
Submitted:
22 March 2024
Posted:
25 March 2024
You are already at the latest version
Abstract
Introduction
Blunt carotid injuries (BCI) in pediatric trauma are quite rare. Due to the low number of cases, only a few reports and studies have been conducted on this topic. This review will discuss how frequent BCI/ BCVI on pediatric patients after blunt trauma is, what routine diagnostics look like, if a CT/ CTA scan on pediatric patients after blunt trauma is always necessary and if there are any negative health effects?
Methods
This literature review includes reviews, systematic reviews, case reports and original studies in english language between 1999 and 2020 that have dealt with pediatric blunt trauma and the diagnostics of BCI and BCVI. Furthermore, publications on the risk of radiation exposure on children were included in the study. For literature research, Medline (PubMed) and the Cochrane library were used.
Results
Pediatric BCI/ BCVI, shows an overall incidence between 0.03 – 0.5% of confirmed BCI/ BCVI cases due to pediatric blunt trauma. 1.1 – 3.5% of pediatric blunt trauma patients underwent CTA to detect BCI. Only 0.17 – 1.2% of all CTA scans shows a positive diagnosis for BCI. In children, the median volume CT dose index on a non-contrast head CT is 33 milligray, a computed tomography angiography needs at least 138 mGy. A cumulative doses of about 50 mGy almost triples the risk of leukemia, and doses of about 60 mGy triples the risk of brain cancer.
Discussion
Knowing that a BCI could have extensive neurologic consequences for children, it is necessary to evaluate routine pediatric diagnostics after blunt trauma. Computed tomography scans (CT) and computed tomography angiography (CTA) are mostly used in routine BCI diagnostics. However, since radiation exposure in children should be as low as reasonably achievable, it should be asked if other diagnostic methods could be used to identify risk groups. Trauma guidelines and clinical scores like the McGovern score are reflect established BCI screening options, as well as using duplex ultrasound.
Keywords:
Blunt carotid injury (BCI)
; blunt trauma
; pediatrics
; CT
; CTA
; radiation
; radiation dose
; radiation risks
; carcinogenesis
; ultrasound
1. Introduction
Blunt carotid injuries (BCI) in pediatric trauma have not been extensively researched. So far, there are only a few publications on this subject. The reason for this might be that BCI in pediatric trauma is very rare. A study on the US national pediatric trauma registry revealed an overall incidence of 0.03%. Only 15 out of over 57.000 children had a BCI after blunt trauma [1]. As well a study on the TraumaRegister DGU could only register an overall prevalence of 0.5%. 48 BCVI cases on 8128 pediatric patients with blunt trauma were registered [2].
The “Gold Standard” for screening patients with suspected BCI is by computed tomography angiography (CTA) followed by alternatives as magnetic resonance angiography (MRA), digital subtraction angiography (DSA) [3,4]. In addition to those instrumental diagnostic tools, clinical scores like the McGovern Score have been published, which shows a sensitivity of 81% and specificity of 71.3% in blunt cerebrovascular injury (BCVI) prediction [4]. Also, ultrasound was named as an excellent possibility to screen for BCI [5,6]. Because there are no guidelines for routine diagnostic work-up in pediatric BCI, we are in urgent need to establish a new diagnostic standard.
Many studies show that even minimal radiation exposure of children could lead to more cases of pediatric cancer [7,8]. Therefore, we should take a critical look at the routine use of radiation to diagnose BCI.
This review aimed to investigate how often computed tomography scans (CT) are performed in pediatric trauma, how often CTA is used to detect BCI after blunt trauma, how many scans with negative results are performed, and if it is possible to define risk groups based on clinical scores or ultrasound findings to prevent radiation exposure to children.
2. Materials and Methods
Definitions
Blunt trauma is defined as any physical impact on the human body, which may lead to any injury of the whole body. Any penetrating or sharp traumata were excluded from research. BCI/ BCVI is defined as an injury of the internal carotid artery, common carotid artery and vertebral artery forced by longitudinal stretching, acceleration-deceleration, rotation, and hyperextension of the neck, stressing the craniocervical vessels through blunt trauma. Children are defined as any patient under the age of 18. In this study, all other synonyms for children were included.
Search Strategy
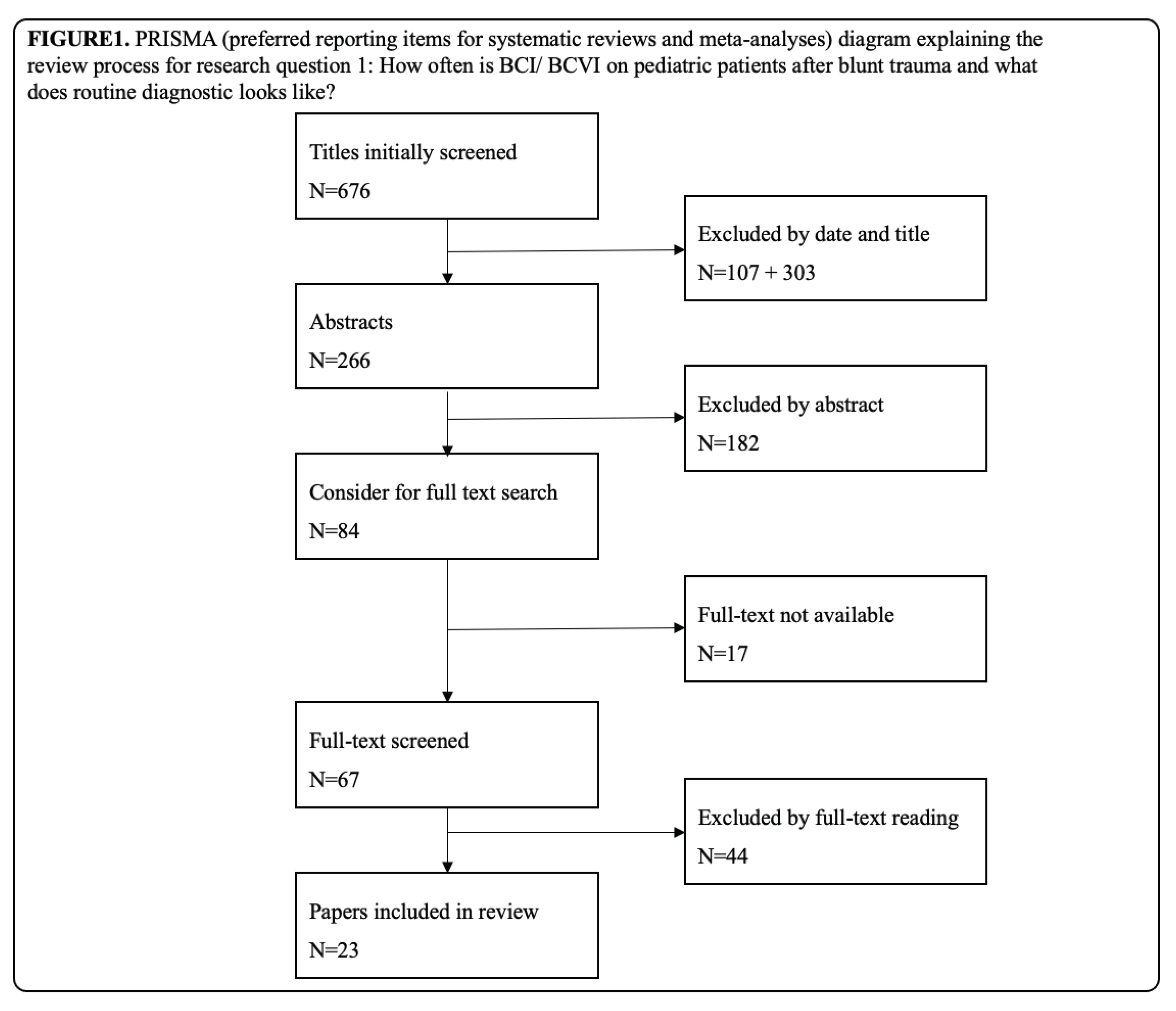
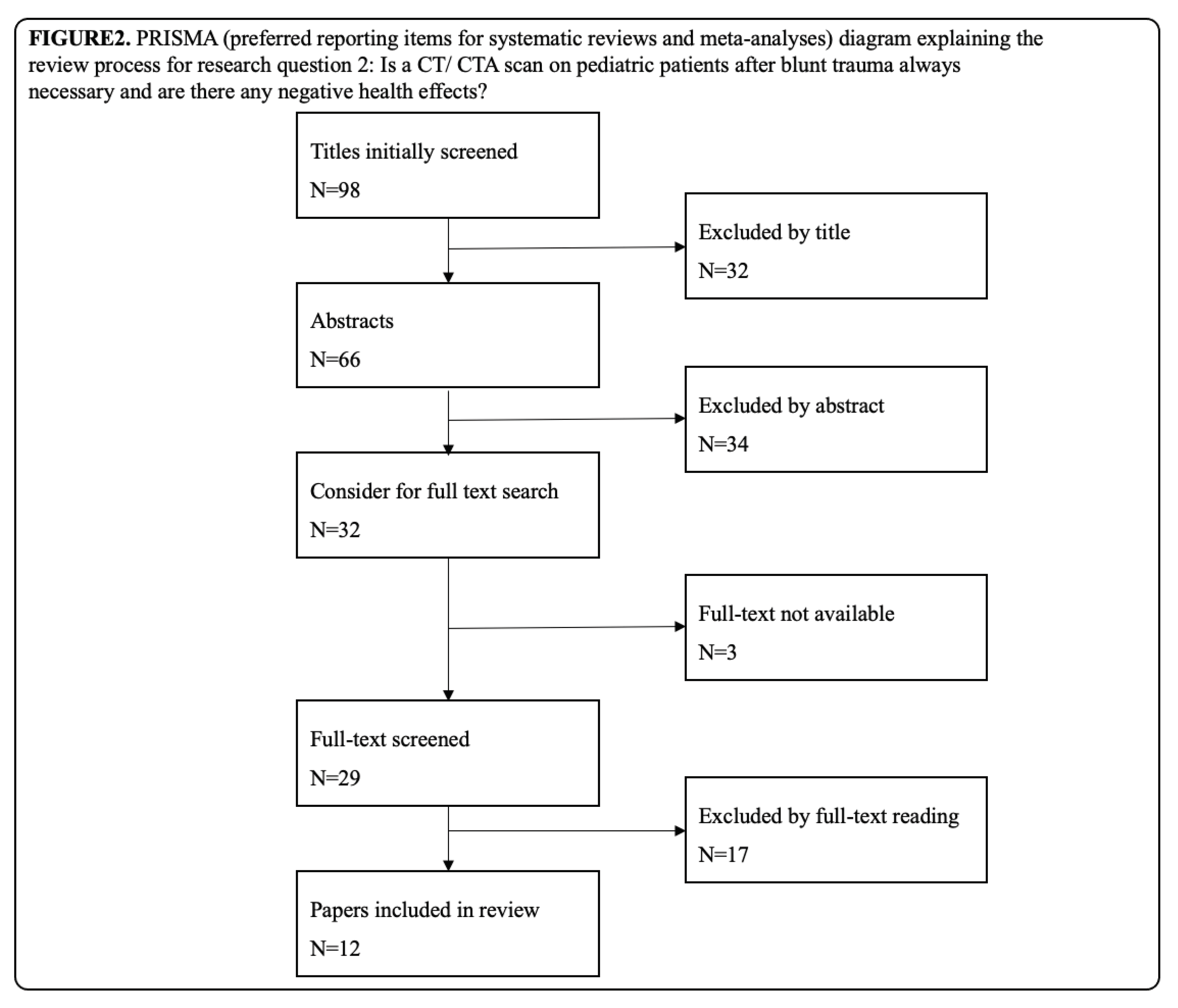
Two clinical questions are discussed in this review; Q1: How frequent is BCI/ BCVI on pediatric patients after blunt trauma, and what does routine diagnostics look like?; Q2: Is a CT/ CTA scan on pediatric patients after blunt trauma always necessary and are there any negative health effects?
To find an answer to Q1, this literature review included publications, that have dealt with pediatric blunt trauma and the diagnostics of BCI and BCVI. Publications dealing with non-pediatric BCI/ BCVI patients were included to check whether there are any diagnostic or therapy guidelines for adults. For literature research, Medline (PubMed) and the Cochrane library were used. MeSH-Terms “Blunt carotid injury” (BCI) AND “pediatric blunt trauma” were used on Medline research. Cochrane library was used to check if there are more potential interesting publications on this topic, which are not included in Medline.
Furthermore, for answering Q2, publications on the risk of radiation exposure on children were included in the study: Different diagnostic modalities were correlated with ultrasound and clinical scores (e.g.,: CTA, MRA, DSA,). We aimed to determine whether risk group stratification based on clinical scores and ultrasound can reduce radiation exposure in children. MeSH-Terms were “pediatric blunt trauma” AND “CT”, OR “CTA”; “radiation dose” AND “radiation risks” AND “carcinogenesis”; and additionally “ultrasound”.
Selection Criteria
Due to lack of research articles, we included reviews, systematic reviews, case reports and original studies for this systematic review. Literature research included all publications in the English language between 1999 and 2020. Due to an enormous change in imaging diagnostics, publications prior to 1999 were excluded. Publications with titles that were irrelevant were excluded immediately. After that, all abstracts of included publications were read, and irrelevant publications were excluded again. For all relevant publications, the full-text version was considered. If the full-text version was not available, the publications were excluded. For an overview of the review process, see the preferred reporting items for systematic reviews and meta-analyses (PRISMA) in Figure 1 and Figure 2.
3. Results
After analyzing all included papers dealing with pediatric BCI/ BCVI, most publications showed an overall incidence between 0.03 – 0.5% of confirmed BCI/ BCVI cases due to pediatric blunt trauma [2,3,9,10,11,12,13]. Only two individual studies found a higher incidence of up to 0.9% and 1.1% [14,15].
About 1.1 – 3.5% of pediatric blunt trauma patients underwent CTA to detect BCI [3,4,16]. Only a few patients underwent other diagnostics like MRA or DSA [3]. Only 0.17 – 1.2% of all CTA scans resulted in the diagnosis of a BCI [3,4,16]. Often, carotid and vertebral arteries were restudied with arteriography 7 - 10 days after the injury [17].
Publications before 2018 mainly used modified Memphis criteria (screening criteria based on adult patients) to screen pediatric patients and decide whether CTA is necessary or not. Modified Memphis criteria classify basilar skull fracture with involvement of petrous bone, basilar skull fracture with involvement of the carotid canal, Le Fort II or III fracture pattern, cervical spine fracture, Horner’s syndrome, neck soft-tissue injury (like seatbelt sign, hanging or hematoma) and focal neurologic deficit not explained by imaging as screening criteria for BCVI (Tabl. 1). If one of those screening criteria is met, the recommendation to perform further workup with angiographic imaging is given [18]. However, those studies showed that carotid or vertebral imaging was performed only in 16.5% of cases with at least one risk factor. Nevertheless, imaging was performed in 1.69% of cases even though no risk factors were detected, and 3 out of 44 scans (6.8%) detected a BCI [3]. Other clinical scores like the Denver [19], EAST [20], and Utah score [21] use other screening tools to detect BCVI. Screening tools are also summarized in Table 1. A study from the University of Missouri-Columbia has shown that modified Memphis criteria misclassified 28.6% of all pediatric trauma cases. Also, other scores like the Denver, EAST, or Utah score misclassified 28.6%, 33.3%, and 47.6%, respectively. Based on the Utah score, the newly created McGovern score was presented with a sensitivity of 81% and a specificity of 71.3% to detect BCVI correctly. The McGovern score includes six elements that were identified as risk factors for BCVI: Glasgow Coma Scale <8, focal neurological deficit, carotid canal fracture, petrous temporal bone fracture, cerebral infarction on CT, and a motor vehicle accident as a mechanism of injury (MOI) [4]. Other risk factors like a seatbelt sign were not associated with BCI [22]. Until now, the McGovern score has not been validated by a second study. Another study of 2019 even showed that the recently added MOI of a motor vehicle accident had no significant correlation with BCI [23].
A CT is often used for diagnostics after blunt trauma to identify injuries because of its fast, extensive, and precise results. 52.5% of all pediatric polytrauma patients get a CT for primary diagnostic work-up [24]. A study on the TraumaRegister DGU has shown that in the control and BCVI groups, children underwent immediate head/neck CT in 85.3% vs. 94.4%, or whole-body CT in 64.6% vs. 86.1% [2]. As diagnosis by imaging is included in almost all scores, a CT of the head and neck is necessary for every patient to screen. Scores that do not require CT or DSA to screen for BCI have not been published so far.
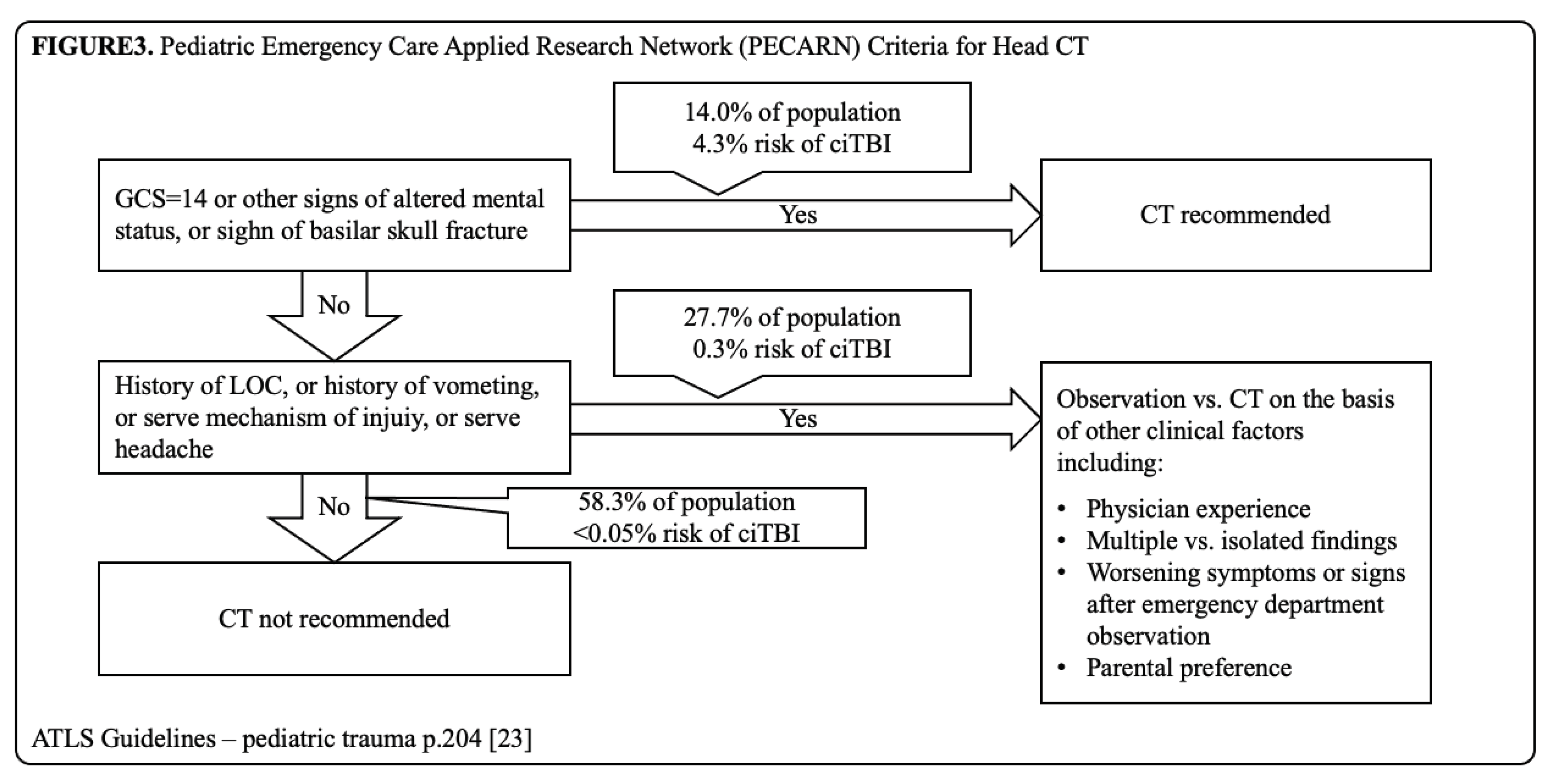
The Advanced Trauma Life Support (ATLS) has released new guidelines (2018) when CT scans on pediatric trauma should be done in its tenth edition. Following this algorithm, 58.3% of the population should not get a CT at all. A group of 27.7%, including patients with a history of loss of consciousness (LOC), or history of vomiting, severe mechanism of injury, or severe headache, should be observed first, and the decision to perform a CT should be taken based on other clinical factors. The indication could be based on physician experience, multiple vs. isolated findings, worsening symptoms or worsening signs after emergency department observation, and parental preference. Only patients with GCS = 14, other signs of altered mental status, or basilar skull fracture signs should get a CT immediately. This group includes only 14% of all pediatric traumata [25] (Figure 3).
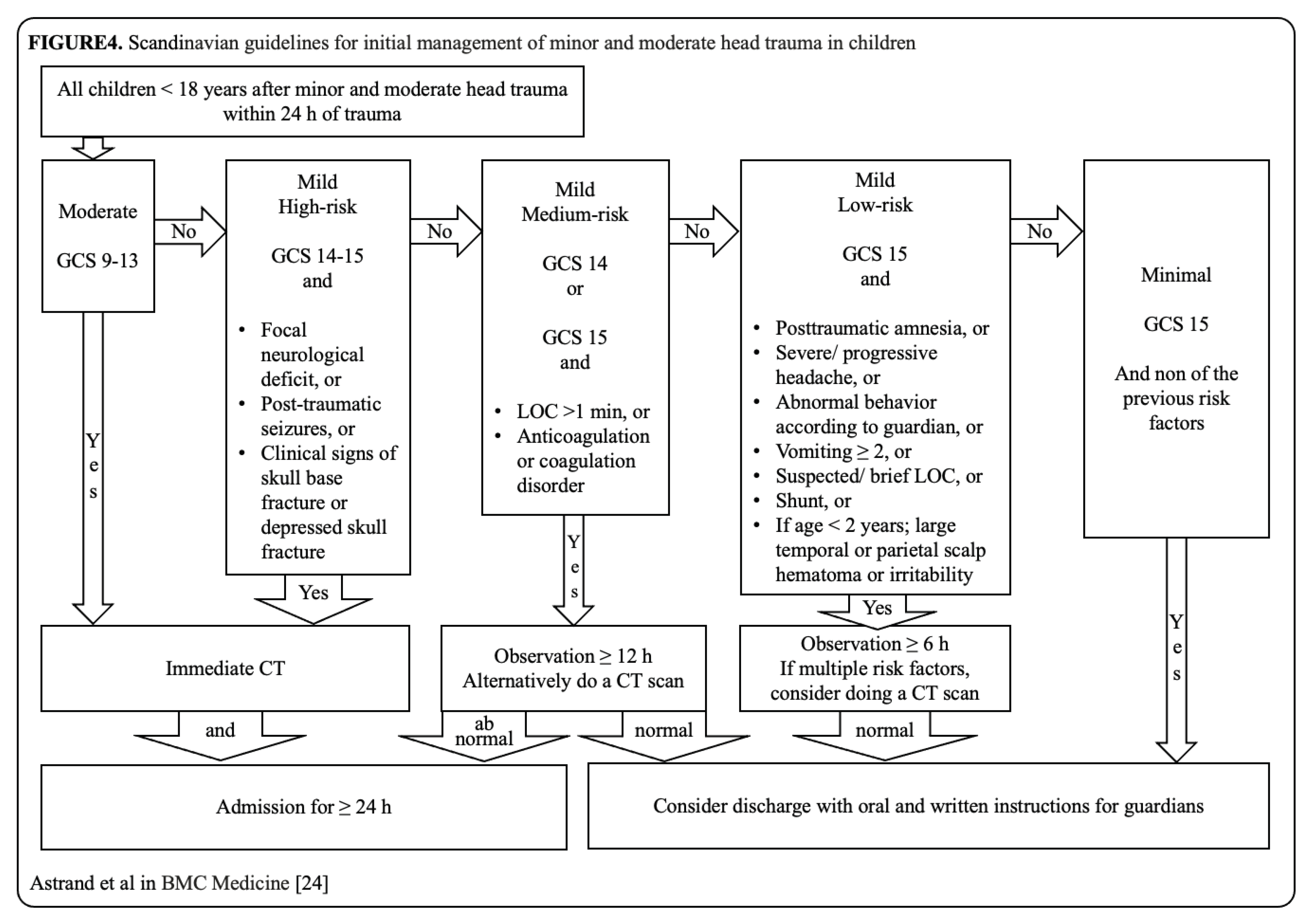
Astrand et al. have published a Scandinavian guideline for initial management of minor and moderate head trauma of children in 2016. Following the flow chart, pediatric patients with moderate head trauma, GCS 9-13, should get a CT scan immediately. Patients with mild head trauma are divided into risk groups. The high-risk group is defined as a GCS 14-15 and focal neurological deficit, or post-traumatic seizures, or clinical signs of skull base fracture or depressed skull fracture. The high-risk group should also get a CT scan immediately. Medium-risk is defined as a GCS 14 or GCS 15 with a LOC >1 min, or anticoagulation or coagulation disorder. The medium-risk group should be clinically observed for over 12 hours. CT scan is only considered as an alternative in this group. Low-risk is defined as a GCS 15 with post-traumatic amnesia, or severe/ progressive headache, or abnormal behavior according to guardian, or vomiting ≥ 2, or suspected/brief LOC, or preexisting cerebral shunt, or if age < 2 years, a large temporal or parietal scalp hematoma or irritability. A clinical observation for 6 hours is considered in the low-risk group, and a CT scan is only advised for patients with multiple risk factors [26] (Figure 4).
As a restricted use of diagnostic radiation in children should be standard, we need to take a look at the dose of radiation exposure of CT scans, the radiation risk, and the alternatives to CT. In children, the median volume CT dose index on a non-contrast head CT is 33 milligray (mGy) [27]. A CT of the skull or facial bones needs 27 – 37 mGy, a scan of the neck 19 – 26 mGy, and a scan of petrous bones 42 – 67 mGy depending on the age group [28]. A computed tomography angiography needs at least 138 mGy [29]. Radiation exposure is associated with a higher cancer incidence. In 2007, the Center for Radiological Research, Columbia University Medical Center, New York, found direct evidence from epidemiologic studies that the organ doses of a standard CT correspond to an increased risk of cancer [7]. A study from the Netherlands described that the cumulative brain dose of a pediatric brain CT scan was 38.5 mGy and was statistically significantly associated with brain tumors risk [30]. The Institute of Health and Society and Northern Institute of Cancer Research Newcastle noted the correlation between radiation dose from CT scans and leukemia and brain tumors. The use of CT scans in children with cumulative doses of about 50 mGy almost triples the risk of leukemia, and doses of about 60 mGy triples the risk of brain cancer [31]. Furthermore, age at the time of exposure and the lifetime attributable risk for children could be identified as an essential risk factor that makes them more vulnerable to radiation exposure than adults [32]. In cases where children received CTs at hospitals without a pediatric trauma center, the median effective radiation dose was two times higher [33].
In a case report on a 12-year-old boy, duplex ultrasound was mentioned as a possible imaging tool to detect BCI. Before treatment, a CTA was conducted to confirm the diagnosis made by ultrasound and detect the injuries’ extent [5]. The same publication illustrates a diagnostic algorithm by ATLS from 2005 for asymptomatic pediatric BCI patients. There, duplex ultrasound is shown as the first diagnostic step on asymptomatic patients. This algorithm can no longer be found in the newest edition (2018) of ATLS. It could be shown that transcranial doppler measurement was significantly associated with the adult blunt cervical vascular injury status. It was suggested that transcranial doppler sonography could be a viable bedside screening tool for trauma [34]. A study on the meaningful use of ultrasound on pediatric BCI has not been published yet.
4. Discussion
Taking these results into consideration, it is confirmed that pediatric BCI is a rare injury. The number of publications on adult BCI after blunt trauma is low and on pediatric BCI even lower. Nevertheless, it could be shown that BCI diagnostic work-up mostly follows the same routine. After patients reach the hospital, an extensive physical examination should be conducted. Asymptomatic patients could be screened by duplex ultrasound to detect BCI and prevent them from unnecessary radiation exposure. Due to better anatomic and physical conditions in pediatric patients, ultrasound should be easier to perform than in adult patients. A positive BCI suspicion on duplex ultrasound needs clarification via CTA. According to the ATLS guidelines, only patients with GCS=14, other signs of altered mental status, or basilar skull fracture signs should get a CT scan immediately. All other patients should be observed, and indications for a CT scan should be set narrowly [25]. If patients show neurological symptoms, a CT scan is irreplaceable.
Assuming that a patient could have a BCI, suspected by clinical examination, ultrasound, or CT scan, the indication for a CTA scan should be checked carefully. Currently, the McGovern score is the only score with a good sensitivity and specificity for BCVI detection. As one study raises concerns about the correlation of the MOI of a motor vehicle accident and BCI’s incidence additional studies’ independent validation of the McGovern score is necessary prior to implementation in routine diagnostics.
Considering the data regarding radiation exposure and the risk of cancer, many publications have proven the correlation between radiation exposure and the probability of the appearance of cancer. Because a cumulative radiation dose of about 50 mGy is sufficient to triple the risk of leukemia and a dose of about 60 mGy to triple the risk of brain cancer, one CTA or two CT scans are enough to reach or even exceed the cumulative radiation threshold dose in children [31]. Taking a critical look at the analyzed studies, only 1.1 – 3.5% of all pediatric blunt trauma patients underwent CTA to detect BCI. Due to the low number of performed CTA scans, the indication for CTA scans was mainly done after careful consideration. Whether these indications were derived by scores or just by expert’s opinion is unclear. Nevertheless, only 0.17 – 1.2% of these CTA scans allowed for a positive BCI diagnosis.
Following the ATLS guidelines, only 14% of all trauma patients should get a CT scan immediately. Another 27.7% of all trauma patients might get a CT scan at a later point after careful observation. In reality, 52,5% of pediatric patients get a CT scan after trauma exceeding the recommendation by ATLS significantly. The stringent use of CT guidelines in the management of pediatric trauma could reduce this number to 42.8% [24].
Validation of the Scandinavian guidelines was recently achieved in 2020. Results have shown that the guidelines have a very high negative predictive value of 99.9% to identify children without traumatic brain injury (TBI), and high sensitivity of 92.3% for detection of TBI. It was proven that the use of the Scandinavian guidelines would potentially reduce the use of CT. In this study 25.0% of the CTs were performed in children with minimal head injury. It was also shown that the guidelines have a high negative predictive value of 96.9% for traumatic findings on CT. The study validation also showed that unnecessary CT scans could be avoided in the mild low-risk head injury group, which accounts for 51.1% of the CT scans. Furthermore, following the guidelines could have saved 76.1% of all CTs performed on those patients [35].
The slim database published so far makes it challenging to reach a generally applicable statement. Almost all published studies, except the Scandinavian guidelines, were conducted in the U.S., making it difficult to refer the results to other countries and health care systems. Other guidelines, expert opinions, and other legal statuses may affect the results analyzed in other countries.
5. Conclusions
We have shown again that BCI in pediatric trauma is rare. The “Gold Standard” diagnostic tool for trauma patients is the plain CT scan, and for BCI, it should be the CTA. As there are many negative and unnecessary scans, radiation containing imaging should be used with caution and should be significantly minimized. Duplex ultrasound and the clinical McGovern score could help to identify risk groups for BCI and could contribute to a less number of unnecessary CTA scans. The McGovern score needs to be validated by other studies. CT guidelines for the management of pediatric trauma and BCI could reduce the number of radiation containing scans, especially in hospitals without a pediatric trauma center.
Author Contributions
Conceptualization, L.B., L.K. and M.D..; methodology, L.B., L.K., K.A. and J.T.; data curation, L.K. and L.B.; writing—original draft preparation, L.K. and L.B.; writing—review and editing, L.K., O.K. K.A., J.T., M.D. and L.B.; visualization, L.K:.; supervision, L.B. and M.D..; project administration, L.B. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lew, S. M.; Frumiento, C.; Wald, S. L. Pediatric blunt carotid injury: a review of the National Pediatric Trauma Registry. Pediatr Neurosurg 1999, 30, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Weber, C. D.; Lefering, R.; Weber, M. S.; Bier, G.; Knobe, M.; Pishnamaz, M.; Kobbe, P.; Hildebrand, F. Predictors for Pediatric Blunt Cerebrovascular Injury (BCVI): An International Multicenter Analysis. World J Surg 2019, 43, 2337–2347. [Google Scholar] [CrossRef] [PubMed]
- Azarakhsh, N.; Grimes, S.; Notrica, D. M.; Raines, A.; Garcia, N. M.; Tuggle, D. W.; Maxson, R. T.; Alder, A. C.; Recicar, J.; Garcia-Filion, P.; et al. Blunt cerebrovascular injury in children: underreported or underrecognized?: A multicenter ATOMAC study. J Trauma Acute Care Surg 2013, 75, 1006–1011; [Google Scholar] [CrossRef]
- Herbert, J. P.; Venkataraman, S. S.; Turkmani, A. H.; Zhu, L.; Kerr, M. L.; Patel, R. P.; Ugalde, I. T.; Fletcher, S. A.; Sandberg, D. I.; Cox, C. S.; et al. Pediatric blunt cerebrovascular injury: the McGovern screening score. J Neurosurg Pediatr 2018, 21, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Cuff, R. F.; Thomas, J. H. Pediatric blunt carotid injury from low-impact trauma: a case report and review of the literature. J Trauma 2005, 58, 620–623. [Google Scholar] [CrossRef] [PubMed]
- Singh, R. R.; Barry, M. C.; Ireland, A.; Bouchier Hayes, D. Current diagnosis and management of blunt internal carotid artery injury. Eur J Vasc Endovasc Surg 2004, 27, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D. J.; Hall, E. J. Computed tomography--an increasing source of radiation exposure. N Engl J Med 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [PubMed]
- Kleinerman, R. A. Cancer risks following diagnostic and therapeutic radiation exposure in children. Pediatr Radiol 2006, 36 (Suppl 2), 121–125. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; D’Ayala, M.; Hirshberg, A.; Briggs, W.; Wise, L.; Tortolani, A. Comparison of conservative and operative treatment for blunt carotid injuries: analysis of the National Trauma Data Bank. J Vasc Surg 2010, 51, 593-599, 599.e591-592. [Google Scholar] [CrossRef]
- Jones, T. S.; Burlew, C. C.; Kornblith, L. Z.; Biffl, W. L.; Partrick, D. A.; Johnson, J. L.; Barnett, C. C.; Bensard, D. D.; Moore, E. E. Blunt cerebrovascular injuries in the child. Am J Surg 2012, 204, 7–10. [Google Scholar] [CrossRef]
- Kraus, R. R.; Bergstein, J. M.; DeBord, J. R. Diagnosis, treatment, and outcome of blunt carotid arterial injuries. Am J Surg 1999, 178, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Wei, C. W.; Montanera, W.; Selchen, D.; Lian, J.; Stevens, C.; de Tilly, L. N. Blunt cerebrovascular injuries: diagnosis and management outcomes. Can J Neurol Sci 2010, 37, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Savoie, K. B.; Shi, J.; Wheeler, K.; Xiang, H.; Kenney, B. D. Pediatric blunt cerebrovascular injuries: A national trauma database study. J Pediatr Surg 2020, 55, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Acker, S. N.; Kulungowski, A. M. Error traps and culture of safety in pediatric trauma. Semin Pediatr Surg 2019, 28, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Kerwin, A. J.; Bynoe, R. P.; Murray, J.; Hudson, E. R.; Close, T. P.; Gifford, R. R.; Carson, K. W.; Smith, L. P.; Bell, R. M. Liberalized screening for blunt carotid and vertebral artery injuries is justified. J Trauma 2001, 51, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Ugalde, I. T.; Claiborne, M. K.; Cardenas-Turanzas, M.; Shah, M. N.; Langabeer, J. R., 2nd; Patel, R. Risk Factors in Pediatric Blunt Cervical Vascular Injury and Significance of Seatbelt Sign. West J Emerg Med 2018, 19, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Biffl, W. L.; Ray, C. E., Jr.; Moore, E. E.; Franciose, R. J.; Aly, S.; Heyrosa, M. G.; Johnson, J. L.; Burch, J. M. Treatment-related outcomes from blunt cerebrovascular injuries: importance of routine follow-up arteriography. Ann Surg 2002, 235, 699–706; [Google Scholar] [CrossRef]
- Ciapetti, M.; Circelli, A.; Zagli, G.; Migliaccio, M. L.; Spina, R.; Alessi, A.; Acquafresca, M.; Bartolini, M.; Peris, A. Diagnosis of carotid arterial injury in major trauma using a modification of Memphis criteria. Scand J Trauma Resusc Emerg Med 2010, 18, 61. [Google Scholar] [CrossRef]
- Cothren, C. C.; Moore, E. E. Blunt cerebrovascular injuries. Clinics (Sao Paulo) 2005, 60, 489–496. [Google Scholar] [CrossRef]
- Bromberg, W. J.; Collier, B. C.; Diebel, L. N.; Dwyer, K. M.; Holevar, M. R.; Jacobs, D. G.; Kurek, S. J.; Schreiber, M. A.; Shapiro, M. L.; Vogel, T. R. Blunt cerebrovascular injury practice management guidelines: the Eastern Association for the Surgery of Trauma. J Trauma 2010, 68, 471–477. [Google Scholar] [CrossRef]
- Ravindra, V. M.; Bollo, R. J.; Sivakumar, W.; Akbari, H.; Naftel, R. P.; Limbrick, D. D., Jr.; Jea, A.; Gannon, S.; Shannon, C.; Birkas, Y.; et al. Predicting Blunt Cerebrovascular Injury in Pediatric Trauma: Validation of the “Utah Score”. J Neurotrauma 2017, 34, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Leraas, H. J.; Kuchibhatla, M.; Nag, U. P.; Kim, J.; Ezekian, B.; Reed, C. R.; Rice, H. E.; Tracy, E. T.; Adibe, O. O. Cervical seatbelt sign is not associated with blunt cerebrovascular injury in children: A review of the national trauma databank. Am J Surg 2019, 218, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Grigorian, A.; Dolich, M.; Lekawa, M.; Fujitani, R. M.; Kabutey, N. K.; Kuza, C. M.; Bashir, R.; Nahmias, J. Analysis of blunt cerebrovascular injury in pediatric trauma. J Trauma Acute Care Surg 2019, 87, 1354–1359. [Google Scholar] [CrossRef]
- McGrew, P. R.; Chestovich, P. J.; Fisher, J. D.; Kuhls, D. A.; Fraser, D. R.; Patel, P. P.; Katona, C. W.; Saquib, S.; Fildes, J. J. Implementation of a CT scan practice guideline for pediatric trauma patients reduces unnecessary scans without impacting outcomes. J Trauma Acute Care Surg 2018, 85, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Ronald, M. Stewart, M. F. R., Sharon M. Henry, Monique Drago, Advanced Trauma Life Support - Student Course Manual, 2018. [Google Scholar]
- Astrand, R.; Rosenlund, C.; Undén, J. Scandinavian guidelines for initial management of minor and moderate head trauma in children. BMC Med 2016, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Sadigh, G.; Kadom, N.; Karthik, P.; Sengupta, D.; Strauss, K. J.; Frush, D.; Applegate, K. E. Noncontrast Head CT in Children: National Variation in Radiation Dose Indices in the United States. AJNR Am J Neuroradiol 2018, 39, 1400–1405. [Google Scholar] [CrossRef] [PubMed]
- Journy, N. M. Y.; Dreuil, S.; Boddaert, N.; Chateil, J. F.; Defez, D.; Ducou-le-Pointe, H.; Garcier, J. M.; Guersen, J.; Habib Geryes, B.; Jahnen, A.; et al. Individual radiation exposure from computed tomography: a survey of paediatric practice in French university hospitals, 2010-2013. Eur Radiol 2018, 28, 630–641. [Google Scholar] [CrossRef]
- Schneider, T.; Wyse, E.; Pearl, M. S. Analysis of radiation doses incurred during diagnostic cerebral angiography after the implementation of dose reduction strategies. J Neurointerv Surg 2017, 9, 384–388. [Google Scholar] [CrossRef]
- Meulepas, J. M.; Ronckers, C. M.; Smets, A.; Nievelstein, R. A. J.; Gradowska, P.; Lee, C.; Jahnen, A.; van Straten, M.; de Wit, M. Y.; Zonnenberg, B.; et al. Radiation Exposure From Pediatric CT Scans and Subsequent Cancer Risk in the Netherlands. J Natl Cancer Inst 2019, 111, 256–263. [Google Scholar] [CrossRef]
- Pearce, M. S.; Salotti, J. A.; Little, M. P.; McHugh, K.; Lee, C.; Kim, K. P.; Howe, N. L.; Ronckers, C. M.; Rajaraman, P.; Sir Craft, A. W.; et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet 2012, 380, 499–505. [Google Scholar] [CrossRef]
- Goodman, T. R.; Mustafa, A.; Rowe, E. Pediatric CT radiation exposure: where we were, and where we are now. Pediatr Radiol 2019, 49, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Nabaweesi, R.; Ramakrishnaiah, R. H.; Aitken, M. E.; Rettiganti, M. R.; Luo, C.; Maxson, R. T.; Glasier, C. M.; Kenney, P. J.; Robbins, J. M. Injured Children Receive Twice the Radiation Dose at Nonpediatric Trauma Centers Compared With Pediatric Trauma Centers. J Am Coll Radiol 2018, 15, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Purvis, D.; Aldaghlas, T.; Trickey, A. W.; Rizzo, A.; Sikdar, S. A novel decision tree approach based on transcranial Doppler sonography to screen for blunt cervical vascular injuries. J Ultrasound Med 2013, 32, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Sönnerqvist, C.; Brus, O.; Olivecrona, M. Validation of the scandinavian guidelines for initial management of minor and moderate head trauma in children. Eur J Trauma Emerg Surg 2021, 47, 1163–1173. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Summary of alle screening criteria for BCI/ BCVI.
| Denver Criteria | EAST Criteria | Modified Memphis Criteria | Utah Criteria | McGovern Criteria |
|---|---|---|---|---|
| Focal neurological deficit | Cervical hyperextension associated w/ displaced midface or complex mandibular fracture or closed head injury consistent with diffuse axonal injury | Basilar skull fracture with involvement of petrous bone | GCS score ≤8 (1Pt.) | GCS score ≤8 (1Pt.) |
| Arterial hemorrhage | Anoxic brain injury due to hypoxia as a result of squeezed arteries | Basilar skull fracture with involvement of the carotid canal | Focal neurological deficit (2Pt.) | Focal neurological deficit (2Pt.) |
| Cervical bruit in patients <50 yrs | Seatbelt abrasion or other soft-tissue injury resulting in swelling or altered mental status | Le Fort II or III fracture pattern | Carotid canal fracture (2Pt.) | Carotid canal fracture (2Pt.) |
| Expanding neck hematoma | Cervical vertebral body fracture or carotid canal fracture in proximity to the internal$$$carotid or vertebral arteries | Cervical spine fracture | Petrous temporal bone fracture (3Pt.) | Petrous temporal bone fracture (3Pt.) |
| Neurological exam findings inconsistent w/ head CT scan | Horner’s syndrome | Cerebral infarction on CT (3Pt.) | Cerebral infarction on CT (3Pt.) | |
| Cerebrovascular accident on follow-up head CT scan not seen on initial head CT scan | Neck soft-tissue injury (seatbelt sign, hanging or hematoma) | MOI (2Pt.) | ||
| Presence of Le Fort II or III fractures | Focal neurologic deficit not explained by imaging | |||
| Cervical spine fracture w/ subluxation | ||||
| C1–3 cervical spine fracture | ||||
| Cervical spine fracture extending into the transverse foramen | ||||
| Basilar skull fracture w/ carotid involvement | ||||
| Diffuse axonal injury w/ GCS score <6 | ||||
| Hypoxic ischemia due to squeezed arteries |
For Denver, EAST, and Modified Memphis Criteria, further workup with angiographic imaging is recommended if any of the listed criteria are met. For Utah and McGovern Criteria, a score ≥ 3 points on both scales signifies high risk for BCI/ BCVI and indicates angiography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



