Submitted:
01 April 2024
Posted:
03 April 2024
You are already at the latest version
Abstract
Background: We assessed the pertinence of yearly updating the International Working Group on the Diabetic Foot (IWGDF) risk classification in people with diabetes by quantifying the changes in the risk group and its accuracy in identifying those developing an ulcer (DFU) in a primary care setting.
Methods: In our retrospective cohort study, we included all people with diabetes with a foot as-sessment registry between January 2016 and December 2018 in the Baixo Alentejo Local Health Unit. Foot-related data was collected at baseline after one and two years. DFU and/or death until December 2019 were registered. The proportion of people changing their risk status each year was calculated. Accuracy measures of the IWGDF classification to predict DFU occurrence at one, two, and three years were calculated.
Results: A total of 2097 people were followed for three years, during which 0.1% died, and 12.4% developed a DFU. After two years, 3.6% of the participants had progressed to a higher-risk group. The IWGDF classification presented specificity values superior to 90% and negative predictive values superior to 99%.
Conclusion: Foot risk status can be safely updated every two years instead of yearly. The IWGDF classification can accurately identify those not at risk of DFU.
Keywords:
Diabetic foot
; screening
; cohort study
; primary care
1. Introduction
According to the International Diabetes Federation (IDF), more than 500 million people are living with diabetes. This number is expected to rise to almost 800 million by 2045, with a marked increase in Africa (134%) and MENA (Middle East and North Africa) region (87%) [1].
In 2021, the world diabetes prevalence in people between 20 and 79 years old was 10.5% and ranged from 9.2% in Europe up to 16.2% in the MENA region [1]. In Portugal, it was 13% affecting almost one million people, with around half still undiagnosed.
Diabetes can lead to micro and macrovascular complications, such as cerebrovascular disease, cardiovascular disease, nephropathy, retinopathy, peripheral artery disease (PAD) and neuropathy (DN). PAD and DN (motor, sensory and/or autonomic), along with repetitive external or minor trauma, are the major causes of the development and worsening of foot ulcers [2].
The diabetes-related foot ulcer (DFU) incidence worldwide is estimated to be between 9.1 to 26.1 million per year, with 19 to 34% of people with diabetes developing at least one DFU during their lifetime, and, although most of them will heal within one year, lower limb amputation (LLA) still occurs in 20% of the cases [2].
LLA remain one of the most threatening types of diabetes-related complications for people living with the condition, mainly for those who have previously experienced foot complications [3]. Foot disease is also the leading cause of global disability burden in people with diabetes and the major reason for hospitalisation [4].
Although it has been considered that DFU and LLA are the most devastating lower extremity complications due to diabetes, it was found that ¾ of the burden arises from people with neuropathy but without these complications [5].
These data stress the importance of characterising not only the risk of people with diabetes to develop DFU or LLA but also the global lower limb health status (namely the presence of foot deformity, PAD, DN or other conditions that may affect the person’s quality of life and ability to identify and manage complications).
Several international guidelines recommend annual foot screening in people with diabetes considered to be at (very) low risk of complications and more regularly for those considered to be at risk with a yearly update on the risk group assessment. However, it is unlikely that once established, the risk factors may retrocede and that a significant proportion of people will have a progression in the risk factors in that time frame [6].
Using the estimate of 500 million people currently living with diabetes [1] and at least two minutes spent per person to collect the information necessary to classify their risk of developing a DFU (which is highly dependent on clinical experience), there is the need for more than 17 million hours for health professionals to spend on this task yearly globally instead on investing on more direct preventive actions. This amount of time will only increase in the next years, with the expected rise of diabetes prevalence.
Additionally, it has been discussed that foot screening may not directly impact reducing foot complications [7]. The stratification of people by similar levels of risk should help health professionals in their clinical management and apply effective preventive measures according to the person's characteristics, focusing on education, adequate footwear, treatment of pre-ulcerative lesions, etc. However, it has been discussed that the registry of foot screening may be only a pro forma and not an act embedded in the clinical management flow, mainly in countries in which it is linked with financial consequences [7].
The International Working Group on the Diabetic Foot (IWGDF) classification is one of the most used stratification systems worldwide, with the last version being proposed in 2015 [8]. Nevertheless, their authors consider that more data on who, how, and when to screen and update the risk status is urgently needed [9].
This study aimed to assess the change in the risk factors and risk group for DFU based on the IWGDF classification (2015 version) at one and two years in a cohort of people with diabetes followed in a primary care setting. As a secondary aim, we assessed the accuracy of the IWGDF classification to identify people who developed a DFU at one, two, and three years.
2. Materials and Methods
2.1. Type of Study and Selection of Participants
This retrospective cohort study consecutively included people with diabetes followed in the Baixo Alentejo Local Health Unit (ULSBA) between January 2016 and December 2018, with at least two foot risk assessment registries.
Subjects had to be 18 years or older and have a foot assessment registered on their Electronic Health Record (EHR) (by SClinico) in at least two appointments with an interval of 12 or 24 months (with a margin of plus or minus 3 months) between them. People with DFU(s) present, bilateral major LLA that were bedridden or unable to cooperate with the foot assessment were excluded.
The beginning of the study was considered as T0 (or baseline), and assessments were conducted around 12 months after that period as T1 and 24 months after as T2, as described in Figure 1.
Due to the observational nature of our study, the STROBE checklist for cohort studies was used to improve its description and reporting [10].
2.2. Setting Characterization
ULSBA provides healthcare for around 115.000 inhabitants in a wide geographical region with a population density of 13,5 persons/Km2. The Baixo Alentejo region has the highest ageing index in the country, with 211,8 elderly people per 100 young people. The counties with more degree of ageing (e.g., Mértola and Ourique have more than 300 elderly per 100 young people) and the region with the highest suicidal rate in elderly people in the country [11].
ULSBA has had 14 level 1 (first level of care) diabetic foot clinics since 2013, managed by a diabetes nurse with the support of a general practitioner. As considered standard in the Portuguese primary care setting, these clinics have the main purpose of maintaining a regular inspection and assessment of the risk of developing foot complications and the need for preventive measures, providing regular education on foot self-care to the person with the diagnosis and caregivers (namely routine wearing of appropriate footwear), providing appropriate treatment for any pre-ulcerative lesions of the foot and superficial DFUs, along with the monitoring of more complex DFUs that are being treated in another level of care [12].
2.3. Data Collection Methods
Data was retrieved between April and September 2019 directly through the institution's database (via SClinico) in an anonymised fashion by using a randomly created code in Microsoft Excel.
SClinico is the platform developed by the Portuguese Ministry of Health that includes the EHR in Portugal, allowing the integration of information between the different levels of care and using ICD-10 codes. It is used by over 300 primary care institutions and 13,000 health professionals [13].
The collection of information by a general practitioner and/or a nurse so that the IWGDF (2015 version) classification can be applied is a part of the routine practice at primary care institutions in Portugal, except for the registry of ESRD. The proportion of people with diabetes who have at least an annual foot assessment and those with at least one DFU, LLA, and/ or hospitalisation due to diabetes-related foot complications are healthcare quality indicators [12].
The IWGDF classification (2015 version) consists of four risk groups [8]. In Group 0 (very low risk), people do not have a loss of protective sensation (LOPS) or PAD. In Group 1 (Low risk), people have LOPS or PAD. In Group 2 (Moderate risk), people have LOPS and PAD, or LOPS or PAD with foot deformity. In Group 3 (High risk), people have LOPS or PAD and at least one of the following: a history of DFU, history of LLA (minor or major), or end-stage renal disease (ESRD).
The definitions and procedures described by the IWGDF were used to collect and apply the respective classification [14,15]. LOPS was defined as altered 10-gram Semmes-Weinstein monofilament (SWM) and/or 128 Hz tuning fork sensation. Thus, only when the results of both tests were available could it be identified. Foot deformity was considered an alteration or deviation from the normal shape or size of the foot. PAD was classified as present when two or fewer foot pulses (out of four possible) were palpable. It was not possible to retrieve data about ESRD, as previously stated.
The presence or absence of SWM and tuning fork sensation, palpable dorsalis pedis and tibial posterior pulses, foot deformity, previous DFU and/or LLA on each foot were collected regularly.
Analysis of these variables was made at an individual level, so the presence of each risk factor was considered when it occurred in at least one of the limbs. For a person with a major LLA, the information available for the remaining limb was assumed to be equal to the amputated limb.
DFU development was assessed and recorded in the persons’ EHR also as part of their routine visits. A DFU was considered a break of the skin of the foot that involves, at minimum, the epidermis and part of the dermis [15]. Participants were followed until December 2019 or death, and analysis was made by person, not by number of events. This follow-up information was collected in June 2021.
The conduction of this study had the approval of the ULSBA ethical committee (number 04/2019 of April 2019), and informed consent was waived due to the study's retrospective nature. Data was handled anonymously.
2.4. Statistical Analysis
All the collected variables are categorical; thus, absolute and relative frequencies were calculated for the sample description. With these variables, the risk category was computed using the described definitions for each available assessment moment.
Cumulative incidence was calculated for DFU development at one, two, and three years and for changes in the presence or absence of risk factors as well as on risk group at one and two years.
Accuracy measures (namely sensitivity, specificity, predictive values, and likelihood ratios) of the IWGDF risk classification for DFU development at one, two and three years and the respective 95% confidence intervals (CI) were calculated.
Data was exported from the institution's database to an Excel spreadsheet and then imported to R studio [16], so that each line consisted of one participant with the assessment on each available time-point (longitudinal analysis).
The database comprised 6448 entries; three were duplicates and were removed along with 659 due to a lack of foot screening appointments outside the defined range (see Figure 1 for participants’ flowchart).
We have not imputed missing data as we considered the number of variables collected too low to allow the development of an accurate imputation model.
3. Results
3.1. Sample Characterisation
We have included 5786 individuals in our study; 8 (0.1%) died, and 48 (0.8%) developed a DFU during the three years of follow-up. However, we only have the baseline assessment of 26 out of the 48 people (54%) who developed a DFU during complete follow-up, as only 2097 (36%) had an assessment registered at this time point. There was an increased number of people with foot risk assessment at each time-point (4083 at T1 and 4612 at T2), and, as described in Figure 1, there were 1383 people with complete registries at T0 and T1, 3574 at T1 and T2 and 1591 at T0 and T2.
Missing data ranged 0.2% for history of previous DFU on T1 up to from 8% for LOPS on the baseline (T0) assessment.
At baseline, 31% of the participants had a registry of diabetes-related complications (retinopathy, nephropathy, cardiovascular and/or cerebrovascular disease), 14% were considered by the responsible nurse to be an active smoker, 23% to have adequate diabetes knowledge, and 33% to have inadequate footwear.
3.2. IWGDF Risk Factors and Degree Progression at One and Two Years
At T0, LOPS was present in 9.2% of the participants, 2.7% had PAD, almost half (48.7%) had foot deformity, 5.6% had a history of previous DFU history, and 2.1% had a history of previous LLA. Using the complete cases with information for all of these variables (n=2097), 90.1% were categorized as being at very low risk (group 0) of developing a new DFU, according to the IWGDF classification, 3.4% at low risk (group 1), 3.9% at moderate risk (group 2) and 2.5% at high risk (Group 3) (see Table 1).
When comparing data, from those with a registry available at T0 and T1 and/ or between T1 and T2 it is possible to observe that progression occurred in at least one of the risk variables in less than 3.5% of the cases. When comparing between T0 and T2 progression increased but was below 5%.
As for risk status, there was a progression in 3% of the people from T0 to T1 (n=1383), 2.6% from T1 to T2 (n=3574) and 3.6% from T0 to T2 (n=1591).
Although most of the variables that compose the IWGDF classification are considered not to be reversible, we identified a regression in the presence of risk variables (mainly in LOPS and foot deformity) and on risk level (between 1.6% when comparing T1 to T2 up to 2.6% when comparing T0 with T2) (see Table 1).
For those with data available at T0 and T1, we observed that foot deformity was the factor with higher progression (3.4%) and history of previous LLA as the one with lower progression (0.2%). The same occurred for those with data at T1 and T2 (progression in 2.3% and 0.1 of the participants, respectively) and also for those with data at T0 and T2 (progression of 4.8% and 0.3%, respectively).
On the other hand, LOPS appears to have receded in 2.3% of the participants from T0 to T1, 1.4% from T1 to T2, and 2.5% from T0 to T2. Being the latter a similar result to the one observed for foot deformity regression (2.6%). Previous LEA was the risk factor with a lower level of apparent regression when comparing all time points (≤0.1%).
As for risk categorisation, we noticed a higher progression of people from being at very low risk (group 0) to any other categories (1 up to 3) with an incidence inferior to 3% in any of the time points, and a progression from being at low risk or moderate risk to any other group inferior to 0.7%. A higher regression was observed from moderate risk (group 2) to very low risk (group 0) with an incidence inferior to 1.5%, for all the remaining risk groups it was inferior to 1%.
3.3. IWGDF Classification Accuracy in Predicting DFU Development at One, Two, and Three Years
From those with data available for IWGDF risk categorization at baseline (n=2097), we identified that after one- and two years of follow-up, people who developed a DFU were considered to be at very low (Group 0) or high risk (Group 3) (n=3 and n=4, respectively). Only at three years, it is observed people from all categories developing DFU, with a cumulative incidence of 0.7% for those in the very low-risk group (Group 0), 1.4% for those in the low-risk (Group 1), 7.4% for those in the moderate risk (Group 2) and 11.3% for those in the high-risk group (Group 3), respectively (see Table 2).
The incidence of DFU in people at very low risk (Group 0) at one year was 0.2%, at two years 0.3%, and at three years 0.7%. People at high risk (Group 3) presented an incidence of 7.5% at one and two years and 11.3% at three years.
As for the IWGDF classification accuracy (see Table 3), positive predictive values were inferior to 11.5% independently of the cut-off and time, with a rise in the values when using higher risk categories and increasing the DFU incidence.
Sensitivity values are inferior to 58%, with lower values as follow-up increases as well as the proportion of people in the very low-risk (group 0) developed DFUs.
On the other hand, specificity was superior to 90%, reaching around 98% when using the high-risk group as a cut-off and after three years of follow-up. Negative predictive values are equal or superior to 99%, with a slight decrease over time (from 99.9 to 90%).
Positive likelihood ratios ranged from 4.6 to 26.5, and negative likelihood ratios from 0.4 to 0.8. For the latter, the 95% CI include the value one.
There were statistically significant differences in specificity when using different cut-offs, but not over time. For the rest of the measures, such a pattern was not detected.
4. Discussion
4.1. Main Findings
Annual risk re-assessment is a recommended part of the diabetes-related foot care clinical practice. In our study, we showed that the change in the risk factors and risk group for DFU based on the IWGDF classification (2015 version) in a cohort of people with diabetes followed in a primary care setting is low with progression of at least one risk factors at two years occurring in less than 5% of the participants and an increase on risk status below 4%.
Also, our results indicate that the IWGDF classification can adequately identify people who is at low risk of developing a DFU at one, two, and three years with negative predictive values equal or above 90% for any follow-up duration or cut-off used. This means that those classified as being in Group 0 to 2 (very low to moderate risk) have a probability below 1% of developing a DFU at three years.
In our full cohort, only 8 people (0.1%) died and 48 (0.8%) developed a DFU during follow-up. Therefore, we have concluded that with such low progression and DFU incidence, the annual periodicity could be safely enlarged (at least) into every two years. This change would provide spare an important amount of time that health professionals could use to reinforce education and surveillance of patients at risk of foot complications.
4.2. Strengths and Weaknesses of the Study
The IWGDF classification is one of the most used classifications around the world. By selecting this classification and by using the provided definitions, our study results are standardized and can be applied worldwide.
The only variable that was not available was concerning the prevalence of ESRD. For a person with ESRD to be categorized as being in the highest risk group (Group 3) it is necessary to also have LOPS or PAD. This indicates that some of the 7.3% of our cohort classified as being at Group 1 or Group 2 at baseline can be incorrectly classified. Being the estimated prevalence of ESRD in people of diabetes of 18.8% [17], and assuming a constant prevalence within each risk group, we can expect a misclassification of only 1.4% of the study participants.
The size of our cohort, with 5786 individuals included in our study and with data on risk status from 2097 (T0) up to 4612 (T2) of them in a given moment, this study is one of the largest conducted on this topic.
In our setting, there was an improvement in the number of people with diabetes with a foot risk assessment registry each year. Most (89%) of the Portuguese population with type 2 diabetes has regular appointments registered in 2022 in public primary care institutions, and 74% of those have a foot screening registry [18]. Knowing that Baixo Alentejo region has 115.000 inhabitants [11], and a diagnosed diabetes prevalence of 8% [18], a steady cohort of around 5400 people would be expected.
We had a cohort of 2380 people on T0, 4597 on T1 and 5148 on T2, but a complete foot assessment registry of 2097 (88%), 4083 (89%) and 4612 (90%) people, respectively. For those with a registry of foot risk assessment in each time point, missing data ranged from 0.2% to 8% for any specific risk factors. This indicates that most people that had their feet checked had a complete assessment registry, but that the initial cohort represented less than half of the accessible population which may be an important limitation as selection bias cannot be excluded.
Due to this fluctuation of the sample size a direct comparison of the results between each timepoint is less straightforward.
Also, we believe that generalizability of our results can be impaired due to the low populational density and high degree of ageing. Despite this, more than 90% of the participants were on the very low risk group (Group 0), foot deformity had a prevalence around 45%, LOPS around 10% and PAD below 3%, and the provided structured care reflects the model used in Portugal. We consider that the specific characteristics of the study setting is expected to overestimate the risk factors and status progression, mainly of foot deformity prevalence and DFU incidence and, thus, to have more certainty of the indication to increase the interval between risk status update.
On the other hand, when comparing to the values of a high risk setting from the North of Portugal (prevalence of foot deformity of 78%, of LOPS superior to 34% and PAD of 37%, and a three year DFU incidence of 27% [19]) it is clear that this study adequately represents a primary care low risk setting.
When comparing our results to one of the largest cohort studies published recently [20], we observe that they described higher prevalence of PAD with 15% of the participants having absent pedal pulses, 17% having DN but a lower incidence of DFU during a three year follow-up (0.5% versus 1.2%).
Although there should be a yearly reassessment of the risk status for the development of diabetes-related foot complications, in real-life such evaluation moments are not exactly 12 months apart. We have determined that 3 months (above or below) would be an acceptable margin that would not affect the results. This range was based upon clinical sense and has no evidence support. Only 659 (n=10%) out of the 6445 individual entries had to be excluded for not complying with these timeframes.
One aspect that is not commonly described is the fact that, although several risk factors are not expected to be reversible without a specific clinical intervention, when using secondary data, we observed that in every timepoint there seemed to be a regression of all risk factors and on risk status (although in less than 2.6% of the sample). These values are very similar to those observed for risk progression, what in fact would almost cancel the overall progression incidence if it was not described separately.
This implies that it may be a limitation of data quality (in minor scale), but it reflects the reality. There is still a controversy about the reliability of the collection of these variables [21,22] that are highly experience-related.
We also acknowledge the retrospective observational nature of this study, that cannot replace a randomized controlled trial (that would be unrealistic to conduct due to ethical reasons) or a real-world evidence study using causal inference analysis. However, another article published by Crawford et al., in 2011, on this topic supports our conclusion that “annual foot screening in people with diabetes may not be cost-effective” [23].
As discussed by other authors, the terminology around this topic is somewhat unclear and potentially confusing [24]. Therefore, we would like to clarify that in this article we are discussing the need for annual (re-)classification of people with diabetes by their risk of developing a DFU according to the IWGDF classification. We are not suggesting that the feet of people with diabetes should not be examined to identify observable (such as foot deformity) or collect information (such as DN or PAD symptoms) about a potential progression of risk factors or the development of pre-ulcerative lesions and/or DFUs.
5. Conclusions
Our article indicates that, in a primary care setting, the update of the risk level of DFU development according to the IWGDF classification (2015 version) can be changed for every two years, instead of yearly. Also, the IWGDF classification can adequately identify those that will not develop a DFU in the next three years.
Author Contributions
Conceptualization, MMS and JD; Methodology, MMS; Software, DFS; Formal Analysis, MMS and DFS; Resources, JD, CP, SG; Data Curation, DS, Writing – Original Draft Preparation, MMS, JD, DFS.; Writing – Review & Editing, MMS; JD, CP, SG, DFS.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Local Health Unit of Baixo Alentejo, EPE (04/2019 of April 2019).
Informed Consent Statement
Patient consent was waived due to anonymized use of data and retrospective nature of the study.
Data Availability Statement
Data is available upon request and justification to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Magliano, D.J. and E.J. Boyko, IDF diabetes atlas. 2022.
- Armstrong, D.G.; Boulton, A.J.; Bus, S.A. Diabetic foot ulcers and their recurrence. New England Journal of Medicine 2017, 376, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Wukich, D.K.; Raspovic, K.M.; Suder, N.C. Patients with diabetic foot disease fear major lower-extremity amputation more than death. Foot & ankle specialist 2018, 11, 17–21. [Google Scholar] [CrossRef]
- Lazzarini, P.A.; et al. Diabetes-related lower-extremity complications are a leading cause of the global burden of disability. Diabetic Medicine 2018, 35, 1297–1299. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; et al. A new declaration for feet's sake: Halving the global diabetic foot disease burden from 2% to 1% with next generation care. Diabetes/metabolism research and reviews 2023, e3747. [Google Scholar] [CrossRef] [PubMed]
- Barshes, N.R.; et al. The system of care for the diabetic foot: objectives, outcomes, and opportunities. Diabetic foot & ankle 2013, 4, 21847. [Google Scholar] [CrossRef]
- Jeffcoate, W. Stratification of foot risk predicts the incidence of new foot disease, but do we yet know that the adoption of routine screening reduces it? Diabetologia 2011, 54, 991–993. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.; et al. IWGDF guidance on the prevention of foot ulcers in at-risk patients with diabetes. Diabetes/metabolism research and reviews 2016, 32, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.A.; et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes/Metabolism Research and Reviews 2024, 40, e3651. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Annals of internal medicine 2007, 147, W-163–W-194. [Google Scholar] [CrossRef]
- Instituto Nacional de Estatistica. Censos 2021. 2024 [cited 2024 21/03/2024].
- (DGS), D.-G.o.H., Norma nº 005/2011: Diagnóstico Sistemático do Pé Diabético 2011: https://normas.dgs.min-saude.pt/2011/01/21/diagnostico-sistematico-do-pe-diabetico/#:~:text=Norma%20n%C2%BA%20005%2F2011&text=O%20exame%20cl%C3%ADnico%20dos%20p%C3%A9s,alto%20risco.
- (SPMS), H.M.S.S. SClínico | Cuidados de Saúde Primários (CSP). 2020 [cited 2024 21/03/2024].
- Schaper, N.C.; et al. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes/Metabolism Research and Reviews, 2023: p. e3657. [CrossRef]
- van Netten, J.J.; et al. Definitions and criteria for diabetes-related foot disease (IWGDF 2023 update). Diabetes/Metabolism Research and Reviews 2023, e3654. [CrossRef]
- Team, R.C. R: A language and environment for statistical computing, Vienna, Austria. Published online 2021.
- Cheng, H.T.; et al. Worldwide Epidemiology of Diabetes-Related End-Stage Renal Disease, 2000-2015. Diabetes Care 2021, 44, 89–97. [Google Scholar] [CrossRef]
- Directorate-General of Health (DGS), National Program for Diabetes – Challenges and Strategies. 2023: Lisbon: NPD.
- Martins-Mendes, D.; et al. The independent contribution of diabetic foot ulcer on lower extremity amputation and mortality risk. Journal of Diabetes and its Complications 2014, 28, 632–638. [Google Scholar] [CrossRef]
- Stoekenbroek, R.M.; et al. How common are foot problems among individuals with diabetes? Diabetic foot ulcers in the Dutch population. Diabetologia 2017, 60, 1271–1275. [Google Scholar] [CrossRef]
- Bubun, J.; et al. Validity and Reliability Diabetic Foot Check-up as a Simple Screening Test of Diabetic Foot Ulcers in a Community. The International Journal of Lower Extremity Wounds 2023, 15347346231178181. [Google Scholar] [CrossRef] [PubMed]
- Edelman, D.; Sanders, L.J.; Pogach, L. Reproducibility and accuracy among primary care providers of a screening examination for foot ulcer risk among diabetic patients. Preventive medicine 1998, 27, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Crawford, F.; et al. The risk of foot ulceration in people with diabetes screened in community settings: findings from a cohort study. QJM: An International Journal of Medicine 2011, 104, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Pallin, J.A; et al. Do we screen, examine or assess to identify the “at-risk” foot in diabetes—time for agreed terms and definitions? Diabetic Medicine 2023, 40. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study time points and participants’ flowchart
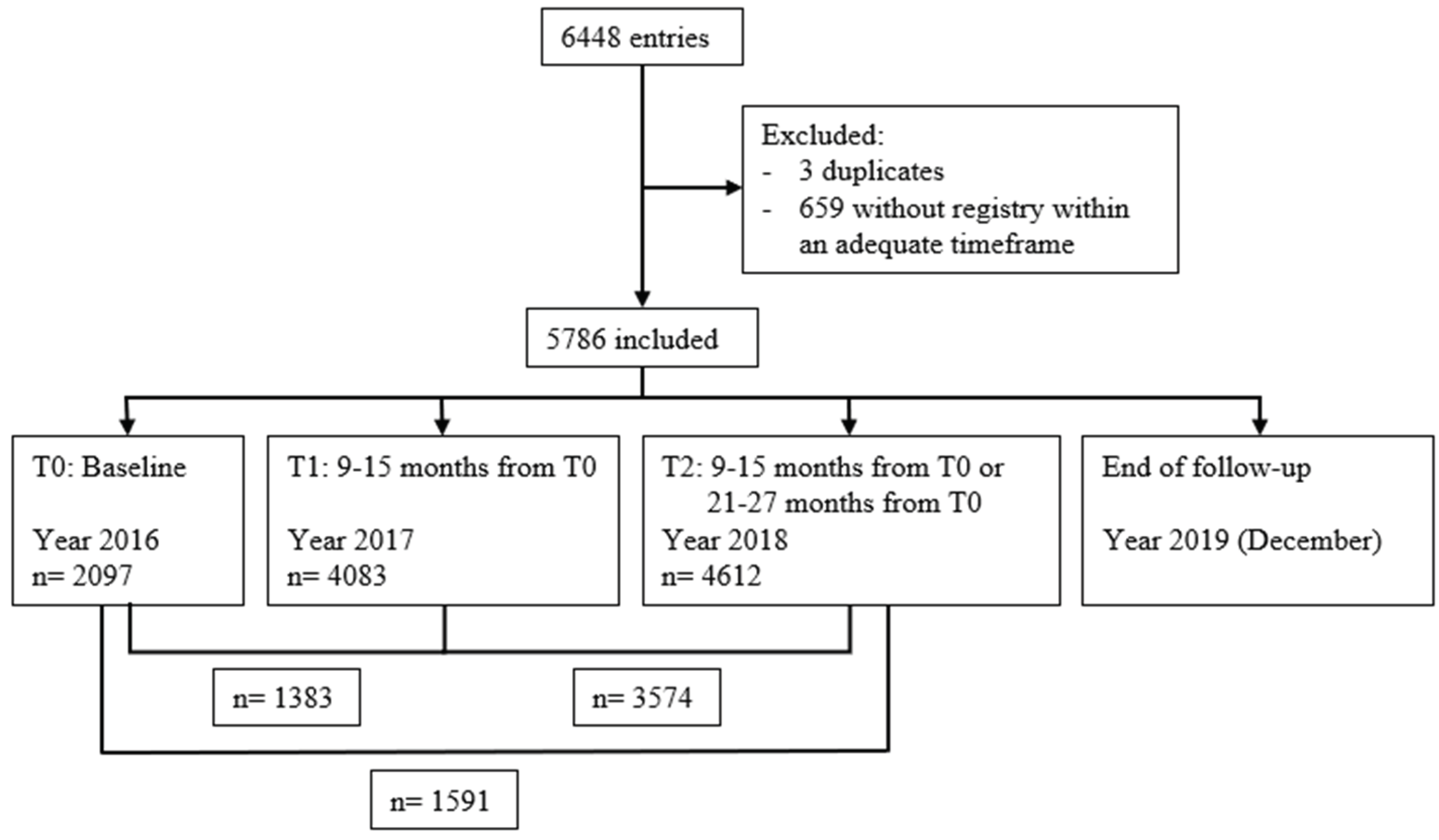

Table 1.
Presence of risk factors and risk categorization according to the IWGDF classification at each time point and respective changes between assessments.
Table 1.
Presence of risk factors and risk categorization according to the IWGDF classification at each time point and respective changes between assessments.
| Baseline (T0) |
1 year (T1) |
Change from baseline to 1 year (T0 to T1) |
2 years (T2) |
Change from 1 to 2 years (T1 to T2) |
Change from baseline to 2 years (T0 to T2) |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Present | Sample | Present | Sample | Progression | Regression | Sample | Present | Sample | Progression | Regression | Sample | Progression | Regression | Sample | |
| Risk factors | |||||||||||||||
|
LOPS [n (%)] |
202 (9.2) |
2190 | 465 (10.8) |
4308 | 36 (2.5) |
34 (2.3) |
1451 | 429 (8.8) |
4863 | 73 (1.9) |
54 (1.4) |
3801 | 48 (2.8) |
42 (2.5) |
1692 |
|
PAD [n (%)] |
60 (2.7) |
2259 | 97 (2.2) |
4323 | 8 (0.5) |
2 (0.1) |
1537 | 115 (2.4) |
4865 | 16 (0.4) |
13 (0.3) |
3814 | 9 (0.5) |
5 (0.3) |
1756 |
| Foot deformity [n (%)] | 1104 (46.8) | 2357 | 1953 (42.5) |
4597 | 55 (3.4) |
24 (1.5) |
1621 | 2184 (42.4) |
5148 | 94 (2.3) |
52 (1.3) |
4100 | 89 (4.8) |
49 (2.6) |
1865 |
| Previous DFU [n (%)] | 133 (5.6) |
2380 | 247 (5.4) |
4590 | 30 (1.8) |
4 (0.2) |
1655 | 312 (6.1) |
5131 | 79 (1.9) |
16 (0.4) |
4091 | 89 (4.7) |
8 (0.4) |
1890 |
| Previous LEA [n (%)] | 48 (2.1) |
2340 | 78 (1.7) |
4542 | 4 (0.2) |
1 (<0.1) |
1602 | 85 (1.7) |
5096 | 5 (0.1) |
2 (<0.1) |
4037 | 6 (0.3) |
2 (0.1) |
1844 |
| Risk group | |||||||||||||||
|
Group 0 (Very low risk) [n (%)] |
1890 (90.1) |
2097 | 3706 (90.8) |
4083 | To 1: 11 (0.8) To 2: 18 (1.3) To 3: 9 (0.7) |
NA | 1383 | 4172 (90.5) |
4612 | To 1: 32 (0.9) To 2: 23 (0.6) To 3: 20 (0.6) |
NA | 3574 | To 1: 13 (0.8) To 2: 17 (1.1) To 3: 16 (1.0) |
NA | 1591 |
|
Group 1 (Low risk) [n (%)] |
72 (3.4) |
143 (3.5) |
To 2: 1 (0.1) To 3: 0 (0.0) |
To 0: 13 (0.9) | 174 (3.8) |
To 2: 2 (0.1) To 3: 2 (0.1) |
To 0: 19 (0.5) |
To 2: 4 (0.3) To 3: 0 (0.0) |
To 0: 14 (0.9) | ||||||
|
Group 2 (Moderate risk) [n (%)] |
82 (3.9) |
137 (3.3) |
To 3: 1 (0.1) | To 0: 16 (1.2) To 1: 0 (0.0) |
136 (2.9) |
To 3: 12 (0.3) | To 0: 25 (0.7) To 1: 1 (<0.1) |
To 3: 6 (0.4) | To 0: 21 (1.3) To 1: 2 (0.1) |
||||||
|
Group 3 (High risk) [n (%)] |
53 (2.5) |
97 (2.4) |
NA | To 0: 4 (0.3) To 1: 0 (0.0) To 2: 0 (0.0) |
130 (2.8) |
NA | To 0: 9 (0.3) To 1: 1 (<0.1) To 2: 2 (<0.1) |
NA | To 0: 4 (0.3) To 1: 0 (0.0) To 2: 0 (0.0) |
||||||
| Total | 40 (3) | 33 (2.4) | 91 (2.6) | 57 (1.6) | 56 (3.6) | 41 (2.6) | |||||||||
NA: Not Applicable.
Table 2.
Diabetes-related foot ulcer development by the IWGDF risk category at one, two, and three years according to the baseline assessment.
Table 2.
Diabetes-related foot ulcer development by the IWGDF risk category at one, two, and three years according to the baseline assessment.
|
IWGDF risk group (based on the baseline assessment) |
Diabetes-related foot ulcer development | |||||
| 1 year | 2 years | 3 years | ||||
| Present | Sample | Present | Sample | Present | Sample | |
| Group 0 (Very low risk) [n (%)] | 3 (0.2) | 1890 | 5 (0.3) | 1890 | 13 (0.7) | 1888* |
| Group 1 (Low risk) [n (%)] | 0 (0.0) | 72 | 0 (0.0) | 72 | 1 (1.4) | 72 |
| Group 2 (Moderate risk) [n (%)] | 0 (0.0) | 82 | 0 (0.0) | 82 | 6 (7.4) | 81 # |
| Group 3 (High risk) [n (%)] | 4 (7.5) | 53 | 4 (7.5) | 53 | 6 (11.3) | 53 |
| Total | 7 (0.3) | 2097 | 9 (0.4) | 2097 | 26 (1.2) | 2097 |
* 2 people died; # 1 person died
Table 3.
Accuracy of the IWGDF classification to predict diabetes-related foot ulcer development at one, two and three years according to the baseline assessment.
Table 3.
Accuracy of the IWGDF classification to predict diabetes-related foot ulcer development at one, two and three years according to the baseline assessment.
| Sensitivity [% (95% CI)] |
Specificity [% (95% CI)] |
PPV [% (95% CI)] |
NPV [% (95% CI)] |
LR+ (95% CI) |
LR- (95% CI) |
|
|---|---|---|---|---|---|---|
| At 1 year | ||||||
| Group 1 to 3 | 57.1 (20.5-93.8) |
90.5 (89.2-91.7) |
2.0 (0.0-0.4) |
99.8 (99.7-100.0) |
6.0 (3.1-11.5) |
0.5 (0.2-1.1) |
| Group 2 to 3 | 93.9 (92.9-94.9) |
3.1 (1.1-6.0) |
99.9 (99.7-100.0) |
9.4 (4.8-18.2) |
||
| Group 3 | 97.8 (97.2-98.5) |
8.2 (0.5-15.8) |
26.5 (13.1-53.5) |
0.4 (0.2-1.0) |
||
| At 2 years | ||||||
| Group 1 to 3 | 44.4 (12.0-76.9) |
90.3 (89.0-91.6) |
1.9 (0.0-0.4) |
99.7 (99.5-100.0) |
4.6 (2.2-9.6) |
0.6 (0.3-1.1) |
| Group 2 to 3 | 93.7 (92.7-94.8) |
3.0 (0.0-0.6) |
99.8 (99.5-100.0) |
7.1 (3.3-15.0) |
||
| Group 3 | 97.7 (97.0-98.3) |
7.6 (0.0-14.7) |
18.9 (8.7-41.4) |
0.6 (0.3-1.0) |
||
| At 3 years | ||||||
| Group 1 to 3 | 50.0 (30.8-69.2) |
90.7 (89.4-91.9) |
6.3 (0.3-9.6) |
99.3 (98.9-99.7) |
5.4 (3.6-8.1) |
0.6 (0.4-0.8) |
| Group 2 to 3 | 46.2 (27.0-65.3) |
94.1 (93.1-95.1) |
9.0 (4.1-13.8) |
7.8 (5.0-12.3) |
||
| Group 3 | 23.1 (0.7-39.3) |
97.7 (97.1-98.4) |
11.3 (2.8-19.9) |
99.0 (98.6-99.5) |
10.2 (4.7-21.6) |
0.8 (0.6-1.0) |
CI Confidence Interval LR- Negative Likelihood Ratio, LR+ Positive Likelihood Ratio, NPV Negative Predictive Value, PPV Positive Predictive Value
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



