
Submitted:
18 March 2024
Posted:
20 March 2024
You are already at the latest version
Abstract
Diabetes mellitus – type 2 (DM2) is a hypercoaguable state with enhanced platelets (PLTs) activation and increased clotting factor production. Simultaneously, the fibrinolytic cell system is inhibited due to formation of clots with high resistance to fibrinolysis. The stages of PLTs "activation" have been well-characterized microscopically, morphometrically and nanomechanically (by light microscope, transmisiion electron microscope - TEM, scanning electron microscope - SEM and atomic force microscope - AFM). Thrombocytes in "acivated" (pro-coagulant) state play central role in two main biological processes: hemostasis and repair of vascular vessels. Pro-coagulant PLTs participate in generation of thrombin and in development of fibrin fibers in the clot matrix. Enhanced PLTs reactivity in dibetic- (diabetes mellitus - DM2) patients is considered as a "pro-thrombotic" state. In the retrospective- and prospective- studies on the topic, the higher are the PLTs' hematometrical indices: PLTs (count), MPV (mean platelet volume), PDW (platelet distribution width), PCR (plateletcrit), as well as PLTs/Ly ratio. The PLТs parameters/indices are usefull biomarkers in early diagnosis and prognosis of DM2. The precise studies of PLTs' state of activation during DM2 might be useful for creation of new diabetes (DM2) treatment strategies and effective medicines. Using the amount of blood glucose, attached to hemoglobin (HbA1c values) as markers of glycemic control in diabetic patients, researchers have observed association between MPV and medications as Insulin, Metformin, sulphonyl ureas. Computational modellng of PLTs' activation in DM2 is also a controlling factor for thrombocyte distribution and margination in bood vessels, associated with micro- and macrovascular disease in DM2. PLTs-derived miRNAs are novel molecular biomarkers for diagnosis and prognosis of DM2, insulin resistance and diabetes complications. We have proposed (2010) oleic acid (OA) as a substance suppressing "PLT hyperactivation" and inhibiting “thrombocyte aggregation”. Antiplatelet agents, natural plant products including, could be effective in the prevention and the secondary treatment of micro- and macrovascular complications in the type 2 Diabetes mellitus. Our proposal on following up of a combination of hematological-, hemorheological- and hemostatic parameters (indices) as a new way in diagnosis, treatment, predicting and management of DM2 and its related vascular complications, probably could be more explored in future studies.
Keywords:
Diabetes mellitus type 2 (DM-2)
; blood platelets (PLTs)
; PLT-hematological / hemorheological / hemostatic parameters (indices)
; PLT "activaion" / "hyperactivation"
; computational modeling of PLTs
; macro- and microvascular deseas (complications) in DM2
Introduction
Blood platelets (thrombocytes) are produced in bone marrow and spleen as small (1-2 µm in diameter), anucleate cell fragments from the cytoplasm of megacaryocytes. Platelets (PLTs) have smooth surface and discoid shape. In the peripheral blood PLTs are involved in thrombogenesis, confirmed in vivo and by in vitro clots formation/modelling [1].
PLTs contain and synthesize cell growth factors, chemokines, coagulation proteins, two type secretory granules (alpha granules and “dense” granules), adhesion molecules, etc. [2,3].
In response to various stimuli and/or damages, PLTs undergo morphological and functional changes, known as PLTs “activation” [4]. Activated (procoagulant) thrombocytes play central role in two main processes – hemostasis and repair of vascular vessels [5,6]. Procoagulant PLTs participate in generation of thrombin and in development of the 3-dimensional fibrin matrix during hemostasis/thrombogenesis. Human platelet membrane derived, small (≤ 0.1 µm) micro-particles with procoagulant effects, are involved in thrombin formation and thus, in thrombotic complications (e.g. attributable to diabetes mellitus type 2 /DM2/) [7,8].
During PLTs activation, changes in the shape of PLTs appear first, from discoid to spherical, with actin-rich philopodia (cytoplasmic extrusions) interacting, flattening and spreading on the surfaces in the last of the activation phases [9,10,11]. The same authors characterized the PLTs activation stages morphometrically and nanomechanically by atomic force microscope (AFM) for diagnostic purposes.
Topics and Results
1. Enhanced PLT Reactivity in Diabetic Patients Has Been Soon Considered as a “Pro-Thrombotic State”
PLTs studies are of main importance for the regular treatment, successful management and improved outcome of DM2. In the retrospective and prospective studies on the topic, the higher values of hematometrical indices – PLTs count, mean platelet volume (MPV) and platelet distribution width (PDW), serve as risk indicators for development of diabetic vascular complications. Easily identifiable during routine automated hematological analysis, the increased thrombocyte volume indices – MPV, PDW and PCR (plateletcrit) could be useful early diagnostic and prognostic markers, especially of thrombogenesis in DM2. The authors characterized PLTs from patients with DM2 as “highly reactive, playing a key role in the development of diabetic vascular complications” [12,13].
2. Platelets Signaling /Abnormalities, Hyperaggregation and Signaling Abnormalities in Patients with DM2 Play Crucial Role in Thrombotic (Clots Formation) Complications and Thromboembolism during DM2 Micro- and Macroangiopathies
The precise studies [13] of these pathological states might be useful for creation and development of new DM2 treatment strategies and effective medicines to reduce PLTs hyperactivation during DM2.
From the pathological and pathophysiological points of view, DM2 and related states (obesity, metabolic syndrome, impaired glucose tolerance, insulin resistance, etc.) are closely associated with subclinical (chronic) inflammation. Thus several inflammatory hematometrical biomarkers for PLTs and erythrocytes (RBCs), as MPV, PDW and MCV, RDW are significantly elevated in DM2 compared to the data for healthy individuals (controls) [16,17,18,19,20]. MPV is significantly elevated in the diabetic study groups, compared to healthy individuals, suggesting that this hematological index is closely associated with DM2 development [16,18]
Further prospective studies with a larger cohort are necessity in the future to characterize the probable relationship of MPV and the level of metabolic (glycemic) control (concomitant HbA1c values as markers of glycemic control in patients with DM2). Further results on the topic could be of great importance for DM treatment on the principle of individual patient specific healthcare in the DM2 management.
3. Hyperglycemia Contributes to the Elevated PLTs Reactivity (Hyperactivation)
Hyperglycemia in DM2 contributes to the elevated thrombocyte activity (hyperactivation). It is possible through direct effects of glucose on PLTs membranes, resulting appearance of “larger” and “giant” PLTs (with elevated MPV and PDW) [16]. Additionally, hyperglycemia could promote glycation of PLTs proteins [21]. The insulin deficiency could also promote PLTs activation. Different bio-products in the diabetic patients’ blood could interfere with hematopoetic cells at the level of bone marrow and spleen influencing “activating” simultaneously erytropoesis and megacaryocytopoesis to produce different in size erythrocytes and platelets (anizocytosis), including “larger” and “giant” PLTs. The higher MPV indicating larger PLT sizes could suggest “stimulated thrombogenesis” and “activated thrombocytes” in blood of diabetics [14].
4. Platelet to Lymphocyte Ratio (P/L)
Platelets to lymphocytes ratio (PLT/Ly), simultaneously with neutrophiles to lymphocytes ratio (Neu/Ly), together with complete blood count (CBC), are bioparameters proposed in the routine laboratory practice [16,22].
The same authors proposed the reference intervals for PLTs: PLT (count) – 142-424; MPV: 6.8 – 10.8 (fl.). In the further routine laboratory practice, simultaneous anisocytosis for PLTs and RBCs could be determined, improving the prognostic biomarkers for DM2.

Table 1.
Thrombocytes (Platelets - PTs) reference data.
| PLTs – platelets count | 140 - 440 x 109 /L |
| MPV - mean platelet volume (MPV) | 7.80 – 11.0 fL |
| PDW - platelet distribution width | 15,5% - 30,5% |
The precise studies of DM2 pathological states (at the level of morphological, cytochemical and ultrastructural methods), might be useful for creation and development of new DM2 treatment medicines and strategies, leading to reduced PLTs hyperactivation in development of DM2 (e.g. treatment of PLTs hyperactivity with oleic acid (OA); [4,23,24].
The physiological mechanisms that underline PLTs homeostasis under the influence of OA remain unclear. OA has potential antithrombotic effects, suppressing the PLTs hyperactivation. OA also inhibits PLTs aggregation, thrombocyte granule release and calcium “mobilization”. Additionally, OA suppresses the spread of the PLTs on fibrinogen, delaying further the development of arterial thrombosis. New studies (Zhou et al., 2023) on OA as a probable antiplatelet activation “hyperactivation” drug of clinical significance for prevention and treatment of DM2, could be further useful in diabetology.
5. Hematological/Hematometrical Investigations, Related to Metabolic/Glycemic Control of DM2
Some authors teams pointed out that the parameter of mean platelet volume (MPV) is a cost-effective tool in primary health care of diabetic patients. The same authors obtained interesting results related to the metabolic/glycemic control of DM: as the glycemic control of DM2 improves, MPV and HbA1c in patients decrease. Improving PLTs activities and functions, the regular glycemic control of diabetics may delay the vascular complications of DM.
The hematometrical laboratory results obtained could be further explored in the clinical practice, as well as in creation of new computational modelling of platelets.
The MPV in diabetics was 11.3 ± 1.0 fl, compared to 9 ± 0.6 fl in non-diabetics, with p value 0.004 [21].
The mean PDW in diabetic patients was 14.2 ± 2.5 fl, where it was 10.7 ± 0.7 fl in healthy individuals (controls). The same authors observed p values of MPV and PDW to be highly significant in diabetic patients (p<0.05). Additionally, a positive statistical Pearson correlation was obtained between MPV and PDW with HbA1c in the group of diabetic patients [12,13,14,15].
Platelet indices MPV and PDW in the diabetic group were higher in diabetics with chronic vascular complications than in patients without blood vessels’ injuries, but data were not statistically significant.
Recently, the clinicians pointed out that a MPV significantly increases in diabetic patients during development of retinopathy (p=0.006) [25]. Performing correlation analysis, the same authors obtained positive correlation between HbA1c and PDW, HbA1c and MPV, as well as HbA1c and PCT.
PDW levels were found to be independently associated with diagnosis of DM2, while MPV – with PLTs activation and impaired glucose regulation [25].
Therefore, the conclusion arises that the regular monitoring of all easily acceptable and inexpensive platelet hematological/hematometrical indices are of clinical importance in diagnosis and prevention of micro- and macrovascular complications of DM2: cardiovascular- and brain- vascular diseases, blood hyper-coagulation, combined with defective fibrinolysis, dysregulated vasodilation and increased risk of vascular clot occlusion.
PLT anisocytosis (elevated MPV and PDW), simultaneously combined with RBC anisocytosis (elevated MCV and RDW), could appear as a tool predicting serious DM2 complications (inflammation, vascular thromboses, endothelial dysfunction, etc.) [26,27,28,29,30].
Association of increased MPV and PDW, related to impaired glucose regulation in DM2 has been described in the different clinical stages of disease: pre-diabetes, diabetes, vascular diabetic complications. As the elevated MPV, the increased levels of PDW are reported in the medical literature to be closely associated with DM2 and its vascular complications [18].
The complex of hematological/hematometrical results, obtained as discussed by different study groups are of great importance in assessing early DM2 diagnosis, prognosis, clinical management and improved outcome of disease [31].
Conflicting results have been also reported – e.g., on the probable relationships between PLTs count and DM development: some authors propose “association”, but several studies supported the opinion “no relationships”. Beside the thrombo-embolic disorders, association of PLTs indices with inflammatory states has been also examined. The large scale of further studies need to be evaluated.
6. Computational Platelets Modeling in DM2
The shear rate of blood is an important factor controlling platelet distribution in the blood vessels [18,32,33,34,35].
Chang et al., (2018), simulate blood with hematocrit at 20% (for controlling different blood cells suspensions) [18,36]. The results indicated that “larger platelets” are more likely to migrate towards the vessel wall. It was suggested that there is roughly 6-10% decrease in the platelet migration rate when the wall shear rate is decreased from 1000 s-1 to 600 s-1.
The weakened platelet migration at lower wall shear rates is probably due to the reduced collision between platelets and RBSs [32].
In order to present and simulate the micro-scale interactions between different types of blood cells, numerous mathematical and computational models have been developed [33,34,35]. Lattice Boltzmann and lattice kinetic Monte Carlo models have been developed to simulate platelet activation and aggregation by treating PLTs as particles under flow [37]. However, applications of these hybrid models are mostly limited to two-dimensions, due to the model complexity and the significant computational costs.
In the further created modelling systems, a multiscale approach could be proposed, facilitating a patient-specific simulation of thrombosis/thrombogenesis in different hemodynamic conditions and under different pharmacological treatments.
Yazdani and Karniadakis (2016) [38] have performed a systematic study on the RBCs and PLTs transport by considering different levels constriction, controlling hematocrit and flow rates. In this work, normal and diabetic RBCs and PLTs models are employed to simulate normal and diabetic blood flow in a rectangular channel. In the numerical framework, the four ket sub-processes of blood clotting were combined: hydrodynamics, PLTs-micromechanics, transport of PLTs coagulation factors and the registration of resulting coagulation reactions. To consider the coagulation cascade, the authors implement the mathematical model of Anand et al., (2008) [39].
Yazdani and Karniadakis (2016) [38] concluded that a higher levels of blood vessel constriction (stenosis) and elevated vessel wall shear rates lead to significantly enhanced migration of platelets. This model – with modifications, could explain the experimental data of active PLTs aggregation in a post-vascular stenosis segment of vessel wall in different pathological states (DM2, atherosclerosis, etc.).
Computational modelling has emerged as a powerful tool for investigating of pathological processes in DM2, but there are still many unexplored areas and different experimental conditions that could be targeted in the future researches on the topic.
In the cellular, tissue and organ-specific modelling of diabetic blood cells and of injured microvasculature (complications as retinopathy, nephropathy, microangiopathy, etc.), the micro-aneurisms could be obtained simultaneously with oedema and/or hemorrhages, directly affecting the organ functions [16,35,40,41].
Instead of the great advantages in bioinformatics and biomechanics, there is a lack of computational models in the medical scientific literature – to connect the prediction of blood glucose levels in diabetic patients by the aid of PLTs hematological and hemorheological biomarkers [17,18].
Altered structure and architecture, as well as the functions of fibrin clots have been reported in patients with DM2, as well as in cases of coronary artery disease (CAD). DM2 affects unfavorably plasma fibrin by lowering its permeability and susceptibility to lysis and simultaneously increasing fibrinogen plasma levels leading to hyperfibrinogenemia. Specifically, changes are attributed to glycation of fibrinogen and fibrin in diabetic patients.
Platelets activation in DM2 is a well-known modifier of fibrin clot properties. In the presence of activated PLTs fibrin clot has specific architecture with local increase in fibrin fiber diameter and density [9]. P-selectin, expressed in alpha-granules of activated platelets of DM2 patients also increases. The role of vWF in the altered plasma fibrin network properties remains to be established, which is closely related to the phenomenon fibrinolysis/thrombolysis [5].
The dynamic changes in the platelet shape and morphology continue – from an “active” to a “procoagulant state” [42,43].
Correlation was found between MPV as a main biomarker of PLTs activation and metabolic status of type 2 diabetic patients [10,17,21,44,45,46]. Important hemogram parameters are: MPV, platelet count (PLT), PDW, PCT, HbA1c and the duration of disease. Some authors suggested that RDW is also an important predictor of vascular complications of DM2 [28]. Prospective studies are needed to define and clarify all these relationsips between hematological/hematometrical indices. MPV and PDW can be easily determined on routine automated hemograms available and are significantly elevated in diabetics, compared to healthy persons; among the diabetics, the mean of MPV and PDW are higher in patients with complications (not statistically significant) [21]. The authors pointed out that monitoring of DM2 and thus, preventing of vascular complications are needed. PDW is also main PLT index, significantly higher in diabetic patients, compared to healthy controls. PLTs indices are useful biomarkers for vascular risk in grading DM. This suggested a role of increased PLT activation in the pathogenesis of DM vascular complications.
Modelling glycemic control in DM2 patients, authors concluded that hematometrical indices MPV and PDW are precise biomarkers in DM2: MPV and PDW levels are significantly elevated in diabetics with HbA1c higher than 6.5% [21].
Additionally, it may be pointed out that a regular glycemic control improves platelets biological activities and functions. Thus, the good glycemic control helps in DM2 treatment and management and could delay micro- and macrovascular complications, attributable to DM2 as a socially significant disease.
Vascular complications appearing in the protrombic/thrombic state of DM2 are mainly related to the risk factors for clot formation. In this stage of DM2, the presence of larger PLTs, as well as “giant paltelets” in the blood smears of patients, may provide simple, effortless and cost-effective diagnostic/prognostic tool, predicting the thrombotic state in the development of DM2 and in other pathological states.
Platelet activation plays important role in the development of vascular DM2 complications, MPV and PDW pathological levels increase, as precise biomarkers of platelets’ activation in DM. In their prospective study, Ulutas et al., 2014, found a statistically significant correlation between MPV and HbA1c values [44].
First Hajek et al., 1979, showed that PLTs have insulin receptors, with density of about 500 receptors/thrombocyte [46,47]. By this way, insulin could regulate directly the functions of PLTs and has an inhibitory effect on platelets’ hyperactivity.
Recent studies [48], provide insight on the potential role of platelet hematological/hematometrical parameters (PLT count, MPV and PDW), as biomarkers in diagnosis, management and prognosis of DM2. Utilizing of such easy and simple biomarkers of DM2 could have important role in the routine medical practice [46,49].
Today, mean platelet volume (MPV) is a commonly used marker of PLT size and indicator of PLT biological activity. The larger PLTs have increased protrombic potential than smaller ones. This conclusion is evaluated not only in routine clinical practice, but is confirmed by SEM and AFM microscopies [5,9,10].
MPV could be indicator of bone marrow and spleen thrombocytogenesis and PLTs turnover rate. In the scientific literature, it has been proposed that MPV is directly related to PLTs aggregation: when aggregation PLT function weakens, the MPV level decreases. This conclusion is related to optimal management of DM2 and other diseases (cardio-vascular, brain-vascular, etc.), where prothrombotic situations correlate to the degree of PLTs activation. MPV is reduced in patients receiving better glycemic control. In state of improved glycemic management, the improvement is related to reduced PLTs activity and lower MPV, respectively.
The platelet distribution width (PDW) is a main hematometrical index – linked to DM2 and other socially-important diseases. PDW demonstrates the size diversity (anisocytosis) of PLTs.
7. Combined Properties of Diabetic RBCs and PLTs Indices
Chang et al., (2018) [36] combined successfully the properties of diabetic RBCs and PLTs indices from the scientific literature. Novel contributions in this field are data on PLTs rolling near the endothelial cells in vessel walls. PLTs adhesion on vessel walls could demonstrate the process of platelets’ activation/hyperactivation [18] - evaluating the blood vessel walls injury, as well as the coagulation cascade during thrombogenesis (clots formation).
Important for DM2 are alterations in the palsma levels of coagulatory proteins, pro-coagulatory particles, metal ions, lipids’ composition and metabolism, endothelial morphology and physiology and a degree of PLTs activation [49].
In the last two decades, numerous computational models have been developed – to simulate the dynamics of all blood cells (RBCs, WBCs and PLTs), under static and dynamic (flow) conditions [32]. It is very important to impact simultaneously on defects in hemostasis and a risk of cardio-vascular diseases [50].
After contributions of Benjamin et al., (2018) [51], in the precise biological and molecular mechanisms of DM2 actively participates the MPV size index.
Researchers observe association between MPV and several medications used to manage DM2: Insulin, Metformin and Sullphonylureas [52]. For instance, Metformin has protective effects on PLTs mitochondria, inhibiting mitochondrial hyperpolarization (induced by hyperglycemia in diabetic patients). After six month treatment only with Metformin, a significant lower levels of MPV was observed in the treated patients [52,53]. The small levels of MPV could prove a useful variables in prediction models for DM2.
Furthermore, DM2 complications (micro- and macrovascular) are associated with elevated RDW and PLT/Ly ratios and thus, need precise glycemic control [46,49,54].
Other main hemorheological parameters (as WBV whole blood viscosity, ED – erythrocyte deformability, EA – erythrocyte aggregability, are also applied in the Clinical diabetology. The hemorheological disorders in DM2 patients increase simultaneously with unfavorable alterations in their glycemic/carbonhydrate metabolism and depend on the intensity of oxidative stress (micro-hemodynamic index OSI – oxidative stress intensity). Micro-hemodynamic indices as ERDI (relative deformability of erythrocyte membrane), WBV (whole blood viscosity), blood plasma viscosity (BPV), erythrocyte aggregation index (EAI) are discussed in relationship to prevention of cardiovascular risks and other vascular complications during DM2 [51,54,55].
Figure 1.
AFM Bruker images (3D topography), of the unfixed blood clot from DM2 patient. Erythrocytes / echinocytes (blue stars) fibrin fibers (blue triangles) , "activated" PLTs, (orange-brown stained; blue arrows) [9,56].
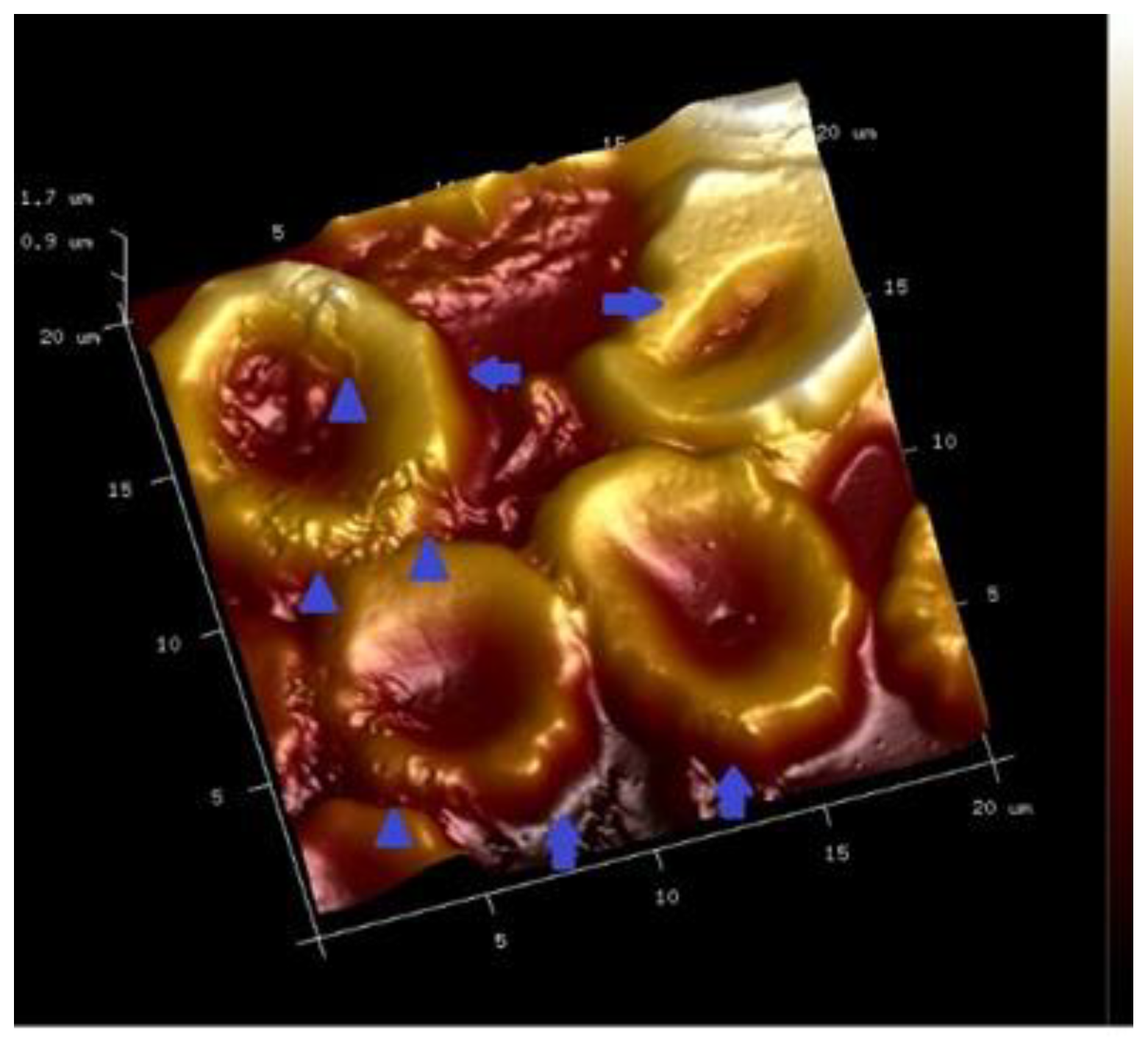
(Echinocytes - blue arrows; fibrin fibers - blue triangles)
Figure 2.
AFM Bruker image (3D topography), of the surface of clot from blood of healthy donor. Erythrocyte /discocyte - white star, platelets - white arrows and fibrin fibers (white triangles) [9,56].
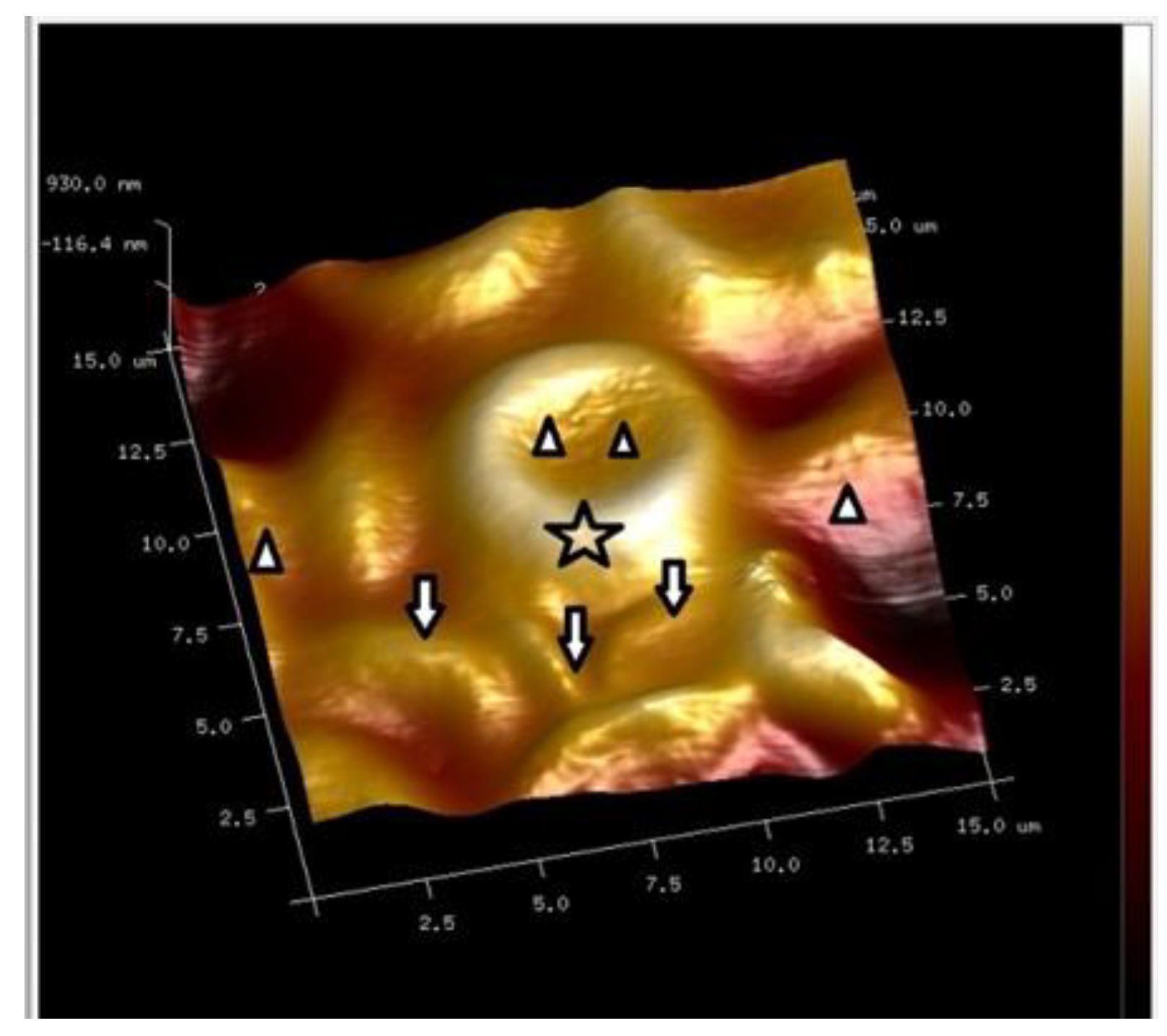
Figure 3.
AFM Bruker image (3D topogtaphy) of PLTs cluster, containing "activated" thrombocytes from the blood of DM2 patient. Abundant thick fibin fibers are organized in the fibrin network [9,56].
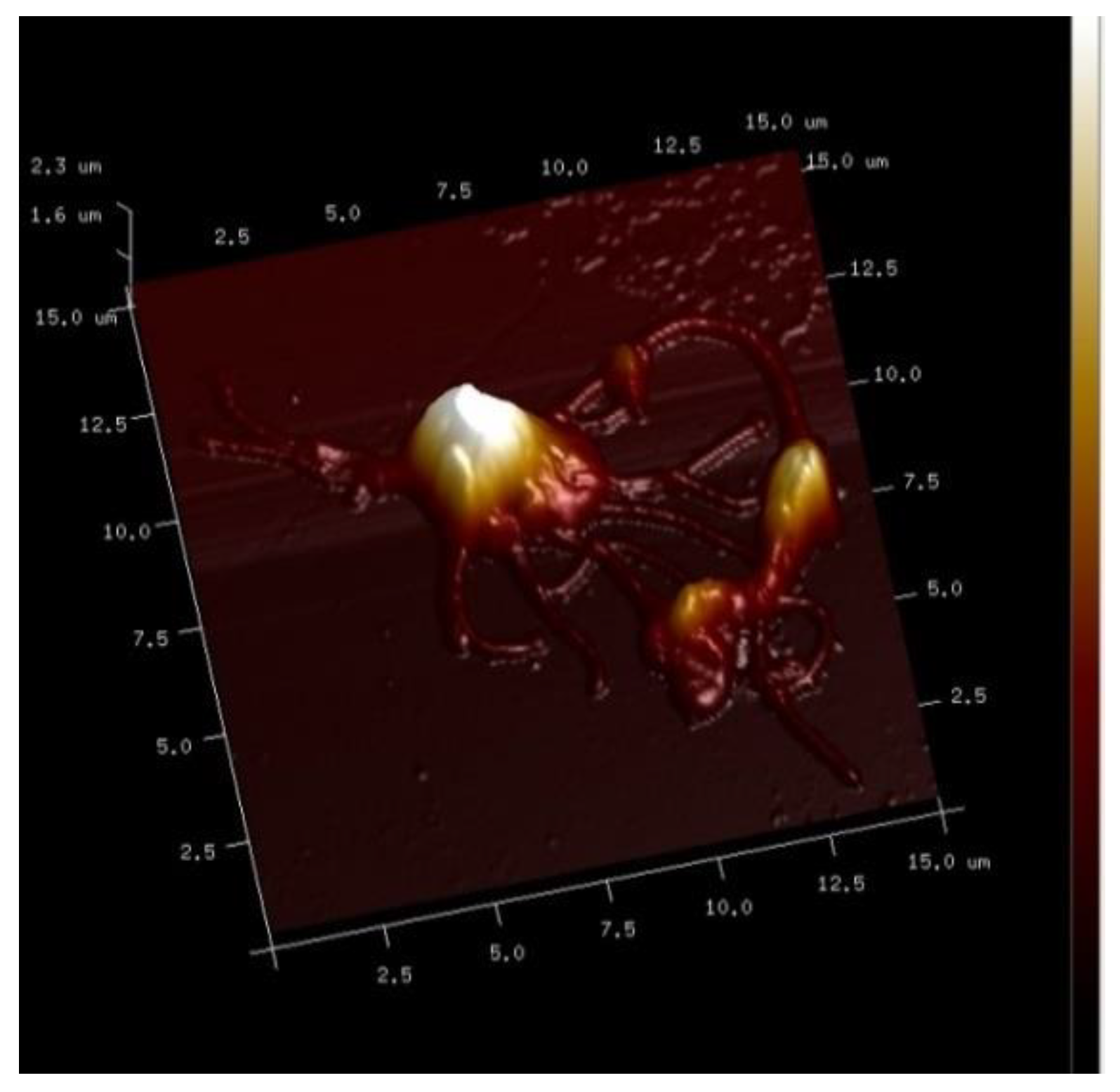
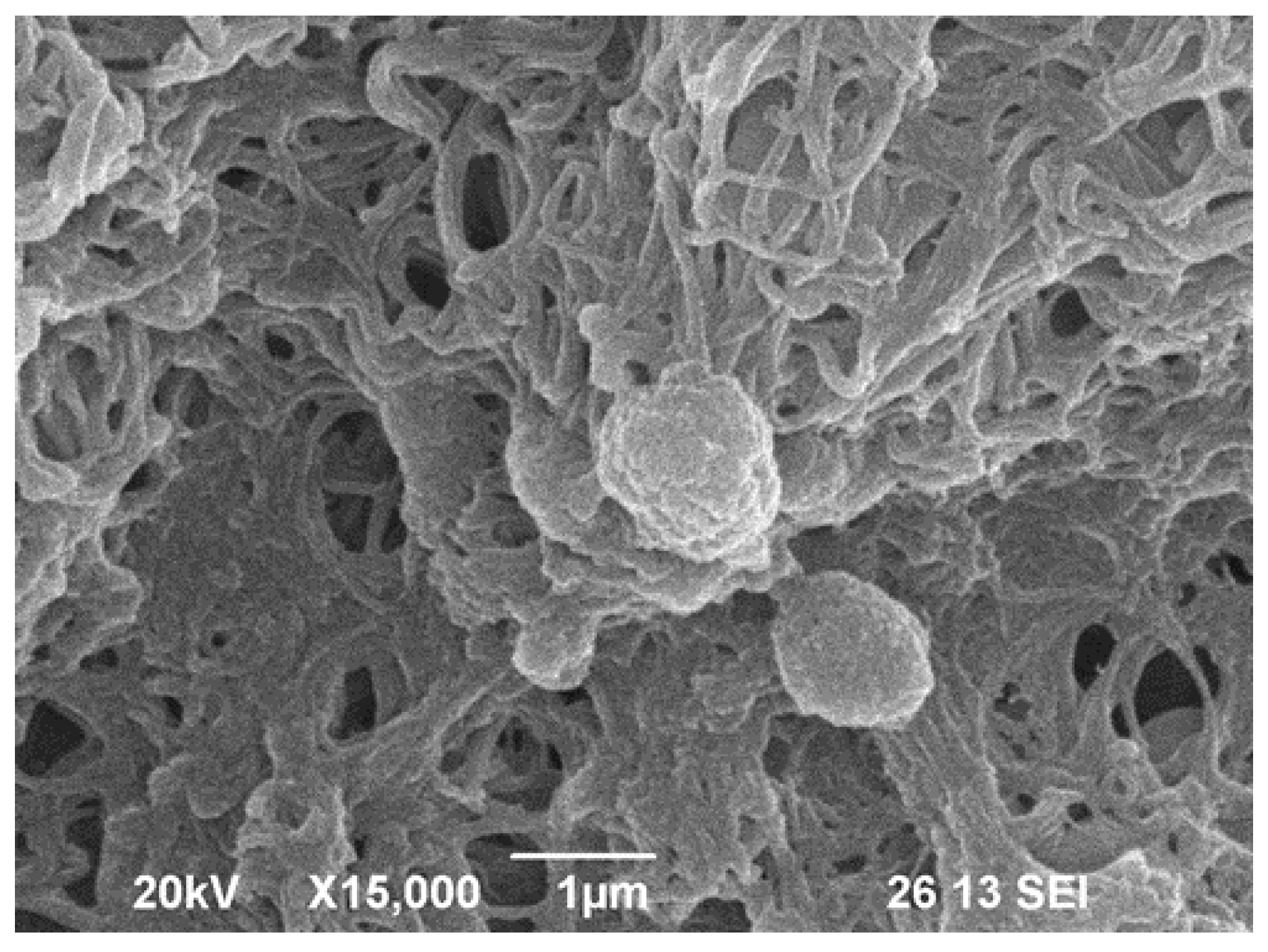
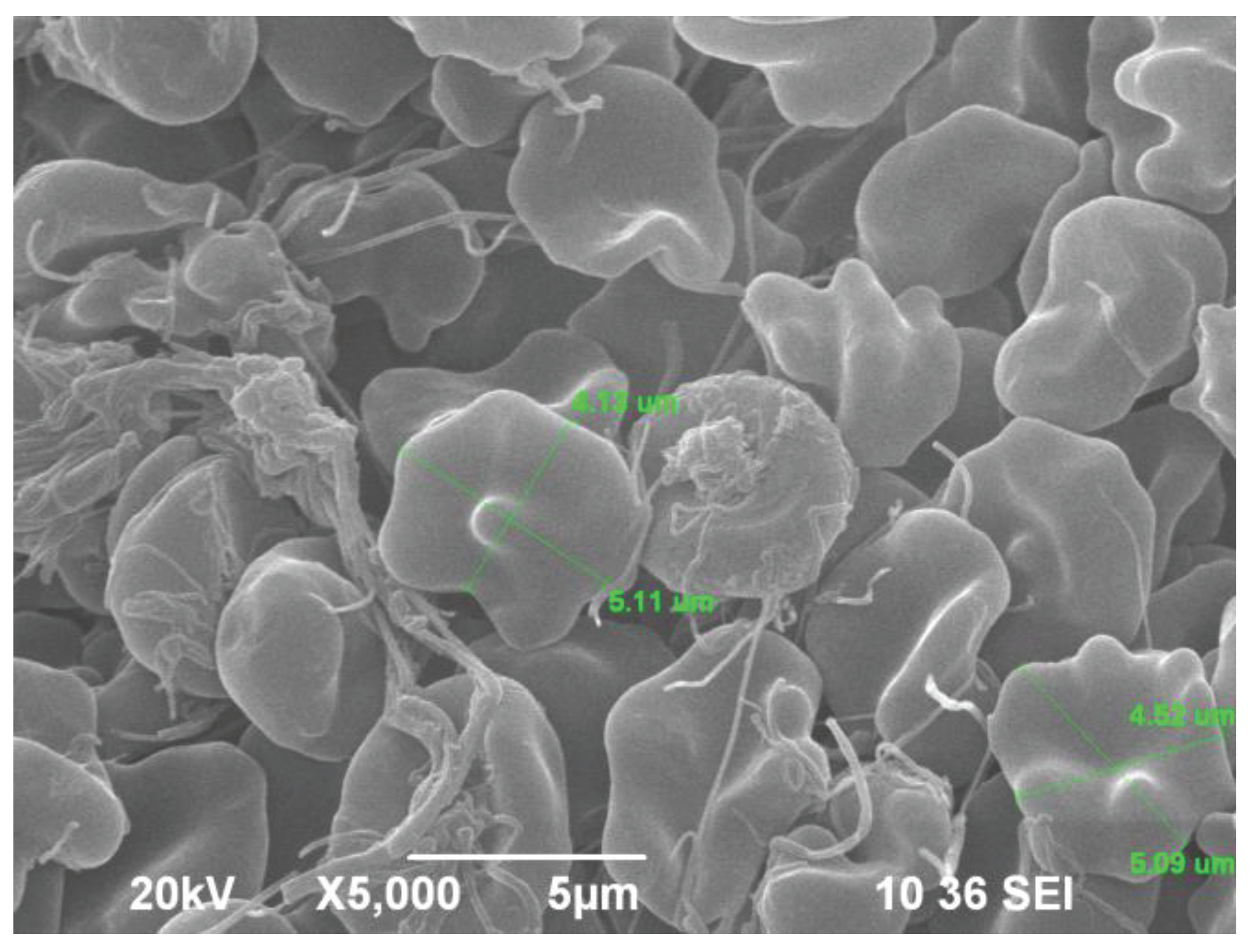
Figure 4.
SEM JSM 6390 image: "activated PLTs" on the fibrin network of a fixed blood clot from a patient with DM-2 ( at magnification x 10 000) [9,56].
8. PLT-Derived microRNAs Are Novel Biomarkers for Early Diagnosis and Prognosis of Type 2 Diabetes Mellitus
PLTs are mayor source of micro RNAs. The endothelial cells are also enriched for miR-126. PLT-derived microRNA=103b (miR=103b) plays a critical role in the regulation of glucose homeostatsis during DM2. The circulating miR=126 was investigated as a potential biomarker of DM2 [56,57,58,59,60].
Recent available data suggest that PLTs contain large amounts of miRNAs-circulating in body fluids. Regulating functions of multiple genes, miRNAs attract scientific interest as diagnostic and prognostic biomarkers of DM2. Today, miRNAs studies are closely associated with the micro- and macrovascular complications of DM2 [25,31,58,60].
Circulating miRNAs are potential biomarkers of DM2, predicting: special class of miRNAs molecules which were altered during T2DM development. These molecular modifications could be observed as potential biomarkers for the prediction, early diagnosis and prognosis of DM2 and related vascular complications. Thus, miRNAs have been discovered to be involved in the regulation of inflammation, insulin resistance and DM2 development (miRNAs changes in T2DM in animals and humans) [58]. E.g., miR126 can serve as a biomarker of micro- and macrovascular disease in DM2 [59]. In pathological condition (such as DM2 -associated with PLT activation), the administration of drugs (as aspirin), may lead to reduced levels of circulating miR126 [59,60].
Sixteen microRNAs met the criteria to identify and validate (of both – statistical and biological significance), as DM2 biomarkers [60]. Future microRNA expression profiling could report detailed data of the clinical utility of new 16 miRNAs.
Using the monitoring of DM2 specific microRNAs [61], would enable earlier predicting, diagnosis and treatment of DM2 as a biomarker of micro- and macrovascular desease in DM2 and its relating vascular complications.
9. Limitations
The studies in this field are limited because “the presence of miRNAs” reflects only the presence of PLT-derived, circulating microRNAs, but not in situ localized in the PLTs’ cytoplasms.
To reduce this limitation and to minimize problems related, we have proposed further visualization of miRNAs in “microclasmatoses/ microvesicles/ clasmatoses/ exosomes” and/or different granules in PLTs’ cytoplasms. For this purpose, we have applied our own staining method for visualization of RNPs (ribonucleoproteins) [23,61,62,63]. By this way, cytoplasmic granules, stained positively for RNP, were observed in our previous studies as good indicator of severity of neoplastic processes. During metastasis appearance, abundant empty vacuoles and lack of RNP-stained granules in PLTs, were visualized with the method of light microscopes [23,63,64].
The cytochemical method for staining of RNPs, applied on platelets of diabetic patients, could characterise PLT-proliferative state ("activation", "hyper-activation"). The management of DM2 is also limited because the cellular/molecular mechanisms of DM2- induced platelet hyper-responsiveness and these of anti-platelet drug resistance, were not clear and could be clarified in further investigations. E.g., the "hyper-activity" of PLT' P2Y12 receptors and its pathway play an important role in cellular mechanisms of PLT-"activation" [65]. In this case, the PLT "hyper- activity" and "high degree of aggregation" could be inhibited by opioid peptides. Some key signaling molecules, which correlate with opioid peptides, probably paticipate in the P2Y12 signaling pathways.
10. Conclusions
Sobol and Watala (2000) investigated the role of platelets (PLTs) in Diabetes mellitus - related to the micro- and macro-vascular DM2 complications. The analysis of results might be helpful in the new pharmacological strategies - to reduce the level of PLTs activation/hyper-activation, in DM-2 [66,67].
"Activated" and "hyper-activated" PLTs in DM2 undergo shape changes and morphological features as membrane blebbing, protrusions/pseudopodia, microvesicules, etc. [68]. The dynamic events in PLTs continue from an "activated" state during transformation in an "procoagulant phase", when PLTs of diabetic patients are involved in micro- and macrovascular complications of disease.
Scientific contributions, clinical trials and efforts create possibilities to improve anti-platelet drugs and to create new medicines, on the basis of successfull applications of combined hematological indices and hemorheological measurements/parameters: PLTs (count), MPV, PDW, PCR, PLT/Ly ratio, PLT-derived miRNAs, as biomarkers in DM2, etc.). Our view on following up the hematological, hemorheological and hemostatical indices, could create a new way in treatment and management of thrombotic micro- and macrovascular complcations of DM 2.
Diabetes mellitus (DM2) is a hypercoagulable state with enhanced PLTs' activation and increased clotting factors' production: prothrombin, thrombin, fibrinogen, factors VII, VIII, Xi, XII, von Willebrand factor, etc. [67,68,69]. Simultaneously , the fibrinolytic cell system is inhibited due to formaion of clots with high resistance to fibrinolysis. Anti-platelet agents (including natural - plant products), could been effective in prevention and secondary treatment of micro- and macrovascular complications in DM2 [4,24,68,70,71,72,73,74].
Acknowledgment
This work has been supported by the Basic Research Project – 2021 КП-06-Н57/14, funded by the Bulgarian National Science Fund.
References
- Windberger, U.; Dibiasi, C.; Lotz, E.; Scharbert, G.; Reinbacher-Koestinger, A.; Ivanov, I.; Ploszczanski, L.; Antonova, N.; Lichtenegger, H. The effect of hematocrit, fibrinogen concentration and temperature on the kinetics of clot formation of whole blood. Clinical Hemorheology and Microcirculation 2020, 75, 431–445. [Google Scholar] [CrossRef] [PubMed]
- Reinhart, W.H. Platelets in vascular disease. Clinical Hemorheology and Microcirculation 2013, 53, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Battinelli, E.M.; Markens, B.A.; Italiano, J.E., Jr. Release of angiogenesis regulatory proteins from platelet alpha granules: modulation of physiologic and pathologic angiogenesis. Blood, The Journal of the American Society of Hematology 2011, 118, 1359–1369. [Google Scholar] [CrossRef]
- Zvetkova, E.; Antonova, N.; Ivanov, I.; Savov, Y.; Gluhcheva, Y. Platelet morphological, functional and rheological properties attributable to addictions. Clinical hemorheology and microcirculation 2010, 45, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Munnix, I.C.; Cosemans, J.M.; Auger, J.M.; Heemskerk, J.W. Platelet response heterogeneity in thrombus formation. Thromb. Haemost. 2009, 102, 1149–1156. [Google Scholar] [PubMed]
- Petrochenko, E.P.; Tikhomirova, I.A.; Ryabov, M.M.; Kislov, N.V.; Petrochenko, A.S. Platelet hemostasis in patients with non-myeloid cancer. Series on Biomechanics 2015, 29. [Google Scholar]
- Nomura, S. Function and clinical significance of platelet-derived microparticles. Int. J. Hematol. 2001, 74, 397–404. [Google Scholar] [CrossRef] [PubMed]
- George, J.N.; Thoi, L.L.; McManus, L.M.; et al. , Isolation of human platelet membrane microparticles from plasma and serum. Blood 1982, 60, 834–840. [Google Scholar] [CrossRef]
- Alexandrova, A.; Antonova, N.; Kyulavska, M.; Velcheva, I.; Ivanov, I.; Zvetkova, E. Hemorheological and atomic force microscopy studies on the experimental clot formation in patients with type 2 diabetes mellitus. Series on Biomechanics 2018, 32, 63–73. [Google Scholar]
- Pretorius, E.; Bester, J.; Vermeulen, N.; Alummoottil, S.; Soma, P.; Buys, A.V.; Kell, D.B. Poorly controlled type 2 diabetes is accompanied by significant morphological and ultrastructural changes in both erythrocytes and in thrombin-generated fibrin: implications for diagnostics. Cardiovascular diabetology 2015, 14, 1–20. [Google Scholar] [CrossRef]
- Andreeva, T.; Komsa-Penkova, R.; Langari, A. Morphometric and nanomechanical features of platelets from women with early pregnancy loss provide new evidence of the impact of inherited thrombophilia. Int. J. Mol. Sci. 2021, 22, 7778. [Google Scholar] [CrossRef]
- Yuan, H.; Liu, Y.; Zhang, J.; Dong, J.F.; Zhao, Z. Transcription factors in megakaryocytes and platelets. Frontiers in Immunology 2023, 14, 1140501. [Google Scholar] [CrossRef] [PubMed]
- El Haouari, M.; Rosado, J.A. Platelet signalling abnormalities in patients with type 2 diabetes mellitus: A review. Blood Cells, Molecules, and Diseases 2008, 41, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Kubisz, P.; Stančiaková; L; Staško, J. ; Galajda, P.; Mokáň; M Endothelial and platelet markers in diabetes mellitus type 2. World Journal of Diabetes 2015, 6, 423. [Google Scholar] [CrossRef] [PubMed]
- Swathi, M.; Ramya, T.; Gangaram, U.; Kumar, K.K.; Sandeep, B. A study of neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) with glycosylated hemoglobin (HBA1C) among type 2 diabetic patients. Int.J. Acad. Med. Pharm. 2023, 5, 1533–1537. [Google Scholar]
- Xu, F.; et al. Mean platelet volume (MPV) new diagnostic indices for co-morbidity of tuberculosis and diabetis mellitus. BMC Infectious Diseases, 2021, 21, article number :461 https// doi.org/10.1186/s12879–021. [Google Scholar] [CrossRef]
- Pujani, M.; Gahlawat, H.; Agarwal, C.; Chauhan, V.; Singh, K.; Lukhmana, S. Platelet parameters: Can they serve as biomarkers of glycemic control or development of complications in evaluation of type 2 diabetes mellitus. Iraqi J Hematol 2018, 7, 72–78. [Google Scholar]
- Alhadas, K.R.; Santos, S.N.; Freitas, M.M.S. Are platelet indices useful in the evaluation of type2 diabetic patients? J.Bras.Pathol.Med.Lab. 52/2, 2016. [CrossRef]
- Joshi, A.A.; Jaison, J. The study of platelet parameters - mean platelet volume (MPV) and platelet distribution width (PDW) in type 2 Diabetes mellitus. Lab Med 8/6, 2019. [CrossRef]
- Olana; Seifu; Menon; M. K. C.; Natesan Abnormal hematological indices and anthropometric parameters associated with type 2 Diabetes. Int J Biomed Adv Res 2019, 10, 1–8.
- Shilpi, K.; Potekar, R.M. A study of platelet indices in Type 2 diabetes mellitus patients. Indian J Hematol Blood Transfus 2018, 34, 115–120. [Google Scholar] [CrossRef]
- Orum, M.H.; Kara, M.Z.; Egilmez, O.B.; Kalenderoglu, A. Complete bood count alterations due to the opioid use: what about the lymphocyte-related ratios, especially in monocytе to lymphocyte ratio аnd platelet to lymphocyte ratio? Journsl of Immunoassay, and Immunochemistry, 2018. [CrossRef]
- Zvetkova, E.; Kostov, G. Extracellular RNA Biomarkers: New Development of Old Conception. Clinical Immunology 2010, S81. [Google Scholar] [CrossRef]
- Zhou, X.; Zhou, X.; Zhu, R.; Ming, Z.; Cheng, Z.; Hu, Y. The mechanism of oleic acid inhibiting platelet activation stimulated by collagen. Cell Communication and Signaling 2023, 21, 278. [Google Scholar] [CrossRef]
- Ji, S. , Zhang, J., Fan, X., Wang, X., Ning, X., Zhang, B.,... & Yan, H. The relationship between mean platelet volume and diabetic retinopathy: a systematic review and meta-analysis. Diabetology & metabolic syndrome 2019, 11, 1–8. [Google Scholar]
- Milosevic, D.; Panin, V.L. Relationship between hematological parameters and glycemic control in type 2 Diabetes mellitus patients. J. Med.Biochem. 2019, 38. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, A.; Amitkumar, K.; Ganapathy, S.; Ayyavoo, S. Evaluation of mean platelet volume and other platelet parameters in subjects with Type-2 diabetes mellitus. National Journal of Physiology Pharmacy and Pharmacology 2017, 7, 51. [Google Scholar] [CrossRef]
- Zvetkova, E.; Fuchs, D. Medical significance of simultaneous application of red blood cell distribution width (RDW) and neopterin as diagnostic/prognostic biomarkers in clinical practice. Pteridines 2017, 28, 133–140. [Google Scholar] [CrossRef]
- E. Zvetkova, Y. Savov, Y. Gluhcheva, I. Ilieva, E. Bichkidjieva, Simultaneous anisocytosis of red blood cells and platelets in chronic heroin addicts, Bloodmed – Slide Atlas, Red cells – Acquired disorders (2006), Blackwell publishing, Oxford, UK (https://www.bloodmed.com/home/slide-atlas).
- Nada, A. M. Red cell distribution width in type 2 diabetic patients. Diabetes, metabolic syndrome and obesity: targets and therapy, Vol. 8 2015, 525-533. [CrossRef]
- Antonova, N.; Veltcheva, L.; Paskova, V. Hemorheological and microvascular disturbances in patients with type 2 diabetes mellitus. Clinical Hemorheology and Microcirculation 2022, 81, 325–341. [Google Scholar] [CrossRef]
- Deng, Y.X.; Chang, H.-Y.; Li, H. Recent Advances in Computational Modeling of Biomechanics and Biorheology of Red Blood Cells in Diabetes. Biomimetics 2022, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Bouchnita, A.; Volpert, V. A multiscale model of platelet-fibrin thrombus growth in the flow. Comput. Fluids 2019, 184, 10–20. [Google Scholar] [CrossRef]
- Zhang, P.; Zhang, N.; Deng, Y.; Bluestein, D. A multiple time stepping algorithm for efficient multiscale modeling of platelets flowing in blood plasma. J. Comput. Phys. 2015, 284, 668–686. [Google Scholar] [CrossRef]
- Li, H.; Sampani, K.; Zheng, X.; Papageorgiou, D.P.; Yazdani, A.; Bernabeu, M.O.; Karniadakis, G.E.; Sun, J.K. Predictive modeling of thrombus formation in diabetic retinal microaneurysms. R. Soc. Open Sci. 2020, 7, 201102. [Google Scholar] [CrossRef]
- Chang, H.Y.; Yazdani, A.; Li, X.; Douglas, K.A.; Mantzoros, C.S.; Karniadakis, G.E. Quantifying platelet margination in diabetic blood flow. Biophys. J. 2018, 115, 1371–1382. [Google Scholar] [CrossRef]
- Lu, Y.; Lee, M.Y.; Zhu, S.; Sinno, T.; Diamond, S.L. Multiscale simulation of thrombus growth and vessel occlusion triggered by collagen/tissue factor using a data-driven model of combinatorial platelet signalling. Math. Med. Biol. A J. IMA 2017, 34, 523–546. [Google Scholar] [CrossRef]
- Yazdani, A.; Karniadakis, G.E. Sub-cellular modeling of platelet transport in blood flow through microchannels with constriction. Soft Matter 2016, 12, 4339–4351. [Google Scholar] [CrossRef] [PubMed]
- Anand, M.; Rajagopal, K.; Rajagopal, K. A model for the formation, growth, and lysis of clots in quiescent plasma. A comparison between the effects of antithrombin III deficiency and protein C deficiency. J. Theor. Biol. 2008, 253, 725–738. [Google Scholar] [CrossRef]
- Cai, S.; Li, H.; Zheng, F.; Kong, F.; Dao, M.; Karniadakis, G.E.; Suresh, S. Artificial intelligence velocimetry and microaneurysmona- chip for three-dimensional analysis of blood flow in physiology and disease. Proc. Natl. Acad. Sci. USA 2021, 118, e2100697118. [Google Scholar] [CrossRef]
- Tosenberger, A.; Ataullakhanov, F.; Bessonov, N.; Panteleev, M.; Tokarev, A.; Volpert, V. Modelling of platelet–fibrin clot formation in flow with a DPD–PDE method. Leiderman, K.; Fogelson, A. An overview of mathematical modeling of thrombus formation under flow. Thromb. Res. 2014, 133, S12–S14. [Google Scholar]
- WM Heemskerk, Pia RM Siljander, Edouard M. Bevers, Richard W. Farndale, Theo Lindhout, J. Receptors and signalling mechanisms in the procoagulant response of platelets. Platelets 2000, 11, 301–306. [Google Scholar] [CrossRef]
- Cakir, E.; Özkoçak Turan, I. PREDICTIVE EFFECTS OF FIRST ERYTHROCYTE AND THROMBOCYTE VOLUME INDICES ON MORTALITY OF GERIATRIC PATIENTS WITH SEPSIS HOSPITALIZED IN INTENSIVE CARE UNITS. Turkish Journal of Geriatrics/Türk Geriatri Dergisi 2021, 24. [Google Scholar]
- Ulutas, K.T.; Dokuilku, R.F. Sefil, Evaluation of mean platelet volume in patients with type-2 diabetes mellitus and blood glucose regulation: а marker for atherosclerosis? Int J Clin Exp Med 2014, 7, 955–961. [Google Scholar] [PubMed]
- Aktas, F.; Aktuglu, M.B. Evaluation of the relation between HbA1c and MPV and PDW levels of patients with Type 2 Diabetes admitted in Internal Medicine Polyclinics. North Clin.Istanb. 2023, 10, 681–686. [Google Scholar] [CrossRef]
- Elsayed, A.M.; Araby, E. Neutrophil-Lymphocyte and Platelet-Lymphocyte ratious as a marker for diabetes control and complications. Benha Medical Journsl 2021, 38, 984–995. [Google Scholar]
- Hajek, A.S.; Joist, J.H.; Baker, R.K.; Jarett, L.E.O.N.A.R.D.; Daughaday, W.H. Demonstration and partial characterization of insulin receptors in human platelets. The Journal of Clinical Investigation 1979, 63, 1060–1065. [Google Scholar] [CrossRef]
- Kelem, S.; Adane, T.; Shiferaw, E. Insulin resistance-induced platelet hyperactivity and a potential biomarker role of platelet parameters, A narrave Review. Diabetes, Metabolic Sydrome and Obesity 2023, 16, 2843–3853. [Google Scholar] [CrossRef]
- Ahmed, S.; Khalid, M.A.; Munir, M.; et al. Association of Neutrophil to Lymphocyte and Platelet to Lymphocyte ratio with glucose regulation in type 2 diabetes patients. Journal of Rawalpindi (JRMC - internet) 2021. [Google Scholar] [CrossRef]
- Sobczak A.I.S., and S.J. Stewart. Coagulatory defects in type-1 and type-2 Diabetes. Int. J. Mol. Sci., 20, 2019, 6345. [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; et al. Heart disease and stroke statistics 2018. Update: a report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar]
- Rodriguez B.A. T., and A.D. Johnson. Platelet measurements and type 2 Diabetes: Investigations in two population-based Cohorts. Front. Cardiovasc. Med., 7, 2020, Article 118. [CrossRef]
- Dolasik I., et al., The effect of metformin on mean platelet volume in diabetic patients. Platelets, 24, 2013, 118 – 121. [CrossRef]
- Magri, C.J.; Xuereb, S.; Huereb, R.A. Sleep measures and cardiovascular disease in type 2 diabetes mellitus. Clinical Medicine 2023, 23, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chkhitauri L., Sanikidze T., Giorgadze, M. Mantskava ..et al., Comprehensive study of the rheological status and intensity of oxidative stress during the progression of type 2 Diabetes mellitus to prevent its complications. Clinical Hemorheology and Microcirculaton 83/1, 20, pp 69 – 79. [CrossRef]
- Alexandrova-Watanabe, A., 2021. Study of rheological, mechanical and morphological properties of blood, its formal elements and parameters of hemocoagulation in type 2 diabetes mellitus. PhD thesis, Institute of Mechanics, Bulgarian Academy of Sciences, Sofia, Bulgaria.
- Liu, Y.; Gao, G.; Yang, C.; Zhou, K.; Shen, B.; Liang, H.; Jiang, X. The role of circulating microRNA-126 (miR-126): a novel biomarker for screening prediabetes and newly diagnosed type 2 diabetes mellitus. International journal of molecular sciences 2014, 15, 10567–10577. [Google Scholar] [CrossRef] [PubMed]
- Afsharmanesh, M.R.; Mohammadi, Z.; Mansourian, A.R.; Jafari, S.M. A Review of micro RNAs changes in T2DM in animals and humans. Journal of Diabetes 2023. [CrossRef] [PubMed]
- de Boer, H.C.; van Solingen, C.; Prins, J.; Duijs, J.M.; Huisman, M.V.; Rabelink, T.J.; van Zonneveld, A.J. Aspirin treatment hampers the use of plasma microRNA-126 as a biomarker for the progression of vascular disease. European heart journal 2013, 34, 3451–3457. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Leung, S.W. MicroRNA biomarkers of type 2 diabetes: Evidence synthesis from meta-analyses and pathway modelling. Diabetologia 2023, 66, 288–299. [Google Scholar] [CrossRef] [PubMed]
- Shantikumar, S.; Caporali, A.; Emanueli, C. Role of microRNAs in diabetes and its cardiovascular complications. Cardiovascular research 2012, 93, 583–593. [Google Scholar] [CrossRef]
- Zvetkova, E.B.; Zvetkov, I.B. A cytological method for the simultaneous staining of nucleoproteids and some cathionic proteins. Acta Histochemica 1976, 57, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Zvetkova, E.; Kostov, G. Microdensitometrical studies on tumour-induced programmed cell death of peripheral blood tumour-infiltrating lymphocytes (TIL) in cancer patients: possible applications for early tumour diagnosis. Асta Morphologica et Anthropologica 2000, 5, 3–10. [Google Scholar]
- Zvetkova, E.B.; Kostov, G.S.; Gluhcheva, Y.G. 30 Years from Creation of the First Cytochemical Method Analysing RNP, DNP and Cationic Proteins in Circulating Leukocytes of Cancer Patients as a Tool for Early Diagnostics of Malignancies. Clinical Immunology 2007, S111. [Google Scholar] [CrossRef]
- Zhang, Q.; Han, Y. Opioid peptides and P2Y12 receptor signling pathway. Progress in Modern Biomedicine 2011, 11, 3787–3790. [Google Scholar]
- Sobol, A.B.; Watala, C. The role of platelets in diabetes-related vascular complications. Diabetes Res. Clin. Ptact. 2000, 50, 1–16. [Google Scholar] [CrossRef]
- Ashby, B.; et al. Mechanisms of platelet activation and inhibition. Hematology/Oncology. Clinica of North America 1990, 4, 1–26. [Google Scholar] [CrossRef]
- Vinik, A.I.; Erbas, T.; Park, T.S. Nolan R., Piterenger G.L. Platelet dysfunction in type-2-Diabetes. Diabetes Care 2001, 24, 1476–1485. [Google Scholar] [CrossRef]
- Carr, M.E. Diabetes mellitus: A hypercoagulable state. Journal of Diabetes and its complications. 2001, 15, 44–54. [Google Scholar] [CrossRef]
- Vinik, A.; Flemmer, M. Diabetes and macrovascular disease. Journal of Diabetes and its complications 2002, 16, 235–246. [Google Scholar] [CrossRef]
- Vinik, A.; Vinik, E. Prevention of the complications of Diabetes. Am. J. Managed Care 2003, 9, S–63. [Google Scholar]
- Hirsch, G.E.; et al. Natural products with antiplatelet action. Curr Pharm Des., 23/8, 2017, 1228 – 1246. [CrossRef]
- K.J. Mhatre, J.R. Patil, G.C. Nikalje. Role of Flavonoids in vasodilation. In the Book: The flavonoids. First edition, 2024, Apple Academic Press, pp. 17, Taylor Frances Group.
- J.E. Freedman, C.Parker lll, L.Li, J.A.Perlman, B. Frei, et al. Select flavonoids and whole juice from purple grapes inhibit platelet function and enhance nitric oxide release. Circulation ( Am. Heart Assoc.), 103, 2001 (12 June), 2792 – 2798. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



