
Submitted:
25 March 2024
Posted:
26 March 2024
You are already at the latest version
Abstract
Circulating cell-free DNA (cfDNA) refers to small fragments of DNA molecules released after programmed cell death and necrosis in several body fluids such as blood, saliva, urine, and cerebrospinal fluid. The discovery of cfDNA has revolutionized the field of non-invasive diagnostics in the oncologic field, in prenatal testing, and in organ transplantation. Despite the potential of cfDNA and the solid results published in recent literature, several challenges remain, represented by low abundance, need for highly sensitive assays and analytical issues.
In this review, the main technical advances in cfDNA analysis are presented and discussed, with a comprehensive examination of the current available methodologies applied in each field.
Considering the potential advantages of cfDNA, this biomarker is increasing its consensus among clinicians, as it consents to monitor patients’ conditions in an easy and non-invasive way, offering a more personalized care. Nevertheless, cfDNA analysis is still considered a research marker to be further validated, and very few centers are implementing its analysis in the real-life assistance. As technical improvements are enhancing the performances of cfDNA analysis, its application will transversally improve patients’ quality of life.
Keywords:
cell-free DNA
; Next-generation Sequencing
; digital PCR
; liquid biopsy
; non-invasive diagnostics
1. Circulating Cell-Free DNA
Cell-free DNA (cfDNA) is represented by double-stranded extracellular DNA fragments released into the bloodstream after apoptosis and necrosis processes in physiological and pathological situations. It was first described in 1948 [1] when Mandel and Matais detected the presence of DNA in plasma samples from healthy and affected individuals. CfDNA originates from many sources within the body and can be isolated from various body effluents such as blood, urine, effusions, and cerebrospinal fluid [2]. In healthy conditions, it derives mainly from blood cells [3,4], but it can arise from inflammatory cells, tumor cells, fetal cells crossing the placenta during pregnancy, or can be released from graft cells after solid organ transplantation [5]. Human plasma DNA consists of a mixture of DNA fragments of different sizes, mostly ranging between 100 and 200 base pairs [6,7], with a peak at 166 bases; this peculiar length was related to the nucleosomal structure [8,9], as during cell death process, proteins associated with DNA seem to protect short fragments from degradation. However, smaller (<100 bases) or larger fragments of several kilobases have also been reported [10,11,12] and associated respectively to mitochondrial and necrotic origin [9,13]. CfDNA concentration in blood widely ranges between undetectable to high concentration (up to 100 ng/mL) in healthy subjects [9,13], but it is known that its levels can be affected by many individual conditions, as age, BMI, circadian rhythm [13], exercise [4], inflammation [5], infections [14,15,16], and pharmacologic treatment [5], that tend to increase cfDNA presence.
2. CfDNA Applications in Clinical Care
Since the discovery of cfDNA, its potential applications in various fields have been continuously explored. The application of cfDNA analysis, which is defined “liquid biopsy”, consents to monitor pathological conditions in oncologic, prenatal and transplantation fields in a non-invasive and revolutionary method [9].
2.1. Oncologic Applications
In oncology, the presence of the circulating tumor cfDNA (ctDNA) and the analysis of its genetic alterations allows the detection of cancer disease, the monitoring of treatment response, and the detection of minimal residual disease, enabling personalized treatment strategies [17,18]. Currently, the most common use of ctDNA analysis is therapy selection and stratification of patients based on the likelihood of response to targeted therapies [19,20,21,22] by searching for specific mutation markers for resistance or sensitivity, such as tyrosine kinase inhibitors, programmed death inhibitors-1 [23], programmed death ligand-1 [24], and cytotoxic T lymphocyte-associated protein 4 [25]. Through ctDNA analysis is, therefore, possible to differentiate and predict immune checkpoint blockade response patterns [26,27], characterize the tumor heterogeneity [28], and early detect resistance for targeted therapy and chemotherapy [29,30,31,32].
2.2. Prenatal Screening
In prenatal testing, the analysis of fetal cfDNA in maternal blood has revolutionized the field, allowing non-invasive prenatal testing (NIPT) that can investigate chromosomal abnormalities and fetal aneuploidies as an alternative to more invasive methods such as karyotyping and FISH on fetal blood, chorionic villus sampling, or amniocentesis [37]. Non-invasive prenatal screening can be performed from 5-7 weeks [38], looking for pathological variations with a targeted or genome-wide approach. In addition, it is possible to noninvasively determine fetal sex, genotype fetal blood group D antigen, and detect variants involved in paternally inherited or de novo disorders [39].
To date, a low fetal fraction is the most important cause of negative results in cfDNA screening and is reported as a cause of test failure in up to 6.1% of tests performed [40,41]. This poor cfDNA concentration may result from an increased maternal fraction due to the physiological condition of the mother [4,13].
2.3. Transplantation
Clinical studies have highlighted the potential of detecting and quantifying the fraction of donor-derived cell-free DNA (dd-cfDNA), i.e., the portion of cfDNA derived from the transplanted organ, to monitor transplant status and detect rejection earlier and with greater sensitivity than traditional methods, such as graft biopsy, allowing early intervention and improved transplantation outcomes [42,43,44]. Dd-cfDNA has been shown to be a potential biomarker of acute rejection, well correlating with biopsy-proven rejection, and more generally it is a signal of graft damage, post-transplant complications, and infection. Differences in the percentage of dd-cfDNA between graft types have been observed, reflecting the effective size and the organ-specific cell turnover [45], similar to results reported for ctDNA changes associated with tumor burden.
Dd-cfDNA is discriminated from recipient cfDNA by exploiting widespread genetic polymorphisms in the genome. The first published approaches to detect dd-cfDNA relied on a panel of short-tandem repeats (STRs), variable-number tandem repeats (VNTRs), single nucleotide (SNPs) or insertion-deletion polymorphisms (INDELs) chosen as polymorphic enough to distinguish all possible donor-recipient pairs, and therefore were defined as "targeted approaches" [46,47] as they target pre-selected sequences in the genome. A particular method to discriminate the portion of dd-cfDNA present in bloodstream is based on the donor and recipient Human Leukocyte Antigen (HLA) typing [48,49]. Since transplant centers generally check the HLA loci to identify the best match for transplantation, this information is therefore available and can be used to discriminate donor cfDNA from than of the recipient.
More recent NGS techniques do not require genotyping and are commonly called “random approaches” since after the sequencing phase, specific donor and recipient polymorphisms are selected based on the genomic profile of both subjects [50,51].
The identification of cfDNA tissue source may represent a valid alternative for graft versus host disease (GVHD) non-invasive detection. Acute GVHD remains an important complication after allogeneic hematopoietic cell transplantation (HCT) [52]. Currently, there are no validated non-invasive biomarkers that are used in routine clinical applications for acute GVHD. Candidate molecules were cytokines and peptides involved in the systemic inflammation and pathophysiology of GVHD, but their performance resulted limited and poorly specific [52]. As liver, skin and intestine are the most involved organ in the disease, a significant increase of cfDNA deriving from these tissues can be informative of the development of the pathology [53].
Each tissue is characterized by an epigenetic signature that consents the identification of the DNA origin through the analysis of its methylation profile [54]. Advanced molecular analysis as whole-genome bisulfite sequencing allow the correct identification and quantification of cfDNA source, consenting the non-invasive monitoring of GVHD [55]. This approach has been tested by Pellan Cheng and colleagues [56], who analyzed a pilot cohort of HCT recipients and the result of their proof-of-principle study showed the potential of cfDNA to assist in personalizing care after HCT.
3. Technical Issues for High-Quality cfDNA Analysis
3.1. The Relevance of Correct Sampling
Performing a liquid biopsy means in the practice the retrieving of cfDNA from a body fluid, mostly peripheral blood. However, the rapid turnover and short half-life of cfDNA [9,13] require proper sampling, considering the relative low concentration of this marker. Most studies were performed using EDTA BD vacutainer [57,58], which does not preserve blood cells from apoptosis and release of genomic DNA, affecting the quantity and quality of cfDNA itself [16,59] if plasma is not rapidly separated from the corpuscular part [13]. To prevent cfDNA degradation and its dilution into genomic DNA, ad hoc collection tubes are available from different companies (Qiagen, Germany, Roche, Switzerland, and Streck, USA), which were successfully used in some studies [60,61]. Their main advantage is that tubes keep cfDNA stable and free from genomic contamination for up to 14 days, improving the performance of the following research studies, drug discovery, and assay development.
3.2. Technical Comparison of cfDNA Analysis Methods
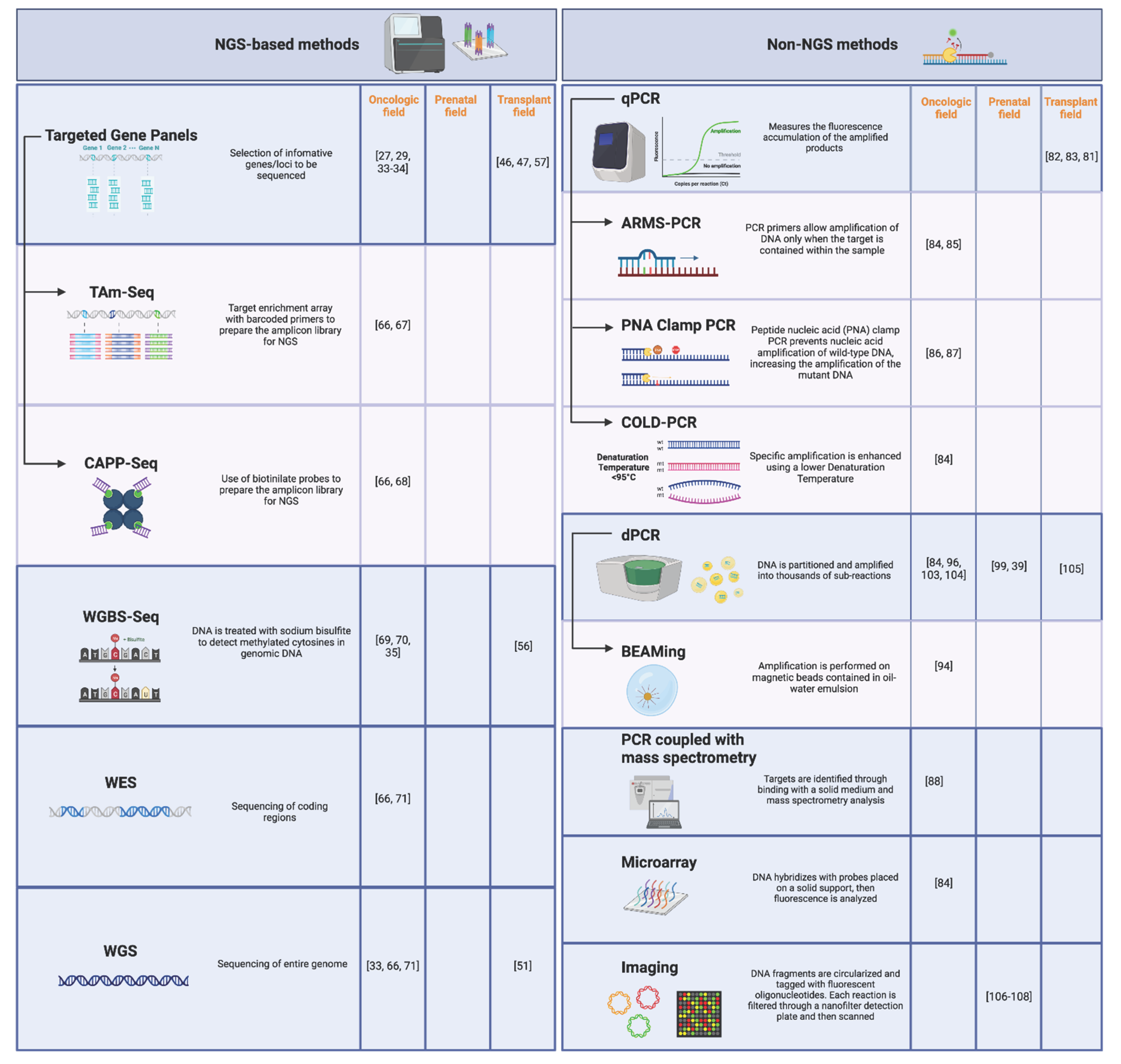
Advancements in technology, particularly the advent of quantitative PCR (qPCR) and next-generation sequencing (NGS), significantly enhanced the detection sensitivity and precision of cfDNA analysis. Methods for cfDNA analysis are generally divided in NGS and non-NGS approaches (Figure 1).
3.2.1. NGS-Based Methods
NGS-based approaches have the potential to simultaneously sequence thousands of targets. Considering the Illumina technology, its high accuracy and flexibility made it the most spread platform for cfDNA analysis compared to competitors, such as Ion Torrent, Oxford Nanopore, and Pacific Biosciences, which are still limited by their technical features that do not apply properly with short cfDNA fragments [62,63].
In NGS workflow, DNA samples are amplified targeting hundreds or thousands of single nucleotide polymorphisms (SNPs) [33,46,64,65] selected depending on the application field, then DNA fragments are tagged by adaptors and indexed before being sequenced with an elevated depth that consents sensitive results after bioinformatics analyses. Assay types can vary according to the aim of the analysis, moving from tagged-amplicon deep sequencing (TAm-Seq) if the target sequence has been previously characterized [66,67], to personalized profiling by deep sequencing, as CAPP-Seq applied in oncology [66,68], to whole genome bisulfite sequencing (WGBS-Seq) for DNA methylation analysis [69,70], and to whole exome (WES) or genome sequencing (WGS), that provide a comprehensive evaluation of tumor mutations, identifying potential oncogenes and tumor suppressor genes, deleterious alterations and variants of unknown significance [66,71]. However, WES and WGS are limited by low sensitivity, excessive time and cost, and difficulties in the interpretation of results [2].
For accurate detection of low-abundance targets, as in the case of liquid biopsy in which the fraction of target DNA within a cfDNA sample is potentially poorly represented, deep sequencing is necessary to provide the required sensitivity [72]. Recent improvements in sequencing instrumentation offer options with extremely high coverage depth for large portions of the entire genome in a single sample [73]. Although the cost of performing NGS has decreased considerably [74], this method can have a relatively consistent cost with a long turnaround time (often at least 3 days) and with variable sensitivity. Indeed, when assays are designed to cover several genetic targets, the comprehensive nature of NGS can provide value in efficiency and cost reduction, while NGS is more expensive and time-consuming when analyzing a small number of variants or samples [75]. Moreover, NGS does not always provide an absolute quantification of cfDNA meant as the total number of DNA copies [42,43,44,50,76,77,78,79,80].
3.2.2. Non-NGS Methods
Real-time or qPCR, microarrays and digital PCR (dPCR) are included in non-NGS methods and offer faster and less expensive detection option compared to NGS. These methods are generally used to detect and quantify the presence of known specific mutation or polymorphisms in cfDNA samples [14,81,82,83,84]. However, to enhance assay sensitivity, improved PCR approaches were developed. To identify single base changes or short deletion, amplification-refractory mutation system (ARMS-PCR) exploits sequence-specific PCR primers that allow amplification of DNA only when the target is contained within the sample, thus lowing the limit of detection in comparison with conventional PCR [84,85]. The same results can be obtained by peptide nucleic acid (PNA) clamp PCR, which prevent nucleic acid amplification of wild-type DNA, increasing the amplification of the mutant DNA [86,87]. Another alternative is the co-amplification at lower denaturation temperature-based PCR (COLD-PCR), which results in the enhancement of both known and unknown minority alleles during PCR, irrespective of mutation type and position. This method is based on exploitation of the critical temperature at which mutation-containing DNA is preferentially melted over wild type [84].
To increase the number of targets that can be examined simultaneously, PCR can be coupled with mass spectrometry. After amplification, PCR products are analyzed with mass spectrometry, searching for dozens of target mutations in a single reaction with great sensitivity [88].
Besides encouraging results, qPCR efficiency may be affected by variations in amplification. Furthermore, qPCR measures the fluorescence accumulation of the amplified product and requires normalization to a standard curve or to a reference, resulting in a relative quantification. The main difference between qPCR and dPCR is that, unlike conventional amplification, the reaction in dPCR is partitioned into thousands of sub-reactions, allowing absolute quantitation and high sensitivity. DPCR was first described in 1992 by Sykes et al., who changed standard amplification with the integration of limiting dilution, end-point PCR, and Poisson statistics [89]. While partitioning the samples in thousands of independent amplification reactions, dPCR reach higher accuracy and an absolute quantification of the target, which is determined by Poisson statistics. The evolution of Sykes method was achieved by Vogelstein and Kinzler who added the detection of the target through fluorescent probes to the partitioning of the sample [90]. Current dPCR technology uses reagents and workflows similar to those used for most standard TaqMan probe-based assays with a smaller sample requirement, reducing cost and preserving precious samples. The methods described by Sykes, Vogelstein and Kinzler have been improved and are commercially available as different platform. dPCR amplification can be performed on a microfluidic chip [91], microarrays [92] or spinning microfluidic discs [93], or can be based on oil-water emulsions [94]. Moreover, dPCR technology enables high-throughput analysis with reduced cost compared with other methods while maintaining great sensitivity and accuracy. Moreover, because cfDNA is poorly concentrated in plasma, repeated testing on different sample aliquots may not be possible. DPCR can overcome this limit, since it consents accurate detection and quantitation without separate calibration reactions [95], resulting in a reagent and sample saving. Compared with commercial qPCR assays [77], dPCR assays achieve a better limit of detection as well as a more accurate result.
However, dPCR shows practical drawbacks. The number of targets that can be detected is significantly lower compared to NGS-based methods due to the possibility to multiplex from 2 to a maximum of 6 fluorophores using the most innovative instruments. Moreover, limitations in droplet-to-droplet volume uniformity can influence quantification accuracy and reproducibility, but fluidics-based dPCR may offer an opportunity to overcome this limitation [96,97]. Then, PCR efficiency can vary due to different amplicon lengths [98], as longer amplicons are amplified less efficiently, which might result in underestimation of the true cfDNA value [99]. Similarly, Dauber et al. demonstrated that cfDNA concentration was 5 times higher when using smaller amplicons compared with larger amplicons [81]. Therefore, the use of short amplicon is recommended for the accurate quantification of cfDNA to avoid underestimation of the target.
NGS and dPCR techniques demonstrated to consents similar results in different application fields. The comparison on kidney transplant recipient samples highlighted no significant differences in the detection of cfDNA, with a significant association between the measurements obtained with both methods [100]. Moreover, lower limits of quantification were similar and in line with what is already reported in literature [101], even though NGS method resulted more sensitive in the lower range than the dPCR method [100]. The quantification of mixed chimerism after hematopoietic stem cell transplantation appeared to be feasible with both methodologies conserving high performances in terms of sensitivity, reproducibility, and linearity [102]. Conversely, dPCR better performed in the detection of KRAS mutation in the oncologic field, with high sensitivity and specificity [103], and a limit of quantification 10-fold lower compared to NGS [104].
A great advantage of dPCR is the possibility to obtain the absolute concentration of the target, expressed as copies/µL or copies/mL, which is not influenced by fluctuations in the background cfDNA, derived from the patient. Indeed, NGS results can be expressed only in a cfDNA percentage that can be biased and underestimated as a consequence of physiological or pathological conditions of the subject (e.g., concomitant infections, BMI, exercise, etc.) [4,5,13,14,15,16]. The use of cfDNA as a concentration has also been shown to be superior to the ratio as a biomarker for allograft rejection [105].
In contrast with amplification-based method, an imaging single DNA molecules method for high precision cfDNA detection was developed. In VANADIS assay (PerkinElmer, Waltham, MA), DNA fragments are labeled with fluorescent oligonucleotides specific for precise genetic targets, then circularized and copied multiple times before being placed on a 96-well nanofilter microplate and analyzed by imaging [106]. This assay is now applied to prenatal screening with high accuracy [107,108]. Since this method does not require DNA amplification and sequencing, is easily implemented in any laboratory, scalable and fully automated.
4. Conclusions
Given the potential applications of cfDNA, this biomarker is increasing the general agreement among clinicians in oncology, prenatal and transplantation fields. Despite the encouraging results, however, the cfDNA analysis is not a reality as it is exploited in a relatively small number of centers, and it is still considered a research marker to be further validated.
Novel and more powerful technologies are improving the sensitivity and the performances of cfDNA analysis, making its application easy, feasible and attracting. NGS and dPCR, which are the main players in liquid biopsy, serve distinct purposes. NGS is a powerful tool for large-scale sequencing and genomics studies, while dPCR excels in quantifying specific cfDNA targets with exceptional precision and sensitivity. Considering the costs, NGS can be cost-effective for high-throughput sequencing projects but may be expensive for small-scale studies, while dPCR is generally more cost-effective for targeted, low-throughput applications. Therefore, the choice between these techniques should be based on the specific research goals and the scale of the project.
In conclusion, the introduction of liquid biopsy offers new insights into disease detection and treatment response monitoring in the evolving field of precision medicine. In the future, cfDNA could be applied transversely to achieve a more personalized medicine, improving patients’ quality of life.
Author Contributions
All authors contributed to this work. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Italian Ministry of Education-University and Research-MIUR, Progetto Strategico di Eccellenza Dipartimentale #D15D18000410001.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mandel, P.; Metais, P. Nuclear Acids In Human Blood Plasma. C R Seances Soc Biol Fil. 1948, 142, 241–243. [Google Scholar] [PubMed]
- Nikanjam M, Kato S, Kurzrock R. Liquid biopsy: current technology and clinical applications. J Hematol OncolJ Hematol Oncol. 2022;15(1):131. [CrossRef]
- Lo YMD, Han DSC, Jiang P, Chiu RWK. Epigenetics, fragmentomics, and topology of cell-free DNA in liquid biopsies. Science. 2021;372(6538):eaaw3616. [CrossRef]
- Tug, S.; Helmig, S.; Deichmann, E.R. Exercise-induced increases in cell free DNA in human plasma originate predominantly from cells of the haematopoietic lineage. Exerc Immunol Rev. 2015, 21, 164–173. [Google Scholar] [PubMed]
- Aucamp J, Bronkhorst AJ, Badenhorst CPS, Pretorius PJ. The diverse origins of circulating cell-free DNA in the human body: a critical re-evaluation of the literature: The diverse origins of circulating cell-free DNA. Biol Rev. 2018;93(3):1649-1683. [CrossRef]
- Grabuschnig S, Bronkhorst AJ, Holdenrieder S, et al. Putative Origins of Cell-Free DNA in Humans: A Review of Active and Passive Nucleic Acid Release Mechanisms. Int J Mol Sci. 2020;21(21):8062. [CrossRef]
- McCoubrey-Hoyer A, Okarma TB, Holman HR. Partial purification and characterization of plasma DNA and its relation to disease activity in systemic lupus erythematosus. Am J Med. 1984;77(1):23-34. [CrossRef]
- Lo YMD, Chan KCA, Sun H, et al. Maternal plasma DNA sequencing reveals the genome-wide genetic and mutational profile of the fetus. Sci Transl Med. 2010;2(61):61ra91. [CrossRef]
- Kustanovich A, Schwartz R, Peretz T, Grinshpun A. Life and death of circulating cell-free DNA. Cancer Biol Ther. 2019;20(8):1057-1067. [CrossRef]
- Rumore PM, Steinman CR. Endogenous circulating DNA in systemic lupus erythematosus. Occurrence as multimeric complexes bound to histone. J Clin Invest. 1990;86(1):69-74. [CrossRef]
- Giacona MB, Ruben GC, Iczkowski KA, Roos TB, Porter DM, Sorenson GD. Cell-free DNA in human blood plasma: length measurements in patients with pancreatic cancer and healthy controls. Pancreas. 1998;17(1):89-97. [CrossRef]
- Thierry AR, El Messaoudi S, Gahan PB, Anker P, Stroun M. Origins, structures, and functions of circulating DNA in oncology. Cancer Metastasis Rev. 2016;35(3):347-376. [CrossRef]
- Edwards RL, Menteer J, Lestz RM, Baxter-Lowe LA. Cell-free DNA as a solid-organ transplant biomarker: technologies and approaches. Biomark Med. 2022;16(5):401-415. [CrossRef]
- Moreira VG, Prieto B, Rodríguez JSM, Alvarez FV. Usefulness of cell-free plasma DNA, procalcitonin and C-reactive protein as markers of infection in febrile patients. Ann Clin Biochem. 2010;47(Pt 3):253-258. [CrossRef]
- Burnham P, Dadhania D, Heyang M, et al. Urinary cell-free DNA is a versatile analyte for monitoring infections of the urinary tract. Nat Commun. 2018;9(1):2412. [CrossRef]
- Siljan WW, Holter JC, Nymo SH, et al. Circulating cell-free DNA is elevated in community-acquired bacterial pneumonia and predicts short-term outcome. J Infect. 2016;73(4):383-386. [CrossRef]
- Cisneros-Villanueva M, Hidalgo-Pérez L, Rios-Romero M, et al. Cell-free DNA analysis in current cancer clinical trials: a review. Br J Cancer. 2022;126(3):391-400. [CrossRef]
- O’Sullivan HM, Feber A, Popat S. Minimal Residual Disease Monitoring in Radically Treated Non-Small Cell Lung Cancer: Challenges and Future Directions. OncoTargets Ther. 2023;16:249-259. [CrossRef]
- Spigel DR, Ervin TJ, Ramlau R, et al. Final efficacy results from OAM4558g, a randomized phase II study evaluating MetMAb or placebo in combination with erlotinib in advanced NSCLC. J Clin Oncol. 2011;29(15_suppl):7505-7505. [CrossRef]
- Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12(8):735-742. [CrossRef]
- Gatzemeier U, Pluzanska A, Szczesna A, et al. Results of a phase III trial of erlotinib (OSI-774) combined with cisplatin and gemcitabine (GC) chemotherapy in advanced non-small cell lung cancer (NSCLC). J Clin Oncol. 2004;22(14_suppl):7010-7010. [CrossRef]
- Oxnard GR, Thress KS, Alden RS, et al. Association Between Plasma Genotyping and Outcomes of Treatment With Osimertinib (AZD9291) in Advanced Non–Small-Cell Lung Cancer. J Clin Oncol. 2016;34(28):3375-3382. [CrossRef]
- Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N Engl J Med. 2018;379(21):2040-2051. [CrossRef]
- Fabrizio D, Lieber D, Malboeuf C, et al. Abstract 5706: A blood-based next-generation sequencing assay to determine tumor mutational burden (bTMB) is associated with benefit to an anti-PD-L1 inhibitor, atezolizumab. Cancer Res. 2018;78:5706-5706. [CrossRef]
- Hellmann MD, Nathanson T, Rizvi H, et al. Genomic Features of Response to Combination Immunotherapy in Patients with Advanced Non-Small-Cell Lung Cancer. Cancer Cell. 2018;33(5):843-852.e4. [CrossRef]
- Kato S, Li B, Adashek JJ, et al. Serial changes in liquid biopsy-derived variant allele frequency predict immune checkpoint inhibitor responsiveness in the pan-cancer setting. Oncoimmunology. 2022;11(1):2052410. [CrossRef]
- Zhang Q, Luo J, Wu S, et al. Prognostic and Predictive Impact of Circulating Tumor DNA in Patients with Advanced Cancers Treated with Immune Checkpoint Blockade. Cancer Discov. 2020;10(12):1842-1853. [CrossRef]
- Bardelli A, Pantel K. Liquid Biopsies, What We Do Not Know (Yet). Cancer Cell. 2017;31(2):172-179. [CrossRef]
- Tie J, Kinde I, Wang Y, et al. Circulating tumor DNA as an early marker of therapeutic response in patients with metastatic colorectal cancer. Ann Oncol Off J Eur Soc Med Oncol. 2015;26(8):1715-1722. [CrossRef]
- Magbanua MJM, Swigart LB, Wu HT, et al. Circulating tumor DNA in neoadjuvant-treated breast cancer reflects response and survival. Ann Oncol Off J Eur Soc Med Oncol. 2021;32(2):229-239. [CrossRef]
- Cao H, Liu X, Chen Y, et al. Circulating Tumor DNA Is Capable of Monitoring the Therapeutic Response and Resistance in Advanced Colorectal Cancer Patients Undergoing Combined Target and Chemotherapy. Front Oncol. 2020;10:466. [CrossRef]
- Ma F, Zhu W, Guan Y, et al. ctDNA dynamics: a novel indicator to track resistance in metastatic breast cancer treated with anti-HER2 therapy. Oncotarget. 2016;7(40):66020-66031. [CrossRef]
- Dawson SJ, Tsui DWY, Murtaza M, et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N Engl J Med. 2013;368(13):1199-1209. [CrossRef]
- Gandara DR, Paul SM, Kowanetz M, et al. Blood-based tumor mutational burden as a predictor of clinical benefit in non-small-cell lung cancer patients treated with atezolizumab. Nat Med. 2018;24(9):1441-1448. [CrossRef]
- Lehmann-Werman R, Neiman D, Zemmour H, et al. Identification of tissue-specific cell death using methylation patterns of circulating DNA. Proc Natl Acad Sci U S A. 2016;113(13):E1826-1834. [CrossRef]
- Jamshidi A, Liu MC, Klein EA, et al. Evaluation of cell-free DNA approaches for multi-cancer early detection. Cancer Cell. 2022;40(12):1537-1549.e12. [CrossRef]
- Rather RA, Saha SC. Reappraisal of evolving methods in non-invasive prenatal screening: Discovery, biology and clinical utility. Heliyon. 2023;9(3):e13923. [CrossRef]
- Wright CF, Burton H. The use of cell-free fetal nucleic acids in maternal blood for non-invasive prenatal diagnosis. Hum Reprod Update. 2009;15(1):139-151. [CrossRef]
- Nectoux J. Current, Emerging, and Future Applications of Digital PCR in Non-Invasive Prenatal Diagnosis. Mol Diagn Ther. 2018;22(2):139-148. [CrossRef]
- Hui L, Bianchi DW. Fetal fraction and noninvasive prenatal testing: What clinicians need to know. Prenat Diagn. 2020;40(2):155-163. [CrossRef]
- Gil MM, Accurti V, Santacruz B, Plana MN, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: updated meta-analysis. Ultrasound Obstet Gynecol Off J Int Soc Ultrasound Obstet Gynecol. 2017;50(3):302-314. [CrossRef]
- De Vlaminck I, Valantine HA, Snyder TM, et al. Circulating cell-free DNA enables noninvasive diagnosis of heart transplant rejection. Sci Transl Med. 2014;6(241):241ra77. [CrossRef]
- De Vlaminck I, Martin L, Kertesz M, et al. Noninvasive monitoring of infection and rejection after lung transplantation. Proc Natl Acad Sci U S A. 2015;112(43):13336-13341. [CrossRef]
- Gielis EM, Ledeganck KJ, Dendooven A, et al. The use of plasma donor-derived, cell-free DNA to monitor acute rejection after kidney transplantation. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc - Eur Ren Assoc. 2020;35(4):714-721. [CrossRef]
- Oellerich M, Budde K, Osmanodja B, et al. Donor-derived cell-free DNA as a diagnostic tool in transplantation. Front Genet. 2022;13:1031894. [CrossRef]
- Grskovic M, Hiller DJ, Eubank LA, et al. Validation of a Clinical-Grade Assay to Measure Donor-Derived Cell-Free DNA in Solid Organ Transplant Recipients. J Mol Diagn JMD. 2016;18(6):890-902. [CrossRef]
- Sigdel TK, Archila FA, Constantin T, et al. Optimizing Detection of Kidney Transplant Injury by Assessment of Donor-Derived Cell-Free DNA via Massively Multiplex PCR. J Clin Med. 2018;8(1):19. [CrossRef]
- Sorbini M, Togliatto GM, Simonato E, et al. HLA-DRB1 mismatch-based identification of donor-derived cell free DNA (dd-cfDNA) as a marker of rejection in heart transplant recipients: A single-institution pilot study. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. 2021;40(8):794-804. [CrossRef]
- Sorbini M, Togliatto G, Mioli F, et al. Validation of a Simple, Rapid, and Cost-Effective Method for Acute Rejection Monitoring in Lung Transplant Recipients. Transpl Int Off J Eur Soc Organ Transplant. 2022;35:10546. [CrossRef]
- Snyder TM, Khush KK, Valantine HA, Quake SR. Universal noninvasive detection of solid organ transplant rejection. Proc Natl Acad Sci U S A. 2011;108(15):6229-6234. [CrossRef]
- Sharon E, Shi H, Kharbanda S, et al. Quantification of transplant-derived circulating cell-free DNA in absence of a donor genotype. PLoS Comput Biol. 2017;13(8):e1005629. [CrossRef]
- Chen YB, Cutler CS. Biomarkers for acute GVHD: can we predict the unpredictable? Bone Marrow Transplant. 2013;48(6):755-760. [CrossRef]
- Waterhouse M, Pennisi S, Pfeifer D, et al. Colon and liver tissue damage detection using methylated SESN3 and PTK2B genes in circulating cell-free DNA in patients with acute graft-versus-host disease. Bone Marrow Transplant. 2021;56(2):327-333. [CrossRef]
- Moss J, Magenheim J, Neiman D, et al. Comprehensive human cell-type methylation atlas reveals origins of circulating cell-free DNA in health and disease. Nat Commun. 2018;9(1):5068. [CrossRef]
- Sun K, Jiang P, Chan KCA, et al. Plasma DNA tissue mapping by genome-wide methylation sequencing for noninvasive prenatal, cancer, and transplantation assessments. Proc Natl Acad Sci. 2015;112(40):E5503-E5512. [CrossRef]
- Cheng AP, Cheng MP, Loy CJ, et al. Cell-free DNA profiling informs all major complications of hematopoietic cell transplantation. Proc Natl Acad Sci. 2022;119(4):e2113476118. [CrossRef]
- Levitsky J, Kandpal M, Guo K, Kleiboeker S, Sinha R, Abecassis M. Donor-derived cell-free DNA levels predict graft injury in liver transplant recipients. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg. 2022;22(2):532-540. [CrossRef]
- Verhoeven JGHP, Boer K, Peeters AMA, et al. A Novel High-throughput Droplet Digital PCR-based Indel Quantification Method for the Detection of Circulating Donor-derived Cell-free DNA After Kidney Transplantation. Transplantation. 2022;106(9):1777-1786. [CrossRef]
- Norton SE, Lechner JM, Williams T, Fernando MR. A stabilizing reagent prevents cell-free DNA contamination by cellular DNA in plasma during blood sample storage and shipping as determined by digital PCR. Clin Biochem. 2013;46(15):1561-1565. [CrossRef]
- Knüttgen F, Beck J, Dittrich M, et al. Graft-derived Cell-free DNA as a Noninvasive Biomarker of Cardiac Allograft Rejection: A Cohort Study on Clinical Validity and Confounding Factors. Transplantation. 2022;106(3):615-622. [CrossRef]
- Clausen FB, Jørgensen KMCL, Wardil LW, Nielsen LK, Krog GR. Droplet digital PCR-based testing for donor-derived cell-free DNA in transplanted patients as noninvasive marker of allograft health: Methodological aspects. PloS One. 2023;18(2):e0282332. [CrossRef]
- Laver T, Harrison J, O’Neill PA, et al. Assessing the performance of the Oxford Nanopore Technologies MinION. Biomol Detect Quantif. 2015;3:1-8. [CrossRef]
- Carneiro MO, Russ C, Ross MG, Gabriel SB, Nusbaum C, DePristo MA. Pacific biosciences sequencing technology for genotyping and variation discovery in human data. BMC Genomics. 2012;13(1):375. [CrossRef]
- Halloran PF, Reeve J, Madill-Thomsen KS, et al. Antibody-mediated Rejection Without Detectable Donor-specific Antibody Releases Donor-derived Cell-free DNA: Results From the Trifecta Study. Transplantation. 2023;107(3):709-719. [CrossRef]
- Bettegowda C, Sausen M, Leary RJ, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med. 2014;6(224):224ra24. [CrossRef]
- Li H, Jing C, Wu J, et al. Circulating tumor DNA detection: A potential tool for colorectal cancer management. Oncol Lett. 2019;17(2):1409-1416. [CrossRef]
- Forshew T, Murtaza M, Parkinson C, et al. Noninvasive identification and monitoring of cancer mutations by targeted deep sequencing of plasma DNA. Sci Transl Med. 2012;4(136):136ra68. [CrossRef]
- Newman AM, Bratman SV, To J, et al. An ultrasensitive method for quantitating circulating tumor DNA with broad patient coverage. Nat Med. 2014;20(5):548-554. [CrossRef]
- Wardenaar R, Liu H, Colot V, Colomé-Tatché M, Johannes F. Evaluation of MeDIP-chip in the context of whole-genome bisulfite sequencing (WGBS-seq) in Arabidopsis. Methods Mol Biol Clifton NJ. 2013;1067:203-224. [CrossRef]
- Hon GC, Hawkins RD, Caballero OL, et al. Global DNA hypomethylation coupled to repressive chromatin domain formation and gene silencing in breast cancer. Genome Res. 2012;22(2):246-258. [CrossRef]
- Imperial R, Nazer M, Ahmed Z, et al. Matched Whole-Genome Sequencing (WGS) and Whole-Exome Sequencing (WES) of Tumor Tissue with Circulating Tumor DNA (ctDNA) Analysis: Complementary Modalities in Clinical Practice. Cancers. 2019;11(9):1399. [CrossRef]
- Lin C, Liu X, Zheng B, Ke R, Tzeng CM. Liquid Biopsy, ctDNA Diagnosis through NGS. Life Basel Switz. 2021;11(9):890. [CrossRef]
- Reuter JA, Spacek DV, Snyder MP. High-throughput sequencing technologies. Mol Cell. 2015;58(4):586-597. [CrossRef]
- Levy SE, Boone BE. Next-Generation Sequencing Strategies. Cold Spring Harb Perspect Med. 2019;9(7):a025791. [CrossRef]
- Schwarz UI, Gulilat M, Kim RB. The Role of Next-Generation Sequencing in Pharmacogenetics and Pharmacogenomics. Cold Spring Harb Perspect Med. 2019;9(2):a033027. [CrossRef]
- Dengu F. Next-generation sequencing methods to detect donor-derived cell-free DNA after transplantation. Transplant Rev. 2020;34(3):100542. [CrossRef]
- Zhao Y, Xia Q, Yin Y, Wang Z. Comparison of Droplet Digital PCR and Quantitative PCR Assays for Quantitative Detection of Xanthomonas citri Subsp. citri. PloS One. 2016;11(7):e0159004. [CrossRef]
- Feingold B, Rose-Felker K, West SC, et al. Early findings after integration of donor-derived cell-free DNA into clinical care following pediatric heart transplantation. Pediatr Transplant. 2022;26(1):e14124. [CrossRef]
- Amadio JM, Rodenas-Alesina E, Superina S, et al. Sparing the Prod: Providing an Alternative to Endomyocardial Biopsies With Noninvasive Surveillance After Heart Transplantation During COVID-19. CJC Open. 2022;4(5):479-487. [CrossRef]
- Kamath M, Shekhtman G, Grogan T, et al. Variability in Donor-Derived Cell-Free DNA Scores to Predict Mortality in Heart Transplant Recipients – A Proof-of-Concept Study. Front Immunol. 2022;13. Accessed May 24, 2023. https://www.frontiersin.org/articles/10.3389/fimmu.2022.825108.
- Dauber EM, Kollmann D, Kozakowski N, et al. Quantitative PCR of INDELs to measure donor-derived cell-free DNA-a potential method to detect acute rejection in kidney transplantation: a pilot study. Transpl Int Off J Eur Soc Organ Transplant. 2020;33(3):298-309. [CrossRef]
- García-Fernández N, Macher HC, Suárez-Artacho G, et al. Donor-Specific Cell-Free DNA qPCR Quantification as a Noninvasive Accurate Biomarker for Early Rejection Detection in Liver Transplantation. J Clin Med. 2022;12(1):36. [CrossRef]
- Fernández-Galán E, Badenas C, Fondevila C, et al. Monitoring of Donor-Derived Cell-Free DNA by Short Tandem Repeats: Concentration of Total Cell-Free DNA and Fragment Size for Acute Rejection Risk Assessment in Liver Transplantation. Liver Transplant Off Publ Am Assoc Study Liver Dis Int Liver Transplant Soc. 2022;28(2):257-268. [CrossRef]
- Galbiati S, Damin F, Burgio V, et al. Evaluation of three advanced methodologies, COLD-PCR, microarray and ddPCR, for identifying the mutational status by liquid biopsies in metastatic colorectal cancer patients. Clin Chim Acta. 2019;489:136-143. [CrossRef]
- Zhang X, Chang N, Yang G, et al. A comparison of ARMS-Plus and droplet digital PCR for detecting EGFR activating mutations in plasma. Oncotarget. 2017;8(67):112014-112023. [CrossRef]
- Simarro J, Pérez-Simó G, Mancheño N, et al. Technical Validation and Clinical Implications of Ultrasensitive PCR Approaches for EGFR-Thr790Met Mutation Detection in Pretreatment FFPE Samples and in Liquid Biopsies from Non-Small Cell Lung Cancer Patients. Int J Mol Sci. 2022;23(15):8526. [CrossRef]
- Watanabe K, Fukuhara T, Tsukita Y, et al. EGFR Mutation Analysis of Circulating Tumor DNA Using an Improved PNA-LNA PCR Clamp Method. Can Respir J. 2016;2016:e5297329. [CrossRef]
- Lamy PJ, van der Leest P, Lozano N, et al. Mass Spectrometry as a Highly Sensitive Method for Specific Circulating Tumor DNA Analysis in NSCLC: A Comparison Study. Cancers. 2020;12(10):3002. [CrossRef]
- Sykes, P.J.; Neoh, S.H.; Brisco, M.J.; Hughes, E.; Condon, J.; Morley, A.A. Quantitation of targets for PCR by use of limiting dilution. BioTechniques 1992, 13, 444–449. [Google Scholar] [PubMed]
- Vogelstein B, Kinzler KW. Digital PCR. Proc Natl Acad Sci U S A. 1999;96(16):9236-9241. [CrossRef]
- Ottesen EA, Hong JW, Quake SR, Leadbetter JR. Microfluidic digital PCR enables multigene analysis of individual environmental bacteria. Science. 2006;314(5804):1464-1467. [CrossRef]
- Morrison T, Hurley J, Garcia J, et al. Nanoliter high throughput quantitative PCR. Nucleic Acids Res. 2006;34(18):e123. [CrossRef]
- Sundberg SO, Wittwer CT, Gao C, Gale BK. Spinning disk platform for microfluidic digital polymerase chain reaction. Anal Chem. 2010;82(4):1546-1550. [CrossRef]
- O’Leary B, Hrebien S, Beaney M, et al. Comparison of BEAMing and Droplet Digital PCR for Circulating Tumor DNA Analysis. Clin Chem. 2019;65(11):1405-1413. [CrossRef]
- Hindson BJ, Ness KD, Masquelier DA, et al. High-throughput droplet digital PCR system for absolute quantitation of DNA copy number. Anal Chem. 2011;83(22):8604-8610. [CrossRef]
- Dueck ME, Lin R, Zayac A, et al. Precision cancer monitoring using a novel, fully integrated, microfluidic array partitioning digital PCR platform. Sci Rep. 2019;9(1):19606. [CrossRef]
- Quan PL, Sauzade M, Brouzes E. dPCR: A Technology Review. Sensors. 2018;18(4):1271. [CrossRef]
- Verhoeven JGHP, Peeters AMA, Hesselink DA, Boer K. Pitfalls in the Detection of Donor-Derived Cell-Free DNA in Transplant Recipients. Clin Chem. 2021;67(7):1030-1032. [CrossRef]
- Sikora A, Zimmermann BG, Rusterholz C, et al. Detection of increased amounts of cell-free fetal DNA with short PCR amplicons. Clin Chem. 2010;56(1):136-138. [CrossRef]
- Verhoeven JGHP, Baan CC, Peeters AMA, Nieboer D, Hesselink DA, Boer K. A comparison of two different analytical methods for donor-derived cell-free DNA quantification. Clin Biochem. 2021;96:82-84. [CrossRef]
- Oellerich M, Christenson RH, Beck J, et al. Donor-Derived Cell-Free DNA Testing in Solid Organ Transplantation: A Value Proposition. J Appl Lab Med. 2020;5(5):993-1004. [CrossRef]
- Picard C, Frassati C, Cherouat N, et al. New methods for the quantification of mixed chimerism in transplantation. Front Immunol. 2023;14:1023116. [CrossRef]
- Ye P, Cai P, Xie J, Wei Y. The diagnostic accuracy of digital PCR, ARMS and NGS for detecting KRAS mutation in cell-free DNA of patients with colorectal cancer: A systematic review and meta-analysis. PloS One. 2021;16(3):e0248775. [CrossRef]
- Dong L, Wang S, Fu B, Wang J. Evaluation of droplet digital PCR and next generation sequencing for characterizing DNA reference material for KRAS mutation detection. Sci Rep. 2018;8(1):9650. [CrossRef]
- Oellerich M, Shipkova M, Asendorf T, et al. Absolute quantification of donor-derived cell-free DNA as a marker of rejection and graft injury in kidney transplantation: Results from a prospective observational study. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg. 2019;19(11):3087-3099. [CrossRef]
- Imaging single DNA molecules for high precision NIPT | Scientific Reports. Accessed June 21, 2023. https://www.nature.com/articles/s41598-018-22606-0.
- Pooh RK, Masuda C, Matsushika R, et al. Clinical Validation of Fetal cfDNA Analysis Using Rolling-Circle-Replication and Imaging Technology in Osaka (CRITO Study). Diagn Basel Switz. 2021;11(10):1837. [CrossRef]
- Saidel ML, Ananth U, Rose D, Farrell C. Non-Invasive prenatal testing with rolling circle amplification: Real-world clinical experience in a non-molecular laboratory. J Clin Lab Anal. 2023;37(6):e24870. [CrossRef]
Figure 1.
List of the NGS-based and non-NGS methods for cfDNA analysis described in the review. The different methodologies are divided according to their technological approaches. The main methods are highlighted in blue, while derived methods are indicated by arrows. References are listed by application field. NGS: Next-generation Sequencing; TAm-Seq: Tagged-amplicon Deep Sequencing; CAPP-Seq: Cancer Personalized Profiling by Deep Sequencing; WGBS-Seq: Whole Genome Bisulfite Sequencing; WES: Whole Exome Sequencing; WGS: Whole Genome Sequencing; qPCR: quantitative PCR; ARMS-PCR: Amplification Refractory Mutation System PCR; PNA Clamp PCR: Peptide Nucleic Acid Clamp PCR; COLD-PCR: Co-amplification at Lower Denaturation Temperature-based PCR; dPCR: digital PCR; BEAMing: Beads, Emulsion, Amplification, Magnetics PCR.
Figure 1.
List of the NGS-based and non-NGS methods for cfDNA analysis described in the review. The different methodologies are divided according to their technological approaches. The main methods are highlighted in blue, while derived methods are indicated by arrows. References are listed by application field. NGS: Next-generation Sequencing; TAm-Seq: Tagged-amplicon Deep Sequencing; CAPP-Seq: Cancer Personalized Profiling by Deep Sequencing; WGBS-Seq: Whole Genome Bisulfite Sequencing; WES: Whole Exome Sequencing; WGS: Whole Genome Sequencing; qPCR: quantitative PCR; ARMS-PCR: Amplification Refractory Mutation System PCR; PNA Clamp PCR: Peptide Nucleic Acid Clamp PCR; COLD-PCR: Co-amplification at Lower Denaturation Temperature-based PCR; dPCR: digital PCR; BEAMing: Beads, Emulsion, Amplification, Magnetics PCR.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



