
Submitted:
20 March 2024
Posted:
20 March 2024
You are already at the latest version
Abstract
Rectal cancer presents a significant burden globally, often requiring multimodal therapy for locally advanced cases. Long-course chemoradiotherapy (LCRT) and short-course radiotherapy (SCRT) followed by surgery have been conventional neoadjuvant approaches. Recent trials favor LCRT due to improved local control. However, tumor distant recurrence remains a concern, prompting exploration of Total Neoadjuvant Therapy (TNT) as a comprehensive treatment strat-egy. Immune checkpoint inhibitors (ICIs) show promise, particularly in mismatch repair-deficient (dMMR) or microsatellite instability-high (MSI-H) tumors, potentially revolutionizing neoadjuvant regimens. Non-operative management (NOM) represents a viable alternative post-neoadjuvant therapy for selected patients achieving clinical complete response (cCR). Additionally, monitoring minimal residual disease (MRD) using circulating tumor DNA (ctDNA) emerges as a non-invasive method for treatment response assessment. This review synthesizes current evidence on TNT, ICIs, NOM and ctDNA, elucidating their implications for rectal cancer management and highlighting avenues for future research and clinical application.
Keywords:
rectal cancer
; total neoadjuvant treatment
; immunocheckpoint inhibitors
; nonoperative management
; ctDNA.
1. Introduction
Colorectal cancer is the third most frequently diagnosed cancer globally, with rectal cancer accounting for approximately 31% of cases. Among patients with rectal cancer, 5 to 10% present with locally advanced disease (i.e. stage II-III) at the time of diagnosis. The standard approach for managing such cases involves multimodal therapy, combining radiotherapy, chemotherapy, and surgery [1,2,3]. For years, long-course chemoradiotherapy (LCRT) and short-course radiotherapy (SCRT), followed by total mesorectal excision (TME) surgery, have emerged as the mainstay neoadjuvant treatments for locally advanced rectal cancer (LARC) [4,5].
Evidence from the CAO/ARO/AIO-94 trial has established the superiority of preoperative LCRT over postoperative chemoradiotherapy in terms of local control, highlighting a 5-year cumulative incidence of local recurrence (LR) of 6% in the preoperative versus 13% in the postoperative arm [6]. Similarly, several studies have affirmed the efficacy of SCRT in reducing the risk of LR [7,8,9,10,11]. Despite randomized studies indicating comparable survival, local control, and late toxicity outcomes between LCRT and SCRT, the latter is associated with a clear reduction in complete pathological responses (pCR), along with an increase in circumferential margin infiltration and LR. Therefore, while acknowledging the advantages of SCRT in terms of economic health and quality of life, the preference for LCRT prevails in cases where achieving a pCR is of utmost importance, as recommended by both clinical practice and international guidelines [12,13].
Despite these recommendations, a substantial proportion of patients (25% to 30% at 5 years) experience tumor distant recurrence. Given the debatable role of adjuvant chemotherapy [14,15,16], a compelling alternative has emerged – administering all systemic treatment before surgery. The introduction of Total Neoadjuvant Therapy (TNT), involving upfront chemotherapy followed or preceded by either LCRT or SCRT, has ushered in a recent paradigm shift in managing LARC [17]. Additionally, the incorporation of immune checkpoint inhibitors (ICIs) in the neoadjuvant treatment paradigm for LARC has emerged as a promising avenue in recent oncological research, especially in mismatch repair-deficient (dMMR) or microsatellite instability-high (MSI-H) tumors [18].
Nonoperative management (NOM) is a viable option for selected rectal cancer patients achieving a clinical complete response (cCR) post-neoadjuvant treatment. It involves active surveillance over immediate surgery, ensuring close monitoring for regrowth.
Monitoring minimal residual disease (MRD) in LARC is crucial for assessing treatment efficacy and predicting the risk of recurrence. In this context, circulating tumor DNA (ctDNA) has garnered increasing interest as a potential biomarker for MRD. The presence and quantity of ctDNA may reflect residual tumor burden following neoadjuvant and surgical treatments. Therefore, ctDNA analysis holds promise as a non-invasive strategy for monitoring MRD in LARC, enabling more personalized and timely management of patients post-treatment [19].
This review aims to delve into the latest evidence regarding the utilization of TNT, ICIs, ctDNA, and NOM strategies in LARC. Through a comprehensive analysis of these topics, we aim to provide a thorough understanding of the new frontiers in LARC management, with particular emphasis on the potential clinical and therapeutic implications of these innovations (Figure 1).
2. Total Neoadjuvant Treatment (TNT)
2.1. Results of Phase III Trials
The introduction of LCRT in the management of LARC, followed by rectal resection with TME, has significantly reduced LR without a corresponding improvement in the rate of distant metastases, which remains at about 25-30%. Due to poor tolerance to adjuvant chemotherapy in this setting, different strategies of TNT have been explored in recent years through clinical trials. TNT is an alternative multimodal strategy aimed at intensifying preoperative treatment by delivering both radiotherapy and chemotherapy before surgery. This approach offers several theoretical advantages, including early treatment of micrometastatic disease and better compliance with chemotherapy compared to adjuvant treatment, albeit with the potential risk of overtreatment in some patients. In particular, two distinct approaches have emerged from several phase II and III trials: induction chemotherapy followed by LCRT, and LCRT or SCRT followed by consolidation chemotherapy. Recently, the results of three phase III trials, namely PRODIGE-23, RAPIDO, and STELLAR, comparing different TNT strategies to standard LCRT have been published (Table 1).
The PRODIGE-23 trial evaluated an induction TNT strategy, including chemotherapy with the mFOLFIRINOX regimen (5-fluorouracil, irinotecan, and oxaliplatin) for 3 months, followed by LCRT, surgery, and 3 months of adjuvant mFOLFOX (5-fluorouracil and oxaliplatin) or capecitabine, compared to standard LCRT and adjuvant treatment for 6 months. The study randomized 461 patients with LARC (cT3/cT4). The primary endpoint of the trial was disease-free survival (DFS), while toxicity, pCR, metastasis-free survival (MFS), overall survival (OS), and quality of life represented secondary endpoints [20]. The study met its primary endpoint with an improved 3-year DFS in patients treated with TNT compared to standard treatment (76% vs 69%, p = 0.034). The experimental arm also showed an increase in 3-year MFS (HR 0.69, 95% CI 0.54–0.90; p = 0.0048) and an increased rate of pCR (27.8% for TNT vs. 12.1% for standard treatment, p < 0.001) [20]. Regarding compliance, a total of 92% of the patients in the TNT group received all the planned six cycles of mFOLFIRINOX. The overall incidence of grade 3-4 adverse events (AEs) in patients in the experimental arm was 46%, comparable to what was observed in the control arm, with neutropenia and diarrhea as the most frequent AEs. Updated results after a median follow-up of 7 years were presented at ASCO 2023. The benefit in DFS was maintained with a median DFS of 67.6% in the TNT arm vs. 62.5% in the control arm. An increase in MFS, cancer-specific survival, and OS was also reported, with a 5-year OS rate of 81.9% vs. 76.1% [21].
The RAPIDO trial investigated a consolidation TNT approach, which consisted of SCRT followed by chemotherapy (six cycles of CAPOX or nine cycles of FOLFOX) and TME, compared to standard LCRT. The study randomized 912 patients with high-risk stage II and III rectal cancer, defined as having at least one of the following criteria at MRI staging: cT4a, cT4b, extramural vascular invasion, cN2 (metastasis in four or more locoregional lymph nodes), involved mesorectal fascia, or enlarged lateral lymph nodes [22]. The primary endpoint was 3-year disease-related treatment failure (DrTF), which included LR, distant metastasis, new primary colon tumor, or treatment-related death, while secondary endpoints included pCR, locoregional failure, OS, and safety [22]. The TNT experimental arm demonstrated an improved DrTF rate compared to the control arm (23.7% vs. 30.4%, HR = 0.75; p = 0.019) and also reached secondary endpoints with a doubled pCR rate (28.4% vs. 14.3%) and a lower rate of distant metastases (20.0% vs. 26.8%, p = 0.005). However, despite the observed increase in pCR, locoregional failures in the experimental group were non-significantly higher than in the standard of care group (8.3% vs. 6.0%; p = 0.12). Regarding safety, Grade 3 or higher adverse events during preoperative treatment occurred in 48% of patients in the experimental group, compared with 25% in the standard of care group, where 34% of G3-4 AEs were observed during adjuvant treatment. Despite the positive results, the RAPIDO trial has some limitations that should be considered. Notwithstanding the observed increase in pCR, LR in the experimental group were numerically higher than in the standard of care group (8.3% vs. 6.0%; p = 0.12) in the initial report, while a recent update of trial results with longer follow-up [23] showed a significantly increased LR rate in the TNT arm compared with the standard of care (12% vs. 8% respectively, p = 0.007). This finding suggests that consolidation chemotherapy cannot compensate for a suboptimal radiotherapy strategy in patients with high-risk features in terms of local control of disease. Another concern is related to the optional adjuvant therapy planned by the study in the control arm and administered only in 47% of resected patients, thus making the control arm not an adequate comparator.
The phase III STELLAR trial evaluated a TNT strategy similar to RAPIDO, with patients randomized to SCRT followed by consolidation chemotherapy with four cycles of XELOX, surgery, and two post-operative cycles of XELOX, versus standard LCRT and adjuvant chemotherapy with six cycles of XELOX [24]. The study demonstrated non-inferiority for the primary endpoint, 3-year DFS, in patients receiving TNT versus standard LCRT (64.5% vs. 62.3%, respectively; P < 0.001 for non-inferiority). Interestingly, the three-year OS was superior, at 86.5% (95% CI, 82.1 to 90.8), in the TNT group compared with 75.1% (95% CI, 69.4 to 80.8) in the LCRT group (HR = 0.67, 95% CI, 0.46 to 0.97; log-rank, P = .033), while no significant difference in MFS or LR rate between the groups was observed. Even though the compliance rate was high in the experimental arm, TNT was associated with a significant increase in the rate of grade 3-4 toxicity (26.5% vs. 12.6%; P < 0.001) and with a lower completion rate (82.6% vs. 95.2%) compared to LCRT.
2.2. Omission of Radiotherapy
Pelvic radiation has traditionally played a leading role in the neoadjuvant treatment of LARC, either alone or in combination with chemotherapy, and has allowed a significant reduction in the LR rate. However, its short-term and long-term toxic effects, particularly concerning bowel and sexual function, together with improvements in systemic chemotherapy, have recently called its role into question.
In the phase III Chinese FOWARC trial, 495 LARC patients were randomly assigned to neoadjuvant treatment with 5-Fluorouracil plus radiotherapy, mFOLFOX6 plus radiotherapy, or mFOLFOX6 alone [25]. The primary endpoint of the study, three-year DFS, was 72.9%, 77.2%, and 73.5% respectively (p= 0.709). No significant difference was observed in terms of LR rate or OS, thus the study failed to demonstrate an improvement in DFS with the use of FOLFOX. Nevertheless, the lack of a significant difference in outcomes between mFOLFOX6 without radiotherapy and 5-Fluorouracil with radiotherapy was intriguing and suggested further investigation of this strategy.
Recently, the phase III non-inferiority PROSPECT trial assessed an alternative strategy of neoadjuvant treatment with FOLFOX and selective use of LCRT reserved for patients whose tumors responded poorly [26]. The study included 1128 patients with rectal cancer staged as T2N+, T3N0, or T3N+ who were randomized between standard preoperative LCRT or an experimental arm of neoadjuvant chemotherapy with FOLFOX for 6 cycles, with LCRT given only if the primary tumor decreased in size by less than 20% or if FOLFOX was discontinued because of side effects. Postoperative chemotherapy was suggested in both arms. The primary endpoint of the study was DFS, while secondary endpoints included OS, LR, R0 resection, pCR, and toxic effects. After a median follow-up of almost 5 years, neoadjuvant FOLFOX was non-inferior to LCRT for DFS (HR= 0.92; 90.2% confidence interval [CI], 0.74 to 1.14; P = 0.005 for non-inferiority). Five-year DFS was 80.8% (95% CI, 77.9 to 83.7) in the FOLFOX group and 78.6% (95% CI, 75.4 to 81.8) in the LCRT group. No significant differences were found in terms of OS (HR= 1.04; 95% CI, 0.74 to 1.44) and LR (HR= 1.18; 95% CI, 0.44 to 3.16), with a low rate of LR in both arms (1.8% vs. 1.6%) as a result of eligibility criteria. Among the 585 patients enrolled in the FOLFOX arm, only 53 (9%) received LCRT. The pCR rate was 21.9% in the FOLFOX group and 24.3% in the LCRT group. Regarding safety, a higher incidence of G3-4 adverse events was reported in the FOLFOX group compared to the LCRT group during the neoadjuvant phase (41.0% vs. 22.8%), while this pattern reversed in the adjuvant part of the study. A patient-reported outcome analysis showed that at 12 months after surgery, patients assigned to FOLFOX reported significantly lower rates of fatigue and neuropathy and better sexual function compared to LCRT [27].
These findings suggest that the omission of radiotherapy may represent a safe and viable option in a subset of patients with LARC, without high-risk features, who are willing to avoid some long-term toxicities associated with radiotherapy, such as young patients aiming for fertility preservation.
2.3. Induction vs Consolidation Chemotherapy
As previously mentioned, two main different TNT strategies have been evaluated in clinical trials, utilizing systemic chemotherapy either before (induction) or after (consolidation) LCRT or SCRT. Both strategies have potential advantages and drawbacks. In particular, induction chemotherapy may allow for the early treatment of micrometastatic disease with the potential risk of hampering the efficacy of subsequent CRT through the selection of resistant tumor clones, while upfront CRT may reduce compliance with consolidation chemotherapy. Currently, the optimal sequence of treatments has not been established, but a few clinical studies have compared these two approaches, offering some interesting insights.
In the CAO/ARO/AIO-12 phase II study, 306 patients with stage II–III rectal cancer were enrolled and randomized to receive oxaliplatin-based chemotherapy (3 cycles of FOLFOX) either before (induction, group A) or after (consolidation, group B) fluorouracil-oxaliplatin-based LCRT. The primary endpoint of the study was pCR, and the trial utilized a pick-the-winner design based on the hypothesis of an increased pCR of 25% after TNT compared to the standard 15% after preoperative chemoradiotherapy [28]. The study showed a pCR rate of 17% for group A and 25% for group B, indicating that only consolidation chemotherapy met the predefined statistical hypothesis. Notably, following the design of the study, the median interval between completion of chemoradiotherapy and surgery was doubled in group B compared to group A (90 vs. 45 days), which may have significantly contributed to the higher observed pCR rate. Compliance with chemoradiotherapy was better in the consolidation arm, with 97% of patients able to receive full-dose radiotherapy and 87% receiving full-dose 5-fluorouracil, compared to 91% and 78% respectively in the induction arm. On the other hand, 92% completed all induction chemotherapy cycles in group A compared to 85% in group B. Recently, long-term results of the study have been published, showing no difference in DFS between the two treatment arms, with a 3-year DFS of 73% in both groups (hazard ratio, 0.95; 95% CI, 0.63-1.45, P = 0.82). The incidence of LR (6% vs. 5%, P = 0.67) and distant metastases (18% vs. 16%, P = 0.52) were also not significantly different, as well as other secondary endpoints, including toxicity, QoL, or stool incontinence [29].
The OPRA trial, a phase II randomized trial, enrolled 324 patients with LARC candidates for abdominoperineal resection or coloanal anastomosis at baseline [30]. Patients were randomly assigned to receive LCRT with either induction or consolidation chemotherapy. The chemotherapy consisted of eight cycles of FOLFOX or six cycles of CAPOX. Tumor restaging was planned within 8 (±4) weeks after TNT. Patients who achieved a complete or near-complete response after finishing treatment were offered watch-and-wait (WW), while TME was recommended for those who achieved an incomplete response. The primary endpoint was DFS, while the secondary endpoint was TME-free survival. The 3-year DFS was not different between the two groups (76%) and was similar to the historical comparison (75%). The proportion of patients who preserved the rectum at 3 years in the intention-to-treat population was 53% for the consolidation group and 41% for the induction group (p = 0.01), while the proportion of patients who actually preserved the rectum (TME-free survival) was 60% in the consolidation group and 47% in the induction group (p = 0.02). At longer follow-up, the 5-year DFS rates were not significantly different between the two arms, with 71% (95% CI, 64 to 79) and 69% (95% CI, 62 to 77) for induction and consolidation treatment, respectively (P =0.68), and the 5-year OS was 88% in both arms. The difference in TME-free survival was maintained. Of the 225 patients initially offered the WW protocol, 42/105 (40%) in the induction group and 33/120 (27%) in the consolidation group developed tumor regrowth during follow-up and were recommended for TME.
3. Immunocheckpoint Inhibitors (ICIs)
ICIs are a class of immunotherapy agents designed to target specific regulatory proteins involved in modulating immune responses, such as Programmed Death 1, Programmed Death-Ligand 1, and cytotoxic T-lymphocyte-associated protein 4. By blocking these checkpoints, these inhibitors unleash the immune system's ability to recognize and attack cancer cells, thereby enhancing anti-tumor immune responses [18]. Trials investigating the efficacy of ICIs in the treatment of LARC are summarized in Table 2.
3.1. Mismatch Repair-Deficient (dMMR) or Microsatellite Instability-High (MSI-H) LARC
The landscape of neoadjuvant therapy for LARC has been significantly impacted by the exploration of ICIs, particularly in the context of dMMR or MSI-H tumors (Table 2) These tumors, which account for approximately 3% of rectal cancer cases, arise from deficient mismatch repair systems, resulting in the accumulation of mutations within microsatellite DNA regions. Patients with MSI-H/dMMR LARC have distinct clinicopathological and molecular features, including higher tumor-infiltrating lymphocytes and overexpression of immune checkpoint receptors like programmed cell death protein 1 (PD-1) and programmed death-ligand 1 (PD-L1), making them particularly sensitive to immunotherapy.
A seminal study conducted by Cercek et al. investigated the application of PD-1 blockade in stage II and III rectal cancer with MMR deficiency [31]. In this prospective phase II trial, the objective was to evaluate the effectiveness of dostarlimab, an anti-PD-1 monoclonal antibody, in patients diagnosed with dMMR LARC. The primary goal was to ascertain the sustained clinical complete response (cCR) or pathological complete response (pCR) subsequent to dostarlimab treatment, administered with or without chemoradiotherapy. The study yielded remarkable findings, with all enrolled patients achieving a cCR rate following neoadjuvant PD-1 blockade. Consequently, no patients required subsequent chemoradiotherapy or underwent surgical intervention, and no instances of disease progression or recurrence were observed. In January 2023, US Food and Drug Administration approved dostarlimab for the treatment of dMMR/MSI-H LARC.
Chen et al. recently published the results of an open-label, single-center phase 2 trial aimed to assess the efficacy of neoadjuvant PD-1 blockade using sintilimab in patients with dMMR LARC [32]. The primary objective was to evaluate the response rate induced by neoadjuvant sintilimab treatment. Not all patients underwent surgery after the neoadjuvant treatment. Among 16 evaluable patients, 12 (75%) achieved a (pathological or clinical) complete response following treatment. The study thus reinforces the potential of PD-1 blockade with sintilimab as an effective neoadjuvant treatment strategy for dMMR LARC.
Another study by Zhang et al. provided valuable insights into the real-world effectiveness and safety profile of neoadjuvant immunotherapy with single agent PD-1 inhibitor in dMMR/MSI-H colon and rectal cancer, contributing to the growing body of evidence supporting the use of immunotherapy in this context [33]. Among the 32 enrolled patients, 3 with LARC achieving clinical complete response (cCR) adopted the watch-and-wait (W&W) strategy, while for the remaining 29 patients who underwent surgery, the rates of PR and pCR were 100% and 75.9%, respectively.
The multiple-center cohort study by Yang et al. investigated the management of dMMR or MSI-H LARC following neoadjuvant anti-PD-1 monotherapy, exploring the possibility of avoiding surgery in case of cCR [34]. In fact, seven of 20 enrolled patients with cCR adopted a W&W strategy. The study showed a cCR rate of 90% and no cases of local or distant recurrence. The findings suggest that patients with dMMR/MSI-H LARC may be considered for excusal from surgery after receiving neoadjuvant anti-PD-1 monotherapy, highlighting the importance of personalized treatment strategies in LARC management.
Moreover, 2 small and retrospective studies further underscored the efficacy and safety of PD-1 inhibitors, providing additional evidence supporting the integration of immunotherapy into the neoadjuvant setting for dMMR LARC [35,36]. These investigations collectively highlight the evolving role of ICIs in reshaping treatment paradigms, with potential implications for surgical decision-making in specific patient cohorts.
3.2. Mismatch Repair-Proficient (pMMR) or Microsatellite Stability (MSS) LARC
Several studies have explored the activity and safety of ICIs in patients with pMMR/MSS LARC. In the NICHE trial, which investigated the combination of Nivolumab and Ipilimumab, fifteen of the enrolled patients were pMMR, and four of them (27%) achieved a pCR [37]. Despite the encouraging results achieved in the above-mentioned study, the benefits from immunotherapy are commonly considered to be restricted to MSI tumors [38]. MSS is thus recognized as the main resistance factor to ICIs and, given its prevalence, a challenging drawback to overcome. Efforts have been made on two fronts to address this limitation: on a translational research front, the identification of ICI-sensitive MSS subsets has been pursued, while on the clinical research front, combination strategies have been proposed to sensitize MSS tumors to immunotherapy.
Regarding the identification of molecular ICI-sensitive MSS subsets, some potential molecular markers have been identified. Tumor mutational burden (TMB) has gained interest in this field. It is widely recognized that dMMR/MSI-H patients are characterized by high mutational rates. Nonetheless, a small proportion of non-MSI-H patients could harbor a TMB-high status. One cohort published by Fabrizio et al. demonstrated that 2.9% of MSS CRC patients harbor a TMB-H status [39]. POLE/POLD1 has also gained interest in this context by enabling the identification of non-MSI-H patients, possibly sensitive to immunotherapy [40]. Although promising, these markers are derived from studies performed on patients with metastatic disease. Moreover, non-POLE, non-TMB-H tumors are supposed to still represent the majority of MSS patients.
Regarding combination strategies, several treatments have been explored to enhance ICI sensitivity (Table 2). Associations with tyrosine kinase inhibitors (TKI) and anti-VEGF have already been explored in the metastatic setting. In the localized setting, the sensitizing role of radiotherapy has gained interest [41], and several studies have been conducted on this topic. In the VOLTAGE-A trial, patients with LARC were enrolled if a cT3 or cT4 stage was present at diagnosis, regardless of the nodal involvement. Two cohorts were created in this study and enrolled MSS and MSI patients respectively. In the MSS cohort, 37 patients were included, and a 30% pCR was achieved [42]. Similarly, the PANDORA trial investigated the efficacy of Durvalumab as consolidation treatment after LCRT. Patients with local nodal involvement or with cT3/cT4 LARC could be included. pCR was achieved in 34.5% of cases. Of interest, 46 out of the 48 patients with available microsatellite status were MSS [43]. Lin et al. investigated the activity of the anti-PD-1 Camrelizumab associated with CAPOX after SCRT in patients affected by LARC, regardless of the MS status. 26 of the included patients were pMMR [44]. A 46% pCR was achieved. The role of the anti-PD-L1 Avelumab has also been investigated. The AVERECTAL trial explored the activity of this molecule when administered in combination with FOLFOX after SCRT. A promising 37% pCR was detected in the MSS cohort [45]. The AVANA trial is an Italian phase II study that has investigated the pre-operative efficacy of 6 cycles of Avelumab (10 mg/kg) administered every two weeks after standard LCRT. The presence of at least one of these criteria was required for inclusion: cN+, cT4, and high-risk cT3. 23% of the 96 evaluable patients showed a pCR. Microsatellite status was available for only 39 patients, and, surprisingly, all of them resulted to be MSS except for one [46].
Novel potential agents are on the way. Some interesting signals of efficacy have been detected in patients treated with the combination of Botensilimab, a novel anti-CTLA-4 antibody, and Balstilimab, a next-generation PD-1 inhibitor [47]. This promising therapeutic strategy has already provided interesting results in the metastatic setting [48] and is currently under investigation in patients with LARC.
5. Non Operative Management (NOM)
Neoadjuvant LCRT followed by radical surgery represents the standard approach for treating LARC [4]. Following LCRT, approximately 15-27% of patients achieve a pCR, defined as the absence of viable tumor cells in the pathological specimen [49]. This rate appears to be even higher in patients undergoing TNT [21,22]. A recent meta-analysis, encompassing 3579 patients from 15 trials, demonstrated that TNT was associated with a pCR rate of 22.7% compared to 13.6% in the standard treatment group, with a pooled odds ratio of 1.85 (p<0.0001) [50]. Furthermore, the pCR rate in MSI/dMMR rectal cancer treated with ICIs may be even higher, showing promising outcomes in the most recent data [31,32]. These findings, combined with the significant mortality and short- and long-term morbidity associated with surgery (including bowel, urinary, and sexual dysfunction due to nerve and sphincter damage), have sparked growing interest in NOM for patients who achieve a cCR after neoadjuvant CTRT. cCR is defined as the absence of residual tumor signs upon reassessment, which typically includes digital rectal examination, endoscopy, and radiological imaging.
The concept of NOM was first introduced in 2004 [51]. In this study, the non-operative group exhibited 5-year OS and DFS rates of 100% and 92%, respectively, compared to 88% and 83% in the surgically resected group. Despite initial skepticism, the "watch and wait (WW) strategy" has gained traction in recent years, leading to a notable increase in the proportion of patients and surgeons opting for organ preservation approaches in rectal cancer [52].

Table 3.
summarizes the findings of studies comprising more than 40 cases in the WW group.
| First Autor | Year | Study design | Control group | Number of patients | DFS (WW vs control) |
|||
|---|---|---|---|---|---|---|---|---|
| Control group | WW group | 3-years | 5-years | |||||
| Araujo [71] | 2015 | Retrospective cohort study | TME | 69 | 42 | 60.9% vs 82.8% (p 0.011) | ||
| Martens [73] | 2016 | Prospective cohort study | TEM | 15 | 85 | [LRFS] 85.8% vs 80% (p 0.57) |
||
| Smith [64] | 2019 | Retrospective case series analysis | TME | 136 | 113 | 75% vs 92% (p N.D.) |
||
| Beard [65] | 2020 | Retrospective cohort study | RS | 42 | 53 | [LRFS] 85 vs 92% (p 0.36) | ||
| Wang [70] | 2021 | Multicenter retrospective cohort study | RS | 94 | 94 | [LRFS] 98% vs 98% (p 0.506) |
||
| Najami [74] | 2021 | Observation descriptive cohort study | LE | 22 | 42 | 74.9% vs 66.2% (p N.D.) | ||
| Han [61] | 2022 | Prospective cohort study | TME | 26 | 58 | 81.1% vs 84.6% (p 0.819) | ||
| Wang [55] | 2023 | Retrospective cohort study | RS | 171 | 89 | 93.3% vs 92% (p 0.66) | ||
DFS: Disease Free Survival; LE: Local Excision; LRFS: Local Recurrence Free Survival, RS: Radical Surgery; TEM: Trans-anal Endoscopic Microsurgery; TME: Total Mesorectal Excision.
The major concern regarding the NOM strategy is the risk of LR, which appears to be higher compared to patients undergoing radical surgery [53]. An analysis from 2018, comprising data from 880 patients in the International Watch and Wait Database, reported a LR rate of 25% within the initial 2 years of follow-up [12]. However, a 2023 analysis comparing patients undergoing TME or WW post-TNT demonstrated a lower LR rate (9.9%) [13]. The majority (83-94%) of local regrowths were observed within 2 years in the conservative group [54,55,56]. The likelihood of remaining free from LR increased over time, with patients maintaining sustained cCR for 3 years having an approximately 5% risk of recurrence [57]. LR predominantly occurs in the bowel wall (97% of cases), allowing for salvage surgery in most patients, with reported rates of R0 resection reaching 97.5% in some studies [54,58,59]. Long-term results from the OPRA trial indicated similar rates of R0 resection in patients undergoing radical surgery post-regrowth and those undergoing radical surgery post-neoadjuvant therapy (91% vs. 90%, p = 1.0) [56]. Sphincter-saving surgery is feasible in nearly half of patients requiring surgery after LR, comparable to those undergoing radical surgery after LCRT [56]. However, a small Spanish study conducted in 2023 found a higher rate of permanent stomas in salvage surgery after NOM compared to patients undergoing radical surgery (48.5% vs. 20%, p < 0.01) [60].
The incidence of distant metastases appears comparable between patients undergoing radical resection and those opting for the NOM strategy [61]. A meta-analysis from 2021 reported distant metastases rates of 10.21% vs. 8.66% (p = 0.67, OR 1.12) for the WW and radical surgery groups, respectively [62]. However, local regrowth appears to be a risk factor for distant metastases development, with patients experiencing LR showing a 5-fold higher risk compared to those without LR [63,64,65]. The heightened risk may arise from a more aggressive biological phenotype, contributing to both LR and the development of metastatic disease. Alternatively, some suggest that metastases may arise from the uncontrolled growth of the primary tumor [66].
Both DFS and OS seem comparable between patients undergoing salvage surgery after NOM and those opting for radical surgery post-neoadjuvant LCRT [58,61,67,68,69,70]. However, a 2015 Brazilian study reported inferior DFS in patients undergoing WW compared to those undergoing radical surgery (60.9% vs. 82.8%, p = 0.011) [71]. Notably, patients undergoing WW often present with more distal tumors, a characteristic associated with lower survival rates (p = 0.011). When focusing solely on low rectal tumors in both groups, no significant differences in OS (85.8% vs. 71.7%, p = 0.970) were observed, and the discrepancy in DFS was not statistically significant (p = 0.081).
The NOM approach could serve as a viable strategy to avoid surgical trauma in patients with cCR; however, careful patient selection and comprehensive information dissemination are crucial. Presently, there exists no consensus on the follow-up protocol for patients considered for the WW approach. The NCCN panel recommends a monitoring regimen comprising digital rectal examination and proctoscopy every 3-4 months for the initial 2 years, followed by semiannual evaluations for 3 years, alongside pelvic MRI every 6 months for at least 3 years [72].
6. Circulating Tumor DNA (ctDNA) Evaluation in LARC Patients
To improve the treatment management of LARC patients, trustworthy biomarkers of treatment efficacy are needed. In this context, the evaluation of ctDNA should help identify patients who would benefit from WW policies and identify those who may need to have their systemic treatment intensified due to a high risk of metastasis.
ctDNA is released into the bloodstream by living cancer cells during cell death, constituting a minute fraction of cell-free DNA. It can be detected by either tumor-informed assays, where probes are designed according to mutations identified in a patient’s tumor tissue or by tumor-agnostic assays, that are independent on prior tumor genomic knowledge of the patient. The former shows high analytical sensitivity, the last may offer a more rapid turnaround time with reduced cost [75]
Available data on ctDNA in LARC patients encompass its utility as a marker of both minimal residual disease (MRD) post-definitive local treatment and treatment response to neoadjuvant therapy [76,77,78,79,80,81]. Regarding MRD, consistent findings indicate that patients with detectable postoperative ctDNA face a higher recurrence risk compared to those with undetectable [82,83,84,85]. Thus, assessing MRD status enables risk stratification and facilitates determining patients likely to benefit from adjuvant chemotherapy.
The relationship between preoperative ctDNA and surgical outcomes has been less explored, with recent interest emerging in the additive value of ctDNA levels for monitoring response in neoadjuvant settings [76,77,78,79,80,81]. Several studies confirmed the association between ctDNA and prognosis, but failed to find a significant association between ctDNA status and pCR [85,86,87,88]. No association was found between ctDNA status and pCR also in the GEMCAD 1402, a phase II randomized, multicentric clinical trial [76]. However, preoperative ctDNA status significantly correlates with postoperative pathological results, indicating its potential as a real-time monitoring indicator reflecting tumor burden [77]. Additionally, undetectable preoperative ctDNA is associated with favorable surgical outcomes, as evidenced by margin-negative, node-negative resections, and neoadjuvant rectal score [86].
Tumor-informed ctDNA detection using ultradeep sequencing in LARC patients may offer clinical value for predicting response following neoadjuvant therapy and surgery [87]. Our study, utilizing a personalized tumor-informed ctDNA assay (Signatera™) assay, demonstrated worse DFS in ctDNA-positive patients post-neoadjuvant therapy and surgery compared to ctDNA-negative counterparts [89]. Furthermore, patients remaining ctDNA-positive post-neoadjuvant therapy, irrespective of pCR status, exhibited inferior DFS compared to ctDNA-negative patients [89]. Combining post-neoadjuvant therapy ctDNA status with neoadjuvant rectal score predicted neoadjuvant therapy response, as already shown in previous research [86]. Notably, the sensitivity of ctDNA assays, whether tumor-agnostic or tumor-informed, impacts baseline ctDNA positivity detection, thereby influencing the number of patients for which the ctDNA dynamic monitoring could be useful [76,85,89].
7. Discussion
The standard management approach for LARC involves multimodal therapy, integrating radiation, chemotherapy, and surgery. While LCRT and SCRT yield comparable survival outcomes, the latter is associated with reduced rates of pCR and increased LR. Despite the introduction of LCRT, distant metastases remain unaffected. Poor tolerance to adjuvant chemotherapy has driven the exploration of diverse TNT strategies, administering both radiotherapy and chemotherapy before surgery. Recently, three phase III trials, PRODIGE-23, RAPIDO, and STELLAR, compared different TNT strategies to standard LCRT. The PRODIGE-23 study confirmed the tolerability and efficacy of the triplet regimen mFOLFIRINOX as induction chemotherapy in a TNT strategy. However, despite the favorable safety profile of the treatment compared to the metastatic setting, this intensive regimen should be reserved for selected patients. Moreover, due to the lack of an arm with a neoadjuvant doublet regimen such as FOLFOX/XELOX, it is difficult to assess the added benefit of irinotecan. Additionally, it should be noted that the trial included mandatory adjuvant treatment in the experimental arm, which was started in about 70% of patients, confirming the poor compliance with post-operative chemotherapy in this setting. RAPIDO and STELLAR trials investigated a consolidation TNT approach. While the RAPIDO trial yielded promising outcomes, it carries certain limitations worth noting. Despite the observed increase in pCR, the experimental group exhibited numerically higher rates of LR compared to the standard of care group. This suggests that consolidation chemotherapy may not fully compensate for suboptimal radiotherapy strategies in patients with high-risk disease features. Additionally, concerns arise regarding the optional adjuvant therapy in the control arm, which was administered to only 47% of resected patients, rendering the control arm an inadequate comparator. The phase III STELLAR trial, assessing a TNT strategy akin to RAPIDO, found no significant differences in LR between TNT and LCRT. The differences in clinical outcome observed between STELLAR and RAPIDO trials may partly be related to different eligibility criteria, with more patients with cT4 and cN2 disease in RAPIDO compared to STELLAR, but also in trial design. Indeed, in STELLAR trial an equivalent number of chemotherapy cycles were planned in the control and experimental arms and this may partly explain the absence of a difference in DFS. Overall, although non-inferiority of experimental arm was shown in the study, some important confounding factors, such as increased toxicity, lack of a benefit in endpoints related to disease control (DFS, MFS and LR) and the significant proportion of patients not undergoing surgery (about 20%) suggest a cautious interpretation of trial results.
Currently, the optimal treatment sequence remains undefined, but some clinical trials have compared induction and consolidation chemotherapy regimens, providing valuable insights. Considering findings from the CAO/ARO/AIO-12 and OPRA trials together, the use of induction chemotherapy results in better chemotherapy compliance but lower radiotherapy compliance compared to consolidation treatment. No differences in terms of DFS or OS have been observed in the two trials between these strategies, but the use of consolidation chemotherapy seems to be associated with higher rates of pCR and clinical response rate, leading to improved TME-free survival. These results may be partly explained by the longer time interval between completion of LCRT and surgery, which may allow for a deeper effect of radiation therapy. Indeed, in the OPRA trial, the median interval from the end of chemoradiotherapy to restaging was 8.0 weeks in the induction arm and 28 weeks in the consolidation arm, and similarly, in the CAO/ARO/AIO-12 trial, the interval after chemoradiotherapy was doubled in the consolidation arm. In both trials, the increase in the time interval between radiotherapy and surgery did not increase surgical morbidity.
Ongoing trials are investigating optimal treatment sequences, evaluating long-term outcomes, and exploring novel therapeutic approaches (Table 4). There is probably no optimal TNT sequence for all LARC patients, but the treatment strategy should be individualized based on the patient’s characteristics and treatment goals. For example, consolidation chemotherapy after chemoradiotherapy may represent the optimal choice in large cT4 or mesorectal fascia-involving tumors or when the organ preservation strategy is pursued. On the other hand, the use of induction chemotherapy, considering the better compliance to chemotherapy, may be preferable in patients with a high risk of micrometastatic disease, such as those with EMVI or N2 tumors.
The presence of MSI-H/dMMR in rectal cancer can serve as both a negative predictor for the efficacy of standard neoadjuvant chemoradiotherapy and a positive predictor for the effectiveness of pre-operative immunotherapy. Studies, such as the phase II trial conducted by Cercek et al., have demonstrated the efficacy of anti-PD-1 monoclonal antibodies, such as dostarlimab, in inducing sustained clinical cCR in patients with MSI-H/dMMR LARC. Future perspectives in this field are promising, with several ongoing clinical trials aiming to further elucidate both efficacy and safety profile (Table 5).
Table 5.
Ongoing clinical trials evaluating Total Neoadjuvant Treatment (TNT).
| NCT Number | Treatment strategy | Status | Phase |
|---|---|---|---|
| NCT03038256 | Ctr: CTRT→S→ADT Exp: CTRT → CAPOX x4→S Exp1: CTRT → CAPOX x6→S |
Recruiting | Phase II |
| NCT05054959 | Exp1: CTRT → CAPOX x6→S Exp 2: CAPOXx4→ CTRT → CAPOX x2→S |
Recruiting | Phase II |
| NCT05673772 | Exp1: SCRT → FOLFOX x4→S→ADT Ctr: CTRT→S→ADT |
Recruiting | Phase II |
| NCT05610163 | Exp1: CTRT → FOLFOX/CAPOX → S or NOM Exp2: CTRT → FOLFIRINOX → S or NOM Ctr: CTRT→S→ADT |
Recruiting | Phase II |
| NCT04246684 | Exp: CTRT (+ Oxa) → CT (FOLFOX x 6/ CAPOX x 4) Ctr: SCRT → CT (FOLFOX x 9/ CAPOX x 6) If cCR → NOM If not cCR → S |
Recruiting | Phase III |
| NCT04215731 | Exp1: FOLFOXIRI + bevacizumab x 4 → FOLFOXIRI x 2 → immediate S or CTRT→ S according to ycT Exp2: FOLFOX x 4 → CTRT → S |
Recruiting | Phase III |
| NCT05646511 | Exp 1: SCRT → CAPOX x 6 → S or NOM Exp 2: SCRT → CAPOXIRI x 6 → S or NOM |
Recruiting | Phase III |
ADT: adjuvant therapy; ctr: control; cCR: complete clinical response; CTRT: chemo-radiotherapy; exp: experimental; NOM: non operative management; S: surgery; NOM: non operative management; oxa: oxaliplatin; SCRT: short-course radiotherapy.
Table 5.
List of ongoing clinical trials evaluating ICIs in the neoadjuvant setting.
| MSI-H Tumors | |||
|---|---|---|---|
| NCT Number | Study Title | Study Status | Phases |
| NCT05645094 | Neoadjuvant Envafolimab in Resectable and Locally Advanced MSI-H/dMMR Rectal Cancer | NOT YET RECRUITING | PHASE2 |
| NCT04411524 | The Combination of Immunotherapy and Neoadjuvant Chemoradiotherapy in MSI-H Locally Advanced Rectal Cancer | UNKNOWN STATUS |
PHASE2 |
| NCT04301557 | PD1 Antibody Toripalimab and Chemoradiotherapy for dMMR/MSI-H Locally Advanced Colorectal Cancer | RECRUITING | PHASE2 |
| NCT05723562 | A Study of Dostarlimab in Untreated dMMR/MSI-H Locally Advanced Rectal Cancer (AZUR-1) | RECRUITING | PHASE2 |
| NCT04357587 | Safety and Feasibility of PD-1 Blockade in the Treatment of dMMR or MSI-H Rectal Cancer | RECRUITING | PHASE2 |
| NCT04304209 | Pd1 Antibody Sintilimab ± Chemoradiotherapy for Locally Advanced Rectal Cancer | ACTIVE, NOT RECRUITING | PHASE2 |
| NCT04751370 | Testing Nivolumab and Ipilimumab With Short-Course Radiation in Locally Advanced Rectal Cancer | SUSPENDED | PHASE2 |
| NCT05732389 | Immunotherapy in Patients With Early dMMR Rectal Cancer (RESET-R) | RECRUITING | PHASE2 |
| NCT04636008 | Neoadjuvant treatment of sintilimab plus hypofractionated radiotherapy for MSI-H/dMMR rectal cancer: A prospective, multicenter, phase Ib study | RECRUITING | PHASE2 |
| NCT05645094 | Neoadjuvant Envafolimab in Resectable and Locally Advanced MSI-H/dMMR Rectal Cancer | NOT YET RECRUITING | PHASE2 |
| NCT04411524 | The Combination of Immunotherapy and Neoadjuvant Chemoradiotherapy in MSI-H Locally Advanced Rectal Cancer | UNKNOWN STATUS |
PHASE2 |
| NCT04301557 | PD1 Antibody Toripalimab and Chemoradiotherapy for dMMR/MSI-H Locally Advanced Colorectal Cancer | RECRUITING | PHASE2 |
| NCT05723562 | A Study of Dostarlimab in Untreated dMMR/MSI-H Locally Advanced Rectal Cancer (AZUR-1) | RECRUITING | PHASE2 |
| NCT04357587 | Safety and Feasibility of PD-1 Blockade in the Treatment of dMMR or MSI-H Rectal Cancer | RECRUITING | PHASE2 |
| NCT04304209 | Pd1 Antibody Sintilimab ± Chemoradiotherapy for Locally Advanced Rectal Cancer | ACTIVE, NOT RECRUITING | PHASE2 |
| NCT04751370 | Testing Nivolumab and Ipilimumab With Short-Course Radiation in Locally Advanced Rectal Cancer | SUSPENDED | PHASE2 |
| NCT05732389 | Immunotherapy in Patients With Early dMMR Rectal Cancer (RESET-R) | RECRUITING | PHASE2 |
| NCT04636008 | Neoadjuvant treatment of sintilimab plus hypofractionated radiotherapy for MSI-H/dMMR rectal cancer: A prospective, multicenter, phase Ib study | RECRUITING | PHASE2 |
| MSS TUMORS | |||
| NCT05215379 | Neoadjuvant Chemoradiation Therapy Combined With Immunotherapy for MSS Ultra-low Rectal Cancer | RECRUITING | PHASE2|PHASE3 |
| NCT04109755 | Neo-adjuvant Pembrolizumab and Radiotherapy in Localized MSS Rectal Cancer | RECRUITING | PHASE2 |
| NCT04895137 | mFOLFOX6+Bevacizumab+PD-1 Monoclonal Antibody in Local Advanced MSS CRC | RECRUITING | PHASE2 |
| NCT04833387 | PD-1 Antibody Following Preoperative Chemoradiotherapy for Locally Advanced pMMR/MSS Rectal Cancer | ACTIVE, NOT RECRUITING | PHASE2 |
| NCT05731726 | Serplulimab Combined With CAPOX + Celecoxib as Neoadjuvant Treatment for Locally Advanced Rectal Cancer | RECRUITING | PHASE2 |
| NCT05972655 | Nodes-sparing Short-course Radiation Combined With CAPOX and Tislelizumab for MSS Middle and Low Rectal Cancer | RECRUITING | PHASE2 |
| NCT04940546 | Neoadjuvant Safety of Sintilimab + XELOX + Bevacizumab in pMMR/MSS CRLM Patients | ACTIVE, NOT RECRUITING | PHASE1|PHASE2 |
| NCT05858567 | Total Neoadjuvant Therapy With Short-course Radiation Followed by Envafolimab Plus CAPOX for MSS Locally Advanced Ultra Low Rectal Adenocarcinoma | RECRUITING | PHASE2 |
| NCT05216653 | Preoperative Short-course Radiation Followed by Envafolimab Plus CAPOX for MSS Locally Advanced Rectal Adenocarcinoma (PRECAM) | ACTIVE, NOT RECRUITING | PHASE2 |
| NCT05752136 | Preoperative Short-course Radiation Followed by Envafolimab Plus CAPOX for MSS Locally Advanced Rectal Adenocarcinoma | RECRUITING | PHASE3 |
| NCT05815303 | XELOX Combined With Cadonilimab Versus XELOX as Neoadjuvant Treatment for Locally Advanced, pMMR Rectal Cancer | RECRUITING | PHASE2 |
| NCT04304209 | Pd1 Antibody Sintilimab ± Chemoradiotherapy for Locally Advanced Rectal Cancer | ACTIVE, NOT RECRUITING | PHASE2 |
These studies may provide valuable insights into optimizing treatment strategies, including the selection of appropriate immunotherapeutic agents, treatment combinations, dosing regimens, and patient selection criteria. Additionally, these trials may shed light on the potential role of immunotherapy in enhancing pathological responses, improving long-term outcomes, and providing the opportunity to avoid chemoradiotherapy and surgery in selected cases of MSI-H LARC. While these findings are based on limited studies, they suggest a promising short-term efficacy of preoperative immunotherapy as a single treatment modality in patients LARC. Several studies have explored ICIs also in patients with pMMR/MSS LARC. While the benefits of immunotherapy are mostly observed in MSI tumors, efforts are underway to identify MSS subsets sensitive to ICIs and explore combination strategies to enhance their efficacy (Table 5). Moreover, ongoing trials are investigating novel agents like Botensilimab and Balstilimab in LARC patients.
Increasing interest in NOM has emerged due to significant surgical morbidity and mortality, prompting a notable rise in organ preservation approaches. Concerns regarding the risk of LR persist, although rates have improved over time, with most local regrowth occurring within the initial 2 years. The incidence of distant metastases appears comparable between radical resection and NOM, yet careful patient selection and comprehensive information dissemination are crucial given differences in outcomes.
Reliable biomarkers like circulating tumor DNA (ctDNA) are crucial for optimizing treatment in LARC patients, aiding in identifying candidates for WW and those requiring intensified therapy. Utilizing tumor-informed ctDNA assays may provide real-time monitoring of tumor burden, guiding treatment decisions and improving outcomes in neoadjuvant settings. Despite its increasing use in clinical studies, ctDNA analysis remains underutilized in routine care for LARC patients due to study heterogeneity regarding ctDNA assay selection, timing of ctDNA collection, treatment variations, and follow-up duration. Incorporating ctDNA analysis into larger randomized trials is imperative to evaluate ctDNA dynamics across neoadjuvant treatment phases and surveillance, thus informing its potential clinical utility, particularly in the context of TNT and organ preservation approaches.
5. Conclusions
The multimodal treatment strategy for LARC is rapidly evolving, representing a significant departure from previous static phases. While TNT offer insights into new neoadjuvant treatment sequences, their findings must be interpreted cautiously due to limitations and variances in patient populations. Additionally, immunotherapy shows promise, particularly in MSI-H/dMMR tumors, but further research is needed to better define its role. The increasing adoption of NOM is justified by the growing effectiveness of neoadjuvant treatments, but caution is required before generalizing it in clinical practice. Biomarkers like ctDNA hold potential for personalized treatment approaches, but their integration into routine care requires standardized protocols. Ultimately, individualized treatment decisions based on patient characteristics and treatment goals are paramount for improving outcomes in LARC.
Author Contributions
Conceptualization, F.G.S., A.P. and A.B.; writing—original draft preparation, all authors.; writing—review and editing, A.P., G.M., A.B., C.M.; supervision, A.B.; All authors have read and agreed to the published version of the manuscript.
Funding
This work was partly supported thanks to the contribution of Ricerca Corrente by the Italian Ministry of Health.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank Cristiano Verna for his support in editing the manuscript and Francesco Mazza for his assistance in improving the figure.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021 May;71(3):209-249. Epub 2021 Feb 4. [CrossRef] [PubMed]
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022 Jan;72(1):7-33. Epub 2022 Jan 12. [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Rectal Cancer. Version 3.2022. Published 2022. Accessed January 28, 2024. [https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf].
- Glimelius B, Tiret E, Cervantes A, Arnold D; ESMO Guidelines Committee. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24 Suppl 6:vi81-8. [CrossRef]
- Molinari C, Passardi A. Why is neoadjuvant chemoradiation therapy underused for locally advanced rectal cancer? Expert Rev Gastroenterol Hepatol. 2016 Dec;10(12):1317-1319. Epub 2016 Oct 19. [CrossRef] [PubMed]
- Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, Martus P, Tschmelitsch J, Hager E, Hess CF, Karstens JH, Liersch T, Schmidberger H, Raab R; German Rectal Cancer Study Group. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004 Oct 21;351(17):1731-40. [CrossRef] [PubMed]
- Sebag-Montefiore D, Stephens RJ, Steele R, Monson J, Grieve R, Khanna S, Quirke P, Couture J, de Metz C, Myint AS, Bessell E, Griffiths G, Thompson LC, Parmar M. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. Lancet. 2009 Mar 7;373(9666):811-20. [CrossRef] [PubMed] [PubMed Central]
- Pettersson D, Cedermark B, Holm T, Radu C, Påhlman L, Glimelius B, Martling A. Interim analysis of the Stockholm III trial of preoperative radiotherapy regimens for rectal cancer. Br J Surg. 2010 Apr;97(4):580-7. [CrossRef] [PubMed]
- Marijnen CA, van de Velde CJ, Putter H, van den Brink M, Maas CP, Martijn H, Rutten HJ, Wiggers T, Kranenbarg EK, Leer JW, Stiggelbout AM. Impact of short-term preoperative radiotherapy on health-related quality of life and sexual functioning in primary rectal cancer: report of a multicenter randomized trial. J Clin Oncol. 2005 Mar 20;23(9):1847-58. [CrossRef] [PubMed]
- Pettersson D, Holm T, Iversen H, Blomqvist L, Glimelius B, Martling A. Preoperative short-course radiotherapy with delayed surgery in primary rectal cancer. Br J Surg. 2012 Apr;99(4):577-83. Epub 2012 Jan 12. [CrossRef] [PubMed]
- Bujko K, Richter P, Smith FM, Polkowski W, Szczepkowski M, Rutkowski A, Dziki A, Pietrzak L, Kołodziejczyk M, Kuśnierz J, Gach T, Kulig J, Nawrocki G, Radziszewski J, Wierzbicki R, Kowalska T, Meissner W, Radkowski A, Paprota K, Polkowski M, Rychter A. Preoperative radiotherapy and local excision of rectal cancer with immediate radical re-operation for poor responders: a prospective multicentre study. Radiother Oncol. 2013 Feb;106(2):198-205. Epub 2013 Jan 17. [CrossRef] [PubMed]
- Ngan SY, Burmeister B, Fisher RJ, Solomon M, Goldstein D, Joseph D, Ackland SP, Schache D, McClure B, McLachlan SA, McKendrick J, Leong T, Hartopeanu C, Zalcberg J, Mackay J. Randomized trial of short-course radiotherapy versus long-course chemoradiation comparing rates of local recurrence in patients with T3 rectal cancer: Trans-Tasman Radiation Oncology Group trial 01.04. J Clin Oncol. 2012 Nov 1;30(31):3827-33. Epub 2012 Sep 24. Erratum in: J Clin Oncol. 2013 Jan 20;31(3):399. [CrossRef] [PubMed]
- Bujko K, Nowacki MP, Nasierowska-Guttmejer A, Michalski W, Bebenek M, Kryj M. Long-term results of a randomized trial comparing preoperative short-course radiotherapy with preoperative conventionally fractionated chemoradiation for rectal cancer. Br J Surg. 2006 Oct;93(10):1215-23. [CrossRef] [PubMed]
- Breugom AJ, van Gijn W, Muller EW, Berglund Å, van den Broek CBM, Fokstuen T, Gelderblom H, Kapiteijn E, Leer JWH, Marijnen CAM, Martijn H, Meershoek-Klein Kranenbarg E, Nagtegaal ID, Påhlman L, Punt CJA, Putter H, Roodvoets AGH, Rutten HJT, Steup WH, Glimelius B, van de Velde CJH. Adjuvant chemotherapy for rectal cancer patients treated with preoperative (chemo)radiotherapy and total mesorectal excision: a Dutch Colorectal Cancer Group (DCCG) randomized phase III trial. Ann Oncol. 2015 Apr;26(4):696-701. Epub 2014 Dec 5. [CrossRef] [PubMed]
- Breugom AJ, Swets M, Bosset JF, Collette L, Sainato A, Cionini L, Glynne-Jones R, Counsell N, Bastiaannet E, van den Broek CB, Liefers GJ, Putter H, van de Velde CJ. Adjuvant chemotherapy after preoperative (chemo)radiotherapy and surgery for patients with rectal cancer: a systematic review and meta-analysis of individual patient data. Lancet Oncol. 2015 Feb;16(2):200-7. Epub 2015 Jan 12. [CrossRef] [PubMed]
- Collette L, Bosset JF, den Dulk M, Nguyen F, Mineur L, Maingon P, Radosevic-Jelic L, Piérart M, Calais G; European Organisation for Research and Treatment of Cancer Radiation Oncology Group. Patients with curative resection of cT3-4 rectal cancer after preoperative radiotherapy or radiochemotherapy: does anybody benefit from adjuvant fluorouracil-based chemotherapy? A trial of the European Organisation for Research and Treatment of Cancer Radiation Oncology Group. J Clin Oncol. 2007 Oct 1;25(28):4379-86. [CrossRef] [PubMed]
- Cercek A, Roxburgh CSD, Strombom P, Smith JJ, Temple LKF, Nash GM, Guillem JG, Paty PB, Yaeger R, Stadler ZK, Seier K, Gonen M, Segal NH, Reidy DL, Varghese A, Shia J, Vakiani E, Wu AJ, Crane CH, Gollub MJ, Garcia-Aguilar J, Saltz LB, Weiser MR. Adoption of Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer. JAMA Oncol. 2018 Jun 14;4(6):e180071. Epub 2018 Jun 14. [CrossRef] [PubMed] [PubMed Central]
- Passardi A, Canale M, Valgiusti M, Ulivi P. Immune Checkpoints as a Target for Colorectal Cancer Treatment. Int J Mol Sci. 2017 Jun 21;18(6):1324. [CrossRef] [PubMed] [PubMed Central]
- Tivey A, Church M, Rothwell D, Dive C, Cook N. Circulating tumour DNA - looking beyond the blood. Nat Rev Clin Oncol. 2022 Sep;19(9):600-612. Epub 2022 Aug 1. [CrossRef] [PubMed] [PubMed Central]
- Conroy, T.; Bosset, J.-F.; Etienne, P.-L.; Rio, E.; François, E.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Etienne, P.-L.; Rio, E.; Evesque, L.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouche, O.; Boileve, A.; Delaye, M.; et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiation in patients with locally advanced rectal cancer: 7-year results of PRODIGE 23 phase III trial, a UNICANCER GI trial. J. Clin. Oncol. 2023, 41, LBA3504. [Google Scholar] [CrossRef]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, E.A.; Nilsson, P.J.; Hospers, G.A.; Bahadoer, R.R.; Kranenbarg, E.M.-K.; Roodvoets, A.G.; Putter, H.; Berglund, Å.; Cervantes, A.; Crolla, R.M.; et al. Locoregional Failure During and After Short-course Radiotherapy followed by Chemotherapy and Surgery Compared to Long-course Chemoradiotherapy and Surgery—A Five-year Follow-up of the RAPIDO Trial. Ann. Surg. 2023, 10–109. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Tang, Y.; Hu, C.; Jiang, L.-M.; Jiang, J.; Li, N.; Liu, W.-Y.; Chen, S.-L.; Li, S.; Lu, N.-N.; et al. Multicenter, randomized, phase III trial of short-term radiotherapy plus chemotherapy versus long-term chemoradiotherapy in locally advanced rectal cancer (STELLAR). J. Clin. Oncol. 2022, 40, 1681–1692. [Google Scholar] [CrossRef] [PubMed]
- Deng Y, Chi P, Lan P, Wang L, Chen W, Cui L, Chen D, Cao J, Wei H, Peng X, Huang Z, Cai G, Zhao R, Huang Z, Xu L, Zhou H, Wei Y, Zhang H, Zheng J, Huang Y, Zhou Z, Cai Y, Kang L, Huang M, Wu X, Peng J, Ren D, Wang J. Neoadjuvant Modified FOLFOX6 With or Without Radiation Versus Fluorouracil Plus Radiation for Locally Advanced Rectal Cancer: Final Results of the Chinese FOWARC Trial J Clin Oncol. 2019 Dec 1;37(34):3223-3233. Epub 2019 Sep 26. [CrossRef]
- Schrag, D.; Shi, Q.; Weiser, M.R.; Gollub, M.J.; Saltz, L.B.; Musher, B.L.; Goldberg, J.; Al Baghdadi, T.; Goodman, K.A.; McWilliams, R.R.; et al. Preoperative Treatment of Locally Advanced Rectal Cancer. N. Engl. J. Med. 2023, 389, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Basch E, Dueck AC, Mitchell SA, Mamon H, Weiser M, Saltz L, Gollub M, Rogak L, Ginos B, Mazza GL, Colgrove B, Chang G, Minasian L, Denicoff A, Thanarajasingam G, Musher B, George T, Venook A, Farma J, O'Reilly E, Meyerhardt JA, Shi Q, Schrag D. Patient-Reported Outcomes During and After Treatment for Locally Advanced Rectal Cancer in the PROSPECT Trial (Alliance N1048). J Clin Oncol. 2023 Jul 20;41(21):3724-3734. Epub 2023 Jun 4. [CrossRef] [PubMed]
- Fokas, E.; Allgäuer, M.; Polat, B.; Klautke, G.; Grabenbauer, G.G.; Fietkau, R.; Kuhnt, T.; Staib, L.; Brunner, T.; Grosu, A.-L.; et al. Randomized Phase II Trial of Chemoradiotherapy Plus Induction or Consolidation Chemotherapy as Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer: CAO/ARO/AIO-12. J. Clin. Oncol. 2019, 37, 3212–3222. [Google Scholar] [CrossRef] [PubMed]
- Fokas, E.; Schlenska-Lange, A.; Polat, B.; Klautke, G.; Grabenbauer, G.G.; Fietkau, R.; Kuhnt, T.; Staib, L.; Brunner, T.; Grosu, A.-L.; et al. Chemoradiotherapy Plus Induction or Consolidation Chemotherapy as Total Neoadjuvant Therapy for Patients with Locally Advanced Rectal Cancer. JAMA Oncol. 2022, 8, e215445. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Aguilar, J.; Patil, S.; Gollub, M.J.; Kim, J.K.; Yuval, J.B.; Thompson, H.M.; Verheij, F.S.; Omer, D.M.; Lee, M.; Dunne, R.F.; et al. Organ Preservation in Patients with Rectal Adenocarcinoma Treated with Total Neoadjuvant Therapy. J. Clin. Oncol. 2022, 40, 2546–2556. [Google Scholar] [CrossRef] [PubMed]
- Cercek A, Lumish M, Sinopoli J, Weiss J, Shia J, Lamendola-Essel M, El Dika IH, Segal N, Shcherba M, Sugarman R, Stadler Z, Yaeger R, Smith JJ, Rousseau B, Argiles G, Patel M, Desai A, Saltz LB, Widmar M, Iyer K, Zhang J, Gianino N, Crane C, Romesser PB, Pappou EP, Paty P, Garcia-Aguilar J, Gonen M, Gollub M, Weiser MR, Schalper KA, Diaz LA Jr. PD-1 Blockade in Mismatch Repair-Deficient, Locally Advanced Rectal Cancer. N Engl J Med. 2022 Jun 23;386(25):2363-2376. Epub 2022 Jun 5. [CrossRef] [PubMed] [PubMed Central]
- Chen G, Jin Y, Guan WL, Zhang RX, Xiao WW, Cai PQ, Liu M, Lin JZ, Wang FL, Li C, Quan TT, Xi SY, Zhang HZ, Pan ZZ, Wang F, Xu RH. Neoadjuvant PD-1 blockade with sintilimab in mismatch-repair deficient, locally advanced rectal cancer: an open-label, single-centre phase 2 study. Lancet Gastroenterol Hepatol. 2023 May;8(5):422-431. Epub 2023 Mar 1. [CrossRef] [PubMed]
- Zhang X, Yang R, Wu T, Cai X, Li G, Yu K, Li Y, Ding R, Dong C, Li J, Hu R, Feng Q and Li Y (2022) Efficacy and Safety of Neoadjuvant Monoimmunotherapy With PD-1 Inhibitor for dMMR/MSI⁃H Locally Advanced Colorectal Cancer: A Single-Center Real-World Study. Front. Immunol. 13:913483. [CrossRef]
- Yang R, Wu T, Yu J, Cai X, Li G, Li X, Huang W, Zhang Y, Wang Y, Yang X, Ren Y, Hu R, Feng Q, Ding P, Zhang X, Li Y. Locally advanced rectal cancer with dMMR/MSI-H may be excused from surgery after neoadjuvant anti-PD-1 monotherapy: a multiple-center, cohort study. Front Immunol. 2023 Jun 27;14:1182299. [CrossRef] [PubMed] [PubMed Central]
- Kothari A, White MG, Peacock O, Kaur H, Palmquist SM, You N, Taggart M, Salem U, Overman M, Kopetz S, Chang GJ. Pathological response following neoadjuvant immunotherapy in mismatch repair-deficient/microsatellite instability-high locally advanced, non-metastatic colorectal cancer. Br J Surg. 2022 May 16;109(6):489-492. [CrossRef] [PubMed]
- Demisse, R., Damle, N., Kim, E., Gong, J., Fakih, M., Eng, C., Oesterich, L., McKenny, M., Ji, J., Liu, J., Louie, R., Tam, K., Gholami, S., Halabi, W., Monjazeb, A., Dayyani, F., & Cho, M. (2020). Neoadjuvant Immunotherapy–Based Systemic Treatment in MMR-Deficient or MSI-High Rectal Cancer: Case Series. Journal of the National Comprehensive Cancer Network J Natl Compr Canc Netw, 18(7), 798-804. [CrossRef]
- Chalabi M, Fanchi LF, Dijkstra KK, Van den Berg JG, Aalbers AG, Sikorska K, Lopez-Yurda M, Grootscholten C, Beets GL, Snaebjornsson P, Maas M, Mertz M, Veninga V, Bounova G, Broeks A, Beets-Tan RG, de Wijkerslooth TR, van Lent AU, Marsman HA, Nuijten E, Kok NF, Kuiper M, Verbeek WH, Kok M, Van Leerdam ME, Schumacher TN, Voest EE, Haanen JB. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat Med. 2020 Apr;26(4):566-576. Epub 2020 Apr 6. [CrossRef] [PubMed]
- Phipps AI, Lindor NM, Jenkins MA, Baron JA, Win AK, Gallinger S, Gryfe R, Newcomb PA. Colon and rectal cancer survival by tumor location and microsatellite instability: the Colon Cancer Family Registry. Dis Colon Rectum. 2013 Aug;56(8):937-44. [CrossRef] [PubMed] [PubMed Central]
- Fabrizio DA, George TJ Jr, Dunne RF, Frampton G, Sun J, Gowen K, Kennedy M, Greenbowe J, Schrock AB, Hezel AF, Ross JS, Stephens PJ, Ali SM, Miller VA, Fakih M, Klempner SJ. Beyond microsatellite testing: assessment of tumor mutational burden identifies subsets of colorectal cancer who may respond to immune checkpoint inhibition. J Gastrointest Oncol. 2018 Aug;9(4):610-617. [CrossRef] [PubMed] [PubMed Central]
- Ma X, Riaz N, Samstein RM, Lee M, Makarov V, Valero C, Chowell D, Kuo F, Hoen D, Fitzgerald CWR, Jiang H, Alektiar J, Alban TJ, Juric I, Parthasarathy PB, Zhao Y, Sabio EY, Verma R, Srivastava RM, Vuong L, Yang W, Zhang X, Wang J, Chu LK, Wang SL, Kelly DW, Pei X, Chen J, Yaeger R, Zamarin D, Zehir A, Gönen M, Morris LGT, Chan TA. Functional landscapes of POLE and POLD1 mutations in checkpoint blockade-dependent antitumor immunity. Nat Genet. 2022 Jul;54(7):996-1012. Epub 2022 Jul 11. [CrossRef] [PubMed] [PubMed Central]
- Zhang Z, Liu X, Chen D, Yu J. Radiotherapy combined with immunotherapy: the dawn of cancer treatment. Signal Transduct Target Ther. 2022 Jul 29;7(1):258. [CrossRef] [PubMed] [PubMed Central]
- Yuki S, Bando H, Tsukada Y, Inamori K. Short-term results of VOLTAGE-A: Nivolumab monotherapy and subsequent radical surgery following preoperative chemoradiotherapy in patients with microsatellite stable and microsatellite instability-high locally advanced rectal cancer. JCO. 2020;38(15_suppl):4100-4100. [CrossRef]
- Grassi E, Zingaretti C, Petracci E, Corbelli J, Papiani G, Banchelli I, Valli I, Frassineti GL, Passardi A, Di Bartolomeo M, Pietrantonio F, Gelsomino F, Carandina I, Banzi M, Martella L, Bonetti AV, Boccaccino A, Molinari C, Marisi G, Ugolini G, Nanni O, Tamberi S. Phase II study of capecitabine-based concomitant chemoradiation followed by durvalumab as a neoadjuvant strategy in locally advanced rectal cancer: the PANDORA trial. ESMO Open. 2023 Oct;8(5):101824. Epub 2023 Sep 27. [CrossRef] [PubMed] [PubMed Central]
- Lin Z, Cai M, Zhang P, Li G, Liu T, Li X, Cai K, Nie X, Wang J, Liu J, Liu H, Zhang W, Gao J, Wu C, Wang L, Fan J, Zhang L, Wang Z, Hou Z, Ma C, Yang K, Wu G, Tao K, Zhang T. Phase II, single-arm trial of preoperative short-course radiotherapy followed by chemotherapy and camrelizumab in locally advanced rectal cancer. J Immunother Cancer. 2021 Nov;9(11):e003554. Erratum in: J Immunother Cancer. 2022 Feb;10(2):. [CrossRef] [PubMed] [PubMed Central]
- Shamseddine, Y. Zeidan, Y. Bouferraa, R. Turfa, J. Kattan, D. Mukherji, S. Temraz, K. Alqasem, R. Amarin, T. Al Awabdeh, S. Deeba, S. Doughan, I. Mohamad, M. Elkhaldi, F. Daoud, M. Al Masri, A. Dabous, A. Hushki, M. Charafeddine, M. Al Darazi, F. Geara. Efficacy and safety of neoadjuvant short-course radiation followed by mFOLFOX-6 plus avelumab for locally-advanced rectal adenocarcinoma: Averectal study. Annals of Oncology. 2021;32:S215. [CrossRef]
- Salvatore L, Bensi M, Corallo S, Bergamo F, Pellegrini I, Rasola C, Borelli B, Tamburini E. Randon G, Galuppo S, Boccaccino A, Viola M, Auriemma A, Fea E, Barbara C, Bustreo S, Smiroldo V, Barbaro B, Gambacorta M, Tortora G. (2021). Phase II study of preoperative (PREOP) chemoradiotherapy (CTRT) plus avelumab (AVE) in patients (PTS) with locally advanced rectal cancer (LARC): The AVANA study.. Journal of Clinical Oncology. 39. 3511-3511. [CrossRef]
- Kasi PM, Hidalgo M, Jafari MD, Yeo H, Lowenfeld L, Khan U, Nguyen ATH, Siolas D, Swed B, Hyun J, Khan S, Wood M, Samstein B, Rocca JP, Ocean AJ, Popa EC, Hunt DH, Uppal NP, Garrett KA, Pigazzi A, Zhou XK, Shah MA, Hissong E. Neoadjuvant botensilimab plus balstilimab response pattern in locally advanced mismatch repair proficient colorectal cancer. Oncogene. 2023 Oct;42(44):3252-3259. Epub 2023 Sep 21. [CrossRef] [PubMed] [PubMed Central]
- El-Khoueiry A, Fakih M, Gordon M, Tsimberidou A, Bullock A, Wilky B, Trent J, Margolin K, Mahadevan D, Balmanoukian A, Sanborn R, Schwartz G, Bockorny B, Moser J, Grossman J, Feliu W, Rosenthal K, O'Day S, Lenz HJ, Schlechter B (2023). Results from a phase 1a/1b study of botensilimab (BOT), a novel innate/adaptive immune activator, plus balstilimab (BAL; anti-PD-1 antibody) in metastatic heavily pretreated microsatellite stable colorectal cancer (MSS CRC).. Journal of Clinical Oncology. 41. LBA8-LBA8. [CrossRef]
- Maas M, Nelemans PJ, Valentini V, Das P, Rödel C, Kuo LJ, Calvo FA, García-Aguilar J, Glynne-Jones R, Haustermans K, Mohiuddin M, Pucciarelli S, Small W Jr, Suárez J, Theodoropoulos G, Biondo S, Beets-Tan RG, Beets GL. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data. Lancet Oncol. 2010 Sep;11(9):835-44. Epub 2010 Aug 6. [CrossRef] [PubMed]
- Zhang X, Ma S, Guo Y, Luo Y, Li L. Total neoadjuvant therapy versus standard therapy in locally advanced rectal cancer: A systematic review and meta-analysis of 15 trials. PLoS One. 2022 Nov 4;17(11):e0276599. [CrossRef] [PubMed] [PubMed Central]
- Habr-Gama A, Perez RO, Nadalin W, Sabbaga J, Ribeiro U Jr, Silva e Sousa AH Jr, Campos FG, Kiss DR, Gama-Rodrigues J. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy: long-term results. Ann Surg. 2004 Oct;240(4):711-7; discussion 717-8. [CrossRef] [PubMed] [PubMed Central]
- Loria A, Tejani MA, Temple LK, Justiniano CF, Melucci AD, Becerra AZ, Monson JRT, Aquina CT, Fleming FJ. Practice Patterns for Organ Preservation in US Patients With Rectal Cancer, 2006-2020. JAMA Oncol. 2024 Jan 1;10(1):79-86. [CrossRef] [PubMed] [PubMed Central]
- Zhang X, Ding R, Li J, Wu T, Shen Z, Li S, Zhang Y, Dong C, Shang Z, Zhou H, Li T, Li G, Li Y. Efficacy and safety of the "watch-and-wait" approach for rectal cancer with clinical complete response after neoadjuvant chemoradiotherapy: a meta-analysis. Surg Endosc. 2022 Apr;36(4):2233-2244. Epub 2022 Jan 3. [CrossRef] [PubMed]
- van der Valk MJM, Hilling DE, Bastiaannet E, Meershoek-Klein Kranenbarg E, Beets GL, Figueiredo NL, Habr-Gama A, Perez RO, Renehan AG, van de Velde CJH; IWWD Consortium. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): an international multicentre registry study. Lancet. 2018 Jun 23;391(10139):2537-2545. [CrossRef] [PubMed]
- Wang J, Zhang L, Wang M, Zhang J, Wang Y, Wan J, Li G, Zhang H, Wang Y, Wu R, Zhang Z, Li X, Xu Y, Zhu J, Shen L, Xia F, Zhang Z. Long-term outcomes in a retrospective cohort of patients with rectal cancer with complete response after total neoadjuvant therapy: a propensity-score weighted analysis. Ther Adv Med Oncol. 2023 Sep 8;15:17588359231197955. [CrossRef] [PubMed] [PubMed Central]
- Verheij FS, Omer DM, Williams H, Lin ST, Qin LX, Buckley JT, Thompson HM, Yuval JB, Kim JK, Dunne RF, Marcet J, Cataldo P, Polite B, Herzig DO, Liska D, Oommen S, Friel CM, Ternent C, Coveler AL, Hunt S, Gregory A, Varma MG, Bello BL, Carmichael JC, Krauss J, Gleisner A, Guillem JG, Temple L, Goodman KA, Segal NH, Cercek A, Yaeger R, Nash GM, Widmar M, Wei IH, Pappou EP, Weiser MR, Paty PB, Smith JJ, Wu AJ, Gollub MJ, Saltz LB, Garcia-Aguilar J. Long-Term Results of Organ Preservation in Patients With Rectal Adenocarcinoma Treated With Total Neoadjuvant Therapy: The Randomized Phase II OPRA Trial. J Clin Oncol. 2024 Feb 10;42(5):500-506. Epub 2023 Oct 26. [CrossRef] [PubMed]
- Fernandez LM, São Julião GP, Figueiredo NL, Beets GL, van der Valk MJM, Bahadoer RR, Hilling DE, Meershoek-Klein Kranenbarg E, Roodvoets AGH, Renehan AG, van de Velde CJH, Habr-Gama A, Perez RO; International Watch & Wait Database Consortium. Conditional recurrence-free survival of clinical complete responders managed by watch and wait after neoadjuvant chemoradiotherapy for rectal cancer in the International Watch & Wait Database: a retrospective, international, multicentre registry study. Lancet Oncol. 2021 Jan;22(1):43-50. Epub 2020 Dec 11. [CrossRef] [PubMed]
- Lin W, Wee IJY, Seow-En I, Chok AY, Tan EK. Survival outcomes of salvage surgery in the watch-and-wait approach for rectal cancer with clinical complete response after neoadjuvant chemoradiotherapy: a systematic review and meta-analysis. Ann Coloproctol. 2023 Dec;39(6):447-456. Epub 2023 Dec 28. [CrossRef] [PubMed] [PubMed Central]
- Dattani M, Heald RJ, Goussous G, Broadhurst J, São Julião GP, Habr-Gama A, Perez RO, Moran BJ. Oncological and Survival Outcomes in Watch and Wait Patients With a Clinical Complete Response After Neoadjuvant Chemoradiotherapy for Rectal Cancer: A Systematic Review and Pooled Analysis. Ann Surg. 2018 Dec;268(6):955-967. [CrossRef] [PubMed]
- Ferri V, Vicente E, Quijano Y, Duran H, Diaz E, Fabra I, Malave L, Ruiz P, Costantini G, Pizzuti G, Cubillo A, Rubio MC, Cañamaque LG, Alfonsel JN, Caruso R. Light and shadow of watch-and-wait strategy in rectal cancer: oncological result, clinical outcomes, and cost-effectiveness analysis. Int J Colorectal Dis. 2023 Dec 5;38(1):277. [CrossRef] [PubMed]
- Han Z, Li M, Chen J, Ji D, Zhan T, Peng Y, Xue W, Li Y, Cai Y, Sun Y, Wu Q, Du C, Gu J. Surgery may not benefit patients with locally advanced rectal cancer who achieved clinical complete response following neoadjuvant chemoradiotherapy. Asian J Surg. 2022 Jan;45(1):97-104. Epub 2021 Apr 20. [CrossRef] [PubMed]
- Yu G, Lu W, Jiao Z, Qiao J, Ma S, Liu X. A meta-analysis of the watch-and-wait strategy versus total mesorectal excision for rectal cancer exhibiting complete clinical response after neoadjuvant chemoradiotherapy. World J Surg Oncol. 2021 Oct 18;19(1):305. [CrossRef] [PubMed] [PubMed Central]
- Fernandez LM, São Julião GP, Renehan AG, Beets GL, Papoila AL, Vailati BB, Bahadoer RR, Kranenbarg EM, Roodvoets AGH, Figueiredo NL, Van De Velde CJH, Habr-Gama A, Perez RO; International Watch & Wait Database (IWWD) Consortium. The Risk of Distant Metastases in Patients With Clinical Complete Response Managed by Watch and Wait After Neoadjuvant Therapy for Rectal Cancer: The Influence of Local Regrowth in the International Watch and Wait Database. Dis Colon Rectum. 2023 Jan 1;66(1):41-49. Epub 2022 Oct 21. [CrossRef] [PubMed]
- Smith JJ, Strombom P, Chow OS, Roxburgh CS, Lynn P, Eaton A, Widmar M, Ganesh K, Yaeger R, Cercek A, Weiser MR, Nash GM, Guillem JG, Temple LKF, Chalasani SB, Fuqua JL, Petkovska I, Wu AJ, Reyngold M, Vakiani E, Shia J, Segal NH, Smith JD, Crane C, Gollub MJ, Gonen M, Saltz LB, Garcia-Aguilar J, Paty PB. Assessment of a Watch-and-Wait Strategy for Rectal Cancer in Patients With a Complete Response After Neoadjuvant Therapy. JAMA Oncol. 2019 Apr 1;5(4):e185896. Epub 2019 Apr 11. [CrossRef] [PubMed] [PubMed Central]
- Beard BW, Rettig RL, Ryoo JJ, Parker RA, McLemore EC, Attaluri V. Watch-and-Wait Compared to Operation for Patients with Complete Response to Neoadjuvant Therapy for Rectal Cancer. J Am Coll Surg. 2020 Dec;231(6):681-692. Epub 2020 Oct 26. [CrossRef] [PubMed]
- Socha J, Kępka L, Michalski W, Paciorek K, Bujko K. The risk of distant metastases in rectal cancer managed by a watch-and-wait strategy - A systematic review and meta-analysis. Radiother Oncol. 2020 Mar;144:1-6. Epub 2019 Nov 8. [CrossRef] [PubMed]
- Meyer VM, Meuzelaar RR, Schoenaker IJH, de Groot JB, Reerink O, de Vos Tot Nederveen Cappel WH, Beets GL, van Westreenen HL. Delayed TME Surgery in a Watch-and-Wait Strategy After Neoadjuvant Chemoradiotherapy for Rectal Cancer: An Analysis of Hospital Costs and Surgical and Oncological Outcomes. Dis Colon Rectum. 2023 May 1;66(5):671-680. Epub 2021 Nov 24. [CrossRef] [PubMed]
- Tan S, Gao Q, Cui Y, Ou Y, Huang S, Feng W. Oncologic outcomes of watch-and-wait strategy or surgery for low to intermediate rectal cancer in clinical complete remission after adjuvant chemotherapy: a systematic review and meta-analysis. Int J Colorectal Dis. 2023 Oct 3;38(1):246. [CrossRef] [PubMed]
- Garcia-Aguilar J, Patil S, Gollub MJ, Kim JK, Yuval JB, Thompson HM, Verheij FS, Omer DM, Lee M, Dunne RF, Marcet J, Cataldo P, Polite B, Herzig DO, Liska D, Oommen S, Friel CM, Ternent C, Coveler AL, Hunt S, Gregory A, Varma MG, Bello BL, Carmichael JC, Krauss J, Gleisner A, Paty PB, Weiser MR, Nash GM, Pappou E, Guillem JG, Temple L, Wei IH, Widmar M, Lin S, Segal NH, Cercek A, Yaeger R, Smith JJ, Goodman KA, Wu AJ, Saltz LB. Organ Preservation in Patients With Rectal Adenocarcinoma Treated With Total Neoadjuvant Therapy. J Clin Oncol. 2022 Aug 10;40(23):2546-2556. Epub 2022 Apr 28. [CrossRef] [PubMed] [PubMed Central]
- Wang QX, Zhang R, Xiao WW, Zhang S, Wei MB, Li YH, Chang H, Xie WH, Li LR, Ding PR, Chen G, Zeng ZF, Wang WH, Wan XB, Gao YH. The watch-and-wait strategy versus surgical resection for rectal cancer patients with a clinical complete response after neoadjuvant chemoradiotherapy. Radiat Oncol. 2021 Jan 19;16(1):16. [CrossRef] [PubMed] [PubMed Central]
- Araujo RO, Valadão M, Borges D, Linhares E, de Jesus JP, Ferreira CG, Victorino AP, Vieira FM, Albagli R. Nonoperative management of rectal cancer after chemoradiation opposed to resection after complete clinical response. A comparative study. Eur J Surg Oncol. 2015 Nov;41(11):1456-63. Epub 2015 Aug 29. [CrossRef] [PubMed]
- Benson AB 3rd, Venook AP, Bekaii-Saab T, Chan E, Chen YJ, Cooper HS, Engstrom PF, Enzinger PC, Fenton MJ, Fuchs CS, Grem JL, Grothey A, Hochster HS, Hunt S, Kamel A, Kirilcuk N, Leong LA, Lin E, Messersmith WA, Mulcahy MF, Murphy JD, Nurkin S, Rohren E, Ryan DP, Saltz L, Sharma S, Shibata D, Skibber JM, Sofocleous CT, Stoffel EM, Stotsky-Himelfarb E, Willett CG, Gregory KM, Freedman-Cass D. Rectal Cancer, Version 2.2015. J Natl Compr Canc Netw. 2015 Jun;13(6):719-28; quiz 728. [CrossRef] [PubMed]
- Martens MH, Maas M, Heijnen LA, Lambregts DM, Leijtens JW, Stassen LP, Breukink SO, Hoff C, Belgers EJ, Melenhorst J, Jansen R, Buijsen J, Hoofwijk TG, Beets-Tan RG, Beets GL. Long-term Outcome of an Organ Preservation Program After Neoadjuvant Treatment for Rectal Cancer. J Natl Cancer Inst. 2016 Aug 10;108(12):djw171. [CrossRef] [PubMed]
- Al-Najami I, Jones HJ, Dickson EA, Muirhead R, Deding U, James DR, Cunningham C. Rectal cancer: Watch-and-wait and continuing the rectal-preserving strategy with local excision for incomplete response or limited regrowth. Surg Oncol. 2021 Jun;37:101574. Epub 2021 Apr 3. [CrossRef] [PubMed]
- Chan HT, Nagayama S, Otaki M, Chin YM, Fukunaga Y, Ueno M, Nakamura Y, Low SK. Tumor-informed or tumor-agnostic circulating tumor DNA as a biomarker for risk of recurrence in resected colorectal cancer patients. Front Oncol. 2023 Jan 26;12:1055968. [CrossRef] [PubMed] [PubMed Central]
- Vidal J, Casadevall D, Bellosillo B, Pericay C, Garcia-Carbonero R, Losa F, Layos L, Alonso V, Capdevila J, Gallego J, Vera R, Salud A, Martin-Richard M, Nogué M, Cillán E, Maurel J, Faull I, Raymond V, Fernández-Martos C, Montagut C. Clinical Impact of Presurgery Circulating Tumor DNA after Total Neoadjuvant Treatment in Locally Advanced Rectal Cancer: A Biomarker Study from the GEMCAD 1402 Trial. Clin Cancer Res. 2021 May 15;27(10):2890-2898. Epub 2021 Mar 16. [CrossRef] [PubMed]
- Zhou J, Wang C, Lin G, Xiao Y, Jia W, Xiao G, Liu Q, Wu B, Wu A, Qiu H, Zhang F, Hu K, Xue H, Shen Z, Wang Z, Han J, Niu B, Xu Y, Yu Z, Yang L. Serial Circulating Tumor DNA in Predicting and Monitoring the Effect of Neoadjuvant Chemoradiotherapy in Patients with Rectal Cancer: A Prospective Multicenter Study. Clin Cancer Res. 2021 Jan 1;27(1):301-310. Epub 2020 Oct 12. [CrossRef] [PubMed]
- Wang Y, Yang L, Bao H, Fan X, Xia F, Wan J, Shen L, Guan Y, Bao H, Wu X, Xu Y, Shao Y, Sun Y, Tong T, Li X, Xu Y, Cai S, Zhu J, Zhang Z. Utility of ctDNA in predicting response to neoadjuvant chemoradiotherapy and prognosis assessment in locally advanced rectal cancer: A prospective cohort study. PLoS Med. 2021 Aug 31;18(8):e1003741. [CrossRef] [PubMed] [PubMed Central]
- Morais M, Pinto DM, Machado JC, Carneiro S. ctDNA on liquid biopsy for predicting response and prognosis in locally advanced rectal cancer: A systematic review. Eur J Surg Oncol. 2022 Jan;48(1):218-227. Epub 2021 Sep 3. [CrossRef] [PubMed]
- Chang L, Zhang X, He L, Ma Q, Fang T, Jiang C, Ma Z, Li Q, Wu C, Tao J. Prognostic Value of ctDNA Detection in Patients With Locally Advanced Rectal Cancer Undergoing Neoadjuvant Chemoradiotherapy: A Systematic Review and Meta-analysis. Oncologist. 2023 Dec 11;28(12):e1198-e1208. [CrossRef] [PubMed] [PubMed Central]
- Piercey O, Tie J. Circulating tumour DNA in the evolving treatment landscape of locally advanced rectal cancer: where does it fit in? Ther Adv Med Oncol. 2023 Mar 14;15:17588359231160138. [CrossRef] [PubMed] [PubMed Central]
- Reinert T, Henriksen TV, Christensen E, Sharma S, Salari R, Sethi H, Knudsen M, Nordentoft I, Wu HT, Tin AS, Heilskov Rasmussen M, Vang S, Shchegrova S, Frydendahl Boll Johansen A, Srinivasan R, Assaf Z, Balcioglu M, Olson A, Dashner S, Hafez D, Navarro S, Goel S, Rabinowitz M, Billings P, Sigurjonsson S, Dyrskjøt L, Swenerton R, Aleshin A, Laurberg S, Husted Madsen A, Kannerup AS, Stribolt K, Palmelund Krag S, Iversen LH, Gotschalck Sunesen K, Lin CJ, Zimmermann BG, Lindbjerg Andersen C. Analysis of Plasma Cell-Free DNA by Ultradeep Sequencing in Patients With Stages I to III Colorectal Cancer. JAMA Oncol. 2019 Aug 1;5(8):1124-1131. Erratum in: JAMA Oncol. 2019 Jun 13. [CrossRef] [PubMed] [PubMed Central]
- Tie J, Cohen JD, Wang Y, Christie M, Simons K, Lee M, Wong R, Kosmider S, Ananda S, McKendrick J, Lee B, Cho JH, Faragher I, Jones IT, Ptak J, Schaeffer MJ, Silliman N, Dobbyn L, Li L, Tomasetti C, Papadopoulos N, Kinzler KW, Vogelstein B, Gibbs P. Circulating Tumor DNA Analyses as Markers of Recurrence Risk and Benefit of Adjuvant Therapy for Stage III Colon Cancer. JAMA Oncol. 2019 Dec 1;5(12):1710-1717. Erratum in: JAMA Oncol. 2019 Dec 1;5(12):1811. [CrossRef] [PubMed] [PubMed Central]
- Khakoo S, Carter PD, Brown G, Valeri N, Picchia S, Bali MA, Shaikh R, Jones T, Begum R, Rana I, Wotherspoon A, Terlizzo M, von Loga K, Kalaitzaki E, Saffery C, Watkins D, Tait D, Chau I, Starling N, Hubank M, Cunningham D. MRI Tumor Regression Grade and Circulating Tumor DNA as Complementary Tools to Assess Response and Guide Therapy Adaptation in Rectal Cancer. Clin Cancer Res. 2020 Jan 1;26(1):183-192. Epub 2019 Dec 18. [CrossRef] [PubMed]
- Murahashi S, Akiyoshi T, Sano T, Fukunaga Y, Noda T, Ueno M, Zembutsu H. Serial circulating tumour DNA analysis for locally advanced rectal cancer treated with preoperative therapy: prediction of pathological response and postoperative recurrence. Br J Cancer. 2020 Sep;123(5):803-810. Epub 2020 Jun 22. [CrossRef] [PubMed] [PubMed Central]
- McDuff SGR, Hardiman KM, Ulintz PJ, Parikh AR, Zheng H, Kim DW, Lennerz JK, Hazar-Rethinam M, Van Seventer EE, Fetter IJ, Nadres B, Eyler CE, Ryan DP, Weekes CD, Clark JW, Cusack JC, Goyal L, Zhu AX, Wo JY, Blaszkowsky LS, Allen J, Corcoran RB, Hong TS. Circulating Tumor DNA Predicts Pathologic and Clinical Outcomes Following Neoadjuvant Chemoradiation and Surgery for Patients With Locally Advanced Rectal Cancer. JCO Precis Oncol. 2021 Jan 12;5:PO.20.00220. [CrossRef] [PubMed] [PubMed Central]
- Hofste LSM, Geerlings MJ, von Rhein D, Rütten H, Westenberg AH, Weiss MM, Gilissen C, Hofste T, van der Post RS, Klarenbeek BR, de Wilt JHW, Ligtenberg MJL; Libic2 collaborators group. Circulating tumor DNA detection after neoadjuvant treatment and surgery predicts recurrence in patients with early-stage and locally advanced rectal cancer. Eur J Surg Oncol. 2023 Jul;49(7):1283-1290. Epub 2023 Jan 31. [CrossRef] [PubMed]
- Tie J, Cohen JD, Wang Y, Li L, Christie M, Simons K, Elsaleh H, Kosmider S, Wong R, Yip D, Lee M, Tran B, Rangiah D, Burge M, Goldstein D, Singh M, Skinner I, Faragher I, Croxford M, Bampton C, Haydon A, Jones IT, S Karapetis C, Price T, Schaefer MJ, Ptak J, Dobbyn L, Silliman N, Kinde I, Tomasetti C, Papadopoulos N, Kinzler K, Volgestein B, Gibbs P. Serial circulating tumour DNA analysis during multimodality treatment of locally advanced rectal cancer: a prospective biomarker study. Gut. 2019 Apr;68(4):663-671. Epub 2018 Feb 2. [CrossRef] [PubMed] [PubMed Central]
- C. Molinari, G. C. Molinari, G. Marisi, G. Laliotis, E. Spickard, I.G. Rapposelli, E. Petracci, G.V. George, S. Sharma, A. Jurdi, H. Sethi, M.C. Liu, P. Ulivi, M. Canale, L. Saragoni, R. Panzacchi, G.L. Frassineti, M. Muratore, A. Romeo, G. Martinelli, A. Passardi. Assessment of circulating tumor (ct)DNA in patients (pts) with locally advanced rectal cancer (LARC) pts treated with neoadjuvant therapy (NAT). Ann Oncol 2023 Vol 34 Issue 52. [CrossRef]
Figure 1.
New developments in the multidisciplinary management of locally advanced rectal cancer.
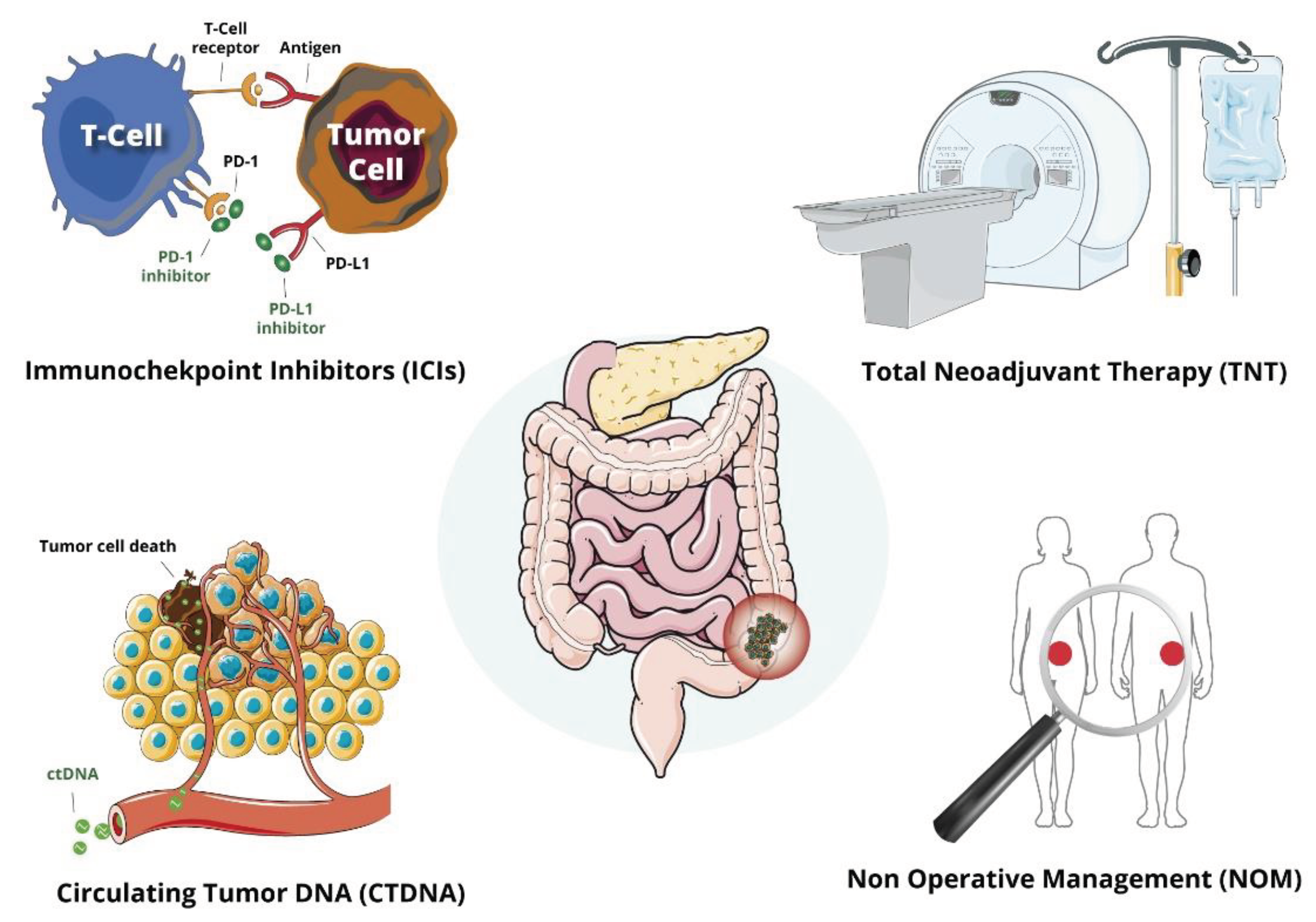
Table 1.
Evaluation of Total Neoadjuvant Treatment (TNT).
| Phase III clinical trials evaluating TNT | |||||||||
| Ref | Study title | Study | N | Stage | Induction | Radiotherapy | Consolidation | pCR | Rec |
| Conroy T. | PRODIGE-23 | Prospective phase III | 461 | cT3-4 or N+ | FOLFIRINOX | LCRT | None | 27.8% | DFS 76% DM 17% |
| Bahadoer, R.R. | RAPIDO | Prospective phase III | 912 | II – III* | None | SCRT | CAPOX/FOLFOX | 28.4% | DrTF 23.7% LLR 8.3% DM 20% |
| Jin J. | STELLAR | Prospective phase III | 599 | cT3-4 or N+ | None | SCRT | CAPOX | cCR 11.1% | DFS 64.5% LLR 8.4% DM 22.8% |
| Omission of radiotherapy | |||||||||
| Ref | Study title | Study | Stage | Chemiotherapy | Radiotherapy | - | pCR | Rec | |
| Deng Y. | FOWARC | Prospective phase III | 495 | cT3-4 or N+ | mFOLFOX6 | None | - | 6.5% | DFS 73.5% LR 1.8% |
| Schrag D. | PROSPECT | Prospective phase III | 1128 | cT2-3 or N+ | FOLFOX | CTRT in selected cases ** | - | 21.9% | DFS 80.8% LR 1.8% |
| Induction vs consolidation chemoterapy | |||||||||
| Ref | Study title | Study | Stage | Induction | Radiotherapy | Consolidation | pCR | Rec | |
| Fokas E. | CAO/ARO/AIO-12 | Prospective phase II | 306 | II - III | FOLFOX (A) | LCRT | FOLFOX (B) | 17% (A) 25% (B) |
LLR 6%vs5% DM 18%vs16% |
| Garcia-Aguilar J. | OPRA | Prospective phase II | 324 | II - III | FOLFOX (A) | LCRT | FOLFOX (B) | 10% (A) 8% (B) | 5y DFS 71% vs 69% |
* High-risk defined as having at least one of the following criteria at MRI staging: cT4a, cT4b, extramural vascular invasion (EMVI), cN2 (metastasis in four or more locoregional lymph nodes), involved mesorectal fascia (MRF), or enlarged lateral lymph nodes. ** Primary tumor decreased in size by less than 20% or FOLFOX discontinued because of side effects.
Table 2.
Trials investigating the efficacy of ICIs in the treatment of LARC.
| ICI | Study title/ Reference |
Patients (N°) |
Induction | Radio therapy |
Consolidation | pCR |
|---|---|---|---|---|---|---|
| dMMR/MSI | ||||||
| Dostarlimab | NCT04165772 | 12 | Dostarlimab | LCRT | None | 100% |
| Sintilimab | NCT04304209 | 17 | Sintilimab | None | None | 75% |
| Tislelizumab, Sintilimab, Pembrolizumab | Zhang X. | 32 | None | Not Specified* | None | 100% |
| Tislelizumab, Sintilimab, Pembrolizumab | Yang R. | 20 | None | None | None | 90% |
| Pembrolizumab, Nivolumab +/- CT | Kothari A. | 9 | None | None | None | 89% |
| Pembrolizumab, Nivolumab +/- CT** | Demisse R. | 3 | None | Not Specified*** | None | 100% |
| MSS | ||||||
| Nivolumab | VOLTAGE-A | 37 | Nivolumab | LCRT | None | 30% 7 |
| Camrelizumab | NCT04231552 | 26 | None | SCRT | CAPOX + Camrelizumab (2 x 21 days cycles) |
46.2%9 |
| Durvalumab | PANDORA | 46 | None | LCRT | Durvalumab | 34.5%,8 |
| Avelumab | AVERECTAL | 26 | None | SCRT | FOLFOX + Avelumab | 37%10 |
| Avelumab | AVANA | 38 | None | LCRT | Avelumab | 23%11 |
*2 patients underwent nCRT (neoadjuvant chemoradiotherapy). ** 1 patient received neoadiuvant Pembrolizumab and FOLFOX. *** 1 patient receveid neoadjuvant chemoradiation, then ICI at progression.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



