
Submitted:
27 March 2024
Posted:
28 March 2024
You are already at the latest version
Abstract
Lung cancer is one of the leading causes of cancer-related mortality globally. Pulmonary nodules are one of the risk factors and their discovery rate has been increasing. Based on the nodule size and growth rate, their malignancy propensity is determined; however, it is very challenging to distinguish between benign and cancerous nodules. Many tumour-associated antigens (TAA) have been studied as blood biomarkers for lung cancer, most commonly the Cytokeratin 19 fragment (CYFRA 21-1), squamous cell carcinoma antigen (SCC Ag), carbohydrate antigen (CA19-9) and carcinoembryonic antigen (CEA). Due to their low sensitivity, TAAs are not recommended as tools for the early detection of lung cancer. However, cancer testis antigens (CTAs) are highly specific for carcinomas but their expression is more commonly associated with advanced stages of cancer and poor prognosis. Despite the fact that TAAs may provide useful insights for the diagnosis and prognosis of early lung cancer, their potential to do so has yet to be demonstrated.
Keywords:
lung cancer
; nodules
; CT scan
; tumour associated antigens (TAAs)
; early diagnosis
; sensitivity
; specificity
; cancer testis antigens (CTA)
1. Introduction
Patients with lung cancer (LC) have poor survival rates predominantly due to late detection (Figure 1) by which time the disease has often spread to other organs of the body and treatment success is limited [1]. About three-quarters of patients present with advanced LC stages which eventually result in high mortality rates within three months of diagnosis [2]. Records have also shown that around 35% of LC patients are diagnosed immediately after emergency admission, while more than 90% of patients with LC are diagnosed at stage III or IV. In comparison, a high 5–year survival rate is seen amongst patients diagnosed in the early stages of LC (stages I and II) and can be as high as 75% following surgical resection [3]. Early diagnosis of LC has the potential to significantly improve survival rates even with the use of existing treatment options. LC is divided into small cell lung carcinomas (SCLC) and non-small cell lung carcinomas (NSCLC) based on histopathology. 80–85% of LC cases are NSCLC while SCLC constitutes 10-15% of lung cancer cases which grows quickly [4], responds well to chemotherapy but often returns.
2. Incidental Lung Nodules
Pulmonary nodules are small growths of cells inside the lung tissue and are classified as benign or malignant. Tammemagi et al. [5] reported incidental lung nodules at a rate of 25–51% among healthy volunteers and in patients undergoing LC screening. Most nodules (around 95%) have a low malignancy potential and it is difficult to identify which nodules are cancerous in the early stages of their detection. Even when using a differential diagnosis based on slight morphological changes, locations and clinical biomarkers, it is still very challenging to determine the propensity of malignancy in those nodules. Early malignant lung nodules are diagnosed through different procedures ranging from clinical settings, computerised tomography (CT) scan analysis (morphological assessment), positron emission tomography (PET) with fludeoxyglucose F18 (FDG) which is a positron-emitting radioisotope used to help diagnose various conditions, often through metabolic assessment), and needle biopsy analysis. However, biopsies are invasive procedures and can increase a patient’s anxiety as well as risking damage to this sensitive and fragile organ [6].
The diagnosis of lung nodules is extremely important for early LC detection. Estimation of the probability of malignancy is crucial for follow-up and further evaluation [7]. The first step is the assessment of clinical parameters as well as a consideration of the risk factors. Then, the radiological features including nodule size and growth rate are the main features for estimating the probability that nodules are malignant or have a high propensity for development into LC [8]. Common features of benign nodules include calcification (dense and uniform), fat content and location - 70% of LC arise from upper lobe of the lung nodules at peripheral lobes are mainly adenocarcinoma (ADC) and squamous cell carcinoma (SCC) arise from a central lesion. In contrast, common predictors of malignant nodules, observed in 33-100% of all nodules include spiculated or lobulated margins. However, more than 50% malignant nodules have smooth margins although the presence or absence of spiculation can assist in nodule characterization [9]. Well known features such as pleural retraction, spiculation, pleural thickening, or a vessel leading directly to a lesion, or partly solid components are all associated with an increased malignancy risk in pulmonary nodules [10]. However, the presence of one of these features represents high sensitivity for the risk of malignancy (91%) but with only 57% specificity as it may also be present in some inflammatory lesions.
3. Molecular Pathology of NSCLC
NSCLC develops due to a variety of distinct somatic mutations occurring in a heterogeneous population of tumour progenitor cells. NSCLC is further sub-classified into: 35% ADC, 30% SCC, 10% large cell carcinoma (LCC), Bronchoalveolar carcinoma (<5%), <5% adenosquamous, and 1% carcinoid [11]. NSCLCs are associated with a high frequency of mutations in p53 (50%), Kristen Rat Sarcoma Viral oncogene homolog (KRAS; 20%), epidermal growth factor receptor (EGFR; 15%-20%) [12], mesenchymal epithelial transition growth factor (MET; 7%) and human epidermal growth factor receptor 2 (HER2; 4-5%) [13,14]. Differences in the frequency of common mutations in ADC and SCC have been reported. ADC arises from epithelial cells in the terminal respiratory airways and frequently expresses thyroid transcription factor 1 (TTF1) and cytokeratin [15], while SCC develops in the central airways has a propensity to form a large solid carcinoma that is associated with phosphatase and tensin homolog (PTEN) and phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA )mutations. Interestingly, non-smokers with ADCs have a higher frequency of EGFR, anaplastic lymphoma kinase (ALK) and reactive oxygen species (ROS) mutations [16] while smokers show high frequency of mutations in KRAS, this suggests that there are different pathogenetic pathways of tumour development between patients with LC who are non-smokers or smokers [17]. The mutation frequency is also affected by ethnic/geographic factors, for example, 60% of patients from Asian background have EGFR and ALK driver mutations while only 10-15% of white Europeans show this pattern of abnormalities [15,18].
4. Tumour Antigens as Biomarkers for Cancer
At the moment, the diagnosis of LC is widely based on imaging techniques and biopsy/histopathology. The cost of LC diagnosis is high and 40% of the cost is associated with benign lesions [19] due to the difficulty in differentiating benign from malignant lesions. Thus high expertise is required for both imaging and histopathology. Non-invasive diagnostic methods such as biomarkers may aid LC diagnosis [19]. The most commonly investigated serological markers (Table 1) in LC include CA125, carcinoembryonic antigen (CEA) and cytokeratin 19 fragments (CYFRA21-1) [20,21,22].
These markers are highly expressed in LC, they also have elevated expression in other benign lung diseases and therefore have low specificity [23,24]. Tumour markers are not recommended as a tool for the early detection of LC. As TAAs are elevated in benign lung diseases, the standard cut-off of biomarkers is doubled [25] to maximize the diagnostic yield of LC when differentiating from non-cancerous diseases.
Such cut-off levels have no benefit in imaging studies when using methods such as CT scans in patients suspected of LC. The positive predictive value (PPV) of the CT scan has a greater value compared to PPV of biomarkers at standard cut-off levels. PPV of biomarkers depends on the prevalence rates of lung carcinoma. High score of the PPV of tumour marker has been observed in patient populations with high prevalence rates [32]. Biomarkers could be useful tools to evaluate effective treatment, to monitor for disease
recurrence after therapy and enable prognostic prediction.
4.1. Cytokeratin 19 Fragment (CYFRA 21-1)
Cytokeratin (CK) 19 is normally expressed in epithelial tissues and forms the epithelial cells’ filament cytoskeleton which increases during in the inflammation. It is rapidly degraded by the increased protease activity of caspase-3, and as a result its C-terminus
(CYFRA 21-1) is released into the circulation of patients with malignant tissues [33]. CYFRA21-1 is expressed in all lung ADC and is considered to be a highly sensitive marker for NSCLC. However, it is also observed in low amounts in some benign diseases such as pre-eclampsia due to endothelial damage/dysfunction. Limiting the value of CYFRA21-1 as a single marker in diagnosis of NSCLC [34].
4.2. Carcinoembryonic Antigen (CEA)
CEA is normally produced in gastrointestinal tissue during foetal development which terminates before birth [35]. It is rarely detected in the blood of healthy people except smokers. It is, however, highly expressed in many cancer types including gastric carcinoma and LC [35,36] and is used as a diagnostic marker for colon cancer [37]. LC patients have levels of serum CEA >3 ng/ml, however this level is slightly higher in smokers compared to non-smokers. High levels of CEA correlate with poor survival rates (Table 2) and serum CEA level could be a useful survival marker at the early stages of disease for patients with NSCLC [38].
According to Seemann et al., [39] CEA is commonly used as a biomarker for distinguishing malignant lesions from benign ones. It has a sensitivity ranging from 40-70% in NSCLC and 30-65% in small cell LC. High concentrations of CEA have been reported in ADCs and large cell LC while SCC have the lowest sensitivity and serum concentrations of CEA [35,40].
The significance of the preoperative levels of serum CEA in females with LC remains unclear and it’s still unclear whether CEA expression has a prognostic value in males with SCC. This is perhaps because SCC is associated with a history of smoking more than ADC. However, there is evidence that high expression of CEA after surgical intervention which is also strongly associated with poor prognosis. Persistently high levels of CEA after a complete resection for stage I NSCLC (confirmed pathologically) indicated poor prognosis for patients with elevated CEA levels compared to those with normal preoperative serum CEA level. This worse prognosis may be associated with the tumour burden or failure to eradicate all lung carcinoma even after surgical resection. High level of preoperative CEA > 50 ng/ml is associated with high frequency of metastasis even following surgical resection. The high preoperative CEA in non-smoking patients and poorer survival are required to be considered in association to smoking status [41]. CEA expression could also be useful for monitoring the response to chemotherapy following surgery [41,42]. As CEA is identified in many carcinomas such as gastric cancer, colon cancer and breast cancer, it has been of limited value for use in the diagnosis of LC due to its poor specificity. Efforts had been made to focus on CEA and other markers to detect LC [43].
4.3. CA19-9
CA19-9 is also known as a sialyl Lewis antigen [44] and was firstly identified in colon cancer [45]. High serum concentrations indicate its production and release from cancer cells into the blood. High levels of CA19-9 have been reported in 44.2% of all NSCLC patients especially the ADC subtype (56.5%). Moreover, its expression was associated with disease stage in positive CA19-9 ADCs with expression rates of 30, 67, and 80% in stages I, II, and III, respectively. High concentrations of CA19-9 are correlated with poor prognosis in preoperative patients. Serum CA19-9 level was linked to tumour CA19-9 concentration using the immunohistochemical technique; but Kawai et al [46] failed to demonstrate a correlation between postoperative survival and serum CA19-9 levels. CA19-9 combined with Tissue polypeptide antigen (TPA) was found to have a higher level of sensitivity (49%) for patients with resectable NSCLC compared to the sensitivity of TPA alone (44%) without significant differences in specificity [47]. Tsumatori et al. [48] studied serum E-selectin and correlated its elevated levels to survival of NSCLC patients suggesting a role for CA19-9 in enhancing metastasis. False positive results for CA19-9 predict LC suggests presence of a concurrent interstitial pneumonia.
4.4. CA125
CA125 is normally found on the ocular epithelial surface, and epithelial lining in the lung and respiratory tract as well as female genital tract epithelium [49]. It plays a role as a non-adhesive protective barrier in these organs and binds to mesothelin and galectin-1. High expression of CA125 was detected in ovarian cancer and it has become a biomarker for disease diagnosis [50]. Upregulation of CA125 was found in 20% of early stage and more than 50% advanced stage NSCLC [51]. Several studies have reported that CA125 could therefore be a useful biomarker for the detection of LC in patients [52,53] and thus have a prognostic value [52]. However, several studies have shown conflicting findings with regards to the predictive value of CA125 in surgical patients with NSCLC in part because CA125 levels are affected by normal ovarian activity and female hormonal status. High CA125 serum levels have been found in pregnancy and endometriosis [51].
4.5. SCC Antigen
SCC antigen (SCCA), also known as TA-4, is a structural cytoplasmic protein that is found in higher levels in patients especially with SCC compared to other NSCLCs. Over-expression of SCCA in blood indicates potential metastasis of the disease. It has a sensitivity that ranges from 15-55% for NSCLC [54]. SCCA is a prognostic indicator that when combined with NSE and CA125, showed that patients with high SCCA had significantly shorter OS than SCC patients. However, poor prognosis is generally correlated with high levels of CA125 and NSE rather than high SCCA. Recently, a comparison study of six markers (CA125, CA19.9, NSE, CEA, CYFRA21-1 and SCCA) showed that CYFRA21-1 serum levels were an independent prognostic factor for the 5-year survival of patients while other markers including SCCA had no notable correlation. Furthermore, high concentrations of SCCA and CYFRA21-1 have been reported in 30% and 59% of NSCLC patients, respectively [53]. SCCA had a low sensitivity of 13% in metastatic patients while the sensitivity of CYFRA21-1 was up to 74%. Due to poor sensitivity, SCCA serum levels are generally an inadequate tool for diagnosis but may be useful in monitoring recurrence for patients with NSCLC [54].
4.6. Neuron Specific Enolase (NSE)
NSE is a glycolytic enzyme with three isozymes of enolase transcribed from different genes. The isozymes are neuron specific and include enolase α which is ubiquitous; enolase β which is muscle-specific and enolase γ. Expression of NSE occurs at the late stage of neural differentiation in the form of dimers such as γγ- and αγ- which are used as indicators for neural maturation. NSE is expressed at low levels in specific tissues such as neurons and peripheral neuroendocrine cells under normal circumstances. It is known as a specific marker for neurons and its high expression is observed in the proliferation of malignant cells. Thus, it could be a useful tool to aid in diagnosis, and staging of related neuroendocrine tumours. In addition, it may serve as a target for treatment [55]. NSE is mainly a tumour marker for SCLC in diagnosis, follow-up and prognosis. However, some reports have identified NSE expression in NSCLC. Its expression is associated with tumour burden, number of metastatic sites and treatment response [56] although it’s high expression has also been reported in a range of cancers including melanoma, renal cell carcinoma, malignant phaeochromocytoma, carcinoid tumours, and immature teratomas [57]. NSE could also improve the diagnosis and evaluation of the outcome for a number of non-cancerous diseases such as seizures, intracerebral haemorrhage, ischaemic stroke and cardiac arrest after cardiopulmonary resuscitation in comatose patients and brain injuries through quantitative evaluation of brain damage [58]. This suggests that specificity will be an issue.
4.7. Serum Amyloid A (SAA)
SAA is a cytokine-induced protein and a precursor in inflammation-associated reactive amyloidosis (AA-type). It is expressed in acute inflammatory phase reactions but its physiological function is not fully understood. SAA proteins have been found to play a housekeeping roles in healthy tissues [59] as well as inflammation and Alzheimer’s Disease. Blood SAA protein has been identified in the early stages of many cancers such as uterine, ovarian, renal, nasopharyngeal, LC and melanoma. Previous studies have shown the relationship between the expression of SAA and LC, and shown its value as a diagnostic marker for LC [31,60].
4.8. Osteopontin (OPN)
Osteopontin (OPN) plays a role in regulating biological processes such as proteolysis, adhesion, migration, invasion, enhanced cell survival, and angiogenesis. It is also the main component of non-collagenous bone matrix protein and is found in haematological cell types, mesenchymal, epithelial and endothelial cells [61]. OPN expression is found in normal and pathological processes in the vascular and immune systems, inflammation, angiogenesis and remodeling of tissues. Interestingly, OPN is highly expressed in many cancer types such as LC and its expression is associated with poor patient outcomes [25]. Subgroup analysis of stage I-II patients alone revealed that OPN expression was significantly linked to both relapse-free and overall survival particularly in ADC patients [62].
4.9. Human Epididymis 4 (HE4)
High expression of HE4 was found in LC with AUC 0.85 especially for early stage disease [63]. This observation was due to overexpression of the HE4 gene, WFDC2, in LC. Lung ADC cell lines show moderate to high expression of different variants of HE4 (V1-4) with predominant expression of the HE4-V3 variant [64]. In clinical studies, one third of patients with LC had high levels of HE4 suggesting its role in malignancy and prognosis, but only limited data is available [65]. Moreover, Nagy et al. showed that a combination of HE4 with CEA and CA125 could be helpful diagnostic markers with 91.8% sensitivity and 92.8% specificity in patients especially in males with LC [65]. In addition to expression in ovarian and LCs, HE4 has been found in other carcinomas such as mesotheliomas, breast ADCs, and less frequently in renal, gastrointestinal, and transitional cell carcinomas [66,67]. High sera levels of HE4 have been reported in patients with LC compared to matched age and gender of healthy controls. The diagnostic efficiency was determined as 89.8% sensitivity and 100% specificity in 36 out 40 patients with LC [68]. High levels of HE4 after chemotherapy is associated with worse overall survival [68]. Therefore, HE4 could be both diagnostic and prognostic biomarker for LC.
4.10. Heat Shock Protein (HSP70)
Hsp70 belongs to a family of molecular chaperones that play a critical role in protein folding, protein transport across membranes, and inhibiting protein aggregation. Thus, HSP plays important functions in the regulation of protein homeostasis and cell survival [69]. It is highly induced and upregulated in cellular stress conditions including biological (cell proliferation and differentiation), environmental (oxidative stress, high temperature, and exposure to heavy metals) and pathological conditions (inflammation and tumour growth) [70] and overexpression is associated with poor prognosis in many cancers such as brain, colon, breast, prostate, and LC [71,72].
Elevated expression of HSP70 can distinguish well-differentiated small hepatocellular carcinoma (HHC) from high-grade dysplastic nodules and HSP70 is therefore considered as a sensitive marker for HHC [73]. Recently, lower levels of circulating HSP70 levels in plasma has been detected in LC compared to healthy individuals using ELISA [74]. HSP70 has shown a higher diagnostic value (AUC: 82.2%, SN: 74.1%, SP: 80.0%) compared to CEA (AUC: 80.1%, SN: 76.8%, SP: 67.3%), and CA19-9 (AUC: 63.7%, SN: 64.2%, SP: 54.0%). Consequently, decreased expression of HSP70 combined to high levels of CEA and CA19-9 could be used as a diagnostic panel for early (stage I and II) LC [74].
5. Cancer Testis Antigen Expression in NSCLC
Cancer testis antigens (CTAs) are not expressed in healthy tissues except immunologically protected sites that lack MHC class I such as the placenta and testes [75]. However CTAs are often aberrantly expressed in cancers such as melanoma, ovarian and oesophageal cancer, and LC [76]. Their reactivated expression in cancer cells is thought to be due to epigenetic mechanisms such as DNA demethylation and histone acetylation. This aligns with the observation that changes in CpG methylation patterns, which are established during embryonic development, can be altered in cancer cells [77]. Specifically, hypomethylation of DNA in tumours have been associated with the activation of genes typically only expressed in the germline, known as "cancer-germline" genes.
About 50% of CTAs are encoded on the X chromosome (CTA-X) and are involved in proliferation of male germ cells and associated with inverted DNA repeats. The rest of CTAs are non-X CTAs that are found in the later stages of germ cell differentiation and encoded by loci dispersed throughout autosomes. Non-X CTAs are not associated with inverted DNA repeats [75]. The CTA-X genes are more frequently activated in cancer cells, and specific gene families are simultaneously de-repressed in a tumour-specific manner. Examples include NY-ESO-1 which is often activated alongside MAGEA1 and MAGE-3 in LC cells [78]. CTAs [78,79] are further subdivided into four groups based on their tissue expression: (i) testis-restricted transcripts such as BAGE; (ii) germline genes expressed in two or fewer non-gametogenic tissues such as MAGE; (iii) differentially expressed CTA expressed in three-six non-gametogenic tissues such as XAGE1; (iv) ubiquitously expressed cancer/germline genes such as OY-TES-1 and found in juxtacentromeric regions (chromosomes 9, 13, 18 and 21). Tumours expressing CTAs could be divided into three groups based on number of CTAs and frequency of their expression. Tumours with high CTA expression (>50% of the CT antigen expression is at >20% frequency) include melanoma and NSCLC. Breast and prostate cancers are examples of tumours with moderate CTA expression while leukaemia could be considered as a low CTA expressor. CTA expression in NSCLC (Figure 2) ranged from 90% of SCC, 62% of bronchiolo-alveolar cancer and 67% of ADC expressing at least one CTA. Expression of CTAs is associated with advanced tumour stages and poor outcome [78].
5.1. The Cancer-Associated Gene (CAGE)
CAGE is a CTA that was initially discovered in the blood of patients diagnosed with gastric cancers [80]. It was found in 53.8% of patients with microsatellite instability-positive endometrial cancer [81] and is expressed in more than 50% of ADC. Its expression increases with the acquisition of EGFR mutations [82].
5.2. NANOS3
NANOS3 is a CTA that is predominantly expressed in adult testicular germ cells and brain tissue but not in most healthy adult somatic tissues [83]. The Nanos proteins (NANOS1, 2, and 3) have been found to play important roles in germline development [84] while NANOS2 and NANOS3 are involved in regulating meiosis. NANOS3 is upregulated in NSCLC and associated with poor survival [77]. In Drosophila, overexpression of germline genes like nos can lead to the growth of malignant brain tumours [85]. Furthermore, the upregulation of NANOS1 and NANOS3 have been linked to the oncogenic growth of pRb-deficient cells, indicating a potential role for Nanos in promoting cancer cell proliferation [86]. NANOS1 is suppressed by E-cadherin and plays a role in promoting invasive properties in lung tumour cells by regulating MMP-14 expression [87].
5.3. Melanoma-Associated Antigen Gene (MAGE)
MAGE proteins are found in the testes, placenta and many cancer types such as melanoma, breast, prostate, brain, and LCs [88,89]. The MAGE proteins play an important role in cancer biology and have been shown to increasingly play a role as cancer biomarkers. This includes the MAGE-A, -B, and -C proteins. Expression of the MAGE proteins are associated with advanced disease and poor prognosis, as well as chemotherapy resistance [75]. MAGE proteins levels increase with cancer cell survival either directly through interactions with the tumour suppressor p53 or indirectly through regulation of E3 RING ubiquitin ligases activity [75,90]. It has also been shown that MAGEs increase cancer metastasis by enhancing cell motility and thus increase invasive capacity into other tissue [75]. MAGE-A1 is prevalent of 30% of NSCLCs using reverse-transcription polymerase chain reaction, whereas it is detected in 43% of NSCLCs by immunohistochemistry (IHC) [91].
MAGE A3 is a recombinant protein [92], which is being used as the adjuvant NSCLC immunotherapy in a phase III MAGRIT trial. CAR-T cells that targeted HLA-A0201 restricted MAGE A3/A12 peptide were used in nine patients but showed that the use of immunotherapy did not improve the disease-free survival. Indeed the trial resulted in severe neurotoxicity and subsequently two patients died. It was found that MAGE A12 is expressed in the brain, explaining the neurotoxicity [93], and leading to the use of MAGE A12 to be cautioned against as an adjuvant therapy.
5.4. XAGE-1 Gene
The XAGE-1 gene has CT-like features and is known as a PAGE/GAGE-related gene on the X chromosome. Four alternative splice variants, XAGE-1a, b, c and d have been identified. XAGE-1b was dominantly expressed in lung ADC [94] with 45% (14/31) lung ADC having XAGE-1b mRNA expression while only 6% (1/18) of other histological types of LC were found to express XAGE-1b transcripts. XAGE-1b protein expression was found in most of the NSCLC tissues examined using immunohistochemistry [95] which is reflected by the fact that 43 of 83 (51.8%) LC patients have been shown to have an immune response targeting the XAGE-1b protein. In addition XAGE-1b expression has been observed in hepatocellular and gastric carcinomas [96].
Patients with ADC whose tumours express both MHC class I and XAGE-1b have prolonged survival post-operatively. However, patients with tumours expressing XAGE-1b may have shorter survival when HLA class I expression is downregulated. MHC class I and XAGE-1b co-expression may eradicate minimal residual disease via eliciting efficient CD8+ T-cell responses following surgery [97]. Consequently, XAGE-1b could represent a promising target for immunotherapy against NSCLC in an adjuvant setting.
6. The State-of-the-Art
We recently used the Preferred Reporting Items for Systematic Review (PRISMA) guidelines [98,99] to perform a systematic review of the literature [100] to address the research question – what are the most promising biomarkers for an early diagnosis of LC? The protocol was registered with PROSPERO (CRD42022336488) and we screened seven literature databases (CINAHL, MEDLINE, PubMed, Scopus, Web of Science, Cochrane library and Clinicaltrial.gov) from 1 January 1970 until 21st May 2023 using the following MeSH terms (cancer* or tumor* or tumour* or neoplasm* or carcinoma* or malignancy*) AND (lung* or pulmonary) AND (antigen* OR protein* OR RNA* OR ctDNA* OR miRNA* OR cell surface marker* OR inflammatory cell*) AND (early detection OR early diagnosis OR early biomarker OR early marker). The initial search, removal of duplicates, title and abstract screening, and full-text reviews were performed by two reviewers independently.
We identified 98 articles that focused on the identification and assessment of diagnostic biomarkers and achieved a pooled area under curve of 0.85 (95% CI 0.82-0.088), indicating that the diagnostic performance of these biomarkers when combined was excellent. However, the heterogeneity was also considerable (I2 = 98%, p < 0.00001). Of the studies, 30 focused on single/antigen panels, 22 on autoantibodies, 31 on miRNA and RNA panels, and 15 suggested the use of circulating DNA combined with CEA or NSE for early LC detection. Verification of blood biomarkers with high sensitivities (Ciz1, exoGCC2, ITGA2B), high specificities (CYFRA21-1, antiHE4, OPNV), or both (HSP90α, CEA) along with miR-15b and miR-27b/miR-21 from sputum were deemed a promising biomarker panel that could improve early LC detection.
Although CEA and CYFRA21-1 were antigens identified with high specificities for LC [32] both showed low sensitivity for the early detection of LC as single biomarkers. The systematic review benefitted from being able to consider all biomarkers studied and published on to date. This provided an opportunity to identify those blood biomarkers with high sensitivity (>90%), high specificity (>90%) or both, and to consider how the incorporation of sputum miRNAs into a diagnostic panel could maximise sensitivity and specificity for the detection of LC in the early stages. But it was notable that none of these antigens were CTAs reflecting the fact that CTAs tend to be overexpressed in advanced stages of cancer [78] rather than the early stages.
7. Discussion
The National Lung Screening Trial showed that there was a 20% reduction in mortality associated with using low-dose CT screening of people with known risk factors for LC. CT scans show a good efficiency in detecting small peripheral lesions particularly ADC [101]. In most of the cases, both benign and malignant nodules have a high degree of similarity in the early stages, and scanning errors as well as the enormous false positive rate for CT scanning techniques are ongoing confounders [102]. This leads to the requirement for additional procedures consisting of bronchoscopy, fine needle aspiration, transthoracic needle aspiration and surgical biopsy for further assessment. As an alternative to CT scanning, FDG-PET and contrast CT were used to assess malignancy risk [103]. While CT scans fail to detect lesions that are centrally located; bronchoscopy and sputum cytology can identify 25% of lung malignancies that cannot be detected by imaging techniques. Positive screening of widespread cancers including breast, colorectal, cervical, prostate, and skin can be quickly followed up with a tissue biopsy at minimal extra-risk to patients [104,105,106]. However, this is not the case in LC as there is the requirement for invasive procedures such as Mediastinoscopy with anesthetic, as lung is a fragile organ and this is associated with an increased risk of tissue damage including significant rates of pneumothorax [107]. Furthermore, cost-benefit analysis showed that more than 40% of the total cost of LC management is attributed to benign diseases being investigated by invasive approaches [19]. Due to these invasive procedures being associated with morbidity, increased costs and delays in diagnosis, the development of non-invasive approaches are needed. Experience of biomarkers for the evaluation symptoms in the fields of endocrine (HbA1C for diabetes) or infectious diseases (HIV viral load) are examples of the successful use of biomarkers in clinical practice [108].
Many studies have investigated the potential for a non-invasive diagnosis of LC in patients with indeterminate pulmonary nodules focusing predominantly on circulating biomarkers. Blood biomarkers has been repurposed to distinguish benign from malignant lung nodules [109]. For example, 552 patients have been studied (113 benign nodules and 339 malignant) for serum C-reactive protein (CRP) levels combined with CEA in the presence or absence of nodule spiculation, calcification, and CT bronchus signals. It has been found that CRP correlates with inflammation while CEA is one of glycoproteins that can assist in cellular adhesion and is thought to be upregulated in many epithelial cancers including LC due to metastasis [110]. Furthermore, phospholipid hydrolase enzyme is known as secretory phospholipase A2-IIa (sPA2-IIa) that facilitates several precursors to eicosanoids release, regulating several mechanisms including immunity, inflammation, and carcinogenesis. The sPA2-IIa was found to be highly expressed in prostate cancer but could also assist in differentiating LCs from healthy individuals. However, sPA2-IIa failed to discriminate between LCs and benign nodules with an AUC of 0.68 [111].
Blood tests have been developed to assign clinical significance to indeterminate nodules including an Early Cancer Detection test (EarlyCDT®) manufactured by Oncimmune and a multianalyte serum biomarker panel by Bigbee et al. [112,113,114]. The Oncimmune test includes a panel of autoantibodies against NY-ESO-1, p53, GBU4-5, annexin I and SOX2 that were examined and validated in early-stage LC patients. However, the sensitivity was low around 39% although specificity was 90% [113,114]. A panel of 10 markers were validated by Bigbee et al. [112] to predict the likelihood of cancer developing in high-risk individuals with indeterminate lung nodules. The markers panel included prolactin, transthyretin, sE-selectin, thrombospondin-1, C-C motif chemokine 5 (CCL5; RANTES), macrophage migration inhibitory factor (MIF), plasminogen activator inhibitor, tyrosine-protein kinase, erbb-2, CYRA 21-1 and SAA. The sensitivity of the combined markers in this panel were 73.3% although the specificity was 93.3% [112]. However this panel has not changed the treatment plan and patients still undergo invasive procedures suggesting that so far it has only had a modest clinical impact. On the other hand, this panel had good negative predictive value of 77.8% in the validation set and could aid in the screening of the population [112]. The PPV needs to be improved through the exploration of some additional biomarker targets. Large-scale validation will allow panels of biomarkers to become a highly efficient tool in clinical practice in large prospective clinical trials [115]. In addition to predicting the propensity of nodules to become malignant, LC is often referred to as a single disease; however, it is more likely a heterogeneous group of diseases rather than a single entity. It is obvious that patients with NSCLC respond differently to treatment and itself is a clinically and biologically heterogeneous group of LCs [116]. The role of intra-tumoural heterogeneity and genetic diversity within a single tumour remains unclear as well as their impact on the sensitivity of tumours to immune modulation [117,118,119].
Blood biomarkers represent an important resource for LC diagnosis due to their ease of access and low risk of secondary effects for patients [109]. From our systematic review it was evident that tumour antigens may assist LC evaluation, and that micro-RNA panels can provide suitable candidates for the early diagnosis of LC, and perhaps surprisingly, that their combination with tumour antigens may worthy of further investigation. Sputum and liquid biopsies are currently being evaluated for LC diagnosis. For example, the detection of folate receptor (FR)-positive circulating tumour cells could aid in the diagnosis of LC with 70% sensitivity and 79% specificity when combined with CEA [120].
Successful biomarker identification and characterisation is required to provide clinical evidence that informs treatment, as well as reducing the need for invasive procedures, diagnosis time and rates of false positive results [109]. Discovery studies should focus on study design, different controls, sample sizes that have the power to achieve statistical significance where it exists, and validated analytical tests for biomarker measurements. Training and validating cohorts are required to ensure robust biomarker performance in two independent centers [121].
8. Conclusions
Tumour antigens have been investigated as biomarkers for the early diagnosis of LC [100], but most have low sensitivity and specificity, and are more accurate at identifying advanced disease. Further research will need to engage advanced methodologies to identify protein signatures associated with the specific cancer type. Most tumour antigens are wild type proteins that are over expressed or mutated to enable them to stimulate the immune response in cancer. It is this altered expression that needs to be detectable to make tumour antigens good biomarkers and targets for therapy in disease. The gold standard procedures for cancer diagnosis still require invasive biopsy procedures and imaging techniques that require skilled expertise, and hi-tech equipment. Identifying biomarkers that may assist in the early diagnosis of LC, especially in the case of incidental lung nodules is essential. Identification of robust biomarkers which correlate with prognosis would not only assist in an accurate diagnosis but may also offer new targets for treatment.
Author Contributions
Conceptualization, funding acquisition, supervision, review and editing, project administration, S.H. and B.G.; data curation, writing—original draft preparation, E.M. All authors have read and agreed to the published version of the manuscript.
Funding
E.M. was funded by a University of Hull PhD studentship awarded to S.H. and B.G.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to it being a review.
Data Availability Statement
N/A
Acknowledgments
E.M. was funded by University of Hull PhD cluster studentship awarded to B.G. and S.H.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ADC | adenocarcinoma | NSCLC | non-small cell lung carcinoma |
| CAGE | cancer-associated gene | NSE | neuron specific enolase |
| CEA | carcinoembryonic antigen | OPN | Osteopontin |
| CT | computer tomography | PET | positron emission tomography |
| CTA | cancer testis antigen | SAA | serum amyloid A |
| CYFRA21-1 | cytokeratin 19 fragments | SCC | squamous cell carcinoma |
| HE4 | human epididymis 4 | SCCA | squamous cell carcinoma antigen |
| HSP70 | heat shock protein 70 | TA | tumour antigens |
| LC | lung cancer | TAA | tumour associated antigens |
| MAGE | melanoma-associated antigen gene |
References
- Verma, V.; Simone, C.B.; Werner-Wasik, M. Acute and late toxicities of concurrent chemoradiotherapy for locally-advanced non-small cell lung cancer. Cancers 2017, 9, 120. [CrossRef]
- O'Dowd, E.L.; McKeever, T.M.; Baldwin, D.R.; Anwar, S.; Powell, H.A.; Gibson, J.E.; Iyen-Omofoman, B.; Hubbard, R.B. What characteristics of primary care and patients are associated with early death in patients with lung cancer in the UK? Thorax 2015, 70, 161-168.
- Balata, H.; Evison, M.; Sharman, A.; Crosbie, P.; Booton, R. CT screening for lung cancer: Are we ready to implement in Europe? Lung Cancer 2019, 134, 25-33. [CrossRef]
- El-Khoury, V.; Béland, M.; Schritz, A.; Kim, S.-Y.; Nazarov, P.V.; Gaboury, L.; Sertamo, K.; Bernardin, F.; Batutu, R.; Antunes, L.; et al. Identification of beta-arrestin-1 as a diagnostic biomarker in lung cancer. British journal of cancer 2018, 119, 580-590. [CrossRef]
- Tammemagi, M.C.; Mayo, J.R.; Lam, S. Cancer in pulmonary nodules detected on first screening CT. The New England journal of medicine 2013, 369, 2060. [CrossRef]
- Gould, M.K.; Donington, J.; Lynch, W.R.; Mazzone, P.J.; Midthun, D.E.; Naidich, D.P.; Wiener, R.S. Evaluation of individuals with pulmonary nodules: When is it lung cancer?: Diagnosis and management of lung cancer: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e93S-e120S. [CrossRef]
- Snoeckx, A.; Reyntiens, P.; Desbuquoit, D.; Spinhoven, M.J.; Van Schil, P.E.; van Meerbeeck, J.P.; Parizel, P.M. Evaluation of the solitary pulmonary nodule: Size matters, but do not ignore the power of morphology. Insights into imaging 2018, 9, 73-86. [CrossRef]
- Callister, M.; Baldwin, D.; Akram, A.; Barnard, S.; Cane, P.; Draffan, J.; Franks, K.; Gleeson, F.; Graham, R.; Malhotra, P. British Thoracic Society guidelines for the investigation and management of pulmonary nodules: Accredited by NICE. Thorax 2015, 70, ii1-ii54. [CrossRef]
- Wahidi, M.M.; Govert, J.A.; Goudar, R.K.; Gould, M.K.; McCrory, D.C. Evidence for the treatment of patients with pulmonary nodules: When is it lung cancer?: ACCP evidence-based clinical practice guidelines. Chest 2007, 132, 94S-107S. [CrossRef]
- Seemann, M.D.; Seemann, O.; Luboldt, W.; Bonél, H.; Sittek, H.; Dienemann, H.; Staebler, A. Differentiation of malignant from benign solitary pulmonary lesions using chest radiography, spiral CT and HRCT. Lung cancer 2000, 29, 105-124. [CrossRef]
- Chikwe, J.; Cooke, D.; Weiss, A. Cardiothoracic surgery; OUP Oxford: 2013.
- Chen, Z.; Fillmore, C.M.; Hammerman, P.S.; Kim, C.F.; Wong, K.-K. Non-small-cell lung cancers: A heterogeneous set of diseases. Nature Reviews Cancer 2014, 14, 535-546. [CrossRef]
- Lynch, T.J.; Bell, D.W.; Sordella, R.; Gurubhagavatula, S.; Okimoto, R.A.; Brannigan, B.W.; Harris, P.L.; Haserlat, S.M.; Supko, J.G.; Haluska, F.G. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non–small-cell lung cancer to gefitinib. New England Journal of Medicine 2004, 350, 2129-2139. [CrossRef]
- Soma, S.; Tsuta, K.; Takano, T.; Hatanaka, Y.; Yoshida, A.; Suzuki, K.; Asamura, H.; Tsuda, H. Intratumoral distribution of EGFR-amplified and EGFR-mutated cells in pulmonary adenocarcinoma. Pathology-Research and Practice 2014, 210, 155-160. [CrossRef]
- Mitsudomi, T. Molecular epidemiology of lung cancer and geographic variations with special reference to EGFR mutations. Translational lung cancer research 2014, 3, 205. [CrossRef]
- Soda, M.; Choi, Y.L.; Enomoto, M.; Takada, S.; Yamashita, Y.; Ishikawa, S.; Fujiwara, S.-i.; Watanabe, H.; Kurashina, K.; Hatanaka, H. Identification of the transforming EML4–ALK fusion gene in non-small-cell lung cancer. Nature 2007, 448, 561-566. [CrossRef]
- Sanders, H.R.; Albitar, M. Somatic mutations of signaling genes in non-small-cell lung cancer. Cancer Genetics and Cytogenetics 2010, 203, 7-15. [CrossRef]
- Gridelli, C.; Rossi, A.; Carbone, D.P.; Guarize, J.; Karachaliou, N.; Mok, T.; Petrella, F.; Spaggiari, L.; Rosell, R. Non-small-cell lung cancer. Nature reviews Disease primers 2015, 1, 1-16.
- Lokhandwala, T.; Bittoni, M.A.; Dann, R.A.; D'Souza, A.O.; Johnson, M.; Nagy, R.J.; Lanman, R.B.; Merritt, R.E.; Carbone, D.P. Costs of diagnostic assessment for lung cancer: A medicare claims analysis. Clinical lung cancer 2017, 18, e27-e34. [CrossRef]
- Patz Jr, E.F.; Campa, M.J.; Gottlin, E.B.; Kusmartseva, I.; Guan, X.R.; Herndon, J.E. Panel of serum biomarkers for the diagnosis of lung cancer. Journal of Clinical Oncology 2007, 25, 5578-5583. [CrossRef]
- Schneider, J. Tumor markers in detection of lung cancer. Advances in clinical chemistry 2006, 42, 1-41. [CrossRef]
- Hanagiri, T.; Sugaya, M.; Takenaka, M.; Oka, S.; Baba, T.; Shigematsu, Y.; Nagata, Y.; Shimokawa, H.; Uramoto, H.; Takenoyama, M. Preoperative CYFRA 21-1 and CEA as prognostic factors in patients with stage I non-small cell lung cancer. Lung cancer 2011, 74, 112-117. [CrossRef]
- Kulpa, J.; Wojcik, E.; Reinfuss, M.; Kołodziejski, L. Carcinoembryonic antigen, squamous cell carcinoma antigen, CYFRA 21-1, and neuron-specific enolase in squamous cell lung cancer patients. Clinical chemistry 2002, 48, 1931-1937. [CrossRef]
- Schneider, J.; Philipp, M.; Velcovsky, H.-G.; Morr, H.; Katz, N. Pro-gastrin-releasing peptide (ProGRP), neuron specific enolase (NSE), carcinoembryonic antigen (CEA) and cytokeratin 19-fragments (CYFRA 21-1) in patients with lung cancer in comparison to other lung diseases. Anticancer research 2003, 23, 885.
- Ayan, A.K.; Erdemci, B.; Orsal, E.; Bayraktutan, Z.; Akpinar, E.; Topcu, A.; Turkeli, M.; Seven, B. Is there any correlation between levels of serum ostepontin, CEA, and FDG uptake in lung cancer patients with bone metastasis? Revista Española de Medicina Nuclear e Imagen Molecular (English Edition) 2016, 35, 102-106. [CrossRef]
- Hammarström, S. The carcinoembryonic antigen (CEA) family: Structures, suggested functions and expression in normal and malignant tissues. Seminars in Cancer Biology 1999, 9, 67-81. [CrossRef]
- Berge, G.; Pettersen, S.; Grotterød, I.; Bettum, I.J.; Boye, K.; Mælandsmo, G.M. Osteopontin—An important downstream effector of S100A4-mediated invasion and metastasis. International journal of cancer 2011, 129, 780-790. [CrossRef]
- Yu, Z.; Zhang, G.; Yang, M.; Zhang, S.; Zhao, B.; Shen, G.; Chai, Y. Systematic review of CYFRA 21-1 as a prognostic indicator and its predictive correlation with clinicopathological features in Non-small Cell Lung Cancer: A meta-analysis. Oncotarget 2017, 8, 4043. [CrossRef]
- Isgrò, M.A.; Bottoni, P.; Scatena, R. Neuron-specific enolase as a biomarker: Biochemical and clinical aspects. In Advances in Cancer Biomarkers; Springer: 2015; pp. 125-143. [CrossRef]
- Urieli-Shoval, S.; Linke, R.P.; Matzner, Y. Expression and function of serum amyloid A, a major acute-phase protein, in normal and disease states. Current opinion in hematology 2000, 7, 64-69. [CrossRef]
- Biaoxue, R.; Hua, L.; Wenlong, G.; Shuanying, Y. Increased serum amyloid A as potential diagnostic marker for lung cancer: A meta-analysis based on nine studies. BMC cancer 2016, 16, 836. [CrossRef]
- Okamura, K.; Takayama, K.; Izumi, M.; Harada, T.; Furuyama, K.; Nakanishi, Y. Diagnostic value of CEA and CYFRA 21-1 tumor markers in primary lung cancer. Lung Cancer 2013, 80, 45-49. [CrossRef]
- Kosacka, M.; Jankowska, R. Comparison of cytokeratin 19 expression in tumor tissue and serum CYFRA 21-1 levels in non-small cell lung cancer. Polskie Archiwum Medycyny Wewnetrznej 2009, 119, 33-37. [CrossRef]
- Wang, P.; Piao, Y.; Zhang, X.; Li, W.; Hao, X. The concentration of CYFRA 21-1, NSE and CEA in cerebro-spinal fluid can be useful indicators for diagnosis of meningeal carcinomatosis of lung cancer. Cancer Biomarkers 2013, 13, 123-130. [CrossRef]
- Grunnet, M.; Sorensen, J. Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung cancer 2012, 76, 138-143. [CrossRef]
- Thomas, S.N.; Zhu, F.; Schnaar, R.L.; Alves, C.S.; Konstantopoulos, K. Carcinoembryonic antigen and CD44 variant isoforms cooperate to mediate colon carcinoma cell adhesion to E-and L-selectin in shear flow. Journal of biological chemistry 2008, 283, 15647-15655. [CrossRef]
- Duffy, M.J. Carcinoembryonic antigen as a marker for colorectal cancer: Is it clinically useful? Clinical chemistry 2001, 47, 624-630.
- Sawabata, N.; Ohta, M.; Takeda, S.-i.; Hirano, H.; Okumura, Y.; Asada, H.; Maeda, H. Serum carcinoembryonic antigen level in surgically resected clinical stage I patients with non-small cell lung cancer. The Annals of thoracic surgery 2002, 74, 174-179. [CrossRef]
- Seemann, M.D.; Beinert, T.; Fürst, H.; Fink, U. An evaluation of the tumour markers, carcinoembryonic antigen (CEA), cytokeratin marker (CYFRA 21-1) and neuron-specific enolase (NSE) in the differentiation of malignant from benign solitary pulmonary lesions. Lung Cancer 1999, 26, 149-155. [CrossRef]
- Pioglitazone Hydrochloride in Treating Patients With Stage IA-IIIA Non-small Cell Lung Cancer.
- Hsu, W.-H.; Huang, C.-S.; Hsu, H.-S.; Huang, W.-J.; Lee, H.-C.; Huang, B.-S.; Huang, M.-H. Preoperative serum carcinoembryonic antigen level is a prognostic factor in women with early non-small-cell lung cancer. The Annals of thoracic surgery 2007, 83, 419-424. [CrossRef]
- Nonaka, M.; Kataoka, D.; Yamamoto, S.; Bito, A.; Matsuoka, J.; Kawada, T.; Takaba, T. Pre-and post-operative serum carcinoembryonic antigen in primary lung adenocarcinoma. Ann Thorac Cardiovasc Surg 2004, 10, 281-284.
- Doseeva, V.; Colpitts, T.; Gao, G.; Woodcock, J.; Knezevic, V. Performance of a multiplexed dual analyte immunoassay for the early detection of non-small cell lung cancer. J Transl Med 2015, 13, 55. [CrossRef]
- Schmiegel, W.; Kreiker, C.; Eberl, W.; Arndt, R.; Classen, M.; Greten, H.; Jessen, K.; Kalthoff, H.; Soehendra, N.; Thiele, H. Monoclonal antibody defines CA 19-9 in pancreatic juices and sera. Gut 1985, 26, 456-460. [CrossRef]
- Herlyn, M.; Sears, H.F.; Steplewski, Z.; Koprowski, H. Monoclonal antibody detection of a circulating tumor-associated antigen. I. Presence of antigen in sera of patients with colorectal, gastric, and pancreatic carcinoma. Journal of clinical immunology 1982, 2, 135-140. [CrossRef]
- Kawai, T.; Suzuki, M.; Kase, K.; Ozeki, Y. Expression of carbohydrate antigens in human pulmonary adenocarcinoma. Cancer 1993, 72, 1581-1587. [CrossRef]
- Toumbis, M.; Rasidakis, A.; Passalidou, E.; Dimitroulis, J.; Gaga, M.; Alchanatis, M.; Orphanidou, D.; Jordanoglou, J. Diagnostic usefulness of 5 tumor-markers in patients with primary lung-cancer. Oncology reports 1995, 2, 1135-1140. [CrossRef]
- Tsumatori, G.; Ozeki, Y.; Takagi, K.; Ogata, T.; Tanaka, S. Relation between the Serum E-Selectin Level and the Survival Rate of Patients with Resected Non-small Cell Lung Cancers. Japanese journal of cancer research 1999, 90, 301-307. [CrossRef]
- Pejovic, T.; Nezhat, F. Effect of screening on ovarian cancer mortality: The prostate, lung, colorectal and ovarian (PLCO) cancer screening randomized controlled trial. Journal of Minimally Invasive Gynecology 2011, 18, 823-825. [CrossRef]
- Bottoni, P.; Scatena, R. The role of CA 125 as tumor marker: Biochemical and clinical aspects. Advances in Cancer Biomarkers: From biochemistry to clinic for a critical revision 2015, 229-244.
- Clevers, M.R.; Kastelijn, E.A.; Peters, B.J.; Kelder, H.; Schramel, F.M. Evaluation of serum biomarker CEA and Ca-125 as immunotherapy response predictors in metastatic non-small cell lung cancer. Anticancer Research 2021, 41, 869-876. [CrossRef]
- Cedrés, S.; Nuñez, I.; Longo, M.; Martinez, P.; Checa, E.; Torrejón, D.; Felip, E. Serum tumor markers CEA, CYFRA21-1, and CA-125 are associated with worse prognosis in advanced non–small-cell lung cancer (NSCLC). Clinical lung cancer 2011, 12, 172-179. [CrossRef]
- Yu, D.; Du, K.; Liu, T.; Chen, G. Prognostic Value of Tumor Markers, NSE, CA125 and SCC, in Operable NSCLC Patients. International Journal of Molecular Sciences 2013, 14, 11145-11156. [CrossRef]
- Kagohashi, K.; Satoh, H.; Ishikawa, H.; Ohtsuka, M.; Sekizawa, K. A re-evaluation of squamous cell carcinoma antigen (SCC) as a serum marker for non-small cell lung cancer. Medical Oncology 2008, 25, 187-189. [CrossRef]
- Barlési, F.; Gimenez, C.; Torre, J.-P.; Doddoli, C.; Mancini, J.; Greillier, L.; Roux, F.; Kleisbauer, J.-P. Prognostic value of combination of Cyfra 21-1, CEA and NSE in patients with advanced non-small cell lung cancer. Respiratory medicine 2004, 98, 357-362. [CrossRef]
- Altintas, Z.; Tothill, I. Biomarkers and biosensors for the early diagnosis of lung cancer. Sensors and Actuators B-Chemical 2013, 188, 988-998. [CrossRef]
- Isgro, M.A.; Bottoni, P.; Scatena, R. Neuron-Specific Enolase as a Biomarker: Biochemical and Clinical Aspects. Adv Exp Med Biol 2015, 867, 125-143. [CrossRef]
- Dittadi, R.; Gion, M. Re: Biological variation of neuroendocrine tumor markers chromogranin A and neuron-specific enolase. Clinical Biochemistry 2013, 12, 1145. [CrossRef]
- Urieli-Shoval, S.; Linke, R.P.; Matzner, Y. Expression and function of serum amyloid A, a major acute-phase protein, in normal and disease states. Curr Opin Hematol 2000, 7, 64-69. [CrossRef]
- Moshkovskii, S. Why do cancer cells produce serum amyloid A acute-phase protein? Biochemistry (Moscow) 2012, 77, 339-341. [CrossRef]
- Berge, G.; Pettersen, S.; Grotterød, I.; Bettum, I.J.; Boye, K.; Mælandsmo, G.M. Osteopontin—An important downstream effector of S100A4-mediated invasion and metastasis. International Journal of Cancer 2011, 129, 780-790. [CrossRef]
- Rud, A.K.; Boye, K.; Øijordsbakken, M.; Lund-Iversen, M.; Halvorsen, A.R.; Solberg, S.K.; Berge, G.; Helland, Å.; Brustugun, O.T.; Mælandsmo, G.M. Osteopontin is a prognostic biomarker in non-small cell lung cancer. BMC cancer 2013, 13, 1-10. [CrossRef]
- Li, J.; Li, Y.; Huo, L.; Sun, R.; Liu, X.; Gu, Q.; Li, A.; Han, S.; Liu, H.; Li, Y.; et al. Detection of serum HE4 levels contributes to the diagnosis of lung cancer. Oncol Lett 2023, 25, 255. [CrossRef]
- Tokuishi, K.; Yamashita, S.-i.; Ohbo, K.; Kawahara, K. Splice variant HE4-V3 expression is associated with favorable prognosis in pulmonary adenocarcinoma. Tumor Biology 2012, 33, 103-109. [CrossRef]
- Nagy, B.; Bhattoa, H.P.; Steiber, Z.; Csobán, M.; Szilasi, M.; Méhes, G.; Müller, M.; Lázár, J.; Kappelmayer, J.; Antal-Szalmás, P. Serum human epididymis protein 4 (HE4) as a tumor marker in men with lung cancer. Clinical Chemistry and Laboratory Medicine (CCLM) 2014, 52, 1639-1648. [CrossRef]
- Bingle, L.; Singleton, V.; Bingle, C.D. The putative ovarian tumour marker gene HE4 (WFDC2), is expressed in normal tissues and undergoes complex alternative splicing to yield multiple protein isoforms. Oncogene 2002, 21, 2768-2773. [CrossRef]
- Drapkin, R.; Von Horsten, H.H.; Lin, Y.; Mok, S.C.; Crum, C.P.; Welch, W.R.; Hecht, J.L. Human epididymis protein 4 (HE4) is a secreted glycoprotein that is overexpressed by serous and endometrioid ovarian carcinomas. Cancer research 2005, 65, 2162-2169. [CrossRef]
- Iwahori, K.; Suzuki, H.; Kishi, Y.; Fujii, Y.; Uehara, R.; Okamoto, N.; Kobayashi, M.; Hirashima, T.; Kawase, I.; Naka, T. Serum HE4 as a diagnostic and prognostic marker for lung cancer. Tumour biology: The journal of the International Society for Oncodevelopmental Biology and Medicine 2012, 33, 1141-1149. [CrossRef]
- Mayer, M.; Bukau, B. Hsp70 chaperones: Cellular functions and molecular mechanism. Cellular and molecular life sciences 2005, 62, 670-684. [CrossRef]
- Morimoto, R.I. Regulation of the heat shock transcriptional response: Cross talk between a family of heat shock factors, molecular chaperones, and negative regulators. Genes & development 1998, 12, 3788-3796. [CrossRef]
- Chuma, M.; Saeki, N.; Yamamoto, Y.; Ohta, T.; Asaka, M.; Hirohashi, S.; Sakamoto, M. Expression profiling in hepatocellular carcinoma with intrahepatic metastasis: Identification of high-mobility group I (Y) protein as a molecular marker of hepatocellular carcinoma metastasis. The Keio journal of medicine 2004, 53, 90-97. [CrossRef]
- Garg, M.; Kanojia, D.; Saini, S.; Suri, S.; Gupta, A.; Surolia, A.; Suri, A. Germ cell-specific heat shock protein 70-2 is expressed in cervical carcinoma and is involved in the growth, migration, and invasion of cervical cells. Cancer 2010, 116, 3785-3796. [CrossRef]
- Wang, B.; Lan, T.; Xiao, H.; Chen, Z.-H.; Wei, C.; Chen, L.-F.; Guan, J.-F.; Yuan, R.-F.; Yu, X.; Hu, Z.-G. The expression profiles and prognostic values of HSP70s in hepatocellular carcinoma. Cancer Cell International 2021, 21, 1-17. [CrossRef]
- Tang, T.; Yang, C.; Brown, H.E.; Huang, J. Circulating Heat Shock Protein 70 Is a Novel Biomarker for Early Diagnosis of Lung Cancer. Dis Markers 2018, 2018, 6184162. [CrossRef]
- Gjerstorff, M.F.; Andersen, M.H.; Ditzel, H.J. Oncogenic cancer/testis antigens: Prime candidates for immunotherapy. Oncotarget 2015, 6, 15772. [CrossRef]
- Fratta, E.; Coral, S.; Covre, A.; Parisi, G.; Colizzi, F.; Danielli, R.; Nicolay, H.J.M.; Sigalotti, L.; Maio, M. The biology of cancer testis antigens: Putative function, regulation and therapeutic potential. Molecular oncology 2011, 5, 164-182. [CrossRef]
- O'Leary, K.; Shia, A.; Schmid, P. Epigenetic regulation of EMT in non-small cell lung cancer. Current cancer drug targets 2018, 18, 89-96. [CrossRef]
- Gure, A.O.; Chua, R.; Williamson, B.; Gonen, M.; Ferrera, C.A.; Gnjatic, S.; Ritter, G.; Simpson, A.J.; Chen, Y.-T.; Old, L.J. Cancer-testis genes are coordinately expressed and are markers of poor outcome in non–small cell lung cancer. Clinical Cancer Research 2005, 11, 8055-8062. [CrossRef]
- John, T.; Starmans, M.H.; Chen, Y.T.; Russell, P.A.; Barnett, S.A.; White, S.C.; Mitchell, P.L.; Walkiewicz, M.; Azad, A.; Lambin, P.; et al. The role of Cancer-Testis antigens as predictive and prognostic markers in non-small cell lung cancer. PLoS ONE 2013, 8, e67876. [CrossRef]
- Cho, B.; Lim, Y.; Lee, D.-Y.; Park, S.-Y.; Lee, H.; Kim, W.H.; Yang, H.; Bang, Y.-J.; Jeoung, D.-I. Identification and characterization of a novel cancer/testis antigen gene CAGE. Biochemical and biophysical research communications 2002, 292, 715-726. [CrossRef]
- Iwata, T.; Fujita, T.; Hirao, N.; Matsuzaki, Y.; Okada, T.; Mochimaru, H.; Susumu, N.; Matsumoto, E.; Sugano, K.; Yamashita, N. Frequent Immune Responses to a Cancer/Testis Antigen, CAGE, in Patients with Microsatellite instability–Positive Endometrial Cancer. Clinical cancer research 2005, 11, 3949-3957. 10.1158/1078-0432.CCR-04-1702.
- Yeon, M.; Lee, H.; Yeo, J.; Jeong, M.S.; Jung, H.S.; Lee, H.; Shim, K.; Jo, H.; Jeon, D.; Koh, J.; et al. Cancer/testis antigen CAGE mediates osimertinib resistance in non-small cell lung cancer cells and predicts poor prognosis in patients with pulmonary adenocarcinoma. Scientific Reports 2023, 13, 15748. [CrossRef]
- Grelet, S.; Andries, V.; Polette, M.; Gilles, C.; Staes, K.; Martin, A.P.; Kileztky, C.; Terryn, C.; Dalstein, V.; Cheng, C.W. The human NANOS3 gene contributes to lung tumour invasion by inducing epithelial–mesenchymal transition. The Journal of Pathology 2015, 237, 25-37. [CrossRef]
- Kusz, K.; Tomczyk, L.; Sajek, M.; Spik, A.; Latos-Bielenska, A.; Jedrzejczak, P.; Pawelczyk, L.; Jaruzelska, J. The highly conserved NANOS2 protein: Testis-specific expression and significance for the human male reproduction. Molecular human reproduction 2009, 15, 165-171. [CrossRef]
- Janic, A.; Mendizabal, L.; Llamazares, S.; Rossell, D.; Gonzalez, C. Ectopic expression of germline genes drives malignant brain tumor growth in Drosophila. Science 2010, 330, 1824-1827. [CrossRef]
- Miles, W.O.; Korenjak, M.; Griffiths, L.M.; Dyer, M.A.; Provero, P.; Dyson, N.J. Post-transcriptional gene expression control by NANOS is up-regulated and functionally important in pR b-deficient cells. The EMBO Journal 2014, 33, 2201-2215. [CrossRef]
- Bonnomet, A.; Polette, M.; Strumane, K.; Gilles, C.; Dalstein, V.; Kileztky, C.; Berx, G.; Van Roy, F.; Birembaut, P.; Nawrocki-Raby, B. The E-cadherin-repressed hNanos1 gene induces tumor cell invasion by upregulating MT1-MMP expression. Oncogene 2008, 27, 3692-3699. [CrossRef]
- Campagnolo, C.; Meyers, K.J.; Ryan, T.; Atkinson, R.C.; Chen, Y.-T.; Scanlan, M.J.; Ritter, G.; Old, L.J.; Batt, C.A. Real-Time, label-free monitoring of tumor antigen and serum antibody interactions. Journal of biochemical and biophysical methods 2004, 61, 283-298. [CrossRef]
- Krishnadas, D.K.; Bai, F.; Lucas, K.G. Cancer testis antigen and immunotherapy. ImmunoTargets and therapy 2013, 2, 11. [CrossRef]
- Doyle, J.M.; Gao, J.; Wang, J.; Yang, M.; Potts, P.R. MAGE-RING protein complexes comprise a family of E3 ubiquitin ligases. Molecular cell 2010, 39, 963-974. [CrossRef]
- Fanipakdel, A.; Seilanian Toussi, M.; Rezazadeh, F.; Mohamadian Roshan, N.; Javadinia, S.A. Overexpression of cancer-testis antigen melanoma-associated antigen A1 in lung cancer: A novel biomarker for prognosis, and a possible target for immunotherapy. Journal of Cellular Physiology 2019, 234, 12080-12086. [CrossRef]
- Tyagi, P.; Mirakhur, B. MAGRIT: The largest-ever phase III lung cancer trial aims to establish a novel tumor-specific approach to therapy. Clinical lung cancer 2009, 10, 371-374. [CrossRef]
- Morgan, R.A.; Chinnasamy, N.; Abate-Daga, D.D.; Gros, A.; Robbins, P.F.; Zheng, Z.; Feldman, S.A.; Yang, J.C.; Sherry, R.M.; Phan, G.Q. Cancer regression and neurologic toxicity following anti-MAGE-A3 TCR gene therapy. Journal of immunotherapy (Hagerstown, Md.: 1997) 2013, 36, 133. [CrossRef]
- Egland, K.A.; Kumar, V.; Duray, P.; Pastan, I. Characterization of overlapping XAGE-1 transcripts encoding a cancer testis antigen expressed in lung, breast, and other types of cancers. Molecular Cancer Therapeutics 2002, 1, 441-450.
- Nakagawa, K.; Noguchi, Y.; Uenaka, A.; Sato, S.; Okumura, H.; Tanaka, M.; Shimono, M.; Ali Eldib, A.M.; Ono, T.; Ohara, N. XAGE-1 expression in non–small cell lung cancer and antibody response in patients. Clinical cancer research 2005, 11, 5496-5503. [CrossRef]
- Sato, S.; Noguchi, Y.; Ohara, N.; Uenaka, A.; Shimono, M.; Nakagawa, K.; Koizumi, F.; Ishida, T.; Yoshino, T.; Shiratori, Y. Identification of XAGE-1 isoforms: Predominant expression of XAGE-1b in testis and tumors. Cancer Immunity 2007, 7, 5.
- Kikuchi, E.; Yamazaki, K.; Nakayama, E.; Sato, S.; Uenaka, A.; Yamada, N.; Oizumi, S.; Dosaka-Akita, H.; Nishimura, M. Prolonged survival of patients with lung adenocarcinoma expressing XAGE-1b and HLA class I antigens. Cancer Immun 2008, 8, 13.
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015, 4, 1. [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. Bmj 2015, 350, g7647. [CrossRef]
- Mohamed, E.; García Martínez, D.J.; Hosseini, M.S.; Yoong, S.Q.; Hart, S.; Guinn, B.A. Identification of biomarkers for the early detection of non-small cell lung cancer: A systematic review and meta-analysis. Carcinogenesis 2023. [CrossRef]
- Field, J.K.; Duffy, S.; Baldwin, D.R.; Whynes, D.; Devaraj, A.; Brain, K.E.; Eisen, T.; Gosney, J.; Green, B.; Holemans, J. UK Lung Cancer RCT Pilot Screening Trial: Baseline findings from the screening arm provide evidence for the potential implementation of lung cancer screening. Thorax 2016, 71, 161-170. [CrossRef]
- Nasrullah, N.; Sang, J.; Alam, M.S.; Mateen, M.; Cai, B.; Hu, H. Automated Lung Nodule Detection and Classification Using Deep Learning Combined with Multiple Strategies. Sensors (Basel) 2019, 19, 3722. [CrossRef]
- MacMahon, H.; Naidich, D.P.; Goo, J.M.; Lee, K.S.; Leung, A.N.; Mayo, J.R.; Mehta, A.C.; Ohno, Y.; Powell, C.A.; Prokop, M. Guidelines for management of incidental pulmonary nodules detected on CT images: From the Fleischner Society 2017. Radiology 2017, 284, 228-243. [CrossRef]
- Welch, H.G.; Prorok, P.C.; O’Malley, A.J.; Kramer, B.S. Breast-cancer tumor size, overdiagnosis, and mammography screening effectiveness. New England Journal of Medicine 2016, 375, 1438-1447. [CrossRef]
- Bretthauer, M.; Kaminski, M.F.; Hassan, C.; Kalager, M.; Holme, Ø.; Hoff, G.; Løberg, M.; Regula, J.; Castells, A.; Adami, H.-O. America, we are confused: The updated US Preventive Services Task Force recommendation on colorectal cancer screening. 2017. [CrossRef]
- Huang, H.; Wang, W.; Lin, T.; Zhang, Q.; Zhao, X.; Lian, H.; Guo, H. Comparison of the complications of traditional 12 cores transrectal prostate biopsy with image fusion guided transperineal prostate biopsy. BMC urology 2016, 16, 68. [CrossRef]
- Wallace, M.B.; Pascual, J.M.; Raimondo, M.; Woodward, T.A.; McComb, B.L.; Crook, J.E.; Johnson, M.M.; Al-Haddad, M.A.; Gross, S.A.; Pungpapong, S. Minimally invasive endoscopic staging of suspected lung cancer. Jama 2008, 299, 540-546. [CrossRef]
- Saenger, A.; Beyrau, R.; Braun, S.; Cooray, R.; Dolci, A.; Freidank, H.; Giannitsis, E.; Gustafson, S.; Handy, B.; Katus, H. Multicenter analytical evaluation of a high-sensitivity troponin T assay. Clinica chimica acta 2011, 412, 748-754. [CrossRef]
- Kammer, M.N.; Massion, P.P. Noninvasive biomarkers for lung cancer diagnosis, where do we stand? Journal of Thoracic Disease 2020, 12, 3317-3330. [CrossRef]
- Yonemori, K.; Tateishi, U.; Uno, H.; Yonemori, Y.; Tsuta, K.; Takeuchi, M.; Matsuno, Y.; Fujiwara, Y.; Asamura, H.; Kusumoto, M. Development and validation of diagnostic prediction model for solitary pulmonary nodules. Respirology 2007, 12, 856-862. [CrossRef]
- Kupert, E.; Anderson, M.; Liu, Y.; Succop, P.; Levin, L.; Wang, J.; Wikenheiser-brokamp, K.; Chen, P.; Pinney, S.M.; Macdonald, T. Plasma secretory phospholipase A2-IIa as a potential biomarker for lung cancer in patients with solitary pulmonary nodules. Bmc Cancer 2011, 11, 513. [CrossRef]
- Bigbee, W.L.; Gopalakrishnan, V.; Weissfeld, J.L.; Wilson, D.O.; Dacic, S.; Lokshin, A.E.; Siegfried, J.M. A multiplexed serum biomarker immunoassay panel discriminates clinical lung cancer patients from high-risk individuals found to be cancer-free by CT screening. Journal of thoracic oncology 2012, 7, 698-708. [CrossRef]
- Boyle, P.; Chapman, C.; Holdenrieder, S.; Murray, A.; Robertson, C.; Wood, W.; Maddison, P.; Healey, G.; Fairley, G.; Barnes, A. Clinical validation of an autoantibody test for lung cancer. Annals of Oncology 2011, 22, 383-389. [CrossRef]
- Murray, A.; Chapman, C.; Healey, G.; Peek, L.; Parsons, G.; Baldwin, D.; Barnes, A.; Sewell, H.; Fritsche, H.; Robertson, J. Technical validation of an autoantibody test for lung cancer. Annals of Oncology 2010, 21, 1687-1693. [CrossRef]
- Daly, S.; Rinewalt, D.; Fhied, C.; Basu, S.; Mahon, B.; Liptay, M.J.; Hong, E.; Chmielewski, G.; Yoder, M.A.; Shah, P.N.; et al. Development and Validation of a Plasma Biomarker Panel for Discerning Clinical Significance of Indeterminate Pulmonary Nodules. Journal of Thoracic Oncology 2013, 8, 31-36. [CrossRef]
- Tufman, A.; Tian, F.; Huber, R.M. Can microRNAs improve the management of lung cancer patients? A clinician's perspective. Theranostics 2013, 3, 953-963. [CrossRef]
- Robbins, P.F.; Lu, Y.-C.; El-Gamil, M.; Li, Y.F.; Gross, C.; Gartner, J.; Lin, J.C.; Teer, J.K.; Cliften, P.; Tycksen, E. Mining exomic sequencing data to identify mutated antigens recognized by adoptively transferred tumor-reactive T cells. Nature medicine 2013, 19, 747. [CrossRef]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in cancer immunotherapy. Science 2015, 348, 69-74. [CrossRef]
- Castle, J.C.; Kreiter, S.; Diekmann, J.; Löwer, M.; Van de Roemer, N.; de Graaf, J.; Selmi, A.; Diken, M.; Boegel, S.; Paret, C. Exploiting the mutanome for tumor vaccination. Cancer research 2012, 72, 1081-1091. [CrossRef]
- Ding, C.; Zhou, X.; Xu, C.; Chen, J.; Ju, S.; Chen, T.; Liang, Z.; Cui, Z.; Li, C.; Zhao, J. Circulating tumor cell levels and carcinoembryonic antigen: An improved diagnostic method for lung adenocarcinoma. Thorac Cancer 2018, 9, 1413-1420. [CrossRef]
- Massion, P.P.; Antic, S.; Ather, S.; Arteta, C.; Brabec, J.; Chen, H.; Declerck, J.; Dufek, D.; Hickes, W.; Kadir, T.; et al. Assessing the Accuracy of a Deep Learning Method to Risk Stratify Indeterminate Pulmonary Nodules. Am J Respir Crit Care Med 2020, 202, 241-249. [CrossRef]
Figure 1.
Five-year survival and incidence of LC by stage. 15 and 7% of LC patients are diagnosed at the early stages, stage I and II, respectively (pink line) with a high 5-year survival rate of 62% for females (light blue bar) and 51% for males (dark blue bar) at stage I. While 19-48% of patients with a known stage, are diagnosed at the later disease stage (stage III or IV), survival rates are conversely poor at 2-3% at stage IV. Image generated using data from (2016-2020) https://www.cancerresearchuk.org/about-cancer/lung-cancer/survival.
Figure 1.
Five-year survival and incidence of LC by stage. 15 and 7% of LC patients are diagnosed at the early stages, stage I and II, respectively (pink line) with a high 5-year survival rate of 62% for females (light blue bar) and 51% for males (dark blue bar) at stage I. While 19-48% of patients with a known stage, are diagnosed at the later disease stage (stage III or IV), survival rates are conversely poor at 2-3% at stage IV. Image generated using data from (2016-2020) https://www.cancerresearchuk.org/about-cancer/lung-cancer/survival.
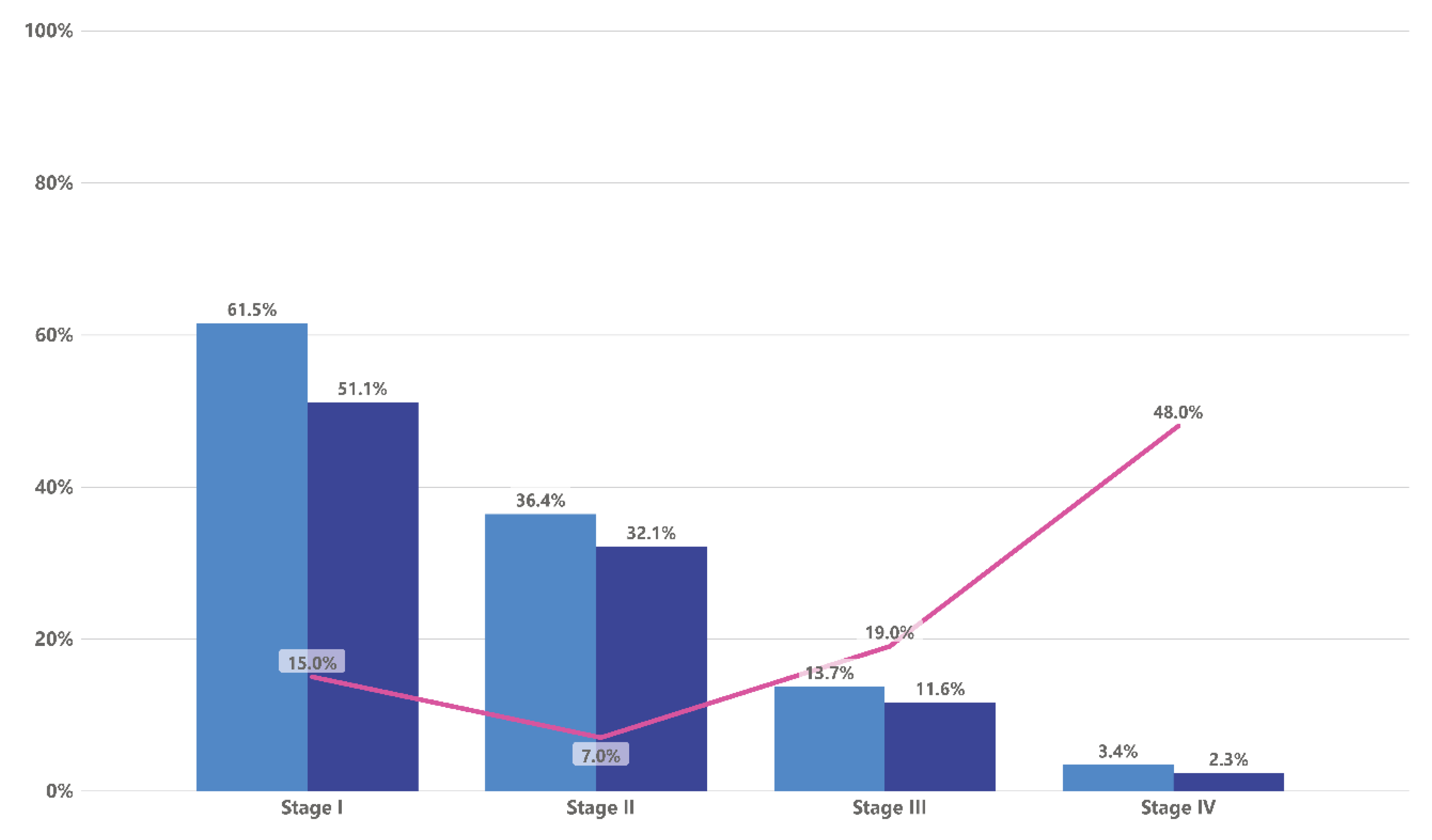
Figure 2.
Expression of CTAs in NSCLC. NSCLC is considered to be a tumour type with high expression of CTAs. CAGE/CT26 and NANOS3 are widely expressed in most samples from patients with NSCLC (100% and 94.7% respectively) while BAGE1, TDRD1 and SYCP1 had limited expression in less than 10% of NSCLC samples. Data was taken from Gure et al. [78].
Figure 2.
Expression of CTAs in NSCLC. NSCLC is considered to be a tumour type with high expression of CTAs. CAGE/CT26 and NANOS3 are widely expressed in most samples from patients with NSCLC (100% and 94.7% respectively) while BAGE1, TDRD1 and SYCP1 had limited expression in less than 10% of NSCLC samples. Data was taken from Gure et al. [78].
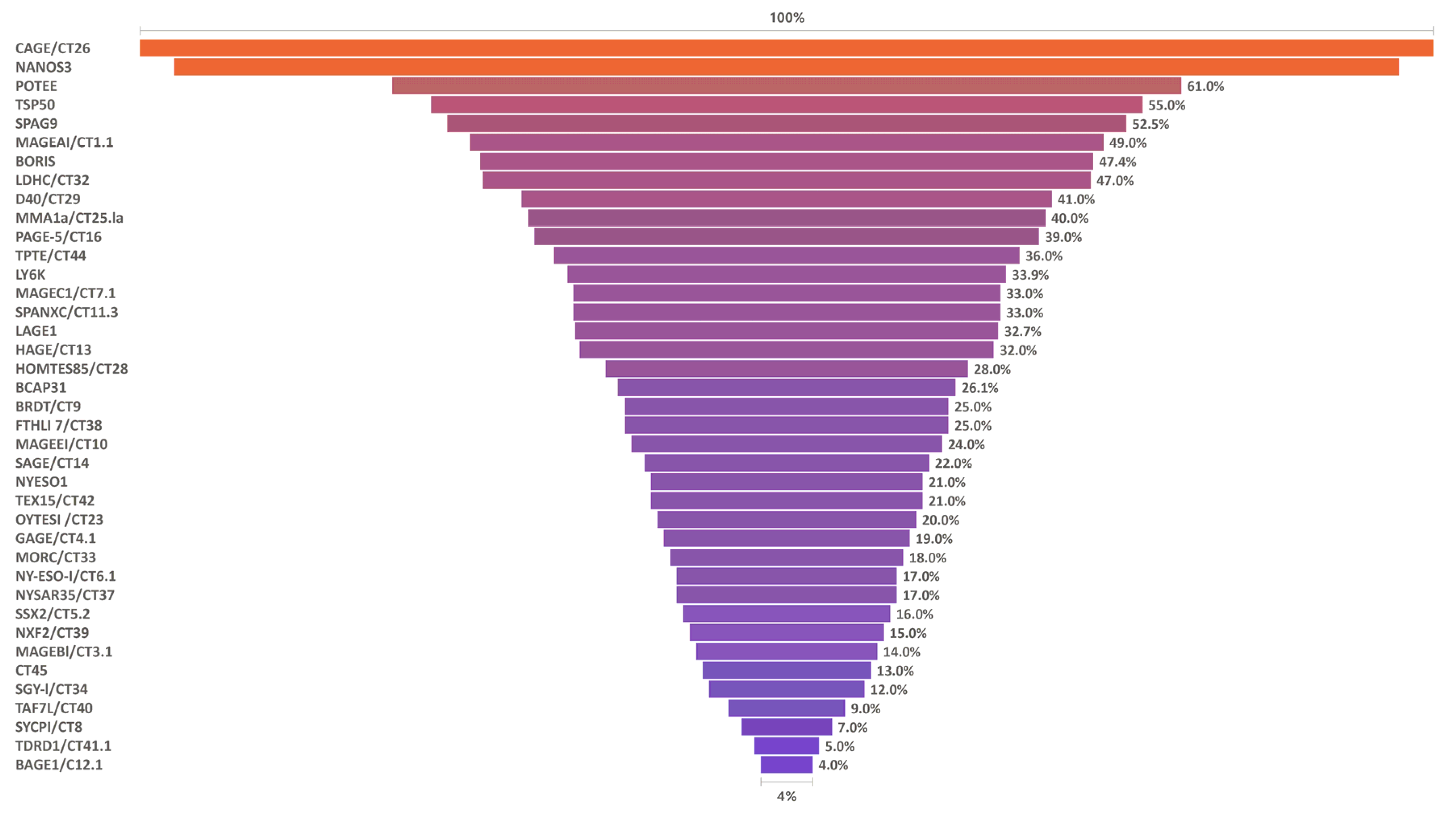

Table 1.
List of antigens known to be expressed in LC.
| Gene name (symbol) | Function | Healthy tissue | Expression in LC(s) | Reference(s) |
|---|---|---|---|---|
| Carcinoembryonic antigen (CEA) | Glycoprotein involved in cell adhesion and signal transduction | Low expression in colon, appendix | High expression all types in advanced stages | [25,26] |
| Osteopontin (OPN) | Cell survival and angiogenesis |
Gall bladder, placenta, brain |
High expression associated with poor prognosis |
[25,27] |
| Cytokeratin 19 fragments (CYFR A 21-1) |
Part of the cytoskeleton of epithelial cells | All epithelial cells |
NSCLC mainly SCC. High expression associated with negative prognosis rather than advanced stages |
[28] |
| Neuron specific enolase (NSE) |
Glycolytic enzyme involved in inflammatory and neurotrophic activity regulating neuronal growth, differentiation, survival and death |
Brain, adrenal, lung | Preferred for SCLC but also NSCLC and a marker of metastasis | [29] |
| Serum amyloid A (SAA) |
Secreted during acute inflammation, transports cholesterol to liver, recruits immune cells to inflammatory sites |
Housekeeping” role in normal human tissues | All types. High expression in late stages |
[30,31] |
Table 2.
CTAs expression in LC using Kaplan Meier plot website for the survival. Data from https://kmplot.com/analysis/.
Table 2.
CTAs expression in LC using Kaplan Meier plot website for the survival. Data from https://kmplot.com/analysis/.
| Gene | Probe set | Survival (mo) | P-value | Gene | Probe set | Survival (mo) | P-value | ||
| Low¶ | High¶ | Low¶ | High¶ | ||||||
| TPX2 | 210052_s_at | 96.2 | 42 | <1e-16 | TSP50 | 220126_at | 81 | 56.7 | 0.0009 |
| DNAJB11 | 223054_at | 119.87 | 52 | 8.40E-12 | CTAGE-1 | 220957_at | 79.27 | 61.3 | 0.0009 |
| MAGEA1 | 207325_x_at | 86.27 | 48.6 | 1.40E-11 | PAGE-4 | 205564_at | 76 | 60.73 | 0.001 |
| SSX2IP | 203015_s_at | 91 | 52 | 2.80E-11 | SSX3 | 211670_x_at | 78.5 | 62.2 | 0.0012 |
| DDX12 | 213378_s_at | 89 | 52 | 1.70E-10 | SYCP1 | 206740_x_at | 79.87 | 60 | 0.0018 |
| (DNAJB14) | 222850_s_at | 52 | 111 | 1.20E-09 | NXF2/CT39 | 220257_x_at | 79.87 | 62.2 | 0.0021 |
| MAGEA3 | 209942_x_at | 86.27 | 49.97 | 2.70E-09 | SSX1 | 206626_x_at | 78 | 64.1 | 0.0023 |
| DDX11/KRG2 | 208149_x_at | 88.7 | 54 | 1.10E-08 | DNAJB4 | 203811_s_at | 75.43 | 62.47 | 0.0035 |
| (GAGE3)/CT4.3 | 207663_x_at | 89 | 54.2 | 1.10E-07 | SGY-1/CT34 | 220284_at | 76 | 59 | 0.0053 |
| MAGEA12 | 210467_x_at | 84 | 52 | 2.70E-07 | MEGEA2 | 214603_at | 74 | 59.53 | 0.0058 |
| GAGE1/4/7/11 | 207086_x_at | 88 | 56 | 6.00E-07 | FATE/CT43 | 231573_at | 86.27 | 63 | 0.0085 |
| GAGE12 E | 207086_x_at | 88 | 56 | 6.00E-07 | FATE1 | 231573_at | 86.27 | 63 | 0.0085 |
| TPTE/CT44 | 220205_at | 80.03 | 59 | 1.30E-05 | GPATCH2 | 239768_x_at | 69 | 89 | 0.0094 |
| SAGE | 220793_at | 79.5 | 56.5 | 2.00E-05 | SSX2 | 216471_x_at | 76 | 63.3 | 0.01 |
| MAGEA10 | 210295_at | 86.27 | 57.33 | 2.40E-05 | SPO11/ CT35 | 222259_s_at | 76 | 62.3 | 0.0185 |
| DDX10/HRH-J8 | 204977_at | 79.54 | 57 | 8.70E-05 | (DNAJB13) | 230936_at | 70 | 90 | 0.0188 |
| NA88A/VENTXP1 | 216726_at | 81.2 | 61.2 | 0.0001 | PLU-1/ KDM5B | 211202_s_at | 63 | 77.6 | 0.019 |
| TEX15/CT42 | 221448_s_at | 79.87 | 59 | 0.0001 | LAGE1 | 215733_x_at | 73.3 | 64.1 | 0.025 |
| DNAJB2 (HSPF3) | 202500_at | 62 | 74 | 0.0002 | TAF7L | 220325_at | 76 | 63.4 | 0.0254 |
| MORC1/CT33 | 220850_at | 79.27 | 57 | 0.0003 | TDRD1/CT41.1 | 221018_s_at | 74 | 65.1 | 0.0284 |
| LDHC/CT32/ | 207022_s_at | 78 | 62.2 | 0.0004 | PAGE-1 | 206897_at | 73.2 | 65 | 0.0299 |
| DDX13 (SKIV2L) | 203727_at | 81 | 59.11 | 0.0004 | MAGE-C2 | 215932_at | 74 | 64.1 | 0.0326 |
| (LDHC)/CT32 | 207022_s_at | 78 | 62.2 | 0.0004 | (DNAJB1)/Sis1 | 200666_s_at | 72.33 | 65.57 | 0.0366 |
| MAGE-C1 | 206609_at | 79.5 | 61.2 | 0.0006 | LUZP4/CT28 | 220665_at | 73.3 | 65 | 0.0461 |
| CAGE1 | 1563787_a_at | 91 | 62 | 0.0008 | |||||
¶ - expression levels; mo: months.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



