Submitted:
18 March 2024
Posted:
19 March 2024
You are already at the latest version
Abstract
Background: Several kinds of research say that adjuvant blood glucose and blood pressure are usual, but an efficient solution for medical application count remains. This review analyzes the pandemic blood pressure and blood glucose to identify the publications which tell about the clinical practices and research gaps in systematic research.Methods: A study guides to identify the research of Blood Pressure (BP) and Blood Glucose. In order to analyze the recent innovations and research on BP and Blood glucose, the relevant publications and literature from journals were identified.Results: Co-morbidity of BP and Blood glucose is reported as very high. The commonness of blood pressure is thrice as high in type I diabetes patients and almost two times higher in type II diabetes patients when compared to others without Diabetes. The pervasiveness of getting depression is more in the female when compared with men. A detailed study about the linkage of BP and blood glucose tells that the relationship between them is not exactly clear.Limitations: Nearly all reviews providing the linkage of BP and blood glucose are with some limitations and they are not providing any clear conclusion.Conclusions: Present research tells that people having high blood glucose will have a greater chance of getting high blood pressure. More research is needed to state the linkage between BP, blood glucose, and the growth of diabetes mellitus issues and to provide support for managing Diabetes.
Keywords:
blood pressure (BP)
; blood glucose
1. Background
Diabetes and depression are severe clinical states which attack most people globally and affect the standard of living. High blood pressure is mostly widespread in the common population, and it is evaluated that 5.8% of males and 9.5% of females are experiencing depression disorder or symptoms during a period of twelve month. Depression has a common association with the increasing risk of hypertension, heart-related diseases, and diabetes [1]. The genetic factor is one of the main characteristics of chronic Diabetes mellitus (DM). Diabetes can be caused in two ways; one is the incapacity of the body to induce adequate insulin, and second is because the cell ignores the insulin which was produced by the body. Type 1, Type 2, and gestational Diabetes are the common types of Diabetes Mellitus. The development of type1 Diabetes is due to the secretion of abnormal β-cells, and this is a cell that helps in controlling the lowering of blood glucose level in blood. Resistiveness of insulin and poor secretion level of insulin are the main causes of type 2 Diabetes [2,3]. TID (Type 1 Diabetes) patients require careful exogenic insulin in order to regulate their glucose level of the blood. If the insulin got overdosed this may create a low blood sugar problem which will cause harmful discomfort, coma, sudden unexpected health issues, or death. In case if the blood glucose level got increased it may also produce many health complications like nerve-related disease, kidney problems, heart-related disease, blindness, etc. Figure 1 shows the regulation of blood glucose. Most of the humans are mostly affected by type2 Diabetes [4,5]. Table 1 explains the features of Type 1 Diabetes and type 2 Diabetes.
The linkage between blood pressure and blood glucose is recognized for numerous years. People having high blood pressure will definitely have a higher chance of getting DM and also people with Diabetes have a higher possibility of getting high BP features. There is a bifacial relation between high blood pressure and high blood glucose because each condition is increasing the risk factor of others. Several kinds of research tell that the risk of high blood glucose is getting an increase from 32% to 60% by the high BP. So, depression is a prime factor to be measured in order to know the diabetic affected case. Diabetes is not able to be healed but it can be maintained below control [6]. Intaking of carbohydrates, which primarily consists of sugar and starch, can promote the release of insulin and lower blood sugar [7]. High Iodine intake can raise blood pressure and blood sugar levels as well as increase the chance of developing Diabetes and hypertension [8,9]. The elderly who walks regularly have considerable improvements in blood pressure and blood glucose levels [10].
IDF (International Diabetes Federation) Diabetes Atlas Ninth edition 2019 on Diabetes worldwide reported that death caused by Diabetes in 2019 was about 4.2 million and in 2019 about 463 million adults (20-79 years) were living with DM. It also stated that it will rise to 700 million by 2045. It is expected to have more Diabetes affected people globally by 2030 in which maximum cases will be from India. It is anticipated that by 2030 about 366 million will gets Diabetes (including 79.4 million Indians). In addition to this, research says that Diabetes or high blood sugar level commonly attacking the women community. Gestational Diabetes in women is affecting the child in upcoming years and increasing early death. Harmful Diabetes causes many problems like heart failure, kidney problems, leg cutdown, vision problems, stroke, nerve-related problems, etc. Timely detection and organized treatment are very important for controlling the blood sugar level or blood glucose level. Not only the medical treatment but also personal care is essential to put a stop to crucial secondary sickness due to diabetes [5].
Various researchers are doing researches on the relationship between stroke and hypertension. United Kingdom Prospective Diabetes Study says that one percent of HbA1c reduction can able to minimize the 4% risk of stroke. Lacunar stroke and Infratentorial stroke are very common for people with Diabetes. Some of the T1D patients instead of using MDI (Multiple Daily Insulin Injection) they started to use CGMs (Continuous Glucose Monitors) and CSII (Continuous Subcutaneous Insulin Infusion) pumps. Only a few CGMs and CSII are regulating the blood sugar level of the blood [4,11]. More than half of type 2 diabetic patients were using insulin injections or taking verbal treatment but most of them fail to follow a healthy good way of life. Many studies tell that the impact of high blood pressure is twice the amount for any diabetic affected people [12]. The finding of type 2 diabetes is very difficult and the techniques for decreasing the risk elements of gestational Diabetes and type 2 diabetes are the great expectation of a medical field [13].
By determining an individual’s high blood pressure one can easily identify the risk status of Diabetes. There are several ways for identifying high blood pressure such as symptom scales of depression, symptomatic interviews, detection through health care workers, and therapy for depression. Symptom scales technique is a common method for measuring blood pressure. Studies state that Antidepressant therapy may be useful for detecting the maximum risk of Diabetes. But the orderly proof is required on explicit proportions of depression and risk of DM [14].
2. Methods
A review was done to find out the published work as well as the research on high BP (depression) and high blood glucose (Diabetes). Searching was performed by considering the titles of a paper, abstracts of a paper, and keywords for the concept of high BP, antidepressant medication, and high blood glucose to find out the possible relevant research. Abstract presented in the conference and not having full paper publications were neglected. Random effects meta regression method was used to check whether it can identify the relationship between the depression and the variation of Diabetes based on blood pressure [15]. BP detection based on ANN and LSTM was introduced. Artificial Neural Network is for extracting the essential morphological parameters from PPG signals and EG signals. Long Short-Term Memory is to extract the time domain related features. The commonness rate of high Blood pressure in diabetic affected people is said to be twice in minimum. Subjects having high blood glucose and high BP are facing higher death risk beyond heart related death [6]. Diabetes is one of the main factors for any heart disease. One research paper tries to detect Diabetes by extracting eight features from each data subject and by the use of the most popular MLP classifier. In this PIMA database is considered for analysis and the performance of the system is validated in the MATLAB platform [16].
By examining the Heart Rate Variability from ECG signals diabetes can be estimated. Analyzing of abnormality of the heart can be done using CNN (Convolutional Neural Network) based deep learning method and CNN-LSTM (Convolutional Neural Network- Long Short-Term Memory) based deep learning method. This method is also differentiating HRV and Diabetes. By examining the Heart Rate Variability from ECG signals diabetes can be estimated. Analyzing of abnormality of the heart can be done using CNN (Convolutional Neural Network) based deep learning method and CNN-LSTM (Convolutional Neural Network- Long Short-Term Memory) based deep learning method. This method is also differentiating HRV and Diabetes. Heart rate signal will be different for normal and diabetic people. Electrocardiogram (ECG) signals can be converted into heart rate series using Pan and Tompkinson’s algorithm. Data extracted were fed into deep learning-based CNN and deep learning-based CNN-LSTM which does not depend on the feature engineering technique it estimates its own feature model but it fails to learn the whole pattern of both diabetic and normal data. Normally this deep learning method is used for finding heart-related diseases like myocardial infarction, coronary artery disease, etc. Several works were done for the detection of blood glucose using Nonlinear method, Discrete wavelet transform, Higher-order spectrum, Deep learning, and Empirical mode decomposition and their accuracy was evaluated [5].
Only the continuous value can be predicted using the linear type regression method. The logistic type regression method is preferred because it reduces the limit and range of the prediction. Diabetes-related good physical management on the mobile was one of the well-organized applications and so the scientists are working on framing a mobile application to detect blood glucose and the blood sugar level. But still, the analysis of medical data needs further improvement [3]. The model predictive control algorithm is introduced and tested with 100 virtual T1D patients. This control algorithm handles any variations in insulin but it is affected by unwanted noises. By examining the RR-interval signal diabetes can be find out. EMD (Empirical Mode Decomposition) technique is introduced to convert the RR-interval to IMF (Intrinsic Mode Function). Features like AASR (Analytic Signal Representation), MFFB (Mean Frequency computed using Fourier-Bessel Expansion), BAM (Bandwidth due to amplitude modulation), ASODP (Area of ellipse evaluated from Second Order Difference Plot), BFM (Bandwidth due to Frequency Modulation) are extracted and given to least square-support vector classifier. This classifies the diabetic RR signal and normal RR signal [4,17].
Cardiovascular Autonomic Neuropathy is the problem that causes due to DM or blood glucose of the blood and this cardiovascular autonomic neuropathy that influences the HRV (Heart Rate Variability). Discrete Wavelet Transform (DWT) Decomposition Method detects the normal and diabetic heart rate signal with 92.02% accuracy by taking out the energy feature and entropy parameter of DWT coefficient. One of the researches shows that the diabetic condition of a patient by analyzing his/her heart rate variability. This research extracted non-linear features and obtained 90% accuracy by using Adaboost Classifier. Higher Order Spectrum method was used for examining the Heart Rate Variability signal and achieved 79.93% accuracy by using the Support Vector Machine classifier for the detection of diabetes [18,19].
People with high blood pressure are at maximum risk of getting Diabetes. There is a glucose pop test in the US which will detect the glucose level using saliva [20]. Type 2 Diabetes can find out by using the report of diagnosed Diabetes from a physician, blood glucose reducing treatment, and clinical blood glucose measurement. One of the studies says that the cut off value used for the identification of fasting plasma glucose and HbA1c is 130 mg/dl and 6.2% respectively [21]. Symptoms of depression and antidepressant treatment are having more association with blood glucose for women of African Americans [22]. One study concluded that the usage of symptom scale of depression is with 17 percentage of diabetic risk and the use of antidepressant treatment is with 33% of high blood glucose risk. But there is no systematic evidence for the relation between high blood pressure and high blood glucose. Few pieces of evidence show that 50% of adults using antidepressant treatment were not with any depression problem. This treatment is just a proxy for high blood pressure and so there is no point in saying this treatment itself can increase the diabetic risk. Only 50 percent patient having depression symptoms are have been treated by the health care physician or health care workers. The risk of getting Diabetes is very much higher for cases with high blood pressure and it is less for nondepressed case.
The changes in cerebrovascular of the brain due to the high pressure of blood will cause depression. Figure 2 shows the blood pressure categories in detail. Uncontrolled high blood pressure is a huge challenge in medical care systems globally. Mobile-based monitoring of blood pressure and blood glucose level was discussed in many of the medical research discussions. One of the studies tells that the high blood pressure condition can directly attack the diabetic people. High blood pressure has 50 to 50 possibilities of creating your insulin resistant [23]. If the blood glucose level goes above 126 mg/dl and the Hemoglobin A1c comes above 6.5% then it is the indication of Diabetes. If the blood glucose lies between 110 mg/dl and 126 mg/dl and the Hemoglobin A1c comes in between 5.7% to 6.4% then it is the indication of prediabetes [2]. There is a helping community for older Diabetes affected people this Diabetes Online Community (DOC) helps them by providing a piece of required health-related information and sufficient support for an older aged people suffering with diabetes [24].
3. Results
We picked out some research papers by searching. The screening was done to select the relevant research papers which have good citations. Full research papers reviewed by reviewing the same paper’s abstract. Table 2 gives a brief view of several findings of Blood Glucose and Blood Pressure assessment. In many papers High blood glucose was detected using self-report, diabetes treatment, clinical diagnosis or medical records. Different varieties of ML (Machine Learning) methods have been introduced for detecting the blood glucose level of the blood in a nonintrusive way [25].
3.1. Pervasiveness of High Blood Glucose and High blood Pressure
The spreading of diabetes problems among adults getting increased day by day. Treatment for T2D may be used for T1D in some cases. One study tells that smart applications for detecting diabetic conditions are better than following diet and tracking blood glucose. Research reveals that, about 16% of diabetic patients managing their blood glucose through proper diet only, 25% of diabetic patients are insulin users without any other agents, and about 58% of diabetic patients are using agents named hypoglycaemic. About 62% of diabetic patients tells that they are taking hypertension treatment [45,46,47,48]. The high glucose level in the blood causes many serious harmful effects and are with a maximum risk for earlier death [49,50]. Diabetic neuropathy which will cause damage in the nerves that manage the heart and control the Blood pressure. This problem is named as CAN (Cardiovascular Neuropathy). The blood vessels and the heart are the portions of the cardiovascular system. Nerve injury in the cardiovascular system gives rise to Blood pressure problem and heart-related problem [51]. Increased risk of high blood glucose or Diabetes is related with a change in diet, less physical exercises, and blood pressure or stress. High blood glucose problem is higher in aged females. Women are more prone to develop blood sugar when they have high blood pressure [52].
Globally, the prevalence risk of high blood glucose is very high in males, but many females are affected by Diabetes than males. In 2030, it is estimated as, India will have 79.4 million diabetic people, China will have 42.3 million diabetic people, the United States will have 30.3 million diabetic people, Indonesia will have 21.3 million diabetic people, Pakistan will have 13.9 million diabetic people. In 2030, it is estimated as, Brazil will have 11.3 million diabetic patients, Bangladesh will have 11.1 million diabetic patients, Japan will have 8.9 million diabetic patients, the Philippines will have 7.8 million diabetic patients, and Egypt will have 6.7 million diabetic people. The ECG approach is an important tool for detecting the hypertensive heart related disease [53,54]. It is needed to know that the harmfulness of Diabetes is increased gradually due to present lifestyles, and development. Based on the prior researches, we have picked few factors of high blood glucose as SBP (Systolic Blood Pressure), DBP (Diastolic Blood Pressure), BMI (Body Mass Index), smoking, etc [55]. A certain review has announced that depression pervasiveness will not get vary with Type 1 and Type 2 diabetes. A study conducted in the place called the Netherlands described that almost the same rates of depressed people with T1D and T2D. People below 30 years old having more risk to have T1D disease. Men have a greater risk of getting T2D (type 2 Diabetes) than women and T2D gets increasing with increase in age and body mass index. It is known well that less sleep can be a risk for TID [56].
3.2. Bifacial Relationship between Blood Glucose and BP
Several studies described that hypertension is not only a risk for the development of Diabetes but also it is an important risk element for many heart-relevant diseases, stroke, obesity, etc. Any activity that diffusely hurts the pancreas can give rise to Diabetes. There are a greater number of unexplored Diabetes in pregnant girls. People with impaired fasting glucose (IFG) and impaired glucose tolerance (IGT) will have prediabetes problem. Impaired fasting glucose and Impaired glucose tolerance are related to hypertension, cholesterol, obesity, etc [57]. According to the WHO definition, if the pressure of the blood is ≥140/≥90 mmHg then it a metabolic syndrome. Metabolic syndrome is a composite disorderliness with many risky elements like obesity, cholesterol, hypertension, and glucose insularity, which increases many heart diseases and also doubles the risk of T2D [58]. Figure 3 shows how blood glucose is connected to blood pressure. Research shows that overweight problems in both males and females are closely related to hypertension and the risk of Diabetes or high blood glucose is also maximum for them [59].
3.3. Prior Research on Blood Glucose and Blood Pressure
Blood Pressure gets increased with low oxygen saturation of the blood. Several works have been done for oxygen saturation monitoring using Bluetooth and Wi-Fi transmission [62,63]. Blood glucose non-invasive measurement based on HRV by using AI algorithms makes the patients feel comfortable [64].Still some of the diabetes patients are using finger pricks to know their blood glucose level. There are several NIGM (Non-invasive Glucose Monitoring) system available for glucose measurement but still, these NIGM are having many difficulties to overcome [65]. Blood glucose monitoring based on sweat facing many difficulties and challenges like a collection of sweat, skin distortion, temperature, and oxidization of glucose due to the secretion of lactic acid. Sweat based glucose monitoring system determine the glucose level of the blood by analyzing the diabetic affected patient’s electrolyte subject of the sweat [66,67]. Detection of blood glucose based on breath samples are also introduced instead of using blood samples [68]. Wearable continuous glucose monitoring devices are having few drawbacks like the trouble of wearing the wearable monitoring device for a long time, giving training for handling the wearable device, and managing the patient’s lifestyle [69]. The blood glucose sensing method has a huge development over a few years. But this sensing technology of blood glucose required further more improvements in improving accuracy, reducing cost, and so on [70].
Research has been done by dealing with biosensing element-based glucose detection. More commonly used carbohydrate for the detection of Diabetes is glucose [71]. BP monitoring based on the convolutional neural network has been proposed and it is using PPG signal for the detection [72]. Cuff based Blood pressure monitoring will disturb the movement of the patient and it is also not suitable for continuous detection. Pulse transit time-based blood pressure detection without cuff is also introduced but the drawback is in order to calculate pulse transit time, ECG and the PPG signals are needed. In most of the research work on Blood Pressure detection PPG based BP monitoring is preferred because of the usage of a single signal and also by using PPG, heart rate can be also estimated [73]. There is a good relationship between Bp, diastolic period, and the delay time between systolic peak and diastolic peak [74]. Uncontrolled iodine consumption may lead to high blood glucose and high BP. It can maximize the risk of Diabetes and hypertension [75]. An increase in blood glucose and blood pressure maximizes the prevalence of Diabetes and hypertension. This will even increase the cardiovascular mortality rate [76]. 20 mm Hg Systolic Blood Pressure (SBP) is related to 58% of diabetes risk, and a 10 mm Hg Diastolic Blood Pressure (DBP) is connected with 52% of Diabetes risk [77]. By lowering the blood pressure one can minimize the mortality rate of many chronic diseases [78]. The rate of masked hypertension in T2D patients increased below 60 years, and the estimation rate of masked hypertension decreases for patients above 60 age [79]. Pulse Arrival Time (PAT) or Pulse transit time (PTT) extracted from the IT point or intersecting tangent point of PPG signal has more correlation to blood pressure. The mean correlation between Pulse transit time and SBP and the mean correlation between PAT and DBP were also estimated [80].
The perfect detection of BP is needed for the diagnosis and control of hypertension. Oscillometric method and Auscultatory methods are thought to be an acceptable method for monitoring the BP of children and young adults [81]. The coincidence of hypertension in Diabetes affected people are more likely to develop heart diseases. Therefore, patients having T2D and hypertension will have a great risk for cardiovascular disorder. Blood pressure and blood glucose are significantly connected. By knowing the blood pressure status one can predict prediabetes and thus it is said that increasing prehypertension will increase the risk of prediabetes [82]. Hypertension is a very risky factor for Diabetes connected with vascular problems, this is because hypertension alone is by several vascular disorders and difficulties [83]. By detecting the blood glucose and blood pressure one can easily predict the status of depression and Diabetes. Supervised ML (Machine Learning) algorithms are proposed for detecting the BP and blood glucose [84].
4. Limitations
There are a few limitations to this research area. Few studies do not neglect unidentified diabetic patients. There are more unidentified diabetic people among depressive people, and this can even increase the relationship between new-onset Diabetes and depression. Publication bias may also sometimes produce some errors while researching the association between blood glucose and blood pressure [85]. The survey clearly tells that the treatment of depression and Diabetes will reduce the complications of several illnesses.
5. Conclusion
Survey-based and administrative-based data collection of blood pressure shows that high BP is associated with an increased risk of high blood glucose or Diabetes. Early determination of depression and Diabetes is essential; otherwise, these chronic disorders cause many complications in life if it is detected later; Much more research is needed to determine the complication and control measures of Diabetes. Upcoming non-invasive modern technology has many more challenges like improving sensitivity, low cost, improving accuracy, and so on.
Funding
No funding is available for this study.
Data Availability Statement
No data was used for this study.
References
- A. Pan, Q. Sun, O. I. Okereke, K. M. Rexrode, and F. B. Hu. Depression and risk of stroke morbidity and mortality: A meta-analysis and systematic review. JAMA 2011, 306, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- G. Swapna, K. P. Soman, and R. Vinayakumar. Diabetes Detection Using ECG Signals: An Overview. in Studies in Big Data 2020, 68, 299–327. [CrossRef]
- H. Wu, S. Yang, Z. Huang, J. He, and X. Wang. Type 2 diabetes mellitus prediction model based on data mining. Inform Med Unlocked 2018, 10, 100–107. [Google Scholar] [CrossRef]
- D. Boiroux et al. Overnight glucose control in people with type 1 diabetes. Biomed Signal Process Control 2018, 39, 503–512. [Google Scholar] [CrossRef]
- G. Swapna, K. P. Soman, and R. Vinayakumar. Automated detection of diabetes using CNN and CNN-LSTM network and heart rate signals. in Procedia Computer Science 2018, 132, 1253–1262. [Google Scholar] [CrossRef]
- T. Roy and C. E. Lloyd. Epidemiology of depression and diabetes: A systematic review. J Affect Disord 2012, 142. [Google Scholar] [CrossRef]
- Q. Yang, X. Lang, W. Li, and Y. Liang. The effects of low-fat, high-carbohydrate diets vs. low-carbohydrate, high-fat diets on weight, blood pressure, serum liquids and blood glucose: a systematic review and meta-analysis. European Journal of Clinical Nutrition 2022, 76, 16–27. [Google Scholar] [CrossRef]
- D. Wang et al. Relationship between excess iodine, thyroid function, blood pressure, and blood glucose level in adults, pregnant women, and lactating women: A cross-sectional study. Ecotoxicol Environ Saf 2021, 208. [Google Scholar] [CrossRef]
- J. Liu, L. Liu, Q. Jia, X. Zhang, X. Jin, and H. Shen. Effects of Excessive Iodine Intake on Blood Glucose, Blood Pressure, and Blood Lipids in Adults. Biol Trace Elem Res 2019, 192, 136–144. [Google Scholar] [CrossRef]
- M. Rizka, R. L. Ambardini, L. O. A. Virama, and D. Yudhistira. The Effect of Walking Exercise on Blood Pressure and Blood Glucose in the Elderly. International Journal of Kinesiology and Sports Science 2022, 10, 30–35. [Google Scholar] [CrossRef]
- A. Alloubani, A. Saleh, and I. Abdelhafiz. Hypertension and diabetes mellitus as a predictive risk factors for stroke. Diabetes and Metabolic Syndrome: Clinical Research and Reviews 2018, 12, 577–584. [Google Scholar] [CrossRef] [PubMed]
- L. Schinckus, F. Dangoisse, S. van den Broucke, and M. Mikolajczak. When knowing is not enough: Emotional distress and depression reduce the positive effects of health literacy on diabetes self-management. Patient Educ Couns 2018, 101, 324–330. [Google Scholar] [CrossRef] [PubMed]
- N. H. Cho et al. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- M. Yu, X. Zhang, F. Lu, and L. Fang. Depression and Risk for Diabetes: A Meta-Analysis. Can J Diabetes 2015, 39, 266–272. [Google Scholar] [CrossRef] [PubMed]
- R. M. Harbord and J. P. T. Higgins. Meta-regression in Stata. 2008.
- S. K. Mohapatra, J. K. Swain, and M. N. Mohanty. Detection of Diabetes Using Multilayer Perceptron. in Advances in Intelligent Systems and Computing 2019, 846, 109–116. [CrossRef]
- R. B. Pachori, M. Kumar, P. Avinash, K. Shashank, and U. R. Acharya. An improved online paradigm for screening of diabetic patients using RR-interval signals. J Mech Med Biol 2016, 16. [Google Scholar] [CrossRef]
- L. W. Jian and T. C. Lim. Automated detection of diabetes by means of higher order spectral features obtained from heart rate signals. J Med Imaging Health Inform 2013, 3, 440–447. [Google Scholar] [CrossRef]
- U. Rajendra Acharya, O. Faust, N. Adib Kadri, J. S. Suri, and W. Yu. Automated identification of normal and diabetes heart rate signals using nonlinear measures. Comput Biol Med 2013, 43, 1523–1529. [Google Scholar] [CrossRef]
- M. Eadie and R. J. Steele. Non-invasive blood glucose monitoring and data analytics. in ACM International Conference Proceeding Series 2017, F130280, 138–142. [CrossRef]
- P. J. Tully et al. Elucidating the biological mechanisms linking depressive symptoms with type 2 diabetes in men: The longitudinal effects of inflammation, microvascular dysfunction, and testosterone. Psychosom Med 2016, 78, 221–232. [Google Scholar] [CrossRef]
- M. Kivimäki and A. Singh-Manoux. Depressive symptoms, antidepressant use, and the incidence of Diabetes in the black women’s health study. Diabetes care 2014, 37, 2211-2217. Diabetes Care 2015, 38, e22–e23. [Google Scholar] [CrossRef]
- A. G. Logan et al. Mobile Phone-Based Remote Patient Monitoring System for Management of Hypertension in Diabetic Patients. Am J Hypertens 2007, 20, 942–948. [Google Scholar] [CrossRef] [PubMed]
- M. L. Litchman, E. Rothwell, and L. S. Edelman. The diabetes online community: Older adults supporting self-care through peer health. Patient Educ Couns 2018, 101, 518–523. [Google Scholar] [CrossRef] [PubMed]
- G. Swapna, R. Vinayakumar, and K. P. Soman. Diabetes detection using deep learning algorithms. ICT Express 2018, 4, 243–246. [Google Scholar] [CrossRef]
- R. I. G. Holt, D. I. W. Phillips, K. A. Jameson, C. Cooper, E. M. Dennison, and R. C. Peveler. The relationship between depression and diabetes mellitus: Findings from the Hertfordshire Cohort Study. Diabetic Medicine 2009, 26, 641–648. [Google Scholar] [CrossRef] [PubMed]
- E. H. B. Lin et al. Depression and increased mortality in diabetes: Unexpected causes of death. Ann Fam Med 2009, 7, 414–421. [Google Scholar] [CrossRef] [PubMed]
- N. Gendelman et al. Prevalence and correlates of depression in individuals with and without type 1 diabetes. Diabetes Care 2009, 32, 575–579. [Google Scholar] [CrossRef]
- M. M. Collins, P. Corcoran, and I. J. Perry. Anxiety and depression symptoms in patients with diabetes: Original Article: Psychology. Diabetic Medicine 2009, 26, 153–161. [Google Scholar] [CrossRef]
- A. Nouwen et al. Type 2 diabetes mellitus as a risk factor for the onset of depression: A systematic review and meta-analysis. Diabetologia 2010, 53, 2480–2486. [Google Scholar] [CrossRef]
- F. Pouwer et al. Prevalence of comorbid depression is high in out-patients with Type 1 or Type 2 diabetes mellitus. Results from three out-patient clinics in the Netherlands. Diabetic Medicine 2010, 27, 217–224. [Google Scholar] [CrossRef]
- A. Pan et al. Bidirectional association between depression and type 2 diabetes mellitus in women. Arch Intern Med 2010, 170, 1884–1891. [Google Scholar] [CrossRef]
- N. Renn, L. Feliciano, and D. L. Segal. The bidirectional relationship of depression and diabetes: A systematic review. Clinical Psychology Review 2011, 31, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- A. M. Paddison et al. Predictors of anxiety and depression among people attending diabetes screening: A prospective cohort study embedded in the ADDITION (Cambridge) randomized control trial. Br J Health Psychol 2011, 16, 213–226. [Google Scholar] [CrossRef] [PubMed]
- R. C. Hermida, D. E. Ayala, A. Mojoń, and J. R. Fernańdez. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hypertensive patientswith type 2 diabetes. Diabetes Care 2011, 34, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- S. S. Franklin et al. Masked Hypertension in Diabetes Mellitus: Treatment Implications for Clinical Practice Europe PMC Funders Group. Hypertension 2013, 61, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Or and, D. Tao. A 3-Month Randomized Controlled Pilot Trial of a Patient-Centered, Computer-Based Self-Monitoring System for the Care of Type 2 Diabetes Mellitus and Hypertension. J Med Syst 2016, 40, 1–13. [Google Scholar] [CrossRef]
- W. Katon, M. Y. Fan, J. Unützer, J. Taylor, H. Pincus, and M. Schoenbaum. Depression and diabetes: A potentially lethal combination. J Gen Intern Med 2008, 23, 1571–1575. [Google Scholar] [CrossRef] [PubMed]
- E. Lloyd, G. Pambianco, and T. J. Orchard. Does diabetes-related distress explain the presence of depressive symptoms and/or poor self-care in individuals with Type 1 diabetes? Diabetic Medicine 2010, 27, 234–237. [Google Scholar] [CrossRef]
- M. Yu, X. Zhang, F. Lu, and L. Fang. Depression and Risk for Diabetes: A Meta-Analysis. Can J Diabetes 2015, 39, 266–272. [Google Scholar] [CrossRef]
- Monte-Moreno. Non-invasive estimate of blood glucose and blood pressure from a photoplethysmograph by means of machine learning techniques. Artif Intell Med 2011, 53, 127–138. [Google Scholar] [CrossRef]
- Z. D. Khan, J. Lutale, and S. M. Moledina. Prevalence of Depression and Associated Factors among Diabetic Patients in an Outpatient Diabetes Clinic. Psychiatry J 2019, 2019, 1–6. [Google Scholar] [CrossRef] [PubMed]
- B. Chireh, M. Li, and C. D’Arcy. Diabetes increases the risk of depression: A systematic review, meta-analysis and estimates of population attributable fractions based on prospective studies. Preventive Medicine Reports 2019, 14. [Google Scholar] [CrossRef]
- G. Z. Réus, M. A. B. dos Santos, A. P. Strassi, H. M. Abelaira, L. B. Ceretta, and J. Quevedo. Pathophysiological mechanisms involved in the relationship between diabetes and major depressive disorder. Life Sciences 2017, 183, 78–82. [Google Scholar] [CrossRef]
- M. A. Atkinson, B. O. Roep, A. Posgai, D. C. S. Wheeler, and M. Peakman. The challenge of modulating β-cell autoimmunity in type 1 diabetes. The Lancet Diabetes and Endocrinology 2019, 7, 52–64. [Google Scholar] [CrossRef] [PubMed]
- J. Karduck and K. Chapman-Novakofski. Results of the Clinician Apps Survey, How Clinicians Working With Patients With Diabetes and Obesity Use Mobile Health Apps. J Nutr Educ Behav 2018, 50, 62–69. [Google Scholar] [CrossRef]
- L. Bowman et al. ASCEND: A Study of Cardiovascular Events iN Diabetes: Characteristics of a randomized trial of aspirin and of omega-3 fatty acid supplementation in 15,480 people with diabetes. Am Heart J 2018, 198, 135–144. [Google Scholar] [CrossRef] [PubMed]
- M. Fang. Trends in the Prevalence of Diabetes Among U.S. Adults: 1999–2016. Am J Prev Med 2018, 55, 497–505. [Google Scholar] [CrossRef]
- U. R. Acharya et al. An integrated diabetic index using heart rate variability signal features for diagnosis of diabetes. Comput Methods Biomech Biomed Engin 2013, 16, 222–234. [Google Scholar] [CrossRef]
- O. Faust, U. R. Acharya, F. Molinari, S. Chattopadhyay, and T. Tamura. Linear and non-linear analysis of cardiac health in diabetic subjects. in Biomedical Signal Processing and Control 2012, 7, 295–302. [CrossRef]
- G. Swapna, U. Rajendra Acharya, S. Vinithasree, and J. S. Suri. Automated detection of diabetes using higher order spectral features extracted from heart rate signals. Intelligent Data Analysis 2013, 17, 309–326. [Google Scholar] [CrossRef]
- P. A. Duodu, P. Agbadi, H. O. Duah, E. Darkwah, and J. J. Nutor. Correlates of blood pressure and blood glucose screenings in Cameroon: Insights from the 2018 Demographic and Health Survey. Int Health 2022, 14, 201–210. [Google Scholar] [CrossRef]
- S. Wild et al. Global Prevalence of Diabetes Estimates for the year 2000 and projections for 2030. 2004. [Online]. Available: http://diabetesjournals.org/care/article-pdf/27/5/1047/566025/zdc00504001047.pdf.
- U. R. Acharya, H. Fujita, S. L. Oh, Y. Hagiwara, J. H. Tan, and M. Adam. Application of deep convolutional neural network for automated detection of myocardial infarction using ECG signals. Inf Sci (N Y) 2017, 415–416, 190–198. [Google Scholar] [CrossRef]
- M. M. Islam, M. J. Rahman, D. Chandra Roy, and M. Maniruzzaman. Automated detection and classification of diabetes disease based on Bangladesh demographic and health survey data, 2011 using machine learning approach. Diabetes and Metabolic Syndrome: Clinical Research and Reviews 2020, 14, 217–219. [Google Scholar] [CrossRef] [PubMed]
- Z. Xie, O. Nikolayeva, J. Luo, and D. Li. Building risk prediction models for type 2 diabetes using machine learning techniques. Prev Chronic Dis 2019, 16. [Google Scholar] [CrossRef]
- “Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33 (Suppl. S1), Suppl–S1. [CrossRef]
- Gahlan, R. Rajput, and V. Singh. Metabolic syndrome in north Indian type 2 diabetes mellitus patients: A comparison of four different diagnostic criteria of metabolic syndrome. Diabetes and Metabolic Syndrome: Clinical Research and Reviews 2019, 13, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Md. A. Uddin. Factors Influencing in Developing Type II Diabetes among Married Women in Bangladesh: Data from Bangladesh Demographic and Health Survey 2011. JOURNAL OF LIFE SCIENCES 2019, 11. [Google Scholar] [CrossRef]
- M. Maniruzzaman et al. Accurate Diabetes Risk Stratification Using Machine Learning: Role of Missing Value and Outliers. J Med Syst 2018, 42. [Google Scholar] [CrossRef]
- M. Maniruzzaman, M. J. Rahman, B. Ahammed, and M. M. Abedin. Classification and prediction of diabetes disease using machine learning paradigm. Health Inf Sci Syst 2020, 8. [Google Scholar] [CrossRef]
- R. Ashisha, X. Anitha Mary, and L. Rose. Design challenges for embedded based wireless postoperative bedside monitoring system. Journal of Interdisciplinary Mathematics 2020, 23, 285–292. [Google Scholar] [CrossRef]
- R. Ashisha, X. Anitha Mary, K. Rajasekaran, and R. Jegan. IoT-Based Continuous Bedside Monitoring Systems. in Advances in Intelligent Systems and Computing 2019, 750, 401–410. [CrossRef]
- M. Gusev et al. Noninvasive Glucose Measurement Using Machine Learning and Neural Network Methods and Correlation with Heart Rate Variability. Journal of Sensors 2020, 2020. [Google Scholar] [CrossRef]
- “Non-invasive blood glucose testing: the horizon. 2016. [Online]. Available: www.hsric.nihr.ac.uk.
- Lee et al. B I O E N G I N E E R I N G Wearable/disposable sweat-based glucose monitoring device with multistage transdermal drug delivery module.” [Online]. Available: http://advances.sciencemag.org/.
- S. Emaminejad et al. Autonomous sweat extraction and analysis applied to cystic fibrosis and glucose monitoring using a fully integrated wearable platform. Proc Natl Acad Sci U S A 2017, 114, 4625–4630. [Google Scholar] [CrossRef] [PubMed]
- C. Todd, P. Salvetti, K. Naylor, and M. Albatat. Towards non-invasive extraction and determination of blood glucose levels. Bioengineering 2017, 4. [Google Scholar] [CrossRef]
- Azhar, S. W. Gillani, G. Mohiuddin, and R. A. Majeed. A systematic review on clinical implication of continuous glucose monitoring in diabetes management. Journal of Pharmacy and Bioallied Sciences 2020, 12, 102–111. [Google Scholar] [CrossRef] [PubMed]
- I. E. Forde, S. Browne, D. Smith, and W. P. Tormey. Glucose sensing technology—current practice? Irish Journal of Medical Science 2019, 188, 125–127. [Google Scholar] [CrossRef] [PubMed]
- H. B. Chandalia and B. R. Boshell. Diagnosis of Diabetes The Size and Nature of Carbohydrate Load.” [Online]. Available: http://diabetesjournals.org/diabetes/article-pdf/19/11/863/345217/19-11-863.pdf.
- O. Schlesinger, N. Vigderhouse, D. Eytan, and Y. Moshe, BLOOD PRESSURE ESTIMATION FROM PPG SIGNALS USING CONVOLUTIONAL NEURAL NETWORKS AND SIAMESE NETWORK. [Online]. Available: http://sipl.technion.ac.il/.
- Z. Taha, L. Shirley, and M. A. Mohd Razman. A review on non-invasive hypertension monitoring system by using photoplethysmography method. Movement, Health & Exercise 2017, 6. [Google Scholar] [CrossRef]
- R. Samria, R. Jain, A. Jha, S. Saini, and S. R. Chowdhury, Noninvasive Cuffless Estimation of Blood Pressure using Photoplethysmography without Electrocardiograph Measurement.
- Liu, L. Liu, Q. Jia, X. Zhang, X. Jin, and H. Shen. Effects of Excessive Iodine Intake on Blood Glucose, Blood Pressure, and Blood Lipids in Adults. Biol Trace Elem Res 2019, 192, 136–144. [Google Scholar] [CrossRef]
- M. Barale, V. Cappiello, E. Ghigo, and M. Procopio. Increased frequency of impaired fasting glucose and isolated systolic hypertension in Paget’s disease of bone. Endocrine 2019, 63, 385–390. [Google Scholar] [CrossRef]
- C. A. Emdin, S. G. Anderson, M. Woodward, and K. Rahimi. Usual Blood Pressure and Risk of New-Onset Diabetes Evidence From 4.1 Million Adults and a Meta-Analysis of Prospective Studies. 2015.
- D. Ettehad et al. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. The Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef]
- I. Zhou, C. Liu, P. Shan, Y. Zhou, E. Xu, and Y. Ji. Prevalence and distinguishing features of masked hypertension in type 2 diabetic patients. J Diabetes Complications 2013, 27, 82–86. [Google Scholar] [CrossRef] [PubMed]
- J. Lee, S. Yang, S. Lee, and H. C. Kim. Analysis of pulse arrival time as an indicator of blood pressure in a large surgical biosignal database: Recommendations for developing ubiquitous blood pressure monitoring methods. J Clin Med 2019, 8. [Google Scholar] [CrossRef]
- P. Muntner et al. Measurement of blood pressure in humans: A scientific statement from the american heart association. Hypertension 2019, 73, E35–E66. [Google Scholar] [CrossRef]
- C. Edeoga et al. Relationships between blood pressure and blood glucose among offspring of parents with type 2 diabetes: Prediction of incident dysglycemia in a biracial cohort. J Diabetes Complications 2017, 31, 1580–1586. [Google Scholar] [CrossRef]
- J. R. Petrie, T. J. 83. J. R. Petrie, T. J. Guzik, and R. M. Touyz. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Canadian Journal of Cardiology 2018, 34, 575–584. [Google Scholar] [CrossRef] [PubMed]
- S. P. Chatrati et al. Smart home health monitoring system for predicting type 2 diabetes and hypertension. Journal of King Saud University - Computer and Information Sciences 2022, 34, 862–870. [Google Scholar] [CrossRef]
- E. A. Graham, S. S. Deschênes, M. N. Khalil, S. Danna, K. B. Filion, and N. Schmitz. Measures of depression and risk of type 2 diabetes: A systematic review and meta-analysis. Journal of Affective Disorders 2020, 265, 224–232. [Google Scholar] [CrossRef]
Figure 1.
Regulation of blood glucose.
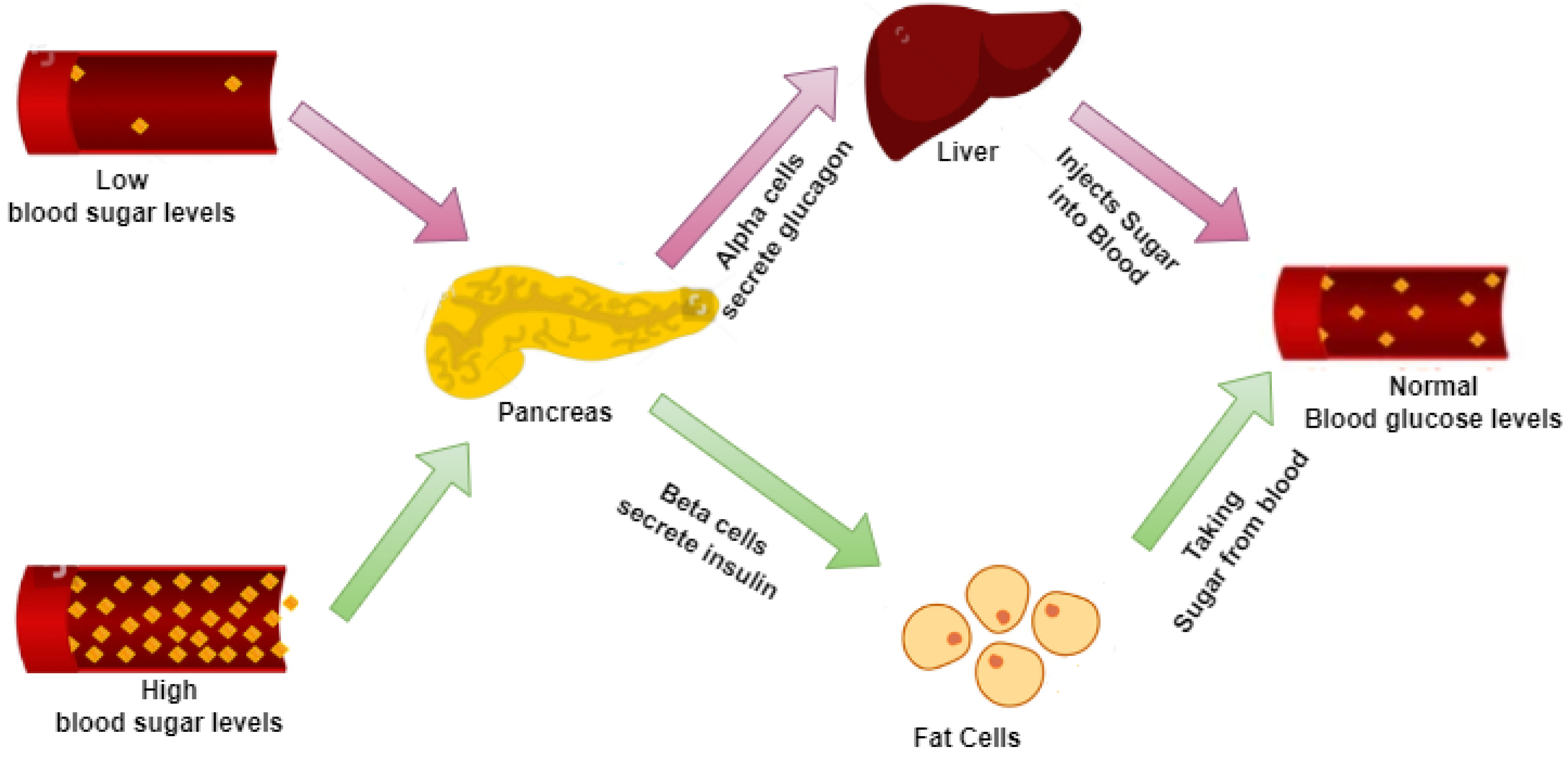
Figure 2.
Blood Pressure Categories.
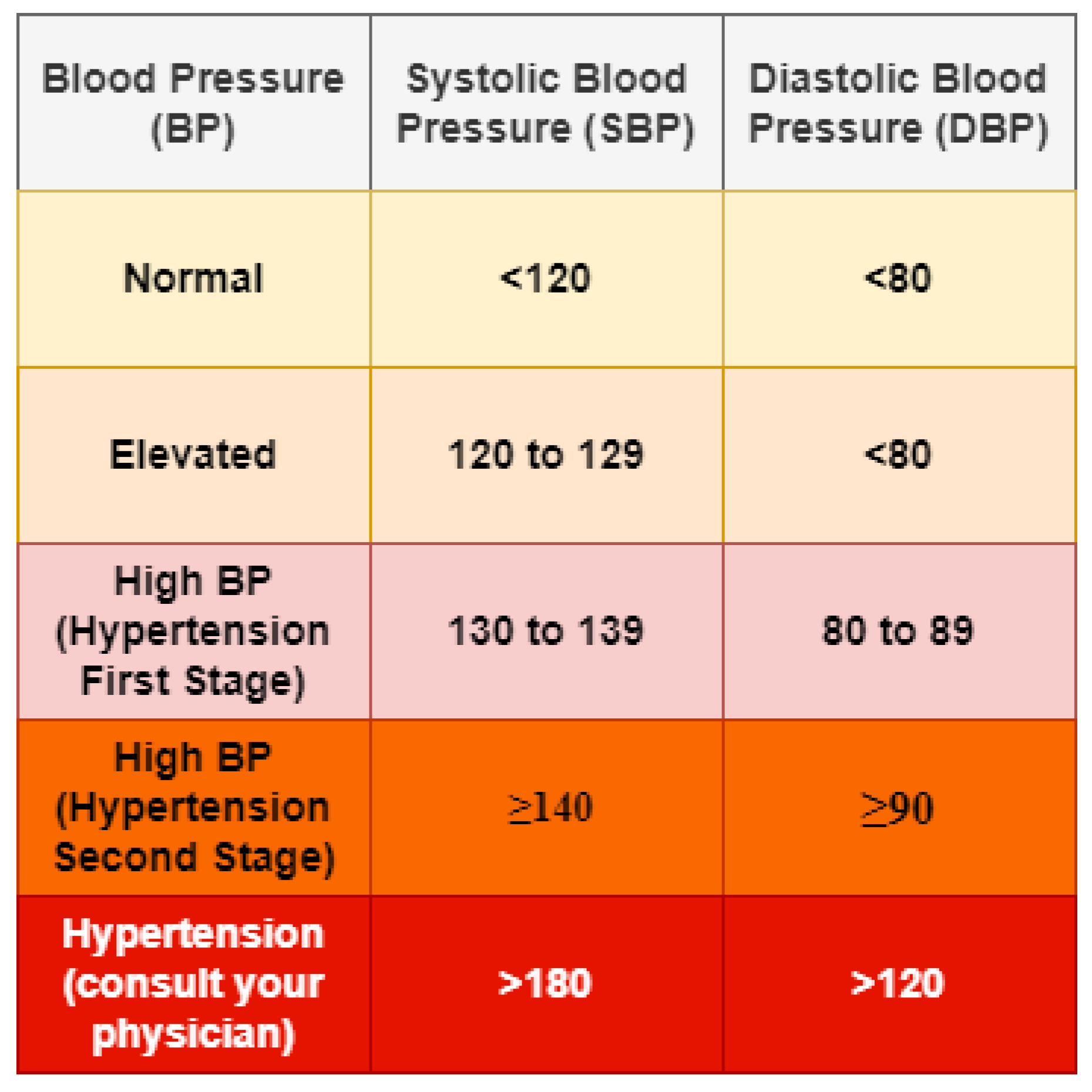
Figure 3.
Association between blood glucose and BP.
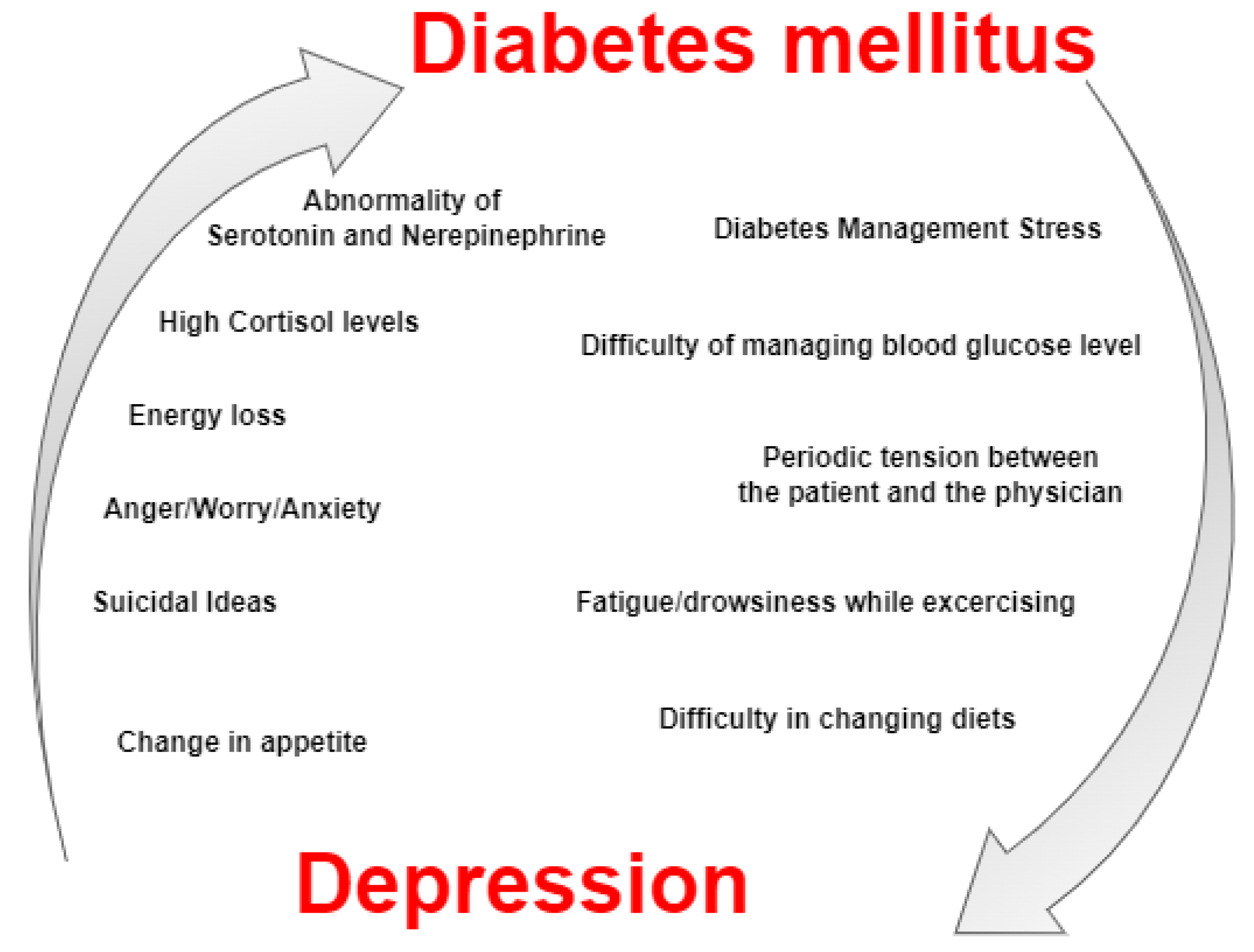

Table 1.
Characteristics of T1D and T2D[6].
Table 1.
Characteristics of T1D and T2D[6].
| Characteristics | T1D | T2D |
| Age | Above 40 years | Above 50 years |
| Length of symptoms | Many weeks | Many weeks to many years |
| Weight | underweight or Normal | Overweight |
| If not treated | death | No immediate death |
| Diabetic family history | Mostly No | Mostly Yes |
Table 2.
Significant Discoveries of Studies Assessed.
| Authors | Blood Glucose Evaluation Methods | Blood Pressure Evaluation Methods | Results |
| Ref [26] | Hospital Anxiety and Depression Scale | WHO standard | The linkage is there between high blood glucose and high blood pressure. The study also finds that there is a association between depression, blood glucose, and insulin concentration in males. High blood pressure can lead to Diabetes. |
| Ref [27] | Patient Health Questionnaire (PHQ-9) | Clinical Records | People with T2D and high blood pressure facing high mortality chances. After adjusting some clinical characteristics, little high pressure is not showing a significant relationship with mortality risk. |
| Ref [28] | Beck Depression Inventory II | Clinical Records | The commonness of high blood pressure is higher in type 1 diabetic patients. The pervasiveness of high blood glucose is significantly high in patients affected by high blood pressure. |
| Ref [29] | Hospital Anxiety and Depression Scale (HADS) | Clinical Records | People having high blood pressure are at a higher chance of getting depression. |
| Ref [30] | Self-report | Self-report, medical record or fasting plasma glucose test (FPG) | Patients with type 2 Diabetes has a 24% risk of getting depression. |
| Ref [31] | World Health Organization-5Well Being Index (WHO-5), Centre for Epidemiologic Studies-Depression scale (CESD), Composite International Diagnostic Interview (CIDI) |
Self-Report, Diagnostic Interview | Depression is a common problem in Type 1 Diabetes and Type 2 Diabetes. There is an increased risk for women affected by Type 2 Diabetes, uncontrollable Type 1 Diabetic Patients, and those who are with diabetic complications. |
| Ref [32] | 5-item Mental Health Index (MHI-5) | Self-Report, Medical Record Review | In depression patients the risk for T2D is high. Alternatively, patients with high blood glucose have a higher risk of developing high blood pressure. |
| Ref [33] | Psychiatric interview, Self-Report | fasting plasma glucose test (FPG), Self-Report, Medical Records | The association between BP and blood glucose are well explained in the literature, but the exact evidence for the association is unclear. |
| Ref [34] | Hospital Anxiety and Depression Scale | WHO Standards | The diabetes testing result was not associated with depression at a 12-month follow-up. The maximum number of self-reports of high blood glucose symptoms was related to depression. |
| Ref [12] | Diabetes website | Self-Report | The health study and the self-effectiveness have direct positive contact with Diabetes. But this positive impact will disappear if the person is affected by depression or high blood pressure. |
| Ref [35] | Bedtime Treatment | Bedtime Treatment | Bedtime treatment with ≥1 blood pressure-reducing medication, enhance BP control, and also reduces the heart-related risk in any patient affected by hypertension and T2 Diabetes. |
| Ref [6] | Systemic Review | Systemic Review | Depression is developing in patients with high blood glucose. But more studies are needed for providing a clear view of the relationship between DM and high BP. |
| Ref [36] | Population-based 11-country International Database |
Population-based 11-country International Database |
29% untreated diabetic patients having masked hypertension and heart-related issues as stage 1 hypertension patient and they need a reasonable reduction in their blood pressure. |
| Ref [37] | Self-Monitoring | Self-Monitoring | The study of three months about the self-monitoring of T2D and hypertension concludes that by using the computer-based self-monitoring systems hypertension can be controlled. |
| Ref [38] | Health Assessment Questionnaire Survey | Self-Report or Clinical Diagnosis | Comorbid depression creates increasing death rates. There is a need for research to find whether the increase in death rate connected with blood pressure is because of a patient's behavior (poor diet, smoking habit) or physical problems correlated with high blood pressure. |
| Ref [39] | Problem Areas in Diabetes (PAID) scale |
Center for Epidemiologic Studies Depression (CES-D) Scale, Beck Depression Inventory (BDI) |
There may be an important impact of high blood pressure on Diabetes. |
| Ref [40] | Egger regression asymmetry test | Egger regression asymmetry test | The patient with high blood pressure has 41% of increasing risk factors for DM and also 32% of increasing risk factors of T2D. The linkage is not clear and so further research is required to prove this result. |
| Ref [22] | Black Women’s Health Study (BWHS) | Black Women’s Health Study (BWHS) | Depression disorder or depression symptoms and the usage of antidepressants has a relationship with the development of Diabetes. |
| Ref [41] | Photoplethysmograph sensor | Photoplethysmograph sensor | This system detects the blood pressure and blood glucose from s PPG sensor. But in 1.9% of cases this system is not properly detecting blood glucose. |
| Ref [42] | 9-item Patient Health Questionnaire (PHQ 9) scale |
9-item Patient Health Questionnaire (PHQ 9) scale |
A larger number of diabetic patients are with the slightest depression and also about 30% of them had mild or moderate depression. Patients with smoking habits and also patients taking insulin treatment are completely related with experiencing mild or moderate hypertension. |
| Ref [43] | Longitudinal Studies | Longitudinal Studies | High blood glucose is a risk element of developing depression. Depressive disorder is maximum in diabetic patients compared to peope without Diabetes. This depression risk is because of the repetition of depression in patients with depression history or due to diabetes complications. |
| Ref [44] | Longitudinal Studies | Longitudinal Studies | People with Major Depressive Disorder (MDD) are having a higher risk of developing Diabetes mellitus (DM) than those are without MDD. But many diabetic patients will not be diagnosed with depressive disorder. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



