
Submitted:
26 March 2024
Posted:
26 March 2024
You are already at the latest version
Abstract
Objective: This study aimed to demonstrate the availability of portable devices for nasal FeNO measurement, which could replace exhaled NO measurement based on the continuous aspiration of multiple flow measurement systems. Methods: A descriptive cross-sectional study. The healthy subjects without rhinosinusis disorders (control group) and those with diagnosed allergic rhinitis (AR group) were enrolled in the study. They underwent nasal and bronchial FeNO measurements by both fixed flow NObreath® connected to nasal mask and multiple flows HypAir FeNO®. Results: A total of 153 people were recruited including 63 healthy subjects and 90 subjects with AR. There were no statistically significant differences in anthropometric characteristics between the two groups (P > 0.05). There were a significant increase in FeNO values in the AR group compared to the control group; concentrations of nasal and bronchial FeNO mearsured by NObreath® were 76.0 ± 50.7 ppb (vs 36.0 ± 28.1 ppb, P < 0.01) and 32.3 ± 15.4 ppb (vs 9.2 ± 5.6 ppb, P < 0.001), and those mearsured by NObreath® Hypair FeNO® were 1796.9 ± 523.3 ppb (vs 400.2 ± 123.1 ppb, P < 0.001) and 37.3 ± 23.0 ppb (vs 17.4 ± 18.3 ppb, P < 0.01). A weak correlation between the values measured by NObreath® and Hypair FeNO® devices was observed (r = 0.023 and r = 0.089, respectively; p < 0.05). Conclusions: The handheld NObreath® device is effective in measuring FeNO concentrations in both normal subjects and AR patients. The advantages in price and size, creating a compact, low-cost device that is convenient for use and research.
Keywords:
fractional exhaled nitric oxide
; nasal FeNO
; bronchial FeNO
1. Introduction
Since the first scientific experimental report thirty years ago in the presence of nitric oxide (NO) in exhaled air [1,2], the measurement of exhaled NO has become a common functional test in the management of allergic rhinitis, asthma, and other airway diseases [3,4,5]. Currently, exhaled NO is officially recognized as a biomarker of eosinophil-induced inflammation in the airway. The measurement of fractional exhaled NO (FeNO) has been standardized for routine use in clinical practice worldwide [6,7]. This technique is now useful with the use of handheld devices which are relatively inexpensive and can be used in hospitals, clinics, and even in patients' homes.
There are different techniques used to measure exhaled NO concentration and the most commonly used is chemiluminescence. This technique is highly sensitive and exhaled NO can be detected at part per billion, allowing a direct measurement of exhaled NO in subjects with upper and lower airway diseases [8,9,10]. Recently a new NO analysis method based on an electroluminescent technique has been developed and used for measuring exhaled NO [11,12]. The electroluminescent technique has been shown to have high accuracy and good correlation with other techniques and has the advantage of being portable due to its small size compared with a fixed routine chemiluminescent device. The measuring principle of these new devices is based on the electrochemical sensors of the instrument for NO analysis. The signal emitted from the sensor corresponds directly to the partial pressure of NO in exhaled breath, and therefore it is equivalent to the concentration of NO in the sample [12].
In the upper airway, the measurement of nasal FeNO is very useful for the diagnosis of different diseases, including allergic rhinitis, primary ciliary dyskinesia, cystic fibrosis, and sinusitis. The current method used to measure of nasal FeNO is based on the continuous aspiration of multiple flow measurement systems. However, these devices are expensive and unfordable for some low-resource health care centers, especially those in developing countries. Therefore, the use of portable devices with fixed expiratory flow to measure bronchial FeNO might be useful for measuring nasal FeNO. Thus, the present study aimed to demonstrate the availability of portable devices in the measurement of nasal FeNO.
2. Methods
2.1. Study Design and Participants
The study was a cross-sectional and descriptive study. The clinical and functional data were recorded for analysis. Briefly, the study participants including healthy subjects without rhinosinusis disorders (control group) and those with diagnosed allergic rhinitis (AR group) were enrolled in the present study. They were referred to the Clinical Research Center of Lam Dong Medical College after signing the written informed consent. The study had been approved by IRB of Lam Dong Medical College - Vietnam (Approval No. LMC.NCKH.06.2022). This study was conducted according to the ethical principles of the Declaration of Helsinki, and all participants gave written informed consent.
The inclusion criteria for this study were including healthy subjects without any medical histories were included and defined as a control group and subjects with AR symptoms (nasal congestion, runny nose, nasal itching, or sneezing) lasting more than 4 days per week and more than 4 consecutive weeks were classified into AR group [4]. Among subjects with AR, those with diagnosed asthma were randomized for measuring bronchial FeNO. Participants were excluded from the study if they had any severe cardio-respiratory diseases, treated with oral or local corticosteroids, diagnosed septal deviation or nasal polyp, acute upper or lower airway infection in the past 15 days. Participants who unable to perform nasal FeNO measurements were also excluded from the present study.
2.2. Measurement of Nasal FENO
Nasal FeNO measurements were performed by using both fixed flow NObreath® (Bedfront Scientis Ltd, Kent, England) connected to nasal mask and multiple flows Hypair FeNO® (Medisoft; Sorinnes, Belgium). The measure of nasal FeNO was done according to the manufacturer's instructions and as recommended by the ATS (American Thoracic Society)/ERS (European Respiratory Society) guidelines [6].
Nasal FeNO done by NObreath® was measured firstly with an expiratory airflow of 50 mL/second and performed mainly by breathing directly into the device; the result was displayed immediately on the device screen. Briefly, the study subject sat in a comfortable position with the nasal mask covering his/her nose to blow out the air from the nasal expiratory breath (Figure 1).
Nasal FeNO done by Hypair FeNO® Machine was done secondly after Nobreath® measurement and as described previously [4]. In brief, the study subject connected a catheter to one of the nostrils, and airflow from the nasal cavity was continuously aspirated and measured by NO electroluminescent sensor. During the analysis, the study subject breathed continuously through an expiratory brake so that the velum was closed to prevent any contamination of nasal air with the air coming from the lower airways. The aspiration flow rate of 100 mL/s was used to measure nasal NO. All the data were reported by Expair Software (Medisoft; Sorinnes, Belgium). The mean value of two correct measurements was used for analysis.
2.3. Measurement of Bronchial FeNO
For the airways, bronchial FeNO measurements were also performed by using both portable device NObreath® and Hypair FeNO® device. The measure of bronchial FENO was done at a standard flow rate (50 ml/s) according to the manufacturer's instructions and as recommended by the ATS (American Thoracic Society)/ERS (European Respiratory Society) guidelines (7).
Firstly, bronchial FENO measurements were performed by the portable device using NO Breath®. The study subjects needed to exhale through the mouthpiece with a flow rate at 50 mL/s; the technician connected the mouthpiece to the NObreath®. The technique was performed similarly to measuring nasal NO until a reading was displayed.
Bronchial FeNO was measured by the Hypair FeNO® device after NOBreath®, also at a flow rate of 50 ml/s. When using the HypAir FeNO, participants inhaled free air through an NO scrubber, thereby excluding the influence of ambient NO. Participants then exhaled back into the machine. A sample of the expired air was collected within the unit and analyzed by a fuel cell to determine the concentration of NO. The results of exhaled NO had been reported by Expair Software (Medisoft). The mean value of two correct measurements was used for analysis.
2.4. Statistical Analysis
The statistics were conducted with SPSS software version 22.0 (Chicago, IL, USA). The data were presented as mean ± standard deviation (SD) and frequency or percentage. The t-student test was used to compare quantitative and continuous values. The correlation between FENO measured by NObreath and Hypair FeNO® was evaluated by the Pearson correlation test. The P-value of less than 0.05 was considered statistically significant.
3. Results
3.1. Anthropometric Characteristics
During the study period, 153 individuals (male accounting for 59.5%), whose mean age was was 38.7 ± 19.5 years, were included. The mean height and weight of study subjects were 153.8 ± 13.5 cm and 50.9 ± 14.2 kg, respectively. The mean BMI of study subjects was 21.2 ± 3.6 kg/m2 (Table 1). There was no statistically significant difference regarding anthropometric characteristics between control group and AR group (Table 1).
3.2. Results of Nasal and Bronchial FeNO Levels in Two Study Groups
In this study, the mean concentrations of bronchial FeNO and nasal FeNO in healthy subjects measured by the NObreath® (handeld device) were 9.2 ± 5.6 ppb and 36.0 ± 28.1 ppb, respectively; that one measured by the Hypair FeNO® device were 17.4 ± 18.3 ppb and 400.2 ± 123.1 ppb, respectively. In subjects with AR, the results showed the significantly increases of FeNO concentrations of the bronchis (measured through the mouth) and the nose when measured by both two devices, compared to control group: 32.3 ± 15.4 ppb (P < 0.001) and 76.0 ± 50.7 ppb (P < 0.01) in the order given, with NObreath®; and 37.3 ± 23.0 ppb (P < 0.01) and 1796.9 ± 523.3 ppb (P < 0.001) done by Hypair FeNO® (Table 2).
3.3. Correlation between FENO Levels Measured by NObreath® and That One Measured by Hypair FeNO®
Research results showed a positive correlation between bronchial FeNO concentration measured by the handheld machine (NObreath®) and by the new generation machine (Hypair FeNO®) (Figure 2). Similar results for nasal FeNO concentrations was also illustrated with (Figure 3). However, Pearson analysis indicated that these correlations were weak (r = 0.023 and r = 0.089, respectively; p < 0.05).
4. Discussion
The FeNO concentrations is very valuable in diagnosing allergic rhinitis. The present study focuses on elucidating the effectiveness of measurement of the handheld machine (NObreath®) and the new generation machine (Hypair FeNO®). Our key findings were that FeNO concentration values measured with NObreath® and Hypair FeNO® were both significantly increased in allergic rhinitis patients compared to healthy subjects (p < 0.05). We also found a weak correlation between the measured values of these two devices (r < 0.1; p < 0.05).
In this study, there were no statistically significant differences in anthropometric characteristics (sex, age, height, weight and BMI) between the control group and the AR group, which limits confounding factors when comparing results of FeNO concentration. The present study subjects in the age of adults had the normal values of height, weight and BMI, were suitable for the physical condition of Vietnamese. The mean age of AR group was 37.1 ± 20.4 and male accounting for 59.5%, which consistent with some previous observations in AR people. Vo-Thi-Kim A et al reported the mean age of subjects with AR to be 36 ± 17 years; regarding gender, men being 1.2 times more likely than women, there were fully no difference between the AR group and the control group (p > 0.05) [4]. Similar findings were found in a prior our study in people with AR with or without asthma [13]. Clearly, the medical literatures also states that Allergic rhinitis typically starts in early childhood with the symptoms usually peaking in the third and fourth decades of life (aged of 20-40) [14,15], and men tend to be more susceptible to the disease [16]. A plausible explanation may come from the pathogenesis of AR, which like other allergic diseases, is characterized by immunological sensitization to environmental substances involving innate and adaptive immune responses [14,15].
In healthy people, the present study shown that FeNO concentration in the nose was much higher than in the bronchis (Table 1). Our previous report also mentioned that concentrations of nasal FeNO and bronchial FeNO measured by using Hypair FeNO® ranged from 300-800 and 5-25, respectively [17]. This result is related to the fact that the paranasal sinuses are an important source of nasal FeNO production. Lundberg JO and colleagues have long indicated that NO in humans is produced by epithelial cells in the paranasal sinuses and is present in very high concentrations in sinus air to maintain sterility in the paranasal sinuses through its bacteriostatic effect [2]. In fact, in the upper airways, NO concentrations measured in the nasal cavity do not only come from the paranasal sinuses by diffusion, but are also produced within the nasal cavity (epithelium) [18,19] and inflammatory cells (eosinophils) related to the upregulation of inducible NO synthase [20,21]. We also found similar findings for the handheld NObreath® device in the study, although the measurements were smaller than for the Hypair FeNO® system, which due to different structural parameters between devices [8]. The Hypair FeNO® instrument measures higher FeNO concentrations than other analyzers. This difference is not consistent enough to be able to calculate the same correction factor [22]. On the other hand, for the NObreath device, FeNO values were consistently lower than for the chemiluminescence analyzer [23]. The recommendation of bronchial FeNO concentrations mesured by electrochemical portable device was in the range of 5-25 ppb [24]. The study of Nerpin E et al demonstrated that FeNO values measured by NIOX MINO® in healthy European population were 18.2 (95% confidence interval (CI): 17.7-18.6) in men and 15.0 (95%CI:14.7-15.4) ppb in women [25]. Other authors also noted similar results in prior studies [26,27]. It is of interest that there was no significant difference in the FeNO concentration obtained using Nobreath® compared to other portable electrochemical devices such as NIOX MINO® [26,28].
In AR group, this study showed a translationally and statisticallly significant increase of the inflammatory markers in the bronchis (measured through the mouth) and in the nose when measured by Hypair FeNO® system compared to control subjects (Table 2). Our previous study found that the concentrations of nasal FeNO and bronchial FeNO in patients with AR were 1614 ± 629 and 12 ± 6 ppb, respectively. If the subject has both AR and asthma, the FeNO concentration is even higher, 1686 ± 614 and 35 ± 28 ppb in that order [13]. Other studies also demonstrated that patients with AR had a higher level of nasal FeNO than healthy subjects [12,21]. The results of these studies also showed that the increased production of FeNO might be triggered by allergens in air and could be measured by constant aspiration or with expiratory flow. Similar to the FeNO values mesured by Hypair FeNO®, there was a translationally increase in bronchial and nasal FeNO measured by handheld NObreath® device in the group with AR compared with the control group (Table 2). Several research have previously argued that measuring nasal FeNO with a portable device is useful in the management of patients with AR [20,21]. Similar to other airway inflammatory disorders such as asthma, the nasal mucosa of AR patients is characterized by high nitric oxide synthase expression and activity [29]. Therefore, nasal FeNO can be considered a suitable biomarker for diagnosing allergic rhinitis and assessing the severity of allergic rhinitis.
The research results showed a positive correlation between bronchial or nasal FeNO levels measured by a handheld machine (NObreath®) and by a new generation machine (Hypair FeNO®) (Figure 1, Figure 2). Some prior studies have also shown a correlation between NObreath and other FeNO measuring devices. Antus B et al reported that FeNO concentrations measured with NObreath and Logan (Logan LR2500) were similar and a very strong linear relationship was found between the two devices (r = 0.923, P < 0.001 ). On the other hand, FeNO concentrations measured by NObreath were slightly higher than by NIOX MINO, but still showed a strong correlation (r = 0.681, P < 0.001) [26]. The research of Saito J et al found that there were strong positive correlations in FeNO levels measured by the NA623NP®, NIOX MINO®, and NObreath® (p < 0.001). FeNO concentration obtained by NObreath® were intermediate [28]. Inoue Y and colleagues compared the NIOX VERO® to NObreath®, two handheld electrochemical analyzers, reporting a high correlation (r = 0.92) but differing agreement for FeNO values, FeNO concentration < 58 ppb suggested NObreath® < NIOX VERO®, whereas FeNO concentration > 58 ppb suggested NObreath® > NIOX VERO® [29]. These result has important implications for the application of handheld NO devices in the diagnosis and monitoring of AR.
The current study shows that Nobreath® device is as effective as Hypair FeNO® system (a new generation machine) in measuring FeNO concentrations in healthy subjects and AR patients. Application of NObreath® device can make the use and the research faster, more convenient, and more suitable due to its compactness. However, the study also has limitations in that the sample size is small and the application of FeNO measurement in patients with AR is relatively complicated and inconsistent. We suggest that the measurement of FeNO concentrations in healthy subjects and in patients with allergic rhinitis be standardized and clearly defined considering its variability with confounding factors. Finally, the accuracy and reproducibility of the method need to be validated in rigorous cohorts [31].
5. Conclusion
The levels of bronchial and nasal inflammatory markers exceeding the normal range indicated the presence of inflammation in the airways. The highlight of our study was the improvement of the NObreath® device to measure FeNO. We indicated a significant increase in FeNO values of AR patients compared to that of healthy subjects, and a positive correlation in FeNO concentrations measured by Nobreath® and Hypair FeNO®. The handheld Nobreath® device with electrochemical technology has the advantages in price and size, creating a compact, low-cost device that is convenient for use and research. Therefore, this technique can be measured at home or in different locations.
References
- Gustafsson LE, Leone AM, Persson MG, Wiklund NP, Moncada S. Endogenous nitric oxide is present in the exhaled air of rabbits, guinea pigs and humans. Biochem Biophys Res Commun. 1991 Dec 16;181(2):852-857. https://10.1016/0006-291x(91)91268-h. [CrossRef]
- Lundberg JO, et al. High nitric oxide production in human paranasal sinuses. Nat Med. 1995 Apr;1(4):370-373. https://10.1038/nm0495-370. [CrossRef]
- Abba AA. Exhaled nitric oxide in diagnosis and management of respiratory diseases. Ann Thorac Med. 2009 Oct;4(4):173-181. https://10.4103/1817-1737.56009. [CrossRef]
- Vo-Thi-Kim A, Van-Quang T, Nguyen-Thanh B, Dao-Van D, Duong-Quy S. The effect of medical treatment on nasal exhaled nitric oxide (NO) in patients with persistent allergic rhinitis: A randomized control study. Adv Med Sci. 2020 Mar;65(1):182-188. https://10.1016/j.advms.2019.12.004. [CrossRef]
- Duong-Quy S, et al. Study of Exhaled Nitric Oxide in Subjects with Suspected Obstructive Sleep Apnea: A Pilot Study in Vietnam. Pulm Med. 2016;2016:3050918. https://10.1155/2016/3050918. [CrossRef]
- American Thoracic Society; European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005 Apr 15;171(8):912-930. https://10.1164/rccm.200406-710ST. [CrossRef]
- Dweik RA, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011 Sep 1;184(5):602-615. https://10.1164/rccm.9120-11ST. [CrossRef]
- Maniscalco M, et al. Fractional exhaled nitric oxide-measuring devices: technology update. Med Devices (Auckl). 2016 Jun 23;9:151-160. https://10.2147/MDER.S91201. [CrossRef]
- Ragnoli B, et al. Fractional nitric oxide measurement in exhaled air (FeNO): perspectives in the management of respiratory diseases. Ther Adv Chronic Dis. 2023 Aug 1;14:20406223231190480. https://10.1177/20406223231190480. [CrossRef]
- Weschta M, Deutschle T, Riechelmann H. Nasal fractional exhaled nitric oxide analysis with a novel hand-held device. Rhinology. 2008 Mar;46(1):23-27.
- Duong-Quy S. Clinical Utility Of The Exhaled Nitric Oxide (NO) Measurement With Portable Devices In The Management Of Allergic Airway Inflammation And Asthma. J Asthma Allergy. 2019 Oct 7;12:331-341. https://10.2147/JAA.S190489. [CrossRef]
- Takeno S, Okabayashi Y, Kohno T, Yumii K, Hirakawa K. The role of nasal fractional exhaled nitric oxide as an objective parameter independent of nasal airflow resistance in the diagnosis of allergic rhinitis. Auris Nasus Larynx. 2017 Aug;44(4):435-441. https://10.1016/j.anl.2016.09.007. [CrossRef]
- Duong-Quy S, et al. Study of nasal exhaled nitric oxide levels in diagnosis of allergic rhinitis in subjects with and without asthma. J Asthma Allergy. 2017 Mar 22;10:75-82. https://10.2147/JAA.S129047. [CrossRef]
- Nur Husna SM, Tan HT, Md Shukri N, Mohd Ashari NS, Wong KK. Allergic Rhinitis: A Clinical and Pathophysiological Overview. Front Med (Lausanne). 2022 Apr 7;9:874114. https://10.3389/fmed.2022.874114. [CrossRef]
- Wang IJ, Tung TH, Tang CS, Zhao ZH. Allergens, air pollutants, and childhood allergic diseases. Int J Hyg Environ Health. 2016 Jan;219(1):66-71. https://10.1016/j.ijheh.2015.09.001. [CrossRef]
- Fröhlich M, et al. Is there a sex-shift in prevalence of allergic rhinitis and comorbid asthma from childhood to adulthood? A meta-analysis. Clin Transl Allergy. 2017 Dec 5;7:44. https://10.1186/s13601-017-0176-5. [CrossRef]
- Duong-Quy S, et al. Study of Nasal Fractional Exhaled Nitric Oxide (FENO) in Children with Allergic Rhinitis. Sinusitis. 2021 Oct 8; 5(2):123-131. https://doi.org/10.3390/sinusitis5020013. [CrossRef]
- Cho WS, et al. Increased expression of arginase I and II in allergic nasal mucosa. Laryngoscope. 2011 Feb;121(2):236-240. https://10.1002/lary.21288. [CrossRef]
- Hood CM, Schroter RC, Doorly DJ, Blenke EJ, Tolley NS. Computational modeling of flow and gas exchange in models of the human maxillary sinus. J Appl Physiol (1985). 2009 Oct;107(4):1195-203. https://10.1152/japplphysiol.91615.2008. [CrossRef]
- Bautista AP, Eisenlohr CP, Lanz MJ. Nasal nitric oxide and nasal eosinophils decrease with levocetirizine in subjects with perennial allergic rhinitis. Am J Rhinol Allergy. 2011 Nov-Dec;25(6):383-7. https://10.2500/ajra.2011.25.3668. [CrossRef]
- Nesic VS, et al. Measuring nasal nitric oxide in allergic rhinitis patients. J Laryngol Otol. 2016 Nov;130(11):1064-1071. https://10.1017/S0022215116009087. [CrossRef]
- Korn S, Telke I, Kornmann O, Buhl R. Measurement of exhaled nitric oxide: comparison of different analysers. Respirology. 2010 Nov;15(8):1203-1208. https://10.1111/j.1440-1843.2010.01847.x. [CrossRef]
- Pisi R, et al. Measurement of fractional exhaled nitric oxide by a new portable device: comparison with the standard technique. J Asthma. 2010 Sep;47(7):805-809. https://10.3109/02770903.2010.485667. [CrossRef]
- Heffler E, et al. Fractional Exhaled Nitric Oxide (FENO) in the management of asthma: a position paper of the Italian Respiratory Society (SIP/IRS) and Italian Society of Allergy, Asthma and Clinical Immunology (SIAAIC). Multidiscip Respir Med. 2020 Feb 19;15(1):36. https://10.4081/mrm.2020.36. [CrossRef]
- Nerpin E, et al. Determinants of fractional exhaled nitric oxide in healthy men and women from the European Community Respiratory Health Survey III. Clin Exp Allergy. 2019 Jul;49(7):969-979. https://10.1111/cea.13394. [CrossRef]
- Antus B, Horvath I, Barta I. Assessment of exhaled nitric oxide by a new hand-held device. Respir Med. 2010 Sep;104(9):1377-1380. https://10.1016/j.rmed.2010.06.005. [CrossRef]
- Rawy A.M. Measurement of exhaled nitric oxide in healthy Egyptian population: normal ranges and factors affecting. Egypt J Bronchol. 2015 Mar 20;9:48-54. https://doi.org/10.4103/1687-8426.153599. [CrossRef]
- Saito J, et al. Comparison of fractional exhaled nitric oxide levels measured by different analyzers produced by different manufacturers. J Asthma. 2020 Nov;57(11):1216-1226. https://10.1080/02770903.2019.1642351. [CrossRef]
- Kawamoto H, Takeno S, Yajin K. Increased expression of inducible nitric oxide synthase in nasal epithelial cells in patients with allergic rhinitis. Laryngoscope. 1999 Dec;109(12):2015-2020. https://10.1097/00005537-199912000-00023. [CrossRef]
- Inoue Y, Sato S, Manabe T, Makita E, Chiyotanda M, Takahashi K, Yamamoto H, Yanagida N, Ebisawa M. Measurement of Exhaled Nitric Oxide in Children: A Comparison Between NObreath® and NIOX VERO® Analyzers. Allergy Asthma Immunol Res. 2018 Sep;10(5):478-489. doi: 10.4168/aair.2018.10.5.478. PMID: 30088368; PMCID: PMC6082813. [CrossRef]
- Högman M, Bowerman C, Chavez L, Dressel H, Malinovschi A, Radtke T, Stanojevic S, Steenbruggen I, Turner S, Dinh-Xuan AT; Global Lung Function Initiative FENO Task Force. ERS technical standard: Global Lung Function Initiative reference values for exhaled nitric oxide fraction (FENO50 ). Eur Respir J. 2024 Jan 25;63(1):2300370. doi: 10.1183/13993003.00370-2023. PMID: 37973177. [CrossRef]
Figure 1.
Nasal FENO measurement was performed by using NObreath® device (left side) and Hypair FeNO® (right side).
Figure 1.
Nasal FENO measurement was performed by using NObreath® device (left side) and Hypair FeNO® (right side).
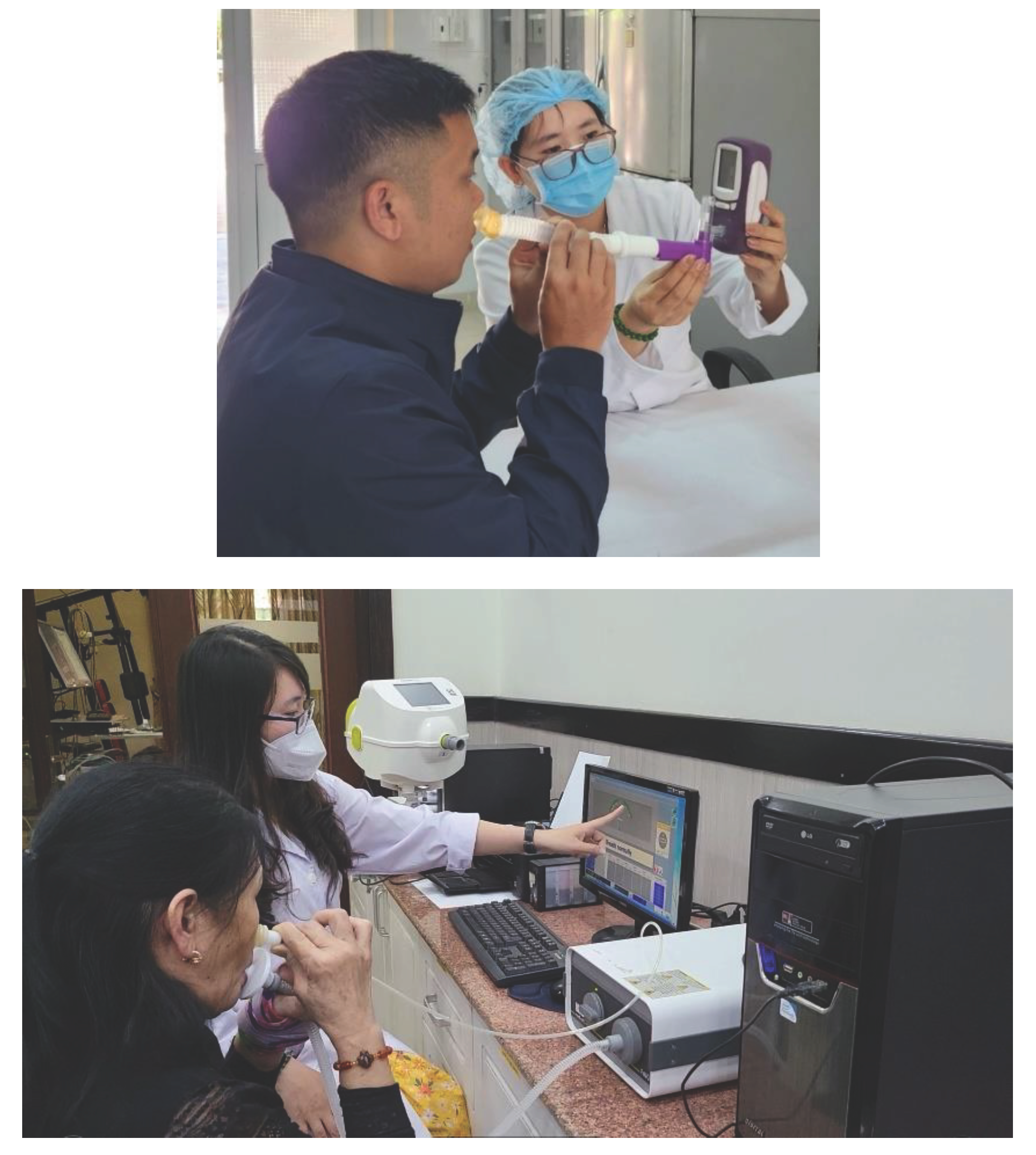
Figure 2.
Correlation between bronchial FeNO levels measured by NObreath® and Hypair FeNO® in subjects with AR and diagnosed asthma (N = 30).
Figure 2.
Correlation between bronchial FeNO levels measured by NObreath® and Hypair FeNO® in subjects with AR and diagnosed asthma (N = 30).
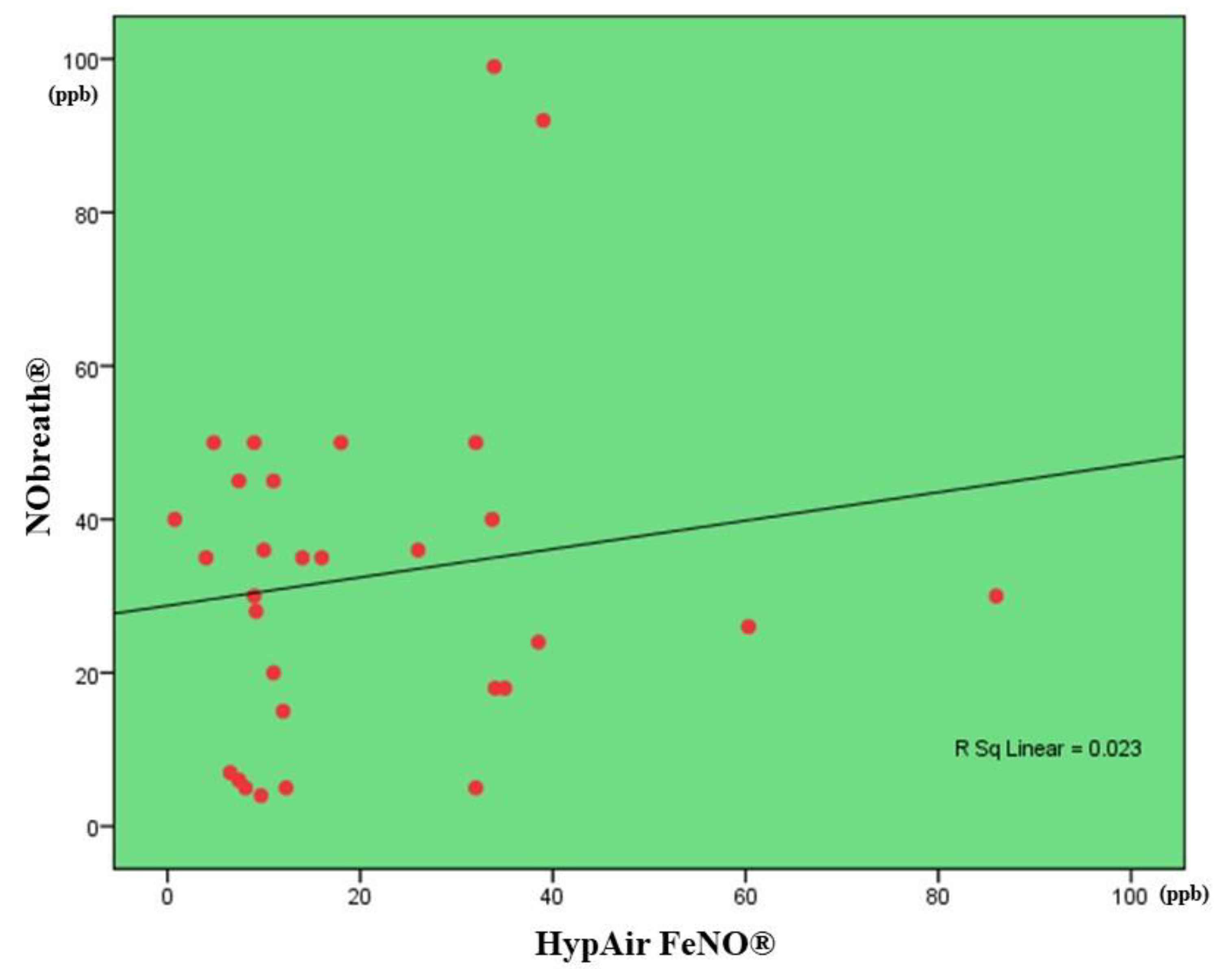
Figure 3.
Correlation between nasal FeNO levels measured by NObreath® and Hypair FeNO® (N = 90).
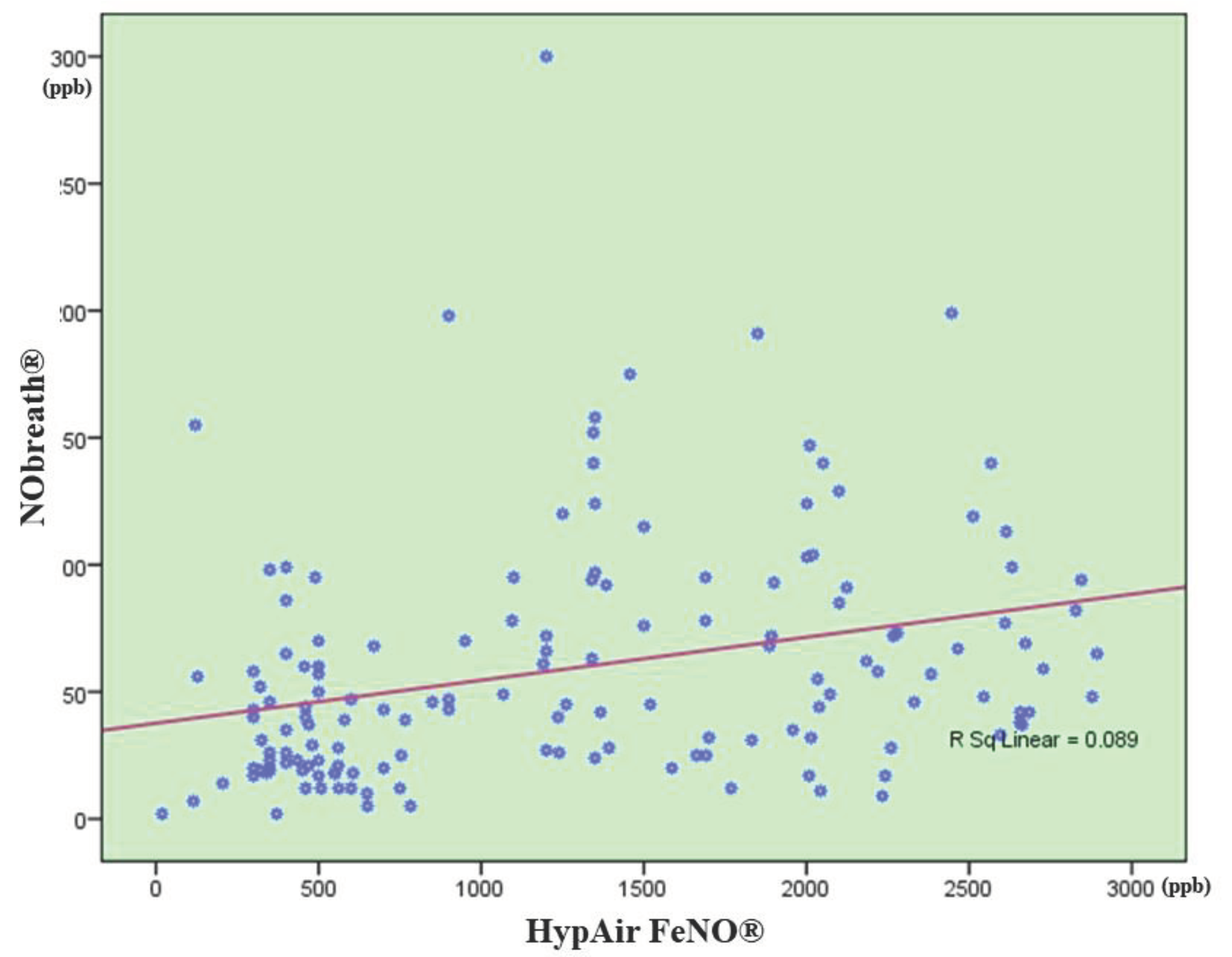

Table 1.
Anthropometric characteristics of the study subjects.
| Factors | All subjects (N = 153) |
Control group (N = 63) |
AR group (N = 90) |
P* |
|---|---|---|---|---|
| Age, years (mean ± SD) | 38.7 ± 19.5 | 38.5 ± 19.7 | 37.1 ± 20.4 | NS |
| Sex Female, N (%) Male, N (%) |
62 (40.5) 91 (59.5) |
29 (46.0) 34 (54.0) |
28 (31.1) 62 (68.9) |
NS NS |
| Height, cm (mean ± SD) | 153.8 ± 13.5 | 155.6 ± 12.9 | 152.7 ± 12.2 | NS |
| Weight, kg (mean ± SD) | 50.9 ± 14.2 | 51.7 ± 14.4 | 50.5 ± 12.7 | NS |
| BMI, kg/m2 (mean ± SD) | 21.2 ± 3.6 | 21.7 ± 3.9 | 20.9 ± 3.3 | NS |
*: patients with AR vs control subjects; NS: not significant (P > 0.05); AR: allergic rhinitis; BMI: body mass index; SD: standard deviation.
Table 2.
Results of nasal and bronchial FeNO measured by NObreath® and by Hypair FeNO®.
| Parameters | Control group | AR group | P |
|---|---|---|---|
| NObreath® | |||
| Nasal FeNO, ppb | 36.0 ± 28.1 (N = 63) |
76.0 ± 50.7 (N = 90) |
< 0.01 |
| Bronchial FeNO, ppb | 9.2 ± 5.6 (N = 63) |
32.3 ± 15.4 (N = 30) |
< 0.001 |
| Hypair FeNO® | |||
| Nasal FeNO, ppb | 400.2 ± 123.1 (N = 63) |
1796.9 ± 523.3 (N = 90) |
< 0.001 |
| Bronchial FeNO, ppb | 17.4 ± 18.3 (N = 63) |
37.3 ± 23.0 (N = 30) |
< 0.01 |
| Parameters | NObreath® (ppb) |
Hypair FeNO® (ppb) |
P |
| Control group (N = 63) | |||
| Nasal FeNO, ppb | 36.0 ± 28.1 (N = 63) |
400.2 ± 123.1 (N = 63) |
N/A |
| Bronchial FeNO, ppb | 9.2 ± 5.6 (N = 63) |
17.4 ± 18.3 (N = 63) |
N/A |
| AR group (N = 90) | |||
| Nasal FeNO, ppb | 76.0 ± 50.7 (N = 90) |
1796.9 ± 523.3 (N = 90) |
N/A |
| Bronchial FeNO, ppb | 32.3 ± 15.4 (N = 30) |
37.3 ± 23.0 (N = 30) |
N/A |
FeNO: fractional exhaled nitric oxide; N/A: not applicable.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



