Submitted:
28 April 2024
Posted:
29 April 2024
You are already at the latest version
Abstract
Background- In India, 26 million children are born every year. These Children (0-6 years) comprise 13% of the country's population. Undernutrition is fallout of malnutrition, malabsorption, and nutritional imbalance which causes problem of underweight in children. It can affect child’s brain development and other developmental milestones. Methods- We used anonymized, publicly available secondary data from the India National Family Health Survey (NFHS-5). Descriptive statistical analysis, correlation coefficient analysis, and regression analysis of the data have been done. Results- Multiple linear regression for independent variables, operational AWCs (%) and women with Internet access (%), and dependent variable underweight children per state (%) developed the model, Underweight children (%) = 37.1607 + 0.5659. operational AWCs (%) – 0.2907. women with Internet Access (%). It shows Ꞵ0= 37.1607, Ꞵ1= 0.5659, and Ꞵ2= -0.2907 as well as R squared value as 0.5709. This shows independent variables have a significant influence on the number of underweight children in the state. Results of the Pearson correlation indicated that there is a significant large positive relationship between operational AWCs (%) and the percentage of underweight children in the state, (r(34) = .58, p < .001). Whereas there is a significant large negative relationship between Internet access to women (%) and the percentage of underweight children in the state, (r(34) = .733/-0.733, p < .001). Conclusion- The study clearly shows that when compared, community daycare centers (AWCs) have a limited role in the child's nutrition, but Internet access to the mothers can be a determinant of the child's nutrition. The internet access to women can help to reduce the number of underweight children under five years and improve overall maternal and child health as well as public health.
Keywords:
Internet Access
; India
; Malnutrition
; under-five children
; population
Introduction
Community daycare centres (Anganwadi centres) in India are started as part of the Integrated Child Development Service program to combat child hunger and malnutrition. A total of 1.396 million Anganwadi Centres (AWCs) are registered in the country [1]. Out of which 0.136 million are in urban areas whereas the rest are in rural areas of the country. Under-weight based on weight-for-age, is recommended as the indicator to assess changes in the magnitude of malnutrition over time [2]. Evidence has shown that the mortality risk of children who are even mildly underweight is increased, and severely underweight children are at even higher risk [3]. Thus, monitoring weight-for-age can help assess the contribution of public health policies or interventions to mortality reduction.
In India, 26 million children are born every year. Children (0-6 years) comprise 13% of the country’s total population [4]. Studying malnutrition in under-five children is important from a public health perspective. Intending to improve the nutritional and health status of children in the age group of 0-6 years, the government of India in 1975 launched ‘The Integrated Child Development Services (ICDS)’; AWCs is part of it [5]. AWCs provide nutrition and nutrition education, non-formal preschool education, and health education. Referral services, health check-up and immunization is also provided at AWCs which is part of public health system.
Earlier studies have found that there are various risk factors associated with malnutrition among under-five children. Gender differences, families with low per capita income, urban-rural lifestyle, lower food consumption in girls compared to boys, poor feeding practices, and lack of knowledge about growth monitoring in children are some of the determinants [6].
Place of residence, household wealth, birth weight, age of a child, awareness regarding diarrheal diseases and acute respiratory tract infection control, maternal education, number of under five years children, and source of drinking water were strong predictors of child nutritional status in developing countries [7]. Maternal factors like age, weight, and anaemia also affect a child’s nutritional status [8]. There is a positive link between the nutritional status of children and the stages of development in the states they live [9].
Recent studies have revealed internet access plays an important role in improving the energy intake of low-income groups which should be considered in terms of the UN’s Sustainable Development Goals (SDGs) of ending malnutrition [10]. A few more studies prove the internet’s role in tackling malnutrition [11,12,13].
The COVID-19 pandemic has unearthed our reliance on broadband internet, not as a luxury but as an essential utility such as water and electricity [14]. Broadband internet access is a super determinant of health because many other social determinants like education, health care, food, income hinge on it [15].
Infrastructure development has a positive role in public health. There is no study available to show whether there is any effect of community infrastructure like public daycare centers or internet access to women on reducing under-five malnutrition, especially in the Indian context. This study is designed to understand, if any positive relation persists between community infrastructure (daycare centers and internet access to women) in the reduction of child malnutrition. The results will be used to fill the knowledge gap and to frame strategic policies to obtain better results.
2. Methods
2.1. Study Population
Our sample consisted of 724,115 women in the age group of 15-49 years. The majority of India’s population growth comes from rural and underprivileged areas, while the rise in income comes from the urban privileged population. So, studying both populations were considered to help better understand the issue. Population is divided into four sub-samples for study-Urban women, rural women, urban children, and rural children. For a detailed understanding of the geographical prevalence of underweight children in the country, the study population was divided into regions.
1)The northern region- has six states- Himachal Pradesh, Punjab, Uttarakhand, Haryana, Delhi, and Uttar Pradesh; 2) The southern region contains five states- Andhra Pradesh, Karnataka, Kerala, Tamil Nadu, and Telangana; 3)Eastern region- is consisting of the states of Bihar, Jharkhand, Odisha and West Bengal, 4)Western region states are Rajasthan, Maharashtra Gujarat and Goa; 5) Central region-It consists of two states- Madhya Pradesh and Chhattisgarh 6)North-East region includes-eight States viz. Arunachal Pradesh, Assam, Manipur, Meghalaya, Mizoram, Nagaland, Sikkim and Tripura. Union territories (Andaman and Nicobar Islands, Chandigarh, Dadra and Nagar Haveli, Daman and Diu, Lakshadweep, Puducherry, Jammu & Kashmir, Ladakh) are grouped as per their geographical locations.
2.2. Database Used for Study
The data related to the percentage of underweight children and the percentage of women getting Internet Access was collected from the Ministry of Health and Family Welfare (MoHFW), Government of India. Data related to the number of Anganwadi centers per state has been collected from the Ministry of Women and Child Development. The NFHS-5 data provides information for 707 districts, 28 states, and 8 Union territories (UTs). The survey work for the NFHS-5 was planned in two phases. The first phase was carried out for 17 states and 5 Union territories from 17 June 2019 to 30 January 2020 and the second phase has been completed in 11 States and 3 UTs from 2 January 2020 to 30 April 2021.
Weight was measured with an electronic SECA 874 flat scale designed for mobile use. Height was measured with a Seca 213. stadiometer. Underweight (assessed via weight-for-age) is a composite index of height-for-age and weight-for-height. It takes into account both acute and chronic undernutrition. Children whose weight-for-age Z-score is below minus two standard deviations (-2 SD) from the median of the reference population are classified as underweight. Children whose weight-for-age Z-score is below minus three standard deviations (-3 SD) from the median are considered severely underweight (based on WHO standards).
2.3. Ethics Approval
Our study is based on the publicly available dataset of the NFHS-5 surveys with no identifiable information on the participants and can be freely accessed from the Ministry of Health and Family Welfare website, India. As per the data, the ethical approval for the NFHS-5 surveys is obtained from the ethics review board of the International Institute for Population Sciences, Mumbai, India. These surveys are reviewed and approved by the ICF Institutional Review Board, USA. Informed written consent for participation in this survey is obtained from the respondents during the survey. Each individual’s approval is sought before the patient interview, as per the consistent methodology followed in these national surveys.
2.4. Study Variables
The primary outcome variable or dependent variable in this study is the percentage of underweight children. The independent variable or explanatory variable is the number of AWCs per state (%) and the percentage of women getting Internet Access. The information on the women getting Internet access and AWCs was obtained by asking ‘yes’ or ‘no’ questions orally. Children whose weight-for-age Z-score is below minus two standard deviations (-2 SD) from the median of the reference population are classified as underweight. Children whose weight-for-age Z-score is below minus three standard deviations (-3 SD) from the median are considered severely underweight (based on WHO standards).
2.5. Statistical Analysis
Descriptive statistical analysis of the data has been done. Mean, median and range was calculated. Pearson correlation coefficient analysis, simple linear regression and multiple linear regression was carried out for independent variables, operational AWCs (%) and women with Internet access (%), and dependent variable underweight children per state (%). Social Science Statistics (www.socscistatistics.com) tools are used for above analysis.
Result
National-level data on the percentage of women with Internet Access shows, urban women (51.8%), rural women (24.6%), and total (33.3%). Whereas the percentage of underweight children in urban India (27.3%), rural (33.8%), and total 32.1% (Table 1) (Figure 1). The regression analysis results in this study show a linear correlation between the variables of internet access to women and children under five years who are underweight (weight-for-age) in India. Here Ꞵ coefficient is -0.36 (p < 0.001) means that when you increase internet access to women by 1, the value of Y which is the percentage of underweight children decreases by 0.3552.
The simple linear regression analysis of the independent variable AWCs (%) in state and dependent variable, percentage of underweight children per state shows Ꞵ= 1.46, p < 0.001. R-squared (R2) equals 0.3366. This means that 33.7% of the variability of Y is explained by X.
Multiple linear regression was done for independent variables, operational AWCs (%) and women with Internet access (%), and dependent variable underweight children per state (%). The model developed is Underweight children (%) = 37.1607 + 0.5659. operational AWCs (%) – 0.2907. women with Internet Access (%). It shows Ꞵ0= 37.1607, Ꞵ1= 0.5659, and Ꞵ2= -0.2907 as well as R squared value as 0.5709. This shows independent variables have a significant influence on the number of underweight children in the state.
Results of the Pearson correlation indicated that there is a significant large positive relationship between operational AWCs (%) and the percentage of underweight children in the state, (r(34) = .58, p < .001). Results of the Pearson correlation indicated that there is a significant large negative relationship between Internet access to women (%) and the percentage of underweight children in the state, (r(34) = .733/-0.733, p < .001).
The above statistical analysis shows that access to the Internet for women has a significant role in reducing the percentage of underweight children when compared to AWCs.
In every state of northern India, the percentage of urban women with internet access is higher than in rural areas (Table 2). The mean of women with internet access is 63.58 in urban areas as compared to 45.35 in rural. The average of total women with internet access is 51.92 for the country’s northern region. Punjab (17.9%), Uttarakhand (21.0%), and Delhi (22.2%) were the northern states where a greater number of urban children were underweight than their rural counterparts. Jammu and Kashmir (21.0%), Himachal Pradesh (25.5%), and Ladakh (20.4%) have shown an increase in the percentage of underweight children when compared to NFHS4 data. In contrast, the rest of the states of northern India have shown a reduction in the percentage of underweight children.
In the northern region of India, Uttar Pradesh has shown the highest number of AWCs (189024) followed by Jammu and Kashmir (28119), Punjab (27314), Haryana (25963), Uttarakhand (20088), Himachal Pradesh (18925), and Delhi (10899). Despite having the maximum number of AWCs in Uttar Pradesh; the highest number (32.1%) of underweight children are observed here. Union territories like Ladakh (1144), and Chandigarh (450) have a smaller number of AWCs. When comparing the results of Union territories of Jammu & Kashmir with Chandigarh the percentage of underweight children is similar. The number of AWCs in Jammu & Kashmir is very high if compared with Chandigarh. The only variable of internet access to women varies here. The UT of Chandigarh has a higher percentage of women with internet access as compared to J & K.
As far as internet access to women is concerned in all the states of southern India, urban women are more in number than rural women. In southern states of India, the Union Territories of Lakshadweep (28.5%) and Puducherry (15.9%) have shown more underweight children in urban areas as compared to rural areas. The states of Telangana (31.8%), Kerala (19.7%), and the Union Territories of Lakshadweep (25.8%) and Andaman & Nicobar (23.7%) have shown an increase in the percentage of total number of underweight children compared to NFHS4 data. In this region, the UT of Puducherry showed the lowest number of underweight children (15.3%) with only 855 AWCS. This is the area where the highest number of women with internet access (61.9%) is seen in the region (Table 3).
In the Eastern region of India, in every state, more urban women have access to the Internet as compared to the rural ones. Jharkhand (31.4%) has the highest percentage of women with internet access in the region compared to the other regional states. It is followed by West Bengal (25.5%), Odisha (24.9%), and Bihar (20.6%). In the Eastern region of India, West Bengal (32.2%) has shown an increased percentage of underweight children compared to NHFS-4 data.
In the eastern region of India, the highest number of underweight children is in Bihar (41.0%) whereas the lowest number of underweight children is in Odisha (29.7%). If the number of AWCs is compared, in Bihar 114989 AWCs are there whereas in Odisha 74157 AWCs are there. The better nutrition results in Odisha might be due to the better internet access for women (Table 4).
In the Western region of India, urban as well as rural women of Goa are more in number for access to the internet. Goa is followed by Maharashtra (38.0%), Rajasthan (36.9%), UT of Dadra and Nagar Haveli (36.7%), and Gujrat (30.8%) for total women who got internet access. In the Western region of India, except Rajasthan, the rest of the states have shown a slight increase in the percentage of underweight children when compared to NFHS-4 data. The lowest number (24.0%) of underweight children are found in Goa with only 1262 AWCs. The state shows the highest number of women (73.7%) with Internet access (Table 5).
In Chhattisgarh and Madhya Pradesh of Central India, double the number of urban women have access to the internet as compared to rural women. In the Central region of India, the declining percentage of underweight children is observed when compared to NHFS-4 data. States of Chhattisgarh and Madhya Pradesh of Central region have similar numbers of women with internet access. At the same time, more or less similar numbers of underweight children. Despite the considerable difference in the number of AWCs between the states, the comparable results might be due to access to the Internet for women (Table 6).
In North-Eastern India, urban Sikkim (90%), followed by Mizoram (83.8%) and Arunachal Pradesh (70.0%) have the highest number of women with internet access, not only in the North-East region but also in the other parts of the country. In rural parts of the states, this number is lower than in urban parts of the region. The state of Tripura has the lowest number of women with internet access in urban (36.6%) as well as in rural (17.7%) parts. In the North-Eastern region of India, Assam (32.8 %), Mizoram (12.7%) and Nagaland (26.9%) have shown an increase in the underweight children population when compared with NHFS-4 data.
Mizoram has shown the lowest number of underweight children (12.7%) in the North-east region whereas the highest number of underweight children (32.8%) are seen in Assam. Mizoram has 2244 AWCs whereas Assam has 61738 AWCs. When the data for Internet access for women is compared, Mizoram has (67.6%) more women with Internet access than the women in Assam (28.2%) (Table 7).
When the mean (average) was compared for the geographical regions of the country the Eastern region showed the highest number of AWCs (87504.75) whereas the Northeast had shown lowest number of AWCs (12807.88). But when the mean of the percentage of underweight children for various geographical regions is analyzed the highest number of underweight children (35.58%) is seen in the eastern region whereas the lowest number of underweight children is seen in the North-east region (22.11%) of the country (Figure 2).
When the mean was calculated for Internet access and the percentage of malnourished children for each geographical region of India, North India has the highest number of women with Internet access (51.92%). North is followed by the northeast (47.21%) region, west (43.22%), south (42.95%), central (26.8%), and east (25.6%) (Figure 3).
The eastern region has shown (35.58%) the highest number of underweight children. This region is followed by west (33.22%), central (32.15%), south (25.1%), north (22.31%), and northeast (22.11%). Compared to NFHS4, the mean of all these geographical regions for underweight children shows a reduction except for the northeast region.
When the range was calculated for various geographical regions, the highest value of range was observed for Internet access for Northeast India (53.8). That means the difference in Internet access to different states here is more. Some states have women with more internet access and some states have less. Northeast is followed by North (44.6), west (42.9), south (40.9), East (10.8), and Central (0.2) regions.
When the range was compared for the percentage of underweight children in various geographical regions, the Northeast showed the maximum value (20.1). It is followed by south (17.6), west (15.7), north (15.2), east (11.3) and central (1.7). When the range was compared for operational AWCs for all geographical regions, the North showed the highest (188574) range followed by west (110024), east (84011), south (65819), north-east (60430), and central (45249).
Discussion
Earlier studies have proved the role of community-based childcare centers in improving child nutrition and development [16]. Our study clearly shows when compared with Internet access to women, AWCs have a limited role in the nutrition of the child. Internet access to the mothers can be one of the possible determinants of improving child’s nutrition.
About half of all fatalities in children under five are attributable to under-nutrition [17]. Asia is home to over 70% of malnourished children, with India, Pakistan, and Bangladesh having the highest prevalence in this region [18]. In the digital age, the penetration of the internet and social media has become the determinants of lifestyle changes and consequent health outcomes [19].
Our study results are similar to the earlier studies where the urban or rural area was the determinant of child malnutrition [20,21]. A study in northern Ethiopia where children born to rural mothers were more likely to be severely underweight than children born to urban mothers. The reason behind the rural-urban gap might be in urban areas women get more access to information regarding child nutrition, health services, and feeding practices [22].
A similar urban-rural divide was noticed in the Bangladesh population where access to primary education, household socioeconomic status, adequate maternal healthcare utilization, improvement of transportation, and awareness about nutrition in urban areas compared to rural ones are the determinants behind this divide [23]. Urban children from families with higher average monthly income do not show the problem of under-nutrition may be due to higher levels of income increasing their ability to provide more than enough nutrition for their growing children [24].
Similar to our study geographical variation and urban-rural variation was noticed in earlier studies [25]. Here children of higher birth orders (4 or more) living in rural areas of Central, eastern, and north-eastern regions of the country are benefitting from Anganwadi centres. Anganwadi centres provide mid-day meals to children throughout the country especially in rural areas via the government-run Integrated Child Development Scheme (ICDS). Urban children generally don’t have access to these Anganwadi centres. Locally available food variety and social customs related to dietary habits are also reasons behind the geographic variations in the adequate diet of children [26].
The contributing factors for undernutrition may differ from one region to another [27]. In our study, the variation was noticed at the state level as well as regional levels. Our results are similar to the results of the study carried out in Ethiopia for understanding the cluster variation of underweight and detecting spatial heterogeneity at the sub-national level over time [28]. This will be useful for identifying gaps in child nutrition programs at the state level and coming up with targeted nutritional interventions for the population at risk.
A prevalence study carried out in the Population of Nepal shows the similar effect of the socioeconomic divide on the outcomes of child nutrition. This study suggests context-specific health information education and communication (IEC)/behaviour change communication (BCC) materials such as radio jingles, posters, pamphlets, and other pictorials can be designed in the local languages and delivered through multiple channels so that messages can be reached out to disadvantaged communities [29]. This applies to the Indian population also where by spreading health information in regional languages via the internet, the government can cost-effectively reach the maximum population.
Studies have proved Internet access significantly facilitates healthcare access and mitigates the negative impact of income inequality on healthcare access [30,31].
In our study, some states have shown a higher number of under-weight children in their urban areas compared to rural ones. Our results match the earlier studies where the prevalence of underweight was more seen in an urban slum than in a rural area [32,33]. It was observed in these studies that the low income of the family had resulted in underweight children from an urban slum.
A study carried out in Bangladesh has also showed more underweight children in urban slums than in rural ones. The study says, that for people living in slums, poverty is perceived with income and consumption patterns. In the majority of cases, the poor are involved in stumpy-earning jobs and often have inadequate income which subsequently results in spending the majority of their earnings on food, mainly staples like rice, cereals, lentils, potatoes, and vegetables, and usually evade costly items like meat and poultry, milk, and fruits. There are schools of thought, that indicate that chronic malnutrition and undernutrition among children are often the result of deprivation of such necessary food items over a long period [34].
In recent years the Internet has become a popular source of health information [35,36]. There are research studies show a relationship between internet technology and dietary health. These effects are mixed. A significant positive association was seen between internet use and fast-food consumption in rural Chinese children [37]. In contrast, a study in Iran shows nutrition knowledge from the Internet can improve dietary quality [38].
A study carried out on the Indian population shows eHealth movement is underway within healthcare systems in developing countries but the adoption of eHealth resources remains low [39]. This study shows demographics, health beliefs, and technology enablers are the significant factors for the use of eHealth. These factors influence the prevalence of Internet Health Information Seeking (IHIS), the diversity of IHIS, and discussing Internet Health Information with doctors. Understanding the factors affecting the health digitization process can help better promote eHealth adoption in developing countries like India.
A study carried out in Africa for the implementation of universal health coverage suggests Innovative strategies such as digital health. Certainly, the successful deployment of it on a wider scale faces several challenges for geographically diverse countries like India. Digital health has several benefits namely improving access to healthcare services, especially for those living in remote areas, improvements in safety and quality of healthcare services and products, improved knowledge and access of health workers and communities to health information; cost savings and efficiencies in health services delivery; and improvements in access to the social, economic and environmental determinants of health, all of which could contribute to the attainment of universal health coverage. Similar to Africa, India too faces the challenges in deployment of digital health like weak health systems, lack of awareness and knowledge about digital health, and poor infrastructure such as unstable power supply, and poor internet connectivity [40].
India has 40 cities with over a million population, 396 cities with between 1,00,000 and 1 million, and 2500 cities with between 10,000 and 1,00,000 [41]. The internet and electricity should be provided in these areas on a priority basis. Studies have shown, that the diffusion of the Internet has dramatically reduced informational frictions and given people unprecedented sources of health information [42,43,44]. The use of the internet by women is directly related to the education of women and the internet access to them.
Nutrition education has a significant impact on increasing maternal knowledge and children’s nutritional status. Earlier studies also suggest that nutrition health education methods and media can be booklets, guidebooks, leaflets, and internet technology applications [45].
Limitations of Study
This study has made considerable contributions to literature but some limitations will be addressed in the future. This study is based on the data the Ministry of Health and Family Welfare, Government of India collected for NFHS-5. The limitations which are related to any secondary data are also related to this data. There are many factors responsible for the weight of the children. Only two factors are controlled in this paper, and there is no way to comprehensively consider the impact of other factors on the results in this paper, such as social and cultural barriers. These are the focus of our next research. There is no data available for the internet access to women in NFHS-4 for comparison with data of NFHS-5.
Conclusion and Policy Implications
Contrary to expectations, though the penetration of the Internet is increasing in India, women still have less access to the Internet. The disparities in access to the internet should be treated as a public health issue as internet access has become a social determinant of health. The outbreak of COVID-19 has highlighted that lack of internet access is a lack of access to health information so it becomes an important determinant of public health. Women should be treated as a focused group and provided with broadband internet as they are responsible not only for their health but for their children’s health. Indeed, women living in rural areas, remote areas, and less educated women can remain deprived of health information which can affect their health. Internet access and health information in regional languages should be provided to women/mothers which can help to achieve SDGs related to maternal and child health.
Author Contributions
1) Conceptualization, methodology, analysis, and investigation, writing, reviewing & editing of the draft - J. S 2) Supervision, statistical analysis, original draft preparation/writing, review, and editing- C. S. All authors have agreed to the submission of this manuscript.
Funding
Not Applicable.
Informed Consent Statement
This study is based on publicly available secondary data so ethical approval is not necessary.
Acknowledgments
Not Applicable.
Conflicts of Interest
The authors declare no competing interests.
References
- Press Information Bureau, 2023. Total 13.96 lakh Anganwadis registered under the Poshan Tracker application. https://pib.gov.in/PressReleasePage.aspx?PRID=1943759.
- https://www.who.int/data/gho/indicator-metadata-registry/imr-details/27.
- https://www.measureevaluation.org/rbf/indicator-collections/health-outcome-impact-indicators/children-aged-under-5-years-who-are-underweight.html.
- https://nhm.goa.gov.in/child-health/.
- https://en.wikipedia.org/wiki/Integrated_Child_Development_Services.
- Sahu SK, Kumar SG, Bhat BV, Premarajan KC, Sarkar S, Roy G, Joseph N. Malnutrition among under-five children in India and strategies for control. J Nat Sci Biol Med. 2015 Jan-Jun;6(1):18-23. [CrossRef] [PubMed]
- Mittal A, Singh J, Ahluwalia SK. Effect of maternal factors on nutritional status of 1-5-year old children in urban slum population. Indian J Community Med. 2007;32:264–7.
- Ganesh Kumar S, Harsha Kumar HN, Jayaram S, Kotian MS. Determinants of low birth weight: A case-control study in a district hospital in Karnataka. Indian J Pediatr. 2010;77:87–9.
- Som S, Pal M, Bharati P. Role of individual and household level factors on stunting: A comparative study in three Indian states. Ann Hum Biol. 2007;34:632–46.
- Xue, P.; Han, X.; Elahi, E.; Zhao, Y.; Wang, X. Internet Access and Nutritional Intake: Evidence from Rural China. Nutrients 2021, 13, 2015. [Google Scholar] [CrossRef]
- Mingwei Yang., Zhiyong Zhang., Zheng Wang. Does Internet use connect smallholder farmers to a healthy diet? Evidence from rural China. Front. Nutr., 20 April 2023 Sec. Nutrition and Sustainable Diets Volume 10 - 2023 |. [CrossRef]
- Ma, Baojie, and Xin Jin. 2022. “Does Internet Use Connect Us to a Healthy Diet? Evidence from Rural China” Nutrients 14, no. 13: 2630. [CrossRef]
- CUI Yi., Zhao Qi-ran, Thomas Glauben, Si Wei. The Impact of Internet Access on Household Dietary Quality: Evidence from Rural China. Journal of Integrative Agriculture. Available online 23 November 2023.
- Early J, Hernandez A. Digital Disenfranchisement and COVID-19: Broadband Internet Access as a Social Determinant of Health. Health Promotion Practice. 2021;22(5):605-610. [CrossRef]
- Bauerly B. C., McCord R. F., Hulkower R., Pepin D. (2019). Broadband access as a public health issue: The role of law in expanding broadband access and connecting underserved communities for better health outcomes. Journal of Law, Medicine & Ethics, 47(Suppl. 2), 39–42. [CrossRef]
- Gelli, A., Margolies, A., Santacroce, M. et al. Improving child nutrition and development through community-based childcare centres in Malawi – The NEEP-IE study: study protocol for a randomized controlled trial. Trials 18, 284 (2017). [CrossRef]
- https://data.unicef.org/topic/nutrition/child-nutrition/.
- Akhtar S. Malnutrition in South Asia-A Critical Reappraisal. Crit Rev Food Sci Nutr. 2016 Oct 25;56(14):2320-30. [CrossRef] [PubMed]
- Deetjen, U. The lifestyle paradox: adverse effects of internet use on self-rated health status. Inf Commun Soc. (2018) 21:1322–36. [CrossRef]
- Rahman A, Rahman MS. Rural-urban differentials of childhood malnutrition in Bangladesh. Int. J. Child Health Nutr. 2019;8(1):35–42. [CrossRef]
- Akram R, Sultana M, Ali N, Sheikh N, Sarker AR. Prevalence and determinants of stunting among preschool children and its urban–rural disparities in Bangladesh. Food Nutr Bull. 2018;39(4):521–35. [CrossRef]
- Haftom Temesgen Abebe, Getachew Redae Taffere, Meseret Abay Fisseha, Afework Mulugeta Bezabih. Risk Factors and Spatial Distributions of Underweight Among Children Under-Five in Urban and Rural Communities in Tigray, Northern Ethiopia: Using Ordinal Logistic Regression Analysis. Nutrition and Dietary Supplements 2022:14 pg 21-37.
- Anik, A.I., Chowdhury, M.R.K., Khan, H.T.A. et al. Urban-rural differences in the associated factors of severe under-5 child undernutrition based on the composite index of severe anthropometric failure (CISAF) in Bangladesh. BMC Public Health 21, 2147 (2021). [CrossRef]
- Gudu, E., Obonyo, M., Omballa, V. et al. Factors associated with malnutrition in children < 5 years in western Kenya: a hospital-based unmatched case control study. BMC Nutr 6, 33 (2020). [CrossRef]
- Khan N., Mozumdar A., Kaur S. Dietary Adequacy among Young Children in India: Improvement or Stagnation? An Investigation From the National Family Health Survey. Food Nutr. Bull. 2019;40:471–487.
- Longvah T, Khutsoh B, Meshram II, et al. Mother and child nutrition among the Chakhesang tribe in the state of Nagaland, North-East India. Matern Child Nutr. 2017;13(suppl 3):e12558.
- Gangurde, Shweta; Jadhav, Sudhir L.1; Waghela, Hetal2; Srivastava, Kajal. Undernutrition among Under-Five Children in Western Maharashtra. Medical Journal of Dr. D.Y. Patil Vidyapeeth 16(3):p 386-392, May–Jun 2023. |. [CrossRef]
- Atalell KA, Alemu TG and Wubneh CA (2022) Mapping underweight in children using data from the five Ethiopia Demographic and Health Survey data conducted between 2000 and 2019: A geospatial analysis using the Bayesian framework. Front. Nutr. 9:988417. [CrossRef]
- Adhikari D, Khatri RB, Paudel YR and Poudyal AK (2017) Factors Associated with Underweight among Under-Five Children in Eastern Nepal: Community-Based Cross-sectional Study. Front. Public Health 5:350. [CrossRef]
- Yu J, Meng S. Impacts of the Internet on Health Inequality and Healthcare Access: A Cross-Country Study. Front Public Health. 2022 Jun 9;10:935608. [CrossRef] [PubMed]
- Duplaga M. The association between Internet use and health-related outcomes in older adults and the elderly: a cross-sectional study. BMC Medical Inform Decis Mak. (2021) 21:1–12. [CrossRef]
- Murarkar, S., Gothankar, J., Doke, P. et al. Prevalence and determinants of undernutrition among under-five children residing in urban slums and rural area, Maharashtra, India: a community-based cross-sectional study. BMC Public Health 20, 1559 (2020). [CrossRef]
- Bhadoria AS, et al. Prevalence of underweight, stunting and wasting among children in urban slums of Delhi. Int J Nutr Pharmacology, Neurological diseases. 2013;3(3):323–4.
- Ahsan, K.Z., Arifeen, S.E., Al-Mamun, M.A. et al. Effects of individual, household and community characteristics on child nutritional status in the slums of urban Bangladesh. Arch Public Health 75, 9 (2017). [CrossRef]
- Javanmardi M, Noroozi M, Mostafavi F, Ashrafi-Rizi H. Internet Usage among Pregnant Women for Seeking Health Information: A Review Article. Iran J Nurs Midwifery Res. 2018 Mar-Apr;23(2):79-86. [CrossRef] [PubMed]
- Sun Y, Yu J, Chiu Y-L and Hsu Y-T (2022) Can online health information sources improve patient satisfaction? Front. Public Health 10:940800. [CrossRef]
- Hansstein, FV, Hong, Y, and Di, C. The relationship between new media exposure and fast-food consumption among Chinese children and adolescents in school: a rural-urban comparison. Glob Health Promot. (2017) 24:40–8. [CrossRef]
- Joulaei, H, Keshani, P, and Kaveh, MH. Nutrition literacy as a determinant for diet quality amongst young adolescents: a cross-sectional study. Prog Nutr. (2018) 20:455–64. [CrossRef]
- Shaohai Jiang, Iccha Basnyat, Piper Liping Liu. Factors Influencing Internet Health Information Seeking In India: An Application of the Comprehensive Model of Information Seeking. International Journal of Communication, [S.l.], v. 15, p. 22, apr. 2021. ISSN 1932-8036. Available at: <https://ijoc.org/index.php/ijoc/article/view/16140>.
- Olu O, Muneene D, Bataringaya JE, Nahimana MR, Ba H, Turgeon Y, Karamagi HC, Dovlo D. How Can Digital Health Technologies Contribute to Sustainable Attainment of Universal Health Coverage in Africa? A Perspective. Front Public Health. 2019 Nov 15;7:341. [CrossRef] [PubMed]
- Jaimini Sarkar, 2022. Are you staying in age ready city? Science Reporter pg 20-23. https://nopr.niscpr.res.in/bitstream/123456789/60624/1/SR%2059%2810%29%2020-23.pdf.
- Tan SS, Goonawardene N. Internet health information seeking and the patient-physician relationship: a systematic review. J Medical Internet Res. (2017) 19:e5729. [CrossRef]
- Benda NC, Veinot TC, Sieck CJ, Ancker JS. Broadband internet access is a social determinant of health! Am J Public Health. (2020) 110:1123–5. [CrossRef]
- Rubin R. Internet access as a social determinant of health. JAMA. (2021) 326:298. [CrossRef]
- Prasetyo, Y.B., Permatasari, P. & Susanti, H.D. The effect of mothers’ nutritional education and knowledge on children’s nutritional status: a systematic review. ICEP 17, 11 (2023). [CrossRef]
Figure 1.
National level data on women with Internet Access (%) and underweight children under five years of age (%).
Figure 1.
National level data on women with Internet Access (%) and underweight children under five years of age (%).
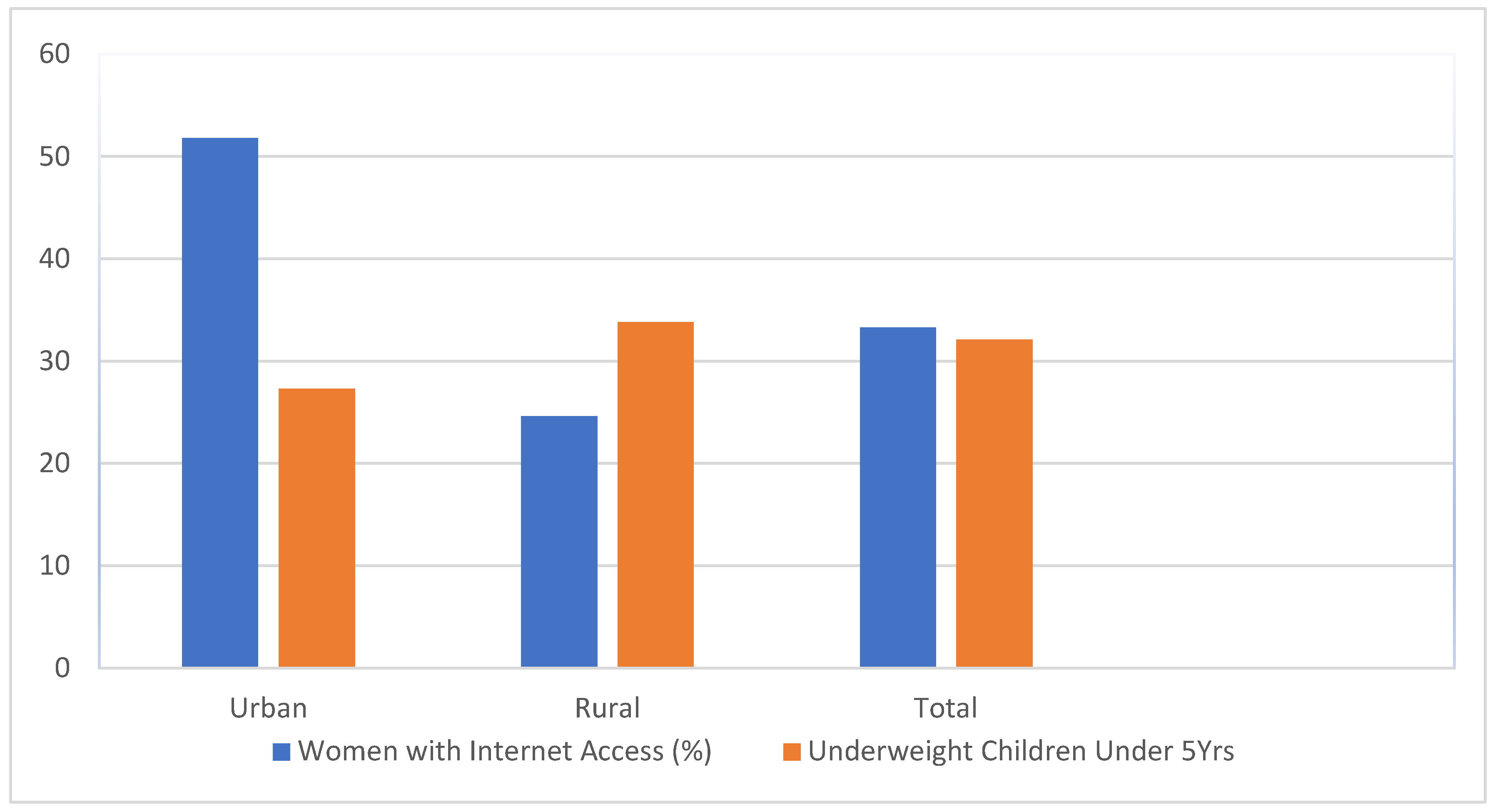
Figure 2.
Mean of Number of operational AWCs and percentage of underweight children which are below 5 years old.
Figure 2.
Mean of Number of operational AWCs and percentage of underweight children which are below 5 years old.
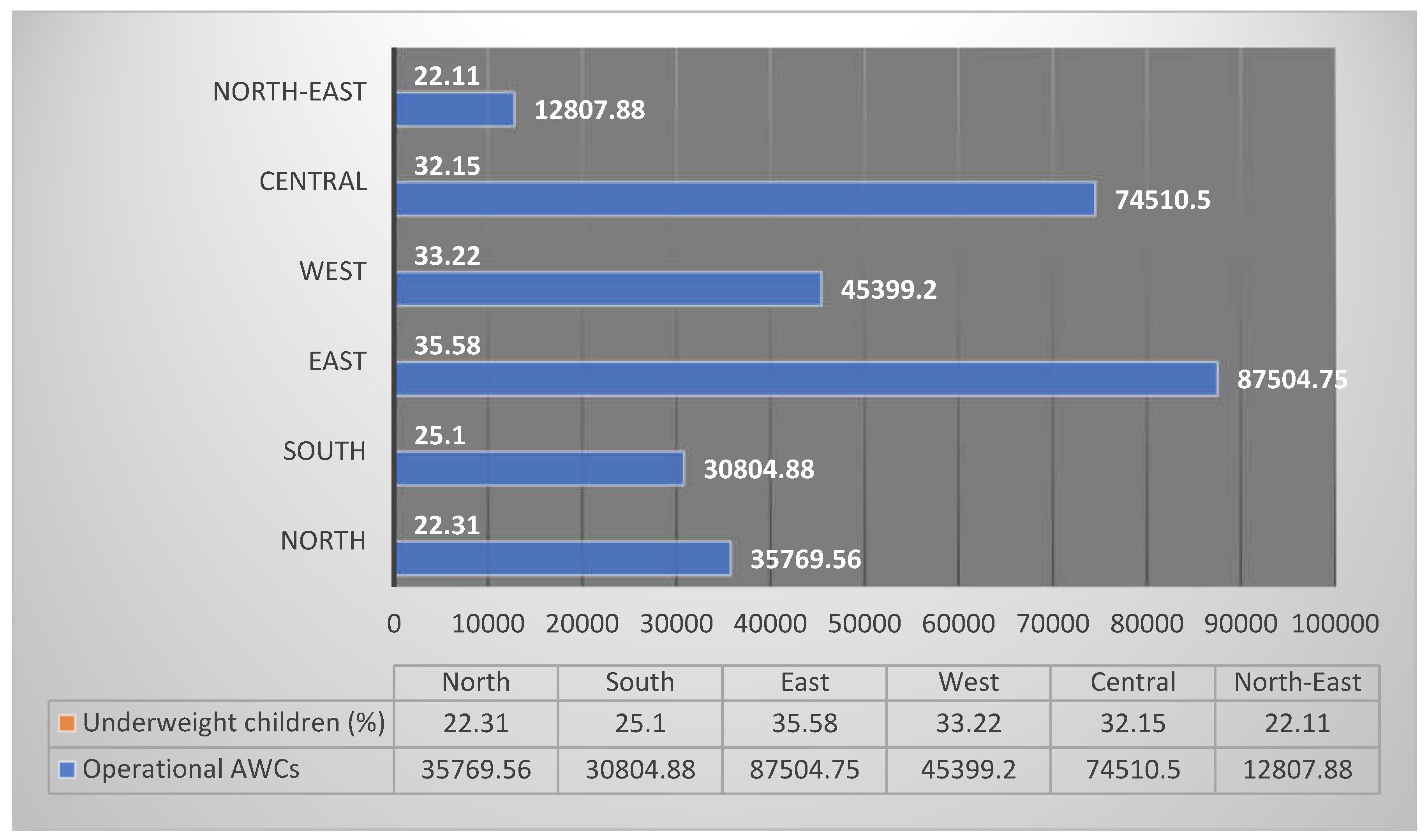
Figure 3.
Geographical distribution of average of women with Internet Access (%) and underweight children under five years (%).
Figure 3.
Geographical distribution of average of women with Internet Access (%) and underweight children under five years (%).
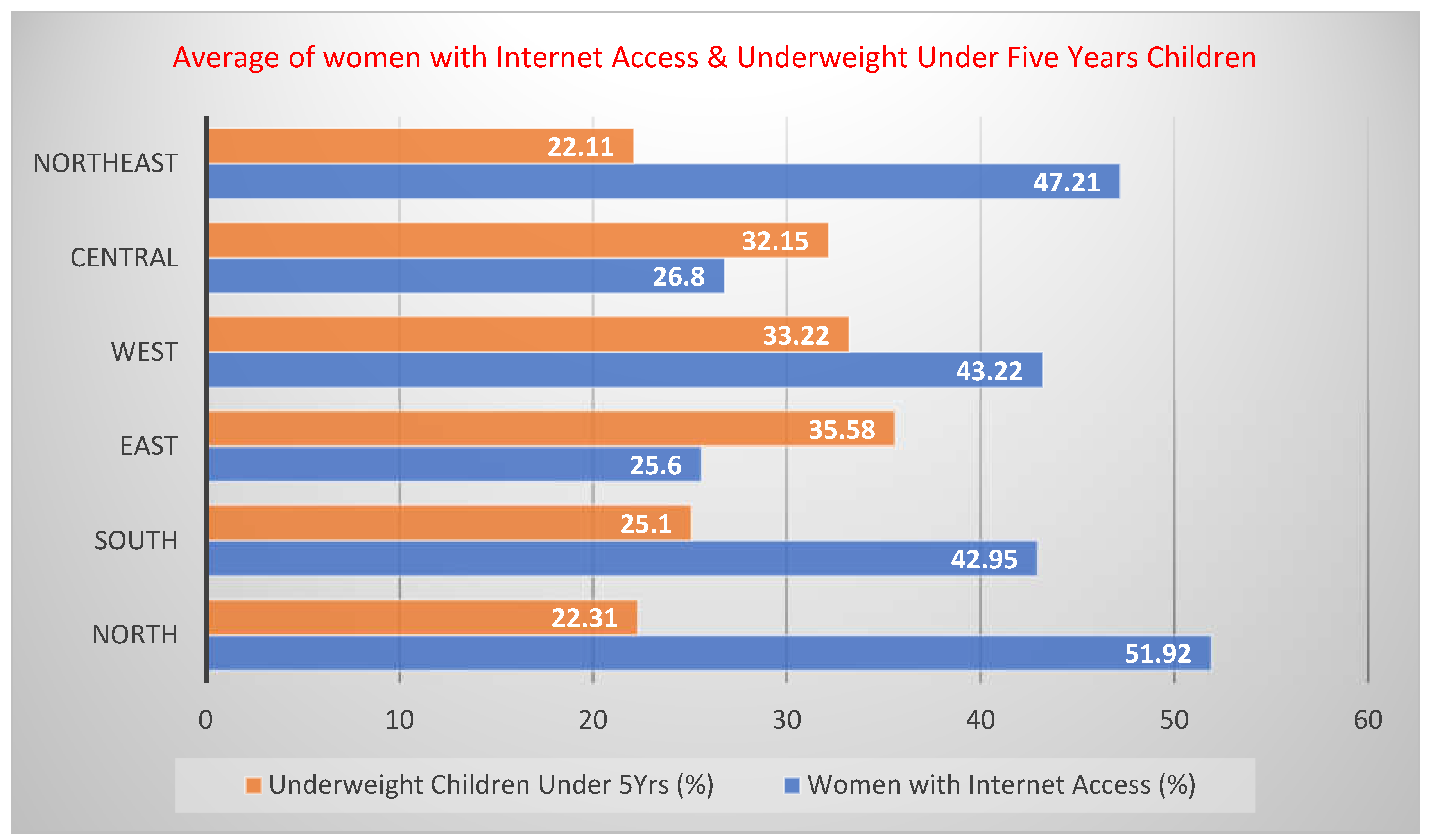

Table 1.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%).
Table 1.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%).
| National level data | % of women with internet access | % Under-weight children under 5 yrs. (weight-for-age) |
|---|---|---|
| Urban women | 51.8 | 27.3 |
| Rural Women | 24.6 | 33.8 |
| Total | 33.3 | 32.1 |
| NFHS 4 (2015-16) | -- | 35.8 |
Table 2.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the Northern region of India.
Table 2.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the Northern region of India.
| States | No. AWC operational | Women with Internet Access (%) | % Under-weight children under 5 yrs. (weight-for-age) NFHS-5 | % Under-weight children under 5 yrs. (weight-for-age) NFHS-4 (2015-16) | ||||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Total | Urban | Rural | Total | Total | ||
| Jammu & Kashmir (UT) | 28119 | 55.0 | 38.9 | 43.3 | 19.4 | 21.5 | 21.0 | 16.6 |
| Himachal Pradesh | 18925 | 78.9 | 45.2 | 49.7 | 24.6 | 25.6 | 25.5 | 21.2 |
| Punjab | 27314 | 64.1 | 48.8 | 54.8 | 17.9 | 16.4 | 16.9 | 21.6 |
| Uttarakhand | 20088 | 58.4 | 39.4 | 45.1 | 21.0 | 20.9 | 21.0 | 26.6 |
| Haryana | 25963 | 60.2 | 42.8 | 48.4 | 20.5 | 21.8 | 21.5 | 29.4 |
| Delhi | 10899 | 63.7 | 69.2 | 63.8 | 22.2 | 11.3 | 21.8 | 27.0 |
| Uttar Pradesh | 189024 | 50.2 | 24.5 | 30.6 | 28.2 | 33.1 | 32.1 | 39.5 |
| Chandigarh (UT) | 450 | 75.2 | -- | 75.2 | 20.2 | -- | 20.6 | 24.5 |
| Ladakh (UT) | 1144 | 66.5 | 54.0 | 56.4 | 17.0 | 21.2 | 20.4 | 18.7 |
| Mean | 35769.56 | 63.58 | 45.35 | 51.92 | 21.22 | 21.475 | 22.311 | 25.01 |
| Median | 20088 | 63.7 | 44.0 | 49.7 | 20.5 | 21.35 | 21.0 | 24.5 |
| Range | 188574 | 28.7 | 44.7 | 44.6 | 11.2 | 21.8 | 15.2 | 22.9 |
Table 3.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the southern region of India.
Table 3.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the southern region of India.
| States | No. AWC operational | Women with Internet Access (%) | % Under-weight children under 5 yrs. (weight-for-age) NFHS-5 | % Under-weight children under 5 yrs. (weight-for-age) NFHS-4 (2015-16) |
||||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Total | Urban | Rural | Total | Total | ||
| Andhra Pradesh | 55615 | 33.9 | 15.4 | 21.0 | 25.1 | 31.4 | 29.6 | 31.9 |
| Karnataka | 65909 | 50.1 | 24.8 | 35.0 | 29.4 | 34.9 | 32.9 | 35.2 |
| Kerala | 33115 | 64.9 | 57.5 | 61.1 | 19.4 | 19.9 | 19.7 | 16.1 |
| Tamil Nadu | 54442 | 55.8 | 39.2 | 46.9 | 20.0 | 23.5 | 22.0 | 23.8 |
| Telangana | 35693 | 43.9 | 15.8 | 26.5 | 25.8 | 35.0 | 31.8 | 28.4 |
| Puducherry (UT) | 855 | 66.9 | 50.4 | 61.9 | 15.9 | 13.7 | 15.3 | 22.0 |
| Andaman & Nicobar (UT) | 720 | 44.1 | 27.9 | 34.8 | 15.1 | 31.1 | 23.7 | 21.6 |
| Lakshadweep (UT) | 90 | 61.8 | 36.0 | 56.4 | 28.5 | 18.4 | 25.8 | 23.6 |
| Mean | 30804.88 | 52.68 | 33.38 | 42.95 | 22.4 | 25.9875 | 25.1 | 25.325 |
| Median | 34404 | 52.95 | 31.95 | 40.95 | 22.55 | 27.3 | 24.75 | 23.7 |
| Range | 65819 | 33 | 42.1 | 40.9 | 14.3 | 21.3 | 17.6 | 19.1 |
Table 4.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the Eastern region of India.
Table 4.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the Eastern region of India.
| States | No. AWC operational | Women with Internet Access (%) | % Under-weight children under 5 yrs. (weight-for-age) NFHS-5 | % Under-weight children under 5 yrs. (weight-for-age) NFHS-4 (2015-16) | ||||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Total | Urban | Rural | Total | Total | ||
| Bihar | 114989 | 38.4 | 17.0 | 20.6 | 35.8 | 41.8 | 41.0 | 43.9 |
| Jharkhand | 38431 | 57.8 | 22.7 | 31.4 | 30.0 | 41.4 | 39.4 | 47.8 |
| Odisha | 74157 | 39.7 | 21.3 | 24.9 | 21.5 | 31.0 | 29.7 | 34.4 |
| West Bengal | 122442 | 48.1 | 14.0 | 25.5 | 28.7 | 33.5 | 32.2 | 31.6 |
| Mean | 87504.75 | 46 | 18.75 | 25.6 | 29 | 36.925 | 35.575 | 39.425 |
| Median | 94573 | 43.9 | 19.15 | 25.2 | 29.35 | 37.45 | 35.8 | 39.15 |
| Range | 84011 | 19.4 | 8.7 | 10.8 | 14.3 | 10.8 | 11.3 | 16.2 |
Table 5.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the western region of India.
Table 5.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the western region of India.
| States | No. AWC operational | Women with Internet Access (%) | % Under-weight children under 5 yrs. (weight-for-age) NFHS-5 | % Under-weight children under 5 yrs. (weight-for-age) NFHS-4 (2015-16) | ||||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Total | Urban | Rural | Total | Total | ||
| Rajasthan | 61873 | 56.1 | 30.8 | 36.9 | 25.4 | 28.1 | 27.6 | 36.7 |
| Maharashtra | 110429 | 54.3 | 23.7 | 38.0 | 33.3 | 38.0 | 36.1 | 36.0 |
| Gujrat | 53027 | 48.9 | 17.5 | 30.8 | 33.3 | 43.5 | 39.7 | 39.3 |
| Goa | 1262 | 78.1 | 68.3 | 73.7 | 22.5 | 26.6 | 24.0 | 23.8 |
| Dadra & Nagar Haveli, Diu & Daman | 405 | 49.4 | 23.8 | 36.7 | 33.6 | 43.5 | 38.7 | 35.8 |
| Mean | 45399.2 | 57.36 | 32.82 | 43.22 | 29.62 | 35.94 | 33.22 | 34.32 |
| Median | 53027 | 54.3 | 23.8 | 36.9 | 33.3 | 38.0 | 36.1 | 36.0 |
| Range | 110024 | 29.2 | 50.8 | 42.9 | 11.1 | 16.9 | 15.7 | 15.5 |
Table 6.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the central region of India.
Table 6.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the central region of India.
| States | No. AWC operational | Women with Internet Access (%) | % Under-weight children under 5 yrs. (weight-for-age) NFHS-5 | % Under-weight children under 5 yrs. (weight-for-age) NFHS-4 (2015-16) | ||||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Total | Urban | Rural | Total | Total | ||
| Chhattisgarh | 51886 | 44.5 | 20.8 | 26.7 | 25.8 | 32.7 | 31.3 | 37.7 |
| Madhya Pradesh | 97135 | 46.5 | 20.1 | 26.9 | 28.6 | 34.2 | 33.0 | 42.8 |
| Mean | 74510.5 | 45.5 | 20.45 | 26.8 | 27.2 | 33.45 | 32.15 | 33.45 |
| Median | 74510.5 | 45.5 | 20.45 | 26.8 | 27.2 | 33.45 | 32.15 | 33.45 |
| Range | 45249 | 2 | 0.7 | 0.2 | 2.8 | 1.5 | 1.7 | 1.5 |
Table 7.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the north-east region of India.
Table 7.
Women with Internet Access (%) and Children Under Five Years Who are underweight (weight-for-age) (%) in the north-east region of India.
| States | No. AWC operational | Women with Internet Access (%) | % Under-weight children under 5 yrs. (weight-for-age) NFHS-5 | % Under-weight children under 5 yrs. (weight-for-age) NFHS-4 (2015-16) | ||||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Total | Urban | Rural | Total | Total | ||
| Arunachal Pradesh | 5642 | 70.0 | 49.6 | 52.9 | 13.1 | 15.8 | 15.4 | 19.4 |
| Assam | 61738 | 49.0 | 24.4 | 28.2 | 25.9 | 33.6 | 32.8 | 29.8 |
| Manipur | 11509 | 50.8 | 40.4 | 44.8 | 12.9 | 13.5 | 13.3 | 13.8 |
| Meghalaya | 5896 | 57.8 | 28.0 | 34.7 | 22.2 | 27.3 | 26.6 | 28.9 |
| Mizoram | 2244 | 83.8 | 48.0 | 67.6 | 9.3 | 15.8 | 12.7 | 12.0 |
| Nagaland | 3980 | 66.5 | 40.3 | 49.9 | 24.5 | 27.7 | 26.9 | 16.7 |
| Sikkim | 1308 | 90.0 | 68.1 | 76.7 | 9.0 | 14.9 | 13.1 | 14.2 |
| Tripura | 10146 | 36.6 | 17.7 | 22.9 | 16.4 | 28.3 | 25.6 | 24.1 |
| Mean | 12807.88 | 63.06 | 39.562 | 47.212 | 16.662 | 22.112 | 22.11 | 19.862 |
| Median | 5769 | 62.15 | 40.35 | 47.35 | 14.75 | 21.55 | 21.55 | 18.05 |
| Range | 60430 | 53.4 | 50.4 | 53.8 | 16.9 | 20.1 | 20.1 | 17.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



