
Submitted:
27 March 2024
Posted:
28 March 2024
You are already at the latest version
Abstract
Heart failure (HF) is a growing issue in developed countries and most patients present with a reduced ejection fraction. This condition significantly impairs quality of life and represents a threat not only for patients, but also for the entire healthcare system due to its high management cost. In the last decade, new medical treatments and devices have been developed to reduce HF hospitalizations and improve prognosis, while reducing the overall mortality rate.
Medical therapy does not achieve the same results in all patients and, whenever it fails, technology comes in handy: novel devices for the management of HF have reduced symptoms. They have also improved the treatment of fluid retention and life threatening arrhythmias.
The present review article gives to the readers a comprehensive overview of the most recent and important findings that need to be considered in HF with reduced ejection fraction patients. Both novel medical treatments and devices have been presented and discussed.
Keywords:
heart failure
; reduced ejection fraction
; SGLT2 inhibitors
; vericiguat
; CardioMEMS
; Cardiac Contractility Modulation
; Left bundle branch area pacing
; Wearable cardioverter defibrillators
; Ultrafiltration
1. Introduction
Heart failure (HF) is a common condition currently defined as a clinical syndrome made of symptoms and signs, and characterized by structural and/or functional cardiac abnormalities leading to inadequate oxygen supply or elevated intracavitary pressures [1].
In this population, the majority of patients is represented by the class of HF with reduced ejection fraction (HFrEF). In these patients, the inability of maintaining an adequate peripheral perfusion induces the activation of neurohormonal pathways which, in the long term, lead to cardiac remodeling and increased afterload thereby exacerbating the underlying disfunction [2]. Patients with HFrEF are also at increased risk of arrhythmic events favored by both neurohormonal activation and myocyte dysfunction; this risk may also be temporary due to the potential disease regression induced by medical treatments [3].
In latest years new drugs have been developed and their capability of acting on different pathways provides complementary benefits; in order to properly express such effectiveness, these treatments should be initiated early and quickly titrated.
Along with pharmacological progression, new technologies have been developed in order to provide additional treatments able to act on the natural course of the disease together with a multiparametric monitoring of HF patients.
The review article is divided into two main chapters: the first one is focused on new medical treatments for HFrEF and different strategies for their application on “naïve” patients, while the second one is targeted on new devices for both monitoring and treating advanced HFrEF patients.
2. New Medical Treatments for HFrEF
2.1. Sodium-Glucose Transport Proteins 2 Inhibitors
Sodium-glucose transport proteins 2 (SGLT2) inhibitors, also called gliflozins, are a class of drugs that inhibit SGLT2 in the proximal convoluted tubule of nephron. The main metabolic effect is to inhibit reabsorption of glucose in the kidney and subsequently lower blood sugar. They were initially prescribed as oral hypoglycemic agents and they are currently used for the treatment of type 2 diabetes mellitus. The investigators of the earlier SGLT2 inhibitor studies found that they had excellent cardiovascular benefits in patients with diabetes mellitus. The exact mechanisms through which SGLT2 inhibitors exert their beneficial effect in HF remain not completely understood and some hypotheses have been raised:
- -) blood pressure reduction: an increase in urine glucose excretion as well as reduced sodium reabsorption have been proposed to explain the reducing effect on blood pressure. SGLT2 inhibitors impacted on weight loss[4]. They also act on cholesterol levels by showing low increase in HDL, LDL and total cholesterol levels, and a small decrease in triglycerides[5]. However, improvement of these secondary risk factors of cardiovascular disease are unlikely to completely explain the marked benefit seen with the use of these drugs in patients with HFrEF [6]. It has been hypothesized that other mechanisms could contribute to the beneficial effects observed in HF patients:
- -) effect on cardiac remodeling and contractility: previous studies have demonstrated that empagliflozin led to a significant reduction of diastolic tension without altering the systolic contractile force. Empagliflozin decreases myofilament stiffness in human myocardium through an enhanced phosphorylation process of titin due to improvement of the nitric oxide (NO) pathway[7].
- -) reduction of inflammation: several studies showed that SGLT2 inhibitors have anti-inflammatory and antioxidant properties[8]. Dapagliflozin reduced the inflammasome and fibrosis in mouse models of type 2 diabetes mellitus and myocardial infarction[9] and empagliflozin decreases oxidative stress, associated with metabolic changes, in mice after myocardial infarction [10].
- -) cardiorenal function improvement: SGLT2 inhibitors cause a natriuretic effect favoring sodium excretion by the distal renal tubules inducing a vasoconstriction of the afferent arteriolar vessel and finally restoring the impaired tubuloglomerular feedback mechanism. As a result, the reduced blood flow elicits the release of erythropoietin [11].
Based on this positive effect of cardiovascular system, SGLT2 inhibitors are currently recommended for patients with HFrEF.
The EMPA-REG OUTCOME trial evaluated cardiovascular outcomes with empagliflozin in type 2 diabetes mellitus patients with established cardiovascular disease. The treatment with SGLT2 inhibitors significantly reduced the primary composite endpoint of major adverse cardiovascular events (cardiovascular mortality, nonfatal stroke, nonfatal myocardial infarction and major cardiovascular adverse events) compared to placebo, primarily attributed to a 38% significant reduction in cardiovascular death. Empagliflozin treatment was able to reduce HF hospitalizations by 35%[12]. The Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes (CANVAS) [13] and the Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes (DECLARE TIMI)[14] trials found similar results with canagliflozin and dapagliflozin, respectively.
Other studies were conducted on the role of SGLT2 inhibitors in the management of HF. The Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF) [15] trial was the first study that evaluated the efficacy of an SGLT-2 inhibitor in 4744 patients with stable chronic HFrEF (LVEF <40%). Dapagliflozin was found to significantly reduce the primary composite outcome of cardiovascular death, HF hospitalizations, and urgent HF visits compared to placebo. Of note, the results were identified independently of baseline diabetes mellitus status.
Another study, named the Empagliflozin Outcome Trial in Patients with Chronic Heart Failure and a Reduced Ejection Fraction (EMPEROR-Reduced) trial[16] evaluated the efficacy of empagliflozin in a similar cohort of 3730 HF patients. Empagliflozin significantly reduced the composite outcome of cardiovascular death and HF hospitalizations compared to placebo with a relative risk reduction of 21%. The results were driven by a significant 31% relative risk reduction in HF hospitalizations.
Given the considerable results of DAPA-HF and EMPEROR-Reduced trials, the SGLT2 inhibitors have become one of the main treatments for heart failure. The European Society of Cardiology (ESC) 2021 HF guidelines [17] and the American Heart Association/American College of Cardiology/Heart Failure Society of America (AHA/ACC/HFSA) 2022 HF guidelines [18] recommend the use of SGLT-2 inhibitors (currently only dapagliflozin and empagliflozin) in the treatment of chronic, stable HFrEF with class 1 recommendation for a reduction in cardiovascular death and HF hospitalizations irrespective of baseline diabetes mellitus (Table 1).
2.2. Vericiguat
One of the principal mechanisms involved in HF is the reduced amount of NO or the resistance to this molecule[19,20]. NO acts directly via stimulation of the soluble guanylate cyclase (sGC), which produces cyclic guanosine monophosphate which in turn contributes to the maintenance of vascular tone and cardiac contractility. Other effects include the reduction in profibrotic and inflammatory pathways, and the counteraction of myocyte hypertrophy[21] [22].
Vericiguat is the first sGC stimulator approved for HF on the market and acts both by directly stimulating sGC and by increasing its sensitivity to NO[23].
The principal study that applied this drug on top of optimized medical therapy (OMT) is the VICTORIA study that showed a significant reduction in the primary outcome of first hospitalization for HF or death from cardiovascular causes. Secondary outcomes of total hospitalizations for HF and death from any cause or first hospitalization for HF were also significantly reduced. The study included patients in New York Heart Association (NYHA) class II-IV, left ventricular ejection fraction (LVEF) < 45%, recent (under six months) hospitalization for HF or intravenous diuretics administration in the previous three months, high levels of natriuretic peptides (in sinus rhythm BNP ≥ 300 pg/mL or NT-proBNP ≥1000 pg/mL, in atrial fibrillation BNP ≥ 500 pg/mL or NT-proBNP ≥1600 pg/mL) and an estimated glomerular filtration rate (eGFR) ≥15 mL/min. The benefit was independent of the ongoing treatment and was more evident in patients with NT-proBNP ≤ 4000 pg/mL. Of note, a significant benefit was not found for NT-proBNP values > 8000 pg/mL. Symptomatic hypotension, syncope and the principal side effects were not different among groups[20,24].
Hypotension may require a temporary down-titration or even interruption of the drug. Data from the trial protocol gives precise recommendations regarding the correct management according to symptoms and blood pressure values [24] (Figure 1).
Despite the benefits shown in hospitalizations and mortality, the effects of vericiguat on the heart are still largely unknown. An echocardiographic substudy [25] of the VICTORIA trial was conducted but failed to identify improvement in LVEF or other echocardiographic parameters compared to the placebo group. The current 2021 ESC guidelines give vericiguat a recommendation IIb, level of evidence B for symptomatic patients (NYHA II-IV) with reduced LVEF and worsening HF despite OMT to reduce cardiovascular mortality and hospitalizations[26].
The starting dose of 2.5 mg can be doubled every two weeks to reach the target dose of 10mg. Its bioavailability is high when taken with food (93%) and the plasma half-life reaches 30 hours in patients with HF [22]. No significant drug-drug interactions have been detected, although proton pump inhibitors may reduce its absorption and the association with phosphodiesterase 5-inhibitors, long-acting nitrates or other sGCS like riociguat should be avoided[23].
2.3. Pharmacological Treatment Strategies for Heart Failure with Reduced Ejection Fraction
Pharmacological treatment is the mainstay of HFrEF therapy and should be calibrated and up-titrated before considering device therapy.
The three main objectives of HFrEF therapy are: 1) reduction in mortality, 2) prevention of recurrent hospitalizations due to worsening HF, and 3) improvement in quality of life [27].
Angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARB), β-blocker, and mineralocorticoid antagonists (MRA) are drugs that have demonstrated to improve survival, decrease HF hospitalizations, and improve symptoms in patients with HFrEF by several studies. Based on these results, these classes of drugs are recommended as the initial therapy for patients with HFrEF, unless these drugs are contraindicated or not tolerated [17].
The pharmacological therapy requires that these drugs should be up titrated to the doses applied in the studies or to maximally tolerated doses (Table 2).
In patients with symptomatic HFrEF on OMT, the administration of an angiotensin receptor neprilysin inhibitor (ARNI) is recommended instead of ACE inhibitor or ARB to further reduce mortality and morbidity. In addition, SGLT2 inhibitors, dapagliflozin or empagliflozin, are recommended independently from diabetes mellitus presence to further decrease the risk of worsening HF or cardiovascular death. ESC guidelines also recommend the use of ARNI as a substitution for ACE inhibitor in patients who remain symptomatic on ACE inhibitor, β-blocker and MRA. However, ARNI may be considered as a first-line therapy instead of an ACE inhibitor/ARB in patients with a severely reduced LVEF for whom a complete recovery of LV function is improbable to achieve [17]. Diuretics are usually required to improve symptoms due to fluid overload in the decompensated phase of HF. However, there is no evidence of their effect on survival.
Ivabradine, a selective inhibitor of If current, may be considered to reduce the risk of HF hospitalization or cardiovascular death in patients with symptomatic HFrEF with a sinus rhythm and heart rate of 70–75 bpm or higher despite OMT [28].
As mentioned previously, the conventional sequencing strategy of OMT for chronic HFrEF recommends starting the treatment with an ACE inhibitors or ARBs, β-blockers, and MRA. In a second phase, ARNI can be administered instead of ACEI/ARB and SGLT2 inhibitors added to the medical treatment (Figure 2). Unfortunately, this step-by step approach may not be coherent with the fact that the most effective therapeutic approaches should be started as early as possible [29]. Thus, a new sequencing strategy has been proposed instead of the traditional approach. The revised approach requires the early initiation of all the major four classes of HF drugs (ARNI, β-blocker, MRA, and SGLT2 inhibitor) [30] at their lower dosages (Figure 3). This revised approach can be particularly efficient if started in hospitalized patients before hospital discharge to verify patient compliance and side effect occurrences.
The principles that support the revised strategy are: first, the level of benefit obtained with any class of drugs is independent of that produced by other classes. Second, it has been demonstrated that low starting doses of foundational drugs are effective in reducing morbidity and mortality. Third, the introduction of a new drug class leads to benefits that are greater than up-titration of ongoing drug classes. Fourth, because a great part of the benefits of foundational medications are observed within the 30 days of initiating treatment, the strategy should entail starting with all four types of drugs within the first month [30].
The revised approach requires tree step as follows:
Step 1: Consists of a simultaneous initiation of treatment with a β-blocker and an SGLT2 inhibitor. Indeed, β-Blockers are the drug class with the largest evidence for reducing the risk of sudden death. SGLT2 inhibitors have a high effectiveness for reducing the risk of hospitalizations for HF. SGLT2 inhibitors due to their diuretic action, may alleviate the short-term risk of worsening HF that may occur after a β-blocker has started.
Step 2: Includes the addition of ARNI/ACEI/ARB, within 1 to 2 weeks of step 1. In case of an early initiation of ARNI, if the patient’s systolic blood pressure is low (<100 mm Hg), it may be useful to first assess hypotension tolerance, with an ARB before switching to ARNI. Usually, hypotension is commonly resolved with reducing the dose or with adjustment of the dose of concurrently administered diuretics.
Step 3: Consists of an addition of a MRA, within 1 to 2 weeks of step 2. Step 3 should be preceded by checking the normality of serum potassium and renal function. In this setting the positive effects of ARNI and SGLT2 inhibitors on renal function and potassium homeostasis may favor MRA prescription [30].
The last proposed pharmacological strategy is the tailored one, described in a consensus document of the ESC [31]. The tailored strategy requires to choose pharmacological therapy in HFrEF based on the patient profile. This strategy adjusts medical therapies to the patient's hemodynamic profile considering blood pressure, heart rate, congestion, and kidney function [31] (Figure 4).
Heart rate (HR), blood pressure (BP) and chronic kidney disease (CKD).
3. New Devices for Monitor or Treat HFrEF Patients
3.1. Cardio-Microelectromechanical Systems
Although many innovations in drug treatment for HF have been introduced, HF patients still require frequent ambulatory visits, and they often require hospitalization for acute decompensated HF. These hospital admissions usually last several days and require large amounts of healthcare resources. Repeated hospital admissions for decompensated HF are associated with a decline in myocardial and renal function, additionally, can worse survival [32]. Thus, one of the targets of HF management is the reduction of HF hospitalizations.
Towards this end, in the early 2000s the Cardio-Microelectromechanical systems (MEMS) has been proposed. The CardioMEMS is a wireless pressure sensor that uses MEMS technology. This device consists of an implantable HF sensor and an electronic monitoring unit. It is implanted by right heart catheterization in the distal pulmonary artery. The main role of the sensor is to measure changes in pulmonary artery pressure (PAP). CardioMEMS does not have any batteries or leads, and it is powered by an external antenna in the form of radiofrequency signals. Patients use an electronic unit and a special pillow which contains an antenna. The PAP recordings are transmitted to a clinical hub for processing. The reading takes place when the antenna is held against the body or when the patient lies on the pillow. This process is pain free and does not result in any abnormal sensation during the reading. The electronic unit transmits the PAP measurements daily. The main advantage of CardioMEMS is that the information can be used by the physicians to adjust the HF therapy (mainly through adjusting the diuretic dose) before congestive symptoms develop [33].
The physiopathological basis for the use of CardioMEMS stands on the fact that the symptomatic congestion in HF is typically preceded by progressive PAP rise.
Normally, the cardiopulmonary reflex is activated by elevation of heart filling pressure (Figure 5).
In healthy individuals, fluid overload activates the pressure baroreceptors in the left ventricle, carotid sinus, and aortic arch. This activation induces the brain to inhibit efferent sympathetic nervous system pathways towards heart, kidney, peripheral vasculature, and inhibition of vasopressin secretion. This reflex leads to an increased renal blood flow inducing sodium and water loss.
This reflex avoids an increase in PAP. In fact, the augmented heart filling pressure, through heart baroreceptors, is transmitted to the vasomotor center in the brain that inhibits the sympathetic nervous system and vasopressin secretion. This reflex finally induces an increase in urinary flow [34], restoring the effective circulatory volume and ventricular preload.
HFrEF is associated with a significant reduction of the cardiopulmonary reflex [35] leaving a persistent high adrenergic state (Figure 6).
Decreased cardiac output seen in HFrEF patients results in constant fluid overload that causes dysfunction of pressure baroceptors. This baroceptor dysfunction induces the brain to activate sympathetic nervous system pathways to target organs, and an increase release of vasopressin. The final effect is a reduced sodium and water loss by the kidneys and water retention.
In addition, HF patients are typically associated with low cardiac output that decreases renal perfusion pressure favoring fluid retention. The combination of these events triggers a strong sympathetic nervous system activation, increase renin, and aldosterone release. Sodium and water retention in the kidney is not effectively counteracted by the inhibitory cardiopulmonary reflex. The final consequence of this detrimental cascade is a rapid and significant increase in intravascular volume [36] leading to a progressive increase of PAP.
CardioMEMS was launched into the clinical practice in 2011 by the CHAMPION trial which enrolled 550 patients with chronic HF in NYHA class III with an HF hospitalization within a year prior to enrollment[37]. These patients were randomly assigned to either the treatment group (active monitoring group), in which clinicians used the daily PAP readings on top of standard care, or the control group. After 15 months, patients in the treatment group had a 37% lower risk of HF-related hospitalizations as compared to the control group, respectively. After this initial randomized access period, PAP data became available for all patients, and patients were then followed for a mean period of 13 months[38]. During this period, there was a large reduction of HF admission rates in the former control group compared with the admission rate in the control group [38]. The rate of device-related complications was very low (1%), and the system was proved to be safe. CardioMEMS received the FDA approval in 2014 for patients in NYHA class III and with an HF hospital admission in the previous year[37,38]. A sub analysis of the CHAMPION trial[39] revealed that medication changes were more frequently observed in the active monitoring group than in the control group. Diuretics were frequently adjusted in both groups, but significantly more often in the active monitoring group as well as vasodilators and other heart failure drugs. This data supported the notion that remote hemodynamic monitoring can significantly impact on HF prognosis due to significant change in drug interventions and reduced HF hospitalization rates [38].
A second randomized clinical trial was the GUIDE-HF trial that was conducted during the COVID-10 pandemic and the enrollment phase was low. The trial ended with a neutral result [40]. No significant differences in the primary endpoint (all-cause mortality and total HF events defined as HF hospitalization and urgent HF hospital visit) were detected.
Therefore, considering the previous trial results, the American Heart Guidelines assigned a class of indication 2b for the use of CardioMEMS in selected adult patients with NYHA class III and history of HF hospitalizations in the previous year or elevated natriuretic peptide levels, on maximally tolerated stable doses of medical treatments and optimal device therapy to reduce the risk of subsequent HF hospitalizations [41].
From a European point of view, in 2020, the MEMS-HF study[42], an observational prospective non-randomized study, included patients with chronic HF with NYHA class III and a recent history of HF-related hospitalization. Outcomes included device or system-related complications, sensor failure, quality of life and clinical endpoints such as the annualized HF rate, all-cause mortality rate and PAP changes from baseline [42]. A total of 234 patients had a CardioMEMS sensor implanted. After 12 months, 98.3% of the patients were free from device or system-related complications. During the first six months post-implant, the HF hospitalization rate decreased by 62%. The reduction over the complete 12-month follow-up period was 66%, which was greater than in the CHAMPION trial. On average, the mean PAP decreased by 3.4 mmHg at 6 months, and 5.5 mmHg at 12 months.
The 2021 ESC-HF guidelines stated that devices that involve invasive assessment of hemodynamic parameters have shown a modest improvement in effort capacity and quality of life. Thus, at the present time, the evidence is considered too low to support specific recommendations for these implantable electrical devices[17].
3.2. Cardiac Contractility Modulation
Despite advances in pharmacologic therapies for treating patients with HFrEF, the prognosis of such patients remains poor; therefore, device-based therapy has become increasingly important in recent years for the treatment of HFrEF[43]. The most widely used device-based therapy for the treatment of HFrEF is cardiac resynchronization therapy, which can lead to improved cardiac performance and prognosis in patients with HFrEF and wide QRS (duration > 150 ms)[44]. Unfortunately, only 30% of HFrEF have a QRS duration > 150 ms[45]. For patients with persistent symptoms or frequent HF-related hospitalizations, but with narrow QRS, a new device (Optimizer Smart®) capable of delivering cardiac contractility modulation (CCM) therapy has been available from several years[46].
This device delivers high amplitude non-excitatory biphasic electrical signals during the myocardial refractory period. The CCM implant procedure does not differ from conventional pacemaker implantation, except for placement of two leads in the right ventricle rather than one. The insertion procedure is performed by cephalic or subclavian vein access. The right side is often used since an implantable cardioverter-defibrillator (ICD) is already present in the left side. Two active fixation leads are secured to the right ventricle septum at least 2–3 cm apart from each other, and at least 3 cm from the defibrillation right ventricle lead. The leads are used for sensing ventricular activity and for bipolar delivery of CCM signals. Electrical testing of the leads includes the standard testing for pacemaker leads with a higher focus on the sensing function. Active CCM treatment is generally programmed to be daily delivered for at least 7 hours per day, in equally spaced of one-hour intervals throughout the day. The target treatment is reaching a minimum of 90% CCM therapy delivery. [47,48,49,50,51,52]
Detail features of CCM “pharmacodynamic” were discussed in our previous paper[53]. Briefly, CCM induces both early and late effects on heart. The early effects derive by increasing the phosphorylation state of troponin and myosin binding protein C[54], leading to a positive inotropic effect. In addition, an increase in phosphorylation state of phospholamban[55] and Titin leads to a positive lusitropic effect[49]. The late-onset effects are obtained by reverting maladaptive gene expression [56] involved in the accumulation of dysfunctional fetal proteins [57]. This effect normalizes expression of key sarcoplasmic reticulum genes by down regulating ryanodine receptor 2, sarco-endoplasmic reticulum Ca2+ ATPase and α-MHC. In addition, CCM favours the increase in chaperones transcription (such as HSP70) which in turn prevent aggregation, and accelerate detoxification and disaggregation of misfolded proteins [53].
The final effect of these actions is a reverse in left ventricular pathological remodelling, together with an increase in cardiac performance. HFrEF patients treated with CCM experienced an improvement in functional capacity, quality of life, and a reduced rate of HF-related hospitalizations[47,50].
Potential candidate to CCM treatment include HFrEF patients with the following criteria[58]:
- LVEF ≥ 25% and ≤ 45%.
- NYHA class II and III despite optimal medical treatment.
- QRS duration < 130 ms or not responder to cardiac resynchronization treatment.
- Left ventricular end diastolic diameter < 70 mm.
- Low arrhythmic burden (<8900 premature ventricular complexes in 24 h).
- No acute coronary events in the last three months.
- No recent hospitalizations (in the last month).
- Absence of comorbidities conditioning a life expectancy lower than one year.
In conclusion, CCM is a promising alternative for individuals suffering from HFrEF, and its unique benefits of increasing contractile force without the requirement for more oxygen consumption have the potential to become a cornerstone in the management of this disease.
3.3. Left Bundle Branch Area Pacing
Left bundle branch block is a conduction defect leading to asynchronous ventricular activation. In HFrEF, it may contribute to systolic dysfunction for a lack of mechanical force due to cellular apoptosis, interstitial fibrosis and adverse remodeling [59]. The current device treatments are biventricular pacing, His-bundle pacing, and left bundle branch area pacing (LBBAP). LBBAP represents a more physiological way to pace the conduction system, and may represent a tailored electrophysiological strategy for advanced heart failure.
LBBAP refers to the stimulation of the left bundle branch pacing, the left fascicular pacing, and the left ventricular septal pacing. The former is a selective stimulation of the left branch before ramification, while the second refers to a direct engagement of one of its fascicles and is thereby divided in left anterior fascicular pacing, left mid-septal fascicular pacing, and left posterior fascicular pacing. Lastly, left ventricular septal pacing directly stimulates the septal endocardium of the left ventricle which rapidly carries the impulse to the left branch[60]. In all cases the ventricular catheter is inserted through the interventricular septum on the right side and reaches the sub endocardium on the opposite side. The target zones are identified by some EKG characteristics indicating the correct positioning of the lead tip[60,61]. Studies show that LBBAP, compared to a conventional biventricular resynchronization strategy, seems to reduce QRS duration and pacing thresholds, while improving left ventricular end-diastolic diameter, hospitalizations for HF and LVEF [59]. Other positive effects have been shown in a recent study that showed a reduced incidence in ventricular arrhythmic events and atrial fibrillation [62]. Despite the early positive effects, there are some cases where a diffuse conduction system failure may impair the efficacy of LBBAP. For these rare cases, a new combination has been developed: the so-called LBBAP-optimized cardiac resynchronization therapy. With this technique both a LBBAP and a coronary sinus catheter are implanted and although limited data is available, a study suggests that, compared to classical LBBAP, there is an improvement in terms of QRS duration. A potential application of this technology is for patients for whom biventricular pacing or LBBAP alone are not successful[63].
LBBAP has some limitations. Firstly, by screwing the lead inside the interventricular septum there is an intrinsic risk of septal perforation, coronary laceration, and lead dislodgement. Secondly, the benefits of such therapy in ischemic cardiomyopathy are not clear due to the unique characteristics of infracted tissue and data from long-term applications are still lacking.
3.4. Wearable Cardioverter Defibrillators
Conditions characterized by an elevated risk of fatal arrhythmias for a presumed limited time frame represent a contraindication to an ICD implantation. The most common scenario is the case of a newly HFrEF diagnosis with a severe reduction of LVEF (i.e., ≤30%) i.e., after extensive myocardial infarction or acute myocarditis. Another issue is that patients with an initial severe reduction in LFEV may undergo significant increase in LV function after medical treatment, leaving the original ICD indication. In fact, in the PROLONG trial[64] only 38% of patients kept the original indication at the end of 12-month follow-up compared to the 58% observed after three months.
The current ESC guidelines recommend the implantation of an ICD if a severe impairment of LV function persists for ≥ 3 months on OMT [17]. However, several studies suggested that the optimal duration for the pharmacological treatment to provide a significant improvement in LVEF must be at least 6 months. Thus, during this time frame, there is an increased risk of life-threatening arrhythmic events (roughly 5%) [65]. In these cases, wearable cardioverter defibrillators (WCDs) might represent a valuable bridge. The first multicentric randomized trial conducted by using WCDs was the VEST study [66]. The study was performed in ischemic cardiomyopathy patients and WCDs did not demonstrate an effective role in reducing the rate of arrhythmic death. However, only 25% of death patients wore the WCD at the time of death and the daily wearing time in the VEST trial was below 20 hours per day. Thus, WCD compliance by patients is a potential issue that impair its efficacy. In the WEARIT-France study[67], patients wore WCD for a longer time (23.4 hours a day), and the device proved its efficacy and safety showing that 1.6% of participants experiencing at least one appropriate shock.
Finally, the SAVE-ICD study[65] showed that HF of an ischemic aetiology was less prone to significant improvements because the scar tissue does not possess a contractile potential and cannot contribute to the overall systolic function. The lower probability of a significant left ventricular improvement after a large anterior myocardial infarction should be considered when a WCD is considered instead of a definitive ICD [17].
WCD also has telemonitoring abilities that allow for checking additional parameters such as physical activity and heart rate, thus providing further information regarding patient condition [68] [69]. In conclusion, current literature reinforces the use of an extensive application of WCDs in clinical practice for patients at risk of ventricular arrhythmias with temporary contraindications to a definitive ICD implantation.
3.5. Ultrafiltration for Acute Decompensated HF
Fluid overload is the most common reason for hospitalization in HFrEF patients[70]. Fluid overload manifests as systemic congestion such as pulmonary oedema and swollen legs.
It also leads to changes at cellular level causing systemic endothelial dysfunction and exaggerated inflammatory response that contributes to renal impairment, reduced absorptive capacity of bowel, and hepatic dysfunction [71]. As a result, an early and fast removal of fluid overload constitutes one of the key treatment goals of acute decompensated HF.
Loop diuretics are the first-line treatment for fluid overload.
Unfortunately, loop diuretics lose their efficacy as the disease progresses determining the so-called diuretic resistance state[72], which is associated with a worse prognosis[72]. The processes behind diuretic resistance are multiple: reduced intestinal absorption, decreased renal blood flow associated with renal venous congestion, and neurohormonal activation. In the clinical setting the diuretic resistance results in insufficient congestion relief and a substantial increase in rehospitalization rates [73].
Different strategies can be employed to overcome diuretic resistance such as up-titration of diuretic dose, intravenous continuous infusion, sequential nephron blockade[74]. Unfortunately, these strategies carry a high rate of failure especially in the end stage of HFrEF [75].
In this setting, the mechanical removal of fluid overload by extracorporeal ultrafiltration (UF) is a valuable option.
UF enables the removal of isotonic plasma water from the blood by the application of hydrostatic pressure gradient that is generated by a pump through a semipermeable membrane (haemofilter) [76]. This process leads to the “intra-vascular refill” phenomenon in which the fluid removed from the blood is constantly replaced by fluid absorbed from the third space. The final effect is a negative water balance and finally a gradual fluid overload resolution.
The fluid removal by UF showed some advantages compared with the one achieved by diuretics. First, UF allowed the removal of a greater quantity of sodium compared with hypotonic urine induced by diuretics [77]. Second, by using UF the clinician can choose the amount of fluid to remove, while it is unpredictable when diuretics are used. This aspect could be of immense importance especially in patients with labile hemodynamic stability. Lastly, UF does not create neuro-hormonal activation conversely to diuretics, unless fluid removal exceeds plasma refilling [78] (Table 3).
The main advantage of UF is that it allows a modifiable ultrafiltration rate, ranging from very low to high rate (up to 500 mL/h) based on patient hemodynamic tolerance [76]. Thus, it can also be carried in hypotensive patients with minimal hemodynamic impact.
The first observations on UF in fluid overload of congestive HFrEF patients were developed between 1993 and 2005. However, the first randomized controlled clinical trial was the Ultrafiltration versus Intravenous Diuretics for Patients Hospitalized for Acute Decompensated Heart Failure (UN-LOAD) trial published in 2007. This trial showed that patients treated with UF experienced significantly greater weight loss and decongestion compared to those who were treated with diuretics[79]. Furthermore, the UF group showed a longer rehospitalization free interval during the 3-month follow-up period.
On the contrary, in the Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARRESS-HF) trial, patients in the UF group did not achieve greater weight loss[80]. Some issues were raised about the design of the trial, since in the pharmacological therapy arm the diuretic dose underwent adjustment based on patient response, while the rate of UF was delivered uniformly at 200 mL/h. Nevertheless, there was not a significant difference in the two groups for mortality during the 2-month follow-up [80].
The Aquapheresis Versus Intravenous Diuretics and Hospitalization for Heart Failure (AVOID-HF) trial [81] compared early adjustable UF therapy and diuretics. Weight loss was greater in the UF group than in the diuretic arm, while the impact of renal function was neutral. Patients in the UF arm showed a hospitalization free interval greater than the patients in the diuretic group within 3 months after discharge.
Several studies and meta-analyses [82] have confirmed the role of UF therapy on a more efficient weight loss and fluid removal compared with diuretic therapy. In addition, UF was shown to be superior in reducing the rate of HF rehospitalisation, while there was no significant difference in mortality or incidence of adverse events.
4. Conclusions
HFrEF is becoming a frequent condition that significantly impacts both patient quality of life and survival. It also significantly impacts health system resource. In the last decade, new medical treatments and devices have been developed to reduce HF hospitalizations, improve management, and reduce the overall rate of mortality.
At the current time, physicians have different drugs that need to be started and up-titrated. Different strategies have been proposed to select which drug should be prescribed first.
Different devices can identify early signs of upcoming HF in asymptomatic patients or treat life threating conditions (arrhythmia or fluid retention) for a limited time frame.
This review article gives the readers a comprehensive view of the most recent and important findings that need to be considered when a HFrEF patiet is encountered.
5. Future Directions
Current approach to HF is still full of many promising avenues that are being explored and could significantly shape the future of our diagnostic and therapeutic approaches. One notable focus is the investigation of novel pharmacological therapies and biomarkers, offering potential advancements beyond current standards[83].
Among experimental pharmacological therapies, a class of novel agents targeting cardiac function, such as omecamtiv mecarbil, shows considerable promise[84]. Omecamtiv mecarbil, a selective cardiac myosin activator, enhances myocardial contractility without increasing intracellular calcium levels, offering a unique approach to improving cardiac performance[85]. Early clinical trials have demonstrated its potential to improve symptoms and functional status in HF patients, making it a compelling candidate for phase III trials more directed to hard cardiovascular endpoints[86].
In the realm of biomarkers, emerging candidates like soluble suppression of tumorigenicity 2 (sST2) and galectin-3 are gaining attention for their prognostic utility in HF[87]. These markers offer insights into the underlying pathophysiology and aid in risk stratification, enabling personalized treatment strategies. Furthermore, ongoing research is exploring the potential of microRNAs as diagnostic and prognostic indicators, offering a glimpse into the molecular mechanisms underlying heart failure progression [88].
While these therapies and biomarkers are not yet endorsed by regulating authorities, their promising results in preclinical and early clinical studies suggest they could play significant roles in shaping the future landscape of HF management within the next five years.
In addition to pharmacological therapies and biomarkers, the integration of artificial intelligence (AI) into HF diagnostic models holds significant promise for the future of HF management. AI-based algorithms, particularly machine learning and deep learning techniques are being leveraged to analyze complex datasets, including electronic health records, medical imaging, and genetic information, to identify patterns and predict heart failure outcomes[89]. These AI-driven diagnostic models have the potential to enhance early detection and risk stratification, ultimately leading to improved clinical outcomes and resource allocation within healthcare systems.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ziaeian, B.; Fonarow, G.C. Epidemiology and aetiology of heart failure. Nat Rev Cardiol 2016, 13, 368–78. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.; Rassekh, N.; Fonarow, G.C.; et al. Guideline-Directed Medical Therapy for the Treatment of Heart Failure with Reduced Ejection Fraction. Drugs 2023, 83, 747–59. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Rev Esp Cardiol 2016, 69, 1167. [Google Scholar] [PubMed]
- Cowie, M.R.; Fisher, M. SGLT2 inhibitors: mechanisms of cardiovascular benefit beyond glycaemic control. Nat Rev Cardiol 2020, 17, 761–72. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, S.; Seufert, J.; Scheen, A.; et al. Dapagliflozin in patients with type 2 diabetes mellitus: A pooled analysis of safety data from phase IIb/III clinical trials. Diabetes Obes Metab 2018, 20, 620–8. [Google Scholar] [CrossRef] [PubMed]
- Pabel, S.; Hamdani, N.; Luedde, M.; et al. SGLT2 Inhibitors and Their Mode of Action in Heart Failure-Has the Mystery Been Unravelled? Curr Heart Fail Rep 2021, 18, 315–28. [Google Scholar] [CrossRef] [PubMed]
- Pabel, S.; Wagner, S.; Bollenberg, H.; et al. Empagliflozin directly improves diastolic function in human heart failure. Eur J Heart Fail 2018, 20, 1690–700. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Atkin, S.L.; Butler, A.E.; et al. Sodium-glucose cotransporter inhibitors and oxidative stress: An update. J Cell Physiol 2019, 234, 3231–7. [Google Scholar] [CrossRef]
- Ye, Y.; Bajaj, M.; Yang, H.C.; et al. SGLT-2 Inhibition with Dapagliflozin Reduces the Activation of the Nlrp3/ASC Inflammasome and Attenuates the Development of Diabetic Cardiomyopathy in Mice with Type 2 Diabetes. Further Augmentation of the Effects with Saxagliptin, a DPP4 Inhibitor. Cardiovasc Drugs Ther 2017, 31, 119–32. [Google Scholar] [CrossRef]
- Yurista, S.R.; Sillje, H.H.W.; Oberdorf-Maass, S.U.; et al. Sodium-glucose co-transporter 2 inhibition with empagliflozin improves cardiac function in non-diabetic rats with left ventricular dysfunction after myocardial infarction. Eur J Heart Fail 2019, 21, 862–73. [Google Scholar] [CrossRef]
- Cherney, D.Z.; Perkins, B.A.; Soleymanlou, N.; et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation 2014, 129, 587–97. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015, 373, 2117–28. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med 2017, 377, 2099. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2019, 380, 347–57. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N Engl J Med 2020, 383, 1413–24. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021, 42, 3599–726. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2022, 79, 1757–80. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.; Usman, M.S.; Anstrom, K.J.; et al. Soluble guanylate cyclase stimulators in patients with heart failure with reduced ejection fraction across the risk spectrum. Eur J Heart Fail 2022, 24, 2029–36. [Google Scholar] [CrossRef]
- Gonzalez-Juanatey, J.R.; Anguita-Sanchez, M.; Bayes-Genis, A.; et al. Vericiguat in heart failure: From scientific evidence to clinical practice. Rev Clin Esp (Barc) 2022, 222, 359–69. [Google Scholar] [CrossRef]
- Rao, V.N.; Diez, J.; Gustafsson, F.; et al. Practical Patient Care Considerations With Use of Vericiguat After Worsening Heart Failure Events. J Card Fail 2023, 29, 389–402. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, M.E.; Ayalasomayajula, S.; Blaustein, R.O.; et al. Vericiguat, a novel sGC stimulator: Mechanism of action, clinical, and translational science. Clin Transl Sci 2023, 16, 2458–66. [Google Scholar] [CrossRef] [PubMed]
- Sahana, U.; Wehland, M.; Simonsen, U.; et al. A Systematic Review of the Effect of Vericiguat on Patients with Heart Failure. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Armstrong, P.W.; Pieske, B.; Anstrom, K.J.; et al. Vericiguat in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2020, 382, 1883–93. [Google Scholar] [CrossRef] [PubMed]
- Pieske, B.; Pieske-Kraigher, E.; Lam, C.S.P.; et al. Effect of vericiguat on left ventricular structure and function in patients with heart failure with reduced ejection fraction: The VICTORIA echocardiographic substudy. Eur J Heart Fail 2023, 25, 1012–21. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; et al. Corrigendum to: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2021, 42, 4901. [Google Scholar]
- Gheorghiade, M.; Shah, A.N.; Vaduganathan, M.; et al. Recognizing hospitalized heart failure as an entity and developing new therapies to improve outcomes: academics', clinicians', industry's, regulators', and payers' perspectives. Heart Fail Clin 2013, 9, 285–90, v. [Google Scholar] [CrossRef]
- Swedberg, K.; Komajda, M.; Bohm, M.; et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet 2010, 376, 875–85. [Google Scholar] [CrossRef]
- Bauersachs, J. Heart failure drug treatment: the fantastic four. Eur Heart J 2021, 42, 681–3. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Packer, M. How Should We Sequence the Treatments for Heart Failure and a Reduced Ejection Fraction?: A Redefinition of Evidence-Based Medicine. Circulation 2021, 143, 875–7. [Google Scholar] [CrossRef]
- Rosano, G.M.C.; Moura, B.; Metra, M.; et al. Patient profiling in heart failure for tailoring medical therapy. A consensus document of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2021, 23, 872–81. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.R.; Roalfe, A.K.; Adoki, I.; et al. Survival of patients with chronic heart failure in the community: a systematic review and meta-analysis. Eur J Heart Fail 2019, 21, 1306–25. [Google Scholar] [CrossRef] [PubMed]
- Pour-Ghaz, I.; Hana, D.; Raja, J.; et al. CardioMEMS: where we are and where can we go? Ann Transl Med 2019, 7, 418. [Google Scholar] [CrossRef]
- Linden, R.J. Atrial reflexes and renal function. Am J Cardiol 1979, 44, 879–83. [Google Scholar] [CrossRef] [PubMed]
- Dibner-Dunlap, M.E.; Thames, M.D. Control of sympathetic nerve activity by vagal mechanoreflexes is blunted in heart failure. Circulation 1992, 86, 1929–34. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M.; Magri, P.; Rao, M.A.; et al. Intrarenal determinants of sodium retention in mild heart failure: effects of angiotensin-converting enzyme inhibition. Hypertension 1997, 30, 168–76. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet 2011, 377, 658–66. [Google Scholar] [CrossRef]
- Abraham, W.T.; Stevenson, L.W.; Bourge, R.C.; et al. Sustained efficacy of pulmonary artery pressure to guide adjustment of chronic heart failure therapy: complete follow-up results from the CHAMPION randomised trial. Lancet 2016, 387, 453–61. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Stevenson, L.W.; Adamson, P.B.; et al. Interventions Linked to Decreased Heart Failure Hospitalizations During Ambulatory Pulmonary Artery Pressure Monitoring. JACC Heart Fail 2016, 4, 333–44. [Google Scholar] [CrossRef]
- Lindenfeld, J.; Zile, M.R.; Desai, A.S.; et al. Haemodynamic-guided management of heart failure (GUIDE-HF): a randomised controlled trial. Lancet 2021, 398, 991–1001. [Google Scholar] [CrossRef]
- 41. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J Card Fail 2022, 28, e1–e167. [CrossRef]
- Angermann, C.E.; Assmus, B.; Anker, S.D.; et al. Pulmonary artery pressure-guided therapy in ambulatory patients with symptomatic heart failure: the CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF). Eur J Heart Fail 2020, 22, 1891–901. [Google Scholar] [CrossRef] [PubMed]
- Komajda, M.; Bohm, M.; Borer, J.S.; et al. Incremental benefit of drug therapies for chronic heart failure with reduced ejection fraction: a network meta-analysis. Eur J Heart Fail 2018, 20, 1315–22. [Google Scholar] [CrossRef] [PubMed]
- Moskovitch, J.; Voskoboinik, A. Cardiac resynchronization therapy: a comprehensive review. Minerva Med 2019, 110, 121–38. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T. Cardiac Resynchronization Therapy and Cardiac Contractility Modulation in Patients with Advanced Heart Failure: How to Select the Right Candidate? Heart Fail Clin 2021, 17, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Campbell, C.M.; Kahwash, R.; Abraham, W.T. Optimizer Smart in the treatment of moderate-to-severe chronic heart failure. Future Cardiol 2020, 16, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Cappannoli, L.; Scacciavillani, R.; Rocco, E.; et al. Cardiac contractility modulation for patient with refractory heart failure: an updated evidence-based review. Heart Fail Rev 2021, 26, 227–35. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Borggrefe, M.; Neuser, H.; et al. Cardiac contractility modulation improves long-term survival and hospitalizations in heart failure with reduced ejection fraction. Eur J Heart Fail 2019, 21, 1103–13. [Google Scholar] [CrossRef] [PubMed]
- Tschope, C.; Van Linthout, S.; Spillmann, F.; et al. Cardiac contractility modulation signals improve exercise intolerance and maladaptive regulation of cardiac key proteins for systolic and diastolic function in HFpEF. Int J Cardiol 2016, 203, 1061–6. [Google Scholar] [CrossRef]
- Lyon, A.R.; Samara, M.A.; Feldman, D.S. Cardiac contractility modulation therapy in advanced systolic heart failure. Nat Rev Cardiol 2013, 10, 584–98. [Google Scholar] [CrossRef]
- Kuschyk, J.; Nagele, H.; Heinz-Kuck, K.; et al. Cardiac contractility modulation treatment in patients with symptomatic heart failure despite optimal medical therapy and cardiac resynchronization therapy (CRT). Int J Cardiol 2019, 277, 173–7. [Google Scholar] [CrossRef] [PubMed]
- Tint, D.; Florea, R.; Micu, S. New Generation Cardiac Contractility Modulation Device-Filling the Gap in Heart Failure Treatment. J Clin Med 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Marchese, P.; Gennaro, F.; Mazzotta, G. Cardiac Contractility Modulation Therapy in Patients with Amyloid Cardiomyopathy and Heart Failure, Case Report, Review of the Biophysics of CCM Function, and AMY-CCM Registry Presentation. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Tschope, C.; Kherad, B.; Klein, O.; et al. Cardiac contractility modulation: mechanisms of action in heart failure with reduced ejection fraction and beyond. Eur J Heart Fail 2019, 21, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Imai, M.; Rastogi, S.; Gupta, R.C.; et al. Therapy with cardiac contractility modulation electrical signals improves left ventricular function and remodeling in dogs with chronic heart failure. J Am Coll Cardiol 2007, 49, 2120–8. [Google Scholar] [CrossRef] [PubMed]
- Rajabi, M.; Kassiotis, C.; Razeghi, P.; et al. Return to the fetal gene program protects the stressed heart: a strong hypothesis. Heart Fail Rev 2007, 12, 331–43. [Google Scholar] [CrossRef] [PubMed]
- Blank, M.; Goodman, R. A mechanism for stimulation of biosynthesis by electromagnetic fields: charge transfer in DNA and base pair separation. J Cell Physiol 2008, 214, 20–6. [Google Scholar] [CrossRef]
- Li, Z.; Liu, Q.; Zhou, S.; et al. Enhancing myocardial function with cardiac contractility modulation: potential and challenges. ESC Heart Fail 2024, 11, 1–12. [Google Scholar] [CrossRef]
- Yousaf, A.; Ahmad, S.; Peltz, J.; et al. Left bundle branch area pacing vs biventricular pacing for cardiac resynchronization: A systematic review and meta-analysis. Heart Rhythm O2 2023, 4, 671–80. [Google Scholar] [CrossRef]
- Burri, H.; Jastrzebski, M.; Cano, O.; et al. EHRA clinical consensus statement on conduction system pacing implantation: executive summary. Endorsed by the Asia-Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS) and Latin-American Heart Rhythm Society (LAHRS). Europace 2023, 25, 1237–48. [Google Scholar] [CrossRef]
- Li, M.; Li, C.; Li, J.; et al. An individualized criterion for left bundle branch capture in patients with a narrow QRS complex. Heart Rhythm 2024, 21, 294–300. [Google Scholar] [CrossRef]
- Herweg, B.; Sharma, P.S.; Cano, O.; et al. Arrhythmic Risk in Biventricular Pacing Compared With Left Bundle Branch Area Pacing: Results From the I-CLAS Study. Circulation 2024, 149, 379–90. [Google Scholar] [CrossRef]
- Vijayaraman, P. Left Bundle Branch Pacing Optimized Cardiac Resynchronization Therapy: A Novel Approach. JACC Clin Electrophysiol 2021, 7, 1076–8. [Google Scholar] [CrossRef]
- Duncker, D.; Konig, T.; Hohmann, S. Avoiding Untimely Implantable Cardioverter/Defibrillator Implantation by Intensified Heart Failure Therapy Optimization Supported by the Wearable Cardioverter/Defibrillator-The PROLONG Study. J Am Heart Assoc 2017, 6. [Google Scholar] [CrossRef]
- Guerra, F.; Ammendola, E.; Ziacchi, M.; et al. Effect of SAcubitril/Valsartan on left vEntricular ejection fraction and on the potential indication for Implantable Cardioverter Defibrillator in primary prevention: the SAVE-ICD study. Eur J Clin Pharmacol 2021, 77, 1835–42. [Google Scholar] [CrossRef] [PubMed]
- Olgin, J.E.; Pletcher, M.J.; Vittinghoff, E.; et al. Wearable Cardioverter-Defibrillator after Myocardial Infarction. N Engl J Med 2018, 379, 1205–15. [Google Scholar] [CrossRef] [PubMed]
- Garcia, R.; Combes, N.; Defaye, P.; et al. Wearable cardioverter-defibrillator in patients with a transient risk of sudden cardiac death: the WEARIT-France cohort study. Europace 2021, 23, 73–81. [Google Scholar] [CrossRef]
- Iliodromitis, K.; Balogh, Z.; Triposkiadis, F.; et al. Assessing physical activity with the wearable cardioverter defibrillator in patients with newly diagnosed heart failure. Front Cardiovasc Med 2023, 10, 1176710. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.; D'Onofrio, A.; De Ruvo, E.; et al. Decongestive treatment adjustments in heart failure patients remotely monitored with a multiparametric implantable defibrillators algorithm. Clin Cardiol 2022, 45, 670–8. [Google Scholar] [CrossRef]
- Munir, M.B.; Sharbaugh, M.S.; Thoma, F.W.; et al. Trends in hospitalization for congestive heart failure, 1996-2009. Clin Cardiol 2017, 40, 109–19. [Google Scholar] [CrossRef]
- Colombo, P.C.; Onat, D.; Harxhi, A.; et al. Peripheral venous congestion causes inflammation, neurohormonal, and endothelial cell activation. Eur Heart J 2014, 35, 448–54. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Testani, J.; Collins, S. Diuretic Resistance in Heart Failure. Curr Heart Fail Rep 2019, 16, 57–66. [Google Scholar] [CrossRef]
- Voors, A.A.; Davison, B.A.; Teerlink, J.R.; et al. Diuretic response in patients with acute decompensated heart failure: characteristics and clinical outcome--an analysis from RELAX-AHF. Eur J Heart Fail 2014, 16, 1230–40. [Google Scholar] [CrossRef] [PubMed]
- Kazory, A.; Elkayam, U. Cardiorenal interactions in acute decompensated heart failure: contemporary concepts facing emerging controversies. J Card Fail 2014, 20, 1004–11. [Google Scholar] [CrossRef] [PubMed]
- Peacock, W.F.; Costanzo, M.R.; De Marco, T.; et al. Impact of intravenous loop diuretics on outcomes of patients hospitalized with acute decompensated heart failure: insights from the ADHERE registry. Cardiology 2009, 113, 12–9. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Jessup, M. Treatment of congestion in heart failure with diuretics and extracorporeal therapies: effects on symptoms, renal function, and prognosis. Heart Fail Rev 2012, 17, 313–24. [Google Scholar] [CrossRef] [PubMed]
- Kazory, A. Cardiorenal syndrome: ultrafiltration therapy for heart failure--trials and tribulations. Clin J Am Soc Nephrol 2013, 8, 1816–28. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Lauri, G.; Grazi, M.; et al. Circulatory response to fluid overload removal by extracorporeal ultrafiltration in refractory congestive heart failure. J Am Coll Cardiol 2001, 38, 963–8. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Guglin, M.E.; Saltzberg, M.T.; et al. Ultrafiltration versus intravenous diuretics for patients hospitalized for acute decompensated heart failure. J Am Coll Cardiol 2007, 49, 675–83. [Google Scholar] [CrossRef]
- Bart, B.A.; Goldsmith, S.R.; Lee, K.L.; et al. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. N Engl J Med 2012, 367, 2296–304. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Negoianu, D.; Jaski, B.E.; et al. Aquapheresis Versus Intravenous Diuretics and Hospitalizations for Heart Failure. JACC Heart Fail 2016, 4, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Agrawal, N.; Kazory, A. Defining the role of ultrafiltration therapy in acute heart failure: a systematic review and meta-analysis. Heart Fail Rev 2016, 21, 611–9. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; De Ponti, R.; Guerra, F.; et al. Sinergy between drugs and devices in the fight against sudden cardiac death and heart failure. Eur J Prev Cardiol 2021, 28, 110–23. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Diaz, R.; Felker, G.M.; et al. Omecamtiv Mecarbil in Chronic Heart Failure With Reduced Ejection Fraction: Rationale and Design of GALACTIC-HF. JACC Heart Fail 2020, 8, 329–40. [Google Scholar] [CrossRef] [PubMed]
- Malik, F.I.; Hartman, J.J.; Elias, K.A.; et al. Cardiac myosin activation: a potential therapeutic approach for systolic heart failure. Science 2011, 331, 1439–43. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Felker, G.M.; McMurray, J.J.; et al. Chronic Oral Study of Myosin Activation to Increase Contractility in Heart Failure (COSMIC-HF): a phase 2, pharmacokinetic, randomised, placebo-controlled trial. Lancet 2016, 388, 2895–903. [Google Scholar] [CrossRef] [PubMed]
- Bayes-Genis, A.; Voors, A.A.; Zannad, F.; et al. Transitioning from usual care to biomarker-based personalized and precision medicine in heart failure: call for action. Eur Heart J 2018, 39, 2793–9. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.K.; Zhu, J.Q.; Zhang, J.T.; et al. Circulating microRNA: a novel potential biomarker for early diagnosis of acute myocardial infarction in humans. Eur Heart J 2010, 31, 659–66. [Google Scholar] [CrossRef]
- Jajcay, N.; Bezak, B.; Segev, A.; et al. Data processing pipeline for cardiogenic shock prediction using machine learning. Front Cardiovasc Med 2023, 10, 1132680. [Google Scholar] [CrossRef]
Figure 1.
Vericiguat dose modifications according to VICTORIA trial protocol.
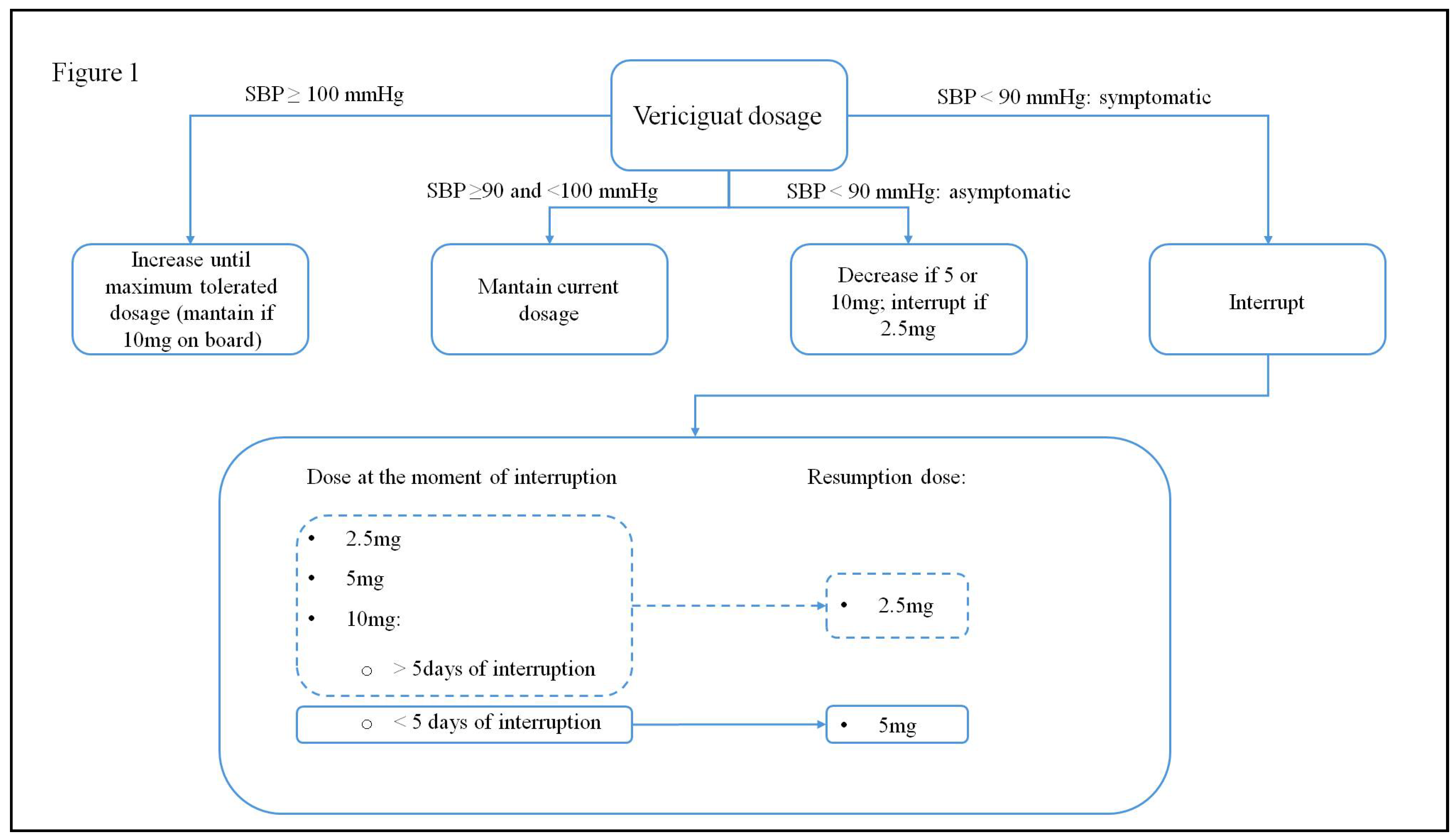
Figure 2.
Conventional sequencing add-on therapy for patient with HFrEF.
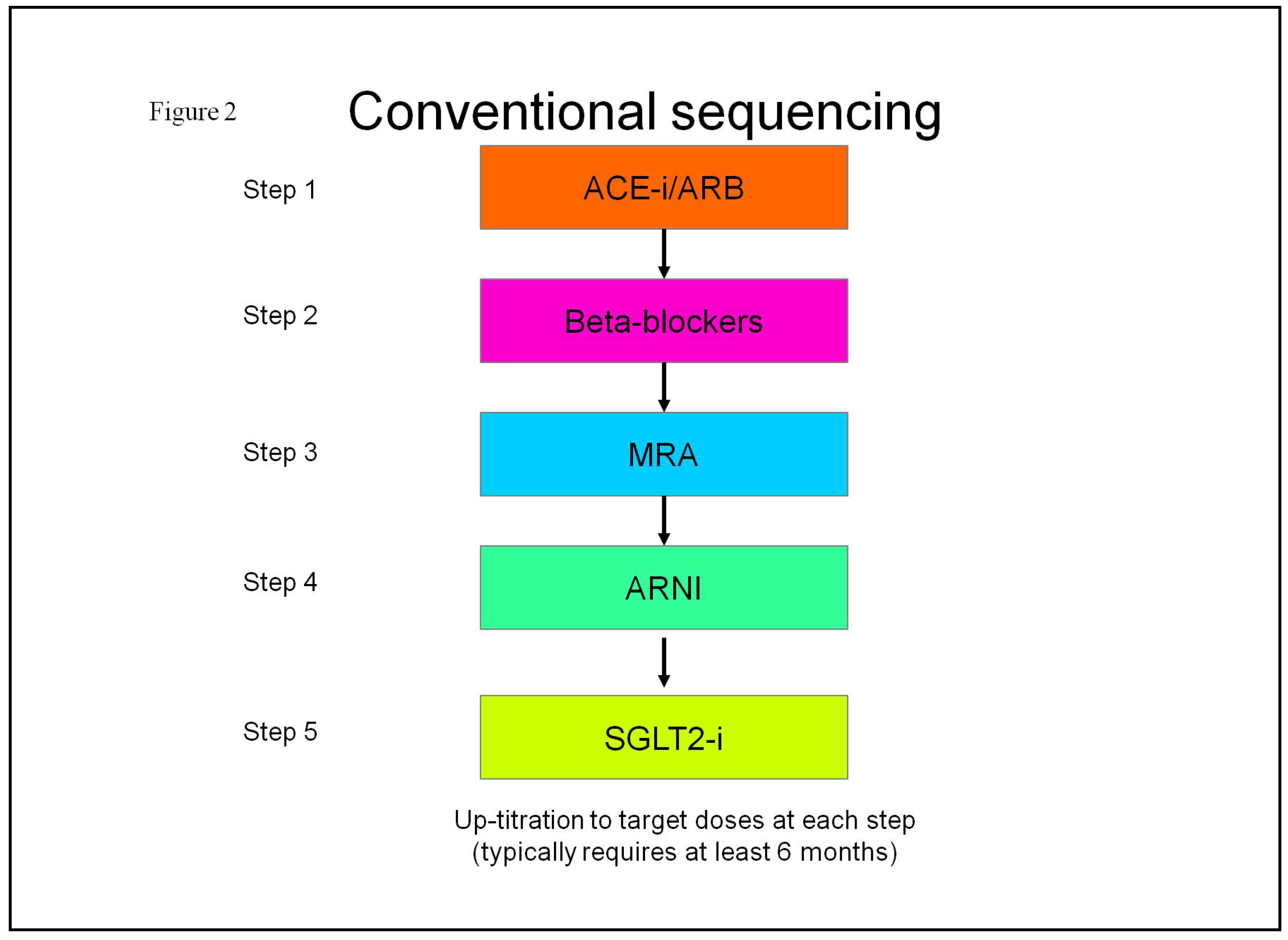
Figure 3.
New sequencing add-on therapy for patient with HFrEF.
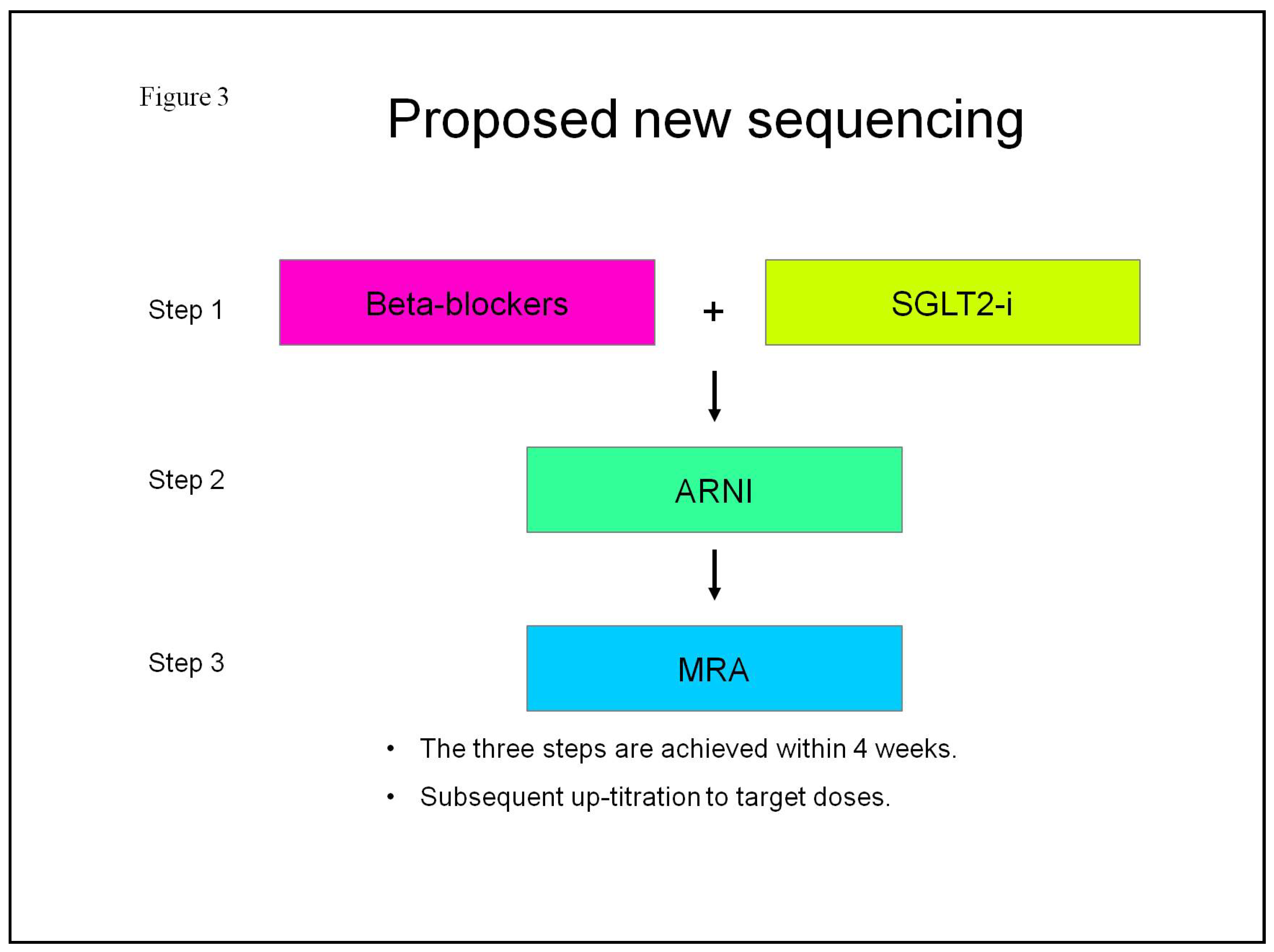
Figure 4.
The tailored strategy depending on patient clinical features.
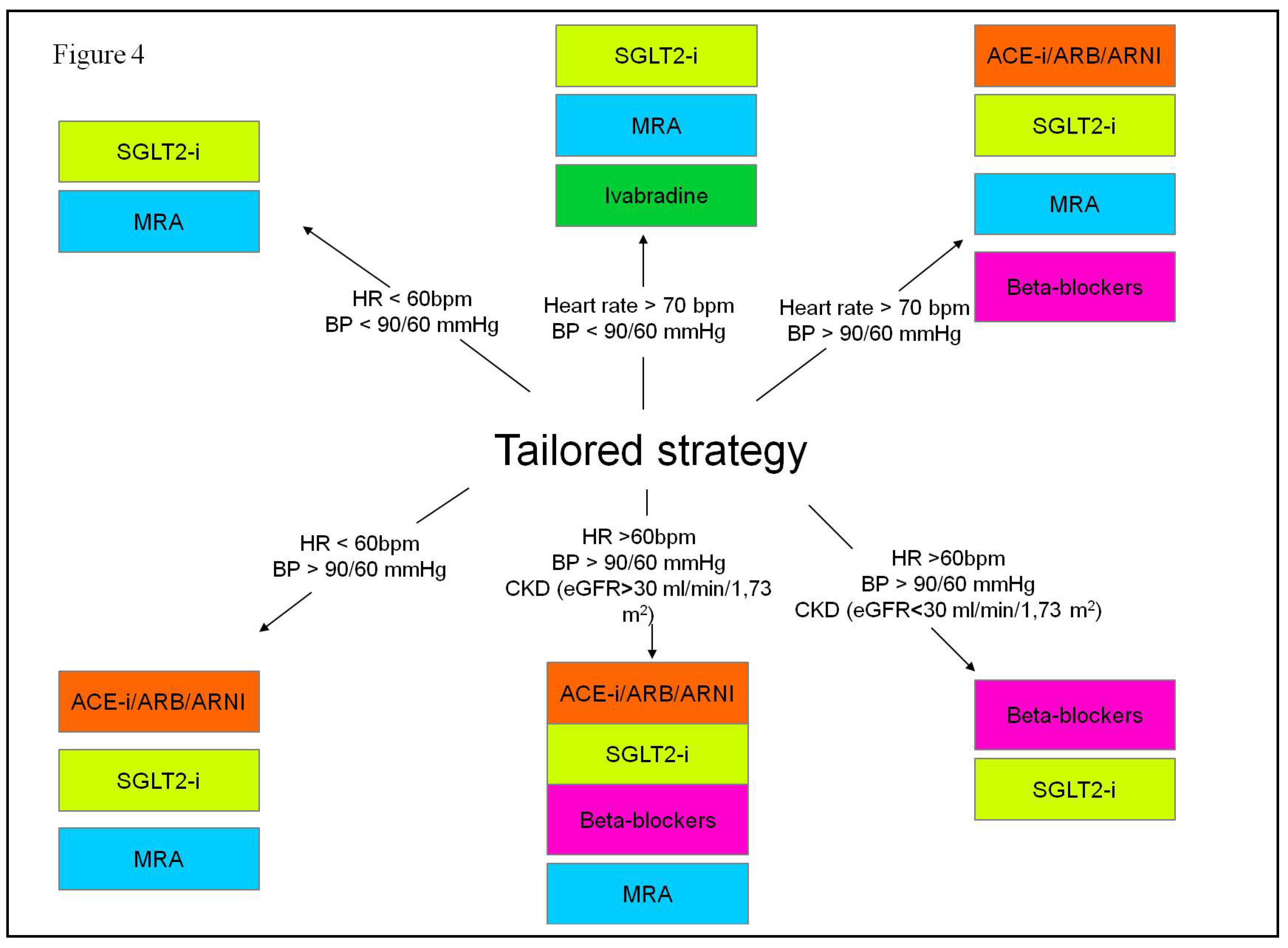
Figure 5.
Physiological activation of neurohormonal systems in healthy individuals.
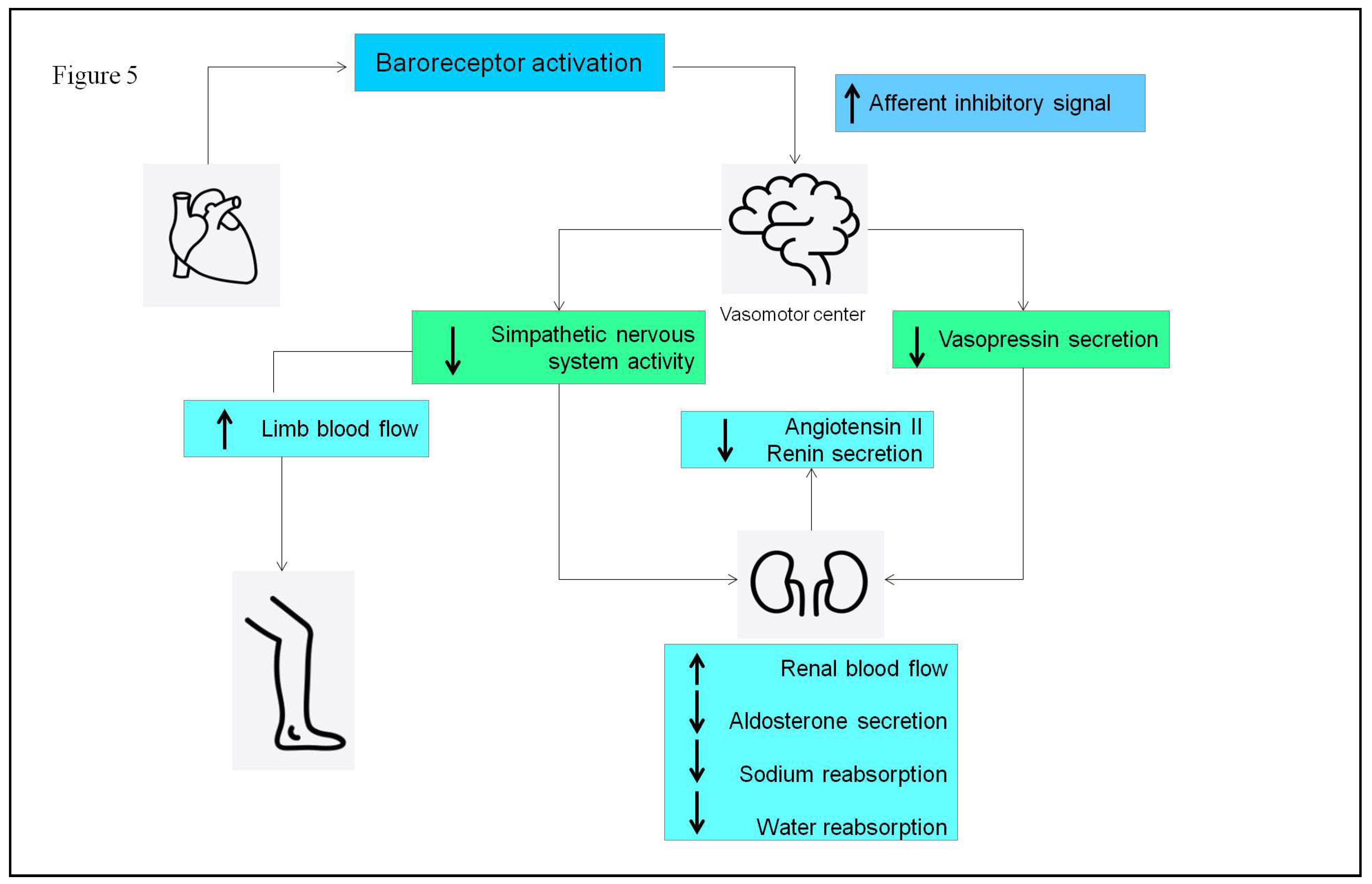
Figure 6.
Pathological activation of neurohormonal systems in HFrEF patients.
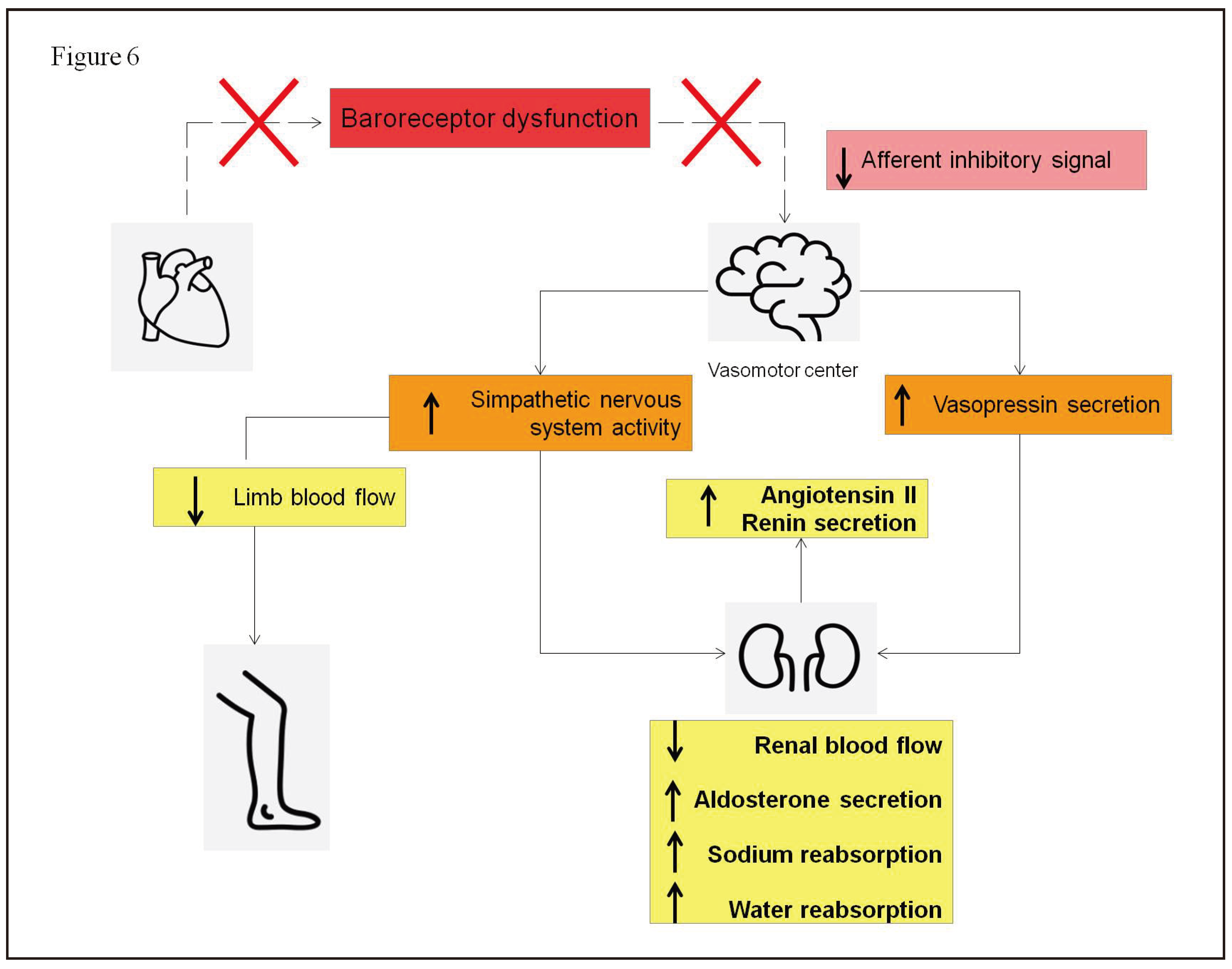

Table 1.
SGLT2-inhibitors approved for HFrEF: main features.
| SGLT2-i molecules | Dosage | Frequency | Contraindications | Side effects |
|---|---|---|---|---|
| Dapagliflozin | 10 mg | once daily | • Kidney failure (eGFR < 30 mL/min/1.73m2) • History of serious hypersensitivity reaction to drug • Pregnancy or breastfeeding • On dialysis |
• Genital fungal infections • Urinary tract infections • Euglycemic diabetic ketoacidosis • Dehydration and hypotension • Hypoglycemia when used with insulin or sulfonylurea • Lower limb ulcerations and soft tissue infections • Dyslipidemia |
| Empagliflozin | 10 mg | once daily | • Kidney failure (eGFR < 20 mL/min/1.73m2) • History of serious hypersensitivity reaction to drug • Pregnancy or breastfeeding • On dialysis |
• Genital fungal infections • Urinary tract infections • Euglycemic diabetic ketoacidosis • Dehydration and hypotension • Hypoglycemia when used with insulin or sulfonylurea • Lower limb ulcerations and soft tissue infections • Dyslipidemia |
eGFR: estimated Glomerular Filtration Rate.
Table 2.
Principal drugs used in HFrEF patients with their starting dose and target dose.
| Starting dose | Target dose | |
|---|---|---|
| ACE-i | ||
| Ramipril | 2.5 mg b.i.d. | 5 mg b.i.d. |
| Enalapril | 2.5 mg b.i.d. | 10-20 mg b.i.d. |
| Lisinopril | 2.5-5 mg o.d. | 20-35 mg o.d. |
| ARB | ||
| Valsartan | 40 mg b.i.d. | 160 mg b.i.d. |
| Candesartan | 4 mg o.d. | 32 mg o.d. |
| Losartan | 50 mg o.d. | 150 mg o.d. |
| ARNI | ||
| Sacubitril/Valsartan | 24/26 mg b.i.d. | 97/103 mg b.i.d. |
| MRA | ||
| Spironolactone | 25 mg o.d. | 50 mg o.d. |
| Eplerenone | 25 mg o.d. | 50 mg o.d. |
| Beta-blockers | ||
| Bisoprolol | 1.25 mg o.d. | 10 mg o.d. |
| Nebivolol | 1.25 mg o.d. | 10 mg o.d. |
| Carvedilol | 3.125 mg b.i.d. | 25 mg b.i.d. |
| SGLT2-i | ||
| Dapagliflozin | 10 mg o.d. | 10 mg o.d. |
| Empagliflozin | 10 mg o.d. | 10 mg o.d. |
| Other agents | ||
| Vericiguat | 2.5 mg o.d. | 10 mg o.d. |
| Ivabradine | 5 mg b.i.d. | 7.5 mg b.i.d. |
O.d.: once daily; b.i.d.: bis in die.
Table 3.
Comparative differences between loop diuretics and extracorporeal ultrafiltration.
| Loop diuretics | Extracorporeal Ultrafiltration | |
|---|---|---|
| Neurohormonal activation | Direct neurohormonal activation | No direct neurohormonal activation |
| Removal | Elimination of hypotonic urine | Removal of isotonic plasma water |
| Control of fluid and waste removal | Unpredictable elimination of sodium and water | Precise control of rate and amount of fluid removal |
| Effect on renal function | Development of diuretic agent resistance with prolonged administration | Restoration of diuretic agent responsiveness |
| Effect of plasma components | Risk of hypokalemia and hypomagnesemia | No effect on plasma concentration of potassium and magnesium |
| Anticoagulation | No need for anticoagulation | Need for anticoagulation |
| Extracorporeal circuit | No extracorporeal circuit | Need for extracorporeal circuit |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



