
Submitted:
18 March 2024
Posted:
20 March 2024
You are already at the latest version
Abstract
Background: Schistosomiasis is the third most important Neglected Tropical Disease, with more than 4 million South Africans being infected. Cases of re-infection with schistosomiasis after being treated using modern medication has opened ways to seeking alternative treatment modalities using medicinal plants. This study aims to explore and understand the way traditional healers diagnose schistosomiasis, the types of traditional medicines they use to treat it in communities with a high prevalence of infection, and to establish whether the unavailability of prescribed anti-schistosomal medicines leads to the use of traditional medicine. Methods: A qualitative exploratory study was conducted using a questionnaire from December 2022 to March 2023 in the iLembe District, KwaZulu-Natal Province, South Africa. In-depth individual interviews were carried out among traditional health practitioners (THPs) involved in managing female urogenital schistosomiasis (FUS). Recorded narrative data was transcribed verbatim, read through thoroughly and coded, and analysed using thematic or content analysis Results: Traditional Health Practitioners provide services to many women who did not want to be treated in the mainstream health care system for their FUS. The disease was perceived and understood the same way by most of the respondents, that being caused by use of fresh water. Various plants species, either alone or in combination, were used to manage bilharzia in women. Senecio serratuloides (Asteraceae) and Hypoxis hemerocallidea (Hypoxidaceae) were prominently used by THPs in FUS management. Conclusion: Traditional Health Practitioners are playing a key role in managing bilharzia in women in rural areas of the iLembe District, this study reported that THPs can diagnose schistosomiasis symptoms based on their knowledge and experience. Respondents indicated that modern conventional treatment was readily available and free in public sector healthcare facilities; however, they consulted patients suffering from FUS. Various traditional herbal medicines are reportedly used by THPs to manage bilharzia in women. Further studies are needed to investigate the views and experiences of clients regarding the success of the treatments used and why they seek care from THPs.
Keywords:
Female urogenital schistosomiasis
; Traditional health practitioners
; Traditional medicine
; Management
; South Africa
; qualitative study
Background
The World Health Organisation (WHO) estimated that a minimum of 206.4 million people were in need of treatment for schistosomiasis in 2016, with almost 91.4% living in Africa (WHO, 2018). Being the third most important Neglected Tropical Disease, Bilharzia, or Schistosomiasis, is an infectious, water-borne parasitic disease in many tropical settings that is caused by worms falling under the Schistosoma genus (Colley et al., 2014, Gurarie et al., 2018, WHO, 2018). People engaging in various activities in contact with fresh/untreated water infected by Schistosoma during activities such as: laundry, plate washing, water fetching for domestic use, bathing, paddling, diving, swimming or drinking as well as fishing and farming, are at risk of contracting the disease. Women and children are the most exposed (WHO, 2015), as they are often involved in activities associated with water. Female urogenital schistosomiasis is presented as an inflammation and ulceration of the genital mucosa, and is listed by the WHO as a research priority (Christinet et al., 2016, Magaisa et al., 2015, Poggensee et al., 1999).
More than four million South Africans are infected with schistosomiasis (Magaisa et al., 2015) , and while Praziquantel is used effectively to control current infections, often through mass-treatment programmes, it may also worsen the symptoms and will not prevent future infections (Berge et al., 2011, Fenwick et al., 2009, WHO, 2011). Treatment is also provided by traditional health practitioners (THP) who use traditional medicine (TM) in rural communities of South Africa, with many people using them as their primary healthcare provider of choice (Zuma et al., 2016). In southern African countries, TM has played a key role in managing schistosomiasis, also known as bilharzia, making it important to document to establish its efficacy (Cock et al., 2018).
Various studies carried out in South Africa have reported that several plants are recognized as having anti-schistosomal activity (Cock et al., 2018, Sparg et al., 2000). The following species have been widely used to manage the disease: Acacia karroo, Maytenus senegalensis, Peltophorum africanum and Ziziphus mucronata, Abrus precatorius, Boswellia carteri, Cissampelos murconata, Euclea natalensis, Sclerocarya birrea, Rumex nepalensis, Protasparagus buchananii, Maytenus senegalensis, Faurea saligna (Cock et al., 2018, Hutchings, 1996, Koenen, 2001, Mangoyi et al., 2011, Watt et al., 1962). Moreover, cases of re-infection with schistosomiasis following the use of modern medication to treat it has opened ways to seeking alternative treatment modalities based on indigenous knowledge (IK) holders through the use of medicinal plants.
There has been little research on THPs knowledge, perceptions and practices regarding the process of traditional healing of bilharzia in women in South Africa. To address this gap, this present study was conducted among THPs from the ILembe District in KwaZulu-Natal Province, South Africa. This study aims to explore and gain an understanding of the way THPs diagnose female urogenital schistosomiasis (FUS) , identify the types of traditional medicines used to treat it in communities with a high prevalence of infection, and to establish whether the unavailability of prescribed anti-schistosomal medicines in the public health sector leads to the use of traditional medicine.
Methods
Study Settings
The ILembe District Municipality is located on the east coast of KwaZulu-Natal Province north of the city of Durban, and is the smallest of the provincial municipalities, with a population of 630 464 in an area of 3,269 km2;. Most of the interior rural areas are tribally controlled and characterized by subsistence agriculture. ILembe consists of four sub-districts: Mandeni, KwaDukuza, Maphumulo and Ndwedwe (Figure 1), its main town being Stanger, which lies on the Tugela River. (http://www.kznonline.gov.za/index.php/government/ 2016-08-02-09-42-02/ilembe-district-municipality).
Study Design
An exploratory qualitative study was undertaken from December 2022 to March 2023 and consisted of eight weeks of fieldwork. A semi-structured questionnaire with open questions administered to participants, using face-to-face interviews to obtain qualitative data (Creswell, 2009).
Study Sample
This study enrolled 22 THPs who were recruited from the Traditional Health Organisation (THO) in the ILembe District using purposeful sampling, followed by snowball sampling, with referrals being made to identify suitable participants (Patton, 1990). Male and female THPs who were aged 18 years old and above were included who had managed FUS in women for at least one year.
Procedure for Recruiting and Selecting Study Participants
This study was approved by the Biomedical Research Ethics Committee of the University of KwaZulu-Natal under reference BE477/17, and informed consents was sought from all participants. They agreed on the findings being published to raise awareness on the contribution of traditional medicine to manage FUS. Contacts were made through the University of KwaZulu-Natal’s Centre in Indigenous Knowledge Systems with THO leaders to identify registered THPs. After being introduced by community leaders, the research team approached THPs at their workplace during business hours, with those being willing to participate being interviewed.
Data Collection Methods
A semi-structured questionnaire with open- and closed-ended questionnaire was administered to participants using face-to-face interviews until saturation was reached (Marshall, 1998). The design of the questionnaire reduced possible bias and misunderstanding between western and indigenous conception of FUS and its bio-medical definition (Reidpath et al., 2011, Vigneron et al., 2005). THPs were interviewed at their houses or any place of their choice and lasted from 15-60 minutes. Study aims and procedures were explained to participants in English and the local language, IsiZulu. The questionnaire was divided into four sections: demographic data, and their knowledge, perceptions and practices about managing FUS, and is presented in Additional File 1. The interview were recorded with the participant’s permission, with notes being taken and observations made throughout.
Data Analysis
The Statistical Package for Social Sciences (SPSS) Version 25 was used for demographic data (Apesoa-Varano and Hinton, 2013). The recorded narrative qualitative data was collected using the Giorgi’s phenomenological framework (Christensen and Practice, 2017, Giorgi, 2012), and transcribed verbatim, read through thoroughly and coded for thematic analysis for step-wideness (Krippendorff, 2004, Mayring, 2015, Patton, 1990). The transcripts were cross-checked with the records, and meaning units corresponding to the study objective extracted, coded, grouped in sub-categories and thematic categories following the deductive technique, and substantiated by quotes (Kuckartz, 2012). The body language, silences and other non-verbal communications are considered in analysing the data (Croucher and Cronn-Mills, 2014).
This study followed the guidelines proposed by Lincoln and Guba (Lincoln and Guba, 1985) for trustworthiness of the findings, with more than one researcher being involved in the study and the voluntarily participation of respondents. The research procedure and design enhanced transparently to provide transferability.
Results
The participants’ demographic details are followed by the themes relating to the THPs knowledge, perceptions and practices of managing FUS.
Demographic Details
The 22 participants who agreed to be interviewed (Table 1) were aged between 26 and 70 years old, with a mean age of 41.05 ± 13.075 (SD). The majority were females (63.6%; 14/22), married were 14 (63.6%) and most participants completed their high schooling (45.5%; 10/22). Most respondents practised as diviners (Izangoma) (17/22, 77, 2%), were Christians (15/22, 68, 2%), and had a mean of 13 years’ experience (±10.170).
Traditional Health Practitioners’ Perceptions, Knowledge and Experiences in Diagnosing of FUS.
A thematic content analysis was carried out that yielded seven major themes: (1) source of knowledge, (2) diagnosing female urogenital schistosomiasis, (3) acceptability and affordability of treatment, (4) Locally used plants to manage FUS, (5) availability of TM treatment in FUS management, (6) concurrent use of TM with prescribed conventional antischistosomal medicines, and (7), knowledge of side effects and perceptions of efficacy of treatment provided by THPs
Theme 1. Source of knowledge
Respondents were questioned about their source of knowledge about healing FUS, and reported that a special calling from ancestors is a requirement of becoming a traditional healer. In most cases, this calling can come in dreams/visions, where trainees are instructed to avail themselves into helping the community by becoming THPs. If they agree, they go through a training after verification of the calling, and in addition, THPs who trains news one are called to do so as well. They are not only traditional healers but trainers, as with the ancestors giving orientation to the newly called person, sending them to a trainer. When asked about their source of the healing process for FUS, a respondent noted that:
“… I didn’t just have knowledge of being sangoma (traditional healer), my ancestor came to me and took me to a training of ukuthwasa (which is to accept the calling of becoming a traditional healer).” THP21
They reported to have learnt from old THPs, identified as trainers, in their respective areas. In the learning process, they go through different healing practices for a period of time. When asked about how he learnt the healing process a respondent said:
“… We use to work up early morning and go to inyanga houses where we had to pass the whole day studying Traditional Medicine and I did it for a year…” THP18
Theme 2. Diagnosing female urogenital schistosomiasis
THPs mentioned that FUS occurs when engaging in various activities close to fresh water, and diagnose the symptoms based on their knowledge and experience, specifically by checking the patient’s urine coloration. A Respondent reported the following that:
“… If the person is urinating constantly blood or if their urine changing colour. The same thing happens in women when they have this disease (FUS)…” THP18
Some respondents indicated that there was a natural process of diagnosing FUS in women that involved mainly physical symptoms. A respondent reported that:
“ … Urine have unusual temperature, tension on bladder, prostate feels itchy for man, it is swollen near the bladder, and bladder feels pain for male and female. If the person is urinating constantly blood or if their urine changing colour and itching when urinating. The same thing happens in women when they have this disease…” THP2.
Some reported that they relied on spiritually diagnosing FUS by consulting their ancestors, and that people sometimes had a curse tossed at them that is why they need spiritual assistance. A participant mentioned the following:
“…We perform the practice called Ukumhlola ngoko moya (spiritual divination) to diagnose bilharzia in patients…” THP9
Some used both natural and spiritual ways to diagnose schistosomiasis in women, the one method confirming the other:
“… Ucama igazi (urinating blood) after swimming in rivers then I throw bones to confirm the diagnostic…” THP15
Theme 3. Acceptability and affordabilityof treatment
The respondents noted that although modern treatments were readily available and free in public sector healthcare facilities, they consulted many women who did not want to be treated in the mainstream health care system (acceptability), preferring to first consult THPs:
“I treat the patient who come to me with bilharzia (isichenene) because they think that it is only for children. They are feeling bad to tell to the doctors that they are urinating blood (ukucama igazi)… “THP1
THPs, as IK holders, contended that traditional medicine is affordable and accessible to community members, with no standard price for consultations and payment being done after being treated. The cost of medicine depended on the level of confidence between the healer and his patients, and varies from healer to healer as well as being based on the severity of the infection. A respondent reported that:
“… I’m not sure of how much it would cost to treat bilharzia at the hospital but traditionally I make the price of all my medicines almost similar, for Ischenene its R150 for the complete treatment…” THP18
In comparing traditional treatment to orthodox treatment, a few participants argued that their treatment price can depend on how and where it was collected from, as well as its price at the Muti market, all of which contribute to the price they charge the patients, which can make some treatment expensive. Participants said:
“… Traditional healers medicine are quite expensive, traditional healers are more expensive than the scientific people…” THP3
The acceptability and affordability of the treatment depends on whether the infection is severe, or the patient is newly infected. The more medication they take the more money they will have to pay. A respondent said that:
“.. Depends on the person sickness and the person intensity to be healed, as well as what the person need, also on the healer’s payment rate…” THP7
Some infections can be beyond the THPs knowledge and understanding, including FUS, for which they refer a patient to healthcare facilities. They advanced that it is not about treatment payment but the patient well-being, and reported that:
“… We cannot say a patient has to choose what they afford or what they see cheaper between traditional medicine and modern medicine. Doctors’ medicines have chemicals that reduce pains quicker, that’s why I recommend them if I can’t manage the disease…” THP 17
THPs combine practices by executing the spiritual part and leaving the treatment to healthcare workers in a collaborative way:
“There are sicknesses that are based on witchcraft, that’s where a traditional healer is needed. When I see that my patient’s sickness is not of witchcraft I then advise them to go to hospitals…” THP21
Both western and unorthodox practitioners can collaborate when needed, as they can complement each other, including for FUS management:
“… Modern doctors and traditional doctors should work here hand-in-hand. Modern doctors are very important. The collaborative approach is good for the wellbeing of the patient in the managing this disease (FUS)…” THP20
Traditional healers testified that they discuss their treatment fees with their patients who give them feedback of the efficacy of the treatment before payment.
Theme 4. Locally used plants to manage FUS
The THPs indicated that they used a combination of traditional medicinal plants to treat FUS, which most (n= 12; 54.5%) indicated were not easily accessible. They used various plants manage FUS in rural areas of KwaZulu-Natal Province, some of which are well known by community members who used them on their own, only sometimes consulting THPs. They reported that the main sources of treatment were plants. Doses were measured depending on the severity of the disease and the experience of each THP. Most of respondents were sceptical about sharing knowledge with the researchers. Table 2 presents a list of the plants used to manage FUS.
Theme 5. Availability of TM treatment in FUS management
To treat their patients, traditional healers have to find the components, including the plants. The availability of plants varies widely, with some being found in the traditional medicine market where they have to buy them, or they need to go into natural areas to find them. There is substantial variability in the availability of plants treating bilharzia, depending on the season that they collect them or their availability in the market. A respondent said:
“It is very easy to get these plants. I get them from the forest and I buy some of them from Durban Berea Market…” THP21
Some participants declared that the ease of finding the plants can be related to the frequency of their use and therefore availability. If they use them regularly they know where to find them, either in the market or in nature. THPs sometimes share their ideas and knowledge among themselves, this collaboration enabling them to get what they do not have from another healer, in this way contributing to the well-being of the community:
“… Yes, we find them easily, depending on experience on using them or got them from other THPs or go at the market… ” THP15
Some participant said that the treatments can be difficult to find for those who are new to the working area. Some need to go back to where they come from to look for plants to treat bilharzia, as said the following participant:
“… Some plants are easy to find while others are very hard to find. I find some plants on the other side of the road and to get others I have to travel to far place …” THP19
Some plants are seasonal and must be collected at a specific time of year, which may not be easy to if it requires going in the bush to collect them, some of which are in limited supply:
“It’s not easy to get these cures because we have to go and look for them in the forest, especially in winter, it is very hard to find them…” THP18
Theme 6. Concurrent use of TM with prescribed conventional anti-schistosomal medicines
Two thirds of the respondents (n=15, 68.2%) reported that their patients did not use TM concurrently with conventional anti-schistosomal medicines. This may suggest that the concurrent use of the two types of medicines is not always disclosed by their patients. This was indicated by one of the respondents:
“Patients go to modern doctors most of time on their own initiative, not mine, they go to medical doctors without telling you…” THP8
Some THPs indicated that their patients consulted mainstream practitioners if they were not satisfied with the treatment from THPs, as indicated by a respondent:
“… No, concurrent use of traditional and modern medicine unless if TM does not work, the patient himself goes there…” THP16
THPs in this study had referred patients to modern healthcare facilities for FUS treatment when the infection was beyond their professional capacities and skills. One of the respondents stated:
“… I’m aware that my patients use sometimes both modern and traditional medicine for managing FUS. As traditional healers, it is important for us to work with modern doctors because we are not after money, but we want to see our patients better. There is a stage of the FUS infection that we cannot treat and there are diseases that modern doctors can not treat, so I send my patients there if they need to use both medicines… ” THP21
The THPs mentioned that they have sent patients to healthcare facilities for medical examination if they were not experienced in schistosomiasis management. A respondent said:
“… I usually send them to hospitals for checking up if my cure that I used worked or not. Sometimes I send them to Hospital when I don’t know how to treat certain diseases…” THP18
Another group of THPs reported that they did not get help from biomedically trained healthcare professionals and did not initiate any collaboration with them. They advanced reasons such as the absence of motivation in communication and collaboration with these professionals and vice versa due to cultural basis and people’s beliefs.
“… No, I don’t mix or allow both uses, but they can rather start with one, if it doesn’t work the patient takes another one. I can do for Lab test but not the treatment because I trust it… Patients use both, but I don’t easily send them to hospitals due to cultural base…” THP12
In addition to the above statement, another respondent reported that:
“… Medical doctors ease the pain but do not permanently remove the problem of FUS…” THP10
THPs showed confidence on their treatment, and indicated that they were of the opinion that western medicine does not heal the infection, while their treatment has shown its success in managing FUS. A respondent reported that:
“… They do use modern medicine, although doctors don’t really get rid of this infection in women. Only traditional medicine can help get rid of bilharzia…” THP20
They do believe that concurrent use of WM and TM is not wise so as to avoid uncontrollable side effects.
Theme 7. Knowledge of side effects and perceptions of efficacy of treatment provided by THPs
The THPs were asked if they knew anything about side effects experienced by women seeking treatment from them for FUS. They indicated that the treatment for FUS was helpful even though side effects could occur sometimes, depending on different factors and dosages. Half of the respondents (11/22; 50.0%) argued that there were side effects when using TM, while the other half (11/22; 50.0%) indicated the absence of significant side effects, which they contended were due to the non-respect of the prescribed dose. Some patients need to have quick results to stop the ongoing bleeding and relieve the pain and took more medication than was indicated, or they used it concurrently with conventional prescribed medicines. A respondent said:
“… Yes, there can be some side effects sometimes. It depends on a patient’s health. Some of my treatments can be dangerous if a patient is suffering severely from bilharzia, big quantities cause that, but we lower the dosage to avoid those effects…” THP15
The respondents reported that side effects could result from patients having diseases other than FUS that were also being treated by THPs. In the provision of care for FUS, they also treated other diseases to make sure that patients recovered fully, with a respondent reporting:
“.. It happens that when a person has bilharzia, he is also having other diseases, but if they manifest after a person has been treated and then I must deal with them too. So, my medicine does not give side effects…” THP20
Regarding the referral system, a respondent argued that in case of complications, he referred patients to healthcare facilities for follow-up when they were difficult to manage with his traditional treatment. He further stated that:
“… There is no side effect so far. But if there are side effects arising, I would treat them too. If I fail to do so I would take my patient to clinic…” THP22
With regards to side effects, others respondents argued that they have not had side effects appearing after giving treatment to women with FUS. From their experience, some of the side effects appearing in the course of the traditional treatment, such as constipation, were beneficial to the wellbeing of the women with FUS. One respondent stated that:
“… There are no side effects after taking the medicine of treating isichenene. The patient does not go to the toilet a lot and the urine changes back to its normal colour…” THP18
THPs said that it happened that patients were scared, that led them to try different healing processes from different THPs to fasten their wellbeing, which could impact negatively on their treatment. A respondent stated:
: “… Yes, sometime due to people having different spiritual lives (behaviour of using weather TM or WM with TM combined)…” THP7
Discussion
This exploratory study was an investigation on the knowledge, practices and experiences of THPs in managing one of the neglected tropical diseases, specifically female urogenital schistosomiasis, in women in the ILembe District, KwaZulu-Natal Province, South Africa. Little is known about the prevalence of schistosomiasis in this district over the last 20 years, with few studies having been conducted since the 1980s (Saathoff et al., 2004, WHO, 2011).
Theme 1. Source of Knowledge
The findings revealed that THPs received a call from their ancestors to join the healing practice, leading them to the initiation (Ukuthwasa), which is the training to become a THP. This has been documented in another study, which reported training to be a lengthy process of months to years’ duration (Mokgobi, 2013). Peek (Peek, 1991) reported that in African traditional healing, this training depended on the trainee’s learning skills.
Theme 2.Diagnostic of female urogenital schistosomiasis
Findings on the diagnostic of FUS showed that the THPs were not limited to cultural practices in this process, with symptoms widely known, such as a change in the color of urine to red, locally called urinate blood (ucama igazi), or the presence of blood in urine (haematuria), change of urine temperature, painful bladder and itching when urinating being reported as the main symptoms by THPs. Some relied on spiritual practices to confirm the diagnostic of the disease which occurred by throwing bones for spiritual divination (ukumhlola ngoko moya). The findings are consistent with other studies carried out with THPs in Mali, which reported that hematuria was the main symptom in urogenital schistosomiasis (Bah et al., 2006, Sylla, 1991). However, Cock et al. (Cock et al., 2018) reported that the FUS signs and symptoms can be unspecific and might be confused with other inflammatory diseases of the urinal tract.
Theme 3.Acceptability and affordability of treatment
The study showed that the THPs felt that traditional medicine was affordable and effective for whoever needed it, depending on the patients’ possibility and level of FUS infection. The THPs reported that they did not have a standard price for treatment and patients did not pay anything until after they had received their formulation. The finding on the cost of TM was supported by another study arguing that there was a need for regulation regarding appropriate costing of TM (Taba et al., 2016). The price varied from one healer to another, depending on the availability of the treatment and how it was collected or obtained by the THP. Treatment cost depended on where (distance, place) the medicinal products were collected and the ease of finding them. In their study, Mander et al. (Mander et al., 2007) found that the pricing of traditional product depended on the fact that several species were extinct in the wild due to their over-collection, which resulted in their being inaccessible to the TM industry. The THPs emphasized that they looked after their clients until the healing process had finished, and were open to easing the treatment process (confidence). In contrast, a study conducted in South Africa by Nxumalo et al. (Nxumalo et al., 2011) showed that three quarters of the poorest quintile spent more than 10% of their income on traditional medicine due to the lack of any regulations regarding the availability and costs medicinal plants. A policy protecting the community from excessive out-of-payments needs to be implemented from the parallel healthcare systems perspective.
Theme 4. Locally treatment used to manage FUS
Our findings reported that medicinal plants were the main source of treat FUS in rural areas of the ILembe District, and were used alone or in combination. The THPs felt that they had adequate knowledge about FUS symptoms as has been reported in other studies on managing schistosomiasis across Africa (Aremu et al., 2012, Bah et al., 2006, Cock et al., 2018, Hutchings, 1996, Maroyi, 2013, Muya et al., 2014, Sparg et al., 2000, Sylla, 1991). The twenty two plant species cited in this study belonged to fourteen families, with the Asteraceae and Hyacinthaceae being often cited. These findings are in line with a study conducted by Sparg et al. and Yineger et al. (Sparg et al., 2002, Yineger et al., 2013)on the anti-schistosomal activity of Hyacinthaceae and Asteraceae species.
In this study, more than two plant species were commonly combined in herbal treatment preparations, as such combined treatments worked better when taken according to THPs requirements. These findings are aligned with a study conducted in Pakistan by Adnan et al. (Adnan et al., 2014), which showed that the combination of herbal medicine can enhance their effect. Where plants were given in combination, Senecio serratuloides (Asteraceae) and Hypoxis hemerocallidea (Hypoxidaceae) were the two most frequently used species, as was reported by Naidoo et al. (Naidoo et al., 2013), their use for urinary tract infections being due to their antimicrobial properties.
The THPs outlined that the length of the management of FUS varied from one to three weeks, depending on whether or not the patients had taken the treatment as prescribed and not mixed it with other formulations without letting them know what they were taking. The successfulness of the treatment also depended on the THPs experience in managing FUS, these findings being consistent with a study by Zuma et al. (Zuma et al., 2016), which reported that THPs as knowledge holders played a key role in diseases management in rural South Africa. Details regarding the specifics of the treatment were not revealed by the THPs, the secrecy issue being a consequence of their fear that orthodox scientists or people not related to them would take their ideas, modifying and use them for commercial gain (Mokgobi, 2013), hence the need to protect their knowledge (Lazarus, 2006). Plants species reported in this study were documented previously in other studies (Aremu et al., 2015, Gould et al., 2015, Grace et al., 2008, Hutchings, 1996, Hutchings, 1989, Nkomo et al., 2010, Ojewole, 2006, Popat et al., 2001, Taylor and Van Staden, 2001) for being used in folk medicine to treat ailments.
Theme 5. Availability of TM treatment
It was reported that TM plants were widely used in FUS management, their treatment being obtained in “muti” market or collected in nature, depending on the THP experience and the plants availability. A study conducted by Chinsamy et al. (Chinsamy et al., 2011) found that medicinal plants used to manage diseases, including schistosomiasis, were traded on markets in different areas of South Africa. Some of them were bought from neighboring countries, such as Mozambique and Swaziland (Mander et al., 2007). A study conducted by Cock et al. (Cock et al., 2018) gave an overview of various medicinal plants that were available and used for managing schistosomiasis in the southern African region.
Theme 6. Concurrent use of TM with conventional orthodox medicine
This study found that the THPs were certain about the efficacy of TM used in FUS management in rural South Africa. However, some did acknowledge that inputs from HCPs might be useful to treat severe cases that they were unable to cure. Thus, collaboration between THPs and HCPs should be a reality for saving people lives. In their study, Zuma et al., (Zuma et al., 2016) showed that traditional medicine was known as the common treatment of people in rural areas of South Africa. The authors suggested further that it was important to identify the role played by THPs and HCPs in diseases management to improve the quality information on the disease and its management. This is in relation to the findings of a study by Stanifer et al. (Stanifer et al., 2015), which reported the importance of sharing information to improve patients’ quality of healthcare, avoid reports of medical non-compliance and adverse medical outcomes, and prevent poorer individual disease understanding. Reportedly, patients were treated first with TM and could only be sent in healthcare facilities when complications occurred, or where they could collect medication to complete the TM treatment. Studies conducted by Peltzer (Peltzer et al., 2010) and Nlooto and Naidoo (Nlooto et al., 2016) showed that the use of TM was prevalent even though medication were free in the South African public health care system. The concurrent use of conventional orthodox and traditional medicine could have an impact on treatment adherence, drug interaction and disease management outcomes, with the integration of TM and WM systems possibly improving the outcomes of managing neglected diseases.
Theme 7. Side effects and assessment of efficacy of medicines by THPs
This study findings reported that some side effects were perceived to be a good result of the treatment given to patients. These findings were similar to a study conducted in Limpopo Province in South Africa by Semenya and Potgieter (Semenya et al., 2014), which showed that side effects could be results of the TM effectiveness. However, comorbidities could lead to the appearance of other symptoms that were also being managed by THPs. In their study, Van Wyk et al. (Van Wyk et al., 2002) reported that experienced THPs had remedies to manage the side effects of TM. This study found that feedback from a patient not urinating blood but experiencing constipation were some signs of healing, while some patients were sent to modern facilities to establish if the disease had been cured. This correlate with Semenya and Potgieter (Semenya et al., 2014), who reporting that the validity of efficacy relied on reported positive feedback from the patient.
In line with our findings, THPs self-assessment of their TM efficacy was not taken seriously as a potential health issue within low- and middle-income countries, but could be very beneficial to local communities that relied on traditional treatment to manage infectious diseases (Cock et al., 2018). It was reported that side effects also depended the dosage being respected as prescribed, or by consulting various people instead of taking one treatment. Very little is known about the side effects of the use of medicinal plants for managing FUS, with Kamsu-Foguem and Foguem (Kamsu-Foguem and Foguem, 2014) reporting that adverse drugs reactions of TM were a consequence of an inappropriate preparation or use. In their study, Aremu et al. (Aremu et al., 2012) suggested that there was a need to undertake further evaluation on the plants toxicity to determine their safety.
Limitations of the Study
In light of the results findings, this study should be seen within its methodological context of THPs’ perceptions, knowledge and practices in managing FUS. In his study, Cock et al. (Cock et al., 2018) found that THPs played a key role in managing various infectious diseases in women. Purposive sampling method was used for this study whereby respondents were selected in regard to the fact that they have treated or were currently treating a patients with bilharzia condition. The sampling methods may have introduced a risk of bias, with purposive and snowball sampling being used due to the problems of identifying THPs who have managed FUS in women through the official organisation. The study was also conducted in one District in KZN, with the results possibly not being generalizable to other areas in the province or in the country, due to the variations in plant types across the affected areas. The occurrence of schistosomiasis is restricted to low lying areas along the eastern seaboard with eastward flowing rivers. The small sample size may have limited the variations in responses, but in the absence of other studies on the topic in South Africa, forms a bases for future research, the qualitative nature of the study providing sufficient details on which to build further qualitative and quantitative research.
Conclusion
THPs are playing a key role in managing FUS in rural areas of the ILembe district, and can diagnose FUS symptoms based on their knowledge and experience. Respondents indicated that while conventional treatment was readily available and free in public sector healthcare facilities, many women wanted to be treated with traditional remedies. Traditional herbal medicines were reportedly used by THPs to manage FUS in women and included Senecio serratuloides (Asteraceae), Hypoxis hemerocallidea (Hypoxidaceae), Tylophora flanaganii (Apocynaceae), Rhoicissus digitata (Vitaceae), Gunnera perpensa (Gunneraceae) and Eucomis autumnalis (Hyacinthaceae). The Asteraceae and Hyacinthaceae were the most cited by THPs as source of TM treatment. Very little is known by THPs about the side effects of using medicinal plants to manage FUS, however, with more research being needed, specifically as some women may take them concurrently with western medication. Further studies are needed to investigate the views and experiences of clients seen by THPs to establish their opinions about the effectiveness of the treatments used for FUS, and to thereby contribute to the larger body of research on the role of traditional medicines in the pursuit of keeping communities health.
Funding
This study has received no funding
Authors’ contributions
Conceptualization, A.G.-A.M. and M.N.; writing—original draft preparation, A.G.-A.M., and M.N.; writing—review and editing, A.G.-A.M., S.C.U., N.A.M.; M.G.R., T.W.M., M.K.G., B.S.A., K.B., H.M.K. and R.B.K. supervision, M.N. All authors have read and agreed to the published version of the manuscript.
Ethics approval and consent to participate
This study was approved by the Biomedical Research Ethics of the University of KwaZulu-Natal under reference BE477/17 and informed consents was sought from all participants. They agreed on the findings to be published to raise awareness on the contribution of traditional medicine in the management of FUS.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgment
The authors acknowledge the tremendous collaboration and support of the Indigenous Knowledge Holders and the Traditional Healers Organisation leaders in the ILembe District. AM received a stipend and running expenses from the College of Health Sciences. In addition, AM also got a stipend from DST/NRF, Centre in Indigenous Knowledge Systems of the University of KwaZulu-Natal. The authors are grateful to the following: Carrin Martin for the editing service of the final version of manuscript, Dr Gunilla Priebe and Dr Lina Magnussen (School of Epidemiology and Social Medicine, University of Gothenburg) for inputs conduction on qualitative studies.
Competing interests
The authors declare that they have no competing interests.
Author’s information
Aganze Gloire-Aimé Mushebenge is a PhD Candidate in the Discipline of Pharmaceutical Sciences, School of Health Sciences, Westville Campus, University of KwaZulu-Natal, P B X54001, Durban 4000, South Africa.
Consent for publication
Consents was sought from all participants to publish the outcome of the study in a peer-reviewed journal.
List of Abbreviations
ATM (African Traditional Medicine), FUS (Female Urogenital Schistosomiasis), HCP (Healthcare Professional), SD (Standard deviation), THP (Traditional Health Practitioner), TM (Traditional medicine), WHO (World Health Organization), WM (Western Medicine)
References
- ADNAN, M. , ULLAH, I., TARIQ, A., MURAD, W., AZIZULLAH, A., KHAN, A. L., ALI, N. J. J. O. E. & Ethnomedicine 2014. Ethnomedicine use in the war affected region of northwest Pakistan. 10, 16. [CrossRef]
- APESOA-VARANO, E. C. & HINTON, L. J. J. O. C.-C. G. 2013. The promise of mixed-methods for advancing Latino health research. 28, 267-282. [CrossRef]
- AREMU, A. , FINNIE, J. & VAN STADEN, J. J. S. A. J. O. B. 2012. Potential of South African medicinal plants used as anthelmintics–Their efficacy, safety concerns and reappraisal of current screening methods. 82, 134-150.
- AREMU, A. O. , MOYO, M., AMOO, S. O. & VAN STADEN, J. J. J. O. E. 2015. Ethnobotany, therapeutic value, phytochemistry and conservation status of Bowiea volubilis: A widely used bulbous plant in southern Africa. 174, 308-316. [CrossRef]
- BAH, S. , DIALLO, D., DEMBÉLÉ, S. & PAULSEN, B. S. J. J. O. E. 2006. Ethnopharmacological survey of plants used for the treatment of schistosomiasis in Niono District, Mali. 105, 387-399.
- BERGE, S. T. , KABATEREINE, N., GUNDERSEN, S. G., TAYLOR, M., KVALSVIG, J. D., MKHIZE-KWITSHANA, Z., JINABHAI, C., KJETLAND, E. F. J. S. A. J. O. E. & INFECTION 2011. Generic praziquantel in South Africa: the necessity for policy change to provide cheap, safe and effcacious schistosomiasis drugs for the poor, rural population. 26, 22-25. [CrossRef]
- BUWA, L. & VAN STADEN, J. J. J. O. E. 2006. Antibacterial and antifungal activity of traditional medicinal plants used against venereal diseases in South Africa. 103, 139-142.
- CHINSAMY, M. , FINNIE, J. & VAN STADEN, J. J. S. A. J. O. B. 2011. The ethnobotany of South African medicinal orchids. 77, 2-9.
- CHRISTENSEN, M. J. J. O. N. E. & PRACTICE 2017. The empirical-phenomenological research framework: Reflecting on its use. 7, 81. [CrossRef]
- CHRISTINET, V. , LAZDINS-HELDS, J. K., STOTHARD, J. R. & REINHARD-RUPP, J. J. I. J. F. P. 2016. Female genital schistosomiasis (FGS): from case reports to a call for concerted action against this neglected gynaecological disease. 46, 395-404. [CrossRef]
- COCK, I. , SELESHO, M. & VAN VUUREN, S. J. J. O. E. 2018. A review of the traditional use of southern African medicinal plants for the treatment of selected parasite infections affecting humans.
- COLLEY, D. G. , BUSTINDUY, A. L., SECOR, W. E. & KING, C. H. J. T. L. 2014. Human schistosomiasis. 383, 2253-2264.
- CRESWELL, J. W. 2009. Research designs: Qualitative, quantitative, and mixed methods approaches. Thousand Oaks, CA: Sage Publications.
- CROUCHER, S. M. & CRONN-MILLS, D. 2014. Understanding communication research methods: A theoretical and practical approach, Routledge.
- DE WET, H. , NZAMA, V. & VAN VUUREN, S. J. S. A. J. O. B. 2012. Medicinal plants used for the treatment of sexually transmitted infections by lay people in northern Maputaland, KwaZulu–Natal Province, South Africa. 78, 12-20.
- FENWICK, A. , WEBSTER, J. P., BOSQUE-OLIVA, E., BLAIR, L., FLEMING, F., ZHANG, Y., GARBA, A., STOTHARD, J., GABRIELLI, A. F. & CLEMENTS, A. J. P. 2009. The Schistosomiasis Control Initiative (SCI): rationale, development and implementation from 2002–2008. 136, 1719-1730. [CrossRef]
- GIORGI, A. J. J. O. P. P. 2012. The descriptive phenomenological psychological method. 43, 3-12. [CrossRef]
- GOULD, A. , PENNY, C., PATEL, C. & CANDY, G. J. S. A. J. O. B. 2015. Enhanced cutaneous wound healing by Senecio serratuloides (Asteraceae/Compositae) in a pig model. 100, 63-68. [CrossRef]
- GRACE, O. , SIMMONDS, M., SMITH, G. & VAN WYK, A. J. J. O. E. 2008. Therapeutic uses of Aloe L.(Asphodelaceae) in southern Africa. 119, 604-614. [CrossRef]
- GURARIE, D. , LO, N. C., NDEFFO-MBAH, M. L., DURHAM, D. P. & KING, C. H. J. P. N. T. D. 2018. The human-snail transmission environment shapes long term schistosomiasis control outcomes: Implications for improving the accuracy of predictive modeling. 12, e0006514. [CrossRef]
- HAO, D.-C. , GU, X. & XIAO, P. J. A. P. S. B. 2017. Anemone medicinal plants: ethnopharmacology, phytochemistry and biology. 7, 146-158. [CrossRef]
- HUTCHINGS, A. 1996. Zulu medicinal plants: An inventory, University of Natal press.
- HUTCHINGS, A. J. B. 1989. A survey and analysis of traditional medicinal plants as used by the Zulu; Xhosa and Sotho. 19, 112-123. [CrossRef]
- IBTISSEM, B. , ABDELLY, C. & SFAR, S. J. A. C. E. S. 2012. Antioxidant and antibacterial properties of Mesembryanthemum crystallinum and Carpobrotus edulis extracts. 2, 359–365. [CrossRef]
- KAMSU-FOGUEM, B. & FOGUEM, C. J. I. M. R. 2014. Adverse drug reactions in some African herbal medicine: literature review and stakeholders’ interview. 3, 126-132. [CrossRef]
- KODURU, S. , GRIERSON, D. & AFOLAYAN, A. J. P. B. 2006. Antimicrobial Activity of Solanum aculeastrum. 44, 283-286. [CrossRef]
- KOENEN, E. V. 2001. Medicinal, poisonous, and edible plants in Namibia, Klaus hess publishers.
- KOMAPE, N. P. M. , ADEROGBA, M., BAGLA, V. P., MASOKO, P., ELOFF, J. N. J. A. J. O. T., COMPLEMENTARY & MEDICINES, A. 2014. Anti-bacterial and anti-oxidant activities of leaf extracts of Combretum vendee (combretecacea) and the isolation of an anti-bacterial compound. 11, 73-77. [CrossRef]
- KRIPPENDORFF, K. J. H. C. R. 2004. Reliability in content analysis: Some common misconceptions and recommendations. 30, 411-433. [CrossRef]
- KUCKARTZ, U. 2012. Qualitative Inhaltsanalyse: Methoden, Praxis, Computerunterstützung, Beltz Juventa.
- LAZARUS, R. S. 2006. Stress and emotion: A new synthesis, Springer Publishing Company.
- LINCOLN, Y. S. & GUBA, E. G. 1985. Naturalistic inquiry. Beverley Hills. ca: sage.
- MAGAISA, K. , TAYLOR, M., KJETLAND, E. F. & NAIDOO, P. J. J. S. A. J. O. S. 2015. A review of the control of schistosomiasis in South Africa. 111, 1-6. [CrossRef]
- MANDER, M. , NTULI, L., DIEDERICHS, N. & MAVUNDLA, K. J. S. A. H. R. 2007. Economics of the traditional medicine trade in South Africa: health care delivery. 2007, 189-196.
- MANGOYI, R. , MUKANGANYAMA, S. J. T. A. J. O. P. S. & BIOTECHNOLOGY 2011. In vitro antifungal activities of selected medicinal plants from Zimbabwe against Candida albicans and Candida krusei. 5, 1-7.
- MAROYI, A. J. J. O. E. 2013. Traditional use of medicinal plants in south-central Zimbabwe: review and perspectives. J Journal of ethnobiology andethnomedicine, 9, 31. [CrossRef]
- MARSHALL, M. N. J. B. 1998. Qualitative study of educational interaction between general practitioners and specialists. 316, 442-445. [CrossRef]
- MAYRING, P. 2015. Qualitative content analysis: Theoretical background and procedures. Approaches to qualitative research in mathematics education. Springer. [CrossRef]
- MOKGOBI, M. J. A. J. F. P. H. E., RECREATION, 2013. Towards integration of traditional healing and western healing: Is this a remote possibility? J African journal for physical health education, recreation,dance, 2013, 47.
- MOKOKA, T. A., MCGAW, L. J., MDEE, L. K., BAGLA, V. P., IWALEWA, E. O., ELOFF, J. N. J. B. C. & MEDICINE, A. 2013. Antimicrobial activity and cytotoxicity of triterpenes isolated from leaves of Maytenus undata (Celastraceae). 13, 111. [CrossRef]
- MUYA, K. , TSHOTO, K., CIOCI, C., ASEHO, M., KALONJI, M., BYANGA, K., KALONDA, E. & SIMBI, L. J. P. 2014. Survol ethnobotanique de quelques plantes utilisées contre la schistosomiase urogénitale à Lubumbashi et environs. 12, 213-228.
- NAIDOO, D. , VAN VUUREN, S., VAN ZYL, R. & DE WET, H. J. J. O. E. 2013. Plants traditionally used individually and in combination to treat sexually transmitted infections in northern Maputaland, South Africa: antimicrobial activity and cytotoxicity. 149, 656-667.
- NKOMO, M. , NKEH-CHUNGAG, B. N., KAMBIZI, L., NDEBIA, E. J., IPUTO, J. E. J. A. J. O. P. & PHARMACOLOGY 2010. Antinociceptive and anti-inflammatory properties of Gunnera perpensa (Gunneraceae). 4, 263-269.
- NLOOTO, M. , NAIDOO, P. J. B. C. & MEDICINE, A. 2016. Traditional, complementary and alternative medicine use by HIV patients a decade after public sector antiretroviral therapy roll out in South Africa: a cross sectional study. 16, 128. [CrossRef]
- NXUMALO, N. , ALABA, O., HARRIS, B., CHERSICH, M. & GOUDGE, J. J. J. O. P. H. P. 2011. Utilization of traditional healers in South Africa and costs to patients: findings from a national household survey. 32, S124-S136. [CrossRef]
- OJEWOLE, J. A. J. J. O. E. 2006. Antinociceptive, anti-inflammatory and antidiabetic properties of Hypoxis hemerocallidea Fisch. & CA Mey.(Hypoxidaceae) corm [‘African Potato’] aqueous extract in mice and rats. 103, 126-134. [CrossRef]
- PATTON, M. Q. 1990. Qualitative evaluation and research methods, SAGE Publications, inc.
- PEEK, P. M. 1991. African divination systems: Ways of knowing, Georgetown University Press.
- PELTZER, K. , FRIEND-DU PREEZ, N., RAMLAGAN, S., FOMUNDAM, H., ANDERSON, J. J. A. J. O. T., COMPLEMENTARY & MEDICINES, A. 2010. Traditional complementary and alternative medicine and antiretroviral treatment adherence among HIV patients in Kwazulu-Natal, South Africa. 7.
- POGGENSEE, G. , FELDMEIER, H. & KRANTZ, I. J. P. T. 1999. Schistosomiasis of the female genital tract: public health aspects. 15, 378-381. [CrossRef]
- POOLEY, B. J. D. N. F. P. T. P.-C. I. I. X. E. I., MAPS. GEOG 1998. A field guide to wild flowers of KwaZulu-Natal and the eastern region. 5.
- POPAT, A. , SHEAR, N. H., MALKIEWICZ, I., STEWART, M. J., STEENKAMP, V., THOMSON, S. & NEUMAN, M. G. J. C. B. 2001. The toxicity of Callilepis laureola, a South African traditional herbal medicine. 34, 229-236. [CrossRef]
- REIDPATH, D. D. , ALLOTEY, P., POKHREL, S. J. H. R. P. & SYSTEMS 2011. Social sciences research in neglected tropical diseases 2: A bibliographic analysis. 9, 1. [CrossRef]
- SAATHOFF, E. , OLSEN, A., MAGNUSSEN, P., KVALSVIG, J. D., BECKER, W. & APPLETON, C. C. J. B. I. D. 2004. Patterns of Schistosoma haematobium infection, impact of praziquantel treatment and re-infection after treatment in a cohort of schoolchildren from rural KwaZulu-Natal/South Africa. 4, 40.
- SEMENYA, S. S. , POTGIETER, M. J. J. J. O. E. & ETHNOMEDICINE 2014. Bapedi traditional healers in the Limpopo Province, South Africa: their socio-cultural profile and traditional healing practice. 10, 4. [CrossRef]
- SPARG, S. , VAN STADEN, J. & JÄGER, A. J. J. O. E. 2000. Efficiency of traditionally used South African plants against schistosomiasis. 73, 209-214. [CrossRef]
- SPARG, S. , VAN STADEN, J. & JÄGER, A. J. J. O. E. 2002. Pharmacological and phytochemical screening of two Hyacinthaceae species: Scilla natalensis and Ledebouria ovatifolia. 80, 95-101. [CrossRef]
- STANIFER, J. W. , PATEL, U. D., KARIA, F., THIELMAN, N., MARO, V., SHIMBI, D., KILAWEH, H., LAZARO, M., MATEMU, O. & OMOLO, J. J. P. O. 2015. The determinants of traditional medicine use in northern Tanzania: a mixed-methods study. 10, e0122638. [CrossRef]
- SYLLA, A. J. S. D. P. , ECOLE NATIONALE DE MÉDECINE ET DE PHARMACIE DU MALI, BAMAKO 1991. Contributiona l’inventaire des Antibilharziens et Molluscicides Traditionnels dans le cercle de Kayes.
- TABA, M. , FAKOYA, M. J. J. O. A. & MANAGEMENT 2016. COST ACCOUNTING PRACTICES IN AFRICAN TRADITIONAL HEALING: A CASE STUDY OF MAKHUDUTHAMAGA TRADITIONAL HEALERS IN SOUTH AFRICA. 6, 75-88.
- TAYLOR, J. & VAN STADEN, J. J. P. G. R. 2001. The effect of age, season and growth conditions on anti-inflammatory activity in Eucomis autumnalis (Mill.) Chitt. Plant extracts. 34, 39-47.
- VAN WYK, B.-E., HEERDEN, F. V. & OUDTSHOORN, B. V. 2002. Poisonous plants of South Africa, Briza Publications.
- VIGNERON, M. , DEPARIS, X., DEHARO, E. & BOURDY, G. J. J. O. E. 2005. Antimalarial remedies in French Guiana: a knowledge attitudes and practices study. 98, 351-360. [CrossRef]
- WATT, J. M. , BREYER-BRANDWIJK, M. G. J. T. M., SOUTHERN, P. P. O., MEDICINAL, E. A. B. A. A. O. T., OTHER USES, C. C., PHARMACOLOGICAL EFFECTS, MAN, T. I. & ANIMAL. 1962. The Medicinal and Poisonous Plants of Southern and Eastern Africa being an Account of their Medicinal and other Uses, Chemical Composition, Pharmacological Effects and Toxicology in Man and Animal.
- WHO, W. H. O. 2011. Helminth control in school-age children: a guide for managers of control programmes, Geneva: World Health Organization.
- WHO, W. H. O. 2015. Investing to overcome the global impact of neglected tropical diseases: third WHO report on neglected tropical diseases 2015, World Health Organization.
- WHO, W. H. O. 2018. Schistosomiasis, Fact Sheet No 115. Available at http://www. who. int/mediacentre/factsheets/fs115/en. Last accessed on 12 December 2018, 12 December.
- YINEGER, H. , KELBESSA, E., BEKELE, T. & LULEKAL, E. J. J. O. M. P. R. 2013. Plants used in traditional management of human ailments at Bale Mountains National Park, Southeastern Ethiopia. 2, 132-153.
- ZUMA, T. , WIGHT, D., ROCHAT, T., MOSHABELA, M. J. B. C. & MEDICINE, A. 2016. The role of traditional health practitioners in Rural KwaZulu-Natal, South Africa: generic or mode specific? 16, 304.
Figure 1.
The four sub-districts of the Ilembe district municipality (http: //www.kznonline.gov.za/index.qphp/government/2016-08-02-09-42-02/ilembe-district-municipality).
Figure 1.
The four sub-districts of the Ilembe district municipality (http: //www.kznonline.gov.za/index.qphp/government/2016-08-02-09-42-02/ilembe-district-municipality).
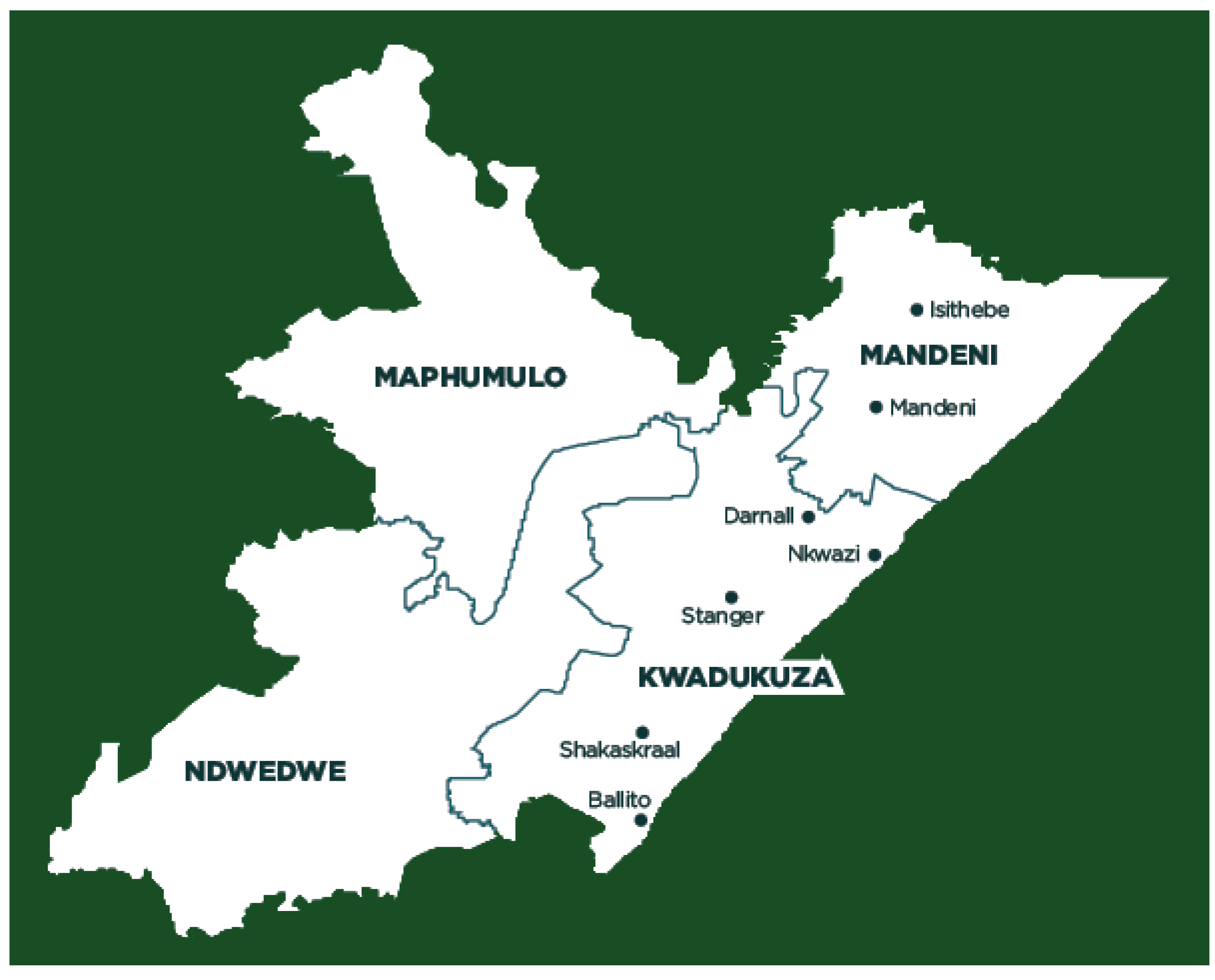

Table 1.
Respondents’ background characteristics.
| Variables | Category | No. | % | Proportion (95% Confidence interval) |
|---|---|---|---|---|
|
Gender |
Female Male |
14 | 63.6 | 40.7 – 82.8 |
| 8 | 36.4 | 17.2 – 59.3 | ||
|
Marital status |
Married Not married |
14 | 63.6 | 40.7 – 82.8 |
| 8 | 36.4 | 17.2 – 59.3 | ||
| Level of Education | High School completed None specified Prim. School completed Postsecondary certificate Degree |
10 | 45.5 | 24.4 – 67.8 |
| 7 | 31.8 | 13.9 – 54.9 | ||
| 3 | 13.6 | 2.9 -34.9 | ||
| 1 | 4.5 | 0.1 – 22.8 | ||
| 1 | 4.5 | 0.12 – 22.8 | ||
|
Profession |
Diviner (Sangoma) Both (Sangoma/Inyanga) Herbalist (Inyanga) |
17 | 77.2 | 54,6 - 92,2 |
| 3 | 13.6 | 2,9 – 34,9 | ||
| 2 | 9.1 | 1.1 – 29.2 | ||
|
Religion |
Christian Traditional religion Hinduism None specified |
15 | 68.2 | 45.1 – 86.1 |
| 5 | 22.7 | 7.8 – 45.4 | ||
| 1 | 4.5 | 0.1 – 22.8 | ||
| 1 | 4.5 | 0.1 – 22.8 | ||
| Mean years of work experience, SD: 13 (10.170) Age (years) Mean age, SD, Range: 41.05 (13.075), 26 – 70 | ||||
Table 2.
Traditional treatments used individually or in combination to manage FUS.
| Botanical name | Family |
isiZulu (Z)/isiXhosa (X), Tshivenda (V) vernacular name (s) given by interviewees | Number of times quoted by THPs | Previous report of ethnomedical uses (reference) |
|---|---|---|---|---|
| Adenostemma caffrum DC. | Asteraceae | Umahogo (Z) | 1 | Used as love charm and for influenza. The infusion is taken as an emetic given to children as enemas (Hutchings, 1996). |
| Albuca fastigiata Dryand. | Hyacinthaceae | uMaphipha (Z) | 1 | Traditionally used as emetics for protection against sorcery and as general protective charms (Pooley, 1998). |
|
Aloe marlothii A.Berger/ Aloe ferox Mill. |
Asphodelaceae | iNhlaba, uMhlaba (Z) | 2 | Used in southern African for infections, particularly sexually transmitted infections and internal parasites, genito-urinary system, , injuries, digestion, pregnancy, skin complaints, sensory system, inflammation, pain, respiratory system, muscular–skeletal system, nutrition (Grace et al., 2008). |
|
Anemone fanninii Harv. ex Mast. |
Ranunculaceae | Emyama/ nManzamnyama (Z) | 1 | The plant has antitumor, antimicrobial, anti-inflammatory, sedative, analgesic activities, anti-convulsant and anti-histamine effects (Hao et al., 2017). |
|
Bowiea volubilis Harv. Ex Hook.f. subsp. volubilis |
Hyacinthaceae | UGibisisila or uGibisila; iguleni (Z); uMgaqana (X) | 2 | Plant widely used against numerous ailments including headache, muscular pains, infertility, cystitis and venereal diseases in southern Africa (Aremu et al., 2015). |
|
Callilepis laureola DC. |
Asteraceae | Amafuthomhlaba, ihlamvu, impila (Z) | 2 | Used for stomach problems, tape worm infestations, impotence, cough, and to induce fertility. Impila is also administered to pregnant women by traditional birth attendants to “ensure the health of the mother and child” and to facilitate labor. It is also taken by young girls in the early stages of menstruation (Popat et al., 2001). |
| Carpobrotus edulis (L.) L.Bolus | Mesembryanthemaceae (Aizoaceae) | mthombozi/Umgongozi (Z) | 1 | The plant is used in soothing itching caused by spider and tick bites. It contains astringent antiseptic juice which can be taken orally for treating sore throat and mouth infections. It has a antimicrobial activity (Ibtissem et al., 2012) |
| Combretum erythrophyllum (Burch.) Sond. | Combretaceae |
Umdubu (Z) | 1 | Used for the treatment of abdominal pains and venereal diseases due to antibacterial compounds in the leaves (Hutchings, 1996). |
| Combretum vendae A.E.van Wyk | Combretaceae | Gopo (gopo-gopo, gopokopo-bani (V). | 1 | Used for the treatment of bacterial related infections and oxidative related diseases by indigenous people of South Africa (Komape et al., 2014). |
| Eucomis autumnalis (Mill.) Chitt. | Hyacinthaceae | uBuhlungu eSimathunzi (X), uMathunga (Z) | 4 | Greatly valued in traditional medicine for the treatment of a variety of ailments, predominantly those involving pain, fever and inflammation (Taylor and Van Staden, 2001). |
|
Gunnera perpensa L. |
Gunneraceae | iPhuzi lomlambo, iGhobo (X); uGobhe, uGobho (Z) |
4 | Used in folk medicine to relieve rheumatoid pain, facilitate childbirth and healing wounds. Zulu traditional healers use it to induce labor, expel the placenta after birth and to relief menstrual pains (Nkomo et al., 2010). |
|
Hypoxis hemerocallidea Fisch., C.A.Mey. & Avé-Lall. |
Hypoxidaceae | iNkomfe (Z), iLabatheka (Xhosa) | 5 | Southern African ‘wonder’ plant medicine being claimed to be an effective remedy against HIV/AIDS-related diseases, arthritis, yuppie flu, hypertension, diabetes mellitus, cancer, psoriasis, gastric and duodenal ulcers, tuberculosis, urinary tract infections, asthma, and some central nervous system (CNS) disorders, especially epilepsy and childhood convulsions (Ojewole, 2006). |
| Knowltonia bracteata Harv. ex J.Zahlbr. | Ranunculaceae | nguthuza or uMvuthuza (Z) | 1 | Used for sexually transmitted diseases (Buwa and Van Staden, 2006). |
| Maytenus undata (Thunb.) Blakelock | Celastraceae | Undubula /iNdabulaluvalo (Z) | 2 | Widely used in folk medicine as anti-tumour, anti-asthmatic, analgesic, anti-inflammatory, antimicrobial and anti-ulcer agents, and as a treatment for stomach problems (Mokoka et al., 2013). |
|
Myrothamnus flabellifolius Welw. |
Myrothamnaceae | uVuka kwa bafile (Z) | 2 | Used for respiratory ailments, nosebleeds and fainting, alleviate backache, kidney problems, haemorrhoids and menstrual pains, abrasions , dressings for burns and wounds, chest pains and asthma, treat infections and pains in the uterus. In central Africa it is used as a tonic and to treat breast complaints. Shona healers have used the plant to treat epilepsy, madness and coughs (Van Wyk et al., 2002). |
| Nidorella Sp. Schimper, G.W. | Asteraceae | uMhlabelo | 2 | Useful in embrocation for fractures, sprains and snakebites (Hutchings, 1996). |
| Ranunculus multifidus Forssk, | Ranunculaceae | Uxhaphozi (Z) | 1 | It used for sexually transmitted infections (De Wet et al., 2012) |
| Rhoicissus sp. Wild & R.B.Drumm), | Vitaceae | iSinwazi (Z) | 4 | Medicinal plants used to treat burns, swelling and malaria, one can expect that they might possess anti-microbial and anti-inflammatory activities as well (Hutchings, 1996). |
| Sclerocarya birrea (A.Rich.) Hochst. | Anacardiaceae | umGanu (Z) | 1 | It is used in treating proctitis. The Vhavenda use it to treat fevers, stomach ailments and ulcers and for many purposes including sore eyes in Zimbabwe. In East Africa, it is an ingredient in an alcoholic medicine taken to treat an internal ailment known as kati, it is used for stomach disorders. The Hausas in West Africa use it as a remedy for dysentery. It could show that extracts inhibit diarrhoea in mice (Mokoka et al., 2013). |
|
Senecio serratuloides var. gracilis Harv., |
Asteraceae | uNsukumbili (Z) | 7 | Traditional herbal remedy used to treat skin wounds in South Africa (Gould et al., 2015). |
| Solanum aculeastrum Dunal subsp. aculeastrum | Solanaceae | Imbuna/iNtuma and water |
1 | Plant used in traditional medicine to treat various human and animal diseases, specifically stomach disorders and various cancers, in the Eastern Cape, South Africa (Koduru et al., 2006). |
| Tylophora flanaganii Schltr. | Apocynaceae | iNhlanhlemhlophe (iNhlanhla) (Z) | 4 | It is taken in Asia and Africa for allergies, asthma, cancer, congestion, constipation, cough, inflamed skin, diarrhoea, bloody diarrhoea, gas, haemorrhoids, tender joints (gout), yellowed skin (jaundice), joint disorder (rheumatoid arthritis), whooping cough, to make someone vomit, and to cause sweating (Hutchings, 1989). |
THPs reported that the treatment period may vary from one to three weeks depending on the patient condition. *Botanical names of the following local plants were not found. They are as follows: Igwalagwala, Impizo, Ukuse kukleneke, Isinya, Imbizani, Iqabunga, Impande/Oyimpande, Oyilitshe, Cigunzi, Umopho and Indonye.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



