
Submitted:
20 March 2024
Posted:
21 March 2024
You are already at the latest version
Abstract
Pathological cleavage of collagen type II (Col2) and generation of Col2 neoepitopes can be good molecular markers of progression of osteoarthritis (OA). One of such potential biomarkers is collagen type II neoepitope C2C. The aim of this study was to correlate the degree of articular cartilage damage in OA patients with C2C expression in histological samples of tissues removed during total knee replacement. Cartilage samples were obtained from 27 patients aged from 55 to 66. In each patient medial and lateral tibia plateau samples were analyzed according to the OARSI histopathology grading system. C2C expression was evaluated on histological slides by semi-quantitative analysis using ImageJ Fiji software. Spearman´s rank correlation analysis showed significant positive correlation (rho=0.289, P=0.0356) between the histological grade of tissue damage and the percentage of C2C staining. In addition, highly significant positive correlation (rho=0.388, P=0.0041) was found between osteoarthritis score (combining the histological grade of damage with the OA macroscopic stage) and the percentage of C2C staining in the samples. The C2C expression was found in all the regions of the articular cartilage (i.e. the superficial zone, mid zone, deep zone and tidemark area and the zone of calcified cartilage). Our study suggests that local expression of C2C correlates with the cartilage damage in the knee affected by OA. This further assures that C2C can be a perspective marker for evaluation of pathological processes in OA course and OA clinical trials.
Keywords:
osteoarthritis
; collagen neoepitope C2C
; cartilage
; immunohistochemistry
1. Introduction
Osteoarthritis (OA) is the most prevalent form of arthritis, resulting in joint pain and disability. This disease is related to the ageing population and obesity and predominantly affects weight-bearing joints. OA mainly affects hips, knees and spine but also hands. The main symptoms of OA are pain, stiffness and dysfunction of joints, which worsen the overall quality of life [1]. Although cartilage loss is the main pathological feature of OA, the whole joint, including subchondral bone, synovium, menisci and ligaments, is affected [2]. It is suggested that factors contributing to the development of OA include advanced age, being overweight or obese, history of injury or surgery to a joint, overuse from repetitive movements of the joint, misalignment of joints and family history (genetics) of OA [3]. As the molecular mechanisms leading to the development of OA are largely unknown, it is complicated to identify therapeutic targets that effectively prevent and treat OA [4]. In recent years, attention has begun to be paid to OA associated molecular biomarkers from biofluids to identify early pathological molecular shifts which are not detected with traditional imaging methodology [5]. Such shifts may be indicative of the deterioration of joint health before any other signs, such as pain or evidence from imaging studies, appear. If proven to be sensitive enough, biomarkers may help to describe the course of the disease and provide evidence if the treatment modalities, such as physiotherapy, are working.
The articular cartilage consists of chondrocytes and the extracellular matrix (ECM). The ECM is composed of two main components: type II collagen (Col2) and aggrecan, the sulfated proteoglycan [6]. Col2 molecule is the fundamental structural component of articular cartilage. It is composed of three identical α polypeptide chains of 1060 amino acid residues, arranged in a large triple helix and comparatively brief nonhelical telopeptides consisting of 19 amino acid residues in N-telopeptide and 27 amino acid residues in C-telopeptide [7,8]. To maintain a healthy cartilage, there is a delicate equilibrium of extracellular matrix remolding: a balance between matrix synthesis and matrix degradation [9]. As previously mentioned, cartilage breakdown is a key feature of OA pathogenesis. Therefore, the focus should be on cartilage ECM associated molecules, in particular Col2 degradation molecules. Many biochemical markers associated with Col2 that reflect a cartilage turnover have been proposed as candidate prognostic markers of rapid progression of OA [10,11,12].
In the early stages of OA, the molecular composition and organization of the extracellular matrix is altered, but the surface of the cartilage remains intact [13]. Col2 undergoes degradation facilitated by proteolytic enzymes, including matrix metalloproteinases (MMPs), cysteine proteases, and collagenase [14]. MMPs, such as MMP-9 and MMP-13, along with collagenases, exhibit the capability to cleave the native triple helix structure of collagen. As a result of the cleaving, two new peptides, threequarter-length and one-quarter-length of mature Col2 are formed with specific neoepitopes at cleavage sites [15,16]. Such neoepitopes are, for example, C-telopeptide of type II collagen (CTX-II), COL2-3/4C Short (C1,2C), C2M and collagen type-II C-terminal cleavage neoepitope (C2C). In addition, ECM degradation products, such as cartilage oligomeric matrix protein (COMP), hyaluronic acid (HA) and proteoglycans (PGs) are the cartilage-derived biomarkers which have been applied to assess disease severity [17]. Biomarkers CTX-II, COMP, C1,2C, PGs, C2M and C2C result from the degradation of articular cartilage, primarily derived from the breakdown of Col2 catalyzed mainly by matrix metalloproteinases MMP-1, MMP-8, and MMP-13 [18]. HA is mainly degraded by hyaluronidases and fragments of it can be released into the serum [19]. CTX-II presence has been identified in serum and urine where it is referred to as sCTX-II and uCTX-II respectively [17,20]. COMP has been detected in the serum of patients with OA, rheumatoid arthritis and articular trauma and referred to as sCOMP. However, besides cartilage, COMP is found in other load-resisting soft tissues like tendon, ligament and meniscus [21]. Therefore, it cannot be considered as a specific marker for cartilage only. Several of these biomarkers are versatile molecules with various functions and implications in different tissues and diseases. Therefore, variations in the correlation of these markers are dependent on differences in patients’ cohorts and the samples analyzed. Nevertheless, both uCTX-II and sCOMP have demonstrated association with OA progression [20]. PGs and HA have not exhibited consistent reliability as biomarkers for OA, as their serum levels have not exhibited robust correlations with the signs and symptoms of the disease [19]. C1,2C levels have demonstrated an association with OA, however, it has been observed that the accuracy of the C1,2C assay is compromised by its tendency to cross-react with type I collagen, primarily indicative of bone turnover [15].
It is important to highlight that there has been relatively little histopathological research specifically looking at neoepitopes in cartilage, like C2C. There are only a few studies that stand out in this area [7,22]. This illustrates that additional biomarkers in characterization of OA are still to be sought and, therefore, there is notable interest in the identification of C2C, which has been detected at elevated levels in OA cartilage and body fluids (serum, urine), presenting a potential laboratory metric for assessing cartilage breakdown [23,24].
Although recent studies have focused on C2C detection in urine by associating C2C and knee OA (kOA) radiographic features [25,26], our study is aimed at histological analysis of C2C in cartilage samples. Given the Human Protein Atlas's identification of Col2 in diverse tissues, including connective tissues, gastrointestinal tissues, endocrine tissues, and eyes, the concern persists that the source of excreted C2C may not exclusively be cartilage. Consequently, the prognostic significance of C2C in OA development remains uncertain. The aim of this study was to detect the local expression levels of C2C in the articular cartilage of kOA removed during total knee replacement (TKR) and to determine if the levels of C2C expression correlate with the cartilage histological damage and the score of OA for the affected knee.
2. Materials and Methods
2.1. Sampling
Cartilage tissue was obtained from 27 patients undergoing primary unilateral TKR due to end-stage kOA at the Traumatology and Orthopedics Clinic of the University of Tartu (Estonia) in 2017–2018. Seventeen women and ten men aged from 55 to 66 years were enrolled in the study. Written informed consent was received from all the patients before participation. The research project was approved by the Ethics Review Committee on Human Research of the University of Tartu (Protocol no. 265T-22, 19.12.2016), and it is in accordance with the Declaration of Helsinki (1975). Tissue punches included cartilage layers and the subchondral bone. In each subject, cylindrical osteochondral explants of 7 mm diameter were drilled perpendicular to the articular surface immediately after TKR from two load-bearing sites of the tibial plateau – one designated as meniscus-covered medial (MTM) and the other as meniscus-covered lateral (LTM) tibial plateau. In one case (patient 6), the sample from the meniscus-covered medial tibial plateau (MTM) was lost due to technical problems (see Table 1).
2.2. Histological Analysis
For histopathological assessment, MTM and LTM samples were fixed in 10% buffered formalin solution. Decalcification was performed using Sakura TDETM 30 Decalcifier System with Decalcifier Solution (Sakura, the Netherlands) during 24 h and embedded in paraffin with a vacuum infiltration processor (Tissue-Tek® VIP 5 Jr, Sakura, USA). 7 µm thick sections were cut with the microtome (HM200, Microm, Germany), mounted on AutoFrost® Microscope Slides (Cancer Diagnostics, Inc, Durham, USA), dried overnight on a slide dryer heating plate at the temperature of 37 °C, deparaffinized with xylene and rehydrated in a series of graded ethanol solutions. Then, the sections were stained using the Safranin O (Sigma-Aldrich Chemie GmbH, Germany) staining method and finally, the sections were dehydrated in graded ethanol solutions, in xylene, and mounted with Eukitt® medium (Sigma-Aldrich) before applying the coverslips. We used the OARSI OA Cartilage Histopathology Assessment System for evaluation of the level of local cartilage pathology ranging from grade 0 (normal cartilage architecture) to grade 6 (severe damage) [27]. Grade 0 is characterized by a normal matrix architecture and smooth surface, cells are intact and in appropriate orientation. For grade 1, only the superficial zone is affected. The surface of the cartilage is generally intact but may show superficial fibrillation. The middle and deep zones are not affected. Grade 2 is characterized by discontinuity of the cartilage superficial zone by focal fibrillation. Small portions of cartilage from the superficial zone are detached due to abrasion from shear forces. Grade 3 is characterized by vertical fissures extending from the superficial zone into the middle zone or even into the deep zone. Grade 4 key feature is erosion. If in the earliest stage, cartilage matrix loss leads to delamination of the superficial zone, then more extensive erosion causes excavation and loss of matrix in fissured domains. Grade 5 key feature is denudation. Unmineralized cartilage is completely eroded to the level of mineralized cartilage or bone. Grade 6 is recognized by deformation. The contour of the articular cartilage is changed by processes of microfracture, repair and bone remodeling. Macroscopic stage of OA was assessed by visually evaluating the tibial plateau removed during the operation. To evaluate the extent of articular surface involved with OA, the staging method ranging from stage 1 (< 10% of involvement of the articular cartilage area) to stage 4 (> 50% of involvement) was used. For OA scoring, a simple formula was used: OA score = OA grade × OA stage [27]. Two independent assessors performed the evaluation of the articular cartilage damage. In the case of the few evaluation disagreements, the specimens were revised to formulate the final assessment.
2.3. Immunohistochemistry (IHC)
For immunohistochemical analysis, 4 µm thick paraffin-embedded sections were cut using the microtome Ergostar (HM200, Microm, Germany), mounted on AutoFrost® Microscope Slides (Cancer Diagnostics, Inc, Durham, USA) and dried overnight on a slide dryer heating plate at the temperature of 37 °C. The sections were deparaffinized in xylene and rehydrated in a series of graded ethanol solutions. To inactivate endogenous peroxidase activity, the sections were treated 10 minutes with freshly prepared 0.6% H2O2 (Fluka, France) dissolved in distilled water. Then, the sections were washed for 3 ×5 minutes in 1X GibcoTM Phospate Buffered Saline (PBS, pH 7.4) solution (Thermo Fischer Scientific, the Netherlands). After washing, the sections were incubated with 100 µl Dako Antibody Diluent (cat no S2022) (Dako Denmark A/S, Denmark) to block nonspecific antibody binding. After blocking, the sections were incubated with 100 µl mouse-α-C2C monoclonal antibody (Ab 5109; produced by IBEX Pharmaceutical Inc, Canada) in dilution 1 : 10000 for one hour at room temperature. The antibody was diluted in Dako Antibody Diluent (cat no S2022) (Dako Denmark A/S, Denmark). Thereafter, to visualize the primary antibody, the commercial kit Dako RealTM EnvisionTM Detection System, Peroxidase/DAB+, Rabbit/Mouse (cat no K5007) (Dako, Glostrup, Denmark) was used. Washing 3 × 5 minutes between each step after incubation with the primary antibody was performed in 1X GibcoTM Phospate Buffered Saline (PBS, pH 7.4) solution (Thermo Fischer Scientific, the Netherlands) containing 0.07% Tween 20 detergent (BioTop, Naxo, Estonia). All incubations were performed at room temperature in a humidified chamber. No positive IHC-staining was noted in negative control slides where the primary antibody was omitted. The sections were stained for 1 minute with Toluidine blue to counterstain the cartilage proteoglycans. Finally, the sections were dehydrated in a series of graded ethanol solutions, in xylene, and mounted with Eukitt® medium (Sigma-Aldrich) before applying the coverslips.
The tissue slides were fully scanned using Leica SCN400 (Leica Microsystems, Wetzlar, Germany) with magnification 20 ×. The proportion of the stained tissue sample was assessed on the scanned images in a semi-quantitative manner with ImageJ software and color threshold function as described by Crove and Yue [28]. In brief, a scanned IHC image was opened with Aperio Image Scope program. The tissue section was selected using the Zoom navigation tool and the selected area was snapshot and saved as a TIFF file. Consequently, the TIFF file was opened in the ImageJ (Fiji) program and the “Color threshold” tool was applied to select the whole stained tissue section area. The selected area was analyzed by using the “Measure” tool. The color threshold was adjusted to the maximum to remove the background signal, without removing the DAB signal area. The results of the DAB signal area in the form of pixels were entered into an MS Excel table and eventually the percentage of DAB staining area was calculated. In essence, the ImageJ software facilitated the assessment of pixel numbers within the tissue section, and the color threshold function enabled the selection and enumeration of pixels corresponding to positively stained regions with the C2C antibody, resulting in the percentage of the positively stained tissue section area for each sample (see Table 1).
2.4. Statistical Analysis
Correlations between the extent of expression of Col2-C2C and the degree of cartilage damage were analyzed using Spearman´s rank correlation. Statistical analysis was performed applying the GraphPad InStat software (GraphPad Software, San Diego, USA). The level of significance was set at P < 0.05.
3. Results
Our results showed the positive immunohistochemical staining for C2C in all samples obtained during TKR. The C2C expression was detected in all the regions of articular cartilage (i.e. the superficial zone, the mid zone, the deep zone, the tidemark area and the zone of calcified cartilage), but the subchondral bone was generally not stained.
The main findings of the study, such as the histopathology grade of the tissue damage, the stage of macroscopic damage of the tibial plateau, the kOA score and the proportion of the tissue sample stained positively for C2C are summarized in Table 1.
In each patient, two tissue samples were analyzed, which were obtained from different load-bearing sites of the knee joint, one from the meniscus-covered medial tibial plateau (MTM) and the other from the meniscus-covered lateral tibial plateau (LTM). As seen in Table 1, kOA histopathology grades (according to OARSI indicators referred to in the methodology section) vary from 0 (patient 20, LTM) to 6.5 (patient 26, MTM). Comparing the same patient’s LTM and MTM samples, the histopathology grades differed in most cases; equal grades were recorded in three patients only (3, 15 and 19). Higher histopathology grades were mostly recorded for the medial side of the joint – in 17 cases MTM samples had higher grades, while only in 6 cases LTM samples had higher grades as compared to the counter side (Table 1).
In Figure 1, representative micrographs are presented to depict histopathology grades 0, 1.5, 3.5 and 6. Moreover, we found that the percentage of C2C immunohistochemical expression correlated significantly with the OARSI histopathology grade (Spearman rho = 0.289 (corrected for ties); 95%CI: 0.0124 to 0.525; P = 0.0356; Figure 1, Table 1). However, this correlation did not remain significant when calculated only for females (Spearman rho = 0.189 (corrected for ties); 95%CI: -0.170 to 0.503; P = 0.285) or for males (Spearman rho = 0.369 (corrected for ties); 95%CI: -0.117 to 0.712; P = 0.121).
Furthermore, significant positive correlation was found between the OA score (combining the histological grade of damage with the OA macroscopic stage) and the percentage of C2C staining in the samples (Spearman rho = 0.388 (corrected for ties); 95%CI: 0.123 to 0.601; P = 0.0041). This correlation remained positive among the female participants (Spearman rho = 0.349 (corrected for ties); 95%CI: 0.002 to 0.621; P = 0.043), but not in the male subgroup (Spearman rho = 0.382 (corrected for ties); 95%CI: -0.102 to 0.720; P = 0.107). The macroscopic stage of OA was visually assessed on the tibial plateau removed during surgery (see Materials and Methods). Our findings suggest indeed that the proportion of tissue stained for C2C may be related to the cartilage damage (see Figure 1).
Additionally, it may be pointed out that OARSI histopathology grade and OA score were significantly correlated with patients’ age (Spearman rho = 0.293 (corrected for ties); 95%CI: 0.016 to 0.528; P = 0.033 and Spearman rho = 0.358 (corrected for ties); 95%CI: 0.089 to 0.578; P = 0.0085 respectively), but the percentage of C2C staining in the samples was not (Spearman rho = 0.169 (corrected for ties); 95%CI: -0.115 to 0.427; P = 0.227).
4. Discussion
While the evaluation of OA traditionally relies on clinical manifestations, including pain, joint mobility loss, and functional impairment, and specific radiographic parameters, there exists a need for a sensitive and early molecular marker that delineates the progression of the disease. A preferable biomarker would ideally be detectable from a readily accessible biological sample, such as urine or blood serum. Such a marker would facilitate a more intricate monitoring of patients, particularly those belonging to high-risk categories, such as individuals exhibiting poor responses to conservative or surgical interventions, those manifesting OA at a relatively young age (below 70) [29] or participants in clinical trials assessing OA treatments.
In the selection of a good disease marker, the objective is to prioritize stability and reliability. When evaluating C2C as a potential marker, it is essential to demonstrate the pathological alterations of the protein in histological samples. This approach provides the strongest evidence for establishing a correlation between the actual tissue damage and the levels of the biomarker in easily accessible samples such as blood or urine. One antibody specific to C2C is used in Collagen Type II Cleavage Sandwich Assay developed by IBEX Pharmaceuticals Inc. Through collaboration with IBEX, we procured the antibody employed in the sandwich assay for our immunohistochemical experiments. Notably, this antibody is not known to have been used in immunohistochemical analyses elsewhere.
Considering that other tissues in the body could contribute to the content of excreted C2C, it is important to investigate the expression and localization of this neoepitope directly in the damaged cartilage. This type of investigation is of significance not only for C2C but also for other biomarkers to prove their pathogenic significance in the context of the disease [30,31].
It is worth emphasizing that, even though detected and measured in body fluids, the investigation and quantification of neoepitopes in articular cartilage have been the subject of limited attention within existing literature, resulting in a restricted pool of studies available for consideration.
Correlation between CTX-II staining and tissue damage have been described in patients with femoral head necrosis [32]. COMP content in tissue has been related to OA progression and also limb development [33]. COL2-3/4C Short (C1,2C) has been detected in the articular cartilage of mice, while C2M has been identified in the articular cartilage of humans. However, there is limited evidence regarding alterations in their expression and their relationship to tissue damage [34,35].
Poole et al introduced an antibody designed to target C2C, but their study did not undertake an exploration of potential immunohistochemical applications, but instead focused on the quantification of the C2C in patients´ serum and urine samples using ELISA test [36]. In a paper by Dejica et al., C2C and C1,2C were detected and described in articular cartilage, but the results of immunohistochemistry were not quantified [7]. An additional neoepitope of the C-terminus of the type-II collagen TC fragment was assessed in equine articular cartilage, but the staining patterns were characterized solely by their intensity, lacking direct quantification [22]. Thus, there has been limited investigation into quantifying the neoepitopes at the tissue structural level and, therefore, it would be of great interest to describe the local immunohistochemical expression pattern of C2C in articular cartilage.
We successfully demonstrated a correlation between C2C expression and both the grade of cartilage damage and the overall knee joint damage score as evaluated by OARSI indicators. This implies that C2C may possess indicative properties for the development of kOA. It is important to note that an ideal biomarker should demonstrate a strong correlation with the advancement of tissue damage, both at the tissue level and in more readily accessible biomaterials like plasma or urine. Subsequent investigations should ascertain whether local tissue alterations of C2C content are reflected in the C2C levels found in urine samples – an aspect explored by other researchers [37]. The identification of a reliable and readily assessable biomarker would not only facilitate more detailed patient monitoring but also serve as a surrogate marker in the context of clinical trials.
Author Contributions
Conceptualization, S.S., K.K., M.A. and A.A.; methodology, T.T., S.S., K.K. and A.A.; software, S.S.; validation, S.S., K.K. and A.A.; formal analysis, S.S., K.K., and A.A.; investigation, T.T.; resources, A.A.; data curation, S.S., K.K. and A.A.; writing—original draft preparation, T.T.; writing—review and editing, S.S., K.K., M.A. and A.A.; visualization, T.T., S.S., K.K., M.A. and A.A.; supervision, S.S., K.K., M.A. and A.A.; project administration, S.S., K.K., M.A. and A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee on Human Research of the University of Tartu (Protocol no. 265T-22, 19.12.2016).
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study to publish this paper.
Data Availability Statement
Data are unavailable due to privacy restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Martel-Pelletier, J.; Barr, A.J.; Cicuttini, F.M.; Conaghan, P.G.; Cooper, C.; Goldring, M.B.; Goldring, S.R.; Jones, G.; Teichtahl, A.J.; Pelletier, J.P. Osteoarthritis. Nat. Rev. Dis. Primers 2016, 2(1). [Google Scholar] [CrossRef]
- O'Neill, T.W.; McCabe, P.S.; McBeth, J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract Res Clin Rheumatol 2018, 32(2), 312–326. [Google Scholar] [CrossRef] [PubMed]
- Yunus, M.H.M.; Nordin, A.; Kamal, H. Pathophysiological Perspective of Osteoarthritis. Medicina (Kaunas) 2020, 56(11), 614. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.R.; Yoo, J.J.; Kim, H.A. Therapeutics in Osteoarthritis Based on an Understanding of Its Molecular Pathogenesis. Int. J. Mol. Sci. 2018, 19(3), 674. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, A.; Rockel, J.S.; Lively, S.; Kapoor, M. Emerging molecular biomarkers in osteoarthritis pathology. Ther Adv Musculoskelet Dis 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Vincent, T.L.; McClurg, O.; Troeberg, L. The Extracellular Matrix of Articular Cartilage Controls the Bioavailability of Pericellular Matrix-Bound Growth Factors to Drive Tissue Homeostasis and Repair. Int J Mol Sci 2022, 23(11), 6003. [Google Scholar] [CrossRef] [PubMed]
- Dejica, V.M.; Mort, J.S.; Laverty, S.; Antoniou, J.; Zukor, D.J.; Tanzer, M.; Poole, A.R. Increased type II collagen cleavage by cathepsin K and collagenase activities with aging and osteoarthritis in human articular cartilage. Arthritis Res Ther. 2012, 14(3), R113. [Google Scholar] [CrossRef] [PubMed]
- Antipova, O.; Orgel, J.P. In situ D-periodic molecular structure of type II collagen. J Biol Chem. 2010, 285(10), 7087–7096. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Sinkeviciute, D.; He, Y.; Karsdal, M.; Henrotin, Y.; Mobasheri, A.; Önnerfjord, P.; Bay-Jensen, A. The minor collagens in articular cartilage. Protein Cell. 2017, 8(8), 560–572. [Google Scholar] [CrossRef] [PubMed]
- Dam, E.B.; Loog, M.; Christiansen, C.; Byrjalsen, I.; Folkesson, J.; Nielsen, M.; Qazi, A.A.; Pettersen, P.C.; Garnero, P.; Karsdal, M.A. Identification of Progressors in Osteoarthritis by Combining Biochemical and MRI-Based Markers. Arthritis Res. Ther. 2009, 11(4), R115. [Google Scholar] [CrossRef]
- van Spil, W.E.; Drossaers-Bakker, K.W.; Lafeber, F.P. Associations of ctx-ii with biochemical markers of bone turnover raise questions on its tissue origin: Data from check, a cohort study of early osteoarthritis. Ann. Rheum. Dis. 2013, 72(1), 29–36. [Google Scholar] [CrossRef]
- Arends, R.H.G.P.; Karsdal, M.A.; Verburg, K.M.; West, C.R.; Bay-Jensen, A.C.; Keller, D.S. Identification of serological biomarker profiles associated with total joint replacement in osteoarthritis patients. Osteoarthr. Cartil. 2017, 25(6), 866–877. [Google Scholar] [CrossRef]
- Goldring, M.B.; Goldring, S.R. Articular cartilage and subchondral bone in the pathogenesis of osteoarthritis. Ann. N. Y. Acad. Sci. 2010, 1192(1), 230–237. [Google Scholar] [CrossRef] [PubMed]
- Burrage, P.S.; Mix, K.S.; Brinckerhoff, C.E. Matrix Metalloproteinases: Role in Arthritis. Front. Biosci. 2006, 11(1), 529–543. [Google Scholar] [CrossRef]
- Bay-Jensen, A.C.; Mobasheri, A.; Thudium, C.S.; Kraus, V.B.; Karsdal, M.A. Blood and urine biomarkers in osteoarthritis - an update on cartilage associated type II collagen and aggrecan markers. Curr Opin Rheumatol. 2022, 34(1), 54–60. [Google Scholar] [CrossRef]
- Bay-Jensen, A.C.; Andersen, T.L.; Charni-Ben Tabassi, N.; Kristensen, P.W.; Kjærsgaard-Andersen, P.; Sandell, L.; Garnero, P.; Delaissé, J.M. Biochemical Markers of Type II Collagen Breakdown and Synthesis Are Positioned at Specific Sites in Human Osteoarthritic Knee Cartilage. Osteoarthr. Cartil. 2008, 16(5), 615–623. [Google Scholar] [CrossRef] [PubMed]
- Oliviero, F.; Ramonda, R. Cartilage-derived biomarkers in osteoarthritis. Indian J Med Res. 2021, 2021153(4), 413–415. [Google Scholar] [CrossRef]
- Charni-Ben Tabassi, N.; Desmarais, S.; Bay-Jensen, A.C.; Delaissé, J.M.; Percival, M.D.; Garnero, P. The type II collagen fragments Helix-II and CTX-II reveal different enzymatic pathways of human cartilage collagen degradation. Osteoarthr. Cartil. 2008, 16(10), 1183–1191. [Google Scholar] [CrossRef]
- Papaneophytou, C.; Alabajos-Cea, A.; Viosca-Herrero, E.; Calvis, C.; Costa, M.; Christodoulides, A.E.; Kroushovski, A.; Lapithis, A.; Lapithi, V.M.; Papayiannis, I.; Christou, A.; Messeguer, R.; Giannaki, C.; Felekkis, K. Associations between serum biomarkers of cartilage metabolism and serum hyaluronic acid, with risk factors, pain categories, and disease severity in knee osteoarthritis: a pilot study. BMC Musculoskelet Disord. 2022, 23(1), 195. [Google Scholar] [CrossRef] [PubMed]
- van Spil, W.E.; DeGroot, J.; Lems, W.F.; Oostveen, J.C.; Lafeber, F.P. Serum and urinary biochemical markers for knee and hip-osteoarthritis: a systematic review applying the consensus BIPED criteria. Osteoarthr. Cartil. 2010, 18(5), 605–612. [Google Scholar] [CrossRef]
- Smith, R.; Önnerfjord, P.; Holmgren, K.; di Grado, S.; Dudhia, J. Development of a Cartilage Oligomeric Matrix Protein Neo-Epitope Assay for the Detection of Intra-Thecal Tendon Disease. Int J Mol Sci. 2020, 21(6), 2155. [Google Scholar] [CrossRef]
- Billinghurst, R.C.; Buxton, E.M.; Edwards, M.G.; McGraw, M.S.; McIlwraith, C.W. Use of an antineoepitope antibody for identification of type-II collagen degradation in equine articular cartilage. Am. J. Vet. Res. 2001, 62(7), 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, L.; Billinghurst, R.C.; Manner, P.; Nelson, F.; Webb, G.; Ionescu, M.; Reiner, A.; Tanzer, M.; Zukor, D.; Chen, J.; et al. Selective Enhancement of Collagenase-Mediated Cleavage of Resident Type II Collagen in Cultured Osteoarthritic Cartilage and Arrest with a Synthetic Inhibitor That Spares Collagenase 1 (Matrix Metalloproteinase 1). Arthritis Rheumat. 2000, 43(3), 673–682. [Google Scholar] [CrossRef] [PubMed]
- Chu, Q.; Lopez, M.; Hayashi, K.; Ionescu, M.; Billinghurst, R.C.; Johnson, K.A.; Poole, A.R.; Markel, M.D. Elevation of a Collagenase Generated Type II Collagen Neoepitope and Proteoglycan Epitopes in Synovial Fluid Following Induction of Joint Instability in the Dog. Osteoarthr. Cartil. 2002, 10(8), 662–669. [Google Scholar] [CrossRef] [PubMed]
- Kuhi, L.; Tamm, A.E.; Kumm, J.; Järv, K.; Märtson, A.; Tamm, A.O.; Kisand, K. Associations of Urinary Collagen II Neoepitope C2C with Total Knee Replacement Outcomes: Is OA a Systemic Disease in Rapidly Progressive Cases? Appl. Sci. 2022, 12(1), 164. [Google Scholar] [CrossRef]
- Kuhi, L.; Tamm, A.E.; Tamm, A.O.; Kisand, K. Cartilage Collagen Neoepitope C2C in Urine as an Integrative Diagnostic Marker for Early Knee Osteoarthritis. Osteoarthr. Cartil. Open 2020, 2(4), 100096. [Google Scholar] [CrossRef] [PubMed]
- Pritzker, K.P.; Gay, S.; Jimenez, S.A.; Østergaard, K.; Pelletier, J.P.; Revell, P.A.; Salter, D.; Van Den Berg, W.B. Osteoarthritis Cartilage Histopathology: Grading and Staging. Osteoarth. Cartil. 2006, 14(1), 13–29. [Google Scholar] [CrossRef] [PubMed]
- Crowe, A.R.; Yue, W. Semi-Quantitative Determination of Protein Expression Using Immunohistochemistry Staining and Analysis: An Integrated Protocol. Bio Protoc 2019, 9(24). [Google Scholar] [CrossRef]
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin Geriatr Med 2010, 26(3), 355–369. [Google Scholar] [CrossRef] [PubMed]
- Bay-Jensen, A.; Reker, D.; Kjelgaard-Petersen, C.F.; Mobasheri, A.; Karsdal, M.A.; Ladel, C.; Henrotin, Y.; Thudium, C.S. Osteoarthritis Year in Review 2015: Soluble Biomarkers and the BIPED Criteria. Osteoarthr. Cartil. 2016, 24(1), 9–20. [Google Scholar] [CrossRef] [PubMed]
- Torga, T.; Suutre, S.; Kisand, K.; Aunapuu, M.; Arend, A. Expression of CILP-2 and DDR2 and Ultrastructural Changes in the Articular Cartilage of Patients with Knee Osteoarthritis Undergoing Total Knee Arthroplasty: A Pilot Morphological Study. Med Mol Morphol 2022, 56(1), 46–57. [Google Scholar] [CrossRef]
- He, M.; Gong, S.D.; Chen, X.J.; Yang, F.; Pang, F.X.; Chen, Z.Q.; Huang, J.Y.; Zhou, Y.C.; Qin, Y.X.; He, W.; Wei, Q.S. Plasma C-terminal cross-linking telopeptide of type II collagen as a biomarker in advanced stages of femoral head osteonecrosis. Biomed Pharmacother. 2019, 111, 1213–1220. [Google Scholar] [CrossRef]
- Koelling, S.; Clauditz, T.S.; Kaste, M.; Miosge, N. Cartilage oligomeric matrix protein is involved in human limb development and in the pathogenesis of osteoarthritis. Arthritis Res Ther. 2006, 8(3), R56. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.P.; Li, P.; Fleming, B.C.; Chen, Q.; Wei, X.; Xiao-Hua, P.; Li, G.; Wei, L. Attenuation of cartilage pathogenesis in post-traumatic osteoarthritis (PTOA) in mice by blocking the stromal derived factor 1 receptor (CXCR4) with the specific inhibitor, AMD3100. J Orthop Res. 2015, 33(7), 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Siebuhr, A.S.; Brandt-Hansen, N.U.; Wang, J.; Su, D.; Zheng, Q.; Simonsen, O.; Petersen, K.K.; Arendt-Nielsen, L.; Eskehave, T.; Hoeck, H.C.; Karsdal, M.A.; Bay-Jensen, A.C. Type X collagen levels are elevated in serum from human osteoarthritis patients and associated with biomarkers of cartilage degradation and inflammation. BMC Musculoskelet Disord. 2014, 15, 309. [Google Scholar] [CrossRef] [PubMed]
- Poole, A.R.; Ionescu, M.; Fitzcharles, M.A.; Billinghurst, R.C. The assessment of cartilage degradation in vivo: development of an immunoassay for the measurement in body fluids of type II collagen cleaved by collagenases. J Immunol Methods 2004, 294(1-2), 145–153. [Google Scholar] [CrossRef]
- Kuhi, L.; Tamm, A.E.; Tamm, A.O.; Kisand, K. Risk Assessment of the Progression of Early Knee Osteoarthritis by Collagen Neoepitope C2C: A Longitudinal Study of an Estonian Middle-Aged Cohort. Diagnostics 2021, 11(7), 1236. [Google Scholar] [CrossRef]
Figure 1.
A – micrograph of a sample with histopathology grade 0: weak C2C immunostaining (brown) in the superficial and deep zones (counterstaining of proteoglycans with Toluidine-blue. The cartilage content of proteoglycans determined by the amount of Toluidine blue staining was decreased in the tissue samples with more advanced OARSI tissue damage grade; B – micrograph of a sample with histopathology grade 1.5: moderate C2C immunostaining (brown) in the superficial and upper parts of the middle zone (counterstaining of proteoglycans with Toluidine-blue); C – micrograph of a sample with histopathology grade 3.5: overall abundant C2C immunostaining (brown), weak counterstaining in the deep zone (counterstaining of proteoglycans with Toluidine-blue); D – micrograph of a sample with histopathology grade 6: abundant C2C immunostaining (brown) in the remaining cartilage; subchondral bone, which occupies most of the specimen, is virtually not stained (counterstaining of proteoglycans with Toluidine-blue). A sample picture of negative control where the primary antibody was omitted is presented as an inset in the upper right corner of micrograph D. All micrographs were taken using a 5 × objective.
Figure 1.
A – micrograph of a sample with histopathology grade 0: weak C2C immunostaining (brown) in the superficial and deep zones (counterstaining of proteoglycans with Toluidine-blue. The cartilage content of proteoglycans determined by the amount of Toluidine blue staining was decreased in the tissue samples with more advanced OARSI tissue damage grade; B – micrograph of a sample with histopathology grade 1.5: moderate C2C immunostaining (brown) in the superficial and upper parts of the middle zone (counterstaining of proteoglycans with Toluidine-blue); C – micrograph of a sample with histopathology grade 3.5: overall abundant C2C immunostaining (brown), weak counterstaining in the deep zone (counterstaining of proteoglycans with Toluidine-blue); D – micrograph of a sample with histopathology grade 6: abundant C2C immunostaining (brown) in the remaining cartilage; subchondral bone, which occupies most of the specimen, is virtually not stained (counterstaining of proteoglycans with Toluidine-blue). A sample picture of negative control where the primary antibody was omitted is presented as an inset in the upper right corner of micrograph D. All micrographs were taken using a 5 × objective.
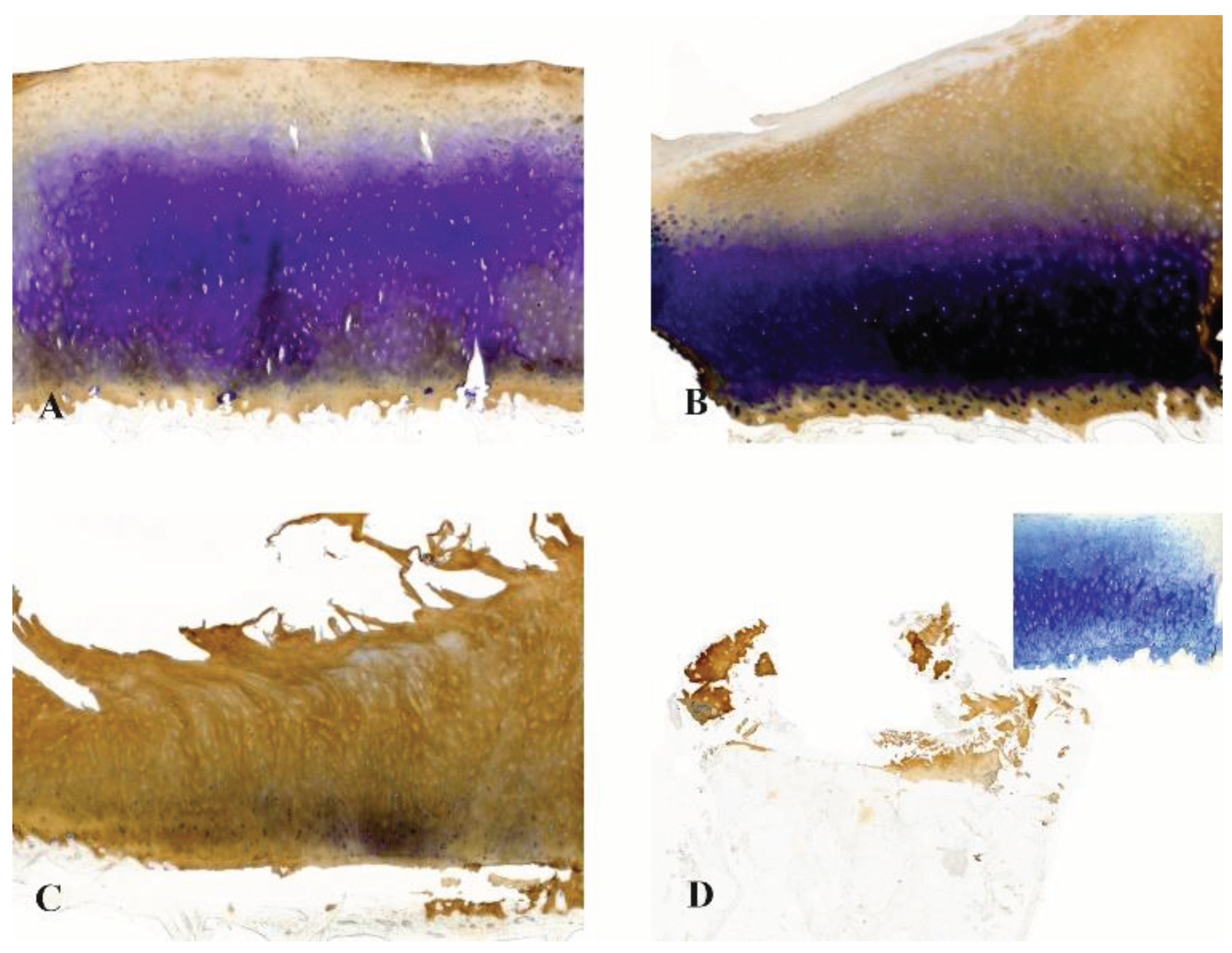

Table 1.
Patients’ characteristics and results of histopathology assessments and C2C staining. F – female patients; M – male patients; LTM – lateral tibial plateau, meniscus-covered area biopsy; MTM – medial tibial plateau, meniscus-covered area biopsy; * Due to technical problems, no MTM sample was obtained from patient 6.
Table 1.
Patients’ characteristics and results of histopathology assessments and C2C staining. F – female patients; M – male patients; LTM – lateral tibial plateau, meniscus-covered area biopsy; MTM – medial tibial plateau, meniscus-covered area biopsy; * Due to technical problems, no MTM sample was obtained from patient 6.
| No of patient | Gender | Age (years) | Tibial plateau site | OARSIhisto- grade | Macroscopic damage (stage) | OARSI score (grade × stage) | Assessment of C2C staining, % |
|---|---|---|---|---|---|---|---|
| 1 | F | 60 | LTM | 6 | 2 | 12 | 57.8 |
| MTM | 3.5 | 7 | 93.7 | ||||
| 2 | M | 58 | LTM | 3.5 | 3 | 10.5 | 28.2 |
| MTM | 1.5 | 4.5 | 80 | ||||
| 3 | F | 58 | LTM | 2.5 | 3 | 7.5 | 87.3 |
| MTM | 2.5 | 7.5 | 60.7 | ||||
| 4 | F | 65 | LTM | 3.5 | 3 | 10.5 | 90.8 |
| MTM | 4.5 | 13.5 | 79.2 | ||||
| 5 | F | 61 | LTM | 2.5 | 4 | 10 | 96.1 |
| MTM | 6 | 24 | 97.8 | ||||
| 6* | M | 59 | LTM | 2.5 | 1 | 2.5 | 51.7 |
| MTM | - | - | - | ||||
| 7 | F | 64 | LTM | 1.5 | 3 | 4.5 | 74.8 |
| MTM | 4.5 | 13.5 | 52.1 | ||||
| 8 | F | 65 | LTM | 3 | 3 | 9 | 64.7 |
| MTM | 4.5 | 13.5 | 99 | ||||
| 9 | F | 65 | LTM | 4 | 2 | 8 | 16.2 |
| MTM | 3 | 6 | 45.6 | ||||
| 10 | F | 55 | LTM | 2.5 | 1 | 2.5 | 44.4 |
| MTM | 2 | 2 | 53.4 | ||||
| 11 | F | 58 | LTM | 3 | 2 | 6 | 52.9 |
| MTM | 2.5 | 5 | 62.8 | ||||
| 12 | F | 59 | LTM | 1.5 | 1 | 1.5 | 55.6 |
| MTM | 2 | 2 | 42.3 | ||||
| 13 | F | 59 | LTM | 2.5 | 2 | 5 | 88.8 |
| MTM | 4 | 8 | 67.5 | ||||
| 14 | M | 58 | LTM | 2 | 3 | 6 | 47.2 |
| MTM | 5.5 | 16.5 | 100 | ||||
| 15 | F | 57 | LTM | 3 | 2 | 6 | 71.5 |
| MTM | 3 | 6 | 79.7 | ||||
| 16 | F | 63 | LTM | 2 | 2 | 4 | 93.1 |
| MTM | 2.5 | 5 | 79.5 | ||||
| 17 | M | 55 | LTM | 1.5 | 2 | 3 | 50.8 |
| MTM | 4.5 | 9 | 74.6 | ||||
| 18 | M | 66 | LTM | 4.5 | 3 | 13.5 | 86.7 |
| MTM | 5 | 15 | 94.4 | ||||
| 19 | M | 65 | LTM | 3.5 | 3 | 10.5 | 82.5 |
| MTM | 3.5 | 10.5 | 91.2 | ||||
| 20 | M | 58 | LTM | 0 | 3 | 0 | 36.5 |
| MTM | 3 | 9 | 100 | ||||
| 21 | M | 62 | LTM | 4.5 | 3 | 13.5 | 29.5 |
| MTM | 5.5 | 16.5 | 80.9 | ||||
| 22 | F | 60 | LTM | 4 | 2 | 8 | 60.4 |
| MTM | 1.5 | 3 | 69.8 | ||||
| 23 | M | 58 | LTM | 2 | 2 | 4 | 90.2 |
| MTM | 4 | 8 | 73.5 | ||||
| 24 | F | 65 | LTM | 2.5 | 2 | 5 | 44.8 |
| MTM | 4 | 8 | 81.2 | ||||
| 25 | F | 56 | LTM | 3.5 | 3 | 10.5 | 60 |
| MTM | 6 | 18 | 99.1 | ||||
| 26 | F | 63 | LTM | 2 | 4 | 8 | 73.2 |
| MTM | 6.5 | 26 | 73.1 | ||||
| 27 | M | 59 | LTM | 2.5 | 2 | 5 | 69.2 |
| MTM | 3.5 | 7 | 95.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



