
Submitted:
21 March 2024
Posted:
22 March 2024
You are already at the latest version
Abstract
Heart failure (HF) affects about 60 million people worldwide, making it one of the chronic conditions with the greatest health and economic impact. The primary objective was to assess the efficacy of lung ultrasound (LUS) in the management of HF in order to intervene early and reduce the rate of hospital readmissions. A systematic search was conducted on PubMed, Embase, Google Scholar, Web of Science, and Scopus, including clinical trials, meta-analysis, systematic reviews, and original articles from 2019/1/1-2023/12/31, about LUS for the assessment of HF, on an outpatient basis, for HF diagnosis or/and decompensation. There may be risk of bias because the effects are dependent on the persons delivering the intervention. The results were synthetized by PRISMA method. A total of 873 articles were identified of which 33 articles were selected: [n=19] focused on prognostic assessment of HF, [n=11] centred on multimodal diagnostic assessments, and [n=2] addressing therapeutic guidance for HF diagnosis. LUS exhibits advantages in the detection of sub-clinical congestion linked to prognostic significance in re-admission and mortality during out-patient follow-up, after hospital discharge, and in complex scenarios as the patients' homes or institutional long-term care facilities. However, there are considerable uncertainties in their interpretation and monitoring changes due to its lack of standardization. The need for an updated international consensus on the use of LUS seems obvious.
Keywords:
Lung ultrasound
; Heart Failure
; B-lines
; prognosis
; mortality
; hospital admissions
; Primary care.
Introduction
The demographic evolution in developed countries is characterized by the emergence of new and complex health needs due to chronic multimorbidity. One of the conditions with the greatest impact is heart failure (HF). Heart failure is a growing problem globally, with a prevalence that is expected to increase in the coming years due to population aging, the increase in cardiovascular risk factors, and improvements in the management of acute cardiovascular events [1]. Currently, it affects about 60 million people worldwide, making it one of the chronic conditions with the greatest health and economic impact [2]. It is estimated that one in five people will develop heart failure at some point in their life [3]. There is a great variability in epidemiological studies, but its prevalence increases with age being higher than 10% in patients over 70 years old and >14% in those over 75 years old [4,5,6]with an average incidence of 2-6 cases per 1000 inhabitants. In Spain, the estimated hospitalization rate is 2.37, with an average stay of 8.5 days and accounts for between 3% and 5% of hospital admissions [7]. The 30-day readmission rate is 20% [1] being the leading cause of hospitalization in patients over 65 years old and the third leading cause of cardiovascular mortality up to 20%. A 55-70% of patients die within 5 years of diagnosis with a mortality rate of 20% per year, 50% at 5 years, and up to 80% at 10 years [8,9,10,11,12,13,14,15,16,17,18,19]. Each new hospitalization increases the mortality risk of these patients by 20%, so avoiding severe decompensation is considered crucial. Hospitalization is the inevitable consequence of this decompensation. Finally, around 40% patients are discharged from HF hospitalization prematurely when they are not ready to be discharged [20].
Studies predict that hospital admissions for heart failure will increase by 50% in the next 25 years [21] with re-hospitalization rates of up to 50% per year. Each hospitalization is a step backwards in the quality of life of patients with heart failure, and no cost-efficient solutions exist that can adequately screen, diagnose and monitor HF. The survival rate for heart failure has plateaued in the last 7 years, suggesting that additional measures are needed in addition to pharmacological treatments [2]. New therapeutic targets have allowed modifying the natural history of heart failure in the last three decades, but mortality rates and recurrent hospitalizations remain very high in patients with HF. Despite these numbers, heart failure is still a relatively unknown disease, with a range of symptoms that many affected individuals initially attribute to other causes, delaying their diagnosis and treatment and, with it, their prognosis. As a result the HF, either alone or in combination with cardiovascular comorbidities, will be one of the main health and economic burdens on the European population.
Since 1997 [22] Lung ultrasound (LUS) technology has become widely used to assess alveolar-interstitial syndrome, which encompasses pulmonary congestion of cardiac origin. B-lines, also known as ultrasound lung comets, are vertical artefacts that appear on ultrasound imaging of the lungs. These lines were associated with interstitial syndrome, a condition characterized by fluid in the interstitial spaces of the lung, and the researchers started recognizing the significance of B-lines in the context of heart failure. The integration of lung ultrasound into Focused Cardiac Ultrasound (FOCUS) was relevant because pulmonary congestion is a common feature of heart failure. In the 2010s, studies supporting the utility of lung ultrasound in heart failure began to accumulate. This led to the inclusion of lung ultrasound in some clinical guidelines for the assessment of heart failure patients. Technological advancements, including portable and handheld ultrasound devices, made it more feasible to perform lung ultrasound at the point of care, allowing for quicker and more widespread implementation. The broader adoption of point-of-care ultrasound (POCUS) facilitated the use of lung ultrasound for rapid and bedside assessment of heart failure in intensive care and emergency settings, for hospitalized patients before hospital discharge, and for patients with HF undergoing outpatient follow-up. Currently, lung ultrasound and its role in the early diagnosis of heart failure continues to be an active area of research and clinical practice.
The knowledge and utilization of LU in primary care are expanding as a clinical support tool for diagnosing and monitoring heart failure. This growth is based on published findings related to the outcomes of implementing a transitional care program between hospitals and primary care [23]. Close follow-up in the first 6 weeks after discharge for an acute HF hospitalization is recommended to reduce HF readmission or all-cause death, and during the follow-up visits, particular attention should be paid to symptoms and signs of congestion [24]. This technique may represent a useful and non-invasive method to track dynamic changes in pulmonary congestion. Furthermore, residual congestion at the time of discharge in acute HF or in ambulatory patients with chronic HF may identify those at high risk for adverse events [25]. Through continuous development and application, lung ultrasound has been proved to be of value in the diagnosis of AHF in recent years, providing clinicians with a simple, rapid, mobile and noninvasive tool [26,27,28]. Also, lung ultrasound has shown better accuracy than physical examination and lung X-ray for the diagnosis of pulmonary congestion, even when performed by physicians lacking training in the method or physicians other than radiologists [29,30]; and it adds value to neuropeptides [brain natriuretic peptide (BNP) and NTpro-BNP] for the diagnosis [31] prognosis and treatment of patients with decompensated HF. There is no evidence about similar effects with the use of CA19 new biomarker. It can be utilized as an indirect prognostic marker during the first three months following hospital discharge, aiming to identify patient subgroups that may benefit from earlier and/or more depletive treatment following an episode of acute heart failure minimizing adverse effects [32,33,34]
In spite of the evidence, there is no systematic implementation of LUS to monitor HF Patients in Primary Care [24]. The most studies make no distinction between HF with preserved ejection fraction (HFpEF) and reduced ejection fraction (HFrEF) subtypes, despite the fact that HFpEF represents nearly half of all heart failure admissions [35,36,37,38,39], though it is clear that the HFpEF occurs predominantly in older females and patients with more comorbidities [40,41].
A coordinated care process from hospital discharge is essential to prevent decompensation and hospital readmissions: accessibility (quick contact to resolve any doubts or report any complications), longitudinally (clinical history and synergistic coordination with hospital care units), and comprehensiveness (ultrasound that improves resolution capacity, medication adjustment, and the need for re-evaluation) are three pillars of this review. Therefore, appropriate monitoring would lead to a decrease in readmissions, costs, and mortality. Providers are incentivized to use the model to identify high-risk patients, as it allows them to intervene early and potentially prevent heart failure exacerbations [42].
This study aimed to conduct a systematic review on the impact of integrating Lung Ultrasound in the management of heart failure patients, stratified by risk, with a focus on mortality and readmissions. Currently, there is a lack of evidence regarding: 1/ the efficacy of B-lines as a determinant for hospital discharge in patients admitted for decompensated heart failure or in ambulatory follow-up settings; 2/ the prognostic significance of B-lines when combined with other commonly utilized biomarkers and risk assessment tools in monitoring HF patients; 3/ the existence of indications or guidelines for employing the predictive value of B-lines to guide outpatient therapeutic interventions during episodes of HF decompensation. The hypothesis is that LUS during follow-up in primary care will reduce the combined risk of worsening heart failure and/or cardiovascular death as well as symptoms and functional status in patients with heart failure regardless of their ventricular function.
Methods and Analysis
Host Organization: The Foundation University Institute for Primary Health Care Research Jordi Gol i Gurina (IDIAPJGol). Ethics Committee number 22/143-P
Faculty or Research Center: University Institute for Primary Health Care Research Jordi Gol i Gurina (IDIAPJGol) and Ebrictus Research Group.
1.1. Search strategy. A systematic search was conducted for scientific articles on PubMed, Embase, Google Scholar, Web of Science, and Scopus, including clinical trials, randomized controlled trials, meta-analysis, systematic reviews, and original articles that were related to the prognostic value of lung ultrasound in patients with HF from 2019/1/1 - 2023/12/31. The Boolean operator AND was used to combine the keywords and narrow down the search. Keywords include: Prognostic scores/Congestive heart failure/Cardiac insufficiency/Heart decompensation/ Heart Failure/ Pulmonary Congestion/ Lung ultrasound/B-lines/Pulmonary echocardiography/Transthoracic echocardiography/ cardiopulmonary ultrasound/Echocardiographic assessment of the lungs/Lung diagnostic imaging/ Ultrasonography Lung/ Transitional care/Readmissions/Mortality.
Further, we manually searched for relevant studies in a reference list of potentially eligible publications. The search in the literature was performed in February 2024. The articles were selected in two steps. In the first, the abstracts were checked and those not meeting the inclusion criteria were excluded. In the second step, the studies selected based on their abstracts were fully read, and those not meeting the inclusion criteria were excluded, according to the PRISMA model (Figure 1). Two researchers independently conducted a comprehensive search of biomedical literature databases, using a combination of subject terms and free words as well snow-ball methodology.
1.1. Inclusion and Exclusion Criteria: All Qualifying Studies Should Meet the Following Criteria: Articles Approaching LUS Managed by Physicians for the Assessment of Congestion in Patients with HF, Followed up on an Outpatient Basis at Their Primary Care Center, and Those Discharged from Hospital for New HF Diagnosis or/and Decompensation; with Preserved Heart Failure.
The gold standard for inclusion was the clinical diagnosis of heart failure by cardiologists or experienced physicians combined with history and relevant clinical examination; the language of the included literature was English; there is no restriction on the type of ultrasound instrument and the method of zonal lung ultrasound scanning, and the location of pulmonary ultrasound examination. The studies were excluded if they met the following criteria: duplicate publications; conference reports, editorials, letters, and case reports were excluded; studies with a sample size of <30 cases, severely reduced ejection fraction (LVEF ≤35%). The LUS may be employed in various scenarios, including emergency situations, as a treatment guide for in-patients, during hospital discharge, and for out-patient follow-up, but the studies using LUS in hospitalized participants were excluded except when was used around 72h from hospital discharge and ambulatory follow-up.
Results were organized according the management process in heart failure: Risk/ early-diagnosis-/follow-up/multimodal assessments/therapeutic guide:
1/ LUS accuracy in Heart failure diagnosis in out-patient settings, follow-up, and risk scores related to outcomes.
2/ Multimodal assessments added to LUS. Modalities of different evaluation (imaging radiography, computerized tomography, bioelectrical impedance analysis (BIA), laboratory biomarkers, and echocardiographic parameters) in heart failure diagnosis and follow-up.
3/ Lung ultrasound as therapeutic guide to assessing lung congestion in out-patient settings.
2.3. Data Extraction and Analysis: the Data Were Extracted, by Two Researchers Independently in a Standardized Way, and Then Cross-Checked the Results. In Case of Disagreement, Discussion or Decision by a Third Person Will Be Carried Out. The Main Extraction Contents Included: First Author, Publication Year, Objectives, Study Design, Methodology (Participants and Instruments), Outcomes, and Main Results. 2.4. Quality Assessment Was Performed Using The Newcastle-Ottawa Scale [43]. Publication Bias Deeks Funnel Plot Asymmetry Test Was Used to Determine whether There was Publication Bias. P < .05 Was Considered Statistically Significant.
3. Results
Figure 1 illustrates the search strategy employed. The present review included a total of 32 articles: 19 focused on the follow-up and prognostic assessment of heart failure, 11 centered on multimodal diagnostic assessments, and 2 addressing therapeutic guidance for heart failure diagnosis in the outpatient setting, encompassing diagnostic, therapeutic, and prognostic defined values.
Figure 1.
Results searching strategy.
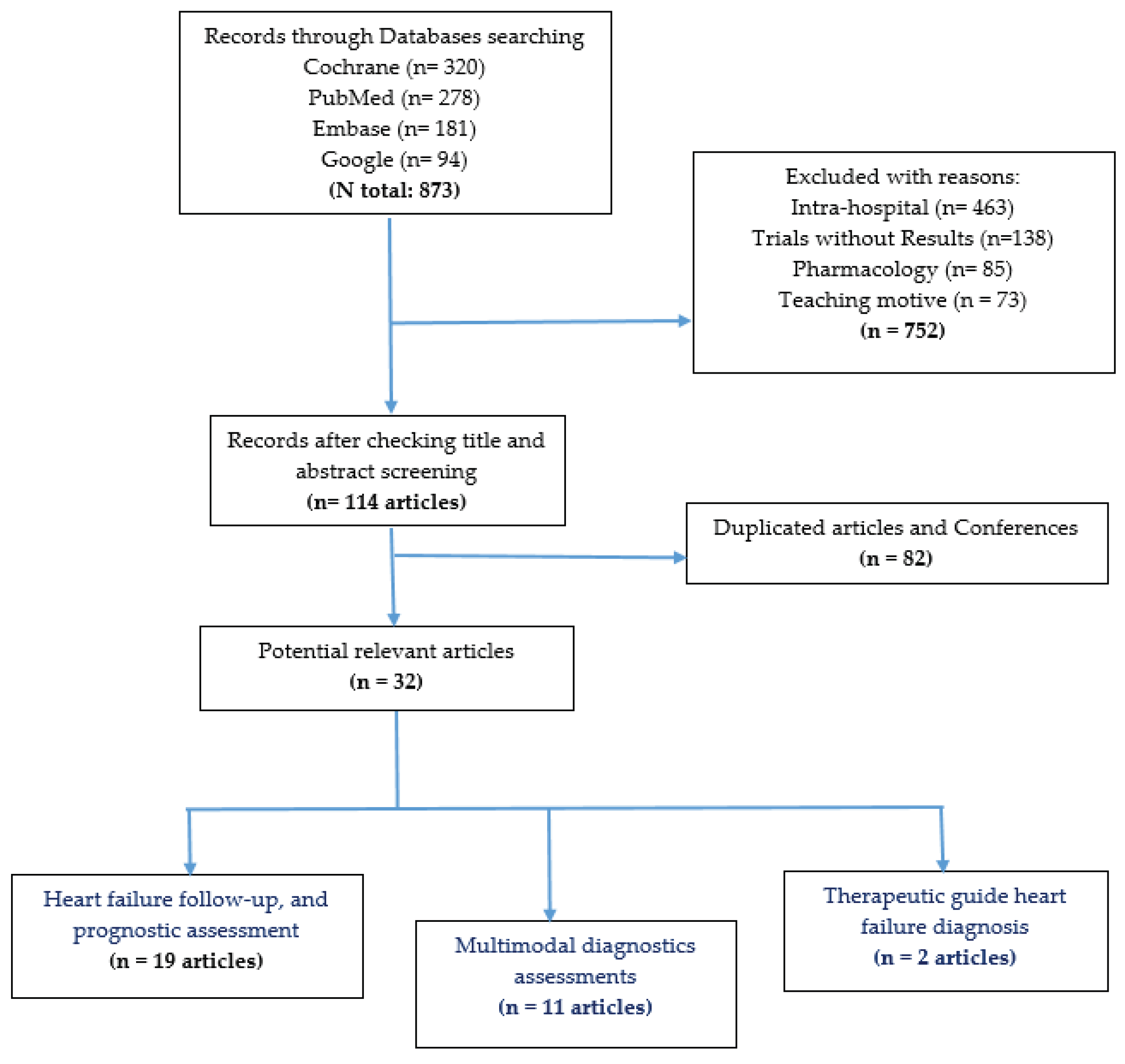
Table 1 includes the chosen articles focusing on the precision of LUS as diagnostic tool as well prognostic criteria of readmission and/or all-cause death after hospital discharge of patients admitted due to an episode of decompensated heart failure and/or ambulatory following-up:
1/ Diagnostic Accuracy in Heart Failure (HF) Suspicion [49,61]: LUS examinations were conducted on specific thoracic areas, including two anterior (A), two lateral (L), and two posterior (P) areas per hemithorax. An area was considered positive if three or more B-lines were observed. Diagnostic accuracy was determined by the number of positive areas identified: two positive areas out of four (Anterior-Lateral) on each hemithorax and two positive areas out of six (A-L-P) on each hemithorax. It was showed that incorporating LUS results may enhance the predictive capability of contemporary HF risk scores [54]. However, the impact of repeated ultrasound scans on prognostic outcomes remains uncertain [58].
2/ LUS in Stable Chronic HF Patients: LUS was effective in identifying stable chronic HF patients at high risk of death or HF hospitalization. At discharge, approximately 48.2% of patients exhibited a normal LUS profile [44,56]. The prognostic significance of the number of B-lines varied across studies. Most studies indicated that a sum of ≥5 B-lines was associated with a higher probability of 12-month all-cause death, and ≥15 B-lines with higher probability of HF readmission [45,50,51,52,56,61,65]. Others [57] suggested that the presence of 30-40 B-lines at admission was a risk factor for readmission or mortality, and the presence of ≥15 B-lines could indicate just an increased risk of persistent pulmonary congestion. Each additional B-line was associated with a 1.82 odds ratio for adverse outcomes [44] with a 3% to 4% increased risk for each 1-line addition [50].
3/ LUS-Guided Treatment: LUS-guided treatment was linked to a 45% reduction in the risk of hospitalization and a decrease in urgent visits [46,47,54,55,58] with follow-up since three months, six months up to one year. However, no significant differences in death rates were observed [46,47,55]. Additionally, LUS-guided treatment was associated with a lower risk of Major Adverse Cardiac Events (MACEs) [59,60]. Nonetheless, while LUS improved fluid status with a significantly greater reduction in the number of B-lines during the first 48 hours, it did not reduce heart failure readmission [53,55,62].
4/ The results of LUS remained independent of NT-proBNP levels [32,48,49,50]. It seems there is any statistically significant association between median NT-proBNP levels among patients with a positive LUS for congestion and basal median NT-proBNP levels in patients with LUS without signs of congestion.

Table 1.
B-lines AND Heart Failure vs outcomes.
| First Author Year of publication Country |
Objectives | Methods | Results | |||
|---|---|---|---|---|---|---|
| Design |
Participants | Instruments, procedure | Outcomes | |||
|
Platz E et al 2019 (EEUU) [44] |
To assess the prevalence, changes in, and prognostic importance of B-lines | Prospective, observational study | N= 349 | 4-zone LUS was performed at discharge. B-lines were quantified off-line, blinded to clinical findings and outcomes. | Risk of HF hospitalization or all-cause death | The OR ratio for each B-line was 1.82 (95% CI 1.14 to 2.88; p = 0.011) after adjusting for important clinical variables. |
|
Kobalava Zh D et al 2019 (Russia) [2,45] |
To assess the prognostic significance of B-lines number at discharge. | Observational descriptive | N= 162 | B lines at hospital discharge | Probability of 12-month all-cause death and probability of HF readmission. | At discharge normal LUS profile was observed in 48.2% of patients. Sum of B-lines ≥5 was associated with higher probability of 12-month all-cause death ([HR] 2.86, 95% CI 1.15-7.13, p=0.024); and B-lines ≥15 B-lines with higher probability of HF readmission (HR 2.83, 95%CI 1.41-5.67, p=0.003). |
| Marini et al 2020 (Italy) [3,46] | To evaluate the usefulness of LUS+physical examination (PE) in the management of outpatients with acute decompensated heart failure (ADHF). | Randomized, multicenter, and unblinded study | N =244 | PE+LUS' group vs 'PE only' group. | Hospitalization rate for ADHF at 90-day follow-up. | The hospitalization was significantly reduced in 'PE+LUS' group with a reduction of risk for hospitalization by 56% (p=0.01). There were no differences in mortality between the two groups. |
| Araiza-Garaigordobil et al 2020 (Mexico) [4,47] | LUS during follow-up of patients with HF may reduce the rate of adverse events compared with usual care. | Randomized, single-center, blinded, and controlled trial CLUSTER-HF study |
N =126 | LUS vs usual care | Urgent visits, rehospitalization for worsening HF, and death from any cause during a 6-month period. | LUS-guided treatment was associated with a 45% risk reduction for hospitalization (HR 0.55, 95% CI 0.31-0.98, p=0.044), and reduction in urgent visits (HR 0.28, 95% CI 0.13-0.62, p = .001). No significant differences in death were found. |
| Rivas-Lasarte M et al 2019 (Spain) [5,48] | To evaluate relationship between results LUS-guided follow-up protocol and reduction NT-proBNP. | Randomized, single-blind clinical trial. | N = 123 | A standard follow-up (n = 62, control group) or a LUS-guided follow-up (n = 61, LUS group) |
urgent visit, hospitalization and death, at 14, 30, 90 and 180 days after discharge | Reduction the number of decompensations and improved walking capacity, but N-terminal pro-B-type natriuretic peptide reduction were not achieved. |
| Conangla et al 2020 (Spain) [6,49] |
LUS improved diagnostic accuracy in HF suspicion. | Prospective study of LUS in ambulatory patients >50 years old | N =223 | LUS was performed on 2 anterior (A), 2 lateral (L), and 2 posterior (P) areas per hemithorax. An area was positive when ≥3 B-lines were observed. | Two diagnostic criteria were used: for LUS-C1, 2 positive areas of 4 (A-L) on each hemithorax; and for LUS-C2, 2 positive areas of 6 (A-L-P) on each hemithorax. | LUS was accurate enough to rule-in HF in a primary care setting irrespective NT-proBNP availability. |
| Domingo M, et al 2021 (BCN) [7,50] |
The prognostic value of LUS. | Observational, prospective, single-center cohort study | N =577 | LUS was performed in situ. The sum of B-lines across all lung zones and the quartiles of this addition were used for the analyses. | The main clinical outcomes were a composite of all-cause death or hospitalization for HF and mortality from any cause during mean follow-up of 31±7 months. |
The mean number of B-lines was 5±6. Having ≥ 8 B-lines doubled the risk of the composite primary event (p <0.001) and increased the risk of death from any cause by 2.6-fold (p <0.001) with a 3% to 4% increased risk for each 1-line addition irrespective NT-proBNP level. |
| Wang Y et al 2021 (Brasil) [8,51] | Prognostic value of lung ultrasound assessed by B-lines | A Systematic Review and Meta-Analysis |
Nine studies involving N =1,212 | HF outpatients | Outcomes of all-cause mortality or HF hospitalization | B-lines > 15 and > 30 at discharge were significantly associated with increased risk of combined outcomes |
| Rueda-Camino JA et al 2021 (Spain) [9,52] |
To determine the diagnostic accuracy of bedside LUS prognostic tool for HF suspicion | Prospective cohort study | ?? | B lines: two groups were formed: less than 15 B-lines (unexposed) and ≥15 B-lines (exposed). | Risk of readmission and mortality with 3-month follow-up | Patients with ≥15 B-lines are 2.5 times more likely to be readmitted (HR: 2.39; 95%CI: 1.12-5.12; P=.024), without differences in terms of mortality. |
| Zisis G et al 2022 (Australia) [10,53] |
To evaluate the efficacy a nurse-led, LUICA-guided disease management program (DMP) | RISK-HF randomized controlled trial | N = 404 | Patients at high risk for 30-day readmission and/or death to LUS-guided DMP or usual care. | LUS was performed at discharge and at least twice in the first month of follow-up | Handheld ultrasound at and after hospital discharge improves fluid status but does not reduce heart failure readmission. |
| Maestro-Benedicto, A et al 2022 (Spain) [11,54] |
contemporary HF risk scores can be improved upon by the inclusion of the number of B-lines detected by LUS | Randomized, single-center, simple blind trial | N = 123 | LUS at discharge contemporary HF risk scores at 15 days, 1, 3 and 6 months after the hospitalization |
predict death, urgent visit, or HF readmission at 6- month | Adding the results of LUS evaluated at discharge improved the predictive value of most of the contemporary HF risk scores in the 1-month score and 1-year. |
| Mhanna M et al. 2022 (EEUU) [12,55] |
A point-of-care lung ultrasound (LUS) is a useful tool to detect subclinical pulmonary edema. | Systematic review and meta-analysis |
N = 493 | LUS plus PE-guided therapy vs. managed with PE-guided therapy alone | HF hospitalization, all-cause mortality, urgent visits for HF worsening, acute kidney injury (AKI), and hypokalemia rates. | Outpatient LUS-guided diuretic therapy of pulmonary congestion reduces urgent visits for worsening symptoms of HF. No significant difference in HF hospitalization rate. Similarly, there was no significant difference in all-cause mortality, and hypokalemia. |
| Rattarasan I et al. 2022 (Thailand) [13,56] |
Evaluate the prognostic value of B-lines for prediction of rehospitalization and death | Prospective cohort | N = 126 | B-lines and the size of the inferior vena cava. Two groups were formed: B-lines (< 12) vs B-lines (≥ 12) | Prediction of readmission hospitalization and death within 6 months | The mean number of B-lines at discharge was 9 ± 9, and the presence ≥ 12 B-lines before discharge was an independent predictor of events at 6 months |
| Dubon-Peralta E et al. 2022 (Spain) [14,57] |
assessment of pulmonary congestion in patients with heart failure | A systematic review |
14 articles | evaluate the prognostic significance of the presence of B lines detected by LUS | Optimization of treatment by monitoring the dynamic changes | The presence of more than 30-40 B lines at admission were considered a risk factor for readmission or mortality as was persistent pulmonary congestion with the presence of ≥15 B-lines. |
| Arvig MD et al. 2022 (Denmark) [15,58] |
investigate if treatment guided by serial LUS compared to standard monitoring | Systematic search | 24 studies N = 2,040 | serial LUS of the inferior vena cava-collapsibility index (IVC-CI) and B-lines on LUS | mortality, readmissions | A single ultrasound measurement can influence prognostic outcomes, but it remains uncertain if repeated scans can have the same impact. |
| Yan Li et al 2022 (China) [16,59] |
to evaluate the usefulness of LUS-guided treatment vs. usual care in reducing the major adverse cardiac event (MACE) rate | systematic review and meta-analysis of randomized controlled trials | 10 studies N= 1,203 | LUS-guided treatment vs. usual care a, LUS-guided treatment | MACEs, all-cause mortality, and HF-related rehospitalization, during mean follow-up of 4.7 months | The meta-regression analysis showed a significant correlation between MACEs and the change in B-line count (p < 0.05). LUS-guided treatment was associated with a significantly lower risk of MACEs. |
| Platz E et al. 2023 (EEUU) [17,60] |
PARADISE-MI Assess the trajectory of pulmonary congestion using lung ultrasound (LUS) |
Prospective cohort study | N = 152 | LUS underwent 8-zone LUS and echocardiography at baseline (±2 days of randomization) and after 8 months. | Patients with acute myocardial Left ventricular ejection fraction, pulmonary congestion or both | The proportion of patients without pulmonary congestion at follow-up was significantly higher in those with fewer B-lines at baseline |
| Cohen et al 2023 (New York) [18,61] |
Association between numbers of B-lines on LUS. | Prospective study of adults | 200 patients at discharge | Number of B-lines. By an 8-zone LUS exam to evaluate for the presence of B-lines |
Risk of 30-day readmission in patients hospitalized for acute decompensated HF. | The presence of B-lines at discharge was associated with a significantly increased risk of 30-day readmission. Compared with patients with 0-1 positive zones, patients with 2-3 positive lung zones was 1.25 times higher (95% CI: 1.08-1.45), and with 4-8 positive lung zones was 1.50 times higher (95% CI: 1.23-1.82. |
| Goldsmith AJ et al 2023 (EEUU) [19,62] |
BLUSHED-AHF study: to explore whether LUS early targeted intervention vs leads improves pulmonary congestion | Multicenter, randomized, pilot trial | N = 130 | LUS-guided protocol | Number of B-lines at 6 hours or in 30 days | LUS conferred no benefit compared with usual care in reducing the number of B-lines at 6 hours or in 30 days, but a significantly greater reduction in the number of B-lines was observed in LUS-guided patients during the first 48 hours. |
Table 2 encompasses selected articles concentrating on the LUS in conjunction with other commonly used assessments. These include clinical assessment versus chest radiography with or without inferior vena cava (IVC) ultrasound, LUS versus computerized tomography (CT), Rx thoracic, bioelectrical impedance analysis (BIA), early diagnosis through exercise LUS, laboratory parameters (pro-BNP, CA125), and echocardiographic parameters.
The LUS showed higher sensitivity ratio 1.2 (95% CI, 1.08-1.34; p < 0.001) compared with CxR [62,63,71], computerized tomography (CT) , and echocardiogram [74] in the diagnosis of HF, and using LUS with the clinical evaluation reduced diagnostic errors as compared to [CxR+Nt-proBNP] combination [64]. However, mortality was associated to significantly lower IVC collapse [65,70,71], and a greater number of lung B-lines; and higher NT-proBNP levels [65,68,69,70] without differences in the BIA parameters. Among the most individuals with ambulatory follow-up and preserved ejection fraction [66,73], the submaximal exercise increases B-lines number to level of higher probability of 12-month all-cause death or/ and higher probability of HF decompensation [45,50,51,52,56,61]. Total B-line sum correlated significantly, although moderately, with congestion and several inflammation biomarkers. Unexpectedly, the highest correlation found was with high-sensitive Troponin T (hsTnT) [67].
Table 3 includes a residual section featuring articles on LUS and therapeutic guidance based on the presence of lung ultrasound signs of congestion in ambulatory patients. Few studies have been found regarding the utility of Lung Ultrasound (LUS) as a guide for heart failure (HF) treatment in the context of outpatient follow-up, and the results obtained do not support the use of LUS in relation to its mortality and/or hospital readmission outcomes [75]. Although in clinical practice there was a higher likelihood of modifying diuretic treatment based on Lung Ultrasound (LUS) results, no differences were observed in the incidence of adverse events related to heart failure (HF) [75,76].
Discussion
This systematic review was conducted with the objective of identifying scientific evidence pertaining to the application of Lung Ultrasound in Heart Failure. Despite encountering a substantial number of trials lacking posted results, the review exhibits notably advantageous in the detection of sub-clinical congestion linked to prognostic significance in terms of re-hospitalization, as indicated by the prognostic value associated with B-lines, and mortality prediction. Both of which constitute pivotal attributes of heart failure in out-patient settings. The enhanced accuracy, surpassing that of physical examination and chest X-ray by 90%, establishes LUS as a superior diagnostic modality for congestion, and facilitates expedited diagnoses in the emergency department. Additionally, it confers incremental prognostic value during the hospital discharge phase of patients experiencing decompensated HF, and it may play a pivotal role in guiding the treatment strategies for individuals with HF.
However, despite the extensive evidence supporting the use of LUS across various medical disciplines, there is a notable scarcity of information regarding its application and interpretation criteria in the outpatient monitoring of HF patients within primary care settings. This knowledge gap persists despite the significant healthcare and economic challenges posed by the aging demographics of society. Recognizing the evolving landscape, a multidisciplinary panel comprising international LUS experts from six countries, encompassing various clinical and technical backgrounds, undertook a thorough review and update of the original international consensus on point-of-care LUS, initially established in 2012 [77,78]. Also has been published a statement aimed at pulmonologists utilizing thoracic ultrasound within the realm of respiratory medicine [79]. The updated consensus reflects the advancements in LUS technology and its applications, providing a contemporary framework for practitioners. Despite these strides, there remains a need for further research and exploration, particularly in the context of outpatient monitoring of HF patients in primary care.
In fact, international clinical practice guidelines on heart failure do not include standardized interpretation criteria for the predictive value of B-lines associated with intervention patterns, differential diagnosis, and the potential benefit of its use in terms of cost-effectiveness. Despite a recommendation (Class I, level B) by the ESC Guidelines [14,24], which suggests an intensive strategy involving the initiation and rapid up-titration of evidence-based treatment before discharge, along with frequent and careful follow-up visits in the first 6 weeks following heart failure hospitalization to reduce the risk of HF rehospitalization or all-cause death at 180 days, it does not specifically advocate the use of lung ultrasound for detecting pulmonary congestion in outpatients with heart failure. Furthermore, approximately 40% of patients are discharged prematurely from HF hospitalization when they may not be adequately prepared for discharge [20].
In the studies that were included, although they present similar results, there are some limitations such as their interpretation, highlighting the challenges in establishing their utility as valuable and non-invasive tools for monitoring changes in pulmonary congestion. These limitations include the absence of studies conducted in comparable populations and the inconsistent reporting of the technique employed and variable quantification of 'B-lines to guarantee the reproducibility of LUS studies,' have all made it difficult to compare published reports. Additionally, there is diversity in the healthcare areas from which the results originate, the dynamic nature of LUS findings in response to therapy, and differences in severity of disease complexity between healthcare levels. This includes interpretability challenges, especially between hospital care and outpatient follow-up in primary care.
Notably, the persistence of residual congestion at the time of hospital discharge serves as an indicator for individuals at heightened risk for adverse events [44,49,50,80]. On the other hand, the observation that in most individuals undergoing ambulatory follow-up with preserved ejection fraction [26,33], submaximal exercise increases the number of B-lines to a level associated with a higher probability of 12-month all-cause death and/or a higher likelihood of heart failure decompensation [2,15,20,911] may be an uncertain finding in terms of its prognostic value and implications for treatment. Recognizing the importance of early diagnosis, particularly in light of its contribution to the prompt implementation of appropriate treatment, is crucial for mitigating heart failure mortality. Finally, there is increased controversy concerning the effectiveness and correlation of changes in the B-lines pattern with monitoring congestion during optimizing therapy, serving as a guide in the outcomes and use of diuretics. Diuretics are considered one of the more affordable treatment approaches in the primary care setting. The need for an updated international consensus on the use of LUS is obvious [81].
Therefore, there are several potential benefits of using LUS to monitor heart failure patients in primary care:
a/ LUS can detect changes in lung function in heart failure patients before they become clinically apparent. Several studies have correlated the presence of B-lines on LUS with a sensitive marker for the diagnosis of decompensated HF; however, B-lines are not an exclusivity of decompensated HF. Residual pulmonary congestion at discharge, as assessed by a B-line count ≥30, is a strong predictor of outcome, though in an HF outpatient clinic, a B-line ≥15 cutoff could be considered for a quick and reliable assessment of decompensation in outpatients with HF [41,80]; and that the B-line pattern usually disappears after proper treatment of acute HF. This early detection can help clinicians intervene earlier, potentially reducing the severity of the patient's condition and preventing the need for hospitalization [1,41,82]. It should not be considered a substitute for imaging technology but rather a complementary tool in emergency and outpatient assessments.
b/ The implementation of lung ultrasound in primary care not only facilitates early detection of changes in lung function and improves patient outcomes but also promotes increased patient engagement [39,40,67]. This patient-centric approach, coupled with the non-invasive and cost-effective nature of lung ultrasound, represents a promising avenue for enhancing the overall quality of care for heart failure patients in primary care settings.
Inici del formulari
c/ As the population ages globally, there is a simultaneous increase in the prevalence of multiple comorbidities. The convergence of these demographic and health trends poses unique challenges for the healthcare system. It becomes increasingly essential to address the healthcare needs of older individuals who may have complex medical conditions and varying degrees of mobility. The LUS has an incremental value in follow-up, the diagnostic and prognostic approach in potential complex scenarios as the bedside in non-traditional healthcare settings such as patients' homes or institutional long-term care facilities. The early detection capabilities of LUS empower clinicians to intervene at an earlier stage, potentially mitigating the severity of the patient's condition and averting the need for readmission [1,82]. This proactive approach to post-hospitalization care aligns with the goals of improving patient outcomes and reducing the burden on healthcare resources.
d/ Non-invasive and cost-effective: Lung ultrasound is a non-invasive and cost-effective method of monitoring heart failure patients. Unlike other diagnostic tests, such as CT scans, it does not expose patients to radiation and is more affordable [1,80]. Though the echocardiography plays a pivotal role in evaluating underlying cardiac structure and function, is highly dependent on the experience of the sonographer for image acquisition, and precise interpretation by an expert reader. As a result, are being developed several Machine Learning-based platforms.
e/ The studies found that lung ultrasound was more accurate than clinical assessment, natriuretic peptides, and echo-Doppler cardiac parameters for detecting pulmonary congestion. Additionally, patients who received lung ultrasound as part of their care had a lower risk of death and hospitalization than those who did not [48,67,80]. Additionally, there were weak [83] or moderate [24] correlations were found between serum biomarkers and LUS scores.
f/ Not just as pharmacologic therapeutic guide, but also LUS is used in other clinical areas such as: out-patient, pre- and per-operative, hemodialysis, septic shock, cardiogenic shock, teach-back educational, pediatric, etc…
Moreover, it must be considered the development of new research about LUS in various objectives, including: 1/Integrating LU technology into primary care to monitor patients at high and moderate risk of hospitalization or mortality due to heart failure. Additionally, using LU technology for post-hospital discharge follow-up of heart failure patients to detect decompensation early; 2/ creating a predictive model that utilizes selected features to forecast the likelihood of heart failure decompensation. This could involve employing a risk score or Artificial Intelligence as a predictive model to enhance early detection and enable timely interventions 3/Assessing the accuracy and performance of the predictive model in a cost-effective manner using a validation dataset; 4/ Identifying high-risk subgroups within the patient population 5/ Exploring gender-associated differences in the context of heart failure; 6/ Coordinating efforts between primary care and the Heart Failure Unit for the comprehensive follow-up of heart failure patients. It is surprising that LUS is neither systematically incorporated as part of routine hospital discharge, nor as clinical activities in primary care in follow-up and early diagnosis of decompensation.
Conclusions
The LUS exhibits notably advantageous in the detection of sub-clinical congestion linked to prognostic significance in terms of re-hospitalization, as indicated by the prognostic value associated with B-lines, and mortality prediction., , and it may play a pivotal role in guiding the treatment strategies for individuals with HF.
Additionally in primary care, it confers incremental prognostic value during the hospital discharge phase, and prognostic approach in potential complex scenarios as the bedside in non-traditional healthcare settings such as patients' homes or institutional long-term care facilities.
There are considerable uncertainties in their interpretation, highlighting the challenges in establishing its utility as a valuable and non-invasive tool for monitoring changes in pulmonary congestion.
The need for an updated international consensus on the use of LUS seems obvious.
Author Contributions
All authors have made substantial contributions to the conception, design, and submitted version of the work; and have approved the submitted version. Their individual contributions were: "Conceptualization, A-PT, R-CA, and JL-CE; Methodology, A-PT, R-CA, M-HM, M-MS, Y-RC, and JL-CE; Software, M-HM, A-PT, and JL-CE; Validation, A-PT, JL-CE, and R-CA; Formal Analysis, A-PT, R-CA, JL-CE, and J-LN; Investigation, A-PT, M-HM, Y-RC, and R-CA; Resources, A-PT, R-CA, and JL-CE; Data Curation, A-PT. R-CA, JL-CE, M-HM, and M-MS; Writing – Original Draft Preparation, A-PT, JL-CE, and R-CA; Writing – Review & Editing, A-PT, JL-CE, and R-CA; Visualization, A-PT, JL-CE, J-LN, and R-CA; Supervision, JL-CE and R-CA; Project Administration, R-CA, and JL-CE.; Funding Acquisition, JL-CE, and J-LN.”. .
Funding
“This research received no external funding” and “The APC received partial funding through a grant to the PREFA-TE project from the Strategic Plan in Research and Innovation in Health (PERIS)”. This funding was obtained in the 2021 call under the expedient file SLT/21/000027.
Institutional Review Board Statement
“Not applicable”.
Informed Consent Statement
“Not applicable.”.
Acknowledgments
We are grateful to the clinical and administrative staff of the participating Primary Care centres. We thank the Primary Care Research Institute-IDIAP Jordi Gol, and the Fundació Dr. Ferran for their technical support on the work. Chat-GPT AI system, as a free-to-use tool, was used as a supporting tool for reviewing or considering options in the English translation of the original language.
Conflicts of Interest
"The authors declare no conflict of interest." “The APC sponsors had no role in the design, execution, interpretation, or writing of the study”.
References
- Pugliese NR, Pellicori P, Filidei F, Del Punta L, De Biase N, Balletti A, Di Fiore V, Mengozzi A, Taddei S, Gargani L, Mullens W, Cleland JGF, Masi S. The incremental value of multi-organ assessment of congestion using ultrasound in outpatients with heart failure. Eur Heart J Cardiovasc Imaging. 2023 Jan 3:jeac254. [CrossRef]
- Bragazzi NL, Zhong W, Shu J, et al. Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur J Prev Cardiol. 2021. [CrossRef]
- Savarese G, Lund LH. Global Public Health Burden of Heart Failure. Card Fail Rev. 2017 Apr; 3(1): 7–11. [CrossRef]
- Díez-Villanueva P, Jiménez-Méndez C, Alfonso F. Heart failure in the elderly. J Geriatr Cardiol. 2021 Mar 28;18(3):219-232. [CrossRef]
- Sicras-Mainar A, et al. Epidemiología de la insuficiencia cardiaca en España: estudio PATHWAYS-HF. Rev Esp Cardiol 2022; 75(1):31-38. [CrossRef]
- Martínez Santos P, et al. Mortalidad hospitalaria y reingresos por insuficiencia cardiaca en España. Un estudio de los episodios índice y los reingresos por causas cardiacas a los 30 días y al año. Rev Esp Cardiol. 2019; 72(12):998-1004. [CrossRef]
- Rodríguez-Artalejo F, Banegas Banegas JR, Guallar-Castillón P. Epidemiología de la insuficiencia cardíaca. Rev Esp Cardiol. 2004. 57(2): 163-70. [CrossRef]
- Use of Levosimendan in Patients with Advanced Heart Failure: An Update. J Clin Med. 2022 Oct 29; 11(21):6408. PMID: 36362634; PMCID: PMC9659135. [CrossRef]
- LION-HEART Study Investigators. Efficacy and safety of intermittent intravenous outpatient administration of levosimendan in patients with advanced heart failure: the LION-HEART multicentre randomised trial. Eur J Heart Fail. 2018 Jul;20(7):1128-1136. Epub 2018 Feb 6. PMID: 29405611. [CrossRef]
- A pragmatic approach to the use of inotropes for the management of acute and advanced heart failure: An expert panel consensus. Int. J. Cardiol. 2019; 297:83–90. [CrossRef]
- Advanced (Stage D) Heart Failure: A Statement from the Heart Failure Society of America Guidelines Committee. J. Card. Fail. 2015; 21:519–534. [CrossRef]
- Evolution of left ventricular assist device therapy for advanced heart failure: a review. JAMA Cardiol. 2018; 3(7):650–658.
- Registro español de trasplante cardiaco. XXXIII informe oficial de la Asociación de Insuficiencia Cardiaca de la Sociedad Española de Cardiología. Rev Española Cardiol. 2022; 75 (11):926–935.
- 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2021 Sep 21; 42(36):3599–726. Available from: . [CrossRef]
- Advanced heart failure: a position statement of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2018 Nov 1; 20(11):1505–35. Available from: . [CrossRef]
- Asistencia ventricular de larga duración en España (2007-2020). I informe del registro REGALAD. Rev Española Cardiol (2022). [CrossRef]
- Association of Clinical Outcomes With Left Ventricular Assist Device Use by Bridge to Transplant or Destination Therapy Intent: The Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy With HeartMate 3 (MOMENTUM 3) Randomized Clinical Trial. JAMA cardiology vol. 5,4 (2020): 411-419. [CrossRef]
- Long-Term Use of a Left Ventricular Assist Device for End-Stage Heart Failure. N Engl J Med [Internet]. 2001 Nov 15;345(20):1435–43. Available from: . [CrossRef]
- The European Registry for Patients with Mechanical Circulatory Support of the European Association for Cardio-Thoracic Surgery: third report. Eur J Cardio-Thoracic Surg [Internet]. 2022 Jul 1; 62(1):ezac032. Available from: . [CrossRef]
- Kleiner Shochat M, Fudim M, Kapustin D, Kazatsker M, Kleiner I, Weinstein JM, Panjrath G, Rozen G, Roguin A, Meisel SR. Early Impedance-Guided Intervention Improves Long-Term Outcome in Patients With Heart Failure. J Am Coll Cardiol. 2021 Oct 26; 78(17):1751-1752. [CrossRef]
- Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure. Eur J Heart Fail. 2020 Aug; 22(8): 1342–1356. Published online 2020 Jun 1. [CrossRef]
- Lichtenstein D, Mézière G, Biderman P, Gepner A, Barré O. The comet-tail artifact, an ultrasound sign of alveolar-interstitial syndrome. Am J Respir Crit Care Med. 1997; 156(5):1640-6.
- Al Sattouf A, Farahat R, Khatri AA. Effectiveness of Transitional Care Interventions for Heart Failure Patients: A Systematic Review with Meta-Analysis. Cureus. 2022 Sep 29;14(9):e29726. [CrossRef]
- Theresa A. McDonagh *† , (Chairperson) (United Kingdom), Marco Metra *† , (Chairperson) (Italy), Marianna Adamo ‡ , (Task Force Co-ordinator) (Italy), Roy S. Gardner ‡ , (Task Force Co-ordinator) (United Kingdom), Andreas Baumbach (United Kingdom), Michael Böhm (Germany), Haran Burri (Switzerland), Javed Butler (United States of America), Jelena Čelutkienė (Lithuania), Ovidiu Chioncel (Romania), John G.F. Cleland (United Kingdom), Maria Generosa Crespo-Leiro (Spain), Dimitrios Farmakis (Greece), Martine Gilard (France), Stephane Heymans (Netherlands), Arno W. Hoes (Netherlands), Tiny Jaarsma (Sweden), Ewa A. Jankowska (Poland), Mitja Lainscak (Slovenia), Carolyn S.P. Lam (Singapore), Alexander R. Lyon (United Kingdom), John J.V. McMurray (United Kingdom), Alexandre Mebazaa (France), Richard Mindham (United Kingdom), Claudio Muneretto (Italy), Massimo Francesco Piepoli (Italy), Susanna Price (United Kingdom), Giuseppe M.C. Rosano (United Kingdom), Frank Ruschitzka (Switzerland), Anne Kathrine Skibelund (Denmark), and ESC Scientific Document Group. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal (2023) 44, 3627–3639 . [CrossRef]
- Rivas-Lasarte M, Maestro A, Fernández-Martínez J, López-López L, Solé- González E, Vives-Borrás M, Montero S, Mesado N, Pirla MJ, Mirabet S, Fluvià P, Brossa V, Sionis A, Roig E, Cinca J, Álvarez-García J. Prevalence and prognostic impact of subclinical pulmonary congestion at discharge in patients with acute heart failure. ESC Heart Fail. 2020 Oct; 7(5):2621-2628. Epub 2020 Jul 7. PMID: 32633473; PMCID: PMC7524099. [CrossRef]
- Picano E, Scali MC, Ciampi Q, et al. Lung ultrasound for the cardiologist. JACC Cardiovasc Imag. 2018; 11:1692–705.
- Bekgoz B, Kilicaslan I, Bildik F, et al.. BLUE protocol ultrasonography in Emergency Department patients presenting with acute dyspnea. Am J Emerg Med. 2019; 37:2020–7.
- Wooten WM, Hamilton LA. Bedside ultrasound versus chest radiography for detection of pulmonary edema: a prospective cohort study. J Ultrasound Med. 2019; 38:967–73.
- Gullett J, Donnelly JP, Sinert R, Hosek B, Fuller D, Hill H, et al. Interobserver agreement in the evaluation of B lines using bedside ultrasound. J Crit Care. 2015; 30(6):1395-9.
- Chiem AT, Chan CH, Ander DS, Kobylivker AN, Manson WC. Comparison of expert and novice sonographers’ performance in focused lung ultrasonography in dyspnea (FLUID) to diagnose patients with acute heart failure syndrome. Acad Emerg Med. 2015; 22(5):564-73.
- Prosen G, Klemen P, Štrnad M, Grmec S. Combination of lung ultrasound (a comettail sign) and Nterminal probrain natriuretic peptide in differentiating acute heart failure from chronic obstructive pulmonary disease and asthma as cause of acute dyspnea in prehospital emergency setting. Crit Care. 2011;15(2):R114. Erratum in: Crit Care. 2011; 15(6):450.
- Núñez J, de la Espriella R, Rossignol P, Voors AA, Mullens W, Metra M, Chioncel O, Januzzi JL, Mueller C, Richards AM, de Boer RA, Thum T, Arfsten H, González A, Abdelhamid M, Adamopoulos S, Anker SD, Gal TB, Biegus J, Cohen-Solal A, Böhm M, Emdin M, Jankowska EA, Gustafsson F, Hill L, Jaarsma T, Jhund PS, Lopatin Y, Lund LH, Milicic D, Moura B, Piepoli MF, Ponikowski P, Rakisheva A, Ristic A, Savarese G, Tocchetti CG, Van Linthout S, Volterrani M, Seferovic P, Rosano G, Coats AJS, Bayes-Genis A. Congestion in heart failure: a circulating biomarker-based perspective. A review from the Biomarkers Working Group of the Heart Failure Association, European Society of Cardiology. Eur J Heart Fail. 2022 Oct; 24(10):1751-1766. Epub 2022 Sep 7. Erratum in: Eur J Heart Fail. 2023 Mar; 25(3):443. [CrossRef]
- Núñez J, Llàcer P, García-Blas S, Bonanad C, Ventura S, Núñez JM, Sánchez R, Fácila L, de la Espriella R, Vaquer JM, Cordero A, Roqué M, Chamorro C, Bodi V, Valero E, Santas E, Moreno MDC, Miñana G, Carratalá A, Rodríguez E, Mollar A, Palau P, Bosch MJ, Bertomeu-González V, Lupón J, Navarro J, Chorro FJ, Górriz JL, Sanchis J, Voors AA, Bayés-Genís A. CA125-Guided Diuretic Treatment Versus Usual Care in Patients With Acute Heart Failure and Renal Dysfunction. Am J Med. 2020 Mar; 133(3):370-380.e4. [CrossRef]
- Núñez J, Bayés-Genís A, Revuelta-López E, Ter Maaten JM, Miñana G, Barallat J, Cserkóová A, Bodi V, Fernández-Cisnal A, Núñez E, Sanchis J, Lang C, Ng LL, Metra M, Voors AA. Clinical Role of CA125 in Worsening Heart Failure: A BIOSTAT-CHF Study Subanalysis. JACC Heart Fail. 2020 May; 8(5):386-397. [CrossRef]
- Lekavich CL et al. Heart failure preserved ejection fraction (HFpEF): an integrated and strategic review. Heart Fail Rev. 2015; 20(6):643-53.
- Steinberg BA et al. Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: prevalence, therapies, and outcomes. Circulation. 2012; 126(1):65-75.
- Bhatia RS et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006; 355(3):260-9.
- Owan TE et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. 2006; 355(3):251-9.
- Burkhoff D. Mortality in heart failure with preserved ejection fraction: an unacceptably high rate. Eur Heart J. 2012; 33(14):1718-20.
- Shah KS et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J Am Coll Cardiol. 2017; 70(20):2476-86.
- Borlaug BA, Paulus WJ. Heart failure with preserved ejection fraction: pathophysiology, diagnosis, and treatment. Eur Heart J. 2011; 32(6):670-9.
- McDonagh T.A., Metra M., Adamo M. y cols., 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC, Eur. Heart J., 2021; 42: 3599-3726.
- Wells G SA, O'Connell D. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in Meta-analysis. [URL:http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm] Accessed 14/February/2024.
- Platz E, Campbell RT, Claggett B, Lewis EF, Groarke JD, Docherty KF, Lee MMY, Merz AA, Silverman M, Swamy V, Lindner M, Rivero J, Solomon SD, McMurray JJV. Lung Ultrasound in Acute Heart Failure: Prevalence of Pulmonary Congestion and Short- and Long-Term Outcomes. JACC Heart Fail. 2019 Oct; 7(10):849-858. [CrossRef]
- Kobalava ZD, Safarova AF, Soloveva AE, et al. [Pulmonary congestion by lung ultrasound in decompensated heart failure: associations, in-hospital changes, prognostic value]. Kardiologiia. 2019 Aug; 59(8):5-14. [CrossRef]
- Marini C, Fragasso G, Italia L, Sisakian H, Tufaro V, Ingallina G, Stella S, Ancona F, Loiacono F, Innelli P, Costantino MF, Sahakyan L, Gabrielyan S, Avetisyan M, Margonato A, Agricola E. Lung ultrasound-guided therapy reduces acute decompensation events in chronic heart failure. Heart. 2020 Dec; 106(24):1934-1939. [CrossRef]
- Araiza-Garaygordobil D, Gopar-Nieto R, Martinez-Amezcua P, Cabello-López A, Alanis-Estrada G, Luna-Herbert A, González-Pacheco H, Paredes-Paucar CP, Sierra-Lara MD, Briseño-De la Cruz JL, Rodriguez-Zanella H, Martinez-Rios MA, Arias-Mendoza A. A randomized controlled trial of lung ultrasound-guided therapy in heart failure (CLUSTER-HF study). Am Heart J. 2020 Sep;227:31-39. [CrossRef]
- Rivas-Lasarte M, Álvarez-García J, Fernández-Martínez J, Maestro A, López- López L, Solé-González E, Pirla MJ, Mesado N, Mirabet S, Fluvià P, Brossa V, Sionis A, Roig E, Cinca J. Lung ultrasound-guided treatment in ambulatory patients with heart failure: a randomized controlled clinical trial (LUS-HF study). Eur J Heart Fail. 2019 Dec;21(12):1605-1613. Epub 2019 Oct 31. [CrossRef]
- Conangla L, Domingo M, Lupón J, Wilke A, Juncà G, Tejedor X, Volpicelli G, Evangelista L, Pera G, Toran P, Mas A, Cediel G, Verdú JM, Bayes-Genis A. Lung Ultrasound for Heart Failure Diagnosis in Primary Care. J Card Fail. 2020 Oct;26(10):824-831. [CrossRef]
- Domingo M, Lupón J, Girerd N, Conangla L, de Antonio M, Moliner P, Santiago- Vacas E, Codina P, Cediel G, Spitaleri G, González B, Diaz V, Rivas C, Velayos P, Núñez J, Bayes-Genís A. Lung ultrasound in outpatients with heart failure: the wet-to-dry HF study. ESC Heart Fail. 2021 Dec;8(6):4506-4516. [CrossRef]
- Wang Y, Shi D, Liu F, Xu P, Ma M. Prognostic Value of Lung Ultrasound for Clinical Outcomes in Heart Failure Patients: A Systematic Review and Meta-Analysis. Arq Bras Cardiol. 2021 Mar;116(3):383-392. English, Portuguese. [CrossRef]
- Rueda-Camino JA, Saíz-Lou EM, Del Peral-Rodríguez LJ, Satué-Bartolomé JÁ, Zapatero-Gaviria A, Canora-Lebrato J. Prognostic utility of bedside lung ultrasound before discharge in patients with acute heart failure with preserved ejection fraction. Med Clin (Barc). 2021 Mar 12;156(5):214-220. English, Spanish. [CrossRef]
- Zisis, G, Yang, Y, Huynh, Q. et al. Nurse-Provided Lung and Inferior Vena Cava Assessment in Patients With Heart Failure. J Am Coll Cardiol. 2022 Aug, 80 (5) 513–523. [CrossRef]
- Maestro-Benedicto A, Rivas-Lasarte M, Fernández-Martínez J, López-López L, Solé-González E, Brossa V, Mirabet S, Roig E, Cinca J, Álvarez-García J, Sionis A. Incremental prognostic value of lung ultrasound on contemporary heart failure risk scores. Front Physiol. 2022 Sep 14;13:1006589. [CrossRef]
- Mhanna M, Beran A, Nazir S, Sajdeya O, Srour O, Ayesh H, Eltahawy EA. Lung ultrasound-guided management to reduce hospitalization in chronic heart failure: a systematic review and meta-analysis. Heart Fail Rev. 2022 May;27(3):821-826. [CrossRef]
- Rattarasarn I, Yingchoncharoen T, Assavapokee T. Prediction of rehospitalization in patients with acute heart failure using point-of-care lung ultrasound. BMC Cardiovasc Disord. 2022 Jul 24;22(1):330. [CrossRef]
- Dubón-Peralta EE, Lorenzo-Villalba N, García-Klepzig JL, Andrès E, Méndez-Bailon M. Prognostic value of B lines detected with lung ultrasound in acute heart failure. A systematic review. J Clin Ultrasound. 2022 Feb;50(2):273-283. [CrossRef]
- Arvig MD, Laursen CB, Jacobsen N, Gæde PH, Lassen AT. Monitoring patients with acute dyspnea with serial point-of-care ultrasound of the inferior vena cava (IVC) and the lungs (LUS): a systematic review. J Ultrasound. 2022 Sep;25(3):547-561. [CrossRef]
- Li Y, Ai H, Ma N, Li P, Ren J. Lung ultrasound-guided treatment for heart failure: An updated meta-analysis and trial sequential analysis. Front Cardiovasc Med. 2022 Aug 22;9:943633. [CrossRef]
- Platz E, Claggett B, Jering KS, Kovacs A, Cikes M, Winzer EB, Rad A, Lefkowitz MP, Gong J, Køber L, McMurray JJV, Solomon SD, Pfeffer MA, Shah A. Trajectory and correlates of pulmonary congestion by lung ultrasound in patients with acute myocardial infarction: insights from PARADISE-MI. Eur Heart J Acute Cardiovasc Care. 2023 Apr 3;12(3):155-164. [CrossRef]
- Cohen A, Li T, Maybaum S, et al. Pulmonary congestion on lung ultrasound predicts increased risk of 30-day readmission in heart failure patients [published online ahead of print February 25, 2023]. J Ultrasound Med. [CrossRef]
- Goldsmith AJ, Jin M, Lucassen R, Duggan NM, Harrison NE, Wells W, Ehrman RR, Ferre R, Gargani L, Noble V, Levy P, Lane K, Li X, Collins S, Pang P, Kapur T, Russell FM. Comparison of pulmonary congestion severity using artificial intelligence-assisted scoring versus clinical experts: A secondary analysis of BLUSHED-AHF. Eur J Heart Fail. 2023 Jul;25(7):1166-1169. [CrossRef]
- Maw AM, Hassanin A, Ho PM, McInnes MDF, Moss A, Juarez-Colunga E, Soni NJ, Miglioranza MH, Platz E, DeSanto K, Sertich AP, Salame G, Daugherty SL. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults With Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-analysis. JAMA Netw Open. 2019 Mar 1;2(3):e190703. [CrossRef]
- Pivetta E, Goffi A, Nazerian P, Castagno D, Tozzetti C, Tizzani P, Tizzani M, Porrino G, Ferreri E, Busso V, Morello F, Paglieri C, Masoero M, Cassine E, Bovaro F, Grifoni S, Maule MM, Lupia E; Study Group on Lung Ultrasound from the Molinette and Careggi Hospitals. Lung ultrasound integrated with clinical assessment for the diagnosis of acute decompensated heart failure in the emergency department: a randomized controlled trial. Eur J Heart Fail. 2019 Jun;21(6):754-766. [CrossRef]
- Jose Curbelo, Pablo Rodriguez-Cortes, Maria Aguilera, Paloma Gil Martinez, Daniel Martín & Carmen Suarez Fernandez (2019) Comparison between inferior vena cava ultrasound, lung ultrasound, bioelectric impedance analysis, and natriuretic peptides in chronic heart failure, Current Medical Research and Opinion, 35:4, 705-713. [CrossRef]
- Reddy YNV, Obokata M, Wiley B, Koepp KE, Jorgenson CC, Egbe A, Melenovsky V, Carter RE, Borlaug BA. The haemodynamic basis of lung congestion during exercise in heart failure with preserved ejection fraction. Eur Heart J. 2019 Dec 1;40(45):3721-3730. [CrossRef]
- Domingo M, Conangla L, Lupón J, Wilke A, Juncà G, Revuelta-López E, Tejedor X, Bayes-Genis A. Lung ultrasound and biomarkers in primary care: Partners for a better management of patients with heart failure? J Circ Biomark. 2020 Oct 16;9:8-12. [CrossRef]
- J. Rubio-Gracia, I. Giménez-López, C. Josa-Laorden, M.M. Sánchez-Marteles, V. Garcés-Horna, F. Ruiz-Laiglesia, P. Sampériz Legarre, E. Bueno Juana, B. Amores-Arriaga, J.I. Pérez-Calvo. Prognostic value of multimodal assessment of congestion in acute heart failure. Revista Clínica Española (English Edition)Volume 221, Issue 4, April 2021, Pages 198-206. [CrossRef]
- Morvai-Illés B, Polestyuk-Németh N, Szabó IA, Monoki M, Gargani L, Picano E, Varga A, Ágoston G. The Prognostic Value of Lung Ultrasound in Patients With Newly Diagnosed Heart Failure With Preserved Ejection Fraction in the Ambulatory Setting. Front Cardiovasc Med. 2021 Dec 2;8:758147. [CrossRef]
- Burgos LM, Baro Vila R, Goyeneche A, Muñoz F, Spaccavento A, Fasan MA, Ballari F, Vivas M, Riznyk L, Ghibaudo S, Trivi M, Ronderos R, Costabel JP, Botto F, Diez M; CAVAL US-AHF group. Design and rationale of the inferior vena CAVA and Lung UltraSound-guided therapy in Acute Heart Failure (CAVAL US-AHF Study): a randomised controlled trial. Open Heart. 2022 Nov;9(2):e002105. [CrossRef]
- Pérez-Herrero S, Lorenzo-Villalba N, Urbano E, Sánchez-Sauce B, Aguilar-Rodríguez F, Bernabeu-Wittel M, Garcia-Alonso R, Soler-Rangel L, Trapiello-Valbuena F, Garcia-García A, Casas-Rojo JM, Beltrán-Romero L, De Jorge-Huerta L, Molina-Puente JI, Andrès E, Iguarán-Bermúdez R, Méndez-Bailón M. Prognostic Significance of Lung and Cava Vein Ultrasound in Elderly Patients Admitted for Acute Heart Failure: PROFUND-IC Registry Analysis. J Clin Med. 2022 Aug 5;11(15):4591. [CrossRef]
- Chiu L, Jairam MP, Chow R, Chiu N, Shen M, Alhassan A, Lo CH, Chen A, Kennel PJ, Poterucha TJ, Topkara VK. Meta-Analysis of Point-of-Care Lung Ultrasonography Versus Chest Radiography in Adults With Symptoms of Acute Decompensated Heart Failure. Am J Cardiol. 2022 Jul 1;174:89-95. [CrossRef]
- Coiro S, Echivard M, Simonovic D, Duarte K, Santos M, Deljanin-Ilic M, Kobayashi M, Ambrosio G, Girerd N. Exercise-induced B-lines for the diagnosis of heart failure with preserved ejection fraction: a two-centre study. Clin Res Cardiol. 2023 Aug;112(8):1129-1142. [CrossRef]
- Xie C, Qi Y, Li D. Value of Thoracic Echocardiography in the Diagnosis of Acute Heart Failure: Systematic Review and Meta-analysis. Altern Ther Health Med. 2023 Sep;29(6):322-327. PMID: 37347689.
- Torres-Macho J, Cerqueiro-González JM, Arévalo-Lorido JC, Llácer-Iborra P, Cepeda-Rodrigo JM, Cubo-Romano P, Casas-Rojo JM, Ruiz-Ortega R, Manzano-Espinosa L, Lorenzo-Villalba N, Méndez-Bailón M. The Effects of a Therapeutic Strategy Guided by Lung Ultrasound on 6-Month Outcomes in Patients with Heart Failure: Results from the EPICC Randomized Controlled Trial. J Clin Med. 2022 Aug 22;11(16):4930. [CrossRef]
- Cruz M, Ferreira JP, Diaz SO, Ferrão D, Ferreira AI, Girerd N, Sampaio F, Pimenta J. Lung ultrasound and diuretic therapy in chronic heart failure: a randomised trial. Clin Res Cardiol. 2024 Mar;113(3):425-432. [CrossRef]
- Libertario Demi, PhD, Frank Wolfram, PhD, Catherine Klersy, PhD, Annalisa De Silvestri, PhD,Virginia Valeria Ferretti, PhD, Marie Muller, PhD, Douglas Miller, PhD, Francesco Feletti, PhD,Marcin Wełnicki, PhD, Natalia Buda, MD, Agnieszka Skoczylas, MD, Andrzej Pomiecko, PhD,Domagoj Damjanovic, PhD, Robert Olszewski, MD, Andrew W. Kirkpatrick, MD, Raoul Breitkreutz, PhD,Gebhart Mathis, MD, Gino Soldati, MD, Andrea Smargiassi, PhD, Riccardo Inchingolo, PhD,Tiziano Perrone, PhD on behalf of American Institute of Ultrasound in Medicine. New International Guidelines andConsensus on the Use of LungUltrasound. J Ultrasound Med 2023; 42:309–344.
- Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, Melniker L, Gargani L, Noble VE, Via G, Dean A, Tsung JW, Soldati G, Copetti R, Bouhemad B, Reissig A, Agricola E, Rouby JJ, Arbelot C, Liteplo A, Sargsyan A, Silva F, Hoppmann R, Breitkreutz R, Seibel A, Neri L, Storti E, Petrovic T; International Liaison Committee on Lung Ultrasound (ILC-LUS) for International Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012 Apr;38(4):577-91. [CrossRef]
- Christian B. Laursen, Amelia Clive, Rob Hallifax, Pia Iben Pietersen, Rachelle Asciak, Jesper Rømhild Davidsen, Rahul Bhatnagar, EihabBedawi, Niels Jacobsen, Courtney Coleman, Anthony Edey, Gabriele Via, Giovanni Volpicelli, Gilbert Massard, Francesco Raimondi, Matthew Evison, Lars Konge, Jouke Annema, Najib M. Rahman, Nick Maskell. European Respiratory Society statement on thoracic ultrasound. European Respiratory Journal 2021 57: 2001519;. [CrossRef]
- Miglioranza MH, Gargani L, Sant'Anna RT, Rover MM, Martins VM, Mantovani A, Weber C, Moraes MA, Feldman CJ, Kalil RA, Sicari R, Picano E, Leiria TL. Lung ultrasound for the evaluation of pulmonary congestion in outpatients: a comparison with clinical assessment, natriuretic peptides, and echocardiography. JACC Cardiovasc Imaging. 2013 Nov;6(11):1141-51. Epub 2013 Oct 2. PMID: 24094830. [CrossRef]
- Platz E, Jhund PS, Girerd N, Pivetta E, McMurray JJV, Peacock WF, Masip J, Martin-Sanchez FJ, Miró Ò, Price S, Cullen L, Maisel AS, Vrints C, Cowie MR, DiSomma S, Bueno H, Mebazaa A, Gualandro DM, Tavares M, Metra M, Coats AJS, Ruschitzka F, Seferovic PM, Mueller C; Study Group on Acute Heart Failure of the Acute Cardiovascular Care Association and the Heart Failure Association of the European Society of Cardiology. Expert consensus document: Reporting checklist for quantification of pulmonary congestion by lung ultrasound in heart failure. Eur J Heart Fail. 2019 Jul;21(7):844-851. [CrossRef]
- Coiro S, Rossignol P, Ambrosio G, Carluccio E, Alunni G, Murrone A, Tritto I, Zannad F, Girerd N. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur J Heart Fail. 2015 Nov;17(11):1172-81. [CrossRef]
- Mousa A, Blok SG, Karssen D, Aman J, Annema JT, Bogaard HJ, Bonta PI, Haaksma ME, Heldeweg MLA, Lieveld AWE, Nanayakkara P, Nossent EJ, Smit JM, Smit MR, Vlaar APJ, Schultz MJ, Bos LDJ, Paulus F, Tuinman PR, Amsterdam Umc Covid-Biobank Investigators. Correlation between Serum Biomarkers and Lung Ultrasound in COVID-19: An Observational Study. Diagnostics (Basel). 2024 Feb 14;14(4):421. [CrossRef]
Table 2.
Multimodal assessment (clinical, laboratory and LUS).
| First Author Year of publication Country |
Objectives | Methods | Results | |||
|---|---|---|---|---|---|---|
| Design |
Participants | Instruments | Outcomes | |||
| Maw AM et al. 2019 (EEUU) [20,63] |
To compare the accuracy of LUS with the accuracy of chest radiography (CxR) in the diagnosis of HF. | Systematic Review and Meta-analysis Prospective cohorts |
6 studies N = 1827 |
LUS vs CxR | Detection of cardiogenic pulmonary edema | Sensitivity LUS vs CxR 0.88 (95% Cl, 0.75-0.95) vs 0.73 (95% CI, 0.70-0.76) Specificity LUS vs CxR 0.90 (95% Cl, 0.88-0.92) vs 0.90 (95% CI, 0.75-0.97). |
| Pivetta E et al. 2019 (Italy) [21,64] |
To evaluate accuracy of combining [LUS] vs [CxR + NT-proBNP] | Randomized trial | N= 518 | Either LUS or [CXR/NT + proBNP] | HF diagnosis accuracy | LUS was higher than [CXR/Nt-proBNP] (AUC 0.95 vs. 0.87, p < 0.01). |
| Curbelo et al. 2019 (Spain) [22,65] |
Comparing the usefulness of inferior vena cava (IVC) ultrasound, lung ultrasound, bioelectrical impedance analysis (BIA), and (NT-proBNP) | Prospective cohort study | N = 99 | LUS IVC BIA NT-proBNP |
Parameters of congestion and mortality | Mortality was associated to significantly lower IVC collapse, and a greater number of lung B-lines; and higher NTproBNP levels. No differences in the BIA parameters. |
| Reddy V et al 2019 (EEUU) [23,66] |
To evaluate increases in Extravascular water at rest and during exercise | Observacional | N = 66 | LUS during invasive hemodynamic submaximal exercise testing | B-lines increase during exercise | 54% (n = 33) either developed new B-lines (n = 23, 38%) or developed an increase in the number B-lines (n = 10, 16%) during exercise. |
| Domingo M et al 2020 (Spain) [24,67] |
To assess relationship between B-lines assessed by LUS and biomarkers | prospective cohort of ambulatory patients | N = 170 | 12-scan LUS protocol (8 anterolateral areas plus 4 lower posterior thoracic areas) and 11 inflammatory and cardiovascular biomarkers | confirmed HF diagnosis | total B-line sum significantly correlated with NT-proBNP (R = 0.29, p < 0.001), growth/differentiation factor-15 (GDF-15; R = 0.23, p = 0.003), high-sensitive Troponin T (hsTnT; R = 0.36, p < 0.001), soluble interleukin-1 receptor-like 1 (sST2; R = 0.29, p < 0.001), cancer antigen 125 (CA-125; R = 0.17, p = 0.03), high-sensitivity C-reactive protein (hsCRP; R = 0.20, p = 0.009), and interleukin (IL)-6 (R = 0.23, p = 0.003). |
| Rubio-Gracia J et al. 2021 (Spain) [25,68] |
Evaluate LUS associated to NT-proBNP, cancer antigen 125, relative plasma volume (rPV) estimation. | Retrospective study | N = 203 | LUS CA 125 NT-proBNP rPV |
Parameters of venous congestion and predictors of mortality after one year of follow-up. |
Values of NT-proBNP ≥3804pg/mL (HR 2.78 [1.27-6.08]; p=.010) and rPV≥-4.54% (HR 2.74 [1.18-6.38]; p=.019) were independent predictors of all-cause mortality |
| Morvai-Illés B et al 2021 (Hungary) [26,69] |
LUS B-lines compared vs echocardiographic parameters and natriuretic peptide level | prospective cohort study | N = 75 | B-lines LUS NT-proBNP |
The prognostic value of B-lines and other novel ultrasound parameters: global longitudinal strain and left atrial reservoir strain. | ≥ 15 B-lines lines was associated with a significantly worse event-free survival, and was similar to the predictive value of NT-proBNP (AUC 0.863 vs. 0.859) |
| Burgos et al 2022 (Buenos Aires) [27,70] |
To evaluate if inferior vena cava (IVC) and lung ultrasound (CAVAL US)-guided therapy. | CAVAL US-AHF Study- Randomized control trial |
N = 58 |
Assigned either LUS + IVC (‘intervention group’) or clinical-guided decongestion therapy (‘control group’), B-lines IVC readmission |
Presence ≥ 5 B-lines and/or an increase in the diameter of the IVC, with and without collapsibility. Endpoints: the composite of readmission for HF, unplanned visit for worsening HF, variation of NT-proBNP or death at 90 days. |
Mortality was associated to significantly lower IVC collapse, and a greater number of lung B-lines; and higher NTproBNP levels B-lines at discharge was associated with a significantly increased risk of 30-day readmission |
| Pérez-Herrero S et al 2022 (Spain) [28, 71] |
To compare the CxR vs B-lines by LUS and collapsibility of IVC. | Observational cohort study based on data collected in the PROFUND-IC study. |
N = 301 |
CxR B-lines by LUS IVC |
prediction of 30-day mortality based on the diameter of the IVC | ≥ 6 B-lines per field and IVC collapsibility ≤ 50% had higher 30-day mortality rates |
| Chiu L et al 2022 (EEUU) [29,72] |
LUS diagnostic accuracy vs a chest x-ray (CxR) | Meta-Analysis | 8 studies N = 2,787 | LUS vs chest radiography | diagnostic accuracy HF | LUS is more sensitive (91.8% vs 76.5%) and more specific than CxR (92.3% vs 87.0%) than CXR in detecting pulmonary edema. |
| Coiro S et al. 2023 (France) [30,73] | Assess the diagnosis value of exercise lung ultrasound (LUS) for HF with preserved ejection fraction (HFpEF) diagnosis. |
Case-control study |
N = 116 | B-line kinetics in submaximal exercise | Peak B-lines for HFpEF diagnosis | Peak B-lines >5 were the best cutoffs for HFpEF diagnosis |
| Xie C et al. 2023 (Xina) [31,74] |
LUS accuracy vs computerized tomography (CT) vs echocardiogram | Systematic review and Metanalysis | N = 345 | LUS, (CT), and conventional echocardiogram | predictive value for HF diagnosis | The accuracy of LUS was significantly higher than that of echocardiogram (P = 0.01). |
Table 3.
Therapeutic guidance based on the presence of lung ultrasound signs of congestion in ambulatory patients.
Table 3.
Therapeutic guidance based on the presence of lung ultrasound signs of congestion in ambulatory patients.
| First Author Year of publication Country |
Objectives | Methods | Results | |||
|---|---|---|---|---|---|---|
| Design |
Participants | Instruments | Outcomes | |||
| Torres-Macho J et al 2022 (Spain) [32] | to evaluate if LUS-guided diuretic therapy could improve short- and mid-term prognosis compared with standard of care (SOC) after discharge |
Randomized, multicentre, single-blind clinical trial (EPICC trial) |
N = 79 | Participants will be assigned 1:1 to receive treatment guided according to LUS signs of congestion (semi-quantitative evaluation of B lines and the presence of pleural effusion) vs SOC. | Combination of cardiovascular death and readmission for HF at 6 months. |
LUS did not show any benefit in survival analysis or a need for intravenous diuretics compared with SOC. |
| Cruz M et al 2023 (Portugal) [33] |
LUS results to the HF assistant physician would change loop diuretic adjustments in "stable" chronic ambulatory HF patients. | Prospective randomised single-blinded trial | N = 139 | 70 were randomised to blind LUS and 69 to open LUS. | The primary outcome was change in loop diuretic dose (up- or down-titration). | Clinicians were more likely to titrate furosemide dose, but the risk of HF events or cardiovascular death did not differ. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



