
Submitted:
02 April 2024
Posted:
03 April 2024
You are already at the latest version
Abstract
The Philippines has the highest HIV incidence rate in the Asia-Pacific region. Previous studies identified multilevel factors contributing to this phenomenon. This scoping review describes the extent of the literature on HIV contributory factors and identifies gaps to guide directions for HIV prevention research. The keywords HIV incidence, individual, sociocultural, environmental factors, and Philippines, were used to search for evidence on Google Scholar, PubMed, Scopus, and Web of Science databases. A total of 1,017 peer-reviewed articles published in the English language from 2014 to 2024 were reviewed using the Joanna Briggs Institute Scoping Review protocol. Thirty articles were included in this review. The majority of the available evidence was quantitative studies published between 2020 and 2024. Individual, sociocultural, economic, educational, political, and environmental factors shaped the Philippines’ HIV epidemic. Low levels of HIV knowledge, low testing rates, high-risk sex behaviors, stigma, lifestyle, location, lack of HIV education in schools, conservative society, and restrictive policies are HIV contributing factors. The Philippine HIV epidemic is multifactorial. Identifying the contributory factors is crucial in developing targeted interventions for high-risk populations. A dedicated HIV research program is needed to provide evidence-based information to guide the development of HIV preventive programs and research.
Keywords:
HIV incidence
; individual
; sociocultural
; environmental
; Philippines
1. Introduction
Human immunodeficiency virus (HIV) infection remains one of the most pressing global health challenges of our time, with its impact reverberating across continents and communities. The World Health Organization (WHO) aims to reduce annual new HIV infections globally from 1.5 million in 2020 to 370,000 by 2025 and 335,000 by 2030 [1]. To achieve this, primary intervention strategies that focus on high-quality, evidence-based, and people-centered services for high-risk and vulnerable populations are needed [1]. Essential services that focus on scientifically accurate, culturally appropriate comprehensive HIV programs are critical in helping individuals and communities promote HIV health [1].
Despite significant advancements in prevention, treatment, and care, the HIV epidemic continues to take a heavy toll on individuals, families, and societies worldwide. Nowhere is this more evident than in the Asia-Pacific region, where the burden of HIV is disproportionately high, and the Philippines, in particular, stands at the forefront of this alarming trend. The Philippines is grappling with a burgeoning HIV epidemic characterized by a sharp rise in new infections over the past decade. According to the latest data [2], the Philippines has the highest HIV incidence rate in the Western Pacific region, a distinction that underscores the urgency of understanding and addressing the underlying factors fueling this epidemic.
Against this backdrop, this scoping review endeavors to provide a comprehensive overview of the factors contributing to the high HIV incidence rate in the Philippines. By synthesizing existing literature spanning a decade from 2014 to the first quarter of 2024, this review seeks to elucidate the multifaceted nature of the HIV epidemic in the country and shed light on the complex interplay of individual, social, cultural, economic, political, educational, and environmental determinants shaping its trajectory.
1.1. HIV Epidemiology
Since the beginning of the AIDS epidemic in 1984, almost 84 million individuals have been infected with HIV, including 40 million AIDS-related deaths [1,3]. In 2023, approximately 40 million people were living with HIV (PLHIV) globally [3], with 1.3 million new HIV infections and 630,000 AIDS-related deaths annually [1]. Despite the decreasing incidence of HIV infections globally, several countries including the Philippines have seen a continuous rise in new HIV infections annually, making it the highest HIV incidence rate in the Asia-Pacific region [2,4,5]. Within the past decade, the Philippines had a 273% increase in HIV cases and a 315% increase in AIDS-associated mortality from 2010 to 2020 [3,6]. From four daily newly diagnosed HIV cases in 2010, this increased tenfold to 41 new HIV diagnoses in 2022 [6], making HIV a national epidemic in the Philippines. From 1,591 total new HIV cases in 2010, it has increased to 14,980 in 2022 and at its current incidence rate, it is projected that new HIV cases will grow by 300% in 2030 [6].
Globally, the majority of HIV cases are females [3]. In contrast, 95% of PLHIVs in the Philippines are predominantly males, with more than 66% of HIV cases affecting the adolescent and young adult population [6]. More than 33% of the country’s HIV cases are aged 25 to 34 years and less than 33% are under 25 years of age [6]. There is a growing HIV incidence in several vulnerable populations such as overseas Filipino workers (OFW), intravenous drug users (IVDU), pregnant women, older adults, and transactional sex workers (TSW) [6].
Four HIV review papers in the Philippine context have been previously published [7,8,9,10]. However, the focus of these reviews was uniquely different from our scoping review: facilitators and barriers to condom use [7], policy interventions on changing HIV-related behaviors [8], HIV risk associated with alcohol venues [9], and HIV-risk groups and prevention approaches [10].
Our review is the first to describe the extent of literature on the multidimensionality of factors that have contributed to the high HIV incidence in the Philippines. The startling HIV landscape in the Philippines calls for a dedicated research program and targeted interventions to address the needs of vulnerable populations and society, in general. This scoping review aims to map the extent of current literature on factors contributing to the high HIV incidence in the country to identify the gaps and serve as a benchmark for the development of an HIV research agenda and prevention programs.
1.2. Scoping Review
Scoping reviews are essential in mapping the current literature on a topic and in identifying gaps in the literature [11]. In this review, we sought to answer the review question: What individual, social, cultural, economic, political, educational, and environmental factors influenced the high HIV incidence rate in the Philippines? Several databases such as Google Scholar, PubMed, Scopus, Semantic Scholar, Crossref, and Web of Science databases were used to search for evidence using the keywords individual, sociocultural, political, educational, environmental factors, HIV, incidence, and Philippines. The Population-Concept-Context (PCC) framework was used to determine the eligibility criteria of the evidence [12]. The Population involves Philippine-based participants or Filipinos with HIV, Concept refers to the factors contributing to high HIV incidence, and Context focuses on Philippine-based studies or studies made on Filipinos with HIV. Research articles relevant to the context of this study from 2014 up to the first quarter of 2024 were investigated. Specifically, the inclusion criteria protocol has been set in selecting journal articles, 1) quality - must be a research article published in a peer-reviewed journal either in full-text or abstract form, 2) recency - must be published between 2014 to 2024, 3) language - must be in English language only, and 4) relevance - must focus on factors affecting HIV incidence in the Philippines. Exclusion criteria include studies published in 2013 or earlier and systematic reviews or literature reviews.
The significance of this endeavor cannot be overstated. HIV is not merely a biomedical issue but a socioecological phenomenon deeply rooted in the fabric of society. Its transmission and impact are influenced by a myriad of factors operating at multiple levels, from individual behaviors to broader structural determinants. Understanding these factors is crucial for designing effective interventions that address the root causes of HIV transmission and mitigate its impact on vulnerable populations. In light of these complexities, this scoping review seeks to map the existing literature on HIV contributory factors in the Philippines and identify gaps to guide future research, policy, and practice. By synthesizing evidence from diverse disciplines and perspectives, we aim to generate insights that inform the development and implementation of targeted interventions that address the structural determinants of HIV transmission and promote health equity for all.
2. Materials and Methods
2.1. Study Search Procedures
The Joanna Briggs Institute Scoping Review (JBI-ScR) protocol guided this scoping review [12] and was conducted consistent with the 2020 guidelines for Preferred Reporting Items for Systematic Reviews and Meta-analyses or PRISMA [13]. Before searching peer-reviewed online journal articles, the researchers set the criteria for inclusion and exclusion. Various meta-search engines were used to gather journal articles including Google Scholar, PubMed, Scopus, Semantic Scholar, Crossref, and Web of Science databases. In addition, the researchers used the software program Publish or Perish [14] to find lists of journal articles and analyze academic citations. The search was purposely delimited to 2014 up to the first quarter of 2024. Further, the descriptors entered in meta-search engines were as follows: HIV incidence, individual, sociocultural, environmental, Philippines. These words were put randomly and interchangeably in the meta-search engine until studies were exhausted. Filtering strategies include keywords, publication dates (2014-2024), availability of full text and abstracts, journal articles, and English language.
2.2. Search Outcome and Quality Appraisal
The database search strategy yielded 1,017 articles. Three authors independently conducted the initial appraisal of articles based on HIV-related titles, which yielded 81 articles. A secondary appraisal of the 81 articles with HIV-related titles and abstracts was done and 51 articles were excluded due to the following reasons: setting (i.e., conducted outside the Philippines, n=25), literature and systematic reviews (n=17), and different HIV focus (n=9). These results were finally narrowed down to 30 studies through an in-depth abstract and full-text analysis of each article using identified inclusion criteria (Figure 1). The interrater reliability for the 30 included evidence is 100%. Though not required for scoping reviews, these articles were subjected to quality assessment using the Critical Appraisal Skills Programme [15] indicators to add rigor to the search and selection process.
2.3. Data Extraction and Synthesis
Based on the data needs, the following data were extracted from each of the articles namely, 1) title and publication year, 2) study purpose, 3) authors, 4) abstract, and 5) results on the factors contributing to the high HIV incidence in the Philippines.
2.4. Coding Procedures
Collected data from the eligible journal articles were coded using the following: 1) study identification (author’s last name and year of publication), 2) methods (research design, sample size, and population), 3) relevant findings, and 4) factors affecting HIV incidence.
2.5. Data Analysis
A descriptive analysis of the review variables (e.g., year of publication, research design, unit of analysis, population, and factors contributing to the high HIV rate) was made using frequency and percentage distribution. Common findings, as well as unusual and unexpected, are highlighted. A narrative analysis and discussion of the review findings from the 30 articles are presented.
2.6. Reporting Review Findings
Findings from the search process are presented in Figure 1 using the PRISMA flow chart. Results of the scoping review are presented in summary tables (Table 1, Table 2 and Table 3) and narrative form. Existing literature and gaps are emphasized to provide directions for future studies and guide the development of tailored HIV prevention programs.
3. Results
3.1. Characteristics of Included Evidence
The majority of the 30 included studies were published between 2020-2024 (53.3%, n=16) and quantitative studies (56.7%, n=17), with sample sizes ranging from nine to 16,155 (Table 1). The population of the studies has wide variability, with the two most common involving MSM and gay men (40%, n=12) and PLHIV (n=9, 30%), followed by three (10%) studies each on women, community-based HIV workers, healthcare professionals, and key informants on HIV programs and policies, and two (6.7%) studies each on overseas Filipino workers (OFW), and transgender women (TGW). It is worthwhile noting that one study focused on prisoners.
3.2. Factors Contributing to the High HIV Incidence in the Philippines
Based on the available evidence from 2014 to 2024, multilevel factors from biological and individual levels to the broader sociocultural, economic, political, educational, and environmental elements have contributed to the high HIV incidence in the Philippines (Table 2). Individual (70.0%, n=21), sociocultural (63.3%, n=19), and economic factors (43.3%, n=13) were the most commonly identified factors contributing to the high HIV incidence in the Philippines.
3.2.1. Individual Factors
Twenty-one studies (70.0%) identified individual factors influencing the high HIV incidence in the Philippines [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,35,39,41,45,46]. Gender orientation, high-risk sex behaviors, lack of general HIV knowledge, lack of awareness of HIV prevention other than condoms, and low rates of condom use, are individual factors influencing the spread of HIV in the Philippines [16,17,18,20,21,23,24,26,27,39,41,45]. In a multi-country study in seven Asia-Pacific countries, Filipinos had the highest sexual risk behavior having a 60% inconsistent use with casual sex partners [22]. Bisexuals and MSM have significantly higher rates of HIV prevalence compared to the general population. Several of the selected evidence point to inconsistent condom use, lack of perceived need for HIV testing, multiple sex partners, unprotected sex with known HIV+ partners, and lack of awareness of the sex partner’s HIV status as common individual factors that might have contributed to the country’s continuously increasing HIV cases [17,19,22,25,41].
Although free HIV treatment is available in government HIV treatment hubs, low HIV testing rates, low treatment and adherence rates, lack of regular medical appointments, low HIV antiretroviral treatment (ART) rates, and those who are under ART, suboptimal adherence and non-adherence were crucial issues that may have adversely impacted HIV treatment goals [16,17,20,25,29,30,46]. Moreover, individual lifestyles such as the use of alcohol and intravenous drug use (IVDU) pose significant risks of contracting HIV [16,21,23,31]. Contraceptive use among women was reported to influence HIV rates [32]. Interestingly, the lack of knowledge and training of healthcare providers on HIV care created hesitancy and uncertainty in dealing with PLHIV under their care, which might have negatively impacted the quality and course of treatment of HIV patients [33].
3.2.2. Sociocultural Factors
Sociocultural factors such as stigma, peer pressure, religion, and social media were identified in 19 articles (63.3%) as contributing to the high HIV incidence in the country [16,17,19,20,21,22,23,24,29,31,32,34,35,37,38,39,41,43]. HIV-related stigma is highly prevalent in Philippine society, which might have impacted PLHIVs’ willingness to seek HIV testing and treatment [20,34,35,36,43]. For those undergoing HIV testing and treatment, stigma from the healthcare providers, such as nurses and physicians, particularly from public health centers may have prevented HIV at-risk individuals from testing and PLHIV from seeking medical treatment [34,35,43].
The conservative and religious nature of the predominantly Catholic Philippine society is detrimental to implementing the government’s HIV programs and making personal decisions to use condoms for HIV protection [24,35,36,37,38,45]. The social pressure among peers [16] not to use condoms [21,43], engage in IVDU [16], and seek sex work engagement [17,22,23] when faced with peer problems were associated with risks to the spread of HIV. Interestingly, one study reported that Muslims are associated with higher HIV prevalence [32]. The use of gay dating mobile applications made finding sexual partners more readily accessible, being compared to “as easy as getting an Uber (ride)” [39]. Lastly, with almost 10% of the Philippine population seeking work abroad as part of their culture to promote family social mobility, the risk of infecting their partners with HIV upon returning from deployment exists [41].
3.2.3. Economic Factors
Thirteen (43.3%) sources of evidence reported microeconomic and macroeconomic factors such as an individual’s occupation and socioeconomic status, high cost of HIV testing and treatment, and a country’s economy were associated with HIV prevalence [17,19,22,24,25,30,32,35,38,40,41,42,45]. Occupational-related factors such as TSWs and OFWs are two vulnerable populations that have increasing HIV incidence [17,22,23,35,41]. One study showed that lack of time due to a busy work schedule prevented OFWs from undergoing HIV testing [25]. A low socioeconomic status was identified as a risk for HIV spread due to the lack of financial capacity to get tested and the high cost of HIV testing and medical care in the Philippines [19,22,24,29,33,40]. Geographical areas with inefficient and low-funded social hygiene clinics (SHCs) have higher HIV prevalence compared to SHCs with more efficiency and funds [42]. At a macro level, low- to middle-income countries (LMIC) with lesser gross domestic product (GDP) are associated with negative HIV outcomes [30,32]. LMICs have higher HIV prevalence rates [32] and higher rates of suboptimal adherence to ART [30].
3.2.4. Environmental Factors
Eleven studies (36.7%) reported the environment as a factor fueling the HIV epidemic [16,20,22,28,29,30,33,34,35,38,42]. The evidence recognizes the role of geographical location [22,29,30], lack of accessibility to healthcare services [20], and prisons [28] as environmental factors that could potentially influence the spread of HIV. Inaccessibility of healthcare facilities [20] and lack of condom availability were issues related to living in rural areas [22,29] that might have contributed to the country’s HIV epidemic. Lifestyle factors that are influenced by the larger environment such as areas known for transactional sex (i.e., red-light districts), the presence of the internet and use of social media (e.g., gay dating sites), and venues that allow IV drug and alcohol use, which are more prevalent in urban areas may increase an individual’s vulnerability to practice high-risk sex behaviors [29].
The type of healthcare facility influences stigma, availability, accessibility, and quality of HIV care [16,33,34,35]. PLHIVs who experience stigma among healthcare providers may affect their participation in healthcare and adversely impact their HIV health outcomes. Areas with ineffective social hygiene clinics have higher HIV prevalence [42]. The lack of availability of resources for HIV testing and treatment in healthcare systems hinders individuals from seeking HIV care when needed [20,38]. Finally, prison management and practices pose a significant risk to HIV spread. The contextual factors of prisoners before incarceration (i.e., low socioeconomic status, IV drug use, low HIV knowledge, etc.) may have created an increased risk of HIV [28]. Environmental conditions in LMICs could have played a role in their higher HIV prevalence and lower treatment adherence rates [30].
3.2.5. Political Factors
Seven studies (23.5%) reported the role of political factors in influencing HIV epidemiology [16,20,24,32,37,42,43]. Government laws and regulations can shape HIV program implementation. Political and economic factors overlap due to legislation for the adequate provision of funds for HIV programs. Limited government funding for facilities and resources for HIV care may lead to inaccessible, unaffordable, and inefficient healthcare facilities, and could result in low HIV testing and treatment rates [16,20,42,43].
Though the Philippines has an HIV/AIDS law, it lacks specific provisions on HIV testing, mandatory HIV reporting, and ART treatment monitoring. Its restrictive policies on disallowing minors (under 18 years of age) to purchase condoms were in effect until its recent amendment in 2018 [24,37]. Furthermore, in an 80-country study including the Philippines, one study claimed that a democratic form of government promotes women empowerment, thus, encouraging women’s participation in reproductive and HIV-related programs, which eventually impact contraceptive use rates and HIV incidence rates [32].
3.2.6. Educational Factors
Four studies (13.3%) reported the lack of HIV education in schools and the lack of quality HIV information as educational factors contributing to the HIV epidemic [20,33,38,43]. The lack of access to quality HIV information was directly linked to poor knowledge about HIV [20]. The lack of implementation of the sex education curriculum [20,38,43] significantly influenced the level of knowledge and uptake of condoms among Filipinx transgender women and cisgender men who have sex with men [33]. Lastly, it has been shown that HIV knowledge is strongly associated with getting HIV test results among Filipino men [29]. Interestingly, the presence of stigma among healthcare providers in the Philippines is attributed to a lack of awareness and training on the health needs of HIV high-risk populations such as MSM and TGW [33].
3.2.7. Biological Factors
Two pieces of evidence were critical in understanding the biological nature of HIV and its role in the Philippine HIV epidemic. A shift in HIV molecular biology and the development of drug-resistant HIV variants with increased local HIV transmission were found in HIV molecular studies in the Philippines [16,17].
4. Discussion
4.1. Characteristics of Included Evidence
Our review shows that the majority of evidence includes quantitative studies published from 2020-2024, and focused on the MSM, gay men, PLHIV, OFW, and TGW populations. This is a shift in the research population of review studies before 2014 that focused on women. Recognizing the shift in Philippine HIV epidemiology from women to MSM, gay men, and TGW as HIV high-risk groups is crucial since they comprise the majority of new HIV infections in the country. The inclusion of OFWs [19,25] and prisoners [28] as HIV-vulnerable populations, as well as community-based HIV healthcare workers [25,36,39,43] and healthcare professionals [27,33,35], in recent studies, reflects an increased awareness of shifts in high-risk groups and multilevel involvement of stakeholders in HIV prevention.
Additionally, there is a dearth of literature on interventional studies to address either the HIV risk factors or vulnerable populations in our scoping review and from previously published HIV reviews from the 1990s to early 2010s [10]. This is a major gap in HIV research and prevention development that needs to be addressed. Innovative and evidence-based tailored interventions for vulnerable populations such as MSM, gay men, IVDUs, OFWs, TSWs, and TGWs are imperative.
4.2. Factors Contributing to the High HIV Incidence in the Philippines
The alarming increase in HIV incidence in the Philippines is multifactorial, ranging from molecular to environmental factors. From a biological standpoint, the changing HIV strain with its increased resistance to antiretroviral treatment and ability to spread more rapidly poses a serious threat to the country’s HIV epidemiology [16,17]. The change in HIV molecular biology can adversely affect the course of existing medical treatments and could result in difficulty achieving viral suppression and HIV treatment failure.
On a broader scale, various individual, sociocultural, educational, political, and environmental factors were identified to have contributed to the Philippine HIV epidemic. The majority of the evidence reported individual factors such as the lack of HIV knowledge, low rate of condom use, the prevalence of high-risk sex behaviors, low HIV testing rates, and low ART treatment rates as the major forces driving the exponential rate of new HIV cases in the Philippines [18,19,20,21,22,23,24,25,26,27,28,29,31]. Lifestyle factors such as the use of alcohol, IVDUs, resorting to transactional sex due to financial need, and the use of gay mobile dating sites [39,44] further compound the HIV vulnerability of high-risk populations. Moreover, two vulnerable occupational groups, TSWs and OFWs, have had a consistent increase in HIV cases over the past decade [6]. There is a paucity of research on these vulnerable populations that needs to be addressed [7]. These factors call for more intensified community-based HIV prevention programs focusing on the high-risk adolescent and young adult populations.
Although sex education is mandated in basic education under the country’s HIV and AIDS law, the lack of implementation of sexual and reproductive health in schools, coupled with the fragmentation of educational and healthcare systems led to inefficient delivery of HIV prevention programs to the youth [20,31,38,43]. The Philippines has a conservative and religious society with Catholicism as the predominant religion. Discussions surrounding sex are cultural taboo, particularly in Catholic schools which comprise a huge proportion of the basic education landscape [24,35,36,37,45]. Furthermore, HIV is not openly discussed among peers, family circles, and mainstream media due to stigma.
HIV-associated stigma is prevalent in society, including among healthcare professionals [34,35]. Stigma can have adverse health outcomes as high-risk individuals or PLHIV may not readily seek HIV testing and treatment, which can eventually lead to late diagnosis and delays in treatment [20,35,36]. The time lag between initial HIV infection, diagnosis, and treatment may result in increased viral transmission, adverse health outcomes such as AIDS-related conditions upon diagnosis, and delay or difficulty in achieving viral suppression. HIV stigma among healthcare providers needs to be addressed with more comprehensive training in HIV care [33,34,35,43].
Government-run HIV treatment hubs providing free ART are located in all geographical regions in the country but they are more situated in more urbanized areas creating accessibility issues for people living in the more remote rural areas [20]. This may have contributed to the low HIV treatment (36%) coverage of the Philippines, which is way below the WHO’s recommended 95% target goal [1]. Moreover, social determinants of health such as socioeconomic status, occupation, lack of transportation, rural location, distance from treatment hubs, the efficiency of social hygiene clinics, and low health literacy about free HIV treatment hamper the availability and accessibility of much-needed HIV services [19,20,22,28,29,42], leading to PLHIV’s suboptimal adherence to treatment [7,30]. HIV-related stigma is reportedly more prevalent in public health facilities, and some individuals resort to seeking treatment in private healthcare facilities [34]. However, the high financial cost of HIV testing and ART in private facilities can be prohibitive causing affordability issues [24,40].
Before 2018, the Philippines AIDS law prohibited minors from buying condoms and voluntary HIV testing without parental consent [2]. The restrictive government policy, coupled with the Catholic society’s view on artificial contraceptive use, limited the accessibility and amplified the stigma of condom use [36,37,45]. The implementation of the new HIV/AIDS law of 2018 that allows minors (at least 15 years of age) to purchase condoms and undergo HIV testing is a positive step toward capturing a potentially undiagnosed segment of this large at-risk population. Early HIV diagnosis and prompt treatment can help reduce the spread of HIV.
5. Conclusion
5.1. Conclusion
This review mapped the existing literature on multilevel factors contributing to the Philippine HIV epidemic. Based on the review findings, while there is a growing scope of HIV studies in the Philippines that have included high-risk populations that were not considered in previous research, a significant gap in HIV intervention research exists. A dedicated research program that focuses on HIV prevention and interventional studies, and targets vulnerable populations is urgently needed. Evidence-based and innovative strategies to improve HIV awareness and HIV testing, encourage condom and pre-exposure prophylaxis (PrEP) use, promote ART use and adherence, and reduce stigma in society in general, and among healthcare professionals in particular, are needed. While the amendment of the prohibitive national AIDS law is a positive move towards allowing condom purchase among minors, conservative and religious Filipino culture, and society still widely oppose the implementation of this evidence-based practice in HIV prevention. An open dialogue with sectarian community leaders and institutions, such as Catholic schools and other faith-based organizations, should be initiated to enhance understanding of HIV prevention best practices. The recent introduction of PrEP can be an alternative approach to HIV prevention. Further, a more comprehensive and aggressive HIV informational campaign for target populations such as MSM, gay men, OFW, IVDU, TSW, and TGW is needed. With a very limited number of studies focusing on HIV in women being conducted and a growing number of maternal-to-child HIV transmission, a focus on this vulnerable population is crucial.
Active multisectoral and community-based involvement in HIV prevention programs is critical in augmenting the government’s efforts to curb the spread of HIV in the country. Basic education and health-related programs in colleges and universities should strengthen the implementation of the government’s mandate on sex and reproductive health education and include a more comprehensive integration of HIV in the curriculum. For instance, nursing schools’ community learning experiences should include regular and continuous HIV prevention activities in their service communities. Moreover, a school-based HIV prevention program could be a targeted intervention to promote HIV awareness among the vulnerable young population.
Government, non-government organizations, and policymakers can use our review findings for an evidence-based approach to policy formulation and decision-making on legislative matters concerning HIV. Lastly, researchers can help address the gaps in the current HIV literature by investigating innovative approaches that will help reduce HIV transmission in the Philippines.
5.2. Limitations
Several limitations were identified in our scoping review. Only peer-reviewed articles and abstracts, excluding systematic and literature reviews, that were published in the English language within the last 10 years were included. Previous studies published before 2014 and systematic reviews on HIV in the Philippines may have captured some of our review variables, that could limit the generalization of our review findings. Gray literature such as documents and websites were not included to focus only on synthesizing empirical data.
Author Contributions
All authors have significant contributions to this article. Conceptualization, J.M., and J.L.; methodology, J.M., J.L., J.C., and J.D.; software, J.C.; validation, J.M., J.C., and J.D.; formal analysis, J.M., J.C., J.L, J.D., and R.L.; investigation, J.M., J.C., J.D.; writing—original draft preparation, J.M., J.C., J.D., and J.L.; writing—review and editing, J.M, J.L, J.C., J.D., and R.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization (WHO). HIV Country Profiles, 2022. Cfs.hivci.org. https://cfs.hivci.org/.
- Gangcuangco, L. M. A., & Eustaquio, P. C. The state of the HIV epidemic in the Philippines: progress and challenges in 2023. Trop Med and Inf Dis, 2023, 8(5), 258. [CrossRef]
- UNAIDS. Philippines. 2016. Unaids.org. https://www.unaids.org/en/regionscountries/countries/philippines.
- Devi, S. Stigma, politics, and an epidemic: HIV in the Philippines. The Lancet, 2019, 394, 2139-2140. [CrossRef]
- Govender, R.D., Hashim, M.J., Khan, M., Mustafa, H., & Khan, G. Global epidemiology of HIV/AIDS: a resurgence in North America and Europe. J of Epidemiology and Global Health, 2021, 11(3), 296-301. [CrossRef]
- Department of Health (DOH). HIV/AIDS & ART Registry of the Philippines – April 2022. 2022. Manila, Philippines. https://drive.google.com/file/d/1BA1SvIP3wkLrpSq1BjV57jjTzh7rQJxC/view?usp=sharing.
- De Torres, R.Q. Facilitators and barriers to condom use among Filipinos: A systematic review of literature. Health Promot Perspect. 2020 Nov 7;10(4):306-315. PMID: 33312926; PMCID: PMC7722996. [CrossRef]
- O’Reilly, K.R., d’Aquila, E., Fonner, V., Kennedy, C., & Sweat, M. Can policy interventions affect HIV-related behaviors? A systematic review of the evidence from low- and middle-income countries. AIDS Behavior, 2017, 21, 626-642. [CrossRef]
- Pitpitan, E.V. & Kalichman, S.C. Reducing HIV risks in the places where people drink: prevention interventions in alcohol venues. AIDS Behavior, 2016, 20:S119. [CrossRef]
- Restar, A., Nguyen, M., Nguyen, K., Adia, A., Nazareno, J., Yoshioka, E., et al. Trends and emerging directions in HIV risk and prevention research in the Philippines: A systematic review of the literature. PLoS ONE, 2018, 13(12): e0207663. [CrossRef]
- Mak, S., & Thomas, A. An Introduction to Scoping Reviews. J of Graduate Med Educ, 2022, 14(5), 561–564. [CrossRef]
- Pollock, D., Peters, M. D. J., Khalil, H., McInerney, P., Alexander, L., Tricco, A. C., Evans, C., de Moraes, É. B., Godfrey, C. M., Pieper, D., Saran, A., Stern, C., & Munn, Z. Recommendations for the extraction, analysis, and presentation of results in scoping reviews. JBI Evidence Synthesis, 2022, Publish Ahead of Print(3). [CrossRef]
- Haddaway, N. R., Page, M. J., Pritchard, C. C., & McGuinness, L. A. (2022). PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis Campbell Systematic Reviews, 18, e1230. [CrossRef]
- Harzing, A.W. Publish or Perish. 2007. https://harzing.com/resources/publish-or-perish.
- Critical Appraisal Skills Programme (CASP). 2018. https://casp-uk.net/casp-tools-checklists/.
- SahBandar, I. N., May, G., Freda, E., Nalyn Siripong, Mahdi Belcaid, Schanzenbach, D., Leano, S., Haorile Chagan-Yasutan, Hattori, T., Shikuma, C., & Ndhlovu, L. C. Ultra-Deep Sequencing Analysis on HIV Drug-Resistance-Associated Mutations Among HIV-Infected Individuals: First Report from the Philippines. AIDS Res and Human Retroviruses, 2017, 33(11), 1099–1106. [CrossRef]
- Salvaña, E. M. T., Schwem, B. E., Ching, P. R., Frost, S. D. W., Ganchua, S. K. C., & Itable, J. R. The changing molecular epidemiology of HIV in the Philippines. Int J of Inf Dis, 2017, 61, 44–50. [CrossRef]
- Calaguas, N. P. Predictors of condom use among gay and bisexual men in the Philippines. Int J of Sexual Health, 2020, 1–11. [CrossRef]
- Ofreneo, M. A. P., Gamalinda, T. B., & Canoy, N. A. Culture-embedded drivers and barriers to (non) condom use among Filipino MSM: a critical realist inquiry. AIDS Care, 2020, 1–6. [CrossRef]
- Adams, J., Coquilla, R., Montayre, J., Manalastas, E. J., & Neville, S. Views about HIV and sexual health among gay and bisexual Filipino men living in New Zealand. Int J of Health Promotion and Educ, 2020, 59(6), 342–353. [CrossRef]
- De Irala, J. Safe sex belief and sexual risk behaviors among adolescents. PubMed, 2016, 31(2), 185–190. [CrossRef]
- Deuba, K., Kohlbrenner, V., Koirala, S., & Ekström, A. M. Condom use behaviour among people living with HIV: a seven-country community-based participatory research in the Asia-Pacific region. Sexually Transmitted Infections, 2017, sextrans-2017-053263. [CrossRef]
- Estacio, L., Estacio, J. Z., & Alibudbud, R. Relationship of psychosocial factors, HIV, and sex work among Filipino drug users. Sexuality Research and Social Policy. 2021. [CrossRef]
- Gohil, J., Baja, E. S., Sy, T. R., Guevara, E. G., Hemingway, C., Medina, P. M. B., Coppens, L., Dalmacion, G. V., & Taegtmeyer, M. Is the Philippines ready for HIV self-testing? BMC Public Health, 2020, 20(1). [CrossRef]
- Hall, B. J., Yang, X., Huang, L., Yi, G. Y., Chan, E. D., Tucker, J. D., & Latkin, C. A. Barriers and facilitators of rapid HIV and syphilis testing uptake among Filipino transnational migrants in China. Aids and Behavior, 2020, 24(2), 418–427. [CrossRef]
- Millalos, M. G., & Cutamora, J. From testing to coping: the voices of people living living with HIV/AIDS. Philippine J of Nursing, 2019, 89(2).
- Mosende, A. G., Lacambra, C. B., & De los Santos, J. A. Knowledge, attitudes, and behaviors toward HIV/AIDS among health care workers in urban cities in Leyte Philippines. Malaysian J of Nursing, 2023, 14(03), 185–193. [CrossRef]
- Palma, D. M., & Parr, J. Behind prison walls: HIV vulnerability of female Filipino prisoners. Int J of Prisoner Health. 2019. [CrossRef]
- Pepito, V. C. F., & Newton, S. Correction: Determinants of HIV testing among Filipino women: Results from the 2013 Philippine National Demographic and Health Survey. PLOS ONE, 2021, 16(1), e0246013. [CrossRef]
- Bijker, R., Jiamsakul, A., Kityo, C., Kiertiburanakul, S., Siwale, M., Phanuphak, P., Akanmu, S., Chaiwarith, R., Wit, F. W., Sim, B. L., Boender, T. S., Ditangco, R., Rinke De Wit, T. F., Sohn, A. H., & Hamers, R. L. Adherence to antiretroviral therapy for HIV in sub-Saharan Africa and Asia: a comparative analysis of two regional cohorts. J of the Int AIDS Society, 2017, 20(1), 21218. [CrossRef]
- Cheng, C.-H. E., Gipson, J. D., Perez, T. L., & Cochran, S. D. Same-Sex Behavior and Health Indicators of Sexually Experienced Filipino Young Adults. Archives of Sex Beh, 2016, 45(6), 1471–1482. [CrossRef]
- Noble, M. D., & Austin, K. F. Gendered dimensions of the HIV pandemic: A cross-national investigation of women’s international nongovernmental organizations, contraceptive use, and HIV prevalence in less-developed nations. Sociological Forum, 2014, 29(1), 215–239. [CrossRef]
- Restar, A. J., Chan, R. C. H., Adia, A., Quilantang, M. I., Nazareno, J., Hernandez, L., Cu-Uvin, S., & Operario, D. Prioritizing HIV Services for Transgender Women and Men Who Have Sex With Men in Manila, Philippines. J of the Asso of Nurses in AIDS Care, 2019, 31(4), 1. [CrossRef]
- De los Santos, J. A., Tuppal, C., & Milla, N. The correlates of health facility-related stigma and health-seeking behaviors of people living with HIV. Acta Medica Philippina. 2022, . [CrossRef]
- Jegonia, F. (2019). “Stigma and level of care among health care providers to HIV/AIDS patients.” 2019. [CrossRef]
- Adia, A. C., Bermudez, A. N. C., Callahan, M. W., Hernandez, L. I., Imperial, R. H., & Operario, D. “An Evil Lurking Behind You”: Drivers, experiences, and consequences of HIV–related stigma among men who have sex with men with HIV in Manila, Philippines. AIDS Educ and Prev, 2018, 30(4), 322–334. [CrossRef]
- Melgar, J. L. D., Melgar, A. R., Festin, M. P. R., Hoopes, A. J., & Chandra-Mouli, V. Assessment of country policies affecting reproductive health for adolescents in the Philippines. Reproductive Health, 2018, 15(1). [CrossRef]
- Restar, A. J., Adia, A., Nazareno, J., Hernandez, L., Sandfort, T., Lurie, M., Cu-Uvin, S., & Operario, D. Barriers and facilitators to uptake of condoms among Filipinx transgender women and cisgender men who have sex with men: A situated socio-ecological perspective. Global Public Health, 2019, 1–12. [CrossRef]
- Hollingshead, B. M., Dowsett, G. W., & Bourne, A. “It’s like getting an Uber for sex”: social networking apps as spaces of risk and opportunity in the Philippines among men who have sex with men. Health Sociology Review, 2020, 29(3), 264–278. [CrossRef]
- Wong, J., Co, S. A., Espinosa, C. I., Zeck, W., Bermejo, R., & Silfverberg, D. Acquired Immune Deficiency Syndrome benefit package: A financial review. Int J of Tech Assessment in Health Care, 2018, 34(S1), 54–55. [CrossRef]
- Ofreneo, M. A., & Canoy, N. Falling into poverty: the intersectionality of meanings of HIV among overseas Filipino workers and their families. Culture, Health & Sexuality, 2017, 19(10), 1122–1135. [CrossRef]
- Seposo, X. T., Okubo, I., & Kondo, M. Assessing frontline HIV service provider efficiency using data envelopment analysis: a case study of Philippine social hygiene clinics (SHCs). BMC Health Services Research, 2019, 19(1). [CrossRef]
- Newman, P. A., Prabhu, S. M., Akkakanjanasupar, P., & Tepjan, S. HIV and mental health among young people in low-resource contexts in Southeast Asia: A qualitative investigation. Global Public Health, 2021, 1–15. [CrossRef]
- Icamina, P. Internet “major” factor in Philippines’ HIV epidemic. Asia & Pacific. 2018, October 18. https://www.scidev.net/asia-pacific/news/internet-major-factor-in-philippines-hiv-epidemic/.
- Canoy, N. A., & Ofreneo, M. A. P. Struggling to care: A discursive-material analysis of negotiating agency among HIV-positive MSM. Health: An Interdisciplinary J for the Soc Study of Health, Illness and Med, 2016, 21(6), 575–594. [CrossRef]
- De Torres, R.Q., Pacquiao, D., Ngaya-an, F., & Tuazon, J. Adherence to antiretroviral therapy and scheduled clinic visits of persons living with HIV in the Philippines. J of Nurs Practice and Rev of Research, 2021, 11(2), 19-30. [CrossRef]
Figure 1.
PRISMA Flow Diagram. Adopted from Haddaway, N.R., Page, M.J., Pritchard, C.C., & McGuinness, L.A. (2022). PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis Campbell Systematic Reviews, 18, e1230.
Figure 1.
PRISMA Flow Diagram. Adopted from Haddaway, N.R., Page, M.J., Pritchard, C.C., & McGuinness, L.A. (2022). PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis Campbell Systematic Reviews, 18, e1230.
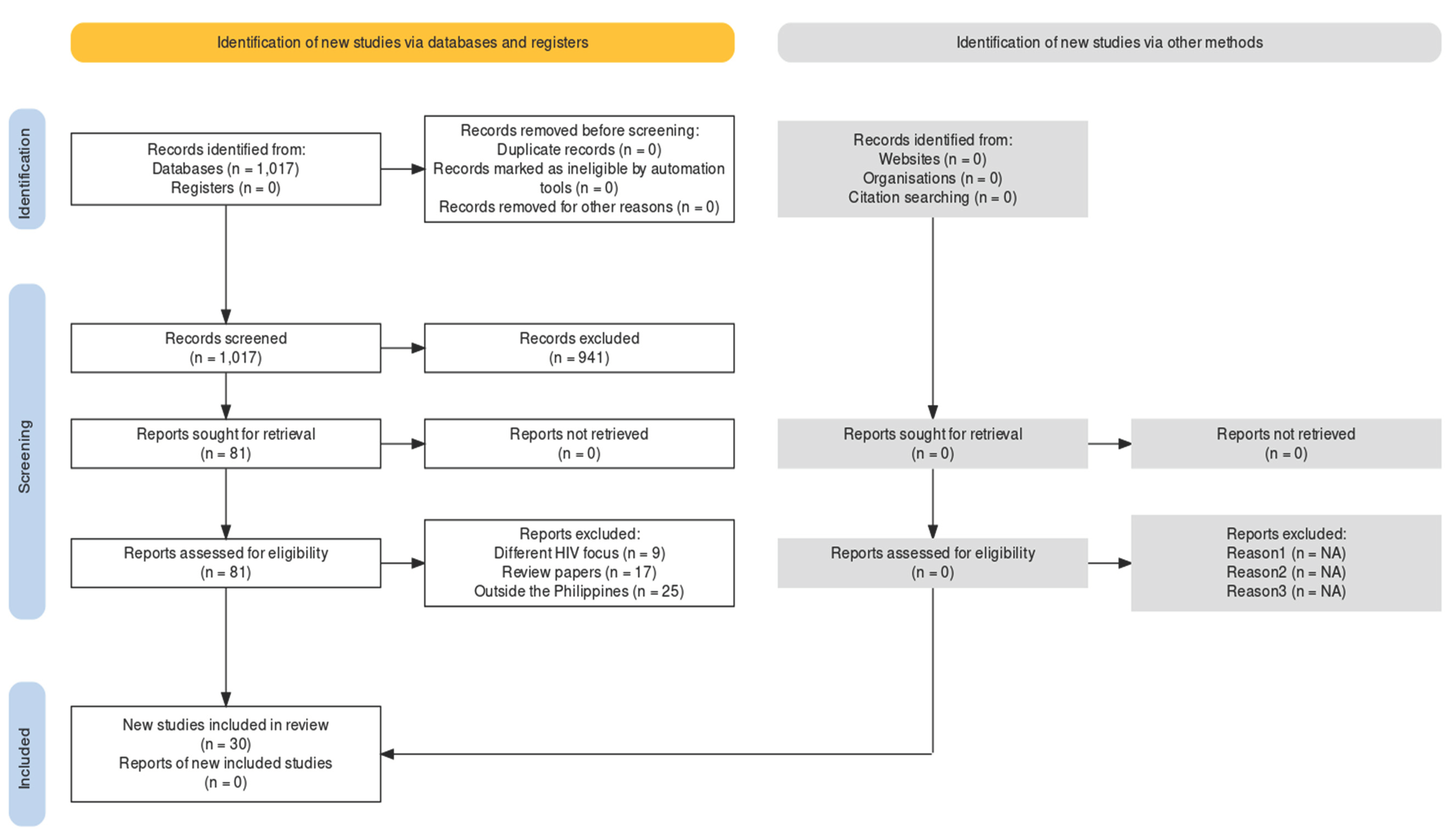

Table 1.
Characteristics of Included Studies.
| Characteristics | N=30 | Percentage(%) |
|---|---|---|
| Year of Publication 2014-2019 2020-2024 |
14 16 |
46.7 53.3 |
| Research Design Quantitative studies Qualitative studies |
17 13 |
56.7 43.3 |
| Population Men who have sex with men/gay men (with and without HIV) People living with HIV Women Community-based workers Healthcare professionals Key informants on HIV programs and policies Overseas Filipino workers Transgender women Prisoners |
12 9 3 3 3 3 2 2 1 |
40.0 30.0 10.0 10.0 10.0 10.0 6.70 6.70 3.33 |
Table 2.
Contributing Factors to the High HIV Incidence.
| Factors | N=30 | Percentage(%) |
|---|---|---|
| HIV Contributory factors Individual factors Sociocultural factors Economic factors Environmental factors Political factors Educational factors Biological factors |
21 19 13 11 7 4 2 |
70.0 63.3 43.3 36.7 23.3 13.3 6.67 |
Summary Table of Relevant Findings.
Table 3.
Summary of relevant findings from selected evidence.
| No. | Author | Year | Methods | Relevant findings | Factors contributing to high HIV incidence |
|---|---|---|---|---|---|
| 1 | Adams et al. | 2021 | Qualitative descriptive n=19 Gay and straight men |
Lack of awareness on prevention other than condoms, unprotected sex; low HIV testing (requirement of immigration process); lack of education, accessibility of healthcare resources, lack of quality information on HIV; shame and stigma; lack of regular check-ups | Individual, sociocultural, political, educational, environmental |
| 2 | Adia et al. | 2018 | Qualitative; n=21 HIV+ MSM, community-based HIV workers |
Stigma influences testing and leads to late diagnosis and causes barriers to access to healthcare; religious society | Sociocultural |
| 3 | Bijker et al. | 2017 | Quantitative; n=3,994 PLHIV in Asia (including the Philippines) and Africa |
Sub-optimal adherence (SOA) is 4.8% in Asia; SOA to treatment is higher in MSM and IVDU; LMICs have higher SOA | Individual, economic, environmental |
| 4 | Canoy & Ofreneo | 2017 | Qualitative n=20 HIV+ gay men |
Fear of disclosure to family, friends, and co-workers due to stigma; entering into same sex relationship for financial support; Catholic culture | Individual, sociocultural, economic |
| 5 | Calaguas | 2020 | Quantitative n=491 MSM, gay men |
MSM, marital status, gender expression, relationship status, their predominant sexual position, and the sexes of their sexual partners are significantly associated with the use or non-use of condoms during their last sexual intercourse. | Individual |
| 6 | Cheng et al. | 2016 | Quantitative n=1,912 Young adults |
Same sex behavior is a predictor of age at first sex, lifetime substance abuse particularly smoking, and drug use. | Individual, sociocultural |
| 7 | Deuba et al. | 2018 | Quantitative n=3,827 in 7 Asia-Pacific countries including the Philippines |
55% has partners who are HIV+, 35% and 10% unknown; 43% practiced inconsistent condom use with regular partner and 46% with a casual partner; Filipinos have the highest sexual risk behavior with 63% inconsistent condom use with regular partner and 60% with a casual partner; lack of condom availability; lack of awareness that condom is still needed if both partners are HIV+. Living in rural areas less likely to report inconsistent condom use. More likely to report inconsistent condom use: sex workers, partners who are HIV+, those who do not know their partner’s status. | Individual, sociocultural, environment, economic |
| 8 | De Irala | 2016 | Quantitative; n=8,994 4 countries including the Philippines |
Low knowledge on condom effectiveness in preventing HIV; peer pressure not to use condom, wanted to feel having sex without condom | Individual, sociocultural |
| 9 | De los Santos et al. | 2022 | Quantitative n=100 |
Health workers who lack awareness of HIV care are prone to discriminating against people with HIV. Health care workers gossip about gay people with HIV. The experience of stigma is more prevalent in RHUs than hospitals, polyclinics and private treatment hubs. | Sociocultural, environment |
| 10 | De Torres et al. | 2021 | Quantitative PLHIV |
9% were non-adherent to treatment; time and activity constraints were the primary reasons for lack of adherence to ART and scheduled clinic visits. | Individual |
| 11 | Estacio et al. | 2021 | Quantitative, cross-sectional; n=292 Sex workers |
Sex work engagement high among drug users, abused individuals, and problems with friends; low HIV testing and case finding | Individual, sociocultural |
| 12 | Gohil et al. | 2020 | Qualitative; n=57 Key informants on HIV policies and HIV test users, MSM, TGW |
Policy and regulatory issues (no policy on HIV self-testing), conservative culture; poor HIV knowledge, cost, fake test kits | Individual, political, sociocultural, economic |
| 13 | Hall et al. | 2020 | Quantitative; n=1,362 OFW in Hong Kong |
Reasons for not having HIV testing: No perceived need, unwillingness, and no time (work) | Individual, economic |
| 14 | Hollingshead et al. | 2020 | Qualitative virtual ethnography MSM, community, key informants |
Use of gay dating mobile apps makes sex partners more accessible | Individual, sociocultural |
| 15 | Jegonia | 2019 | Quantitative Nurses and physicians Sample not specified |
Marked stigma among healthcare workers correlates with care and services provided. Religion, profession, workplace, and years of experience were significantly correlated with stigma. Stigma is inversely related with level of care. | Individual, sociocultural, economic, environment |
| 16 | Melgar et al. | 2018 | Qualitative Records analysis |
Restrictive policies, conservative religious society | Political, sociocultural |
| 17 | Milallos & Cutamora | 2019 | Qualitative, Husserlian phenomenology, n=7 PLHIV | High-risk sex practices | Individual |
| 18 | Mosende et al. | 2023 | Quantitative n=171 health care workers |
Lack of knowledge on HIV transmission | Individual |
| 19 | Newman et al. | 2022 | Qualitative n=132 Youth and key informants |
Peer, family (fear of disclosure), school (lack of discussion on sexual issues; fragmentation between educational and healthcare systems), and healthcare factors (lack of gender-affirmative health services); stigma and negative beliefs about HIV | Sociocultural, political, educational |
| 20 | Noble & Austin | 2014 | Quantitative n=women in 80 less-developed countries |
Democracy encourages women’s participation in HIV programs, female empowerment measured by schooling, having birth attendant at delivery, and fertility rates influence contraceptives rates and HIV rates; GDP influences women empowerment; Muslim influences HIV prevalence | Sociocultural, economic, political |
| 21 | Ofreneo & Canoy | 2017 | Qualitative n=13 OFW |
Risk of infecting spouse upon return from overseas work | Individual, sociocultural, economic |
| 22 | Ofreneo et al. | 2021 | Qualitative n=105 MSM |
Low socioeconomic status bisexual, multiple sex partners are unsafe | Individual, sociocultural, economic |
| 23 | Palma & Parr | 2021 | Qualitative n=18 Female prisoners |
Prison management and practices increases HIV risk, low HIV knowledge, increased vulnerability before prison | Individual, environment |
| 24 | Pepito & Newton | 2020 | Quantitative, secondary data analysis n=16,155 Women |
Low HIV testing (2.4%); tobacco use, middle class, TV/internet access, rural area, Muslim were more likely to get tested | Individual, sociocultural, environment |
| 25 | Restar et al. | 2019 | Qualitative phenomenology n=15 Health care providers (HCP) |
Hesitancy in providing HIV services due lack of awareness and training on health needs of MSM and TGW, and unsure how to prioritize HIV services. | Environment, education |
| 26 | Restar et al. | 2020 | Qualitative n=30 MSM, TGW |
Friends, lack of education in schools, church, cost, accessibility | Sociocultural, education, economic, environmental |
| 27 | SahBandar et al. | 2017 | Quantitative n=110 PLHIV |
Low ART treatment rate (0.9%); high HIV prevalence in IVDU; drug-resistant HIV variants; limited resources | Individual, sociocultural, environment, biological, political |
| 28 | Salvana et al. | 2017 | Quantitative n=81 |
Shift in HIV molecular biology with more resistant HIV strain and increased local transmission, low consistent condom use, transactional sex, sex with HIV+ individuals | Biological, individual, sociocultural, economic |
| 29 | Seposo et al. | 2019 | Quantitative; n=9 Social hygiene clinics (SHC) |
Higher HIV prevalence in areas with suboptimal SHCs | Environmental, economic, political |
| 30 | Wong et al. | 2020 | Quantitative | High cost and inconsistent implementation of AIDS treatment package | Economic |
Note: ART-antiretroviral treatment; BPO-business process outsourcing; IVDU-intravenous drug users; LGU-local government unit; MSM-men who have sex with men; OFW-overseas Filipino workers; TGW-transgender women.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



