
Submitted:
03 April 2024
Posted:
03 April 2024
You are already at the latest version
Abstract
Quality of life (QoL) assessments are integral to cancer care, yet their effectiveness in providing essential information for supporting survivors varies. This study aimed to elucidate key indicators of QoL among colorectal cancer survivors from the perspective of healthcare professionals, and to evaluate existing QoL questionnaires in relation to these indicators. Two studies were conducted: a Delphi study to identify key QoL indicators and a scoping review of questionnaires suitable for colorectal cancer survivors. Fifty-four healthcare professionals participated in the Delphi study's first round, with 25 in the second. The study identified two primary QoL domains (Physical and Psychological) and 17 subdomains deemed most critical. Additionally, a review of 12 questionnaires revealed two instruments assessing the most important general domains. Findings underscored a misalignment between existing assessment tools and healthcare professionals' clinical priorities in working with colorectal cancer survivors. To enhance support for survivors' QoL, efforts are needed to develop instruments that better align with the demands of routine QoL assessment in clinical practice.
Keywords:
quality of life
; surveys and questionnaires
; adult oncology
; colorectal cancer survivors
; Delphi study
; scoping review
; expert consensus
1. Introduction
The burden of cancer incidence and mortality is rapidly growing, reflecting the population growth and aging, among other factors [1]. It is estimated that cancer burden will increase globally by almost 50% from 2020 to 2040 [1,2]. That is, while cancer death rate decreased significantly in the last few decades (e.g., in United States by 33 % from 1991 to 2020), the survival rates are increasing (e.g., for all types of cancer combined the 5-year relative survival rate increased from 49 % in the mid-1970’s to 68 % in the previous decade; [3]), which holds true also for generally more lethal cancers [4]. One of the most burdensome cancers is colorectal cancer, being the second leading cause of cancer-related death [1] and the third most common cancer in males and females [1,5] representing 10.7 % of new cases in 2020 [2] with its incidence still expected to grow [6]. With the current five-year survival rates in most developed countries ranging from 50 % to over 70 % [4,6,7] and increasing, the population of colorectal cancer survivors is also growing [8].
Cancer survivorship is being recognized as an essential component of cancer care [9]. However, the population of cancer survivors, i.e., those that have completed primary cancer treatment [7], often does start to suffer from physical disability, distress and reduced quality of life (QoL) over time [10,11]. The burden of cancer and cancer treatment is therefore not evident only in the morbidity and mortality, but also in the impact on survivors’ QoL in the long term [12]. Overall burden of cancer diagnosis, cancer symptomatology and other clinical characteristics (e.g., fatigue, difficulty sleeping, psychological challenges), and intensive treatment pattern (e.g., radiotherapy, chemotherapy, colostomy [5,13]) have been found to negatively impact various aspects of survivors’ QoL. 30 – 40 % cancer survivors report at least at least mild levels of anxiety and depression [14], that may interfere with the ability to effectively cope with cancer diagnosis, symptoms, and treatment. Additionally, cancer survivors suffer from negative impacts also on other areas of life directly linked to cancer, such as treatment adherence and healthcare utilization [15], but also importantly on various areas of QoL [12], e.g., physical, psychological, and social QoL. A recent meta-analysis [5] found that colorectal cancer survivors have a 51 % increased risk of experiencing depression after diagnosis and do experience high levels of anxiety and depression regarding health related QoL and mortality. Even though the major deterioration of health related QoL occurs during the first six months after diagnosis and treatment [8], many cancer survivors still report on negatively impacted QoL well into survivorship period [8,15]. Improving QoL of colorectal cancer survivors is important, not only from the survivors’ perspective to be provided with appropriate and tailored care, but also as the growing population of survivors is posing an increasing burden on health-care systems due to their persistent health problems and decreased levels of QoL [8,15]. This need is also reflected in the actions promoted by the European Commission, such as Mission Cancer recognizing the QoL as one of the most important areas of intervention [16], and EU Beating Cancer Plan urging to change focus from the length of life after diagnosis, to length and QoL after diagnosis [17].
With increasing attention on addressing the survivors’ QoL in research and clinical care (e.g., [18], important improvements have been made in focusing on what matters most to patients, together with providing insights into the importance of the aspects relevant to the health-care professionals (HCPs), even though these do not always completely align [12,19]. Of course, to improve QoL, it first needs to be measured. Routine assessment of QoL has been shown to have a role in improving outcomes, such as overall survival, functional outcomes, and health related QoL [12]. Additionally, such assessments have been repeatedly recommended as an important part of cancer care, meeting the patients’ needs to a broader extent than physical issues. This also contributes to ensuring that the appropriate further care and support is provided to the survivors [20].
Even though historically, QoL has not been addressed and assessed as rigorously as traditional disease-related outcomes (e.g., overall survival), important improvements have been achieved, especially in the last decade [12]. A plethora of questionnaires was developed for the assessment of QoL of cancer patients and survivors. These questionnaires differ in its intended population: from those for the general population and used in colorectal cancer population (e.g., SF-36v2 Health survey (SF-36v2), [21]; World Health Organization Quality-of-Life Scale (WHOQOL-BREF),[22], cancer survivors’ population (e.g. Quality of Working Life Questionnaire for Cancer Survivors (QWLQ-CS), [23]) to those colorectal cancer specific (e.g., Functional Assessment of Cancer Therapy – Colorectal (FACT-C), [24]) or specific to the subgroups of these survivors, such as those with stoma (e.g., Modified City of Hope Quality of Life – Ostomy questionnaire (mCOH-QOL-O); [25]), and in their scope from the assessment of general QoL and its main domains (e.g., WHOQOL-BREF, [22]) to those assessing a specific aspect of QoL (e.g., QWLQ-CS, [23]). They also heavily differ in their development process, i.e., the theoretical underpinnings they are based on, and which kind of cancer survivors’ samples were included in the validation process, as well as on the information that is available regarding their psychometric properties [26]. Varied characteristics and therefore the usability of available questionnaires make the selection of the most appropriate tool quite complex, presenting another barrier to the integration of the assessment and its outputs meaningfully into practice by HCPs, on top of already existing barriers, such as their lack of time and knowledge [27].
Therefore, the first aim of this study was to establish an expert consensus on the key domains of QoL of colorectal cancer survivors that HCPs identify as important in clinical practice. The first research question (RQ1), i.e., What is the expert consensus regarding the important QoL domains of colorectal cancer survivors?, was addressed in a modified two-stage Delphi study in which HCPs evaluated already established domains and subdomains of QoL depicting cancer survivors’ perspective. The second aim of the study was to review existing QoL questionnaires regarding their overlap of the domains assessed with the key domains identified in the Delphi study. The second research question (RQ2), i.e., What questionnaires exist for the assessment of QoL in colorectal cancer survivors and how do they correspond to the most important QoL domains by expert consensus?, was addressed in a scoping review study.
2. Study 1: Establishing Expert Consensus on Key Indicators of QoL in Colorectal Cancer Survivors
2.1. Materials and Methods
In Study 1, we followed a modified Delphi procedure which was already described in detail previously in study conducted on the QoL of breast cancer survivors [28]. The two-step procedure was adapted from related studies, such as Pietersma et al. [29] and Tung et al. [30]. In the first step, we identified a pool of domains and subdomains of QoL, and in the second, an interdisciplinary panel of experts participated in a two-round Delphi process, evaluating their importance in monitoring in the care of colorectal cancer survivors.
2.1.1. Identification of the Initial Pool of Quality of Life Domains and Subdomains
The first phase of a Delphi methodology most often consists of a survey on expert opinions on the topic [31,32], or it is customized to better suit the research problem [33]. Following the latter and a similar approach of Tung et al. [30], we chose a model of QoL in cancer survivors by Ferrel and colleagues [34] and its variations [35,36,37] as a theoretical basis for the identification of the initial pool of QoL domains and subdomains. First, we mapped the subdomains of the models and identified overlapping ones and those specific for each model. Second, eight clinical experts and researchers of the research team of project [name of the project hidden for review] (Project Acronym; [38]) reviewed the list of extracted (sub)domains, and added two subdomains, often observed in clinical practice (in Physical domain a subdomain of Health distress, and in Psychological domain Loss of interest in usual activities). The final list consisted of four QoL domains (i.e., Physical, Psychological, Social, and Spiritual) with 35 subdomains, which represented the questionnaire items of the 1st round of the Delphi process.
2.1.2. Evaluation of the Importance of (Sub)Domains
The second phase of Study 1 consisted of two rounds of evaluation of the importance of identified (sub)domains and was conducted in spring and fall of 2020. Potential participants received an email invitation with the explanation of the study and a link to the online questionnaire. Informed consent was sought before filling out the questionnaire. Participants constructed their own unique IDs following the provided instructions, by which their responses were followed through both rounds. The study was performed in accordance with the Helsinki Declaration and its amendments, and ethical standards of the institutional and national research committees.
Participants
An adapted method of Borgiel and colleagues ([39], see also [30]) was applied for the recruitment of HCPs involved in the follow-up of colorectal cancer survivors, i.e., members of the research team recruited professional peers to participate in the present study. In this phase, special attention was given to the recruitment of various HCP profiles (e.g., Oncologists, Physiotherapists, Nurses, Psychologists), from different European countries (i.e., Austria, Belgium, Latvia, Portugal, Slovenia, Spain, and Switzerland) due to the differences in healthcare systems and care paths for cancer survivors.
The Delphi studies usually include the same experts in all survey rounds of the study, which needed to be modified in the present study, as many of the participants of the 1st round were not available to participate in the 2nd round due to the COVID-19 pandemic. Therefore, as only 16,67 % of the participants of the 1st round participated in the 2nd round, we supplemented the sample of the 2nd round by inviting additional HCPs to participate following the same method as for the initial recruitment with the aim of obtaining more representative results. Altogether, 70 HCPs participated in Study 1.
Questionnaire
The questionnaire for the 1st round consisted of 4 domains and 35 subdomains of QoL identified in the preparatory phase of this study. Participants rated the importance of the (sub)domains in the follow-up of the colorectal cancer survivors on a 7-point scale (1 – not important; 7 – very important). (Sub)domains that reached consensus in the 1st round were retained to be evaluated in the 2nd round, where also the results for the 1st round in the form of the median answer and percentage of participants giving that answer were presented. Again, participants rated the importance of the retained (sub)domains on a 7-point scale in the 2nd round.
Consensus Criterion and Analyses
Most common approach for establishing the criterion for consensus in Delphi studies is to specify a percentage level of agreement, which in existing studies varies from 51 to 100 % [31,32]. Similar to Vanmeerbeek and colleagues [40] and Freitas and colleagues [41] we set the criterion at 75 % in the present study. For the 1st round, consensus for each item was reached when at least 75 % of participants agreed with the item as being important with top three scores on 7-point scale, while for the 2nd round consensus was reached when 75 % of participants evaluated the item within the top two scores on 7-point scale.
To assess the consistency of the participants’ ratings for each round, intraclass correlation coefficients (ICC) based on a mean-rating 2-way random effects model were calculated [42]. For assessing potential differences in two groups of participants in the 2nd round (i.e., those who participated already in the 1st round and new participants to the 2nd round), t-test were calculated. Analyses were conducted in R version 4.1.1 ([43]; packages psych [44], and rstatix [45]).
2.2. Results
2.2.1. Round 1
54 HCPs participated in the 1st round of the Delphi study (Table 1). Their inter-rater reliability was good [42] with ICC(2, 54) = 0.87, 95 % CI [0.82, 0.90].
The consensus was reached for three out of four general domains (75 %, i.e., Physical, Psychological, and Social domain; see Table 2), and for 31 out of 35 subdomains (88,6 %). Within Physical and Psychological domains, all of the subdomains reached consensus (i.e., 10, 100.0 % for both), while in the Social domain 8 out of 10 subdomains (80.0 %) reached consensus. In the Spiritual domain, none of the subdomains reached consensus in the 1st round.
2.1.2. Round 2
In the 2nd round of the Delphi study 25 HCPs participated (Table 1). 9 of them already participated in the 1st round (Group 1), while 16 participants were newly recruited only to participate in the 2nd round (Group 2). The reliability of all participants’ ratings was good [42] with ICC(2, 25) = 0.87, 95 % CI [0.81, 0.92]. Independent samples t-tests (see Table 2) revealed no significant differences of the mean evaluations of the QoL (sub)domains between the two groups, therefore we present the results on the reached consensus for all of the participants of the 2nd round together.
The consensus was reached for two out of three general domains (66.7 %, i.e., Physical and Psychological domains; see Table 2), and for 11 out of 31 subdomains (35.5 %). Within the Physical domain, 6 out of 10 subdomains reached consensus (60.0 %), within the Psychological domain 3 out of 10 (30.0 %), and within the Social domain none of the subdomains reached consensus in the 2nd round.
After two rounds of the Delphi process, most important QoL (sub)domains for monitoring in the follow-up of colorectal cancer survivors by experts’ opinion were identified. On the level of the QoL domains consensus was reached for Physical and Psychological domains, and on the level of subdomains, the following were identified as most important: Functional ability and mobility, Activities of daily living, Fatigue/vitality, Pain and discomfort, Physical symptoms, and Physical health and comorbidities (all from the Physical domain), and Depression, Psychological distress, and Loss of interest in usual activities (from Psychological domain).
3. Study 2: Scoping Review of Quality of Life Questionnaires for Colorectal Cancer Survivors
3.1. Materials and Methods
3.1.1. Overview
Conducting this scoping review, the methodological framework by Arksey and O’Malley (47) and Levac and colleagues [48] was followed. It proposes six stages: (1) identifying the research question, (2) identifying the relevant studies, (3) study selection, (4) charting the data, (5) collating, summarizing, and reporting results, and (6) consultation exercises. Ensuring that the process was transparent, complete, and systematic, PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews [49]) was followed.
3.1.2. Identifying the Research Questions
First, following the aim of the paper, we formed specific research questions (RQs) to guide the scoping review:
- -
- RQ2a: Which quality of life questionnaires for colorectal cancer survivors exist?
- -
- RQ2b: What domains of quality of life do they assess?
- -
- RQ2c: How do the identified domains of reviewed quality of life questionnaires overlap with the identified key indicators of quality of life by expert consensus?
3.1.3. Identifying Relevant Studies
For identifying the relevant papers, three large and commonly used databases, i.e., SCOPUS, Web of Science, and PubMed, were used. We conducted a preliminary search in all three databases, helping us to refine the search strategy and ensuring that coverage of the topic was adequate. We performed the main search on August 29, 2022.
Our search strategy combined terms related to colorectal cancer (“colorectal cancer”, “colon cancer”), quality of life (“quality of life”, quality-of-life, well-being), questionnaires (questionnaire, scale, survey, instrument, “measurement tool”, “assessment tool”, assessment), psychometric validation (validation, psychometric), and survivorship (survivor*). We excluded all types of reviews (review, meta-analysis, “state of the art”, state-of-the-art), and limited our search to papers in English, and published from the year 2000 forward to limit the results to the more recent questionnaires. Listed groups of keywords were combined into a nested format using Boolean operators (AND, OR, NOT). Titles, abstracts, and keywords were searched. The example of final search string for SCOPUS is: “TITLE-ABS-KEY ( ( "colorectal cancer" OR "colon cancer" ) AND ( "quality of life" OR "quality-of-life" OR "well-being" ) AND ( questionnaire OR scale OR survey OR instrument OR "measurement tool" OR "assessment tool" OR "assessment" ) AND ( validation OR psychometric ) AND ( survivor* ) AND NOT ( review OR meta-analysis OR "state of the art" OR state-of-the-art ) ) AND LANGUAGE ( english ) ) AND PUBYEAR > 1999”. We also performed an additional search in Google Scholar using different combinations of search terms, as this could lead to the identification of additional unique papers [50].
Inclusion and exclusion criteria were formed on the basis of our research questions and were set a priori. These required studies to be (1) published (i.e., excluding preprints and other unpublished papers), and (2) provide sufficient information regarding the questionnaire (at least dimensionality or subscales information), and were required not to (3) focus on any other constructs than quality of life (or health-related quality of life), (4) include questionnaires specific for other types of cancer (but allowing for general cancer-related quality of life questionnaires), (5) be intended to use with patients with cancer (only cancer survivors or both, patients and survivors), and (6) be focusing on children or adolescents. Since the aim of this review was to review what quality of life questionnaires for colorectal cancer survivors do exist and what they measure, we did not exclude primary studies based on their methodological quality [47].
3.1.4. Identifying Relevant Studies
Citations of all the records identified (i.e., 45 papers, Figure 1) in the electronic databases were exported to Excel spreadsheets (Microsoft Inc). After duplicate records were removed, 33 titles and abstracts were screened independently by two authors (US and CL) to exclude irrelevant papers. After this step, two authors (US and CL) independently reviewed full texts of the remaining papers and excluded papers not complying to the inclusion and exclusion criteria. Disagreements in each of the stages were settled through discussion. In the process of full-text reviews, one additional eligible paper was identified. The process resulted in 15 papers containing information on 12 questionnaires that fulfilled the predetermined criteria and were included in the scoping review.
3.1.5. Charting the Data
For charting the data, we formed a spreadsheet based on research questions, determining variables to be extracted from the reviewed papers. The following data was extracted from each paper: (1) authors, (2) year of publication, (3) type of paper (e.g., original questionnaire development/validation paper, questionnaire adaptation paper), (4) name of the questionnaire reported on in the paper, (5) construct for which the questionnaire is intended to measure, (6) subscales/dimensions of the questionnaire and their descriptions, (7) number of items by subscales and in total, (8) response scale format, (9) focus population for the use of the questionnaire (e.g., cancer survivors in general, only colorectal cancer survivors), (10) language of the questionnaire. The process of data extraction was completed by one author (SAC) and reviewed by another (US) in an iterative process during the review of the papers. The final chart was used for the analysis of the extracted information.
3.1.6. Collating, Summarizing, and Reporting Results
After charting the data, information on questionnaires were summarized in order to address the first two research questions of this study, i.e., to identify what QoL questionnaires for colorectal cancer survivors exist and which domains of QoL they assess. Preparation of this part of the study was done by US.
3.1.7. Consultation Exercises
The finals step in the proposed methodological framework for scoping reviews [47,48] proposes the (optional) consultation exercises with experts or stakeholders in the topic. For the purpose of this study, the final step was adapted to address the third research question of this study, i.e., to explore how the identified domains in the reviewed QoL questionnaires for colorectal cancer survivors correspond to the key indicators of QoL identified in the Delphi study. This final step of the study was performed by US.
3.2. Results
3.2.1. Characteristics of the Reviewed Questionnaires
The final selection of this review included 12 questionnaires that were identified in 15 studies (Table 3). In the following sections, we will be commenting only on questionnaires, not studies, with the exception of instances where studies provided differing information on the same questionnaire. The inclusion criteria for the papers and questionnaires to be included in the review stated that the questionnaire needs to assess (health-related) quality of life. In the selection process a slightly loose approach towards that criterion was taken, as there are several constructs that are heavily overlapping with the QoL construct. As such, the final selection consists of seven questionnaires assessing QoL [22,24,25,51,52,53,54,55,56,57,58,59,60,61], two assessing Functional health and well-being [21,57,58], one Well-being [24], one Experienced burden and lifestyle parameters [62], and one Quality of life in the work domain [23].
The target population of questionnaires varies slightly among them. Most (i.e., 6 out of 12) of the questionnaires are intended to be used with adult patients with colorectal cancer (i.e., Assessment of Burden of Colorectal Cancer – tool (ABCRC), European Organisation for Research and Treatment of Cancer, Quality of Life Questionnaire for Colorectal Cancer-38 (EORTC QLQ-CR38), European Organisation for Research and Treatment of Cancer, Quality of Life Questionnaire for Colorectal Cancer-29 (EORTC QLQ-CR29), FACT-C, mCOH-QOL-O). Three of the questionnaires are intended to be used with adult patients and/or cancer survivors (i.e., European Organisation for Research and Treatment of Cancer, Quality of Life of Cancer Patients, version 3 (EORTC QLQ-C30), Quality of Life in Adult Cancer Survivors questionnaire (QLACS); QWLQ-CS), of which one (i.e., EORTC QlQ-C30) was also validated in the population of patients with colorectal cancer. Similarly, another questionnaire (i.e., European Organisation for Research and Treatment of Cancer, Quality of Life Questionnaire – Elderly Cancer Patients Module (EORTC QLQ-ELD14)) intended to be used with ageing patients with cancer and has also been validated in a group of ageing patients with colorectal cancer. Among the reviewed questionnaires, there were three originally intended for assessing QoL in general population, that have also been validated in population of patients with colorectal cancer (SF-36v2, SF-12v2 Health Survey (SF-12v2), WHOQOL-BREF). There were also two questionnaires, i.e., ABCRC and mCOH-QOL-O, suitable for patients with anastomosis and/or stoma, the first one for cancer patients, and the latter for patients with or without cancer.
Other characteristics of the questionnaires, such as number of items, response scale, and languages of the reviewed questionnaires, are provided in Table 3.
3.2.2. Overview of the QoL Domains Assessed by Reviewed Questionnaires
In this section, we provide an overview of the QoL domains addressed by the reviewed questionnaires and relate them to the key indicators of QoL that were identified in the Delphi study.
On the level of general domains (Supplemental Table 1), six out of 12 questionnaires had specific subscales or items addressing this level of QoL. Three of them assessed general QoL, seven Physical Health and Well-being domain, two Psychological Health and Well-being, three Social Health and Well-being, and two Spiritual Health and Well-being. In the Delphi study on the level of general domains, Physical and Psychological Health and Well-being were identified as important indicators of QoL. Questionnaires that do assess both domains are mCOH-QOL-O and WHOQOL-BREF. Additionally, several questionnaires assess only the Physical Health and Well-being among the identified key indicators, i.e., EORTC QLQ-C30, FACT-C, mCOH-QOL-O, SF-36v2, SF-12v2 and WHOQOL-BREF.
In the following text we focus on the overview of subdomains of QoL. Within the Physical Health and Well-being domain (Supplemental Table 2), nine questionnaires assess at least one of the subdomains (or a part of a subdomain) included in Study 1, while eight questionnaires also assess other subdomains of Physical Health and Well-being outside of those of Study 1. Focusing first on the subdomains identified in the Delphi study as key indicators, two questionnaires assessed Functional ability and mobility (i.e., ABCRC and EORTC QLQ-ELD14), one Activities of daily living (i.e., ABCRC), five Fatigue/vitality (i.e., ABCRC, EORTC QLQ-C30, QLACS, SF-36v2, SF-12v2), five Pain and discomfort (i.e., EORTC QLQ-C30, EORTC QLQ-CR29, QLACS, SF-36v2, SF-12v2), four Physical symptoms (i.e., ABCRC, EORTC QLQ-C30, EORTC QLQ-CR38, EORTC QLQ-CR29), and none of them Physical health and comorbidities. While none of the questionnaires assess all six subdomains identified as key indicators in the Delphi study, most of them, i.e., 4, are assessed by ABCRC questionnaire. Other questionnaires assess one or two of the key subdomains. Additionally, some questionnaires also assess other Physical Health and Well-being subdomains that were not identified as key indicators. These are Sleep and rest assessed by one questionnaire, Health perceptions assessed by two questionnaires, Weight loss/gain assessed by one questionnaire.
Within the Psychological Health and Well-being domain (Supplemental Table 3), three subdomains were identified as key indicators in Delphi 1 study, i.e., Depression, Psychological Distress, and Loss of interest in usual activities. Among reviewed questionnaires, only one assesses at least one of these subdomains, i.e., EORTC QLQ-ELD14 questionnaire that assesses Psychological distress. Other questionnaires assess subdomains that were not identified as key indicators: Anxiety is assessed by one questionnaire, Cognitive functioning and concentration by three, and other subdomains considered by only one of the questionnaires include: Uncertainty, Fear of recurrence, Isolation/abandonment and feelings of belonging, Positive feelings and affect, Negative feelings and affect. Six questionnaires also assessed other subdomains that were not included in Study 1.
Within the Social Health and Well-being domain (Supplemental Table 4), none of the subdomains were identified as key indicators in the Delphi study. Among other subdomains, Family functioning is assessed by two questionnaires, Marital functioning by one, Affection/Sexuality by none, Self-concept/Appearance by four, Enjoyment/leisure (participation and opportunities) by none, Social activity and limitations by one, Financial concerts by three, Social support by none, Employment by two, and Role limitations due to health or physical problems by three questionnaires. Five questionnaires also assessed other subdomains that were not included in Study 1.
Within the Spiritual Health and Well-being domain (Supplemental Table 5), none of the subdomains were identified as key indicators in the Delphi study. Also, none of the reviewed questionnaires assessed any of the subdomains.
Reviewed questionnaires also assessed other (sub)domains of QoL, that we were not able to classify under any of general domains, which is presented in Supplemental Table 6.
4. Discussion
With the growing population of colorectal cancer survivors [8], the focus in their clinical care and support is shifting towards the recognition of the importance of their QoL [16,17] consequently raising a need for regular assessments and monitoring of QoL that are necessary to detect areas that might need to be addressed for each individual patient. Even though several barriers to the implementation of such assessments in the clinical routine persist [27], identifying the QoL domains that are of utter importance not only to the survivors, but also to their HCPs, along with providing the appropriate questionnaires that address those domains, is critical to assist this process. Therefore, in the present study, we established an expert consensus on the key domains of QoL of colorectal cancer survivors in a modified Delphi study and reviewed the existing QoL questionnaires for this population regarding their correspondence to the identified key QoL domains.
In the Delphi study, the expert consensus regarding the QoL general domains has been reached for Physical and Psychological domains. HCPs also evaluated QoL subdomains where the consensus was reached for the following subdomains of Physical domain: Functional ability and mobility, Activities of daily living, Fatigue/vitality, Pain and discomfort, Physical symptoms, and Physical health and comorbidities, and for the following subdomains of Psychological domain: Depression, Psychological distress, and Loss of interest in usual activities. In the scoping review study of existing QoL questionnaires, 12 of them were identified and the domains that they assessed were mapped onto the list of (sub)domains that were evaluated by HCPs in the Delphi study. On the level of general domains, only two questionnaires assess both domains that were identified as important by HCPs, i.e., mCOH-QOL-O [25] and WHOQOL-BREF [22]. On the level of Physical QoL subdomains, none of the questionnaires addresses all key subdomains, but most of them, i.e., 4 out of 6, are covered by ABCRC questionnaire [62], while some other questionnaires assess one or two key subdomains (see Supplemental Table 1). On the level of Psychological QoL subdomains, no questionnaire addressed all three key subdomains and only one, i.e., EORTC QLQ-ELD14 [56], addressed one of these three subdomains. On the level of Social and Spiritual QoL subdomains for none of them the consensus was reached in the Delphi study, however, several of the questionnaires addressed the Social, but none addressed Spiritual QoL subdomains. It is also important to note that most of the reviewed questionnaires also assess several other (sub)domains that were not identified as important in the clinical routine for the HCPs in our study, which does not mean that they are not important for the survivors or in some other contexts.
Following the results of this study, we can conclude that two questionnaires, mCOH-QOL-O [25], and WHOQOL-BREF [22], address both key general domains, and on the level of subdomains, ABCRC [62] and EORTC QLQ-ELD14 [56] assess the most of those identified as key by HCPs, while none of them addresses them all. Even though there is a lot of room left for improvement in the assessment of cancer survivors’ QoL [12], the reason for relatively low correspondence between HCPs’ identified key QoL domains and domains addressed by the reviewed questionnaires could lie in the fact that in the Delphi study involved various profiles of HCPs. As these results represent a wide and general consensus among several professional profiles that are in contact with colorectal cancer survivors in clinical routine, it would be worth to explore whether the key domains identified differ among these profiles which may reflect the specific focus regarding the survivors’ health aspects.
Nevertheless, questionnaires that provide the information most needed by HCPs regarding survivors’ QoL are important. Beyond the QoL domains that they provide information on, they of course, need to be psychometrically validated and standardized, which was not the focus of the present study. However, metric characteristics should be evaluated before any of these questionnaires is implemented [12]. For instance, of the two questionnaires that address both key general domains, WHOQOL-BREF is provided with a plethora of studies and evidence in support of its psychometric quality in several languages and populations [22,63,64,65], while mCOH-QOL-O is much less supported in this regard. In both cases, however, additional studies on the population of colorectal cancer survivors would substantially benefit their justified use in this population.
High quality questionnaires that address the domains that are of the highest importance for both, survivors and HCPs, can aid in providing appropriate care and support in the areas needed, especially if they can be integrated in the clinical routine. However, the appropriateness of most of the reviewed questionnaires for frequent assessments is questionable, i.e., questionnaires contain from 27 up to 107 items (except for EORTC QLQ-ELD14 and SD-12v2 which contain 14 and 12 items, respectively), and as such present an additional burden for the survivors if requested to be filled in regularly. Therefore, before integration in the regular assessment, developing shorter, but still telling versions of appropriate questionnaires would be beneficial to have a strong potential to be employed in evaluating outcomes of colorectal cancer survivors [66]. Such efforts might be additionally supported by other advances in the field, e.g., prediction models of individuals with heightened risk of lowered QoL levels [8], adaptive approaches to assessing QoL dimensions [67], and even research in quality measurements in health care [68].
4.1. Limitations of the Study
While the current paper offers a valuable contribution to the area of assessment of QoL with colorectal cancer survivors, its findings are limited due to the following aspects: The Delphi procedure employed in the first study deviated from the standard Delphi methodology [31,32] in the sample of participants involved, as there was relatively low overlap in the samples of both rounds. However, since the outcomes of Delphi studies do not necessarily represent the opinions of all experts due to relatively small sample sizes [30], the inclusion of additional experts in the second round could aid in achieving a higher-level of generalizability. This is additionally supported by the inclusion of international and multidisciplinary sample. Therefore, our results represent a consensus on key QoL domains in clinical routine of various HCP profiles. To establish a consensus specific for each HCP profile involved in the clinical care of colorectal cancer survivors, further studies are needed. Similarly, as age and length of survivorship are important variables in the QoL of cancer survivors [69], the specifics in the most important QoL domains to be monitored may also vary depending on these factors, therefore further studies are needed. In the scoping review study of current QoL questionnaires for colorectal cancer survivors, we have not assessed the psychometric quality of these questionnaires [12]. Therefore, for each of the questionnaires discussed in this paper, researchers/HCPs need to explore their characteristics before employing them in their work with colorectal cancer survivors.
5. Conclusions
The first part of the current study established an expert consensus on QoL domains of colorectal cancer survivors most important in clinical practice from the HCPs perspective via two-round process of a Delphi study. The results show that consensus was reached on the Physical and Psychological domains, and on 17 of 30 subdomains, all within the Physical and Psychological domains. In the second part, i.e., scoping review, 12 QoL questionnaires were identified and reviewed regarding their correspondence to the domains identified in the Delphi study. On the level of general domains, there are two questionnaires that assess Physical and Psychological domain. On the level of subdomains, none of the questionnaires assess all key domains established in the Delphi study, but several of them are appropriate for assessing a few of these subdomains. The findings of this study clearly point to the relative mismatch between currently available assessment tools and the areas HCPs are most interested in during their clinical work with colorectal cancer survivors. Therefore, this study may serve as an indicator of what kind of questionnaires would serve the HCPs better, which could also aid in the process of integration of routine QoL assessments in monitoring the colorectal cancer survivors, to enhance the efforts of health care to aid and support survivors’ QoL.
Author Contributions
Conceptualization, Urška Smrke, Catherine Loly, Jean-Paul Calbimonte, Simon Lin, Alberto Sánchez, Sara Tement and Izidor Mlakar; Data curation, Urška Smrke, Sara Abalde-Cela, Catherine Loly and Liliana Pires; Formal analysis, Urška Smrke, Sara Abalde-Cela and Izidor Mlakar; Funding acquisition, Sara Abalde-Cela, Catherine Loly, Jean-Paul Calbimonte, Liliana Pires, Simon Lin, Alberto Sánchez and Izidor Mlakar; Investigation, Urška Smrke, Sara Abalde-Cela, Catherine Loly, Liliana Pires and Izidor Mlakar; Methodology, Urška Smrke, Simon Lin, Sara Tement and Izidor Mlakar; Writing – original draft, Urška Smrke, Jean-Paul Calbimonte and Izidor Mlakar; Writing – review & editing, Urška Smrke, Sara Tement and Izidor Mlakar. All authors have read and agreed to the published version of the manuscript.
Funding
This work received funding from the European Union Horizon 2020 Research and Innovation Program, the project PERSIST, supported under Grant Agreement no. 875406, and was partially funded by Research Programme Advanced methods of interaction in telecommunication (grant number: P2-0069). The content of this paper does not reflect the official opinion of the European Union or any other institution. Responsibility for the information and views expressed therein lies entirely with the authors.
Institutional Review Board Statement
This study is part of a clinical study carried out under the project PERSIST, a study protocol registered under ISRCTN97617326, for which ethical approvals were obtained from the Institutional Ethics Committee of CHU de Liège (Approval Ref. No: 2020/248), the Riga Eastern Clinical University Hospital Support Foundation Medical and Biomedical Research Ethics Committee (Approval Ref. No: 8-A/20), the National Ethics Committee, Ministry of Health, Slovenia (Approval Ref. No. 0120-352/2020/5), and the Pontevedra-Vigo-Ourense Research Ethics Committee (Approval Ref. No. 2020/394).
Informed Consent Statement
Informed consent of the participants of the Delphi study was sought at the beginning of the study. All procedures in this study were performed in accordance with the ethical standards of the Institutional and National Research Committees and with the Helsinki Declaration and its amendments.
Data Availability Statement
The dataset used and analyzed during the current study is available from the corresponding author upon reasonable request.
Acknowledgments
Not Applicable
Conflicts of Interest
The authors declare no conflict of interest. At the time of submission, Simon Lin was employed by Symptoma and Sara Abalde-Cela and Liliana R. Pires were employed by RUBYnanomed. These had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Appendix A: Supplemental Tables

Supplemental Table 1.
Questionnaires’ QoL areas of assessment and key QoL indicators – general QoL domains.
Supplemental Table 1.
Questionnaires’ QoL areas of assessment and key QoL indicators – general QoL domains.
| QoL domain | Consensus reached in Study 1 | ABCRC | EORTC QLQ-C30 | EORTC QLQ-CR38 | EORTC QLQ-CR29 | EORTC QLQ-ELD14 | FACT-C | mCOH-QOL-O | QLACS | QWLQ-CS | SF-36v2 | SF-12v2 | WHOQOL-BREF | ||
| a | b | a | b | ||||||||||||
| Physical Health and Well-being | * | X | X | X | X | X | X | X | |||||||
| Psychological Health and Well-being | * | X | X | X | |||||||||||
| Social Health and Well-being | X | X | X | ||||||||||||
| Spiritual Health and Well-being | X | X | |||||||||||||
| General QoL | X | X | X | ||||||||||||
| QoL areas assessed | |||||||||||||||
| … of all domain areas of Study 1 (4 + 1 general QoL)) | 2 | 1 | 2 | 3 | 5 | 1 | 1 | 3 | |||||||
| … of areas of consensus reached in Study 1 (2) | 1 | 1 | 2 | 2 | 1 | 1 | 2 | ||||||||
Notes. Questionnaires’ references: ABCRC (62); EORTC QLQ-C30 (51,52)M; EORTC QLQ-CR38 (24); EORTC QLQ-CR29 ver. A (53,54); EORTC QLQ-CR29 ver. B (55); EORTC QLQ-ELD14 (56) ; FACT-C (24); mCOH-QOL-O ver. A (25); mCOH-QOL-O ver. B (57,58); QLACS (59–61); QWLQ-CS (23); SF-36v2 (21,58); SF-12v2 (57); WHOQOL-BREF (22).
Supplemental Table 2.
Questionnaires’ QoL areas of assessment and key QoL indicators – physical QoL domain.
Supplemental Table 2.
Questionnaires’ QoL areas of assessment and key QoL indicators – physical QoL domain.
| QoL domain | Consensus reached in Study 1 | ABCRC | EORTC QLQ-C30 | EORTC QLQ-CR38 | EORTC QLQ-CR29 | EORTC QLQ-ELD14 | FACT-C | mCOH-QOL-O | QLACS | QWLQ-CS | SF-36v2 | SF-12v2 | WHOQOL-BREF | ||
| a | b | a | b | ||||||||||||
| Functional ability and Mobility | * | X | X | ||||||||||||
| Activities of daily living | * | X | |||||||||||||
| Fatigue/Vitality | * | X | X | X | X | X | |||||||||
| Sleep and rest | X | ||||||||||||||
| Pain and discomfort | * | X | X | X | X | X | |||||||||
| Abdominal pain | X | ||||||||||||||
| Buttock pain | X | ||||||||||||||
| Health perceptions | X | X | |||||||||||||
| Physical symptoms | * | X | |||||||||||||
| General gastrointestinal | X | X | |||||||||||||
| Hair loss | X | X | |||||||||||||
| Dry mouth | X | X | |||||||||||||
| Dyspnea | X | ||||||||||||||
| Taste problems | X | X | |||||||||||||
| Nausea, vomiting | X | ||||||||||||||
| Skin problems | X | X | |||||||||||||
| Urinary problems | X | ||||||||||||||
| Urinary frequency | X | ||||||||||||||
| Urinary incontinence | X | ||||||||||||||
| Painful urination | X | ||||||||||||||
| Stool frequency | X | ||||||||||||||
| Defecation problems | X | X | |||||||||||||
| Stool irregularities | X | ||||||||||||||
| Constipation | X | ||||||||||||||
| Diarrhea | X | ||||||||||||||
| Faecal incontinence | X | X | |||||||||||||
| Intoxications | X | ||||||||||||||
| Bloated abdomen | X | X | |||||||||||||
| Flatulence | X | ||||||||||||||
| Health distress | |||||||||||||||
| Weight loss/gain | X | X | |||||||||||||
| Physical Health and comorbidities | * | ||||||||||||||
| Other in physical domain | |||||||||||||||
| Appetite, nutrition | X | X | |||||||||||||
| Sexual enjoyment | X | ||||||||||||||
| Sexual functioning | X | ||||||||||||||
| Sexual problems | X | ||||||||||||||
| Sexual dysfunction, impotence | X | X | X | ||||||||||||
| Sexual interest | X | X | |||||||||||||
| Dysapreunia | X | X | |||||||||||||
| Disease-specific effects on physical well-being | X | ||||||||||||||
| Change in health | X | ||||||||||||||
| QoL areas assessed | |||||||||||||||
| … of all domain areas of Study 1 (10) | 4 | 3 | 1 | 2 | 2 | 1 | 2 | 3 | 3 | ||||||
| … of areas of consensus reached in Study 1 (6) | 4 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | |||||||
| … of ‘Other’ domain areas (9) | 1 | 1 | 3 | 3 | 3 | 1 | 1 | 1 | |||||||
Notes. Italic QoL areas are the ones additionally identified in the questionnaires of Study 2, but are not present in Study 1 QoL area pool.Questionnaires’ references: ABCRC (62); EORTC QLQ-C30 (51,52)M; EORTC QLQ-CR38 (24); EORTC QLQ-CR29 ver. A (53,54); EORTC QLQ-CR29 ver. B (55); EORTC QLQ-ELD14 (56) ; FACT-C (24); mCOH-QOL-O ver. A (25); mCOH-QOL-O ver. B (57,58); QLACS (59–61); QWLQ-CS (23); SF-36v2 (21,58); SF-12v2 (57); WHOQOL-BREF (22).
Supplemental Table 3.
Questionnaires’ QoL areas of assessment and key QoL indicators – psychological QoL domain.
Supplemental Table 3.
Questionnaires’ QoL areas of assessment and key QoL indicators – psychological QoL domain.
| QoL domain | Consensus reached in Study 1 | ABCRC | EORTC QLQ-C30 | EORTC QLQ-CR38 | EORTC QLQ-CR29 | EORTC QLQ-ELD14 | FACT-C | mCOH-QOL-O | QLACS | QWLQ-CS | SF-36v2 | SF-12v2 | WHOQOL-BREF | ||
| a | b | a | b | ||||||||||||
| Anxiety | X | X | |||||||||||||
| Depression | * | ||||||||||||||
| Psychological distress | * | X | |||||||||||||
| Cognitive functioning, concentration and attention | X | X | X | ||||||||||||
| Uncertainty | X | ||||||||||||||
| Fear of Recurrence | X | ||||||||||||||
| Isolation/Abandonment and feelings of belonging | |||||||||||||||
| Positive feelings and affect | X | ||||||||||||||
| Negative feelings and affect | X | ||||||||||||||
| Loss of interest in usual activities | * | ||||||||||||||
| Other in psychological domain | |||||||||||||||
| General mental health | X | X | |||||||||||||
| Emotional functioning and well-being | X | X | X | ||||||||||||
| Disease-specific effects on psychological well-being | X | ||||||||||||||
| QoL areas assessed | |||||||||||||||
| … of all domain areas of Study 1 (10) | 1 | 1 | 1 | 1 | 1 | 1 | 4 | ||||||||
| … of areas of consensus reached in Study 1 (3) | 1 | ||||||||||||||
| … of ‘Other’ domain areas (3) | 1 | 1 | 1 | 1 | 1 | 1 | |||||||||
Notes. Italic QoL areas are the ones additionally identified in the questionnaires of Study 2, but are not present in Study 1 QoL area pool. Questionnaires’ references: ABCRC (62); EORTC QLQ-C30 (51,52)M; EORTC QLQ-CR38 (24); EORTC QLQ-CR29 ver. A (53,54); EORTC QLQ-CR29 ver. B (55); EORTC QLQ-ELD14 (56) ; FACT-C (24); mCOH-QOL-O ver. A (25); mCOH-QOL-O ver. B (57,58); QLACS (59–61); QWLQ-CS (23); SF-36v2 (21,58); SF-12v2 (57); WHOQOL-BREF (22).
Supplemental Table 4.
Questionnaires’ QoL areas of assessment and key QoL indicators – social QoL domain.
Supplemental Table 4.
Questionnaires’ QoL areas of assessment and key QoL indicators – social QoL domain.
| QoL domain | Consensus reached in Study 1 | ABCRC | EORTC QLQ-C30 | EORTC QLQ-CR38 | EORTC QLQ-CR29 | EORTC QLQ-ELD14 | FACT-C | mCOH-QOL-O | QLACS | QWLQ-CS | SF-36v2 | SF-12v2 | WHOQOL-BREF | ||
| a | b | a | b | ||||||||||||
| Family functioning | X | X | |||||||||||||
| Martial functioning | X | ||||||||||||||
| Affection/Sexuality | |||||||||||||||
| Self Concept/Appearance | X | X | X | X | |||||||||||
| Enjoyment/Leisure (participation and opportunities) | |||||||||||||||
| Social activity and limitations | X | ||||||||||||||
| Financial Concerns | X | X | X | ||||||||||||
| Social Support | |||||||||||||||
| Employment | X | X | |||||||||||||
| … general feelings about working life | X | ||||||||||||||
| … job characteristics | X | ||||||||||||||
| … social structure and culture | X | ||||||||||||||
| … contact with supervisor | X | ||||||||||||||
| … contact with other actors at work | X | ||||||||||||||
| … organisational characteristics | X | ||||||||||||||
| … work perceptions | X | ||||||||||||||
| … effects of the disease and treatment (on work) | X | ||||||||||||||
| Role limitations due to health or psychical problems | X | ||||||||||||||
| … due to physical problems | X | X | |||||||||||||
| … due to emotional problems | X | X | |||||||||||||
| Other in social domain | |||||||||||||||
| Social adjustment to ostomy | X | ||||||||||||||
| Social functioning | X | X | X | ||||||||||||
| QoL areas assessed | |||||||||||||||
| … of domain areas of Study 1 (10) | 4 | 2 | 1 | 1 | 1 | 4 | 1 | 1 | 1 | ||||||
| … of ‘Other’ domain areas (2) | 1 | 1 | 8 | 1 | 1 | ||||||||||
Notes. Italic QoL areas are the ones additionally identified in the questionnaires of Study 2, but are not present in Study 1 QoL area pool. Questionnaires’ references: ABCRC (62); EORTC QLQ-C30 (51,52)M; EORTC QLQ-CR38 (24); EORTC QLQ-CR29 ver. A (53,54); EORTC QLQ-CR29 ver. B (55); EORTC QLQ-ELD14 (56) ; FACT-C (24); mCOH-QOL-O ver. A (25); mCOH-QOL-O ver. B (57,58); QLACS (59–61); QWLQ-CS (23); SF-36v2 (21,58); SF-12v2 (57); WHOQOL-BREF (22).
Supplemental Table 5.
Questionnaires’ QoL areas of assessment and key QoL indicators – spiritual QoL domain.
Supplemental Table 5.
Questionnaires’ QoL areas of assessment and key QoL indicators – spiritual QoL domain.
| QoL domain | Consensus reached in Study 1 | ABCRC | EORTC QLQ-C30 | EORTC QLQ-CR38 | EORTC QLQ-CR29 | EORTC QLQ-ELD14 | FACT-C | mCOH-QOL-O | QLACS | QWLQ-CS | SF-36v2 | SF-12v2 | WHOQOL-BREF | ||
| a | b | a | b | ||||||||||||
| SPIRITUAL QOL | |||||||||||||||
| Meaning of Illness | |||||||||||||||
| Religiosity | |||||||||||||||
| Hope | |||||||||||||||
| Transcendence | |||||||||||||||
| Inner Strength | |||||||||||||||
| QoL areas assessed | |||||||||||||||
| … of domain areas of Study 1 (5) | |||||||||||||||
Notes. Italic QoL areas are the ones additionally identified in the questionnaires of Study 2, but are not present in Study 1 QoL area pool. Questionnaires’ references: ABCRC (62); EORTC QLQ-C30 (51,52)M; EORTC QLQ-CR38 (24); EORTC QLQ-CR29 ver. A (53,54); EORTC QLQ-CR29 ver. B (55); EORTC QLQ-ELD14 (56) ; FACT-C (24); mCOH-QOL-O ver. A (25); mCOH-QOL-O ver. B (57,58); QLACS (59–61); QWLQ-CS (23); SF-36v2 (21,58); SF-12v2 (57); WHOQOL-BREF (22).
Supplemental Table 6.
Questionnaires’ QoL areas of assessment and key QoL indicators – other QoL areas.
Supplemental Table 6.
Questionnaires’ QoL areas of assessment and key QoL indicators – other QoL areas.
| QoL domain | Consensus reached in Study 1 | ABCRC | EORTC QLQ-C30 | EORTC QLQ-CR38 | EORTC QLQ-CR29 | EORTC QLQ-ELD14 | FACT-C | mCOH-QOL-O | QLACS | QWLQ-CS | SF-36v2 | SF-12v2 | WHOQOL-BREF | ||
| a | b | a | b | ||||||||||||
| Cancer-specific scale | X | ||||||||||||||
| Treatment-related symptoms | X | ||||||||||||||
| Stoma-related symptoms etc. | X | X | X | X | |||||||||||
| Embarrassment (by stoma, bowel movement, ...) | X | X | |||||||||||||
| Environment domain | X | ||||||||||||||
| Disease burden | X | ||||||||||||||
| Benefits of cancer | X | ||||||||||||||
| Functional well-being | X | ||||||||||||||
| Maintenance purposes | X | ||||||||||||||
| Private life | X | ||||||||||||||
| Other QoL areas assessed | 1 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | ||||||
Notes. Italic QoL areas are the ones additionally identified in the questionnaires of Study 2 but are not present in Study 1 QoL area pool. Questionnaires’ references: ABCRC (62); EORTC QLQ-C30 (51,52)M; EORTC QLQ-CR38 (24); EORTC QLQ-CR29 ver. A (53,54); EORTC QLQ-CR29 ver. B (55); EORTC QLQ-ELD14 (56) ; FACT-C (24); mCOH-QOL-O ver. A (25); mCOH-QOL-O ver. B (57,58); QLACS (59–61); QWLQ-CS (23); SF-36v2 (21,58); SF-12v2 (57); WHOQOL-BREF (22).
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021 May 4;71(3):209–49. [CrossRef]
- WCFR. https://www.wcrf.org/cancer-trends/worldwide-cancer-data/. 2022.
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023 May;73(3):233–54.
- Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. The Lancet. 2018 Mar;391(10125):1023–75. [CrossRef]
- Cheng V, Oveisi N, McTaggart-Cowan H, Loree JM, Murphy RA, De Vera MA. Colorectal Cancer and Onset of Anxiety and Depression: A Systematic Review and Meta-Analysis. Current Oncology. 2022 Nov 15;29(11):8751–66. [CrossRef]
- Sihvola S, Kuosmanen L, Kvist T. Resilience and related factors in colorectal cancer patients: A systematic review. European Journal of Oncology Nursing. 2022 Feb;56:102079. [CrossRef]
- Lim CYS, Laidsaar-Powell RC, Young JM, Kao SC, Zhang Y, Butow P. Colorectal cancer survivorship: A systematic review and thematic synthesis of qualitative research. Eur J Cancer Care (Engl). 2021 Jul 18;30(4). [CrossRef]
- Révész D, van Kuijk SMJ, Mols F, van Duijnhoven FJB, Winkels RM, Kant Ij, et al. External validation and updating of prediction models for estimating the 1-year risk of low health-related quality of life in colorectal cancer survivors. J Clin Epidemiol. 2022 Dec;152:127–39.
- Chan RJ, Chan A, Yates P, Molassiotis A. A step forward in addressing cancer survivorship in the Asia-Pacific region. BMC Med. 2017 Dec 26;15(1):17. [CrossRef]
- von Blanckenburg P, Seifart U, Conrad N, Exner C, Rief W, Nestoriuc Y. Quality of life in cancer rehabilitation: the role of life goal adjustment. Psychooncology. 2014 Oct;23(10):1149–56. [CrossRef]
- Joshy G, Thandrayen J, Koczwara B, Butow P, Laidsaar-Powell R, Rankin N, et al. Disability, psychological distress and quality of life in relation to cancer diagnosis and cancer type: population-based Australian study of 22,505 cancer survivors and 244,000 people without cancer. BMC Med. 2020 Dec 1;18(1):372. [CrossRef]
- Briggs LG, Sentana-Lledo D, Lage DE, Trinh QD, Morgans AK. Optimal assessment of quality of life for patients with prostate cancer. Ther Adv Med Oncol. 2022 Jan 10;14:175883592211413. [CrossRef]
- Miller KA, Stal J, Gallagher P, Weng Z, Freyer DR, Kaslander JN, et al. Time from Diagnosis and Correlates of Health-Related Quality of Life among Young Adult Colorectal Cancer Survivors. Cancers (Basel). 2021 Aug 11;13(16):4045. [CrossRef]
- The ACTION Study Group. Health-related quality of life and psychological distress among cancer survivors in Southeast Asia: results from a longitudinal study in eight low- and middle-income countries. BMC Med. 2017 Dec 13;15(1):10.
- Tay MRJ, Wong CJ, Aw HZ. Assessment of Health-Related Quality of Life and Distress in an Asian Community-Based Cancer Rehabilitation Program. Current Oncology. 2022 Sep 27;29(10):7012–20. [CrossRef]
- European Commission (EC). Research and Innovation. Conquering Cancer: Mission Possible Report of the Mission Board for Cancer. Luxembourg; 2020.
- European Commission (EC). Europe’s Beating Cancer Plan Communication from the Commission to the European Parliament and the Council. Brussels; 2021.
- Bianchi V, Spitale A, Ortelli L, Mazzucchelli L, Bordoni A. Quality indicators of clinical cancer care (QC 3 ) in colorectal cancer. BMJ Open. 2013 Jul;3(7):e002818. [CrossRef]
- Harrison M, Milbers K, Hudson M, Bansback N. Do patients and health care providers have discordant preferences about which aspects of treatments matter most? Evidence from a systematic review of discrete choice experiments. BMJ Open. 2017 May 17;7(5):e014719. [CrossRef]
- Aldaz BE, Treharne GJ, Knight RG, Conner TS, Perez D. Oncology healthcare professionals’ perspectives on the psychosocial support needs of cancer patients during oncology treatment. J Health Psychol. 2017 Sep 1;22(10):1332–44. [CrossRef]
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992 Jun;30(6):473–83.
- Lin CY, Hwang JS, Wang WC, Lai WW, Su WC, Wu TY, et al. Psychometric evaluation of the WHOQOL-BREF, Taiwan version, across five kinds of Taiwanese cancer survivors: Rasch analysis and confirmatory factor analysis. Journal of the Formosan Medical Association. 2019 Jan;118(1):215–22. [CrossRef]
- de Jong M, Tamminga SJ, de Boer AGEM, Frings-Dresen MHW. The Quality of Working Life Questionnaire for Cancer Survivors (QWLQ-CS): a Pre-test Study. BMC Health Serv Res. 2016 Dec 2;16(1):194.
- Rotonda C, Conroy T, Mercier M, Bonnetain F, Uwer L, Miny J, et al. Validation of the French version of the colorectal-specific quality-of-life questionnaires EORTC QLQ-CR38 and FACT-C. Quality of Life Research. 2008 Apr 13;17(3):437–45. [CrossRef]
- Grant M, Ferrell B, Dean G, Uman G, Chu D, Krouse R. Revision and Psychometric Testing of the City of Hope Quality of Life–Ostomy Questionnaire. Quality of Life Research. 2004 Oct;13(8):1445–57. [CrossRef]
- Muzzatti B, Annunziata MA. Assessing quality of life in long-term cancer survivors: a review of available tools. Supportive Care in Cancer. 2013 Nov 1;21(11):3143–52. [CrossRef]
- Nguyen H, Butow P, Dhillon H, Sundaresan P. A review of the barriers to using Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs) in routine cancer care. J Med Radiat Sci. 2021 Jun 19;68(2):186–95. [CrossRef]
- Mlakar I, Lin S, Nateqi J, Gruarin S, Diéguez L, Piairo P, et al. Establishing an Expert Consensus on Key Indicators of the Quality of Life among Breast Cancer Survivors: A Modified Delphi Study. J Clin Med. 2022 Apr 5;11(7):2041. [CrossRef]
- Pietersma S, de Vries M, van den Akker-van Marle ME. Domains of quality of life: results of a three-stage Delphi consensus procedure among patients, family of patients, clinicians, scientists and the general public. Quality of Life Research. 2013 Nov 17. [CrossRef]
- Tung J, Speechley KN, Gofton T, Gonzalez-Lara LE, Graham M, Naci L, et al. Towards the assessment of quality of life in patients with disorders of consciousness. Quality of Life Research. 2020 May 14;29(5):1217–27. [CrossRef]
- Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000 Oct 28;32(4):1008–15. [CrossRef]
- Powell C. The Delphi technique: myths and realities. J Adv Nurs. 2003 Feb 10;41(4):376–82. [CrossRef]
- Beiderbeck D, Frevel N, von der Gracht HA, Schmidt SL, Schweitzer VM. Preparing, conducting, and analyzing Delphi surveys: Cross-disciplinary practices, new directions, and advancements. MethodsX. 2021;8:101401. [CrossRef]
- Ferrell BR, Hassey Dow K, Grant M. Measurement of the quality of life in cancer survivors. Quality of Life Research. 1995 Dec;4(6):523–31. [CrossRef]
- Lavdantini M, Tsitsis N. Definitions and conceptual models of quality of life in cancer patients. Health Science Journal. 2015;9:1–5.
- Muñoz C, Juarez G, Muñoz ML, Portnow J, Fineman I, Badie B, et al. The Quality of Life of Patients with Malignant Gliomas and Their Caregivers. Soc Work Health Care. 2008 Oct 22;47(4):455–78. [CrossRef]
- Mollica M, Nemeth L, Newman SD, Mueller M. Breast Cancer in African Americans: From Patient to Survivor. Journal of Transcultural Nursing. 2014;25(4):334–40.
- Mlakar I, Lin S, Aleksandraviča I, Arcimoviča K, Eglītis J, Leja M, et al. Patients-centered SurvivorShIp care plan after Cancer treatments based on Big Data and Artificial Intelligence technologies (PERSIST): a multicenter study protocol to evaluate efficacy of digital tools supporting cancer survivors. BMC Med Inform Decis Mak. 2021 Dec 14;21(1):243. [CrossRef]
- Borgiel AEM, Dunn E V., Lamont CT, Macdonald PJ, Evensen MK, Bass MJ, et al. Recruiting family physicians as participants in research. Fam Pract. 1989;6(3):168–72. [CrossRef]
- Vanmeerbeek M, Govers P, Schippers N, Rieppi S, Mortelmans K, Mairiaux P. Searching for consensus among physicians involved in the management of sick-listed workers in the Belgian health care sector: a qualitative study among practitioners and stakeholders. BMC Public Health. 2016 Dec 17;16(1):164. [CrossRef]
- Freitas Â, Santana P, Oliveira MD, Almendra R, Bana e Costa JC, Bana e Costa CA. Indicators for evaluating European population health: a Delphi selection process. BMC Public Health. 2018 Dec 27;18(1):557. [CrossRef]
- Koo TK, Li MY. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med. 2016 Jun;15(2):155–63. [CrossRef]
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria; 2020.
- Revelle W. Psych: Procedures for Psychological, Psychometric, and Personality Research . Evanston: Northwestern University; 2019.
- Kassambara A. Rstatix: Pipe-Friendly Framework for Basic Statistical Tests. San Francisco: GitHub, Inc.; 2021.
- Benjamini Y, Hochberg Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. Journal of the Royal Statistical Society: Series B (Methodological). 1995 Jan 5;57(1):289–300. [CrossRef]
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005 Feb;8(1):19–32. [CrossRef]
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implementation Science. 2010 Dec 20;5(1):69. [CrossRef]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018 Oct 2;169(7):467–73.
- Martín-Martín A, Orduna-Malea E, Thelwall M, Delgado López-Cózar E. Google Scholar, Web of Science, and Scopus: A systematic comparison of citations in 252 subject categories. J Informetr. 2018 Nov;12(4):1160–77. [CrossRef]
- Calderon C, Ferrando PJ, Lorenzo-Seva U, Ferreira E, Lee EM, Oporto-Alonso M, et al. Psychometric properties of the Spanish version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30). Quality of Life Research. 2022 Jun 20;31(6):1859–69. [CrossRef]
- El Alami Y, Essangri H, Majbar MA, Boutayeb S, Benamr S, El Malki HO, et al. Psychometric validation of the Moroccan version of the EORTC QLQ-C30 in colorectal Cancer patients: cross-sectional study and systematic literature review. BMC Cancer. 2021 Dec 27;21(1):99. [CrossRef]
- Gujral S, Conroy T, Fleissner C, Sezer O, King PM, Avery KNL, et al. Assessing quality of life in patients with colorectal cancer: An update of the EORTC quality of life questionnaire. Eur J Cancer. 2007 Jul;43(10):1564–73. [CrossRef]
- Al-Shandudi M, Al-Mandhari M, Chan MF, Al-Hajri T, Al-Balushi M, Al-Azri M. Health-Related Quality of Life of Omani Colorectal Cancer Survivors. Cancer Control. 2022 Jan 11;29:107327482210841. [CrossRef]
- Whistance RN, Conroy T, Chie W, Costantini A, Sezer O, Koller M, et al. Clinical and psychometric validation of the EORTC QLQ-CR29 questionnaire module to assess health-related quality of life in patients with colorectal cancer. Eur J Cancer. 2009 Nov;45(17):3017–26. [CrossRef]
- Lorca LA, Sacomori C, Fasce Pineda G, Vidal Labra R, Cavieres Faundes N, Plasser Troncoso J, et al. Validation of the EORTC QLQ-ELD 14 questionnaire to assess the health-related quality of life of older cancer survivors in Chile. J Geriatr Oncol. 2021 Jun;12(5):844–7. [CrossRef]
- Wendel CS, Grant M, Herrinton L, Temple LKF, Hornbrook MC, McMullen CK, et al. Reliability and validity of a survey to measure bowel function and quality of life in long-term rectal cancer survivors. Quality of Life Research. 2014 Dec 3;23(10):2831–40. [CrossRef]
- Jane Mohler M, Joel Coons S, Hornbrook MC, Herrinton LJ, Wendel CS, Grant M, et al. The Health-Related Quality of Life in Long-Term Colorectal Cancer Survivors Study: objectives, methods and patient sample. Curr Med Res Opin. 2008 Jul 1;24(7):2059–70. [CrossRef]
- Avis NE, Smith KW, McGraw S, Smith RG, Petronis VM, Carver CS. Assessing Quality of Life in Adult Cancer Survivors (QLACS). Quality of Life Research. 2005 May;14(4):1007–23. [CrossRef]
- Ashley L, Smith AB, Jones H, Velikova G, Wright P. Traditional and Rasch psychometric analyses of the Quality of Life in Adult Cancer Survivors (QLACS) questionnaire in shorter-term cancer survivors 15months post-diagnosis. J Psychosom Res. 2014 Oct;77(4):322–9. [CrossRef]
- Escobar A, Trujillo-Martín M del M, Rueda A, Pérez-Ruiz E, Avis NE, Bilbao A. Cross-cultural adaptation, reliability and validity of the Spanish version of the Quality of Life in Adult Cancer Survivors (QLACS) questionnaire: application in a sample of short-term survivors. Health Qual Life Outcomes. 2015 Dec 16;13(1):182. [CrossRef]
- Boome I te, Somers AMJ, Graupner C, Kimman ML, Gidding- Slok AHM, Breukink SO. Development and content validation of the Assessment of Burden of ColoRectal Cancer (ABCRC)-tool. European Journal of Surgical Oncology. 2022 Aug;48(8):1807–14.
- Siafaka V, Mavridis D, Tsonis O, Tzamakou E, Christogiannis C, Tefa L, et al. The WHOQOL-BREF instrument: Psychometric evaluation of the Greek version in patients with advanced cancer and pain and associations with psychological distress. Palliat Support Care. 2022 Aug 19;1–11. [CrossRef]
- Oliveira SEH, Carvalho H, Esteves F. Toward an understanding of the quality of life construct: Validity and reliability of the WHOQOL-Bref in a psychiatric sample. Psychiatry Res. 2016 Oct;244:37–44. [CrossRef]
- Leung KF, Wong WW, Tay MSM, Chu MML, Ng SSW. Development and validation of the interview version of the Hong Kong Chinese WHOQOL-BREF. Quality of Life Research. 2005 Jun 1;14(5):1413–9. [CrossRef]
- McNair AGK, Whistance RN, Forsythe RO, Macefield R, Rees J, Pullyblank AM, et al. Core Outcomes for Colorectal Cancer Surgery: A Consensus Study. PLoS Med. 2016 Aug 9;13(8):e1002071.
- Dirven L, Petersen MAa, Aaronson NK, Chie WC, Conroy T, Costantini A, et al. Development and Psychometric Evaluation of an Item Bank for Computerized Adaptive Testing of the EORTC Insomnia Dimension in Cancer Patients (EORTC CAT-SL). Appl Res Qual Life. 2021 Apr 6;16(2):827–44. [CrossRef]
- Saver BG, Martin SA, Adler RN, Candib LM, Deligiannidis KE, Golding J, et al. Care that Matters: Quality Measurement and Health Care. PLoS Med. 2015 Nov 17;12(11):e1001902.
- Bellizzi KM, Mustian KM, Palesh OG, Diefenbach M. Cancer survivorship and aging. Cancer. 2008 Dec 3;113(S12):3530–9. [CrossRef]
Figure 1.
Search and study selection flowchart.
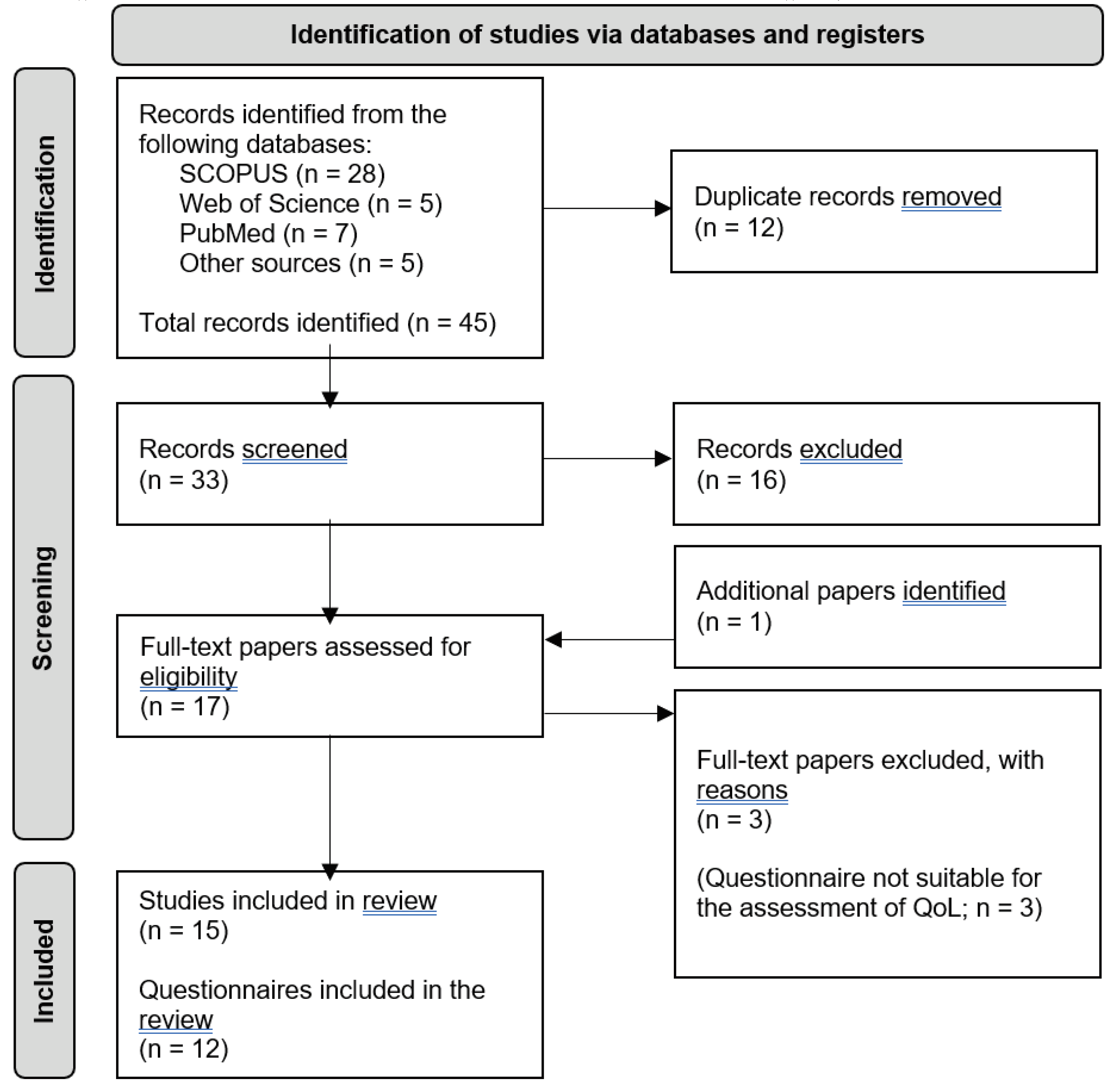
Table 1.
Participants’ characteristics.
| Round 1 | Round 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| All participants | Group 1 | Group 2 | |||||||
| f | % | f | % | f | % | f | % | ||
| N | 54 | 25 | 9 | 16 | |||||
| Gender | Female | 33 | 61.1 | 16 | 64.0 | 4 | 44.4 | 12 | 75.0 |
| Male | 21 | 38.9 | 9 | 36.0 | 5 | 55.6 | 4 | 25.0 | |
| Speciality* | Gastroenterology | 4 | 7.4 | 1 | 4.0 | - | - | 1 | 6.3 |
| Medical Oncology | 16 | 29.6 | 9 | 36.0 | 4 | 44.4 | 5 | 31.3 | |
| Nutrition | 2 | 3.7 | 2 | 8.0 | 1 | 11.1 | 1 | 6.3 | |
| Oncology Nursing | 5 | 9.3 | - | - | - | - | - | - | |
| Physiotherapy | 1 | 1.9 | 4 | 16.0 | - | - | 4 | 25.0 | |
| Psychology | 5 | 9.3 | - | - | - | - | - | - | |
| Psychotherapy | - | - | - | - | - | - | - | - | |
| Radiology | 1 | 1.9 | - | - | - | - | - | - | |
| Radiotherapy Oncology | 2 | 3.7 | 2 | 8.0 | 2 | 22.2 | - | - | |
| Surgery | 8 | 14.8 | 5 | 20.0 | 2 | 22.2 | 3 | 18.8 | |
| Other | 11 | 20.4 | 3 | 12.0 | 1 | 11.1 | 2 | 12.5 | |
| Country | Austria | - | - | 3 | 12.0 | - | - | 3 | 18.8 |
| Belgium | 10 | 18.5 | 10 | 40.0 | 3 | 33.3 | 7 | 43.8 | |
| Latvia | 6 | 11.1 | 5 | 20.0 | 3 | 33.3 | 2 | 12.5 | |
| Portugal | 22 | 40.7 | 2 | 8.0 | - | - | 2 | 12.5 | |
| Slovenia | 2 | 3.7 | 3 | 12.0 | 2 | 22.2 | 1 | 6.3 | |
| Spain | 13 | 24.1 | 1 | 4.0 | 1 | 11.1 | - | - | |
| Switzerland | 1 | 1.9 | 1 | 4.0 | - | - | 1 | 6.3 | |
| Years in practice | M | 15.7 | 10.2 | 12.2 | 9.1 | ||||
| SD | 10.3 | 8.3 | 9.7 | 7.6 | |||||
Notes. Group 1: participants included in both rounds; Group 2: participants included only in the 2nd round.* In Speciality for the Round 2 frequencies do not add up to exact N of the Group 1 and consequently to All participants of Round 2, as one participant indicated two Specialities, i.e. Medical oncology and Surgery.
Table 2.
Delphi Rounds 1 and 2 – QoL (sub)domains, mean ratings with standard deviations and consensus.
Table 2.
Delphi Rounds 1 and 2 – QoL (sub)domains, mean ratings with standard deviations and consensus.
| Round 1 | Round 2 | ||||||||||||||
| All participants | Group 1c | Group 2d | t-teste | ||||||||||||
| M | SD | % Agreementa | CRb | M | SD | M | SD | M | SD | df | t | Adj. pf | % Agreementg | CRh | |
| General domains | |||||||||||||||
| Physical Health and Well-being | 6.3 | 1.0 | 94.4 | * | 6.3 | 0.5 | 6.1 | 0.3 | 6.4 | 0.5 | 23 | -1.41 | 0.87 | 100.0 | * |
| Psychological Health and Well-being | 6.0 | 1.0 | 94.4 | * | 6.3 | 0.8 | 6.1 | 0.8 | 6.4 | 0.8 | 23 | -0.79 | 0.87 | 80.0 | * |
| Social Health and Well-being | 5.6 | 1.0 | 83.3 | * | 5.8 | 0.9 | 5.7 | 0.5 | 5.9 | 1.0 | 23 | -0.57 | 0.88 | 68.0 | - |
| Spiritual Health and Well-being | 4.9 | 1.6 | 61.1 | - | - | - | - | - | - | - | - | - | - | - | - |
| Physical QoL | |||||||||||||||
| Functional ability and Mobility | 6.2 | 0.9 | 96.0 | * | 6.5 | 0.7 | 6.7 | 0.5 | 6.5 | 0.8 | 20 | 0.70 | 0.87 | 90.9 | * |
| Activities of daily living | 6.1 | 0.9 | 94.0 | * | 6.6 | 0.6 | 6.7 | 0.5 | 6.6 | 0.7 | 20 | 0.20 | 0.94 | 95.5 | * |
| Fatigue/Vitality | 5.9 | 0.8 | 96.0 | * | 6.0 | 0.6 | 6.2 | 0.4 | 5.9 | 0.6 | 20 | 1.21 | 0.87 | 95.5 | * |
| Sleep and rest | 5.7 | 1.1 | 90.0 | * | 5.7 | 0.8 | 5.4 | 0.7 | 5.9 | 0.9 | 20 | -1.36 | 0.87 | 68.2 | - |
| Pain and discomfort | 6.4 | 0.9 | 94.0 | * | 7.0 | 0.2 | 7.0 | 0.0 | 6.9 | 0.3 | 20 | 0.83 | 0.87 | 100.0 | * |
| Health perceptions | 5.6 | 0.9 | 90.0 | * | 5.3 | 0.8 | 5.2 | 0.4 | 5.4 | 1.0 | 20 | -0.47 | 0.91 | 31.8 | - |
| Physical symptoms | 6.2 | 0.8 | 98.0 | * | 6.4 | 0.5 | 6.4 | 0.5 | 6.3 | 0.5 | 20 | 0.63 | 0.87 | 100.0 | * |
| Health distress | 5.7 | 1.0 | 94.0 | * | 5.3 | 0.8 | 5.0 | 0.7 | 5.5 | 0.9 | 20 | -1.31 | 0.87 | 31.8 | - |
| Weight loss/gain | 6.0 | 0.9 | 92.0 | * | 5.8 | 1.0 | 6.3 | 0.7 | 5.5 | 1.0 | 20 | 2.30 | 0.50 | 68.2 | - |
| Physical Health and comorbidities | 6.0 | 0.9 | 94.0 | * | 5.9 | 0.8 | 5.8 | 0.8 | 5.9 | 0.9 | 20 | -0.39 | 0.92 | 77.3 | * |
| Psychological QoL | |||||||||||||||
| Anxiety | 5.8 | 1.1 | 88.0 | * | 5.7 | 1.0 | 5.7 | 1.1 | 5.8 | 0.9 | 19 | -0.19 | 0.94 | 66.7 | - |
| Depression | 5.9 | 1.0 | 90.0 | * | 6.0 | 0.9 | 6.1 | 1.1 | 5.8 | 0.8 | 19 | 0.67 | 0.87 | 76.2 | * |
| Psychological distress | 5.8 | 1.1 | 84.0 | * | 6.0 | 0.7 | 6.1 | 0.8 | 6.0 | 0.7 | 19 | 0.33 | 0.92 | 76.2 | * |
| Cognitive functioning, concentration and attention | 5.5 | 1.3 | 82.0 | * | 5.5 | 1.0 | 5.3 | 1.2 | 5.6 | 0.9 | 19 | -0.54 | 0.88 | 52.4 | - |
| Uncertainty | 5.2 | 1.1 | 76.0 | * | 5.0 | 0.9 | 5.0 | 0.7 | 5.1 | 1.0 | 19 | -0.21 | 0.94 | 28.6 | - |
| Fear of Recurrence | 5.6 | 1.0 | 86.0 | * | 5.8 | 0.8 | 5.8 | 1.0 | 5.8 | 0.7 | 19 | -0.15 | 0.94 | 66.7 | - |
| Isolation/Abandonment and feelings of belonging | 5.5 | 1.2 | 82.0 | * | 5.6 | 0.9 | 5.0 | 0.9 | 6.0 | 0.6 | 19 | -3.13 | 0.17 | 61.9 | - |
| Positive feelings and affect | 5.6 | 1.0 | 88.0 | * | 5.8 | 0.8 | 5.4 | 0.7 | 6.0 | 0.7 | 19 | -1.72 | 0.87 | 66.7 | - |
| Negative feelings and affect | 5.5 | 1.1 | 86.0 | * | 5.8 | 0.5 | 5.7 | 0.5 | 5.8 | 0.6 | 19 | -0.69 | 0.87 | 71.4 | - |
| Loss of interest in usual activities | 5.5 | 1.3 | 80.0 | * | 6.0 | 0.8 | 5.8 | 1.2 | 6.2 | 0.4 | 19 | -1.06 | 0.87 | 90.5 | * |
| Social QoL | |||||||||||||||
| Family functioning | 5.7 | 1.2 | 78.0 | * | 5.9 | 1.1 | 6.1 | 1.1 | 5.7 | 1.3 | 17 | 0.77 | 0.87 | 68.4 | - |
| Martial functioning | 5.2 | 1.4 | 72.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Affection/Sexuality | 5.2 | 1.3 | 68.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Self Concept/Appearance | 5.4 | 1.2 | 78.0 | * | 5.3 | 0.7 | 5.3 | 0.5 | 5.3 | 0.9 | 17 | 0.09 | 0.94 | 36.8 | - |
| Enjoyment/Leisure (participation and opportunities) | 5.4 | 1.3 | 78.0 | * | 5.7 | 0.9 | 5.7 | 0.9 | 5.7 | 1.1 | 17 | -0.07 | 0.94 | 57.9 | - |
| Social activity and limitations | 5.6 | 1.2 | 80.0 | * | 5.8 | 0.8 | 5.8 | 0.4 | 5.9 | 1.0 | 17 | -0.34 | 0.92 | 73.7 | - |
| Financial Concerns | 5.2 | 1.3 | 76.0 | * | 4.8 | 1.1 | 4.7 | 0.7 | 5.0 | 1.3 | 17 | -0.67 | 0.87 | 21.1 | - |
| Social Support | 5.5 | 1.1 | 84.0 | * | 5.5 | 0.7 | 5.3 | 0.7 | 5.7 | 0.7 | 17 | -1.16 | 0.87 | 63.2 | - |
| Employment | 5.5 | 1.2 | 82.0 | * | 5.7 | 0.7 | 5.6 | 0.5 | 5.8 | 0.8 | 17 | -0.78 | 0.87 | 57.9 | - |
| Role limitations due to health or psychical problems | 5.4 | 1.2 | 78.0 | * | 5.5 | 0.6 | 5.3 | 0.5 | 5.7 | 0.7 | 17 | -1.33 | 0.87 | 47.4 | - |
| Spiritual QoL | |||||||||||||||
| Meaning of Illness | 5.2 | 1.5 | 72.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Religiosity | 4.1 | 1.9 | 48.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Hope | 5.2 | 1.4 | 68.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Transcendence | 4.4 | 1.6 | 50.0 | - | - | - | - | - | - | - | - | - | - | - | - |
| Inner Strength | 5.0 | 1.5 | 64.0 | - | - | - | - | - | - | - | - | - | - | - | - |
Notes. a % of all participants evaluating the item with top three measures on a 7-point scale. b * = consensus reached (criterion: % Agreement for round 1 < 75 %), - = consensus not reached. c Group 1: Participants included in both Delphi rounds. d Group 2: Participants included only in the 2nd Delphi round. e Independent samples t-test, 2-tailed, equal variances assumed. f p adjustment method = BH (46). g % of all participants evaluating the item with top two measures on a 7-point scale. h * = consensus reached (criterion. % Agreement for round 2 < 75 %), - = consensus not reached.
Table 3.
An overview of the characteristics of the papers and studies identified.
| Questionnaire | Reference | Type of paper | Construct assessed | Target population | Number of items | Response scale | Language of the questionnaire |
|---|---|---|---|---|---|---|---|
|
ABCRC (Assessment of Burden of Colorectal Cancer-tool) |
Boome et al., 2022 (62) | Development, content validation | Experienced burden of colorectal cancer and lifestyle parameters | Adult patients with colon and rectal cancer, patients with anastomosis, and patients with stoma | 27 (version for patients with stoma), 28 (version for colon cancer), 29 (version for rectal cancer) | 3- and 4-point; one open question | Dutch |
|
EORTC QLQ-C30 (European Organisation for Research and Treatment of Cancer, Quality of Life of Cancer Patients, version 3) |
Calderon et al., 2022 (51) | Validation | Quality of life | Adult patients with cancer (general) | 30 | 4-point Likert type and 7-point | Spanish |
| El Alami et al., 2021 (52) | Validation (Moroccan Arabic Version) | Adult patients with cancer (general); in this study colorectal cancer patients | Moroccan Arabic | ||||
|
EORTC QLQ-CR38 (European Organisation for Research and Treatment of Cancer, Quality of Life Questionnaire for Colorectal Cancer-38)1 |
Rotonda et al., 2008 (24) | Validation (French version) | Quality of life | Adult patients with colorectal cancer | 38 | 4-point Likert type and 7-point | French |
|
EORTC QLQ-CR29 (European Organisation for Research and Treatment of Cancer, Quality of Life Questionnaire for Colorectal Cancer-29)1, 2 |
Gujral et al., 2007 (53) | Content validation study (adaptation of the EORTC QLQ-CR38) | Quality of life | Adult patients with colorectal cancer | 29 | [no information available in the paper] | English |
| Al-Shandudi et al., 2022 (54) | Empirical study | Arabic | |||||
| Whistance et al., 2009 (55) | Clinical and psychometric validation | 4-point Likert type and 7-point | English, French, Taiwanese, Italian, German, Spanish | ||||
|
EORTC QLQ-ELD14 (European Organisation for Research and Treatment of Cancer, Quality of Life Questionnaire - Elderly Cancer Patients Module) |
Lorca et al., 2021 (56) | Validation for ageing cancer survivors | Quality of life | Ageing patients (>60 years) with cancer (in this study colorectal cancer survivors) | 14 | 7-point Likert scale and 4-point scale | Spanish version |
|
FACT-C (Functional Assessment of Cancer Therapy – Colorectal) |
Rotonda et al., 2008 (24) | Validation | Well-being | Adult patients with colorectal cancer | 34 | 5-point scale | French |
|
mCOH-QOL-O (Modified City of Hope Quality of Life - Ostomy questionnaire) |
Grant et al., 2004 (25) | Validation | Quality of life | Ostomy patients (cancer and non-cancer) | 41 | 11-point scale | English |
| Wendel et al., 2014 (57) | Rectal cancer survivors | 43 | |||||
| Mohler et al., 20083 (58) | Empirical paper | Colorectal cancer (CRC) survivors with and withoutostomies | 34 | English | |||
|
QLACS (Quality of Life in Adult Cancer Survivors questionnaire) |
Avis et al., 2005 (59) | Questionnaire development | Quality of life | Long-term cancer survivors (> or equal to 5 years post-diagnosis) | 47 | 7-point scale | English |
| Ashley et al., 2014 (60) | Psychometric validation | Short-term cancer survivors | |||||
| Escobar et al., 2015 (61) | Cross-cultural adaptation, reliability andvalidity of the Spanish version | Spanish | |||||
|
QWLQ-CS (Quality of Working Life Questionnaire for Cancer Survivors) |
De Jong et al., 20164 (23) | Item-development study | Quality of life in the work domain | Cancer survivors | 104 | 4-point scale | English |
|
SF-36v2 (SF-36v2 Health Survey) |
Ware & Sherbourne, 1992 (21) | Item selection study | Functional health and well-being | General population | 36 | several types of response scales differing by items | English |
| Mohler et al., 2008 (58) | Empirical study | ||||||
|
SF-12v2 (SF-12v2 Health Survey) |
Wendel et al., 2014 (57) | Validation paper – for use with long-term rectal cancer survivors | Functional health and well-being | [no information] | 12 | [no information] | English |
|
WHOQOL-BREF (World Health Organization Quality-of-Life Scale) |
Lin et al., 2019 (22) | Psychometric validation of Taiwan version | Quality of life | General population (sample of this study: cancer survivors, also colorectal) | 28 (original 26 items + 2 added in this study) | 5-point scale | Taiwanese |
Notes. 1 To be used with the core questionnaire EORTC QlQ-C30. 2 Additionally included paper, since the Al-Shandudi et al. (54) referred to it regarding the questionnaire. 3 Modified version of the questionnaire (omitted ostomy-specific items) was used with control subjects in the study. 4 Not a validation paper, but only item-generation study paper, resulting in a preliminary questionnaire without tested psychometric properties.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



