
Submitted:
30 March 2024
Posted:
02 April 2024
You are already at the latest version
Abstract
Severe cancer pain significantly diminishes patients' quality of life, leading to increased reliance on caregivers. Although opioid analgesics are effective, they may induce opioid-induced bowel dysfunction (OIBD) with symptoms such as nausea, vomiting, drowsiness, and constipation. While controlled-release oxycodone is a viable option, its prolonged use can lead to opi-oid-induced constipation (OIC). Addressing this, a relative novel formulation - a fixed 2:1 ratio of oxycodone and naloxone in prolonged release - aims to provide analgesia while alleviating OIC. This review critically assesses the evidence on the efficacy, safety, and patient experience of ox-ycodone/naloxone prolonged release in managing severe cancer pain, emphasizing the necessity for a targeted approach in this patient population.
Keywords:
severe cancer pain
; oxycodone/naloxone
; pain management
1. Introduction
Cancer is a widespread disease affecting millions of patients globally, resulting in physical, emotional, and psychological distress [1]. Despite recent investigations indicating a decrease in both the prevalence and severity of cancer pain, nearly half of all cancer patients still experiences pain [2]. Effectively managing severe pain poses a significant challenge, as it can substantially impact the patient’s quality of life, resulting in higher dependency on caregivers [3]. Relief from pain can be achieved through various medications, with opioid analgesics considered the gold standard for treating severe cancer pain [1]. Nevertheless, opioids can cause some significant side effects named Opioid-induced bowel dysfunction (OIBD), which may include nausea, vomiting, drowsiness, and constipation. In the last decades, the introduction of controlled-release oxycodone has emerged as an effective option for controlling severe cancer-related pain [2]. However, like other opioids, prolonged oxycodone use may be associated with abdominal adverse events such as opioid-induced constipation (OIC) [3]. OIC poses a substantial challenge for both patients and healthcare providers, as it not only leads to physical discomfort and reduced quality of life but also affects treatment adherence and patient satisfaction. In the last decades, a novel pharmaceutical formulation has been introduced to address this challenge. A fixed 2:1 ratio combination of oxycodone and naloxone in prolonged released (PR) provides analgesia by binding to opioid receptors in the central nervous system, and simultaneously acting as a peripheral antagonist targeting opioid receptors in the gut [4] (Figure 2). The bioavailability of oral naloxone is poor (<3%) due to extensive hepatic first-pass metabolism, preventing naloxone from interfering with the central analgesic action of oxycodone [4]. Thus, naloxone alleviates the constipating effects of oxycodone, reducing the incidence and severity of OIC. Even though the topic has been previously discussed [5,6], a careful analysis of the literature reveals that a targeted approach in cancer pain patients alone is still lacking. Given the implication of managing severe cancer pain and the potential benefits of oxycodone/naloxone PR in addressing the challenges of opioid-induced constipation, this comprehensive review aims to critically evaluate the current evidence surrounding the efficacy, safety, patient experience, and overall impact of oxycodone/naloxone PR in the management only in severe cancer pain.
2. Cancer Pain Peculiarities
Cancer is a complex entity, not just consisting of primary cancer cells but also including a host-derived stroma composed of a variety of immune cells, mesenchymal cells, and endothelial cells. The stroma plays a crucial role in tumor development and progression by providing support and promoting interactions with surrounding tissues [7]. The relationship between the tumor and its microenvironment is dynamic and multifaceted. Both the tumor cells and the stromal cells secrete various mediators that modulate this relationship [8]. These mediators can influence processes such as angiogenesis, immune response, and tissue remodeling, ultimately shaping the tumor microenvironment and affecting tumor behavior. Interestingly, the development of many tumor types appears to involve the exploitation of host neuronal tissue [9]. Tumors can produce neurotrophic factors, such as nerve growth factor, which promote the survival and growth of nerves within and around the tumor. This phenomenon may contribute to the observed increase in neuronal density in the vicinity of tumors [10]. Moreover, tumors release a range of molecules that modulate pain perception. These molecules include hydrogen ions, inflammatory cytokines such as Tumor Necrosis Factor-alpha (TNF-α) and Interleukins (IL-1, IL-6), growth factors like Transforming Growth Factor-beta (TGF-β), and prostaglandins [11,12]. These substances sensitize and activate sensory nerve fibers, leading to the experience of pain. This localized release of pain-modulating agents contributes to the phenomenon of tumor-associated pain, which can significantly impact the quality of life of patients [13,14]. Additionally, central effects of these molecules are observed, leading to neuronal hyperexcitability and further amplification of pain signals. This central sensitization process involves changes in the excitability of neurons in the central nervous system, leading to enhanced responses to painful stimuli [15,16]. In summary, the interaction between tumors and their microenvironment is complex and involves various cellular and molecular components (Figure 1).
3. The Safety and Efficacy of Oxycodone/Naloxone PR in Cancer Pain
The efficacy of oxycodone/naloxone PR in the management of severe cancer pain has been extensively studied. Oxycodone is a full opioid receptor agonist with an affinity for endogenous mu, kappa and delta opiate receptors in the brain, spinal cord, and peripheral organs. Binding of oxycodone to endogenous opioid receptors in the central nervous system results in pain relief. Other pharmacological actions of oxycodone include respiratory depression, constipation, and cardiovascular system via histamine release and peripheral vasodilation [2]. Compared with morphine, which has an absolute bioavailability of approximately 30%, oxycodone has a high bioavailability of up to 87% following oral administration. Following absorption, oxycodone is distributed throughout the body. Approximately 45% is bound to plasma protein. Naloxone reduces bowel function disorders such as constipation that typically arise during opioid analgesic treatment due to its local competitive antagonism of the opioid receptor-mediated oxycodone effect in the gut. Diarrhea may be a possible effect of naloxone, especially at the beginning of treatment, and tends to be transient. Oral administration of naloxone is unlikely to result in a clinically relevant systemic effect due to a pronounced first-pass effect and its very low oral bioavailability upon oral administration. A recent metanalysis including thirteen studies, indicated that naloxone could significantly reduce the occurrence of nausea, and vomiting induced by opioids, without relieving pain and somnolence [17]. Clinical trials comparing oxycodone/naloxone to traditional opioid regimens have consistently demonstrated comparable analgesic efficacy. Among randomized controlled study on the efficacy and improved bowel function of oxycodone/naloxone PR, improvement in bowel function, analgesic efficacy, and safety profile in patients with non-malignant or malignant pain were confirmed in a phase III clinical trial [18]. A randomized, double-blind, active-controlled, study investigated the efficacy of receiving up to 120 mg/day of oxycodone/naloxone PR in patients affected by moderate to severe cancer pain as compared to oxycodone alone or shifted from other opioids [19]. The authors showed how patients who were switched directly from other opioids to oxycodone/naloxone PR experienced a similar analgesic effect, with a mean Brief Pain Inventory Short-Form (BPI-SF) scores comparable for the two groups and with a slight rating decrease during the observation period. Furthermore, a comparison between the administration of oral oxycodone/naloxone PR and transdermal fentanyl was proposed in patients with moderate-to-severe cancer pain [20]. Despite a similar analgesic activity, oxycodone/naloxone PR was characterized by lower daily dosages, less need for drug escalation, and fewer side effects. In patients with chronic cancer pain, oxycodone/naloxone PR provided an analgesic effect that was like oxycodone alone, with early and sustained benefits in tolerability [21]. The overall incidence of drug-related adverse events was 28.9% in the oxycodone group and 8.2% in the oxycodone/naloxone group, with a quality of life improved to a significantly greater extent in this group. Studies have also shown that oxycodone/naloxone maintains pain control without compromising the opioid’s analgesic effect. The analgesic response was assessed in 176 cancer patients experiencing moderate to severe pain and receiving oxycodone/naloxone PR [22]. The results demonstrated a reduction in both average and worst pain intensity over time, along with a decrease in the prevalence of breakthrough pain. Furthermore, 81.3% of patients exhibited a positive response to the treatment. In an open-label extension of a randomized, double-blind study 128 patients with moderate-to-severe cancer pain were randomized to receive oxycodone/naloxone PR or oxycodone alone [23]. Average pain scores based on the modified Brief Pain Inventory-Short Form were low and stable over the study period. In cancer-pain patients randomized, double-blind treatment a comparison between oxycodone/naloxone PR with controlled-release oxycodone or controlled-release morphine showed how a stable analgesia was achieved by 83% of controlled-release oxycodone and 81% of controlled-release morphine patients [24]. The findings from RCTs are supported by open-label studies, including 60-day observational study patients who required oxycodone/naloxone PR at high daily doses. The results showed how compared with baseline oxycodone/naloxone PR reduced pain intensity, the impact of pain on quality of life, and the number of breakthrough pain episodes [25]. In an observational study of patients affected by lung cancer associated with neuropathic pain, more than 80% of patients significantly reduced the average pain intensity improving health-related patient-reported outcomes [26]. A significant improvement in pain intensity was showed in exploratory, non-randomized, open-label, mono-center study in which the principal aim was to evaluate whether patients with advanced cancer and moderate to severe cancer pain will benefit from treatment with oxycodone/naloxone PR [27]. An additional observational study reported significant improvements in pain scores [28]. Finally, the effectiveness and safety of oxycodone/naloxone PR were evaluated in a subgroup of patients with severe cancer pain coming from a prospective, multicenter non-interventional study [29]. The results showed clinically relevant improvements in pain intensity both in opioid-naïve patients and in patients pretreated with weak or strong opioids, as reflected by reductions in pain scores of more than 50%. A multi-center, open-label, randomized, phase IV study is still proceeding to evaluate pain difference on Brief Pain Inventory-Short Form (BPI-SF) in cancer pain patients marked by a numerical pain score of ≥4/10 at baseline [30]. The oxycodone/naloxone’s efficacy is represented also by its potential to reduce the need for additional laxatives. In fact, by mitigating the occurrence of OIC, patients can avoid the use of adjunct medications [31]. A multicenter study reported the effectiveness of oxycodone/naloxone PR in patients with severe pain who had laxative refractory OIC with their previous opioid [32]. The results showed how more than 60% of patients reported both an improvement in constipation and in quality of life. In summary, oxycodone/naloxone PR has demonstrated considerable efficacy in providing pain relief for cancer patients experiencing severe pain. The combination’s ability to effectively address opioid-induced constipation while maintaining analgesic potency represents a significant advancement in cancer pain management.
Figure 1.
Mechanisms of cancer pain as a direct or indirect consequence of tumor.
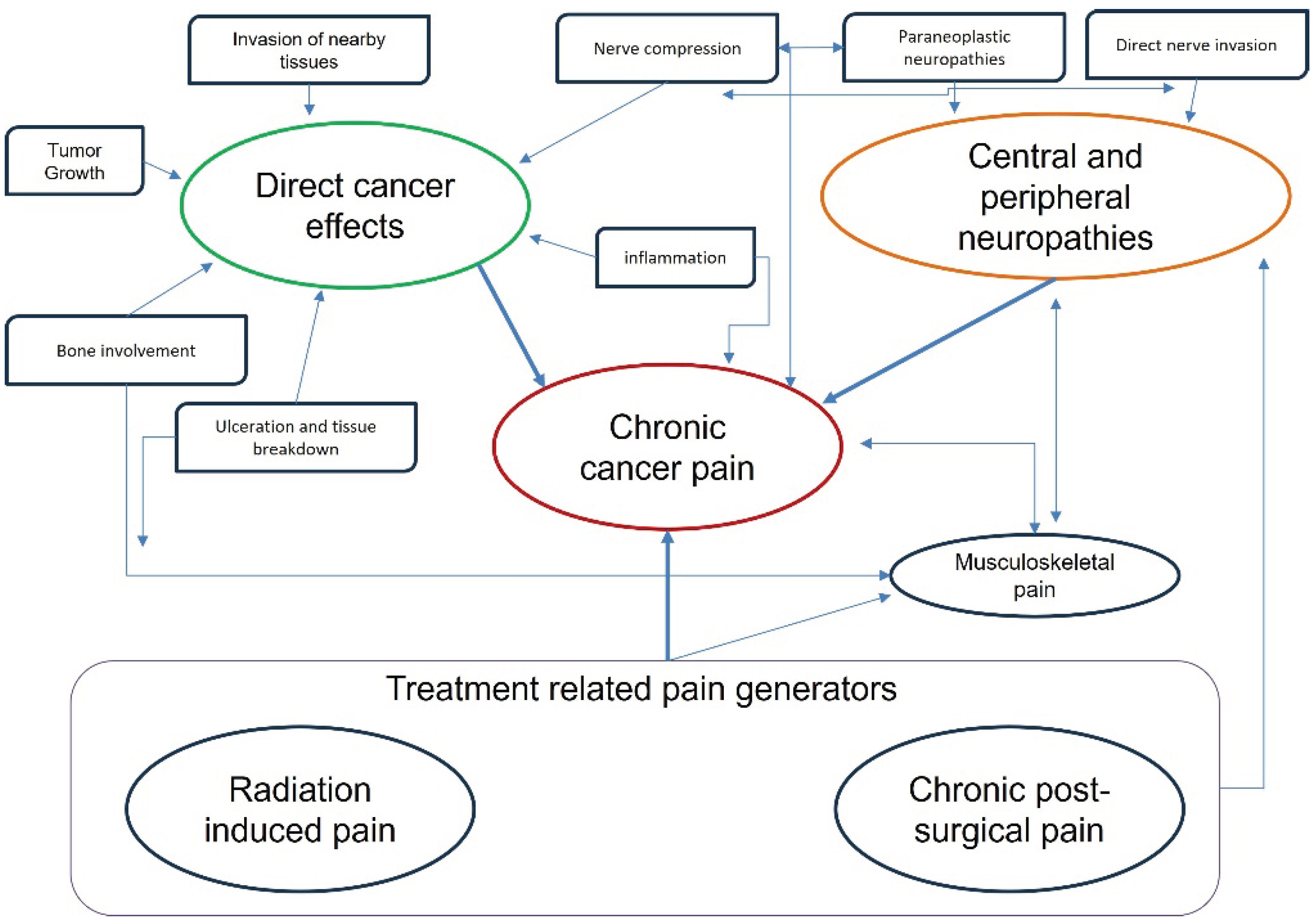
Figure 2.
Schematic diagram of mechanism involved in Oxycodone/naloxone PR.
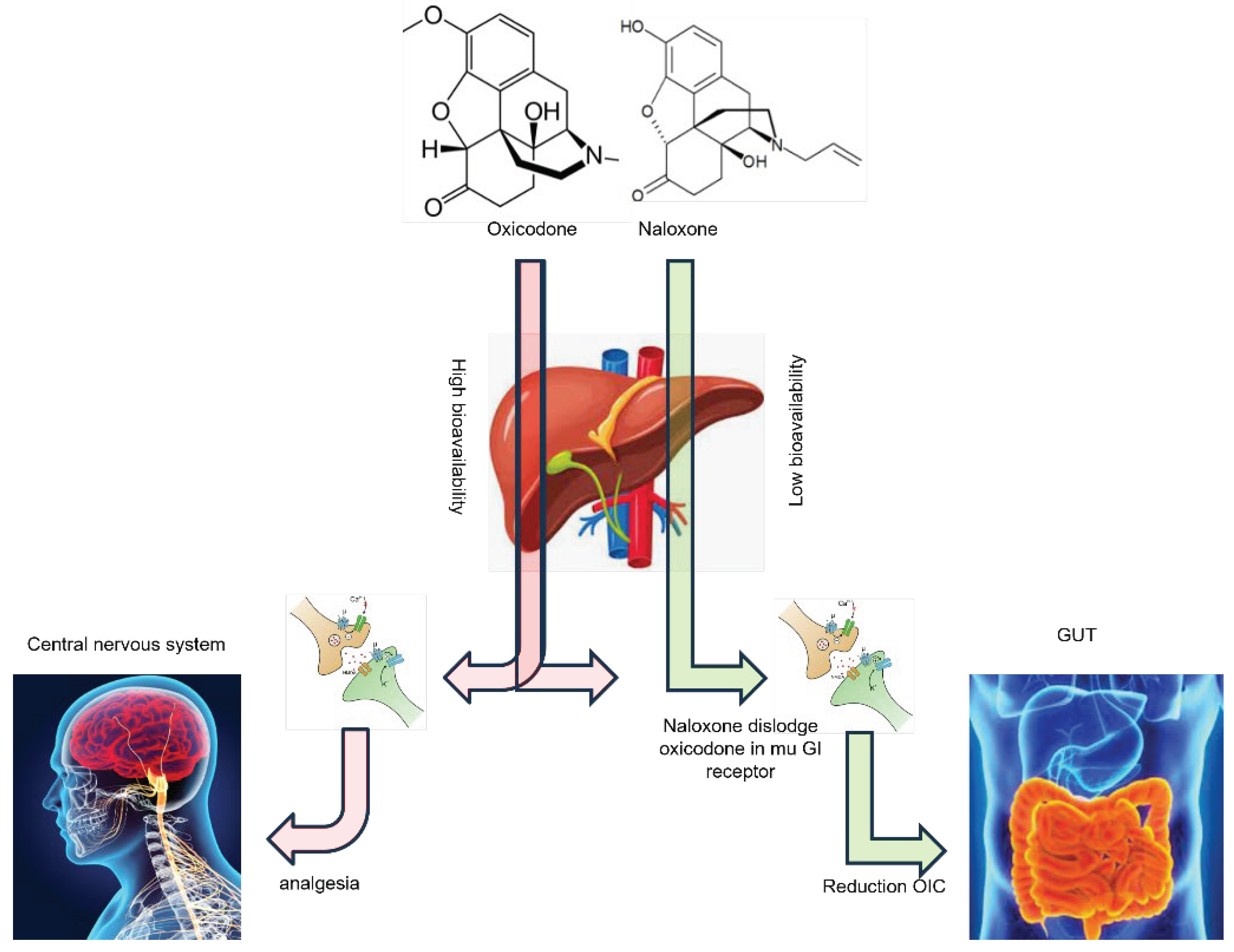
Conventional opioids typically exert a systemic impact by binding to μ-opioid receptors in both the central nervous system and gastrointestinal tract (GUT). The binding of opioids to the CNS produces analgesic effects, while their interaction with the GUT can lead to complications such as opioid-induced constipation. On the other hand, the 2:1 combination of opioid agonist-antagonist demonstrated effectiveness in alleviating opioid-induced constipation. This is achieved by naloxone binding to μ-opioid receptors in the GUT and displacing oxycodone from the receptor. Consequently, the adverse effects of opioids on the GUT are mitigated, while the analgesic effects of oxycodone remain intact due to naloxone’s low bioavailability and its initial metabolism by the liver.

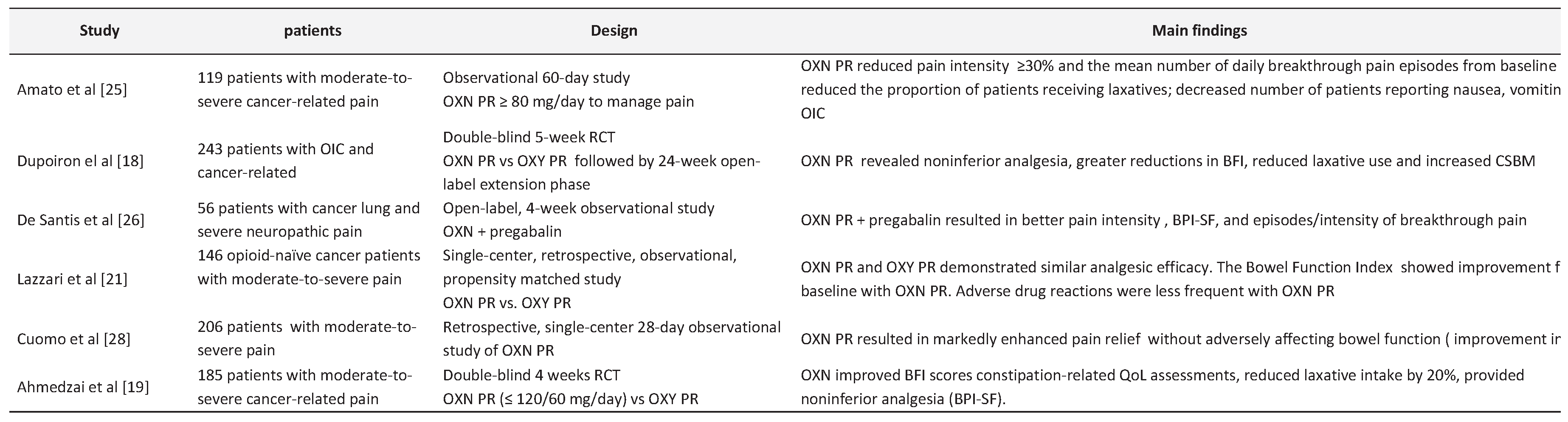
Table 1.
Principal studies regarding the use of oxycodone/naloxone prolonged relies in severe cancer related pain.
Table 1.
Principal studies regarding the use of oxycodone/naloxone prolonged relies in severe cancer related pain.
4. Patient Experience and Quality of Life
A substantial portion of individuals diagnosed with cancer and those who have survived the disease deal with various forms of social isolation, with one-third expressing recurrent feelings of loneliness [33]. In this context, the patient’s experience, and quality of life (QoL) are crucial considerations in the management of severe cancer pain. Since opioids are one of the cornerstones of pain therapy in oncology patients, the potential to reduce their side effects represent a significant aspect for improving the QoL and adherence to chronic treatment. QoL is a multidimensional parameter for which coverage may be categorized within five dimensions including physical, material, social, and emotional wellbeing [34]. Unfortunately, there is a lack of uniformity in the assessment of QoL across different studies, making it challenging to draw definitive conclusions. In many cases, the impact of pain on patients’ QoL is evaluated using the domains included in the BPI-SF [35]. These domains (general activity, walking ability, normal work, mood, enjoyment of life, sleep, relations with other people) are rated on an eleven-point NRS with scores ranging from 0 (no impairment) to 10 (most severe impairment), and which are summarized by calculating the arithmetic means for these seven items. Oxycodone/naloxone has shown positive effects on patient experience, not only because it is well-tolerated and offers adequate analgesic value, but also because of its ability to alleviate OIBD [36,37,38]. A recent Cochrane literature revision assessed OIBD prevalence, and the safety of mu-opioid antagonists as compared to different dosage, alternative pharmacological/non-pharmacological interventions, or placebo [39]. The mu-opioid antagonists evaluated the effects of oral naldemedine, and naloxone taken in combination with an opioid treatment in cancer patients. Within the study, naldemedine and methylnaltrexone were compared with placebo, while naloxone was compared with a placebo or opioid treatment only. The results showed how in 1343 patients included the evidence were very low to moderate because of the design of studies, including under-reporting of trial methods. There was low confidence in the evidence that there was no impact from naloxone in combination with an opioid in pain relief and there was uncertain evidence that naloxone taken with an opioid treatment improved symptom of constipation. Despite these recent observations, few papers report improvement in Opioid-induced bowel dysfunction as defined by The Bowel Function Index (BFI) which is a clinician-administered, patient-reported, 3-item questionnaire [40]. Patients treated with oxycodone/naloxone PR as compared with oxycodone alone showed improved BFI scores, constipation related, QoL assessments and reduced laxative intake by 20% [19]. Moreover, BFI scores significantly improved from baseline and the proportion of patients receiving laxatives and/or enemas declined in patient switched to higher doses of oxycodone/naloxone PL [25]. In patients diagnosed with OIC, oxycodone/naloxone PR was associated with significant improvements in BFI, stool consistency, spontaneous bowel movements, and Patient Global Impression [27]. In the double-blind RCT that compare oxycodone/naloxone PR vs. oxycodone alone in patients with OIC and cancer-related pain showed greater reductions in BFI, less laxative use, and more complete spontaneous bowel movement [18]. Nolte et al. [29] showed relevant improvements in bowel function as described by the reductions in the mean BFI of −20.5 and −36.5 in patients pretreated with weak and strong opioids. Furthermore, a substantial improvement in QoL was described by the decrease of pain-related functional impairment across all domains included in the BPI-SF. Otherwise, an observational study of cancer patients treated in an outpatient setting reported no clinically significant change in BFI scores or laxative intake as compared with prior analgesic therapy [28]. The combination of pain relief and reduced OIC-related side effects contributes to improved treatment adherence. In fact, adherence to cancer pain therapy is often suboptimal due to several factors which include the fear of addiction, physiological and harmful effects, tolerance, disease progression, and opioid side effects [41]. Numerous data suggest that, for many opioid-treated patients, poor tolerability with bowel dysfunction rather than inadequate analgesia may have been the motivating factor for opioid switching, which is known as an option that can be used to optimize analgesia and to reduce opioid-induced side effects [42]. Another aspect, sometimes overlooked but which can have a positive impact on both quality of life and treatment adherence, is the fact that since the medication is a combination of molecules, the total number of drugs the patient must take daily is significantly reduced [43]. There are no studies that have specifically verified this aspect, but it is reasonable to assume that the reduction in the number of medications may have a positive impact on patients’ overall treatment experience and may also result in cost savings, such as the avoidance of additional laxatives or stool softeners.
5. Controversial and Limitations
Despite all that has been described previously, there are some controversial aspects and limitations regarding the use of oxycodone/naloxone PR in cancer pain patients which include the individual variability, the pain sensitivity, opioid tolerance, comorbidities and concomitant medications, physical and social factors. One of the critical factors to consider in the management of severe cancer pain with oxycodone/naloxone is the significant variability in individual responses to opioids [44]. A 2010 analysis found that one-third of patients taking long-term opioid therapy for nonmalignant chronic pain either experienced the medication to be ineffective or poorly tolerated the treatment [45]. Pain management frequently involves a trial-and-error process over time. By asking if there was a way to choose the right medication at the right dose for a patient, the answer, in some cases, may lie in pharmacogenomics, an emerging field of genetic prediction of medication response [46]. Pharmacogenomics shifts our current medical paradigm from reactive to preventive by studying the genetic variations that are among the factors responsible for the wide variability in drug responses that we encounter today. A well-described example of pharmacogenetic variation is cytochrome (CY) P450 enzymes, which are involved in opiate metabolism [47]. There are clinical recommendations provided to help guide therapy of multiple opioids based on the CYP2D6 genotype, although the level of evidence varies between each medication [48]. Clinical Pharmacogenetics Implementation Consortium guidelines provide CYP2D6 genotype-based recommendations for oxycodone and other opioids, based on the available clinical evidence [49]. Even though in CYP2D6 normal metabolizers patients less the 10% of oxycodone is metabolized to oxymorphone which have higher affinity for mu-receptor. Oxycodone is still the main contributor to pain relief [50]. In patients with cancer receiving oxycodone, serum concentrations of oxymorphone were not statistically significantly different between CYP2D6 ultrarapid metabolizers and normal metabolizers as showed by a cross sectional multicenter study [51]. Clinical studies in postoperative patients and in patients with cancer failed to demonstrate a significant difference in analgesia or adverse events to oxycodone by CYP2D6 phenotype [52]. Similarly, the presence of comorbidities and the use of other medications can affect the effectiveness of pharmacokinetics and pharmacodynamics of opioids. For instance, oxycodone/naloxone PR needs to be given cautiously and monitored carefully in patients with mild hepatic or renal impairment (and is contraindicated in moderate to severe hepatic impairment) as plasma levels of naloxone may be raised, which can antagonize the analgesic effect of oxycodone [53,54]. In the brief 4-week RCT already mentioned above [19], it was observed that oxycodone/naloxone PR exhibited comparable analgesic efficacy to PR oxycodone in cancer patients, with a concurrent alleviation of constipation symptoms. The statistical significance in the reduction of the primary outcome, as measured by the change in constipation symptoms using the BFI, was noteworthy between the two groups. Although the reported difference approached borderline clinical significance, specifically a minimum of 12 points, the authors asserted its clinical relevance based on a comprehensive consideration of additional analyses. It is crucial to note that while various secondary outcome measures and analyses corroborate a reduction in constipation symptoms, the authors’ claim of clinical relevance is not unequivocally robust. The findings of this trial, despite its limited duration, align with prior investigations conducted in non-cancer patient populations. Nevertheless, akin to preceding studies, it does not offer insights into whether oxycodone/naloxone PR confers advantages over standard treatment involving strong opioids (such as modified-release morphine) and traditional prophylactic laxative interventions. After that, a prolonged exposure to opioids therapy may lead to the development of tolerance, that means that patients progressively require higher doses over time to achieve the same level of pain relief [25]. This issue may be less significant in the case of cancer pain when considered from the temporal perspective in which it is used, even if tolerance may result in diminishing efficacy and necessitate dose adjustments. Finally, multimodal analgesia should also be considered in the management of cancer pain [55]. This is an approach in which various analgesics are combined to maximize pain relief while simultaneously minimizing their adverse effects [56]. In cancer pain setting, multimodal pain management approaches - which may include non-opioid analgesics, physical therapy, psychological interventions, and complementary therapies to balance the analgesic effects of oxycodone/naloxone PR, should be implemented to minimize the risk of opioid tolerance and dependence [57].
6. Conclusion
Oral oxycodone/naloxone PR represents a valid option in the management of severe cancer pain. The combination of oxycodone and naloxone offers a dual mechanism of action that provides effective pain relief while successfully mitigating the constipating effects of opioids in the gastrointestinal tract. The reduction in OIC-related complications significantly improves patients’ bowel function and overall comfort, enhancing their quality of life and treatment adherence.
Author Contributions
Conceptualization, PF, MU, AP.; methodology, PF, MP,GS.; software, MU.; validation, MG, GT, AM; investigation, PF, MG, AM, LD.; data curation, PF.; writing—original draft preparation, PF, MG, AM.; writing—review and editing, MP, GT, GS.; supervision, AP, AG.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
not applicable.
Informed Consent Statement
not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
Author 3 (M.P.) is an employee of company” Contenuto Ed Net Communications SL”. The company had no role in the design, execution, interpretation, or writing of the study.
References
- Mestdagh, F.; Steyaert, A.; Lavand’homme, P. Cancer Pain Management: A Narrative Review of Current Concepts, Strategies, and Techniques. Curr Oncol 2023, 30, 6838–6858. [Google Scholar] [CrossRef]
- Kalso, E. Oxycodone. Journal of Pain and Symptom Management 2005, 29 (5, Supplement), 47–56. [Google Scholar] [CrossRef]
- Sizar, O.; Genova, R.; Gupta, M. Opioid-Induced Constipation. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2023. [Google Scholar]
- Morlion, B.J.; Mueller-Lissner, S.A.; Vellucci, R.; Leppert, W.; Coffin, B.C.; Dickerson, S.L.; et al. Oral Prolonged-Release Oxycodone/Naloxone for Managing Pain and Opioid-Induced Constipation: A Review of the Evidence. Pain Pract 2018, 18, 647–665. [Google Scholar] [CrossRef]
- Leppert, W. Oxycodone/naloxone in the management of patients with pain and opioid-induced bowel dysfunction. Curr Drug Targets 2014, 15, 124–135. [Google Scholar] [CrossRef]
- Kim, E.S. Oxycodone/Naloxone Prolonged Release: A Review in Severe Chronic Pain. Clin Drug Investig 2017, 37, 1191–1201. [Google Scholar] [CrossRef]
- Anderson, N.M.; Simon, M.C. Tumor Microenvironment. Current biology : CB 2020, 30, R921. [Google Scholar] [CrossRef]
- Le Bitoux, M.-A.; Stamenkovic, I. Tumor-host interactions: the role of inflammation. Histochem Cell Biol 2008, 130, 1079–1090. [Google Scholar] [CrossRef]
- Nguyen, T.M.; Ngoc, D.T.M.; Choi, J.-H.; Lee, C.-H. Unveiling the Neural Environment in Cancer: Exploring the Role of Neural Circuit Players and Potential Therapeutic Strategies. Cells 2023, 12, 1996. [Google Scholar] [CrossRef]
- Wang, W.; Li, L.; Chen, N.; Niu, C.; Li, Z.; Hu, J.; et al. Nerves in the Tumor Microenvironment: Origin and Effects. Frontiers in Cell and Developmental Biology 2020, 8. [Google Scholar] [CrossRef]
- Kartikasari, A.E.R.; Huertas, C.S.; Mitchell, A.; Plebanski, M. Tumor-Induced Inflammatory Cytokines and the Emerging Diagnostic Devices for Cancer Detection and Prognosis. Front Oncol 2021, 11, 692142. [Google Scholar] [CrossRef]
- Zhao, H.; Wu, L.; Yan, G.; Chen, Y.; Zhou, M.; Wu, Y.; et al. Inflammation and tumor progression: signaling pathways and targeted intervention. Signal Transduct Target Ther 2021, 6, 263. [Google Scholar]
- Falk, S.; Bannister, K.; Dickenson, A.H. Cancer pain physiology. Br J Pain 2014, 8, 154–162. [Google Scholar] [CrossRef]
- Yam, M.F.; Loh, Y.C.; Tan, C.S.; Khadijah Adam, S.; Abdul Manan, N.; Basir, R. General Pathways of Pain Sensation and the Major Neurotransmitters Involved in Pain Regulation. Int J Mol Sci 2018, 19, 2164. [Google Scholar] [CrossRef]
- Latremoliere, A.; Woolf, C.J. Central Sensitization: A Generator of Pain Hypersensitivity by Central Neural Plasticity. J Pain 2009, 10, 895–926. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152(3 Suppl), S2–15. [Google Scholar] [CrossRef]
- He, F.; Jiang, Y.; Li, L. The effect of naloxone treatment on opioid-induced side effects. Medicine (Baltimore) 2016, 95, e4729. [Google Scholar] [CrossRef]
- Dupoiron, D.; Stachowiak, A.; Loewenstein, O.; Ellery, A.; Kremers, W.; Bosse, B.; et al. A phase III randomized controlled study on the efficacy and improved bowel function of prolonged-release (PR) oxycodone-naloxone (up to 160/80 mg daily) vs oxycodone PR. Eur J Pain 2017, 21, 1528–1537. [Google Scholar] [CrossRef]
- Ahmedzai, S.H.; Nauck, F.; Bar-Sela, G.; Bosse, B.; Leyendecker, P.; Hopp, M. A randomized, double-blind, active-controlled, double-dummy, parallel-group study to determine the safety and efficacy of oxycodone/naloxone prolonged-release tablets in patients with moderate/severe, chronic cancer pain. Palliat Med 2012, 26, 50–60. [Google Scholar] [CrossRef]
- Roberto, A.; Greco, M.T.; Legramandi, L.; Galli, F.; Galli, M.; Corli, O. A comparison between the administration of oral prolonged-release oxycodone-naloxone and transdermal fentanyl in patients with moderate-to-severe cancer pain: a propensity score analysis. JPR 2017, 10, 2123–2133. [Google Scholar] [CrossRef]
- Lazzari, M.; Greco, M.T.; Marcassa, C.; Finocchi, S.; Caldarulo, C.; Corli, O. Efficacy and tolerability of oral oxycodone and oxycodone/naloxone combination in opioid-naïve cancer patients: a propensity analysis. DDDT 2015, 9, 5863–5872. [Google Scholar] [CrossRef]
- Corli, O.; Iorno, V.; Legramandi, L.; Rulli, E.; Roberto, A.; Azzarello, G.; et al. Oral prolonged-release Oxycodone-Naloxone: analgesic response, safety profile, and factors influencing the response in advanced cancer patients. Pain Pract 2019. [CrossRef]
- Ahmedzai, S.H.; Leppert, W.; Janecki, M.; Pakosz, A.; Lomax, M.; Duerr, H.; et al. Long-term safety and efficacy of oxycodone/naloxone prolonged-release tablets in patients with moderate-to-severe chronic cancer pain. Support Care Cancer 2015, 23, 823–830. [Google Scholar] [CrossRef]
- Mucci-LoRusso, P.; Berman, B.S.; Silberstein, P.T.; Citron, M.L.; Bressler, L.; Weinstein, S.M.; et al. Controlled-release oxycodone compared with controlled-release morphine in the treatment of cancer pain: a randomized, double-blind, parallel-group study. Eur J Pain 1998, 2, 239–249. [Google Scholar] [CrossRef]
- Amato, F.; Ceniti, S.; Mameli, S.; Pisanu, G.M.; Vellucci, R.; Palmieri, V.; et al. High dosage of a fixed combination oxycodone/naloxone prolonged release: efficacy and tolerability in patients with chronic cancer pain. Support Care Cancer 2017, 25, 3051–3058. [Google Scholar] [CrossRef]
- De Santis, S.; Borghesi, C.; Ricciardi, S.; Giovannoni, D.; Fulvi, A.; Migliorino, M.R.; et al. Analgesic effectiveness and tolerability of oral oxycodone/naloxone and pregabalin in patients with lung cancer and neuropathic pain: an observational analysis. Onco Targets Ther 2016, 9, 4043–4052. [Google Scholar] [CrossRef]
- Clemens, K.E.; Quednau, I.; Klaschik, E. Bowel function during pain therapy with oxycodone/naloxone prolonged-release tablets in patients with advanced cancer. Int J Clin Pract 2011, 65, 472–478. [Google Scholar] [CrossRef]
- Cuomo, A.; Russo, G.; Esposito, G.; Forte, C.A.; Connola, M.; Marcassa, C. Efficacy and gastrointestinal tolerability of oral oxycodone/naloxone combination for chronic pain in outpatients with cancer: an observational study. Am J Hosp Palliat Care 2014, 31, 867–876. [Google Scholar] [CrossRef]
- Nolte, T.; Schutter, U.; Loewenstein, O. Cancer pain therapy with a fixed combination of prolonged-release oxycodone/naloxone: results from a non-interventional study. Pragmat Obs Res 2014, 5, 1–13. [Google Scholar] [CrossRef]
- Wong, A. K.; Grobler, A.; Le, B. ENhANCE trial protocol: A multi-centre, randomised, phase IV trial comparing the efficacy of oxycodone/naloxone prolonged release (OXN PR) versus oxycodone prolonged release (Oxy PR) tablets in patients with advanced cancer. Contemp Clin Trials Commun 2022, 30, 101036. [Google Scholar] [CrossRef]
- Dorn, S.; Lembo, A.; Cremonini, F. Opioid-induced bowel dysfunction: epidemiology, pathophysiology, diagnosis, and initial therapeutic approach. Am J Gastroenterol Suppl 2014, 2, 31–37. [Google Scholar] [CrossRef]
- Bantel, C.; Tripathi, S.S.; Molony, D.; Heffernan, T.; Oomman, S.; Mehta, V.; et al. Prolonged-release oxycodone/naloxone reduces opioid-induced constipation and improves quality of life in laxative-refractory patients: results of an observational study. Clin Exp Gastroenterol 2018, 11, 57–67. [Google Scholar] [CrossRef]
- Kannan, V.D.; Veazie, P.J. US trends in social isolation, social engagement, and companionship ⎯ nationally and by age, sex, race/ethnicity, family income, and work hours, 2003–2020. SSM - Population Health 2023, 21, 101331. [Google Scholar] [CrossRef]
- Alonso, J.; Ferrer, M.; Gandek, B.; Ware, J.E.; Aaronson, N.K.; Mosconi, P.; et al. Health-related quality of life associated with chronic conditions in eight countries: results from the International Quality of Life Assessment (IQOLA) Project. Qual Life Res 2004, 13, 283–298. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singap 1994, 23, 129–138. [Google Scholar]
- Bell, T.J.; Panchal, S.J.; Miaskowski, C.; Bolge, S.C.; Milanova, T.; Williamson, R. The prevalence, severity, and impact of opioid-induced bowel dysfunction: results of a US and European Patient Survey (PROBE 1). Pain Med 2009, 10, 35–42. [Google Scholar] [CrossRef]
- Pappagallo, M. Incidence, prevalence, and management of opioid bowel dysfunction. Am J Surg 2001, 182(5A Suppl), 11S–18S. [Google Scholar] [CrossRef]
- Penning-van Beest, F.J.A.; van den Haak, P.; Klok, R.M.; Prevoo, Y.F.D.M.; van der Peet, D.L.; Herings, R.M.C. Quality of life in relation to constipation among opioid users. J Med Econ 2010, 13, 129–135. [Google Scholar] [CrossRef]
- Candy, B.; Jones, L.; Vickerstaff, V.; Larkin, P.J.; Stone, P. Mu-opioid antagonists for opioid-induced bowel dysfunction in people with cancer and people receiving palliative care. Cochrane Database Syst Rev 2022, 9, CD006332. [Google Scholar] [CrossRef]
- Ueberall, M.A.; Müller-Lissner, S.; Buschmann-Kramm, C.; Bosse, B. The Bowel Function Index for evaluating constipation in pain patients: definition of a reference range for a non-constipated population of pain patients. J Int Med Res 2011, 39, 41–50. [Google Scholar] [CrossRef]
- Vanneste, L.; Lefebvre, T.; Tack, L.; Van Eygen, K.; Cool, L.; Schofield, P.A.; et al. Pain Medication Adherence in Patients with Cancer: A Pragmatic Review. Pain Med 2022, 23, 782–798. [Google Scholar] [CrossRef]
- McNicol, E.; Horowicz-Mehler, N.; Fisk, R.A.; Bennett, K.; Gialeli-Goudas, M.; Chew, P.W.; et al. Management of opioid side effects in cancer-related and chronic noncancer pain: a systematic review. J Pain 2003, 4, 231–256. [Google Scholar] [CrossRef] [PubMed]
- Burness, C.B.; Keating, G.M. Oxycodone/Naloxone prolonged-release: a review of its use in the management of chronic pain while counteracting opioid-induced constipation. Drugs 2014, 74, 353–375. [Google Scholar] [CrossRef] [PubMed]
- Solhaug, V.; Molden, E. Individual variability in clinical effect and tolerability of opioid analgesics - Importance of drug interactions and pharmacogenetics. Scand J Pain 2017, 17, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Noble, M.; Treadwell, J.R.; Tregear, S.J.; Coates, V.H.; Wiffen, P.J.; Akafomo, C.; et al. Long-term opioid management for chronic noncancer pain. Cochrane Database Syst Rev 2010, 2010, CD006605. [Google Scholar] [CrossRef] [PubMed]
- Roden, D.M.; McLeod, H.L.; Relling, M.V.; Williams, M.S.; Mensah, G.A.; Peterson, J.F.; et al. Pharmacogenomics. Lancet 2019, 394, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Bugada, D.; Lorini, L.F.; Fumagalli, R.; Allegri, M. Genetics and Opioids: Towards More Appropriate Prescription in Cancer Pain. Cancers (Basel) 2020, 12, 1951. [Google Scholar] [CrossRef]
- Tadje, M. Genetic Variants Influencing Patient Response to Opioid Therapy. Oncol Nurs Forum 2015, 42, 420–422. [Google Scholar] [CrossRef] [PubMed]
- Crews, K.R.; Monte, A.A.; Huddart, R.; Caudle, K.E.; Kharasch, E.D.; Gaedigk, A.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin Pharmacol Ther 2021, 110, 888–896. [Google Scholar] [CrossRef]
- Klimas, R.; Witticke, D.; El Fallah, S.; Mikus, G. Contribution of oxycodone and its metabolites to the overall analgesic effect after oxycodone administration. Expert Opin Drug Metab Toxicol 2013, 9, 517–528. [Google Scholar] [CrossRef]
- Andreassen, T.N.; Eftedal, I.; Klepstad, P.; Davies, A.; Bjordal, K.; Lundström, S. Do CYP2D6 genotypes reflect oxycodone requirements for cancer patients treated for cancer pain? A cross-sectional multicentre study. Eur J Clin Pharmacol 2012, 68, 55–64. [Google Scholar] [CrossRef]
- Zwisler, S.T.; Enggaard, T.P.; Mikkelsen, S.; Brosen, K.; Sindrup, S.H. Impact of the CYP2D6 genotype on post-operative intravenous oxycodone analgesia. Acta Anaesthesiol Scand 2010, 54, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Davison, S.N. Clinical Pharmacology Considerations in Pain Management in Patients with Advanced Kidney Failure. Clin J Am Soc Nephrol 2019, 14, 917–931. [Google Scholar] [CrossRef] [PubMed]
- Le, B.H.; Aggarwal, G.; Douglas, C.; Green, M.; Nicoll, A.; Ahmedzai, S. Oxycodone/naloxone prolonged-release tablets in patients with moderate-to-severe, chronic cancer pain: Challenges in the context of hepatic impairment. Asia Pac J Clin Oncol 2022, 18, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; et al. Management of cancer pain in adult patients: ESMO Clinical Practice Guidelines. Ann Oncol 2018, 29 (Suppl 4), iv166–91. [Google Scholar] [CrossRef] [PubMed]
- Helander, E.M.; Menard, B.L.; Harmon, C.M.; Homra, B.K.; Allain, A.V.; Bordelon, G.J.; et al. Multimodal Analgesia, Current Concepts, and Acute Pain Considerations. Curr Pain Headache Rep 2017, 21, 3. [Google Scholar] [CrossRef]
- Carlson, R.H. Multimodal Pain Management Minimizes Need for Opioids. Oncology Times 2015, 37, 36. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



