Submitted:
25 March 2024
Posted:
27 March 2024
You are already at the latest version
Abstract
In chronic myeloid leukemia (CML), a clonal proliferative disorder of granulocytic lineage, the 90%‐95% of cases are characterized by t(9;22) (q34.1;q11.2) translocation, leading to the Philadelphia chromosome (1). Rarely, CML patients directly present a blast crisis, mostly of myeloid origin (2, 3). Herein, we describe one rare CML case, showing an unusual early T lymphoid blastic crisis.
Keywords:
chronic myeloid leukemia
; T lymphoid blastic crisis
Introduction
Chronic myeloid leukemia (CML) is an uncontrolled malignant proliferation of bone marrow myeloid cells, driven by the expression of the constitutively active fusion product tyrosine kinase BCR/ABL (1).
The predisposing risk factors are unknown, it was evaluated an increased incidence of CML among survivors experienced the atomic bombing (4).
CML occurs in about 0.7 to 1 in 100,000 individuals per year according to several European registries and involves patients in the ages of 40 to 70s, with a male predominance (5).
Prognosis and outcome of patients considerably improved (6) and progress in the use of the tyrosine kinase inhibitors (TKIs) is ongoing. CML often presents with nonspecific symptoms and the quality of life in patients with CML has strongly improved because of TKIs therapy. Most patients are asymptomatic in the chronic phase, but complications of CML including the risk of transforming into life-threatening myeloid blast crises continue to exist (7).
In this case report, we discuss of a young male patient who presented an accelerated phase of atypical T-lymphoid blast crisis of CML without previously distinct features reported.
Case Report
A 40-year-old male patient, admitted to the Emergency Department for pallor, skin rash and facial swelling, presented hepatosplenomegaly and bilateral multidistrict lymphadenopathies involving the submandibular, laterocervical, axillary, and inguinal regions; in addition, he presented profuse night sweats associated with fatigue; no weight loss was reported. Patient resulted positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with mild symptoms and was hospitalized in the Infectious Diseases Department.
Biochemical parameters, performed on Roche Cobas® 8000, shown no critical abnormalities, except for LDH high levels (825 U/L).
Peripheral whole blood cell count was performed on Sysmex XN-9100™ automatic hematology analyzer. Whole blood cell count showed leukocytosis (WBC 310,0 x 109/L), anemia (Hb 8,2 g/dL) and thrombocytopenia (PLT 85,0 x 109/L). The differential leukocyte count channel showed an anomalous WBC scattergram, with unseparated cell clusters and flags indicating the presence of atypical lymphocytes and presence of blasts cells.
Peripheral blood smear was performed using an automatic smear-making/staining device (Sysmex SP-1000i™) and the microscopic revision of the blood smear showed a double pathological cell population with blast appearance showing immature chromatin, basophilic cytoplasm, and evident nucleoli (62% of total cells): a small one with lymphoid characteristics and a second one of larger size, sometimes with fine granulations [Figure 1A].
A comprehensive flow-cytometry antigen panel was used for the immunophenotypic characterization. Data acquisition was carried out on a BD FACSCanto™ II equipped with BD FACSDiVA™ software.
The antigen profile confirmed the presence of two abnormal cell populations: a first one (50% of total cells) with immature T-lymphoid phenotype (CD34+, TdT+, cyCD3+, sCD3) and a second one (20% of total cells) with immature myeloid progenitors’ phenotype (CD117+, CD33+) showing an aberrant CD7 expression [Figure 1B].
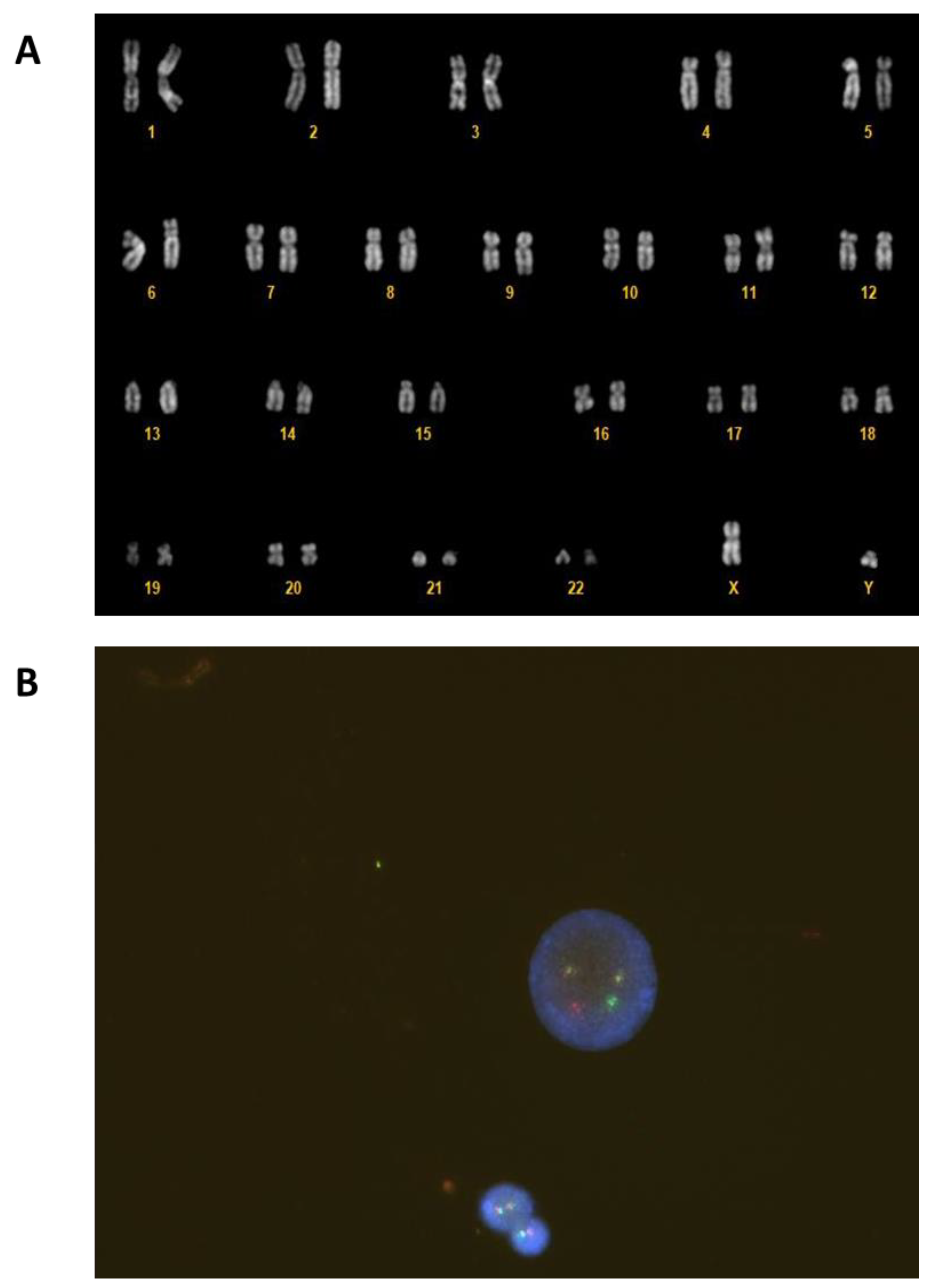
The cytogenetic analysis was performed on a bone marrow (BM) sample after 24 hours the culture was harvested, and the slides were GTG banded. Fluorescence in situ hybridization (FISH) was performed on an uncultured sample with MetaSystems™ XL BCR/ABL probe. Both FISH and cytogenetic analysis showed the Philadelphia translocation [Figure 2].
After two weeks, patient resulted SARS-CoV-2 negative and was transferred to the Hematology Department. During hospitalization, genetic analysis was performed.
Next-generation sequencing (NGS) analysis was done on BM sample using Ion GeneStudio™ S5 System and Oncomine™ Myeloid Assay kit.
NGS documented two somatic mutations in the WT1 gene: the previously described c.1372C>T; p.R458X [VAF: 43%], (8), and the unknown c.1108_1109insA; p.R370Qfs*15 [VAF: 42%].
Taken together, all these features were consistent with early T-lymphoid blast crisis of chronic myeloid leukemia.
Figure 1.
Peripheral blood leukocytosis with left shift and blasts of different size (arrows) (May-Grunwald-Giemsa stain, ×100) (A). Representative flow cytometry dot plot graphs showing two abnormal populations: one characterized by immature T-lymphoid phenotype (CD34+, TdT+, cyCD3+, sCD3-) in blue and one with characteristics of immature myeloid phenotype (CD117+, CD33+) and CD7 aberrant expression in red (B).
Figure 1.
Peripheral blood leukocytosis with left shift and blasts of different size (arrows) (May-Grunwald-Giemsa stain, ×100) (A). Representative flow cytometry dot plot graphs showing two abnormal populations: one characterized by immature T-lymphoid phenotype (CD34+, TdT+, cyCD3+, sCD3-) in blue and one with characteristics of immature myeloid phenotype (CD117+, CD33+) and CD7 aberrant expression in red (B).
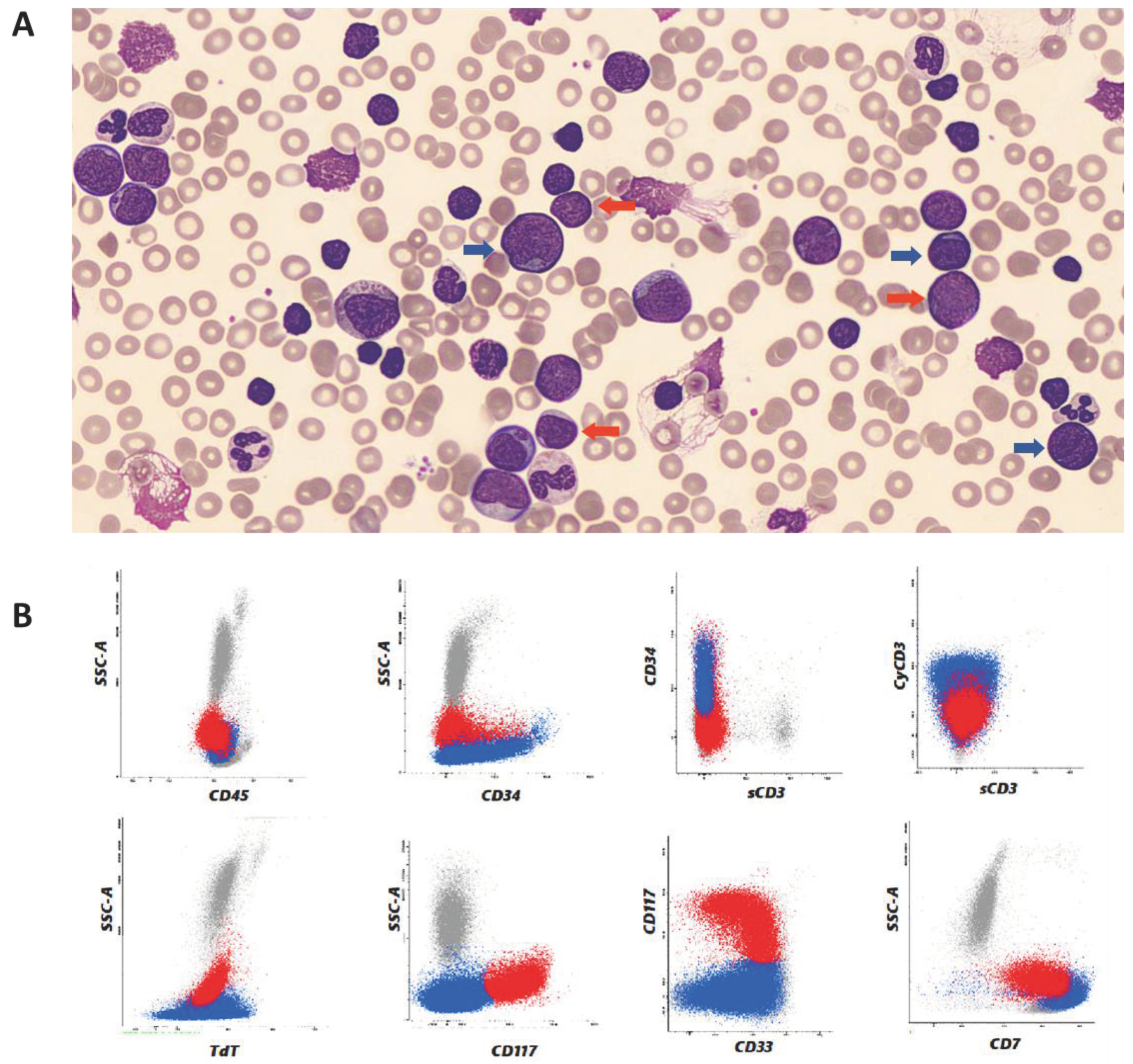
Figure 2.
G-banded karyotype on cells from BM sample with the classic Philadelphia translocation t(9;22)(q34;q11) (A). Fluorescence in situ hybridization (FISH) showed BCR/ABL1 fusion on interphase nuclei with a dual fusion translocation probe (B).
Figure 2.
G-banded karyotype on cells from BM sample with the classic Philadelphia translocation t(9;22)(q34;q11) (A). Fluorescence in situ hybridization (FISH) showed BCR/ABL1 fusion on interphase nuclei with a dual fusion translocation probe (B).
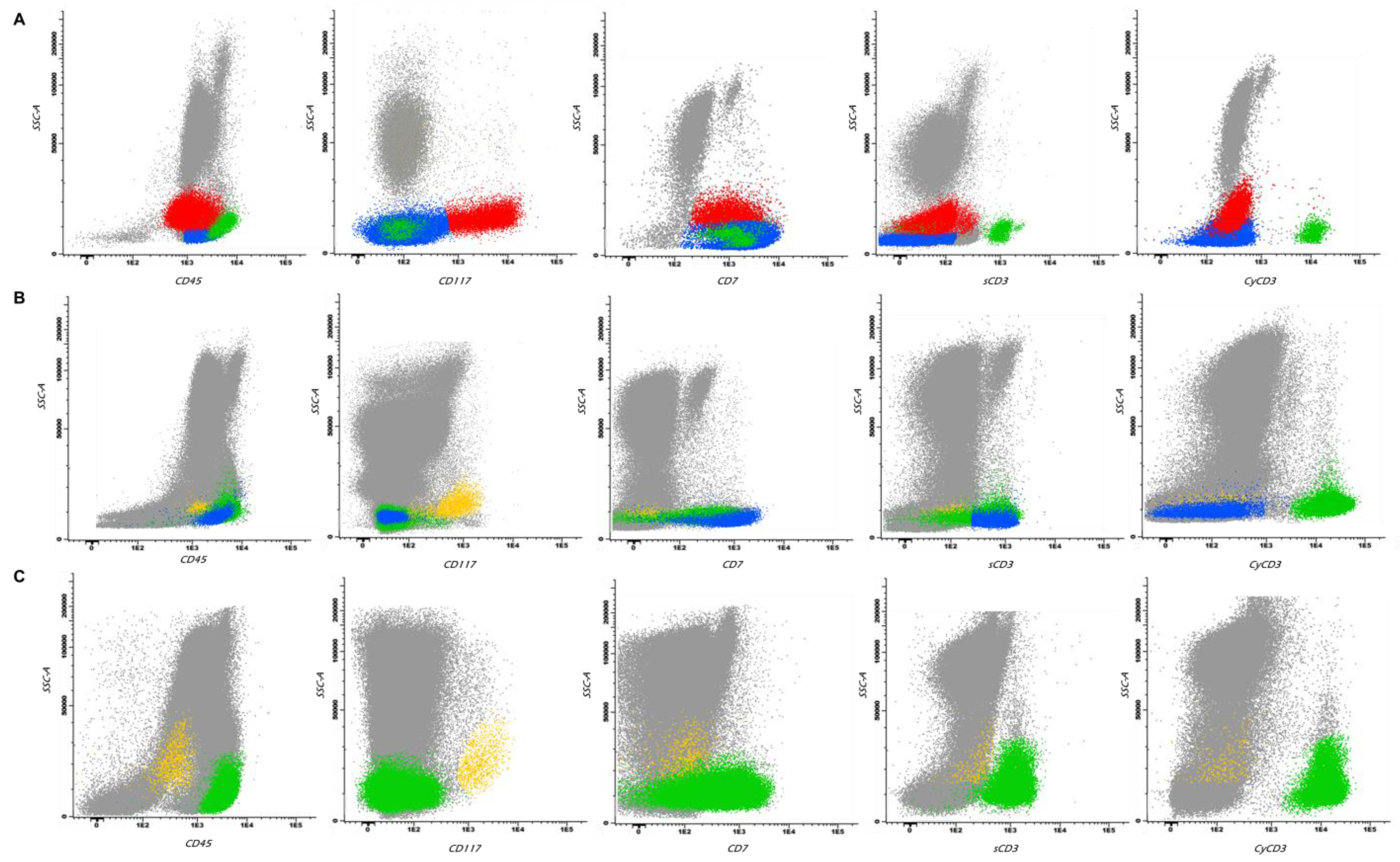
Flow cytometry analysis was performed also in BM samples, to confirm the diagnosis and to better characterized phenotypically blast cells [Figure 3A].
Because of the leukocytosis at onset, the patient was cytoreduced with prednisone and hydroxyurea; in order to avoid tumor lysis syndrome, he also started a prophylactic treatment with intravenous hydration and uricosuric agents. He was induced with a cyclophosphamide, idarubicin, vincristine, dexamethasone regimen and dasatinib.
From genetic analysis performed in the BM sample after the induction treatment, the presence of a 63.0% transcript BCR/ABL1 was detected and flow cytometry analysis showed the presence of residual T-lymphoid phenotype blasts, while myeloid progenitors did not show aberrations [Figure 3B]. Considering these results, Tyrosine Kinase Inhibitor (TKI) therapy was switched to ponatinib.
Figure 3.
Representative flow cytometry dot plot graphs showing: immature T-lymphoid phenotype blasts in blue, myeloid blasts with CD7 aberrant expression in red and mature T lymphocytes in green at diagnosis (A); residual immature T-lymphoid cells in blue, myeloid progenitors with no aberrations in orange and mature T lymphocytes after induction (B); myeloid progenitors with no aberrations and mature T lymphocytes at follow up after transplantation with negative measurable disease (C).
Figure 3.
Representative flow cytometry dot plot graphs showing: immature T-lymphoid phenotype blasts in blue, myeloid blasts with CD7 aberrant expression in red and mature T lymphocytes in green at diagnosis (A); residual immature T-lymphoid cells in blue, myeloid progenitors with no aberrations in orange and mature T lymphocytes after induction (B); myeloid progenitors with no aberrations and mature T lymphocytes at follow up after transplantation with negative measurable disease (C).
In view of the suboptimal clearance of the BCR/ABL transcript, he underwent a second cycle of chemotherapy with methotrexate and high dose cytarabine. Routine prophylactic intrathecal treatment, with cytarabine, methotrexate and dexamethasone, was performed, demonstrating no meningeal CML localization. After two cycles of chemotherapy, BCR/ABL1 transcript significantly decreased in bone marrow (ratio BCR/ABL1 to ABL1 = 0.93%), confirmed by qRT-PCR.
Five months after diagnosis, due to the underlying disease risk, allogeneic hematopoietic stem cell transplantation (allo-HSCT) from a 10/10 fully matched unrelated donor (MUD) was performed. Maintenance treatment with ponatinib was introduced sixty days after the transplant procedure.
Follow-up bone marrow examinations, performed at different time-points, included morphological analysis, multiparametric flow cytometry (MFC), quantitative monitoring of BCR/ABL1 transcript and quantitative analysis of donor chimerism [Table 1].
Multiparametric flow cytometry level of measurable residual disease (MRD) was performed using two different strategies: a “different from normal” approach for the myeloid compartment study and a MRD T-ALL approaches to evaluate the immature T-lymphoid phenotype. T-lymphoblast were not detectable by flow cytometry (LOD 0.0006%, LOQ 0.001%) and no “different from normal” cells were found by flow cytometry in the myeloid patterns of maturations demonstrating an MFC-MRD negativity [Figure 3C]. Moreover, follow-up BM examinations demonstrated barely or no detectable BCR/ABL1 fusion transcript levels, consistent with a deep molecular response (above MR 4.0). Same results were obtained on peripheral blood (PB).
Fifteen months after transplantion, the patient is in good health, leads a normal life, has no signs of GvHD (Graft versus Host Disease) and all hematochemical and biochemical parameters returned within normal range.
Conclusion
This clinical case report refers to a young patient who presented to the Emergency Department with typical symptoms of acute leukemia, without clinical history. Patient’s pathology was later identified as lymphoid T blast crisis of CML.
The early identification of two blast cell lines from a peripheral blood smear guided clinicians and laboratorians to the characterization of two different blast cell population. Morphological examination, flow cytometry and cytogenetics allowed to the rapid characterization of lymphoid T blast crisis of CML. The early diagnosis and the different characterization in bone marrow samples allowed to a quick change of therapy and helped to perform an early transplant, contributing to its success.
This case confirmed the relevance of the multidisciplinary collaboration for the CML management. In fact, the patient had hematologic, cytogenetic, and molecular features present in both CML and acute lymphoblastic leukemia (ALL). All in-depth analyses described above were strongly indicative of a diagnosis of CML and were crucial in outlining a correct treatment plan for the patient. Additional cases may be useful to explore how to improve the diagnostic workflow for patients experiencing blast crisis in CML, facilitating a more precise characterization of the leukemic population and aiding in the selection of optimal therapeutic interventions to enhance patient outcomes.
Conflict of interest
The authors of this manuscript declare that no one has a conflict of interest to disclose.
Author contributions
Study design was performed by Alessandra Mongia, Francesca Romano and Sara Ciullini Mannurita. Clinical data were collected by Laura Fasano. Alessandra Mongia, Francesca Romano, Sara Ciullini Mannurita Sara Bencini, Benedetta Peruzzi and Daniela Parrini carried out data analysis and completed the imagine visualization. The draft of the manuscript was written by Alessandra Mongia, Francesca Romano and Benedetta Peruzzi. Alessandra Fanelli supervised the manuscript. All the authors read and approved the final manuscript.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. The study protocol was in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments, using residual whole-blood clinical samples.
Patient consent agreement
Informed consent has been obtained from the patient.
Data availability
The authors declare that data supporting the findings of this study are available within the article.
References
- Faderl, S.; Talpaz, M.; Estrov, Z.; et al. The biology of chronic myeloid leukemia. N Engl J Med 1999, 341, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Huang, X.; Yan, Q.; Lin, Y.; Liu, E.; Mi, Y.; Liang, S.; Wang, H.; Xu, J.; Ru, K. The Diagnosis of Chronic Myeloid Leukemia with Deep Adversarial Learning. Am J Pathol 2022, 192, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Perrotti, D.; Jamieson, C.; Goldman, J.; Skorski, T. Chronic myeloid leukemia: Mechanisms of blastic transformation. J Clin Invest 2010, 120, 2254–2264. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, H.; Iwanaga, M.; Miyazaki, Y. Late effect of atomic bomb radiation on myeloid disorders: leukemia and myelodysplastic syndromes. Int J Hematol 2012, 95, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, M.M.; Santos, M.L.C.; Marques, H.S.; Goncalves, V.L.S.; Araujo, G.R.L.; Lopes, L.W.; Apolonio, J.S.; et al. Chronic myeloid leukemia-from the Philadelphia chromosome to specific target drugs: A literature review. World J Clin Oncol 2021, 12, 69–94. [Google Scholar] [CrossRef] [PubMed]
- Granatowicz, A.; Piatek, C.I.; Moschiano, E.; El-Hemaidi, I.; Armitage, J.D.; Akhtari, M. An overview and update of chronic myeloid leukemia for primary care physicians. Korean J Fam Med 2015, 36, 197–202. [Google Scholar] [CrossRef] [PubMed]
- DeFilipp, Z.; Khoury, H.J. Management of advanced-phase chronic myeloid leukemia. Curr Hematol Malig Rep 2015, 10, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; Gundem, G.; Van Loo, P.; Martincorena, I.; Ganly, P.; Mudie, L.; McLaren, S.; O’Meara, S.; Raine, K.; Jones, D.R.; Teague, J.W.; Butler, A.P.; Greaves, M.F.; Ganser, A.; Döhner, K.; Schlenk, R.F.; Döhner, H.; Campbell, P.J. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N Engl J Med 2016, 374, 2209–2221. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Chimerism and minimal residual disease monitoring on bone marrow aspirate samples after allogeneic stem cell transplantation.
Table 1.
Chimerism and minimal residual disease monitoring on bone marrow aspirate samples after allogeneic stem cell transplantation.
| Months after transplant | Complete morphological remission (CMR) | Multiparametric flow cytometry – Measurable residual disease (MFC-MRD) | BCR/ABL MR | Chimerism |
| 1 | Yes | Negative | MR4 (0.0037%) | 99.7% |
| 2 | Yes | Negative | MR4.5 (0.0015%) | 99.8% |
| 3 | Yes | Negative | MR4.5 (0.0016%) | 99.9% |
| 6 | Yes | Negative | MR5 | 99.7% |
| 12 | Yes | Negative | Undetected | 99.9% |
| 15 | Yes | Negative | Undetected | 99.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



