
Submitted:
23 March 2024
Posted:
25 March 2024
You are already at the latest version
Abstract
A screening questionnaire for autism symptoms is not yet available in Poland, and there are no recommendations regarding screening for developmental disorders in Polish primary health care. The aim of the study was to assess the opinions of parents and physicians on the legitimacy and ne-cessity of screening for autism spectrum disorders, potential barriers to the implementation of the screening program, and the evaluation and presenting the process of the online ASD screen-ing, which was part of the validation program of the Polish version of one of the screening tools. The study involved 418 parents whose children were screened online and 95 primary care physi-cians who expressed their opinions in prepared surveys. The results indicate that both parents and doctors perceive the need to screen children for ASD in general population without a clear preference as to the screening method (online or in-person). Online screening may prove to be at least a partial method of solving numerous indicated systemic difficulties - including: time con-straints, lack of experienced specialists in the field of developmental disorders or related to the organizational difficulties of health care.
Keywords:
autism spectrum disorders
; population screening
; autism screening
; online screening
1. Introduction
Autism spectrum disorders (ASD) are neurodevelopmental condition of undetermined etiology, most often manifested in early childhood, which affect daily activity and are characterized primarily by difficulties in the sphere of communication and interpersonal interactions as well as restricted interests or repetitive behaviors, with prevalence estimated to 1/100 worldwide [1,2]. There are no reliable data available on the prevalence of ASD in Poland - according to official data from the Polish National Health Fund from 2012, the prevalence rate of ASD in individuals under the age of 18 in Poland is 3.4 cases per 10,000 children [3]. More recent preliminary data from two Polish provinces estimate that ASD occurs in one in 286 children [4]. It is not entirely clear why the reported prevalence of ASD in Poland is lower than in neighboring countries (e.g. in Germany - 0.38%) and lower than assumed, based on newer data from European Union countries [5,6] – it may be the result of lacking readily available tools for the screening and diagnosis of ASD, insufficient awareness of this problem of healthcare professionals (HCPs) and systemic difficulties and constraints.
Accelerated diagnosis of ASD enables initiation of an early, appropriately adjusted therapy. First symptoms of ASD usually appear during infancy or early childhood - prodromal symptoms may be visible even as early as 6 months of a child's life [7,8] and usually reliable diagnosis of ASD in a child can be made as early as 2-3 years of age [9]. The younger the child, the better the results of therapy can be achieved in the area of communication and social interaction, cognitive abilities, speech development or behavior appropriate to the situation, which improves the quality of life of people with ASD, reduces the risk of mental disorders, and significantly reduces ASD's burden [10,11,12,13].
For this reason, the American Academy of Pediatrics recommends screening at 18 and 24 months of age as part of primary care during well-child care visits. [14]. It appears that the increasing availability of screening significantly lowered the age of ASD diagnosis in the US, with diagnosis before the age of 4 made in 71% of children (2018) compared to 58% in 2014 [15,16]. However, a US Preventive Services Task Force from 2016 report shows insufficient evidence to recommend universal ASD screening [17]. On the other hand, there is evidence suggesting that including screening tools in routine medical appointments may result in earlier and more accurate identification of children who need further help than relying solely on clinical impressions, which is particularly important when care providers are less experienced in diagnosing ASD [18]. Moreover, the use of public ASD screening may reduce social inequalities in terms of the age of diagnosis and access to further therapeutic activities [19,20]. The conclusions of both reports indicate the need for further research on screening tools and their effectiveness, as well as on the effectiveness of further proceedings after screening [21].
Throughout infancy and early childhood, primary care professionals are the professionals with whom a young child most often comes into contact. During this time, numerous meetings with doctors, nurses, midwives and other HCPs take place - as a result of visits due to the child's illness, well-child check-ups or qualifying for vaccinations. This enables close observation of development of the child and detection of developmental disorders. Primary care professionals are believed to have the greatest influence on the early diagnosis of ASD (especially due to performing screening for developmental disorders (DD)), and they are responsible for the significant trend in the decline in the average age of children when diagnosed with autism spectrum disorders [22]. In addition, family doctors are coordinators of diagnostics and treatment performed by many of the further specialists, as well as "caregivers" of their patients not only on the health issues, but also on the social issues - which is necessary in the event of ASD in a child.
In order to increase the effectiveness of early detection of autism spectrum symptoms, many tools have been created to facilitate this process for health care workers. Due to the lack of standardized tools for ASD screening in Poland we started the “Spojrzeć w oczy” (eng. "Look in the eyes") project. The aim of the project was to validate the Polish version of the Communication and Symbolic Behavior Scale-Developmental Profile Infant-Toddler Checklist (CSBS-DP ITC). CSBS-DP ITC is one of the available tools for the early detection of symptoms of autism spectrum disorders consisting of 24 items, filled out by parents and guardians [23]. CSBS-DP ITC can be used in ASD screening for general population of children aged 6 to 24 months in a primary care setting. In previous studies, we showed that the Polish version of the CSBS-DP ITC has good psychometric properties and relatively high specificity and sensitivity and can be used as an effective screening tool [24,25].
During the planning of the study, the COVID-19 pandemic began in the world, which prevented the efficient conduct of the stationary study in primary health care clinics. The pandemic has made it necessary to introduce solutions that would allow to access remote medical services, which reduced the risk of coronavirus infection [26,27]. For this reason, it was necessary to create an electronic version of the CSBS-DP ITC questionnaire to be completed by parents at home. Then, the results of examination, instead of being assessed by individual healthcare professionals (HCPs, e.g. GPs, pediatricians, nurses, psychologists), were assessed directly by specialists involved in the project. Epidemiological situation forced the screening to be carried out in a unique way, using the online version, without direct contact with the examined person. The use of telemedicine made it possible to contact the patient, perform the screening, conduct follow-up tests and possibly dispel the parents' doubts and questions.
The aim of this paper is to assess opinions of HCPs and parents performing electronic screening and to present the experiences from one of the first attempts to conduct such screening program. In addition, we wanted to assess the possible constraints in usage of ASD screening tools in HCPs everyday practice. Approval from the Bioethics Committee of the Wroclaw Medical University was obtained to conduct the study (number KB – 641/2020). All procedures were performed in accordance with the 1964 Helsinki declaration and its later amendments.
2. Materials and Methods
2.1. Assessment of ASD Electronic Screening by Parents
We sent invitations to 1461 parents of children whose applications in the first phase of the "Spojrzec w oczy" project were included in the assessment of the psychometric values of the CSBS-DP ITC (the criteria for inclusion of children in the study regarding the properties of the questionnaire were being a resident of Poland and the age of 6-24 months). We asked parents to fill out an electronic short questionnaire about their feelings about electronic screening for developmental disorders with a record of their age, level of education, place of residence and subjective information technology (IT) proficiency in scale from 1 to 10 (where 1 – is the lowest, 10 – the highest). A translated version of the survey is available as Supplementary File 1. We did not link parents' answers to their child's results in the CSBS-DP ITC questionnaire to maintain anonymity, however, we asked them to select if they benefited from additional contact with people involved in the project (e.g. further diagnostics, specialist advice) or if their child was diagnosed with ASD or other developmental disorders. The survey was made available on the project's website - it is available only through the appropriate link, sent only to the parents included in the study. Invitations to evaluate the project were sent on January 9, 2023 and responses were collected until January 18, 2023.
2.2. Assessment of ASD Electronic Screening by Doctors and Potential Difficulties in Implementing the ASD Screening Program
In order to recruit physicians for the study, we sent e-mail invitations to members associated in the Polish Society of Family Medicine and we propagated the training on the project's social media profiles. The survey consisted of 18 questions, 7 of which concerned statistical data - age, sex, main place of work, work experience, and the percentage of children with developmental disorders (DD) under their own medical care. The remaining ones touched upon aspects of the use of diagnostic methods in clinical practice, further proceedings when DD is suspected, the willingness to use screening methods during medical visits, the assessment of potential difficulties and limitations in introducing screening tests, and the positives and negatives resulting from online DD screening. A translated version of the survey for doctors is available as Supplementary File 2. Applications were collected from July 31, 2023 to February 1, 2024.
2.3. Statistical Analysis
All the analyses presented in this manuscript were performed using Statistica 13 software. The Shapiro–Wilk normality test was applied to check the normal distribution using 0.05 as a significance level. None of the examined variables met the criterion of normality of distribution, therefore non-parametric tests were used for further analysis. The dependence of the variables on the categories of qualitative variables was tested using the non-parametric Kruskal-Wallis’s test. This test enabled a direct comparison of the value of a quantitative variable between the two categories of a qualitative variable. In the case of qualitative variables, the uniformity of the category distribution was tested with the Chi-square uniformity test (one sample proportions test). In some cases, Spearman's rank correlation was used, allowing variables on ordinal and quantitative scales that did not have a normal distribution to be correlated with each other. In the case of a small number of respondents in subgroups, the Yates correction was used in the chi-square test. A significance level of 0.05 was set for all tests. In the case of some of the examined features only a descriptive interpretation was possible. This is mainly due to the inability to conduct further statistical analyses — these variables cannot be tested for homogeneity. The respondents could indicate several categories at the same time, so the categories do not meet the separability condition required for homogeneity testing.
3. Results
We received a positive response and a fully completed survey from 418 parents taking part in “Spojrzeć w oczy” project, giving a response rate of 28.6%. Due to forcing the answers to individual questions and the full anonymity of the survey, it was not necessary to exclude any submissions. The number of participants exceeds the minimum sample size to have a confidence level of 95% and a margin of error of 5% in the Polish population (the calculated minimum sample size was 384) [28]. All submission were completed by female except one. Mean age of the parents was 33.86 years (SD = 4.12) and mean subjective IT proficiency was 8.52 (SD = 1.25). Full parents’ sociodemographic characteristics are presented in Table 1.
Among the parents who took part in the ASD electronic screening assessment, 38 additionally contacted us for more information and diagnostic and therapeutic assistance via e-mail and telephone. 30 of their children were diagnosed with a developmental disorder - 21 with ASD, 8 with speech development delay, and 1 with sensory integration disorder.
Of all the parents, only 4 (0.95%) had not heard of ASD before and 184 (44.02%) did not suspect any developmental disorders in their child - in this group, one child was diagnosed with ASD, the other 3 – with language delay (LD). Each parent was asked to answer questions about ASD awareness and opinions on ASD screening – both online and in-person. Chi-square tests and the Kruskal-Wallis test were used for this analysis, depending on the nature of the studied variables. The collected results are presented in Table 2 and Table 3.
The significant majority of parents (99.04% of all, N = 414) participating in the study were aware of the issue of ASD at least to a basic extent before the screening test. Nevertheless, there is a significant difference in the level of awareness of ASD among parents with lower education, living in rural areas and with lower IT proficiency compared to other parents (χ2 = 13.013, p = 0.005; χ2 = 13.398, p = <0.001; H = 14.801, p = 0.011 respectively). Moreover, as many as 98.09% of parents (N = 410) believe that ASD screening should be mandatory, 98.56% (N = 412) would participate in screening for developmental disorders in their next child again, and 97.13% (N = 406) – in online screening. The percentage of parents willing to participate again for another child is lower for parents living in smaller towns. The parents' opinion differs widely in the case of preferences for the form of screening (online or stationary) - a slight majority prefers the online version (52.15%, N = 218), but this does not depend on place of residence, education or the fact of receiving a diagnosis of developmental disorders in a child – the only factor influencing the preference for the online method is higher IT proficiency (H = 16.212; p = 0.006).
A rather intriguing issue is the fact that parents whose children were finally diagnosed with developmental disorders report much more often than others that they have had the thought that their child may be at risk of suffering from ASD (χ2 = 12.350, p = <0.001).
We also asked parents four questions regarding their assessment of the electronic screening carried out by us as part of the "Spojrzeć w oczy" project using the Polish online-version of the CSBS-DP ITC questionnaire. Responses to questions were based on a five-point Likert scale. The Kruskal-Wallis test and Spearman Rank Correlation were used for this analysis. The results regarding the assessment of the quality of online screening and satisfaction with participation in the study depending on age, IT proficiency, place of residence and education are included in Table 4 and Table 5.
Collected data indicate a very high overall assessment of the online screening conducted as part of the project by parents. Opinions are characterized by high homogeneity in terms of the examined features, with a few exceptions. Parents living in small towns rated the possibility of contact and the possibility of receiving help the lowest (H = 10.794, p = 0.013 and H = 21.323, p = <0.001, respectively); similarly, people with higher education rated the possibility of obtaining appropriate help lower than parents with secondary education (H = 6.043, p = 0.048). Moreover, there is a very weak negative correlation indicating that older parents evaluate the possibility of obtaining further information and answers from examiners during online screening lower than younger parents (R = -0.104, p = 0.033).
In order to obtain doctors' opinions on electronic ASD screening and potential limitations in the implementation of ASD screening in everyday practice, doctors from the Polish Society of Family Medicine were invited to participate in the second part of the study. Finally, 95 doctors took part in the study. The exact number of Society members is not officially available; according to Facebook data, the post reached approximately 1,320 users. Mean age of the doctors was 32.58 years (SD = 5.24) and mean subjective IT proficiency was 8.33 (SD = 1.32). The average length of service in primary health care facilities of the respondents was 5.23 years (SD = 4.68). Full doctors’ sociodemographic characteristics are presented in Table 6.
Physicians were asked about their own methods of management a pediatric patient in case of suspected developmental disorders - whether they rely on their own clinical assessment or the results of additional tests when choosing further treatment, and whether they use screening methods in their everyday work. In addition, we asked for information whether they use given methods in all children or only those from the risk group, and what actions are taken when observing DD in a patient; finally, we asked doctors to choose their preferred ASD screening option. Chi-square tests and the Kruskal-Wallis test were used for this analysis, depending on the nature of the studied variables. The collected data is presented in Tables S1, 7 and 8. Table S1 is provided as Supplementary File.

Table 8.
The usage of screening methods, the choice of management in case of suspected DD and preferred screening method (online vs stationary) depending on the age, estimated number of children with DD under medical care and length of work experience of physicians.
Table 8.
The usage of screening methods, the choice of management in case of suspected DD and preferred screening method (online vs stationary) depending on the age, estimated number of children with DD under medical care and length of work experience of physicians.
| Variables | H | df | p |
|---|---|---|---|
| Usage of screening methods for DD (in all children/only in children at risk or suspected of DD) | |||
| age | 22.435 | 17 | 0.169 |
| self-estimated IT proficiency | 5.496 | 6 | 0.482 |
| estimated number of children with DD under medical care | 22.133 | 18 | 0.226 |
| length of work experience in primary care facilities | 6.089 | 14 | 0.964 |
| Management of a child under 2 years of age in the event of subtle symptoms of developmental disorders | |||
| age | 15.675 | 17 | 0.547 |
| self-estimated IT proficiency | 6.881 | 6 | 0.332 |
| estimated number of children with DD under medical care | 24.169 | 18 | 0.150 |
| length of work experience in primary care facilities | 24.553 | 14 | 0.039 |
| Management of a child above 2 years of age in the event of subtle symptoms of developmental disorders | |||
| age | 18.120 | 17 | 0.381 |
| self-estimated IT proficiency | 19.757 | 6 | 0.003 |
| estimated number of children with DD under medical care | 13.250 | 18 | 0.777 |
| length of work experience in primary care facilities | 30.081 | 14 | 0.007 |
| Preferred screening method | |||
| age | 27.876 | 17 | 0.046 |
| self-estimated IT proficiency | 5.277 | 6 | 0.501 |
| estimated number of children with DD under medical care | 24.435 | 18 | 0.141 |
| length of work experience in primary care facilities | 24.384 | 14 | 0.041 |
Note. DD – developmental disorders, df – degrees of freedom, H - Kruskal-Wallis test statistic result.
The vast majority of surveyed physicians use basic methods to detect symptoms of developmental disorders - the most common ones include observing the child during the physical examination (94.74%), attempting to communicate and establish contact with the child (93.68%), and assessing the pace of achieving developmental milestones (89.47%). Risks related to family history are slightly less frequently taken into account; diagnostic tools completed by caregivers or health care workers are used much less frequently (21.05 and 15.79% of respondents, respectively). Moreover, active use of the above-mentioned methods is more common only in children suspected of having DD features; less frequently in the entire pediatric patient population. Quite a significant part of the surveyed doctors has a wait-and-see attitude in the case of subtle features of DD in a child under two years of age (37.89%); in the case of children over two years of age, the vast majority of doctors refer children with DD symptoms for further evaluation (94.74%). These issues are independent of doctors' age, gender, place of work and age; the analyzes showed the significance of the percentage of pediatric patients among all patients on the frequency of screening use in the entire population (the highest in the "up to 20%" and "above 50%" groups, not showing a linear nature; X2 = 19.216, p = 0.002), self-estimated IT proficiency on the frequency of referring patients for further evaluation after the age of 2) (the higher it is, the greater the percentage of referring physicians) and the length of work experience in primary care facilities (the longer it is, the more physicians refer patients for further evaluation - both below and over 2 years of age).
As in the case of parents, preferences regarding the type of screening (online vs. stationary) are strongly divided (53.68% of doctors are in favor of online screening). Dependencies were observed only in terms of age and work experience of doctors (younger doctors and those working in primary care for a shorter period more often preferred the online version (H = 27.876, p = 0.046 and H = 24.384, p = 0.041, respectively).
If the stationary version was preferred over the electronic version, we asked doctors who would be responsible for calculating the questionnaire results and analyzing the screening results. The vast majority (n = 36, 81.82%) believe that this should be done by the child's doctor; then - the doctor with the most experience in DD (n = 6, 13.64%). Interestingly, none of the doctors would hand over this function to nurses or the clinic coordinator (in Poland, these are HCPs responsible for helping patients set appointments with specialists outside the clinic and helping with the care of chronically ill patients).
Physicians were also asked how willing they would be to use questionnaires to perform screening of DDs during individual visits (e.g., peri-vaccination visits, well-child visits, when observing DD symptoms during the visit). Kruskal-Wallis test was used to perform this analysis. The results are summarized in Table 9.
The respondents' answers show a clear, statistically significant difference in the willingness to use screening questionnaires during various situations in the physicians’ office (H = 46.069, p < 0.001); doctors are significantly more willing to use screening tools to confirm noticed symptoms (M = 4.362) and to confirm or dispel parents' doubts (M = 4.362). The willingness to use these methods for general screening is significantly lower (in the case of 18 months - M = 3.512; 24 months - M = 3.828).
While preparing the Polish version of the CSBS-DP ITC questionnaire, we encountered many difficulties reported by health care professionals (HCPs) regarding the implementation of additional ASD screening. We collected their and our observations in order to obtain a broader opinion of HCPs potentially responsible for screening. The answers are summarized in Figure 1 and Table S2. Table S2 is provided as Supplementary File.
The surveyed physicians most often point out that there is insufficient time during the patient’s visit to be able to carry out screening test for developmental disorders - this answer was given by almost 92% of doctors. It is also clearly the most frequently occurring most serious obstacle according to doctors; almost half of the respondents point out that excessive time burden is the main barrier to conducting population screening tests. Slightly fewer physicians report difficulties in access to specialists (both the lack of specialists and queues to practicing HCPs) and the lack of clear clinical recommendations regarding DD screening.
Parents and doctors were also asked to rate whether they agreed with the opinions about the positives and negatives of online ASD screening. These opinions were collected based on contacts with parents, specialists and the authors' own experiences. Chi-square test analysis was performed to obtain results. The respondents' answers are presented in Table 10.
Both in the groups of doctors and parents, positive features of online screening were more often marked than negative ones. What parents most often appreciate are the convenience of online screening (saving time and the possibility of conducting the test from home - 68.18% and 78.23% of parents, respectively) and easier access to the evaluation. Among the negatives, parents most often point out the inability to verify the result and assess the child's development directly by a specialist (57.89%) and the lack of personal contact with examiners (46.65%). Similar results were obtained among doctors - they also noted the comfort of online screening, however, this effect was significantly lower than in parents (p = 0.025 and 0.002). Doctors also mainly pointed out the lack of direct contact with the person conducting the examination as main flaw of online screening (55.79%). What is noteworthy is that both groups (especially parents) rarely considered a potential lack of trust in people responsible for screening as a disadvantage.
3.2. Figures, Tables and Schemes
4. Discussion
In Poland, well-child care visits have been conducted in primary health care clinics since the 1950s. The system of preventive health care for children is based on the principle of continuity of care - according to this assumption, the same doctor looks after a child in health and in sickness. After the newborn is discharged from the hospital, parents are obliged to report the child to a selected primary care clinic. Well-child care visits take place at the age of in between 2 and 6 months, 9, 12 months and later in 2, 4 and 5 years of age. During the latter an indicative examination of hearing (assessment of hearing behavior and the "show what you hear" test) and vision (especially in the direction of strabismus, later - also other disorders) is performed [29]. At 5-6 years of age, an indicative study of motor and psychosocial development should be carried out on the basis of interview and observation, but it is rarely a validated, structured study [30]. Until then, the assessment of psychomotor development is primarily an assessment of the child's time to reach milestones - there are no other established guidelines for the use of any tools for DD screening in children. In the case of suspicion of DDs, the child is referred to appropriate psychological and pedagogical clinics, where further examinations and consultations are carried out [31]. The validated diagnostic methods available in Poland include: Level 2 tools Autism Spectrum Rating Scales (ASRS) and Social Communication Questionnaire (SCQ) and Level 3 tools - Autism Diagnostic Observation Schedule (ADOS-2) and Psychoeducational Profile, Third Edition—PEP-3-PL [32,33,34,35]. Research on the Polish version of Autism Diagnostic Interview-Revised (ADI-R) is in progress [36]. Children during the final diagnosis with visible developmental disorders may be covered by the Early Development Support program - comprehensive, multidisciplinary activities to support the child's psychomotor development through the intervention of therapists (psychologists, speech therapists, educators, SI therapists) however, they must be referred there by a doctor or preschool teacher.
However, in order to start further diagnostic and therapeutic activities described above, it is necessary for a family doctor or pediatrician to suspect that the child may have DD. In order to increase the effectiveness of early detection of DD, numerous screening questionnaires have been created, which, as research conducted in the United States shows, may be a useful tool to increase the percentage of early detected cases of developmental disorder [15]. In order to enable the use of this method to accelerate the diagnosis of developmental disorders, a version of CSBS-DP ITC adapted to Polish conditions was prepared by authors of this paper, which was linguistically and culturally adapted to increase the effectiveness of the tool and reduce the likelihood of obtaining incorrect results. When designing the whole project methodology, it was necessary to adapt to the dynamically changing conditions during the COVID-19 pandemic. The pandemic forced the entire study to be conducted online or via telephone consultation. Nevertheless, this form of conducting the study made it possible - apart from assessing the effectiveness of the Polish version of CSBS-DP ITC - to examine how parents evaluate on-line screening method.
Preparing a Polish version of a fully validated ASD screening questionnaire could, at least partially, fill the gap related to the low frequency of use of diagnostic methods in the field of developmental disorders in the daily work of doctors, as evidenced by our study results. Polish doctors more often use their own clinical assessment of a child's development, based, among others, on assessing the time of reaching appropriate milestones or observing the child's behavior during visit, which, unfortunately, may result in a delay in diagnosis [15]. The use of tools in the practice of Polish primary care physicians is clearly lower than, for example, in the USA (where ASD screening programs are the most popular - 63% of pediatricians use screening questionnaires in their practice, and up to 73% of all children are screened in this direction) which allows for lowering the average age of ASD diagnosis [37,38]. Another example of unintentional omissions may be the quite large percentage of Polish physicians observing the child's development in the event of subtle symptoms of developmental disorders in children under two years of age - almost half of the respondents would continue close observation or refer the child for further evaluation based on parental pressure, which may also lead to a potential delay in the detection of developmental disorders. In the case of an older child (over 2 years of age), only 5% of respondents would decide to further observe it’s development.
The most frequently raised issue by respondents, which may potentially hinder the implementation of a screening program for developmental disorders in Poland, is the insufficient amount of time that can be allocated for screening during a visit of a young patient. Paying attention to the occurrence of ASD symptoms in a child or conducting an appropriate screening test requires spending more time on these activities than is usually allocated to a visit to a primary care facility [39]. Insufficient time during the visit to conduct observations for ASD is also the most frequently mentioned obstacle in studies conducted in other countries, e.g. the USA, Canada or Oman [40,41,42,43]. The problem of time constraints is becoming more crucial - data from the UK shows increasing workload for doctors and nurses working in primary care [44]. In Poland, this problem is probably even more severe due to the shortage of doctors and the resulting overwork - the number of practicing doctors and nurses in Poland is among the lowest in the EU and amounts to 2.4 doctors and 5.1 nurses per 1,000 inhabitants; this problem is particularly severe in small counties around large cities and in rural areas [45]. However, there is a lack of precise data on the professional burden of Polish HCPs - in one of the studies conducted during the COVID-19 pandemic, Polish healthcare workers reported high levels of burnout and stress - related to, among others, increased workload [46] Rising costs may also be a problem, including: costs related to the preparation of materials for screening (although, as the collected data indicate, according to Polish doctors, this should not be a major obstacle) or, above all, with further care for children with suspected or ultimately diagnosed ASD. Healthcare financing in Poland is lower than the EU average (6.5% to 9.9% of GDP in 2019), most of which is spent on inpatient care; funds for outpatient care are half of the average in the European Union [45]. Low expenditure on outpatient health care and a small number of practicing HCPs are also related to the issue of difficulties in access to specialists in the immediate area, which is pointed out by as many as 54% of doctors - psychologists, speech therapists, educators, and child psychiatrists. Over the last decade (2014-2023), the number of child psychiatrists in Poland increased from 346 to 532, while in the years 2019-2023 there was an increase in the number of patients from nearly 150,000. to over 266,000 which means that the difficulties in obtaining appropriate specialist help are constantly increasing [47]. This is an important problem because experience from other countries (e.g. Taiwan) indicates that only increasing access to ASD screening without improving access to further evaluation or therapy may cause increasing frustration and confusion in families due to the lack of a coherent procedural and diagnostic system for people at risk of DD. To address the unmet needs of families with children with ASD, resource imbalances between screening and follow-up interventions in public pediatric care settings must be simultaneously addressed [48].
Another problem potentially troubling the implementation of screening is the lack of appropriate education of HCPs and the lack of systemic activities regarding the early diagnosis of ASD - gaps in knowledge regarding ASD and the ability to use screening tools are indicated by 33 and 36% of respondents, respectively. An even greater percentage of doctors report uncertainty regarding further treatment of a patient suspected of having ASD. Insufficient knowledge about ASD among physicians is a common global problem - a study conducted in 2020 showed that only 23% of primary care physicians had sufficient knowledge about ASD, and the percentage of such doctors was higher in countries with higher income [49]. This is probably due to the lack of experience in working with people with disabilities during medical studies, the small number of classes devoted to developmental disorders, as well as the specific image of people with ASD created by the mass media [50]. The problem of lack of knowledge is intensified by the lack of clear guidelines (either Polish or European) regarding ASD screening and further diagnostic activities. Existing American guidelines do not fully correspond to the Polish primary care setting and their recommendations are difficult to implement into practice.
In Poland, fully validated screening questionnaires for ASD are virtually unavailable, which is indicated by 30% of respondents as a barrier to the implementation of screening. In addition to the mentioned work on CSBS-DP ITC, so far, there are only preliminary data on the Polish version of Quantitative Checklist for Autism in Toddlers (Q-CHAT). Research on most frequently used in Poland M-CHAT organized as part of the Badabada project is still in progress [51,52]. Until now, direct translations of the above-mentioned questionnaires available on the Internet were usually used without any cultural and linguistic adaptation and without a validation process. Using incorrectly prepared diagnostic tools may reduce the accuracy of the diagnostic process; the diagnostic tool should be fully adapted to the population in which it will be used so that its psychometric properties are at the highest possible level [53]. Nevertheless, the vast majority of physicians would be willing to use diagnostic materials if they were available, especially when detecting clinically significant signs of developmental disorders or to allay or confirm parental concerns. Unfortunately, there is significantly less willingness in physicians to use these tools during peri-vaccination or well-child visits at 18 or 24 months of age, which would be the recommended course of action according to American Academy of Pediatrics guidelines [54]. Experience from preliminary screening programs in Spain and the Netherlands indicates that the use of screening methods for ASD during well-baby check-up visits increases the attendance rate [55]. Less willingness to conduct population screening may lead to delays in diagnosis, especially in the case of more subtle symptoms occurring in a child with undiagnosed DD.
Additionally, blurred responsibility for a child with DD makes it difficult to further guide the child in the diagnostic and therapeutic process. Care for a child with DD in Poland is divided into health care (within primary care clinics, specialist mental health clinics, community psychological care centers and early intervention centers) and educational care (within special/integrated kindergartens, psychological and pedagogical counseling centers, early childhood supporting child development and leading centers coordinating rehabilitation and care (pol. Wiodący Ośrodek Koordynujący Rehabilitacyjno-Opiekuńczy, WOKRO)) . The multitude of facilities whose scope of competences are sometimes unclear and unregulated (e.g. early intervention centers do not have their own legal normative acts) means that obtaining appropriate, full assistance can be troublesome for child's guardians who are placed in a stressful situation. The difficult situation is complemented by the fact that some of the mentioned forms of support are insufficient for all those in need - for example, in Poland there are only forty early intervention centers [56]. The situation is further complicated by the fact that due to the underfunding of the public system, parents often use private health care. This significantly complicates the coordination of ASD diagnosis and therapy in Poland. Similar difficulties are also observed in other European countries - a survey conducted in south-eastern European countries indicates that many parents experienced difficulties or delays in therapy due to queues to specialists, high costs or difficulties in obtaining information; difficulties also concerned problems with obtaining assistance in the field of education [57].
The results of our study prove that respondents more often pay attention to the positive rather than negative effects of electronic screening. Both the groups of doctors and parents indicated primarily the convenience of this solution method, which is consistent with previous research results on the use of teleconsultations and online services in health care, which unanimously note greater availability and convenience of use compared to stationary services [58]. However, parents most often pointed out as a flaw that screening is carried out solely on the basis of a questionnaire completed by the parent, without direct contact with the examiner who could observe the child (and potentially confirm or deny the diagnosis resulting from screening). This is probably related to the subjective assessment of the doctor's role as more important during the diagnostic process - not only related to the doctor's experience, but also to interpersonal and communication qualifications, as well as empathy and understanding. Research data indicate that over 50% of patients do not fully believe in medical suggestions using artificial intelligence (AI), even though AI achieves better diagnostic results in some issues [59]. Probably, even in the case of a simple screening questionnaire (such as CSBS-DP ITC), the issue of trust in the doctor is an important aspect for parents; it was proven that patients were more willing to implement recommendations given by doctors than those given by computers [60,61]. This effect may be even more important due to the fact that the diagnosis of ASD in a child is associated with a huge caregiving burden, even greater than for parents of children with Down syndrome or type 1 diabetes [62]. Preliminary information collected during the study indicates the need to take this fact into account when designing subsequent ASD screening services.
The collected data show that for parents the ability to initially confirm or deny fears is very important - despite this, the vast majority of parents believe that ASD screening should be mandatory for every child and that they would subject their next child to a similar test - regardless of the form of screening. Interestingly, both doctors and parents show an almost equal division in preferences for online or stationary screening. In the case of implementing the former in a larger population, attention should be paid to the possible effect of digital exclusion, observed more often among people with lower IT proficiency and from rural areas. Nevertheless, conducting diagnostic methods using electronic technologies potentially should speed up the provision of medical assistance and facilitate access to screening [63].
Despite all the positives regarding online screening described above, conducting screening with usage of online technologies is not yet popular - as of November 29, 2023, the phrase "electronic screening" is found in 275 and "online screening" in 258 scientific articles contained in the PubMed database. In the same database, only 2 studies on ASD screening can be found - one conducted in Italy, the other in China - assessing only the effectiveness of ASD online screening [64,65]. Additionally, one large study evaluates the effectiveness of screening using electronic techniques during inpatient visits [66]. We found no study addresses the issue of online screening assessment by parents or doctors. Our work is likely to be the beginning of a future discussion on the role of further online electronic services in the daily work of physicians.
The last issue worth mentioning is the fact that parents whose children were finally diagnosed with DD had previously suspected the occurrence of some developmental disorders in their children. Due to the fact that similar experiences also result from previous studies, it is worth paying attention in everyday practice to the possibilities of dispelling these concerns of caregivers as safely as possible - even in the case of negative tests and screening observations [67].
4.1. Limitations
This study has several limitations. Firstly, parents' assessment of satisfaction with the screening was in some cases carried out a considerable time after the end of participation in the study - this may result in an incomplete and slightly inadequate assesement. Moreover, the selection of the study group does not fully reflect the structure of Polish society. The answers in the section regarding parents’ assessment were provided almost exclusively by mothers - this is consistent with the sex structure obtained in previous studies on the diagnostic accuracy of CSBS-DP ITC and is probably related to the culturally preferred family model in Poland, where mothers take most of the care of offspring, especially when children they are younger [68]. Percentage of people with higher education and living in large cities took part more often in the ASD screening during the "Spojrzeć w oczy" project; their participation increased even further in this study [69]. Similarly, the largest group of surveyed doctors are those living in large urban centers, with potential underrepresentation of rural areas of Poland. A large part of the surveyed physicians were younger doctors – residents – who are also overrepresented in the study group. Ultimately, both parents and doctors participated in the study completely voluntarily - there is a risk of biasing the group among people with a keen interest in the subject of ASD, which may result in inflated results regarding, for example, awareness of ASD issues or more frequent use of additional diagnostic materials.
5. Conclusions
The data collected from our study clearly prove that Polish parents and doctors expect the implementation of screening for developmental disorders as part of routine child health care. Due to numerous possible limitations - primarily time constraints, human resources and systemic difficulties the introduction of ASD screening in primary care must be preceded by a thorough analysis of potential changes that will facilitate its implementation. Online screening could partially facilitate access to the test and reduce the workload, but it must be introduced taking into account limitations - especially the possibility of quick verification of the result using more accurate methods during stationary visit. Moreover, it will not fully replace the doctor-patient relationship, which is one of the factors determining the effectiveness of therapy. However, it may be one of the ways to speed up the diagnostic and therapeutic process, which may improve the functioning of people affected by ASD.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: The usage of screening diagnostic methods for developmental disorders in the practice of Polish family doctors and pediatricians; Table S2: Potential obstacles to the implementation of screening in primary health care facilities according to surveyed physicians; File S1: Survey for parents; File S2: Survey for family doctors and pediatricians.
Author Contributions
Conceptualization, M.S. and M.M.B.F.; methodology, M.S. and M.M.B.F.; validation, M.S. and M.M.B.F.; formal analysis, M.S.; investigation, M.S., U.G.B. and M.M.B.F.; resources, M.S.; data curation, M.S..; writing—original draft preparation, M.S., U.G.B. and M.M.B.F.; writing—review and editing, M.S. and M.M.B.F..; visualization, M.S.; supervision, M.M.B.F.; project administration, M.S..; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Bioethics Committee) of Wroclaw Medical University (KB – 641/2020, approved 21th October 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are openly available in FigShare at https://doi.org/10.6084/m9.figshare.25465744
Acknowledgments
The researchers would like to thank Róża Hajkuś and Kamila and Tomasz Chadaj for their help in recruiting study participants.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American Psychiatric Association Cautionary Statement for Forensic Use of DSM-5; American Psychiatric Association Publishing: Washington DC, 2014; ISBN 9780890425541.
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global Prevalence of Autism: A Systematic Review Update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef] [PubMed]
- Piskorz-Ogórek, K.; Ogórek, S.; Cies̈lińska, A.; Kostyra, E. Autism in Poland in Comparison to Other Countries. Polish Ann. Med. 2015, 22, 35–40. [Google Scholar] [CrossRef]
- Skonieczna-Żydecka, K.; Gorzkowska, I.; Pierzak-Sominka, J.; Adler, G. The Prevalence of Autism Spectrum Disorders in West Pomeranian and Pomeranian Regions of Poland. J. Appl. Res. Intellect. Disabil. 2017, 30, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, C.J.; Gerste, B.; Hoffmann, F. Diagnoses of Autism Spectrum Disorders in Germany: Time Trends in Administrative Prevalence and Diagnostic Stability. Autism 2018, 22, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Rasoulpoor, S.; Rasoulpoor, S.; Shohaimi, S.; Jafarpour, S.; Abdoli, N.; Khaledi-Paveh, B.; Mohammadi, M. The Global Prevalence of Autism Spectrum Disorder: A Comprehensive Systematic Review and Meta-Analysis. Ital. J. Pediatr. 2022, 48, 1–16. [Google Scholar] [CrossRef]
- Zwaigenbaum, L.; Bryson, S.; Garon, N. Early Identification of Autism Spectrum Disorders. Behav. Brain Res. 2013, 251, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Canu, D.; Van der Paelt, S.; Canal-Bedia, R.; Posada, M.; Vanvuchelen, M.; Roeyers, H. Early Non-Social Behavioural Indicators of Autism Spectrum Disorder (ASD) in Siblings at Elevated Likelihood for ASD: A Systematic Review. Eur. Child Adolesc. Psychiatry 2021, 30, 497–538. [Google Scholar] [CrossRef]
- Chawarska, K.; Klin, A.; Paul, R.; Volkmar, F. Autism Spectrum Disorder in the Second Year: Stability and Change in Syndrome Expression. J. Child Psychol. Psychiatry Allied Discip. 2007, 48, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Orinstein, A.J.; Helt, M.; Troyb, E.; Tyson, K.E.; Barton, M.L.; Eigsti, I.M.; Naigles, L.; Fein, D.A. Intervention for Optimal Outcome in Children and Adolescents with a History of Autism. J. Dev. Behav. Pediatr. 2014, 35, 247–256. [Google Scholar] [CrossRef]
- MacDonald, R.; Parry-Cruwys, D.; Dupere, S.; Ahearn, W. Assessing Progress and Outcome of Early Intensive Behavioral Intervention for Toddlers with Autism. Res. Dev. Disabil. 2014, 35, 3632–3644. [Google Scholar] [CrossRef]
- Smith, T.; Klorman, R.; Mruzek, D.W. Predicting Outcome of Community-Based Early Intensive Behavioral Intervention for Children with Autism. J. Abnorm. Child Psychol. 2015, 43, 1271–1282. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of Co-Occurring Mental Health Diagnoses in the Autism Population: A Systematic Review and Meta-Analysis. The Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Hyman, S.L.; Levy, S.E.; Myers, S.M.; Kuo, D.Z.; Apkon, C.S.; Davidson, L.F.; Ellerbeck, K.A.; Foster, J.E.A.; Noritz, G.H.; O’Connor Leppert, M.; et al. Identification, Evaluation, and Management of Children with Autism Spectrum Disorder. Pediatrics 2020, 145. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.A.; Maenner, M.J.; Baio, J.; Washington, A.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; White, T.; Rosenberg, C.R.; et al. Early Identification of Autism Spectrum Disorder among Children Aged 4 Years - Early Autism and Developmental Disabilities Monitoring Network, Six Sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder among Children Aged 8 Years-Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Siu, A.L. Screening for Autism Spectrum Disorder in Young Children US Preventive Services Task Force Recommendation Statement. JAMA - J. Am. Med. Assoc. 2016, 315, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Sheldrick, R.C.; Merchant, S.; Perrin, E.C. Identification of Developmental-Behavioral Problems in Primary Care: A Systematic Review. Pediatrics 2011, 128, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Fein, D. Commentary on USPSTF Final Statement on Universal Screening for Autism. J. Dev. Behav. Pediatr. 2016, 37, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Coury, D.L. Babies, Bathwater, and Screening for Autism Spectrum Disorder: Comments on the USPSTF Recommendations for Autism Spectrum Disorder Screening. J. Dev. Behav. Pediatr. 2015, 36, 661–663. [Google Scholar] [CrossRef]
- Mandell, D.; Mandy, W. Should All Young Children Be Screened for Autism Spectrum Disorder? Autism 2015, 19, 895–896. [Google Scholar] [CrossRef]
- James, S.N.; Smith, C.J. Early Autism Diagnosis in the Primary Care Setting. Semin. Pediatr. Neurol. 2020, 35, 100827. [Google Scholar] [CrossRef] [PubMed]
- Wetherby, A.M.; Allen, L.; Cleary, J.; Kublin, K.; Goldstein, H. Validity and Reliability of the Communication and Symbolic Behavior Scales Developmental Profile with Very Young Children. J. Speech, Lang. Hear. Res. 2002, 45, 1202–1218. [Google Scholar] [CrossRef] [PubMed]
- Sobieski, M.; Kopszak, A.; Wrona, S.; Bujnowska-Fedak, M.M. Screening Accuracy and Age-Based Scoring Procedures of the Polish Version of Communication and Symbolic Behavior Scales-Developmental Profile Infant-Toddler Checklist. medRxiv, 2430. [Google Scholar] [CrossRef]
- Sobieski, M.; Wrona, S.; Flakus, M.; Pierchała, K.; Sobieska, A.; Podgórska, K.; Wołowicz, A.; Sekułowicz, M.; Bujnowska-Fedak, M.M. Reliability and Theoretical Validity of the Polish Version of Communication and Symbolic Behavior Scales-Developmental Profile – Infant-Toddler Checklist. SSRN 2024. [Google Scholar] [CrossRef]
- Kruszyńska-Fischbach, A.; Sysko-Romańczuk, S.; Rafalik, M.; Walczak, R.; Kludacz-Alessandri, M. Organizational E-Readiness for the Digital Transformation of Primary Healthcare Providers during the Covid-19 Pandemic in Poland. J. Clin. Med. 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Siow, M.Y.; Walker, J.T.; Britt, E.; Kozy, J.P.; Zanzucchi, A.; Girard, P.J.; Schwartz, A.K.; Kent, W.T. What Was the Change in Telehealth Usage and Proportion of No-Show Visits for an Orthopaedic Trauma Clinic during the COVID-19 Pandemic? Clin. Orthop. Relat. Res. 2020, 478, 2257–2263. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.A.J.; Lo, S.; Hollestein, L.M. Research Techniques Made Simple: Sample Size Estimation and Power Calculation. J. Invest. Dermatol. 2018, 138, 1678–1682. [Google Scholar] [CrossRef]
- Oblacińska, A.; Jodkowska, M.; Sawiec, P. ABC Bilansów Zdrowia Dziecka. Podręcznik Dla Lekarzy; Medycyna Praktyczna: Kraków, 2017. [Google Scholar]
- Jaroszyńska-Szymczuk, M. Orientacyjne Badanie Rozwoju Motorycznego i Psychospołecznego Pod Kątem Dojrzałości Szkolnej Dziecka. In Profilaktyczne badania lekarskie i inne zadania lekarza w opiece zdrowotnej nad uczniami; Oblacińska, A., Woynarowska, B., Eds.; Instytut Matki i Dziecka: Warszawa, 2002. (in Polish) [Google Scholar]
- Lenart, A.; Pasternak, J. Resources, Problems and Challenges of Autism Spectrum Disorder Diagnosis and Support System in Poland. J. Autism Dev. Disord. 2023, 53, 1629–1641. [Google Scholar] [CrossRef] [PubMed]
- Chojnicka, I.; Pisula, E. Adaptation and Validation of the ADOS-2, Polish Version. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Wrocławska-Warchala, E.; Wójcik, R. ASRS Zestaw Kwestionariuszy Do Diagnozy Spektrum Autyzmu; Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warszawa, 2016. (in Polish) [Google Scholar]
- Pisula, E. Profil Psychoedukacyjny, Wydanie 3, Wersja Polska. Podręcznik Diagnosty; EduProf: Warszawa, 2019; ISBN 9788395381102. [Google Scholar]
- Rynkiewicz, A.; Szura, M.; Bernaciak, D.; Kozak, A.; Karwowska, M. Polish Adaptation of the Social Communication Questionnaire (Scq) and Female Autism Phenotype: An Investigation of Potentially Sex-Biased Items in the Screening Assessment and Their Impact on Scores. Brain Sci. 2021, 11. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A Revised Version of a Diagnostic Interview for Caregivers of Individuals with Possible Pervasive Developmental Disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Carbone, P.S.; Campbell, K.; Wilkes, J.; Stoddard, G.J.; Huynh, K.; Young, P.C.; Gabrielsen, T.P. Primary Care Autism Screening and Later Autism Diagnosis. Pediatrics 2020, 146, 20192314. [Google Scholar] [CrossRef]
- Lipkin, P.H.; Macias, M.M.; Chen, B.B.; Coury, D.; Gottschlich, E.A.; Hyman, S.L.; Sisk, B.; Wolfe, A.; Levy, S.E. Trends in Pediatricians’ Developmental Screening: 2002–2016. Pediatrics 2020, 145. [Google Scholar] [CrossRef]
- Buckley, C. Making Your Practice Autism Friendly. InnovAiT Educ. Inspir. Gen. Pract. 2017, 10, 327–331. [Google Scholar] [CrossRef]
- Das, J.; Hartman, L.; King, G.; Jones-Stokreef, N.; Moore Hepburn, C.; Penner, M. Perspectives of Canadian Rural Consultant Pediatricians on Diagnosing Autism Spectrum Disorder: A Qualitative Study. J. Dev. Behav. Pediatr. 2022, 43, 149–158. [Google Scholar] [CrossRef]
- Morelli, D.L.; Pati, S.; Butler, A.; Blum, N.J.; Gerdes, M.; Pinto-Martin, J.; Guevara, J.P. Challenges to Implementation of Developmental Screening in Urban Primary Care: A Mixed Methods Study. BMC Pediatr. 2014, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Dosreis, S.; Weiner, C.L.; Johnson, L.; Newschaffer, C.J. Autism Spectrum Disorder Screening and Management Practices among General Pediatric Providers. J. Dev. Behav. Pediatr. 2006, 27. [Google Scholar] [CrossRef]
- Al Maskari, T.; Melville, C.; Al Farsi, Y.; Wahid, R.; Willis, D. Qualitative Exploration of the Barriers to, and Facilitators of, Screening Children for Autism Spectrum Disorder in Oman. Early Child Dev. Care 2020, 190, 1762–1777. [Google Scholar] [CrossRef]
- Hobbs, F.D.R.; Bankhead, C.; Mukhtar, T.; Stevens, S.; Perera-Salazar, R.; Holt, T.; Salisbury, C. Clinical Workload in UK Primary Care: A Retrospective Analysis of 100 Million Consultations in England, 2007–14. Lancet 2016, 387, 2323–2330. [Google Scholar] [CrossRef] [PubMed]
- OECD/European Observatory on Health Systems and Policies Spain: Country Health Profile 2021; 2021.
- Izdebski, Z.; Kozakiewicz, A.; Białorudzki, M.; Dec-Pietrowska, J.; Mazur, J. Occupational Burnout in Healthcare Workers, Stress and Other Symptoms of Work Overload during the COVID-19 Pandemic in Poland. Int. J. Environ. Res. Public Health 2023, 20, 2428. [Google Scholar] [CrossRef] [PubMed]
- Opłakany Stan Psychiatrii Dziecięcej - Aktualności - Psychiatria Dzieci i Młodzieży - Medycyna Praktyczna Dla Lekarzy Available online:. Available online: https://www.mp.pl/psychiatria-dzieci-i-mlodziezy/aktualnosci/320826,oplakany-stan-psychiatrii-dzieciecej (accessed on 23 March 2024).
- Yi, H.; Siu, Q.K.Y.; Ngan, O.M.Y.; Chan, D.F.Y. Parents’ Experiences of Screening, Diagnosis, and Intervention for Children with Autism Spectrum Disorder. Am. J. Orthopsychiatry 2020, 90, 297–311. [Google Scholar] [CrossRef]
- McCormack, G.; Dillon, A.C.; Healy, O.; Walsh, C.; Lydon, S. Primary Care Physicians’ Knowledge of Autism and Evidence-Based Interventions for Autism: A Systematic Review. Rev. J. Autism Dev. Disord. 2020, 7, 226–241. [Google Scholar] [CrossRef]
- Havercamp, S.M.; Ratliff-Schaub, K.; Macho, P.N.; Johnson, C.N.; Bush, K.L.; Souders, H.T. Preparing Tomorrow’s Doctors to Care for Patients with Autism Spectrum Disorder. Intellect. Dev. Disabil. 2016, 54, 202–216. [Google Scholar] [CrossRef] [PubMed]
- Niedźwiecka, A.; Pisula, E. Symptoms of Autism Spectrum Disorders Measured by the Qualitative Checklist for Autism in Toddlers in a Large Sample of Polish Toddlers. Int. J. Environ. Res. Public Health 2022, 19, 3072. [Google Scholar] [CrossRef] [PubMed]
- Badabada.Pl - M-CHAT-R/F PL Available online:. Available online: http://badabada.pl (accessed on 23 March 2024).
- DuBay, M.; Watson, L.R.; Baranek, G.T.; Lee, H.; Rojevic, C.; Brinson, W.; Smith, D.; Sideris, J. Rigorous Translation and Cultural Adaptation of an Autism Screening Tool: First Years Inventory as a Case Study. J. Autism Dev. Disord. 2021, 51, 3917–3928. [Google Scholar] [CrossRef]
- Zwaigenbaum, L.; Bauman, M.L.; Stone, W.L.; Yirmiya, N.; Estes, A.; Hansen, R.L.; McPartland, J.C.; Natowicz, M.R.; Choueiri, R.; Fein, D.; et al. Early Identification of Autism Spectrum Disorder: Recommendations for Practice and Research. Pediatrics 2015, 136, S10–S40. [Google Scholar] [CrossRef]
- García-Primo, P.; Hellendoorn, A.; Charman, T.; Roeyers, H.; Dereu, M.; Roge, B.; Baduel, S.; Muratori, F.; Narzisi, A.; Van Daalen, E.; et al. Screening for Autism Spectrum Disorders: State of the Art in Europe. Eur. Child Adolesc. Psychiatry 2014, 23, 1005–1021. [Google Scholar] [CrossRef]
- Wyszukaj Placówki - Umów Wizytę Available online:. Available online: https://placowki.mp.pl/home/szukaj.html?is_pharmacy=0&name=ośrodek+wczesnej+interwencji&find=Szukaj&specs[0]=&offset=20 (accessed on 23 March 2024).
- Daniels, A.M.; Como, A.; Hergüner, S.; Kostadinova, K.; Stosic, J.; Shih, A. Autism in Southeast Europe: A Survey of Caregivers of Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2017, 47, 2314–2325. [Google Scholar] [CrossRef]
- Ford, J.; Reuber, M. Comparisons of Communication in Medical Face-To-Face and Teleconsultations: A Systematic Review and Narrative Synthesis. Health Commun. 2023. [Google Scholar] [CrossRef]
- Robertson, C.; Woods, A.; Bergstrand, K.; Findley, J.; Balser, C.; Slepian, M.J. Diverse Patients’ Attitudes towards Artificial Intelligence (AI) in Diagnosis. PLOS Digit. Heal. 2023, 2, e0000237. [Google Scholar] [CrossRef]
- Shaffer, V.A.; Probst, C.A.; Merkle, E.C.; Arkes, H.R.; Medow, M.A. Why Do Patients Derogate Physicians Who Use a Computer-Based Diagnostic Support System? Med. Decis. Mak. 2013, 33, 108–118. [Google Scholar] [CrossRef]
- Promberger, M.; Baron, J. Do Patients Trust Computers? J. Behav. Decis. Mak. 2006, 19, 455–468. [Google Scholar] [CrossRef]
- Picardi, A.; Gigantesco, A.; Tarolla, E.; Stoppioni, V.; Cerbo, R.; Cremonte, M.; Alessandri, G.; Lega, I.; Nardocci, F. Parental Burden and Its Correlates in Families of Children with Autism Spectrum Disorder: A Multicentre Study with Two Comparison Groups. Clin. Pract. Epidemiol. Ment. Heal. 2018, 14, 143–176. [Google Scholar] [CrossRef]
- Hincapié, M.A.; Gallego, J.C.; Gempeler, A.; Piñeros, J.A.; Nasner, D.; Escobar, M.F. Implementation and Usefulness of Telemedicine During the COVID-19 Pandemic: A Scoping Review. J. Prim. Care Community Heal. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Colombo, P.; Buo, N.; Ceccarelli, S.B.; Molteni, M. Integrating a New Online Platform in Primary Care for Early Detection, Referral, and Intervention in Autism Spectrum Disorder: The First Italian Pivotal Clinical Study. Brain Sci. 2022, 12, 256. [Google Scholar] [CrossRef] [PubMed]
- Qiu, T.; Zhang, H.; Zhou, C.; Tang, Q.; Wang, L.; Ke, X. Application of Telemedicine for Preliminary Screening of Autism Spectrum Disorder. Front. Pediatr. 2022, 9. [Google Scholar] [CrossRef]
- Guthrie, W.; Wallis, K.; Bennett, A.; Brooks, E.; Dudley, J.; Gerdes, M.; Pandey, J.; Levy, S.E.; Schultz, R.T.; Miller, J.S. Accuracy of Autism Screening in a Large Pediatric Network. Pediatrics 2019, 144. [Google Scholar] [CrossRef]
- Ryan, S.; Salisbury, H. ‘You Know What Boys Are like’: Pre-Diagnosis Experiences of Parents of Children with Autism Spectrum Conditions. Br. J. Gen. Pract. 2012, 62. [Google Scholar] [CrossRef]
- Zięba-Kołodziej, B. Partnerstwo Rodziców w Opiece Nad Dzieckiem i w Jego Wychowywaniu. In Rodzicielstwo w kontekście współczesnych przemian społecznych; Brągiel, J., Górnicka, B., Eds.; Wydawnictwo Uniwersytetu Opolskiego: Opole, 2012; pp. 149–163 (in Polish). ISBN 978-83-7395-505-9. [Google Scholar]
- Central Statistical Office Mały Rocznik Statystyczny Polski / Concise Statistical Yearbook of Poland; Warszawa, 2022.
Figure 1.
Obstacles to the implementation of screening in primary health care facilities according to surveyed physicians.
Figure 1.
Obstacles to the implementation of screening in primary health care facilities according to surveyed physicians.
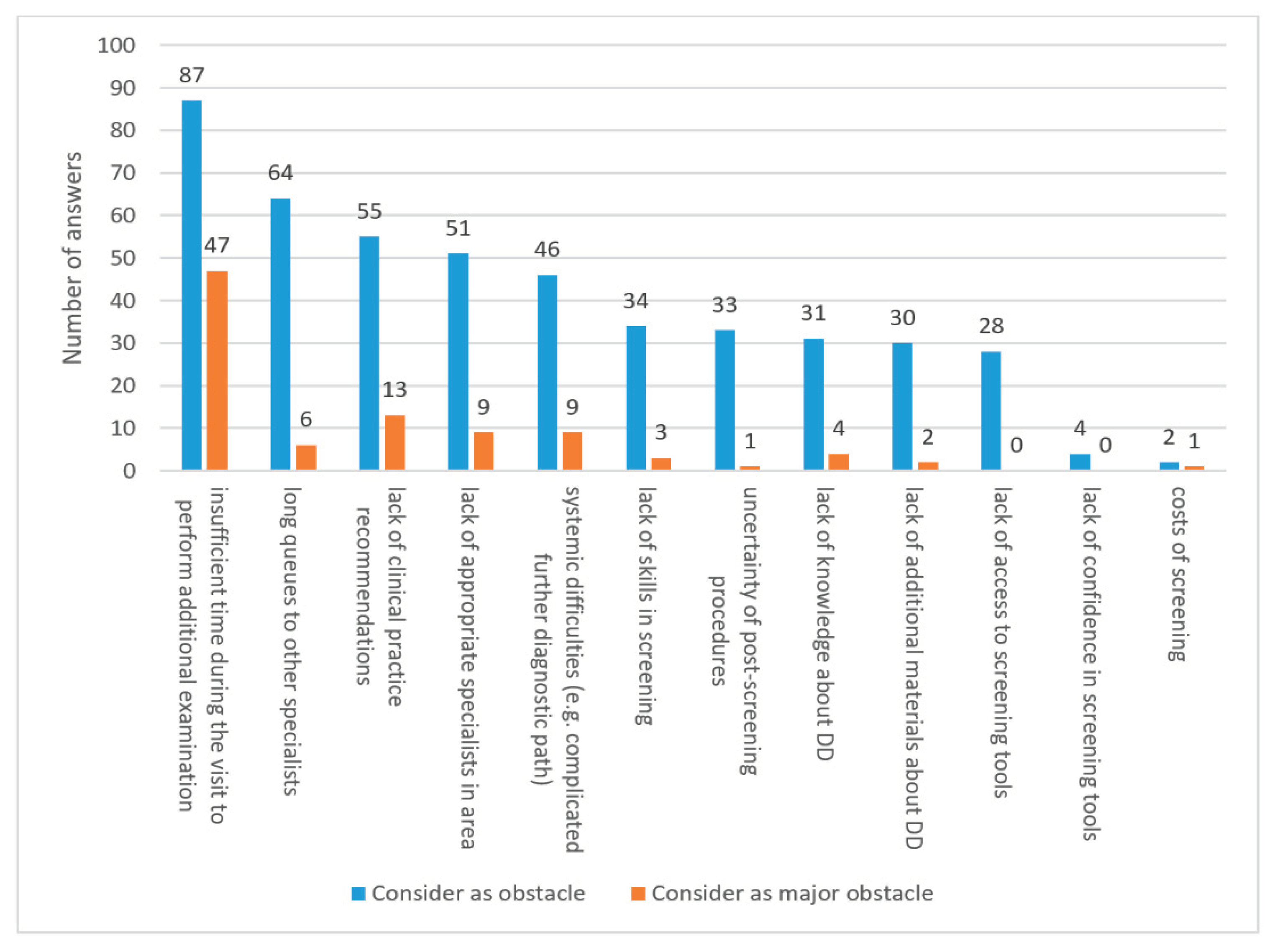
Table 1.
Sociodemographic characteristics of parents taking part in the study.
| Characteristic | n | % |
| Sex | ||
| Female | 417 | 99.76% |
| Male | 1 | 0.24% |
| Using additional contact with researchers | ||
| Yes | 38 | 9.09% |
| No | 380 | 90.91% |
| Diagnosed DD in their child during the project | ||
| Yes | 30 (21 ASD, 8 LD, 1 SI) | 7.18% |
| No | 388 | 92.82% |
| Education level | ||
| Lower education | 0 | 0% |
| Secondary education+ | 58 | 13.88% |
| Higher education | 360 | 86.12% |
| Place of residence | ||
| Village | 99 | 23.68% |
| Town inhabited by less than 20,000 people | 33 | 7.89% |
| City inhabited by 20,000-100,000 people | 59 | 14.11% |
| City inhabited by more than 100.000 people | 227 | 54.31% |
1 Note. Secondary education is basic vocational, general or technical secondary education with or without a high school diploma and post-secondary studies which are not higher education). DD – developmental disorders.
Table 2.
Opinions on ASD screening (also online) and awareness of the problem among parents depending on place of residence, education and final diagnosis of the child.
Table 2.
Opinions on ASD screening (also online) and awareness of the problem among parents depending on place of residence, education and final diagnosis of the child.
| Number of positive responses | Number of negative responses | % of positive responses | df | Χ2 | p | |
|---|---|---|---|---|---|---|
| Before screening, had you heard about ASD? | ||||||
| Place of residency | 13.013 | 0.005 | ||||
| Village | 95 | 4 | 95.96% | 3 | ||
| Town inhabited by less than 20,000 people | 33 | 0 | 100% | |||
| City inhabited by 20,000-100,000 people | 59 | 0 | 100% | |||
| City inhabited by more than 100.000 people | 227 | 0 | 100% | |||
| Education level | 13.398 | <0.001 | ||||
| Secondary education | 54 | 4 | 93.10% | 1 | ||
| Higher education | 360 | 0 | 100% | |||
| Received diagnosis of DD | ||||||
| Yes | 30 | 0 | 100% | 1 | 0.312 | 0.576 |
| No | 384 | 4 | 98.97% | |||
| Has it occurred to you that there may be possibility that your children may have ASD? | ||||||
| Place of residency | 9.581 | 0.022 | ||||
| Village | 50 | 49 | 50.51% | 3 | ||
| Town inhabited by less than 20,000 people | 23 | 10 | 69.70% | |||
| City inhabited by 20,000-100,000 people | 25 | 34 | 42.37% | |||
| City inhabited by more than 100.000 people | 136 | 91 | 59.91% | |||
| Education level | 0.189 | 0.663 | ||||
| Secondary education | 32 | 26 | 55.17% | 1 | ||
| Higher education | 202 | 158 | 56.11% | |||
| Received diagnosis of DD | ||||||
| Yes | 26 | 4 | 86.67% | 1 | 12.350 | <0,001 |
| No | 208 | 180 | 53.61% | |||
| Should screening for ASD be mandatory? | ||||||
| Place of residency | 6.749 | 0.081 | ||||
| Village | 99 | 0 | 100% | 3 | ||
| Town inhabited by less than 20,000 people | 31 | 2 | 93.94% | |||
| City inhabited by 20,000-100,000 people | 59 | 0 | 100% | |||
| City inhabited by more than 100.000 people | 221 | 6 | 97.36% | |||
| Education level | 1.028 | 0.311 | ||||
| Secondary education | 56 | 2 | 96.55% | 1 | ||
| Higher education | 354 | 6 | 98.33% | |||
| Received diagnosis of DD | ||||||
| Yes | 30 | 0 | 100% | 1 | 0.631 | 0.427 |
| No | 380 | 8 | 97.94% | |||
| Would you participate in screening for ASD in your other children? | ||||||
| Place of residency | 8.497 | 0.037 | ||||
| Village | 99 | 0 | 100% | 3 | ||
| Town inhabited by less than 20,000 people | 31 | 2 | 93.94% | |||
| City inhabited by 20,000-100,000 people | 57 | 2 | 96.61% | |||
| City inhabited by more than 100.000 people | 225 | 2 | 99.12% | |||
| Education level | 0.913 | 0.339 | ||||
| Secondary education | 58 | 0 | 100% | 1 | ||
| Higher education | 354 | 6 | 98.33% | |||
| Received diagnosis of DD | ||||||
| Yes | 30 | 0 | 100% | 1 | 0.471 | 0.493 |
| No | 382 | 6 | 98.45% | |||
| Would you participate in online screening for ASD in your other children? | ||||||
| Place of residency | 11.429 | 0.010 | ||||
| Village | 96 | 3 | 96.97% | 3 | ||
| Town inhabited by less than 20,000 people | 29 | 4 | 87.88% | |||
| City inhabited by 20,000-100,000 people | 58 | 1 | 98.31% | |||
| City inhabited by more than 100.000 people | 223 | 4 | 98.24% | |||
| Education level | 0.143 | 0.705 | ||||
| Secondary education | 56 | 2 | 96.55% | 1 | ||
| Higher education | 350 | 10 | 97.22% | |||
| Received diagnosis of DD | ||||||
| Yes | 28 | 2 | 93.33% | 1 | 1.670 | 0.196 |
| No | 378 | 10 | 97.42% | |||
| Do you prefer screening to be carried out stationary at your clinic? | ||||||
| Place of residency | 4.084 | 0.254 | ||||
| Village | 42 | 57 | 42.42% | 3 | ||
| Town inhabited by less than 20,000 people | 19 | 14 | 57.58% | |||
| City inhabited by 20,000-100,000 people | 33 | 26 | 55.93% | |||
| City inhabited by more than 100.000 people | 106 | 121 | 46.70% | |||
| Education level | 0.371 | 0.542 | ||||
| Secondary education | 24 | 34 | 41.38% | 1 | ||
| Higher education | 176 | 184 | 48.89% | |||
| Received diagnosis of DD | ||||||
| Yes | 186 | 202 | 47.94% | 1 | 0.471 | 0.493 |
| No | 14 | 16 | 46.67% |
Note. ASD – autism spectrum disorders, DD – developmental disorders, df – degrees of freedom, Χ2 - chi-square test statistic result.
Table 3.
Opinions on ASD screening (also online) and awareness of the problem among parents depending on parents’ age and IT proficiency.
Table 3.
Opinions on ASD screening (also online) and awareness of the problem among parents depending on parents’ age and IT proficiency.
| Variables | H | df | p |
|---|---|---|---|
| Before screening, had you heard about ASD? | |||
| Age | 16.327 | 19 | 0.635 |
| IT proficiency | 14.801 | 5 | 0.011 |
| Has it occurred to you that there may be possibility that your children may have ASD? | |||
| Age | 12.970 | 19 | 0.840 |
| IT proficiency | 8.374 | 5 | 0.137 |
| Should screening for DD be mandatory? | |||
| Age | 19.114 | 19 | 0.450 |
| IT proficiency | 3.277 | 5 | 0.657 |
| Would you participate in screening for DD in your other children? | |||
| Age | 27.965 | 19 | 0.084 |
| IT proficiency | 7.550 | 5 | 0.183 |
| Would you participate in online screening for DD in your other children? | |||
| Age | 16.013 | 19 | 0.656 |
| IT proficiency | 9.911 | 5 | 0.078 |
| Do you prefer screening to be carried out stationary at your clinic? | |||
| Age | 9.599 | 19 | 0.962 |
| IT proficiency | 16.212 | 5 | 0.006 |
Note. ASD – autism spectrum disorders, DD – developmental disorders, df – degrees of freedom, H - Kruskal-Wallis test statistic result.
Table 4.
Assessment of online ASD screening conducted in “Spojrzeć w oczy” project by parents depending on place of residence and education level.
Table 4.
Assessment of online ASD screening conducted in “Spojrzeć w oczy” project by parents depending on place of residence and education level.
| Variable | M | Me | SD | df | H | p |
|---|---|---|---|---|---|---|
| The information available during screening was understandable and easily accessible | ||||||
| Place of residency | 3.821 | 0.252 | ||||
| Village | 4.773 | 5 | 0.516 | 3 | ||
| Town inhabited by less than 20,000 people | 4.801 | 5 | 0.392 | |||
| City inhabited by 20,000-100,000 people | 4.925 | 5 | 0.254 | |||
| City inhabited by more than 100.000 people | 4.751 | 5 | 0.532 | |||
| Education level | 1.317 | 0.517 | ||||
| Secondary education | 4.811 | 5 | 0.381 | 1 | ||
| Higher education | 4.781 | 5 | 0.504 | |||
| I felt that I could refer any questions regarding my children's development to the people responsible for screening | ||||||
| Place of residency | 10.794 | 0.013 | ||||
| Village | 4.350 | 5 | 0.896 | 3 | ||
| Town inhabited by less than 20,000 people | 3.877 | 4 | 1.088 | |||
| City inhabited by 20,000-100,000 people | 4.284 | 5 | 0.760 | |||
| City inhabited by more than 100.000 people | 4.000 | 5 | 1.003 | |||
| Education level | 1.710 | 0.452 | ||||
| Secondary education | 3.900 | 5 | 1.165 | 1 | ||
| Higher education | 4.144 | 5 | 0.927 | |||
| I would receive appropriate help or advice in case of suspicion DD from people involved in online screening | ||||||
| Place of residency | 21.323 | <0.001 | ||||
| Village | 4.433 | 5 | 0.778 | 3 | ||
| Town inhabited by less than 20,000 people | 3.913 | 4 | 0.918 | |||
| City inhabited by 20,000-100,000 people | 4.240 | 5 | 0.863 | |||
| City inhabited by more than 100.000 people | 3.919 | 4 | 0.972 | |||
| Education level | 6.043 | 0.048 | ||||
| Secondary education | 4.264 | 5 | 0.935 | 1 | ||
| Higher education | 4.051 | 4 | 0.925 | |||
| Overall, I am satisfied with my participation in electronic ASD screening | ||||||
| Place of residency | 3.450 | 0.278 | ||||
| Village | 4.722 | 5 | 0.639 | 3 | ||
| Town inhabited by less than 20,000 people | 4.769 | 5 | 0.415 | |||
| City inhabited by 20,000-100,000 people | 4.705 | 5 | 0.544 | |||
| City inhabited by more than 100.000 people | 4.655 | 5 | 0.607 | |||
| Education level | 2.067 | 0.356 | ||||
| Secondary education | 4.734 | 5 | 0.614 | 1 | ||
| Higher education | 4.679 | 5 | 0.590 |
Note. Answers were given on a Likert scale, where 1 - I completely disagree with this sentence, 5 - I completely agree with this sentence. ASD – autism spectrum disorders, DD – developmental disorders, df – degrees of freedom, H - Kruskal-Wallis test statistic result, M – mean, Me – median, SD – standard deviation.
Table 5.
Assessment of online ASD screening conducted in “Spojrzeć w oczy” project by parents depending on parents’ age and IT proficiency.
Table 5.
Assessment of online ASD screening conducted in “Spojrzeć w oczy” project by parents depending on parents’ age and IT proficiency.
| Variables | r | t | p |
|---|---|---|---|
| Age & The information available during screening was understandable and easily accessible | -0.093 | -1.895 | 0.059 |
| Age & I felt that I could refer any questions regarding my children's development to the people responsible for screening | -0.104 | -2.140 | 0.033 |
| Age & I would receive appropriate help or advice in case of suspicion DD from people involved in online screening | 0.033 | 0.677 | 0.499 |
| Age & Overall, I am satisfied with my participation in electronic ASD screening | -0.030 | -0.618 | 0.537 |
| IT proficiency & The information available during screening was understandable and easily accessible | 0,058 | 1.176 | 0.240 |
| IT proficiency & I felt that I could refer any questions regarding my children's development to the people responsible for screening | 0,024 | 0.492 | 0.623 |
| IT proficiency & I would receive appropriate help or advice in case of suspicion DD from people involved in online screening | -0,009 | -0.185 | 0.853 |
| IT proficiency & Overall, I am satisfied with my participation in electronic ASD screening | -0.026 | -0.528 | 0.598 |
Note. ASD – autism spectrum disorders, DD – developmental disorders, r - Spearman's rho statistic result, t - the value of the t statistic testing the significance of the correlation coefficient.
Table 6.
Sociodemographic characteristics of doctors taking part in the study.
| Characteristics (Total N = 95) | n | % |
|---|---|---|
| Sex | ||
| Female | 62 | 65.26% |
| Male | 33 | 34.74% |
| Main place of practicing a profession | ||
| Village | 7 | 7.37% |
| Town inhabited by less than 20,000 people | 9 | 9.47% |
| City inhabited by 20,000-100,000 people | 22 | 23.16% |
| City inhabited by more than 100.000 people | 57 | 60.00% |
| Percentage of pediatric patients among all doctor's patients | ||
| up to approx. 10% of total | 22 | 23.15% |
| up to approx. 20% of total | 27 | 28.42% |
| up to approx. 30% of total | 19 | 20.00% |
| up to approx. 40% of total | 6 | 6.32% |
| up to approx. 50% of total | 10 | 10.53% |
| more than 50% of total | 11 | 11.58% |
Table 7.
The usage of screening methods, the choice of management in case of suspected DD and preferred screening method (online vs stationary) depending on the sex, primary place of work of physicians and percentage of pediatric patients among all patients.
Table 7.
The usage of screening methods, the choice of management in case of suspected DD and preferred screening method (online vs stationary) depending on the sex, primary place of work of physicians and percentage of pediatric patients among all patients.
| Variable | Total N = 95 |
Sex | Χ2/H* | p | Primary place of work | Χ2/H* | p | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Females N = 62 |
Males N = 33 |
VillageN = 7 | Town N = 9 |
Small city N = 22 | Big cityN = 57 | ||||||||||||||||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||||||||||||||||
| Usage of screening methods for DD (e.g. ASD) | 1.246 | 0.265 | |||||||||||||||||||||||||||
| in all children | 39 | 41.05% | 28 | 45.16% | 11 | 33.33% | 2 | 28.57% | 3 | 33.33% | 7 | 31.82% | 27 | 47.37% | 2.388 | 0.496 | |||||||||||||
| in at-risk children or suspected of having DD | 55 | 57.89% | 33 | 53.23% | 22 | 66.67% | 5 | 71.43% | 6 | 66.67% | 15 | 68.18% | 29 | 50.88% | |||||||||||||||
| lack of use of screening tools | 1 | 1.05% | 1 | 1.61% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 1 | 1.75% | |||||||||||||||
| Management of a child under 2 years of age in the event of subtle symptoms of developmental disorders | 0.897 | 0.343 | |||||||||||||||||||||||||||
| referral for further diagnostics | 51 | 53.68% | 32 | 51.61% | 19 | 57.58% | 2 | 28.57% | 8 | 88.89% | 13 | 59.09% | 28 | 49.12% | 1.162 | 0.762 | |||||||||||||
| referral for further diagnostics at the insistence of parents | 8 | 8.42% | 4 | 6.45% | 4 | 12.12% | 1 | 14.29% | 0 | 0.00% | 2 | 9.09% | 5 | 8.77% | |||||||||||||||
| further observation of the child's development | 36 | 37.89% | 26 | 41.94% | 10 | 30.30% | 4 | 57.14% | 1 | 11.11% | 6 | 27.27% | 24 | 42.11% | |||||||||||||||
| Management of a child above 2 years of age in the event of subtle symptoms of developmental disorders | 0.538 | 0.463 | |||||||||||||||||||||||||||
| referral for further diagnostics | 90 | 94.74% | 57 | 91.94% | 33 | 100.00% | 5 | 71.43% | 9 | 100.00% | 21 | 95.45% | 55 | 96.49% | 12.706 | 0.005 | |||||||||||||
| referral for further diagnostics at the insistence of parents | 1 | 1.05% | 1 | 1.61% | 0 | 0.00% | 1 | 14.29% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |||||||||||||||
| further observation of the child's development | 4 | 4.21% | 4 | 6.45% | 0 | 0.00% | 1 | 14.29% | 0 | 0.00% | 1 | 4.55% | 2 | 3.51% | |||||||||||||||
| Preferred screening method | |||||||||||||||||||||||||||||
| stationary | 44 | 46.32% | 30 | 48.39% | 14 | 42.42% | 0.304 | 0.581 | 3 | 42.86% | 3 | 33.33% | 6 | 27.27% | 32 | 56.14% | 6.001 | 0.112 | |||||||||||
| on-line | 51 | 53.68% | 32 | 51.61% | 19 | 57.58% | 4 | 57.14% | 6 | 66.67% | 16 | 72.73% | 25 | 43.86% | |||||||||||||||
| Variable | Percentage of pediatric patients among all patients | Χ2/H* | p | ||||||||||||||||||||||||||
| <10% N = 22 | <20% N = 27 | <30% N = 19 | <40% N = 6 | <50% N = 10 | >50% N = 11 | ||||||||||||||||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||||||||||||||||||
| Usage of screening methods for DD (e.g. ASD) | |||||||||||||||||||||||||||||
| in all children | 4 | 18.18% | 18 | 66.67% | 7 | 36.84% | 0 | 0.00% | 3 | 30.00% | 7 | 63.64% | 19.216 | 0.002 | |||||||||||||||
| in at-risk children or suspected of having DD | 18 | 81.82% | 8 | 29.63% | 12 | 63.16% | 6 | 100.00% | 7 | 70.00% | 4 | 36.36% | |||||||||||||||||
| lack of use of screening tools | 0 | 0.00% | 1 | 3.70% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | |||||||||||||||||
| Management of a child under 2 years of age in the event of subtle symptoms of developmental disorders | |||||||||||||||||||||||||||||
| referral for further diagnostics | 15 | 68.18% | 12 | 44.44% | 11 | 57.89% | 3 | 50.00% | 6 | 60.00% | 4 | 36.36% | 10.271 | 0.068 | |||||||||||||||
| referral for further diagnostics at the insistence of parents | 0 | 0.00% | 1 | 3.70% | 2 | 10.53% | 0 | 0.00% | 2 | 20.00% | 3 | 27.27% | |||||||||||||||||
| further observation of the child's development | 7 | 31.82% | 14 | 51.85% | 6 | 31.58% | 3 | 50.00% | 2 | 20.00% | 4 | 36.36% | |||||||||||||||||
| Management of a child above 2 years of age in the event of subtle symptoms of developmental disorders | |||||||||||||||||||||||||||||
| referral for further diagnostics | 20 | 90.91% | 26 | 96.30% | 19 | 100.00% | 6 | 100.00% | 9 | 90.00% | 10 | 90.91% | 8.590 | 0.127 | |||||||||||||||
| referral for further diagnostics at the insistence of parents | 0 | 0.00% | 0.00% | 0 | 0.00% | 0 | 0.00% | 1 | 10.00% | 0 | 0.00% | ||||||||||||||||||
| further observation of the child's development | 2 | 9.09% | 1 | 3.70% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 1 | 9.09% | |||||||||||||||||
| Preferred screening method | |||||||||||||||||||||||||||||
| stationary | 13 | 59.09% | 11 | 40.74% | 5 | 26.32% | 4 | 66.67% | 6 | 60.00% | 5 | 45.45% | 6.524 | 0.259 | |||||||||||||||
| on-line | 9 | 40.91% | 16 | 59.26% | 14 | 73.68% | 2 | 33.33% | 4 | 40.00% | 6 | 54.55% | |||||||||||||||||
Note. ASD – autism spectrum disorders, DD – developmental disorders, H - Kruskal-Wallis test statistic result, Χ2 - chi-square test statistic result. Kruskal-Wallis’ H test used only in preferred screening method analysis.
Table 9.
Willingness to use DD screening diagnostic questionnaires during specific visits at primary care facilities.
Table 9.
Willingness to use DD screening diagnostic questionnaires during specific visits at primary care facilities.
| How willingly would you use tools for screening developmental disorders in the following situations? | M | Me | SD | H | p |
|---|---|---|---|---|---|
| during the vaccination qualifying visit at 18 months of age | 3.512 | 4 | 1.094 | 46.069 | <0.001 |
| during the well-child visit in 2nd year of life | 3.828 | 4 | 1.022 | ||
| when noticing symptoms of developmental disorders in child during the visit | 4.415 | 5 | 0.736 | ||
| when a parent expresses concerns about their child's development | 4.362 | 5 | 0.735 | ||
| if the child has a sibling with ASD or another developmental disorder | 4.207 | 4 | 0.787 |
Note. Answers were given on a Likert scale, where 1 – very reluctantly, 5 – very willingly. ASD – autism spectrum disorders, DD – developmental disorders, df – degrees of freedom, H - Kruskal-Wallis test statistic result.. Three respondents did not provide answers regarding this part.
Table 10.
Evaluation of the advantages and positives of online ASD screening by parents and physicians.
Table 10.
Evaluation of the advantages and positives of online ASD screening by parents and physicians.
| Variable | Parents N = 418 |
Doctors N = 95 |
Χ 2(df=1) |
p | ||||
|---|---|---|---|---|---|---|---|---|
| n | % of parents | % of total answers | n | % of doctors | % of total answers | |||
| Which of the positives of online ASD screening are the most important to you? | ||||||||
| possibility of contact with health care professionals qualified in the field of developmental disorders | 153 | 36.60% | 13.08% | 31 | 32.63% | 13.19% | 0.53 | 0.466 |
| saving time on screening (possibility to perform screening at home) | 285 | 68.18% | 24.36% | 61 | 64.21% | 25.96% | 0,56 | 0.456 |
| no potential stigmatization of the child in the event of developmental disorders (person examining does not personally know the family/child) | 118 | 28.23% | 10.09% | 30 | 31.58% | 12.77% | 0.42 | 0.515 |
| possibility of performing the test at any convenient time | 327 | 78.23% | 27.95% | 64 | 67.37% | 27.23% | 5.04 | 0.025 |
| easier access to the screening (it is not necessary to look for people qualified to perform screening) | 287 | 68.66% | 24.53% | 49 | 51.58% | 20.85% | 9.99 | 0.002 |
| Total | 1170 | n/a | 100% | 235 | n/a | 100% | ||
| What are the greatest difficulties in conducting online screening in your opinion? | ||||||||
| lack of direct (physical) contact with the examiner (e.g. doctor, nurse, psychologist) | 195 | 46.65% | 29.64% | 53 | 55.79% | 31.18% | 2.59 | 0.108 |
| inability to confirm the result of the screening test in clinical observation by a doctor/psychologist | 242 | 57.89% | 36.78% | 50 | 52.63% | 29.41% | 0.87 | 0.350 |
| the need to wait for an explanation of the obtained result | 50 | 11.96% | 7.60% | 19 | 20.00% | 11.18% | 3.63 | 0.057 |
| inability to quickly clarify doubts regarding the development of the child's behavior | 163 | 39.00% | 24.77% | 39 | 41.05% | 22.94% | 0.14 | 0.711 |
| lack of trust in people responsible for online screening | 8 | 1.91% | 1.22% | 9 | 9.47% | 5.29% | 11.55 | <0.001 |
| Total | 658 | n/a | 100% | 170 | n/a | 100% | ||
Note. ASD – autism spectrum disorders, Χ2 - chi-square test statistic result.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



