
Submitted:
20 March 2024
Posted:
22 March 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The effect of COVID-19 infection, versus the indirect effect of the pandemic on body composition remains unclear. This study investigates long-term changes in body composition in COVID–19 survivors compared to a contemporary control group.
Method: This is a prospective study involving adults who had a pre-pandemic whole-body DXA scan (DXA#1) performed between 2017 and 2019. Participants were asked to return for a repeat whole-body DXA scan (DXA#2) after the pandemic. Detailed data were collected including medical and COVID history. Inflammation markers and fasting lipids were measured. For those participants who had a COVID-19 infection between the 2 DXAs, DXA#2 was acquired at least one year after COVID-19 infection.
Results: Overall, 160 adults were enrolled; 32.5% females, 51.8% non-white, with mean age of 43.2 years. Half (n=80) of the participants had documented COVID infection between their 2 DXA scans (COVID+ group), and the other half never had COVID. COVID-negative participants had an increase in annualized trunk fat (g) [922.5 vs. 159.7; P=0.01], total fat (g) [1564.3 vs. 199.9; P=0.2], and LBM (g) [974.9 vs. -64.5; P=0.0002], when compared to COVID+ group. However, among the COVID+ group, no differences were seen in annualized trunk fat, total fat mass, or LBM between those with PASC and without (p>0.05).
Conclusion: During the pandemic, both COVID-19-survivors and COVID-negative groups exhibited increases in weight, and total and trunk fat, likely associated with pandemic-linked lifestyle modifications. However, only COVID-19-survivors had a decline in lean body mass over the same period, regardless of PASC symptoms.
Keywords:
long-COVID
; PASC
; Body composition
; COVID pandemic
1. Introduction
The Coronavirus disease-2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus-2 (SARS–CoV-2) has had a massive influence on health, including millions of individuals globally who suffer from Long-COVID, also known as Post-Acute Sequelae of SARS-CoV-2 (PASC) [1]. In addition to fatigue, brain fog, and loss of sense of taste or smell, long-COVID also encompasses any new onset condition apparently triggered by COVID infection, such as new onset diabetes or autoimmune disease [2,3,4]. The multifaceted direct impact of COVID-19 on individuals, combined with the indirect consequences of lockdown measures and reduced physical activity, has raised concerns about alterations in body composition factors such as weight, fat, bone mineral density (BMD), and lean body mass (LBM) [5,6,7,8].
Studies conducted during and after the pandemic have focused on exploring the relationship between the severity of COVID-19 infection, lockdown, and body composition. Some of these studies have looked at the impact of body composition on COVID-19 outcomes and severity [9,10], while others have assessed the risks associated with the pandemic on body composition outcomes after recovery. The first meta-analysis conducted after the initial lockdown in 2020 found a significant increase in body weight among individuals 16 years and older [5]. Another study reported a worsening in BMD, fat mass, and hand grip strength in women with unhealthy lifestyles after 13 weeks of lockdown [6].
While confinement, unhealthy diet, increased alcohol intake, and reduced physical activity can contribute to deterioration in overall health, body composition [11] and induce sarcopenia [12,13], SARS-Cov-2 may influence these parameters as well. The mechanism of action of this virus on human cells was identified by multiple studies [14,15]. This lineage B Beta-coronavirus can enter human cells expressing Angiotensin Converting Enzyme 2 (ACE2) receptors including bone and muscle cells [14,16,17]. ACE2 receptors regulate inflammation by converting angiotensin II (inflammatory) to angiotensin 1–7 (anti–inflammatory) [17]. Upon infection, SARS-CoV-2 infiltrates specific host cells via spike protein–ACE2 receptor binding leading to a decrease in ACE2 expression with subsequent elevated angiotensin-II levels. This triggers extensive inflammation in affected organs [17,18]. Additionally, the immune response to SARS–CoV–2 infection may contribute to musculoskeletal damage via the excessive production of pro-inflammatory cytokines such as IL-6, IL-17, IL-18, TNF-α, and MCP1 [17,19]. The literature extensively documents the muscular consequences of the initial acute COVID-19 infection, including myalgia, muscle weakness and loss, and reduced physical performance post-COVID-19 infection [20,21].
Few studies have evaluated changes in body composition in individuals with long-COVID. Sampalo described a high prevalence of sarcopenia three months post-COVID infection and an increase in weight and fat mass after 1 year [7]. In a cross-sectional study conducted by Velez R comparing individuals with long-COVID-19 to a control group, those with long-COVID exhibited higher total fat and visceral adiposity, along with lower lean muscle [8].
To our knowledge, no one has studied the long term effect of COVID–19 infection on body composition particularly in comparison to pre-infection baseline data, and an uninfected control group from the same pandemic period. This study aims for the first time to investigate long-term changes in LBM, total BMD, and total and trunk fat in COVID-19 survivors compared to a control group of never infected participants, using pre-pandemic and post-pandemic DXA scans accounting for COVID-19 infection status.
2. Methods
2.1. Study Design
This study is an observational prospective cohort that consists of post-pandemic follow- up of a cohort of individuals with available pre-pandemic data including whole body DXA scan obtained between 2017 and 2019. Study aimed to enroll 160 participants with prior available data; 80 COVID-19 survivors and 80 participants who never had SARS-CoV-2 infection. The whole-body DXA scan available from pre-pandemic period is referred to as DXA#1, while the post-pandemic DXA as DXA#2. Comprehensive demographics, clinical data and medical history was obtained on these participants, retrospectively from pre-pandemic era and prospectively collected during the post-pandemic follow-up. At both time points, we measured inflammation markers, fasting lipids, and creatine kinase (CK) levels, the latter two were ran in real time in a CLIA-certified laboratory at University Hospitals Cleveland Medical Center (UHCMC), Cleveland, Ohio.
2.2. Recruiting and Study Population
All participants who previously enrolled in studies conducted at the Metabolic Research Center of UHCMC were approached if they had expressed willingness to be contacted for future research projects, were at least 18 years of age, and had a whole-body DXA scan performed between 2017 and 2019.
In addition, to be included, participants had to either 1) have no history of COVID-19 or suggestive symptoms/illness since DXA#1, with negative antibody tests (negative nucleocapsid antibody and negative spike antibody if unimmunized) done at the post-pandemic evaluation; COVID-negative group, or 2) participants had to have at least one documented COVID-19 infection (by positive PCR or antigen test, or documented in the electronic medical records, EMR) since DXA#1 and the COVID infection dated back at least 1 year prior to the post-pandemic visit. We excluded women who are pregnant or lactating, and those with cognitive impairment unable to consent. The study was approved by the Institutional Review Board of UHCMC and a signed consent was obtained from each participant before any study activity.
2.3. Study Measurements
2.3.1. Baseline Characteristics
The same questionnaires were used for all participants to obtain the following information: demographic characteristics (age, race/ethnicity, sex), smoking and alcohol consumption, family history (cardiovascular disease, diabetes, hypertension, strokes, or hip fracture) and the level of physical activity (in minutes/week). A detailed review of their medical history was obtained from participants and their EMRs including co-morbidities, clinical diagnoses, COVID infection(s) dates, tests performed, and course of illness. Weight and height were measured using standardized protocol.
The group of individuals who had at least 1 COVID infection (COVID+ group) was divided based on whether they displayed symptoms of PASC or not (referred to respectively as COVID+ PASC+ or COVID+ No PASC). Where PASC is considered as having ≥2 persistent symptoms that started after COVID infection and lasted for at least 3 months, symptoms captured in the questionnaires filled by patients included: fatigue, loss of energy, shortness of breath, cough, change or loss of smell or taste, feeling pain in any part of the body, trouble thinking or concentrating, feeling sad or anxious, sweat chills and fever, post exertional malaise, excessive thirst, and gastrointestinal symptoms.
2.3.2. Inflammatory Markers and Oxidized LDL
Fasting blood (>8 hours fast) was obtained and sent to a CLIA-certified laboratory at UHCMC for measurements of lipids, creatine kinase, glucose and insulin with Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) derived from the latter 2 tests. Additional blood was processed within 2 hours, aliquoted, and stored at -80 until shipment on dry ice to Dr. Funderburg’s laboratory, Ohio State University, for measurements of biomarkers using enzyme-linked immunosorbent assay (ELISA). The following were measured: Markers of monocyte activation soluble CD14 and CD163 (sCD14 and sCD163), markers of inflammation high-sensitivity C-reactive protein (hs-CRP), interleukin (IL)-6, interferon-gamma inducible protein of 10 kDa (IP-10), tumor necrosis factor receptor 1 and 2 (TNF-RI and TNF-RII), and vascular cell adhesion molecule (VCAM) were measured using R&D Systems (Minneapolis, Minnesota, USA); oxidized low-density lipoprotein (oxLDL) using kits (Upsala, Mercodia, Sweden), and D-dimer (Diagnostica Stago, Parsippany, NJ, USA).
2.3.3. Body Composition Measurements
Both DXA#1 and DXA#2 were performed on the same machine on all participants using Hologic, Horizon A, 5.6.0.4 DXA system. DXA quantified total fat, limb fat, and trunk fat, total LBM, and total BMD.
2.4. Statistical Analysis
Characteristics of study participants were described using frequency (n) and percentage (%) for categorical variables and mean ±standard deviation (std) or median and interquartile range (IQR) for continuous variables. Differences between groups at DXA#1 were assessed using independent t-test, Kruskal-Wallis, or chi-square. To account for the difference in time between DXA#1 and DXA#2, longitudinal generalized linear mixed models with random intercept were used to estimate within and between group changes in inflammation. DXA outcomes were transformed to reflect annualized change and annualized percent (%) change. Annualized change was calculated by dividing the mean difference in each outcome between DXA measures by the difference in follow-up time . Annualized % change was derived by dividing annualized change by the mean outcome at DXA 1 Adjusted models included COVID and HIV status, age at DXA#1, sex, race, and the difference between DXA#1 and DXA#2 for each inflammation marker was modeled separately. All analyses were conducted using SAS 9.4 (SAS Inc., Cary, N.C., USA) and p-values less than alpha <.05 were considered statistically significant.
3. Results
3.1. Characteristics of Study Participants
A total of 160 prospectively enrolled adults were included in the analysis. The average age was 43.2 ± 14.5 years, 32.5% were female (n=52), and 51.8% (n=83) of non-white race. Eighty participants (50% had documented COVID infection (COVID+) between DXA#1 and DXA#2 (Table 1). All participants living with HIV (HIV-positive) who were on antiretroviral therapy with viral load below the limit of detection. At the pre-pandemic visit, COVID+ had a smaller proportion of smokers [53% (COVID-) vs. 30% (COVID+); P=0.002] and HIV-positive participants [78% (COVID-) vs. 58% (COVID+); P=0.004s]. However, there was not enough evidence to suggest any differences (P>0.05) in weight, HOMA-IR, alcohol consumption, weekly physical activity, HDL, non-HDL, creatinine kinase, or body composition measures between the groups. The median number of days between DXA measurements among COVID- was 500 days and 899 days among COVID+ (P<.0001). Among the COVID-infected group, 55% (n=44) had PASC (COVID+ PASC+). Among COVID+ without PASC (COVID+ No PASC), the median number of days between DXA visits was 743 (IQR: 420, 1560) and 915.5 (IQR: 673.5, 1489.5) days among COVID+ PASC+. The five most frequently reported symptoms were fatigue (58.2%), trouble thinking or concentrating (51.2%), shortness of breath (44.2%), feeling sad, down, depressed, or anxious (39.5%), and feeling pain in any body part (34.9%). During the acute COVID-19 illness, 92% of the COVID+ group had managed their symptoms at home without hospitalization; only one participant was hospitalized for 2 days without ICU admission. Additionally, only 3.75% received steroids during the study period, none of them specifically for COVID-19.
3.2. Changes in Inflammation
Accounting for the differences in time between DXA#1 and DXA#2 (Table 2), increases in VCAM (71.5 ng/mL; P=0.06) and oxLDL (33.5 U/L; P<.001) among COVID+ group were observed. Within the COVID- group, decreases in TNF-RII (-877.9 pg/mL; P<.001) and D-dimer (-473.1 ng/mL; P=0.04) were observed. Comparing the changes in inflammation over time between the 2 groups, there is evidence that COVID-infection has an effect on VCAM (P=0.02), TNF-RII (P<.0001), and oxLDL (P<.0001).
3.3. Annualized Change in Body Composition
In Figure 1, COVID- participants had larger annualized increase in trunk fat (g) [922.5 vs. 159.7 (Δ=-762.9); P=0.01], total fat (g) [1564.3 vs. 199.9 (Δ=-1364.3); P=0.2], and LBM (g) [974.9 vs. -64.5 (Δ=-1039.4); P=0.0002], compared to COVID+. There was no effect of HOMA-IR or alcohol consumption on measures of body composition. Because of the potential effect of HIV status on body composition, we adjusted for both HIV and COVID status. In adjusted models (Table 3), the between groups differences in trunk fat (P=0.004) and LBM (P=0.001) remained. Among inflammation markers, only hsCRP was associated with trunk fat (P=0.01) and total fat mass (P=0.04).
3.4. Effect of PASC Status on Body Composition among COVID-Survivors
Among COVID+ without PASC, the median annualized trunk fat was 150.2 (IQR: -217.6, 743.1), total fat mass was 166.2 (IQR: -623.6, 1258.7), and LBM was 113.3 (IQR: -371.9, 965.2). Among COVID-survivors with PASC+, the median annualized trunk fat was 300 (IAR: -449.9, 1159.3), fat mass was 471 (IQR: -1073.4, 1764.8), and LBM was -242.4 (IQR: -1203.6, 483.2). However, the differences in annualized trunk fat, total fat mass, or LBM were not significantly different (p>0.05 for all) between those with or without PASC.
4. Discussion
In this prospective longitudinal study, we investigated the long-term changes in body composition of COVID-19 survivors compared to a contemporary control group. We were the first to dissociate the effect of COVID-19 infection from the indirect effect of the pandemic on body composition. Each patient underwent a pre-pandemic whole body DXA scan and a post-pandemic DXA scan within five years. After adjusting for possible confounders, we found that both groups had increased their total fat, trunk fat, and weight during the study period. The changes were even more prominent in the COVID-negative group. These findings are in line with the longitudinal study by Marcos-Pardo which showed a significant increase in trunk fat mass and total fat mass after 13 week-lockdown in Spanish older women [6]. A meta-analysis published in 2021 also demonstrated an increase in weight during the pandemic [5]. Furthermore, in a meta-analysis, some athletes were found to gain weight during the COVID pandemic despite all efforts to maintain their physical performance [22].
These results can be explained by the impact of the pandemic, regardless of COVID-19 infection status, while also taking into account the decline in health caused by a sedentary lifestyle, as well as the lockdown measures [23]. Although our study did not specifically consider the participants' lifestyle habits during the pandemic, previous research has shown a significant reduction in physical activity, along with an increase in snacking frequency, carbohydrate, and fast-food consumption, during this period [23,24,25].
On the other hand, our study found that individuals who had contracted COVID-19 infection during the study period showed a slight decrease in LBM over time, while those who remained uninfected experienced an increase in LBM. Our results align with a cross-sectional study conducted by Ramirez-Velez et al., which found that individuals diagnosed with long-COVID-19 syndrome had significantly lower levels of total and appendicular lean mass tissue, and muscle strength parameters compared to controls [8] . In addition, our study's findings support a previous cross-sectional study by Lopez-Sampalo, which revealed higher percentages of sarcopenia among older individuals three months after COVID-19 infection with reduced muscle strength. It is worth noting that muscle strength in the mentioned study was measured by dynamometry using grip strength, while body composition was obtained using bioelectrical impedance [7].
The observed difference in LBM between the two groups in our study may be due to the direct effect of SARS-COV-2 infection on muscle cells given that only COVID+ group showed deterioration in LBM as opposed to uninfected individuals. The majority of our participants were not taking steroids during the study period, suggesting that our findings are not confounded and independent of steroid use. Studies have shown that SARS-CoV-2 enters muscle cells through ACE receptors, disrupting their homeostasis and causing inflammation within these cells, which affects their function during acute infection causing a wide range of muscle symptoms [14,17,18]. Although the etiology of PASC remains unclear, a recent study used electromyography and muscle biopsies to investigate the cause of post-COVID-19 fatigue, myalgia, and weakness that lasted up to 14 months after infection. This study found muscle fiber atrophy, regeneration, mitochondrial alterations, inflammation, and capillary damage, changes that suggest that SARS-CoV-2 may target skeletal muscles, which may lead to long-term myopathy, even in cases of mild or moderate acute infection [26]. Another recent study supports this evidence by showing pathophysiological changes in muscle biopsies taken from individuals diagnosed as having PASC with post-exertional malaise. The biopsies showed a reduction in skeletal muscle mitochondrial enzyme activity together with blunted T-cell response following acute exercise, an increased accumulation of amyloid-containing deposits and signs of severe muscle tissue damage [27].
Our study did not find significant differences in annualized LBM, trunk fat, and total fat between individuals who had PASC and those who seemingly had full recovery after COVID-19 infection. This suggests that individuals who have had COVID-19 may experience the same changes in body composition including muscle involvement as individuals who did develop PASC despite the absence of symptoms. Further studies investigating muscle involvement in PASC should always have a control group of COVID-19 survivors who did not develop PASC.
Finally, our study failed to demonstrate any change in total BMD between groups, although total BMD is a less sensitive marker of worsening in BMD when compared to lumbar or hip BMD. Previously, Berktas reported a decrease in BMD after COVID-19 illness [28]. Similarly, Elmedany observed a significant decline in BMD among individuals with osteoporosis 9 months after contracting COVID-19. [29]. These results can be explained by the fact that inflammatory mediators affect the expression of RANK (osteoclast receptor) and RANKL (osteoblast ligand), thereby disrupting bone remodeling and increasing bone resorption [30,31]. Further studies are necessary to evaluate longer term effects of COVID-19 on bone health, using hip and lumbar BMD.
It is known that COVID-survivors have elevated levels of several inflammation markers [32]. We measured different biomarkers of inflammation to study their relationship to changes in body composition. We did show that COVID survivors had increases in several markers of inflammation when compared to COVID-negative group, specifically sTNF-RII, VCAM and oxLDL; however, none of these markers were associated with body composition measurements. Only hs-CRP was associated with changes in total and trunk fat, a finding known to occur in the general population outside of COVID-19 infection. It is notable that our finding of increased oxLDL in COVID-19 survivors align with previous research [33,34], highlighting a correlation between this marker and COVID-19 infection, in particular in individuals who develop PASC.
There are a few limitations to our study that should be addressed. First, we did not report on lifestyle habits such as detailed physical activity and diet during the study period. Second, our study estimated total body BMD which is not sensitive at detecting small changes in BMD; future studies should use lumbar spine and hip BMD.
In conclusion, we demonstrated changes in body composition in a group of COVID survivors when compared to a group of individuals who did not have COVID-19 infection during the study period. Both groups exhibited increases in total fat, trunk fat, and weight over the study, potentially linked to lifestyle changes during the pandemic. Notably, all COVID-19 survivors regardless of PASC status witnessed a decline in lean body mass and increase in several inflammatory biomarkers over the same period, suggesting a direct impact of COVID-19 on muscle, possibly related to enhanced inflammation. Further larger and longer term studies should assess the effect on body composition of COVID infection, and the pathological mechanisms associated with these changes.
Author Contributions
JD: CM, and GM contributed to study concept and design. All authors contributed to acquisition of data. JD, OA and GM. contributed to analysis and interpretation of data. JD contributed to statistical analysis. GM obtained funding and supervised the study. OA, JB, JD, and GM drafted the manuscript, and all authors contributed to critical revision of the manuscript for important intellectual content. Part of this work was showcased as a poster during the 31st Conference on Retroviruses and Opportunistic Infections (CROI), held from March 3 to 6, 2024, Denver, Colorado.
Funding
This project was supported by the Clinical and Translational Science Collaborative (CTSC) of Northern Ohio (UM1TR004528 for GM) which is funded by the National Institutes of Health, National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Conflicts of Interest
Dr. Grace A McComsey has served as consultant for Gilead, Janssen, Merck and ViiV. All other authors declare no conflict of interest that could have influenced the conduct or reporting of this research.
References
- Long COVID or Post-COVID Conditions | CDC. Accessed August 24, 2023. https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html.
- Dotan A, Muller S, Kanduc D, David P, Halpert G, Shoenfeld Y. The SARS-CoV-2 as an instrumental trigger of autoimmunity. Autoimmun Rev. 2021;20(4):102792. [CrossRef]
- Buonsenso D, Moscato U, Sisti G, Tchounwou PB, Wrona M, Skrypnik D. New-Onset Diabetes Mellitus, Hypertension, Dyslipidaemia as Sequelae of COVID-19 Infection-Systematic Review. Published online 2022. [CrossRef]
- Davis PB, Xu R. COVID-19 and Incident Diabetes-Recovery Is Not So Sweet After All. Published online 2023. [CrossRef]
- Bakaloudi DR, Barazzoni R, Bischoff SC, Breda J, Wickramasinghe K, Chourdakis M. Impact of the first COVID-19 lockdown on body weight: A combined systematic review and a meta-analysis. Clinical Nutrition. 2022;41(12):3046-3054. [CrossRef]
- Marcos-Pardo PJ, Abelleira-Lamela T, González-Gálvez N, Esparza-Ros F, Espeso-García A, Vaquero-Cristóbal R. Impact of COVID-19 lockdown on health parameters and muscle strength of older women: A longitudinal study. Exp Gerontol. 2022;164. [CrossRef]
- López-Sampalo A, Cobos-Palacios L, Vilches-Pérez A, et al. COVID-19 in Older Patients: Assessment of Post-COVID-19 Sarcopenia. Biomedicines. 2023;11(3). [CrossRef]
- Ramírez-Vélez R, Legarra-Gorgoñon G, Oscoz-Ochandorena S, et al. Reduced muscle strength in patients with long-COVID-19 syndrome is mediated by limb muscle mass. J Appl Physiol (1985). 2023;134(1):50-58. [CrossRef]
- Manolis AS, Manolis AA, Manolis TA, Apostolaki NE, Melita H. COVID-19 infection and body weight: A deleterious liaison in a J-curve relationship. Obes Res Clin Pract. 2021;15(6):523-535. [CrossRef]
- Wang Y, Tan S, Yan Q, Gao Y. Sarcopenia and COVID-19 Outcomes. Clin Interv Aging. 2023;18:359-373. [CrossRef]
- Martinez-Ferran M, de la Guía-Galipienso F, Sanchis-Gomar F, Pareja-Galeano H. Metabolic impacts of confinement during the COVID-19 pandemic due to modified diet and physical activity habits. Nutrients. 2020;12(6). [CrossRef]
- Ali AM, Kunugi H. Screening for Sarcopenia (Physical Frailty) in the COVID-19 Era. Int J Endocrinol. 2021;2021. [CrossRef]
- Kirwan R, McCullough D, Butler T, Perez de Heredia F, Davies IG, Stewart C. Sarcopenia during COVID-19 lockdown restrictions: long-term health effects of short-term muscle loss. Geroscience. 2020;42(6):1547-1578. [CrossRef]
- Letko M, Marzi A, Munster V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat Microbiol. 2020;5(4):562-569. [CrossRef]
- Zhang H, Penninger JM, Li Y, Zhong N, Slutsky AS. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020;46(4):586. [CrossRef]
- Obitsu S, Ahmed N, Nishitsuji H, et al. Potential enhancement of osteoclastogenesis by severe acute respiratory syndrome coronavirus 3a/X1 protein. Arch Virol. 2009;154(9):1457. [CrossRef]
- Sapra L, Saini C, Garg B, et al. Long-term implications of COVID-19 on bone health: pathophysiology and therapeutics. Inflammation Research. 2022;71(9):1025-1040. [CrossRef]
- Kuba K, Imai Y, Penninger JM. Angiotensin-converting enzyme 2 in lung diseases. Curr Opin Pharmacol. 2006;6(3):271-276. [CrossRef]
- Meftahi GH, Jangravi Z, Sahraei H, Bahari Z. The possible pathophysiology mechanism of cytokine storm in elderly adults with COVID-19 infection: the contribution of “inflame-aging.” Inflammation Research. 2020;69(9):825-839. [CrossRef]
- Evcik D. Musculoskeletal involvement: COVID-19 and post COVID 19. Turk J Phys Med Rehabil. 2023;69(1):1-7. [CrossRef]
- Besutti G, Pellegrini M, Ottone M, et al. Modifications of Chest CT Body Composition Parameters at Three and Six Months after Severe COVID-19 Pneumonia: A Retrospective Cohort Study. Nutrients. 2022;14(18). [CrossRef]
- Rosa BV, Maldonado AJ, de Araújo AO, Neves LM, Rossi FE. Impact of the COVID-19 Lockdown on the Body Composition and Physical Performance of Athletes: A Systematic Review with Meta-Analysis and Meta-Regression. Healthcare (Switzerland). 2023;11(16). [CrossRef]
- Ghosh A, Arora B, Gupta R, Anoop S, Misra A. Effects of nationwide lockdown during COVID-19 epidemic on lifestyle and other medical issues of patients with type 2 diabetes in north India. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2020;14(5):917-920. [CrossRef]
- Al Zaman K, Ahmed S, Alshamsi A, et al. Impact of COVID-19 Pandemic on Weight Change Among Adults in the UAE. Published online 2023. [CrossRef]
- Daniel MM, Liboredo JC, Anastácio LR, et al. Incidence and Associated Factors of Weight Gain During the Covid-19 Pandemic. Front Nutr. 2022;9. [CrossRef]
- Hejbøl EK, Harbo T, Agergaard J, et al. Myopathy as a cause of fatigue in long-term post-COVID-19 symptoms: Evidence of skeletal muscle histopathology. Eur J Neurol. 2022;29(9):2832-2841. [CrossRef]
- Muscle abnormalities worsen after post-exertional malaise in long COVID - s41467-023-44432-3.
- Berktaş BM, Gökçek A, Hoca NT, Koyuncu A. COVID-19 illness and treatment decrease bone mineral density of surviving hospitalized patients. Eur Rev Med Pharmacol Sci. 2022;26(8):3046-3056. [CrossRef]
- Elmedany SH, Badr OI, Abu-Zaid MH, Tabra SAA. Bone mineral density changes in osteoporotic and osteopenic patients after COVID-19 infection. Egyptian Rheumatology and Rehabilitation. 2022;49(1). [CrossRef]
- Epsley S, Tadros S, Farid A, Kargilis D, Mehta S, Rajapakse CS. The Effect of Inflammation on Bone. Front Physiol. 2021;11. [CrossRef]
- Hu CL, Zheng MJ, He XX, Liu DC. COVID-19 and Bone Health.
- Yong SJ, Halim A, Halim M, et al. Inflammatory and vascular biomarkers in post-COVID-19 syndrome: A systematic review and meta-analysis of over 20 biomarkers. Rev Med Virol. 2023;33(2). [CrossRef]
- Mouchati C, Durieux JC, Zisis SN, et al. Increase in gut permeability and oxidized ldl is associated with post-acute sequelae of SARS-CoV-2. Published online 2023. [CrossRef]
- Sokratis Zisis AN, Durieux JC, Mouchati C, et al. Arterial Stiffness and Oxidized LDL Independently Associated With Post-Acute Sequalae of SARS-CoV-2 GA. Arterial Stiffness and Oxidized LDL Independently Associated With Post-Acute Sequalae of SARS-CoV-2. Pathogens and Immunity. Pathog Immun. 2023;8(2):1-15. [CrossRef]
Figure 1.
Annualized Percent (%) Change in Body Weight, Total Fat, Trunk Fat, and Lean Body Mass. FOOTNOTE: Annualized Percent (%) Change (APC) = (annualized change/DXA1)*100. P-value is the between-group probability. The derived APC is shown at DXA 1(baseline) and DXA 2 stratified by COVID Negative and COVID Positive groups. Panel A is the APC in body weight (kg), panel B is the APC in Total Fat (g), panel C is the APC in Trunk Fat (g), and panel D is the APC in Lean Body Mass (g).
Figure 1.
Annualized Percent (%) Change in Body Weight, Total Fat, Trunk Fat, and Lean Body Mass. FOOTNOTE: Annualized Percent (%) Change (APC) = (annualized change/DXA1)*100. P-value is the between-group probability. The derived APC is shown at DXA 1(baseline) and DXA 2 stratified by COVID Negative and COVID Positive groups. Panel A is the APC in body weight (kg), panel B is the APC in Total Fat (g), panel C is the APC in Trunk Fat (g), and panel D is the APC in Lean Body Mass (g).
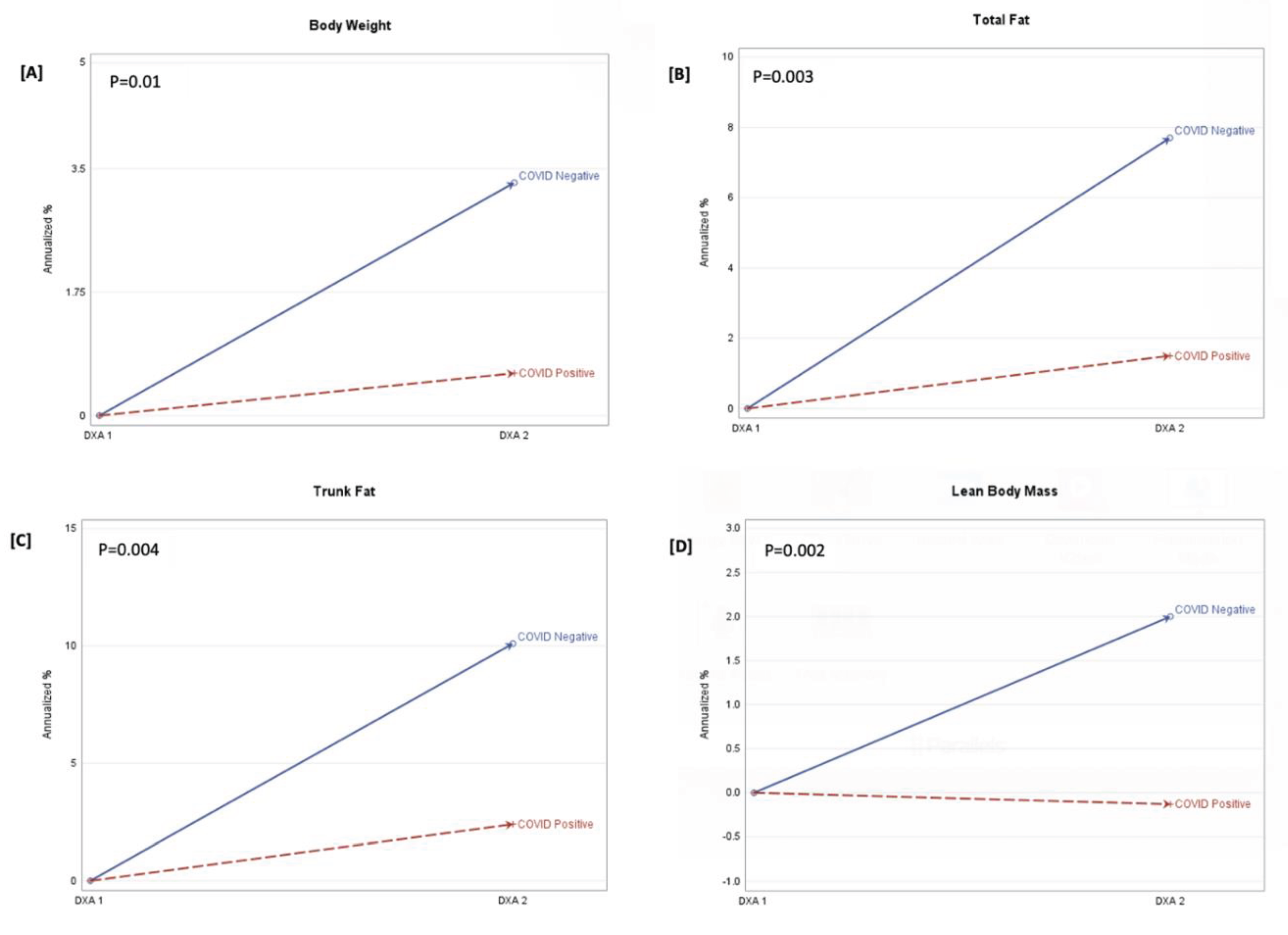

Table 1.
Baseline Characteristics (at DXA#1) among COVID-survivors and COVID-negative participants.
| COVID- (n=80) | COVID+ (n=80) | P-value | |
| n (%), median (IQR), or mean ± std | |||
| Characteristics | |||
| Age (years) | 43.2 ± 15.4 | 42.9 ± 13.6 | 0.9 |
| Female Sex | 25 (28.4) | 27 (33.8) | 0.5 |
| Non-white Race* | 55 (63) | 33 (41.3) | 0.01 |
| Weight (kg) | 83 ± 20.3 | 87 ± 22.2 | 0.4 |
| Body Mass Index (kg/m2) | 28.4 ± 6.3 | 29.7 ± 6.8 | 0.2 |
| Current Smoker (Yes) | 47 (53.4) | 24 (30) | 0.002 |
| Current Alcohol Use (Yes) | 57 (71.3) | 56 (70) | 0.9 |
| Physical Activity (min/week) | 2520 (870, 3735) | 2310 (1260, 3525) | 0.7 |
| Mid-Waist Circumference (cm) | 95.8 ± 17.6 | 98.2 ± 16.9 | 0.3 |
| HIV Status (+) | 69 (78) | 46 (58) | 0.004 |
| Days between DXA 1 and 2 | 500 (399, 936) | 899 (569, 1495) | 0.0001 |
| HDL (mg/dL) | 46.2 ± 12.9 | 48.1 ± 12.9 | 0.4 |
| non-HDL | 120.5 ± 34.5 | 129.2 ± 37.5 | 0.07 |
| Creatine Kinase (uL) | 207.3 ± 159.5 | 167.9 ± 117.2 | 0.2 |
| Homa-IR | 2.6 ± 2.2 | 3.7 ± 4.9 | 0.6 |
| DXA Markers | |||
| Total Body BMD | 1.2 (1.1, 1.2) | 1.1 (1.1, 1.2) | 0.33 |
| Trunk Fat (g) | 11806.4 (6907.5, 17260.8) | 13206.3 (10113.7, 17745.4) | 0.07 |
| Total Fat (g) | 24921.4 (16809.8, 34842.2) | 26782.6 (21737.7, 34204.1) | 0.08 |
| Total LBM (g) | 52423 (45930.1, 58476.8) | 52956.2 (45096.4, 62194.1) | 0.4 |
| Inflammation Markers | |||
| IL-6 (pg/mL) | 2.8 (1.8, 5.6) | 2.5 (1.5, 3.8) | 0.1 |
| VCAM (ng/mL) | 830.2 (673.7, 1018.5) | 739.8 (642.6, 963.1) | 0.06 |
| TNF-RI (pg/mL) | 1046.8 (847.8, 1328.6) | 1006.4 (771.7, 1141.1) | 0.05 |
| TNF-RII (pg/mL) | 2961.1 (2364, 4366.7) | 2190.2 (1874, 2898.2) | <.0001 |
| hsCRP (ng/mL) | 3512.4 (1287.5, 7684.6) | 2696.8 (880.4, 8651.2) | 0.3 |
| IP10 (pg/mL) | 181.4 (135.4, 328.5) | 124.5 (97.5, 196.7) | 0.001 |
| D-dimer (ng/mL) | 411.6 (274.8, 600.2) | 316.4 (195.8, 517.1) | 0.02 |
| oxLDL (U/L) | 43.4 (35.3, 52.9) | 50.9 (38.1, 65.7) | 0.02 |
| sCD14 (ng/mL) | 1711.9 (1435.1, 2117.8) | 1592.5 (1305.9, 1949.8) | 0.1 |
| sCD163 (ng/mL) | 708.6 (530.9, 1148.4) | 624.9 (410.2, 851.2) | 0.01 |
* Includes African American, Asian, Hispanic, and Other; ** Abbreviations: HDL=High-density liproprotein; IL-6=Interleukin-6; VCAM=Vascular Cell Adhesion Molecule-1; TNF-RI=Tumor Necrosis Factor Receptor-1; TNF-RII=Tumor Necrosis Factor Receptor-2; hsCRP=High-sensitivity C-reactive protein; I-CAM=Intercellurlar Adhesion Molecule-1; IP10=Interferon-gamma Inducible Protein of 10-kDa; oxLDL=Oxidized LDL; sCD14=Soluble CD14; sCD163=Soluble CD163.
Table 2.
Changes in inflammation between DXA 1 and DXA 2 by COVID Status.
| COVID- | COVID+ |
P-value (between group) |
|
| mean ± std (P-vaue)* | |||
| VCAM | -53.03 ± 37.3 (0.2) | 71.5 ± 38.4 (0.06) | 0.02 |
| TNF_RI | -53.2 ± 46.0 (0.3) | 62.5 ± 47.0 (0.2) | 0.08 |
| TNF-RII | -877.9 ± 181.9 (<.001) | 41.0 ± 185.9 (0.8) | <.0001 |
| hsCRP | -2390.3 ± 1668.5 (0.2) | -312.2 ± 1693.0 (0.8) | 0.4 |
| D-dimer | -473.1 ± 230.1 (0.04) | 93.2 ± 235.1 (0.7) | 0.08 |
| oxLDL | 47.2 ± 42.4 (0.3) | 33.5 ± 45.1 (<.001) | <.0001 |
*P-value for within-group comparison. ** Abbreviations: VCAM=Vascular Cell Adhesion Molecule-1; TNF-RI=Tumor Necrosis Factor Receptor-1; TNF-RII=Tumor Necrosis Factor Receptor-2; hsCRP=High-sensitivity C-reactive protein; oxLDL=Oxidized LDL.
Table 3.
Annualized change in trunk fat, total fat, and lean body mass.
| TRUNK FAT | TOTAL FAT MASS | TOTAL LBM | ||||||||||
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |||||||
| COVID Status (+ vs -) | -762.9 ± 279.02 | (0.01) | -895.8 ± 301.6 | (0.004) | -1364.3 ± 484.2 | (0.2) | -1607.6 ± 523.7 | (0.2) | -1039.4 ± 269.7 | (0.0002) | -963.3 ± 293.0 | (0.001) |
| VCAM | -1.02 ± 0.42 | (0.02) | -1.1 ± 0.42 | (0.01) | -1.97 ± 0.72 | (0.2) | -2.11 ± 0.72 | (0.2) | -0.7 ± 0.41 | (0.1) | -0.7 ± 0.41 | (0.1) |
| TNF-RI | -0.06 ± 0.4 | (0.9) | 0.17 ± 0.4 | (0.7) | -0.4 ± 0.7 | (0.6) | -0.05 ± 0.7 | (0.9) | -0.6 ± 0.4 | (0.1) | -0.2 ± 0.4 | (0.6) |
| TNF-RII | -0.14 ± 0.1 | (0.1) | -0.06 ± 0.1 | (0.5) | -0.3 ± 0.2 | (0.4) | -0.13 ± 0.2 | (0.6) | -0.13 ± 0.1 | (0.1) | -0.02 ± 0.1 | (0.8) |
| hsCRP | 0.03 ± 0.01 | (0.01) | 0.03 ± 0.01 | (0.01) | 0.03 ± 0.02 | (0.3) | 0.04 ± 0.02 | (0.04) | 0.01 ± 0.01 | (0.2) | 0.02 ± 0.01 | (0.1) |
| D-dimer | -0.003 ± 0.07 | (0.9) | -0.01 ± 0.1 | (0.8) | -0.03 ± 0.1 | (0.8) | -0.04 ± 0.1 | (0.8) | -0.04 ± 0.1 | (0.6) | -0.04 ± 0.1 | (0.6) |
| oxLDL | 0.004 ± 0.01 | (0.4) | 0.01 ± 0.01 | (0.1) | 0.01 ± 0.01 | (0.5) | 0.02 ± 0.01 | (0.3) | -0.001 ± 0.01 | (0.8) | 0.003 ± 0.01 | (0.5) |
*Adjusted models included COVID and HIV status, age at DXA 1, sex, race, and the difference between pre-pandemic and post-pandemic markers of inflammation; ** Abbreviations: VCAM=Vascular Cell Adhesion Molecule-1; TNF-RI=Tumor Necrosis Factor Receptor-1; TNF-RII=Tumor Necrosis Factor Receptor-2; hsCRP=High-sensitivity C-reactive protein; oxLDL=Oxidized LDL.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



