.; Nagy, F.; Kovacs, I.; Majoros, L. Comparison of in vivo pathogenicity of four Candida auris clades in a neutropenic bloodstream infection murine model. Emerg. Microbes Infect. 2020, 9, 1160–1169. [Google Scholar] [CrossRef]
- Tian, S.; Bing, J.; Chu, Y.; Chen, J.; Cheng, S.; Wang, Q.; Zhang, J.; Ma, X.; Zhou, B.; Liu, L.; et al. Genomic epidemiology of Candida auris in a general hospital in Shenyang, China: a three-year surveillance study. Emerg. Microbes Infect. 2021, 10, 1088–1096. [Google Scholar] [CrossRef]
- Calvo, B.; Melo, A.S.A.; Perozo-Mena, A.; Hernandez, M.; Francisco, E.C.; Hagen, F.; Meis, J.F.; Colombo, A.L. First report of Candida auris in America: Clinical and microbiological aspects of 18 episodes of candidemia. J. Infect. 2016, 73, 369–374. [Google Scholar] [CrossRef]
- Ruiz, G.B.; Lorenz, A. What do we know about the biology of the emerging fungal pathogen of humans Candida auris? Microbiol. Res. 2021, 242, 126621. [Google Scholar] [CrossRef]
- Morales-López, S.E.; Parra-Giraldo, C.M.; Ceballos-Garzón, A.; Martínez, H.P.; Rodríguez, G.J.; Álvarez-Moreno, C.A.; Rodríguez, J.Y. Invasive Infections with Multidrug-Resistant Yeast Candida auris, Colombia. Emerg. Infect. Dis. 2017, 23, 162–164. [Google Scholar] [CrossRef] [PubMed]
- Geremia, N.; Brugnaro, P.; Solinas, M.; Scarparo, C.; Panese, S. Candida auris as an Emergent Public Health Problem: A Current Update on European Outbreaks and Cases. Healthcare 2023, 11, 425. [Google Scholar] [CrossRef]
- Briano, F.; Magnasco, L.; Sepulcri, C.; Dettori, S.; Dentone, C.; Mikulska, M.; Ball, L.; Vena, A.; Robba, C.; Patroniti, N.; et al. Candida auris Candidemia in Critically Ill, Colonized Patients: Cumulative Incidence and Risk Factors. Infect. Dis. Ther. 2022, 11, 1149–1160. [Google Scholar] [CrossRef]
- Cortegiani, A.; Misseri, G.; Fasciana, T.; Giammanco, A.; Giarratano, A.; Chowdhary, A. Epidemiology, clinical characteristics, resistance, and treatment of infections by Candida auris. J. Intensive Care 2018, 6, 69. [Google Scholar] [CrossRef]
- Xin, H.; Mohiuddin, F.; Tran, J.; Adams, A.; Eberle, K. Experimental Mouse Models of Disseminated Candida auris Infection. mSphere 2019, 4, e00339–19. [Google Scholar] [CrossRef] [PubMed]
- Magnasco, L.; Mikulska, M.; Giacobbe, D.R.; Taramasso, L.; Vena, A.; Dentone, C.; Dettori, S.; Tutino, S.; Labate, L.; Di Pilato, V.; et al. Spread of Carbapenem-Resistant Gram-Negatives and Candida auris during the COVID-19 Pandemic in Critically Ill Patients: One Step Back in Antimicrobial Stewardship? Microorganisms 2021, 9, 95. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Alfouzan, W. Candida auris: Epidemiology, Diagnosis, Pathogenesis, Antifungal Susceptibility, and Infection Control Measures to Combat the Spread of Infections in Healthcare Facilities. Microorganisms 2021, 9, 807. [Google Scholar] [CrossRef]
- Chowdhary, A.; Voss, A.; Meis, J.F. Multidrug-resistant Candida auris: ‘New kid on the block’ in hospital-associated infections? J. Hosp. Infect. 2016, 94, 209–212. [Google Scholar] [CrossRef]
- Chaabane, F.; Graf, A.; Jequier, L.; Coste, A.T. Review on Antifungal Resistance Mechanisms in the Emerging Pathogen Candida auris. Front. Microbiol. 2019, 10, 2788. [Google Scholar] [CrossRef] [PubMed]
- Kean, R.; McKloud, E.; Townsend, E.M.; Sherry, L.; Delaney, C.; Jones, B.L.; Williams, C.; Ramage, G. The comparative efficacy of antiseptics against Candida auris biofilms. Int. J. Antimicrob. Agents 2018, 52, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Sansom, S.; Gussin, G.M.; Singh, R.D.; Bell, P.B.; Jinal, E.B.; Makhija, J.; Froilan, R.; Saavedra, R.; Pedroza, R.; Thotapalli, C.; et al. Multicenter evaluation of contamination of the healthcare environment near patients with Candida auris skin colonization. Antimicrob. Steward. Heal. Epidemiology 2022, 2, s78–s79. [Google Scholar] [CrossRef]
- de Almeida, J.N.; Brandão, I.B.; Francisco, E.C.; de Almeida, S.L.R.; Dias, P.d.O.; Pereira, F.M.; Ferreira, F.S.; de Andrade, T.S.; Costa, M.M.d.M.; Jordão, R.T.d.S.; et al. Axillary Digital Thermometers uplifted a multidrug-susceptible Candidaauris outbreak among COVID-19 patients in Brazil. Mycoses 2021, 64, 1062–1072. [Google Scholar] [CrossRef] [PubMed]
- Decker, B.K.; Clancy, C.J. Lanyards as Source of a Candida auris Outbreak: As You Investigate the Environment, Do Not Overlook Hand Hygiene*. Crit. Care Med. 2021, 49, 714–716. [Google Scholar] [CrossRef] [PubMed]
- Patterson, C.A.M.; Wyncoll, D.F.; Patel, A.B.; Ceesay, Y.M.; Newsholme, W.F.; Chand, M.F.; Mitchell, H.; Tan, M.B.; Edgeworth, J.D. Cloth Lanyards as a Source of Intermittent Transmission of Candida auris on an ICU*. Crit. Care Med. 2021, 49, 697–701. [Google Scholar] [CrossRef]
- Ong, C.W.; Chen, S.C.; Clark, J.E.; Halliday, C.L.; Kidd, S.E.; Marriott, D.J.; Marshall, C.L.; Morris, A.J.; Morrissey, C.O.; Roy, R.; et al. Diagnosis, management and prevention of Candida auris in hospitals: position statement of the Australasian Society for Infectious Diseases. Intern. Med. J. 2019, 49, 1229–1243. [Google Scholar] [CrossRef]
- Ilie, M.I. CANDIDA AURIS: THE UNWELCOME SUPERFUNGUS. FARMACIA 2023, 71, 225–235. [Google Scholar] [CrossRef]
- Chowdhary, A.; Kumar, V.A.; Sharma, C.; Prakash, A.; Agarwal, K.; Babu, R.; Dinesh, K.R.; Karim, S.; Singh, S.K.; Hagen, F.; et al. Multidrug-resistant endemic clonal strain of Candida auris in India. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 33, 919–926. [Google Scholar] [CrossRef]
- Lee, W.G.; Shin, J.H.; Uh, Y.; Kang, M.G.; Kim, S.H.; Park, K.H.; Jang, H.-C. First Three Reported Cases of Nosocomial Fungemia Caused by Candida auris. J. Clin. Microbiol. 2011, 49, 3139–3142. [Google Scholar] [CrossRef]
- Mizusawa, M.; Miller, H.; Green, R.; Lee, R.; Durante, M.; Perkins, R.; Hewitt, C.; Simner, P.J.; Carroll, K.C.; Hayden, R.T.; et al. Can Multidrug-Resistant Candida auris Be Reliably Identified in Clinical Microbiology Laboratories? J. Clin. Microbiol. 2017, 55, 638–640. [Google Scholar] [CrossRef]
- Odds, F.C.; Bernaerts, R. CHROMagar Candida, a new differential isolation medium for presumptive identification of clinically important Candida species. J. Clin. Microbiol. 1994, 32, 1923–1929. [Google Scholar] [CrossRef]
- de Jong, A.W.; Dieleman, C.; Carbia, M.; Tap, R.M.; Hagen, F. Performance of Two Novel Chromogenic Media for the Identification of Multidrug-Resistant Candida auris Compared with Other Commercially Available Formulations. J. Clin. Microbiol. 2021, 59. [Google Scholar] [CrossRef]
- Kwon, Y.J.; Shin, J.H.; Byun, S.A.; Choi, M.J.; Won, E.J.; Lee, D.; Lee, S.Y.; Chun, S.; Lee, J.H.; Choi, H.J.; et al. Candida auris Clinical Isolates from South Korea: Identification, Antifungal Susceptibility, and Genotyping. J. Clin. Microbiol. 2019, 57, 01624–18. [Google Scholar] [CrossRef]
- Lepak, A.J.; Zhao, M.; Berkow, E.L.; Lockhart, S.R.; Andes, D.R. Pharmacodynamic Optimization for Treatment of Invasive Candida auris Infection. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef]
- Treatment and Management of C. auris Infections and Colonization | Candida auris | Fungal Diseases | CDC. (2022) Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-treatment.html (accessed on 3 February 2024.
- Biagi, M.J.; Wiederhold, N.P.; Gibas, C.; Wickes, B.L.; Lozano, V.; Bleasdale, S.C.; Danziger, L. Development of High-Level Echinocandin Resistance in a Patient With Recurrent Candida auris Candidemia Secondary to Chronic Candiduria. Open Forum Infect. Dis. 2019, 6, ofz262. [Google Scholar] [CrossRef]
- O'Brien, B.; Liang, J.; Chaturvedi, S.; Jacobs, J.L.; Chaturvedi, V. Pan-resistant Candida auris: New York subcluster susceptible to antifungal combinations. Lancet Microbe 2020, 1, e193–e194. [Google Scholar] [CrossRef] [PubMed]
- Balla, N.; Kovács, F.; Balázs, B.; Borman, A.M.; Bozó, A.; Jakab. ; Tóth, Z.; Kobaissi, O.; Majoros, L.; Kovács, R. Synergistic Interaction of Caspofungin Combined with Posaconazole against FKS Wild-Type and Mutant Candida auris Planktonic Cells and Biofilms. Antibiotics 2022, 11, 1601. [Google Scholar] [CrossRef] [PubMed]
- John, L.L.; Thomson, D.D.; Bicanic, T.; Hoenigl, M.; Brown, A.J.; Harrison, T.S.; Bignell, E.M. Heightened Efficacy of Anidulafungin When Used in Combination with Manogepix or 5-Flucytosine against Candida auris In Vitro. Antimicrob. Agents Chemother. 2023, 67, e0164522. [Google Scholar] [CrossRef] [PubMed]
- Tóth, Z.; Forgács, L.; Locke, J.B.; Kardos, G.; Nagy, F.; Kovács, R.; Szekely, A.; Borman, A.M.; Majoros, L. In vitro activity of rezafungin against common and rare Candida species and Saccharomyces cerevisiae. J. Antimicrob. Chemother. 2019, 74, 3505–3510. [Google Scholar] [CrossRef] [PubMed]
- Ham, Y.Y.; Lewis, J.S.; Thompson, G.R. Rezafungin: a novel antifungal for the treatment of invasive candidiasis. Futur. Microbiol. 2021, 16, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Huband, M.D.; Rhomberg, P.R.; Bien, P.A.; Castanheira, M. Activities of Manogepix and Comparators against 1,435 Recent Fungal Isolates Collected during an International Surveillance Program (2020). Antimicrob. Agents Chemother. 2022, 66, e0102822. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, J.A.; Pappas, P.G.; Boffard, K.; Paruk, F.; Bien, P.A.; Tawadrous, M.; Ople, E.; Wedel, P.; Oborska, I.; Hodges, M.R. Clinical Efficacy and Safety of a Novel Antifungal, Fosmanogepix, in Patients with Candidemia Caused by Candida auris : Results from a Phase 2 Trial. Antimicrob. Agents Chemother. 2023, 67, e0141922. [Google Scholar] [CrossRef] [PubMed]
- Fakhim, H.; Chowdhary, A.; Prakash, A.; Vaezi, A.; Dannaoui, E.; Meis, J.F.; Badali, H. In Vitro Interactions of Echinocandins with Triazoles against Multidrug-Resistant Candida auris. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef]
- Jaggavarapu, S.; Burd, E.M.; Weiss, D.S. Micafungin and amphotericin B synergy against Candida auris. Lancet Microbe 2020, 1, e314–e315. [Google Scholar] [CrossRef]
- CDC; Infection Prevention and Control for Candida auris. (2021) Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-infection-control.html (accessed on 10 September 2023).
- European Centre for Disease Prevention and Control. Candida auris in healthcare settings – Europe; (2016). Available online: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/Candida-in-healthcare-settings_19-Dec-2016.pdf (accessed on 10 September 2023).
Figure 1.
Histogram of C. auris onset of iliness.
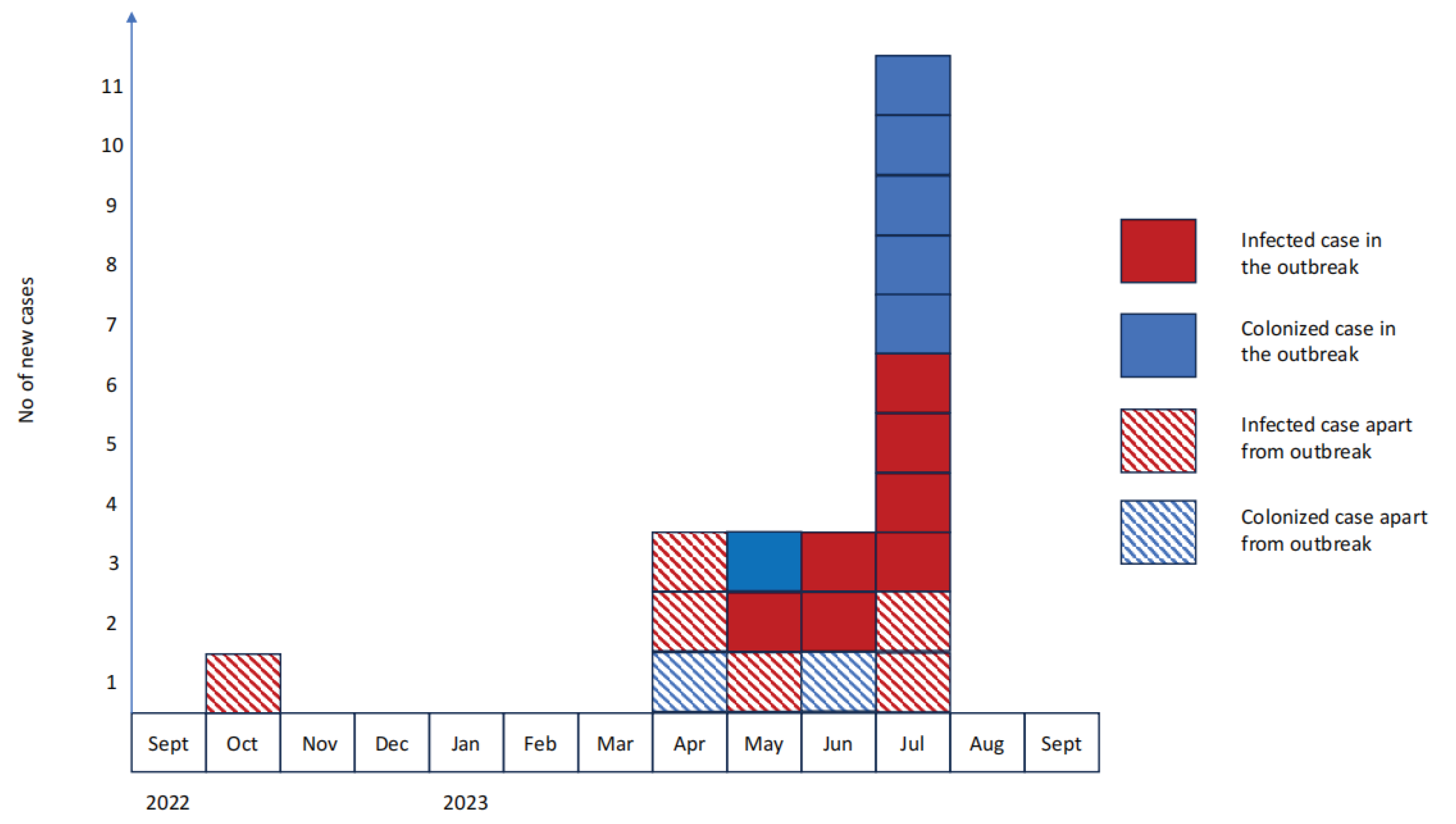
Figure 2.
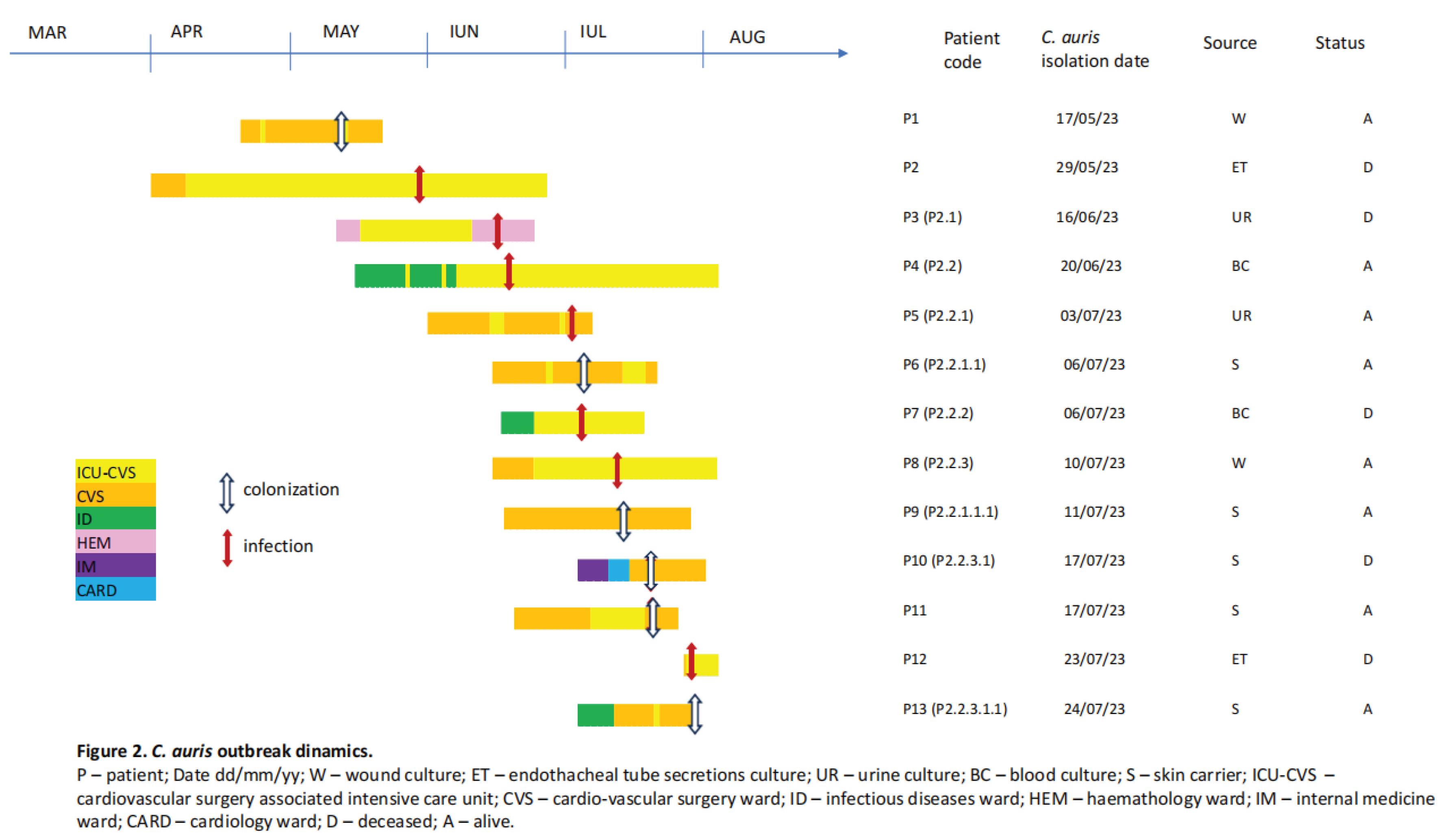
Figure 3.


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



