
Submitted:
27 March 2024
Posted:
28 March 2024
You are already at the latest version
Abstract
Background/Aim: Baricitinib (BAR) is the first oral selective Janus kinase inhibitor approved in Europe for rheumatoid arthritis (RA). Real-world data are still needed to clarify its long-term benefit/risk profile. This study aimed to evaluate the effectiveness, persistence, adherence, and safety of BAR in a real-world setting. Methods: An ambispective study was conducted between October 2017 and December 2021 in RA patients starting BAR. Effectiveness was evaluated by change from baseline in the Disease Activity Score using 28-joint counts-C reactive protein (DAS28CRP), and achievement of low disease activity/remission. Drug persistence was evaluated by Kaplan-Meier analysis. Adherence was estimated by medication possession ratio (MPR) and the 5-item Compliance Questionnaire for Rheumatology. Safety was assessed by global incidence proportion and adjusted incidence rates of adverse events. Results: 61/64 recruited patients were finally analyzed, 83.6% female, 78.7% seropositive, mean age of 58.1 (15.4) years, and disease duration of 13.9 (8.3) years. 32.8% were naïve to biologics and 16.4% received BAR on monotherapy. After a median exposure to BAR of 12.4 (6.6-31.2) months (range 3.1-51.4), a significant change in DAS28CRP was observed (difference -1.2, p=0.000). A total of 70.5% and 60.7% patients achieved low disease activity or remission, respectively and 50.8% (31/61) patients remained on BAR during follow-up with a median persistence of 31.2 (9.3-53.1) months. The average MPR was 0.96 (0.08) and all patients were “good adherents” by questionnaire. 21.3% patients discontinued baricitinib due to toxicity. Conclusion: In our real-world practice, BAR demonstrated effectiveness, large persistence, high adherence to treatment and acceptable safety profile.
Keywords:
JAK-inhibitor
; baricitinib
; rheumatoid arthritis
; real-word data
; persistence
; adherence
; safety
; unmet needs.
1. Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease, typically characterized by polyarticular joint inflammation, with potential extra-articular involvement and frequent comorbidities. The persistent inflammation produces a decrease in the patients’ functional capacity and in their quality of life [1].
The physiopathology of RA includes chronic inflammation of the synovial membrane with the subsequent destruction of the joint cartilage and bone [2]. The current pathogenic model proposes autoimmunity as the main trigger for the disease, in genetically predisposed individuals, with the early presence of circulating autoantibodies to environmental induced neoepitopes (anti-citrullinated protein antibodies [ACPAs] and antibodies against immunoglobulin G, such as rheumatoid factor [RF]) [3].
The main goal of RA treatment is to achieve remission or, at least, low disease activity (LDA) through a “treat to target” strategy [2]. Briefly, disease activity target goals are defined at disease onset, and this activity is tightly monitored aiming to adjust treatment until predefined goals are achieved. The disease activity can be assessed by composite indices such as the Disease Activity Score using 28-joint counts (DAS28), the Clinical Disease Activity Index (CDAI), and the Simplified Disease Activity Index (SDAI) [2].
Current treatment guidelines for RA recommend conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs) as the first step in treatment, and when treatment goals are not met, they endorse adding or switching to either a biologic DMARD (bDMARD), or a targeted synthetic DMARD (tsDMARD) [4]. tsDMARDs inhibit intracellular signalling pathways, specifically the Janus kinase/signal transducer and activator of transcription (JAK-STAT) pathway. BAR, which predominantly inhibits JAK1 and JAK2 isoenzymes, was one of the first JAK inhibitor (JAKi) available for RA treatment [1].
In randomized clinical trials (RCT), BAR demonstrated efficacy in patients naïve to bDMARDs and those with inadequate response to csDMARDs, or Tumour Necrosis Factor inhibitors (TNFi) [5,6,7]. Furthermore, BAR in combination with methotrexate (MTX) achieved better results in some early disease activity outcomes than combination of MTX with adalimumab (ADA) [8].
The increasing incorporation of JAKi into RA therapy, as well as recently arisen safety issues regarding tofacitinib [9] and even BAR [10], warrant more real-world data (RWD) on effectiveness, safety and persistence of BAR, in order to consolidate this drug as one of the alternatives for RA treatment. In addition, the complexity and chronicity of anti-rheumatic treatment may influence adherence; therefore, monitoring adherence is mandatory to identify adherence problems and tailor the interventions to solve them [11]. The lack of persistence or non-adherence can lead to early treatment failure and switch to more intensive treatments. Therefore, the present study was designed to evaluate the effectiveness, persistence, adherence, and safety of BAR in a real-world setting.
2. Materials and Methods
2.1. Study Design and Population
This was a longitudinal ambispective chart review conducted between October 2017 and December 2021 in La Princesa University Hospital (LPUH) in Madrid, Spain (See Figure 1 for study design). Patients eligible for inclusion were aged ≥ 18 years, diagnosed with RA according to the American College of Rheumatology (ACR)/European League against Rheumatism (EULAR) 2010 classification criteria [12], and had initiated BAR between October 2017 and June 2021. The index date was defined as the first BAR prescription date and follow-up as the period between the index date and death, loss to follow-up or last chart review data, whichever came first. The patient recruitment period started in September 2019 until June 2021. For patients who initiated BAR before September 2019, data were collected retrospectively until that date and subsequently all patients on treatment were followed until December 2021, to assure that patients initiating BAR in June 2021 had a minimum follow-up of 6 months. Due to the observation period, the indication for BAR did not include recommendations recently published by The Pharmacovigilance Risk Assessment Committee (PRAC) and endorsed by the European Medicines Agency to minimize the risk of serious side effects of JAKi [13].
2.2. Outcomes
Pre-defined primary endpoints for effectiveness were change from baseline in DAS28-C reactive protein (CRP), and rates of low disease activity (LDA) (2.6<DAS28-ESR≤3.2) and disease remission (DAS28CRP<2.6) [14] at months 6, 12, 24, and at the end of follow-up. As secondary endpoints, rates of EULAR response at the end of follow-up were also assessed. DAS28CRP score was chosen to evaluate effectiveness, based on EULAR/ACR recommendations for defining RA activity in studies with patients and its extended use in clinical practice [15].
The other primary endpoint, treatment persistence, was defined as the maximum days on BAR treatment until discontinuation or end of follow-up (compiled from electronic prescribing and dispensing records) [16] and by the rate of patients who maintained baricitinib at 6, 12, 24, 36 and 48 months and at the end of follow-up. Besides overall persistence, median persistence was differentially assessed in patients who discontinued treatment due to loss of effectiveness, and patients who discontinued treatment due to toxicity. Adherence was calculated by two methods. The first method was the medication possession ratio (MPR), defined as the sum the days’ supply for all fills of the drug in a given time period divided by the number of days in this period (compiled from electronic prescribing and dispensing records). Patients were considered adherent when the MPR≥0.8 [17]. The second method was the 5-item Compliance Questionnaire for Rheumatology (CQR5), a simplified and validated Spanish version of the 19-item CQR [18,19,20]. The questionnaire was only applied to patients with a prospective follow-up.
To evaluate safety, the global incidence proportion (IP) and adjusted incidence rate (IR) per 100 patient-years (PY) of adverse events (AEs) were calculated. Deviations in laboratory values were defined according to the specifications in the BAR summary of product characteristics [21]. AEs were classified according to the Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0 [22].
2.3. Statistical Analysis
Summary statistics are expressed as mean, (standard deviation) or median (25-75 interquartile range) for quantitative variables, or n (percentage) for qualitative variables. Paired analysis of DAS28CRP and laboratory values was performed with the Wilcoxon signed-rank test. Stratified analyses for disease activity and persistence were performed with the Pearson’s chi-squared test in different subgroups according to: presence/absence of RF and/or ACPAs; previous exposure to bDMARDs or JAKi; and combination treatment with csDMARDs or BAR monotherapy. Kaplan-Meier curves were plotted for evaluation of BAR persistence. SPSS version 22.0 was used.
3. Results
3.1. Baseline Population Demographics and Treatments Patterns
Sixty-four patients started treatment with BAR during the inclusion period, but only 61 finally fulfilled the inclusion criteria and were included in the statistical analysis. Fifteen patients initiated BAR before the prospective study started and 13 discontinued treatment until that date. Therefore, those data were collected retrospectively.
Baseline demographics and clinical characteristics are shown in Table 1. Most patients were female, 51/61 (83.6%), with a mean (SD) age at initiation of BAR of 58.1 (15.4) years and mean RA disease duration of 13.9 (8.3) years. Forty-eight (78.7%) patients were positive for RF and/or ACPA, and more than a half, 34/61 (55.7%), had erosive disease. Thirty (49.1%) patients were under glucocorticoid treatment when BAR treatment started.
Regarding previous exposure to bDMARDs, 20 (32.8%) patients were naïve to bDMARDs or JAKi, and the median (25-75 IQR) number of previous bDMARDs or JAKi was 2 (0-4). Seven (11.5%) patients had experienced previous failure to one JAKi, tofacitinib. In relation to combination treatment with csDMARDs, 51 (83.6%) patients used BAR in combination. The mean follow-up time was 19.1 (1.4) months with a range of 3.1-51.4 months.
3.2. Effectiveness
At the end of follow-up, with a median exposure to BAR of 12.4 (6.6-31.2) months, a significant change in DAS28CRP was observed (difference of 1.2, p=0.000) (Table 2).
According to DAS28CRP, 37/61 (60.7%) patients achieved disease remission whereas 43/61 (70.5%) achieved LDA along the follow-up. The evolution of DAS28CRP along follow-up and proportion of patients who achieved disease remission or LDA at months 6, 12, and 24 are shown in Figure 2.
At the end of follow up, 33/61 (54.1%) patients had good response, 10/61 (16.4 %) moderate response, and 18/61 (29.5%) no response according to EULAR criteria.
Combined LDA/remission rates under BAR treatment were similar in patients with RF and/or ACPA positive status and in those with negative status, (70.8% [34/48] vs. 69.2% [9/13] [p=0.911]). Notably, LDA/remission rates were significantly higher in bDMARDs/JAKi-naïve patients compared to previously exposed patients, (95.0% [19/20] vs. 58.5% [24/41], respectively [p=0.014]). According to the number of previous bDMARDs/JAKi, global LDA/remission rates varied from 95.0% (19/20) in bDMARDs/JAKi-naïve patients to 66.7% (4/6) in patients with one previous bDMARDs/JAKi, and 57.1% (20/35) patients with two or more previous drugs (p=0.040). Finally, no significant differences were found between patients in monotherapy with BAR and patients in combination regimen with csDMARDs, 70.0% (7/10) vs. 70.6% (36/51), respectively (p=0.970).
3.3. Persistence
Thirty-one (31/61, 50.8%) patients remained on treatment with BAR at the end of follow-up, with a mean time of 12.4 (6.6-31.2) months on treatment and median persistence of 31.2 (9.3-53.1) months. Kaplan-Meier curves for the global population and stratified for the reason of BAR discontinuation are shown in Figure 3.
During follow-up, BAR treatment was discontinued in 16/61 (26.2%) patients due to lack of effectiveness, whereas 13/61 (21.3 %) patients discontinued BAR due to intolerance/safety reasons. Finally, 1/61 (1.6%) patients ended BAR treatment by own decision. The retention rates at different time points are shown in Figure 4.
The stratified analysis of persistence according to presence/absence of RF and/or ACPAs, previous exposure to sdDMARDs or JAKi, and combination treatment with csDMARDs or BAR monotherapy are shown in Figure 5. The log-rank test indicated a significant difference only in the stratified analysis by previous exposure to bDMARDs/JAKi: median persistence was not reached in naïve patients vs. 11.2 (0.1-25.4) months in the group of patients with prior exposure (p = 0.039).
3.4. Adherence
MPR was calculated in all patients with an average value of 0.96 (0.08). All patients but one were adherent to treatment. Forty-six patients in the prospective study completed the CQR5 questionnaire, and all of them were considered “good adherents”.
3.5. Safety
AEs occurred in 40/61 (65.6%) patients, with an IR per 100 PY of 15.2 (95% CI 15.4-15.1), while severe AEs (SAEs) occurred in 9/61 (14.8%) patients, with an IR per 100 PY of 3.5 (3.3-3.7) (Table 3).
The most prevalent AEs were anaemia in 24/61 (39.3%) patients, infection in 22/61 (36.1%), hypercholesterolemia in 20/61 (32.8%), and abnormal liver enzymes in 19/61 (31.1%). Herpes Zoster (HZ) infection occurred in 7/61 (11.5%) patients (Table 3). Regarding laboratory values during BAR treatment, significant changes from baseline were only found in mean haemoglobin level (13.5 [1.5] g/dL vs. 12.9 [1.4] g/dL, p=0.000) (Table 2).
Thirteen out of 61 (21.3%) patients discontinued BAR treatment due to toxicity. Three patients discontinued treatment due to HZ infection; three due to cancer (two lung and one breast carcinoma), two due to grade 2 anaemia; two due to grade 2 abnormal liver enzymes; one patient due to grade 4 hypertriglyceridemia, grade 4 abnormal liver enzymes, and grade 3 urticaria; one patient due to increased platelet count (>1.000.000 cells/mm3); and one patient due to central retinal vein occlusion. No deaths were recorded.
4. Discussion
The main findings in our study were the high rates of effectiveness, persistence and adherence of BAR in a longstanding and mostly bDMARD experienced population with a significant proportion of seropositivity and erosive disease; nonetheless, biologic-naïve patients achieved a better response to baricitinib treatment.
BAR has recently been incorporated into RA therapy after favorable efficacy results in randomized clinical trials [5,6,7,8]. In clinical practice, BAR has been postulated as one of the therapeutic alternatives for unmet needs in RA patients; in addition, recent safety concerns with tofacitinib [9] have led regulatory agencies to endorse measures to minimize risk across all JAKi in chronic inflammatory diseases [13,23]. Therefore, a repurposing of these drugs in RA armamentarium, at least in some subpopulations, have arisen. Our safety data in a population not selected by current recommendations can provide additional information to that on published RWD on BAR treatment [24,25,26]. Unlike most real-world studies, we provide long-term safety data through adjusted incidence rates (IR) per 100 patient-years, where BAR demonstrated an acceptable safety profile.
The characteristics of our patients (age about 60 years, long established RA and few number of patients naïve to biologics or JAKi) are in line with other real-world studies [24,26], whereas our use of BAR in monotherapy is inferior to that of most published studies, that also shows a wide geographical heterogeneity [24].
Regarding effectiveness, a recent systematic review of BAR RWD points that most of the studies reported LDA/disease remission rates after a six-month follow-up [26]. Herein we report high rates of LDA/disease remission in extended timeframes, as well as EULAR response at the end of follow-up. Rapid decrease of DAS28CRP was detected in the first six months, which led to sustained remission, i.e., more than 70% of patients in remission at 6 months of follow-up and more than 90% at 12 or successive months. These findings corroborate the effectiveness of BAR observed in other real-world studies [27,28,29,30,31,32,33,34,35,36].
The effectiveness of BAR treatment was not significantly affected by the presence of RF and/or ACPAs, nor by combination treatment with csDMARDs, in accordance with studies by Takahasi et al. [27] and Guidelli et al. [37], but contrary to that of Iwamoto el al. [28], where patients in combination treatment with MTX achieved a better response. On the other hand, patients naïve to bDMARDs or JAKi treatment had higher LDA and disease remission rates than patients with previous exposure to one bDMARDs, or two or more bDMARDs, in line with previous studies [27,28,37]. Accordingly, this result supports that patients naïve to bDMARDs may benefit more from BAR treatment.
In our population, persistence of BAR treatment was large; median persistence was 31 months, and half of the patients remained on treatment at the end of follow-up. Moreover, retention rates at 6, 12, and 24 months were high and similar to those described in others observational studies [27,29,30,31,32,38,39,40]. Beyond these time points, available RWD are limited [24,26,41]. In our study, around 40% of the refractory patients who completed the 36 or 48-month follow-up were still on treatment. In a long-term study, Smolen et al. [41] described a lower discontinuation rate of BAR at 36 months, but it should be noted that the patients were recruited in a RCT and were naïve to cs/bDMARDs, reflecting a selected population far from the context of RWD studies.
The Kaplan-Meier curve of persistence in patients who discontinued BAR treatment due to lack of effectiveness showed a rapid initial decrease followed by a stabilisation in the following months. This pattern indicates that most discontinuations due to lack of effectiveness were due to primary failure, as they occurred in the first months of treatment, in accordance with results of other studies [27,38]. Treatment discontinuations due to toxicity were more gradual over time. Furthermore, those trends suggest that the initial decrease observed in the overall curve could be mainly attributed to lack of effectiveness, whereas discontinuation due to toxicity occurred more frequently in advanced treatments.
Median persistence was much bigger in bDMARD- or JAKi-naïve patients than in those with prior exposure to bDMARDs or JAKi, in accordance with previous data reported from a larger Spanish cohort [31] and with the conclusions of an exhaustive review of real-world studies [24]. By contrast, in the retrospective Japanese ANSWER cohort [40], the number of prior bDMARDs or JAKi did not affect JAKi (BAR and tofacitinib) retention, although the analysed persistence was limited to 20 months. On the other hand, in our study, statistical significance was not reached in stratified analysis according to presence/absence of RF/ACPA, and we cannot rule out that the size population was behind those results. Indeed, the median persistence was much bigger in patients with seropositive status than in those with seronegative status (44.0 vs 9.7 months). Interestingly, a similar trend in persistence associated to seropositive status was also described in a Spanish multicentre cohort [31] and reached statistical significance in a multicentre Italian study [37]. However, this finding was not corroborated in a recent single-centre study [42] and therefore further research is warranted to clarify this discrepancy. Finally, no difference in persistence was found in stratified analysis in patients with BAR monotherapy or combination treatment with csDMARDs, also in accordance with previous reports [28,31,40].
Adherence to treatment, assessed by RMP and CQR5, was high, close to 100%. These results contrast with the low adherence to RA oral treatment determined in two studies conducted in Spain with csDMARDs [43,44]. According to our findings, a high adherence to both JAKi BAR and tofacitinib was demonstrated in the study by Codes-Mendez et al. [45], suggesting that a good tolerance and rapid abrogation of symptoms can improve patients’ compliance with treatment. Nonetheless, due to the high adherence rates, no comparison between effectiveness and adherence was performed in our population.
Concerning safety, more than half of our patients reported AEs. However, most of them were moderate, leading to BAR discontinuation in thirteen patients and SAE occurrence in nine patients. However, to adjust for population size and exposure time, our safety data are shown as incidence rate per 100 PY. Comparison with similar published real-world studies is challenging as they are cohorts with limited sample or shorter follow-up than ours and do not estimate incidence rates per PY [26]. Therefore, for SAEs we must use publications of national databases or registries, taking in mind that our values reflect crude and not standardized IRs. In our study, the AE with the highest IR per 100 PY was anaemia. In contrast to findings by Takahashi et al. [27], and Deprez et al. [46], which reported normalization of haemoglobin values after a decrease in the first months of treatment, we observed a significant decrease in haemoglobin values along the follow-up that never led to BAR discontinuation. Regarding infections, HZ was the most common reported infection and one of the main causes of BAR discontinuation, similarly to other publications [8,27,28,47,48,49,50], but none was considered SAE. It should be noted that all but one patient with HZ were under glucocorticoid treatment at time of infection. Indeed, glucocorticoid treatment and older age have been described as risk factors for HZ and other infections [51]. Vaccination against HZ is currently recommended for all patients prior to initiation of JAKi treatment and could be considered for those already on treatment [52]. Only bacterial pneumonia was considered serious infection with an IR per 100 PY of 1.1 (0.8-1.4), which ranges within the lowest SAE rates for BAR reported by Salinas et.al in a meta-analysis of multi-databases using disease registries and claims [53], although we use crude and not standardized adjusted IRs.
Regarding cardiovascular SAEs, besides findings with tofacitinb in the Oral surveillance trial for RA [9], several RWD studies with JAKi have observed an increased risk of major adverse cardiovascular events (MACE) or thromboembolism in elderly patients with certain cardiovascular risk factors [53,54,55]. No MACE was recorded in our cohort and only one venous thrombotic event was observed, in line with standardized incidence rates described by Uchida et al. [51] or in the meta-analysis by Salinas et al. [53].
Three patients discontinued BAR due to a new diagnosis of cancer, with a crude IR per 100 PY of 1.1 (0.8-1.4), consistent with known data from RWD studies [35,48,50,51,53,56]. The two patients with lung carcinoma were ≥ 65 years old and smokers, two conditions in which treatment with BAR would not have been initiated according to the current recommendations.
To conclude, despite our severe RA population, we have not found any increase in SAEs compared with the safety profile reported in RWD studies. However, and given the recent recommendations, it is necessary to assess inter-individual risk-benefit ratio at the initiation of BAR treatment.
This study has some limitations. First, those related to the non-interventional, ambispective design. Second, the limited sample size; we cannot rule out that a larger population could have provided significant differences in some outcomes of the stratified group analysis. Third, the unicentric population can limit the generalization of the results, although our findings are consistent with those reported in multicentric experiences in our country [31]. Finally, we did not collect smoking status, body mass index, or other confounding variables that could interfere with the therapeutic response [57] or interpretation of safety data.
5. Conclusions
In this real-world study, BAR was mainly used in patients with moderate, erosive, seropositive, long-standing RA, previously exposed to more than one b/tsDMARDs. These characteristics have been associated with more severe disease and greater difficulty to reach the therapeutic target. Despite this, BAR can provide significant benefits in several outcomes in rheumatoid arthritis patients, even in those with longstanding, severe and refractory disease. However, patients without previous exposure to biologics appear to benefit more from the drug. A good adherence and the acceptable safety profile, contribute to a high persistence. Together with considering safety concerns, which are mandatory in the selection of treatment candidates, all previous data support a good risk/benefit ratio of BAR in daily clinical practice. Additional prospective studies with a greater sample size are needed to confirm these findings.
Author Contributions
Conceptualization, Esther Ramírez Herráiz, Alberto Morell Baladrón and Rosario García-Vicuña ; Data curation, Alberto Calvo-Garcia and Esther Ramírez Herráiz; Formal analysis, Alberto Calvo-Garcia and Esther Ramírez Herráiz; Funding acquisition, Alberto Morell Baladrón; Investigation, Alberto Calvo-Garcia, Esther Ramírez Herráiz, Irene Llorente Cubas, Blanca Varas De Dios and Rosario García-Vicuña ; Methodology, Esther Ramírez Herráiz and Rosario García-Vicuña ; Project administration, Esther Ramírez Herráiz; Resources, Esther Ramírez Herráiz, Irene Llorente Cubas, Blanca Varas De Dios, Alberto Morell Baladrón and Rosario García-Vicuña ; Supervision, Esther Ramírez Herráiz, Juana Benedí González and Rosario García-Vicuña ; Validation, Esther Ramírez Herráiz and Rosario García-Vicuña ; Writing – original draft, Alberto Calvo-Garcia; Writing – review & editing, Esther Ramírez Herráiz and Rosario García-Vicuña. All the authors have substantially reviewed the draft manuscript and approved the submitted version.
Funding
This research received no external funding. The APC was funded by a grant to AMB through the Biomedical Research Foundation (FIB) of the Hospital Universitario la Princesa.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board Hospital Universitario de La Princesa (IRB 25 April 2019, approval number 3742,).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors thanks to Manuel Gómez-Gutierrez, form the Methodology Unit, Hospital Universitario la Princesa, for his help in the translation and editing.
Conflicts of Interest
AC-G and ILLC declares personal fees for participating in research from Lilly, outside the submitted work. RG-V reports research or educational grants to her institution from Abbvie, BMS, MSD, Janssen, Lilly, Novartis, and Sanofi; has received personal fees for participating at advisory boards or delivered presentations sponsored by Abbvie, Biogen, BMS, Lilly, Pfizer, Sandoz and Sanofi; all outside the submitted work. ERH, BVdeD, JBG and AMB declare that they have no conflict of interest.
References
- Castañeda, S.; González-Álvaro, I. Novedades en el panorama terapéutico de la Artritis Reumatoide. Reumatol Clin 2017, 13, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Smolen, J. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef] [PubMed]
- Firestein, G.; McInnes, I.B. Immunopathogenesis of rheumatoid arthritis. Immunity 2017, 46, 183–196. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.B.M.; Bergstra, S.A.; Kerschbaumer, A.; Sepriano, A.; Aletaha, D.; Caporali, R.; Edwards, C.J.; Hyrich, K.L.; Pope, J.E.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis 2023, 82, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.; Schiff, M.; van der Heijde, D.; Ramos-Remus, C.; Spindler, A.; Stanislav, M.; Zerbini, C.A.; Gurbuz, S.; Dickson, C.; de Bono, S.; el, al.; el al. Baricitinib, Methotrexate, or Combination in Patients With RA and No or Limited Prior DMARDs Treatment. Arthritis Rheumatol 2017, 69, 506–517. [Google Scholar] [CrossRef] [PubMed]
- Dougados, M.; van der Heijde, D.; Chen, Y.C.; Greenwald, M.; Drescher, E.; Liu, J.; Beattie, S.; Witt, S.; de la Torre, I.; Gaich, C.; et al. Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: results from the RA-BUILD study. Ann Rheum Dis 2017, 76, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Genovese, M.C.; Kremer, J.; Zamani, O.; Ludivico, C.; Krogulec, M.; Xie, L.; Beattie, S.D.; Koch, A.E.; Cardillo, T.E.; Rooney, T.P.; et al. Baricitinib in Patients with Refractory Rheumatoid Arthritis. N Engl J Med 2016, 374, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.C.; Keystone, E.C.; van der Heijde, D.; Weinblatt, M.E.; Del Carmen Morales, L.; Reyes Gonzaga, J.; Yakushin, S.; Ishii, T.; Emoto, K.; Beattie, S.; et al. Baricitinib versus Placebo or Adalimumab in Rheumatoid Arthritis. N Engl J Med 2017, 376, 652–662. [Google Scholar] [CrossRef]
- Ytterberg, S.R.; Bhatt, D.L.; Mikuls, T.R.; Koch, G.G.; Fleischmann, R.; Rivas, J.L.; Germino, R.; Menon, S.; Sun, Y.; Wang, C.; et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N Engl J Med 2022, 386, 316–326. [Google Scholar] [CrossRef]
- Taylor, P.C.; Bieber, T.; Alten, R.; Witte, T.; Galloway, J.; Deberdt, W.; Issa, M.; Haladyj, E.; De La Torre, I.; Grond, S.; et al. Baricitinib Safety for Events of Special Interest in Populations at Risk: Analysis from Randomised Trial Data Across Rheumatologic and Dermatologic Indications. Adv Ther 2023, 40, 1867–1883. [Google Scholar] [CrossRef]
- Sabaté, E. Adherence to long-term therapies: evidence for action. 2003. Available online: http://www.who.int/chronic_conditions/adherencereport/en/ (accessed on 15 July 2023).
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Europen Medicine Agency. EMA confirms measures to minimise risk of serious side effects with Janus kinase inhibitors for chronic inflammatory disorders. Available online: https://www.ema.europa.eu/en/medicines/human/referrals/janus-kinase-inhibitors-jaki (accessed on 06 March 2023).
- Fransen, J.; van Riel, P.L. The Disease Activity Score and the EULAR response criteria. Rheum Dis Clin North Am 2009, 35, 745–757. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Landewe, R.; Karonitsch, T.; Bathon, J.; Boers, M.; Bombardier, C.; Bombardieri, S.; Choi, H.; Combe, B.; Dougados, M.; et al. Reporting disease activity in clinical trials of patients with rheumatoid arthritis: EULAR/ACR collaborative recommendations. Ann Rheum Dis 2008, 67, 1360–1364. [Google Scholar] [CrossRef] [PubMed]
- Raebel, M.A.; Schmittdiel, J.; Karter, A.J.; Konieczny, J.L.; Steiner, J.F. Standardizing terminology and definitions of medication adherence and persistence in research employing electronic databases. Med Care 2013, 51, S11–S21. [Google Scholar] [CrossRef] [PubMed]
- Martínez-López de Castro, N.; Álvarez-Payero, M.; Samartín-Ucha, M.; Martín-Vila, A.; Piñeiro-Corrales, G.; Pego Reigosa, J.M.; Rodríguez-Rodríguez, M.; Melero-González, R.B.; Maceiras-Pan, F.J. Adherence to biological therapies in patients with chronic inflammatory arthropathies. Farm Hosp 2019, 43, 134–139. [Google Scholar] [CrossRef]
- de Klerk, E.; van der Heijde, D.; Landewé, R.; van der Tempel, H.; van der Linden, S. The compliance-questionnaire-rheumatology compared with electronic medication event monitoring: a validation study. J Rheumatol 2003, 30, 2469–2475. [Google Scholar] [PubMed]
- Hughes, L.D.; Done, J.; Young, A. A 5 item version of the Compliance Questionnaire for Rheumatology (CQR5) successfully identifies low adherence to DMARDs. BMC Musculoskelet Disord 2013, 14, 286. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Avila, D.G.; Accini, M.; Tobón, M.; Moreno, S.; Rodriguez, V.; Matín Gutierrez, J. Validación y calibración al español del cuestionario CQR para la medición de adherencia a la terapia antirreumática en un grupo de pacientes colombianos con artritis reumatoide. Clin Exp Rheumatol 2019, 26, 105–110. [Google Scholar] [CrossRef]
- Agencia Española de Medicamentos y Productos Sanitarios. Ficha técnica Olumiant (Baricitinib). Available online: https://cima.aemps.es/cima/pdfs/ft/1161170010/FT_1161170010.pdf (accessed on 15 July 2022).
- United Stated Deparment of Health and Human Service. Common Terminology Criteria for Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 15 July 2022).
- US Food and Drug Administration. FDA requires warnings about increased risk of serious heart-related events, cancer, blood clots, and death for JAK inhibitors that treat certain chronic inflammatory conditions. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-requires-warnings-about-increased-risk-serious-heart-related-events-cancer-blood-clots-and-death (accessed on 06 March 2023).
- Taylor, P.C.; Laedermann, C.; Alten, R.; Feist, E.; Choy, E.; Haladyj, E.; De La Torre, I.; Richette, P.; Finckh, A.; Tanaka, Y. A JAK Inhibitor for Treatment of Rheumatoid Arthritis: The Baricitinib Experience. J Clin Med 2023, 12, 4527. [Google Scholar] [CrossRef]
- Kearsley-Fleet, L.; Davies, R.; De Cock, D.; Watson, K.D.; Lunt, M.; Buch, M.H.; Isaacs, J.D.; Hyrich, K.L. Biologic refractory disease in rheumatoid arthritis: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann Rheum Dis 2018, 77, 1405–1412. [Google Scholar] [CrossRef]
- Hernández-Cruz, B.; Kiltz, U.; Avouac, J.; Treuer, T.; Haladyj, E.; Gerwien, J.; Gupta, C.D.; Conti, F. Evidence on Baricitinib for the Treatment of Rheumatoid Arthritis. Rheumatol Ther 2023, 10, 1417–1457. [Google Scholar] [CrossRef]
- Takahashi, N.; Asai, S.; Kobayakawa, T.; Kaneko, A.; Watanabe, T.; Kato, T.; Nishiume, T.; Ishikawa, H.; Yoshioka, Y.; Kanayama, Y.; et al. Predictors for clinical effectiveness of baricitinib in rheumatoid arthritis patients in routine clinical practice: data from a Japanese multicenter registry. Sci Rep 2020, 10, 21907. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, N.; Sato, S.; Kurushima, S.; Michitsuji, T.; Nishihata, S.; Okamoto, M.; Tsuji, Y.; Endo, Y.; Shimizu, T.; Sumiyoshi, R. , et al. Real-world comparative effectiveness and safety of tofacitinib and baricitinib in patients with rheumatoid arthritis. Arthritis Res Ther 2021, 23, 197. [Google Scholar] [CrossRef] [PubMed]
- Fitton, J.; Melville, A.R.; Emery, P.; Nam, J.L.; Buch, M.H. Real-world single centre use of JAK inhibitors across the rheumatoid arthritis pathway. Rheumatology (Oxford) 2021, 60, 4048–4054. [Google Scholar] [CrossRef] [PubMed]
- Barbulescu, A.; Askling, J.; Chatzidionysiou, K.; Forsblad-d’Elia, H.; Kastbom, A.; Lindström, U.; Turesson, C.; Frisell, T. Effectiveness of baricitinib and tofacitinib compared with bDMARDs in RA: results from a cohort study using nationwide Swedish register data. Rheumatology (Oxford) 2022, 61, 3952–3962. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Cruz, B.; Rosas, J.; Díaz-Torné, C.; Belzunegui, J.; García-Vicuña, R.; Inciarte-Mundo, J.; Pons, A.; Millán, A.M.; Jeria-Navarro, S.; Valero, J.A.; et al. Real-World Treatment Patterns and Clinical Outcomes of Baricitinib in Rheumatoid Arthritis Patients in Spain: Results of a Multicenter, Observational Study iRoutine Clinical Practice (The ORBIT-RA Study). Rheumatol Ther 2022, 9, 589–608. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, F.R.; Ceccarelli, F.; Garufi, C.; Duca, I.; Mancuso, S.; Cipriano, E.; Dell’Unto, E.; Alessandri, C.; Di Franco, M.; Perricone, C.; et al. Effectiveness and safety of baricitinib in rheumatoid arthritis: a monocentric, longitudinal, real-life experience. Clin Exp Rheumatol 2021, 39, 39,525–31. [Google Scholar] [CrossRef] [PubMed]
- González-Freire, L.; Giménez-Candela, R.M.; Castro-Luaces, S.; Veiga-Villaverde, A.B.; Crespo-Diz, C. Baricitinib and tofacitinib in patients with rheumatoid arthritis: results of regular clinical practice. Farm Hosp 2021, 45, 165–169. [Google Scholar] [CrossRef]
- González Mazarío, R.; Fragío Gil, J.J.; Ivorra Cortés, J.; Grau García, E.; Cañada Martínez, A.J.; González Puig, L.; Negueroles Albuixech, R.M.; Román Ivorra, J.A. Efectividad y seguridad en el mundo real de los inhibidores de JAK en la artritis reumatoide: Estudio unicéntrico. Reumatol Clin (Barc.) 2022, 18, 523–530. [Google Scholar] [CrossRef]
- Takagi, M.; Atsumi, T.; Matsuno, H.; Tamura, N.; Fujii, T.; Okamoto, N.; Takahashi, N.; Nakajima, A.; Nakajima, A.; Tsujimoto, N.; et al. Safety and Effectiveness of Baricitinib for Rheumatoid Arthritis in Japanese Clinical Practice: 24-Week Results of All-Case Post-Marketing Surveillance. Mod Rheumatol. [CrossRef]
- Alten, R.; Burmester, G.R.; Matucci-Cerinic, M.; Salmon, J.H.; Lopez-Romero, P.; Fakhouri, W.; de la Torre, I.; Zaremba-Pechmann, L.; Holzkämper, T.; Fautrel, B. The RA-BE-REAL Multinational, Prospective, Observational Study in Patients with Rheumatoid Arthritis Receiving Baricitinib, Targeted Synthetic, or Biologic Disease-Modifying Therapies: a 6-Month Interim Analysis. Rheumatol Ther 2023, 10, 73–93. [Google Scholar] [CrossRef]
- Guidelli, G.M.; Viapiana, O.; Luciano, N.; De Santis, M.; Boffini, N.; Quartuccio, L.; Birra, D.; Conticini, E.; Chimenti, M.S.; Bazzani, C.; et al. Efficacy and safety of baricitinib in 446 patients with rheumatoid arthritis: a real-life multicentre study. Clin Exp Rheumatol 2021, 39, 868–873. [Google Scholar] [CrossRef]
- Rosas, J.; Senabre-Gallego, J.M.; Santos-Soler, G.; Antonio Bernal, J.; Pons Bas, A. Efficacy and Safety of Baricitinib in Patients with Rheumatoid Arthritis and Inadequate Response to Conventional Synthetic DMARDs and/or Biological DMARDs: Data from a Local Registry. Reumatol Clin (Engl Ed) 2022, 18, 188–189. [Google Scholar] [CrossRef]
- Retuerto, M.; Trujillo, E.; Valero, C.; Fernandez-Espartero, C.; Soleto, C.Y.; Garcia-Valle, A.; Aurrecoechea, E.; Garijo, M.; Lopez, A.; Loricera, J.; et al. Efficacy and safety of switching Jak inhibitors in rheumatoid arthritis: an observational study. Clin Exp Rheumatol 2021, 39, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Ebina, K.; Hirano, T.; Maeda, Y.; Yamamoto, W.; Hashimoto, M.; Murata, K.; Onishi, A.; Jinno, S.; Hara, R.; Son, Y.; et al. Drug retention of sarilumab, baricitinib, and tofacitinib in patients with rheumatoid arthritis: the ANSWER cohort study. Clin Rheumatol 2021, 40, 2673–2680. [Google Scholar] [CrossRef]
- Smolen, J.S.; Xie, L.; Jia, B.; Taylor, P.C.; Burmester, G.; Tanaka, Y.; Elias, A.; Cardoso, A.; Ortmann, R.; Walls, C.; et al. Efficacy of baricitinib in patients with moderate-to-severe rheumatoid arthritis with 3 years of treatment: results from a long-term study. Rheumatology (Oxford), 2021, 60, 2256–2266. [Google Scholar] [CrossRef]
- Baldi, C.; Berlengiero, V.; Falsetti, P.; Cartocci, A.; Conticini, E.; D’Alessandro, R.; D’Ignazio, E.; Bardelli, M.; Fabbroni, M.; Cantarini, L.; et al. Baricitinib retention rate: ‘real-life’ data from a mono-centric cohort of patients affected by rheumatoid arthritis. Front Med (Lausanne), 1176. [Google Scholar] [CrossRef]
- Marras, C.; Monteagudo, I.; Salvador, G.; de Toro, F.J.; Escudero, A.; Alegre-Sancho, J.J.; Raya, E.; Ortiz, A.; Carmona, L.; Mestre, Y.; et al. Identification of patients at risk of non-adherence to oral antirheumatic drugs in rheumatoid arthritis using the Compliance Questionnaire in Rheumatology: an ARCO sub-study. Rheumatol Int 2017, 37, 37,1195–02. [Google Scholar] [CrossRef]
- Ibarra Barrueta, O.; Morillo Verdugo, R.; Rudi Sola, N.; Ventura, J.M.; Navarro Aznárez, H. Adherencia en pacientes en tratamiento crónico: resultados del “Día de la Adherencia” del 2013. Farm Hosp 2015, 39, 109–113. [Google Scholar]
- Codes-Mendez, H.; Martinez-Molina, C.; Masip, M.; Riera, P.; Pagès Puigdemont, N.; Riera Magallón, A.; Lobo Prat, D.; Sainz Comas, L.; Corominas, H.; et al. Therapeutic adherence and persistence of tofacitinib and baricitinib in rheumatoid arthritis patients in daily clinical practice. Ann Rheum Dis 2022, 81, 1330. [Google Scholar] [CrossRef]
- Deprez, V.; Le Monnier, L.; Sobhy-Danial, J.M.; Grados, F.; Henry-Desailly, I.; Salomon-Goëb, S.; Rabin, T.; Ristic, S.; Fumery, M.; Fardellone, P.; et al. Therapeutic Maintenance of Baricitinib and Tofacitinib in Real Life. J Clin Med. 2020, 9, 3319. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Xiao, K.; Ottaviani, S.; Stebbing, J.; Wang, Y.J. A real-world disproportionality analysis of FDA Adverse Event Reporting System (FAERS) events for baricitinib. Expert Opin Drug Saf 2020, 19, 1505–1511. [Google Scholar] [CrossRef]
- Taylor, P.C.; Takeuchi, T.; Burmester, G.R.; Durez, P.; Smolen, J.S.; Deberdt, W.; Issa, M.; Terres, J.R.; Bello, N.; Winthrop, K.L. Safety of baricitinib for the treatment of rheumatoid arthritis over a median of 4.6 and up to 9.3 years of treatment: final results from long-term extension study and integrated database. Ann Rheum Dis 2022, 81, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Ahn, S.M.; Kim, Y.G.; Lee, C.K.; Yoo, B.; Hong, S. Safety of JAK inhibitor use in patients with rheumatoid arthritis who developed herpes zoster after receiving JAK inhibitors. Clin Rheumatol 2022, 41, 1659–1663. [Google Scholar] [CrossRef] [PubMed]
- Frisell, T.; Bower, H.; Morin, M.; Baecklund, E.; Di Giuseppe, D.; Delcoigne, B.; Feltelius, N.; Forsblad-d’Elia, H.; Lindqvist, E.; Lindström, U.; et al. Safety of biological and targeted synthetic disease-modifying antirheumatic drugs for rheumatoid arthritis as used in clinical practice: results from the ARTIS programme. Ann Rheum Dis 2023, 82, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Iwamoto, N.; Fukui, S.; Morimoto, S.; Aramaki, T.; Shomura, F.; Aratake, K.; Eguchi, K.; Ueki, Y.; Kawakami, A. Comparison of risks of cancer, infection, and MACEs associated with JAK inhibitor and TNF inhibitor treatment: a multicenter cohort study. Rheumatology (Oxford) 2023, 62, 3358–3365. [Google Scholar] [CrossRef] [PubMed]
- Waldman, R.A.; Sharp, K.L.; Adalsteinsson, J.A.; Grant-Kels, J.M. Herpes zoster subunit vaccine for patients initiating a Janus kinase inhibitor. J Am Acad Dermatol 2022, 88, 697–698. [Google Scholar] [CrossRef] [PubMed]
- Salinas, C.A.; Louder, A.; Polinski, J.; Zhang, T.C.; Bower, H.; Phillips, S.; Song, Y.; Rashidi, E.; Bosan, R.; Chang, H.C.; et al. Evaluation of VTE, MACE, and Serious Infections Among Patients with RA Treated with Baricitinib Compared to TNFi: A Multi-Database Study of Patients in Routine Care Using Disease Registries and Claims Databases. Rheumatol Ther 2023, 10, 201–223. [Google Scholar] [CrossRef]
- Gouverneur, A.; Avouac, J.; Prati, C.; Cracowski, J.L.; Schaeverbeke, T.; Pariente, A.; Truchetet, M.E. JAK inhibitors and risk of major cardiovascular events or venous thromboembolism: a self-controlled case series study. Eur J Clin Pharmacol 2022, 78, 1981–1990. [Google Scholar] [CrossRef]
- Hoisnard, L.; Pina Vegas, L.; Dray-Spira, R.; Weill, A.; Zureik, M.; Sbidian, E. Risk of major adverse cardiovascular and venous thromboembolism events in patients with rheumatoid arthritis exposed to JAK inhibitors versus adalimumab: a nationwide cohort study. Ann Rheum Dis 2023, 82, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Xue, X.; Shannon, J. Characteristics of adverse event reporting of Xeljanz/Xeljanz XR, Olumiant, and Rinvoq to the US Food and Drug Administration. J Manag Care Spec Pharm 2022, 28, 1046–1052. [Google Scholar] [CrossRef]
- Kiely, P.D. Biologic efficacy optimization--a step towards personalized medicine. Rheumatology (Oxford) 2016, 55, 780–788. [Google Scholar] [CrossRef]
Figure 1.
Overall study design. Index data is defined as the first baricitinib prescription date. Follow-up is defined as the period from the index date until the date of the earliest event that led to the end of follow-up, treatment withdrawal, final chart review or missing to follow-up, whichever comes first.
Figure 1.
Overall study design. Index data is defined as the first baricitinib prescription date. Follow-up is defined as the period from the index date until the date of the earliest event that led to the end of follow-up, treatment withdrawal, final chart review or missing to follow-up, whichever comes first.
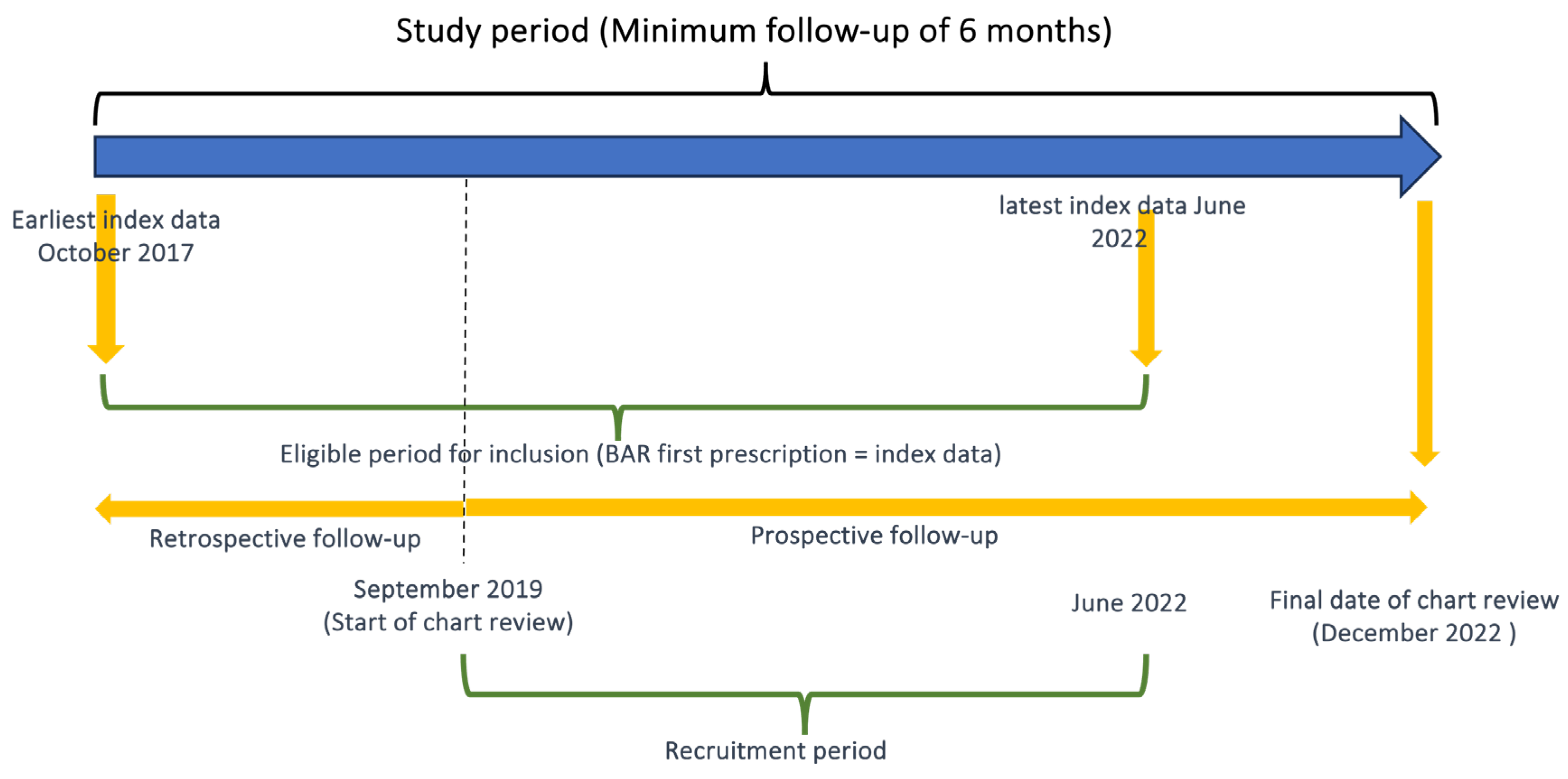
Figure 2.
Baricitinib effectiveness. Change in disease activity from baseline, assessed by disease activity score using 28-joint counts-C reactive protein (a) and proportion of patients who achieved disease remission or low disease activity at months 6, 12 and 24 (b). DAS28CRP: Disease activity score using 28-joint counts-C reactive protein; SD: standard dasviation; LDA: low disease activity.
Figure 2.
Baricitinib effectiveness. Change in disease activity from baseline, assessed by disease activity score using 28-joint counts-C reactive protein (a) and proportion of patients who achieved disease remission or low disease activity at months 6, 12 and 24 (b). DAS28CRP: Disease activity score using 28-joint counts-C reactive protein; SD: standard dasviation; LDA: low disease activity.
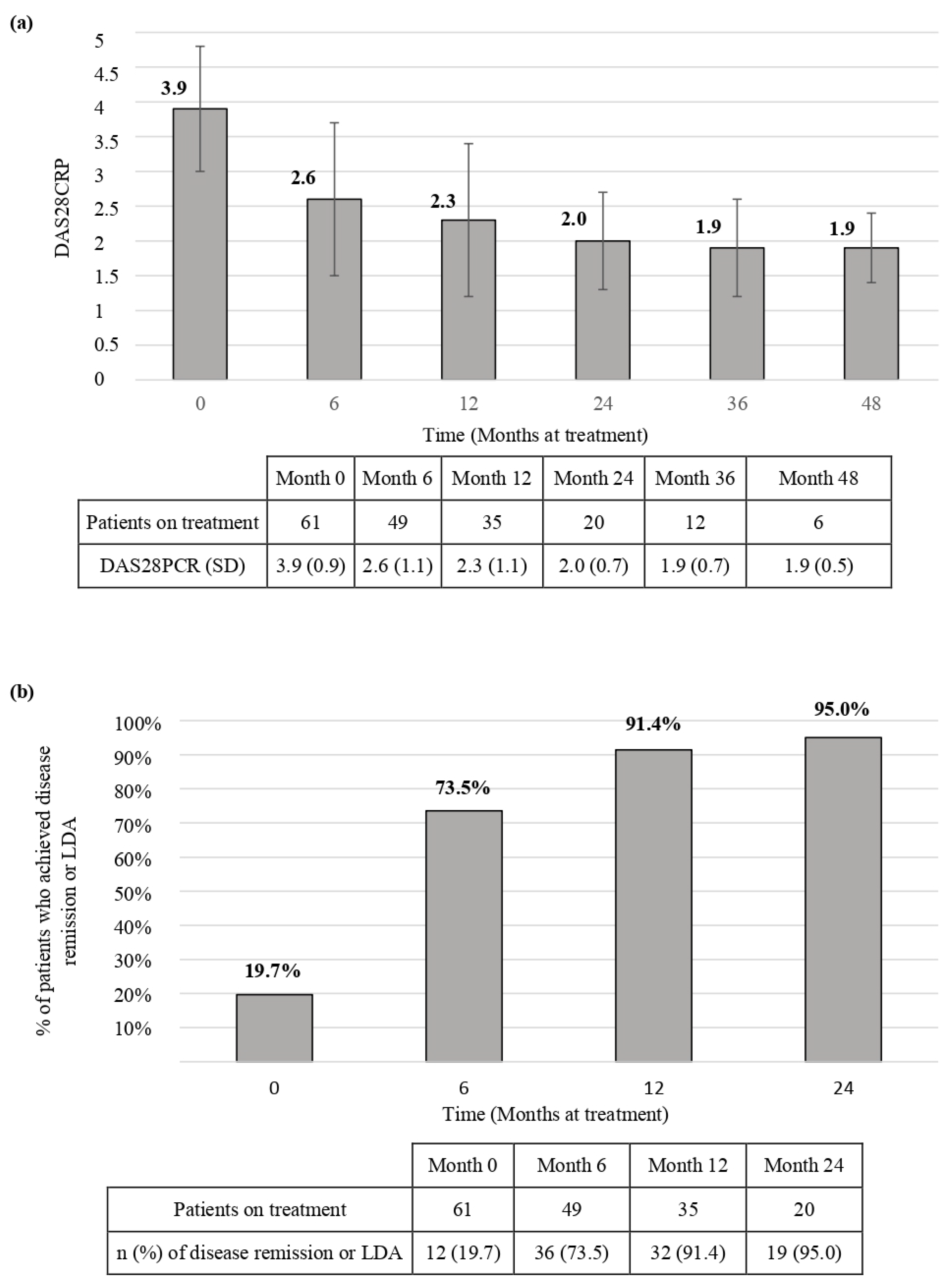
Figure 3.
Baricitinib persistence. Drug retention in the global population (n=61) (a); in patients who discontinued treatment due to loss of effectiveness (n=16) (b), or due to intolerance/safety reasons (n=10) (c). CI: confidence interval.
Figure 3.
Baricitinib persistence. Drug retention in the global population (n=61) (a); in patients who discontinued treatment due to loss of effectiveness (n=16) (b), or due to intolerance/safety reasons (n=10) (c). CI: confidence interval.
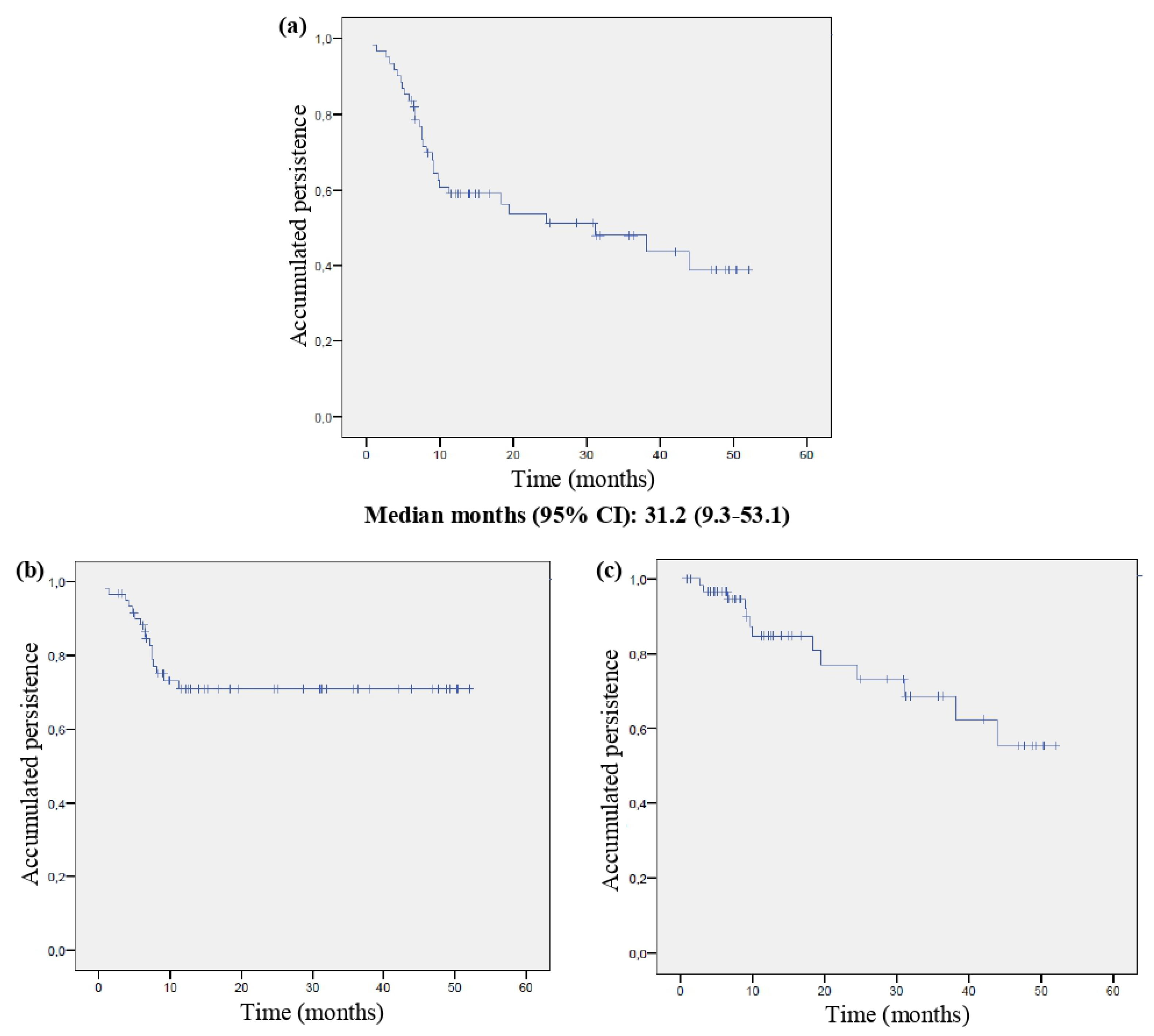
Figure 4.
Retention rates of baricitinib treatment at different time points.
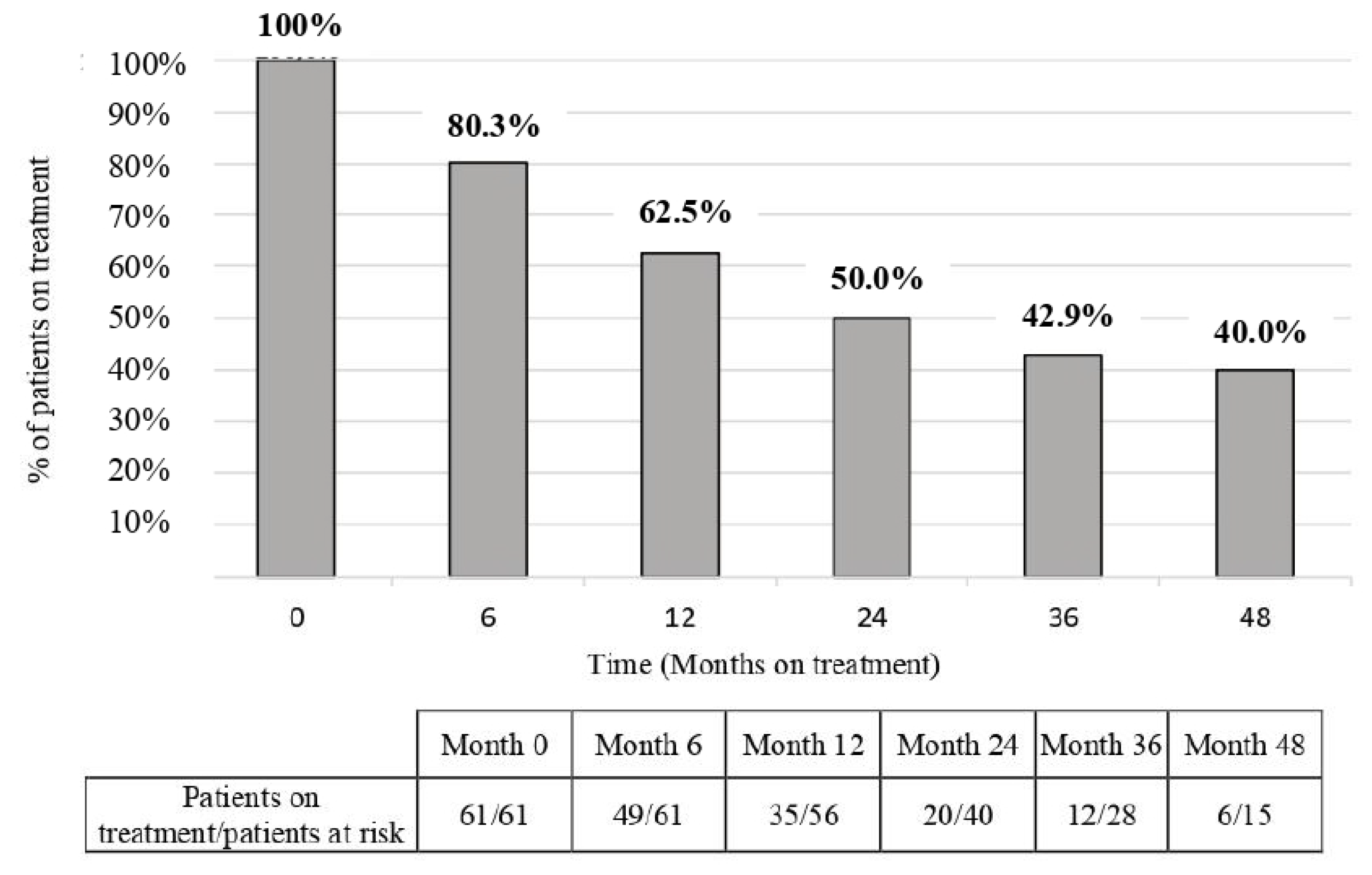
Figure 5.
Baricitinib persistence in different subgroups: (a) according to presence/absence of rheumatoid factor and/or anti-citrullinated protein antibodies; (b) previous exposure to bDMARDs or JAKi; (c) and combination treatment with csDMARDs or baricitinib monotherapy. The log-rank test was used to compare Kaplan-Meier curves. CI: confidence interval; csDMARDs: conventional synthetic disease-modifying anti-rheumatic drugs, bDMARDs: biological disease-modifying anti-rheumatic drugs; JAKi: Janus Kinase inhibitors.
Figure 5.
Baricitinib persistence in different subgroups: (a) according to presence/absence of rheumatoid factor and/or anti-citrullinated protein antibodies; (b) previous exposure to bDMARDs or JAKi; (c) and combination treatment with csDMARDs or baricitinib monotherapy. The log-rank test was used to compare Kaplan-Meier curves. CI: confidence interval; csDMARDs: conventional synthetic disease-modifying anti-rheumatic drugs, bDMARDs: biological disease-modifying anti-rheumatic drugs; JAKi: Janus Kinase inhibitors.
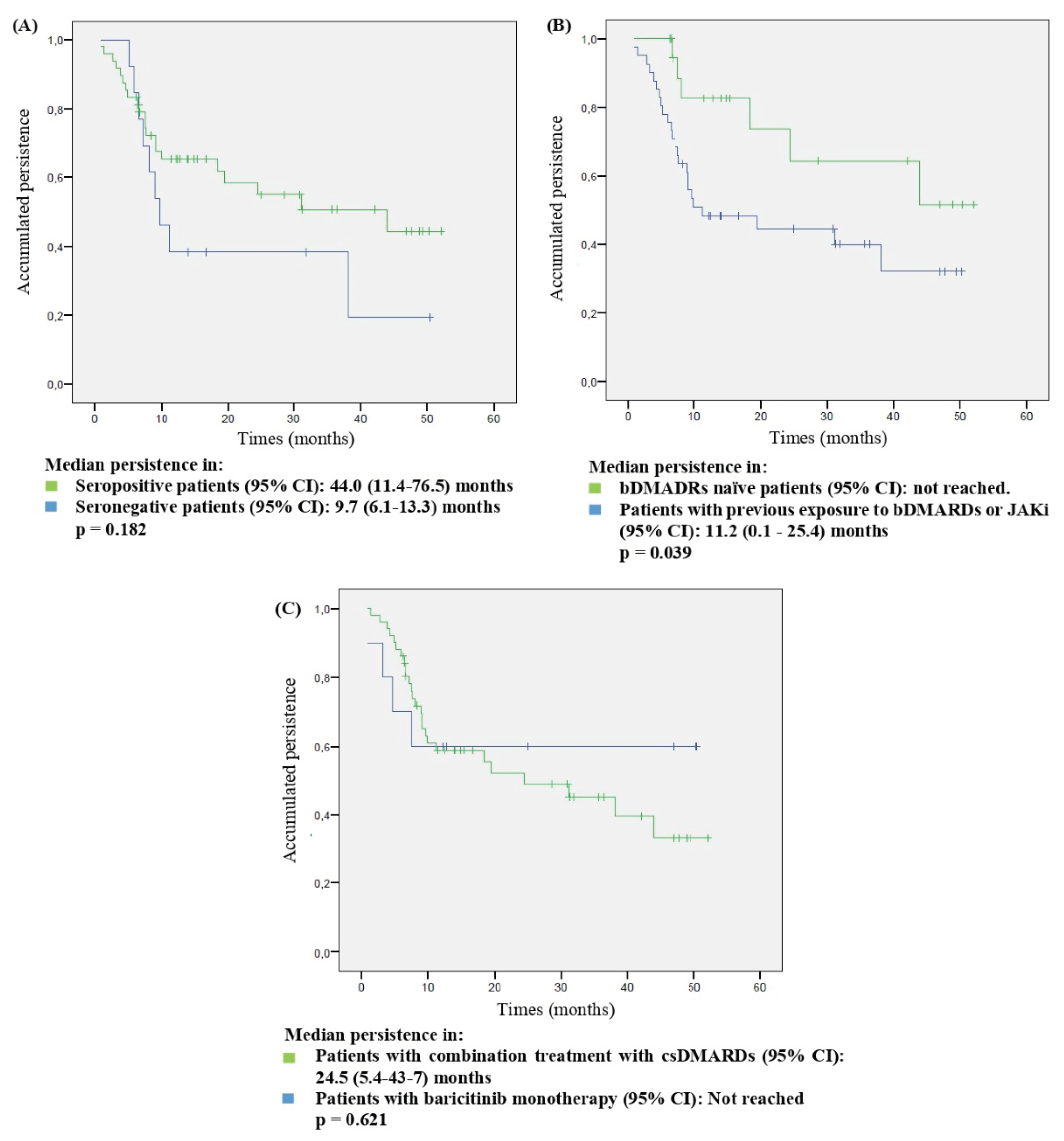

Table 1.
Baseline characteristics of the study population (n=61).
| Gender (n, %, female) | 51 (83.6) |
| Age at initiation of BAR (years, mean, SD) | 58.1 (15.4) |
| Disease duration (years, mean, SD) | 13.9 (8.3) |
| RF positive (n, %) | 47 (77.0) |
| ACPAs positive (n, %) | 43 (70.5) |
| Erosive disease (n, %) | 34 (55.7) |
| Extra-articular disease (n, %) Rheumatic nodules Sjögren syndrome Interstitial pneumonitis Neuropathies Peripheral ulcerative keratitis Raynaud syndrome Felty syndrome |
26 (42.6) 10 (16.4) 7 (11.5) 4 (6.6) 2 (3.3) 1 (1.6) 1 (1.6) 1 (1.6) |
| Glucocorticoid treatment (n, %) | 30 (49.1) |
| Naïve to bDMARDs or JAKi treatment (n, %) | 20 (32.8) |
| Previous exposure to bDMARDs or JAKi (n, %) One previous bDMARD Two previous bDMARDs Three previous bDMARDs Four previous bDMARDs Five previous bDMARDs Six previous bDMARDs Seven previous bDMARDs Eight previous bDMARDs |
41 (67.2) 6 (9.8) 14 (23.0) 8 (13.1) 7 (11.5) 2 (3.3) 2 (3.3) 1 (1.6) 1 (1.6) |
| Previous exposure to one JAKi (tofacitinib) (n, %) | 7 (11.5) |
| BAR monotherapy (n, %) | 10 (16.4) |
| BAR in combination with csDMARDs Methotrexate Leflunomide Hydroxychloroquine Sulfasalazine Methotrexate plus leflunomide |
51 (83.6) 31 (50.8) 14 (23.0) 3 (4.9) 2 (3.3) 1 (1.6) |
| Baseline DAS28CRP (mean, SD) | 3.9 (0.9) |
| Baseline ESR (mml/h, mean, SD) | 27.8 (23.2) |
| Baseline CRP (mg/dl, mean, SD) | 2.0 (4.8) |
BAR: baricitinib; SD: Standard deviation; RF: Rheumatoid factor; ACPAs: Anti-citrullinated protein antibodies; bDMARDs: biologic disease-modifying anti-rheumatic drugs; csDMARDs: conventional synthetic disease-modifying anti-rheumatic drugs; DAS28CRP: Disease activity score using 28-joint counts-C reactive protein; ESR: Erythrocyte sedimentation rate.
Table 2.
Variation in disease activity and laboratory values under baricitinib treatment.
| Baseline | Final | p | |
|---|---|---|---|
| DAS28CRP (average, SD) | 3.9 (0.9) | 2.7 (1.3) | 0.000 |
| CRP (mg/dl, average, SD) | 2.0 (4.8) | 1.1 (1.7) | 0.105 |
| ESR (mml/h, average, SD) | 29.0 (23,2) | 25.7 (22.9) | 0.604 |
| Lymphocyte count (cells/mm3, mean, SD) | 2641 (1501) | 2482.6 (1505) | 0.154 |
| Neutrophil count (cells/mm3, mean, SD) | 4198 (2126) | 4157 (2132) | 0.865 |
| Haemoglobin (g/dl, mean, SD) | 13.5 (1.5) | 12.9 (1.4) | 0.000 |
DAS28CRP: Disease activity score using 28-joint counts-C reactive protein; SD: Standard deviation; ESR:Erythrocyte sedimentation rate.
Table 3.
Adverse events during baricitinib exposure.
| IR (n, %) | IR per 100 PY (95% CI) | |
|---|---|---|
| Patients with any AE (Total AEs=104) | 40/61 (65.6) | 15.2 (15.1-15.3) |
| Anaemia | 24/61 (39.3) | 9.1 (9.0-9.2) |
| Any infection Herpes Zoster URTI Skin and soft tissue infection Bacterial pneumonia Influenza A Oral herpes simple |
22/61 (36.1) 7/61 (11.5) 7/61 (11.5) 5/61 (8.2) 3/61 (4.9) 2/61 (3.3) 2/61 (3.3) |
8.4 (8.2-8.6) 2.7 (2.4-3.0) 2.7 (2.4-3.0) 1.9 (1.7-2.1) 1.1 (0.8-1.4) 0.8 (0.6-1.0) 0.8 (0.6-1.0) |
| Hypercholesterolemia | 20/61 (32.8) | 7.6 (7.4-7.8) |
| Abnormal liver enzymes (ALAT or ASAT) | 19/61 (31.1) | 7.2 (6.9-7.5) |
| Nausea and vomiting | 4/61 (6.6) | 1.5 (1.3-1.7) |
| Cancer | 3/61 (4.9) | 1.1 (0.8-1.4) |
| Alopecia | 2/61 (3.3) | 0.8 (0.6-1.0) |
| Skin disorders | 2/61 (3.3) | 0.8 (0.6-1.0) |
| Asthenia | 2/61 (3.3) | 0.8 (0.6-1.0) |
| Weight gain | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Venous thrombotic event | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Hypertriglyceridemia | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Rhabdomyolysis | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Platelet increase | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Patients with SAEs (Grade 3-4) (Total SAEs=11) | 9/61 (14.8) | 3.5 (3.3-3.7) |
| Bacterial pneumonia with intravenous treatment | 3/61 (4.9) | 1.1 (0.8-1.4) |
| Cancer | 3/61 (4.9) | 1.1 (0.8-1.4) |
| Abnormal liver enzymes (ALT or AST) | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Venous thrombotic event | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Hypertriglyceridemia | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Skin disorders (Urticarial) | 1/61 (1.6) | 0.4 (0.2-0.6) |
| Platelet increase | 1/61 (1.6) | 0.4 (0.2-0.6) |
IP: incidence proportion; IRs: incidence rates; PY: patient-year; CI: Confidence interval; AEs: adverse events; SAEs: severe AEs; URTI: upper respiratory tract infection; ALT: alanine transaminase; AST: aspartate transaminase.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



