
Submitted:
12 March 2024
Posted:
18 March 2024
You are already at the latest version
Abstract
Introduction: Atrial fibrillation (AF) is a common cardiac arrhythmia whose prevalence rises with age and is linked to increased morbidity and mortality due to the risk of thromboembolism. Management typically involves anticoagulation and rhythm control, but the treatment of elderly patients with multiple comorbidities requires careful consideration of drug side effects and interactions. Cibenzoline, a Vaughan-Williams class IA antiarrhythmic, is effective against AF but has risks of toxicity, especially in older people and those with renal impairment, due to its renal excretion and prolonged half-life in these populations. Discussion: This paper presents a case of an 80-year-old woman with paroxysmal AF who suffered cardiac arrest due to cibenzoline toxicity despite receiving standard adjusted dosages. The patient's cibenzoline blood concentration was significantly higher than the therapeutic range, leading to cardiotoxicity, which was exacerbated by drug interactions with bisoprolol and edoxaban, both metabolized by the CYP3A4 enzyme. Venoarterial extracorporeal membrane oxygenation (V-A ECMO) and intra-aortic balloon pump (IABP) successfully managed the cardiac arrest. This case emphasizes the unpredictable pharmacokinetics of cibenzoline in elderly patients with renal impairment and the need for vigilant therapeutic drug monitoring to avoid adverse events. Conclusions: Cibenzoline can pose a significant risk of severe toxicity in elderly patients with renal impairment, and drug interactions may potentiate this risk. The paper underscores the importance of careful dose adjustment and monitoring of drug levels in this population. In cases of cibenzoline-induced cardiac arrest, V-A ECMO and IABP are effective treatment modalities. The case study serves as a critical reminder for clinicians to remain vigilant for drug-induced complications and to apply aggressive supportive treatments when necessary.
Keywords:
cibenzoline succinate
; drug toxicity
; drug interaction
; Extracorporeal Membrane Oxygenation
1. Introduction
Atrial fibrillation (AF) is a common arrhythmia, and its prevalence increases with age. It is associated with mortality and morbidity due to thromboembolism [1,2]. The primary management of paroxysmal atrial fibrillation is anticoagulation and return to sinus rhythm, often with the use of antiarrhythmic drugs. Because of the increasing number of elderly patients with multiple comorbidities and medications, strict attention must be paid to drug side effects and complications in the management of atrial fibrillation. Cibenzoline is an antiarrhythmic drug of the Vaughan-Williams class IA and is mainly used for atrial arrhythmias[1]. Cibenzoline blocks fast sodium channels. It exerts its antiarrhythmic effects by reducing the automaticity of ectopic pacemakers and prolonging the refractory period of atrial myocardium. This is effective in suppressing supraventricular arrhythmias, especially AF. Cibenzoline is a drug that is excreted by the kidneys. Monitoring is necessary for the elderly and patients with renal impairment because the half-life of cibenzoline is significantly prolonged, increasing the risk of drug accumulation and toxicity[2]. Side effects include arrhythmia-inducing effects, hypoglycemia[3,4]. Lethal arrhythmias due to intentional cibenzoline overdose have been reported [5], but severe toxicity is rare in routine clinical practice. We report a case where short-term administration of cibenzoline and drug interactions led to cardiac arrest, which was successfully treated with venoarterial extracorporeal membrane oxygenation (V-A ECMO).
2. Case Report
An 80-year-old woman with a history of gallstones and transverse colon cancer surgery, as well as mild cognitive impairment, presented to our hospital with intermittent chest pain. The patient was diagnosed with paroxysmal atrial fibrillation three days before admission, and 70 mg cibenzoline was administered intravenously twice, followed by 100 mg cibenzoline, 30 mg edoxaban, and 0.625 mg bisoprolol daily by oral. On admission, she experienced transient loss of consciousness, and the Glasgow Coma Scale score was E4V5M6. The patient’s body temperature, heart rate, blood pressure, respiratory rate, and oxygen saturation on room air were 35.6 °C, 97 bpm, 89/73 mmHg, 20/min, and 97%, respectively. Except for peripheral coldness, no other significant findings were observed. Blood tests revealed mild renal impairment and metabolic acidosis with elevated lactate levels (Table 1). Echocardiography revealed an ejection fraction of 15% and global left ventricular hypokinesia. An electrocardiogram showed ST depression in leads V5 and V6 and a prolonged QTc interval of 0.522 s (Figure 1). The patient experienced cardiac arrest 2 h after admission and was resuscitated with chest compressions and 1 mg of intravenous adrenaline. Coronary angiography ruled out significant coronary artery stenosis or acute coronary syndrome, and blood tests revealed a cibenzoline concentration of 1515 ng/mL. Despite high-dose vasopressors, the patient required V-A ECMO and intra-aortic balloon pump (IABP), that were initiated 4 h after admission. On the second day, the patient’s cardiac output improved, and she was weaned off V-A ECMO and IABP on the third day. On the fifth day, her ejection fraction recovered to 40%, and vasopressor support was discontinued. The patient was extubated on the sixth day and was discharged from the intensive care unit on the eighth day without any sequelae.
3. Discussion
A Cibenzoline succinate, with a molecular weight of 380 and a protein-binding rate of 50–60%, is primarily excreted by the kidneys; its half-life is typically 5–6 hours[2]. Therapeutic drug monitoring is crucial, especially in elderly patients or those with renal impairment, as the half-life is extended in such cases. The therapeutic range is 200–800 ng/mL, and side effects increase at concentrations >800 ng/mL[1]. Cardiotoxicity that results in cardiac arrest may have multiple causes. One of these causes is the suppression of Na+ channels, which reduces Na+ influx in cardiomyocytes. This reduction leads to diminished myocardial contractility due to an increased efflux of Ca2+. Sodium channel blockade is attributed to premature ventricular contractions and an elongation of the QRS complex, which increases the arrhythmogenic potential [2]. Furthermore, inhibiting potassium channels can prolong the QT interval, increasing the risk of torsade de pointes. It is important to note that there is a significant correlation between plasma concentration and these effects [6]. Nakamura et al. reported a direct relationship between cibenzoline succinate serum levels and left ventricular contractile function and an inverse relationship with arrhythmia prevalence [7]. In this case, the patient experienced an overdose of cibenzoline, resulting in a blood level of 1500 ng/mL despite receiving a standard intravenous dose and a reduced oral dose based on renal function and age. A decreased cardiac output and ventricular arrhythmia were observed due to reduced myocardial contractility. The blood level was lower than in previously reported cases of cardiac arrest[3]. The presented case underscores the complexities of antiarrhythmic drug use in elderly patients with renal impairment. The pharmacokinetics of cibenzoline can be unpredictable in this demographic due to altered drug clearance, as highlighted by the patient's elevated drug levels post-standard dosing. Currently, there is no established treatment method for Cibenzoline poisoning; no available antagonists exist. The concentration in the blood must naturally decrease over time. Fourteen cases of severe cibenzoline intoxication have been reported in the past. Among them, two were treated with IABP and three with V-A ECMO for circulatory failure [5.7]. In these cases, mechanical circulatory support resulted in a good outcome. Recently, V-A ECMO has been used to treat other drug intoxications with similar efficacy [8]. V-A ECMO is a practical approach for the treatment of severe cases of acute toxic poisoning associated with significant cardiac dysfunction or cardiac arrest. Simultaneous prescription of a beta-blocker (bisoprolol) and anticoagulant (edoxaban) may have influenced the outcome. This is because the same CYP3A4 metabolizes all of these drugs, and increased blood levels of the drugs and their interactions may have inhibited their metabolism by CYP3A4, thereby enhancing their effects and toxicity [2,9,10]. This is evidenced by a significantly prolonged PT-INR in the patient, suggesting a possible inhibition of drug metabolism. Therapeutic drug monitoring remains crucial, particularly in the elderly population, to prevent adverse events associated with polypharmacy and the altered pharmacokinetic profiles in this age group. In clinical practice, while cibenzoline toxicity is rare, this case highlights the need for vigilance when prescribing standard doses, even when adjusted for renal function and age. The prompt recognition of drug-induced complications and aggressive supportive treatment, including the use of V-A ECMO and IABP, can be lifesaving, as demonstrated in this case.
4. Conclusions
Clinicians should be aware that cibenzoline, an antiarrhythmic drug, carries a significant risk of severe toxicity, particularly in elderly patients with renal impairment, even at doses slightly above therapeutic levels. In addition, drug interactions with medications that are metabolized by the CYP3A4 enzyme may further increase the risk of cibenzoline toxicity. V-A ECMO and IABP are effective treatments for cibenzoline-induced cardiac arrest.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Harron, D.W.G.; Brogden, R.N.; Faulds, D.; Fitton, A. Cibenzoline. Drugs 1992, 43, 734–759. [Google Scholar] [CrossRef] [PubMed]
- Ono K, Iwasaki YK, Akao M, et al. JCS/JHRS 2020 Guideline on Pharmacotherapy of Cardiac Arrhythmias. Circ J. 2022 ;86(11):1790-1924.
- Aoyama, N.; Sasaki, T.; Yoshida, M.; Suzuki, K.; Matsuyama, K.; Aizaki, T.; Izumi, T.; Kondo, R.; Kamijo, Y.; Soma, K.; et al. Effect of charcoal hemoperfusion on clearance of cibenzoline succinate (cifenline) poisoning. J. Toxicol. Clin. Toxicol. 1999, 37, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Takada, M.; Fujita, S.; Katayama, Y.; Harano, Y.; Shibakawa, M. The relationship between risk of hypoglycemia and use of cibenzoline and disopyramide. Eur. J. Clin. Pharmacol. 2000, 56, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Kyan, R.; Uemura, S.; Toyo, Y.; Wada, K.; Nomura, K.; Bunya, N.; Narimatsu, E. Usefulness of venoarterial extracorporeal membranous oxygenation for fatal cibenzoline succinate poisoning. Acute Med. Surg. 2020, 7, e507. [Google Scholar] [CrossRef]
- Wang, D.W.; Kiyosue, T.; Sato, T.; Arita, M. Comparison of the Effects of Class I Anti-arrhythmic Drugs, Cibenzoline, Mexiletine and Flecainide, on the Delayed Rectifier K+Current of Guinea-pig Ventricular Myocytes. J. Mol. Cell. Cardiol. 1996, 28, 893–903. [Google Scholar] [CrossRef]
- Nakamura Takuya, Seki Masahiko, et al.A case where percutaneous cardiopulmonary support device was used to save a life from cardiac arrest due to Sibenadet overdose.Japanese Journal of Emergency Medicine in 2019, Vol. 30 (2), pp. 50-56.
- Wang, G.S.; on Behalf of the Toxicology Investigators Consortium. ; Levitan, R.; Wiegand, T.J.; Lowry, J.; Schult, R.F.; Yin, S. Extracorporeal Membrane Oxygenation (ECMO) for Severe Toxicological Exposures: Review of the Toxicology Investigators Consortium (ToxIC). J. Med Toxicol. 2015, 12, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Dresser, G.K.; Spence, J.D.; Bailey, D.G. Pharmacokinetic-Pharmacodynamic Consequences and Clinical Relevance of Cytochrome P450 3A4 Inhibition. Clin. Pharmacokinet. 2000, 38, 41–57. [Google Scholar] [CrossRef] [PubMed]
- Grymonprez, M.; Vanspranghe, K.; Capiau, A.; Boussery, K.; Steurbaut, S.; Lahousse, L. Impact of P-glycoprotein and/or CYP3A4-interacting drugs on effectiveness and safety of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: A meta-analysis. Br. J. Clin. Pharmacol. 2022, 88, 3039–3051. [Google Scholar] [CrossRef]
Figure 1.
Electrocardiogram on admission. Rhythm is irregular, and the QT interval is prolonged.
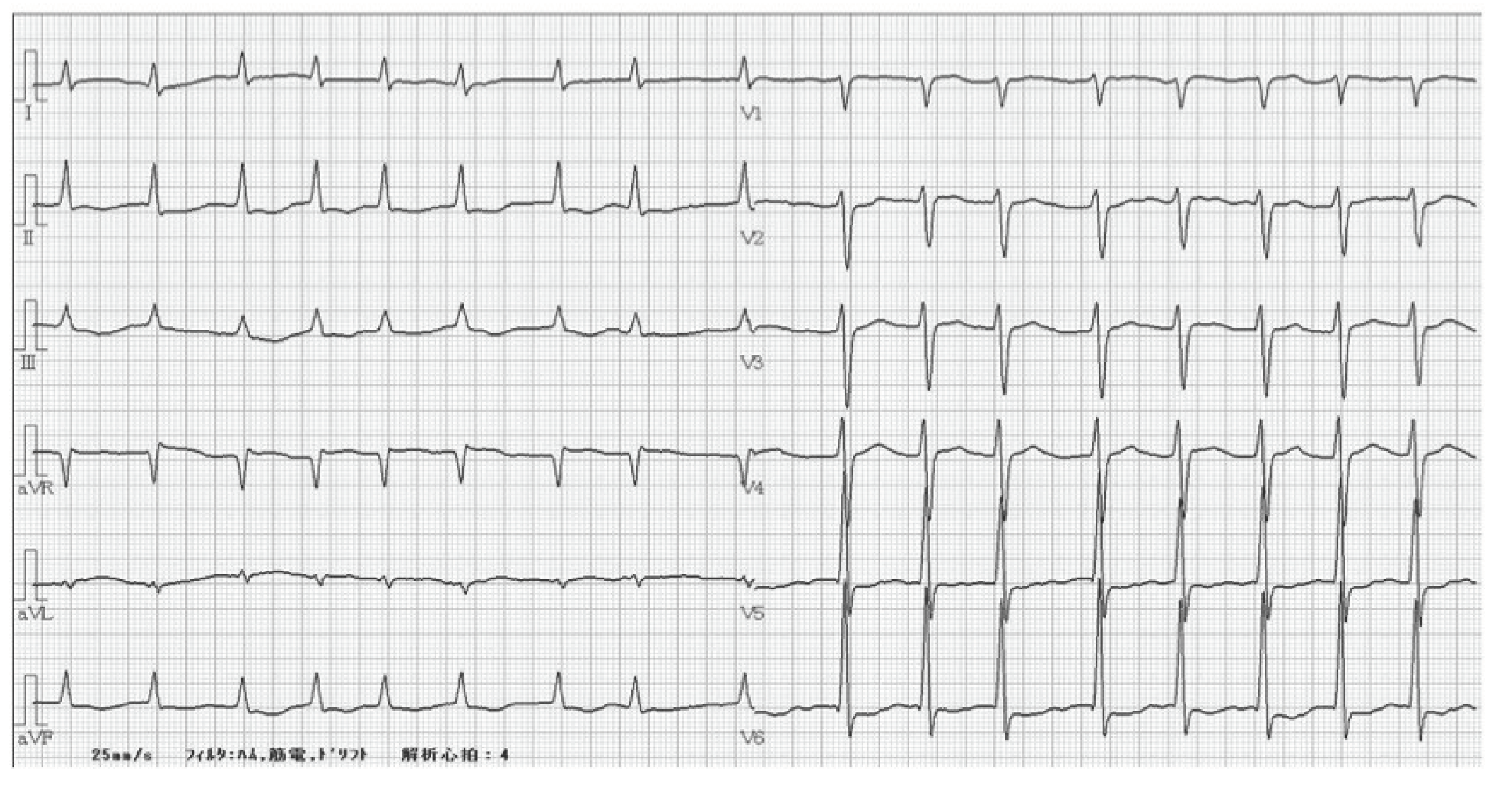

Table 1.
T Blood test results on admission. Mild renal dysfunction, metabolic acidosis, and elevated lactate levels are observed. Blood levels of cibenzoline were reported few days later.
Table 1.
T Blood test results on admission. Mild renal dysfunction, metabolic acidosis, and elevated lactate levels are observed. Blood levels of cibenzoline were reported few days later.
| <CBC> | <Chemistry> | <Arterial Blood Gas> | ||||||
| WBC | 5900 | /μL | AST | 61 | U/L | pH | 7.303 | |
| RBC | 363 | *4 / μL | ALT | 37 | U/L | pCO2 | 39.1 | mmHg |
| Hb | 13.1 | g/dL | LDH | 347 | U/L | pO2 | 120 | mmHg |
| Hct | 39.3 | % | ALP | 105 | U/L | HCO3- | 19.5 | mmol/L |
| MCV | 108.3 | fl | CK | 87 | U/L | Lactate | 4.5 | mmol/L |
| PLT | 9.7 | *4 /μL | T-Bil | 1.3 | mg/dL | Glucose | 90 | mg/dL |
| <Coagulation> | Alb | 3.7 | g/dL | |||||
| PT-INR | 4.17 | BUN | 18 | U/L | ||||
| APTT | 36.4 | sec | Cr | 1.43 | mg/dL | |||
| Fib | 232 | mg/dL | Na | 141 | mmol/L | |||
| K | 3.7 | mmol/L | ||||||
| Cl | 107 | mmol/L | ||||||
| CRP | 0.28 | mg/dL | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



