
Submitted:
25 March 2024
Posted:
26 March 2024
You are already at the latest version
Abstract
Background: Factors that could predict which patients will benefit from Immune Checkpoint Inhibitors (ICIs) are not fully understood. This study aimed to investigate the prognostic value of KRAS biomarker in patients with advanced non-small cell lung cancer (NSCLC) in relation to clinical characteristics, treatment response and PDL1 expression. Patients and methods: The study included 100 patients with NSCLC who received immunotherapy with or without chemotherapy as 1st line treatment. In biopsy samples, the PDL1 biomarker expression rate and somatic mutations of KRAS gene were determined. Results: The mean age of the patients was 67 ± 8 years. Patients were all male and 66% were found with adenocarcinoma whereas 34% with squamous cell carcinoma. The KRAS G12C mutation was found with the highest percentage (73%). In the Kaplan-Meier survival analysis, patients with PDL1>49% in combination with a negative KRAS result had a median survival of 40 months compared to patients with a positive KRAS result (9 months, p<0.05). In addition, patients diagnosed with adenocarcinoma, PDL1<49% and negative KRAS result had a median survival of 39 months compared to patients with a positive result (28 months, p<0.05). Conclusions: Our study suggests that the presence of KRAS mutations in advanced NSCLC patients has a poor prognostic value, regardless of their PDL1 expression values, after receiving immunotherapy as first-line treatment.
Keywords:
lung cancer
; KRAS
; PDL1
; immunotherapy
; survival
1. Introduction
According to the World Health Organization (WHO), lung cancer is still the leading cause of cancer-related deaths worldwide and the second most common cancer in Europe, after breast cancer [1]. Recently, the development of immunotherapy based on the theory that the immune system plays a protective role by recognizing cancer cells has led to considerable progress in the treatment of non–small-cell lung cancer (NSCLC) with a substantial reduction in mortality [2]. Despite the benefits that have been established with immunotherapy in the metastatic setting, there are still many patients that do not benefit from this treatment regardless the PDL1 expression status, indicating the need to identify novel predictive factors [3,4]. In addition, spatial and temporal heterogeneity of the solid tumor is the main obstacle for consistency in PDL1 testing [5]. Currently, PDL1 expression remains a predictive biomarker for response to single-agent immunotherapy, to median progression free survival, to median overall survival and clinical outcome. Besides, the efforts to better identify cancer patients have led to the approvals of targeted therapies for patients with specific oncogenic driver mutations. Checkpoint inhibitors have also been improved for patients without an actionable driver mutation given either as monotherapy or in combination with chemotherapy. However, the prognosis for advanced NSCLC patients remains unsatisfactory, with a median progression-free survival of only 2 to 4 months associated with chemotherapy agents or checkpoint inhibitors [6]. Predictive and prognostic biomarkers are at need to help physicians determine subgroup of patients who may benefit from specific treatments.
Concerning the targeted therapies, the most prevalent genomic driver event in NSCLC is activating mutations in Kirsten rat sarcoma viral oncogene homologue (KRAS) in about 25 to 30% of non–squamous-cell NSCLCs in Western countries [7]. The most common KRAS mutation subtype is the G12C mutation, which accounts for approximately 13% of all KRAS mutations in NSCLC [8]. Other less common KRAS mutation subtypes include G12D, G12V, G13C, and Q61H/L which have been implicated with differences in the prognosis and response to treatment in KRAS positive patients [9,10]. KRAS mutations are found with different frequencies in males than in females and vary also according to patient ethnicity [11] and in specific they are more common in Western versus Asian patients (26% versus 11%) [12]. In addition, they are more commonly found in patients with a history of smoking (30% versus 11%) [13]. Furthermore, it has been reported that KRAS mutations are more common in adenocarcinoma (20–40%) and less common in squamous cell carcinoma (<5%) [14].
Overall, KRAS mutations constitute a distinct NSCLC subset of patients as KRAS mutations where standard of care provides modest clinical benefit. It has also been demonstrated that KRAS mutations are mutually exclusive with other oncogene mutations such as epidermal growth factor receptor (EGFR) mutations [15]. Several meta-analyses have tried to elucidate the prognostic value of KRAS mutation in patients with advanced NSCLCs, however with inconsistent results [8,15,16]. Thus, there is a need to further clarify the role of KRAS mutations in overall survival of NSCLC patients.
The aim of the current retrospective cohort study was the investigation of the role of KRAS mutational status as predictive biomarker on overall survival (OS) and its relation to PDL1 expression and other clinical characteristics of patients diagnosed with advanced NSCLC after receiving immunotherapy with or without platinum-based chemotherapy.
2. Patients and Methods
2.1. Study Cohort
This is a monocenter retrospective study of patients followed up in Pulmonary-Oncology Unit of ‘Theageneio’ Cancer Hospital in Thessaloniki, approved by the Local Ethics Committee of the same Hospital. We included 100 patients with pathologically documented with locally advanced or metastatic NSCLC according to World Health Organization classification and guidelines [17], who had disease progression after the receipt of anti–programmed death 1 (PD-1) immunotherapy (pembrolizumab, nivolumab, ipilimumab and atezolizumab) or after the receipt of both immunotherapy and platinum-based chemotherapy according to ASCO guidelines [1,18]. Response assessment was performed after 2 cycles, then every 2-4 cycles with CT of known or high-risk sites of disease with or without contrast. Patients enrolled in the analysis had either no adverse events due to immunotherapy or adverse events grade 1 according to the Common Terminology Criteria for Adverse Events (CTCAE) v5.0. and their performance status was between 0-2.
2.2. Genetic Analysis and Immunohistochemistry Analysis
Molecular testing of somatic mutations of the KRAS gene was retrospectively performed with Real-Time PCR technology for each NSCLC patient. KRAS Mutation Test (KRAS-RT50 CE-IVD kit) by EntroGen, Incorporation in the system of Applied Biosystems ABI 7500 was used, able to investigate 16 mutations in exons 2, 3, 4 of KRAS gene [19]. PDL1 expression was assessed in 5-μm sections cut from formalin-fixed and paraffin-embedded NSCLC tissue blocks using an anti-PDL1 antibody (clone IHC411, GenomeMe, Richmond, Canada) on the LEICA BOND-III platform. Stained slides were then observed under a light microscope to assess positivity. Two pathologists blindly calculated both biomarkers for interobserver and intraobserver variability. The PDL1 tumor proportion score (TPS) was calculated as the percentage of at least 100 viable cancer cells with complete or partial membrane staining. Necrotic areas were excluded from scoring. PDL1 positivity and PDL1 high expression, was defined as staining in ≥1% and ≥49 % of all tumor cells, as used in other clinical trials [20]. No differences were reported among calculations of the two pathologists.
2.3. Statistical Analysis
Statistical analysis was performed using the SPSS (version-21.0 IBM-SPSS-statistical-software, Armonk, NY, USA). Descriptive statistics were performed, and quantitative data were summarized as means with standard deviation (SD). Qualitative variables were summarized as frequencies in the entire population and percentages. Shapiro–Wilk test was performed for normality test. The differences between groups regarding KRAS mutational status, NSCLC histology or PDL1 expression cut-off points were determined with a two-tailed Student’s t-test and Mann–Whitney U test for non-parametric variables. Kaplan-Meier curve with log-rank test was used for survival analyses regarding the comparison of the previous groups. Chi-square was used to compare groups of categorical variables regarding KRAS mutational status and PDL1 expression. Differences were considered statistically significant at p<0.05.
3. Results
3.1. Clinical Characteristics
The mean age of NSCLC patients was 67 ± 8 years old, and all patients were male. The demographics and clinical characteristics are shown in Table 1. Median survival was 15 months. Of the 100 NSCLC samples analyzed, 43% (n=43) harbored a KRAS mutation (Table 2). The prevalence of KRAS mutations was 43% (n=33) among adenocarcinoma (Table 2) and 29% (n=10) among squamous cell carcinoma samples (p<0.05). The smoking status was categorized as never smokers (4%), light smokers (3%) (designated as less than 15 packs per year) and current smokers (93%). Among KRAS mutation status, 46% of current smokers were found positive (Table 2). No statistically significant differences were found in patients with positive KRAS results, among the histology subtypes in relation to clinical characteristics (Table 3). The most common was G12C (72%) followed by the others with of 7% each (G12A, G12D, G12R, G12V) with no statistically significant differences in relation to age and OS (Table 4). KRAS mutational distribution in all NSCLC histology samples appear in Figure 1. No statistically significant difference was found in age between KRAS subtypes.
3.2. Patients’ Survival Regarding KRAS Mutational Status in Relation to NSCLC Histology
Concerning overall survival, statistical significance was found in Kaplan-Meier survival curves for patients diagnosed with adenocarcinoma in relation to KRAS mutational status, (log-rank p value: 0.005) (Figure 2a). Median survival of patients with adenocarcinoma found positive with KRAS mutation was statistical significantly lower when compared to patients with negative KRAS mutation status (25.3 vs 15.1, p<0.001) (Table 2). In addition, statistical significance was found in Kaplan-Meier survival curves for patients with negative KRAS status, when comparing those diagnosed with adenocarcinoma in relation to patients with squamous cell carcinoma, (log-rank p value: 0.001) (Figure 2b), whereas no statistical significance was found in Kaplan-Meier survival curves for patients with positive KRAS status (log-rank p value: 0.501) (Figure 2c). Overall, patients with negative KRAS results, diagnosed with adenocarcinoma were found with better survival compared to those with squamous cell carcinoma (25.3 vs 19.4 months) (Table 2).
3.3. PDL1 Expression in Relation to KRAS Mutational Status and Clinical Characteristics
PDL1 expression was found >49% in 26% of NSCLC patients as appeared in Table 1. PDL1 expression values were distributed across NSCLC histology subtypes with statistical significance (p=0.045). Eleven patients with positive KRAS mutations were found with high values of PDL1 expression (>49%) (Table 2). Higher percentages of patients with PDL1 expression <49% were found in patients diagnosed with adenocarcinoma (Figure 3a). Additional analysis demonstrated that there were no significant differences between PDL1 expression and KRAS mutation subtypes (Figure 3b). Furthermore, no statistically significant difference was found among patients’ response after 6 months of immunotherapy treatment in relation to PDL1 expression and KRAS mutational status (Table 5). The higher percentage (20%) of NSCLC patients with progression disease after 6 months of treatment was found in patients with positive KRAS mutational status with PDL1 expression <49%. In addition, 12% of our cohort with positive KRAS result, were found with partial response, complete response, or standard disease. Besides, Kaplan-Meier survival analysis was performed and patients with PDL1 expression >49% and negative KRAS mutation were found with median survival of 40 months when compared to patients with positive KRAS mutation (9 months, p<0,05), (Figure 4a). Also, Kaplan-Meier survival analysis in patients with PDL1 expression < 49% diagnosed with adenocarcinoma and negative KRAS mutation were found with median survival of 39 months when compared to patients with positive KRAS mutation (28 months, p<0,05), (Figure 4b). As the expression threshold defining positive and negative PDL1 expression is also widely debated, to perform more comparisons in different subgroups, threshold of 1% was also used. However, no significant differences were reported at threshold of 1% as a cutoff point concerning PDL1 expression.
4. Discussion
As the prevalence of KRAS mutations in lung cancer is high, there has been significant interest in developing targeted therapies that specifically address these mutations. Although preclinical and clinical studies have provided encouraging data, there is a notable variation in treatment outcomes, response duration, and resistance mechanisms [21]. Such variations may be influenced by specific co-mutations that are present at the time of diagnosis [22]. Due to this inconsistent response to therapy, the development of effective treatments for lung cancer patients with KRAS mutations remains a challenge. Therefore, there is a need for prognostic biomarkers that can help physicians identify a subgroup of patients who may benefit from certain treatments. To our knowledge, this is the first study conducted in a Greek population that investigated the role of the mutational heterogeneity of KRAS status and its relation to PDL1 expression, as predictive biomarkers in a treated cohort. Our study suggests that the presence of KRAS mutations in advanced NSCLC patients has a poor prognostic value, regardless of their PDL1 expression values, after receiving immunotherapy as first-line treatment.
More specifically, the most significant result in our study was the identification of subgroup of patients negative to KRAS mutations regardless of PDL1 expression values that were found with statistically higher median overall survival when compared to patients with positive KRAS mutation. Our results indicate that KRAS mutational status is a biomarker of poor prognosis. Similarly, in previous studies, KRAS mutational status has been associated with a poorer prognosis in previous studies [23,24]. Additionally, in another study, researchers suggested that KRAS mutation was an independent predictor of worse overall survival in patients with lung adenocarcinoma treated with first line pembrolizumab monotherapy [25]. Besides, in a Danish cohort study, KRAS mutation status was associated with PD-L1 expression in tumors, but not with patient survival [26]. It has also been reported that the impact of KRAS mutations on prognosis may vary depending on the histologic subtype of NSCLC, the smoking history, the stage of the cancer, and the presence of other genetic mutations [27]. In the present study, 33% of patients diagnosed with adenocarcinoma were found with positive KRAS mutations whereas 10% in patients diagnosed with squamous cell carcinoma which is in accordance with previous studies reporting that KRAS mutations are more common in adenocarcinoma and less common in squamous cell carcinoma [14]. Nevertheless, no significant differences were found in patients with positive KRAS results among these two different pathologies, regarding clinical characteristics or survival. However, statistical significance was found in Kaplan-Meier survival curves for patients with negative KRAS status, demonstrating that those diagnosed with adenocarcinoma had better survival prognosis compared to patients with squamous cell carcinoma. Previous studied have already reported that squamous cell carcinoma may be a more malignant type in comparison with adenocarcinoma [28].
Furthermore, in our study, KRAS G12C was the most frequent KRAS mutation in our cohort of patients and was also the most prevalent in current smokers. Our results are in accordance with other studies [9,10,29]. Concerning immunotherapy treatment, we found no statistically significant differences among patients’ response after 6 months in relation to PDL1 expression and KRAS mutational status. According to some studies, tumors with KRAS mutations may have higher levels of PDL1 expression, suggesting that these tumors may be more responsive to immune checkpoint inhibitors [30,31]. In our study, 11 patients (11%) with positive KRAS mutation were found with high values of PDL1 expression (>49%). However, the higher percentage (20%) of NSCLC patients with progression disease after 6 months of immunotherapy treatment with or without chemotherapy was found in patients with positive KRAS mutational status with PDL1 expression <49%. On the contrary, recently, in a small cohort, patients with PDL1 overexpression combined with G12C mutation treated with ICIs as first line of treatment, showed significantly longer progression-free survival [27]. In addition, 12% of our cohort with positive KRAS result and PDL1 expression <49% were reported with partial response, complete response or standard disease. Previous studies suggest that KRAS-mutant lung cancer patients with low PDL1 expression may still benefit from immune checkpoint inhibitor therapy [32]. Moreover, the results of meta-analysis confirmed that anti-PDL1 with chemotherapy or without was better than chemotherapy alone, with greater OS benefit for the subgroup with KRAS-mutant NSCLCs than wild-type KRAS tumors [8]. They suggest that anti-PDL1 therapy could be a reference therapy for evaluating the effectiveness of targeted therapies being developed for KRAS-mutant NSCLC patients, especially the subgroup with the KRAS G12C mutation. Overall, the presence of KRAS mutations may decrease the effectiveness of immunotherapy, regardless of PDL1 expression levels. This information could be useful for clinicians when deciding on the best treatment options for NSCLC patients with KRAS mutations.
One limitation of our study is the size number, to support results for genetic analysis for a population. Another limitation is that no data were available concerning different types of co-mutations that may co-exist with KRAS mutations and may contribute to worse clinical outcomes. Studies have shown that KRAS mutations often co-occur with other genetic alterations in NSCLC, including mutations in TP53 and STK11 or CDKN2A [22,33]. As co-occurring mutations may contribute to more aggressive disease and worse outcomes, understanding their occurrence could help clinicians identify patients who require more aggressive treatment strategies. Besides, it is critical to understand the mechanisms of resistance to KRAS G12C inhibitors [31]. The identification of patients at high risk, could lead to the development of more effective and durable treatment strategies for KRAS-mutant NSCLC.
Recently, sotorasib, formerly AMG 510, a small molecule was approved for 3rd line of treatment in patients with KRAS G12C-mutated NSCLC after previous immunotherapy and/or chemotherapy [34]. It is important to continue conducting research to better understand the impact of KRAS mutations in different treatment contexts [33]. At this concept, a study evaluated KRAS mutations in minor clones in patients with lung adenocarcinoma treated with EGFR-TKI, concluding that KRAS mutations might hinder the effectiveness of anti-EGFR therapy [35]. Furthermore, a Greek study, recently showed that the presence of KRAS mutations resulted in a significantly worse survival among patients receiving platinum-based first line treatment [36]. Future studies could explore the impact of KRAS mutations on prognosis in NSCLC patients receiving different types of treatments, such as chemotherapy or targeted therapies.
5. Conclusions
Our study suggests that the presence of KRAS mutations in advanced NSCLC patients has a poor prognostic value, regardless of their PDL1 expression values, after receiving immunotherapy as first-line treatment. Thus, NSCLC patients with KRAS mutations are likely to have a worse outcome, even if they are treated with immunotherapy as their first-line therapy, regardless of whether they have high or low levels of PDL1 expression. However, the relationship between KRAS mutational status and PDL1 expression remains complex and varies depending on the specific cancer type and other factors and further research is at need.
Author Contributions
Author Contributions: Conceptualization, A.C.; Methodology and Laboratory sample analysis, K.D., A.C.; Patient’s Data, K.K., K.P., P.P., and V.B.; Statistical Analysis: K.D. and E.B.; Writing – Original Draft Preparation, TS and K.D.; Writing – Review & Editing, K.D. T.S. and K.P.; Supervision, A.C.; All authors provided critical feedback and helped shape the research, analysis, and manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and was approved by the Scientific and Ethical Committee of “Theageneio” Cancer Hospital (101_04/FEB/2022).
Informed Consent Statement
Written informed consent was obtained from patients.
Data Availability Statement
The datasets used and/or analyzed during the present study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cordero, R.; Devine, W.P. Targeted Therapy and Checkpoint Immunotherapy in Lung Cancer. Surg Pathol Clin. 2020, 13, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat Rev Cancer. 2016, 16, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Perez-Gracia, J.L.; Han, J.Y.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016, 387, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Wang, S.; Trapani, J.A.; Neeson, P.J. Challenges of PD-L1 testing in non-small cell lung cancer and beyond. J Thorac Dis. 2020, 12, 4541–4548. [Google Scholar] [CrossRef] [PubMed]
- Perol, M.; Felip, E.; Dafni, U.; Polito, L.; Pal, N.; Tsourti, Z.; et al. Effectiveness of PD-(L)1 inhibitors alone or in combination with platinum-doublet chemotherapy in first-line (1L) non-squamous non-small-cell lung cancer (Nsq-NSCLC) with PD-L1-high expression using real-world data. Ann Oncol. 2022, 33, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Carbone, D.P.; Garassino, M.; Barlesi, F. Targeting KRAS in non-small-cell lung cancer: recent progress and new approaches. Ann Oncol. 2021, 32, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- Landre, T.; Justeau, G.; Assie, J.B.; Chouahnia, K.; Davoine, C.; Taleb, C.; et al. Anti-PD-(L)1 for KRAS-mutant advanced non-small-cell lung cancers: a meta-analysis of randomized-controlled trials. Cancer Immunol Immunother. 2022, 71, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Judd, J.; Abdel Karim, N.; Khan, H.; Naqash, A.R.; Baca, Y.; Xiu, J.; et al. Characterization of KRAS Mutation Subtypes in Non-small Cell Lung Cancer. Mol Cancer Ther. 2021, 20, 2577–2584. [Google Scholar] [CrossRef]
- Ricciuti, B.; Alessi, J.V.; Elkrief, A.; Wang, X.; Cortellini, A.; Li, Y.Y.; et al. Dissecting the clinicopathologic, genomic, and immunophenotypic correlates of KRAS(G12D)-mutated non-small-cell lung cancer. Ann Oncol. 2022, 33, 1029–1040. [Google Scholar] [CrossRef]
- Nassar, A.H.; Adib, E.; Kwiatkowski, D.J. Distribution of KRAS (G12C) Somatic Mutations across Race, Sex, and Cancer Type. N Engl J Med. 2021, 384, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Reita, D.; Pabst, L.; Pencreach, E.; Guerin, E.; Dano, L.; Rimelen, V.; et al. Direct Targeting KRAS Mutation in Non-Small Cell Lung Cancer: Focus on Resistance. Cancers (Basel). 2022, 14. [Google Scholar] [CrossRef]
- Chapman, A.M.; Sun, K.Y.; Ruestow, P.; Cowan, D.M.; Madl, A.K. Lung cancer mutation profile of EGFR, ALK, and KRAS: Meta-analysis and comparison of never and ever smokers. Lung Cancer. 2016, 102, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.; Leighl, N.B.; Tsao, M.S.; Shepherd, F.A. KRAS mutations as prognostic and predictive markers in non-small cell lung cancer. J Thorac Oncol. 2013, 8, 530–542. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Byers, L.A.; Diao, L.; Papadimitrakopoulou, V.A.; Tong, P.; Izzo, J.; et al. Co-occurring genomic alterations define major subsets of KRAS-mutant lung adenocarcinoma with distinct biology, immune profiles, and therapeutic vulnerabilities. Cancer Discov. 2015, 5, 860–877. [Google Scholar] [CrossRef] [PubMed]
- Wankhede, D.; Bontoux, C.; Grover, S.; Hofman, P. Prognostic Role of KRAS G12C Mutation in Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Diagnostics (Basel). 2023, 13. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.H.; Robinson, A.G.; Temin, S.; Baker, S.; Jr Brahmer, J.R.; Ellis, P.M.; et al. Therapy for Stage IV Non-Small-Cell Lung Cancer With Driver Alterations: ASCO and OH (CCO) Joint Guideline Update. J Clin Oncol. 2021, 39, 1040–1091. [Google Scholar] [CrossRef] [PubMed]
- Hancer, V.S.; Buyukdogan, M.; Turkmen, I.; Bassullu, N.; Altug, T.; Diz-Kucukkaya, R.; et al. Comparison of KRAS mutation tests in colorectal cancer patients. Genet Test Mol Biomarkers. 2011, 15, 831–834. [Google Scholar] [CrossRef]
- Rebelatto, M.C.; Midha, A.; Mistry, A.; Sabalos, C.; Schechter, N.; Li, X.; et al. Development of a programmed cell death ligand-1 immunohistochemical assay validated for analysis of non-small cell lung cancer and head and neck squamous cell carcinoma. Diagn Pathol. 2016, 11, 95. [Google Scholar] [CrossRef]
- Skoulidis, F.; Goldberg, M.E.; Greenawalt, D.M.; Hellmann, M.D.; Awad, M.M.; Gainor, J.F.; et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discov. 2018, 8, 822–835. [Google Scholar] [CrossRef] [PubMed]
- Adderley, H.; Blackhall, F.H.; Lindsay, C.R. KRAS-mutant non-small cell lung cancer: Converging small molecules and immune checkpoint inhibition. EBioMedicine. 2019, 41, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Mascaux, C.; Iannino, N.; Martin, B.; Paesmans, M.; Berghmans, T.; Dusart, M.; et al. The role of RAS oncogene in survival of patients with lung cancer: a systematic review of the literature with meta-analysis. Br J Cancer. 2005, 92, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Kartolo, A.; Feilotter, H.; Hopman, W.; Fung, A.S.; Robinson, A. A single institution study evaluating outcomes of PD-L1 high KRAS-mutant advanced non-small cell lung cancer (NSCLC) patients treated with first line immune checkpoint inhibitors. Cancer Treat Res Commun. 2021, 27, 100330. [Google Scholar] [CrossRef] [PubMed]
- Noordhof, A.L.; Damhuis, R.A.M.; Hendriks, L.E.L.; de Langen, A.J.; Timens, W.; Venmans, B.J.W.; et al. Prognostic impact of KRAS mutation status for patients with stage IV adenocarcinoma of the lung treated with first-line pembrolizumab monotherapy. Lung Cancer. 2021, 155, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Cronin-Fenton, D.; Dalvi, T.; Movva, N.; Pedersen, L.; Hansen, H.; Fryzek, J.; et al. PD-L1 expression, EGFR and KRAS mutations and survival among stage III unresected non-small cell lung cancer patients: a Danish cohort study. Sci Rep. 2021, 11, 16892. [Google Scholar] [CrossRef] [PubMed]
- Pao, W.; Girard, N. New driver mutations in non-small-cell lung cancer. Lancet Oncol. 2011, 12, 175–180. [Google Scholar] [CrossRef] [PubMed]
- 28. Wen Wang HL, Guoli Li. What’s the difference between lung adenocarcinoma and lung squamous cell carcinoma? Evidence from a retrospective analysis in a cohort of Chinese patients. Front Endocrinol, 2022; 13, 947443.
- Riely, G.J.; Kris, M.G.; Rosenbaum, D.; Marks, J.; Li, A.; Chitale, D.A.; et al. Frequency and distinctive spectrum of KRAS mutations in never smokers with lung adenocarcinoma. Clin Cancer Res. 2008, 14, 5731–5734. [Google Scholar] [CrossRef] [PubMed]
- Toki, M.I.; Mani, N.; Smithy, J.W.; Liu, Y.; Altan, M.; Wasserman, B.; et al. Immune Marker Profiling and Programmed Death Ligand 1 Expression Across NSCLC Mutations. J Thorac Oncol. 2018, 13, 1884–1896. [Google Scholar] [CrossRef]
- Li, Y.; Hu, L.; Peng, X.; Xu, H.; Tang, B.; Xu, C. Resistance to immune checkpoint inhibitors in KRAS-mutant non-small cell lung cancer. Cancer Drug Resist. 2022, 5, 129–146. [Google Scholar] [CrossRef]
- Chen, W.; Li, L.; Cheng, S.; Yu, J. The Efficacy of Immune Checkpoint Inhibitors vs. Chemotherapy for KRAS-Mutant or EGFR-Mutant Non-Small-Cell Lung Cancers: A Meta-Analysis Based on Randomized Controlled Trials. Dis Markers. 2022, 2022, 2631852. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.R.; Rosenberg, S.C.; McCormick, F.; Malek, S. Author Correction: RAS-targeted therapies: is the undruggable drugged? Nat Rev Drug Discov. 2020, 19, 902. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, E.C.; Drezner, N.; Li, X.; Mishra-Kalyani, P.S.; Liu, Y.; Zhao, H.; et al. FDAApproval Summary: Sotorasib for KRASG12C-Mutated Metastatic, N. S.C.L.C. Clin Cancer Res. 2022, 28, 1482–1486. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, A.; Milella, M.; Felicioni, L.; Cappuzzo, F.; Irtelli, L.; Del Grammastro, M.; et al. Clinical implications of KRAS mutations in lung cancer patients treated with tyrosine kinase inhibitors: an important role for mutations in minor clones. Neoplasia. 2009, 11, 1084–1092. [Google Scholar] [CrossRef]
- Linardou, H.; Kotoula, V.; Kouvatseas, G.; Mountzios, G.; Karavasilis, V.; Samantas, E.; et al. Genotyping KRAS and EGFR Mutations in Greek Patients With Non-small-cell Lung Cancer: Incidence, Significance and Implications for Treatment. Cancer Genomics Proteomics. 2019, 16, 531–541. [Google Scholar] [CrossRef]
Figure 1.
a) KRAS mutational distribution in αdenοcarcinoma samples, b) KRAS mutational distribution in Squamous cell carcinoma samples.
Figure 1.
a) KRAS mutational distribution in αdenοcarcinoma samples, b) KRAS mutational distribution in Squamous cell carcinoma samples.
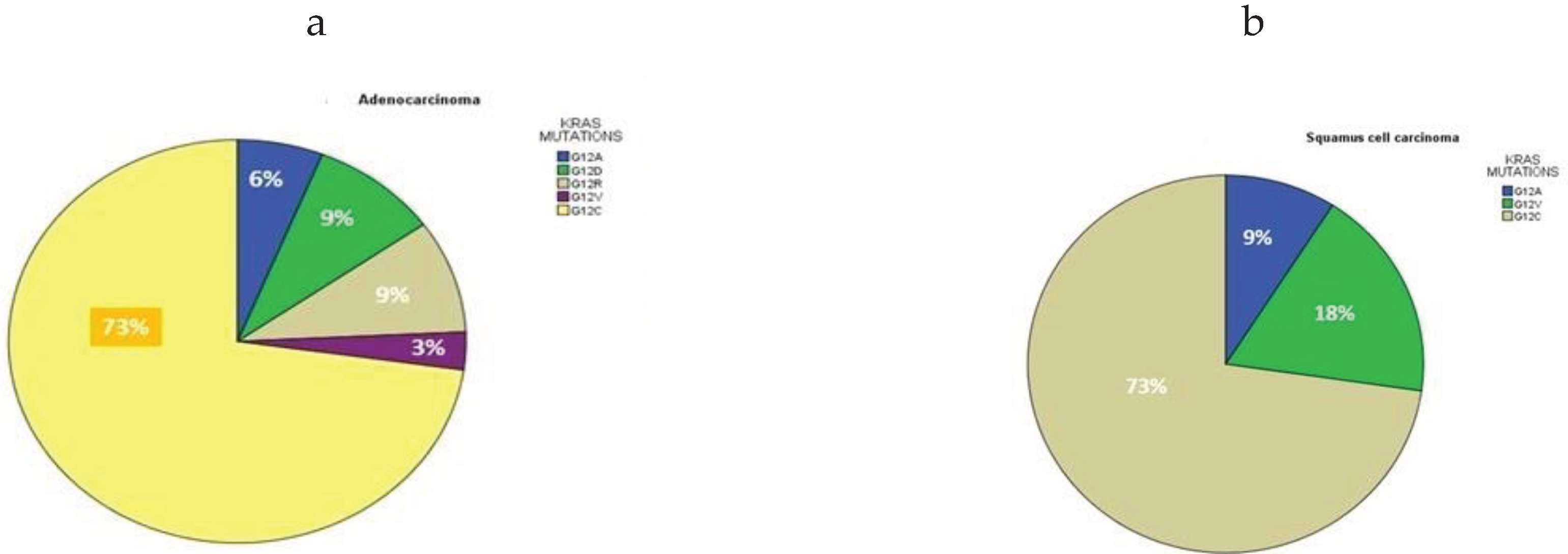
Figure 2.
a) Kaplan-Meier survival curves for patients diagnosed with adenocarcinoma in relation to KRAS mutational status, (log-rank p value: 0.005) b) Kaplan-Meier survival curves for patients with negative KRAS status, diagnosed with adenocarcinoma in relation to patients with squamous cell carcinoma, (log-rank p value: 0.001), c) Kaplan-Meier survival curves for patients with positive KRAS status, diagnosed with adenocarcinoma in relation to patients with squamous cell carcinoma, (log-rank p value: 0.501).
Figure 2.
a) Kaplan-Meier survival curves for patients diagnosed with adenocarcinoma in relation to KRAS mutational status, (log-rank p value: 0.005) b) Kaplan-Meier survival curves for patients with negative KRAS status, diagnosed with adenocarcinoma in relation to patients with squamous cell carcinoma, (log-rank p value: 0.001), c) Kaplan-Meier survival curves for patients with positive KRAS status, diagnosed with adenocarcinoma in relation to patients with squamous cell carcinoma, (log-rank p value: 0.501).
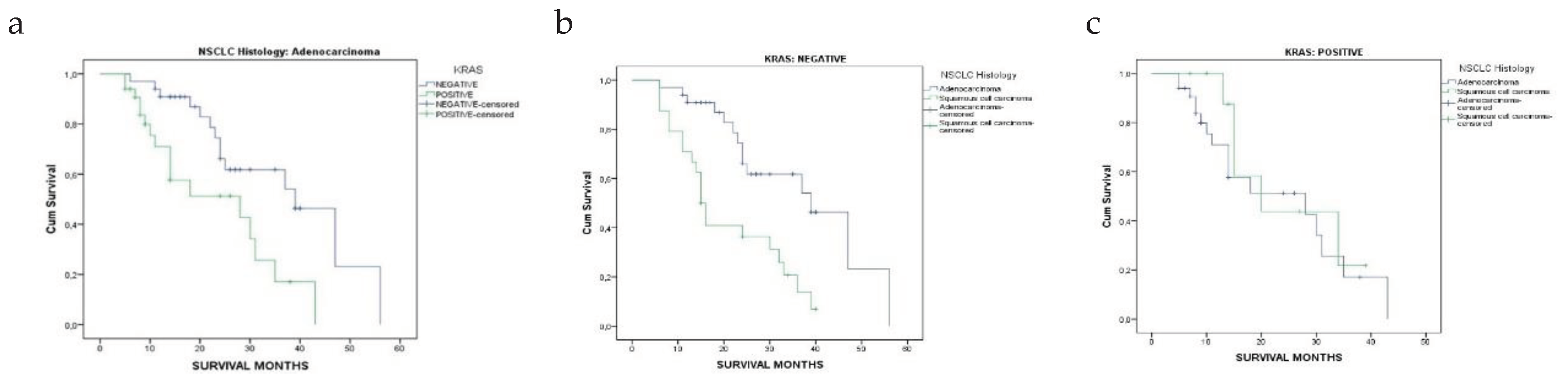
Figure 3.
a) Distribution of PDL1 expression across NSCLC histology subtypes (p<0.05), b) Frequency of KRAS mutation subtypes in PDL1 expression cut offs.
Figure 3.
a) Distribution of PDL1 expression across NSCLC histology subtypes (p<0.05), b) Frequency of KRAS mutation subtypes in PDL1 expression cut offs.
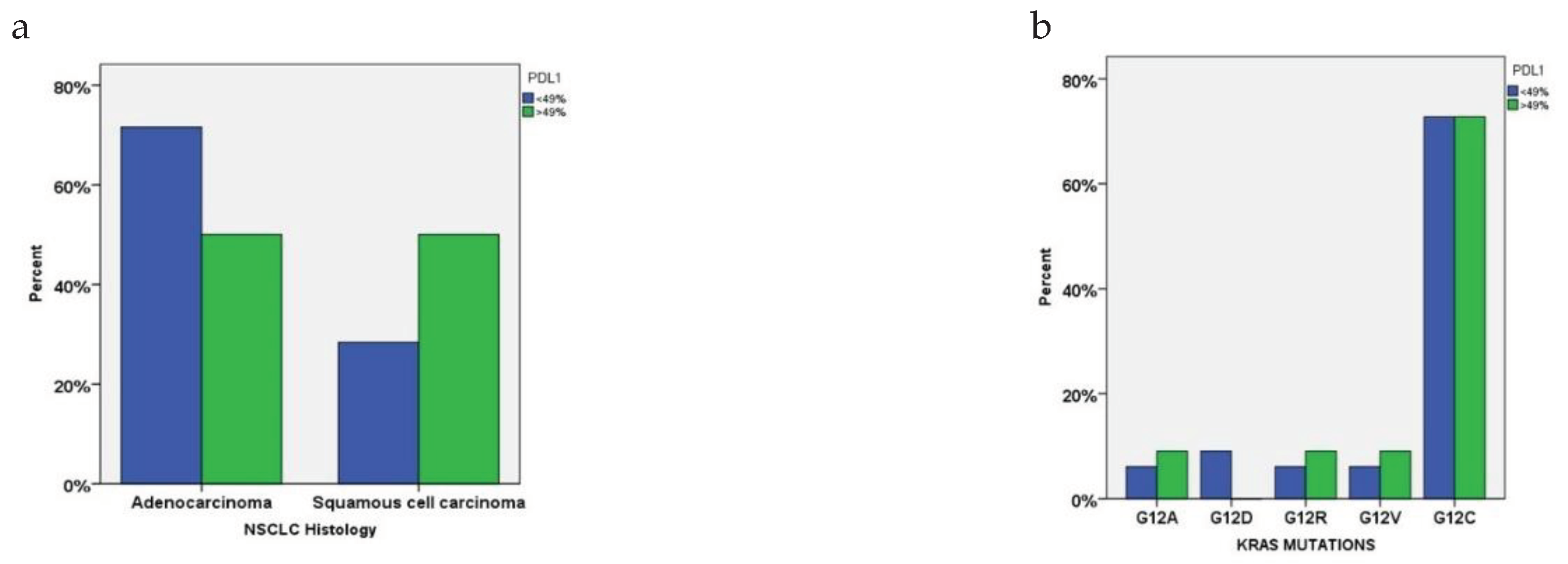
Figure 4.
a) Kaplan-Meier survival curves for NSCLC patients with PDL1 expression >49%, (log-rank p value: 0.013) b) Kaplan-Meier survival curves for patients diagnosed with adenocarcinoma with PDL1 expression <49%, (log-rank p value: 0.023).
Figure 4.
a) Kaplan-Meier survival curves for NSCLC patients with PDL1 expression >49%, (log-rank p value: 0.013) b) Kaplan-Meier survival curves for patients diagnosed with adenocarcinoma with PDL1 expression <49%, (log-rank p value: 0.023).
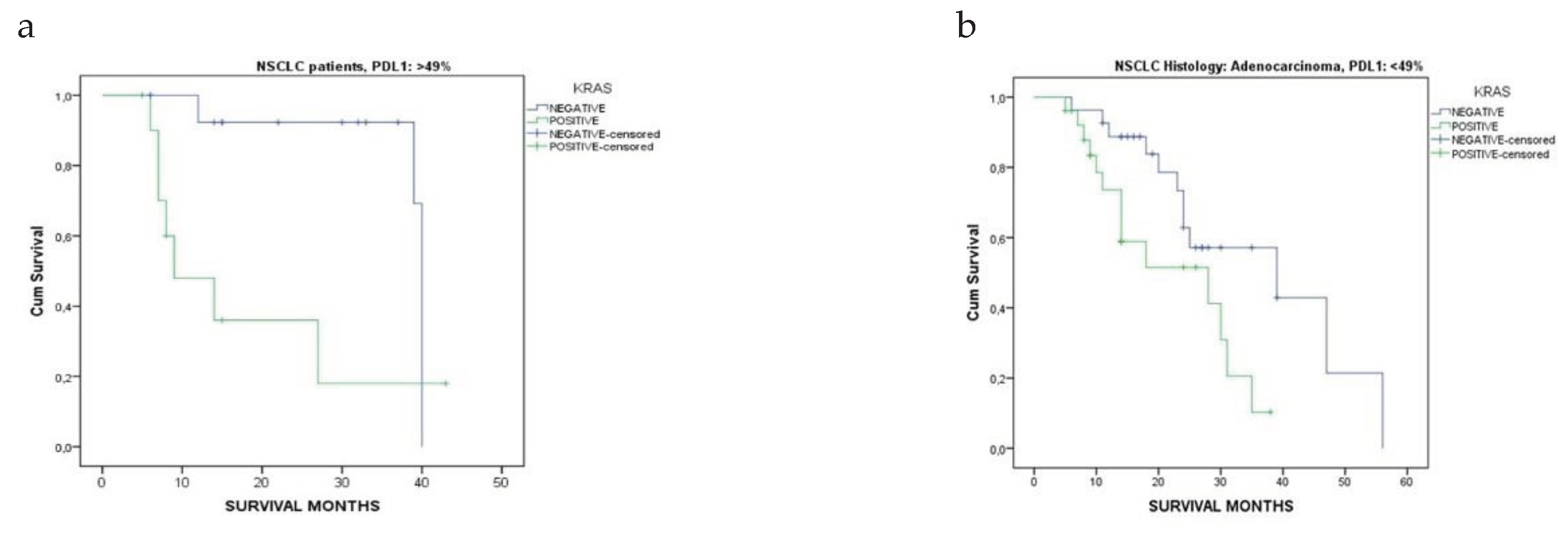

Table 1.
Demographics and clinical characteristics of NSCLC patients included in the study.
| Characteristics | Patients (n=100) |
|---|---|
| Age, mean ± SD, years Age distribution 30-50 40-50 50-60 60-70 70-80 80-90 |
67 ± 8 1% (n=1) 3% (n=3) 13% (n=13) 41% (n=41) 38% (n=38) 4% (n=4) |
| Sex, (Male/Female) | 100%/0% |
| BMI (Mean ± SD) | 26 ± 4.8 |
| Smoking Status Never smokers Light smokers Current smokers |
4% 3% 93% |
| Pack/years | 77 |
| NSCLC Histology Adenocarcinoma/Squamous cell carcinoma |
66%/34% |
| PDL1 expression <49% ≥49% |
74% 26% |
| Overall survival, months, Mean ± SD (Median) | 15 ± 12 (22.5) |
Table 2.
KRAS mutational status distribution across NSCLC patients’ clinical characteristics.
| NEGATIVE KRAS | POSITIVE KRAS |
P-value | |
|---|---|---|---|
| Patients n=100 | 57% | 43% | - |
| PDL1 | |||
| <49% | 74% (n=42) | 74% (n=32) | 0.934 |
| >49% | 26% (n=15) | 26% (n=11) | |
| NSCLC Histology | |||
| Adenocarcinoma | 33% (n=33) | 33% (n=33) | 0.049* |
| Squamous Cell Carcinoma | 24% (n=24) | 10% (n=10) | |
| Smoking status | |||
| Never smokers | 7% (n=4) | 0 | 0.058 |
| Light smokers | 5% (n=3) | 0 | |
| Current smokers | 88% (n=50) | 100% (n=43) | |
| Overall survival, months, Mean ± SD, (Median) | |||
| Adenocarcinoma | 25.3 ± 11.8 [24] | 15.1 ± 10.5 [11] | <0.001* |
| Squamous Cell Carcinoma | 19.4 ± 11.2 [15] | 19.4 ± 10.6 [15] | 1.000 |
*with statistical significant difference p<0.05.
Table 3.
Positive KRAS status distribution across adenocarcinoma and squamous cell carcinoma characteristics.
Table 3.
Positive KRAS status distribution across adenocarcinoma and squamous cell carcinoma characteristics.
| KRAS Positive n=43 |
Adenocarcinoma n=33 |
Squamous Cell Carcinoma n=10 |
p-values |
|---|---|---|---|
| Age, mean ± SD, years | 68.0 ± 5.6 | 63.7 ± 12.1 | 0.782 |
| Age distribution 40-50 50-60 60-70 70-80 |
0 9% (n=3) 36% (n=12) 55% (n=18) |
20% (n=2) 10% (n=1) 40% (n=4) 9% (n=3) |
0.056 |
| PDL1 <49% >49% |
79% (n=26) 21% (n=7) |
60% (n=6) 40% (n=4) |
0.233 |
| Response after 6 months PR CR SD PD |
18% (n=6) 9% (n=3) 12% (n=4) 61% (n=20) |
30% (n=3) 10% (n=1) 20% (n=2) 40% (n=4) |
0.695 |
| Overall survival, months, Mean ± SD, (Median) |
15 ± 10.5 [11] |
19 ± 10.6 [15] |
0.128 |
PR: partial response, CR: complete response, SD: standard disease, PD: progressive disease.
Table 4.
KRAS mutation subtype distribution in age and in overall survival.
| KRAS mutations |
Number of patients n=44 |
Age Years, Mean ± SD |
Median Age | P-value | Overall Survival Months, mean ± SD | Median Survival Months |
P-value |
|---|---|---|---|---|---|---|---|
| G12A | 3 (7%) | 59 ± 4.5 | 59 | 0.232 | 17.0 ±13.1 | 15 | 0.215 |
| G12D | 3 (7%) | 71 ± 2.6 | 70 | 19.6 ± 13.4 | 14 | ||
| G12R | 3 (7%) | 65 ± 9.5 | 60 | 6.6 ± 1.5 | 7 | ||
| G12V | 3 (7%) | 68.3 ± 6 | 69 | 11 ± 4 | 11 | ||
| G12C | 32 (73%) | 67.6 ± 7.9 | 70 | 17 ± 10.6 | 14 | ||
| Total | 44 | 66 ± 8.9 | 65.5 | 23 ± 11.9 | 22.5 | ||
Table 5.
Patients’ response after 6 months of treatment in relation to KRAS mutational status and PDL1 expression.
Table 5.
Patients’ response after 6 months of treatment in relation to KRAS mutational status and PDL1 expression.
| PDL1 expression | Response after 6 months |
KRAS mutational status Negative Positive |
P-values | |
|---|---|---|---|---|
| <49% | PR | 11% | 6% | 0.303 |
| CR | 5% | 2% | ||
| SD | 9% | 4% | ||
| PD | 17% | 20% | ||
| >49% | PR | 5% | 3% | 0.978 |
| CR | 3% | 2% | ||
| SD | 2% | 2% | ||
| PD | 5% | 4% | ||
PR: partial response, CR: complete response, SD: standard disease, PD: progressive disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



