
Submitted:
20 March 2024
Posted:
26 March 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Objective: To summarize the prevalence of PASC/Long COVID symptoms among the general population reported in published articles. This narrative review examined 21 PASC symptoms. Methods: A PubMed/manual search returned 114 articles on general PASC/Long COVID symptoms. Manuscripts were excluded if they were not research studies, didn’t report symptom prevalence, or used a pediatric population. Ninety-eight studies were selected for review and 59 met criteria for inclusion. Risk of bias was assessed with the Hoy critical appraisal tool. Results: After excluding studies with high risk of bias, meta-analysis of prevalence for 21 symptom categories ranged from 2.6-28.7% in studies based on surveys to 0.3%-7.1% in studies based on EHR data. Conclusions: PASC symptom studies are limited by variability in study design and representation of the general population. Further research is needed to effectively cluster symptoms in meaningful ways that enable focused treatment.
Keywords:
narrative review
; long COVID
; PASC
1. Introduction
1.1. Overview
It is now well-recognized that SARS-CoV-2 is associated with post-viral sequelae and these appear to be heterogeneous. The definition of post-acute sequela of SARS-CoV2 (PASC), or “Long COVID” by the lay public, is generally defined as new, recurrent, or continuous symptoms starting 3 to 4 weeks after SARS-CoV2 infection [1,2,3,4]. SARS-CoV2 has infected 671 million people world-wide as of February 2023 [5]. PASC has been reported in multiple studies from throughout the world, most of which have focused on individual symptom frequency; the primary goal of this narrative review is to summarize current literature on this topic focusing on reported prevalence of individual symptoms. Commonly reported symptoms are dyspnea, fatigue, pain, cognitive problems, and changes in or loss of smell or taste. It is likely that PASC is a heterogeneous set of syndromes, potentially with variable etiologies (e.g., initial organ injury from acute infection, viral persistence, immune dysregulation, autoimmunity, unrepaired tissue damage, dysbiosis of microbiome or virome) [6,7]. However, PASC could be a multi-system disease with a single underlying etiology. Moreover, it is possible that PASC has evolved over the course of the pandemic because of different viral strains, treatments, and vaccination rates.
1.2. Historical Perspective
Post-COVID sequela were first reported in small clinical follow-up studies published in mid to late 2020, soon after the initial wave of the COVID-19 pandemic, which were focused on post-hospital discharge cohorts. These publications were followed by outpatient studies that led to recognition that mild COVID cases could suffer from post-viral sequela. The Patient-Led Collaborative’s high impact manuscript on more than 200 symptoms, many of which were exacerbated by physical or mental exertion or stress, produced a paradigm shift with widespread media attention. Their presentation to the US Congress ultimately lead to $1.3B in funding to study post-acute sequelae of SARS-CoV-2 The NIH-funded Researching COVID to Enhance Recovery (RECOVER) Adult Cohort (RECOVER-Adult), a longitudinal cohort study of adults with and without SARS-CoV-2 infection across 85 recruitment sites in the US, includes acute onset COVID cases with data collected during the first 5-28 days post-infection and symptom surveys every 3 months. A primary goal of this initiative is to provide prospective data on symptom frequency and patterns over time, as well as impacts on quality of life and overall physical health. RECOVER has reported PASC prevalence of 10% among acute infected participants based on symptoms reported 6 months after infection [8]. Further deep phenotyping and testing among individuals with prolonged symptoms will enhance discovery of PASC etiology(ies).
1.3. Goal of Current Review
The goal of this narrative review was to identify and synthesize the PASC symptoms most commonly reported by patients in published scientific articles and provide data to future studies to aid in better defining PASC phenotypes. The current review examined the 21 most prevalent individual PASC symptoms reported by more than one study in the included total of 59 studies.
2. Materials and Methods
2.1. Article Search Strategy
The article search was conducted on PubMed and manual review of recent systematic reviews. The specific MeSH terms and query used in the PubMed search was as follows: (Long COVID[MeSH Major Topic]) OR (PASC[MeSH Major Topic]) AND symptoms. The PubMed database was searched at least thrice monthly from October 2022 through February 2023. As of February 2023, the search returned 111 potentially eligible papers.
2.2. Eligibility Criteria
Peer-reviewed studies were considered eligible if they included at least 30 individuals with laboratory confirmed and/or clinically diagnosed COVID-19. We included studies that reported symptoms or outcomes assessed at 3 or more weeks post COVID-19 onset. Articles were excluded if they were systematic or narrative reviews, book chapters, editorials, responses, case studies, research design descriptions, or focused on institutional topics such as research management. The remaining full texts were assessed and excluded if they were meta-analyses, assessed symptoms at less than 3 weeks post-infection, addressed only acute COVID-19 symptoms, symptom outcomes were relative to a specific disease in addition to COVID-19, focused on experimental treatments, did not report prevalence data, contained no symptom data, used a pediatric sample, or in one case, a mixed adult/pediatric sample for which results were not reported separately (Figure 1). See (Table 1) for a complete overview of study characteristics. Three other eligible studies were identified through review of references of other scientific articles.
2.3. PASC Symptom Categories
Symptoms were categorized into 25 different phenotypic bins in an a priori fashion based on symptoms assessed in the NIH-funded Researching COVID to Enhance Recovery (RECOVER) Adult Cohort (www.recovercovid.org), grouped by CTCAE (Common Terminology Criteria for Adverse Events) for the symptoms [9]. Any symptom that fell into one of the following categories was added to the review table (Supplemental Figure A): General symptoms included fatigue, fever, chills, sweats or flushing, post-exertional malaise; cardiac symptoms included general cardiac symptoms such as tachycardia and chest pain; respiratory symptoms included cough, shortness of breath, sleep problems; neurologic symptoms included problems thinking or concentrating, dizziness, headache, nerve problems (tremor, shaking, abnormal movements, numbness, tingling, burning, can’t move part of body, seizures), and loss of or changes in smell or taste; psychiatric symptoms include mental health concerns such as depression, and anxiety; musculoskeletal symptoms included joint or muscle pain, weakness in arms or legs; gastrointestinal (GI) symptoms included abdominal pain and/or feeling full or vomiting after eating, diarrhea, constipation weight loss, dry mouth; metabolic symptoms included excessive thirst; urinary problems included incontinence, trouble passing urine or emptying bladder); dermatologic symptoms included hair loss, skin rash, hair loss; ear symptoms included hearing problems; eye symptoms included vision problems. Two symptoms, swelling of the legs and changes in skin coloration, were not reported in the top 25 symptoms of the 59 reviewed papers and were thus left out of further analyses. Two additional symptoms, dry mouth and excessive thirst, were reported in only one study. Therefore, this review used an end total of 21 phenotypic categories.
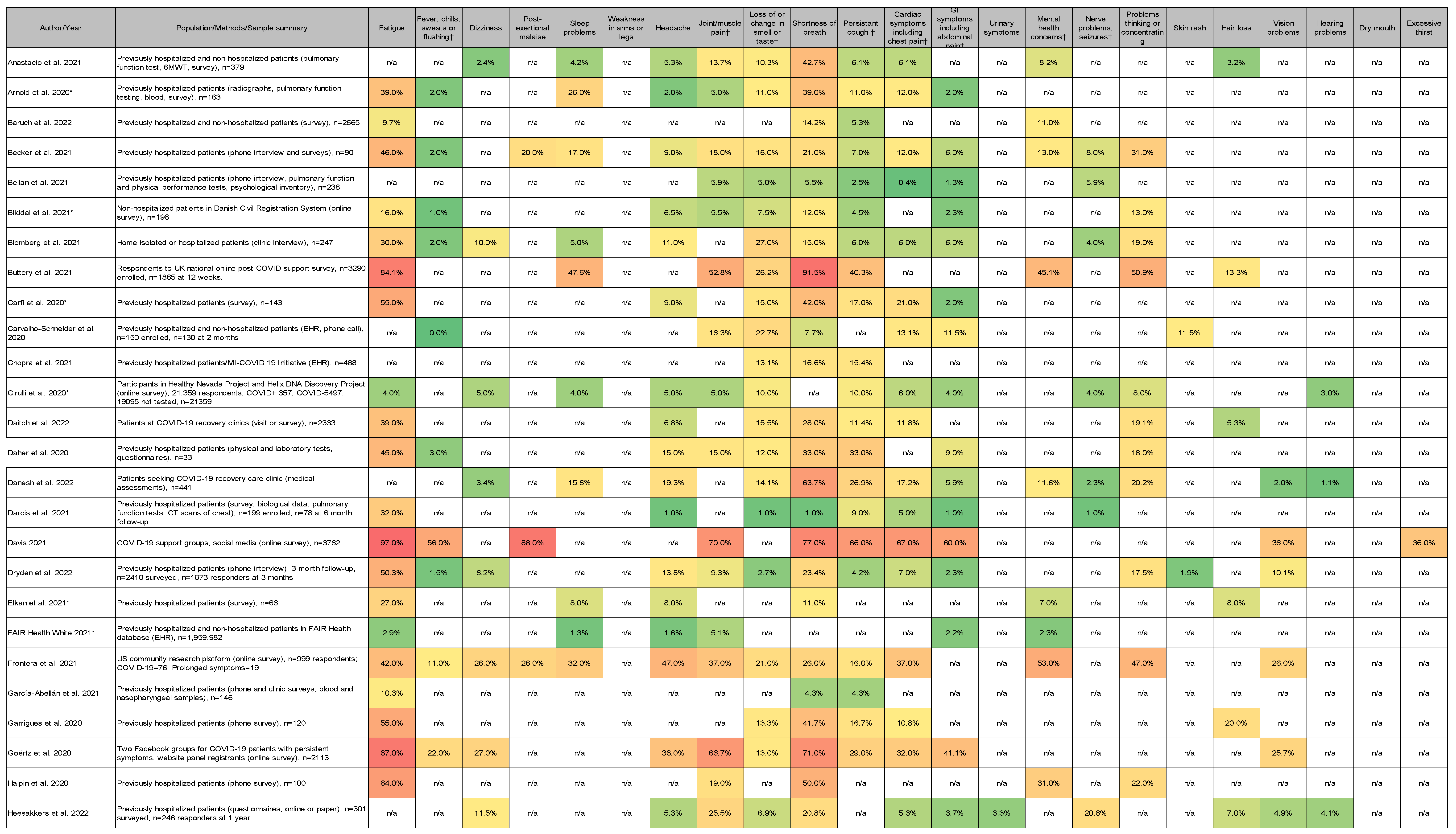
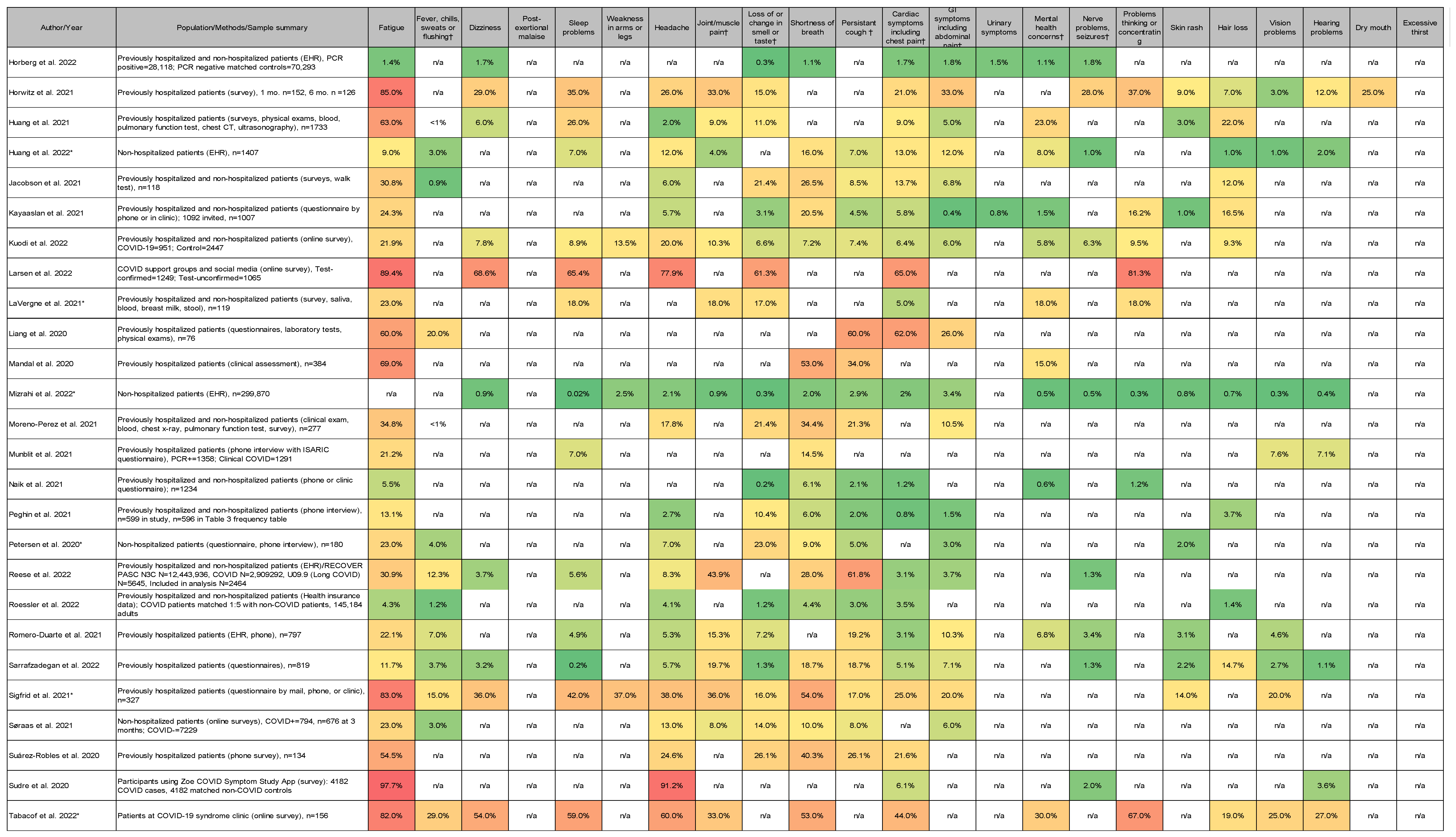
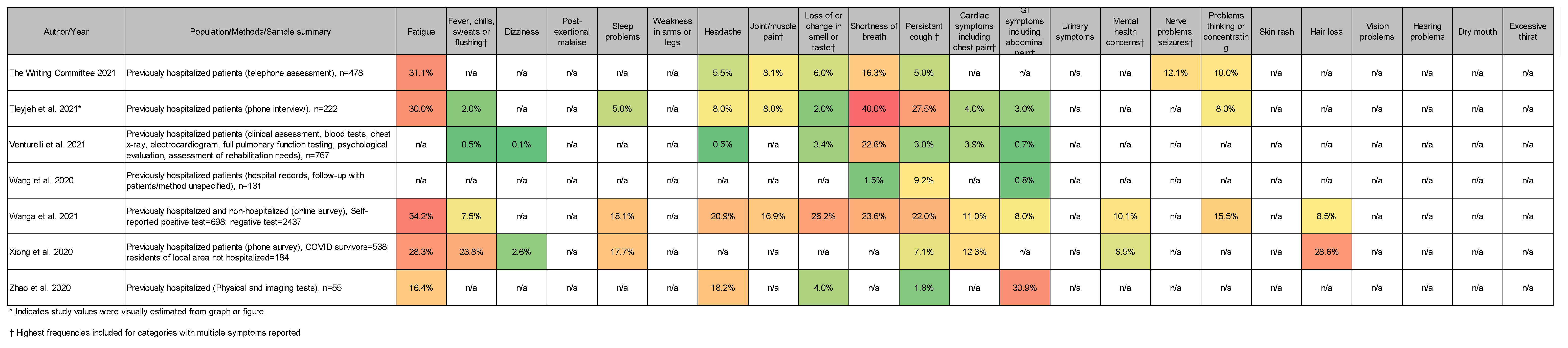
2.4. PASC Symptom Reporting
The methods used to evaluate and measure PASC symptoms were heterogeneous across the 59 studies reviewed that reported individual symptoms as prevalence (n=59). To be exhaustive in our representation of symptom data, all methods with numerical values were included and like data were grouped when possible (Table 2).
2.5. Risk of Bias Assessment
The included studies were assessed for risk of bias using the Hoy et al. [10] critical appraisal tool for prevalence studies. The critical appraisal checklist for studies reporting prevalence consists of nine topics: (a) target population representativeness (b) sample frame suitability, (c) sampling method appropriateness, (d) likelihood of non-response bias (e) direct data collection from subjects, (f) usage of valid methods for identification of the condition, (g) use of valid, reliable study instrument to measure parameter of interest (h) same mode of data collection for all subjects, and (i) adequate response rate. Each study was assessed across each of these areas, with results reported as Yes, No, or Unclear. Studies were assigned an overall score, reflecting the number of questions with a Yes response.
2.6. Statistical Methods
Sample sizes and populations in each paper are summarized in (Table 1). Frequencies were summarized across studies using random-effects meta-analyses. Where available, exact number of events and total number of respondents for each symptom was included in the meta-analyses For studies that only report proportions, number of events were estimated by multiplying number of respondents by proportion with event and rounding up. Studies were grouped in three ways, by type of study (EHR, survey, Long Covid), risk of bias (low, medium, high) and hospitalization of respondents (hospitalized only versus non-hospitalized and mixed). Comparisons of proportion within each symptom category were done using a fixed-effects model using the “metafor” package in R (Supplemental Figure B) [11]. All analyses were performed using R.
3. Results
3.1. Population Characteristics
The global population was surveyed thanks in part to authors’ efforts to include COVID support groups and social media groups in an online survey across 34 countries [12]. Study populations were reported from around the world including the USA, UK, Italy, Malta, South Africa, Netherlands, Belgium, China, Turkey, Switzerland, Denmark, Norway, France, Israel, Spain, Germany, Belgium, Russia, India, Faroe Islands, Iran, and Saudi Arabia. Twenty-one of the studies included had a COVID-19 patient sample size >950, with the largest sample at nearly 2 million [13]. The most common reasons for patients to be excluded from analyses were incomplete follow-up data, cognitive or neuropsychiatric conditions that prevented participation, death, current COVID-19 infection, and chronic or severe illness unrelated to/predating the COVID infection (Table 1).
3.2. Study Designs and Case Definitions
Study designs varied in the reviewed papers and included cohort (prospective, retrospective, and longitudinal), COVID case-uninfected control, cross-sectional, case series, and diverse combinations thereof. Many studies required clinical diagnosis via laboratory confirmation of a past COVID-19 infection such as a positive PCR-test. However, we also included survey studies that relied on self-reports of COVID-19 infection. Control groups were not commonly present (n=8/59 or 14% of reviewed studies included controls) but usually identified patients as COVID negative via formal laboratory testing, although self-reports of negative infection status were sometime used for inclusion (Table 1).
3.3. Definitions of PASC
Definitions varied for PASC in terms of length of time necessary for symptoms to persist or emerge. The lower ends of post-infection follow-up times started at just over 3 weeks [14,15]. Remaining studies investigated symptoms from 30+ days onward, even up to 1 year after the initial COVID-19 infection, hospital admission, or hospital discharge (Table 1). Several studies also utilized multiple time points for comparison [15,16,17,18,19,20,21,22,23,24,25,26,27]. Definitions of symptom-based phenotypes were also diverse across studies. Most included symptom checklists without assessment of PASC symptom severity.
3.4. Most Common Symptoms Reported across 59 Studies
Due to the focus on utility in this review, article symptom lists were capped at 25 with priority given to the most common symptoms [8]. Of note, a handful of studies reported highly comprehensive lists of PASC symptoms at 39 [13], 58 [28], 68 [21], and 203 [29]. The general symptoms that patients experienced most often, and that were reported by at least two of the studies reviewed, were: respiratory problems such as shortness of breath, fatigue, pain of various kinds, cognitive problems such as brain fog, changes in or loss of smell or taste, weakness, mental health issues such as anxiety and depression, cardiac symptoms such as palpitations or chest pain, hair loss, fever/chills, sleep problems, gastrointestinal symptoms, and flu-like symptoms. Symptoms reported by patients but not repeatedly captured in the selected studies included hyperlipidemia, post-exertional malaise, worse performance at usual activities, neurological disorders and unintentional weight loss (Supplemental Figure C).
3.5. Data Collection Methods
Three studies utilized electronic health records (EHR) to create comprehensive data sets of COVID cases and uninfected controls [19,30,31]. Three used EHR data on COVID cases only [13,20,32]. Four studies conducted national or community surveys among self-reported COVID test positive cases and COVID test negative controls [18,33,34,35]. One study utilized a COVID Symptom Study app, for which 4,223,955 adults registered from the UK (88.2%), US (7.3%), and Sweden (4.5%); in this study, a small subset (<0.1%) reported prospective data on symptoms after 28 days [27]. Seven studies were limited to populations with reported Long COVID symptoms. Four studies conducted surveys using social media and online outreach to support groups for individuals with post-COVID symptoms [12,14,18,29]. Two studies surveyed patients visiting local clinics for Long COVID symptoms [28,36]. One study relied on EHR data and used the Long COVID ICD-10 code to identify the cohort [37].
Davis and colleagues from the Patient-Led Research Collaborative conducted an online survey that was distributed via COVID-19 support groups and social media to patients from 56 countries with symptoms lasting >28 days, and onset prior to June 2020 [29]. They estimated the prevalence of 203 symptoms among 3762 respondents. The most common symptoms were fatigue, post-exertional malaise, and cognitive dysfunction, with 85.9% of participants experiencing relapses triggered by physical or mental activity, and stress. Buttery et. al. studied survey responses from a UK online post-COVID-19 support and information hub, completed ≥4 weeks after onset of symptoms [18]. Goertz et al. studied 21,113 members of Facebook groups for COVID patients with persistent symptoms in The Netherlands and Belgium [14]. Larsen et. al. studied an online survey of 2,314 adults with PASC recruited through long COVID support groups and social media channels between October 2020 and August 2021 for 53 symptoms including autonomic symptoms assessed with COMPASS-31 [12]. Tabacof et al. conducted a survey of 156 patients attending Mount Sinai’s PASC clinic [36]. Danesh et al. conducted interviews of 441 patients from an integrated health system multispecialty telemedicine-based consultation service for post-COVID patients [28].
Multiple studies conducted post-discharge surveys by telephone or email with COVID infected inpatients who were recently hospitalized [15,16,17,21,22,23,24,25,26,36,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67]. Five of these studies also included either follow-up surveys [22,56] or EHR data [19,31,37] from hospitalized and non-hospitalized COVID patients, while three studies focused only on non-hospitalized COVID patients using surveys [52,60] or EHR data [30]. For this review and meta-anaylsis, we limited the data extracted from manuscripts to PASC symptoms.
We classified study design into 3 categories: 1) “EHR” studies that included data on COVID cases and/or uninfected controls; 2) “Survey” studies of general population groups, COVID patients post-hospitalization/or post-outpatient infections; and 3) “Long COVID” survey studies of patients attending Long COVID clinics or that used social media and outreach to survey Long COVID support groups, or EHR data on COVID cases specifically using Long COVID ICD-10 codes.
The denominator for calculating frequency varied and was based on the specific population studied. For example, the population included for symptom frequency in Long COVID studies were limited to people with PASC symptoms, patients seen in long COVID clinics, or patients with Long COVID ICD-10 codes in EHR [12,14,18,29,36,37], whereas studies classified as “Survey” aimed to assess frequency among populations that included people with no PASC symptoms at all. For the 59 studies that reported prevalence, averaged PASC symptom frequencies for 21 of the phenotypic symptom categories are presented in (Figure 2), stratified into Long COVID, Survey, and EHR groups. Two symptoms, dry mouth and excessive thirst, were reported in one study each and were excluded from the meta-analyses; thus 21 symptoms were included in the final meta-analyses. Marked differences were observed in symptom prevalence across the three different study design groups (Long COVID (n=7), EHR (n=6), Survey (n=46), (Figure 2) where the highest frequencies were observed in studies that only included respondents with Long COVID symptoms [12,14,18,29], patients seen at Long COVID clinics [28,36], or with EHR Codes for Long COVID [37]. Across studies stratified by risk of bias (Figure 3), eleven categories were reported across all groups (fatigue, fever/sweats, dizziness, sleep problems, headache, joint/muscle pain, loss of or change in smell or taste, shortness of breath, persistent cough, cardiac symptoms, GI symptoms, mental health concerns, nerve problems, problems thinking or concentrating, hair loss, hearing problems). These symptoms were among the most commonly reported across studies as noted in (Supplemental Figure C).
3.6. Risk of Bias Comparisons
Using the Hoy [10] critical appraisal tool, 25 studies were classified as high risk of bias, 19 as moderate risk of bias, 15 as low risk of bias. Comparing symptom prevalence across three risk of bias categories demonstrated differences in results across high risk of bias studies (largest difference seen for fatigue, post exertional malaise, cardiac symptoms including chest pain, persistent cough, problems thinking or concentrating, dizziness, headache, mental health concerns, joint or muscle pain) with less variation comparing moderate risk of bias studies to low risk of bias studies. The highest variation between studies was seen in the high risk of bias studies (Figure 3). High risk of bias studies included those with small sample size that did not reflect the general population characteristics in a country, studies with low response rates suggesting selection bias, and studies without general population data on symptom prevalence. Since the primary goal of this meta-analysis was to summarize the prevalence of PASC symptoms among the general population, all Long COVID studies were classified as high risk of bias.
3.7. Low-to Moderate Risk fo Bias, EHR Versus Survey Collection
Among the low- and moderate-risk of bias studies, PASC symptoms were compared between the EHR and survey studies (Figure 4a). Twenty-seven studies were classified as surveys, while five were classified as EHR studies. A higher prevalence was recorded across 20 of 21 symptoms when evaluated with the survey compared to that of the EHR. Eight of those symptoms were found to have a statistically significant difference including fatigue, problems thinking of concentrating, and weakness in arms or legs. The prevalence across the two study designs were relatively similar for certain symptoms including cardiac/chest pain, GI/abdominal pain, and persistent cough.
3.8. Low-to Moderate Risk of Bias, Hospitalized Versus Hospitalized and Non-Hospitalized among Survey Studies
Among the low- and moderate-risk of bias survey studies, PASC symptoms were then compared between studies including patients who were hospitalized at the time of the incident COVID-19 event versus studies from non-hospitalized patients, and mixed studies of hospitalized and non-hospitalized patients. Sixteen studies were from patients exclusively hospitalized with COVID-19 versus 11 studies that were from a non-hospitalized and mixed studies. 20 of 21 PASC symptoms had a higher prevalence among the hospitalized group. Only dizziness had a higher prevalence among the non-hospitalized and mixed studies (Figure 4b). Four of the symptoms were found to have a statisically significant difference. See (Supplemental Figure D) for a visual summary of meta-analysis groupings.
4. Discussion
In 59 studies of symptoms lasting more than 3 weeks after acute COVID infection, we found wide ranges of symptom frequencies, variable categories of symptoms included, and marked variation in study design. Most studies to date have focused largely on individual symptom prevalence but are limited by lack of controls and retrospective data. The current review examined the most prevalent PASC symptoms in 59 scientific articles as fitted to a 21-symptom phenotype grid. Individual symptom prevalence varied widely depending on study design with lower prevalence in studies based on EHR to moderate prevalence through surveys conducted by outreach to general population samples, infected inpatients after hospital discharge, or mixed studies of hospitalized and non-hospitalized outpatients to highest symptom prevalence reported from surveys on recorded in the EHR of individuals with suspected Long COVID. After excluding studies with high risk of bias, meta-analysis of symptom prevalence for 21 symptom categories ranged widely from 2.6-28.7% in studies based on surveys to 0.3%-7.1% in studies based on EHRs. The challenges with varied study design include potential biases resulting in under-ascertainment of symptoms in EHR studies to including symptom frequencies only among individuals with suspected Long COVID that do not reflect general population prevalence.
EHR studies demonstrated the lowest prevalence rates for PASC symptoms, shortness of breath, fatigue, pain, cognitive problems, changes in smell and/or taste compared to other methods with some symptoms not available in EHR data. The challenges in survey design include assuring a representative sample of the general population. Many of the studies that surveyed hospitalized patients or mixed hospitalized and non-hospitalized outpatients used smaller populations and were classified as high risk of bias. Some large studies that surveyed general population samples with low response rates, thus raising the issue of representativeness of responders, were also rated as high risk of bias. For studies that assessed symptoms only among individuals with suspected Long COVID (Long COVID clinics, diagnosis code, Long COVID support groups/social media), prevalence data demonstrates much higher symptom rates The most striking of these are post-exertional malaise (88%) and fatigue (80%), followed by shortness of breath (55%), cognitive problems (53%), changes in smell and/or taste (26%), joint/muscle pain (42%), and fever/chills/sweats (36%), illustrating the burden of symptoms among people with Long COVID symptoms.
Differences in data collection methods across the studies can affect how prevalence is reported. Potential biases in symptom assessment in EHR data include absence of diagnosis codes for many symptoms, incomplete symptom assessment or documentation by providers, potential limited access to care by vulnerable patients, and lack of full data on individuals who receive care outside the EHR system. Many of these limitations could result in underestimates of symptom prevalence. This may contribute to the lower frequencies reported in EHR studies. Conversely, survey studies could be impacted by response bias whereby symptomatic individuals are more likely to respond than asymptomatic individuals. Surveys among individuals seeking resources for Long COVID, such as in specialty clinics or social media support groups, are most likely to exhibit selection bias. The very high prevalence among support groups and Long COVID clinics implies that their symptoms may have been more likely to be severe or disruptive to their quality of life. Nevertheless, symptom prevalence data amongst the moderate and low risk of bias studies supports substantial prevalence of symptoms across a wide array of organ systems and suggests that PASC/Long COVID is a multi-system disorder.
While EHR and survey studies each can have their own biases, this meta-analysis identifies which of the PASC symptoms have similar measurements between study designs. For example, chest pain, GI pain, and persistent cough were all detected with similar prevalence in the EHR and survey studies. This would suggest that future PASC studies that use EHR should expect the prevalence of these specific symptoms to be more accurate. However, the prevalence of fatigue, post-exertional malaise, and weakness in arms and legs were significantly different between the EHR and the survey studies. Therefore, these symptoms may not be as reliably measured. Given that collecting prospective or retrospective data from EHR’s can be easier and less expensive than setting up a survey study, future PASC studies could rely on the EHR to track symptoms such as chest pain and gastrointestinal discomfort in PASC. However, they should consider alternative ways to measure symptoms like fatigue and post-exertional malaise.
In addition, it has already been observed that a longer recovery course is expected in patients requiring hospitalization or prolonged stays in the hospital [41,45,68]. While this meta-analysis validates increased prevalence of PASC among hospitalized patients, it provides further insight into exactly how these differences manifest across the various PASC symptoms. Interestingly, for certain symptoms such as headaches, nerve problems/seizures, and changes in smell, no statistically significant difference was observed between the two cohorts. While these data suggest the severity of the acute COVID-19 episode may directly lead to increased prevalence of fatigue, weakness, and shortness of breath in the subsequent recovery phase, an alternative mechanism (auto-immune response, persistent viral reservoir) may explain why that difference is not as significant for PASC symptoms like headache and changes in smell. These findings may also prepare health care providers for what to expect with patients depending on their acute COVID-19 level of severity.
Other limitations to the published studies include incomplete symptom lists in some studies and lack of control groups to assess frequency of symptoms in a representative uninfected group. Many of these PASC symptoms, taken individually, are non-specific, prevalent in the population, vary widely, and overlap with many other conditions. The heterogeneity of symptoms suggests that PASC is a set of syndromes with variable etiologies [6,7]. Because of the substantial short- and long-term effects of PASC, including impacts on quality of life, healthcare costs, and economic productivity [69], it is imperative to better characterize PASC, and PASC sub-phenotypes, in a prospective design with uniform data collection from a diverse group of uninfected and infected participants as the RECOVER Initiative intends to do.
We acknowledge that PASC symptoms—especially considering the introduction of vaccinations, virus variants, and pre-existing conditions—are difficult to fully capture and describe. A comprehensive overview of symptom phenotypes was attempted in this review, however, 200+ symptoms have been reported post-COVID. Knowledge of PASC is still evolving. Another challenge in this review was reliability of self-reports compared to EHR, for example, and wide variation in the quality of symptom reporting. Occasionally, values had to be visually estimated from graphs and figures when exact numbers were not provided. We have attempted to summarize extant research in a way that is helpful for clinicians, the patient community, and researchers alike while keeping these caveats in mind.
The striking variability in symptom prevalence across studies of PASC/Long COVID illustrates the challenge with defining criteria for this novel, multi-system condition. Studies to date have focused largely on individual symptom prevalence but some are limited by lack of controls, small sample size, potentially biased study designs. Symptom prevalence ranges widely, with lowest prevalence in EHR studies and higher prevalence in Survey studies, as illustrated by a range of 1-8% in EHR studies versus 2-28% in Survey studies in the low to moderate risk of bias studies. When limiting the study population to only participants who report Long COVID, the prevalence is much higher, reflecting a change in the denominator for prevalence calculations and a different study question, namely: “what is the prevalence of symptoms among participants who have any long term symptoms after SARS-CoV-2 infection?” rather than “what is the prevalence among a population infected with SARS-CoV-2”. The challenges are that many of these symptoms, taken individually, can be common in the population regardless of COVID infection. PASC symptoms are also heterogeneous and overlap with many other conditions. Major questions remain about the effect of vaccination status, the role of viral variants, the role of COVID therapies, comorbidities, social determinants of health, and clinical risk factors on the development of PASC/Long COVID to enable studies on the underlying pathobiology of individual symptoms and clusters of symptoms. Further research into PASC phenotypes is needed to effectively cluster symptoms in meaningful ways that enable focused pathobiology studies and clinical trials.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: A. Symptom Categories; Figure S2: Meta Analysis; Figure S3: Top 3 Most Prevalent Symptoms (n = 59 studies); Figure S4: Meta-Analysis Categories.
Author Contributions
All authors contributed equally to this work. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by National Heart Lung and Blood Institute, grant number 1OT2HL161841.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Michelen M, Manoharan L, Elkheir N, et al. Characterising long COVID: a living systematic review. BMJ Glob Health 2021;6(9). [CrossRef]
- Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nat Med 2021;27(4):601-615. [CrossRef]
- Crook H, Raza S, Nowell J, Young M, Edison P. Long covid-mechanisms, risk factors, and management. BMJ 2021;374:n1648. [CrossRef]
- Greenhalgh T, Knight M, A’Court C, Buxton M, Husain L. Management of post-acute covid-19 in primary care. BMJ 2020;370:m3026. [CrossRef]
- OWID. Our World in Data. (ourworldindata.org).
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 2023;21(3):133-146. [CrossRef]
- Merad M, Blish CA, Sallusto F, Iwasaki A. The immunology and immunopathology of COVID-19. Science 2022;375(6585):1122-1127. [CrossRef]
- Thaweethai T, Jolley SE, Karlson EW, et al. Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection. JAMA 2023;329(22):1934-1946. [CrossRef]
- CTEP. Common Terminology Criteria for Adverse Events NIH National Cancer Institute, DCTD Division of ZCancer Treatment & Diagnosis 2021 (https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_60).
- Hoy D, Brooks P, Woolf A, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol 2012;65(9):934-9. [CrossRef]
- Borenstein M, Higgins JP. Meta-analysis and subgroups. Prev Sci 2013;14(2):134-43. [CrossRef]
- Larsen NW, Stiles LE, Shaik R, et al. Characterization of autonomic symptom burden in long COVID: A global survey of 2,314 adults. Front Neurol 2022;13:1012668. (In eng). [CrossRef]
- 13. FAIR H. A detail study of patients with long-haul COVID: An analysis of Private Healthcare Claims. A FAIR Health White Paper: 2021.
- Goërtz YMJ, Van Herck M, Delbressine JM, et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: the post-COVID-19 syndrome? ERJ Open Res 2020;6(4) (In eng). [CrossRef]
- Wang X, Xu H, Jiang H, et al. Clinical features and outcomes of discharged coronavirus disease 2019 patients: a prospective cohort study. QJM 2020;113(9):657-665. (In eng). [CrossRef]
- Bliddal S, Banasik K, Pedersen OB, et al. Acute and persistent symptoms in non-hospitalized PCR-confirmed COVID-19 patients. Sci Rep 2021;11(1):13153. (In eng). [CrossRef]
- Blomberg B, Mohn KG, Brokstad KA, et al. Long COVID in a prospective cohort of home-isolated patients. Nat Med 2021;27(9):1607-1613. (In eng). [CrossRef]
- Buttery S, Philip KEJ, Williams P, et al. Patient symptoms and experience following COVID-19: results from a UK-wide survey. BMJ Open Respir Res 2021;8(1) (In eng). [CrossRef]
- Horberg MA, Watson E, Bhatia M, et al. Post-acute sequelae of SARS-CoV-2 with clinical condition definitions and comparison in a matched cohort. Nat Commun 2022;13(1):5822. (In eng). [CrossRef]
- Huang Y, Pinto MD, Borelli JL, et al. COVID Symptoms, Symptom Clusters, and Predictors for Becoming a Long-Hauler Looking for Clarity in the Haze of the Pandemic. Clin Nurs Res 2022;31(8):1390-1398. (In eng). [CrossRef]
- LaVergne SM, Stromberg S, Baxter BA, et al. A longitudinal SARS-CoV-2 biorepository for COVID-19 survivors with and without post-acute sequelae. BMC Infect Dis 2021;21(1):677. (In eng). [CrossRef]
- Naik S, Haldar SN, Soneja M, et al. Post COVID-19 sequelae: A prospective observational study from Northern India. Drug Discov Ther 2021;15(5):254-260. (In eng). [CrossRef]
- García-Abellán J, Padilla S, Fernández-González M, et al. Antibody Response to SARS-CoV-2 is Associated with Long-term Clinical Outcome in Patients with COVID-19: a Longitudinal Study. J Clin Immunol 2021;41(7):1490-1501. (In eng). [CrossRef]
- Horwitz LI, Garry K, Prete AM, et al. Six-Month Outcomes in Patients Hospitalized with Severe COVID-19. J Gen Intern Med 2021;36(12):3772-3777. (In eng). [CrossRef]
- Darcis G, Bouquegneau A, Maes N, et al. Long-term clinical follow-up of patients suffering from moderate-to-severe COVID-19 infection: a monocentric prospective observational cohort study. Int J Infect Dis 2021;109:209-216. (In eng). [CrossRef]
- Becker C, Beck K, Zumbrunn S, et al. Long COVID 1 year after hospitalisation for COVID-19: a prospective bicentric cohort study. Swiss Med Wkly 2021;151:w30091. (In eng). [CrossRef]
- Sudre CH, Murray B, Varsavsky T, et al. Attributes and predictors of long COVID. Nat Med 2021;27(4):626-631. (In eng). [CrossRef]
- Danesh V, Arroliga AC, Bourgeois JA, et al. Symptom Clusters Seen in Adult COVID-19 Recovery Clinic Care Seekers. J Gen Intern Med 2023;38(2):442-449. (In eng). [CrossRef]
- Davis HE, Assaf GS, McCorkell L, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021;38:101019. (In eng). [CrossRef]
- Mizrahi B, Sudry T, Flaks-Manov N, et al. Long covid outcomes at one year after mild SARS-CoV-2 infection: nationwide cohort study. BMJ 2023;380:e072529. (In eng). [CrossRef]
- Roessler M, Tesch F, Batram M, et al. Post-COVID-19-associated morbidity in children, adolescents, and adults: A matched cohort study including more than 157,000 individuals with COVID-19 in Germany. PLoS Med 2022;19(11):e1004122. (In eng). [CrossRef]
- Chopra V, Flanders SA, O’Malley M, Malani AN, Prescott HC. Sixty-Day Outcomes Among Patients Hospitalized With COVID-19. Ann Intern Med 2021;174(4):576-578. (In eng). [CrossRef]
- Frontera JA, Lewis A, Melmed K, et al. Prevalence and Predictors of Prolonged Cognitive and Psychological Symptoms Following COVID-19 in the United States. Front Aging Neurosci 2021;13:690383. (In eng). [CrossRef]
- Cirulli E, KM SB, Riffle S, et al. Long-term COVID_19 symptoms in large unselected population. BMJ Yale [Preprint]2020.
- Wanga V, Chevinsky JR, Dimitrov LV, et al. Long-Term Symptoms Among Adults Tested for SARS-CoV-2 - United States, January 2020-April 2021. MMWR Morb Mortal Wkly Rep 2021;70(36):1235-1241. (In eng). [CrossRef]
- Tabacof L, Tosto-Mancuso J, Wood J, et al. Post-acute COVID-19 Syndrome Negatively Impacts Physical Function, Cognitive Function, Health-Related Quality of Life, and Participation. Am J Phys Med Rehabil 2022;101(1):48-52. (In eng). [CrossRef]
- Reese JT, Blau H, Casiraghi E, et al. Generalisable long COVID subtypes: findings from the NIH N3C and RECOVER programmes. EBioMedicine 2023;87:104413. (In eng). [CrossRef]
- Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 2021;397(10270):220-232. (In eng). [CrossRef]
- Kuodi P, Gorelik Y, Zayyad H, et al. Association between BNT162b2 vaccination and reported incidence of post-COVID-19 symptoms: cross-sectional study 2020-21, Israel. NPJ Vaccines 2022;7(1):101. (In eng). [CrossRef]
- Garrigues E, Janvier P, Kherabi Y, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect 2020;81(6):e4-e6. (In eng). [CrossRef]
- Halpin SJ, McIvor C, Whyatt G, et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J Med Virol 2021;93(2):1013-1022. (In eng). [CrossRef]
- Daher A, Balfanz P, Cornelissen C, et al. Follow up of patients with severe coronavirus disease 2019 (COVID-19): Pulmonary and extrapulmonary disease sequelae. Respir Med 2020;174:106197. (In eng). [CrossRef]
- Arnold DT, Hamilton FW, Milne A, et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: results from a prospective UK cohort. Thorax 2021;76(4):399-401. (In eng). [CrossRef]
- Bellan M, Soddu D, Balbo PE, et al. Respiratory and Psychophysical Sequelae Among Patients With COVID-19 Four Months After Hospital Discharge. JAMA Netw Open 2021;4(1):e2036142. (In eng). [CrossRef]
- Carfì A, Bernabei R, Landi F, Group GAC-P-ACS. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020;324(6):603-605. (In eng). [CrossRef]
- Liang L, Yang B, Jiang N, et al. Three-month Follow-up Study of Survivors of Coronavirus Disease 2019 after Discharge. J Korean Med Sci 2020;35(47):e418. (In eng). [CrossRef]
- Moreno-Pérez O, Merino E, Leon-Ramirez JM, et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J Infect 2021;82(3):378-383. (In eng). [CrossRef]
- Morin L, Savale L, Pham T, et al. Four-Month Clinical Status of a Cohort of Patients After Hospitalization for COVID-19. JAMA 2021;325(15):1525-1534. (In eng). [CrossRef]
- Zhao YM, Shang YM, Song WB, et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine 2020;25:100463. (In eng). [CrossRef]
- Munblit D, Bobkova P, Spiridonova E, et al. Incidence and risk factors for persistent symptoms in adults previously hospitalized for COVID-19. Clin Exp Allergy 2021;51(9):1107-1120. (In eng). [CrossRef]
- Sarrafzadegan N, Mohammadifard N, Javanmard SH, et al. Isfahan COVID cohort study: Rationale, methodology, and initial results. J Res Med Sci 2022;27:65. (In eng). [CrossRef]
- Petersen MS, Kristiansen MF, Hanusson KD, et al. Long COVID in the Faroe Islands: A Longitudinal Study Among Nonhospitalized Patients. Clin Infect Dis 2021;73(11):e4058-e4063. (In eng). [CrossRef]
- Xiong Q, Xu M, Li J, et al. Clinical sequelae of COVID-19 survivors in Wuhan, China: a single-centre longitudinal study. Clin Microbiol Infect 2021;27(1):89-95. (In eng). [CrossRef]
- Dryden M, Mudara C, Vika C, et al. Post-COVID-19 condition 3 months after hospitalisation with SARS-CoV-2 in South Africa: a prospective cohort study. Lancet Glob Health 2022;10(9):e1247-e1256. (In eng). [CrossRef]
- Kayaaslan B, Eser F, Kalem AK, et al. Post-COVID syndrome: A single-center questionnaire study on 1007 participants recovered from COVID-19. J Med Virol 2021;93(12):6566-6574. (In eng). [CrossRef]
- Peghin M, Palese A, Venturini M, et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin Microbiol Infect 2021;27(10):1507-1513. (In eng). [CrossRef]
- Venturelli S, Benatti SV, Casati M, et al. Surviving COVID-19 in Bergamo province: a post-acute outpatient re-evaluation. Epidemiol Infect 2021;149:e32. (In eng). [CrossRef]
- Anastasio F, Barbuto S, Scarnecchia E, et al. Medium-term impact of COVID-19 on pulmonary function, functional capacity and quality of life. Eur Respir J 2021;58(3) (In eng). [CrossRef]
- Sigfrid L, Drake TM, Pauley E, et al. Long Covid in adults discharged from UK hospitals after Covid-19: A prospective, multicentre cohort study using the ISARIC WHO Clinical Characterisation Protocol. Lancet Reg Health Eur 2021;8:100186. (In eng). [CrossRef]
- Søraas A, Kalleberg KT, Dahl JA, et al. Persisting symptoms three to eight months after non-hospitalized COVID-19, a prospective cohort study. PLoS One 2021;16(8):e0256142. (In eng). [CrossRef]
- Heesakkers H, van der Hoeven JG, Corsten S, et al. Clinical Outcomes Among Patients With 1-Year Survival Following Intensive Care Unit Treatment for COVID-19. JAMA 2022;327(6):559-565. (In eng). [CrossRef]
- Tleyjeh IM, Saddik B, AlSwaidan N, et al. Prevalence and predictors of Post-Acute COVID-19 Syndrome (PACS) after hospital discharge: A cohort study with 4 months median follow-up. PLoS One 2021;16(12):e0260568. (In eng). [CrossRef]
- Mandal S, Barnett J, Brill SE, et al. ‘Long-COVID’: a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2021;76(4):396-398. (In eng). [CrossRef]
- Suárez-Robles M, Iguaran-Bermúdez MDR, García-Klepizg JL, Lorenzo-Villalba N, Méndez-Bailón M. Ninety days post-hospitalization evaluation of residual COVID-19 symptoms through a phone call check list. Pan Afr Med J 2020;37:289. (In eng). [CrossRef]
- Jacobson KB, Rao M, Bonilla H, et al. Patients With Uncomplicated Coronavirus Disease 2019 (COVID-19) Have Long-Term Persistent Symptoms and Functional Impairment Similar to Patients with Severe COVID-19: A Cautionary Tale During a Global Pandemic. Clin Infect Dis 2021;73(3):e826-e829. (In eng). [CrossRef]
- Elkan M, Dvir A, Zaidenstein R, et al. Patient-Reported Outcome Measures After Hospitalization During the COVID-19 Pandemic: A Survey Among COVID-19 and Non-COVID-19 Patients. Int J Gen Med 2021;14:4829-4836. (In eng). [CrossRef]
- Baruch J, Zahra C, Cardona T, Melillo T. National long COVID impact and risk factors. Public Health 2022;213:177-180. (In eng). [CrossRef]
- Barman MP, Rahman T, Bora K, Borgohain C. COVID-19 pandemic and its recovery time of patients in India: A pilot study. Diabetes Metab Syndr 2020;14(5):1205-1211. [CrossRef]
- Groff D, Sun A, Ssentongo AE, et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw Open 2021;4(10):e2128568. [CrossRef]
Figure 1.
PRISMA Diagram.
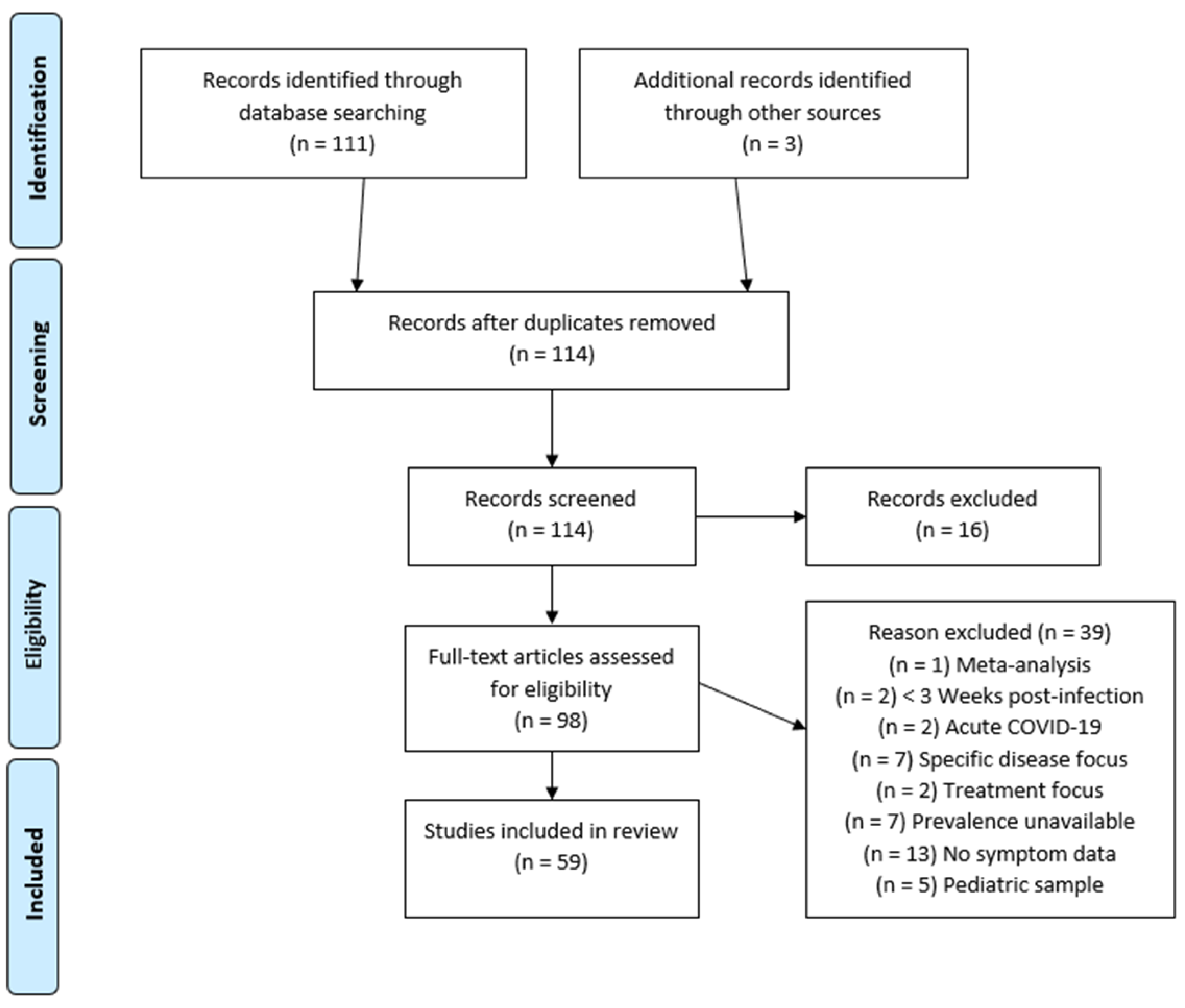
Figure 2.
PASC symptom frequencies (n=59 studies) according to three study design groups: Long COVID, Survey and EHR studies. Bars around the means indicate 95% CI.
Figure 2.
PASC symptom frequencies (n=59 studies) according to three study design groups: Long COVID, Survey and EHR studies. Bars around the means indicate 95% CI.

Figure 3.
PASC symptom frequency across High, Moderate, Low risk of bias groups. Bars around the means indicate 95% CI.
Figure 3.
PASC symptom frequency across High, Moderate, Low risk of bias groups. Bars around the means indicate 95% CI.
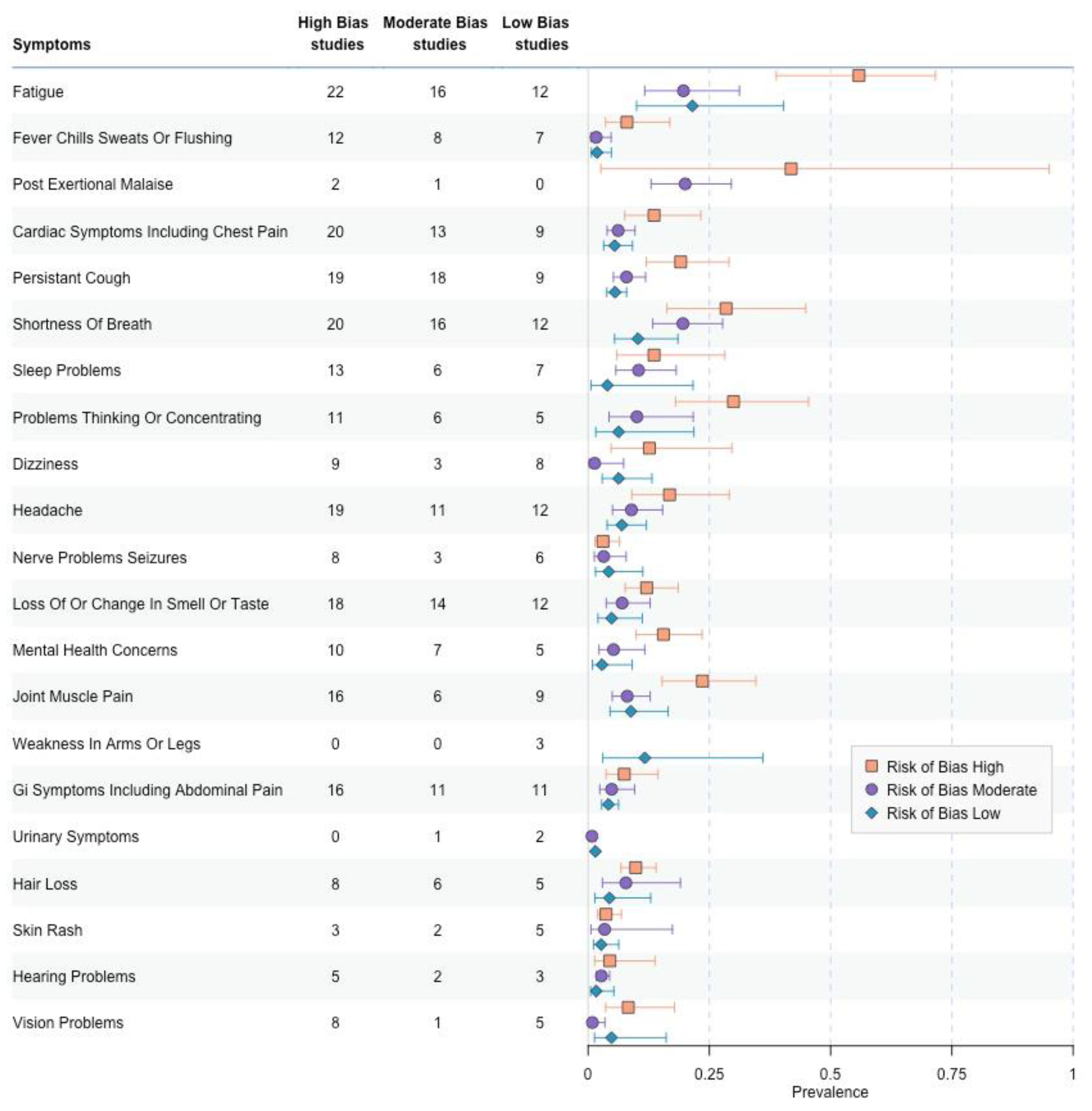
Figure 4.
a. PASC symptom prevalence Limited to Moderate or Low Risk of Bias Studies Stratified by EHR or Survey Data. Bars around the means indicate 95% CI. An asterisk indicates a statistically significant comparison of proportion for a given symptom category after multiple hypothesis correction (p < 0.0024) Figure 4b. PASC symptom prevalence in Moderate or Low Risk of Bias Studies Stratified by Hospitalized or Mixed Studies with Hospitalized and Non-Hospitalized Survey Data. Bars around the means indicate 95% CI. An asterisk indicates a statistically significant comparison of proportion for a given symptom category after multiple hypothesis correction (p < 0.0024).
Figure 4.
a. PASC symptom prevalence Limited to Moderate or Low Risk of Bias Studies Stratified by EHR or Survey Data. Bars around the means indicate 95% CI. An asterisk indicates a statistically significant comparison of proportion for a given symptom category after multiple hypothesis correction (p < 0.0024) Figure 4b. PASC symptom prevalence in Moderate or Low Risk of Bias Studies Stratified by Hospitalized or Mixed Studies with Hospitalized and Non-Hospitalized Survey Data. Bars around the means indicate 95% CI. An asterisk indicates a statistically significant comparison of proportion for a given symptom category after multiple hypothesis correction (p < 0.0024).
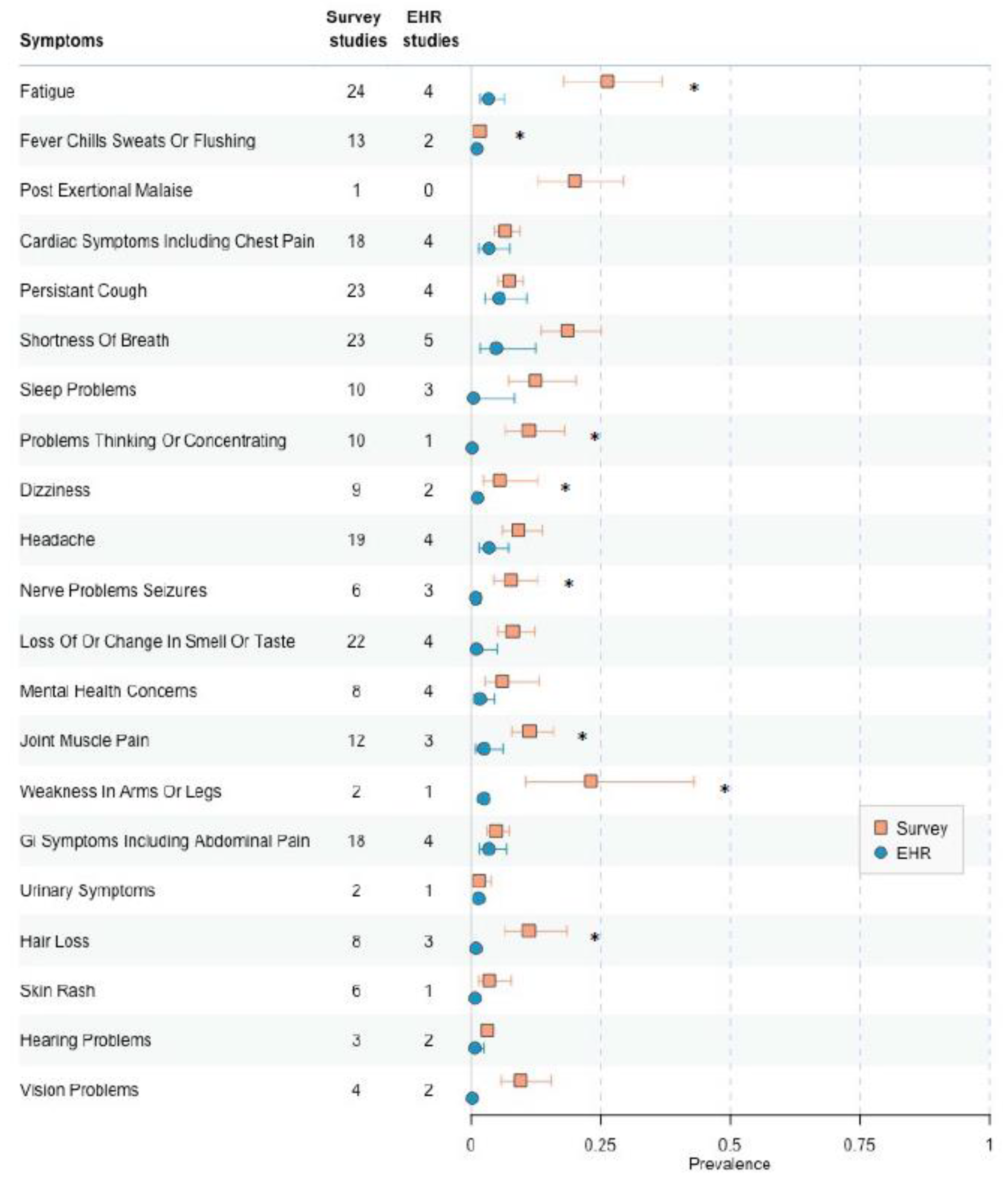
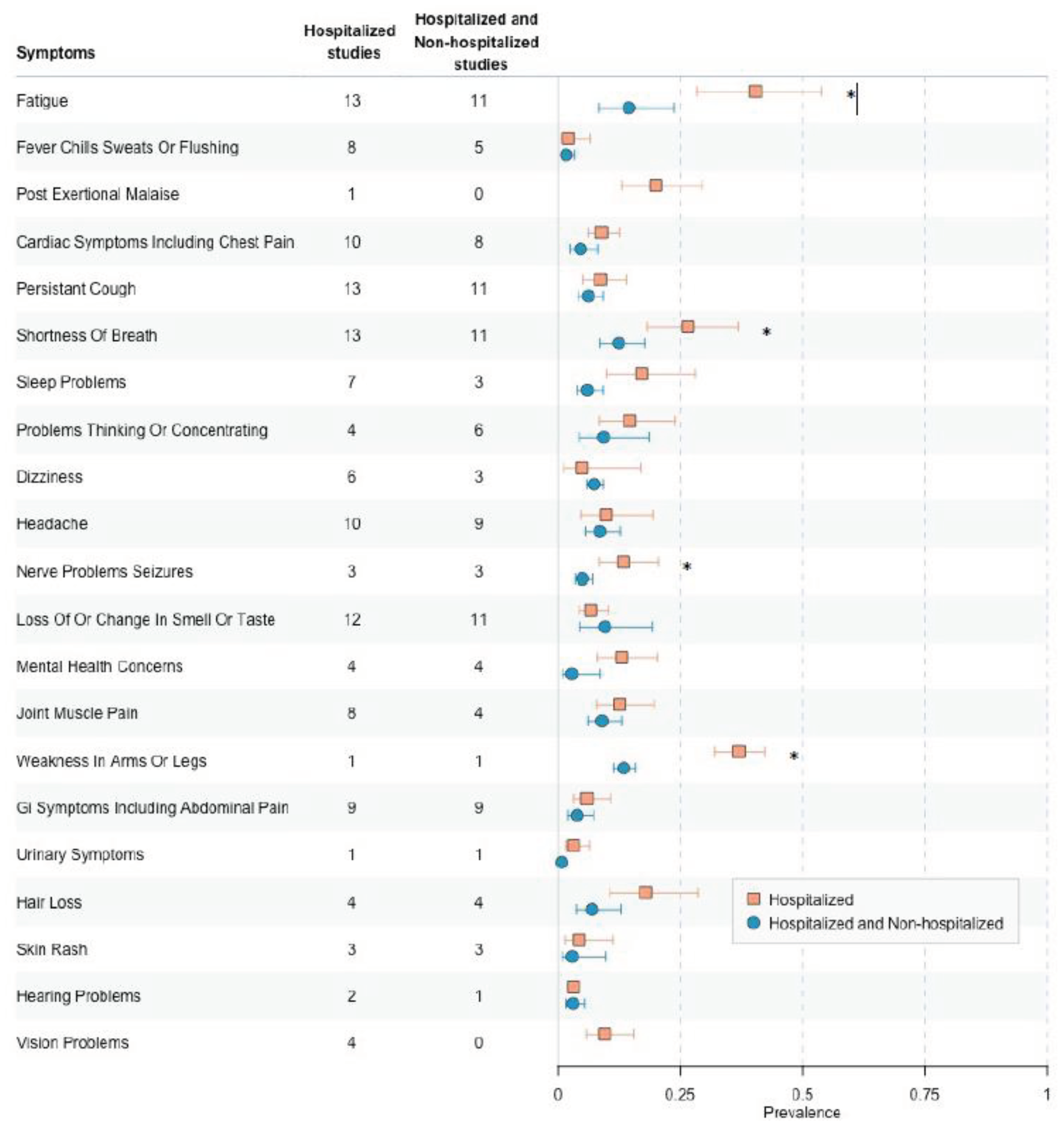

Table 1.
Summary review table for PASC symptom studies.
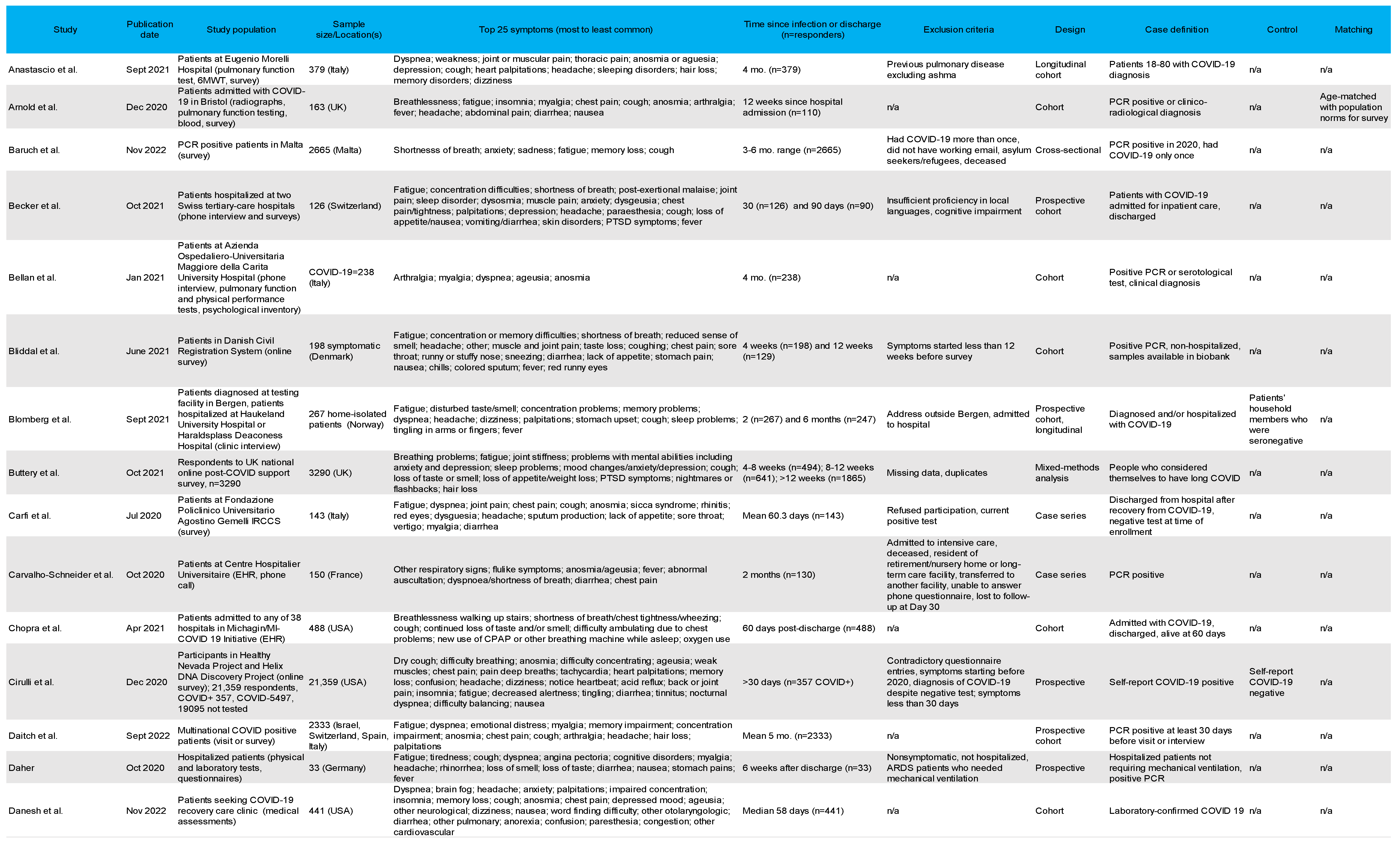
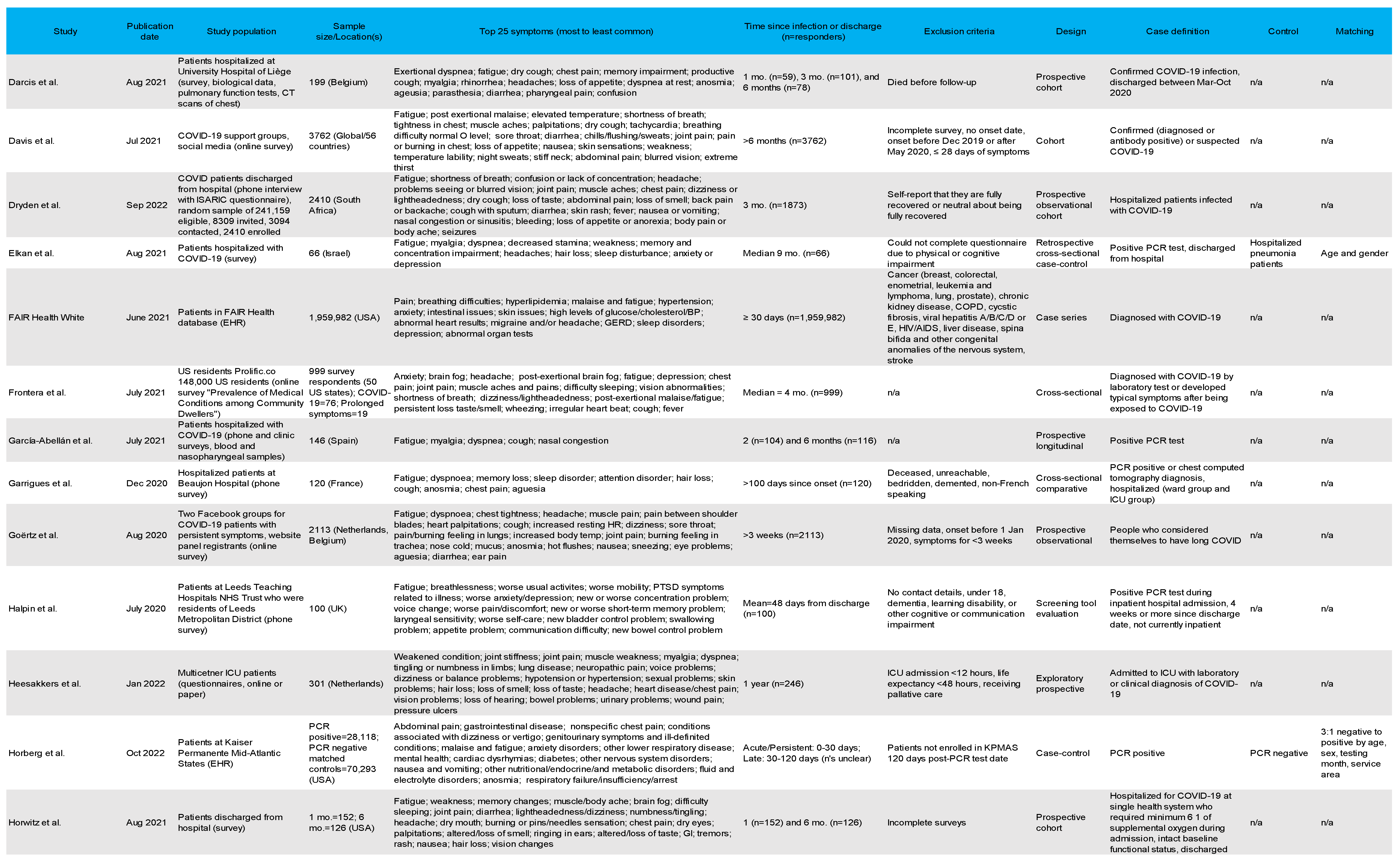
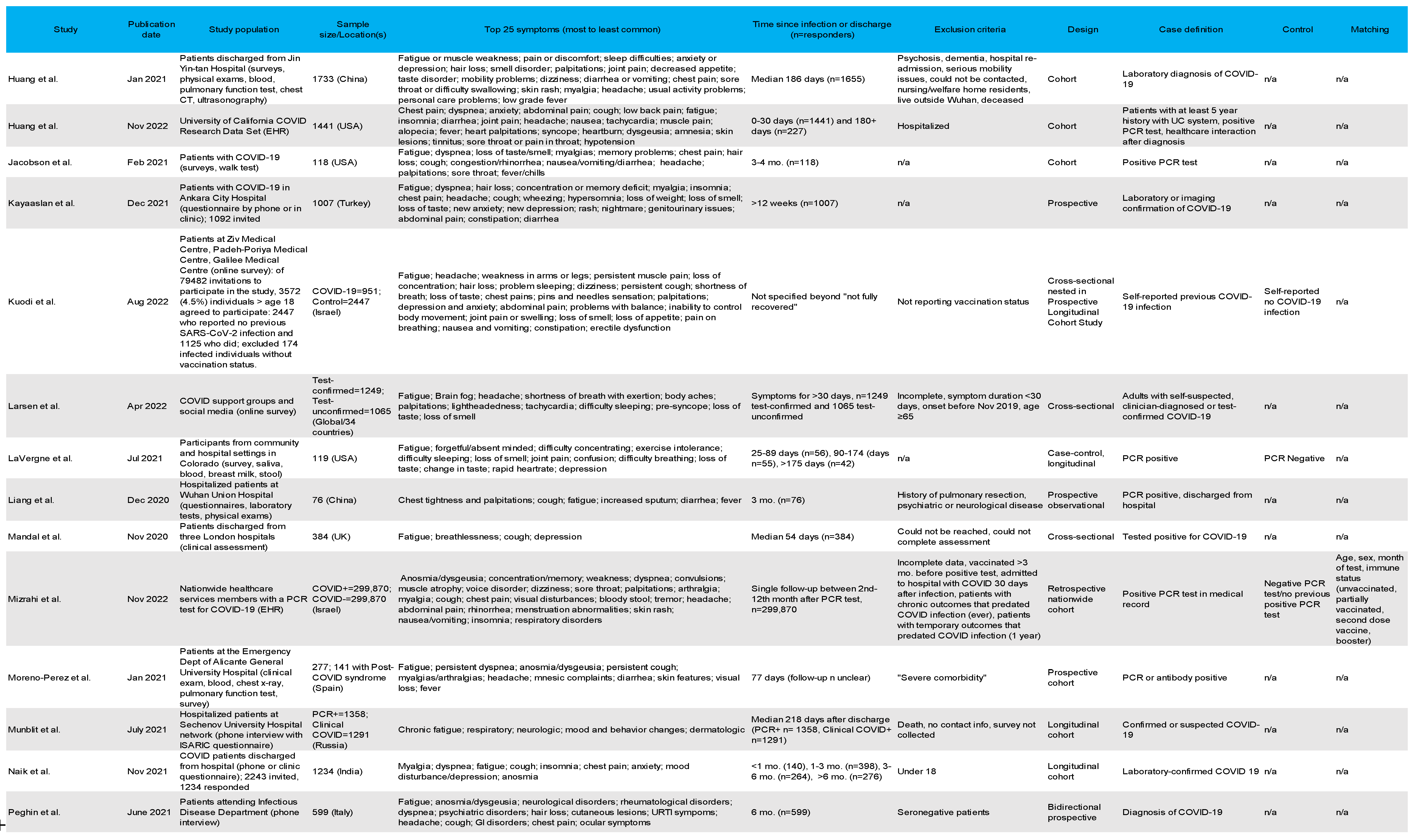
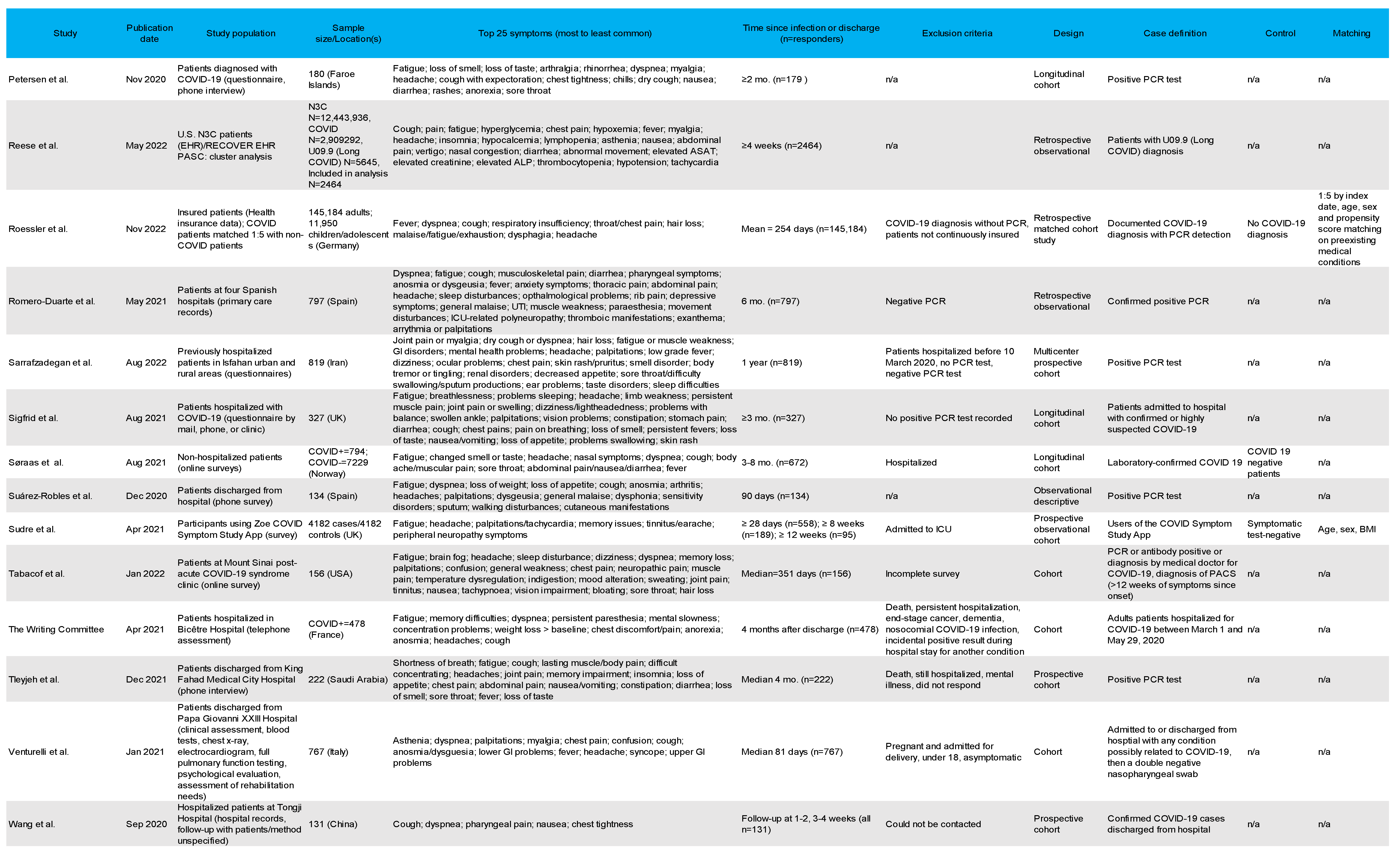

Table 2.
PASC symptom reports for all studies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



