
Submitted:
20 March 2024
Posted:
21 March 2024
You are already at the latest version
Abstract
Abstract. Introduction: BMD study gives partial information on bone health in patients with TSH suppression therapy due to Differentiated Thyroid Cancer (DTC). TBS, a new parameter of bone microarchitecture is propose for bone quality study. This study analyze their long-term use in patients with DTC. Methods: BMD was measured by DXA and TBS with iNsigth software in 145 postmenopausal DTC patients. Vertebral Fractures (VFs) with a semi-quantitative x-ray method. Results: BMD at the end study was not different from initial. TBS decreased from 1.35±0.1 to 1.27±0.1 (p=0.002). PTH, Osteocalcin, and BAP were increased, suggesting increased bone remodeling. There was an increase in osteoporosis and osteopenia (40.6% and 16.5% to 46.6% and 18.6%); 31% had partially degraded and 15.1% degraded TBS changed to 48,9% and 24,8% at the end study. VFs in 30 patients, was not different in age, BMI, calcium and alcohol ingestion, smoking, radioiodine, or thyroid parameters vs. without VFs. Odds ratio for VFs increased with osteopenia (OR 2.63). Combination of TBS plus TBS did not improve discrimination. Conclusions: TBS was lowered while BMD did not differ. Percentage of osteoporosis and osteopenia and of partially degraded and degraded TBS was higher at the end study. Predominant discordance rate was found in partially degraded microarchitecture, in which the proportion of osteopenia was higher than normal or osteoporotic patients. AUC of TBS plus BMD did not improve discrimination. TBS, radioactive iodine, and sedentary lifestyle were the main differential data for patients with DTC and VFs.
Keywords:
differentiated thyroid cancer
; TSH suppression therapy
; bone mineral density
; Trabecular Bone Score
; levothyroid
1. Introduction
Thyroid Carcinoma is the most common endocrine malignancy, and the increasing use of diagnostic and imaging modalities has contributed to its higher prevalence [1]. Patients with Differentiated Thyroid Carcinoma (DTC) are a majority in this group, in which TSH suppressive therapy with levothyroxine (LT4) has been recommended to reduce the stimulatory effects of TSH [2]. Up to now, thyroidectomy followed by radioactive iodine therapy and long-term TSH suppression with LT4 is recommended for DTC. It has been reported that postmenopausal patients with DTC could be at risk for bone loss and fractures, related to the suppressive effect of TSH [3]. For men and premenopausal women, these risks have not been clearly demonstrated. Also, a high prevalence of vertebral fractures (VFs) has been reported and is now considered the most common type of fracture associated with this condition [4].
Although measurement of bone mineral density (BMD) using dual-energy X-ray absorptiometry (DXA) is considered the gold technique for the diagnosis of bone loss, it is also recognized, that DXA has an important limitation because the majority of fractures occur in osteopenic women or even at normal BMD [5]. On the other hand, it is well-recognized that BMD can have higher scores in the presence of osteoarthritis, vascular and joint calcification, and lumbar scoliosis[6]. Therefore measurement of BMD can not estimate the overall severity of the impact on bone of any disease or drug.
There is an effort to evaluate if bone quality determination can improve the selection of high-risk patients for fractures, besides DXA. For the analysis of bone quality, techniques such as trabecular bone score (TBS), semiquantitative radiology, QCT, MRI, microindentation, and SHAFT 3D have been proposed. The use of TBS has the advantage of being non-invasive and lower cost. It is a gray-scale textural analysis of anteroposterior Lumbar Spine DXA, obtained for BMD measurement, sensitive to change over time, with treatments and progression bone disease in a wide range of secondary osteoporosis. TBS has been shown to capture morphometric properties of vertebral bone by using pixel-based gray-level variations, thus giving information beyond DXA alone. TBS is a BMD-independent predictor of skeletal strength and fracture risk that can be a complement to the prediction of future osteoporotic fracture [7]. Studies to evaluate bone quality using TBS in DCT patients are scarce.
This study aimed to analyze the concordance and difference evolution in TBS, BMD, and Vertebral Fractures (VFs) after a long-term follow-up of postmenopausal DTC patients with total thyroidectomy due to differentiated thyroid cancer and L-thyroxine (LT4) suppressive therapy.
2. Patients and Methods
2.1. Study Population
We performed a study, including postmenopausal patients who underwent a total thyroidectomy due to DTC and underwent DXA three months after surgery, with a mean follow-up of 10 years with TSH suppression treatment with LT4 at our center. These patients were supervised in our Thyroid Unit and followed every 6-12 months. Patients were included if they were one year with menopause, and had maintained the TSH suppression (<0.5 µU/mL) during 80% of visits at our Center. Informed consent was required from all patients. There were no included if they had taken medications that could affect bone metabolism (calcium or vitamin D, antiresorptive, hormone replacement therapy) or had other diseases that could affect bone metabolism (hyper and hypoparathyroidism, hyper and hypothyroidism, rheumatoid arthritis, asthma, Paget disease) and abnormal kidney or liver function. Calcium ingestion and physical activity standard questionnaires were performed. The study was approved by the Ethical Committee of the University Hospital 12 de Octubre, Madrid, Spain.
2.2. Laboratory Determinations
Fasting serum samples were obtained at the baseline study after 3 months of thyroidectomy and suppressive TSH therapy and at the end study, between 8 and 9 AM and immediately frozen at -70 ºC until the assays were performed. Serum Calcium (corrected for albumin binding), Phosphate, and creatinine were measured by automated standard laboratory methods (Modular P800; Roche Diagnostic). Serum TSH was measured by chemiluminescence (Architect), free T4 by electrochemiluminescence (E, CLIA)(functional sensitivity <0.01 ug/mL ), thyroglobulin using Immulite 2000 (functional sensitivity 0,9 ng/ml)(normal range ). Serum intact PTH was determined using chemiluminescent immunoassays (IMMULITE 2000, DPC) (normal range: 7-57pg/ml. Serum 25–hydroxyvitamin D3 [25OHD] was measured by enzyme immunoassay (automated IDS EIA, kit. Vitamin D deficiency was considered for values below 20 ng/ml. Osteocalcin: OC (N-MID Osteocalcin, Roche Diagnostics, electrochemiluminescence (normal range: 8-48 ng/ml), Bone Alkaline Phosphatase: BAP (IDS EIA)(normal range: 15-40 U/L) and β-cross-laps: β-CTX (ELECSYS 1010, Roche, electrochemiluminescence) (normal range: 0.2-0.704 ng/ml).].
BMD was assessed by DXA, (densitometer QDR 4500, Hologic, Waltham MA) at the lumbar spine(L-BMD), femoral neck (FN-BMD), total hip (TH-BMD) and distal third of the radius (1/3DR-BMD). The Coefficient of Variation was 0.90 % at LS-BMD and 0.70% at FN-BMD. The least significant change was 1.8% and 2.9% for L-BMD and TH-BMD. BMD values were expressed as absolute values (g/cm2) and as standard deviations (SD) from the expected adult BMD for T scores. Reference databases corresponding to the Spanish population were used and were obtained from a multicenter densitometric study with 1305 healthy women, aged 20-80 years [8]. Patients had the same bone densitometry scan initially and after, using the same DXA system. The diagnosis was carried out according to the WHO criteria (T scores); Osteoporosis if an individual´s BMD is equal to or less than -2.5 standard deviations below the mean normal BMD value of healthy young adults; osteopenia between -1≥ and > -2.5; and normal > -1 [9].
Trabecular Bone Score (TBS) measurements were performed by applying the TBS iNsight 2.0 software (Med-Imaps, Swiss) to the L-BMD DXA exams. Lumbar TBS was calculated as the mean value of individual measurements for vertebrae L1-L4. Patients according to the reference values were categorized into three groups: TBS ≥1.350 is considered normal; TBS between 1.350 and 1.200 is consistent with partially degraded microarchitecture, and TBS ≤1.200 with degraded microarchitecture [10]. The coefficient of variation of TBS calculated from 3 repeated measurements in 15 women was 0.8%.
Lateral and anterioposterior radiographs of the thoracic and lumbar spine were obtained in the upright position for all subjects during the study. Vertebral fractures were identified on X-ray films according to the method of Genant et al. by a trained radiologist [11].
2.3. Statistical Analysis
Quantitative variables were expressed as mean and standard deviation or median and interquartile range. The normal distribution pattern was confirmed by the Kolmogorov-Smirnov test. Qualitative variables were described as absolute and relative percentages. Contingency tables and Chi-square or Fisher Exact test were used to compare categorical parameters. McNemar´s test or Simmetry’s test compared the change in the distribution of classification of patients with Thyroid Cancer according to DXA and TBS scores. The non-parametric U-Mann-Whitney-Wilcoxon test or Student's t-test was used for the cross-sectional study and Student's t-test for the longitudinal study. Pearson correlation was performed to assess correlations between clinical parameters and DXA and TBS parameters.
Linear regression was performed to evaluate the dependence and influence between variables with TBS and BMD Lumbar Spine, expressed by the coefficient and 95% confidence interval. Also, a logistic regression was carried out to study the association between the possible risk factors and the final fractures, expressing the results in odds ratio (OR) together with the 95% confidence interval (95%CI). The statistical study was completed with multivariate analysis, considering both those risk factors with a significant result in the univariate analysis and those that have a certain relevance within the objectives of the study. The use of stepwise selection was employed, to highlight the most relevant factors, identify those significant sets among the possible variables, and avoid confounding the model due to possible relationships between them since the method determines the significance of the effect of a variable in the presence of those already in the model. The accuracy, along with its 95% confidence interval was estimated using the ROC curve.
All analyses were done using Stata InterCooled for Windows version 16 (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC) and SAS for Windows version 9.4 (SAS Instute Inc., Cary, North Carolina, U.S.A.) and a significance level of 5%.
3. Results
Table 1 represents the baseline and final data of the 145 postmenopausal DTC caucasian patients that meet the criteria selection. The mean age of patients at surgery was 51 years. Mean BMI was slightly higher at the end study after a mean of twelve years (28±45 kg/m2 vs. 27±0.6 kg/m2). Mean LT4 doses were lower and there was a significant increase in serum TSH levels at the end study (0.89±0.3 µU/mL vs. 0.23±0.4 µU/mL). Serum-free T4 levels did not change. A significant increase in serum PTH, and in bone markers (Serum Osteocalcin, Bone Alkaline Phosphatase)was found at the end study. Beta-Crosslaps only measured at the end study, were in the normal postmenopausal reference values. There was a non-significantly tendency to lower BMD values at the lumbar, hip, and radial sites. TBS values were significantly decreased in the end study from 1.35±0.14 to 1.27±0.13. Initially, patients with DXA osteoporosis (n=24) had lower TBS values (1.28±0.11) compared to those with normal-osteopenia BMD values(n=121, 1.36±0.14, p=0.029) performed initially and the end of study (Figure 1).
Patients were classified according to the DXA and TBS study. In the initial study, (Table 2) 42.7% had DXA scores in the normal range, vs. 40.6% and 16.5% in the osteopenia and osteoporosis range respectively. At the end study (Table 3), 34.4% had normal DXA values, vs. 46.6 % and 18.65% in the osteopenia (n=69) and osteoporosis (n=27) range respectively. Therefore there was an increase in the number of patients with osteoporosis and osteopenia. In the initial study, 31% of patients had partially degraded TBS values, degraded TBS 15.1%, and normal scores 53.7%. At the end study, the number of patients with partially degraded and degraded TBS had a significant increase to 48,9%, and 24.8% respectively, while the number of patients that remained with normal TBS scores was reduced to 26.2%.
When comparing these differences in TBS and DXA scores changes (Table 4), we found an increase in patients with degraded TBS (36 in the end study, vs. 22 in the initial study), associated with osteopenia and osteoporosis. There was also a significant decrease in TBS values in this group (1.22±0.07) when compared with the group with normal-osteopenia BMD (1.29±0.13, p=0.019). Therefore the predominant discordance rate of TBS with DXA was found in patients with partially degraded microarchitecture, in which the proportion of patients with osteopenia was higher than normal or osteoporotic patients (Figure 2). At the end study, we performed a questionnaire concerning calcium intake, without finding differences in this parameter between the groups with normal (561±195 mg/d), osteopenia (572±301 mg/d ), and osteoporosis (588±294 mg/d).
The association between TBS and lumbar DXA scores of baseline and end study was found to be significant when analyzed with Fisher´s exact test (<0.0001). The symmetry between Table 2 and Table 3 was confirmed (p<0.0001). The partial analysis yielded significant results when comparing the T Score of Lumbar BMD with TBS values in the baseline study (Chi-Square 0.0057)and in the second study (<0.0001). Also, the analysis of the same variables, TBS values of the baseline study with TBS values of the end study confirmed association (Test of Symmetry <.0001), although this was not found with T scores of lumbar BMD, of the first and second studies (Test of Symmetry 0.2123).
When comparing VFs incidence found in 30 patients during the follow-up (Table 5), with patients without VFs (n=115) there were no differences in age, BMI, smoking, calcium intake, or ethanol ingestion. Osteoporosis was diagnosed in 13 of the patients (11.3%) without VFs, and in 4 of 30 with VFs (13.3%). Thyroid parameters as well as bone markers were also similar. Three patients with DXA in the osteoporosis range and partially degraded TBS had VFs, 17 in the densitometric osteopenic range (3 normal, 9 with partial, and 5 with degraded TBS). Of the 10 patients with normal DXA values, 2 had degraded TBS (Table 6).
There were no differences in VFs between patients with strong TSH suppression levels (n=13, <0.1 µU/ml) versus those with moderate TSH suppression (n=17, 0.1-0.5 µU/ml). When comparing TBS and DXA T scores of the second study, of the 30 patients with vertebral fractures, there were significant changes in values as shown with Fisher´s Exact Test (P=0.0009).
In the baseline study, L-BMD was correlated with TBS (r=0.38, p=<0.001) while the latter variable was inversely correlated to BMI (r=-0.35, p=0.0003). At the end study, an inverse correlation was found between L-BMD and BMI (r=0.32, p=0.0001), and a weak correlation with 25OHD vitamin D levels (r=-0.17, p=0.45). As expected, TBS was also inverse-related to BMI the the end study (r=-0.41,p=0.0000). Bone markers(Osteocalcina, Beta-Cross Laps) were not correlated with any variable in both studies. There was no correlation between L-BMD and free thyroxine levels in the initial or end studies, while TBS was inverse correlated with free thyroxine levels (r=-0.20, p=0.040) in the initial and not in the final study. The AUC for the TBS plus BMD model was 0.5261(0.4423-0.6679)( (Figure 3 ) and did not improve discrimination of TBS alone. In the multivariate logistic regression analysis, using VFs as the dependent variable, the Odd Ratio for incidental fractures was 0.96 (95% CI .93-.99, p=0.037), since diagnostic to end DXA study OR 1.08, (95%CI 1.02-1.14, p=0.004), for TSH levels OR 2.32, (95% CI 1.074-5,01,p= 0.032). The odds ratio for incident fractures was increased in patients having osteopenia (OR 2.63, 95%CI 1.11-6.24, p=0.028). For BMD T-scores, TBS OR was significant at degraded (4.33, CI 1.079-17-388,p=0.039) and partially degraded (4.06, CI 1.2277-13.489, p=0.022).
4. Discussion
In our study, we found a slight non-significant decrease in BMD in postmenopausal women with DTC and TSH suppression after 12 years of follow-up. In contrast, TBS scores were significantly decreased in this period. This is in agreement with previous reports, that a significative BMD loss is only found after a long disease duration [12]. Also, bone microarchitecture was found to diminish more in patients who had incidental VFs during this long period. There were lower serum 25OHD levels and, an increase in serum PTH together with serum Osteocalcin and BAP,(bone formation markers) with normal β-CTX (bone resorptive marker) suggesting a slight imbalance overtime of bone turnover, which could be according to the tendency to lower BMD values found at the end of the study.
There were no differences in dietary calcium intake and smoking in our patients between the initial and end studies. The average calcium intake was in the range of the mean calcium dietary intake (629 ±290 mg/day) reported in a large Spanish population study [13]. There was also no difference in calcium intake between fractured (477.50-750 mg/d) and non-fractured (250-750 mg/d) patients. Our patients had low serum 25OHD levels, in the initial and end studies. Hu et al, reported that the serum concentration of 25OHD was inversely correlated to thyroid cancer risk: OR was 1.42 (95 CI 1.17-1.73) in vitamin D deficient compared with those with normal levels [14]. We also found in a study performed with 134 postmenopausal women with DTC that serum 25OHD deficiency was present in 43%, and was associated with abnormal trabecular microarchitecture, compared with patients with levels below 30 ng/ml, suggesting a contribution of lower 25OHD levels to increased fracture risk.
In studies with two years of patient follow-up, it has been reported that TSH suppressive therapy did not induce a significant difference in BMD compared to healthy controls [12,16,17]. In contrast, a meta-analysis described lower spine bone mineral density in 177 postmenopausal patients, and a duration of TSH suppression of more than 5 years, compared with 69 patients with less than 5 years of treatment duration [18]. Also, it has been reported that TBS in patients with DTC treated with long-term TSH suppression have lower TBS that can predict the relative fracture risk in these patients [19,20].
TBS was found not to deteriorate in 43 DTC patients with suppressed TSH compared with 20 on LT4 replacement for less than 4 years [21]. However, when analysed the 31 postmenopausal patients were found to have significative lower degraded TBS compared with the 32 premenopausal. In the study of Moon et al, data showed that 4.2 years of TSH suppression in postmenopausal DTC patients was associated with a significant decrease in TBS independent of BMD changes [20]. In our experience, moderate suppression of TSH in the range of 0.1-0.5 uUI/ml was associated with lower values of TBS [22]. It is therefore possible that earlier damage to trabecular architecture can increase susceptibility to bone fractures in this disease. Patients with higher TBS can have a better trabecular architecture, and therefore be more resistant to these events.
We detected VFs during the follow-up in 20.6% of our DTC patients. Data on fracture risk in patients with DTC on TSH suppression therapy are scarce. Our study was not designed to evaluate VFs incidence. We performed a semiquantitative visual assessment of spinal X-rays.
There have been two small cross-sectional studies in postmenopausal women after total thyroidectomy for DTC studying VFs. In the first, Fujiyama et al found no difference in incidental VFs in 12 compared with 12 TSH non-suppressed patients [23]. In the other study, Heijckmann et al, found a prevalence of 7% of VFs in 59 patients, concluding that was lower than the 12% of the European population [24]. On the other hand, in a larger study, Mazziotti et al., assessed by quantitative morphometric approach VFs in 178 postmenopausal women treated for DTC for at least one year, and VFs were detected in 51 (28%); with older age, osteoporosis, TSH level <0.1 mU/L, and duration of LT4 treatment, significantly associated. However in this study, TSH was measured on a single occasion, and patients with VFs had a higher duration of treatment and lower BMD compared with those without [4]. In the NHANES 2005-2006 analysis, it was shown that older women with higher levels of physical activity had higher TBS [25]. Our patients with DTC and VFs practice lower daily exercise (less stimulus for bone remodeling), with no difference in age, smoking, ethanol, or calcium ingestion. Recently in a larger study with 74.774 thyroidectomized patients with a mean follow-up period of 4.5 years, the group that had exercise showed a significant decrease in the risk of any fracture (VFs: HR 0.848) compared with those that lacked physical activity [26]. It is possible therefore the lack of physical activity can contribute to the lower TBS and fracture risk. Histology type, Thyroglobulin levels, TNM stage as well as radioactive iodine was not found significantly different.
The finding that patients with DTC have a lower TBS, even in the presence of normal BMD, is of major clinical importance. It has been accepted, that patients with normal BMD, have lower fracture risk, but in the clinical setup, many patients with VFs have normal BMD scores. Recently TBS measurement has been useful for the detection of VFS in patients with secondary osteoporosis [27]. We agree with the potential use of TBS, as complementary for fracture risk, especially in the presence of normal BMD. This could be due because our older patient populations can have degenerative changes in the lumbar spine, which can increase BMD, and disease-induced changes in trabecular structure could contribute to an increase in the fracture risk.
In our study, 3% of patients transitioned to osteoporosis and 6% to osteopenia during the long follow-up different from other series followed during shorter years [28]. TSH suppression duration referred to in this study was quite variable (15-85 months), and the transition from normal BMD and mild osteopenia to osteoporosis was 0.6% and 3.2% respectively in this report.
TBS showed an overall significant correlation with all BMD sites analyzed, particularly with L- BMD in all the studies. However, when patients with osteopenia, osteoporosis, and normal BMD were related to their degree of TBS scores, there were significant discrepancies. Patients with lower BMD had a major proportion of TBS scores in the range of degraded and partially degraded. In this study correlations between BMI and bone parameters were found (L-BMD r=0.32,p=0.0001 and TBS r=-0.41, p=0.00009. Therefore, an increase in adiposity overlying the region of interest may lower the signal-to-noise ratio, favoring lower TBS. In this study, the BMI of our non-obese patients was well within the working range recommended for TBS (15-37 kg/m2) [29].
Our study has several limitations. The study was performed in only one center, and therefore extrapolation should be considered, as well as the retrospective design, which could interfere with establishing the relationship between TSH suppression and its bone effects. Although TSH levels in the study were periodically assessed to confirm maintenance within the intended level, fluctuation in TSH levels cannot be ruled out. Data on other factors such as the familiar history of fractures and falls were not registered. Although there were 30 fractures, the number of participants was relatively small. As a strength, patients were followed by the same physicians, with a single expert in densitometry. Also, VFs were radiologically analyzed by an expert. To our knowledge is the first study to compare in a group of postmenopausal DCT women in which the average TSH suppression level was maintained, the changes of TBS and DXA after a long follow-up.
5. Conclusions
Our study demonstrates that in DTC postmenopausal women with TSH suppressive therapy, BMD is only slightly diminished after a long follow-up of 12 years, while TBS was significantly diminished. Our results suggest an association between TSH suppression and the risk of bone quality damage. Patients with VFs have similar clinical and hormonal data, to those without VFs, but display a low exercise performance and a lower TBS. TBS scores with degraded microarchitecture were more associated with osteopenia, suggesting that these patients should be followed and assessed for higher fracture risk.
Authorship Contributions
FH and GM designed and analyzed the study, CM, SL, and MBL contributed to data interpretation, collected the data, and analyzed the data. MBL drafted the manuscript. All authors agreed on the final context of the manuscript
Funding
This study received no external funding
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and complies with the principles of Good Clinical Practice. The study was approved by the Ethical Committee of University Hospital 12 de Octubre. Written informed consent from participants was required.
Data Availability Statement
The data of these reported results are available from the corresponding author upon request.
Conflict of Interest
The authors declare no conflict of interest
References
- Cabanillas ME, McFadden DG. , DuranteC. Thyroid cancer. Lancet 2016, 388, 2783–2795. [Google Scholar] [CrossRef] [PubMed]
- D. S. Cooper, B. Specker, M. Ho, M.Sperling M, P.W. Ladenson, D.S. Ross, K.B. Ain, S.T. Bigos, J.D. Brierley, B.R. Haugen, I. Klein, J.Robbins, S.I. Sherman, T. Taylor, H.R. Maxon. Thyrotropin suppression and disease progression in patients with DTC. Results from the National Thyroid Cancer Treatment Cooperative Registry. Thyroid 1998, 8, 737–744. [Google Scholar]
- M. Papaleontiou,S.T.Hawley, M.R. Haymart MR. Effect of thyrotropin suppression therapy on bone in thyroid cancer patients. The Oncologist 2016, 21, 165–171. [Google Scholar] [CrossRef] [PubMed]
- G. Mazziotti, A.M. Formenti, S. Frara, R. Olivetti, G. Banfi, M.Memo, R, Maroldi, R Giubbini, A Giustina. A High prevalence of radiological vertebral fractures in women on TSH suppressive therapy for thyroid carcinoma. Journal of Clinical Endocrinology and Metabolism 2017, 103, 956–964. [Google Scholar]
- E S Siris, P D Miller, E Barrett-Connor, K G Faulkner, L E Wehren, T A Abbott, M L Berger, A C Santora, L M Sherwood. Identification and fracture outcomes of undiagnosed low bone mineral density in postmenopausal women; results from the national osteoporosis Risk Assessment. JAMA 2001, 286, 2815–22. [Google Scholar] [CrossRef] [PubMed]
- Jie-Eun Lee, Kyoung Min Kim, Lee-Kyung Kim, Kyong Young Kim, Tae Jung Oh, Jae Hoon Moon, Sung Hee Choi, Soo Lim, Sang Wan Kim, Chan Soo Shin, Hak Chul Jang. Comparisons of TBS and lumbar spine BMD in the associations with vertebral fractures according to the T-scores: A cross-sectional observation Bone 2017, 105, 269–275.
- McCloskey Ev, Oden A, HarveyN, Leslie WD, Hans D, Johansson H, Barkmann R, Boutroy S, Brown J, Chaputlat R, et al. Meta-analysis of trabecular bone score in fracture risk prediction and its relationship to FRAX. J Bone Miner Res 2018; 31:940-8.
- 8. M. Diaz Curiel, J.L.Carrasco de la Peña, J. Honorato Perez, R. Perez Cano, A. Rapado,I. Ruiz Martinez. Study of bone mineral density in lumbar spine and femoral neck in a Spanish population. Multicentre Research Project on Osteoporosis. Osteoporosis International 1997; 7: 59-64 .
- JA Kanis, LJ Melton, C Christiansen, CC Johnston, N Khaltaev. The Diagnosis of Osteoporosis. Journal of Bone and Mineral Research 1994, 9, 1137–41. [Google Scholar] [CrossRef] [PubMed]
- V.B.C. Silva, W.D. Leslie, H. Resch, O. Lamy, O.Lesnyak, N.Binkley, E.V.McCloskey, J.A. Kanis. J.P. Bilezikian. Trabecular bone score: a noninvasive analytical method based upon the DXA image. . J Bone Miner Res 2014; 29: 518-530.
- H K Genant, C Y Wu, C van Kuijk, M C Nevitt. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 1993, 8, 1137–48. [Google Scholar] [CrossRef]
- Wang S, Wang Y, Zhu L, He L, Lv M, Zhang H, Wang H, Zhang F, Lai Y, Li Y, ShanZ, Teng W. Effects of TSH suppressive therapy on bone mineral density (BMD) and bone turnover markers (BMT) in patients with differentiated thyroid cancer in Northeast China: a prospective controlled cohort study. Endocrine 2023, 79, 113–124. [Google Scholar]
- Olza J, Aranceta-Bartrina J, González-Gross M, Ortega RM, Serra-Majem L, Varela-Moreiras G, Gil Á. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study. Nutrients. 2017; 21;9(2). pii: E168. [CrossRef]
- Hu, MJ, Zhang Q, Liang L, Wang SY, Zhen XC, Zhou MM, Yang YW, Zhong Q, Huan F. Association between vitamin D deficiency and risk of thyroid cancer: A case-control study and meta-analysis. J Endocrinol Invest 2018, 41, 1199–1210. [Google Scholar] [CrossRef]
- Hawkins F, Guadalixs, De Mingo ML, Allo G, Martin Ariscado C, Lopez B, Martinez Diaz, G. Association of low serum 25OHD levels with abnormal bone microarchitecture in well-differentiated thyroid cancer. 8, 2020; 8.
- Guo CY, Weetman AP, Eastell R. Longitudinal changes of bone mineral density and bone turnover in postmenopausal women on thyroxine. Clin Endocrinol (Oxf) 1997, 46, 301–7. [Google Scholar] [CrossRef] [PubMed]
- Zhang P, Xi H, Yan R. Effects of thyrotropin suppression on lumbar bone mineral density in postmenopausal women with differentiated thyroid carcinoma. Onco Targets Ther 2018, 11, 5587–6692. [Google Scholar]
- Ku EJ, Sang Yoo W, Kyung Lee E, Young Ahn H, Hoon Woo S, Hwa Hong J, Kyung Chung H, Woo Park J. Effect of TSH suppression therapy on bone mineral density in differentiated thyroid cancer: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2021, 106, 3655–3667. [Google Scholar]
- De Mingo Dominguez ML, Guadalix Iglesias S, Martin-Arriscado Arroba C, López Alvarez B, Martínez Diaz-Guerra G, Martinez-Pueyo JI, Ferrero Herrero E, Hawkins F. Low trabecular bone score in postmenopausal women with differentiated thyroid carcinoma after long-term TSH suppressive therapy. Endocrine. 2018, 62, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Moon, JH. Kim KM, Oh TJ, Choi SH, Lim S, Park YJ, Park DJ, Jang HC. The effect of TSH suppression on vertebral trabecular bone scores in patients with differentiated thyroid carcinoma. Journal of Clinical Endocrinology and Metabolism 2017, 102, 78–85. [Google Scholar] [PubMed]
- 21. Sousa BECA, Silva BC,de Oliveria Guidotti T,Pires MC, Soares MM, Kakehasi AM. Trabecular bone score in women with differentiated thyroid cancer on long-term TSH suppressive therapy. Journal of Endocrinological Investigation 2023; 44:2295-2305.
- Hawkins F, Guadalix S, De Mingo ML, Martin Arriscado C, Lopez B, Allo G, Martinez Diaz G. Trabecular bone deterioration in differentiated thyroid cancer: impact of long-term TSH suppressive therapy. Cancer Med. 2020, 9, 5746–5755. [Google Scholar] [CrossRef] [PubMed]
- Sugitani I, Fujimoto Y. Effect of postoperative thyrotropin suppressive therapy on bone mineral density in patients with papillary thyroid carcinoma: a prospective controlled study. Surgery 2011, 150, 1250–7. [Google Scholar] [CrossRef] [PubMed]
- 24. Heijckmann AC, Huijberts MS,Geusens P, de Vries J, Meneere PP, Wolffenbuttel BH. Hip bone mineral density, bone turnover and risk of fractures in patients on long-term suppressive L-thyroxine therapy for differentiated thyroid carcinoma. Eur.J Endocrinol 2005; 153, 23-29.
- Rajesh K Jain, Tamara Vokes. Physical activity as measured by accelerometer in NHANES 2005-2006 is associated with better bone density and trabecular bone score in older adults. Arch Osteoporos. 2019, 14, 29. [Google Scholar] [CrossRef]
- Kim J, Han K, Jung JH, Ha J, Jeong C, Heu JY, Lee SE, Lee J, LimY, Kim MK, Kwon HS, Son KH, Baek KH. Physical activity and reduced risk of fracture in thyroid cáncer after thyroidectomy - a nationwide cohort study. Front Endocrinol (Lausanne). 2023, 14, 1173781. [Google Scholar] [CrossRef]
- Shevroja E,Pio Cafarelli FP,Guglielmi G, HansD. DXA parameters, Trabecular Bone Score (TBS) and Bone Mineral density (BMD) in fracture risk prediction in endocrine-mediated secondary osteoporosis. Endocrine 2021, 74, 2028. [Google Scholar]
- Park H, Park J, Yoo H, Kim S, Koh JH, Jee JH, Min YK, Chung JH, Kim TH, Kang M, Kim SW. Bone density testing interval and transition to osteoporosis in differentiated thyroid carcinoma patients on TSG suppression therapy. Clinical Endocrinology 2022, 97, 130–136. [Google Scholar] [CrossRef]
- Messina C, Buonomenna C, Menon G, Magnani S, Albano D, Gitto S, Ulivieri FB, Sconfienza LM. Fat Mass does not increase the precision error of trabecular bone score measurements. Journal of Clinical Densitometry: Assessment and Management of Musculoskeletal Health, 2023, 22/3, 359–366.
Figure 1.
Results of the three-step classification approach for Differentiated Thyroid Cancer patients with TSH suppression. The first step concerns a T-score: normal (>1 SD), osteopenia (-2.5 and ≤-1 SD), and osteoporosis (<-2.5 SD) and three subdivisions: I initial visit, II end visit, and DIF= difference. The step is based on TBS classification: normal (>1.35), partially degraded (1.2 and 1.35), and degraded (<1.2), which are represented linearly by a color. Patients in the osteopenia group with a partially degraded TBS were the major group increased in the end study.
Figure 1.
Results of the three-step classification approach for Differentiated Thyroid Cancer patients with TSH suppression. The first step concerns a T-score: normal (>1 SD), osteopenia (-2.5 and ≤-1 SD), and osteoporosis (<-2.5 SD) and three subdivisions: I initial visit, II end visit, and DIF= difference. The step is based on TBS classification: normal (>1.35), partially degraded (1.2 and 1.35), and degraded (<1.2), which are represented linearly by a color. Patients in the osteopenia group with a partially degraded TBS were the major group increased in the end study.
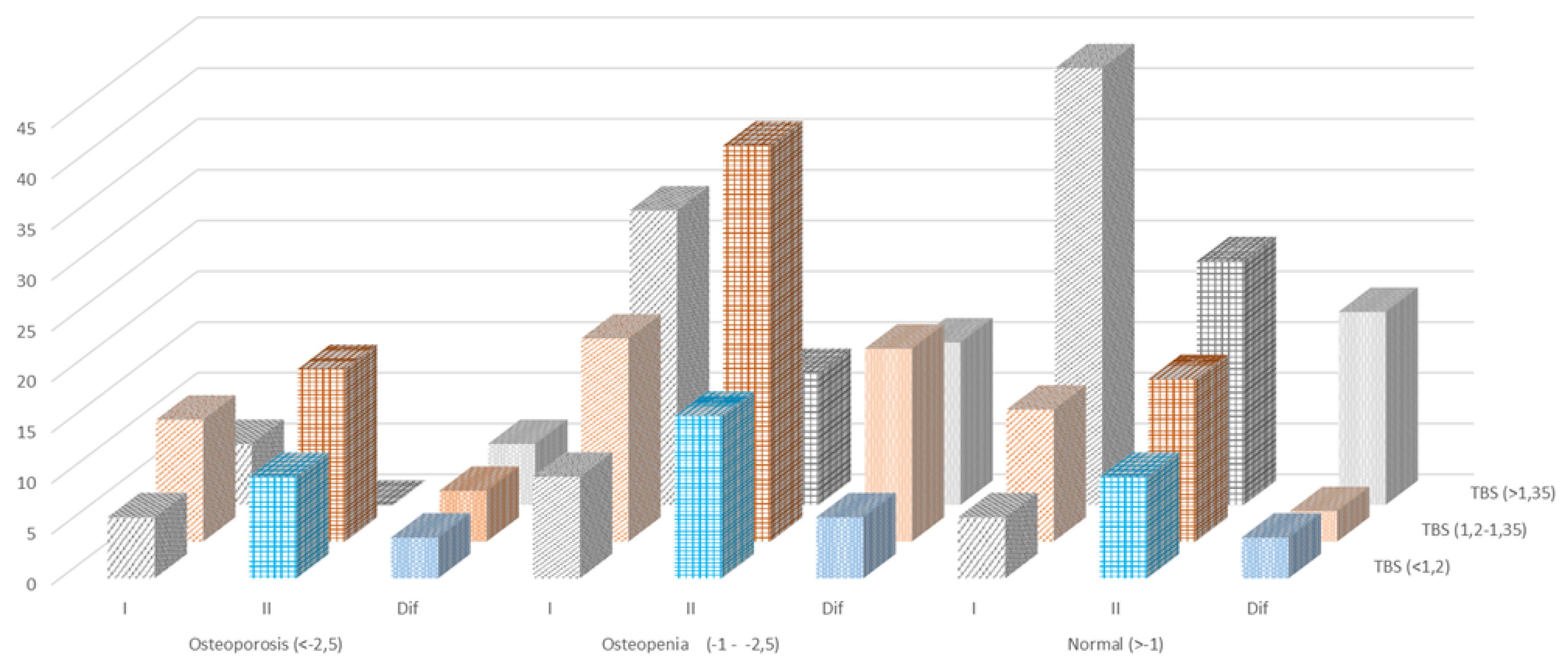
Figure 2.
Long-term changes in TBS and BMD in 145 patients with Differentiated Thyroid Cancer in the initial and end study.
Figure 2.
Long-term changes in TBS and BMD in 145 patients with Differentiated Thyroid Cancer in the initial and end study.
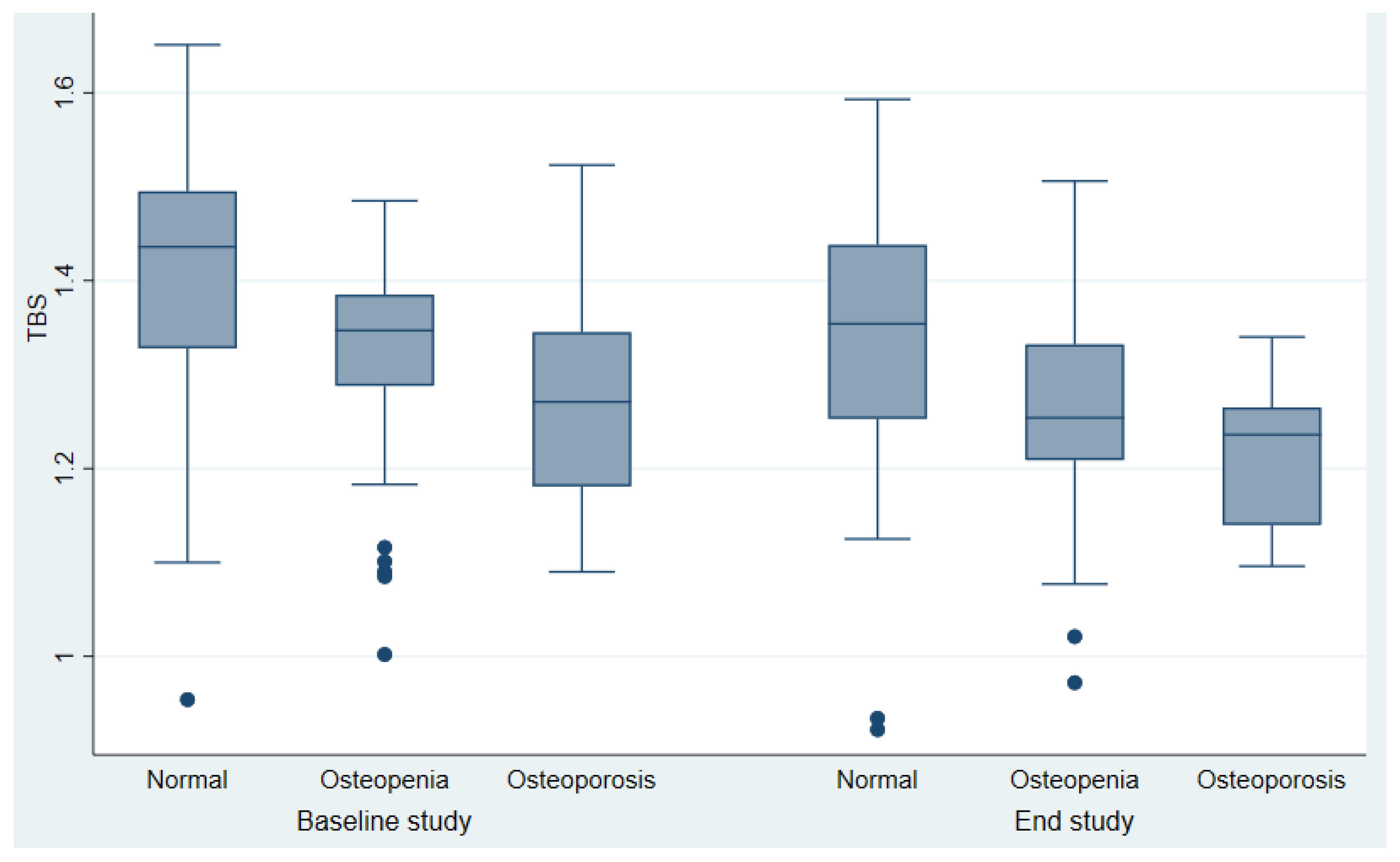
Figure 3.
Area under the receiver operating curve determined by results of the logistic regression analysis, taking TBS and Lumbar BMD as input parameters. Discriminative value of BMD alone and TBS alone or in combination with BMD in our cohort.
Figure 3.
Area under the receiver operating curve determined by results of the logistic regression analysis, taking TBS and Lumbar BMD as input parameters. Discriminative value of BMD alone and TBS alone or in combination with BMD in our cohort.
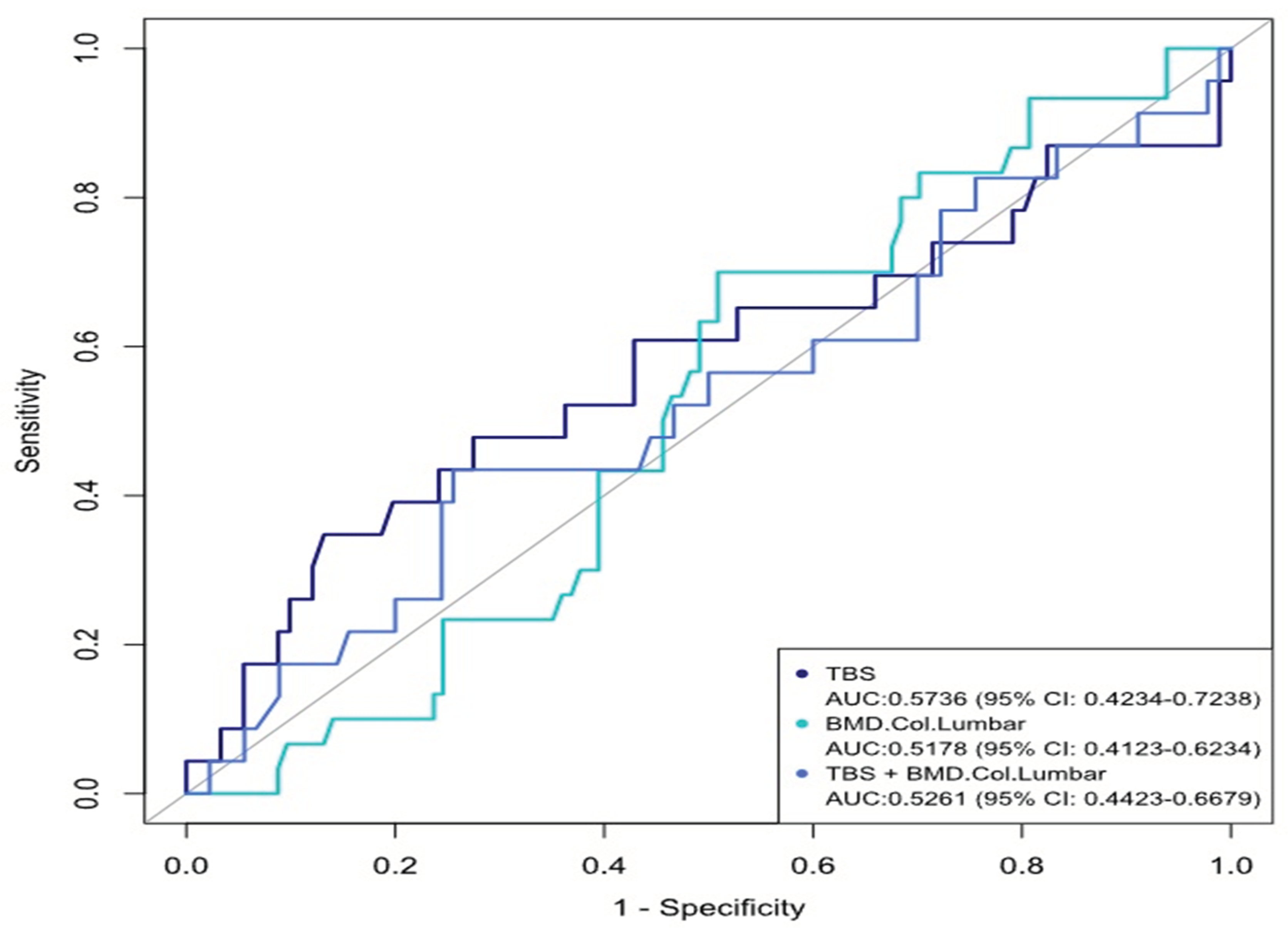

Table 1.
Clinical and biochemical parameters of Differentiated Thyroid Cancer patients at baseline and end studies.
Table 1.
Clinical and biochemical parameters of Differentiated Thyroid Cancer patients at baseline and end studies.
| Studied parameters | Baseline Study (n=145) |
End study (n=145) |
P value |
|
Clinical and hormonal data Age(years) Weight(kg) BMI (kg/m2) Menopausia (years) Smoking yes/no Alcohol ingestion LT4 (mcg/ Kg ) Serum TSH (µU/mL) Serum Free T4 (ng/dl) Duration years (range) Radioactive iodine doses mCi (range) --------------------------------- Bone markers Serum PTH (pg/mL) Serum Osteocalcin(ng/ml) β-CTX (ng/ml) BAP (U/L) Serum 25OHD (ng/ml) Densitometric parameters L-BMD (g/m2) FN-BMD(g/cm2) TH BMD(g/cm2) UD-R BMD(g/cm2) 1/3 RD-BMD(g/cm2) TBS Normal Partial degraded Degraded |
51.48±1.9 67.3 ±11.8 27,27 ± 0.6 61 (57.9%) 25(17.2%) 1(0.69%) 2.29± 0.6) 0.23±0.4 1.64 ± 0.4 - - ------------------------------- 31.03±12.1 6.93±3.5(4.53-9.86) - 10.90±7.42 26.43 ± 10,1 0.91±0.16) 0.74± 0.14) 0.91±0.16 0.42±0.06 0.62±0.05 1.35±0.14 53,79% 30.35% 15,86% |
63.96±10.65 70.28±13.3 28.45±5.3 131 (90.3%) 17(11.7%) 0 1.70± 0.4 0.89±0.1 1.60±0.3 12.23±5.9) 209.17±119.86 --------------------------- 45.65 ± 16.2 19.56(15.68-23.46) 0.30 (0.19-0.47) 22.50±4.9 22.65 ± 12.37 0.89±0.13 0.70±0.11 0,86±0.13 0.40±0.06 0.63±0.08 1.26± 0.13) 26.21% 48,97% 24,83 |
<0.001 0.054 <0.001 <0.001 0.18 0.32 0.0417 <0.001 0.9464 ----------------------- <0.001 <0.001 <0.001 0.013 0.16 0.047 0.42 0.35 0.97 0.002 |
Table 2.
Clasificacion of patients with Differentiated Thyroid Cancer according to DXA and. TBS scores in the baseline study.
Table 2.
Clasificacion of patients with Differentiated Thyroid Cancer according to DXA and. TBS scores in the baseline study.
|
DXA T-Scores. |
TBS scores | Total | ||
| ≥1.350 (normal) |
1.200-1.350 (partially degraded) |
≤1.200 (degraded) |
||
| T score ≥1 SD (normal) |
43 (2.6) | 13 (8.9) | 6(4.1) | 62 (42.7) |
| T score <-1.0 and >-2.5 SD (osteopenia) |
29 (20) | 20 (13.7) | 10 (6.8) |
59 (40.6) |
| T score- ≤2.5 SD (osteoporosis) |
6 (4.1) | 12(8.3) | 6 (4.1) | 24 (16.5) |
| Total |
78 (53.7) | 45 (31) | 22(15.1) | 145 (100) |
Number of patients (% ). Chi-Square= 0.0057
Table 3.
Classification according to DXA and TBS scores in the end study after 12 years of follow-up. in patients with Differentiated Thyroid Cancer
Table 3.
Classification according to DXA and TBS scores in the end study after 12 years of follow-up. in patients with Differentiated Thyroid Cancer
|
DXA T-Scores. |
TBS scores | Total | ||
| ≥1.350 (normal) |
1.200-1.350 (partially degraded) |
≤1.200 (degraded) |
||
| T score ≥1 SD (normal) |
25 (17.2) | 16 (11.0) | 9 (6.2) 10 |
50(34.4%) |
| T score <-1.0 and >-2.5 SD (osteopenia) |
13 (8.9) | 38 (26.2) | 17(11.7) | 68 (46.8) |
| T score - ≤2.5) SD Osteoporosis |
0 (0) | 17 (11.7) | 10(6.9) 0 |
27 (18.6) |
| Total |
38 (26.2) | 71 (48.9) | 36(24.8) | 145(100) |
Number of patients (% ). Chi-Square= <,0001. The change rate was statistically significant:. Pearson chi-square =0.000
Table 4.
Differences in overall BMD and TBS outcome at the end study in the145 Differentiated Thyroid Cancers.
Table 4.
Differences in overall BMD and TBS outcome at the end study in the145 Differentiated Thyroid Cancers.
| Methods |
BMD <-2,5 SD osteoporosis |
BMD -1 - -2,5 SD osteopenia |
BMD >-1 SD normal |
||||||
| Initial Study |
End Study |
Difference | Initial Study |
End Study |
Difference | Initial Study |
End Study |
Difference |
|
| TBS (<1,2) degraded |
6 | 10 | -4 | 10 | 16 | -6 |
6 |
10 |
-4 |
| TBS (1,2-1,35) Partially degraded |
12 | 17 | -5 | 20 | 39 | -19 | 13 | 16 | -3 |
| TBS (>1,35) normal |
6 | 0 | 6 | 29 | 13 | 16 | 43 | 24 | 19 |
Number of patients. The change rate was statistically significant: Pearson Chi-square= 0.042
Table 5.
Comparison of patients with Differentiated Thyroid Cancer with and. without Vertebral Fractures at the end of the study.
Table 5.
Comparison of patients with Differentiated Thyroid Cancer with and. without Vertebral Fractures at the end of the study.
| Without Vertebral fractures |
With Vertebral fractures |
p | |
| Clinical and hormonal data | |||
| N | 115 | 30 | - |
| Age(years) | 52.0±11.5 | 50.3±13.5 | 0.50 |
| BMI | 26.6 (24.5-30.3) | 25.8 (22.8-28.7) | 0.32 |
| Menarchia (years) | 12.95 | 12.96 | 0.97 |
| Histology Papilar Follicular Others |
89 (85.%) 13 (11%) 4 (3.4%) |
29(96.6%) 1 (3.3%) 0 (0%) |
0.40 |
| TNM initial stage I II III IV |
81(71.8%) 15 (13.2%) 13(11.5%) 4 (3.54 |
18 (64.2) 4(14.2%) 6 (21.4%) 0 (0%) |
0.42 |
| Osteoporosis | 13/102 | 4/26 | 0.76 |
| Exercise (walking-minutes) | 55.00(30-60.00) | 30.00(30-45.00) | 0.043 |
| Milk ingestions (mg/day) | 500 (477.50-750) | 500 (250-750) | 0.29 |
| Smoking yes/no | 19/96 | 6/24 | 0.65 |
| Etanol ingestión yes/no | 1/114 | 0/30 | 0.61 |
| Radioactive iodine doses: mCi (range) | 150.00(126-250.000) | 150.00(100-150.00) | 0.042 |
| Serum Biochemical parameters | |||
| TSH (µU/ml) | 0.03 (0.03-0.15) | 0.10 (0.03-0.40) | 0.20 |
| T4L (ng/ml) | 1.64 (0.42) | 1.63 (0.45) | 0.87 |
| Tiroglobulin (ng/ml) | 0.20 (0.00-1.00) | 0.30 (0.00-1,20) | 0.67 |
| Calcium(mg/dl) | 9.26 (0.57) | 9.24 (0.50) | 0.89 |
| Phosphorus(mg/dl) | 3.40 (3.0-3.90) | 3.60 (3.3-4.o) | 0.15 |
| Creatinine(mg/ml) | 0.71 (0,53.0,83) | 0.75 (0.66-0.86) | 0.50 |
| PTH (pg/ml) | 32.4 (0.63-0.83) | 28.4 (24.5-40.6) | 0.45 |
| 2OHD (ng/ml) | 26.08 (17.0-33.4) | 28.2(22.2-33.6) | 0.37 |
| BAO (U/L) | 10.7 7(7,42-13.70) | 11.30(6.39.13.3) | 1.00 |
| Osteocalcin (ng/ml) | 7.08 (4,66-9.89) | 6.20 (3.74-9.2) | 0.30 |
| Densitometric parameters | |||
| L-BMD | 0.91±0,17 | 0.88±o,12 | 0.27 |
| FN-BMD | 0.75±0.14 | 0.72±0.12 | 0.56 |
| TH-BMD | 0.85±0.11 | 0.83±0.12 | 0.63 |
| UDR-BMD | 0.44±0.04 | 0.38±0.06 | 0.12 |
| 1/3RD-BMD | 0,63±0.5 | 0.65±0.5 | 0.72 |
| TBS Normal Partial degraded Degraded |
1.35±0.14 53.9% 29.8% 16.5% |
1.22±0.14 53.3% 33.3% 13.3% |
0.001 |
Table 6.
TBS and DXA scores in 30 Differentiated Thyroid Cancer patients with Vertebral Fractures.
| TBS | ||||
| Partial degraded | Degraded | Normal | Total | |
| DXA -2.5- -1 | 9 (30%) | 5 (16.7%) | 3 (10%) | 17 (56.7%) |
| <.2,5 | 3 (10%) | 0 | 0 | 3 (10%) |
| >-1 | 0 | 2(6.6%) | 8 (26.7%) | 10 (33.3%) |
| Total | 12(40%) | 7 (23.3%) | 11 (36.7%) | 30 (100%) |
Fisher´s Exact Test=0.0009
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



