Submitted:
19 March 2024
Posted:
21 March 2024
You are already at the latest version
Abstract
Abstract: Exercise has been repeatedly shown to be safe and beneficial for cancer survivors. However, there is no normative guideline for exercise prescription, and it is under exploration. Therefore, this literature review aims to provide some advice for the formulation of exercise prescriptions for patients with breast cancer-related lymphedema (BCRL) from the perspective of reducing lymphedema severity. A review of relevant studies published before November 2023 was conducted using three scientific databases PubMed, Embase, and Scopus. A total of 2696 articles were found. Eventually, 13 studies fulfilled the inclusion criteria and were included in this literature review. We concluded daily, or nearly daily exercise at home can be recommended. Moreover, reduced lymphedema severity may not be maintained after ceasing the exercise program, so exercise should be a lifelong practice.
Keywords:
Breast cancer-related lymphedema
; exercise
; physical activity
; Yoga
; resistance exercise
1. Introduction
Breast cancer is the most common cancer in females and the most common cancer overall [1]. Recent statistics reported by the World Health Organization indicate that 2.3 million women were diagnosed with breast cancer and 685,000 of them passed away globally in 2020, with 7.8 million women diagnosed with breast cancer in the past 5 years [2]. The 5-year relative survival rate for women with localized breast cancer can be up to 99% with the improvement of early detection, according to statistics from diagnosis between 2011 and 2017 [3]. However, they may face a challenge, lymphedema. Some researchers believe that 20% of breast cancer survivors suffer from lymphedema [4,5]. In fact, the data is unclear, and the percentage could be much higher. One study shows lymphedema occurs in 94% of breast cancer survivors based on various methods, timing, and criteria of diagnosis as well as the design of studies [6]. Moreover, lymphedema can occur at any time from the initial of the treatments and this risk continues to the end of their life [7]. Due to the high incidence of breast cancer and its related lymphedema, more exploration is critical.
Lymphedema is defined as the inability of the lymphatic system to transport lymph fluid out of the affected area resulting in an abnormal accumulation of protein-rich fluid in the interstitial tissues [8,9]. Generally, it can be divided into 2 types: primary and secondary lymphedema [10]. BCRL is the most prevalent form of secondary lymphedema [10]. During the cancer treatment, the lymphatic system can be partially removed, disturbing the filtration and normal flow of the lymphatic fluid so that it accumulates in the lymphatic vessel and finally exits to interstitial tissues through the vessel wall [11].
It is important to note that lymphedema is incurable and chronic [12]. Fortunately, there are some effective management methods available, and they are more likely to be useful at the early stage than late stage [13]. Although some recent studies show that surgical treatments may be superior to non-surgical treatments to some extent, non-surgical treatments are still emphasized as indispensable [14,15]. Moreover, surgical treatments may be suggested when non-surgical treatments cannot control the symptoms, especially in the early stage of lymphedema [13]. Non-surgical treatments consist of complete decongestive therapy (CDT), manual lymph drainage (MLD), compression therapy, compression garments, skin care, advanced pneumatic compression pumps, exercise, and laser therapy [14]. Of those, CDT, also called complex decongestive physiotherapy (CDP), including MLD, bandaging, compression, skin care, and exercise, has been most widely used as a standard treatment [10,16,17]. However, exercise, as part of the standard management, is far less understood because it was thought to be unsafe for breast cancer survivors to be involved in upper body exercise as it could induce and aggravate lymphedema [18].
In 1998, a study of dragon boat racing, as a milestone, was reported to suggest that exercise might play an important role in recovering from BCRL [19]. Since then, a series of studies with exercise interventions in cancer survivors with lymphedema have been conducted, followed by literature reviews. Present literature reviews have predominantly focused on determining the effects of a certain type of exercise, such as resistance training [12,20], Yoga [21,22], and water-based exercise [23] on cancer survivors with lymphedema, and exercise has been repeatedly shown to be safe and beneficial for cancer survivors. However, there is no normative guideline for exercise prescription, and it is under exploration. Therefore, this literature review aims to provide some advice for the formulation of exercise prescriptions for patients with BCRL from the perspective of reducing lymphedema severity.
2. Methods
A review of relevant studies published before November 2023 was conducted using three scientific databases PubMed, Embase, and Scopus. The key terms searched were “breast cancer” AND “lymphedema” OR “lymphoedema” AND “exercise”. Further searching terms were “weightlifting” OR “physical activity” OR “Yoga” OR “Pilates” OR “resistance training” OR “swimming” OR “strength training” OR “aerobic exercise” OR “water-based exercise” OR “aqua therapy” and possible variations of each exercise type. The inclusion criteria were: (i) randomized controlled trials (RCTs), (ii) inclusion of adult participants (>18) living with BCRL, (iii) peer-reviewed and published in the English language, (iv) completed studies with objective measurement of lymphedema severity as one of the outcomes reported, and (v) an organized exercise plan. The exclusion criteria were: (i) some or all participants at high risk of lymphedema, (ii) randomized cross-over control trials, (iii) articles without English translations, (iv) studies with experimental study variables (such as weight control through dietary management) other than exercise, but the effects of exercise cannot be isolated; (v) ongoing experimental studies, (vi) physical therapy as the intervention, (vii) the control group was given any kind of exercise interventions except for self-care or standard care.
A total of 2696 articles were found. After the removal of duplicates, 1587 articles were eligible. The process of selection could be divided into 3 stages, carried out by 2 researchers independently. Most of these articles could be excluded by titles and abstracts, and 101 articles entered the second stage — the full-text review. Controversial results were discussed for inclusion. Eventually, 15 RCTs were identified but lymphedema severity was not measured objectively in 2 studies, so finally, 13 studies fulfilled the inclusion criteria and were included in this literature review (Figure 1).
3. Results
The risk of bias of these studies was analyzed by Review Manager 5.4.1. (Figure 2). It showed good methodological quality with low or unclear risk of bias in 11 articles overall but 2 studies were with high risk of bias (Figure 2). Moreover, the modalities of exercise were different among these studies: participants in 2 studies performed Yoga, in 5 studies performed resistance exercise alone, in 4 studies performed a combination of aerobic and resistance exercise, and in 2 studies performed water-based exercise. The duration of the intervention was from 8 weeks to 1 year. The frequency of exercise fluctuated between once per week and daily. The number of subjects ranged from 14 to 177. The outcome that is of primary concern in this literature review, lymphedema severity, was reflected by different indicators and measured by different methods: limb volume by water displacement or Perometer, limb circumference by non-stretch tape, extracellular fluid by Bioimpedance spectroscopy (BIS), tissue composition by dual energy X-ray absorptiometry.
3.1. Yoga
Two RCTs with Yoga intervention by Loudon et al. (2014) and Pasyar et al. (2019) were reviewed (Table 1). The participants in the intervention groups of the two studies had been doing Yoga for a total of 8 weeks, and they were followed up for 4 weeks by Loudon et al. (2014) [24]. However, the frequencies and modes of doing Yoga were not the same. The participants had a 90-minute weekly teacher-led Yoga class and a 45-minute daily DVD-led session in the Loudon et al. (2014) [24] while 3 sessions per week, 2 sessions under the supervision and 1 DVD-led session in the Pasyar et al. (2019) [25]. Moreover, the mean arm volume assessed by water displacement was not reduced in the intervention group, and there was no statistical difference in upper extremity volume between the two groups after 8 weeks in Pasyar et al. (2019) [25]. Nevertheless, in Loudon et al. (2014) [24], the mean arm volume significantly reduced in the intervention group although no significant mean change in arm volume, and extracellular fluid between the two groups was detected after 8 weeks. In the follow-up, the mean arm volume of the intervention group increased [24].
3.2. Resistance Exercise
Five studies with the intervention of resistance exercise were reviewed (Table 2). In Schmitz et al. (2009), 71 women in the weight-lifting group performed a progressive weightlifting program twice per week in a community fitness center for 12 months, and they were professionals-led and group-based for the first 13 weeks [26]. Seventy women in the control group did not change their exercise level during the study. The percentage of women with a change in swelling of 5% or more was similar and the percentage of mean interlimb volume discrepancy between baseline and 12 months was not statistically different between the two groups [26].
The aim of Kim et al. (2010) was to evaluate the different effects of CDP along with or without active resistance exercise [27]. Twenty patients in the active resistive exercise group did progressive resistance exercise (PRE) for 15 minutes per day, 5 times per week for 8 weeks, after CDP, while twenty patients in the nonactive resistive exercise group completed CDP only [27]. The researchers found that the proximal volume of the affected arm had a notable reduction (p < 0.05) in both groups after the interventions [27]. Moreover, the proximal volume of the affected arm had a greater improvement in the active resistive exercise group than in the nonactive resistive exercise group (p < 0.05). However, there were no statistical changes in the distal volume and total volume of the affected arm whether between pre- and post-intervention or between the groups after 8 weeks [27].
Jeffs and Wiseman carried out a study in 2013 [28]. Eleven women in the intervention group completed a daily (about 10-15 minutes) home-based gravity resistive isotonic arm exercise program for 26 weeks, while 13 women in the control group performed self-care only. Limb volume was measured by Perometer. A significant reduction in %excess limb volume (ELV) was found in the intervention group (p = 0.013) at week 26 but not in the control group (p = 0.1), although there was no great difference between the two groups (p = 0.187) [28]. In Bok et al. (2016) [29], 16 patients in the PRE group conducted PRE and CDP, starting from 5 repetitions of 6 exercises, twice a day, and increasing by another 5 repetitions every week, while 16 patients in the non-PRE group were given CDP only. After 8 weeks, both the proximal and distal circumferences of the affected arm measured by tape had a great decrease (p < 0.05) in the PRE group, but this was not found in the non-PRE group [29].
Cormie et al. (2013) performed the first RCT to assess the possibility of different intense resistance exercises as management for patients with BCRL [30]. In their study, two experimental groups completed two 60-minute sessions per week in a group of 8-10 participants under supervision for 3 months and one control group that performed the usual care [30]. In the experimental groups, twenty-two women performed high-intensity resistance exercise (10-6 reps of 75-85% of 1 repetition maximums (RM), 1-4 sets per exercise), while 21 women performed low-intensity resistance exercise (20-15 reps of 55-65% of 1RM, 1-4 sets per exercise) [30]. No difference between these groups was found in terms of swelling of the affected arm, which was assessed by three methods: (1) BIS, (2) dual energy X-ray absorptiometry, and (3) arm circumference measurements [30].
3.3. Complex Exercise
There were 4 RCTs investigating the effect of resistance exercise combined with aerobic exercise on patients with BCRL (Table 3). Nonetheless, the measurements collection and analysis were blinded to the group's allocation in the 3 of 4 trials, Hayes et al. (2009) [31], Schmitz et al. (2019) [32], and Kilbreath et al. (2020) [33], but this was not mentioned in McKenzie & Kalda (2003) [34]. The exercise plans in these studies were various although all training programs were progressive. However, significant differences in lymphedema severity between the intervention group and the control group were observed in none of the studies.
In McKenzie & Kalda (2003), women completed an 8-week progressive upper extremity complex exercise plan, 3 times per week [34]. Lymphedema severity was measured by water displacement and calculated from arm circumference, but there was a great difference in neither method between the exercise group (n = 7) and the control group (n = 7) [34]. Forty-one women in Kilbreath et al. (2020) completed three 1-hour exercise sessions every week (only the first week under supervision), consisting of 10-min warm-up, 30-minute resistance training (progressive, moderate to vigorous) and two 10-min vigorous-intensity aerobic sessions, whereas 47 women in the control group were not given any exercise advice [33]. The BIS ratio in the exercise group had a considerable decrease in the breast compared with the control group (p = 0.018) but no change in the arms and legs [33].
Hayes et al. (2009) provided a 12-week training program that gradually increased in frequency, intensity, duration, and type, including a total of 20 supervised group-based sessions [31]. The frequency progressed from 3 times to ≥ 4 times per week, the intensity progressed from low to high, and the duration progressed from 20-30 minutes per session to ≥ 45 minutes per session [31]. Walking, floor-based, and water-based aerobic exercises combined with water-based, free-weight, and machine-weight resistance were carried out. Lymphedema status, which was measured by BIS and Perometry, had no significant difference between the intervention group (n = 16) and the control group (n = 16) during either the 12-week intervention or the 12-week follow-up [31].
Eighty-seven participants in the exercise intervention group in Schmitz et al. (2019) performed two sets of 10 repetitions of 9 resistance exercises, twice per week with dumbbells in the first 6 weeks but progressed to 3 sets thereafter [35]. The weights of dumbbells were tailored to each individual and progressed by 0.45-0.9 kg every 2 weeks from 0.45 kg to 9.45 kg. Moreover, six 90-minute weekly classes were offered followed by monthly classes from week 7 [35]. Meanwhile, participants were asked to do aerobic exercise, walking 90 minutes at week 1-3, and gradually increasing to 180 minutes per week by week 7 [35]. After this 52-week exercise program, there was no significant difference between the exercise group and the control group in the percentage of interlimb volume differences assessed by Perometry [35].
3.4. Water-Based Exercise
Two studies implemented water-based exercise or aqua exercise in the intervention group (Table 4). The participants completed 45-minute aqua lymphatic therapy once a week consisting of low-intensity resistance exercise in Tidhar & Katz-Leurer (2010) [36] while a 30-min session of moderate exercise, 3 times a week in Johansson et al. (2013) [37]. Additionally, lymphedema severity was assessed by different methods. The limb volume was measured by using water displacement in Tidhar & Katz-Leurer (2010) [36] but by Perometry in Johansson et al. (2013) [37]. In the latter study, BIS was used to measure the impedance of extracellular fluid, and tissue dielectric constant measurement was used to assess local tissue water. However, whichever methods were used in these two studies, neither a vicious incident nor reduced lymphedema severity was reported [36,37].
4. Discussion
BCRL comes with a multitude of symptoms such as pain, heaviness, tightness, limited range of motion, etc. Localized swelling, which is caused by reserved lymphatic fluid in the interstitial tissue, can be one of the main concerns of cancer survivors with lymphedema [38]. Lymphedema severity may not only affect their physical fitness but also mental health, socialization, and career as well as eventually, QoL may dramatically decline [39]. Unfortunately, lymphedema is incurable so far, but some methods can help manage it [40]. Exercise has been proposed to be safe and effective for managing BCRL in the last twenty years [19]. However, there is limited understanding regarding the effects of various exercise modalities on lymphedema severity.
The effect of exercise on lymphedema severity was shown in 4 of 13 RCTs, 3 studies with resistance exercise alone [27,28,29] and one study with Yoga intervention [24]. In the 3 studies with resistance exercise alone, a significant reduction of lymphedema severity was observed in the intervention group but not in the control group in Bok et al. (2016) [29] and Jeffs & Wiseman (2013) [28]. In Kim et al. (2010) [27], the reduction was noticed in both groups but was statistically greater in the intervention group than in the control group. On the other hand, randomization method and measurement blinding were no reported by Kim et al. (2010), and in Bok et al. (2016), the protocol showed the QoL would be assessed by questionnaire, but the result was not mentioned in the following part, which leads to a high risk of reporting bias although this was not primarily concerned in this review.
However, not all included studies with resistance exercise alone reported reduced lymphedema severity. In Cormie et al. (2013) [30], no considerable change in the extent of swelling was found. Moreover, although significant change in the breast was shown between groups in Kilbreath et al. (2020) [33], BIS is an appropriate tool to measure limb swelling but worked unwell for assessing breast edema, and there was no great change in the BIS ratio in the limbs. Furthermore, the reduction of lymphedema severity was not reported in any other studies with complex exercise although it is a combination of resistance exercise and aerobic exercise. There is no evidence showing that aerobic exercise may weaken the effectiveness of resistance training in mitigating lymphedema severity [35]. Such that, the reduction of lymphedema severity may not be related to the exercise modality itself, like resistance exercise. By looking at the elements of the exercise programs, they are high-frequency (daily or nearly daily), low-intensity (using 0.5 kg dumbbells or gravity-resistance), and short-duration (10-15 minutes per session) in all three studies with reduced lymphedema severity.
Similarly, the daily yoga session can also be used to manage lymphedema symptoms [41], although the relatively high dropout rate had unclear impact on the result and Loudon et al. (2014) assumed that the significant reduction of arm volume in the yoga group may be related to its high mean arm value at the baseline compare with the control group [24]. On the other hand, there was no reduced lymphedema severity noticed in the other studies without a high-frequency exercise program. Overall, exercise frequency is likely to play a significant role in reducing lymphedema severity. Furthermore, this reduction may not be kept after terminating training programs. The reduction in lymphedema severity gained in the intervention period disappeared after the 4-week follow-up in Loudon et al. (2014) [24]. Therefore, people with BCRL may have to maintain a lifelong dedication to exercising.
Another point that has been discussed is whether exercise programs should be supervised. The previous study suggested that supervision should be applied for safety and lessening fear [42], but this review has different findings. Most exercise programs in the reviewed studies were semi-supervised that participants completed some supervised sessions at the designated locations and performed the rest of the sessions at home. In Schmitz et al. (2019) [35], there were 6 weekly professional-led sessions followed by monthly supervised sessions from week 7 to week 52, and no significant difference in lymphedema severity between the intervention and the control groups after 1 year was found. This was partially attributed to inadequate supervision in the study [35]. The researchers claimed that the elements of exercise programs may not get enough attention to be adjusted as needed in the exercise programs with low-frequency supervised sessions [35]. However, reduced lymphedema severity was reported by Jeffs & Wiseman (2013) and Bok et al. (2016) with home-based resistance exercise programs [28,29]. An easy-to-go home-based exercise program can increase adherence because participants can self-determine the time and location of performing the exercise program [28]. In other words, supervision may not be necessary to reduce lymphedema severity and patients with BCRL are likely to benefit from a home-based exercise program with some other means, such as a checklist, exercise diary, unexpected calling [29], instruction sheets provided [28] to increase compliance and adherence.
However, it should be noted there are some limitations. This is a qualitative review given the limited number of eligible studies, various measuring methods, and high heterogeneity of exercise programs, etc. There are several different definitions of “lymphedema” used for participants inclusion criteria in the different studies. Furthermore, the total number of participants in all studies with daily or near-daily exercise is 123, so a larger trial is needed to investigate whether high-frequency exercise can help reduce lymphedema severity.
5. Conclusions
By reviewing these 13 RCTs, we noticed reduced lymphedema severity is shown in 4 studies with 2 different exercise types, resistance exercise alone and Yoga. After looking at and comparing the elements of exercise programs in these studies, reduced lymphedema severity may be associated with “high frequency” exercise programs. Additionally, supervision may not be necessary while home-based exercise programs can be beneficial for cancer survivors to reduce lymphedema severity. Therefore, daily, or nearly daily exercise at home is recommended. Moreover, reduced lymphedema severity may not be maintained after ceasing the exercise program, so exercise should be a lifelong practice.
Author Contributions
Conceptualization, Yanxue Lian and Ananya Gupta; methodology, Yanxue Lian, Ananya Gupta, Yamikani Asefa, and Simran Sandhu; search, Yanxue Lian and Yamikani Asefa; writing—original draft preparation, Yanxue Lian, Yamikani Asefa, and Simran Sandhu; writing—review and editing, Yanxue Lian and Ananya Gupta; supervision, Ananya Gupta; project administration, Ananya Gupta. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Cancer Research Fund International Breast Cancer Statistics. Available online: https://www.wcrf.org/cancer-trends/breast-cancer-statistics/ (accessed on 14 November 2023).
- World Health Organization Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 14 November 2023).
- American Cancer Society Survival Rates for Breast Cancer. Available online: https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/breast-cancer-survival-rates.html (accessed on 3 January 2023).
- DiSipio, T.; Rye, S.; Newman, B.; Hayes, S. Incidence of Unilateral Arm Lymphoedema after Breast Cancer: A Systematic Review and Meta-Analysis. Lancet Oncol 2013, 14, 500–515. [Google Scholar] [CrossRef] [PubMed]
- Erickson, V.S.; Pearson, M.L.; Ganz, P.A.; Adams, J.; Kahn, K.L. Arm Edema in Breast Cancer Patients. JNCI: Journal of the National Cancer Institute 2001, 93, 96–111. [Google Scholar] [CrossRef] [PubMed]
- Armer, J.M.; Stewart, B.R. POST-BREAST CANCER LYMPHEDEMA: INCIDENCE INCREASES FROM 12 TO 30 TO 60 MONTHS. Lymphology 2010, 43, 118. [Google Scholar] [PubMed]
- Manahan, M. Breast Cancer: Lymphedema After Treatment. Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/breast-cancer/breast-cancer-lymphedema-after-treatment (accessed on 3 January 2023).
- Grada, A.A.; Phillips, T.J. Lymphedema: Pathophysiology and Clinical Manifestations. J Am Acad Dermatol 2017, 77, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Kayiran, O.; De La Cruz, C.; Tane, K.; Soran, A. Lymphedema: From Diagnosis to Treatment. Turk J Surg 2017, 33, 51–57. [Google Scholar] [CrossRef]
- Brix, B.; Sery, O.; Onorato, A.; Ure, C.; Roessler, A.; Goswami, N. Biology of Lymphedema. Biology (Basel) 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Hull, M.M. Lymphedema in Women Treated for Breast Cancer. Semin Oncol Nurs 2000, 16, 226–237. [Google Scholar] [CrossRef]
- Hasenoehrl, T.; Palma, S.; Ramazanova, D.; Kölbl, H.; Dorner, T.E.; Keilani, M.; Crevenna, R. Resistance Exercise and Breast Cancer-Related Lymphedema-a Systematic Review Update and Meta-Analysis. Supportive Care in Cancer 2020, 28, 3593–3603. [Google Scholar] [CrossRef]
- Ciudad, P.; Sabbagh, M.D.; Agko, M.; Huang, T.C.T.; Manrique, O.J.; Carmen Román, L.; Reynaga, C.; Delgado, R.; Maruccia, M.; Chen, H.C. Surgical Management of Lower Extremity Lymphedema: A Comprehensive Review. Indian J Plast Surg 2019, 52, 81–92. [Google Scholar] [CrossRef]
- Ciudad, P.; Bolletta, A.; Kaciulyte, J.; Losco, L.; Manrique, O.J.; Cigna, E.; Mayer, H.F.; Escandón, J.M. The Breast Cancer-related Lymphedema Multidisciplinary Approach: Algorithm for Conservative and Multimodal Surgical Treatment. Microsurgery 2023, 43, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Shimbo, K.; Kawamoto, H.; Koshima, I. Comparative Study of Conservative Treatment and Lymphaticovenular Anastomosis with Compression Therapy for Early-Stage Breast Cancer-Related Lymphoedema. Journal of Plastic, Reconstructive & Aesthetic Surgery 2024, 88, 390–396. [Google Scholar] [CrossRef]
- Lasinski, B.B.; Thrift, K.M.K.; Squire, D.C.; Austin, M.K.; Smith, K.M.; Wanchai, A.; Green, J.M.; Stewart, B.R.; Cormier, J.N.; Armer, J.M. A Systematic Review of the Evidence for Complete Decongestive Therapy in the Treatment of Lymphedema From 2004 to 2011. PM&R 2012, 4, 580–601. [Google Scholar] [CrossRef]
- Michopoulos, E.; Papathanasiou, G.; Vasilopoulos, G.; Polikandrioti, M.; Dimakakos, E. Effectiveness and Safety of Complete Decongestive Therapy of Phase I: A Lymphedema Treatment Study in the Greek Population. Cureus 2020, 12. [Google Scholar] [CrossRef]
- S G Rockson Precipitating Factors in Lymphedema: Myths and Realities - PubMed. Cancer 1998, 83, 2814–2816. [CrossRef]
- McKenzie, DC. Abreast in a Boat—a Race against Breast Cancer. Cmaj 1998, 159, 376–378. [Google Scholar] [PubMed]
- Nelson, N.L. Breast Cancer-Related Lymphedema and Resistance Exercise: A Systematic Review. J Strength Cond Res 2016, 30, 2656–2665. [Google Scholar] [CrossRef] [PubMed]
- Wanchai, A.; Armer, J.M. The Effects of Yoga on Breast-Cancer-Related Lymphedema: A Systematic Review. J Health Res 2020, 34, 409–418. [Google Scholar] [CrossRef]
- Wei, C.W.; Wu, Y.C.; Chen, P.Y.; Chen, P.E.; Chi, C.C.; Tung, T.H. Effectiveness of Yoga Interventions in Breast Cancer-Related Lymphedema: A Systematic Review. Complement Ther Clin Pract 2019, 36, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Yeung, W.; Semciw, A.I. Aquatic Therapy for People with Lymphedema: A Systematic Review and Meta-Analysis. Lymphat Res Biol 2018, 16, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Loudon, A.; Barnett, T.; Piller, N.; Immink, M.A.; Williams, A.D. Yoga Management of Breast Cancer-Related Lymphoedema: A Randomised Controlled Pilot-Trial. BMC Complement Altern Med 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Pasyar, N.; Barshan Tashnizi, N.; Mansouri, P.; Tahmasebi, S. Effect of Yoga Exercise on the Quality of Life and Upper Extremity Volume among Women with Breast Cancer Related Lymphedema: A Pilot Study. European Journal of Oncology Nursing 2019, 42, 103–109. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Ahmed, R.L.; Troxel, A.; Cheville, A.; Smith, R.; Lewis-Grant, L.; Bryan, C.J.; Williams-Smith, C.T.; Greene, Q.P. Weight Lifting in Women with Breast-Cancer-Related Lymphedema. N Engl J Med 2009, 361, 664–673. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.S.; Sim, Y.J.; Jeong, H.J.; Kim, G.C. Effect of Active Resistive Exercise on Breast Cancerrelated Lymphedema: A Randomized Controlled Trial. Arch Phys Med Rehabil 2010, 91, 1844–1848. [Google Scholar] [CrossRef] [PubMed]
- Jeffs, E.; Wiseman, T. Randomised Controlled Trial to Determine the Benefit of Daily Home-Based Exercise in Addition to Self-Care in the Management of Breast Cancer-Related Lymphoedema: A Feasibility Study. Support Care Cancer 2013, 21, 1013–1023. [Google Scholar] [CrossRef] [PubMed]
- Bok, S.K.; Jeon, Y.; Hwang, P.S. Ultrasonographic Evaluation of the Effects of Progressive Resistive Exercise in Breast Cancer-Related Lymphedema. Lymphat Res Biol 2016, 14, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; Pumpa, K.; Galvão, D.A.; Turner, E.; Spry, N.; Saunders, C.; Zissiadis, Y.; Newton, R.U. Is It Safe and Efficacious for Women with Lymphedema Secondary to Breast Cancer to Lift Heavy Weights during Exercise: A Randomised Controlled Trial. Journal of Cancer Survivorship 2013, 7, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Reul-Hirche, H.; Turner, J. Exercise and Secondary Lymphedema: Safety, Potential Benefits, and Research Issues. Med Sci Sports Exerc 2009, 41, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.H.; Troxel, A.B.; Dean, L.T.; Demichele, A.; Brown, J.C.; Sturgeon, K.; Zhang, Z.; Evangelisti, M.; Spinelli, B.; Kallan, M.J.; et al. Effect of Home-Based Exercise and Weight Loss Programs on Breast Cancer-Related Lymphedema Outcomes Among Overweight Breast Cancer Survivors: The WISER Survivor Randomized Clinical Trial. JAMA Oncol 2019, 5, 1605–1613. [Google Scholar] [CrossRef]
- Kilbreath, S.L.; Ward, L.C.; Davis, G.M.; Degnim, A.C.; Hackett, D.A.; Skinner, T.L.; Black, D. Reduction of Breast Lymphoedema Secondary to Breast Cancer: A Randomised Controlled Exercise Trial. Breast Cancer Res Treat 2020, 184, 459–467. [Google Scholar] [CrossRef]
- McKenzie, D.C.; Kalda, A.L. Effect of Upper Extremity Exercise on Secondary Lymphedema in Breast Cancer Patients: A Pilot Study. Journal of Clinical Oncology 2003, 21, 463–466. [Google Scholar] [CrossRef]
- Winkels, R.M.; Sturgeon, K.M.; Kallan, M.J.; Dean, L.T.; Zhang, Z.; Evangelisti, M.; Brown, J.C.; Sarwer, D.B.; Troxel, A.B.; Denlinger, C.; et al. The Women in Steady Exercise Research (WISER) Survivor Trial: The Innovative Transdisciplinary Design of a Randomized Controlled Trial of Exercise and Weight-Loss Interventions among Breast Cancer Survivors with Lymphedema. Contemp Clin Trials 2017, 61, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Tidhar, D.; Katz-Leurer, M. Aqua Lymphatic Therapy in Women Who Suffer from Breast Cancer Treatment-Related Lymphedema: A Randomized Controlled Study. Support Care Cancer 2010, 18, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Johansson, K.; Hayes, S.; Speck, R.M.; Schmitz, K.H. Water-Based Exercise for Patients with Chronic Arm Lymphedema: A Randomized Controlled Pilot Trial. Am J Phys Med Rehabil 2013, 92, 312–319. [Google Scholar] [CrossRef]
- Whatley, J.; Street, R.; Kay, S. Experiences of Breast Cancer Related Lymphoedema and the Use of Reflexology for Managing Swelling: A Qualitative Study. Complement Ther Clin Pract 2018, 32, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Hinrichs, C.S.; Watroba, N.L.; Rezaishiraz, H.; Giese, W.; Hurd, T.; Fassl, K.A.; Edge, S.B. Lymphedema Secondary to Postmastectomy Radiation: Incidence and Risk Factors. Ann Surg Oncol 2004, 11, 573–580. [Google Scholar] [CrossRef]
- Hasenoehrl, T.; Keilani, M.; Palma, S.; Crevenna, R. Resistance Exercise and Breast Cancer Related Lymphedema – a Systematic Review Update. https://doi-org.nuigalway.idm.oclc.org/10.1080/09638288.2018.1514663 2019, 42, 26–35. [Google Scholar] [CrossRef]
- Saraswathi, V.; Latha, S.; Niraimathi, K.; Vidhubala, E. Managing Lymphedema, Increasing Range of Motion, and Quality of Life through Yoga Therapy among Breast Cancer Survivors: A Systematic Review. Int J Yoga 2021, 14, 3. [Google Scholar] [CrossRef]
- Wang, L.; Shi, Y.X.; Wang, T.T.; Chen, K.X.; Shang, S.M. Breast Cancer-Related Lymphoedema and Resistance Exercise: An Evidence-Based Review of Guidelines, Consensus Statements and Systematic Reviews. J Clin Nurs 2023, 32, 2208–2227. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the literature search and the process of selection.
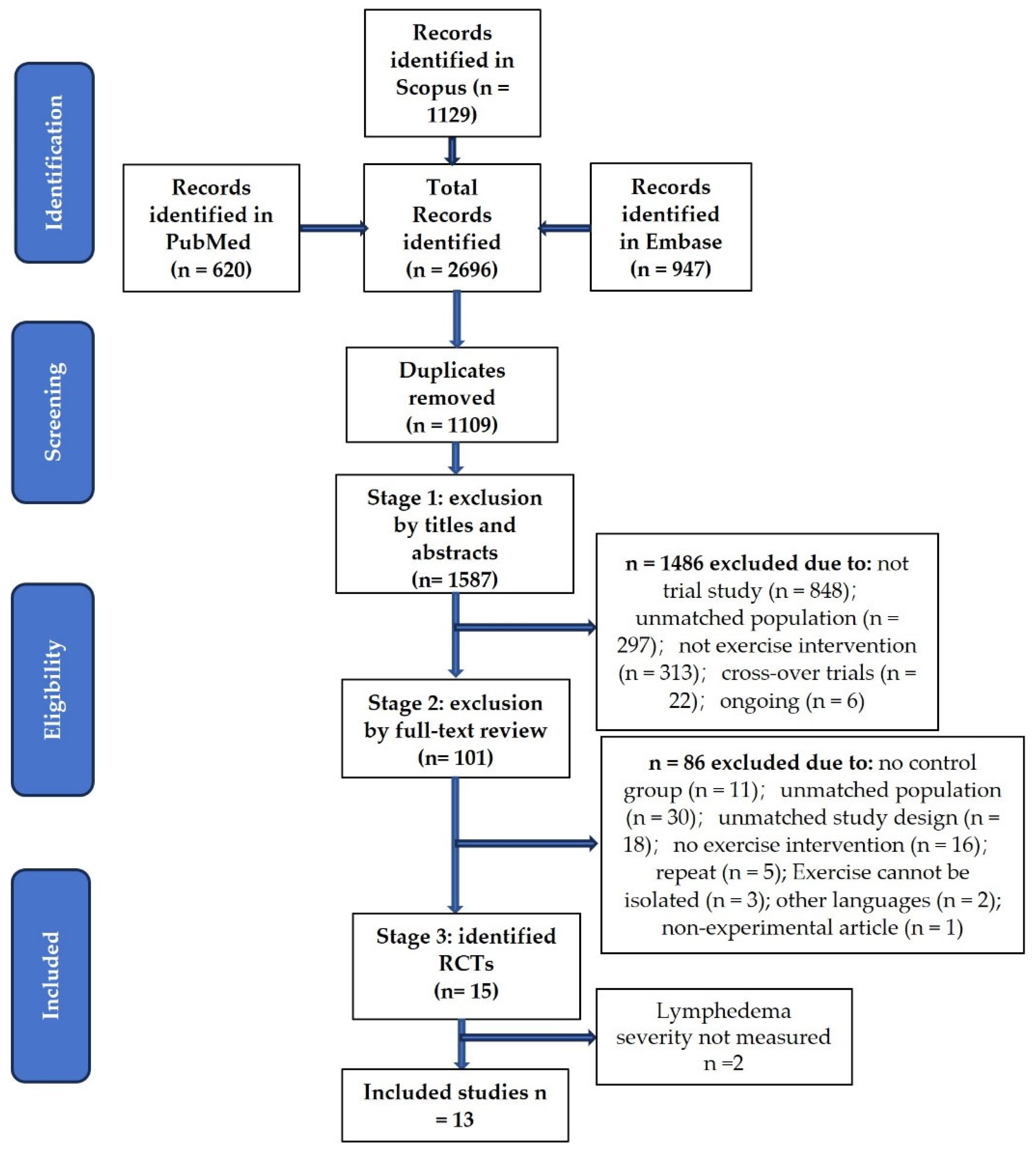
Figure 2.
Risk of bias analysis of the included studies.
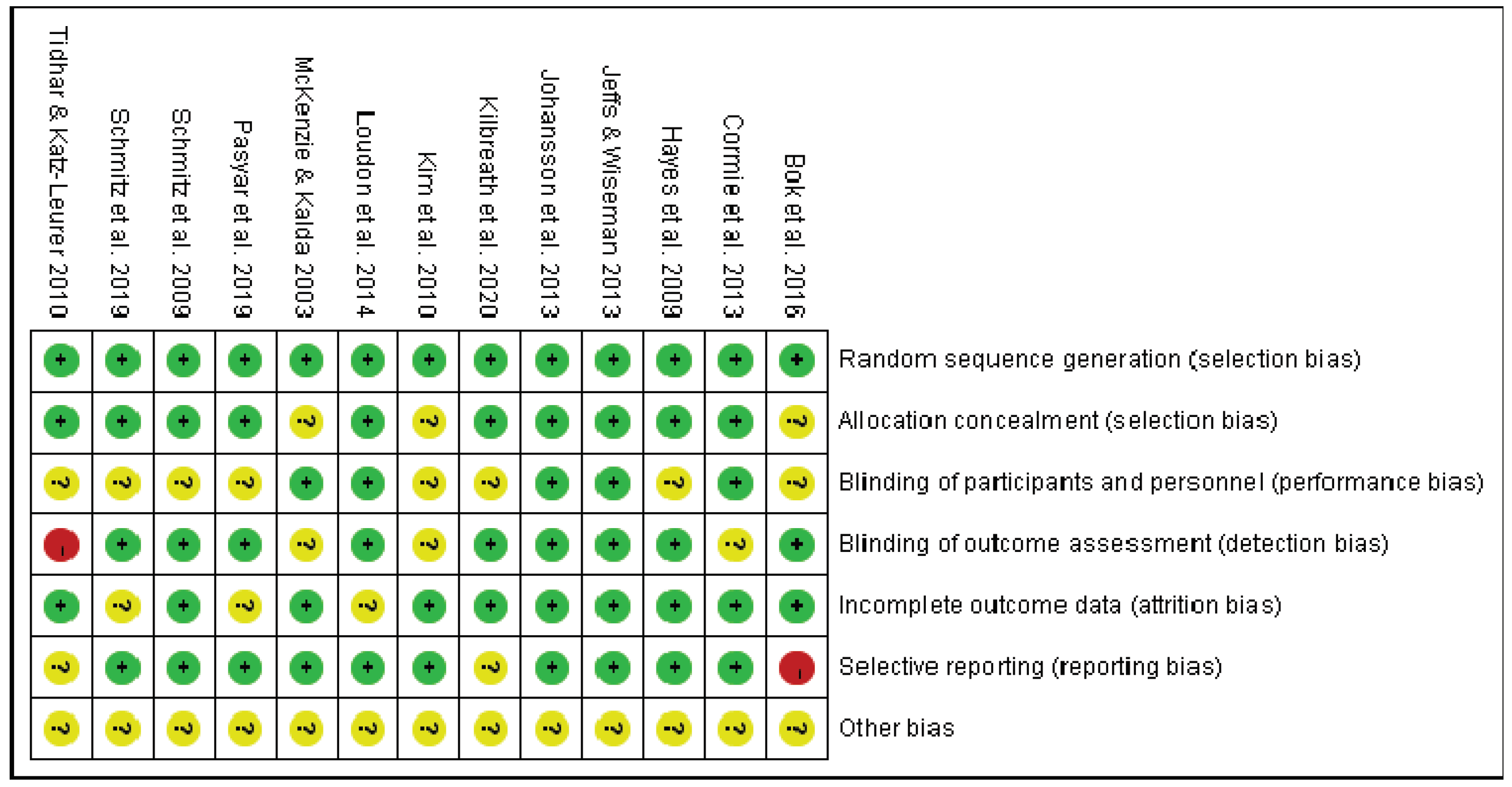

Table 1.
Participants’ characteristics, intervention details, and outcomes in the studies with Yoga.
Table 1.
Participants’ characteristics, intervention details, and outcomes in the studies with Yoga.
| Study | No.of Participants and Characteristics | Intervention Details (Frequency, Time, Duration, and Supervision) | Measure and Outcomes |
|---|---|---|---|
| Loudon et al. (2014) [24] | Twenty-eight women (age from 34 to 80) completed breast cancer treatment before ≥ 6 months, with stage one unilateral BCRL | 90-min teacher-led Yoga weekly, 45-min DVD-led Yoga daily for 8 weeks | No significant mean change in arm volume (assessed by a Jobst non-stretch tape), and extracellular fluid (measured by BIS) between the two groups were detected after 8 weeks. The mean arm volume reduced to 72.03 ± 80.77 from 101.45 ± 75.08 in the intervention group after 8 weeks. After another 4 weeks of follow-up, the mean arm volume in the intervention group was increased |
| Pasyar et al. (2019) [25] | Forty women (> 18 years old) with BCRL and an average age of 51.7 years old | Three sessions weekly (2 sessions under supervision and 1 session by using DVD at home) for 8 weeks | The mean upper extremity volume was not reduced in the intervention group after 8 weeks. No statistical difference in upper extremity volume was assessed by water displacement between the two groups. |
Table 2.
Participants’ characteristics, intervention details, and outcomes in the studies with resistance exercise.
Table 2.
Participants’ characteristics, intervention details, and outcomes in the studies with resistance exercise.
| Study | No. of Participants and Characteristics | Intervention Details (Frequency, Intensity, Time, Duration, and Supervision) | Measure and Outcomes |
|---|---|---|---|
| Schmitz et al. (2009) [26] | One hundred and forty-one patients (average age of 56 ± 9 in the study group and 58 ± 10 in the control group) with stable BCRL after unilateral non-metastatic breast cancer 1 to 15 years |
Frequency and duration: Twice weekly for 1 year Intensity, time, progression, and supervision: in the first 13 weeks, 90-minute professional-led sessions in the group, starting from little-to-no resistance and 1-3 new exercises were taught each session (of those weeks, in the first 5 weeks, increasing the number of sets from 2 to 3, after 2 sessions of 3 sets of 10 reps, the resistance were increased gradually), and then unsupervised exercise for the rest 39 weeks |
Limb swelling was measured by water displacement. The percentage of women who had a change in interlimb volume difference of 5% or more and the percentage of mean interlimb volume discrepancy between baseline and 12 months were not statistically different between the two groups. |
| Kim et al. (2010) [27] | Forty women (age from 27 to 76) with unilateral BCRL |
Frequency and duration: 5 days per week for 8 weeks Intensity, time, progression: 6 exercises (seated row, bench press, latissimus dorsi pull-down, 1-arm bent-over row, triceps extension, and biceps curl) with 0.5-kg dumbbells for 15 minutes; after the first 2 weeks, 1-kg dumbbells were used unless participants felt they were too heavy. Supervision: for the first 2 weeks |
The volume (measured circumference by tape) of the proximal arm statistically reduced within both groups after 8 weeks. The reduced volume of the proximal arm was significantly greater in the intervention group than in the control group. |
| Cormie et al. (2013) [30] | Sixty-two women (average age of 56.1±8.1 in the high-load group, 57.0±10.0 in the low-load group, and 58.6±6.7 in the control group) diagnosed with breast cancer at least 1 year before |
Frequency and duration: twice per week (in a group of 8-10 persons) for 12 weeks Intensity and supervision: fully supervised moderate to high-intensity exercise (low-load group: 55-65% of 1RM using 20-15 RM; high-load group 75-85% of 1RM using 10-6 RM) Time: 1-4 sets per exercise (chest press, seated row/lat pulldown, shoulder press/lateral raise, bicep curl, triceps extension, wrist curl, leg press/leg extension, squat/lunge) for a total of 60 minutes per session Progression: increased in 5–10 % increments if participants were able to perform more repetitions than the prescribed RM during a set without worsening arm symptoms. |
There was no mean change difference in the extent of swelling (measured by three methods: (1) BIS, (2) dual energy X-ray absorptiometry, and (3) arm circumference measurements) between groups either at the baseline or at 12 weeks. |
| Jeffs & Wiseman (2013) [28] | Twenty-three women (age from 51 to 73.5) with stable unilateral BCRL ≥ 3 months |
Frequency, time, and duration: 10-15 mins of breathing and gravity-resistive isotonic arm exercises daily for 26 weeks Supervision: no |
%ELV (calculated from limb volume measured by Perometer) decreased significantly in the intervention group but not in the control group, with no statistically significant difference between the two groups. |
| Bok et al. (2016) [29] | Thirty-two women (average age of 45.4 ± 8.8 in the PRE group and 53.3 ± 9.54 in the non-PRE group) with unilateral BCRL |
Frequency: Twice daily for 8 weeks Intensity and progression: 5 repetitions of 6 exercises (dumbbell fly, triceps extension, one-arm bent-over row, biceps curl, dumbbell side raise, and lifting the arms forward) with 0.5-kg dumbbells, adding 5 additional repetitions every week Supervision: no |
Both distal and proximal upper limb circumferences measured by tape reduced significantly in the intervention group after 8 weeks. |
Table 3.
Participants’ characteristics, intervention details, and outcomes in the studies with complex exercise.
Table 3.
Participants’ characteristics, intervention details, and outcomes in the studies with complex exercise.
| Study | No. of participants and characteristics | Intervention details (Frequency, Intensity, time, duration, and supervision) | Measure and outcomes |
|---|---|---|---|
| McKenzie & Kalda (2003) [34] | Fourteen women (an average age of 56.6 ± 9.0 years old) completed stage I or II breast cancer treatment for at least 6 months with unilateral lymphedema. |
Frequency and duration: 3 times per week for 8 weeks Intensity, time, progression, and supervision: Resistance exercise started from 2 sets of 10 repetitions of 6 exercises (seated row, bench press, latissimus dorsi pull down, one arm bent-over rowing, triceps extension, and bicep curl) with light weights; after the first week, it increased to 3 sets of 10 repetitions, and weights were gradually processed for each participant. The aerobic exercise started from 5-7 minutes of warm-up aerobic exercise; after 2 weeks, an arm cycle ergometer was used (under supervision), 5 bouts of 1-min cycling at a resistance of 8.3 W and then processed to 20 minutes of continuous cycling with a resistance of up to 25 W |
No statistical change in arm circumference and arm volume (calculated from arm circumference and measured by water displacement) in either group was observed. |
| Hayes et al. (2009) [31] | Thirty-two women (average age of 59 ± 7 in the intervention group and 60 ± 11 in the control group) with unilateral BCRL at least 6 months |
Frequency and supervision: 3 times (2 supervised) per week at week 1-4, 4 times (2 supervised) per week at week 5-8, and at least 4 times (1 supervised) per week at week 9-12 Intensity, time, and progression: Low-to-moderate-intensity (RPE 3-5) aerobic exercise only for 20-30 minutes in the first 2 weeks; Low-to-moderate-intensity (RPE 3-5) aerobic exercise and low-intensity (20 reps per exercise) resistance exercise for 20-30 minutes at week 3 and 4; moderate-intensity aerobic (RPE 4-6) and moderate-intensity (finally completed 15 reps per exercise) resistance exercises for 30-45 minutes at week 5-8;moderate-to-high-intensity (RPE 4-7) aerobic and moderate- to-high (finally completed 10 reps per exercise) resistance exercises for 45+ minutes at week 9-12 |
The changes in lymphedema status (measured by BIS and Perometry) were not statistically different between the two groups. No significant change within the groups was observed. |
| Schmitz et al. (2019) [32] | One hundred and seventy-seven (the number in the control and exercise groups) women (body mass index of 25 to 50) diagnosed with BCRL and completed treatment for at least 6 months, not engaging in resistance training or 3 or more weekly aerobic sessions in the past 1 year, no current weight management surgery or medication taken, no weight loss greater than 4.5 kg in the past 3 months |
Frequency and duration: Twice weekly for 52 weeks Intensity, time, and progression: Two sets of 10 repetitions of 9 resistance exercises with 0.45 to 9.45 kg dumbbells and one 90-minute weekly class in the first 6 weeks; from week 7, it increased to 3 sets per session with increased weights by 0.45 to 0.9 kg every two weeks with an upper limit of 9.45 kg and monthly classes provided; aerobic exercise started from 90 minutes per week, gradually increased walking time to 180 minutes per week |
There was no significant difference between the two groups in the percentage of interlimb volume differences (measured by Perometry) either at the baseline or after 12 months |
| Kilbreath et al. (2020) [33] | Eighty-nine women (≥ 18 years old, average age of 59.5±8.0 in the control group and 53.7±10.4 in the exercise group) with BCRL at least 3 months |
Frequency and duration: Three sessions per week for 12 weeks Intensity and time: One-hour exercise session consisted of 10-min warm-up, 30-min resistance exercise, and 20-min aerobic exercise. Resistance exercise: 10–12 repetitions moderate-intensity (5-7 on the OMNI-RES) for weeks 1-6 and high-intensity resistance exercise (7-9 on the OMNI-RES) for weeks 7–12. Aerobic exercise: 60%-85% of HRR, perceived exertion of 11-17. Progression: For resistance exercise, the intensity was increased if the weight could be lifted more than 12 times, but if participants could not lift the new weight, the number of repetitions was increased from 12 to 14 and then increased weight. For aerobic exercise, new types of exercise (stationary bike, treadmill, rower, etc.) were added every 4 weeks. |
The change in BIS ratio was significant for breasts but not significant for arms and legs between the two group |
Note: RPE=Rate of perceived exertion.
Table 4.
Participants’ characteristics, intervention details, and outcomes in the studies with water-based exercise.
Table 4.
Participants’ characteristics, intervention details, and outcomes in the studies with water-based exercise.
| Study | No. of Participants and Characteristics | Intervention Details (Frequency, Intensity, Time, Duration, and Supervision) | Measure and Outcomes |
|---|---|---|---|
| Johansson et al. (2013) [37] | Twenty-nine women (age 56-74 years old) with unilateral BCRL for at least 6 months but without active treatment for the last 3 months |
Frequency, duration, supervision: three 30-minute sessions per week for 8 weeks, supervision only for the first session Intensity: moderate intensity (11-13 RPE on the Borg scale) |
No change in lymphedema status (measured by Perometry and BIS) was identified. |
| Tidhar & Katz-Leurer (2010) [36] | Forty-eight women with (average age of 56.2 ±10.7 years old in the study group and 56.5±8.8 years old in the control group) unilateral BCRL and completed intensive CDT for the last 2 weeks |
Frequency, intensity, time, and duration: one 45-minute session of gentle exercises (in a group setting) for 12 weeks Supervision: no |
No long-term effect of water-based exercise on limb volume (assessed by water displacement) was observed although it reduced limb volume immediately after sessions. |
Note: RPE=Rate of perceived exertion.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



