
Submitted:
19 March 2024
Posted:
20 March 2024
You are already at the latest version
Abstract
Background: Orthostatic hypotension (OH) is associated with higher risk of mortality in general population however not studied in cancer population. The study aimed to assess the prevalence of OH in cancer patients compared to the non-cancer population. Methods: A total of 411 patients (mean age 63.5 ± 10.6 years) were recruited: patients with active cancer (n = 223) and patients hospitalized for other reasons but without cancer diagnosis (n = 188). Medical history was collected and an orthostatic challenge test was performed. OH was defined as blood pressure (BP) decrease on standing ≥ 20 mmHg for systolic or ≥ 10 mmHg for diastolic BP in 1 or 3 minutes; or systolic BP decrease < 90 mmHg. Results: The prevalence of OH in cancer was significantly higher than in subjects without cancer- 28.7% vs. 16.5%, respectively, P = 0.003). OH was the most common in lung cancer, 57.5%. In single variable analysis, the predictors of OH were: cancer presence, age ≥ 65 years, and body mass index (BMI) ≥ 30 kg/m2. In the multivariable model, the strongest independent predictor of OH was cancer status doubling the risk of OH; BMI ≥ 30 kg/m2 and diabetes. Conclusions: Cancer patients are characterized by a high prevalence of OH. In this population, the recommendation of routine orthostatic challenge tests should be considered.
Keywords:
blood pressure
; cancer
; orthostatic hypotension
1. Introduction
Orthostatic hypotension (OH) is the result of the inability of the autonomic nervous system to control postural hemodynamic homeostasis caused by cardiovascular autonomic dysfunction [1,2]. Cardiovascular autonomic dysfunction is one of the most poorly understood complications associated with cancer patients [3,4]. Several mechanisms have been proposed as explanations for the cause including OH, changes in heart rate (HR) frequency and loss of blood pressure (BP) and HR circadian variability [5,6].
Patients with chronic diseases such as hypertension, heart failure, diabetes, kidney dysfunction, autoimmune disorders and at older age suffer from OH more frequently [7]. On the other hand, little is known about the prevalence of OH in cancer patients, although they are particularly susceptible and prone to dysregulation of BP [8,9]. On this background, we decided to conduct this study to investigate the prevalence of OH in hospitalised active cancer patients compared to patients without cancer.
2. Materials and Methods
Patients at age ≥ 40 years who were hospitalized in 2 centers: Subcarpathian Oncological Center of the University Clinical Hospital in Rzeszow and in the New Medical Techniques Specialist Hospital of the Holy Family in Rzeszow were recruited for the study (Table 1).
The study groups included patients with actively treated cancer by chemotherapy and/or radiation therapy (Table 1) and the non-oncological group, which were patients hospitalized for other reasons, but without cancer diagnosis. Measurements for OH in the oncology group were taken 3 weeks after the administration of chemotherapy or the use of radiation therapy, or in patients with newly diagnosed cancer even before oncological treatment was implemented. Patients with significant anemia requiring blood transfusion, diarrhea, after recent surgical procedures or with acute life-threatening conditions were excluded. The analysis was subjected to the type of cancer, the severity of cancer disease, the presence of brain metastases, along with concurrent diseases and medications, including especially those that may cause OH such as alfa- and beta-blockers, nitrates, diuretics, calcium channel blockers, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and antiparkinsonian agents.
The data collected included demographic and medical history data, as well as measurements of sitting, supine, and standing BP on the orthostatic challenge test. BP measurements were performed according to the most recent standards of Polish Hypertension Society [10] with validated automatic upper arm device (Omron M3 Comfort, Omron Healthcare Co, Japan). OH was defined according to the criteria shown in Figure 1.
BP and HR were measured in the following order in each patient qualified for the project: three BP and HR measurements at intervals of 1-2 minutes in a sitting position, followed by a 5-minute rest period; a double BP and HR measurement in the supine position after lying down for 5 minutes; a single BP and HR measurement 1 and 3 minutes after standing upright. For analysis, we calculated the mean of the last two measurements in a sitting position and the mean of double measurements while sitting. During active standing, the following grades of accompanying symptoms were recorded: grade I: no dizziness, grade II: dizziness, grade III: syncope, and grade IV: prolonged disturbance of consciousness.
The study was approved by a local Bioethics Committee no. 89/2022/B and the patients gave their written informed consent to participate in the study.
Statistical Analysis
For comparing two groups with respect to continuous variables, we used Student t test with separate variance estimators and Mann-Whitney nonparametric test. For qualitative variables, the chi-square test for independence has been used, with test statistic calculated by the maximum likelihood approach. Risk factors analysis was done by logistic regression. Multivariable model has been obtained by backword step-wise approach. For all analyses, the significance level α has been set at 0.05. All calculations and graphs were prepared in STATISTICA 13 software.
3. Results
The current study included in total 411 patients (229 women and 182 men, mean age 63.5 ± 10.6 years). The distribution of patients in hospital departments is presented in Table 1. The cancer group consisted of 223 patients and a non-oncological group of 188 subjects. Data on the baseline demographic profile and clinical characteristics of enrolled patients are presented in Table 2.
In patients with active cancer, 64 patients had OH (28.7%), while in patients without cancer diagnosis, the frequency of OH was significantly lower- 31 patients (16.5%)- P = 0.003. Cancer patients were statistically older, had a lower body mass index (BMI), a lower baseline HR, less frequent dyslipidaemia, and diabetes (Table 2). No statistically significant differences were observed with respect to sex, baseline systolic and diastolic BP values, the presence of other accompanying diseases, including hypertension, and drugs that can cause OH.
In single variable analysis the predictors of OH were: the presence of cancer, age ≥ 65 years, and BMI ≥ 30 kg/m2 which showed negative correlation (Table 3). In multivariable model the strongest independent predictor of OH was cancer status- the patients with cancer were twice more prone for OH than non-oncological patients (Table 3). The remaining independent predictors for OH in multivariable analysis were BMI ≥ 30 kg/m2 (negative correlation) and diabetes, while older age lost statistical significance. No significant differences were observed with respect to the sex of the patients, the presence of hypertension, and stroke.
The difference between the values of systolic BP, diastolic BP and HR in supine and during 1 and 3 minutes of active tilting was calculated. Delta BP was defined as the difference in BP in upright position and BP in supine calculated separately for systolic and diastolic BP. Delta HR was defined as the difference in HR in upright position and HR in supine. Figure 2 presents different patterns of BP behaviour during the orthostatic challenge test – systolic BP was decreasing, while diastolic BP was increasing. Some differences were noted with respect to cancer status. The delta for systolic BP both in 1 and 3 minutes of standing was greater in cancer patients compared to noncancer subjects (P = 0.02 and P = 0.04 respectively). The greatest fall in systolic BP was observed in 1 minute of tilt. Diastolic BP showed different pattern- it increased on standing more in non-cancer patients, with significant difference between studied groups in 3 minute (Figure 2). HR increased in both groups during tilt, in 1 minute of standing it was greater in cancer than noncancer subjects.
In the analysis of different types of cancer, we noticed that OH was most common in patients with lung cancer (n = 23/40; 57.5%), breast cancer (n = 6/16; 37.5%), male genitourinary cancers (n = 7/21; 33.3%), head and neck cancers (n = 8/26; 30.8%). OH was less prevalent in gastrointestinal cancers (n = 10/52; 19.2%) and gynecological cancers (n = 10/60; 16.7%)- Figure 3. OH was significantly more frequent in lung cancer compared to other groups of malignancies except breast cancer. OH did not depend on the stage of cancer progression (stage I-III versus stage IV, P = 0.19) and the presence of brain metastases (P = 0.52).
4. Discussion
Our study for the first time shows that the presence of cancer is a significant and independent predictor of OH. Cancer presence doubles the risk of OH compared to the noncancer population. In multivariable analysis the cancer status was more powerful risk factor for OH than older age, BMI and the presence of diabetes- widely known risk factors for OH.
OH may occur in cancer patients due to cancer itself (tumour mass effect, secretory cancer activity, pro-inflammatory microenvironment), as a consequence of various oncologic therapies (chemotherapy, radiotherapy, surgery, analgesics) or due to the negative side effects of systemic treatment that lead to dehydration and favour low BP. On the other hand, cancer patients that are usually older and share typical cardiovascular risk factors with cardiac patients (i.e., lung cancer) may suffer from multiple age-related disorders like diabetes, hypertension, chronic kidney disease, which along with some drugs may further increase the risk of OH. In Figure 4 we proposed several mechanisms as explanations for the increased prevalence of OH in cancer patients.
Most of the available data on OH in cancer patients are only case reports [11,12,13,14,15]. Head and neck cancer patients undergoing radiation therapy have been shown to experience OH due to baroreflex insufficiency many years after treatment [16,17]. In ovarian cancer, chemotherapy with paclitaxel and carboplatin has been shown to negatively affect cardiac sympathetic and parasympathetic nerves, which was associated with an increased risk of OH [18]. In turn, it was observed that the combination of vinorelbine and cisplatin caused OH in some patients with metastatic breast cancer previously treated with anthracyclines and docetaxel [19]. In another study, it was discovered that patients with haematopoietic malignancies who undergo autologous stem cell transplantation or haematopoietic stem cell transplantation develop OH and often require treatment to control OH symptoms [20,21,22]. According to a prospective single-centre study conducted by Eriksen et al., orthostatic intolerance was a common problem in patients undergoing laparoscopic resection of colorectal cancer and was associated with delayed recovery [23]. Furthermore, OH has also been reported in patients with lung cancer after anatomical lung resections with thoracotomy, as well as lobectomy and segmentectomy assisted by thoracoscopy [24,25].
As information on the prevalence of OH in cancer patients is scarce, we decided to conduct this study to confirm for the first time that OH occurs more often in the oncologic population compared to subjects without cancer. Another interesting finding of our study was the surprising high prevalence of OH in patients with lung cancer. In our opinion, lung cancer patients are at an exceptional risk of cardiovascular autonomic dysfunction and related OH. Among possible causes of high prevalence of OH in this group of patients are: combination of various oncological treatment strategies (chemotherapy, radiation therapy, and surgery), frequently advanced stage of disease, presence of paraneoplastic syndromes, weight loss, and frequently overlapping cardiovascular diseases [3,26,27].
OH has been widely studied and several associations with adverse events have been reported; therefore, it has been an established marker of a worse prognosis. The frequency of OH in the general population ranges from 5% in patients < 50 years of age to 30% in those over 70 years of age [28], which is consistent with the results of our study – the prevalence of OH in noncancer patients over 40 years was approximately 17%. According to numerous clinical studies, OH is associated with adverse cardiovascular outcomes such as coronary artery disease, heart failure, atrial fibrillation, stroke, chronic kidney disease, and venous thromboembolism. The presence of OH is considered an independent predictor of all-cause mortality and non-cardiac mortality in large studies, therefore, its increased prevalence in cancer patients is of high clinical importance and requires particular attention [29].
During the orthostatic challenge test, the physiological transition from supine to upright position is accompanied by a transient reduction in venous return with the pooling of intravascular blood volume in the lower extremities due to gravity. This leads to a decrease in transient stroke volume and consequently also a decrease in BP. In the normal scenario, the reflexes generated by the carotid sinus and aortic arch baroreceptors stimulate the sympathetic system and diminish the activity of the parasympathetic system. Due to increased HR, cardiac contractility and vascular tone, normal BP levels are restored [1]. In case of dysregulation of any phase of these mechanisms, excessive BP fall may occur, leading to OH.
Age is a significant risk factor for OH, and the incidence of OH is about 20% among people over 65 years [30]. The importance of age as a significant predictor of OH was also confirmed in our study. From this perspective, OH is a clinically relevant disorder, particularly for elderly patients who are more likely to fall, develop cardiovascular diseases or cancer [31] increasing as well significantly risk of mortality from any cause [32,33,34].
Treatment-related OH has been observed with many drugs that affect the cardiovascular system and the central nervous system. Among these drugs are alpha- and beta-blockers, nitrates, diuretics, calcium channel blockers, angiotensin-converting-enzyme inhibitors, and angiotensin II receptor blockers, benzodiazepines, antipsychotics, opioids, etc [35]. In our study, we did not observe significant differences between the frequency of these drugs between cancer and noncancer patients, and they were not significant predictors of OH maybe due to the relatively small population studied.
OH can also be due to weight loss due to active cancer treatment or advanced stages of the disease [36]. A study of 250 patients with a history of hypertension but without cancer showed that OH occurred in 9% of patients with a BMI greater than 30 kg/m2. With the adoption of milder criteria for the diagnosis of OH, it was shown that the percentage of patients with a 10 mmHg decrease in systolic BP was significantly higher among obese (30.8%) than among patients of normal weight (16%); P < 0. 05) [37]. In our study, we found the opposite. In the single-factor analysis, we found that the higher BMI lowers the risk of OH. In the multifactor analysis, we found that BMI above 30 kg/m2 is an independent predictor of absence of OH. Our results can be attributed to cachexia, a debilitating, multifactorial, and often irreversible systemic syndrome that results in significant weight loss (primarily skeletal muscle and body fat). Around 50-80% of cancer patients suffer from cachexia, which contributes significantly to cancer-related mortality [38]. Therefore, it can be assumed that higher BMI and obesity are a protective factor against OH in cancer patients.
The study by Van Hateren et al. showed that the prevalence of OH was higher in diabetic patients compared to healthy patients [39]. Our multifactor analysis confirmed that patients with diabetes have a higher risk of OH, although the correlation was weaker than in the case of cancer presence. In another prospective study by Beretta et al., it was shown that patients with diabetes and OH were 2.7 times more likely to have falls in hospital and 1.54 times more likely to die in hospital compared to patients without diabetes and OH [40]. In our opinion, by introducing routine measurements to detect OH in the cancer population, especially in lung cancer patients, we could identify patients at such risk, implement effective treatment, and prevent the consequences of OH. Furthermore, early detection and prevention of OH consequences could improve quality of life in cancer patients, which is already low due to other reasons.
5. Conclusions
Cancer patients are characterised by a high prevalence of OH. The prevalence of OH prevalence differs with respect to the type of cancer, being the highest among patients with lung cancer. In cancer population screening and monitoring of OH presence is necessary, and recommendation of routine orthostatic challenge tests in this population is needed. More research is needed to evaluate OH prevention methods and determine possible treatment interventions to avoid adverse events.
Author Contributions
Conceptualization, M.A.I. and K.S.; methodology, M.A.I., A.S., A.S., R.W., K.S.; software, M.A.I.; A.S. and K.S.; validation, M.A.I., A.S., A.S., R.W., K.S.; formal analysis, M.A.I.; A.S. and K.S.; investigation, M.A.I.; A.S. and K.S.; resources, M.A.I., A.S., A.S., R.W., K.S.; data curation, M.A.I.; A.S. and K.S.; writing—original draft preparation, M.A.I. and K.S.; writing—review and editing, M.A.I. and K.S.; visualization, M.A.I.; A.S. and K.S.; supervision, K.S.; project administration, M.A.I. and K.S.; funding acquisition, M.A.I. and K.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee at the Regional Medical Chamber in Rzeszow no. 89/2022/B and the patients gave their written informed consent to participate in the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Magkas, N.; Tsioufis, C.; Thomopoulos, C.; Dilaveris, P.; Georgiopoulos, G.; Sanidas, E.; Papademetriou, V.; Tousoulis, D. Orthostatic hypotension: From pathophysiology to clinical applications and therapeutic considerations. J. Clin. Hypertens. 2019, 21, 546–554. [Google Scholar] [CrossRef]
- Freeman, R.; Abuzinadah, A.R.; Gibbons, C.; Jones, P.; Miglis, M.G.; Sinn, D.I. Orthostatic Hypotension: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 1294–1309. [Google Scholar] [CrossRef]
- Walsh, D.; Nelson, K.A. Autonomic nervous system dysfunction in advanced cancer. Support. Care Cancer 2002, 10, 523–528. [Google Scholar] [CrossRef]
- Noor, B.; Akhavan, S.; Leuchter, M.; Yang, E.H.; Ajijola, O.A. Quantitative assessment of cardiovascular autonomic impairment in cancer survivors: a single center case series. Cardiooncology 2020, 6, 11. [Google Scholar] [CrossRef]
- Teng, A.E.; Noor, B.; Ajijola, O.A.; Yang, E.H. Chemotherapy and Radiation-Associated Cardiac Autonomic Dysfunction. Curr Oncol Rep. 2021, 23, 14. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; Cutter, D.J.; de Azambuja, E.; de Boer, R.A.; Dent, S.F.; Farmakis, D.; Gevaert, S.A.; Gorog, D.A.; Herrmann, J.; Lenihan, D.; Moslehi, J.; Moura, B.; Salinger, S.S.; Stephens, R.; Suter, T.M.; Szmit, S.; Tamargo, J.; Thavendiranathan, P.; Tocchetti, C.G.; van der Meer, P.; van der Pal, H.J.H.; ESC Scientific Document Group. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef] [PubMed]
- Mosnaim, A.D.; Abiola, R.; Wolf, M.E.; Perlmuter, L.C. Etiology and risk factors for developing orthostatic hypotension. Am. J. Ther. 2010, 17, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Streeten, D.H., Jr. Anderson, G.H. Mechanisms of orthostatic hypotension and tachycardia in patients with pheochromocytoma. Am. J. Hypertens. 1996, 9, 760–769. [Google Scholar] [CrossRef]
- Gosney, M.A.; Gosney, J.R.; Lye, M. Orthostatic hypotension and vasodilatory peptides in bronchial carcinoma. J. Clin. Pathol. 1995, 48, 1102–1105. [Google Scholar] [CrossRef]
- Tykarski, A.; Filipiak, K.J.; Januszewicz, A.; Litwin, M.; Narkiewicz, K.; Prejbisz, A.; Ostalska-Nowicka, D.; Widecka, K.; Kostka-Jeziorny, K. Zasady postępowania w nadciśnieniu tętniczym – 2019 rok. Wytyczne Polskiego Towarzystwa Nadciśnienia Tętniczego. Nadciśnienie Tętnicze w Praktyce. 2019, 5, 1–86. [Google Scholar]
- Lavi, S.; Aharon-Peretz, J.; Haim, N.; Vlodavsky, E.; Jacob, G. Unusual cause of partially reversible severe cardiovascular autonomic failure. Am. J. Med. Sci. 2003, 326, 159–163. [Google Scholar] [CrossRef]
- Shah, R.V.; Patel, K.P.; Manion, C.; Runkana, A.; Hama Amin, A.; Jain, A. Third-degree atrioventricular block followed by syncope, labile hypertension, and orthostatic hypotension in a patient with nasopharyngeal cancer: baroreflex failure. Am. J. Cardiovasc. Dis. 2018, 8, 39–42. [Google Scholar] [PubMed]
- Ashraf, W.; Farrow, L.J. Severe orthostatic hypotension in carcinoma of the pancreas. Br. J. Clin. Pract. 1992, 46, 278–279. [Google Scholar] [CrossRef] [PubMed]
- Bortnik, M.; Occhetta, E.; Marino, P. Orthostatic hypotension as an unusual clinical manifestation of pheochromocytoma: a case report. J. Cardiovasc. Med. 2008, 9, 839–841. [Google Scholar] [CrossRef]
- Lee, S.; Chary, M.; Petersen, B.; Mascarenhas, J.O. Paraneoplastic orthostatic hypotension associated with acute myeloid leukemia. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2934–2937. [Google Scholar] [PubMed]
- Sharabi, Y.; Dendi, R.; Holmes, C.; Goldstein, D.S. Baroreflex failure as a late sequela of neck irradiation. Hypertension. 2003, 42, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, H.; Norcliffe-Kaufmann, L.; Palma, J.A. Baroreflex Dysfunction. N. Engl. J. Med. 2020, 382, 163–178. [Google Scholar] [CrossRef]
- Dermitzakis, E.V.; Kimiskidis, V.K.; Lazaridis, G.; Alexopoulou, Z.; Timotheadou, E.; Papanikolaou, A.; Romanidou, O.; Georgiadis, G.; Kalogeras, K.T.; Tsiptsios, I.; Tarlatzis, B.; Fountzilas, G. The impact of paclitaxel and carboplatin chemotherapy on the autonomous nervous system of patients with ovarian cancer. BMC Neurol. 2016, 16, 190. [Google Scholar] [CrossRef]
- Vassilomanolakis, M.; Koumakis, G.; Demiri, M.; Missitzis, J.; Barbounis, V.; Efremidis, A.P. Vinorelbine and cisplatin for metastatic breast cancer: a salvage regimen in patients progressing after docetaxel and anthracycline treatment. Cancer Invest. 2003, 21, 497–504. [Google Scholar] [CrossRef]
- Ho, M.; Moscvin, M.; Low, S.K.; Evans, B.; Close, S.; Schlossman, R.; Laubach, J.; Prada, C.P.; Glotzbecker, B.; Richardson, P.G.; Bianchi, G. Risk factors for the development of orthostatic hypotension during autologous stem cell transplant in patients with multiple myeloma. Leuk. Lymphoma. 2022, 63, 2403–2412. [Google Scholar] [CrossRef]
- Vecchié, A.; Thomas, G.; Bressi, E.; Bonaventura, A.; Canada, J.M.; Chuquin, D.; Kadariya, D.; Piracha, U.; Endicott, D.; Markley, R.; Toor, A.; Hess, M.; Abbate, A. Orthostatic intolerance syndromes after hematopoietic cell transplantation: clinical characteristics and therapeutic interventions in a single-center experience. Cardiooncology. 2021, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Fradley, M.G.; Beckie, T.M.; Brown, S.A.; Cheng, R.K.; Dent, S.F.; Nohria, A.; Patton, K.K.; Singh, J.P.; Olshansky, B. Recognition, Prevention, and Management of Arrhythmias and Autonomic Disorders in Cardio-Oncology: A Scientific Statement From the American Heart Association. Circulation. 2021, 144, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, J.R.; Munk-Madsen, P.; Kehlet, H.; Gögenur, I. Orthostatic intolerance in enhanced recovery laparoscopic colorectal resection. Acta Anaesthesiol. Scand. 2019, 63, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Unaldi, H.E. Effects of mobilization within the first 4 h following anatomical lung resection with thoracotomy. Updates Surg. 2023, 75, 2027–2031. [Google Scholar] [CrossRef]
- Nakada, T.; Shirai, S.; Oya, Y.; Takahashi, Y.; Sakakura, N.; Ohtsuka, T.; Kuroda, H. Four Hours Postoperative Mobilization is Feasible After Thoracoscopic Anatomical Pulmonary Resection. World J. Surg. 2021, 45, 631–637. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, C.; Wang, Y.; Feng, F.; Wang, H.; Zhang, Y.; Lin, X.; Xu, B. Lambert-Eaton Myasthenic Syndrome in Lung Cancer. Contrast Media Mol. Imaging. 2022. [Google Scholar] [CrossRef]
- Worrall, A.P.; Doyle, C.P.; Ní Dhomhnall, R.; Lorton, C.; Barrett, M.; Uí Dhuibhir, P.; O’Higgins, C.; Brady, B.; Walsh, D. Blood Pressure, Orthostatic Hypotension and Falls in Patients with Advanced Cancer. Ir. Med. J. 2022, 115, 596. [Google Scholar]
- Ricci, F.; De Caterina, R.; Fedorowski, A. Orthostatic Hypotension: Epidemiology, Prognosis, and Treatment. J. Am. Coll. Cardiol. 2015, 66, 848–860. [Google Scholar] [CrossRef]
- Fedorowski, A.; Ricci, F.; Sutton, R. Orthostatic hypotension and cardiovascular risk. Kardiol. Pol. 2019, 77, 1020–1027. [Google Scholar] [CrossRef]
- Low, P.A. Prevalence of ortostatic hypotension. Clin. Auton. Res. 2008, 18, 8–13. [Google Scholar] [CrossRef]
- Fedorowski, A.; Ricci, F.; Hamrefors, V.; Sandau, K.E.; Hwan Chung, T.; Muldowney, J.A.S.; Gopinathannair, R.; Olshansky, B. Orthostatic Hypotension: Management of a Complex, But Common, Medical Problem. Circ. Arrhythm. Electrophysiol. 2022, 15, e010573. [Google Scholar] [CrossRef]
- Ricci, F.; Radico, F.; Romanello, M. Morbidity and mortality related to orthostatic hypotension: results of a meta-analysis of non-randomized observational studies. Eur. Heart J. 2013, 34, 4462. [Google Scholar] [CrossRef]
- Ricci, F.; Fedorowski, A.; Radico, F.; Romanello, M.; Tatasciore, A.; Di Nicola, M.; Zimarino, M.; De Caterina, R. Cardiovascular morbidity and mortality related to orthostatic hypotension: a meta-analysis of prospective observational studies. Eur. Heart J. 2015, 36, 1609–1617. [Google Scholar] [CrossRef]
- Ali, A.; Ali, N.S.; Waqas, N.; Bhan, C.; Iftikhar, W.; Sapna, F.; Jitidhar, F.; Cheema, A.M.; Ahmad, M.Q.; Nasir, U.; Sami, S.A.; Zulfiqar, A.; Ahmed, A. Management of Orthostatic Hypotension: A Literature Review. Cureus. 2018, 10, 3166. [Google Scholar] [CrossRef]
- Rivasi, G.; Rafanelli, M.; Mossello, E.; Brignole, M.; Ungar, A. Drug-Related Orthostatic Hypotension: Beyond Anti-Hypertensive Medications. Drugs Aging. 2020, 37, 725–738. [Google Scholar] [CrossRef]
- Sever, P. Severe orthostatic hypotension and weight loss associated with cancer therapy. Br. J. Cardiol. 2021, 28, 40. [Google Scholar] [CrossRef] [PubMed]
- Grześkowiak, A.; Rojek, A.; Szyndler, A.; Śmiałek, K.; Szczęch, R.; Chrostowska, M.; Narkiewicz, K. Prevalence of postural hypotension in patients with treated hypertension. Arterial Hypertension. 2005, 9, 452–457, https://journals.viamedica.pl/arterial_hypertension/article/view/12599. [Google Scholar]
- Argilés, J.M.; López-Soriano, F.J.; Stemmler, B.; Busquets, S. Cancer-associated cachexia - understanding the tumour macroenvironment and microenvironment to improve management. Nat. Rev. Clin. Oncol. 2023, 20, 250–264. [Google Scholar] [CrossRef]
- van Hateren, K.J.; Kleefstra, N.; Blanker, M.H.; Ubink-Veltmaat, L.J.; Groenier, K.H.; Houweling, S.T.; Kamper, A.M. , van der Meer, K.; Bilo, H.J. Orthostatic hypotension, diabetes, and falling in older patients: a cross-sectional study. Br. J. Gen. Pract. 2012, 62, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Beretta, M.V.; Milan, V.B.; Hoffmeister, M.C.; Rodrigues, T.C. Orthostatic hypotension, falls and in-hospital mortality among elderly patients with and without type 2 diabetes. J. Hypertens. 2023, 41, 388–392. [Google Scholar] [CrossRef]
Figure 1.
Outline of the methodology and diagnosis criteria of orthostatic hypotension. Abbreviations: BP, blood pressure; HR, heart rate.
Figure 1.
Outline of the methodology and diagnosis criteria of orthostatic hypotension. Abbreviations: BP, blood pressure; HR, heart rate.
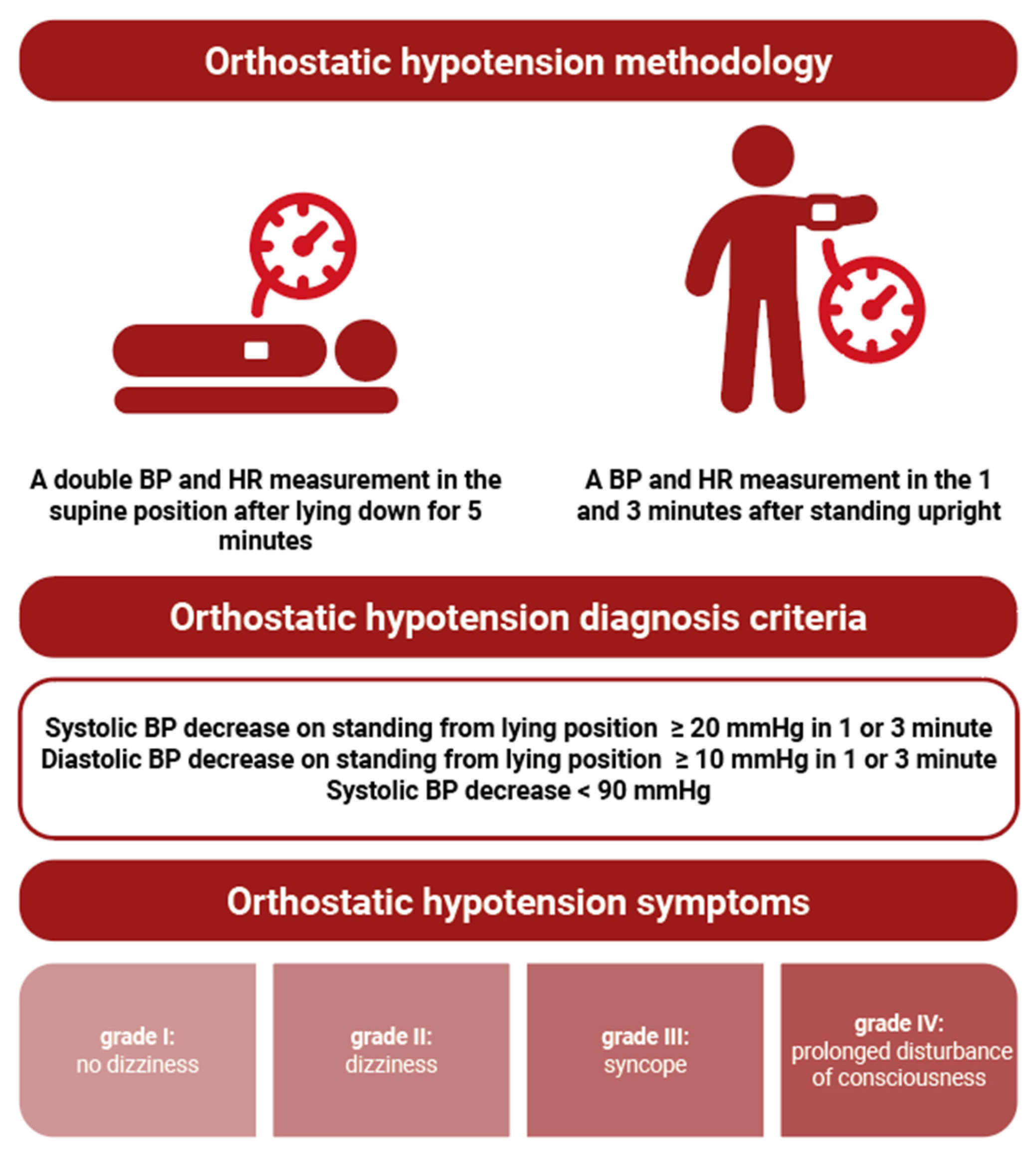
Figure 2.
Blood pressure (BP) and heart rate (HR) changes on orthostatic challenge test according to cancer status. During tilting significant fall of systolic blood pressure is noted in cancer patients compared to non-cancer subjects (A), diastolic BP however rises during standing being in 3 minute of test significantly higher in non-oncological group than in cancer patients (B). HR is increasing during tilt, in 1 minute significantly more in cancer than noncancer patients (C). Abbreviations: Δ BP, delta blood pressure- difference in BP in upright position and BP in supine calculated separately for systolic BP and diastolic BP. Δ HR, delta heart rate- difference in HR in upright position and HR in supine.
Figure 2.
Blood pressure (BP) and heart rate (HR) changes on orthostatic challenge test according to cancer status. During tilting significant fall of systolic blood pressure is noted in cancer patients compared to non-cancer subjects (A), diastolic BP however rises during standing being in 3 minute of test significantly higher in non-oncological group than in cancer patients (B). HR is increasing during tilt, in 1 minute significantly more in cancer than noncancer patients (C). Abbreviations: Δ BP, delta blood pressure- difference in BP in upright position and BP in supine calculated separately for systolic BP and diastolic BP. Δ HR, delta heart rate- difference in HR in upright position and HR in supine.
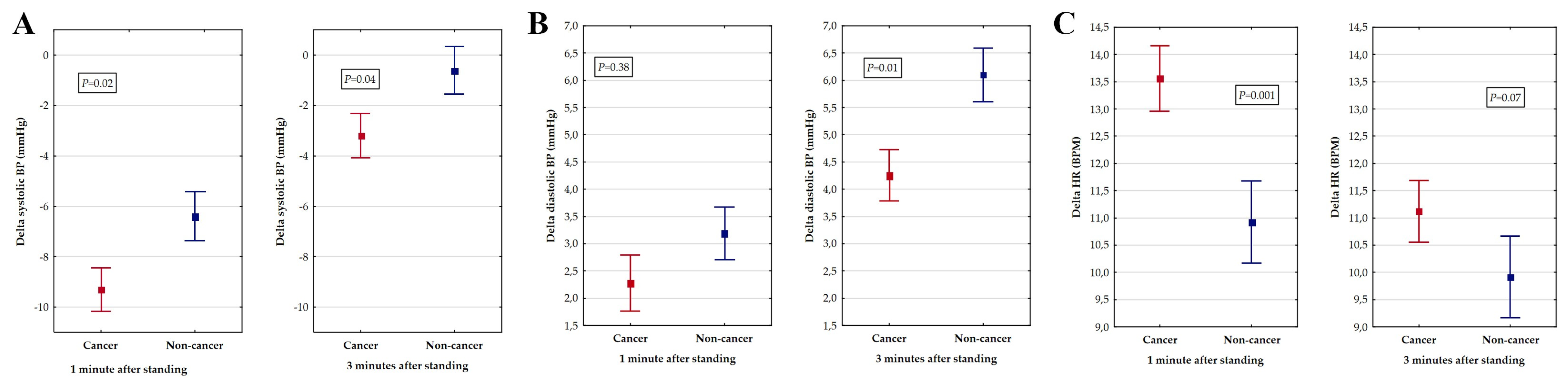
Figure 3.
Prevalence of orthostatic hypotension according to the type of cancer. In lung cancer, orthostatic hypotension is significantly more prevalent compared to other cancer groups, except breast cancer.
Figure 3.
Prevalence of orthostatic hypotension according to the type of cancer. In lung cancer, orthostatic hypotension is significantly more prevalent compared to other cancer groups, except breast cancer.
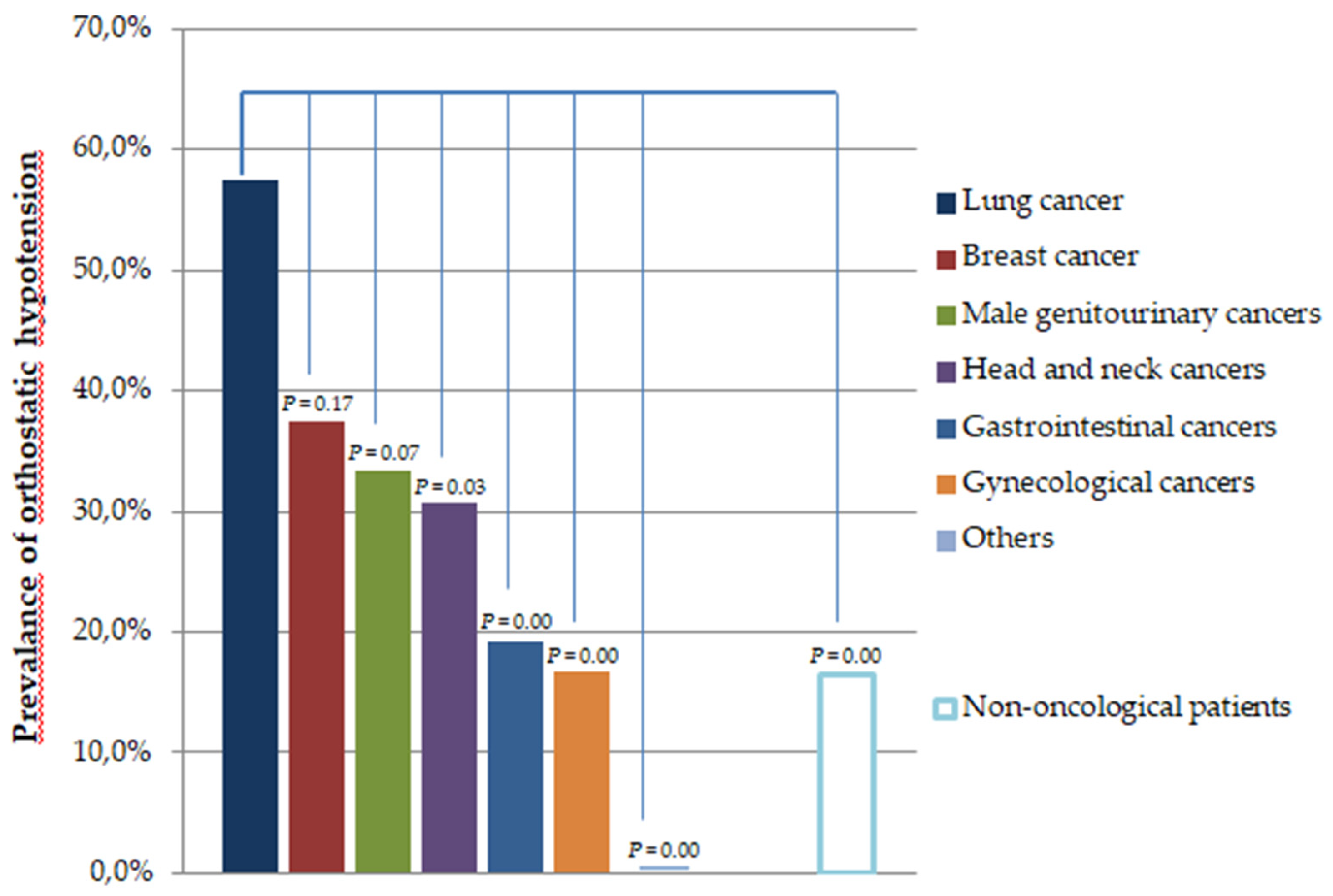
Figure 4.
Main causes of orthostatic hypotension in cancer patients (description in the text).
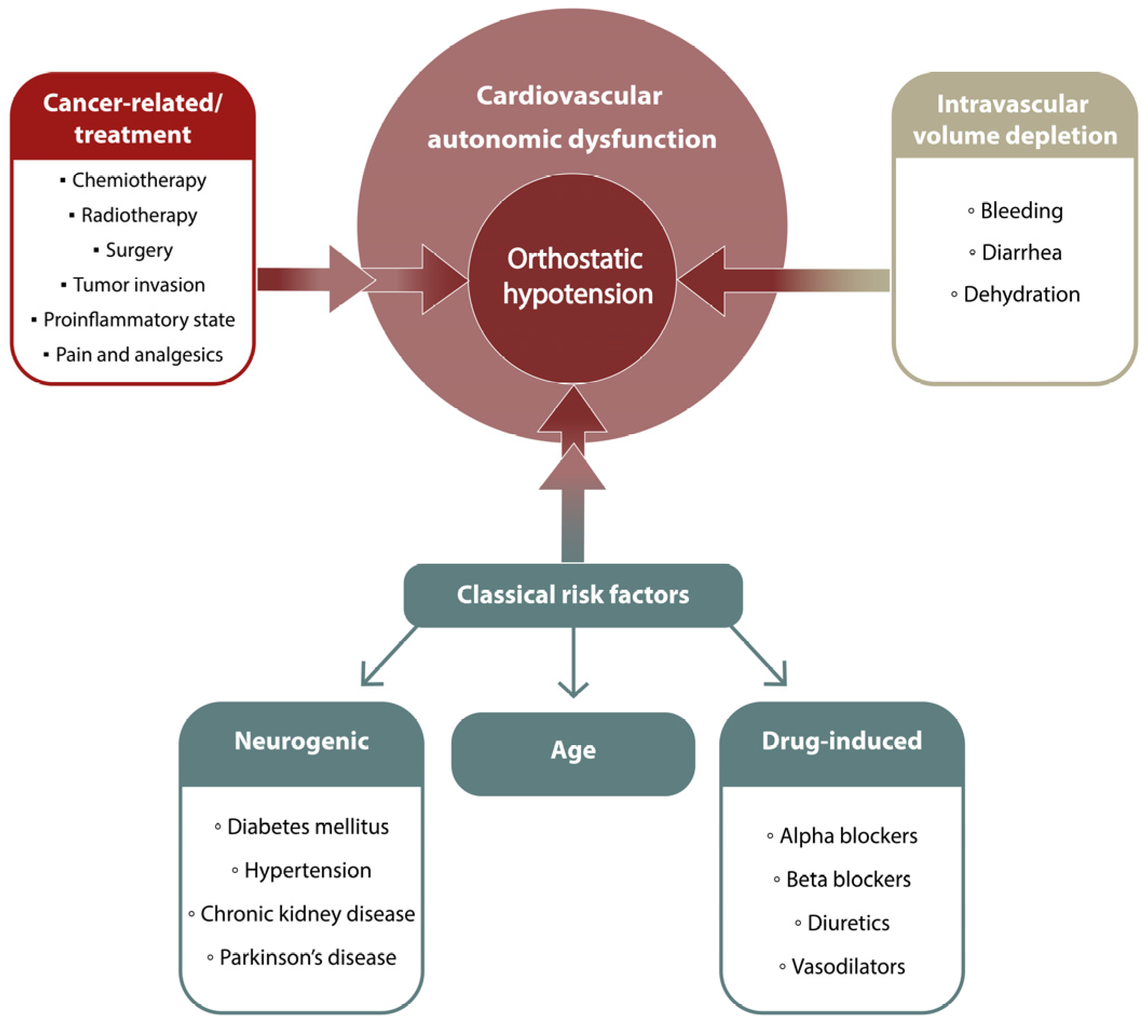

Table 1.
Distribution of patients according to hospital units and number of cases according to type of cancer.
Table 1.
Distribution of patients according to hospital units and number of cases according to type of cancer.
| Hospital Department | Number of Cases | % |
|---|---|---|
| Clinical Oncology | 106 | 25.8 |
| Oncological Gynecology | 58 | 14.1 |
| Radiotherapy | 56 | 13.6 |
| Neurology | 108 | 26.3 |
| Internal diseases | 49 | 11.9 |
| Dermatology | 20 | 4.9 |
| Rehabilitation | 10 | 2.4 |
| Urology | 4 | 1.0 |
| Total | 411 | 100 |
| Type of cancer | Number of Cases | % |
| Lung cancer | 40 | 17.9 |
| Breast cancer | 16 | 7.2 |
| Male genitourinary cancers | 21 | 9.4 |
| Head and neck cancers | 26 | 11.7 |
| Gastrointestinal cancers | 52 | 23.3 |
| Gynecological cancers | 60 | 26.9 |
| Others | 8 | 3.6 |
| Total | 223 | 100 |
Table 2.
Baseline demographic and clinical characteristics with respect to cancer status.
| Oncological (n = 223) | Non-oncological (n = 188) | P-value | |
|---|---|---|---|
| Age in years, mean (SD) | 65.0 (8.9) | 61.5 (12.2) | 0.01 |
| Female sex, n (%) | 116 (52.0) | 113 (60.1) | 0.09 |
| BMI (kg/m2), mean (SD) | 26.2 (5.7) | 28.1 (5.0) | 0.01 |
| SBP (SD) | 127.7 (16.6) | 129.2 (18.4) | 0.35 |
| DBP (SD) | 80.0 (10.4) | 79.3 (9.7) | 0.42 |
| HR (SD) | 69.4 (12.4) | 78.4 (14.0) | 0.001 |
| Orthostatic hypotension, n (%) | 64 (28.7) | 31 (16.5) | 0.003 |
| Orthostatic hypotension symptoms: grade I, n (%) grade II, n (%) grade III, n (%) grade IV, n (%) |
198 (88.8) 25 (11.2) 0 0 |
187 (99.5) 1 (0.5) 0 0 |
0.00001 |
| Hypertension, n (%) | 114 (51.1) | 98 (52.1) | 0.83 |
| CAD, n (%) | 22 (9.9) | 21 (11.2) | 0.66 |
| Stroke, n (%) | 5 (2.2) | 9 (4.8) | 0.15 |
| Dyslipidemia, n (%) | 25 (11.2) | 43 (22.9) | 0.001 |
| Diabetes, n (%) | 38 (17.0) | 48 (25.5) | 0.03 |
| CKD, n (%) | 5 (2.2) | 7 (3.7) | 0.37 |
| Thyroid diseases, n (%) | 19 (8.5) | 20 (10.6) | 0.46 |
| VTE, n (%) | 15 (6.7) | 7 (3.7) | 0.17 |
| PD, n (%) | 1 (0.5) | 3 (1.6) | 0.23 |
| Diuretics, n (%) | 42 (18.8) | 27 (14.4) | 0.22 |
| ACEi, n (%) | 59 (26.5) | 56 (29.8) | 0.45 |
| ARBs, n (%) | 20 (9.0) | 22 (11.7) | 0.36 |
| Beta- blockers, n (%) | 82 (36.8) | 60 (31.9) | 0.30 |
| Nitrates, n (%) | 10 (4.5) | 6 (3.2) | 0.49 |
| Alpha-blockers, n (%) | 5 (2.2) | 6 (3.2) | 0.55 |
| CCB, n (%) | 34 (15.3) | 38 (20.2) | 0.18 |
| Antiparkinsonian agents, n (%) | 1 (0.5) | 3 (1.6) | 0.23 |
Abbreviations: ACEi, angiotensin converting enzyme inhibitors; ARBs, angiotensin II receptor blockers; BMI, body mass index; CAD, coronary artery disease; CCB, calcium channel blockers; CKD, chronic kidney disease; DBP, diastolic blood pressure; HR, heart rate; VTE, venous thromboembolism; PD, Parkinson disease; SBP, systolic blood pressure.
Table 3.
Single and multivariable analysis of clinical predictors of orthostatic hypotension.
| Variable | Single-variable analysis | Multivariable analysis | ||||
| OR | 95% CI | P-value | OR | 95% CI | P-value | |
| Cancer | 2.04 | 1.26-3.31 | 0.003 | 2.06 | 1.24-3.43 | 0.005 |
| Age ≥ 65 | 2.45 | 1.44-4.18 | 0.0002 | - | - | - |
| Male sex | 1.31 | 0.83-2.08 | 0.24 | - | - | - |
| BMI ≥ 30 kg/m2 | 0.47 | 0.26-0.82 | 0.007 | 0.40 | 0.22-0.72 | 0.002 |
| Hypertension | 1.47 | 0.92-2.35 | 0.10 | - | - | - |
| Diabetes | 1.61 | 0.94-2.74 | 0.07 | 1.90 | 1.06-3.40 | 0.03 |
| Stroke | 2.60 | 0.87-7.70 | 0.08 | - | - | - |
Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



