
Submitted:
22 March 2024
Posted:
26 March 2024
You are already at the latest version
Abstract
Health comprises physical, mental and social dimensions whose interactions influence users’ experiences. Health experiences are within the context of environments. These contexts are definitive contributors to experiences – primarily because of the link to social dimensions as human beings - psychological and economic. Therefore, the study aims to investigate health resort users’ psycho-social and socio-economic characteristics to improve their access to quality healthcare. The objectives are identifying the socio-economic characteristics of an inclusive health resort, analysing the psycho-social characteristics of the inclusive health resort user, and analysing the effects of users’ psycho-social and socio-economic characteristics on their access to healthcare. The study employs the mixed research method (qualitative and quantitative). The researchers engaged in a pragmatic research philosophy that underscores positivist and interpretivist paradigms. The data collection instruments include survey questionnaires, an interview guide with a digital recorder, a direct participant observation schedule, field notes and photographs. The data analysis process involves the clustering and categorisation of data and examining concepts and themes. The research findings show a correlation between the users’ socio-economic status and access to quality healthcare in an inclusive health resort. The result further reveals that psycho-social and socio-economic characteristics of health resort users are quality healthcare access predictors. Therefore, the users’ social, psychological, and economic status should play a vital role in the design of an inclusive health resort by all stakeholders.
Keywords:
Health seeker' Behaviour
; User Psycho-social Characteristics
; Socio-economic Characteristics
; Health Resort Design
; Social Factors
1. Introduction
Recent studies indicate that the occurrence and potential of social factors lead to poor health [1,2]. Hence, several health institutions, systems and organisations are interested in addressing unmet social needs via services [3]. Services fundamentally affect our lives and well-being as individuals, families, and communities [4]. Healthcare is a service. And health is connected to social factors, which are conditions for any human environment [5]. These conditions include economic, psychological, and social factors. In the quest for health services, needs and choices are subject to social factors. Social factors constrain the response to meet our health-related needs and influence behavioural patterns. Understanding social dimensions prevalent among health resort (services) users may inform decision-making in health-resort architectural design programming [6]. It corroborates recent studies that opine that the success of health resorts as care facilities may result from understanding the users’ behaviour to ensure services meet needs and choices [7]. Social factors here are two-fold—psychological and economic. However, according to Abraham Maslow’s hierarchy of needs, human needs are classified into eight interdependent categories [8].
Considering current global trends of disease outbreaks such as COVID-19 and their societal impacts (including economic and psychological health), health is pluralistic in influence. The study focuses on psycho-social and socio-economic characteristics and the social connections of a health-seeking group—health resort users. Therefore, the research aims to investigate the psycho-social and socio-economic features of health resort users to improve their access to excellent health. The study seeks to test the theory that these characteristics influence components of human behaviour on their needs and choices in the usage of healthcare facilities/ services (health resorts). Thus, the questions include: What are health resort users’ socio-economic characteristics? What are the psycho-social features of health resort users? What is the relationship between user’s psycho-social and socio-economic characteristics on their access to healthcare?
2. Literature Review
After the COVID-19 pandemic outbreak, achieving and maintaining good health has become vital [9,10]. Healthy living is a basic human need and a fundamental right [11]. Health encompasses three dimensions—physiological, psychological, and social [12,13]. The complex ‘mind-body-health-well-being’ permits us to share in loving, enduring relationships with family and friends, contribute to our communities, or fully participate in work [14]. Interacting factors affect mental health and social, economic, psychological, physiological, behavioural, and environmental influences [15].
The built environment includes several material determinants of health that shape the social, economic and environmental conditions for good health [16]. Environmental and socio-economic contexts influence people’s actions to improve their health status. Socio-economic and psycho-social factors affect access to healthcare [17]. In the built environment, healthcare buildings can support health, well-being, and social interactions [18]. Health resorts are tranquil places with unique therapeutic landscapes and attractive public spaces for improving users’ quality of life (QoL) [19,20]. Health resorts have a connection with disease prevention, health education and health-seeking behaviour [21]. The user needs and user-humanist perspective on spaces and features should be the basis for designing health resorts [22,23].
Human conduct is cognitive, emotional, or physical activities that influence behaviour, needs and choices [24]. The built environment interventions (healthcare facilities) provide a sustained effect on behaviour [25]. Users’ behavioural intentions are generally associated with health resort attraction indicators [26]. These intentions include affordable social activities and health consciousness, which define health-seeking individuals [27,28]. Hardan-Khalil (2020) observed that health promotion behaviours correlate with age, education, psychological stress, health, and social support. Health-seeking behaviours (HSB) are closely linked with health status and extend to economic development. Also, [29] reported that, in Nigeria, appropriate HSB is high among civil servants. Behaviour influences health, and a healthy lifestyle decreases health risks [30,31]. Socio-economic status (SES) and the family system promote HSB [32]. Hence, understanding the interplay between social and behavioural factors and their relevance to healthcare service utilisation has become a vital healthcare policy consideration [33]. According to [34], the predictors of the perceived quality of healthcare were the age of respondents, level of education, house type lived in, the number of persons in the house, toilet facility types, the primary source of water supply, waste disposal practices, and level of education.
[35] revealed that healthcare assessments include social dimensions of health in patients’ assessment. [36,37] explained that reducing social isolation improves health and disease interventions. The underlying causes of health disparities are social and structural health determinants, economic and educational disadvantages, healthcare access and quality, and individual behaviour, among other factors [38,39]. Several easily measurable social factors determine the health-related quality of life (HRQoL) [40]. The existing literature presents a socio-economic index among the beneficial indices of a natural health environment, such as a health resort [41]. People’s SES affects their access to nature and quality health services [42,43,44,45]. Money and social support are variables of homelessness and health risk [13,46]. Again, Quality of life (QoL) correlates with SES [47]. The RUCAS-analytic framework shows a link among socio-economic variables, health inequities, the built environment and health [48,49,50]. Socio-economic variables, such as education and gender, determine work type, workplace conditions and earnings [51,52]. Psycho-social health outcome combines SES and gender [53].
[54] identified and grouped psycho-social needs along with Abraham Maslow’s hierarchy of needs as psychological, safety, social, esteem, aesthetics, self-actualisation and self-transcendence. [55] recon that social factors affect disease preventive measures. Similarly, [56] opine that improving a sense of community by reducing social isolation and loneliness enhances health. [57] agree that the quality of living spaces is a quality health determinant. In health resorts, research links nature experience to psychological dimensions, perceptions and interactions with stimuli from the natural world through sensory modalities-sight, hearing, taste, touch, and smell [58]. Psycho-social factors influence the senses that connect humans to the environment [14,59,60]. Sensory features are inevitably present in architectural design [61].
3. Materials and Method
The researchers designed the methodology section of this study to address the research aim and objective. The study investigates health resort users’ psycho-social and socio-economic characteristics to improve their access to quality healthcare. The intents include identifying the socio-economic characteristics of an inclusive health resort, analysing the psycho-social characteristics of the inclusive health resort user, and studying the effect of socio-economic and psycho-social characteristics of users on their access to quality healthcare in a health resort. However, health has physical, mental, and social components, so assessing users’ characteristics may be challenging. The researchers must consider the feasibility of collecting data, sampling, ease of observation, or data availability. Therefore, the study employs the mixed research method (qualitative and quantitative). The study used a pragmatic research philosophy that measures from the positivist and interpretivist paradigms, as presented in Figure 1. This mixed-method approach allows for a healthy triangulation of quantitative and qualitative data and reliable responses to the research questions raised in the introduction. The study population is Port-Harcourt residents’, in Port-Harcourt, Nigeria. According to the United Nations, the estimated population of the Port Harcourt Metropolitan area is 3,171,076. The 2022 population of the Port Harcourt metro area is 3,325,000, at a 4.86% growth rate from 2021 [62]. The population elements are 1. Port-Harcourt Residents; 2. Professionals/experts in Port-Harcourt local government.
3.1. Sampling Techniques
According to [63], the projected population of the purposely selected Port Harcourt metro area is about 3,325,000 residents. [64] determined the sample size by using simple calculations. [65] argued that the result from the sample might be an overview of the entire population as long as it is representative. Therefore, the formula for the sample size is in equation (i) at the confidence interval of 95% with a significance level of 5%.
The Formula for sample size: n ==N/1+N (e) 2 -------------------- (i)
Where:
n = Sample size to be studied
N = Population size
e = margin of error (0.05)
n = 3,325,000/1+3,325,000 (0.05)2
n = 3,325,000/1+8312.5
n = 399.95
The sample in this study is 399.95
From the above formula, the required sample size for this study was 399 people. The researcher used purposive and random sampling to select the participants. The sample sizes for the Port Harcourt metro area, Port Harcourt, were picked from the total eligible households listed and some professionals.
3.2. Research Design
[66] explain that research design is the specific procedure involved in the research process: data collection, analysis, and report writing. The research design in this research uses an analysis research design. Therefore, the theories underpinning the study define the research method used [67]. Based on all the considerations, the authors chose the mixed-method research approach. In mixed methods research, the researcher blends quantitative and qualitative research techniques, concepts, or language into a single analysis and theoretically by providing a reasonable and realistic alternative. However, a mixed analysis involves quantitative and qualitative data analysis techniques and allows a rational approach and framework within the same study. Its inquiry logic includes inference, deduction, and abduction [68]. A mixed-methods study is an effort to legalise several approaches to address research questions rather than limiting the researchers’ choices. It is an expansive and innovative type of analysis. It is inclusive and balanced and indicates that researchers take a broad approach to the selection methods, study thought, and behaviour. It entails collecting both types of data at the same time; assessing information using parallel constructs for both data types; separately analysing both data types; and comparing results through side-by-side comparison in a discussion, transforming the qualitative data set into quantitative scores, or jointly displaying both forms of data [69]. Therefore, mixed methods are effective for understanding gaps between quantitative and qualitative data and participants’ views. Mixed methods ensure those study findings are grounded in participants’ experiences. Promotes scholarly interaction by improving the validity and reliability of the resulting data and strengthens causal inferences by providing the opportunity to observe data convergence. Since health and well-being are multi-faceted issues, this paper has employed the sequential explanatory mixed-method approaches (qualitative and quantitative) to investigate the effect of Health resort user characteristics on their access to quality healthcare in Nigeria.
3.3. Communal Survey
The researcher conducted social surveys among two respondent groups: health facilities users (residents) and Amenities providers (design/planning and health experts). The questionnaire asked respondents about their preferences for healthcare in the inclusive health resort and socio-demographic criteria such as age and overall situation. The study connected the following questions with the issues of psycho-social and socio-economic characteristics. Therefore, the co-author and three (3) other research assistants-M.Sc. Students in the architecture department at Rivers State University (RSU), Nigeria, distributed the questionnaires. It was a controlled distribution systematically organised and conducted on weekends (usually Friday through Sunday), in the mornings and evenings (10:00–12:00 am and 5:00–7:00 pm). The research assistants randomly distributed the surveys to residents-in the Port Harcourt metro area and professionals-designers/planners and health officials-in the Port Harcourt Local Government Area (PHALGA). This approach provided the necessary tuning of research and enabled the identification of various daily routines and behaviours among residents. The authors retrieved 305 filled questionnaires (270 from Port Harcourt metro area residents, 35 from staff/professionals) reflecting the socio-demographic characteristics of residents in the study area.
3.4. Recruitment Procedure
Participants for the study were 12 experts or professionals: Built Environment Professionals-BEPs and health and medical professionals-HMPs). Each in-depth individual interview (IDI) lasted for 60 to 90 minutes. The investigators distributed 12 signed consent forms to participate in the study, and they all expressed interest in the interview exercise. Following the recommendation in qualitative research to ensure a suitable representation of the lived experiences and diversity of the experts, the investigators used a purposive sampling method with six criteria: age, gender, marital status, education, occupation and years of experience, as shown in Table 1 below.
3.5. Data Collection
The authors extracted data from both primary and secondary sources. The primary data collection instruments consisted of survey questionnaires, an In-depth interview (IDI) guide with a digital recorder, a direct participants’ observation schedule, field notes and photographs. The authors distributed three hundred and ninety-nine (399) questionnaires among the Healthcare facilities users and industry specialists within the study areas, as shown in Table 2. Out of 399 questionnaires distributed, the researchers retrieved 305. The authors interviewed twelve (12) selected professionals/experts (health officials and design),—five (5) Interviewees from Port Harcourt LGA and one (1) each of the other seven (7) LGAs. The study also used an observation schedule, field notes, and photographs to record data on the available healthcare facilities in Port Harcourt. The authors used a semi-structured questionnaire to identify healthcare facility users’ psycho-social and socio-economic characteristics. The co-author and three (3) research assistants undertook the data gathering process for twelve (12) weeks –morning and evening during the weekend, Fridays to Sundays.
3.6. Ethics
During the survey data collection process, the research assistants captured no photographs of respondents during the interview. This aspect involves direct participation, so the co-author and three research assistants distributed the questionnaires. Therefore, there was no need for an ethical approval certificate for the questionnaires. However, for the participants interviewed, a consent form approval came from the ethics committee.
3.7. Data Analysis
The study used the explanatory sequential mixed approach in the analysis (i.e., collecting quantitative data first, then using qualitative data to explain the quantitative findings). The Users’ psycho-social characteristics were analysed using descriptive statistical analysis of the 7-Likert scale, and the result was in tables, charts, screen plots, and graphs. The questionnaire survey employed the co-author and three (3) research assistants across the eight LGAs of the Port Harcourt Metropolitan Area. The co-author covered Port Harcourt LGA (PHALGA), and the other three research assistants covered seven (7) LGA. The investigators used IBM-SPSS version 26 and Microsoft Excel to code and analyse the data. The analysis process involves data clustering and categorisation and examining concepts and themes. The study identifies the socio-economic characteristics of an inclusive health resort through questionnaires and interview guides to the residents and professionals across the eight (8) LGAs. In analysing the psycho-social characteristics of the all-inclusive health resort user, Descriptive means analysis on data collected from questionnaires administered to residents and professionals and interviews with professionals from across the Port Harcourt Metropolitan Area to ensure an optimum result. The researchers analysed objective three (- studying the effect of the users’ socio-economic status on their access to quality healthcare in a health resort) using Correlation coefficients (r) to check the relationship between the user characteristics (psycho-social and socio-economic) and their access to quality healthcare across the selected Healthcare facilities case studies in Port Harcourt.
4. Results
The authors obtained psycho-social and socio-economic characteristics of health resort users using survey questionnaires. The researcher distributed one short of four hundred questionnaires with a return rate of 76% (i.e., 305 questionnaires). The authors presented the twelve (12) participants’ experiences and expertise through direct quotes.
4.1. Result of Socio-economic Characteristics of Health Resort Users
According to the medical director of Okrika General Hospital, Okrika LGA, Port-Harcourt: “Socio-economic characteristics include occupation, education, income, wealth and housing”. He added that “these characteristics can significantly affect how well and how long people live, and their ability to make healthy choices, afford medical care, and manage stress”.
(Medical Doctor, IDI: 2023)The medical director of General Hospital Ogu, Ogu–Bolo LGA, Port-Harcourt, said: “During an assessment, SES is typically broken into three levels (high, middle, and low) to describe the three places a family or an individual may fall into when placing a family or individual into one of these categories, or all of the three variables (income, education, and occupation)”. According to him“People’s SES defines their occupation, income, and education. Lower SES, such as low-income neighbourhood living or having a high-stress, low-control job, is often linked to a wide range of health problems and higher mortality. Therefore, the higher the SES, the healthier they tend to be – a phenomenon often termed the social gradient of health”.(Medical Doctor, IDI: 2023)
The socio-economic characteristics recorded include gender, age, marital status, highest educational qualification, employment status and income level (Figure 2).
The study’s result represents a highly educated population, with most respondents having completed higher education ranging from NCE/OND at 8%, first degree/HND at 37.7%, and postgraduate studies at 21% (Table 3 above). Fewer than 8% of those surveyed lack formal education. It shows that most respondents have the educational background necessary to be part of the research. The study’s population is intellectually endowed to be aware of and seek quality healthcare services. Most respondents are either students or those who work for a salary or pay, with students making up a 4% larger share of respondents than wage earners. 41% of the population makes a living via paid employment and self-employment and is considered an active earner. Less than 21% are high earners, defined as those earning more than 300,000 Naira monthly, whereas 77% receive between 5,000 to 300,000 Naira. Quality health service is expensive to procure [70,71]. Therefore, in a well-informed population interested in maintaining quality health, the question is what quality healthcare is readily accessible (from a User’s socio-economic perspective). To further bolster this socio-economic character of the population, with the depreciating value of the national currency (Nigerian Naira) to global currencies (e.g., United States Dollar), the low-to-average income earners, which make up the most population (77%) are at an increased risk of reduced access to quality health services.
4.2. Result of Psycho-Social Characteristics of the Inclusive Health Resort User
The selected health facilities within the study area were ten (10) of the eight LGAs, as shown in Table 3. Each facility is from seven (7) local governments in the Port Harcourt metropolis—three (3) health facilities from the PHALGA. PHALGA is the largest and most populated LGA in the Port Harcourt metropolis. Hence, it covers more facilities than other LGAs.
However, the HOD, Psychiatric at General Hospital, Ebubu Eleme, Eleme LGA, Port-Harcourt, said: “Psycho-social characteristics influence an individual psychologically and socially. Explaining that: “Such characteristics can describe individuals with their social environment and how these affect physical and mental health”. Also, he believes that “Better health can lead to healthier lifestyles, better physical health, greater opportunities for educational attainment, greater productivity and economic participation, better relationships with people, more social cohesion, and improved quality of life”.(Psychiatric, IDI: 2023)
The CMO of Heritage Medicare Hospital, Oyigbo LGA, Port-Harcourt, describe psycho-social characteristics as the influences of social factors on individual mental health and behaviour. “Psycho-social adaptations are important because they affect the quality of life and are on the causal pathway to somatic disease”. He further said:“Psycho-social characteristics in healthcare included social resources (social ties, relationships, group work, social integration and emotional support), psychological resources (perceived control, self-esteem, sense of place and privacy, sense of home, sense of safety, sense of coherence, and trust), and psychological risk factors (air quality, water quality, quality of sleep, orderliness, cynicism, vital exhaustion, hopelessness, and depressiveness)”. The findings corroborated the literature in Table 4.(Medical Doctor, IDI: 2023)
Psycho-social characteristics of health resort users connect Abraham Maslow’s eight levels of human needs. Thus, sixteen factors corresponding to Maslow’s eight tiers, justified through literature, were presented to respondents to gauge the psycho-social traits of health resort users. The researchers listed these sixteen characteristics in Table 5, and literature justifications are in the Empirical Support column. The authors asked the respondents to rate these Characteristics concerning four (4) main facilities identified as making up a health resort, including the hospitality category (hotel and spa), the exercise and recreational category (gyms/fitness centres), and the medical category (hospital).
The authors ranked the first eleven (11) measured characteristics, as shown in Table 4, on a 7-point Likert scale ranging from very poor to excellent, while the twelfth to sixteenth characteristics were from strongly disagree to agree. As already stated, recall that healthcare is primarily a service, and like all services, it is to meet needs. Also, as a service, healthcare would attempt to satisfy a range of user choices, taking into cognisance the diverse behavioural responses of its service users. The perception of health as a service has guided the development of these sixteen psycho-social characteristics. On close examination, it would be evident that each of the sixteen measured characteristics can be in at least one category of Maslow’s levels of human needs. In healthcare (health service), these characteristics are akin to human health on various psycho-social levels.
4.3. Results of Analysing the Effects of Users’ Psycho-Social and Socio-Economic Characteristics on Their Access to Healthcare
Good access to healthcare is the ability of patients to get the care and services needed when due [90]. It is essential to providing high-quality healthcare and ensuring that patients receive proper treatment. Therefore, patient access to healthcare benefits include better care, improved health outcomes, reduced costs, disease progression prevention, reduced wait times, and better quality of life. However, research has shown that psycho-social variables, including stress, emotions, and social characteristics, may contribute to the association between socio-economic status (SES) and access to health.
The medical director of Military Hospital, Port Harcourt LGA (PHALGA), Port-Harcourt, corroborated the statement and said: “From experience, lower SES concomitant with reduced access to healthcare, poorer health outcomes, and increased mortality and morbidity. Similarly, higher incomes are usually associated with better nutritional status and medical services. In addition, people with higher levels of education tend to have better health awareness and health-related knowledge. Consequently, higher SES may be simultaneous with better physical health”.(Medical Doctor, IDI: 2023)
In another interview with the chief medical director (CMD) of the University of Port Harcourt Teaching Hospital, Obio-Akpor LGA, Port-Harcourt, he said: “Individuals with low socio-economic status (SES) tend to have less access to healthcare. Adding that SES can significantly affect a patient access to healthcare”. According to him“Low SES adults are less likely to receive preventive services for chronic conditions such as diabetes, cancer, and cardiovascular disease”. Also: “The consequences of Low SES are significant and include the use of fewer preventive services, poorer health outcomes, higher mortality and disability rates, lower annual earnings because of sickness and disease, and the advanced stage of illness”.(Medical Doctor, IDI: 2023)
Responses show that in the health-seeking experiences of users, accommodation is vital regarding their psycho-social characteristics. In Table 5, ten (10) of 16 characteristics feature accommodation with the highest mean score per variable. Also, the sense of place, privacy, and home, which recorded the lowest overall mean scores, further bolsters users’ accommodation-related concerns. It indicates their expectations of healthcare facilities’ environment—a homely one offers a sense of place and privacy. And so, from a psycho-social context, users’ health-seeking behaviour is influenced by how efficiently a health facility communicates homeliness, privacy, and a sense of place. Responses on the medical component (Table 6) returned the least means scores per variable, consistently across all the psycho-social characteristics. It is because the form of healthcare in Nigeria (Port Harcourt) is medical (hospitals). Therefore, if users rate the main form of healthcare in the study area (Nigeria) as low in its psycho-social characteristics, then psycho-social characteristics should be a vital consideration for providing health services.
The correlation test in Table 6 reveals a positive correlation between educational qualification and Users’ expectation of orderliness in healthcare facilities, particularly regarding accommodation services. Table 6 further shows a connection between Users’ educational qualification and their perception of a facility that befits their status or otherwise. Interestingly, orderliness and perception of facilities befitting Users’ status returned the highest overall mean scores, as highlighted in Table 6.
Table 7, on the other hand, presents an inverse relationship between income levels and a sense of safety and sleep quality in health facilities. It could indicate that health service users with greater income levels who are more likely to afford better quality services would have fewer concerns about their safety in health facilities. It could be due to better security services and safety measures in such facilities. Therefore, it offers a complementary environment that favours quality sleep.
5. Discussion
The outcomes of the analysis in this study have confirmed the positions of literature on the influence of the socio-economic characteristics of health-seeking individuals on their health-seeking behaviours—particularly regarding their access to quality healthcare. The levels of enlightenment (formal education) and income are socio-economic factors determining people’s choice of where to go for quality healthcare [91,92,93]. These factors determine health seekers’ ability to secure health services in facilities they perceive to offer the best service. It is such that an individual by the level of enlightenment (educational qualification) might be aware of what quality health services are available and, at the same time, constrained by the economics to access the best services. This constraining influence portends a resort to alternatives and behavioural choices to meet health needs. Besides the role of fiscal requirements as a socio-economic decimal in quality healthcare acquisition, this study also reveals some psycho-social connections.
While it is easy to appreciate the socio-economic characteristics of quality healthcare acquisition/access, it is unclear how psycho-social features relate to accessing quality healthcare services [94]. The study results indicate that accommodation, privacy and homely environments are key psycho-social considerations for health services users in Port Harcourt. It further reveals that for individuals with socio-economic capabilities to access quality services, the need for a homely atmosphere determines their behavioural choices. Separately, they have established that psycho-social and socio-economic indices influence access to healthcare [95]. The correlation test connects both indexes as a co-joining influence on users’ access to healthcare services. However, accommodation affects persons with higher educational qualifications. Therefore, users’ levels of exposure influence their preferences for and expectations from a health facility. Observation shows that the clamour for decent accommodation does have a connection with their appeal for homeliness within health facilities, as earlier highlighted. Of interest is the correlation between a sense of safety plus status sleep quality and the income levels of healthcare-seeking individuals.
6. Conclusions
This study corroborates a perspective of literature indicating that socio-economic factors influence the consumption behaviour of health resort users. However, it is interesting to note that the findings from this study drive a new perspective beyond the individual fiscal capacity to purchase quality healthcare service, which is an interest in healthcare service in a homely environment. The health service users’ interest seems to exceed the effectiveness of medical science in treating illness, the setting to receive medical care and other forms of healthcare. These psycho-social perspectives are not entirely new but seem neglected. However, given their complementary impact in providing quality healthcare service and the benefits of fostering population health, such environments should be cultured in our healthcare services. Achieving this would involve the collaborative action of various stakeholders ranging from the government, healthcare service providers, healthcare practitioners, built environment design professionals and the users of these services. This study is essentially a stimulus to engineer this process for a health resort facility in Port Harcourt, Nigeria, that aims to improve residents’ health-related quality of life (HRQoL).
Author Contributions
Dr Eghosa N Ekhaese was involved in the conceptualisation and methodology, data collection and curation, qualitative analysis, writing—original draft, writing—review and editing, project administration, research aim and objective, design of methodology, research supervision, final draft, and collation of all sections of the paper. Onyedikachukwu O, Ndimako did the literature reviews, investigation, data collection and writing—original draft. All authors have read and agreed to the published version of the manuscript.
Funding
N/A. However, Covenant University, Ota Nigeria, will provide the needed financial support for the APC (article processing charges).
Institutional Review Board Statement
The study is in accordance with the Declaration of Helsinki and with approval from the research ethics committees of Covenant University, Nigeria, and CHREC.
Informed Consent Statement
Investigators obtained Informed consent from all subjects involved in the study.
Data Availability Statement
The datasets generated during the present study are available from the corresponding author upon reasonable request. The datasets are not publicly available owing to privacy or ethical restrictions.
Acknowledgements
The author sincerely appreciates Covenant University’s financial assistance in publishing this article. We are indeed grateful for the contributions of all the authors. Also, appreciation goes to the research assistants for their involvement in the data collection and writing of an aspect of the literature review. However, the authors take responsibility for every error and omission in this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Alcañiz, M.; Solé-Auró, A. Feeling good in old age: factors explaining health-related quality of life. Heal. Qual. Life Outcomes 2018, 16, 48. [Google Scholar] [CrossRef] [PubMed]
- Ekhaese, E.N.; A Adejuwon, G.; Evbuoma, I.K. Promoting Green Urbanism in Nigerian Purlieus as Therapy for Psychological Wellbeing/Health. IOP Conf. Series: Earth Environ. Sci. 2021, 665, 012015. [Google Scholar] [CrossRef]
- Palakshappa, D.; Furgurson, K.F.; Harley, M.G.; Bundy, R.; Moses, A.; Taxter, A.J.; Bensinger, A.S.; Cao, X.; Denizard-Thompson, N.; Rosenthal, G.E.; et al. Feasibility of Mobile Technology to Identify and Address Patients' Unmet Social Needs in a Primary Care Clinic. Popul. Heal. Manag. 2021, 24, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Ostrom, A.L. Transformative Service Research. J. Serv. Res. 2015, 18, 243–249. [Google Scholar] [CrossRef]
- Blacker, A.; Dion, S.; Grossmeier, J.; Hecht, R.; Markle, E.; Meyer, L.; Monley, S.; Sherman, B.; VanderHorst, N.; Wolfe, E. Social Determinants of Health—an Employer Priority. Am. J. Heal. Promot. 2020, 34, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Deesilatham, S. Wellness tourism: determinants of incremental enhancement in tourists’ quality of life. Royal Holloway, University of London; 2016 May. http://www.tourism.jurmala.lv/upload/turisms/petijumi/4wr_wellnesstourism_2020_fullreport.
- Hardan-Khalil, K. Factors Affecting Health-Promoting Lifestyle Behaviors Among Arab American Women. J. Transcult. Nurs. 2019, 31, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Acevedo, A. A Personalistic Appraisal of Maslow’s Needs Theory of Motivation: From “Humanistic” Psychology to Integral Humanism. J. Bus. Ethic- 2015, 148, 741–763. [Google Scholar] [CrossRef]
- Badiora, A.I. ; Abiola OB Quality of life (QoL) of rural dwellers in Nigeria: a subjective assessment of residents of Ikeji-Arakeji, Osun-State. Annals of Ecology and Environmental Science. 2017; 1(1):69-75.
- Masiero, S.; Maccarone, M.C. Health resort therapy interventions in the COVID-19 pandemic era: what next? Int. J. Biometeorol. 2021, 65, 1995–1997. [Google Scholar] [CrossRef] [PubMed]
- Raheem, T.Y.; Adewale, B.; Adeneye, A.K.; Musa, A.Z.; Ezeugwu, S.M.C.; Yisau, J.; Afocha, E.; Sulyman, M.A.; Adewoyin, O.O.; Olayemi, M.; et al. State of Health Facilities in Communities Designated for Community-Based Health Insurance Scheme in Nigeria: A Case Study of Kwara and Ogun States. Int. J. Trop. Dis. Heal. 2019, 1–10. [Google Scholar] [CrossRef]
- World Health Organization. Global action plan on physical activity 2018-2030: more active people for a healthier world. World Health Organization; 2019 Jan 21. 9241.
- Ekhaese, E.N.; Evbuoma, I.K.; A Adejuwon, G.; A Odukoya, J. Homelessness Factors and Psychological Wellbeing Concerns in Nigerian Cities. IOP Conf. Series: Earth Environ. Sci. 2021, 665. [Google Scholar] [CrossRef]
- Eijkelenboom, A.; Verbeek, H.; Felix, E.; van Hoof, J. Architectural factors influencing the sense of home in nursing homes: An operationalization for practice. Front. Arch. Res. 2017, 6, 111–122. [Google Scholar] [CrossRef]
- Brown, L.M. SKILLS FOR PSYCHOLOGICAL RECOVERY DURING AND AFTER DISASTERS TO STRENGTHEN SOCIAL SUPPORT. Innov. Aging 2019, 3, S391–S391. [Google Scholar] [CrossRef]
- Ellena, M.; Breil, M.; Soriani, S. The heat-health nexus in the urban context: A systematic literature review exploring the socio-economic vulnerabilities and built environment characteristics. Urban Clim. 2020, 34, 100676. [Google Scholar] [CrossRef]
- Soedarsono, S.; Mertaniasih, N.M.; Kusmiati, T.; Permatasari, A.; Juliasih, N.N.; Hadi, C.; Alfian, I.N. Determinant factors for loss to follow-up in drug-resistant tuberculosis patients: the importance of psycho-social and economic aspects. BMC Pulm. Med. 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nathan, A.; Villanueva, K.; Rozek, J.; Davern, M.; Gunn, L.; Trapp, G.; Boulangé, C.; Christian, H. The Role of the Built Environment on Health Across the Life Course: A Call for CollaborACTION. Am. J. Heal. Promot. 2018, 32, 1460–1468. [Google Scholar] [CrossRef] [PubMed]
- Belčáková, I.; Galbavá, P.; Majorošová, M. HEALING AND THERAPEUTIC LANDSCAPE DESIGN – EXAMPLES AND EXPERIENCE OF MEDICAL FACILITIES. Int. J. Arch. Res. Archnet-IJAR 2018, 12, 128–151. [Google Scholar] [CrossRef]
- Bernat, S. Sustainable Development of Health Resorts in Poland. Barom. Reg. Anal. i Prognozy 2018, 16, 43–52. [Google Scholar] [CrossRef]
- Roberts, J.D.; Ada, M.S.; Jette, S.L. NatureRx@UMD: A Review for Pursuing Green Space as a Health and Wellness Resource for the Body, Mind and Soul. Am. J. Heal. Promot. 2020, 35, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Rao, V. Choudhury R. A study of the factors influencing customer satisfaction in medical tourism in India. International Journal of Business and General Management. 2017; 6(5):7-22. www.iaset.us.
- Ystgaard, K.F.; Atzori, L.; Palma, D.; Heegaard, P.E.; Bertheussen, L.E.; Jensen, M.R.; De Moor, K. Review of the theory, principles, and design requirements of human-centric Internet of Things (IoT). J. Ambient. Intell. Humaniz. Comput. 2023, 14, 2827–2859. [Google Scholar] [CrossRef]
- Cherubino, P.; Martinez-Levy, A.C.; Caratù, M.; Cartocci, G.; Di Flumeri, G.; Modica, E.; Rossi, D.; Mancini, M.; Trettel, A. Consumer Behaviour through the Eyes of Neurophysiological Measures: State-of-the-Art and Future Trends. Comput. Intell. Neurosci. 2019, 2019, 1–41. [Google Scholar] [CrossRef]
- Engineer, A.; Gualano, R.J.; Crocker, R.L.; Smith, J.L.; Maizes, V.; Weil, A.; Sternberg, E.M. An integrative health framework for wellbeing in the built environment. J. Affect. Disord. 2021, 205, 108253. [Google Scholar] [CrossRef]
- Majeed, S.; Lu, C.; Majeed, M.; Shahid, M.N. Health Resorts and Multi-Textured Perceptions of International Health Tourists. Sustainability 2018, 10, 1063. [Google Scholar] [CrossRef]
- Tyagi, R.; Vishwakarma, S.; Yadav, S.S.; Stanislavovich, T.A. Community self-help projects. InNo Poverty 2021 (pp. 120-128). Cham: Springer International Publishing. 25 May. [CrossRef]
- Asselmann, E.; Borghans, L.; Montizaan, R.; Seegers, P. The role of personality in the thoughts, feelings, and behaviors of students in Germany during the first weeks of the COVID-19 pandemic. PLOS ONE 2020, 15, e0242904. [Google Scholar] [CrossRef]
- Latunji, O.; Akinyemi, O. FACTORS INFLUENCING HEALTH-SEEKING BEHAVIOUR AMONG CIVIL SERVANTS IN IBADAN, NIGERIA. 2018, 16, 52–60.
- Huang, Y.; Liu, P. An Evaluation of College Students’ Healthy Food Consumption Behaviors. J. Culin. Sci. Technol. 2020, 19, 408–423. [Google Scholar] [CrossRef]
- Nielsen, S.S.; Skou, S.T.; Larsen, A.E.; Bricca, A.; Søndergaard, J.; Christensen, J.R. The Effect of Occupational Engagement on Lifestyle in Adults Living with Chronic Pain: A Systematic Review and Meta-analysis. Occup. Ther. Int. 2022, 2022, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed]
- Sterling, S.; Chi, F.; Weisner, C.; Grant, R.; Pruzansky, A.; Bui, S.; Madvig, P.; Pearl, R. Association of behavioral health factors and social determinants of health with high and persistently high healthcare costs. Prev. Med. Rep. 2018, 11, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Oladosun, M.; Azuh, D.; Fasina, F.F.; Akanbi, M.; Amoo, E.; Osabuohien, E.S.; Adekola, P.; Okorie, U. Atteinte des objectifs de developpement durable au Nigeria: Informations sur la dynamique de la population, les relations entre les sexes, les inegalites et l’insecurite. African Journal of Reproductive Health. 2021, 25, 27–34. [Google Scholar]
- Nicolaus, S.; Crelier, B.; Donzé, J.D.; E Aubert, C. Definition of patient complexity in adults: A narrative review. J. Multimorb. Comorbidity 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, L.Y.; Hansel, T.C.; Bordnick, P.S. Loneliness, isolation, and social support factors in post-COVID-19 mental health. Psychol. Trauma: Theory Res. Pract. Policy. [CrossRef]
- Brady, S.; D’Ambrosio, L.A.; Felts, A.; Rula, E.Y.; Kell, K.P.; Coughlin, J.F. Reducing Isolation and Loneliness Through Membership in a Fitness Program for Older Adults: Implications for Health. J. Appl. Gerontol. 2020, 39, 301–310. [Google Scholar] [CrossRef]
- Tull, M.T.; Edmonds, K.A.; Scamaldo, K.M.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological Outcomes Associated with Stay-at-Home Orders and the Perceived Impact of COVID-19 on Daily Life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef] [PubMed]
- Hooper, M.W.; Nápoles, A.M.; Pérez-Stable, E.J. COVID-19 and Racial/Ethnic Disparities. JAMA J. Am. Med. Assoc. 2020, 323, 2466. [Google Scholar] [CrossRef] [PubMed]
- Phyo, A.Z.Z.; Presidents Malaria Initiative. Quality of life and mortality in the general population: A systematic review and meta-analysis. BMC Public Health 2020, 20, 1596. [Google Scholar] [CrossRef] [PubMed]
- Jessel, S.; Sawyer, S.; Hernández, D. Energy, Poverty, and Health in Climate Change: A Comprehensive Review of an Emerging Literature. Front. Public Heal. 2019, 7, 357. [Google Scholar] [CrossRef] [PubMed]
- Ede, J.; Initiative, P.M.; The Nigerian Demographic and Health Survey (DHS) 2013 report; Profile, F. A.A.O.O.T.U.N.; 2015, N.C.C.N.; Newspaper, T.L. Increasing access to quality health care using health technology to ‘cut-out’ urban communities in Nigeria. Ann. Glob. Heal. 2016, 82, 454. [Google Scholar] [CrossRef]
- Aloh, H.E.; Onwujekwe, O.E.; Aloh, O.G.; Okoronkwo, I.L.; Nweke, C.J. Impact of socioeconomic status on patient experience on quality of care for ambulatory healthcare services in tertiary hospitals in Southeast Nigeria. BMC Heal. Serv. Res. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Ade, R.; Rehm, M. Home is where the health is: what indoor environment quality delivers a “healthy” home? Pac. Rim Prop. Res. J. 2019, 26, 1–17. [Google Scholar] [CrossRef]
- Fasina, F.; Oni, G.; Azuh, D.; Oduaran, A. Impact of mothers’ socio-demographic factors and antenatal clinic attendance on neonatal mortality in Nigeria. Cogent Soc. Sci. 2020, 6. [Google Scholar] [CrossRef]
- Mao, P.; Wang, X.; Wang, R.; Wang, E.; Li, H. Passengers’ Sensitivity and Adaptive Behaviors to Health Risks in the Subway Microenvironment: A Case Study in Nanjing, China. Buildings 2022, 12, 386. [Google Scholar] [CrossRef]
- Uysal, M.; Sirgy, M.J. Quality-of-life indicators as performance measures. Ann. Tour. Res. 2019, 76, 291–300. [Google Scholar] [CrossRef]
- Baeza, F.; Vergara, A.V.; González, F.; Orlando, L.; Valdebenito, R.; Cortinez-O’ryan, A.; Slesinski, C.; Roux, A.V.D. The Regeneración Urbana, Calidad de Vida y Salud - RUCAS project: a Chilean multi-methods study to evaluate the impact of urban regeneration on resident health and wellbeing. BMC Public Heal. 2021, 21, 1–15. [Google Scholar] [CrossRef] [PubMed]
- McCrae, J.S.; Robinson, J.A.L.; Spain, A.K.; Byers, K.; Axelrod, J.L. The Mitigating Toxic Stress study design: approaches to developmental evaluation of pediatric health care innovations addressing social determinants of health and toxic stress. BMC Heal. Serv. Res. 2021, 21, 1–14. [Google Scholar] [CrossRef]
- Rojas, D.; Melo, A.; Moise, I.K.; Saavedra, J.; Szapocznik, J. The Association Between the Social Determinants of Health and HIV Control in Miami-Dade County ZIP Codes, 2017. J. Racial Ethn. Heal. Disparities 2020, 8, 763–772. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.; Silva, S.; Cline, D.; Freiermuth, C.; Tanabe, P. Social and Behavioral Factors in Sickle Cell Disease: Employment Predicts Decreased Health Care Utilization. J. Heal. Care Poor Underserved 2018, 29, 814–829. [Google Scholar] [CrossRef]
- Wagg, E.; Blyth, F.M.; Cumming, R.G.; Khalatbari-Soltani, S. Socioeconomic position and healthy ageing: A systematic review of cross-sectional and longitudinal studies. Ageing Res. Rev. 2021, 69, 101365. [Google Scholar] [CrossRef]
- Hoisington, A.J.; Stearns-Yoder, K.A.; Schuldt, S.J.; Beemer, C.J.; Maestre, J.P.; Kinney, K.A.; Postolache, T.T.; Lowry, C.A.; Brenner, L.A. Ten questions concerning the built environment and mental health. J. Affect. Disord. 2019, 155, 58–69. [Google Scholar] [CrossRef]
- Dwivedi, E.A.D.P. Maslow Theory Revisited-Covid-19 - Lockdown Impact on Consumer Behaviour. Turk. J. Comput. Math. Educ. (TURCOMAT) 2021, 12, 2445–2450. [Google Scholar] [CrossRef]
- Díaz de León-Martínez, L.; de la Sierra-de la Vega, L.; Palacios-Ramírez, A.; Rodriguez-Aguilar, M.; Flores-Ramírez, R. Critical review of social, environmental and health risk factors in the Mexican indigenous population and their capacity to respond to the COVID-19. Sci. Total. Environ. 2020, 733, 139357–139357. [Google Scholar] [CrossRef]
- Balki, E.; Hayes, N.; Holland, C. Effectiveness of Technology Interventions in Addressing Social Isolation, Connectedness, and Loneliness in Older Adults: Systematic Umbrella Review. JMIR Aging 2022, 5, e40125. [Google Scholar] [CrossRef]
- Marzo, R.R.; Khanal, P.; Shrestha, S.; Mohan, D.; Myint, P.K.; Su, T.T. Determinants of active aging and quality of life among older adults: systematic review. Front. Public Heal. 2023, 11, 1193789. [Google Scholar] [CrossRef]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef] [PubMed]
- Zhang Y, Tzortzopoulos P, Kagioglou M. Healing built-environment effects on health outcomes: Environment–occupant–health framework. Building research & information. 2019, 47, 747–66. [Google Scholar]
- Mashaly, E.T.; Elsayad, N.A.E.; El-Gezawy, L.S.E.-D. THE INFLUENCE OF THE SENSUAL ENVIRONMENT OF THE URBAN SPACE ON THE USERS. Bull. Fac. Eng. Mansoura Univ. 2020, 42, 1–12. [Google Scholar] [CrossRef]
- Almaz, A.F.H.; Zeina, A.A.M.A. The Perceived Interaction of Sensory Processing in Internal Space, Architectural Surrounds, and Endless Space. International Design Journal 2023, 13, 331–338. [Google Scholar] [CrossRef]
- Uzosike, T.C.; Jaja, I.D. A household-based survey of the morbidity profile of under-five children in Port Harcourt Metropolis, Southern Nigeria. Pan Afr. Med J. 2022, 42, 182. [Google Scholar] [CrossRef]
- Okwakpam, A.N.; Ohochukwu, C.P. Rural Insecurity and Urbanization: Empirical Evidence from Port Harcourt, Rivers State, Nigeria. IIARD International Journal of Geography and Environmental Management. E-ISSN 2504-8821 P-ISSN 2695- 1878, 2022, 8:1 wwwiiardjournalsorg. [Google Scholar]
- Serdar, C.C.; Cihan, M.; Yücel, D.; A Serdar, M. Sample size, power and effect size revisited: simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Medica 2021, 31, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Vimont, A.; Leleu, H.; Durand-Zaleski, I. Machine learning versus regression modelling in predicting individual healthcare costs from a representative sample of the nationwide claims database in France. Eur. J. Heal. Econ. 2021, 23, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Hirose, M. Mixed methods and survey research in family medicine and community health. Fam. Med. Community Heal. 2019, 7, e000086. [Google Scholar] [CrossRef]
- Tie, Y.C.; Birks, M.; Francis, K. Grounded theory research: A design framework for novice researchers. SAGE Open Med. 2019, 7. [Google Scholar] [CrossRef]
- Proudfoot, K. Inductive/Deductive Hybrid Thematic Analysis in Mixed Methods Research. J. Mix. Methods Res. 2022, 17, 308–326. [Google Scholar] [CrossRef]
- Finlay, J.M.; Kobayashi, L.C. Social isolation and loneliness in later life: A parallel convergent mixed-methods case study of older adults and their residential contexts in the Minneapolis metropolitan area, USA. Soc. Sci. Med. 2018, 208, 25–33. [Google Scholar] [CrossRef]
- Azuh, D.; Oladosun, M.; Chinedu, S.; Azuh, A.; Duh, E.; Nwosu, J. Socio-demographic and environmental determinants of child mortality in rural communities of Ogun State, Nigeria. 2021.
- Akanbi, M.A. ; Ope BW; Adeloye D.O.; Amoo EO; Iruonagbe T.C.; Omojola, O. Influence of socio-economic factors on the prevalence of teenage pregnancy in Nigeria. African Journal of Reproductive Health, 2021; 25(5s), 138-146.
- Timm, S.; Gray, W.A.; Curtis, T.; Sung, S.; Chung, E. Designing for Health: How the Physical Environment Plays a Role in Workplace Wellness. American Journal of Health, 2018; 32(6), 1468–1473.
- Wolkoff, P.; Nielsen, G.D. Effects by inhalation of abundant fragrances in indoor air – An overview. Environ. Int. 2017, 101, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.T.Q.; Navaratnam, S.; Mendis, P.; Zhang, K.; Barnett, J.; Wang, H. Fire safety of composites in prefabricated buildings: From fibre reinforced polymer to textile reinforced concrete. Compos. Part B Eng. 2020, 187, 107815. [Google Scholar] [CrossRef]
- Lachance, C.C.; Jurkowski, M.P.; Dymarz, A.C.; Robinovitch, S.N.; Feldman, F.; Laing, A.C.; Mackey, D.C. Compliant flooring to prevent fall-related injuries in older adults: A scoping review of biomechanical efficacy, clinical effectiveness, cost-effectiveness, and workplace safety. PLOS ONE 2017, 12, e0171652. [Google Scholar] [CrossRef] [PubMed]
- Pinkus, R.T. Love and Belongingness Needs. In: Zeigler-Hill, V., Shackelford, T.K. (eds) Encyclopedia of Personality and Individual Differences. Springer, Cham. 2020. [CrossRef]
- Cameron, J.J.; Granger, S. Self-Esteem and Belongingness. In: Zeigler-Hill, V., Shackelford, T.K. (eds) Encyclopedia of Personality and Individual Differences. Springer, Cham. 2020:4749-51. [CrossRef]
- Dienst, F.; Forkmann, T.; Schreiber, D.; Höller, I. Attachment and need to belong as moderators of the relationship between thwarted belongingness and suicidal ideation. BMC Psychol. 2023, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Barbour, E.K.; Smallwood, S.W.; Hurt, Y. Examining social activity, need to belong, and depression among college students. J. Am. Coll. Heal. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lunen, J.C. Reflection, Sense of Belonging, and Empathy in Medical Education—Introducing a “Novel” Model of Empathetic Development by Literature. J. Med Educ. Curric. Dev. 2023, 10. [Google Scholar] [CrossRef]
- Rijnaard, M.D.; van Hoof, J.; Janssen, B.M.; Verbeek, H.; Pocornie, W.; Eijkelenboom, A.; Beerens, H.C.; Molony, S.L.; Wouters, E.J.M. The Factors Influencing the Sense of Home in Nursing Homes: A Systematic Review from the Perspective of Residents. J. Aging Res. 2016, 2016, 1–16. [Google Scholar] [CrossRef]
- van Hoof, J.; Janssen, M.L.; Heesakkers, C.M.C.; van Kersbergen, W.; Severijns, L.E.J.; Willems, L.A.G.; Marston, H.R.; Janssen, B.M.; Nieboer, M.E. The Importance of Personal Possessions for the Development of a Sense of Home of Nursing Home Residents. J. Hous. Elder. 2016, 30, 35–51. [Google Scholar] [CrossRef]
- Center for Population Health. Healthy Built Environment Checklist. NSW Ministry of Health. 2020. https://www.health.nsw.gov.au/urbanhealth/Publications/healthy-built-enviro-check.
- Soga, M.; Gaston, K.J.; Yamaura, Y. Gardening is beneficial for health: A meta-analysis. Prev. Med. Rep. 2017, 5, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Ndibuagu, E.O.; Omotowo, B.I.; Chime, O.H. Patients Satisfaction with Waiting Time and Attitude of Health Workers in the General Outpatient Department of a State Teaching Hospital, Enugu State, Nigeria. Int. J. Trop. Dis. Heal. 2020, 1–10. [Google Scholar] [CrossRef]
- Worth, P.; Smith, M.D. Clearing the Pathways to Self-Transcendence. Front. Psychol. 2021, 12, 648381. [Google Scholar] [CrossRef]
- Abdullah, F. Senada: Harmonising Architectural Elements for the Recovery of Post-partum Depression. Design Ideals Journal, 2021; 3(1). https://journals.iium.edu.my/kaed/index.php/dij/article/view/637.
- Weclawowicz-Bilska, E.; Wdowiarz-Bilska, M. Revitalisations in Polish Health Resorts vs. European Measures. IOP Conf. Series: Mater. Sci. Eng. 2019, 471, 112049. [Google Scholar] [CrossRef]
- Ahmed, S.A.K.S.; Ajisola, M.; Azeem, K.; Bakibinga, P.; Chen, Y.-F.; Choudhury, N.N.; Fayehun, O.; Griffiths, F.; Harris, B.; Kibe, P.; et al. Impact of the societal response to COVID-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: results of pre-COVID and COVID-19 lockdown stakeholder engagements. BMJ Glob. Heal. 2020, 5, e003042. [Google Scholar] [CrossRef] [PubMed]
- Mobosi, I.A.; Okonta, P.O.; Ameh, C.A. Socio-economic determinants of demand for healthcare utilization in Nsukka Local Government Area of Enugu State Nigeria. Afr. Soc. Sci. Humanit. J. 2022, 3, 22–35. [Google Scholar] [CrossRef]
- Shen, Y.; Tao, Y. Associations between spatial access to medical facilities and health-seeking behaviors: A mixed geographically weighted regression analysis in Shanghai, China. Appl. Geogr. 2022, 139, 102644. [Google Scholar] [CrossRef]
- Siyoum, M.; Teklesilasie, W.; Alelgn, Y.; Astatkie, A. Inequality in healthcare-seeking behavior among women with pelvic organ prolapse: a systematic review and narrative synthesis. BMC Women's Heal. 2023, 23, 1–10. [Google Scholar] [CrossRef]
- Algren, M.H.; Ekholm, O.; Nielsen, L.; Ersbøll, A.K.; Bak, C.K.; Andersen, P.T. Social isolation, loneliness, socioeconomic status, and health-risk behaviour in deprived neighbourhoods in Denmark: A cross-sectional study. SSM - Popul. Heal. 2020, 10, 100546. [Google Scholar] [CrossRef]
- Grifferty, G.; Shirley, H. ; McGloin, /.J.; Kahn, J.; Orriols, A.; Wamai, R. Vulnerabilities to and the Socioeconomic and Psychosocial Impacts of the Leishmaniases: A Review. Res. Rep. Trop. Med. 12. [CrossRef]
Figure 1.
Structure of the Research Methodology; Source: Authors (2024).
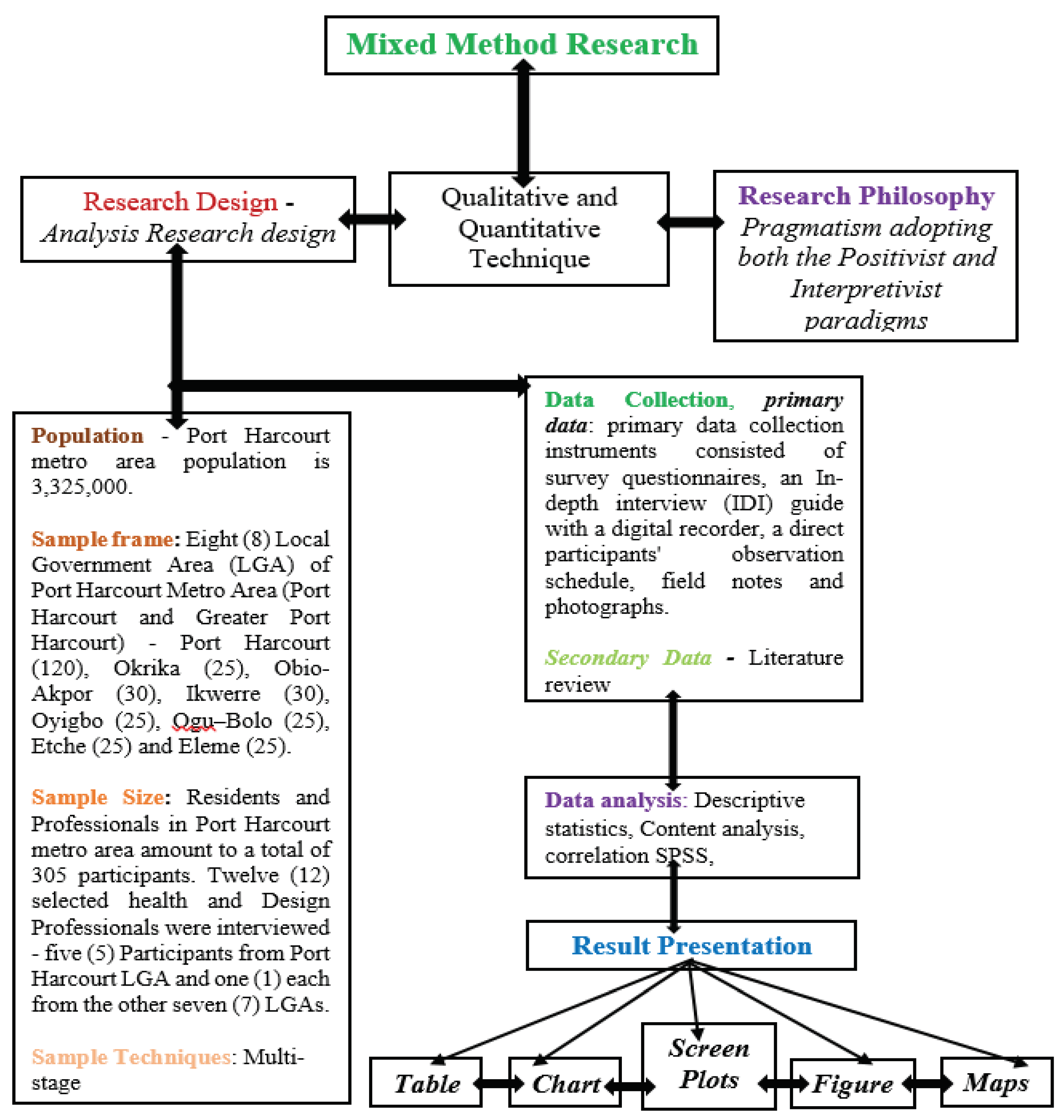
Figure 2.
Socio-economic Characteristics of Health Resort Users.
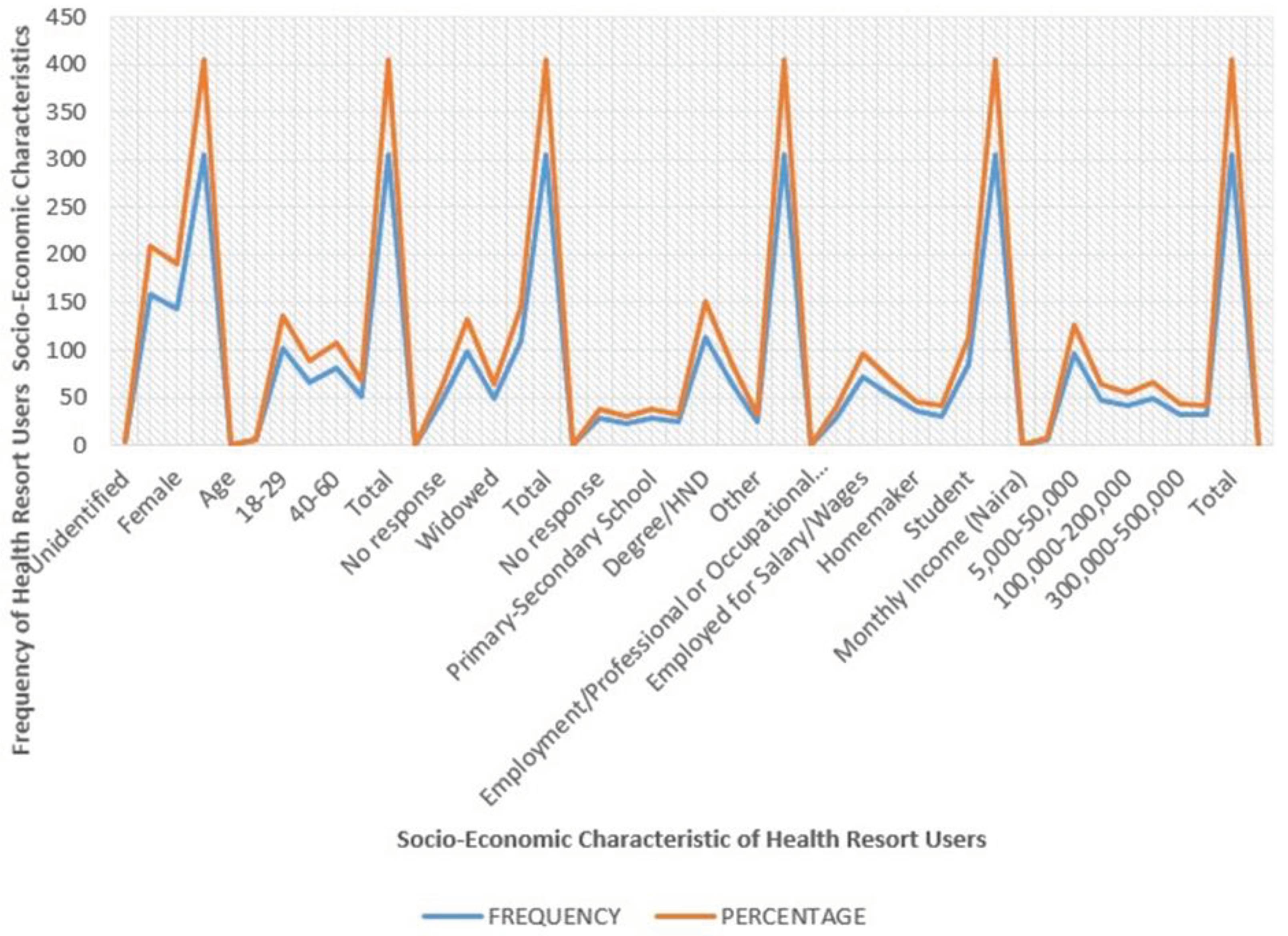

Table 1.
Demographic Information of the Participants.
| S/N | Name | Age | Sex | Marital Status |
Education | Occupation | Years of experience |
|---|---|---|---|---|---|---|---|
| 1 | AB | 52 | M | Married | MD | Medical Doctor | 25 |
| 2 | KSA | 55 | M | Married | PhD | Psychiatrist | 30 |
| 3 | LBO | 61 | M | Married | MBChB | Medical Doctor | 35 |
| 4 | SA | 56 | M | Married | M.PH | Public health | 28 |
| 5 | ED | 55 | M | Married | PhD | Biomedical Engineer | 26 |
| 6 | SY | 47 | F | Married | MD | Medical Doctor | 24 |
| 7 | QC | 52 | F | Married | PhD | Quantity surveyor | 26 |
| 8 | BB | 32 | M | Married | M.Sc. | Architect | 17 |
| 9 | AC | 65 | M | Married | B.Eng. | Civil Engineer | 35 |
| 10 | OA | 39 | M | Married | PhD | Medical Doctor | 15 |
| 11 | YM | 46 | M | Married | MBBS | Medical Doctor | 19 |
| 12 | HA | 43 | F | Married | PhD | Architect | 20 |
| Note: Mean Age: 42.3, Mean Years of E: 25.4 MD- Doctor of Medicine, PhD- Doctor of Philosophy, MBChB- Bachelor of Chirurgery, M.PH- Master of Public Health, M.Sc.-Master of Science, B.Eng.-Bachelors of Engineering, MBBS- Bachelor of Surgery, M-Male, F-Female | |||||||
Table 2.
Number of Questionnaires Administered and the Response Rate.
| S/N | Port Harcourt Metro Area (Port Harcourt and Greater Port Harcourt – Eight (8) Local Government Areas (LGA) | No. of Questionnaires administered | No. of questionnaires retrieved | Response Rate (%) |
|---|---|---|---|---|
| 1 | Port Harcourt LGA (PHALGA) | 150 | 120 | 80 |
| 2 | Okrika LGA | 38 | 25 | 66 |
| 3 | Obio-Akpor LGA | 39 | 30 | 77 |
| 4 | Ikwerre LGA | 40 | 30 | 75 |
| 5 | Oyigbo LGA | 34 | 25 | 74 |
| 6 | Ogu–Bolo LGA | 34 | 25 | 74 |
| 7 | Etche LGA | 34 | 25 | 74 |
| 8 | Eleme LGA | 38 | 25 | 74 |
| Total | 399 | 305 | 76% | |
Table 3.
Selected Local Governments and Health Facilities.
| S/N | Port Harcourt (PH) Metro Area (PH and Greater pH – Eight (8) Local Government Areas (LGA) |
Health Facilities in respective Local Government Areas (LGA) |
|---|---|---|
| 1 | Port Harcourt LGA (PHALGA) | Military Hospital, New Mile One Hospital & Rivers State University Teaching Hospital |
| 2 | Okrika LGA | Okrika General Hospital |
| 3 | Obio-Akpor LGA | University of Port Harcourt Teaching Hospital |
| 4 | Ikwerre LGA | General Hospital Isiokpo |
| 5 | Oyigbo LGA | Heritage Medicare Hospital |
| 6 | Ogu–Bolo LGA | General Hospital Ogu |
| 7 | Etche LGA | Okomoko General Hospital |
| 8 | Eleme LGA | General Hospital, Ebubu Eleme |
| Total | 10 | |
Table 4.
Sixteen (16) Psycho-social Characteristics Measured.
| S/N | Psycho-Social Characteristic | Maslow’s Tier Of Human Need | Empirical Support |
|---|---|---|---|
| 1. | Water Quality | Biological and Physiological | [2,54,55,72,73] |
| 2. | Air Quality | Biological and Physiological | |
| 3. | Thermal Comfort | Biological and Physiological | |
| 4. | Quality of Sleep | Biological and Physiological | [2,59,74] |
| 5. | Sense of Safety | Safety | [2,75] |
| 6. | Orderliness | Safety | [9] |
| 7. | Quality of Intimate Atmosphere | Belongingness and Love | [76] |
| 8. | Sense of Trust and Acceptance | Belongingness and Love | [77,78,79] |
| 9. | Value of Lasting Relationships | Belongingness and Love | [80,81] |
| 10. | Features Befit Status | Esteem Needs | [54] |
| 11. | Self Esteem | Esteem Needs | |
| 12. | Sense of Home | Aesthetics and Belongingness and Love | [14,82,83] |
| 13. | Unwind and Rejuvenate | Self-actualisation | [54] |
| 14. | Social Ties, Relationships, Group Work | Belongingness and Love | [52,55,84,85] |
| 15. | Sense of Place and Privacy | Transcendence and Self-actualisation | [86,87] |
| 16. | Aesthetic Experience | Aesthetic | [88,89] |
Table 5.
Descriptive Means of Psycho-social Characteristics of Health Resort Users across Component Facilities of a Health Resort.
Table 5.
Descriptive Means of Psycho-social Characteristics of Health Resort Users across Component Facilities of a Health Resort.
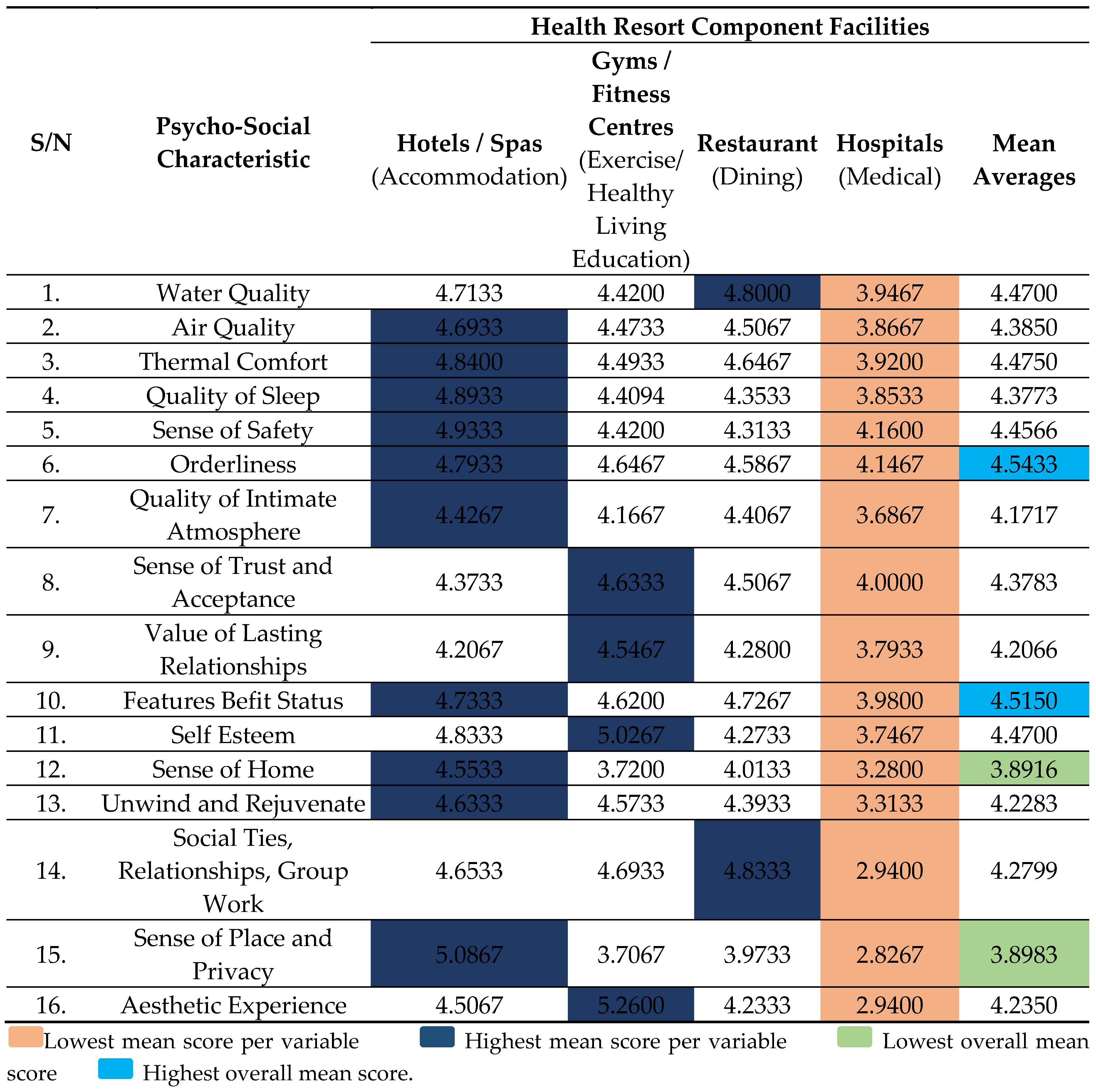
Table 6.
It shows a connection between Users’ educational qualifications and access to facilities that benefit their status.
Table 6.
It shows a connection between Users’ educational qualifications and access to facilities that benefit their status.
| S/N | Psycho-Social Characteristic | Hotel | GYM | Restaurant | Hospital |
|---|---|---|---|---|---|
| 1 | Water Quality | 0.078 | *0.187 | 0.157 | 0.058 |
| 2 | Air Quality | - 0.074 | 0.130 | 0.027 | - 0.004 |
| 3 | Thermal Comfort | 0.067 | 0.096 | 0.142 | - 0.052 |
| 4 | Quality of Sleep | - 0.002 | 0.135 | 0.121 | 0.063 |
| 5 | Sense of Safety | 0.098 | 0.113 | 0.067 | 0.080 |
| 6 | Orderliness | *0.169 | 0.141 | 0.090 | 0.067 |
| 7 | Quality of Intimate Atmosphere | 0.030 | 0.093 | 0.012 | - 0.004 |
| 8 | Sense of Trust and Acceptance | 0.095 | *0.185 | 0.070 | 0.034 |
| 9 | Value of Lasting Relationships | 0.085 | 0.125 | *0.162 | 0.065 |
| 10 | Features Befit Status | 0.118 | *0.177 | *0.174 | - 0.025 |
| 11 | Self Esteem | 0.081 | 0.150 | 0.042 | - 0.008 |
| 12 | Sense of Home | 0.001 | 0.102 | 0.129 | - 0.002 |
| 13 | Unwind and Rejuvenate | 0.054 | -0.015 | - 0.001 | 0.040 |
| 14 | Social Ties, Relationships, Group Work | 0.087 | 0.081 | 0.004 | 0.116 |
| 15 | Sense of Place and Privacy | - 0.009 | 0.051 | 0.071 | 0.035 |
| 16. | Aesthetic Experience | - 0.028 | 0.074 | - 0.033 | 0.137 |
*Highlighted r-values reflect variables which returned significant results at an α-level of 5% (0.05)
Table 7.
It shows a correlation between Monthly Income and access to facilities that benefit their status.
Table 7.
It shows a correlation between Monthly Income and access to facilities that benefit their status.
| S/N | Psycho-Social Characteristic | Hotel | GYM | Restaurant | Hospital |
|---|---|---|---|---|---|
| 1 | Water Quality | 0.031 | 0.076 | 0.051 | 0.155 |
| 2 | Air Quality | *- 0.213 | 0.068 | - 0.044 | 0.108 |
| 3 | Thermal Comfort | - 0.089 | 0.097 | 0.044 | 0.069 |
| 4 | Quality of Sleep | *- 0.196 | *0.174 | 0.044 | 0.065 |
| 5 | Sense of Safety | *- 0.176 | 0.084 | - 0.083 | 0.039 |
| 6 | Orderliness | - 0.022 | 0.074 | - 0.017 | 0.094 |
| 7 | Quality of Intimate Atmosphere | - 0.092 | 0.123 | - 0.079 | 0.180 |
| 8 | Sense of Trust and Acceptance | - 0.040 | 0.121 | 0.004 | 0.105 |
| 9 | Value of Lasting Relationships | 0.149 | - 0.040 | 0.027 | *0.162 |
| 10 | Features Befit Status | 0.061 | 0.089 | - 0.058 | 0.061 |
| 11 | Self Esteem | - 0.150 | - 0.027 | - 0.019 | 0.076 |
| 12 | Sense of Home | - 0.086 | 0.018 | 0.010 | 0.116 |
| 13 | Unwind and Rejuvenate | 0.112 | - 0.096 | - 0.142 | 0.033 |
| 14 | Social Ties, Relationships, Group Work | 0.108 | 0.057 | - 0.017 | *0.166 |
| 15 | Sense of Place and Privacy | - 0.042 | 0.134 | 0.009 | 0.088 |
| 16 | Water Quality | - 0.040 | - 0.021 | - 0.115 | - 0.061 |
*Highlighted r-values reflect variables which returned significant results at an α-level of 5% (0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



