
Submitted:
26 March 2024
Posted:
26 March 2024
You are already at the latest version
Abstract
Background: Amyotrophic lateral sclerosis (ALS) is an incurable disease. There are no defined valid biomarkers for evaluating therapeutic outcomes of this disease. Numerous approaches have been made to meet this impact. Stem cells, one of these approaches, that might give various hopeful results that can be interpreted as a treatment for ALS This study aims to evaluate Mesenchymal Stem Cell (MSC) therapy as a promising novel treatment modality by estimating some parameters, such as immunological and biochemical factors. Methods: This study course involved 15 confirmed patients with ALS and was designed as an open-label, one-arm retrospective study to evaluate potential diagnostic biomarkers of repeated infusions of autologous bone marrow-derived mesenchymal stem cells (BM-MSC) administered at a dose of 1×106cells/kg BW with 1-month interval, in equal amounts in both intravenous (IV) and intrathecal (IT) simultaneously, by various biochemical and immunological parameters were evaluated during the three-month follow-up period. Results: Our study indicated that in the case of Immunological biomarkers ,Tumor Necrosis Factor-alpha (TNF-α) levels in the Cerebrospinal fluid (CSF) showed a significant decrease at month three after transplantation compared to levels at month zero, and the P-value was (P<0.01). No statistically significant changes were observed for other immunological and biochemical parameters and P-value (P>0.05). Conclusions: These results can indicate the benefit of stem cell transfusion in patients with ALS and suggest some diagnostic biomarkers. Several studies are required to approve these results.
Keywords:
ALS
; Tumor Necrosis Factor-alpha
; GDNF
; Creatine kinase
; ferritin
; BM-MSC.
1. Introduction
Amyotrophic lateral sclerosis (ALS) is a disease characterized by an adult neurodegenerative onset with progressive deterioration and loss of cortical and spinal motor neurons. The disease begins as an insidious localized muscle weakness and gradually spreads to impair most skeletal muscles, eventually resulting in total paralysis. Death occurs after a few years due to respiratory failure [1]. To date, there has been no defined treatment for ALS patients, and the available drugs have complementary roles without desirable outcomes[2]. Therefore, it is urgent to find new treatment strategies and specific prognostic and diagnostic biomarkers to speed up treatment in this area. Stem cell therapy is a promising approach in this course[3].
Taking into account that, and according to the cellular and molecular mechanisms involved in this disease's pathogenesis, like neuronal network dysregulation[4]and immune dysfunction[5]. Thus, some related immunological and biochemical parameters might help those with ALS through various mechanisms. Revision of the ALS functional rating scale (ALSFRS) and forced vital capacity (FVC) are considered clinical biomarkers[6]. Furthermore, one of the primary proinflammatory cytokines produced by reactive glia and lead to neuroinflammation are Tumor Necrosis Factor-alpha (TNF-α), interleukin IL-6, and reactive oxygen (RO) [7]. In ALS, many cells, like astrocytes and microglia, can express receptors for TNF-α and excrete this marker [8]. Another significant factor that can be exploited to help identify ALS Neurofilaments (NFs), consisting of Heavy (H), medium (M), and light (L) heteropolymer-based intermediate filament proteins[9], Which expressed by many neurons and serve as intracellular signalling, structural support, and axon development regulation[10]. A neuroprotective factor impact in several neurodegenerative diseases and also enrolled in this study is a glial cell-derived neurotropic factor (GDNF) [11], which increases during embryonic development and gradually decreases in level during adulthood [12] and can participate in axon regeneration, neuropathic pain reduction, and inflammation reduction [13]. On the other hand, iron and its various forms, such as storage form (ferritin) and total iron binding capacity (TIBC), are other indicators of ALS because studies show that iron can be collected in the spinal cord and cerebrospinal fluid in ALS patients [14] and within the skeletal muscles in rat models of ALS[15]. Creatine kinase (CK) is another valuable biochemical indicator of muscle injury in ALS patients [16].
Concerning the above information, the area focus of this study is to estimate the effectiveness of using stem cells as a therapy to help the decline of damaging neurons by estimating some immunological and chemical parameters that can help interpret this type of therapy clinically.
2. Materials and Methods
2.1. Study Design
This study was a single-centre, open-label, retrospective trial without a control group, carried out in 15 defined patients with ALS. All international standards were followed during the trial execution at Pastoor Hospital, Iran [17].
2.2. Participants
Fifteen defined ALS patients, according to El Escorial criteria [18], confirmed by a neurologist's diagnosis, were considered eligible and entered the study. All patients were in the (23-60) years age range, having FVC (> 65%) and a history of ALS disease at least 1 year at the time of admission, and signed an informed written consent form. Additionally, ventilator dependency, any malignancy, or infection 1 week before transplantation were considered exclusion criteria[17].
2.3. Bone Marrow Extraction and Product Preparation
The patient's bone marrow was aspirated under sterile conditions and local anaesthesia to harvest the stem cells used in the injections; a specialist doctor aspirated the samples, and the patients' aspiration sites were examined the day after withdrawal to rule out any adverse reactions.
Mesenchymal stem cells were isolated, cultured, and analyzed in conditions consistent with grade B clean room with good manufacturing practices (GMP). Bone marrow mononuclear cells were isolated using a special centrifugation known as Ficoll density gradient centrifugation (Ficoll-Paque Premium; GE Healthcare Bio-Sciences, Uppsala, Sweden). Peripheral mononuclear cells (PBMC) were raised in special culture media (α-MEM, Lonza, Basel, Switzerland) that had fetal bovine serum (10%) (Life Technologies, Grand Island, USA) and 1% penicillin-streptomycin (Biochrom, Berlin, Germany). Changing the liquid culture medium eliminated cells that did not adhere to the flask. After the non-adherent cells were removed, the culture medium was changed twice a week. When primary BM-MSC cultures reached 80% confluence, cells were harvested, passaged, and treated with 0.125% trypsin-EDTA (Life Technologies, Darmstadt, Germany) based on routine methods. The cell viability rate was between 95% and 98% before transplant. The samples were tested for sterility using endotoxin, Reverse transcription-polymerase chain reaction (RT-PCR), and Bactec tests. Furthermore, the flow cytometry method and differentiation tests were used for MSC characterization based on our previous work. Finally, at a temperature between 2 and 8 Cº and in sterile conditions, the product was transferred to the clinical site.
2.4. BM-MSC Transplantation and Sampling
Stem cells were transplanted to patients in the simultaneous IT (via a lumber puncture in the L3-L4 region, suspended in 2 ml of normal saline) and IV (suspended in 50-60 ml of normal saline) routes at a rate of 1× 106cells/kg BW). All patients received their routine pharmacotherapy during the study, as well.Stem cells were transplanted three times in the patients with a 1-month interval. Also, for biological evaluation, blood samples from patients were collected three times (months -1 (1 month before intervention), 1, and 3), and CSF samples were collected three times (months 0, 1, and 3).
2.5. Immunological Factor Estimation
This study was estimated to have three immunological factors: TNF-α, NFL, and GDNF. Estimation was performed using an Enzyme-Linked Immunosorbent Assay (ELISA) kit for each factor (ZellBio GmbH, Origen; Germany).
2.6. Biochemical Evaluation
Serum iron (Fe), transferrin, ferritin, total iron binding capacity (TIBC), and serum creatine kinase (CK) were evaluated in our study .
The ELISA kit was used for ferritin estimation (DiaMetra, Italy), and the microplate was read at 450 nm. For CK and iron, reagents were used from (Parsazmun, IRAN), and TIBC (biorexfars, IRAN) was tested on an autoanalyzer (Tokyo BoEkI MEDI SYS INC, Japan). Iron was read at 600 nanometers (nm), TIBC at 660 nm, and CK at 340 nm. Transferrin saturation as a percentage was calculated as serum iron / TIBC ×100[19].
2.7. Outcomes
In this study we investigate the safety of repeated transplantation of BM-MSC in ALS patients through evaluate specific immunological and biochemical factors to find diagnostic and/or prognostic biomarkers in this area.
2.8. Statistical Analysis
Statistical analysis was done using the SPSS 23.0 software package (SPSS GmbH Software, Germany). Testing normality was done by using the Shapiro-Wilk test. Generalized Linear Model (GLM) and Repeated Measure ANOVA (RM ANOVA) analysis were used to test the effect of time on normally distributed data. Non-normally distributed continuous variables are reported as the median (interquartile range, IQR). The comparison of the medians between two related groups was made by paired T-test or Wilcoxon signed ranks. Continuous variables are expressed as the mean (for normally distributed data) or median (for non-normally distributed data) ± SEM (standard error of the mean/median). Comparison of the statistical differences of the patient's data was done 3 times (before the intervention, months 1 and 3) for serum, and (months 0, 1, and 3) for CSF samples. The correlation was also estimated by the Spearman test. P-values less than 0.05 were considered as a level of significance. The statistical graphs were created using the Graph Pad Prism8.1 software program (Graph Pad Software, San Diego, CA, USA).
3. Results
3.1. Patients' Characterization and Safety Evaluation
Fifteen patients (11 male and 4 female) participated as published previously . The results were encouraging, demonstrating that MSC transplantation was safe with no significant patient side effects. However, temporary headaches were among the most frequent transplant-related side effects of patients that quickly subsided with supportive therapies. Moreover, the clinical evaluation of ALSFRS showed stability throughout the study (P-value <0.05) , and FVC indicating increasing in trend with significant difference (P-value >0.05), as published previously [17].
3.2. Immunological Assessment
Changes in the level of specific cytokines were investigated three times (months -1, 1, and 3) in serum samples and three times in CSF samples (months 0, 1, and 3) of patients, and the results were as follows.
3.2.1. Tumor Necrosis Factor-Alpha (TNF-α) Levels
As presented in Figure. 1 (A), the initial measurement showed that the serum levels of TNF-α cytokine in patients 1 month before intervention (month -1) were (16.19±1.05) compared to 1 month (16.95±0.40) and 3 months (15.44±1.65) after cell transplantation, the P value was (0.68, 0.66) respectively, which did not change significantly and remained constant.
Furthermore, as shown in Figure. 1 (B), the amount of this cytokine in the CSF of the patients remained statistically constant at month 1 (20.29± 0.68) compared to the beginning of the experiment (19.46± 0.41). However, significant differences were observed between month 3 (16.41±1.49, P= 0.003) and month 0 (baseline), and between month 1 and month 3 (P = 0.007), respectively.
3.2.2. Neurofilament Light Chain (NFL) Levels
Analysis of NFL serum levels showed statistically non-significant differences (P=0.90) at the end of the study (7.62± 1.00) compared to baseline (7.75± 0. .82), and this was the same when comparing month -1 to month one (8.49±0.25), (P=0.56). Indeed, as shown in (Figure 1. C). Serum levels of this cytokine remained stable during the three-month follow-up period of patients after cell transplantation.
Furthermore, measurement of this cytokine in the patient's CSF during the follow-up period showed a non-significant decrease (P=0.23) in its levels at the end of the study (8.28±0.27) compared to baseline (9.41± 0.38). The same results noted in the case of month one (8.31±0.94) compared to month three were observed. (Figure 1. D).
3.2.3. Glial cell-derived neurotrophic factor (GDNF) levels
Serum measurement of GDNF cytokine levels showed that there was no statistically significant change (P=0.90, 0.56) in the amount of this cytokine at the beginning (2.43±0.17) and the end of the experiment (2.44± 0.25) and after one month of receiving the MSCs (2.47±0.23) ( Figure 1. E).
Also, as shown in (Figure 1. F), a slight and non-significant increase (P = 0.21) in month one of transplantation in the amount of this cytokine (3.20± 0.51) compared to the initial amount (2.90±0.02) has been observed in the level of CSF during the follow-up period. For month one (2.91±0.18), non-statically differences were observed compared to baseline.
3.3. Biochemical Evaluation
Changes in the level of specific biochemical factors were investigated three times (months -1, 1, and 3) in serum samples from the patients, and the results were as follows.
3.3.1. Iron (Fe) Levels
Statistical analysis of iron (Fe) levels with a normal range of (23-149 µg/dl) showed that the level of this factor in months -1 (74.55±9.42) in comparison to month1 (67.40±9.16) and month 3 (56.85± 9.91) did not change statistically, (P = 0.62, 0.19), respectively. However, this test showed a gradual decrease in means over these three months, but it was still within the normal range, as mentioned above (Figure 2. A).
3.3.2. Ferritin Levels
The statistical results of ferritin with the normal range of (16.8-276.4 ng/ml), showed that this factor had a decreasing trend during the three months, so its amount at baseline (383.62±92.73) had a statistically non-significant difference compared to month 3 (266.27± 67.07, P=0.34), and this is the same for month 1 (375.40±109.25, P=0.95) (Figure2.B).
3.3.3. Total Iron Binding Capacity (TIBC) Levels
Analysis of TIBC serum levels with the normal range of (239-450 µg/dl) showed statistically non-significant differences (P=0.61) at the end of the study (296.60±14.01) compared to baseline (277.26±25.15). A non-significant increase was also observed during month one (335.36±109.25) was observed as well (Figure 2. C).
3.3.4. Transferrin Levels
3.3.5. Creatine Kinase (CK) Levels
As shown in (Figure 2. E), there was a non-significant difference in serum CK levels (24-195 µ/l) in patients before injection (391.77±152.59) and after one (383.80±195.35, P=0.97) and three (270.13± 171.71, P= 0.60) months of stem cell transplantation, respectively.
3.4. Correlation between Biochemical and Immunological Factors
A significant negative correlation was found between ferritin and TNF-α, the P-values were (0.01). Fe and CK revealed a positive correlation with NFL, and the P value was statically significant (0.02, 0.04), as illustrated in Table 1.
4. Discussion
As published previously [17], the IT and IV transplantation of the bone marrow-derived mesenchyme stem cell (BM-MSC) were safe for ALS patients, did not cause any significant adverse effects, and resulted in early clinical improvement. The most frequent adverse reaction to therapy was a slight headache during observation. Furthermore, during a 3-month follow-up period after cell therapy, FVC levels increased by percentage, while ALSFRS-R did not change statistically. In this study, we further evaluated the effect of stem cell transplantation through estimation of the concentrations of specific immunological and biochemical factors in ALS cases.
Several studies have shown the importance of stem cell transplantation. Mesenchyme stem cell MSCs can play a vital role in controlling immune response through the up-regulation of neuroprotective cytokines like IL-10 and down-regulating proinflammatory cytokines, TNF-α and IL-1 by releasing neurotropic factors and enhancing neurogenesis[21], and this is the same note in different neurological disease[22],[23]. Others showed that Endogenous neural stem cells (NSCs) can differentiate directly into a mature neuron or indirectly into neural progenitor cells (NPCs) [24], according to a study by Zhang, Qi, et al. 2016, Using NSC implantation dramatically led to decline microgliosis and glial markers, proinflammatory cytokine (TNF-α, IL-6, IL-1) expressions and (TLR4) toll-like receptor 4 [25]. Our investigation showed the outcomes regarding TNF-α that decreased in concentration in the case of CSF and was stable in serum samples. One of the important features of muscle atrophy is the destruction of the neuromuscular junction, which leads to motor neuron depletion and accumulation of macrophage and other immunological elements, such as TNF-α that play a principal role in the relapsing of motor neurons [26].
For NFL, this study indicated the stability of NFL levels after transplantation through months in serum and CSF. One study showed that MSC-NTF cells were administrated, which led to a decrease in the level of NFL and pNfH in ALS participants throughout the experimental [27], another revealed the level of NFL would not change in the early trial of studied ALS patients [28]. However, when ALS progression was noted, increased levels of NFL in blood and CSF [29], highlighting the severe impairment to motor neurons and axons [30], and low levels of NFL were linked to functional decline was slower [31]. Other researchers showed that the NFL and phosphorylated NFL (p-NFL) were estimated in the CSF sample in other neurological diseases; for example, patients treated with stem cells in multiple sclerosis revealed stability in concentration [32].In contrast, others showed that the estimated level of CSF NFL was reduced[33].
As another immunological factor, we evaluated GDNF levels in our study after MSC transplantation, which shows a non-significantly increasing trend in serum and CSF samples through the months, which is another promising result. Administration of hematopoietic mesenchymal stem cells (hMSCs) intra-spinally in an ALS rat model increased the rate of survival and improved motor neuron (MN) viability, possibly by up-regulating glial cell line-derived NTF (GDNF) [34,35].
Axon regeneration, reduction of neuropathic pain, reduction of cortical infarction, neurogenesis, and reduction of inflammation are all facilitated by GDNF[13].
In addition, this study showed that iron (Fe) decreased in trend but remained within the normal range. It is well-recognized that changes in cellular iron metabolism can cause oxidative stress ( one of the main causes of ALS pathogenesis)[36]. Iron can be collected in the spinal cord and cerebrospinal fluid in ALS patients[14]; some studies showed an increased level of Fe in plasma[37] and CSF[38] in ALS patients. The decreasing trend of Fe levels after MSC transplantation in our study may be due to the antioxidant properties of these cells[39].
Increased levels of ferritin may be due to inflammation that occurs through the ALS disease. It is possible to consider ferritin as an indicated marker of inflammation related to the severity of the disease [40]; in this study, there was a decrease in the level of ferritin throughout the experiment despite these levels being above the normal range. According to (Goodall EF.etal.,2008). an increased serum ferritin level may indicate elevated stored iron in the body or result in muscle deterioration [41]. A meta-analysis study found the possibility of increased levels of Ferritin, CK, TSC, and FBG and a decrease in the level of TIBC in ALS cases in comparison to control [36], and this may indicate that ALS diseases have multifactorial causes with degeneration of motor neuron activation. Also, changes in muscle masses are one of the signs of ALS disease, and one of the biochemical parameters that can be assessed in this case is CK. According to the study by Hertel et al., increased CK level can increase survival time and provide a good interpretation of the ALSFRS-R score[42]. However, the decreased level was indicated in the case of muscle atrophy [16].
Our result showed a gradual decrease in CK (but still above the normal range) after MSC transplantation, and ALS-FRS showed stability after injection, along with an increase in FVC levels. A positive correlation was noted in this study, interpreted between Fe, CK, and NFL. NFL was noted to play an essential role in neurons through the elastic support capacity that controls the axonal diameter and modulates the stimulation of neuronal response[10]. Furthermore, we also noted a negative correlation between ferritin and TNF-α in our study, Ferritin can prevent iron from creating reactive oxygen species(ROS) and has anti-oxidative effects [43], which is effective in reducing the level of proinflammatory cytokines (like TNF-α). Activated microglia (M1) in ALS leads to TNF-α release [44], and anti-inflammatory microglia (M2) release ferritin in response, which promotes neural reparation [45]. Additionally, a negative correlation between ferritin and GDNF was also indicated in our study, this may be due to Ferritin can participate in inflammation that occurs throughout ALS disease[40,41], and GDNF acts as the anti-inflammatory effect that improves nerve ability [34,35,13].
This study has some limitations, such as a small sample size, a need for a control group, and a short follow-up period. Definitely, larger clinical trials with the control placebo group can confirm these results with precision.
5. Conclusions
According to this study, a significant decrease in the level of TNF-α in the CSF of ALS patients after repeated MSC transplantation after three months of follow-up period. Additionally, the concentration of NFL and GDNF showed stability in levels. Specific biochemical markers also changed favourably but not significantly. To sum up, overall improvement in patient status after cell therapy was a promising result of this study. More studies are needed, including an increasing number of participants and a longer follow-up period, to adequately substantiate the advantageous long-term effectiveness of our strategy in slowing disease development.
Author Contributions
Conceptualization of this draft, J.T.A; Z.A.A; original draft writing, Z.A.A; J.T.A.; review and editing, S.S.N; A.R.B; investigation, Z.A.A; J.T.A; data curation, Z.A.A.; N.K.F; M.A.K. All authors read and agree to published this draft.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was achieved by the rules and morals of the Helsinki Medical Principle of Clinical Practice and under the direction of the Ethics Committee of the Mashhad University of Medical Sciences, Mashhad, Iran. (Reg. No. IR.MUMS.REC.1399.269). Furthermore, this clinical trial was registered with the Iranian Organization for Clinical Trials (ID: IRCT20160809029275N2).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that used in this study can be requested from the corresponding author
Acknowledgments
We thank all employees and patients who helped complete this investigation.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Brown, R.H.; Al-Chalabi, A. Amyotrophic Lateral Sclerosis. N. Engl. J. Med. 2017, 377, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Feldman, E.L.; Goutman, S.A.; Petri, S.; Mazzini, L.; Savelieff, M.G.; Shaw, P.J.; Sobue, G. Amyotrophic Lateral Sclerosis. Lancet 2022, 400, 1363–1380. [Google Scholar] [CrossRef] [PubMed]
- Mazzini, L.; Vescovi, A.; Cantello, R.; Gelati, M.; Vercelli, A. Stem Cells Therapy for ALS. Expert Opin. Biol. Ther. 2016, 16, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Wijesekera, L.C.; Nigel Leigh, P. Amyotrophic Lateral Sclerosis. Orphanet J. Rare Dis. 2009, 4, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Béland, L.-C.; Markovinovic, A.; Jakovac, H.; De Marchi, F.; Bilic, E.; Mazzini, L.; Kriz, J.; Munitic, I. Immunity in Amyotrophic Lateral Sclerosis: Blurred Lines between Excessive Inflammation and Inefficient Immune Responses. Brain Commun. 2020, 2, fcaa124. [Google Scholar] [CrossRef] [PubMed]
- Czaplinski, A.; Haverkamp, L.J.; Yen, A.A.; Simpson, E.P.; Lai, E.C.; Appel, S.H. The Value of Database Controls in Pilot or Futility Studies in ALS. Neurology 2006, 67, 1827–1832. [Google Scholar] [CrossRef] [PubMed]
- Colonna, M.; Butovsky, O. Microglia Function in the Central Nervous System during Health and Neurodegeneration. Annu. Rev. Immunol. 2017, 35, 441. [Google Scholar] [CrossRef] [PubMed]
- Olmos, G.; Lladó, J. Tumor Necrosis Factor Alpha: A Link between Neuroinflammation and Excitotoxicity. Mediators Inflamm. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Yuan, A.; Rao, M.V.; Nixon, R.A. Neurofilaments and Neurofilament Proteins in Health and Disease. Cold Spring Harb. Perspect. Biol. 2017, 9, a018309. [Google Scholar] [CrossRef]
- Sainio, M.T.; Rasila, T.; Molchanova, S.M.; Järvilehto, J.; Torregrosa-Muñumer, R.; Harjuhaahto, S.; Pennonen, J.; Huber, N.; Herukka, S.-K.; Haapasalo, A. Neurofilament Light Regulates Axon Caliber, Synaptic Activity, and Organelle Trafficking in Cultured Human Motor Neurons. Front. cell Dev. Biol. 2022, 9, 820105. [Google Scholar] [CrossRef]
- Barua, S.; Pathak, Y.V. Unilateral Ex Vivo Gene Therapy by GDNF in Neurodegenerative Diseases. In Gene Delivery Systems; CRC Press, 2022; pp. 155–161 ISBN 1003186068.
- Hellmich, H.L.; Kos, L.; Cho, E.S.; Mahon, K.A.; Zimmer, A. Embryonic Expression of Glial Cell-Line Derived Neurotrophic Factor (GDNF) Suggests Multiple Developmental Roles in Neural Differentiation and Epithelial-Mesenchymal Interactions. Mech. Dev. 1996, 54, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Haney, M.J.; Jin, Y.S.; Uvarov, O.; Vinod, N.; Lee, Y.Z.; Langworthy, B.; Fine, J.P.; Rodriguez, M.; El-Hage, N. GDNF-Expressing Macrophages Restore Motor Functions at a Severe Late-Stage, and Produce Long-Term Neuroprotective Effects at an Early-Stage of Parkinson’s Disease in Transgenic Parkin Q311X (A) Mice. J. Control. Release 2019, 315, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Kokić, A.N.; Stević, Z.; Stojanović, S.; Blagojević, D.P.; Jones, D.R.; Pavlović, S.; Niketić, V.; Apostolski, S.; Spasić, M.B. Biotransformation of Nitric Oxide in the Cerebrospinal Fluid of Amyotrophic Lateral Sclerosis Patients. Redox Rep. 2005, 10, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Halon, M.; Kaczor, J.J.; Ziolkowski, W.; Flis, D.J.; Borkowska, A.; Popowska, U.; Nyka, W.; Wozniak, M.; Antosiewicz, J. Changes in Skeletal Muscle Iron Metabolism Outpace Amyotrophic Lateral Sclerosis Onset in Transgenic Rats Bearing the G93A HmSOD1 Gene Mutation. Free Radic. Res. 2014, 48, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.-P.; Wei, Q.-Q.; Ou, R.-W.; Hou, Y.-B.; Zhang, L.-Y.; Yuan, X.-Q.; Yao, Y.-Q.; Jia, D.-S.; Zhang, Q.; Li, W.-X. Creatine Kinase in the Diagnosis and Prognostic Prediction of Amyotrophic Lateral Sclerosis: A Retrospective Case-Control Study. Neural Regen. Res. 2021, 16, 591. [Google Scholar] [CrossRef] [PubMed]
- Tavakol-Afshari, J.; Boroumand, A.R.; Farkhad, N.K.; Moghadam, A.A.; Sahab-Negah, S.; Gorji, A. Safety and Efficacy of Bone Marrow Derived-Mesenchymal Stem Cells Transplantation in Patients with Amyotrophic Lateral Sclerosis. Regen. Ther. 2021, 18, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Brooks, B.R.; Miller, R.G.; Swash, M.; Munsat, T.L. El Escorial Revisited: Revised Criteria for the Diagnosis of Amyotrophic Lateral Sclerosis. Amyotroph. lateral Scler. other Mot. neuron Disord. 2000, 1, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Faruqi, A.; Mukkamalla, S.K.R. Iron Binding Capacity. 2020.
- Koerper, M.A.; Dallman, P.R. Serum Iron Concentration and Transferrin Saturation in the Diagnosis of Iron Deficiency in Children: Normal Developmental Changes. J. Pediatr. 1977, 91, 870–874. [Google Scholar] [CrossRef] [PubMed]
- Colpo, G.D.; Ascoli, B.M.; Wollenhaupt-Aguiar, B.; Pfaffenseller, B.; Silva, E.G.; Cirne-Lima, E.O.; Quevedo, J.; Kapczinski, F.; Rosa, A.R. Mesenchymal Stem Cells for the Treatment of Neurodegenerative and Psychiatric Disorders. An. Acad. Bras. Cienc. 2015, 87, 1435–1449. [Google Scholar] [CrossRef]
- Rufino, R.A.; Pereira-Rufino, L.D.S.; Vissoto, T.C.S.; Kerkis, I.; Neves, A.D.C.; da Silva, M.C.P. The Immunomodulatory Potential Role of Mesenchymal Stem Cells in Diseases of the Central Nervous System. Neurodegener. Dis. 2022. [Google Scholar] [CrossRef]
- Cui, G.; Guo, H.; Li, H.; Zhai, Y.; Gong, Z.; Wu, J.; Liu, J.; Dong, Y.; Hou, S.; Liu, J. RVG-Modified Exosomes Derived from Mesenchymal Stem Cells Rescue Memory Deficits by Regulating Inflammatory Responses in a Mouse Model of Alzheimer’s Disease. Immun. Ageing 2019, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Homem, C.C.F.; Repic, M.; Knoblich, J.A. Proliferation Control in Neural Stem and Progenitor Cells. Nat. Rev. Neurosci. 2015, 16, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wu, H.; Wang, Y.; Gu, G.; Zhang, W.; Xia, R. Neural Stem Cell Transplantation Decreases Neuroinflammation in a Transgenic Mouse Model of Alzheimer’s Disease. J. Neurochem. 2016, 136, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.-H.; Allen, K.; Oei, F.; Leoni, E.; Kuhle, J.; Tree, T.; Fratta, P.; Sharma, N.; Sidle, K.; Howard, R. Systemic Inflammatory Response and Neuromuscular Involvement in Amyotrophic Lateral Sclerosis. Neurol. Neuroinflammation 2016, 3. [Google Scholar] [CrossRef] [PubMed]
- Cudkowicz, M.E.; Lindborg, S.R.; Goyal, N.A.; Miller, R.G.; Burford, M.J.; Berry, J.D.; Nicholson, K.A.; Mozaffar, T.; Katz, J.S.; Jenkins, L.J. A Randomized Placebo-controlled Phase 3 Study of Mesenchymal Stem Cells Induced to Secrete High Levels of Neurotrophic Factors in Amyotrophic Lateral Sclerosis. Muscle Nerve 2022, 65, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Berry, J.D.; Cudkowicz, M.E.; Windebank, A.J.; Staff, N.P.; Owegi, M.; Nicholson, K.; McKenna-Yasek, D.; Levy, Y.S.; Abramov, N.; Kaspi, H. NurOwn, Phase 2, Randomized, Clinical Trial in Patients with ALS: Safety, Clinical, and Biomarker Results. Neurology 2019, 93, e2294–e2305. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Chen, Y.; Dong, S.; Yang, W.; Qian, T.; Liu, X.; Cheng, Q.; Wang, J.; Chen, X. Role of Blood Neurofilaments in the Prognosis of Amyotrophic Lateral Sclerosis: A Meta-Analysis. Front. Neurol. 2021, 1731. [Google Scholar] [CrossRef] [PubMed]
- Feneberg, E.; Oeckl, P.; Steinacker, P.; Verde, F.; Barro, C.; Van Damme, P.; Gray, E.; Grosskreutz, J.; Jardel, C.; Kuhle, J. Multicenter Evaluation of Neurofilaments in Early Symptom Onset Amyotrophic Lateral Sclerosis. Neurology 2018, 90, e22–e30. [Google Scholar] [CrossRef]
- Sun, Q.; Zhao, X.; Li, S.; Yang, F.; Wang, H.; Cui, F.; Huang, X. CSF Neurofilament Light Chain Elevation Predicts ALS Severity and Progression. Front. Neurol. 2020, 11, 919. [Google Scholar] [CrossRef]
- Cohen, J.A.; Lublin, F.D.; Lock, C.; Pelletier, D.; Chitnis, T.; Mehra, M.; Gothelf, Y.; Aricha, R.; Lindborg, S.; Lebovits, C. Evaluation of Neurotrophic Factor Secreting Mesenchymal Stem Cells in Progressive Multiple Sclerosis. Mult. Scler. J. 2023, 29, 92–106. [Google Scholar] [CrossRef]
- Petrou, P.; Kassis, I.; Levin, N.; Paul, F.; Backner, Y.; Benoliel, T.; Oertel, F.C.; Scheel, M.; Hallimi, M.; Yaghmour, N. Beneficial Effects of Autologous Mesenchymal Stem Cell Transplantation in Active Progressive Multiple Sclerosis. Brain 2020, 143, 3574–3588. [Google Scholar] [CrossRef] [PubMed]
- Cabanes, C.; Bonilla, S.; Tabares, L.; Martínez, S. Neuroprotective Effect of Adult Hematopoietic Stem Cells in a Mouse Model of Motoneuron Degeneration. Neurobiol. Dis. 2007, 26, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Monsour, M.; Garbuzova-Davis, S.; Borlongan, C. V Patching Up the Permeability: The Role of Stem Cells in Lessening Neurovascular Damage in Amyotrophic Lateral Sclerosis. Stem Cells Transl. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Chen, Y.; Shang, H. Aberrations of Biochemical Indicators in Amyotrophic Lateral Sclerosis: A Systematic Review and Meta-Analysis. Transl. Neurodegener. 2021, 10, 1–12. [Google Scholar] [CrossRef]
- Mitchell, R.M.; Simmons, Z.; Beard, J.L.; Stephens, H.E.; Connor, J.R. Plasma Biomarkers Associated with ALS and Their Relationship to Iron Homeostasis. Muscle Nerve 2010, 42, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Hozumi, I.; Hasegawa, T.; Honda, A.; Ozawa, K.; Hayashi, Y.; Hashimoto, K.; Yamada, M.; Koumura, A.; Sakurai, T.; Kimura, A. Patterns of Levels of Biological Metals in CSF Differ among Neurodegenerative Diseases. J. Neurol. Sci. 2011, 303, 95–99. [Google Scholar] [CrossRef]
- Moghadam, M.S.; Azimian, H.; Afshari, J.T.; Toossi, M.T.B.; Farkhad, N.K.; Aghaee-Bakhtiari, S.H. Chromosomal Instability in Various Generations of Human Mesenchymal Stem Cells Following the Therapeutic Radiation Doses. 2023. [Google Scholar] [CrossRef]
- Devos, D.; Moreau, C.; Kyheng, M.; Garçon, G.; Rolland, A.S.; Blasco, H.; Gelé, P.; Timothée Lenglet, T.; Veyrat-Durebex, C.; Corcia, P. A Ferroptosis–Based Panel of Prognostic Biomarkers for Amyotrophic Lateral Sclerosis. Sci. Rep. 2019, 9, 2918. [Google Scholar] [CrossRef]
- Goodall, E.F.; Haque, M.S.; Morrison, K.E. Increased Serum Ferritin Levels in Amyotrophic Lateral Sclerosis (ALS) Patients. J. Neurol. 2008, 255, 1652–1656. [Google Scholar] [CrossRef]
- Hertel, N.; Kuzma-Kozakiewicz, M.; Gromicho, M.; Grosskreutz, J.; de Carvalho, M.; Uysal, H.; Dengler, R.; Petri, S.; Körner, S. Analysis of Routine Blood Parameters in Patients with Amyotrophic Lateral Sclerosis and Evaluation of a Possible Correlation with Disease Progression—a Multicenter Study. Front. Neurol. 2022, 13. [Google Scholar] [CrossRef]
- Sheykhansari, S.; Kozielski, K.; Bill, J.; Sitti, M.; Gemmati, D.; Zamboni, P.; Singh, A.V. Redox Metals Homeostasis in Multiple Sclerosis and Amyotrophic Lateral Sclerosis: A Review. Cell Death Dis. 2018, 9, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Rathore, K.I.; Redensek, A.; David, S. Iron Homeostasis in Astrocytes and Microglia Is Differentially Regulated by TNF-α and TGF-β1. Glia 2012, 60, 738–750. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Wang, T.; Cheng, Y.; Wu, Y.; Zhu, L.; Gu, Z.; Wu, Y.; Cai, L.; Wu, Y.; Zhang, Y. Melatonin Ameliorates Neurological Deficits through MT2/IL-33/Ferritin H Signaling-Mediated Inhibition of Neuroinflammation and Ferroptosis after Traumatic Brain Injury. Free Radic. Biol. Med. 2023, 199, 97–112. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic diagram of the immunological parameters through months in serum and CSF ( A, B; Tumor Necrosis Factor-alpha (TNF-α), C, D; Neurofilaments light chain (NFL), and D, E; glial cell-derived neurotropic factor (GDNF), respectively. In serum, tested in three times (before as (month -1), after 1 and 3 months of transplantation). In CSF, tested as (before (month 0), after 1, and 3 months of transplantation). Levels tested done in ELISA kit, ** (P-value <0.01). ng/ml; nanograms per milliliter. CSF; Cerebrospinal fluid (CSF)This is a figure. Schemes follow the same formatting.
Figure 1.
Schematic diagram of the immunological parameters through months in serum and CSF ( A, B; Tumor Necrosis Factor-alpha (TNF-α), C, D; Neurofilaments light chain (NFL), and D, E; glial cell-derived neurotropic factor (GDNF), respectively. In serum, tested in three times (before as (month -1), after 1 and 3 months of transplantation). In CSF, tested as (before (month 0), after 1, and 3 months of transplantation). Levels tested done in ELISA kit, ** (P-value <0.01). ng/ml; nanograms per milliliter. CSF; Cerebrospinal fluid (CSF)This is a figure. Schemes follow the same formatting.
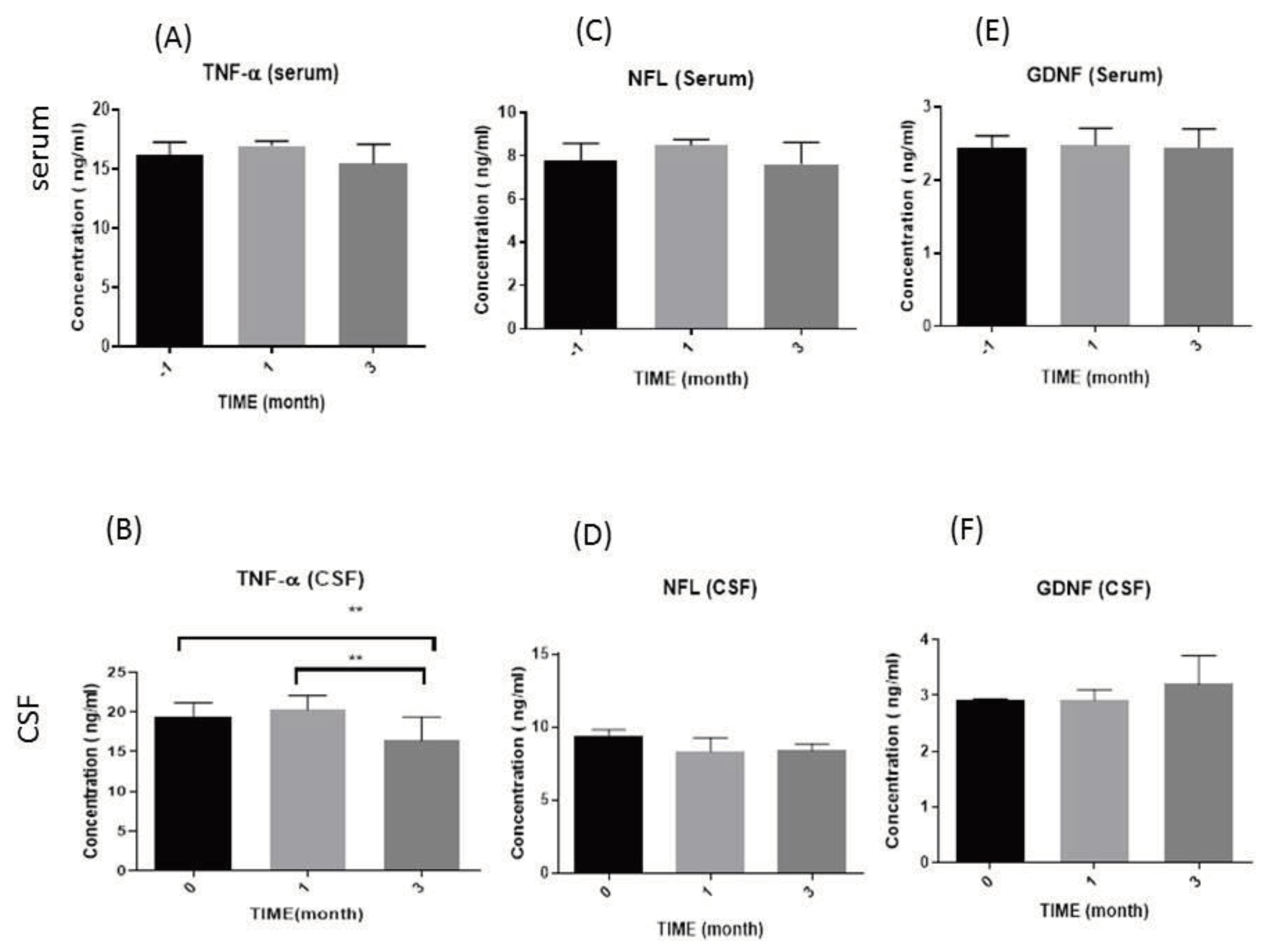
Figure 2.
Schematic diagram of the biochemical serum levels during the study. (A) Iron (Fe), (B) Ferritin, (C) Total Iron Binding Capacity (TIBC), (D) Transferrin (as percentage %), and (E) Creatine kinase(CK)), respectively. Three times were estimated as before (month -1), after 1 and 3 months of transplantation). P value >0.05, µg/dl; Microgram per deciliter, u/l; units of enzyme activity per Liter, ng/ml; nanograms per milliliter.
Figure 2.
Schematic diagram of the biochemical serum levels during the study. (A) Iron (Fe), (B) Ferritin, (C) Total Iron Binding Capacity (TIBC), (D) Transferrin (as percentage %), and (E) Creatine kinase(CK)), respectively. Three times were estimated as before (month -1), after 1 and 3 months of transplantation). P value >0.05, µg/dl; Microgram per deciliter, u/l; units of enzyme activity per Liter, ng/ml; nanograms per milliliter.
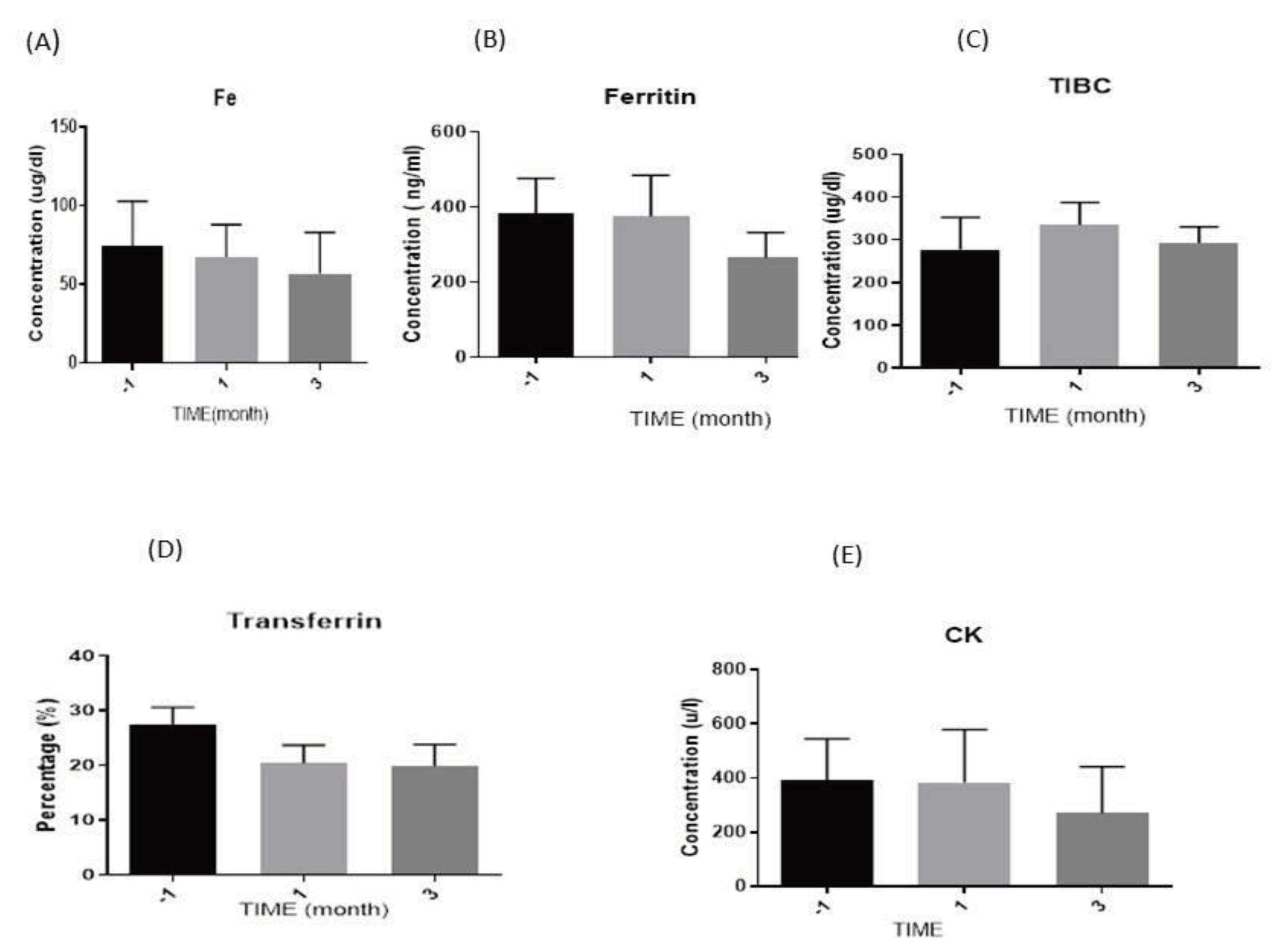

Table 1.
Correlations between the biochemical and the immunological parameters. .
| Biochemical parameters | Immunological parameters | ||
|---|---|---|---|
| NFL(ng/ml) | TNF-α (ng/ml) | GDNF(ng/ml) | |
| Ferritin (ng/ml) | ...... | -(0.52*) | -(0.48*) |
| Fe (µg/dl) | 0.48* | ...... | ...... |
| CK (u/l) | 0.44* | ...... | ...... |
NFL; Neurofilaments light, TNF-α; Tumor Necrosis Factor-alpha, GDNF; glial cell-derived neurotropic factor, Fe; Iron, CK; Creatine kinase. *The correlation is significant at the 0.05 level (2-tailed). * P-value <0.05, ng/ml; nanograms per milliliter, µg/dl; Microgram per deciliter, u/l; units of enzyme activity per Liter.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



