
Submitted:
25 March 2024
Posted:
26 March 2024
You are already at the latest version
Abstract
Background: Autism spectrum disorder (ASD) is a persistent neurodevelopment disorder frequently co-occurring with Attention-Deficit/Hyperactivity Disorder (ADHD) and behavior-related disorders. While behavioral therapy is the first-line option to manage ASD core symptoms, pharmacological therapy is sometimes needed to treat acute problems, such as agitation and aggressive behaviors. Recent guidelines recommend neuroleptics to reduce psychomotor agitation in people with ASD. However, since children with ASD are often drug-resistant, alternative treatments are often justified.
Reports from literature showed that intra-venous valproate (IV-VPA) can be effective in reducing agitation in psychiatric patients, with lower frequency of adverse events compared to convention-al treatments. However, since findings are occasionally inconsistent, IV-VPA is not an approved option in clinical psychiatry. We aim at improving the knowledge on the IV-VPA treatment option in emergency psychiatry in the pediatric age.
Methods: We report the case of a 11-year-old boy suffering from a complex neurodevelopmental condition, who experienced a psychotic episode with severe aggressive and disruptive behaviors, successfully treated with IV-VPA. Besides, we conducted an up-dated literature review on this topic.
Conclusion: In our case, first-line therapies proved to be ineffective. On the contrary, IV-VPA led to a safe and prompt clinical success, in line with other reports. Based on our literature review, IV-VPA can be highly effective and can reduce the risk of adverse events that frequently occur with the use of high-dose standard medications in emergency psychiatry.
Keywords:
Autism
; ADHD
; agitation
; intravenous valproate.
1. Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder that affects communication, social interaction and behavioral skills. It is characterized by restricted interests, repetitive and stereotyped behaviors, and abnormal sensory processing. Neurodevelopmental atypia can be observed early in the development of most children with ASD [1], and it persists life long. Both clinical presentation of symptoms and their severity can vary greatly depending on age, cognitive and language abilities. Frequently co-occurring conditions include Attention-deficit hyperactivity disorder (ADHD), depression, phobias, anxiety, intellectual disability, sleep issues, restrictive/avoidant food intake, sensory processing issues, and genetic alterations. Comorbidities often make diagnosis and clinical management of ASD extremely complex [2]. Furthermore, an unpredictable response to treatment associated with the frequent apperance of side effects can make the pharmacological therapy of ASD a heavy challenge for clinicians. However, indirect improvement has been seen when therapies are targeted to comorbidity symptoms [3].
ADHD is a neurodevelopmental disorder characterized by inattention, hyperactivity, and impulsivity, causing functional impairment. Its prevalence is approximately 5% in children and adolescents and about 2.5% in adults [4]. According to international guidelines, the most efficient managing for ADHD include a multimodal approach that involves both behavioral and pharmacological treatments. Methylphenidate (MPH) is the most frequently prescribed medication for the treatment of ADHD in children and adolescents in many countries, including Europe, where it is the first treatment choice [5,6].
Comorbidity between ADHD and ASD is a common condition, being ADHD the commonest disorder to co-occur with ASD. Clinical similarities between the two disorders are frequent as they share symptoms of inattention and hyperactivity/impulsivity and a high occurrence of at least one psychiatric condition (around 80% in ADHD and 2/3 in ASD patients) [7]. In individuals where ASD and ADHD co-occur, pharmacological interventions may facilitate their participation in behavioral therapy and enhance their daily functioning. However, children with ASD are more sensitive to medication side-effects and have a higher likelihood of experiencing adverse events compared to those without ASD. Therefore, in patients with ASD-ADHD comorbidity, the pharmacological treatment should be started at lower doses and adjusted slower than in subjects with ADHD diagnosis alone [2].
Furthermore, these patients frequently experience psychomotor agitation, defined as a state of heightened anxiety, irritability, increased motor and verbal activities, uncooperativeness, and threatening gestures. Pharmacological treatment in acute agitations and aggressive behaviours is sometimes challenging for clinicians. Complex neurodevelopmental disorders associated with ASD and ADHD, but also with schizophrenia, schizoaffective disorder, bipolar mania, and illicit drug use are even more complex and risky to treat [8]. In principle, an effective psychopharmacological intervention should obtain reduction of psychoagitation, reach calmness and restore contact, within two hours [9]. Most severe agitations can be treated with neuroleptics and a close monitoring of their total daily dose. Olanzapine is potentially the most sedating second-generation antipsycotic (SGA) compared to risperidone and haloperidol, with a lower risk of cardiac adverse events and extrapyramidal signs [10]. Due to the risk of respiratory suppression when given add-on, olanzapine should not be given parenterally within one hour from benzodiazepines administration [10].
Valproate (2-propylpentanoate, VPA) is available as valproic acid, sodium valproate and semisodium formulations. Its mechanism of action involves the enhancement of inhibitory neurotransmission and the modulation of voltage-gated ion channels. It has actions on dopamine, GABA and glutamate neurotransmission and intracellular signaling. VPA is a common and approved drug used in children and adults as a safe and effective antiepileptic, both with oral [11] and intravenous (IV) administration routes [12,13,14]. Apart from its FDA indications for treatment of epilepsy, oral VPA can find off-label applications in several psychiatric conditions, such as maniac episodes associated with bipolar disorder, impulsivity, agitation, and aggression [15,16,17]. Oral VPA has also been shown to reduce aggressive, repetitive symptoms and irritability in children with ASD compared to controls [18,19,20].
A recent study shows that off-label IV-VPA can be effective and safe in treating psychomotor agitation of adolescents aged between 13 and 17 years [22]. Overall, data on the efficacy of IV-VPA in acute and aggressive agitations of children with ASD are currently not available in literature.
To implement the increasing knowledge on IV-VPA treatment option in emergency psychiatry, and ASD in particular, we describe a clinical case in the light of previous related reports and a literature review.
2. Methods and Case Report
With the present study we aim at reviewing the available literature, i.e., clinical reports (case or clinical series), narrative and systematic reviews, on the use of VPA in the treatment of acute agitation. Pertinent literature was obtained from PubMed database, which included only English-written, full-text clinical studies, clinical reports and reviews. With regard to interventional studies, we only included those that provided the ethical approval code. The search was started on September 18th, 2023 by applying the following key terms: “autism” and “aggressive behavior” and “acute agitation” and “valproic acid”. The temporal interval for search was between 1995 and 2023. Data extraction consisted of a total of 93 articles and study selection flow chart, in line with the PRISMA 2020 flow diagrams, is reported in the Figure 1. After removal of duplicated, among a total 65 articles, 34 were screened by title and abstract, and 20 were considered eligible with respect to key words and methods criteria, and evaluated at a full-text level. Of them, in order to produce a qualitative synthesis on treatment efficacy, 4 studies were considered eligible with respect to the patients’ age (children and adolescents) and IV administration of VPA.
This figure shows the flow-chart selection criteria of the collected articles.
To date, to the best of our knowledge, only one report describes the use of IV-VPA in acute agitation in children with autism; we found no studies evaluating its efficacy in complex neurodevelopmental conditions or in patients with co-occurring ASD and ADHD. We report a case of a young boy with a complex neurodevelopmental disorder characterized ASD with comorbid ADHD.
3. Case Report
We describe a 11-years-old boy with a diagnosis of level 1-ASD, Attention-Deficit/Hyperactivity Disorder - Combined presentation, Oppositional Defiant Disorder and Adjustment Disorder, according with DSM-5 criteria.
On March 2023, he was re-admitted in our emergency Hospital department due to the acute onset of a bizarre behavior (e.g., stripped naked in public), disruptive mood (verbal oppositional and role-breaking behaviours with all people including family members), and severe aggressive symptoms (he destroyed tools and furniture complements). His parents dated a decline in their child behavior since January 2023, the alleged trigger being represented by the unsupervised internet access and the contact with unknown adults who had solicited virtual sexual interactions.
Medical history: The patient had a family history for alcohol abuse and socio-economical problems. He was born by a regular pregnancy, through a natural delivery at the 41 week of pregnancy. Parents denied any suffering at birth. A delay in language skills was reported with first words at 2 years. Firsts problems in social abilities were reported at kindergarden, for a deficit in showing spontaneously interest to others and in starting any interaction during activities with peers. He also showed difficulty accepting variations from his routines, in removing the diapers, putting on new clothes or shoes, or eating foods other than unseasoned pasta or bread. The game was extremely poor, excessively chaotic, but characterized by repetitiveness: rolling objects, throwing them and going up and down in rigid and afinalistic sequences.
Repetitive patterns overactivity, delay aversion and concentration problems emerged during preschool stages and he received a diagnosis of Pervasive Developmental Disorder and rehabilitation treatments at local Community Services for Child and Adolescent Neuropsychiatry since he was 3 years old.
In 2019, at the age of 7 years, he was firstly admitted to our Unit of Child Neuropsychiatry of Sassari Hospital, due to progressively increasing psychomotor agitation and aggressive behaviors towards teachers and peers at school. He experienced agitation with both self- and hetero-aggressiveness in response to minimal frustrations. During hospitalization, he exhibited quantitative and qualitative abnormalities in social interaction skills, communication deficits, narrow and repetitive interests, poor flexibility and intolerance to frustrations, difficulty in maintaining and modulating eye contact, and poor abilities in theory of mind understanding. The child also tended to have high levels of hyperactivity with impulsiveness, acting without previous reflection and engaging in danger awareness. To quantify ADHD symptoms severity, several standardized tests were performed: Swanson, Nolan, and Pelham Rating Scale-SNAP-IV [23], Conners’ Parent Rating Scale [24], and Child Behavior Check List to parents [25], resulting in high scores for both hyperactivity and impulsivity and Oppositional Defiant Disorder (ODD) symptoms. To assess cognitive functioning, we administered the Leiter International Performance Scale - Third Edition [26] which showed fluid reasoning of 77 and a short nonverbal IQ of 74. He received a diagnosis of severe ADHD with combined clinical manifestation with severe Oppositional and Defiant Disorder (ODD). Finally the 2nd version of the Autism Diagnostic Observational Schedule - ADOS-2 [27] test was administered, which confirmed a co-occurring, level 1, ASD condition. Genetics analysis (karyotype, FMR1A gene, Pompe disease, Duchenne/Becker disease, Gaucher and Niemann-Pick disease), electroencephalogram, brain MRI, complete abdomen ultrasound and cardiological examination with echocardiogram, all resulted negative; dermatological examination showed 6 café-au-lait macules, neck and large folds hyperpigmentation and follicular hyperkeratosis. At discharge, a psycho-stimulant therapy, in addition to a Cognitive Behavioral Therapy (CBT) to treat ADHD were suggested, but his parents initially refused. After one year, when kids was 8 years old, they come back for a new visit at our outpatients service to evaluate the introduction of methilphenidate (MPH) treatement due to difficulties in manging ADHD symptoms at school and at home. Immediate-release MPH was initially introduced at a dose of 0.3 mg/kg. Absence of adverse events, good control of inattention symptoms and a reduction in motor hyperactivity were observed. For this reason, the equivalent dose of prolonged-release MPH was subsequently prescribed to continue the therapy at home. The child continueted the prescribed therapy and for the following three years the effectiveness was reported in periodic checks.
Emergency Acceptance
At the emergency room, blood exams (including kidneys, liver and thyroid), neurological assessment and urine toxicological tests were all normal. On 2nd March 2023 a preliminar Electrocardiogram was performed, to search for possible contraindications of pharmacological treatment, was also normal (see Table 1).
After this preliminary step, the boy was immediately treated with multiple medications at high dosages (haloperidol, benzodiazepines, and chlorpromazine), although with poor efficacy on aggressive behavior and with the rapid appearance of several adverse event, e.g., sedation, sialorrhea and rigidity (pharmacological timeline is detailed on Figure 1).
MPH was immediately interrupted to avoid a maniac phase induction. Olanzapine was introduced and used at a dosage to 10 mg/die, before being interrupted after four days, due to the lack of a positive response. Risperidone was gradually modulated up to 6 mg per day and extended-release Lithium sulfate therapy was introduced, to potentiate the neuroleptic effect, and titrated up until the blood range of 0.8 mEq/L (Figure 1).
Unfortunately, acute symptoms persisted. Therefore, on the third day of hospitalization, we carried out a IV bolus of 20 mg/kg VPA in a temporal range of 30 minutes. After that, we started a 24-h infusion with the same dosage, followed by three days IV infusion at a lower dosage (15 mg/kg/day). Vital signs, blood pressure and heart frequency were costantly checked.
An immediate response was observed after the first few hours and IV-VPA. On the fourth day, IV-VPA was replaced by its extended oral formulation and tapered off in one week (Figure 2) with a good response and no adverse drug effects. Contextually, benzodiazepines and olanzapine were gradually tapered off and Lithium continuated.
We used the Modified Version of the Overth Aggression Scale (MOAS) [28] to assess and measure aggressive behaviors, which showed a decrease from a score of 49 upon admission to a score of 0 upon discharge. Despite a mild sedation, an important and rapid decrease of aggressive behavior occurred after IV-VPA, associated with a reduction in the MOAS score (Figure 3).
During hospitalization, electrocardiograms and regular blood tests were carried out to monitor serum levels of VPA, ammonia, lithium, and liver enzymes. During acute IV treatement, the highest value of VPA was 92.7 μg/mL (in the normality range). All the other range are reported in Tabel 1 above. After 11 days, he was discharged with a DSM-5-oriented diagnoses of psychotic onset with psychomotor agitation in patient with co-morbidity for ASD level 1, severe ADHD-Combined clinical presentation, adjustment disorder with mixed emotionality and conduct symptoms. Home therapy with long-acting Lithium sulfate 249 mg/day and Risperidone 3.5 mg/day. In fact, VPA is used during the state of agitation and then replaced by another stabilizer: lithium.
One-year follow-up. The patient attended all the monthly programmed outpatient visits at our Unit. He had come back to school two weeks after the last hospital discharge and continued his psychotherapy twice per week. In October 2023 he presented with occasional agitation episodes, irritable mood with anger and frustration over small things (i.e., after denial of food). He displayed short temper and might snap at people in different contexts (classmates, teacher, medical doctors and caregivers). Lithium blood level was reduced (0.45 mEq/l) compared to one month before (0.66). Therefore long-acting lithium solfate was increased. A good clinical response was reported in some weeks. At last examination on March 2024, pharmacological therapy was substantially stable. Parents received benefit supports from the social assistence and pursued a specific parent’s program to improve their educational competences.
This little boy still refers at the outpatiens service at our institution. Him history and clinical trajectory are at high risk to develop other mood or psychosis event, moreover when further environmental stressors will occur.
4. Results of Literature Review
Thirty-four articles evaluating the efficacy of both oral and IV VPA, in different clinical psychiatric settings of children, adolescents and adults, were screened by title and abstract. Among these, three (8.8%) case reports, one (2.9%) cohort study, one (2.9%) case-control study, three (8.8%) clinical trials, four (11.7%) meta-analyses, seven (20.6%) systematic reviews, twelve (35.3%) literature reviews, three (8.8%) randomized clinical trial and one (2.9%) thematic analysis, were found (Table 2).
With regard to VPA administration, nine (26.4%) report on IV-VPA administration, twenty-two (64.7%) on oral VPA administration; in 3 studies the route of administration was not specified (8.8%). All recruited participants had a condition of acute agitation, aggressivity, sometimes during maniac acute phases.
In order to better classify the acute agitation with aggressivity, we identified four cathegorical clinical diagnoses that had preceeded the acute psychiatric phase. The most frequent diagnosis associated to aggressive agitation was Mood Disorders (MD), particularly Bipolar Disorder (17 reports), followed by Schizophrenia Spectrum Disorders (SSD; 15 reports), detailed Schizophrenia (8 reports) and Schizoaffective Disorder (7 reports). We also found Disruptive Behaviours Disorders (DBD) in 6 case descriptions: 3 cases had Conduct Disorder and 3 other cases had Oppositional and Defiant Disorder. Finally, we found 5 articles describing Trauma and Stressor-related Disorders (TSD), with clinical descriptions of Post-Traumatic Stress (n= 4) and Adjustment Disorder (n= 1).
As to the comorbibity issue, the co-occurrence of MD and acute agitation were more frequently reported when a diagnosis of neurodevelopmental disorders occured, particulary ADHD and ASD, sometimes in association with anxiety symptoms. Acute agitation in SSD were reported alone or, in some cases, in association with stressors events, in people with a long clinical history. In 9 articles, DBD was reported in patients with a previous diagnosis of ADHD and, in 4 of them, in association with Substance Abuse disorder. TSD was usually described as a trigger factor in patients with neurodevelopmental, mood and/or anxiety disorders.
As regards treatment efficacy, we selected twenty articles at a full-text level and in line with inclusion criteria. Of these, 14 reports were not retrieved and further 2 studies were excluded due to the involvement of adults; finally only 4 studies were considered eligible for a literature review: one systematic review, two literature reviews and two case reports. Papers were classified in relation to the efficacy of IV-VPA treatment in children and adolescents (1= yes; 0= no; X= no differences) as summarized onTable 3. Overall, an immediated relief from acute aggressive agitation symptoms with IV-VPA, was reported in all studies. Differents dosages were used depending on the stage of the acute episode: in the hyperacute stage the induction dose was 1400 mg per day (15-20 mg/kg). The duration of the first phase ranged between ten minutes (single IV dose) and five days. All reports described a gradual dose reduction within a range of 3 to 17 days. After IV-VPA tapering-off, oral VPA was prescribed up to six months, or until the complete clinical remission. In this cases, oral VPA doses were maintained between 355 and 1000 mg per day.
All patients underwent a concomitant medication started either some time before the acute agitation or in add-on. The most prescribed were anticholinergic, benzodiazepines, first generation antipsychotics, mood stabilizer and second generation antipsychotics.
The most used instruments to quantify the reduction of aggressive behaviours were the Modified Overt Aggression Scale, the Overt Aggression Scale, the Aberrant Behavior Checklist, the Brief psychiatric rating scale, the Bech–Rafaelsen Mania Scale and the Clinical global impression. In some cases, when a psychiatric exam was possible, authors reported the Mini mental state examination.
In conclusion, a significant symptom reduction emerges when IV-VPA is used for resistant agitation with aggressive behaviours in children and adolescents with all different scales and interviews. The safety profile was satisfactory with only a mild to moderate sedaction and no significant alteration of blood analyses.
4. Discussion
Treating young patients with acute agitation and comorbid neurodevelopmental conditions of ASD and ADHD, is one of the most challenging task for clinicians [2,8,9]. Most severe agitations are treated with neuroleptics although, in complex neurodevelopmental disorders, they should be started at lower doses and with slower adjustement compared to other patients [2]; also, a close monitoring of the total daily dose is recommended. Oral second generation antipsychotics, such as risperidone, olanzapine, aripiprazole and ziprasidone, or the first generation haloperidol, in monotherapy or in association with benzodiazepines, have been shown to be at least similarly effective than oral VPA.
Our case report as well as our literature review both indicate that, compared to oral VPA [18,19,20], the IV use of VPA in add-on with neuroleptics in critical patients between 8 and 17 years, is rapidly effective and fairly safe [22] even in the presence of ASD comorbidity [21,22].
The IV route of administration of VPA in children and adolescents is, currently, limited to non-responders and non-compliant patients which is mainly due to the evidence that it has been tested mainly in adults patients with Bipolar disorder. However, the qualitative analysis of our selected papers and the description of our case, can encourage IV-VPA as an effective and safe treatement for acute agitation and aggressive behaviours in children and adolescents with neurodevelopmental disorders, such as ASD and ADHD. Furthermore, the safety profile of IV VPA can make it the elective drug even in agitated situations in patients with a history of substance abuse [42].
In literature, stressor events contribute to promote acute symptoms in patients with previous diagnosis of neurodevelopmental disorders; accordingly, our case was exposed to a traumatic event some months before the acute phase. This may be important to consider in order prevent environmental factors to trigger aggressive behaviours and agitation in susceptible children.
There are limitations while interpreting overall results. The first is that among the 34 selected reports, only 4 met the requirements to be included in our review. The second is that IV-VPA has a limited degree of evidence, particularly in children and adolescents with neurodevelopmental disorders; also, the majority of observations are reviews, retrospective case-control studies or anecdotal reports and, with the exception of our case (one-year follow-up), clinical monitoring is not longer than 6 months.
5. Conclusions
Our case is the first clinical case on the empirical use of IV-VPA for acute agitation and aggressive behaviors in a child boy with co-occurring ASD and ADHD.
Our report and our review of the recent studies, suggest IV-VPA as an effective alternative treatment that limits the risk of adverse events related to the high-dose standard medications in the emergency psychiatry.
Further studies are needed to assess whether IV-VPA might be a first-line choice therapy to treat acute and drug-resistant agitation in children.
Author Contributions
Conceptualization, A.C. and V.C.; methodology, A.C. and VC; software, M.P.; validation, G.S.; A.C., V.C. and S.S.; formal analysis, M.P.; investigation, A.C. and V.C; resources, S.S.; data curation, V.C.; writing—original draft preparation, A.C.; V.C. and R.A.; writing—review and editing, A.C.; V.C.; M.P.; R.A.; G.S.; G.V; S.V. and S.S.; visualization, R.A.; G.S.; G.V. and S.V; supervision, G.S.; G.V.; S.V. and S.S; project administration, A.C. and S.S. ; funding acquisition, S.S. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the reason that this is a review article and a case-report paper.
Informed Consent Statement
Written informed consent for publication has been obtained from parent’s patient, although he cannot be identified, to publish this paper.
Data Availability Statement
Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
Authors acknowledge support given by the medical and nursery staff. A special thanks goes to all patients with neurodevelopmental disorders and their families.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Di Luzio, M.; Guerrera, S.; Pontillo, M.; Lala, M.R.; Casula, L.; Valeri, G.; Vicari, S. Autism spectrum disorder, very-early onset schizophrenia, and child disintegrative disorder: the challenge of diagnosis. A case-report study. Front. Psychiatry 2023, 14, 1212687. [Google Scholar] [CrossRef]
- Aishworiya, R.; Valica, T.; Hagerman, R.; Restrepo, B. An Update on Psychopharmacological Treatment of Autism Spectrum Disorder. Neurotherapeutics 2022, 19, 248–262. [Google Scholar] [CrossRef] [PubMed]
- Persico, A.M.; Ricciardello, A.; Lamberti, M.; Turriziani, L.; Cucinotta, F.; Brogna, C.; Vitiello, B.; Arango, C. The pediatric psychopharmacology of autism spectrum disorder: A systematic review - Part I: The past and the present. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2021, 110, 110326. [Google Scholar] [CrossRef] [PubMed]
- Mechler, K.; Banaschewski, T.; Hohmann, S.; Häge, A. Evidence-based pharmacological treatment options for ADHD in children and adolescents. Pharmacol. Ther. 2021, 230, 107940. [Google Scholar] [CrossRef]
- Carucci, S.; Balia, C.; Gagliano, A.; Lampis, A.; Buitelaar, J.K.; Danckaerts, M.; Dittmann, R.W.; Garas, P.; Hollis, C.; Inglis, S.; et al. Long term methylphenidate exposure and growth in children and adolescents with ADHD. A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2020, 120, 509–525. [Google Scholar] [CrossRef] [PubMed]
- Man, K.K.C.; Häge, A.; Banaschewski, T.; Inglis, S.K.; Buitelaar, J.; Carucci, S.; Danckaerts, M.; Dittmann, R.W.; Falissard, B.; Garas, P.; et al. Long-term safety of methylphenidate in children and adolescents with ADHD: 2-year outcomes of the Attention Deficit Hyperactivity Disorder Drugs Use Chronic Effects (ADDUCE) study. Lancet Psychiatry 2023, 10, 323–333. [Google Scholar] [CrossRef]
- Carta, A.; Fucà, E.; Guerrera, S.; Napoli, E.; Valeri, G.; Vicari, S. Characterization of Clinical Manifestations in the Co-occurring Phenotype of Attention Deficit/Hyperactivity Disorder and Autism Spectrum Disorder. Front. Psychol. 2020, 11, 861. [Google Scholar] [CrossRef]
- Marzullo, L.R. Pharmacologic Management of the Agitated Child. Pediatr. Emerg. Care 2014, 30, 269–275. [Google Scholar] [CrossRef]
- Bak, M.; Weltens, I.; Bervoets, C.; De Fruyt, J.; Samochowiec, J.; Fiorillo, A.; Sampogna, G.; Bienkowski, P.; Preuss, W.U.; Misiak, B.; et al. The pharmacological management of agitated and aggressive behaviour: A systematic review and meta-analysis. Eur. Psychiatry 2019, 57, 78–100. [Google Scholar] [CrossRef]
- Gerson, R.; Malas, N.; Feuer, V.; Silver, G.H.; Prasad, R.; Mroczkowski, M.M.; Pena-Nowak, M.; Gaveras, G.; Goepfert, E.; Hartselle, S.; et al. Best Practices for Evaluation and Treatment of Agitated Children and Adolescents (BETA) in the Emergency Department: Consensus Statement of the American Association for Emergency Psychiatry. WestJEM 21.2 March Issue 2019, 20, 409–418. [Google Scholar] [CrossRef]
- Janković, S.M.; Janković, S.V. Lessons learned from the discovery of sodium valproate and what has this meant to future drug discovery efforts? Expert Opin. Drug Discov. 2020, 15, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Yang, J.; Zhu, X. Combined effects of levetiracetam and sodium valproate on paediatric patients with epilepsy: a systematic review and meta-analysis. Seizure 2021, 95, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Nevitt, S.J.; Sudell, M.; Cividini, S.; Marson, A.G.; Smith, C.T. Antiepileptic drug monotherapy for epilepsy: a network meta-analysis of individual participant data. Emergencias 2022, 2022, CD011412. [Google Scholar] [CrossRef]
- Malamiri, R.A.; Ghaempanah, M.; Khosroshahi, N.; Nikkhah, A.; Bavarian, B.; Ashrafi, M.R. Efficacy and safety of intravenous sodium valproate versus phenobarbital in controlling convulsive status epilepticus and acute prolonged convulsive seizures in children: A randomised trial. Eur. J. Paediatr. Neurol. 2012, 16, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Bridle, C.; Palmer, S.; Bagnall, A.-M.; Darba, J.; Duffy, S.; Sculpher, M.; Riemsma, R. A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder. Heal. Technol. Assess. 2004, 8. [Google Scholar] [CrossRef]
- Yee, C.S.; Vázquez, G.H.; Hawken, E.R.; Biorac, A.B.; Tondo, L.M.; Baldessarini, R.J. Long-Term Treatment of Bipolar Disorder with Valproate: Updated Systematic Review and Meta-analyses. Harv. Rev. Psychiatry 2021, 29, 188–195. [Google Scholar] [CrossRef]
- Cipriani, A.; Reid, K.; Young, A.H.; Macritchie, K.; Geddes, J. Valproic acid, valproate and divalproex in the maintenance treatment of bipolar disorder. Emergencias 2013, 2013, CD003196. [Google Scholar] [CrossRef]
- Hellings, J.A.; Weckbaugh, M.; Nickel, E.J.; Cain, S.E.; Zarcone, J.R.; Reese, R.M.; Hall, S.; Ermer, D.J.; Tsai, L.Y.; Schroeder, S.R.; et al. ADouble-Blind, Placebo-Controlled Study of Valproate for Aggression in Youth with Pervasive Developmental Disorders. J. Child Adolesc. Psychopharmacol. 2005, 15, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Hollander, E.; Chaplin, W.; Soorya, L.; Wasserman, S.; Novotny, S.; Rusoff, J.; Feirsen, N.; Pepa, L.; Anagnostou, E. Divalproex Sodium vs Placebo for the Treatment of Irritability in Children and Adolescents with Autism Spectrum Disorders. Neuropsychopharmacology 2009, 35, 990–998. [Google Scholar] [CrossRef]
- Hollander, E.; Soorya, L.; Wasserman, S.; Esposito, K.; Chaplin, W.; Anagnostou, E. Divalproex sodium vs. placebo in the treatment of repetitive behaviours in autism spectrum disorder. Int. J. Neuropsychopharmacol. 2005, 9, 209–213. [Google Scholar] [CrossRef]
- Olivola, M.; Civardi, S.; Damiani, S.; Cipriani, N.; Silva, A.; Donadeo, A.; Politi, P.; Brondino, N. Effectiveness and safety of intravenous valproate in agitation: a systematic review. Psychopharmacol. 2021, 239, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Tripodi, B.; Matarese, I.; Carbone, M.G. A Critical Review of the Psychomotor Agitation Treatment in Youth. Life 2023, 13, 293. [Google Scholar] [CrossRef] [PubMed]
- J. Swanson, W. J. Swanson, W. Nolan e W. Pelham, «The SNAP rating scale for the diagnosis of attention deficit disorder,» in Meeting of the American Psychological Association, Los Angeles, 1981.
- M. Nobile, B. M. Nobile, B. Alberti e A. Zuddas, CRS-R. Conners’ Rating Scales. Revised. Manuale, Firenze: Giunti Editore, 2007.
- T. M. Achenbach, «The Child Behavior Checklist and related instruments,» The use of psychological testing for treatment planning and outcomes assessment, pp. 429-466, 1999.
- H. GaleRoid, L. J. H. GaleRoid, L. J. Miller, M. Pomplun e C. Koch, Leiter International Performance Scale – Third Edition, 2016.
- C. Lord, M. C. Lord, M. Rutter, P. C. DiLavore, S. Risi, R. J. Luyster, K. Gotham, S. L. Bishop e W. Guthrie, Autism Diagnostic Observation Schedule, Second Edition, Western Psychological Services, 2012.
- Kay, S.R.; Wolkenfeld, F.; Murrill, L.M. Profiles of Aggression among Psychiatric Patients. J. Nerv. Ment. Dis. 1988, 176, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Asadollahi, S.; Heidari, K.; Hatamabadi, H.; Vafaee, R.; Yunesian, S.; Azadbakht, A.; Mirmohseni, L. Efficacy and safety of valproic acid versus haloperidol in patients with acute agitation. Int. Clin. Psychopharmacol. 2015, 30, 142–150. [Google Scholar] [CrossRef]
- Gobbi, G.; Gaudreau, P.-O.M.; Leblanc, N.B. Efficacy of Topiramate, Valproate, and Their Combination on Aggression/Agitation Behavior in Patients With Psychosis. J. Clin. Psychopharmacol. 2006, 26, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Rosa, A.; Fountoulakis, K.; Siamouli, M.; Gonda, X.; Vieta, E. Is Anticonvulsant Treatment of Mania a Class Effect? Data from Randomized Clinical Trials. CNS Neurosci. Ther. 2009, 17, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Tseng, P.-T.; Chen, Y.-W.; Chung, W.; Tu, K.-Y.; Wang, H.-Y.; Wu, C.-K.; Lin, P.-Y. Significant Effect of Valproate Augmentation Therapy in Patients With Schizophrenia. Medicine 2016, 95, e2475–e2475. [Google Scholar] [CrossRef]
- Maina, G.; Albert, U.; Salvi, V.; Mancini, M.; Bogetto, F. Valproate or olanzapine add-on to lithium: An 8-week, randomized, open-label study in Italian patients with a manic relapse. J. Affect. Disord. 2007, 99, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.W.; Quarles, E.; Pharm. D., E.Q. Intravenous Valproate in Neuropsychiatry. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2000, 20, 88–92. [Google Scholar] [CrossRef]
- Soares-Weiser, K.; Vergel, Y.B.; Beynon, S.; Dunn, G.; Barbieri, M.; Duffy, S.; Geddes, J.; Gilbody, S.; Palmer, S.; Woolacott, N. A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder. Heal. Technol. Assess. 2007, 11. [Google Scholar] [CrossRef]
- Chengappa, K.; Chalasani, L.; Brar, J.S.; Parepally, H.; Houck, P.; Levine, J. Changes in body weight and body mass index among psychiatric patients receiving lithium, valproate, or topiramate: An open-label, nonrandomized chart review. Clin. Ther. 2002, 24, 1576–1584. [Google Scholar] [CrossRef] [PubMed]
- DeVane, C.L. Pharmacokinetics, drug interactions, and tolerability of valproate. . 2003, 25–42. [Google Scholar]
- Adamou, M.; Puchalska, S.; Plummer, W.; Hale, A.S. Valproate in the treatment of PTSD: systematic review and meta analysis. Curr. Med Res. Opin. 2007, 23, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, D.J.; Fontaine, G.V.; Smith, K.E.; Riker, R.R.; Miller, R.R.; Lerwick, P.A.; Lucas, F.; Dziodzio, J.T.; Sihler, K.C.; Fraser, G.L. Valproate for agitation in critically ill patients: A retrospective study. J. Crit. Care 2017, 37, 119–125. [Google Scholar] [CrossRef]
- Basan e, S. Leucht, «Valproate for schizophrenia,» The Cochrane database of systematic reviews, vol. 1; 2004; [CrossRef]
- Guay, D.R. The Emerging Role of Valproate in Bipolar Disorder and Other Psychiatric Disorders. Pharmacother. J. Hum. Pharmacol. Drug Ther. 1995, 15, 631–647. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, C.; Averna, R.; Labonia, M.P.; Riccioni, A.; Vicari, S. Intravenous Valproic Acid Add-On Therapy in Acute Agitation Adolescents With Suspected Substance Abuse: A Report of Six Cases. Clin. Neuropharmacol. 2018, 41, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Fontana, E.; Mandolini, G.; Delvecchio, G.; Bressi, C.; Soares, J.; Brambilla, P. Intravenous valproate in the treatment of acute manic episode in bipolar disorder: A review. J. Affect. Disord. 2020, 260, 738–743. [Google Scholar] [CrossRef]
- Yang, C.-S.; Zhang, L.-L.; Lin, Y.-Z.; Guo, Q. Sodium valproate for the treatment of Tourette׳s syndrome in children: A systematic review and meta-analysis. Psychiatry Res. 2015, 226, 411–417. [Google Scholar] [CrossRef]
- C. Schwarz, A. C. Schwarz, A. Volz, C. Li e S. Leucht, «Valproate for schizophrenia.,» The Cochrane database of systematic reviews, vol. 3; 2008; [CrossRef]
- Fenn, H.H.; Sommer, B.R.; A Ketter, T.; Alldredge, B. Safety and tolerability of mood-stabilising anticonvulsants in the elderly. Expert Opin. Drug Saf. 2006, 5, 401–416. [Google Scholar] [CrossRef]
- Sun, L.; Yagoda, S.; Yao, B.; Graham, C.; von Moltke, L. Combination of Olanzapine and Samidorphan Has No Clinically Significant Effect on the Pharmacokinetics of Lithium or Valproate. Clin. Drug Investig. 2019, 40, 55–64. [Google Scholar] [CrossRef]
- Müller-Oerlinghausen, B.; Retzow, A.; Henn, F.A.; Giedke, H.; Walden, J. Valproate as an Adjunct to Neuroleptic Medication for the Treatment of Acute Episodes of Mania: A Prospective, Randomized, Double-Blind, Placebo-Controlled, Multicenter Study. J. Clin. Psychopharmacol. 2000, 20, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Siriwardena, S.; McAllister, N.; Islam, S.; Craig, J.; Kinney, M. The emerging story of Sodium Valproate in British newspapers- A qualitative analysis of newspaper reporting. Seizure 2022, 101, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, J.A.; Koike, A.K.; Simmons, J.E.; Telles, S.; Eggleston, C. Adjunctive Valproic Acid for Delirium and/or Agitation on a Consultation-Liaison Service: A Report of Six Cases. J. Neuropsychiatry 2005, 17, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Hilty, D.M.; Rodriguez, G.D.; Hales, R.E. Intravenous Valproate for Rapid Stabilization of Agitation in Neuropsychiatric Disorders. J. Neuropsychiatry 1998, 10, 365–366. [Google Scholar] [CrossRef] [PubMed]
- Sher, Y.; Cramer, A.C.M.; Ament, A.; Lolak, S.; Maldonado, J.R. Valproic Acid for Treatment of Hyperactive or Mixed Delirium: Rationale and Literature Review. Psychosomatics 2015, 56, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xia, J.; Helfer, B.; Li, C.; Leucht, S. Valproate for schizophrenia. Emergencias 2016, 2016, CD004028. [Google Scholar] [CrossRef] [PubMed]
- Aman, M.G.; Singh, N.N.; Stewart, A.W.; Field, C.J. The aberrant behavior checklist: a behavior rating scale for the assessment of treatment effects. . 1985, 89, 485–91. [Google Scholar] [PubMed]
- W. O. Faustman e E. Overall J, «Brief Psychiatric Rating Scale,» The use of psychological testing for treatment planning and outcomes assessment, pp. 791-830, 1999.
- Bech, P. The Bech-Rafaelsen Mania Scale in Clinical Trials of Therapies for Bipolar Disorder. CNS Drugs 2002, 16, 47–63. [Google Scholar] [CrossRef] [PubMed]
- Jagadheesan, K.; Duggal, H.S.; Gupta, S.C.; Basu, S.; Ranjan, S.; Sandil, R.; Akhtar, S.; Nizamie, S.H. Acute Antimanic Efficacy and Safety of Intravenous Valproate Loading Therapy: An Open-Label Study. Neuropsychobiology 2003, 47, 90–93. [Google Scholar] [CrossRef]
- Teng, E.L.; Chui, H.C. The Modified Mini-Mental State (3MS) examination. . 1987, 48, 314–8. [Google Scholar]
- J. M. Silver e S. C. Yudofsky, «The Overt Ag- gression Scale: overview and guiding principles,» J Neuropsychiatry Clin Neu- rosci, 1991.
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study Selection Flowchart. PRISMA 2020 flow diagram for new systematic reviews which included searches of databases. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/.
Figure 1.
Study Selection Flowchart. PRISMA 2020 flow diagram for new systematic reviews which included searches of databases. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/.
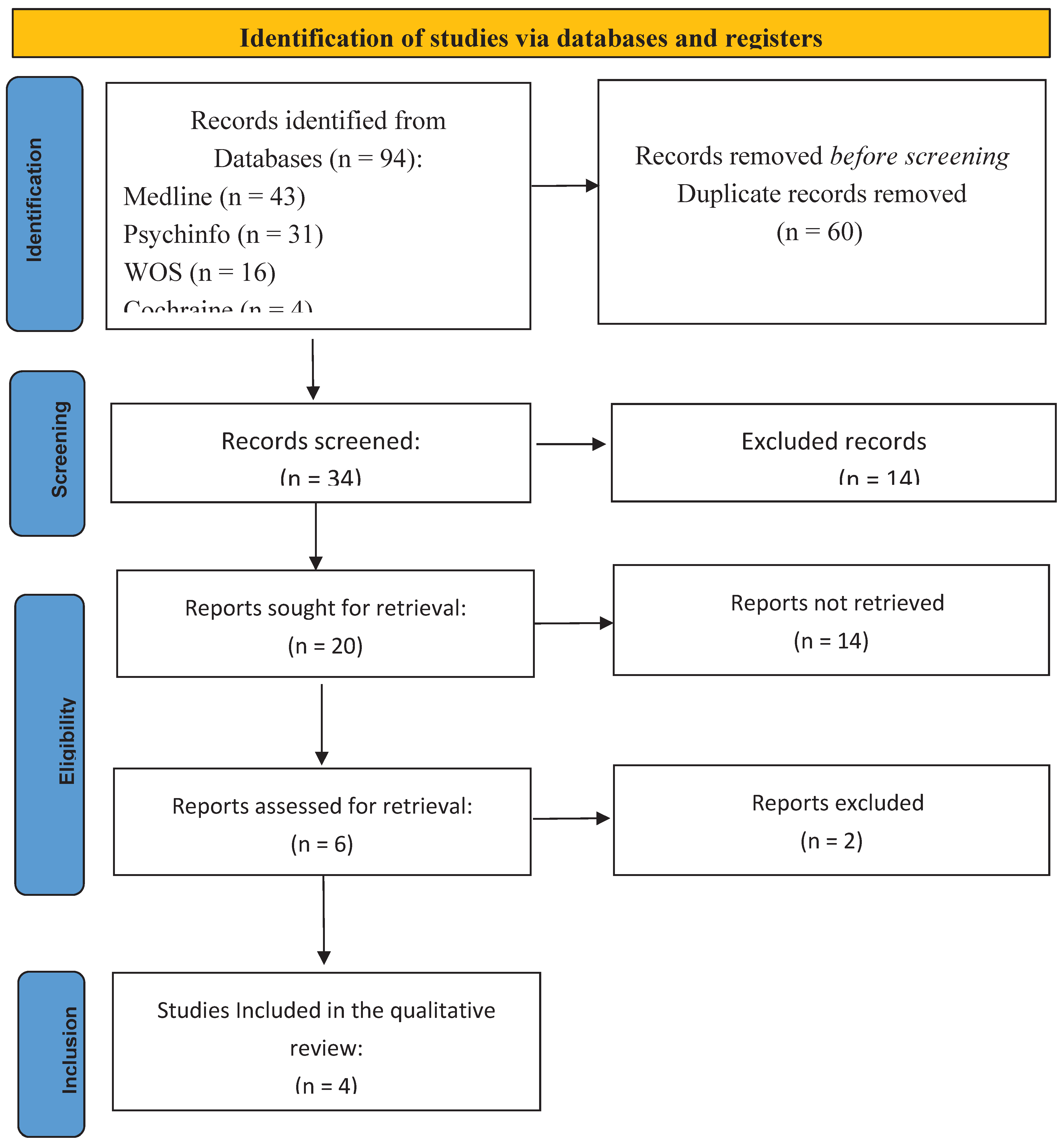
Figure 2.
Pharmacological treatment history of the clinical case.
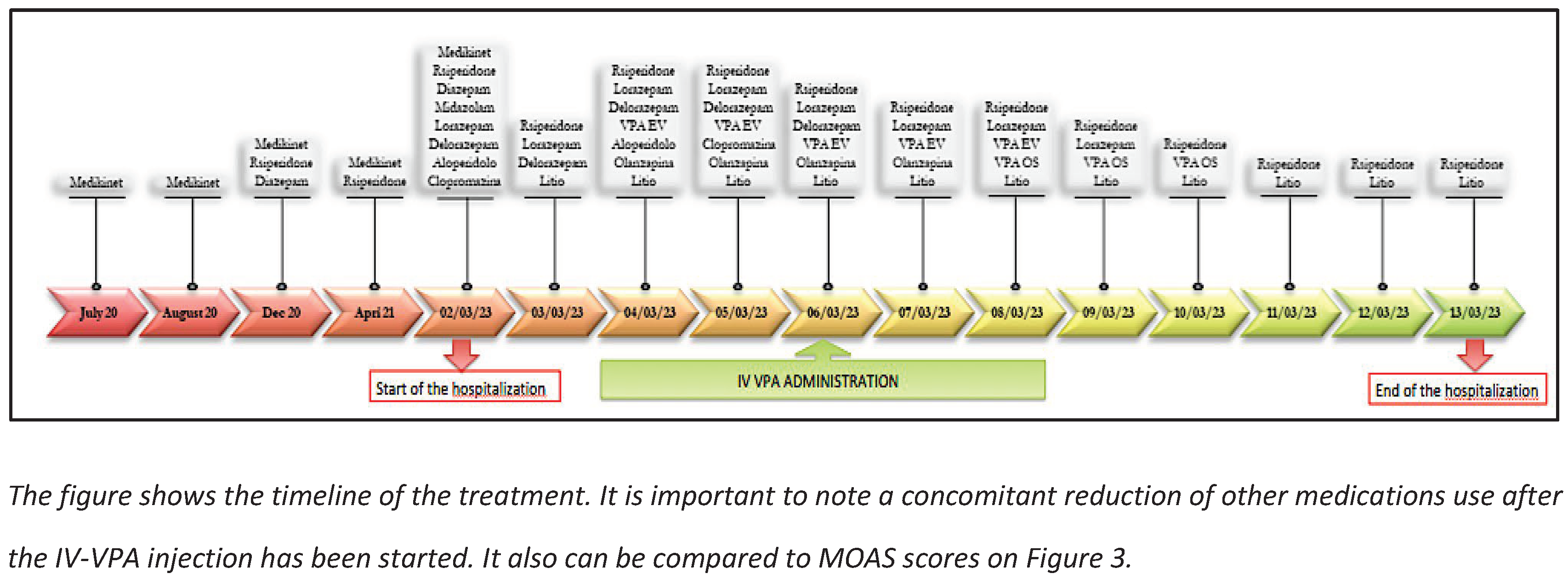
Figure 3.
MOAS aggressive behaviours scale.
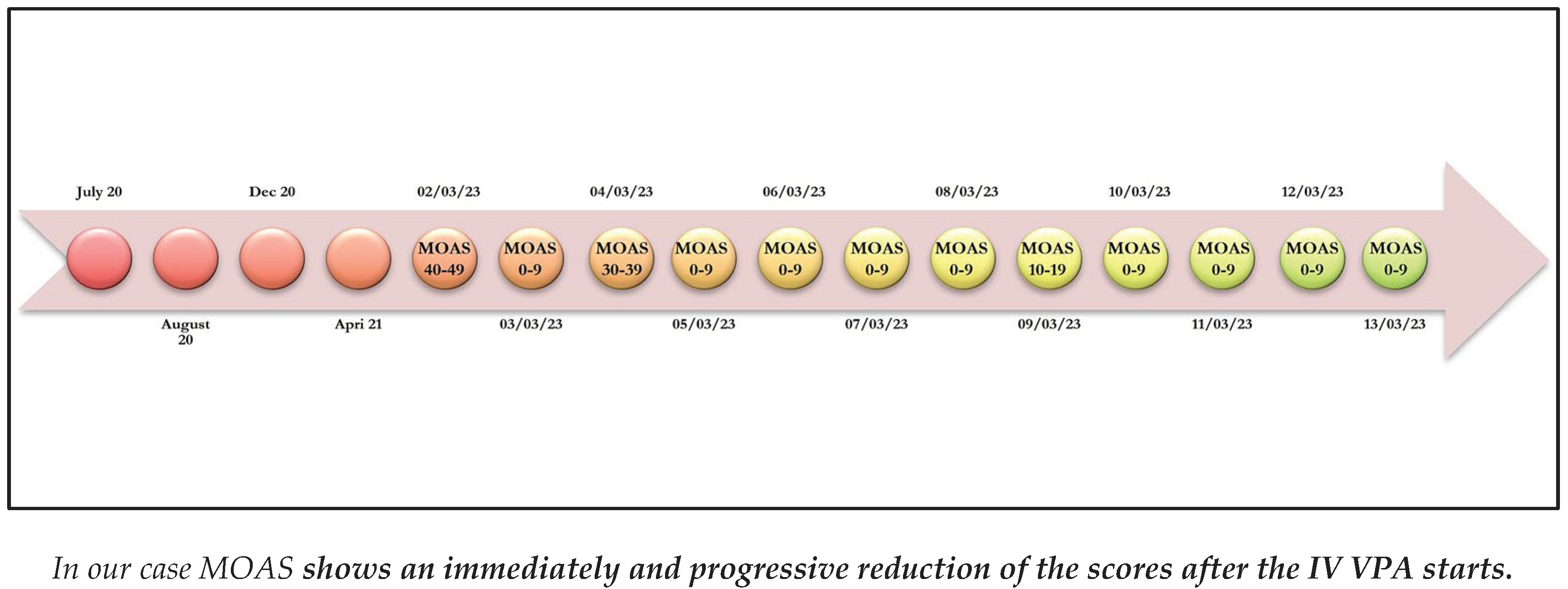

Table 1.
Blood and instrumental tests.
| Exams (blood levels) |
Range | 02/03/23 | 04/03/23 | 06/03/23 | 08/03/23 | 10/03/23 |
|---|---|---|---|---|---|---|
| Lithium |
0.6-1.2 mEq/L |
* | * | * | 0.35 | 0.53 |
| Ammonia |
19-54 μg/mL |
46 | * | 73 | 97 | 96 |
| VPA |
50-100 μg/mL |
* | * | 92.7 | 83.4 | 63.8 |
| PRL |
3.2-13.5 ng/mL |
* | 16.9 | * | 41.38 | 43.01 |
| AST |
<34 U/L |
58 | 42 | 32 | 27 | 27 |
| ALT |
10-49 U/L |
34 | 29 | 24 | 16 | 16 |
| LDH |
120-246 U/L |
433 | 401 | 367 | 280 | 277 |
| GGT |
<73 U/L |
18 | * | 19 | 17 | 18 |
| TBIL |
0.3-1.2 mg/dL |
0.7 | 0.5 | 0.5 | 0.6 | 0.4 |
| Cr |
0.6-1.1 mg/dL |
0.69 | 0.69 | 0.68 | 0.75 | 0.71 |
| ECG | Range | 02/03/23 | 04/03/23 | 06/03/23 | 08/03/23 | 10/03/23 |
| QTC | < 440 msec | 422 | 406 | 439 | 395 | 397 |
| LEGEND: * not evaluated; VPA= valproic acid; PRL= prolactin; AST= aspartate transaminase; ALT= alanine aminotransferase; LDH= lactate dehydrogenase; GGT= gamma-glutamyl transferase; TBIL= total bilirubine; Cr= creatinine; QTc= correct QT interval | ||||||
Table 2.
Screened articles on the use of VPA to treat acute agitation.
| Title | Author (s) | Study | Previous Diagnosis | Age | Administration |
|---|---|---|---|---|---|
| 1. Effectiveness and safety of intravenous valproate in agitation: a systematic review. | Olivola et al. (2022) [21] | SR | AD;ADHD; ASD; BD; CD; MD; MDD; ODD; PSY; PTSD; SA; Schizoph. | C; Ado; Adu | IV |
| 2. Efficacy and safety of valproic acid versus haloperidol in patients with acute agitation: results of a randomized, double-blind, parallel-group trial. | Asadollahi et al. (2015) [29] | RCT | AJ; MD; PSY | Adu | IV |
| 3. Efficacy of topiramate, valproate, and their combination on aggression/agitation behavior in patients with psychosis. | Gobbi G. et al. (2006) [30] | CCS | BD; SAD; Schizoph. | Adu | O |
| 4. Is anticonvulsant treatment of mania a class effect? Data from randomized clinical trials. | Rosa AR et al. (2011) [31] | SR | Mania | NA | O |
| 5. Significant Effect of Valproate Augmentation Therapy in Patients With Schizophrenia: A Meta-analysis Study. | Tseng PT et al. (2016) [32] | MA | SAD; Schizoph. | NA | O |
| 6. Valproate or olanzapine add-on to lithium: an 8-week, randomized, open-label study in Italian patients with a manic relapse. | Maina G et al. (2007) [33] | RCT | BD | Adu | O |
| 7. Intravenous valproate in neuropsychiatry | Norton JW & Quarles E. (2000) [34] | SR | BD; Mania | Adu | IV |
| 8. Lessons learned from the discovery of sodium valproate and what has this meant to future drug discovery efforts? | Janković SM & Janković SV. (2020) [11] | R | BD | C; Ado | O |
| 9. A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder. | Bridle C et al. (2004) [15] | R | BD | C; Ado; Adu | O |
| 10. Long-Term Treatment of Bipolar Disorder with Valproate: Updated Systematic Review and Meta-analyses. | Yee CS et al. (2021) [16] | R; MA | BD | Adu | O |
| 11. A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder. | Soares-Weiser K et al. (2007) [35] | SR | BD | Adu | O |
| 12. Changes in body weight and body mass index among psychiatric patients receiving lithium, valproate, or topiramate: an open-label, nonrandomized chart review | Chengappa KN et al. (2002) [36] | R | BD; SA; SAD; MDD; Schizoph. | NA | NA |
| 13. Pharmacokinetics, drug interactions, and tolerability of valproate. | DeVane CL (2003) [37] | R | BD | C; Ado; Adu | O |
| 14. Valproate in the treatment of PTSD: systematic review and meta analysis. | Adamou M et al. (2007) [38] | SR, MA | PTSD | Adu | O |
| 15. Valproate for agitation in critically ill patients: A retrospective study. | Gagnon DJ et al. (2017) [39] | RS | AD; ADHD; BD; MDD; PTSD | Adu | O |
| 16. Valproate as an adjunct to antipsychotics for schizophrenia: a systematic review of randomized trials. | Basan A et al. (2004) [40] | SR | SAD; Schizoph. | NA | O |
| 17. The emerging role of valproate in bipolar disorder and other psychiatric disorders. | Guay DR (1995) [41] | R | BD; SAD | C; Ado; Adu | O |
| 18. Intravenous Valproic Acid Add-On Therapy in Acute Agitation Adolescents With Suspected Substance Abuse: A Report of Six Cases. | Battaglia C et al. (2018) [42] | CR | CD; MD; ODD; PSY; SA | Ado | IV |
| 19. Intravenous valproate in the treatment of acute manic episode in bipolar disorder: A review. | Fontana E (2019) [43] | R | BD | C; Ado; Adu | IV |
| 20. Sodium valproate for the treatment of Tourette׳s syndrome in children: a systematic review and meta-analysis. | Yang CS et al. (2015) [44] | SR, MA | TS | C; Ado | O |
| 21. Valproate for schizophrenia. | Schwarz C et al. (2008) [45] | R | PSY; Schizoph. | Adu | O |
| 22. Safety and tolerability of mood-stabilising anticonvulsants in the elderly. | Fenn HH et al. (2006) [46] | R | MD | Adu | O |
| 23. Combination of Olanzapine and Samidorphan Has No Clinically Significant Effect on the Pharmacokinetics of Lithium or Valproate. | Sun L et al. (2019) [47] | CS | BD | Adu | O |
| 24. Valproic acid, valproate and divalproex in the maintenance treatment of bipolar disorder. | Cipriani A et al. (2013) [17] | R | BD | C; Ado; Adu | O |
| 25. Valproate as an adjunct to neuroleptic medication for the treatment of acute episodes of mania: a prospective, randomized, double-blind, placebo-controlled, multicenter study. European Valproate Mania Study Group. | Müller-Oerlinghausen B et al. (2000) [48] | CT | Mania | Adu | O |
| 26. The emerging story of Sodium Valproate in British newspapers- A qualitative analysis of newspaper reporting. | Siriwardena S et al. (2022) [49] | TA | SAD | C; Ado; Adu | NA |
| 27. Adjunctive valproic acid for delirium and/or agitation on a consultation-liaison service: a report of six cases | Bourgeois JA et al. (2005) [50] | CR | A, BD,PTSD, Schizoph. | Adu | IV |
| 28. Intravenous valproate for rapid stabilization of agitation in neuropsychiatric disorders | Hilty DM et al. (1998) [51] | CR | ASD | C | IV |
| 29. Valproic acid for treatment of hyperactive or mixed delirium: rationale and literature review | Sher Y et al. (2015) [52] | R | Delirium | Ado; Adu | IV |
| 30. A Critical Review of the Psychomotor Agitation Treatment in Youth | Tripodi B et al. (2023) [22] | R | AD;ADHD; ASD; BD; CD; MD; ODD; PSY; PTSD, SA | C; Ado; Adu | IV |
| 31. A double-blinde, placebo-controlled study of valproate for aggression in youth with pervasive developmental disorders | Hellings J.A. et al. (2005) [18] | RCT | ASD | C; Ado; Adu | O |
| 32. Divalproex sodium vs. placebo in the treatment of repetitive behaviours in autism spectrum disorder | Hollander E. et al. (2005) [20] | CT | ASD | C; Ado; Adu | O |
| 33. Divalproex sodium vs. placebo in the treatment of irritability in children and adolescent with autism spectrum disorder | Hollander E. et al. (2010) [19] | CT | ASD | C; Ado | O |
| 34. Valproate for schizophrenia (Review) | Wang J et al. (2016) [53] | R | SAD; Schizoph. | Adu | NA |
LEGEND: Study: CR= Case Report; CS=cohort study; CCS=case control study; CT=clinical trial; MA=meta-analysis; PS=comparative study; SR= systematic review; R=literature review; RCT=randomized clinical trial; TA= thematic analysis. Diagnosis: A=Agitation; AD=Anxiety Disorder; ADHD= Attention Deficit Hyperactive Disorder; AJ=Adjustment Disorder; ASD= Autism Spectrum Disorder; BD= Bipolar Disorder; CD= conduct disorder; MD= mood disorder; ODD= Oppositionale Defiant Disorder; Ot= Others; PSY=psycosis; SA=substance abuse; SAD= schizoaffective disorder; Schizoph=Schizophrenia; Age: C= children (<13 y); Ado=adolescent (13>Age<18); Adu= adult (>18y); NA=not specified. Administration: IV= Intravenous; O= Oral; NA=not specified.
Table 3.
Response to IV VPA in children and adolescents with acute aggressive agitation.
| Study | Study design | Diagnosis | Administration | Dosage/phases | Period of treatment | Concomitant medication | Outcomes | Response |
|---|---|---|---|---|---|---|---|---|
| 1. Intravenous Valproic Acid Add-On Therapy in Acute Agitation Adolescents With Suspected Substance Abuse: A Report of Six Cases. (Battaglia C et al. 2018) [42] | Case report | CD; MD; ODD; PSY; SA | IV | 1200-1800 mg/day | 5-17 days | SGAs MS BDZ |
MOAS BPRS |
1 |
| 2. Intravenous valproate in the treatment of acute manic episode in bipolar disorder: A review (Fontana E 2019) [43] | Review | BD | IV |
|
3 days 15 days |
|
BRMAS YMRS CGI-S MMSE |
1 |
| 3. Intravenous valproate for rapid stabilization of agitation in neuropsychiatric disorders ( Hilty DM et al. 1998) [51] | Case report | ASD | IV O |
Loading fase- 2000 mg/day(40 mg/kg) Maintenance dose 1000 mg/day |
10’ 6 months |
SGAs, ACH | OAS | 1 |
| 4. A Critical Review of the Psychomotor Agitation Treatment in Youth ( Tripodi B et al. 2023) [22] | Review | ASD; CD; MD; ODD; PSY; SA |
|
|
|
NA | / | 1 |
LEGEND: Diagnosis: AD=Anxiety Disorder; ADHD= Attention Deficit Hyperactive Disorder; ASD= Autism Spectrum Disorder; BD= Bipolar Disorder; CD= conduct disorder; MD= mood disorder; ODD= Oppositionale Defiant Disorder; PSY=psycosis SA=substance abuse; Schizophr.=Schizophrenia; Administration: IV= Intravenous; O= Oral; Concomitant medication: ACH= anticholinergic; BDZ= benzodiazepines ; FGAs= first generation antipsychotics ; MS= mood stabilizer; SGAs= second generation antipsychotics. Outcomes: ABC= Aberrant Behavior Checklist [54]; BPRS= Brief psychiatric rating scale [55]; BRMAS= Bech–Rafaelsen Mania Scale [56]; CGI= Clinical global impression [57]; CY-BOCS= Children’s Yale-Brown Obsessive Compulsive Scale [25]; MMSE= Mini mental state examination [58]; MOAS= Modified Overt Aggression Scale [28]; OAS= Overt Aggression Scale [59]; Results: 0= worst outcome; 1= better outcome; .X= no difference
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



