
Submitted:
21 March 2024
Posted:
23 March 2024
You are already at the latest version
Abstract
This investigation aimed to explore the impact of acute and regular physical exercise on Brain-Derived Neurotrophic Factor (BDNF) levels in individuals with obesity. Using the Population, Intervention, Comparator, Outcome, and Study design (PICOS) approach, the inclusion criteria were defined as follows: i) population - individuals with overweight or obesity of any age or gender; ii) intervention - acute or chronic interventions involving aerobic or anaerobic methodologies; iii) comparator - for acute effect studies, pre- and post-evaluations served as comparators, while interventions included at least one experimental group or the inclusion of a control group; iv) outcome - BDNF variability concerning the applied methodology; v) study design - restricted to experimental studies exclusively. Conducted in August 2022, the searches were carried out on PubMed, Academic Search Complete, and Web of Science. The risk of bias was assessed using the Risk of Bias in Non-randomized Studies (RoBANS) tool. Out of 98 potentially relevant articles, 16 met the eligibility criteria, encompassing 23 trials. Substantial heterogeneity was observed for both acute (I2 = 80.4%) and long-term effects (I2 = 88.7%). Additionally, RoBANS analysis indicated a low risk of bias for the included studies. The study's findings revealed a significant increase in the concentration of circulating BDNF in individuals with obesity compared to the control group following acute exercise. However, such an effect was not evident in the context of long-term physical exercise, with a small effect size (ES = 0.49) recorded in the latter scenario. The observed significant increase in BDNF levels post-acute exercise suggests a potential acute response mechanism contributing to the intricate interplay between exercise and neurotrophic factors in this population. Nevertheless, the absence of a similar effect in the context of long-term physical exercise implies a potential adaptation or ceiling effect. These findings underscore the importance of considering both the duration and nature of exercise interventions when exploring the neurobiological responses associated with obesity and exercise. The study provides valuable insights for future research and clinical implications in understanding the nuanced relationship between exercise, neurotrophic factors, and obesity.
Keywords:
Obesity
; BDNF
; physical exercise
; meta-analysis
1. Background
The World Health Organization (WHO) stated that, worldwide, obesity has nearly tripled since 1975 [1]. Despite being deemed preventable, the ramifications of overweight and obesity are pervasive, impacting almost 60% of adults and nearly one in three children, with 29% of boys and 27% of girls affected, within the WHO European Region. Currently, obesity is considered as disease by several medical institutions (as The American Medical Association, WHO, Obesity Society, among others), and the World Obesity Federation see obesity from an epidemiological model, with an agent affecting the host and producing disease [2]. In fact, it is now clear from long-term follow-up studies, that obesity is related to a greater probability to develop heart diseases, type 2 diabetes mellitus, some cancers, dementia, osteoarthritis, among others [3,4,5,6]. Recently, attentions have been given to the link between obesity and neurobiological impairments, since the high levels of dysfunctional adipose tissue observed in patients with obesity population may aggravate metabolic abnormalities, which increase the risk of mood disorders as depression [7,8] and affect the balance of energy expenditure control [9,10]. Indeed, the brain-derived neurotrophic factor (BDNF), which is a protein that has a significant role in the energy homeostasis of body fluids and blood pressure in humans [11], registered significantly lower levels in the patients with obesity [7,12]. Reduced satiety and hyperphagia manifest as discerning features of BDNF deficiency, providing a plausible rationale for fat accumulation. This phenomenon is undeniably associated with the pivotal role of BDNF in the intricate regulation of dietary intake [13]. Furthermore, diminished levels of circulating BDNF have been ascertained in individuals diagnosed with type 2 diabetes [14]. Notably, an inverse correlation has been established between peripheral BDNF concentration and key anthropometric parameters, such as body mass index (BMI), in both pediatric and adult populations [15]. Additionally, in adult males, a negative relationship has been identified between peripheral BDNF levels and fat mass [16].
BDNF is a member of the neurotrophin family and exhibits abundant expression within the hippocampus and cerebral cortex [17,18]. It is mainly produced by the central nervous system, but also by peripheral tissues [19,20], in immune cells, adipocytes, endothelial cells, and monocytesand also by skeletal muslces during contraction [21]. Thus, its levels are detectable in different tissues including brain and blood (6–8 do 4). The significance of its role is intricately tied to its regulatory influence on synaptic activity, neurotransmission, and plasticity across various cohorts of mature neuron [22,23]. This impact extends to neurological development, synaptic plasticity, as well as the processes of learning and memory [17,24].
Physical exercise has been shown to be a way to improve the BDNF concentration in our body, thus inducing brain plasticity and cognitive enhancement [25,26]. In a general context, physical exercise broadly elicits the release of neurotransmitters and neurotrophins in an activity-dependent manner. This acute stimulation not only potentiates neural function but also initiates a cascade of events that actively contribute to the promotion of structural and functional plasticity within the brain. [27,28,29]. Empirical evidence has established that physical exercise induces an elevated rate of mitochondrial respiration and cerebral oxygen consumption[30]. This physiological response engenders several advantageous outcomes, including heightened levels of BDNF[31,32,33] and enhanced functionality of the prefrontal cortex in individuals without pre-existing health condition [34]. Nonetheless, the comprehensive inflationary processes associated with obesity may impede the realization of these aforementioned benefits. Consequently, the main objective of this current review, supplemented by a meta-analysis, is to investigate the influence of physical exercise on BDNF levels in people suffering from obesity. It was hypothesized that physical exercise would have the potential to increase BDNF levels in individuals with obesity, thereby potentially mitigating neurobiological impairments associated with the condition.
2. Method
The present review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [35,36], as well as the PRISMA guidelines specifically designed for scoping reviews (PRISMA-ScR) [37].
2.1. Protocol and Registration
The review protocol was meticulously formulated and pre-released to facilitate transparency in the search methodology. The comprehensive protocol is accessible on the Open Science Framework (OSF) under the registration number DOI 10.17605/OSF.IO/4UM3B, documented on the 10th of August 2022. Interested parties can review the protocol through the following web address: https://archive.org/details/osf-registrations-4um3b-v1.
2.2. Eligibility Criteria
Research articles considered for inclusion in this study must be published in peer-reviewed journals, without imposing any restrictions on the publication date. The eligibility criteria are constructed according to the Participants, Intervention, Comparators, Outcomes, and Study Design (PICOS) framework below [38,39]:
Participants (P): As a criterion for inclusion, studies involving subjects classified as overweight (Body Mass Index-BMI= 25-30 kg/m2) or obese (BMI= 30 kg/m2 or greater) according to the BMI have been accepted. The classification employed in the original studies will be disregarded. Studies conducted with participants of both genders and aged 18 years and older, spanning any age within this range, have been included in our meta-analysis. Contrastingly, studies involving athletes or those incorporating subjects with normal body weight have been excluded from our investigation.
Intervention (I): Both acute (single-session) and chronic interventions (multiple sessions, with no minimum session requirement) employing aerobic or anaerobic methodologies will be included. Studies lacking physical exercise programs or containing only cognitive programs will be excluded.
Comparators (C): In acute effect studies, the comparator will encompass pre- and post-evaluations. For interventions, comparators will involve at least one experimental group or the inclusion of a control group.
Outcomes (O): The primary outcome of interest is Brain-Derived Neurotrophic Factor (BDNF) variability, with a focus on the methodology applied during the session or sessions.
2.3. Information Sources
The current review involved searching the following databases on the same day (05/08/2022): (i) PubMed; (ii) Academic Search Complete; and (iii) Web of Science. The search encompassed files up to the present year, with no lower limit. Additionally, a manual search was carried out to identify potentially relevant articles not covered in the automated searches, including sources such as Google Scholar and ResearchGate. The manual search focused on: (i) scrutinizing the reference lists of included full-texts to identify potentially relevant titles; (ii) reviewing abstracts for adherence to inclusion criteria; and, if necessary, (iii) revising the full-text. Furthermore, errata/retractions were examined to ensure the accuracy of the included articles [37].
2.4. Search Strategy
The search strategy employed Boolean operators AND/OR without applying any filters or limitations (e.g., date, study design) to enhance the likelihood of identifying relevant studies [40]. The primary search strategy comprised the following terms:
“BDNF” OR “brain-derived neurotrophic factor”
AND
“aerobic*” OR “HIIT” OR “high intensity interval training” OR “anaerobic*”
AND
“obesity” OR “overweight”
2.5. Selection Process
The initial phase of the study involved a meticulous screening process conducted by two authors, namely HC and AFS, who independently evaluated the titles and abstracts of the retrieved records. Following this initial screening, the same authors independently assessed the full texts of the gathered literature. Discrepancies that arose between these two authors were subjected to thorough discussion in a collaborative reanalysis. In instances where a consensus could not be achieved, a fourth author, EMC, assumed the responsibility of making the final decision. To ensure a comprehensive and unbiased selection process, all co-authors actively participated by sharing their opinions whenever uncertainties arose. This collaborative approach aimed to facilitate a collective decision-making process and enhance the robustness of the study's methodology. Furthermore, the management of bibliographic records was executed with precision using Mendeley, version 3.2.72. This software facilitated the efficient handling of records, including the automatic or manual removal of duplicate entries. The systematic utilization of Mendeley underscored the commitment to maintaining data integrity and streamlining the organizational aspects of the research process.
2.6. Data Collection Process
The data collection process commenced with AFS as the primary investigator (November 2022), who meticulously gathered the data. To ensure the accuracy and completeness of the collected information, a dual verification process was implemented, involving two co-authors, namely HC and EMC. This collaborative effort aimed to confirm the fidelity of the data through rigorous scrutiny. A specially designed Microsoft® Excel datasheet was employed as the tool for extracting and organizing the data, encompassing key information pertinent to the study[41]. In instances where essential data were absent from the full text of the included studies, proactive measures were taken by author HC, who initiated direct communication with the corresponding authors via email and/or ResearchGate. This communication sought to obtain the requisite information, with an anticipated response time of approximately 10 business days. The systematic extraction of pre- and post-intervention means, coupled with the standard deviation of dependent variables, from the included studies was methodically carried out using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) [41]. In situations where studies reported data in formats other than means and standard deviations—specifically, presenting values such as median, range, interquartile range, or standard error—a methodically standardized conversion procedure was systematically implemented, strictly adhering to established recommendations[42,43,44]. The statistical analysis of diverse data formats employed the Comprehensive Meta-Analysis Software, Version 2, developed by Biostat in Englewood, NJ, USA. This software was chosen for its versatility in handling various data structures inherent in the included studies [45]. In instances where the required data were not transparently or exhaustively reported in the literature, the authors of the respective studies were engaged through direct communication to seek clarification. This proactive approach aimed to enhance the accuracy and completeness of the dataset under consideration. Following a standard protocol, if no response was received from the authors after two attempts, with a 72-hour waiting period between attempts, or if the authors were unable to provide the requested data, the corresponding study outcome was deemed ineligible for further analysis. Moreover, when data were visually presented in figures without accompanying numerical values, a validated software tool, WebPlotDigitizer, version 4.5 (https://apps.automeris.io/wpd/), was employed. This software, validated with a correlation coefficient (r = 0.99, p < 0.001) [46], facilitated the extraction of numerical data from the graphical representations. The extraction process was spearheaded by one author, AFS, with another author, HC, responsible for confirming the accuracy of the extracted data. Any discrepancies between the two authors, such as disagreements on mean values for specific outcomes, were judiciously resolved through consensus with a third author, ensuring the reliability and consistency of the data extraction process throughout the analytical phase[47].
2.7. Data Items
The primary outcomes of interest were systematically extracted from each study, encompassing a comprehensive set of information categories:
Descriptive characteristics of study participants, including age, sex, and weight, were meticulously documented to provide a contextual understanding of the study population.
Context-related information played a pivotal role in the data extraction process and included, though was not restricted to, the presence of other clinical complications such as diabetes and hypertension, among others.
Methodological-related details were integral to the analysis and included information on the specific physical exercise protocols employed in the studies. This encompassed details such as the type of exercise (aerobic or anaerobic), as well as the number, volume, and intensity of the exercise sessions.
The main outcome of interest, namely the changes in BDNF in response to the prescribed physical exercise protocols, formed the core focus of the data extraction process. Variations in BDNF levels, whether indicative of increases or decreases, were systematically recorded to discern the effects of different exercise methodologies.
In addition to the aforementioned categories, supplementary information was gathered, including citation details, the publication year, and any potential competing interests declared by the authors.
2.8. Study Risk of Bias Assessment
The evaluation of the risk of bias within each study was a rigorous process conducted independently by two authors, namely EM and AFS. In instances where discrepancies emerged between the two assessors, a collaborative reanalysis was undertaken to resolve differences. In instances where a consensus could not be attained, a third author, RRC, assumed the responsibility of making the final decision, ensuring a robust and impartial assessment. The Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS) was employed as the standardized instrument for evaluating the risk of bias in the included studies [48]. This tool has demonstrated moderate reliability, as well as trustworthy feasibility and validity [48], making it a suitable choice for the present analysis. The RoBANS framework encompasses six pivotal domains: participant selection, confounding variables, exposure measurement, outcome assessment blinding, handling of incomplete outcome data, and avoidance of selective outcome reporting[48]. Each of these domains was systematically assessed, and the risk of bias within each domain was classified as low, high, or unclear. The utilization of the RoBANS tool, in conjunction with a meticulous and independent assessment by multiple authors, underscores the commitment to a robust evaluation of the risk of bias in the included non-randomized studies.
2.9. Data Management and Synthesis Methods
The analytical approach adhered to a previously established methodology, as outlined in references [49,50], wherein the analysis and interpretation of results were undertaken only when a minimum of three studies provided both baseline and follow-up data for the same outcome measure. The effect size (ES), denoted by Hedge's g, was computed for each outcome measure within the experimental groups by utilizing pre- and post-exercise mean values in conjunction with standard deviations (SD)[42,43]. Standardization of data involved the utilization of post-intervention SD values. A random-effects model was employed to accommodate variations between studies that might influence the impact of interventions on BDNF response [51,52]. Effect sizes were presented with 95% confidence intervals (CIs) and interpreted as follows: <0.2, trivial; 0.2–0.6, small; >0.6–1.2, moderate; >1.2–2.0, large; >2.0–4.0, very large; >4.0, extremely large [52]. The assessment of heterogeneity was conducted using the I2 statistic, with low heterogeneity characterized by values <25%, moderate heterogeneity when values fell between 25% and 75%, and high heterogeneity observed with values >75% [53]. The risk of bias was evaluated utilizing the extended Egger’s test [51]. In instances where bias was identified, the trim and fill method was applied, with L0 serving as the default estimator for missing studies [54,55]. All statistical analyses were performed using Comprehensive Meta-Analysis software (version 2; Biostat, Englewood, NJ, USA)[45]. Statistical significance was set at p ≤ 0.05. Moderators associated with acute or interventional studies, physical exercise frequency, and type were considered in cases where two or more studies provided relevant data, enhancing the depth of the analysis and interpretation of results.
3. Results
3.1. Study Identification and Selection
The initial phase of the literature search yielded a total of 98 titles, which were systematically managed using the EndNoteTM reference manager software (version 20.2, Clarivate Analytics, Philadelphia, PA, USA). Subsequent to the removal of duplicates, totaling 35 titles, through an automated or manual process, the dataset was refined to 63 unique titles. These were then subjected to a screening process based on their relevance, involving an assessment of the title and abstract. This screening led to the exclusion of 32 titles. The remaining 31 titles underwent a thorough evaluation in their full-text versions, resulting in the exclusion of an additional 15 studies for various reasons. Specifically, one study focused on pregnant individuals, five studies did not incorporate physical exercise and were merely report-based, one study constituted a review paper, and eight studies were excluded due to issues related to the outcome measure. In the latter case, one study evaluated proBDNF instead of mBDNF, while in the remaining eight studies, no pertinent data were available in the manuscripts, and attempts to obtain information from the au-thors were unsuccessful. Following this meticulous selection process, 16 studies remained eligible for data extraction and subsequent analysis. This final set of studies formed the basis for the comprehensive examination and synthesis of data to address the research objectives (Figure 1)
3.2. Study Characteristics and Context
The characteristics and contexts of studies showing the effect of acute and regular exercise on BDNF are shown in Table 2, Table 3, Table 4, Table 5, Table 6 and Table 7.
The Risk of Bias Assessment Tool for Non-Randomized Studies (RoBANS) was diligently applied by two independent authors to evaluate potential biases in six distinct do-mains. Notably, the selection of participants posed challenges in several studies, as the recruitment methods were not consistently explained, raising concerns about potential convenience sampling without clear contextual information. However, given that the ma-jority of studies adhered to clinical trial assumptions, the domains of confounding varia-bles, exposure measurements, and blinding of outcome assessments exhibited a low risk of bias. The comprehensiveness of protocols was generally high, with 16 studies provid-ing detailed explanations, while a few studies lacked minor protocol characteristics. One study, in particular, lacked information regarding training load characteristics. Regarding outcome data, biases were identified in some studies (3 at high risk), where explanations for discrepancies in sample sizes from the beginning to the end of the study were not provided. In the overall analysis, the included studies appeared to have a low risk of bias, with none exhibiting a high risk in more than three domains. Despite uncertainties in par-ticipant selection methodologies in some studies, the majority adhered to rigorous clinical trial principles in other key domains, contributing to the overall robustness of the studies. These findings underscore the methodological quality of the included studies in this assessment of bias risk.
3.3. Synthesis of Results
This systematic review with meta-analysis synthesized findings from three studies encompassing a total of six trials, involving 104 participants, to assess the impact of acute exercise on BDNF levels (see Figure 2). The meta-analysis revealed a statistically significant increase in circulating BDNF levels in individuals with obesity compared to controls (Effect Size, ES: 1.25, indicating a large effect, p < 0.05). However, it is important to note that there were indications of heterogeneity in the results, as evidenced by an I² statistic of 80.4%.
The current study provides a comprehensive summary of findings from 13 studies, encompassing 17 trials and involving a total of 571 participants, to investigate the impact of exercise intervention on circulating BDNF levels (see Figure 3). Contrary to initial expectations, the results revealed that exercise interventions did not yield a statistically significant change in BDNF levels when compared to control groups (p > 0.05). Despite the lack of statistical significance, a small positive effect on BDNF levels was observed in the exercise intervention group (Effect Size, ES: 0.49, indicating a small effect). This suggests a potential trend toward a positive influence of exercise on BDNF levels, even though the effect size is considered small. It is noteworthy that the analysis identified high heterogeneity among the studies investigating the impact of exercise intervention on BDNF levels (I² = 88.7%).
4. Discussion
The objective of this systematic review with meta-analysis is to understand the short-term and long-term effects of physical activity on BDNF levels in patients with obesity. Our results showed that acute exercise led to a significant increase in the concentration of circulating BDNF patients with obesity compared to the control group. Despite long-term physical exercise, there was no significant increase in BDNF levels when compared to the control group. Although the results were not statistically significant, it was revealed a small effect size of long-term physical exercise interventions on BDNF levels. (ES = 0.49). Our study also found high levels of heterogeneity in both acute effects (I2 = 80.4%) and long-term effects (I2 = 88.7%). Finally, the quality of the methodologies used in the included studies was determined to be low risk of bias, with none of the studies exhibiting high risk in more than three of the six evaluated domains.
Acute physical exercise has been shown to be an effective stimulant that arise peripheral BDNF levels [72]. The present study found that acute exercise led to a statistically significant augment in BDNF level compared to the control group (ES: 1.25). This review synthesized the findings of three studies involving 104 participants to specify the impact of acute physical exercise on BDNF levels. This result confirms previous systematic reviews nd meta-analysis studies showing that acute exercise increases BDNF levels in healthy adults [72,73,74,75], and older adults [76]. Regarding the included studies, Dominguez-Sanchéz et al. [56] found that acute combine exercise (high-intensity interval exercise and resistance) led to a greater increases (+11.6%, p=0.029) in BDNF levels compared with acute resistance (+9.3%, p= 0.066), and high intensity interval exercises (+6.8%, p= 0.134) in overweight men adults. Likewise, another study notified that acute high-intensity exercise (20 minutes at 85% of VO2max) triggered a rise in serum BDNF levels in inactive adult patients with obesity [57].Additionally, Wheeler et al.[58] (2020) observed that 30 minutes of aerobic exercise (65% and 75% HRmax) performed in the morning hours elevated BDNF levels in inactive elderly men patients with obesity and postmenopausal women. Based on the studies mentioned (3 studies, 6 trials), regardless of the type of exercise, it has been shown that BDNF levels increase in patients with obesity after both acute moderate (1 trial) and high-intensity exercises (5 trials)
Considering the studies mentioned above (3 studies, 6 studies), regardless of the type of exercise (aerobic, resistance and high intensity exercise), it is seen that the BDNF levels of patients with obesity increase after both acute moderate (1 trials), and high-intensity exercise (5 trials). Regarding the studies analyzed, it was concluded that high-intensity exercise protocols were commonly used in patients with obesity, resulting in elevated BDNF levels. The elevation in BDNF levels after acute exercise can be linked to intensity of the exercise. For instance; previous systematic review studies indicated that BDNF levels augmented in a manner dependent on both intensity [74,77], and duration (lasting more than 30 minutes) of the exercise [73]. Furthermore, a recent meta-analysis of 22 studies in healthy adults (aged 20-31 years) with a total of 552 participants noted that greater BDNF levels were observed after acute high-intensity exercise compared to light and moderate-intensity exercise conditions [78].
In literature and our study, several potential mechanisms behind the elevation of BDNF after acute exercise have been proposed, one of which is exercise-induced thrombocytosis. Due to the fact that the most of peripheral BDNF is found in thrombocytes, exercise can lead to a rise in BDNF levels through exercise-induced thrombocytosis, which is thought to occur due to splenic contractions releasing BDNF-rich platelets [79,80]. However, the increase in platelets and peripheral blood BDNF after exercise was reported to be temporary and returned to pre-exercise levels within 15-30 minutes of ceasing physical activity [81]. Despite its temporary nature, it was stated that the increased BDNF response to acute exercise could have the potential to enhance cognitive function by triggering various neuronal processes [82]. Second, the contraction of skeletal muscle during physical activity boosts the manufacture and activity of certain proteins involved in mitochondrial biogenesis, such as PGC-1α, Erra, and FNDC5/irisin. These factors regulate BDNF transcription in the brain and energy metabolism in skeletal and fat tissue [83]. Third, exercise elevates insulin-like growth factor-1 (IGF-1). This hormone has been shown to have a close relationship with an increase in BDNF level in the hippocampus, playing a role in mediating exercise-induced changes in synaptic function and cognitive plasticity [84]. Lastly, a single high-intensity exercise has been linked to higher levels of brain hydrogen peroxide (H2O2) and Tumor Necrosis Factor -α (TNF-α). These molecules are among the many stimulators of PGC-1α signaling, which in turn increases BDNF synthesis in neurons [85].
Furthermore, BDNF, like leptin, promotes feelings of satiety. Recent studies has shown that it actively controls food intake, regulates body weight, and balances energy at the hypothalamic level [86,87]. According to these studies, the BDNF-producing neurons in the paraventricular hypothalamus were found to limit food intake and serve as an anorexigenic factor, resulting in feelings of satiety. These neurons also improve energy consumption by the way of excitement of thermogenesis in brown adipose tissue. Also, research revealed that mutations in the BDNF gene and its receptor TrkB in mice and humans caused an increase in food consumption, and contributed to the onset of severe obesity [88,89]. Based on these studies, the rise of BDNF levels, which are lower baseline in patients with obesity compared to normal-weight individuals[89,90,91], following high-intensity exercise may be related to decreased hunger and an increased sense of fullness. This can minimize the likelihood of obesity developing arising from excessive appetite sensation or appetite signal disorder, and in addition, it can make an additional contribution to the treatment of various neuropsychological diseases (especially brain health) accompanying obesity. More mechanisms of neuropsychological disturbance, especially related to the depression state has been summarised by Murawska-Cialowicz et. al.[92]. Moreover, a previous study noted that administering BDNF to mice increased the levels of glucose transporter 4 (GLUT4) in skeletal muscle[93]. This suggests that the possible impact of increased BDNF levels following acute high-intensity exercise on substrate utilization may enhance the management of metabolic disorders related to obesity [94].
Numerous studies indicate that there is communication between organs and that substances in the nature of growth factors, including BDNF, which is one of the most important factors communicating skeletal muscle with brain and adipose tissue, among others, are involved in this communication. Therefore, the term, metabolokine, is used in relation to BDNF, which is a neurokinin, adipokine and myokine [95]. We can think that one of the main mechanisms of BDNF synthesis during very intense exercise, is the production of lactate [La-]. High-intensity exercise is an effort that stimulates anaerobic energy processes, the product of which is a very large increase in the concentration of lactate [La-] that exceeds the anaerobic threshold. Not so long ago it was thought that [La-] was an unnecessary product of anaerobic metabolism. Nowadays, it is known to be a very important substance acting as a transmitter involved in various metabolic processes [96,97,98]. In the brain [La-] W mediated by monocarboxylate transporters (MCT) [99,100] enters neurons (via MCT2) and astrocytes (via MCT4) supporting, among other things, glucose transport into neurons, their energy metabolism and ion [101].
Current studies indicate that [La-] transport from astrocytes to neurons plays a key role in memory formation [102,103] and may represent a link between exercise and neuroplasticity and BDNF synthesis [97], although the mutual mechanisms are not fully understood. One of them may be the activation by [La-] of various G protein-related receptors, as well as the silent information regulator 1 (SIRT1). With relation to adipose tissue, activation of the PGC1α/FNDC5/BDNF pathway seems to be a convincing one [104]. Lactate can induce the PGC1α/FNDC5/BDNF pathway through activation of SIRT1. Intraperitoneal infusion of lactate in mice was shown to induce SIRT1 activity, thereby enhancing the PGC1α/FNDC5/BDNF pathway, resulting in improved spatial learning and memory retention [105].
FNDC5 (Fibronectin type III domain-containing protein 5) is a precursor protein called irisin, which is an exercise hormone involved in carbohydrate and fat utilization and fat reduction. Expression/secretion of irisin promotes the conversion of white adipose tissue (WAT) into brown adipose tissue (BAT) (browning) as a result of increased expression of UCP-1 (uncoupling protein 1). WAT browning was found to be induced by irisin through p38MAPK and ERK MAPK signaling [106]. A recent study found that lack of irisin is associated with poor adipocyte browning and impaired glucose/lipid levels [107]. The another study shows that irisin concentrations are increased after intense exercise in healthy men [108] as well as in obese subjects in whom aerobic exercise showed no change in irisin levels [109] which given the common mechanism of action of irisin with BDNF, may potentiate BDNF secretion during exercise.
Chronic physical activity increases BDNF in answer to an acute exercise [75]. Regarding the relationship between long-term exercise intervention and BDNF, this systematic review and meta-analysis summarized the findings of 13 studies comprising a total of 571 participants, regarding the impact of exercise intervention on BDNF levels. The associations between chronic exercise interventions and BDNF is complicated [80]. In the literature, recent meta-analysis studies indicated that peripheral BDNF concentrations significantly increased after exercise intervention in healthy individuals [74,110], older adults [76], individuals with multiple sclerosis [111], and neurodegenerative disorders [112]. Contrary to the studies mentioned, the present study observed that long term exercise did not significantly augment BDNF levels compared to the control group. Although not statistically significant, it was found a small effect size of long-term physical exercise on BDNF levels (ES = 0.49; trivial, p=0.089). Consistent with our study, previous meta-analysis studies demonstrated that chronic exercise had a minimal impact on BDNF level in healthy [73,75] and elderly individuals [113]. The current meta-analysis of included studies showed inconsistent findings considering the effect of chronic physical activity on BDNF level. According to this, it was notified that BDNF level significantly increased [59,60,64,65,67,68,69,70], decreased [61,62], and remained unchanged [63,66,71] after exercise intervention in patients with obesity. However, the lack of significant changes in BDNF levels following regular exercise in our meta-analysis could be due to the high heterogeneity in the studies included, which explains the inconsistent results. Moreover, the high heterogeneity could be attributed to differences in the methodology of the included studies, including the characteristics of participants, exercise applications (frequency, intensity, type, time, volume), measurement methods, methodological quality of studies, and type of Elisa kits used. Also, the absence of a significant difference in exercise intervention compared to acute exercise may be related to difficulties in controlling too many variables that may affect the results depending on the duration of the program. In this sense, Fleitas et al. [113] emphasized that some factors should be considered in the lack of significant effects of chronic physical exercise on peripheral BDNF levels. Failure to control participants' nutritional status or energy intake during the study and before blood samples are collected may have a negative impact on BDNF results. When the included studies were examined, it was observed that the energy intake of the participants during the exercise program was not considered in many studies. Conducting more controlled studies in the laboratory environment by applying standardized nutrition programs to the participants during the study may contribute to obtaining more accurate results. Additionally, BDNF levels fluctuate throughout the day due to the diurnal variations of the cortisol and various hormonal fluctuations [114]. Thus, time of the day on both exercise interventions and data collection (blood collection time), and non-standardization of the collection may have a negative impact on BDNF-related measurements [113]. In this context, it is important to conduct quality and randomized controlled studies with larger sample groups, taking into account the energy intake of the participants in order to elevate BDNF in response to exercise intervention in patients with obesity.
The important seems to be also the analytical material type-serum/plasma, sample storage time and centrifugation [115]. The different levels of BDNF are reported in serum and plasma. This can be connected with thrombocytosis mechanism and utilization of BDNF after chronic, intensive or long-lasting exercise. Higher production of growth factors in platelates and utilization of BDNF for reparation and regeneratin of skeletal muscle and nerve fibers at the muscle levels is quite possible mechanism of BDNF reduction in serum and plasma [16,116].
Moreover, in our study, it was revealed that the BDNF level did not differ significantly following the six months of high-intensity [63], and ten weeks of moderate-intensity [66] regular resistance exercises, and 6 months of moderate-intensity aerobic exercise [71]. In literature, studies have shown that resistance exercise had no significant effect on BDNF concentration in both healthy [72,74,110], and elderly [113] individuals. Nevertheless, despite all these, it was seen that the BDNF level increased after regular exercise in many studies included in present study. Regarding the studies in which the BDNF level increased (1 study: moderate aerobic exercise, the other 7 studies: high-intensity aerobic exercise, a total of 8 studies), it was observed that high-intensity aerobic exercise programs performed for approximately 8-12 weeks were more likely to trigger the increase in BDNF levels. In the light of this information, recent meta-analysis study suggested that moderate and high-intensity aerobic exercise programs (3-5 times a week and 20-60 minutes, 12 weeks) were an effective strategy to increase BDNF levels in adolescents [117]. Considering the all studies mentioned above, it can be said that aerobic exercises are effective in increasing BNDF level compared to resistance exercises. Consistent with this finding, previous studies indicated that regular exercise augmented circulating BDNF, while resistance exercise did not [72,110,113]. This is due to the fact that aerobic exercise is linked to physiological processes that enhance BDNF, including improved endothelial function, insulin sensitivity, and cerebral blood flow [72,80]. The another study by Walsh et al. [80] suggested that high-intensity short-duration physical activities might increase BDNF levels and improve brain health. Subsequently, the same researchers stated that combining aerobic and anaerobic exercise at approximately 60% of VO2max may have the greatest effect on BDNF elevation due to mechanisms such as cardiovascular changes and lactate release.
The present meta-analysis study has several limitations. One such limitation is the potential confounding effect of age among participants included in the studies analyzed. Unfortunately, due to the small number of studies analyzing exercise-induced changes in BDNF concentrations in obese subjects, subjects of different ages were included in the analysis. Moreover, age-related differences in physiological responses to exercise could impact the magnitude of BDNF upregulation, thereby influencing the overall effect size observed in our meta-analysis. Therefore, future studies with age-stratified analyses could provide more nuanced insights into the relationship between exercise, BDNF, and obesity. Another limitation may be the gender of the subjects. Changes were not differentiated separately for male and female subjects. Older patients may exhibit differential responses to exercise interventions compared to younger individuals, which could influence the observed effects on BDNF levels. Future investigations should consider stratified analyses based on gender, allowing for a more nuanced understanding of how exercise-induced changes in BDNF levels may differ between male and female participants, especially in the context of obesity. Lastly, previous studies on different populations showed that duration of the exercise intervention (weeks) [78,111,112,113], intensity of exercise [72,80], the weekly volume of the exercise [112] did not significantly affect the circulating BDNF level. Although the studies above do not show a significant effect, the last limitation in our study is that, due to the small number of studies in obese individuals, separate submodular analyzes were not performed to examine the effects of individual components of exercise prescription such as time, intensity, type and frequency on BDNF responses. These components are critical determinants of the physiological responses to exercise, and their nuanced exploration could provide valuable insights into the specific parameters influencing BDNF levels in individuals with obesity. For instance; diverse exercise modalities, such as aerobic, resistance, or combined training may elicit distinct molecular responses, and the variability in exercise interventions could introduce heterogeneity into our meta-analysis. Recognizing this limitation is essential for interpreting our findings and emphasizing the need for more focused investigations into the specific effects of different exercise regimens on BDNF in the context of obesity. Thus, more studies are needed to provide a clearer understanding of which type of physical activity has the greatest impact on BDNF in patients with obesity. By acknowledging these limitations, we aim to provide a comprehensive and transparent assessment of the findings while highlighting areas for future research to address these potential sources of bias and variability. Well designed and quality randomized controlled studies with greater populations are recommended to determine how different exercise configurations may affect BDNF levels in patients with obesity [112].
5. Conclusion
The present meta-analysis represents a pioneering effort in investigating the impact of acute and regular physical activity on BDNF levels, focusing exclusively on individuals afflicted by obesity. This study distinguishes itself by synthesizing findings exclusively from randomized control group studies, thereby contributing a specialized perspective to the existing literature. The principal objective was to discern whether a single session of exercise or a more sustained physical activity intervention could elicit alterations in BDNF levels in comparison to a control group within the context of obesity. The meta-analysis reveals that a singular episode of exercise induces a noteworthy elevation in BDNF levels among individuals with obesity when juxtaposed with the control group. However, intriguingly, interventions involving sustained physical exercise did not yield a statistically significant alteration in BDNF levels when compared to the control group. Although the observed effect of exercise interventions on circulating BDNF did not attain statistical significance, there was a discernible small-scale impact, underscoring the nuanced nature of the relationship. This investigation underscores the potential utility of both acute and regular exercise regimens in positively modulating BDNF levels in the context of obesity. Given the intricate interplay of BDNF with appetite regulation, neuroplasticity, and cognitive functions, augmenting the diminished basal levels inherent in obesity through non-pharmacological means, such as physical exercise, emerges as a promising avenue for mitigating the condition. Moreover, the potential ancillary benefits extend beyond mere weight management, encompassing the amelioration of psychological comorbidities associated with obesity, including cognitive disorders and depression. Additionally, given the complex processes regulating BDNF levels in tissues, it is challenging to explain the relationship between BDNF and obesity. Therefore, further research is needed to understand the mechanisms of exercise and BDNF regulation in order to develop more effective therapies for obesity and optimize exercise-based treatments. Consequently, the findings of this meta-analysis contribute valuable insights that may inform the development of comprehensive and multifaceted interventions for individuals grappling with obesity, addressing both the physiological and psychological dimensions of the condition.
Author Contributions
Conceptualization, H.İ.C. and A.F.S.; methodology, A.F.S.; formal analysis, R.R.C; investigation, A.F.S., H.İ.C., F.M.C..; writing—original draft preparation, A.F.S., H.İ.C., R.R.C., F.M.C., E.M.C.; writing—review and editing, A.F.S., H.İ.C., R.R.C., F.M.C., E.M.C.; supervision, F.M.C.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The protocol can be observed in the Open Science Framework (OSF) with the registration number DOI 10.17605/OSF.IO/4UM3B on the 10/08/2022. The protocol can be accessed by the web address https://archive.org/details/osf-registrations-4um3b-v1.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available for research purposes upon reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Health, W. WHO European regional obesity report; 2022.
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Danaei, G.; Ding, E.L.; Mozaffarian, D.; Taylor, B.; Rehm, J.; Murray, C.J.L.; Ezzati, M. Correction: The Preventable Causes of Death in the United States: Comparative Risk Assessment of Dietary, Lifestyle, and Metabolic Risk Factors. PLoS Med. 2011, 8, e1000058. [Google Scholar] [CrossRef]
- Hubert, H.B.; Feinleib, M.; McNamara, P.M.; Castelli, W.P. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation 1983, 67, 968–977. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, P.D.; Hinder, L.M.; Callaghan, B.C.; Feldman, E.L. Neurological consequences of obesity. Lancet Neurol. 2017, 16, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Prospective Studies Collaboration Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [CrossRef]
- Cellik-Guzel, E.; Bakkal, E.; Guzel, S.; Eroglu, H.E.; Acar, A.; Topcu, B.; Kucukyalcin, V. Can low brain-derived neurotrophic factor levels be a marker of the presence of depression in obese women? Neuropsychiatr. Dis. Treat. 2014, 10, 2079–86. [Google Scholar] [CrossRef] [PubMed]
- de Assis, G.G.; Murawska-Ciałowicz, E. Leptin—A Potential Bridge between Fat Metabolism and the Brain’s Vulnerability to Neuropsychiatric Disorders: A Systematic Review. J. Clin. Med. 2021, 10, 5714. [Google Scholar] [CrossRef]
- Chaldakov, G.N.; Fiore, M.; Ranćić, G.; Beltowski, J.; Tunçel, N.; Aloe, L. An Integrated View: Neuroadipocrinology of Diabesity. Serbian J. Exp. Clin. Res. 2014, 15, 61–69. [Google Scholar] [CrossRef]
- van Reedt Dortland, A.K.B.; Giltay, E.J.; van Veen, T.; Zitman, F.G.; Penninx, B.W.J.H. Longitudinal Relationship of Depressive and Anxiety Symptoms With Dyslipidemia and Abdominal Obesity. Psychosom. Med. 2013, 75, 83–89. [Google Scholar] [CrossRef]
- Ramos, L.W.F.; Murad, N.; Goto, E.; Antônio, E.L.; Silva, J.A.; Tucci, P.F.; Carvalho, A.C. Ischemia/reperfusion is an independent trigger for increasing myocardial content of mRNA B-type natriuretic peptide. Heart Vessels 2009, 24, 454. [Google Scholar] [CrossRef]
- Koizumi, M.; Watanabe, H.; Kaneko, Y.; Iino, K.; Ishida, M.; Kosaka, T.; Motohashi, Y.; Ito, H. Impact of obesity on plasma B-type natriuretic peptide levels in Japanese community-based subjects. Heart Vessels 2012, 27, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Rosas-Vargas, H.; Martínez-Ezquerro, J.D.; Bienvenu, T. Brain-Derived Neurotrophic Factor, Food Intake Regulation, and Obesity. Arch. Med. Res. 2011, 42, 482–494. [Google Scholar] [CrossRef] [PubMed]
- Krabbe, K.S.; Nielsen, A.R.; Krogh-Madsen, R.; Plomgaard, P.; Rasmussen, P.; Erikstrup, C.; Fischer, C.P.; Lindegaard, B.; Petersen, A.M.W.; Taudorf, S.; et al. Brain-derived neurotrophic factor (BDNF) and type 2 diabetes. Diabetologia 2007, 50, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Lommatzsch, M.; Zingler, D.; Schuhbaeck, K.; Schloetcke, K.; Zingler, C.; Schuff-Werner, P.; Virchow, J.C. The impact of age, weight and gender on BDNF levels in human platelets and plasma. Neurobiol. Aging 2005, 26, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Murawska-Ciałowicz, E.; de Assis, G.G.; Clemente, F.M.; Feito, Y.; Stastny, P.; Zuwała-Jagiełło, J.; Bibrowicz, B.; Wolański, P. Effect of four different forms of high intensity training on BDNF response to Wingate and Graded Exercise Test. Sci. Rep. 2021, 11, 8599. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Poo, M. Neurotrophin regulation of neural circuit development and function. Nat. Rev. Neurosci. 2013, 14, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Quirié, A.; Hervieu, M.; Garnier, P.; Demougeot, C.; Mossiat, C.; Bertrand, N.; Martin, A.; Marie, C.; Prigent-Tessier, A. Comparative Effect of Treadmill Exercise on Mature BDNF Production in Control versus Stroke Rats. PLoS One 2012, 7, e44218. [Google Scholar] [CrossRef] [PubMed]
- Babaei, P.; Damirchi, A.; Mehdipoor, M.; Tehrani, B.S. Long term habitual exercise is associated with lower resting level of serum BDNF. Neurosci. Lett. 2014, 566, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, P.; Brassard, P.; Adser, H.; Pedersen, M. V.; Leick, L.; Hart, E.; Secher, N.H.; Pedersen, B.K.; Pilegaard, H. Evidence for a release of brain-derived neurotrophic factor from the brain during exercise. Exp. Physiol. 2009, 94, 1062–1069. [Google Scholar] [CrossRef]
- Matthews, V.B.; Åström, M.-B.; Chan, M.H.S.; Bruce, C.R.; Krabbe, K.S.; Prelovsek, O.; Åkerström, T.; Yfanti, C.; Broholm, C.; Mortensen, O.H.; et al. Brain-derived neurotrophic factor is produced by skeletal muscle cells in response to contraction and enhances fat oxidation via activation of AMP-activated protein kinase. Diabetologia 2009, 52, 1409–1418. [Google Scholar] [CrossRef]
- Farinas, I. Neurotrophin actions during the development of the peripheral nervous system. Microsc. Res. Tech. 1999, 45, 233–242. [Google Scholar] [CrossRef]
- McAllister, A.K. Neurotrophins and neuronal differentiation in the central nervous system. Cell. Mol. Life Sci. 2001, 58, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Zagrebelsky, M.; Korte, M. Form follows function: BDNF and its involvement in sculpting the function and structure of synapses. Neuropharmacology 2014, 76, 628–638. [Google Scholar] [CrossRef] [PubMed]
- Berchtold, N.C.; Chinn, G.; Chou, M.; Kesslak, J.P.; Cotman, C.W. Exercise primes a molecular memory for brain-derived neurotrophic factor protein induction in the rat hippocampus. Neuroscience 2005, 133, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Intlekofer, K.A.; Berchtold, N.C.; Malvaez, M.; Carlos, A.J.; McQuown, S.C.; Cunningham, M.J.; Wood, M.A.; Cotman, C.W. Exercise and Sodium Butyrate Transform a Subthreshold Learning Event into Long-Term Memory via a Brain-Derived Neurotrophic factor-Dependent Mechanism. Neuropsychopharmacology 2013, 38, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.-A. Exercise builds brain health: key roles of growth factor cascades and inflammation. Trends Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, G.F.; Rhodes, J.S. Exercise Regulation of Cognitive Function and Neuroplasticity in the Healthy and Diseased Brain. In; 2015; pp. 381–406.
- Wrann, C.D.; White, J.P.; Salogiannnis, J.; Laznik-Bogoslavski, D.; Wu, J.; Ma, D.; Lin, J.D.; Greenberg, M.E.; Spiegelman, B.M. Exercise Induces Hippocampal BDNF through a PGC-1α/FNDC5 Pathway. Cell Metab. 2013, 18, 649–659. [Google Scholar] [CrossRef]
- Picard, M.; McEwen, B.S. Mitochondria impact brain function and cognition. Proc. Natl. Acad. Sci. 2014, 111, 7–8. [Google Scholar] [CrossRef] [PubMed]
- Griffin, É.W.; Mullally, S.; Foley, C.; Warmington, S.A.; O’Mara, S.M.; Kelly, Á.M. Aerobic exercise improves hippocampal function and increases BDNF in the serum of young adult males. Physiol. Behav. 2011, 104, 934–941. [Google Scholar] [CrossRef]
- Neeper, S.A.; Gómez-Pinilla, F.; Choi, J.; Cotman, C.W. Physical activity increases mRNA for brain-derived neurotrophic factor and nerve growth factor in rat brain. Brain Res. 1996, 726, 49–56. [Google Scholar] [CrossRef]
- Vaynman, S.; Ying, Z.; Gomez-Pinilla, F. Hippocampal BDNF mediates the efficacy of exercise on synaptic plasticity and cognition. Eur. J. Neurosci. 2004, 20, 2580–2590. [Google Scholar] [CrossRef]
- Yanagisawa, H.; Dan, I.; Tsuzuki, D.; Kato, M.; Okamoto, M.; Kyutoku, Y.; Soya, H. Acute moderate exercise elicits increased dorsolateral prefrontal activation and improves cognitive performance with Stroop test. Neuroimage 2010, 50, 1702–1710. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Higgins JPT, & Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Cochrane, 2011.
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg. Med. J. 2020, 37, 387–387. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.S.-L.; Wilczynski, N.L.; Haynes, R.B. ; Hedges Team Developing optimal search strategies for detecting clinically relevant qualitative studies in MEDLINE. Stud. Health Technol. Inform. 2004, 107, 311–6. [Google Scholar] [PubMed]
- Group CCCR Data extraction template for included studies; 2016.
- Higgins, J.D.J. Selecting studies and collecting data. In Cochrane Handbook for Systematic Reviews of Interventions Version 510; S.Green, J.P.T.H.&, Ed.; The Cochrane Collaboration, 2011; pp. 168–182.
- Lee, D.K.; In, J.; Lee, S. Standard deviation and standard error of the mean. Korean J. Anesthesiol. 2015, 68, 220. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Silva, A.F.; Afonso, J.; Sampaio, A.; Pimenta, N.; Lima, R.F.; Castro, H. de O.; Ramirez-Campillo, R.; Teoldo, I.; Sarmento, H.; González Fernández, F.; et al. Differences in visual search behavior between expert and novice team sports athletes: A systematic review with meta-analysis. Front. Psychol. 2022; 13. [Google Scholar] [CrossRef]
- Drevon, D.; Fursa, S.R.; Malcolm, A.L. Intercoder Reliability and Validity of WebPlotDigitizer in Extracting Graphed Data. Behav. Modif. 2017, 41, 323–339. [Google Scholar] [CrossRef]
- Claudino, J.G.; Afonso, J.; Sarvestan, J.; Lanza, M.B.; Pennone, J.; Filho, C.A.C.; Serrão, J.C.; Espregueira-Mendes, J.; Vasconcelos, A.L.V.; de Andrade, M.P.; et al. Strength Training to Prevent Falls in Older Adults: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 3184. [Google Scholar] [CrossRef] [PubMed]
- Park, J, Lee Y, Seo H, Jang B, Son H, Kim S, Shin S, & H.S. Risk of Bias Assessment tool for Non-randomized Studies (RoBANS): Development and validation of a new instrument. In Proceedings of the 19th Cochrane Colloquium; 2011; pp. 19–22.
- Ramirez-Campillo, R.; Castillo, D.; Raya-González, J.; Moran, J.; de Villarreal, E.S.; Lloyd, R.S. Effects of Plyometric Jump Training on Jump and Sprint Performance in Young Male Soccer Players: A Systematic Review and Meta-analysis. Sport. Med. 2020, 50, 2125–2143. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Campillo, R.; Sanchez-Sanchez, J.; Romero-Moraleda, B.; Yanci, J.; García-Hermoso, A.; Manuel Clemente, F. Effects of plyometric jump training in female soccer player’s vertical jump height: A systematic review with meta-analysis. J. Sports Sci. 2020, 38, 1475–1487. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sport. Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Sanchéz, M.A.; Bustos-Cruz, R.H.; Velasco-Orjuela, G.P.; Quintero, A.P.; Tordecilla-Sanders, A.; Correa-Bautista, J.E.; Triana-Reina, H.R.; García-Hermoso, A.; González-Ruíz, K.; Peña-Guzmán, C.A.; et al. Acute Effects of High Intensity, Resistance, or Combined Protocol on the Increase of Level of Neurotrophic Factors in Physically Inactive Overweight Adults: The BrainFit Study. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef]
- Roh, H.-T.; Cho, S.-Y.; So, W.-Y. Obesity promotes oxidative stress and exacerbates blood-brain barrier disruption after high-intensity exercise. J. Sport Heal. Sci. 2017, 6, 225–230. [Google Scholar] [CrossRef]
- Wheeler, M.J.; Green, D.J.; Ellis, K.A.; Cerin, E.; Heinonen, I.; Naylor, L.H.; Larsen, R.; Wennberg, P.; Boraxbekk, C.-J.; Lewis, J.; et al. Distinct effects of acute exercise and breaks in sitting on working memory and executive function in older adults: a three-arm, randomised cross-over trial to evaluate the effects of exercise with and without breaks in sitting on cognition. Br. J. Sports Med. 2020, 54, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Roh, H.T. Effects of aerobic exercise training on peripheral brain-derived neurotrophic factor and eotaxin-1 levels in obese young men. J. Phys. Ther. Sci. 2016, 28, 1355–1358. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-Y.; So, W.-Y.; Roh, H.-T. Effects of aerobic exercise training and cranial electrotherapy stimulation on the stress-related hormone, the neurotrophic factor, and mood states in obese middle-aged women: a pilot clinical trial. Salud Ment. 2016, 39, 249–256. [Google Scholar] [CrossRef]
- Damirchi, A.; Tehrani, B.S.; Alamdari, K.A.; Babaei, P. Influence of Aerobic Training and Detraining on Serum BDNF, Insulin Resistance, and Metabolic Risk Factors in Middle-Aged Men Diagnosed With Metabolic Syndrome. Clin. J. Sport Med. 2014, 24, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Glud, M.; Christiansen, T.; Larsen, L.H.; Richelsen, B.; Bruun, J.M. Changes in Circulating BDNF in relation to Sex, Diet, and Exercise: A 12-Week Randomized Controlled Study in Overweight and Obese Participants. J. Obes. 2019, 2019, 1–7. [Google Scholar] [CrossRef]
- Goldfield, G.S.; Kenny, G.P.; Prud’homme, D.; Holcik, M.; Alberga, A.S.; Fahnestock, M.; Cameron, J.D.; Doucette, S.; Hadjiyannakis, S.; Tulloch, H.; et al. Effects of aerobic training, resistance training, or both on brain-derived neurotrophic factor in adolescents with obesity: The hearty randomized controlled trial. Physiol. Behav. 2018, 191, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Gyorkos, A.; Baker, M.H.; Miutz, L.N.; Lown, D.A.; Jones, M.A.; Houghton-Rahrig, L.D. Carbohydrate-restricted Diet and Exercise Increase Brain-derived Neurotrophic Factor and Cognitive Function: A Randomized Crossover Trial. Cureus 2019, 11, e5604. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Yoo, J.H.; Kang, S.; Woo, J.H.; Shin, K.O.; Kim, K.B.; Cho, S.Y.; Roh, H.T.; Kim, Y. Il The Effects of 12 Weeks Regular Aerobic Exercise on Brain-derived Neurotrophic Factor and Inflammatory Factors in Juvenile Obesity and Type 2 Diabetes Mellitus. J. Phys. Ther. Sci. 2014, 26, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Levinger, I.; Goodman, C.; Matthews, V.; Hare, D.L.; Jerums, G.; Garnham, A.; Selig, S. BDNF, Metabolic Risk Factors, and Resistance Training in Middle-Aged Individuals. Med. Sci. Sport. Exerc. 2008, 40, 535–541. [Google Scholar] [CrossRef]
- Li, X.; Han, T.; Zou, X.; Zhang, H.; Feng, W.; Wang, H.; Shen, Y.; Zhang, L.; Fang, G. Long-term high-intensity interval training increases serum neurotrophic factors in elderly overweight and obese Chinese adults. Eur. J. Appl. Physiol. 2021, 121, 2773–2785. [Google Scholar] [CrossRef]
- Osali, A. Aerobic exercise and nano-curcumin supplementation improve inflammation in elderly females with metabolic syndrome. Diabetol. Metab. Syndr. 2020, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Roh, H.-T.; So, W.-Y. The effects of aerobic exercise training on oxidant–antioxidant balance, neurotrophic factor levels, and blood–brain barrier function in obese and non-obese men. J. Sport Heal. Sci. 2017, 6, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Saleh V, Afroundeh R, Siahkohiyan M, & A.A. Anaerobic gymnastics exercises evoke systemic brain-derived neurotrophic factor in obese and normal-weight children. Int. J. Pediatr. 2020; 8, 12533–12544. [CrossRef]
- Žlibinaitė, L.; Solianik, R.; Vizbaraitė, D.; Mickevičienė, D.; Skurvydas, A. The Effect of Combined Aerobic Exercise and Calorie Restriction on Mood, Cognition, and Motor Behavior in Overweight and Obese Women. J. Phys. Act. Heal. 2020, 17, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhou, H.; Luo, Q.; Cui, S. The effect of physical exercise on circulating brain-derived neurotrophic factor in healthy subjects: A meta-analysis of randomized controlled trials. Brain Behav. 2022, 12, e2544. [Google Scholar] [CrossRef] [PubMed]
- Dinoff, A.; Herrmann, N.; Swardfager, W.; Lanctôt, K.L. The effect of acute exercise on blood concentrations of brain-derived neurotrophic factor in healthy adults: a meta-analysis. Eur. J. Neurosci. 2017, 46, 1635–1646. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Larsen, K.T.; Ried-Larsen, M.; Møller, N.C.; Andersen, L.B. The effects of physical activity and exercise on brain-derived neurotrophic factor in healthy humans: A review. Scand. J. Med. Sci. Sports 2014, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Szuhany, K.L.; Bugatti, M.; Otto, M.W. A meta-analytic review of the effects of exercise on brain-derived neurotrophic factor. J. Psychiatr. Res. 2015, 60, 56–64. [Google Scholar] [CrossRef]
- Marinus, N.; Hansen, D.; Feys, P.; Meesen, R.; Timmermans, A.; Spildooren, J. The Impact of Different Types of Exercise Training on Peripheral Blood Brain-Derived Neurotrophic Factor Concentrations in Older Adults: A Meta-Analysis. Sport. Med. 2019, 49, 1529–1546. [Google Scholar] [CrossRef]
- Knaepen, K.; Goekint, M.; Heyman, E.M.; Meeusen, R. Neuroplasticity – Exercise-Induced Response of Peripheral Brain-Derived Neurotrophic Factor. Sport. Med. 2010, 40, 765–801. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Álvarez-Bueno, C.; Martínez-Ortega, I.A.; Martínez-Vizcaíno, V.; Mesas, A.E.; Notario-Pacheco, B. Immediate effect of high-intensity exercise on brain-derived neurotrophic factor in healthy young adults: A systematic review and meta-analysis. J. Sport Heal. Sci. 2022, 11, 367–375. [Google Scholar] [CrossRef]
- Fujimura, H.; Altar, C.A.; Chen, R.; Nakamura, T.; Nakahashi, T.; Kambayashi, J.; Sun, B.; Tandon, N.N. Brain-derived neurotrophic factor is stored in human platelets and released by agonist stimulation. Thromb. Haemost. 2002, 87, 728–34. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.I.; Smith, L.; Northey, J.; Rattray, B.; Cherbuin, N. Towards an understanding of the physical activity-BDNF-cognition triumvirate: A review of associations and dosage. Ageing Res. Rev. 2020, 60, 101044. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.J.; Scribbans, T.D.; Bentley, R.F.; Kellawan, J.M.; Gurd, B.; Tschakovsky, M.E. Neurotrophic growth factor responses to lower body resistance training in older adults. Appl. Physiol. Nutr. Metab. 2016, 41, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Bechara, R.G.; Lyne, R.; Kelly, Á.M. BDNF-stimulated intracellular signalling mechanisms underlie exercise-induced improvement in spatial memory in the male Wistar rat. Behav. Brain Res. 2014, 275, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Inoue, D.S.; Monteiro, P.A.; Gerosa-Neto, J.; Santana, P.R.; Peres, F.P.; Edwards, K.M.; Lira, F.S. Acute increases in brain-derived neurotrophic factor following high or moderate-intensity exercise is accompanied with better cognition performance in obese adults. Sci. Rep. 2020, 10, 13493. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.; Vaynman, S.; Akhavan, M.; Ying, Z.; Gomez-Pinilla, F. Insulin-like growth factor I interfaces with brain-derived neurotrophic factor-mediated synaptic plasticity to modulate aspects of exercise-induced cognitive function. Neuroscience 2006, 140, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Saucedo Marquez, C.M.; Vanaudenaerde, B.; Troosters, T.; Wenderoth, N. High-intensity interval training evokes larger serum BDNF levels compared with intense continuous exercise. J. Appl. Physiol. 2015, 119, 1363–1373. [Google Scholar] [CrossRef]
- Rios, M. BDNF and the central control of feeding: accidental bystander or essential player? Trends Neurosci. 2013, 36, 83–90. [Google Scholar] [CrossRef]
- Cordeira, J.; Rios, M. Weighing in the Role of BDNF in the Central Control of Eating Behavior. Mol. Neurobiol. 2011, 44, 441–448. [Google Scholar] [CrossRef]
- Xu, B.; Xie, X. Neurotrophic factor control of satiety and body weight. Nat. Rev. Neurosci. 2016, 17, 282–292. [Google Scholar] [CrossRef]
- Pandit, M.; Behl, T.; Sachdeva, M.; Arora, S. Role of brain derived neurotropic factor in obesity. Obes. Med. 2020, 17, 100189. [Google Scholar] [CrossRef]
- Alomari, M.A.; Khabour, O.F.; Alawneh, K.; Alzoubi, K.H.; Maikano, A.B. The importance of physical fitness for the relationship of BDNF with obesity measures in young normal-weight adults. Heliyon 2020, 6, e03490. [Google Scholar] [CrossRef]
- Lee, I.-T.; Wang, J.-S.; Fu, C.-P.; Lin, S.-Y.; Sheu, W.H.-H. Relationship between body weight and the increment in serum brain-derived neurotrophic factor after oral glucose challenge in men with obesity and metabolic syndrome. Medicine (Baltimore). 2016, 95, e5260. [Google Scholar] [CrossRef] [PubMed]
- Murawska-Ciałowicz, E.; Wiatr, M.; Ciałowicz, M.; Gomes de Assis, G.; Borowicz, W.; Rocha-Rodrigues, S.; Paprocka-Borowicz, M.; Marques, A. BDNF Impact on Biological Markers of Depression—Role of Physical Exercise and Training. Int. J. Environ. Res. Public Health 2021, 18, 7553. [Google Scholar] [CrossRef] [PubMed]
- Suwa, M.; Yamamoto, K.-I.; Nakano, H.; Sasaki, H.; Radak, Z.; Kumagai, S. Brain-Derived Neurotrophic Factor Treatment Increases the Skeletal Muscle Glucose Transporter 4 Protein Expression in Mice. Physiol. Res. 2010, 59, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.L.; Whitehurst, M.; Fico, B.G.; Dodge, K.M.; Ferrandi, P.J.; Pena, G.; Adelman, A.; Huang, C.-J. Acute high-intensity interval exercise induces greater levels of serum brain-derived neurotrophic factor in obese individuals. Exp. Biol. Med. 2018, 243, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Chaldakov, G.N.; Tonchev, A.B.; Aloe, L. NGF and BDNF: from nerves to adipose tissue, from neurokines to metabokines. Riv. Psichiatr. 2009, 44, 79–87. [Google Scholar] [PubMed]
- Magistretti, P.J.; Allaman, I. Lactate in the brain: from metabolic end-product to signalling molecule. Nat. Rev. Neurosci. 2018, 19, 235–249. [Google Scholar] [CrossRef]
- Proia, P.; Di Liegro, C.; Schiera, G.; Fricano, A.; Di Liegro, I. Lactate as a Metabolite and a Regulator in the Central Nervous System. Int. J. Mol. Sci. 2016, 17, 1450. [Google Scholar] [CrossRef]
- Müller, P.; Duderstadt, Y.; Lessmann, V.; Müller, N.G. Lactate and BDNF: Key Mediators of Exercise Induced Neuroplasticity? J. Clin. Med. 2020, 9, 1136. [Google Scholar] [CrossRef]
- Adeva-Andany, M.; López-Ojén, M.; Funcasta-Calderón, R.; Ameneiros-Rodríguez, E.; Donapetry-García, C.; Vila-Altesor, M.; Rodríguez-Seijas, J. Comprehensive review on lactate metabolism in human health. Mitochondrion 2014, 17, 76–100. [Google Scholar] [CrossRef]
- Bergersen, L.H. Is lactate food for neurons? Comparison of monocarboxylate transporter subtypes in brain and muscle. Neuroscience 2007, 145, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Dienel, G.A. The metabolic trinity, glucose–glycogen–lactate, links astrocytes and neurons in brain energetics, signaling, memory, and gene expression. Neurosci. Lett. 2017, 637, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Stern, S.A.; Bozdagi, O.; Huntley, G.W.; Walker, R.H.; Magistretti, P.J.; Alberini, C.M. Astrocyte-Neuron Lactate Transport Is Required for Long-Term Memory Formation. Cell 2011, 144, 810–823. [Google Scholar] [CrossRef] [PubMed]
- Steinman, M.Q.; Gao, V.; Alberini, C.M. The Role of Lactate-Mediated Metabolic Coupling between Astrocytes and Neurons in Long-Term Memory Formation. Front. Integr. Neurosci. 2016, 10. [Google Scholar] [CrossRef] [PubMed]
- Jodeiri Farshbaf, M.; Ghaedi, K.; Megraw, T.L.; Curtiss, J.; Shirani Faradonbeh, M.; Vaziri, P.; Nasr-Esfahani, M.H. Does PGC1α/FNDC5/BDNF Elicit the Beneficial Effects of Exercise on Neurodegenerative Disorders? NeuroMolecular Med. 2016, 18, 1–15. [Google Scholar] [CrossRef] [PubMed]
- El Hayek, L.; Khalifeh, M.; Zibara, V.; Abi Assaad, R.; Emmanuel, N.; Karnib, N.; El-Ghandour, R.; Nasrallah, P.; Bilen, M.; Ibrahim, P.; et al. Lactate mediates the effects of exercise on learning and memory through SIRT1-dependent activation of hippocampal brain-derived neurotrophic factor (BDNF). J. Neurosci. 2019, 1661–18. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, R.; Meng, Y.; Li, S.; Donelan, W.; Zhao, Y.; Qi, L.; Zhang, M.; Wang, X.; Cui, T.; et al. Irisin Stimulates Browning of White Adipocytes Through Mitogen-Activated Protein Kinase p38 MAP Kinase and ERK MAP Kinase Signaling. Diabetes 2014, 63, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Qiao, X.; Ma, Y.; Deng, H.; Xu, C.C.; Xu, L. Disordered metabolism in mice lacking irisin. Sci. Rep. 2020, 10, 17368. [Google Scholar] [CrossRef]
- Murawska-Cialowicz, E.; Wolanski, P.; Zuwala-Jagiello, J.; Feito, Y.; Petr, M.; Kokstejn, J.; Stastny, P.; Goliński, D. Effect of HIIT with Tabata Protocol on Serum Irisin, Physical Performance, and Body Composition in Men. Int. J. Environ. Res. Public Health 2020, 17, 3589. [Google Scholar] [CrossRef]
- Archundia-Herrera, C.; Macias-Cervantes, M.; Ruiz-Muñoz, B.; Vargas-Ortiz, K.; Kornhauser, C.; Perez-Vazquez, V. Muscle irisin response to aerobic vs HIIT in overweight female adolescents. Diabetol. Metab. Syndr. 2017, 9, 101. [Google Scholar] [CrossRef]
- Dinoff, A.; Herrmann, N.; Swardfager, W.; Liu, C.S.; Sherman, C.; Chan, S.; Lanctôt, K.L. The Effect of Exercise Training on Resting Concentrations of Peripheral Brain-Derived Neurotrophic Factor (BDNF): A Meta-Analysis. PLoS One 2016, 11, e0163037. [Google Scholar] [CrossRef] [PubMed]
- Shobeiri, P.; Karimi, A.; Momtazmanesh, S.; Teixeira, A.L.; Teunissen, C.E.; van Wegen, E.E.H.; Hirsch, M.A.; Yekaninejad, M.S.; Rezaei, N. Exercise-induced increase in blood-based brain-derived neurotrophic factor (BDNF) in people with multiple sclerosis: A systematic review and meta-analysis of exercise intervention trials. PLoS One 2022, 17, e0264557. [Google Scholar] [CrossRef]
- Ruiz-González, D.; Hernández-Martínez, A.; Valenzuela, P.L.; Morales, J.S.; Soriano-Maldonado, A. Effects of physical exercise on plasma brain-derived neurotrophic factor in neurodegenerative disorders: A systematic review and meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2021, 128, 394–405. [Google Scholar] [CrossRef]
- Fleitas, J.C.; Hammuod, S.F.P.; Kakuta, E.; Loreti, E.H. A meta-analysis of the effects of physical exercise on peripheral levels of a brain-derived neurotrophic factor in the elderly. Biomarkers 2022, 27, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Begliuomini, S.; Lenzi, E.; Ninni, F.; Casarosa, E.; Merlini, S.; Pluchino, N.; Valentino, V.; Luisi, S.; Luisi, M.; Genazzani, A.R. Plasma brain-derived neurotrophic factor daily variations in men: correlation with cortisol circadian rhythm. J. Endocrinol. 2008, 197, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Gejl, A.K.; Enevold, C.; Bugge, A.; Andersen, M.S.; Nielsen, C.H.; Andersen, L.B. Associations between serum and plasma brain-derived neurotrophic factor and influence of storage time and centrifugation strategy. Sci. Rep. 2019, 9, 9655. [Google Scholar] [CrossRef]
- Roeh, A.; Holdenrieder, S.; Schoenfeld, J.; Haeckert, J.; Halle, M.; Falkai, P.; Scherr, J.; Hasan, A. Decreased Serum Brain-Derived Neurotrophic Factor Concentrations 72 Hours Following Marathon Running. Front. Physiol. 2021, 12. [Google Scholar] [CrossRef]
- Azevedo, K.P.M. de; de Oliveira, V.H.; Medeiros, G.C.B.S. de; Mata, Á.N. de S.; García, D.Á., Martínez, D.G., Leitão, J.C., Knackfuss, M.I., Eds.; Piuvezam, G. The Effects of Exercise on BDNF Levels in Adolescents: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6056. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2020 flow diagram.
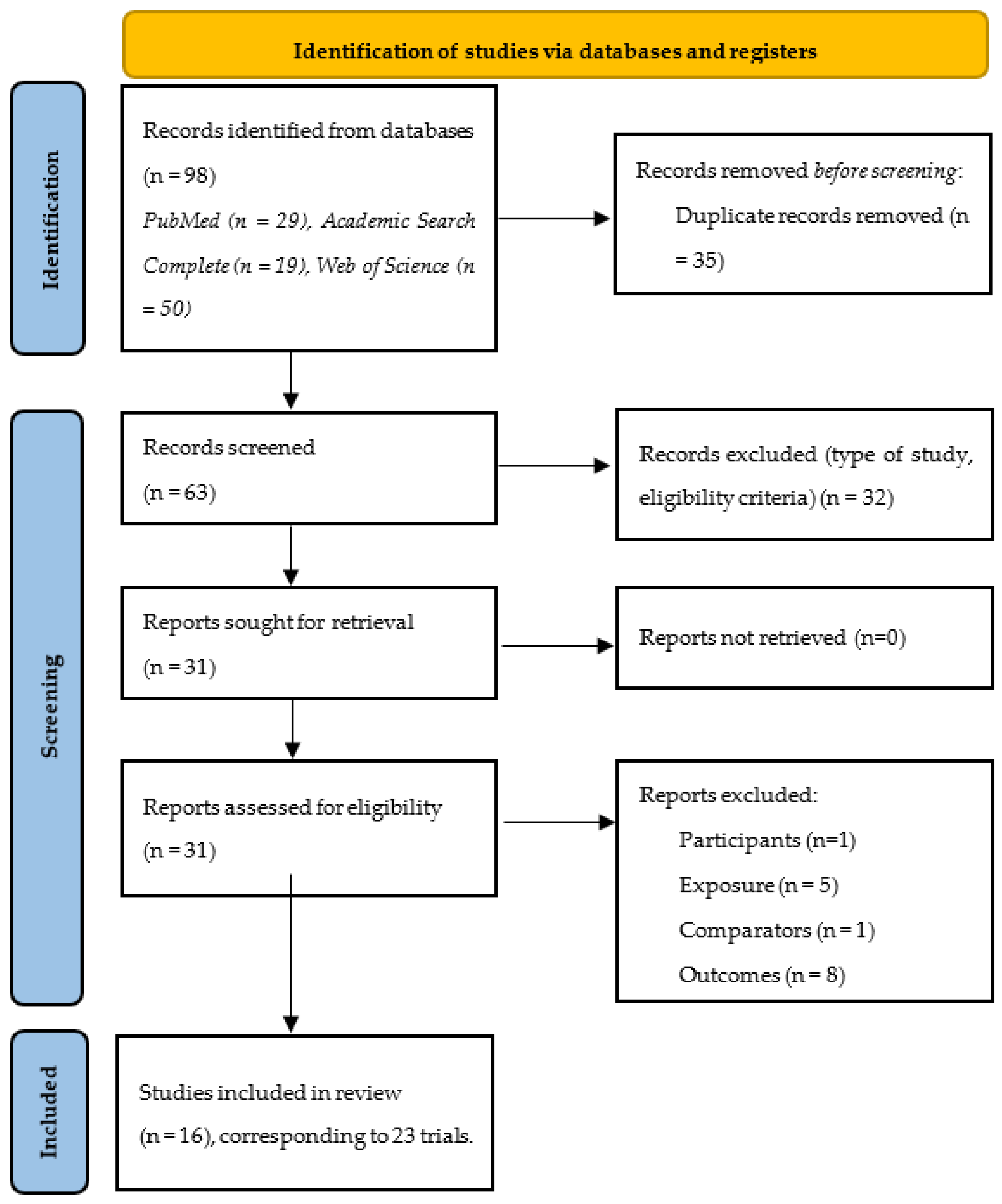
Figure 2.
Forest plot illustrating acute exercise-related improvements in BDNF levels in comparison to controls. Forest plot values are shown as effect sizes (Hedges’ g) with 95% confidence intervals (CI). Black squares: individual studies. The size represents the relative weight. Black rhomboid: summary value. Mean results: ES = 1.25, 95% CI = 0.19 to 2.30, p=0.021, I2 = 80.4%, N total participants = 104.
Figure 2.
Forest plot illustrating acute exercise-related improvements in BDNF levels in comparison to controls. Forest plot values are shown as effect sizes (Hedges’ g) with 95% confidence intervals (CI). Black squares: individual studies. The size represents the relative weight. Black rhomboid: summary value. Mean results: ES = 1.25, 95% CI = 0.19 to 2.30, p=0.021, I2 = 80.4%, N total participants = 104.
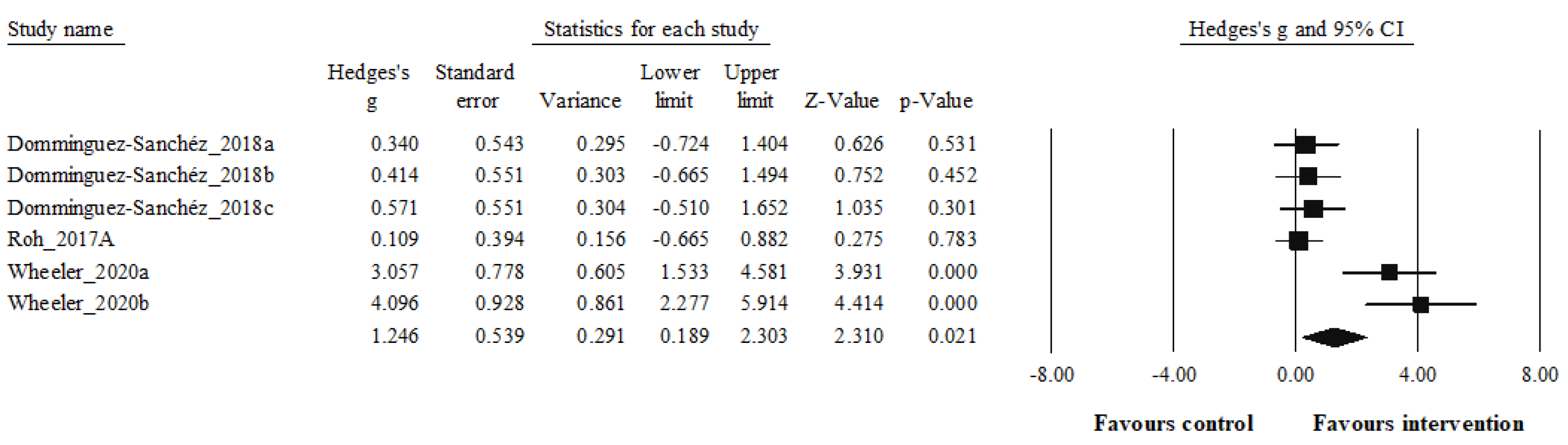
Figure 3.
Forest plot illustrating exercise intervention-related improvements in BDNF lev-els in comparison to controls. Forest plot values are shown as effect sizes (Hedges’ g) with 95% confidence intervals (CI). Black squares: individual studies. The size represents the relative weight. Black rhomboid: summary value. Mean results: ES = 0.49, 95% CI = -0.08 to 1.06, p=0.089, I2 = 88.7%, N total participants = 571.
Figure 3.
Forest plot illustrating exercise intervention-related improvements in BDNF lev-els in comparison to controls. Forest plot values are shown as effect sizes (Hedges’ g) with 95% confidence intervals (CI). Black squares: individual studies. The size represents the relative weight. Black rhomboid: summary value. Mean results: ES = 0.49, 95% CI = -0.08 to 1.06, p=0.089, I2 = 88.7%, N total participants = 571.
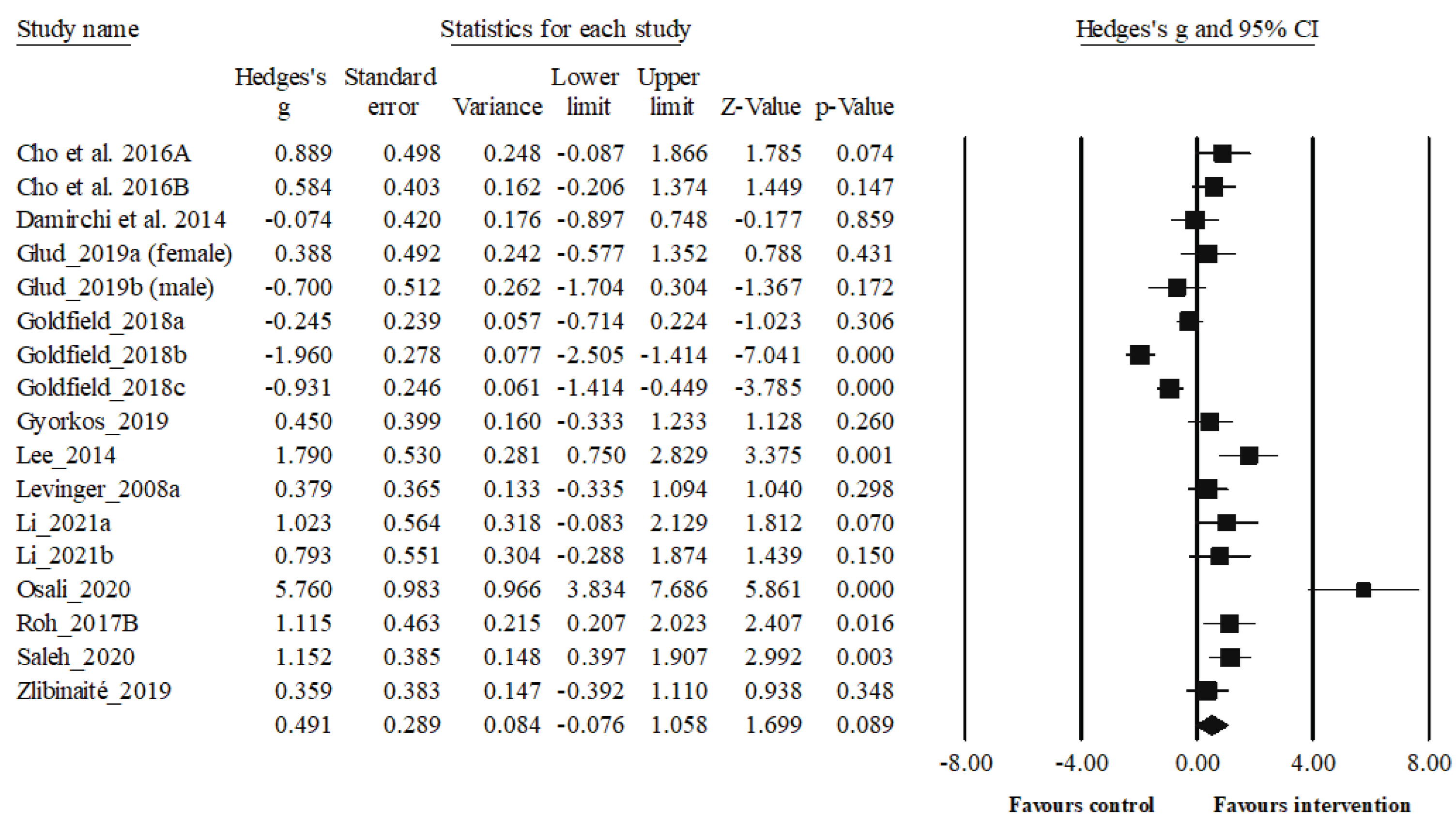

Table 1.
Full search strategy for each database.
| Database | Specificities of the databases | Search Strategy |
|---|---|---|
| PubMed | None to report | ("brain derived neurotrophic factor"[MeSH Terms] OR ("brain derived"[All Fields] AND "neurotrophic"[All Fields] AND "factor"[All Fields]) OR "brain derived neurotrophic factor"[All Fields] OR "bdnf"[All Fields] OR ("brain derived neurotrophic factor"[MeSH Terms] OR ("brain derived"[All Fields] AND "neurotrophic"[All Fields] AND "factor"[All Fields]) OR "brain derived neurotrophic factor"[All Fields] OR ("brain"[All Fields] AND "derived"[All Fields] AND "neurotrophic"[All Fields] AND "factor"[All Fields]) OR "brain derived neurotrophic factor"[All Fields])) AND ("aerobic*"[All Fields] OR "HIIT"[All Fields] OR ("high intensity interval training"[MeSH Terms] OR ("high intensity"[All Fields] AND "interval"[All Fields] AND "training"[All Fields]) OR "high intensity interval training"[All Fields] OR ("high"[All Fields] AND "intensity"[All Fields] AND "interval"[All Fields] AND "training"[All Fields]) OR "high intensity interval training"[All Fields]) OR "anaerobic*"[All Fields]) AND ("obeses"[All Fields] OR "obesity"[MeSH Terms] OR "obesity"[All Fields] OR "obese"[All Fields] OR "obesities"[All Fields] OR "obesity s"[All Fields] OR ("overweight"[MeSH Terms] OR "overweight"[All Fields] OR "overweighted"[All Fields] OR "overweightness"[All Fields] OR "overweights"[All Fields])) |
| Academic Search Complete | Search for title and abstract also includes keywords | "(BDNF OR brain-derived neurotrophic factor) AND (aerobic* OR HIIT OR high intensity interval training OR anaerobic*) AND (obesity OR overweight) |
| Web of Science | Search for title and abstract also includes keywords and its designated “topic” | BDNF OR brain-derived neurotrophic factor (All Fields) and aerobic* OR HIIT OR high intensity interval training OR anaerobic* (All Fields) and obesity OR overweight (All Fields) |
Table 2.
Characteristics of the included studies for acute effect on BDNF level (N: 3, 6 trials).
| Study | Study design | Population (n) | Sex | Sample characteristics | Mean age (years) | BMI (kg/m2) | Training Status |
|---|---|---|---|---|---|---|---|
| Dominguez-Sanchez 2018a,b,c [56] | RCT (parallel-group | 51 Overweight adults (BMI ≥25 and ≤30 kg/m2) | Men | -HIIT group: 14 -RT group: 12 -CT group: 12 -Non-exercising control: 12 |
- HIIT group: 24.5±3.7 - RT group: 22.8±3.1 - CT group: 22.2±3.4 -Non-exercising control: 24.7±3.4 |
-HITT group: 27.4±1.7 -RT group: 27.8±1.3 -CT group: 28.1±1.2 -Non-exercising control: 28.7±2.0 |
Physically inactive |
| Roh et al. 2017a [57] | RCT (parallel-group | 24 obese and non-obese healthy | Men | -Obese group: 12 -Non-obese group: 12 |
-Obese group: 22.9±2.2 -Non-obese group: 22.9±2.2 |
-Obese group: 29.3±3.0 -Non-obese group: 21.5±1.6 |
Untrained |
| Wheeler et al. 2020 a,b [58] | RCT (parallel-group | 65 overweight/obese older adults with normal cognitive function | Men and postmenopausal women (≥55 to ≤80 years; BMI ≥25 kg/m2 to <45 kg/m2) | -Sitting: 22 - EX+SIT: 23 - EX+BR: 20 |
67±7 years | 31.2±4.1 | Sedentary |
Abbreviations: RCT= Randomized controlled trial; BMI= Body mass index; HIIT= High intensity interval training; RT= Resistance training; CT= Combined training; EX+SIT =exercise + sitting; EX+BR= exercise + breaks.
Table 3.
Characteristics of acute exercise protocols and main results.
| Study | Physical Exercise protocol | Comparators | Main outcome | Brand/company name of BDNF kits | Main Results |
|---|---|---|---|---|---|
| Dominguez-Sanchez 2018a,b,c [56] | -HIIT group: 5-min warm-up and ended with a 4-min cooldown at a 65% HRmax; HIIT: four bouts of 4-min intervals at 85– 95% HRmax interspersed with 4 min of active recovery at 75–85% HRmax -RT group: initiated with ≈12–15 repetitions per set of six exercises that targeted all the major muscle groups at high intensity included both upper and lower body large-muscle exercises using weight machines (bicep screw curl, triceps extension, dumbbell side lateral raise, military press, dumbbell squat, and dumbbell front) CG group: underwent both the HIIT and RT protocols, as described above, in that order. |
Non-exercising control: Without exercise training | Plasma BDNF (ng/mL) | SPR Biosensors methods, an amino-coupling chemistry kit KAN-50 Coupling Kit (GE Healthcare, Uppsala, Sweden) | -HIIT group: BDNF increased (+6.8 %, p= 0.134) -RT group: BDNF increased (+9.3 %, p= 0.066) -CT: BDNF increased +11.6 %, p=0.029) -CG: BDNF increased +0.6 %, p=0.804) -Compared to the CG, the greatest increase was as follows: CG (+20.8 %), RT (14.3 %), HIIT (9.8 %) |
| Roh et al. 2017a [57] | Acute exercise on the treadmill was applied to both groups. Treadmill run of 20 min at an intensity of 85% of the anthropometrically measured VO2max (Bruce protocol) | - | Serum BDNF (pg/mL) | Human BDNF enzyme-linked immunosorbent assay (ELISA) kit (cat. no. DBD00; R&D Systems, Minneapolis, MN, USA) |
-BDNF increased in both groups (obese and non-obese) after acute exercise. -Compared to the non-obese, BDNF increased more in the obese group after exercise. |
| Wheeler et al. 2020a,b [58] | -EX+SIT: sitting (1 hour), moderate-intensity walking (30 min, the speed was set at 3.2 km/hour, between 65% and 75% of age predicted HRmax), uninterrupted sitting (6.5 hours), that is, 30 min. aerobic exercise, 109±12 bpm, 71%±8% HRmax, 11±2 RPE -EX+BR: sitting (1 hour), moderate-intensity walking (30 min, the speed was set at 3.2 km/hour, HR between 65% and 75% of age predicted HRmax), sitting interrupted every 30 min with 3 min of light-intensity walking (6.5 hours), that is, 30 min. aerobic exercise 109±12 bpm, 71%±8% HRmax, 11±2 RPE. |
SIT: uninterrupted sitting (8 hours, control) |
Serum BDNF (ng/mL) | Human BDNF ELISA Kits (R&D Systems, Wiesbaden, Germany | -Serum BDNF was increased in both EX+SIT, +171 (−449 to +791, p=0.03 vs SIT), and EX+BR, +139 (−481 to +759, p=0.045 vs SIT), relative to SIT, −227 (−851 to +396). -No significant differeence was observed between EX+SIT and EX+BR |
Abbreviations: RCT= Randomized controlled trial; BDNF= Brain-derived neurotrophic factor; BMI= Body mass index; HIIT= High intensity interval training; RT= Resistance training; CT= Combined Training; CG= Control group; HRmax= maximum heart rate; HRR= Heart rate reserve; VO2max= Maximum oxygen intake; RPE= Rate of perceived exertion; EX+SIT =exercise + sitting; EX+BR= exercise + breaks; SIT= Sitting; bpm= beat per minute; SPR: Surface Plasmon Resonance, Elisa: Enzyme-linked immunosorbent assay.
Table 4.
Characteristics of the included studies for exercise intervention on BDNF level (N: 13, 17 trials).
Table 4.
Characteristics of the included studies for exercise intervention on BDNF level (N: 13, 17 trials).
| Study | Study design | Population (n) | Sex | Sample characteristics | Mean age (years) | BMI (kg/m2) | Training Status |
|---|---|---|---|---|---|---|---|
| Cho et al. 2016a [59] | RCT (parallel-group) | 16 obese young men with a BMI greater than 25 kg/m2. | Men | -EG: 8 -CG: 8 |
-EG: 22.9±2.5 -CG: 22.3±2.1 |
-EG: 28.7±2.5 -CG: 27.7±2.2 |
No participation in regular physical activity programs |
| Cho et al. 2016b [60] | RCT (parallel-group) | 36 obese middle-aged Korean women | Women | -AE group: 12 -AE+CES group: 12 -CG: 12 |
-AE group: 54.83± 2.79 -AE+CES group : 54.75±2.45 -CG: 54.67±3.03 |
-AE group: 26.87±2.15 -AE+CES group: 26.90±2.82 -CG: 26.28±1.67 |
No participation in regular physical activity programs |
| Damirchi et al. 2014 [61] | RCT (parallel-group) | 21 middle-aged men diagnosed with MetS | Men | -EG: 11 -CG: 10 |
-EG: 54.12±2.77 -CG: 55.57±3.45 |
-EG: 29.8±3.75 -CG: 27.04±2.89 |
None of the subjects followed a training program within the past 2 year |
| Glud et al. 2019ab [62] | RCT (parallel-group) | 50 overweight or obese (26 women, 24 men) but healthy individuals | Men and Women | -EXO: 7 women, 9 men -DIO: 8 women, 6 men -DEX: 11 women, 9 men |
-EXO: 31.2±2.9- 35±1.3 -DIO: 32.4±2.4- 37.2±2.7 -DEX: 33.4±2.1-35.1 ± 3.9 |
-EXO: 31.2±2.9- 35±1.3 -DIO: 32.4±2.4- 37.2±2.7 -DEX: 33.4±2.1-35.1 ±3.9 |
Physically inactive |
| Goldfield et al. a,b,c 2018 [63] | RCT (parallel-group) | 282 adolescents with overweight and obesity (84 boys, 198 girls) |
Boys and girls | -AE group: n=69 -RT group: n=70 -CT group: n=74 -CG: n=69 |
-AE group: 15.5±1.3 -RT group: 15.8±1.5 -CT group: 15.5±1.3 -CG: 15.6±1.3 |
-AE group= 34.6±4.2 -RT group= 35.3±4.8 -CT group= 34.5±4.1 -CG= 34.3±5.0 |
Irregularly active |
| Gyorkos et al. 2019 [64] | RCT (parallel-group) | 12 obese with MetS | Free-Living İndividuals | -CRPD-Sed: 5 -CRPD-Ex: 7 |
40.9±20.2 years of age | - | Sedentary (defined as not engaged in physical activity at least 3 days/week for three months) |
Abbreviations: RCT= Randomized controlled trial; BDNF= Brain-derived neurotrophic factor; BMI= Body mass index; MetS=Metabolic syndrome; EG= Exercise Group; RT= Resistance training; CT= Combined Training; CG= Control group; EXO= Exercise-only; DIO= Diet-only; DEX= Diet and exercise; AE= Aerobic exercise; CES=Cranial electrotherapy stimulation; CRPD-Sed= Carbohydrate-restricted paleolithic-based diet with sedentary behavior; CRPD-Ex= Carbohydrate-restricted Paleolithic-based diet with high intensity interval training.
Table 5.
Characteristics of the included studies for exercise intervention on BDNF level (N: 13, 17 trials) (Continuation of Table 4).
Table 5.
Characteristics of the included studies for exercise intervention on BDNF level (N: 13, 17 trials) (Continuation of Table 4).
| Study | Study design | Population (n) | Sex | Sample characteristics | Mean age (years) | BMI (kg/m2) | Training Status |
|---|---|---|---|---|---|---|---|
| Lee et al. 2014 [65] | RCT (parallel-group) | 26 juveniles (boys = 15, girls = 9) | Boys and girls | -Obesity group (OG, n= 8) -T2DM group (TG, n=7) -CG (CG, n = 11) |
-Obesity group= 16.37±0.91 -T2DM group= 15.57±2.14 -CG= 16.45±1.36 |
-Obesity group= 27.47±2.51 -T2DM group= 23.72±4.47 -CG= 22.35±3.94 |
Physically inactive |
| Levinger et al. 2008a [66] | RCT (parallel-group) | 49 men (N = 25) and women (N = 24) | Men and women | -HiMF training: 15 -HiMF control: 14 -LoMF training: 10 -LoMF control: 10 |
-HiMF training: 51.0±7.0 -HiMF control: 51.9±5.8 -LoMF training: 50.3±4.1 -LoMF control : 48.9±7.4 |
-HiMF training: 31.6±4.6 -HiMF control: 30.3±3.7 -LoMF training: 23.9±3.4 -LoMF control: 23.8±3.0 |
Physically inactive |
| Li et al. 2021a,b [67] | RCT (parallel-group) | 29 (18 males and 11 females) older adults | Male and female | -HIIT (group: 10 -VICT group: 10 -CG: 9 |
-HIIT group: 64.9±3.45 -VICT group: 66.4±4.50 -CG: 63.9±3.95 |
-HIIT group: 27.8±1.04 -VICT group: 27.7±2.84 -CG: 27.1±1.50 |
Physically inactive |
| Osali et al. 2020 [68] | RCT (parallel-group) | 44 women with Mets | Women | -MetS exercise+Nano-Curcumin: 11 -MetS exercise: 11 -MetS Nano-Curcumin: 11 -MetS control: 11 |
62.3±1.23 years | MetS exercise+Nano-Curcumin: 31.24±3.12 MetS exercise: 32.22±2.46 MetS Nano-Curcumin: 29.54±2.67 MetS control: 29.02±1.56 |
Pysically inactive (<30 min of physical activity or exercise training per day) |
| Roh et al. 2017b [69] | RCT (parallel-group) | 20 healthy |
Men | -Obese group:10 -Non-obese group: 10 |
-Obese group: 23.00±2.36 -Non-obese group: 22.80±2.35 |
-Obese group: 29.74±3.12 -Non-obese group: 22.00±1.22 |
Physically inactive |
| Saleh et al. 2020 [70] | RCT (parallel-group) | 60 subjects with age range of 8 to 12 years old | -Obese experimental group: 15 -Obese control group: 15 -Normal weight experimental group: 15 -Normal weight control group: 15 |
-Obese experimental group: 10.13±1.35 -Obese control group: 9.80±1.32 -Normal weight experimental group: 9.80±1.47 -Normal weight control group: 9.86±1.30 |
Body fat (%) -Obese experimental group: 27.33±0.67 -Obese control group: 27.03±0.69 -Normal weight experimental group: 6.74±0.35 -Normal weight control group: 6.79±0.45 |
Participants who enrolled in the elementary level of gymnastics | |
| Zibinaite et al. 2019 [71] | RCT (parallel-group) | 26 overweight and obese participants | Women | EG: 13 CG: 13 |
EG: 44.2±8.7 CG: 44.1±5.8 |
EG: 31.9±3.4 CG: 32.5±3.6 |
Women with a sedentary lifestyle (regular exercise ≤1 h/week) |
Abbreviations: RCT= Randomized controlled trial; BDNF= Brain-derived neurotrophic factor; MetS=Metabolic syndrome; T2DM= Type 2 diabetes mellitus; HiMF= number of metabolic risk factors ≥2; LoMF= number of metabolic risk factors ≤1; HIIT= High intensity interval training; VICT = Vigorous-intensity continuous training; EG= Exercise group; CG= Control Group.
Table 6.
Characteristics of exercise intervention and main results.
| Study | Physical Exercise protocol | Comparators | Main outcome | Brand/company name of BDNF kits | Main Results |
|---|---|---|---|---|---|
| Cho et al. 2016a [59] | EG had undergone the supervised treadmill running exercise [70% of the HRR, 40 min each] sessions 3 times a week for 8 weeks | CG just maintained their usual lifestyles | Serum BDNF (ng/mL) | A human BDNF ELISA Kit (R&D Systems, Minneapolis, MN, USA). | After intervention, BDNF increased significantly only in EG (20.56 %) |
| Cho et al. 2016b [60] | The AE group was subjected to three sessions of 40-minute treadmill running a week for 8 weeks. The program consisted of 10-minutes of warm-up stretching before the exercise and 10-minutes of cool-down stretching after the exercise. Exercise intensity of treadmill running was set at 70% of HRR determined using Karvonen’s formula. | CG maintained their own lifestyles with no intervention. | Serum BDNF (pg/mL) | A human BDNF ELISA Kit (Cat. no. DBD00; R&D Systems, Minneapolis, MN, USA) |
Serum BDNF levels were significantly increased in the AE group compared to CG (p <.05). |
| Damirchi et al. 2014 [61] | The participants followed a 6-week aerobic training Programs (3 sessions per week; 25-40 minutes walking, running by 50%-60% of V̇O2peak adjusted by heart rate determined by a graded exercise test. There were 20 minutes for warm-up and calisthenics at the beginning of each session and also a 10-minute cool down period at the end. |
The CG was asked not to change their sedentary lifestyle during the study | Serum BDNF (pg/mL) | A human BDNF ELISA Kit (R&D Systems, Minneapolis, MN, USA) | High BDNF level in patients with MetS decreased significantly after AE. |
| Glud et al. 2019ab [62] | -EXO; 12 weeks of aerobic exercise and isocaloric diet= The exercise consisted of supervised aerobic exercise three times per week with a duration of 60–75 min per training session, an estimated energy expenditure of 500–600 kcal per session, and an intensity of 70% of HRR -DEX; 12 weeks of aerobic exercise in parallel with 8 weeks of VLED (800 kcal/day) followed by a 4-week weight maintenance diet) |
DIO; 8 weeks of VLED 600 kcal/day followed by a 4-week weight maintenance diet | Serum BDNF (ng/mL) | Quantikine ELISA Human Free BDNF immunoassay (DBD00, R&D Systems, Abingdon OX14, UK) |
EXO: BDNF decreased significantly 22.4% in women, and 22.1% in men DIO: BDNF decreased significantly 29.9% in women, and 4.2% in men DEX: BDNF decreased significantly 32.5% in women. |
| Goldfield et al. a,b,c 2018 [63] | -AE group: Aerobic group exercised on treadmills, elliptical machines and/or bicycle ergometers (6 months intervention, twice a week, 20–45 min, 65–85% HRmax) -RT group: 6 months intervention, twice a week, RT group also progressed from 20 to 45 min per session, performing 7 exercises using weight machines or free weights, and progressing from 2 sets of 15 repetitions at moderate intensity to 3 sets of 8 repetitions at the maximum resistance that could be moved 8 times (8-RM)) -CT group: aerobic+resistance |
The CG received only dietary counselling with no exercise prescription | Serum BDNF (ng/mL) | Human Free BDNF Quantikine ELISA kit, R&D systems, Cat# DBD00) | No significant within- or between-group changes in BDNF level. Although not significant, after 6 months intervention; AE group: (+1.80) RT group: (−2.00) CT group: (−1.70) |
Abbreviations: RCT= Randomized controlled trial; BDNF= Brain-derived neurotrophic factor; MetS=Metabolic syndrome; HRR= Heart rate reserve; EG= Exercise Group; AE= Aerobic exercise; CT= Combined Training; CG= Control group HRmax= maximum heart rate; V̇O2peak= Highest oxygen uptake; 1RM=1 repetition maximum; EXO= Exercise-only; DIO= Diet-only; DEX= Diet and exercise; VLED= very low energy diet; Elisa: Enzyme-linked immunosorbent assay.
Table 7.
Characteristics of exercise intervention and main results (Continuation of Table 6).
Table 7.
Characteristics of exercise intervention and main results (Continuation of Table 6).
| Study | Physical Exercise protocol | Comparators | Main outcome | Brand/company name of BDNF kits | Main Results |
|---|---|---|---|---|---|
| Gyorkos et al. 2019 [64] | Each session consisted of HIIT on a cycle ergometer, including a 3-min warm-up, 10 x 60s cycling intervals interspersed with 60s of active recovery, ~90% HRmax, and a 3-min cool down, 3 day/week for four-week. | -CRPD-Sed: (<50gCHO) | Serum BDNF (ng/mL) |
Human BDNF Elisa Kit (#DBD00, Thermo Fisher Scientific) | -Basal BDNF protein content was significantly increased following CRPD-Sed (+20%; P < 0.05) and CRPD-Ex (+38%; p< 0.05) when compared to baseline. -The addition of HIIT exercise to the diet resulted in a significant increase in circulating serum BDNF when compared to CRPD-Sed. |
| Lee et al. 2014 [65] | Aerobic exercise was conducted for a total of 40–60 minutes per session at a VO2max of 50~60%, 3 sessions a week, for 12 weeks. |
-CG maintained their own lifestyles with no intervention. |
Serum BDNF (pg/mL) | A human BDNF Elisa Kit (R&D Systems, Minneapolis, MN, USA) | -There was an increase in BDNF level after 12 weeks of regular aerobic exercise program, only in the obese group. |
| Levinger et al. 2008a [66] | 10 weeks, two sets of 15–20 repetitions at 40–50% 1RM. From weeks 2–10, participants performed each exercise for three sets, 8–20 repetitions, at 50–85% 1RM. | CG: did not perform regular exercise during the study period. | Serum BDNF (pg/mL) | Human BDNF Elisa Kit (Catalog number: DY248; Minneapolis, MN) |
-Resistance training had no effect on BDNF levels or other risk factors for MetS. |
| Li et al. 2021a,b [67] | HIIT: 4 × 3 min at 90% VO2max interspersed with 3 min at 60% VO2max, about 45 min., 3 training sessions per week for 12 week, VICT: 25 min at 70% VO2max, about 45 min.,3 training sessions per week for 12 week |
The subjects in the CG lived normally and did not participate in any training | Serum BDNF (pg/mL) | Human BDNF Elisa Kit (Abcam Inc., Cambridge, UK) | -BDNF increased significantly in both HIIT and VICT group. -There was no significant difference between HIIT and VICT in terms of BDNF. |
| Osali et al. 2020 [68] | Exercise with moderate intensity: Each subject walked or ran at 65–75% HRR on a treadmill for 3×12–17 min, 6 weeks. | continued the regular daily life | Serum BDNF (pg/mL) | Human BDNF Elisa Kits (Adipo Bioscience, USA) | BDNF increased significantly in EG |
| Roh et al. 2017b [69] | Subjects performed treadmill exercise for 40 min 3 times weekly for 8 weeks at 70% HRR, totally 60 min.exercise program | Non-obese | Serum BDNF (pg/mL) | Human BDNF ELISA Kit (#DBD00; R&D Systems, Minneapolis, MN, USA) |
BDNF increased significantly only in obese group, not non-obese group. |
| Saleh et al. 2020 [70] | 45 minutes anaerobic gymnastics exercise including 10-minute warm up, 30- minutes of main exercises, and 5 minutes cool down, 3 times per week for 8 weeks. | Normal weight and obese control groups continued the regular daily life | Saliva BDNF (pg/mL) | Human BDNF PicoKine™ ELISA Kit (Catalog No. EK0307; R&D Systems, Austria) |
BDNF increased in obese group (+33.80%, p=0.002), and normal-weight group (+31.36%, p=0.003). |
| Zibinaite et al. 2019 [71] | Participants underwent 72 supervised aerobic exercise training sessions on cycle ergometers during 6 months, including 3 sessions of training per week. A 50 min aerobic training 80 at an intensity between 60% and 70% of the HRmax was performed. | CG did not undergo any intervention and were instructed to maintain their regular physical activity and diet regime for 6 months | Serum BDNF (pg/mL) | Human BDNF Elisa Kits (Gemini; Stratec Biomedical, Birkenfeld, Germany). | BDNF level remained unchanged (p>0.05) |
Abbreviations: BDNF= Brain-derived neurotrophic factor; CG= Control group; HIIT= High intensity interval training; VICT = Vigorous-intensity continuous training; 1RM=1 repetition maximum; HRmax= maximum heart rate; HRR= Heart rate reserve; VO2max= Maximum oxygen intake; CRPD-Sed=carbohydrate-restricted Paleolithic-based diet with sedentary behavior; CRPD-Ex= Carbohydrate-restricted Paleolithic-based diet with exercise. Elisa: enzyme-linked immunosorbent assay; MetS=Metabolic syndrome Risk of bias in individual studies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



