
Submitted:
03 April 2024
Posted:
03 April 2024
You are already at the latest version
Abstract
. Background/Objectives: Crohn's disease is a chronic and debilitating intestinal disorder that alternates between remission and active flare-ups, often leading to hospitalization. Social support is known to enhance adaptation to the disease and modulate stress perception in patients, while stress may exacerbate symptoms. The aim of this study was to examine the roles of perceived stress and social support in Crohn's disease and their impact on the frequency of flare-ups. Methods: A cross-sectional observational study was conducted, assessing stress and social support in a cohort of 91 patients with Crohn's disease during flare-up and remission phases. The Perceived Stress Scale (PSS-14) and a Social Support Questionnaire were utilized for evaluation. We examined the relationship between stress and social support in Crohn's disease. The interaction between the variables studied was also studied, considering the stage of the disease. Finally, we realized analysis of the influence of these two variables on the development of flares in Crohn's disease. Results: The study revealed that patients experience higher stress levels during flare-ups and that these levels are amplified by a lack of social support. A significant relationship was identified between the levels of social support and the occurrence of flare-ups, indicating that better social support is associated with fewer flare-ups.. Conclusions: Patients with Crohn's disease in the flare-up phase are subject to considerable stress. Deficit in social support is linked to an increase in stress levels. The interplay of social support and stress plays a critical role in the development of flare-ups.
Keywords:
Social Support
; Stress
; Crohn's disease
; Flare-up
1. Introduction
1.1. Crohn's Disease
Crohn's disease is an inflammatory bowel disease of unknown origin that can affect any section of the gastrointestinal tract, from the mouth to the anus [1,2]. Determining the exact incidence of new cases each year is challenging due to inconsistencies in reporting and variations in diagnostic criteria. Nevertheless, it is recognized as a condition with a rising incidence, especially in Western countries [3]. The symptoms commonly include abdominal pain, diarrhea, fatigue, weight loss, and in more severe cases, the occurrence of fissures, abscesses, or fistulas that may require surgical intervention. Additionally, surgery might be necessary to excise nonfunctional segments of the bowel. The disease's clinical course is often punctuated by episodes of remission and exacerbations, which significantly affect the patient's overall well-being. The progression of the disease is marked by flare-ups, with a relapse risk estimated to be between 30% and 60% per year [4]. Identified as an autoimmune disorder, the immune system in Crohn's disease mistakenly attacks the body's own tissues as if they were foreign antigens. It is a chronic, progressive, relapsing, and highly debilitating disease, and the primary treatment goal is to manage the signs and symptoms [5]. While the etiology of Crohn's disease is not fully understood, it is hypothesized by healthcare professionals that stress levels and the presence or absence of social support can influence the likelihood of relapse in individuals with this condition.
1.2. Stress
Psychological stress arises from the interaction between an individual and their environment, which is perceived as threatening or surpassing their resources, potentially compromising well-being [6]. Stress, therefore, is not inherent to the individual or the environment, but rather is a product of the unique interaction between them. It is also a response to the demands placed upon an individual, which may be incompatible with their normal adaptation to the environment, potentially impacting both physical and psychological health [7]. This view of stress corresponds with contemporary understandings of disease, where illness is not solely the result of an external agent but also involves the organism's vulnerability.
Stress has been extensively researched and is associated with the emergence and progression of various diseases [8,9], exerting a detrimental effect on several pathologies [10,11]. Specifically concerning Crohn's disease, studies have indicated that stress affects the disease course, treatment response, and exacerbation, including the onset of flare-ups. A study from 2011 [12] highlighted that stress impacts the brain-gut axis, precipitating the release of neurotransmitters and pro-inflammatory cytokines, leading to alterations in gastrointestinal motility and adverse effects on the intestinal mucosa and microbiota. Similarly, research by De Punder and Pruimboom in 2015 [13] confirmed that stress not only exacerbates the disease but also causes inflammation of the intestinal mucosa, increasing permeability and enabling the entry of foreign substances. This effect of stress on the intestinal barrier has been corroborated by a review of various studies conducted in 2019 [14].
In the same vein, research led by Shaler et al. [15] demonstrated that psychological stress contributes to the exacerbation of Crohn's disease by inducing changes in the gut microbiota, which may play a role in its pathogenic process, influencing protective immunity.
Furthermore, the role of social support has been identified as a significant factor in the context of stress. Professional experience suggests that social support is crucial not only for its direct impact but also for its indirect influence on stress levels, which, in turn, affect the stress relationship in the exacerbation of Crohn's disease.
1.3. Social Support
Social support is recognized as a pivotal psychosocial factor that influences the perception and development of coping mechanisms, facilitating adaptation to various circumstances [16,17]. It also serves as a mitigating element in the stress associated with illness [18,19]. Social support encompasses the gamut of emotional, informational, and material aid that one receives from personal informal networks or broader group associations. This includes the actual support transactions, the individual's perception of these transactions, and their satisfaction with the assistance provided [18].
The seminal research on the psychological benefits of social support in the context of illness was conducted by Cassel [20]. Another early contributor to this field, Cobb [21], posited that the advantages of social support stem from the affirmation it provides individuals that they are cared for and valued within their social networks.
The fundamental concept is that social support bolsters an individual's sense of being cherished and valued, fostering a robust identity as part of a community. The beneficial impacts of social support have been underscored in numerous studies [22,23,24]. It includes all forms of environmental resources that encourage social connections, individual adaptation, and overall well-being within the context of community life. Therefore, social support refers to the array of emotional, material, informational, or companionship resources that a person perceives or receives from various members of their social network [25].
1.4. Social Support and Stress: Hobfoll's Model
In Hobfoll's model, stress is defined as a response to the environment in which there is a perceived threat of loss of resources, or where there is an investment of resources without any gain [26]. Thus, individuals interact with their environment to improve their situation or prevent it from deteriorating, and such actions precede the emergence of stressors. In this model, the essence of coping is rooted in the investment of resources, as this leads to the acquisition of new resources, which are then utilized in the coping process.
Moreover, the model considers a series of strategies through which social support resources strengthen resistance to stress, both preemptively (preventive or primary) and after an individual has been exposed to it (palliative or secondary). Social support provides a sense of connectedness and mitigates the perception of loneliness, prevents individuals from experiencing the loss of additional resources, and can directly forestall resource loss by averting stress. Once stress is perceived, social support can directly or indirectly replenish lost resources, and it can also promote a more effective use of available resources by a stressed individual, as well as foster the creation of new ones. In essence, each stressful situation is multidimensional and, as such, can lead to varied needs for social support. The protective role of social support against stress has been corroborated by several studies [27,28]. A 2022 study among individuals with alcoholism [29] demonstrated that low levels of social support contribute to the activation of the reward axis (ventral medial prefrontal cortex and ventral striatum) during alcohol exposure, while high levels of social support do not trigger such activation. Furthermore, those with scant social support exhibit greater activation of the stress circuit (ventral medial prefrontal cortex, dorsal striatum, and periaqueductal gray), which is not observed in individuals with ample social support. These findings affirm that social support significantly modulates the stress response. Therefore, high levels of social support diminish both the neural and subjective stress responses, whereas low levels of social support intensify alcohol craving and the neural stress response.
Regarding Crohn's disease, specific studies focusing on social support are lacking. Research on other digestive disorders and inflammatory bowel disease at large exists. For instance, Lee and colleagues [30] discovered that patients with functional dyspepsia perceived less social support compared to healthy individuals. In the context of inflammatory bowel disease, Sewitch et al. [31] found that the interplay between stress and disease activity was inversely proportional to the satisfaction with perceived social support.
In conclusion, stress and social support are significant factors to consider in the context of disease. There is a dearth of research on these two variables and their impact on the onset of flare-ups in Crohn's disease. Hence, investigating the relationship between stress, social support, and their influence on the occurrence of flare-ups in Crohn's disease is imperative.
This study aimed to examine the roles of perceived stress and social support in Crohn's disease and their influence on the development of flare-ups, based on the hypothesis that stress impacts the occurrence of Crohn's disease flare-ups, and that social support is implicated in this relationship.
2. Materials and Methods
2.1. Design
A cross-sectional observational study was carried out, employing validated scales to assess the impact of both stress and social support on Crohn's disease.
2.2. Participants
The study was conducted at the Digestive Unit of Gregorio Marañón University Hospital, focusing on patients diagnosed with a flare-up of Crohn's disease, and at the Madrid Association for Crohn's Disease and Ulcerative Colitis. The inpatient group experiencing flare-ups were admitted to the hospital presenting symptoms such as cachexia, fever, vomiting, and, in some cases, pseudo-obstruction of the bowel. These patients had an established diagnosis of Crohn's disease and were on daily pharmacological and dietary regimens.
The outpatient group, associated with the Madrid Association for Crohn's Disease and Ulcerative Colitis, consisted of individuals in the remission phase of Crohn's disease. They were asymptomatic during the study and were not receiving prednisone treatment. These individuals reported a good quality of life, with no abdominal pain and passing 0 to 2 formed stools per day without rectal bleeding.
For inclusion in the study, patients were required to have a confirmed diagnosis of Crohn's disease by a gastroenterologist. Exclusion criteria encompassed those who met the inclusion requirements but had other organic diseases such as heart disease, peptic ulcers, chronic headaches, respiratory diseases, etc., or psychological or mental illnesses diagnosed by a psychologist or psychiatrist.
2.3. Procedure
In all cases, the study was presented to the participants in person, and instructions were given on the criteria for participation in the study. The questionnaires were given to those who showed interest in participating in the study, after checking that they had understood everything correctly.
In all cases participation was voluntary and disinterested. All signed the informed consent form. The study was approved by the Ethics Committee of the Faculty of Psychology, Complutense University of Madrid (ref. 2018/19-022). The sample was collected between July 2019 and February 2020.
2.4. Instruments
Three questionnaires were utilized in this research: a socio-demographic questionnaire, the Perceived Stress Scale (PSS-14) and a Social Support Questionnaire.
2.4.1. Perceived Stress Scale (PSS-14)
2.4.2. Social Support Questionnaire
The Perceived Social Support Questionnaire, developed by Díaz-Veiga [34], was used to measure social support. This scale evaluates the level of satisfaction with the social, emotional, material and informational support received from family, friends, other people and health professionals.
2.5. Statistical Analysis
The socio-demographic questionnaire variables were analyzed using percentages and measures of central tendency, including mean and standard deviation.
To examine the relationship between stress and social support in Crohn's disease, patients were divided into groups with high and low social support based on the level of stress they reported. The median was employed as the measure of central tendency to avoid bias. This analysis also utilized mean and standard deviation.
To further explore the relationship between stress and social support, a specific analysis was conducted to determine how these two variables interacted, considering the participants' disease status (flare-up or remission phase). Pearson's linear correlation coefficient was applied in this analysis.
A more in-depth examination of the relationship between the stress and social support variables and their impact on the occurrence of flare-ups was achieved through binary logistic regression analysis, distinguishing between groups with high and low social support. This assessed the effect of stress on predicting flare-ups, factoring in the level of social support (low or high).
The global accuracy of the test was gauged using the area under the receiver operating characteristic (AUROC) curve.
The Statistical Package for the Social Sciences, Version 23 (SPSS 23), was utilized for the descriptive statistics, hypothesis testing, and analyses of internal consistency, reliability, and validity of the instruments used in this research. All tests were conducted with a 95% confidence level, considering a p-value below 0.05 as significant.
3. Results
The sample consisted of 91 patients with Crohn's disease, with an average age of 34.60 years. Of these, 44 were male (48.36%) ranging in age from 17 to 50 years, with an average age of 35.87 years, and 47 were female (51.64%) ranging in age from 16 to 51 years, with an average age of 33.41 years.
3.1. Relationship between Stress and Social Support in Crohn's Disease
The results of the analysis of the level of stress in patients experiencing flare-ups and those in the latency phase, taking into account their classification as either high or low social support, were significant for those with high social support. The results are presented in Table 1.
In addition, this table shows that subjects experiencing a flare-up are also highly stressed with similar scores. And those with low levels of social support also have high levels of stress.
For the Pearson linear correlation coefficient analysis, the two groups of patients were considered separately (flare-up or latency phase). The results are presented in Table 2.
In the variables correlation analysis for the group of Crohn's patients in the latency phase, there was a significant positive correlation (r = -.476; p< .05) between the variables social support and stress.
3.2. Relationship between Social Support and Stress and Their Influence on the Prediction of the Existence of Flare-Ups
The aim was to determine the influence of stress and social support on the likelihood of experiencing flare-ups in Crohn's disease. Accordingly, we examined the impact of stress on flare-up probability, considering the patients' social support levels.
The t-test for equal means revealed that subjects in the high social support group had a higher mean stress level (28.21) compared to those in the low social support group (19.45). Table 1.
To further understand the influence of stress in relation to social support in Crohn's disease, a binary logistic regression model was created. This model used the presence of flare-ups as a binomial and categorical dependent variable, with two possible outcomes: YES or NO. The model was estimated using the introduction method.
In the logistic regression analysis predicting flare-up likelihood for the high social support group, the main effects model was statistically significant (χ2 = 7.798; p = .005). In contrast, the main effects model for the low social support group was not significant (χ2 = 1.275; p < .259), as shown in Table 3.
The predictive power of the model for the high social support group (significant model) explained approximately 31% of the variance in the dependent variable (Existence of flare-up), with Nagelkerke's R2 = .313. The classification table indicated an accuracy of 63.6% for predicting flare-ups (cut-off point: 0.05).
Further analysis in the high social support group examined the relationship between the independent variable (stress) and the dependent variable (existence of flare-up), with results presented in Table 5.
It was found that stress (with an odds ratio of 1.15) significantly predicts the occurrence of flare-ups, making it a reliable predictive variable.
Consequently, the predictive formula for the probability of a flare-up in the group of Crohn's patients with high social support is:
P(flare-up) =1/1+e(2.841−(0.143×stress))
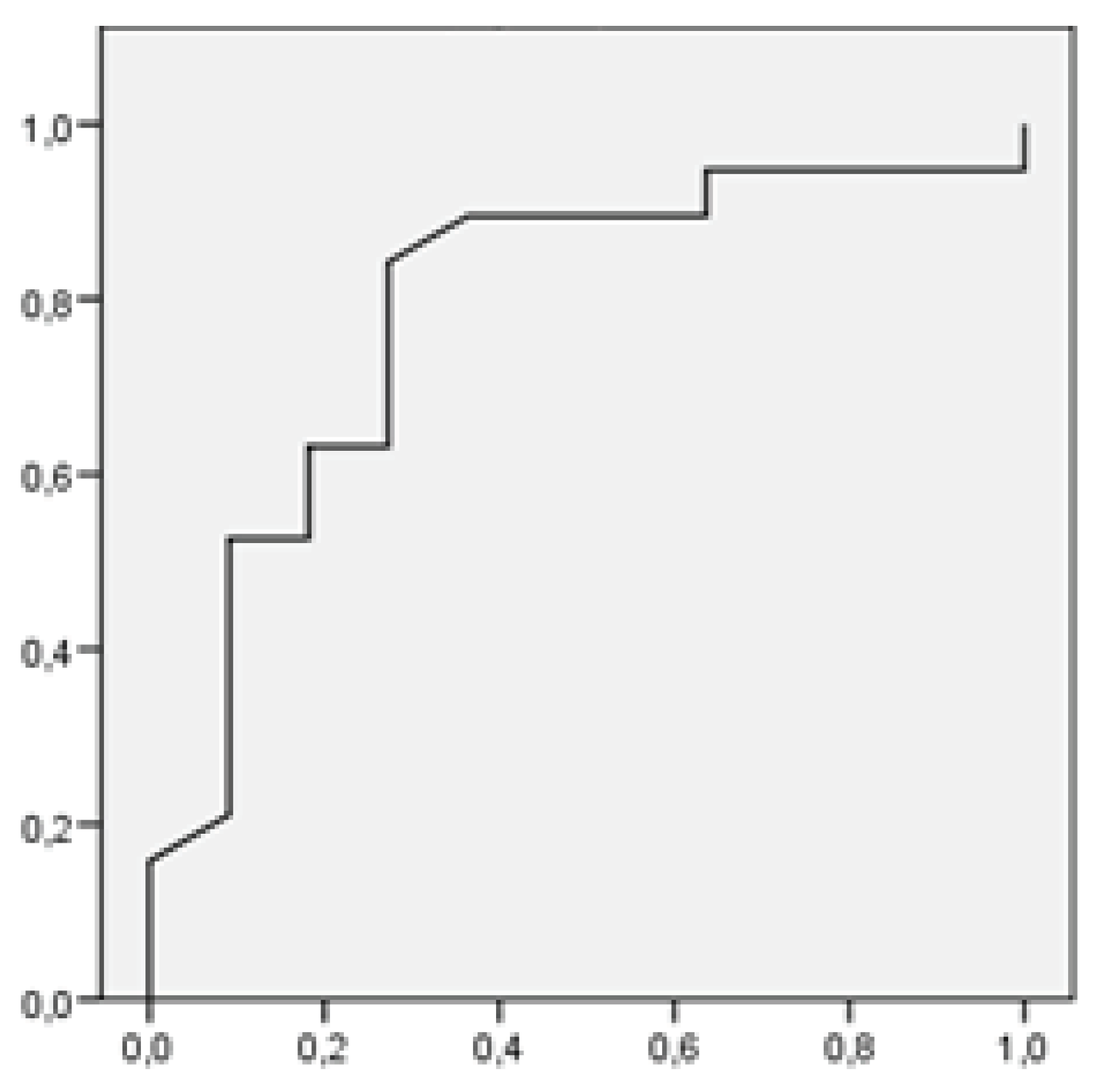
Moreover, the ROC curve was applied to assess the effectiveness of the contrasts in the logistic regression analysis. This test's accuracy in predicting a flare-up, using the stress variable in the high social support group (significant model), was demonstrated by the ROC curve being positioned upward and to the left, enlarging the area under the curve and thus indicating high sensitivity and specificity.
Figure 1.
ROC curve for Crohn's patients belonging to the group with high social support.
4. Discussion
4.1. Discussion
The objectives of this research were to examine the role of perceived stress and social support in Crohn's disease and their impact on the occurrence of flare-ups.
Concerning stress, our study's findings indicate that individuals experiencing a flare-up exhibit high stress levels. These findings align with prior research on different diseases, which has established that stress can trigger disease activity. The heightened stress may correlate with an increase in symptoms and a diminished treatment response [12,13,14,15].
These insights are in agreement with the dynamics between stress and the exacerbation of inflammatory bowel disease, which patients often cite as the primary aggravator of their deteriorating condition [12,13,14].
In terms of social support, our study observed that patients with lower levels of social support reported higher stress levels, while those with robust social support exhibited lower stress levels. These outcomes are in accordance with those of other studies [27,28], suggesting that social support affects how patients perceive their illness, develop coping strategies, and adapt to their condition, ultimately improving their status.
Regarding the impact of social support and stress on the development of Crohn's disease flare-ups, we were able to construct a significant predictive model for flare-up likelihood in patients with high social support levels, underscoring the role of social support on stress and the combined effect of these variables on flare-ups.
The research illustrates both direct and indirect effects of social support. Directly, during the remission phase, patients demonstrated lower stress levels, suggesting that social support contributes to the acquisition of new resources that aid in adapting to the disease and bolstering stress resistance, with the least stress observed in this phase. Indirectly, social support seems to mitigate stress perception, allowing for the formulation of a predictive model for disease flare-up when social support levels are high. This buffering role of social support has been corroborated by other studies [18,19].
It is important to highlight that stress influences not only the patient's condition but also the activation of the disease itself, aligning with findings from other researchers [27,28,29].
Consequently, these findings suggest the necessity for interventions that assist individuals in expanding their social networks and engaging in self-help or support groups, which could enhance their social support levels.
4.2. Strengths and Limitations
The primary strength of this study is the use of mathematical modeling to show the influence of both stress and social support on the development of Crohn's disease flare-ups.
Another advantage is the demonstration of social support's direct impact on the disease. Additionally, its indirect effects relate to reduced stress levels in patients, which correspondingly decrease the likelihood of flare-ups.
As for the limitations, the most significant is the sample size, which necessitates a cautious interpretation of our conclusions.
4.3. Practice Implications
We advocate for care and support strategies that include counseling, education, and initiatives in health prevention and promotion for individuals with Crohn's disease. These strategies should focus on self-managed stress reduction and management throughout all disease phases. Interventions should also prioritize enhancing social support, specifically by expanding patients' social networks. These measures are expected to prolong the disease's latency periods, collectively contributing to more effective management and treatment of Crohn's disease.
5. Conclusions
In conclusion, our study has demonstrated that patients with Crohn's disease undergoing a flare-up are in a state of high stress. Those with low levels of social support are also found to have elevated stress levels. Additionally, there is a discernible relationship between social support and stress in Crohn's disease, with these variables influencing the occurrence of flares in patients who have high levels of social support.
It is important to acknowledge that social support exerts both direct and indirect effects. Directly, it influences the perception process and the development of positive coping mechanisms in Crohn's disease. Indirectly, it is associated with a reduction in stress levels.
Moreover, our findings enable us to establish a predictive model for the likelihood of a flare-up based on the level of perceived stress, particularly in patients with substantial social support.
Author Contributions
Conception and study design, M.J.d.D.-D., A.A. and A.B. Methodology, M.J.d.D.-D., A.A. and A.B. Data collection, M.J.d.D.-D. Data analysis, M.J.d.D.-D., A.A. Draft of manuscript, M.J.d.D.-D. and A.B. Revision for content, M.J.d.D.-D., A.A. and A.B. Approval of final manuscript, M.J.d.D.-D., A.A. and A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Faculty of Psychology of the Complutense University of Madrid (Ref. 2018/19-022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request through the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- González Lara, V. Enfermedad Inflamatoria Intestinal. Madrid: Ergon; 2001.
- Ortigosa, L. Concepto actual y aspectos clínicos de la Enfermedad de Crohn y la Colitis Ulcerosa. Colomb Med. 2005; 36(2): 16-24.
- Bernstein CN, Loftus EV, Lakatos PL, et al. Epidemiology and Natural History Task Force of the International Organization for the Study of Inflammatory Bowel Disease (IOIBD). Hospitalisations and surgery in Crohn's disease. Gut. Apr 2012;61(4):622-9.
- Toh, J.W.; Wang, N.; Young, C.J.; Rickard, M.J.; Keshava, A.; Stewart, P.; Kariyawasam, V.; Leong, R. Major Abdominal and Perianal Surgery in Crohn’s Disease: Long-term Follow-up of Australian Patients With Crohn’s Disease. Dis. Colon Rectum 2018, 61, 67–76. [Google Scholar] [CrossRef] [PubMed]
- van der Have, M.; Minderhoud, I.M.; Kaptein, A.A.; Leenders, M.; Siersema, P.D.; Fidder, H.H.; Oldenburg, B. Substantial impact of illness perceptions on quality of life in patients with Crohn's disease. J. Crohn’s Colitis 2013, 7, e292–e301. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, RS, Folkman, S. Estrés y procesos cognitivos. Barcelona: Martínez Roca; 1986.
- Fernández Seara, JL. Estrés y salud. Granada: Grupo editorial universitario; 2002.
- Steptoe, A.; Kivimäki, M. Stress and cardiovascular disease. Nat. Rev. Cardiol. 2012, 9, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, T.; Alter, A. Occupational stress and hypertension. J. Am. Soc. Hypertens. 2012, 6, 2–22. [Google Scholar] [CrossRef]
- Kashani, M.; Eliasson, A.; Vernalis, M. Perceived stress correlates with disturbed sleep: A link connecting stress and cardiovascular disease. Stress 2011, 15, 45–51. [Google Scholar] [CrossRef]
- Pérez, M.d.C.R.; Alonso, S.R.L. Influencia de los factores psicosociales en adolescentes con Diabetes Mellitus tipo I. Cult. de Los Cuid. 2017, 21, 190–198. [Google Scholar] [CrossRef]
- Konturek, P.C.; Brzozowski, T.; Konturek, S.J. Stress and the gut: pathophysiology, clinical consequences, diagnostic approach and treatment options. J. Physiol. Pharmacol. 2011, 62, 591–599. [Google Scholar]
- de Punder, K.; Pruimboom, L. Stress Induces Endotoxemia and Low-Grade Inflammation by Increasing Barrier Permeability. Front. Immunol. 2015, 6, 223. [Google Scholar] [CrossRef]
- Oligschlaeger, Y.; Yadati, T.; Houben, T.; Oliván, C.M.C.; Shiri-Sverdlov, R. Inflammatory Bowel Disease: A Stressed “Gut/Feeling”. Cells 2019, 8, 659. [Google Scholar] [CrossRef]
- Shaler, C.R.; Parco, A.A.; Elhenawy, W.; Dourka, J.; Jury, J.; Verdu, E.F.; Coombes, B.K. Psychological stress impairs IL22-driven protective gut mucosal immunity against colonising pathobionts. Nat. Commun. 2021, 12, 1–17. [Google Scholar] [CrossRef]
- Cutrona, CE, Russell, DW. The provisions of social relationships and adaptation to stress. Adv Personal Relatnshps. 1987; 1(1): 37-67.
- Fontibón, L.F.; Acosta, L.L.; Valdelamar, J.J.; Valdelamar, A.A.; Sánchez, R.R. Asociación entre variables sociodemográficas, clínicas y calidad de vida con el apoyo social percibido en pacientes colombianos con cáncer. Av Psicol Latinoam. 2015, 33, 387–395. [Google Scholar] [CrossRef]
- Barrón, A, Chacón, F. Efectos directos y protectores frente al estrés del apoyo social. Invest Psicol. 1990; 8: 197-206.
- Pastor, MA, Rodríguez Marín, J, López-Roig, et al. Coping with chronic pain and social support in rheumatic patients. In: Johnston, M, Herbert, M, Marteau, Th. (Eds.). European Health Psychology. Leicester, England: Bocardo Press; 1991. p.112-113.
- Cassel, J. An epidemiological perspective of psychosocial factors in disease etiology. Am. J. Public Heal. 1974, 64, 1040–1043. [Google Scholar] [CrossRef] [PubMed]
- Cobb, S. Presidential Address-1976. Social support as a moderator of life stress. Psychosom Med. 1976 Sep-Oct;38(5):300-14.
- Salinas-Rehbein, B.; Schleef, J.; Neira-Vallejos, S.; Ortiz, M.S. Apoyo social y obesidad: el papel de los síntomas depresivos y la alimentación emocional en un modelo estratificado por sexo. Glob. Heal. Promot. 2022, 29, 171–179. [Google Scholar] [CrossRef] [PubMed]
- https://doi.org/10.1177/17579759221076584.
- Wang, Y.; Chung, M.C.; Wang, N.; Yu, X.; Kenardy, J. Social support and posttraumatic stress disorder: A meta-analysis of longitudinal studies. Clin. Psychol. Rev. 2021, 85, 101998. [Google Scholar] [CrossRef] [PubMed]
- Kadambi, S.; Soto-Perez-De-Celis, E.; Garg, T.; Loh, K.P.; Krok-Schoen, J.L.; Battisti, N.M.L.; Moffat, G.T.; Gil-Jr, L.A.; Mohile, S.; Hsu, T. Social support for older adults with cancer: Young International Society of Geriatric Oncology review paper. J. Geriatr. Oncol. 2019, 11, 217–224. [Google Scholar] [CrossRef] [PubMed]
- https://doi.org/10.1016/j.jgo.2019.09.005.
- Gracia, E, Herrero, J, Musitu, G. El apoyo social. Madrid: Promociones y Publicaciones Universitarias; 1995.
- Hobfoll, S E. The limitations of social support in the stress process. In: Sarason, IG, Sarason, BR. (Eds.). Social support: Theory, research and application. The Hague, The Netherlands: Nijhoff; 1985. p.
- Szkody, E.; Stearns, M.; Stanhope, L.; McKinney, C. Stress-Buffering Role of Social Support during COVID-19. Fam. Process. 2020, 60, 1002–1015. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S.; Creaven, A.-M.; Howard, S.; Ginty, A.T.; Whittaker, A.C. Gratitude, social support and cardiovascular reactivity to acute psychological stress. Biol. Psychol. 2021, 162, 108090. [Google Scholar] [CrossRef] [PubMed]
- Fogelman N, Hwang S, Sinha R, et al. Social Support Effects on Neural Stress and Alcohol Reward Responses. Curr Top Behav Neurosci. [Serial online]. 2022; 54:461-482. [CrossRef]
- Lee, S.-Y.; Park, M.-C.; Choi, S.-C.; Nah, Y.-H.; E Abbey, S.; Rodin, G. Stress, coping, and depression in non-ulcer dyspepsia patients. J. Psychosom. Res. 2000, 49, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Sewitch, M.J.; Abrahamowicz, M.; Bitton, A.; Daly, D.; Wild, G.E.; Cohen, A.; Katz, S.; Szego, P.L.; Dobkin, P.L. Psychological Distress, Social Support, and Disease Activity in Patients With Inflammatory Bowel Disease. Am. J. Gastroenterol. 2001, 96, 1470–1479. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Heal. Soc. Behav. 1983, 24, 385–96. [Google Scholar] [CrossRef]
- Remor, E. Psychometric Properties of a European Spanish Version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Veiga, P. Evaluación del apoyo social. In: Fernández-Ballesteros, R. (Eds.). El ambiente. Análisis psicológico. 3nd ed. Madrid: Pirámide. 1987. p. 125-149.

Table 1.
Stress averages according to the social support.
| n | Average | p-value | ||
|---|---|---|---|---|
| Low social support | Latency | 23 | 23.56 | 0.262 |
| Flare-up | 26 | 28.06 | ||
| High social support | Latency | 16 | 19.45 | 0.008 * |
| Flare-up | 26 | 28.21 |
Table 2.
Pearson’s Correlation Matrix considering the groups separately.
| Social support | Stress | ||
|---|---|---|---|
| Latency phase | Social support | 1 | - .476* |
| Stress | - .476* | 1 | |
| Flare-up | Social support | 1 | .057 |
| Stress | .057 | 1 |
*Correlation is significant at level .05 (bilateral).
Table 3.
Omnibus Test for the coefficients of the model.
| SS Grp | Chi-squared | df | Sig. | ||
|---|---|---|---|---|---|
| Low SS | Step 1 | Step | 1.275 | 1 | .259 |
| Block | 1.275 | 1 | .259 | ||
| Model | 1.275 | 1 | .259 | ||
| High SS | Step 1 | Step | 7.798 | 1 | .005 |
| Block | 7.798 | 1 | .005 | ||
| Model | 7.798 | 1 | .005 |
Table 4.
Prediction of the probability of a Flare-up in subjects with a high social support.
| SS Grp | Step | -2 log of likelihood | R-squared Cox and Snell | R-squared Nagelkerke |
|---|---|---|---|---|
| High SS | 2 | 31.631 (b) | .229 | .313 |
Table 5.
Binary logistic regression model for Flare-up prediction.
| B | E.T. | Wald | df | Sig. | Exp (B) | ||
|---|---|---|---|---|---|---|---|
| High social support | Stress | .143 | .060 | 5.707 | 1 | .017 | 1.154 |
| Constant | - 2.841 | 1.422 | 3.994 | 1 | .046 | .058 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



