Submitted:
05 April 2024
Posted:
08 April 2024
You are already at the latest version
Abstract
Background: The pandemic caused by the SARS-CoV-2 virus demonstrated the importance of prevention through a healthy diet and lifestyle, the most vulnerable people being those with severe chronic conditions, those who are overweight, and those with an unbalanced immune system. Methods: The evaluation of the eating habits and lifestyle of the Romanian population in the post-pandemic period was carried out based on a cross-sectional observational study with the help of a questionnaire. Results: 4704 valid answers were registered (3136 female and 1568 male respondents). Among the respondents, most of them belong to the young population, 2892 between the ages of 18 and 40, i.e., 61.5%. Most male respondents are overweight (1400) and obese (780). Most respondents indicated a tendency to consume 1-2 meals per day irregularly (p=0.6167). Only 974 respondents adopted a healthy diet, and 578 a healthy lifestyle. Conclusion: The present study reports low adherence to a healthy diet (20.7%) and healthy lifestyle (12.28%), especially among the young population (< 30 years). In the current context, it reports a reduced tendency to consume vegetables and fruits among the population, below the daily average recommended by the nutrition guidelines, a tendency towards sedentary behavior, and even deficient hydration of some of the respondents; these negative aspects can create a long term a series of nutritional and psycho-emotional imbalances. Our results evidence that complex surveys among the population are regularly required to investigate nutritional or lifestyle deficiencies; moreover, it could be helpful in further educational measures in nutrition, food, and environmental safety.
Keywords:
healthy diet
; balanced lifestyle
; metabolic disorders
; healthy habits
; public health
; nutritional education
1. Introduction
The quality of food and lifestyle strongly influence the quality of life and the body's resistance to the aggressions of environmental factors (pollution, microorganisms, climate changes). The statistics regarding the categories most vulnerable to the attacks of the SARS-Cov-2 virus indicate the elderly population, people with severe chronic conditions (diabetes, cardiovascular diseases, lung diseases, oncological diseases, morbid obesity), triggered and primarily aggravated by significant nutritional imbalances [1,2,3]. World Health Organization (WHO) indicates that obesity complications caused approximately 90% of deaths in 2021. The leading factors of the increase in the rate of non-communicable diseases are smoking, physical inactivity, excessive alcohol consumption, and unhealthy diet [3]. Many countries have begun to place increasing emphasis on stimulating nutritional programs for the prevention and balancing of nutritional imbalances. At the European Level, a series of cooperative multinational programs have been financed by stimulating collaborations between European Union states in order to reduce the incidence of obesity among the population, stimulating physical activity and strengthening healthy eating habits for the prevention of metabolic diseases, such as the European ERA4Health program [4].
On May 5, 2023, WHO declared that the threat posed by the COVID-19 pandemic has finally ended after more than three challenging years for global public health [5]. Throughout this period, the world faced immense social, economic, and health challenges, witnessing a significant loss of lives due to the SARS-CoV-2 virus, with a total death toll of 6,953,743 [6].
A healthy lifestyle means more than a set of rules to prevent or treat specific conditions; it represents a life concept that allows us to live healthily and build a world where people reach maximum physical and emotional potential [7]. A healthy lifestyle requires a constant balance between a harmonious diet, physical activity, adequate hydration of the body, rest, the absence of unhealthy habits (smoking, drug use, excessive alcohol consumption) as well as an environment as clean as possible, free of toxic agents and pathogens [8,9,10,11]. All these recommendations are ideal for increasing longevity, maintaining emotional well-being and mental balance, maintaining good general condition, and combating risk factors that endanger health.
A healthy diet must ensure sufficient macro and micronutrients to meet the body's physiological needs, which differ from one organism to another, depending on sex, age, physiological state, physical activity, and metabolism [12,13,14]. For a balanced and correct diet, we must consume plenty of fruits and vegetables because they represent an essential source of antioxidants, vitamins, mineral salts and fibers, and macronutrients. It also involves consuming diverse foods from all groups, rich in valuable nutrients, for all the body's needs [15,16,17,18]. Food is recommended to be consumed fresh or prepared using healthy cooking techniques. Vegetables and fruits should be eaten raw as much as possible to preserve their content rich in enzymes, vitamins, and minerals [19,20,21,22,23,24,25]. Food sources must be controlled, thus avoiding contamination with microplastics, pesticides, or heavy metals. Polluted marine areas for harvesting seafood or fish should also be avoided [26,27,28]. Eating contaminated food can seriously affect health [29,30,31]. In addition, it is essential to avoid excessive administration of drugs or their consumption without the supervision of a specialist [32,33] due to their potential toxicity.
Physical activity and sports practice are permanent means of maintaining health, increasing work capacity, and prolonging life, so it is recommended that people exercise for at least 30 minutes every day [34,35,36,37,38,39,40]. Under normal conditions, adults metabolize 2.5-3 liters of water daily, covered by water consumption as such and the water contained in the ingested food. Water intake and loss are regulated by thirst and hormonal mechanisms. During intense physical exercises, the need for water is increased, as it also happens in the case of increased temperatures in the external environment [41,42,43,44,45,46]. On the other hand, sleep is fundamental to the individual's physical and psycho-emotional health; 7-9 hours of sleep per night are recommended for people between 18 and 64 years old and 7-8 hours for people over 65 years old [47,48,49,50].
An analysis of the factors involved in the life span highlights an involvement percentage of approximately 25% of the genetic influence, while the environment and the lifestyle exert 75%. As a result, lifestyle and eating habits are essential for life quality and longevity [51,52,53], simultaneously influenced by the emotional state (Figure 1).
According to the data published in 2020 related to Romania's health profile, life expectancy, which increased after 2000, was seriously affected by the COVID-19 pandemic, falling far below the European Union (EU) average. In addition, the rate of alcohol consumption and unhealthy food among Romanians is above the EU average. Generally, behavioral risk factors (tobacco consumption, alcohol, unhealthy diet, and lack of physical activity) and environmental ones (pollution) cause over half of the number of deaths, and the mortality rate from treatable causes in Romania is the highest in the EU [55].
In this context, the present study aims to evaluate the nutritional status and lifestyle among the Romanian population, reporting the results to the standards of balanced nutrition by calculating adherence to a healthy diet and lifestyle. An investigation of the dietary patterns and lifestyle of the post-pandemic Romanian people was performed using a questionnaire to explore connections between dietary choices, behavioral aspects, and individuals' health status. This survey evaluated how respondents' commitment to a healthy lifestyle and well-rounded diet correlated with their overall health. An extensive statistical analysis highlighted the deviations from the healthy lifestyle. Our results could be a potential database for formulating suitable solutions to help the population get closer to normal standards.
2. Materials and Methods
2.1. Study Design
A cross-sectional observational study was conducted using an online questionnaire via the Google Forms platform from May 15 to August 15, 2023, to assess the Romanian population's dietary patterns and lifestyle choices. The survey, comprising 48 items, was circulated through official student networks, professional organizations, and social media platforms in Romania. Participation in the questionnaire was voluntary, with the only stipulation being age (participants had to be over 18 years old). Various Romanian institutions were involved, and the study was conducted on a sample of the country's general population. They agreed to disseminate the questionnaire to employees or students through the institutional email, and the responses of the volunteer participants after completing the questionnaire were automatically recorded on the Google Forms platform in real-time. Respondents were also asked to share the survey link with their colleagues and friends. The questionnaire aims to collect some socio-demographic information (age, sex, occupation, area of residence, studies), anthropometric data (height, weight), information related to eating habits correlated with lifestyle, psycho-emotional state correlated with health problems as well as the identification of factors that affect the psycho-emotional balance of the respondents. The final database was downloaded as a Microsoft Excel spreadsheet. The requirements related to participation in the survey conducted based on a questionnaire were: minimal age of 18 years, individual agreement to participate in the study with the guarantee of identity protection, and residence in Romania. In the first part of the questionnaire, the respondents were informed about the study's purpose and coordinating team.
Moreover, participants were guaranteed confidentiality concerning their sensitive personal information in compliance with the General Data Protection Regulation (GDPR). This assurance enabled the utilization and publication of the research results. The questionnaire dissemination process implied no discrimination based on gender, religion, or political beliefs. The present study agrees with the updated Declaration of Helsinki and received approval from the University of Medicine and Pharmacy Craiova Ethics Committee (No.121/07.05.2023).
2.2. Questionnaire Validation
Initially, the questionnaire underwent a pilot phase and was tested among a cohort of 250 participants over 18 years. Subsequently, a panel of 3 experts was convened to scrutinize the responses collected during the pilot phase, aiming to validate and enhance the questionnaire. The content validity ratio (CVR) and content validity index (CVI) were calculated [56,57]. Connelly (2008) proposed that the pilot study sample size should constitute a minimum of 10% of the intended sample size for the overall study [58]. In adherence to this recommendation, this study utilized the sample size calculation formula outlined by Viechtbauer et al. (2004), with parameters set at a 95% confidence level and a margin of error of ±4% [59]. The calculated sample size required for the pilot study was 94, which was deemed necessary for detecting feasibility issues. Given the potential variability in eating habits across different geographical regions of Romania, 250 participants were recruited.
In the pilot study, exploratory factor analysis (EFA) was conducted. The Kaiser-Meyer-Olkin (KMO) statistic yielded a value of 0.827, indicating the adequacy of the data for EFA [60,61]. Additionally, Bartlett's Test of Sphericity returned a statistically significant result (p < 0.001), suggesting the absence of multicollinearity within the dataset [62].
The 3 experts processed the final form of the questionnaire in such a way as to increase its clarity and accuracy, and the final corrected version after irrelevant items were removed is presented in Appendix A. The internal consistency of the questionnaire was analyzed using the Cronbach's α coefficient. For the present questionnaire, the value of Cronbach's α was 0.84, indicating good internal consistency and reliability of the scale [63,64].
After the questionnaire's distribution, 4704 valid responses were collected, with a confidence interval of 95% and a margin of error of ±3.05%.
2.3. Statistical Analysis
All variables are displayed using absolute frequencies (n) and relative frequencies (%). Recognizing that age significantly influences eating habits and lifestyle, shaped by various experiences, environmental shifts, and potential health issues, we categorized respondents into five age groups for data analysis. Hence, we restructured the continuous age variable into five categories: young individuals up to 30, early adults aged 31 to 40, middle-aged adults between 41 and 50, aging adults between 51 and 60, and seniors over 60. Additionally, we classified the people using Body Mass Index (BMI) value into four groups: underweight, normal weight, overweight, and obese.
The data were completed with new categorical variables named "Adherence to a healthy diet," which was constructed based on the answers to questions 9-21, and "Adherence to a healthy lifestyle" based on the answers to questions 27-28, 36, 38, 39, 43 and 44 all questions having answers from 1 ("very little" or "not at all") up to 5 ("a lot" or "always").
In assessing "Adherence to a healthy diet," the summation of responses constituted a raw score, subsequently converted into a T score (standardized). This conversion utilized an average of 54 and a standard deviation of 7 (ranging from a minimum of 28 to a maximum of 73). Scores surpassing 60 signified maximum adherence to a healthy diet, while those falling below 42 indicated adherence to an unhealthy diet.
In evaluating "Adherence to a healthy lifestyle," the aggregation of responses generated a raw score converted into a T score (standardized). This transformation utilized an average of 20 and a standard deviation of 4.5 (ranging from a minimum of 8 to a maximum of 33). Scores exceeding 26 indicated the highest adherence to a healthy lifestyle, while scores below 17 indicated an unhealthy one.
Pearson's Chi-square and Fischer tests were used to examine the potential association among variables (Gender, Body Mass Index groups, Residence, Education, Marital status, Employment status, Adherence to a healthy diet, and lifestyle) in connection with other ones included in the study, Spearman's correlation coefficient was calculated for associated continuous variables. All statistical analysis and graphic presentations were performed in IBM SPSS (Version 23.0) [65] and XLSTAT software [66]; the statistical significance level was considered at p-value < 0.05.
Finally, we analyzed the association between the outcome variables "Adherence to a healthy diet" and "Adherence to a healthy lifestyle" with the predictor variables such as Gender, Age groups, and BMI groups by applying logistic regression for a multinomial model. The results were expressed by odd ratio (OR), interval confidence (95%IC), and the associated p-values [67].
3. Results
3.1. Socio-Demographic and Anthropometric Data
The research conducted through the questionnaire dissemination obtained 4704 valid responses, with 66.7% from female respondents and 33.3% from male ones. Utilizing anthropometric measurements (weight and height) to compute Body Mass Index (BMI) via the Quetelet equation [body mass (kg)/height (m2)], the data was interpreted following the WHO's criteria [68]. Upon analyzing the anthropometric data, it was noted that most respondents, especially women (1726), fell into the normal weight category (2288). Conversely, a considerable proportion of the male group, totaling 718, was overweight [69]. Regarding their age, 61.5% are young, up to 40. All socio-demographic and anthropometric characteristics of the participants are presented in Table 1.
As can be seen from the data presented in Table 1, most participants in the study had higher education (61.6%), 17.8% were students, and 67.5% were employed. Most respondents live in the city (77.6%) and are married (57.6%).
3.2. Adherence to a Healthy Diet
In determining the respondents' adherence to a healthy diet, the assessment relied on the principles of a well-rounded and nutritious diet, as outlined in the introductory section. Healthy food intake with heightened nutritional value is aligned with the nutritional guidelines, emphasizing both frequency and quantity of consumption. An unhealthy diet, accompanied by unfavorable habits, corresponded to the lowest score, while a balanced diet with healthy habits received the highest score. A moderately healthy diet fell in the middle category.
As depicted in Table 2, most respondents were categorized under the moderately healthy diet group (3476), with 20.7% falling under the healthy diet category and 5.4% under the unhealthy diet category. Notably, a significant proportion of individuals in the unhealthy diet group were under 40 years old (73.2%), classified as overweight or obese (58.2%), residing in urban areas (75.6%), and engaging in daily work-related movements (48.8%).
Regarding adherence to a healthy diet within specific age groups, 16.62% of individuals up to 30 years old, 23.76% up to 40 years old, 21.47% up to 50 years old, and 22.45% up to 60 years old adhered to a healthy diet. Interestingly, 34.15% of individuals over 60 who completed the questionnaire were in the healthy diet group. Predominantly, respondents in the healthy diet group were female (698), had a normal weight (524), lived in urban areas (788), possessed higher education (66.9%), were married (596), and commuted daily for work (486).
According to the probability associated with the Chi-square tests, the variables that most influence the choice of group are Age: χ2=51.082, p<0.0001, Gender: χ2=9.763, p= 0.0076, BMI_group: χ2=22.368, p=0.0010, Level and education: χ2=15.96, p=0.0430 and Marital status: χ2=9.855.96, p=0.0429.
The healthy diet group was considered as a reference in the multinomial logistic regression model (Figure 2), and in the model, age, gender, BMI, Level of education, and marital status appeared to be significant predictors of leading an unhealthy diet (p < 0.05).
Men were 1.93 times more likely to achieve an unhealthy diet (95%CI = 1.26-2.96, p=0.024). Individuals between 18 and 30 years were more likely to score 1 and 2 for unhealthy diets (OR = 3.82, 95% CI = 1.76-4.28, p=0007) than those aged 51-60, used as the reference category. Single respondents were likelier to have an unhealthy diet than their married counterparts (OR = 1.89, 95% CI = 1.26-2.85, p=0.02). Moreover, participants with post-secondary education were more inclined to exhibit an unhealthy diet compared to those with higher education as the reference category (OR = 2.43, 95% CI = 1.23-4.8, p=0.01).
Obese participants demonstrated a higher likelihood of having an unhealthy diet (OR=1.88, 95% CI = 1.07-3.30), whereas those with normal weight were less likely to have an unhealthy diet (OR=0.5, 95% CI = 0.3-0.82, p=0.028).
In the multinomial logistic regression analysis, several significant factors were linked to maintaining a moderately healthy diet, including age, gender, and educational Level. Those aged over 60 years were less likely to uphold a moderately healthy diet (OR = 0.43, 95% CI = 0.26-0.7). Men exhibited a 1.27 times higher likelihood than women to achieve a moderately healthy diet (OR = 1.27, 95% CI = 1.08-1.61, p=0.085). Moreover, individuals with a general/primary education level (OR = 1.92, 95% CI = 1.1-3.34, p=0.02) were more inclined to maintain a moderately healthy diet than those with higher educational attainment.
Young people (18-30 years) showed the lowest adherence to a healthy diet among all the age groups participating in the study. As seen from Figure 3, in the diet of this age category, foods rich in fats and carbohydrates (fats, eggs, bread, sweetened carbonated drinks) predominate, while the consumption of vegetables, fruits, fish, and seafood is considerably reduced.
Using correspondence analysis (CA), significant differences (χ2=28.56, p < 0.0001) among four BMI groups and the type of food consumed were identified (Figure 4). Low consumption of vegetables, fruits, fish, seafood, cereals, and dairy products and more significant amounts of food, fats, sweets, and pastries in obese and underweight respondents compared to those with normal BMI.
With CA, significant differences (χ2=27.43, p=0.0002) were identified among the four age groups (Figure 5). The bi-plot indicated that 99.06% of the variability observed could be attributed to the two principal components (F1: 85.35%, F2: 13.71%). The younger generations aged 18–30 preferred sweets, pastries, cereals, and pasta, while those aged 41-50 had vegetables, fruits, and meat. Respondents over 50 had a significantly lower consumption of fish, seafood, and high-fat products compared to the other age groups.
The breakdown of BMI and gender concerning adherence to a healthy diet (Figure 6) reveals that individuals, regardless of gender, predominantly within the normal weight or underweight categories, align themselves with a healthy or moderately healthy diet. Conversely, those classified as overweight or obese are more inclined to follow a moderately healthy or unhealthy diet (p˂0.003).
3.3. Eating Habits and Lifestyle
The predominance of healthy habits (reduced alcohol consumption, smoking frequency, sports, recreational activities, sleep duration) and how meals are taken and distributed were examined to analyze the adherence to a healthy lifestyle.
According to the data presented in Table 3, 12.28% of the respondents belong to the group of those with a healthy lifestyle, 66.45% belong to the group of those with a moderately healthy lifestyle, and 21.25% belong to the group of those with an unhealthy lifestyle. Most of the respondents with increased adherence to the unhealthy lifestyle are young people up to 40 years old (65.6%), women (71%), overweight or obese (56.8%), they live in the urban environment (78%), are married (53.4%) and commute daily to work (50%). Respondents over 50 are more likely to be among those with increased adherence to a healthy lifestyle compared to those younger than them.
According to the probability associated with the Chi-square tests, the variables that most influence the choice of group are Gender: χ2=16.763, p=0.0002, BMI_group: χ2=81.752, p<0.0001, Marital status: χ2=9.595, p=0.0478 and Employment status χ2=34.644, p=0.0017.
The healthy lifestyle group was considered the reference in the multinomial logistic regression model (Figure 7).
The multinomial logistic regression analysis found that statistically significant factors associated with leading an unhealthy and moderately healthy lifestyle were gender, BMI, Marital status, and Employment status.
Men were 0.49 times less likely to achieve an unhealthy lifestyle (95%CI = 0.34-0.69, p<0.0001) and 0.67 times less likely to achieve a medium unhealthy lifestyle (95%CI = 0.5-0.9, p=0.0083) compared to women.
The obese people were more likely to have an unhealthy lifestyle (OR=1.98, 95% CI = 1.17-3.37, p=0.01), and those with normal weight and underweight were less exposed (OR=0.32, 95%CI = 0.22-0.46, p<0.0001; OR=0.17, 95%CI = 0.08-0.36, p<0.0001) and moderately healthy lifestyle (OR=0.39, 95%CI = 0.22-0.46; OR=0.57, 95%CI = 0.41-0.78).
Single respondents were more likely to have unhealthy lifestyles than married ones as reference category (OR = 1.66, 95%CI = 1.1-2.51, p=0.0154).
The participants who work in a mixed regime (OR = 0.42, 95%CI = 0.22-0.78, p=0.0064) and teleworking (OR = 0.59, 95%CI = 0.35-0.99, p=0.0493) were less likely to have an unhealthy lifestyle. The same observation regarding moderately unhealthy lifestyles is available for retired ones (OR = 0.46, 95%CI = 0.23-0.93, p=0.031).
As can be seen from Figure 8, in the case of both sexes, the overweight and obese respondents are mainly found in the group of those with lower adherence to a healthy lifestyle.
Based on the responses gathered (Figure 9), a more significant inclination towards insomnia was evident among obese respondents, with 12% experiencing this issue, compared to other categories, notably contrasting with underweight individuals at 3%. Furthermore, within the obese category, a higher tendency to sleep less than 7 hours per night was observed (43%) compared to other categories, particularly when compared to underweight respondents at 29%. Conversely, the underweight group displayed the highest tendency to sleep for 7-9 hours per night (61%) in contrast to other categories, especially the obese group, where only 41% reported this sleep duration (p˂0.001).
There is a close correlation between the quality of the diet and the adopted lifestyle, in the sense that people with greater adherence to the diet and healthy lifestyle have optimal body weight; the lower the adherence, the greater the risk of imbalances related to problems that in time lead to health complications (Figure 10).
Concerning adopting a restrictive diet for weight reduction (Figure 11), 53.5% of respondents claimed they never employed such a regimen, 26.9% stated occasional use, and 19.6% acknowledged frequent use. Surprisingly, among those using restrictive diets were individuals classified as underweight, suggesting either excessively stringent diets causing bodily issues or a lack of awareness regarding their below-normal body weight. Notably, 23% of overweight and 38% of obese respondents frequently resorted to restrictive diets, while only 14% of individuals with normal weight reported frequent use.
Among those who never employed a restrictive diet, approximately 87% were underweight, 61% had normal weight, 49% were overweight, and 28% were obese (p˂0.001). Female respondents predominantly admitted frequent use of restrictive diets (25%), contrasting sharply with male respondents at 8%. 71% of male respondents stated they never opted for a particular diet for weight loss (p˂0.001).
In line with the gathered responses, a significant part of individuals with excessive weight—37% among the overweight and 53% among the obese—admitted to excessive food consumption (p˂0.002). Interestingly, only 35% of underweight ones acknowledged insufficient food intake, suggesting a lack of awareness among respondents regarding their dietary habits corresponding to their body's requirements. Notably, other underweight persons did not acknowledge deficient food intake, although their body weight indicates otherwise. A mere 17.5% of respondents monitor their body weight, and a minimal part (1-2% across each BMI group) claimed to adhere to a nutritionist's recommended food intake ratio.
The data revealed a similar distribution across categories regarding the periodic health status assessment. Approximately 28% of respondents never evaluate their health status, with 24.3% doing so very rarely. Only 34.5% habitually assess their health status annually, and merely 11.4% do so at least twice a year—likely individuals with significant health concerns.
Analysis of the questionnaire data highlights that 47.2% of all respondents consume roughly 2L of water daily. However, a notable proportion do not hydrate adequately—12.8% consume less than 1L per day, and 33.6% consume approximately 1L daily. Surprisingly, this pattern remains consistent across BMI groups despite the expectation that water intake should correlate with body mass, not solely physical activity. Specifically, 11% of overweight and 12% of obese individuals consume less than 1L daily, while 33% of overweight and 30% of obese individuals consume around 1L per day (p=0.005).
The percentage of individuals engaging in daily sports activities for less than an hour or at least an hour is minimal, falling below 20%. Sedentary behavior is frequent among obese individuals (36% rarely engage in sports) and overweight ones (24% do not participate in sports, and 45% rarely do so). Surprisingly, even underweight respondents exhibit low activity levels (24% do not participate in sports, and 53% rarely do). Comparatively, individuals with normal weight show slightly better engagement in physical or sports activities than other BMI groups (p˂0.002). Although, as shown by the processed data from the questionnaire, very few respondents are used to frequently monitor their body weight or call a nutritionist to monitor their caloric intake from food, 37.7% of the respondents believe that they need the advice of a specialist to be able to choose healthy foods and 26.6% of them to eat balanced (Figure 12).
The leading causes that depreciate the state of health are considered stress (71.7%), lack of movement (55.1%), low sleep quality (48.5%), unhealthy diet (45.3%), and excessive work (34.1%). Only 29% of the respondents know the seriousness of pollution on their health (Figure 13).
Generally, the psycho-emotional state is mainly affected by stress (78.4%) and fatigue (58.1%). It is also negatively influenced by overworking, lack of communication, financial and family problems, and lifestyle (Figure 14).
Figure 15 shows that the main problems affecting well-being are fatigue (52.5%) and nervousness (31%).
There is a relatively high percentage of respondents who admit that they do not know if they have health problems (almost 20%), which is to be expected considering that many of them either do not turn to specialized medical personnel when encountering health problems by calling the first phase of self-medication, either do not regularly access specialized medical personnel when they encounter (Figure 16).
The main factors blamed by the respondents for depreciating the lifestyle are sedentariness (51.8%), sleep quality (47.7%), and lack of free time (44.9%). For the adverse effects, a series of unsolved stressful problems, insufficient financial resources, and the quality of the food products consumed can be noted (Figure 17).
Spending free time is essential in restoring the body and balancing the psycho-emotional. The top preferences include watching movies and TV programs (62.2%) and activities with family or friends (61.8%). Also, the tendency to spend free time on social networks, in the open air, or reading as a recreation is noticeable (Figure 18).
4. Discussion
The processing of the socio-demographic data collected from the survey participants highlights the presence in particular of young people under the age of 50 (Table 1), who represent 83.5% of the total number of respondents, the majority coming from the urban area (77.6 %) and having higher education (61.6%). More than 50% of the people interviewed commute to work every day and are married. The processing of the anthropometric data (Table 1) indicates that almost half of the respondents have problems with body weight (46.1%) because, according to BMI, they belong to the group of underweight (4.3%), overweight (28.3%) or obese (13.5%) people, which suggests from the start that there are nutritional imbalances. Regarding eating habits, the following aspects were observed: 30.3% of the respondents mainly consume saturated fats (butter in particular, but also lard or margarine), only 31.6% are used to consuming virgin or extra virgin vegetable oils, approximately 60% consume vegetables and fruits very rarely or at most only one portion per day, 43.3% consume fish and seafood very rarely or not at all and 41.8% only once a week, 33% consume meat daily, 42% consume meat more than two portions per week, 44% do not hydrate appropriately by consuming up to 1L of water per day. A first aspect worthy of note is represented by the fact that many of the respondents do not consume enough fiber. In combination with inadequate hydration of the body, there is an increased risk of accumulating toxins that can affect the state of health in the long term. The increased consumption of meat, correlated with a reduced intake of fiber and water, also represents a long-term aggravating factor that can lead to the appearance of metabolic diseases. Some studies indicate the tendency to reduce consumption of fruits and vegetables, especially among young people [70,71]. In a statistic published by the European Commission in 2019 based on a survey in the member states, there is an increased tendency to consume vegetables and fruits (at least 5 daily portions), especially among people with a high level of education. There are European countries where the population is used to consuming more significant amounts of vegetables daily (Spain, Portugal). However, Romania is included among the countries with a low daily consumption of vegetables [72]. In addition, surveys carried out during the pandemic to assess eating habits have indicated the reduced consumption of vegetable products among the Romanian population [73,74]. In order to increase the consumption of vegetables and fruits, it is necessary to implement some nutritional education actions starting from kindergartens and schools; moreover, paying particular attention to the menus in canteens in schools and kindergartens to include as many seasonal vegetables and fruits as possible. It is also necessary to carry out campaigns to raise awareness of the optimal hydration of the population, primarily since the state of dehydration of the body, even in reduced forms, affects the ability to concentrate and memory. Drivers who must react as efficiently as possible must know that inadequate long-term hydration can affect their driving skills and even cause accidents [75,76].
The low adherence of the respondents to the healthy diet (4.3%), according to the results obtained from the processing of the data collected with the help of the survey (Table 2), confirms the need to improve the eating habits of the Romanian population by stimulating the consumption of nutritious foods: vegetables, fruits, fish, seafood, unrefined vegetable fats. In addition to campaigns to promote nutritional information related to the quality of different food groups and their nutritional value, it would also be helpful to develop social measures aimed at stimulating domestic production of some essential foods (milk, eggs, cereals, vegetables, and fruits, fish) and to facilitate their commercialization on the domestic market by granting subsidies and facilities on the condition of limiting price increases in order to stimulate domestic consumption at all social levels of the population. It is known that shortening the distribution chain for food products usually implies the use of much smaller amounts of chemical additives.
A positive aspect worth noting is that in culinary preferences, food cooked at home, boiled, or steamed in the oven predominates. The preferred type of meat is represented by chicken (53.4%) and pork (30.5%).
In terms of lifestyle, the following aspects are noteworthy: most respondents have an irregular, even unbalanced, distributed meal schedule if we take into account the fact that 43.1% of them consume 1-2 meals a day, 40.8% of the respondents declared that they chaotically consume excess or insufficient food, 61.2% serve the meal in a hurry or during the meal they tend to do something else, 64.4% do not tend to do sports or exercise at all or only very rarely in the conditions in which 57.6% of the respondents work at the office or in front of the computer and 27.3% spend more than 8 hours a day in front of the computer, 18.5% spend around 6-7 hours a day in front of the computer, and 22.3% spend about 4-5 hours a day. Under these conditions, it is understandable that 40.4% of the respondents have insomnia or insufficient rest, 18.8% consider that they have a weakened immune system, 26.1% regularly use various methods to strengthen the immune system, 78.4% of the respondents are stressed, 52.5% are tired, and 31% are frequently tired. Alteration of the psycho-emotional status is the result of an unbalanced lifestyle, with a chaotic diet and low consumption of vegetable products, insufficient hydration, an accentuated tendency to be sedentary, a recreational activity that takes place predominantly in front of the television or on social networks (Figure 18), as well as a neglect of the periodic evaluation of the state of health. The neglect of the state of health is also noticeable by the reduced tendency of underweight or overweight people to resort to measures to help them balance the body, given that many respondents are aware of the negative aspects that affect their health: monitoring food consumption and body weight, hydration corresponding to the body (a measure that helps overweight people in particular to consume smaller amounts of food), calling on the services of a nutritionist. Furthermore, in this direction, a series of measures are required to help reduce imbalances: the promotion of outdoor party campaigns both through festive activities and through sports competitions aimed at the population, the intensification of recreational activities through exercise in schools and kindergartens in order to combat sedentary lifestyle, the implementation of mandatory legislative measures to monitor the state of health based on the package of free analyzes existing in the rights of insured persons (mostly neglected rights), the introduction of psychological counseling services in large communities (schools, high schools, universities, large companies with over 21 employees). Excessive work, inadequate rest, lack of engaging recreational activities that increase self-esteem (participation in socio-cultural activities), communication problems related to unhealthy habits, and an unbalanced diet affects not only the state of health but also pro-duce disorders of psycho-emotional behavior such as states of nervousness, anxiety, depression, loss of appetite or emotional eating, altering the ability to work but also to integrate into communities (Figure 15 and Figure 17).
The positive aspects of the lifestyle highlighted by the present study consist of reduced consumption of alcoholic beverages among the respondents (63% declared that they consume very rarely or not at all) and diminished tendency to smoke. Comparing this rate with the results collected in the last 16 years [77] (70.4% are non-smokers), only 17.6% of the respondents declared that they smoke excessively.
Moreover, all these observed imbalances confirm the health problems highlighted by the National Study on the Prevalence of Diabetes, Prediabetes, Overweight, Obesity, Dyslipidemia, Hyperuricemia and Chronic Kidney Disease (PREDATORR), started in 2013 and carried out by the Romanian Society of Nephrology in partnership with The Romanian Society of Diabetes, Nutrition and Metabolic Diseases, for almost a year and a half, on a representative sample of approximately 3000 people (20-79 years), from 101 centers in Romania.
According to the PREDATORR epidemiological study, approximately 11.6% of the adult population of Romania (20-79 years old) has diabetes. This value is 31.8% higher than the global average (8.8%) reported and 70% above the European average. Following the study, it was also found that over 80% of the adult population of Romania aged between 20-79 years have abnormalities of serum lipids (19% have dyslipidemia, 81% have dyslipidemia with disorders of one or more lipid factors), while over 16% of Romanians in the same age range have hyperuricemia. Regarding body weight, the study data indicate that 31.4% of Romanians have first-degree obesity, 21.5% second-degree, and 2.7% have morbid obesity. Also, 34.6% are overweight and on the verge of obesity. The study also indicates a high prevalence of 6.7-7.7% (depending on the calculation formula) for chronic kidney disease and 61.7% for blood pressure. The study also highlighted the fact that about 2.4% of patients with diabetes were undiagnosed [78,79,80].
The implementation of measures to increase the quality of public health by promoting a favorable nutritional status and a healthy lifestyle correlated with an environment with as little pollution as possible is the key to ensuring an efficient workforce, a population with a low incidence of various diseases, including the mental nature with direct benefits on the public health system by reducing the costs related to the protection programs of the various chronic patients but also on the increase in the life expectancy of the population.
It is also necessary to boost the consumption of vegetable proteins (especially legumes, nuts, and seeds) in the context in which health specialists draw attention to the fact that animal breeding activity is becoming more and more polluting with the demographic expansion of the population at the world level. The aim is to create a sustainable food future that will serve more than nine billion people by 2050 [81].
Our study has several limitations, including the lower participation of male respondents, elderly participants, and rural residents. The obtained data report an alteration of the psycho-emotional state caused by the disordered lifestyle and unbalanced diet. More detailed studies are required to evaluate the degree of alteration of the psycho-emotional components under the influence of lifestyle and eating habits.
5. Conclusions
The present study, performed on 4704 Romanian participants over the age of 18, reports low adherence to a healthy diet (20.7%) and healthy lifestyle (12.28%), especially among the young population (< 30 years). In the current context, it highlights a series of problems related to the lifestyle and diet of the Romanian population. Our results evidence that complex surveys among the population are regularly required to investigate nutritional or lifestyle deficiencies. This study could be helpful in further educational measures in nutrition, food, and environmental safety. Moreover, data analysis could underline further administrative and legislative regulations regarding potential assistance in large autochthonous communities to increase the population's adherence to a healthy diet by periodically evaluating their health status. It also highlights the progressive need for people's involvement in environmental protection to ensure pollution reduction, a suitable lifestyle, and optimal psycho-emotional balance with beneficial effects on the well-being and health of the Romanian population.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, M.M. and V.P.; methodology, M.M., S.M.N., E.G. and C.T.S.; software, S.B. and C.E.L.; validation, M.M. and V.P.; formal analysis, S.S.B., E.O., N.K. and C.E.L.; investigation, A.M., C.T.S., E.G. and D.L.; resources, S.S.B. and E.O.; data curation, M.M.; writing—original draft preparation, S.M.N. and A.M.M.; writing—review and editing, S.M.N. and A.M.M.; visualization, V.P., supervision, M.M. and V.P.; project administration, M.M. and V.P.; funding acquisition, S.B. and D.L. All authors have read and agreed to the published version of the manuscript.
Funding
No funding was available for the current study.
Institutional Review Board Statement
The University of Medicine and Pharmacy Ethics Commission in Craiova approved the study with Consent Doc.—121/07.05.2023.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
QUESTIONNAIRE regarding adherence to the healthy lifestyle and balanced diet of the Romanian population
Personal data:
1. Please mention your age (in years):
2. Please mention your gender:
Male
Feminine
Other
3. Please mention your currently reside:
Town
Commune/Village
4. Please mention your employment status:
Unemployed
Socially assisted
Householder
Retired
Student
Teleworking
I go to work every day
I work in a mixed regime (telework and commuting)
5. Please state your marital status:
Single
Divorced / separated
Married
6. Please mention the Level of education:
General/primary studies
Secondary education (baccalaureate degree)
Post-secondary studies
Higher education (bachelor's degree)
Postgraduate studies (master's, residency, doctorate, other specializations)
Anthropometric data
7. Please mention your weight (in kg):
8. Please mention your height (in cm):
Eating habits:
9. What is the main type of dietary fat consumed?
Margarine
Lard, tallow
Butter
Refined vegetable oil
Extra virgin or virgin vegetable oil
10. How many servings of vegetzables (approx. 100 g) do you eat every day?
Very rarely or not at all
One
Two
Three
More than three
11. How many servings of fruit (approx. 100 g) do you eat every day?
Very rarely or not at all
One
Two
Three
More than three
12. How often do you eat meat?
Very rarely or not at all
Once a week
Twice a week
More than 2 times a week
Daily
13. How often do you consume carbonated or sweetened drinks (1 portion = 330 ml, a glass)?
Daily
More than 2 times a week
Twice a week
Once a week
Very rarely or not at all
14. How often do you consume alcoholic beverages (1 glass of wine=125ml, 1 glass of soft drink spirits =50ml)?
Daily more than one serving
One serving daily
More than 2 times a week
Twice a week
Once a week
Very rarely or not at all
15. How often do you eat fish or seafood?
Very rarely or not at all
Once a week
Twice a week
More than 2 times a week
Daily
16. How often do you eat sweets / pastries?
Daily
More than 2 times a week
Twice a week
Once a week
Very rarely or not at all
17. How often do you eat pasta, rice or other grains?
Very rarely or not at all
Once a week
Twice a week
More than 2 times a week
Daily
18. How much bread do you eat per day?
More than 12 slices
8-12 slices
5-7 slices
1-4 slices
Very rarely or not at all
19. How often do you consume dairy products?
Very rarely or not at all
Once a week
Twice a week
More than 2 times a week
Daily
20. How many eggs do you eat per week?
Very rarely or not at all
1 - 2 eggs
3 - 4 eggs
5 - 7 eggs
More than 7 eggs
21. Which food category do you eat most often?
Fast food products
Pizza, snacks, pastries, sweets
Products made from sausages and preserves
Food cooked in restaurants
Home cooked food
22. What type of cooked food do you eat most often?
Fried foods
Food prepared by cooking on wood or coals
Grilled food
Food prepared in the oven
Boiled or steamed foods
Non-thermally processed foods
23. How much water do you drink per day?
Under 1L
1 L
2 L
3 L
Over 3 L
24. Which category of liquids do you tend to consume most often?
Alcoholic drinks: sparkling drinks/wine, beer, etc.
Carbonated or sweetened non-alcoholic drinks
Coffee
What do you have
Plain water and natural juices
25. Which category of food products predominates in the daily diet?
Produce
Fish and seafood preparations
Cereals and pasta
Dairy products
Meat and meat preparations
Sweets and pastries
Foods high in fat
26. What type of meat do you eat most often?
Fish and/or seafood
Bird meat
Rabbit meat
Beef
Game meat
Pork
Mutton
Goat meat
Other
I don't eat meat
Lifestyle:
27. How are meals distributed per day?
Consuming 1-2 meals a day without a fixed schedule
I eat 3 meals a day without a fixed schedule
I eat 3 meals a day and 1-2 snacks without a fixed schedule
Consume 3 meals a day according to a fixed schedule
Consume 3 meals a day and 1-2 snacks according to a fixed schedule
28. How do you rate the amount of food consumed daily?
I consider myself a chaotic, excessive eater
I believe that I eat chaotically, insufficiently
Weighted food consumption, without excesses
Consume food according to the needs of the body by monitoring the weight
I eat food according to the ration established by a specialist
29. Do you think that your diet has affected your health?
I do not know
Yes, because I eat junk food
Yes, because I overeat
Yes, because I don't eat enough
No
30. When you serve the meal how do you do it?
I generally eat in a hurry
During the meal I usually do something else
They serve the meal quietly and unhurriedly
31. Do you think you need the advice of a nutritionist?
Yes, to help me choose healthy foods
Yes, to help me eat weighted
No
32. Which of the following factors do you consider to be most likely to affect your current state of health?
Overwork
Sleep quality
The stress
Unhealthy diet
Lack of movement
pollution
Excessive smoking
Excessive consumption of alcohol or drugs
Financial problems
33. What type of diet are you currently on?
Normal, omnivorous diet
Vegetarian diet/variants
Vegan diet/variants
Ketogenic diet
Mediterranean diet
Other
34. Have you ever gone on a diet to lose weight?
Yes, often
Yes, very rarely
No
35. What type of activity do you do?
Work in difficult and dangerous conditions (construction site, factory, mine, etc.)
Work in front of the computer or special devices
Office work or activity with minimal movement
Work standing
Work outdoors in non-hazardous conditions
36. Do you usually do sports / exercise?
Not
Yes, very rarely
Yes, 2-3 times a week
Yes, daily under an hour
Yes, daily at least one hour
37. Where do you do sports / exercise?
The home
Outdoor
Gym
I don't do sports / exercise
38. Do you smoke?
Yes, excessively daily
Yes, daily 1-2 cigarettes
Yes, 2-3 times a week
Yes, occasionally
No
39. How many hours a night you usually sleep?
I have frequent insomnia
Under 7 hours per night
Over 9 hours a night
7-9 hours a night
40. How do you rate the state of your immune system?
I consider myself to have a strong immune system
I believe I have a weakened immune system
I regularly use various methods to strengthen the immune system
41. What do you consider to be the main factors affecting your mental state?
Health problems
Fatigue state
The stress
Overwork
Problems at work
Lack of communication, isolation
Inappropriate surroundings
Family problems
Financial problems
42. What kind of problems do you encounter?
I am often tired
I am often nervous
I am often depressed
I have frequent panic attacks / anxiety states
I eat emotionally
I'm not hungry
I'm fine, I have no problem
43. Do you go to specialist doctors when you have health problems?
Never
Yes, only in very serious cases
Yes, generally when self-medication doesn't work
Yes, when the state of health deteriorates more
Yes, every time there are problems
44. Do you regularly assess your health?
No
Yes, very rarely
Yes, after two years
Yes, once a year
Yes, at least twice a year
45. How much time do you spend on average per day in front of the computer, tablet, phone or TV?
Over 8 hours
6-7 hours
4-5 hours
2-3 hours
Under 1 hour
46. What type of chronic conditions do you have?
Arterial Hypertension
Cardiovascular diseases
Diabetes
Gout
Obesity
Pulmonary diseases
Renal diseases
Autoimmune diseases
Gastric conditions
Liver diseases
Respiratory diseases
Rheumatic diseases
Bone disorders
Mental disorders
Other
I am clinically healthy
I do not know
47. What do you feel is currently lacking in a healthier lifestyle?
Free time
Peaceful sleep, rest
Financial resources
Advice from a nutritionist
Access to quality medical services
Solving stressful problems
Communication and socialization
Reducing time spent on social networks or various sites
Nutritional knowledge
Movement, physical activity
Quality food products
Nothing
48. How do you spend your free time?
Watching movies and TV programs
On social networks or various websites
Reading
DIY (Do It Yourself)
With family or friends
Outdoor activities
Participation in cultural activities
Participation in charity events
Participation in training courses
Other ways.
References
- Ahmad Malik, J.; Ahmed, S.; Shinde, M.; Almermesh, M.H.S.; Alghamdi, S.; Hussain, A.; Anwar S. The Impact of COVID-19 On Comorbidities: A Review Of Recent Updates For Combating It. Saudi J Biol Sci. 2022, 29(5):3586-3599. [CrossRef]
- Moccia, F.; Gerbino, A.; Lionetti, V.; Miragoli, M.; Munaron, L.M.; Pagliaro, P.; Pasqua, T.; Penna, C.; Rocca, C.; Samaja, M.; Angelone T. COVID-19-associated cardiovascular morbidity in older adults: a position paper from the Italian Society of Cardiovascular Researches. Geroscience, 2020, 42(4):1021-1049. [CrossRef]
- WHO European Regional Obesity Report 2022. Copenhagen: WHO Regional Office for Europe; 2022. Licence: CC BY-NC-SA 3.0 IGO. https://apps.who.int/iris/bitstream/handle/10665/353747/9789289057738-eng.pdf, accessed on 1.08.2023.
- https://www.era-learn.eu/network-information/networks/era-for-health; accessed on 1.08.2023.
- World Health Organization. Statement on the fifteenth meeting of the IHR (2005) Emergency Committee on the COVID-19 pandemic. https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic; accessed on 1.08.2023.
- WHO Coronavirus (COVID-19) Dashboard; https://covid19.who.int/; accessed on 5.08.2023.
- Svalastog, A.L.; Donev, D.; Jahren Kristoffersen, N.; Gajović, S. Concepts and definitions of health and health-related values in the knowledge landscapes of the digital society. Croat Med J., 2017, 58(6):431-435. [CrossRef]
- Ng, R.; Sutradhar, R.; Yao, Z.; Wodchis, W.P.; Rosella, L.C. Smoking, drinking, diet and physical activity-modifiable lifestyle risk factors and their associations with age to first chronic disease. Int J Epidemiol., 2020, 49(1):113-130. [CrossRef]
- Hu, F.B. Globalization of diabetes: the role of diet, lifestyle, and genes. Diabetes Care. 2011, 34(6):1249-57. PMID: 21617109. [CrossRef]
- Thavorn, K.; Maxwell, C.J.; Gruneir, A.; Bronskill, S.E.; Bai, Y.; Koné Pefoyo, A.J.; Petrosyan, Y.; Wodchis W.P. Effect of socio-demographic factors on the association between multimorbidity and healthcare costs: a population-based, retrospective cohort study. BMJ Open. 2017, 7(10):e017264. [CrossRef]
- Hall, K.D.; Heymsfield, S.B.; Kemnitz, J.W.; Klein, S.; Schoelle, D.A.; Speakman, J.R. Energy balance and its components: implications for body weight regulation. Am J Clin Nutr. 2012, 95(4):989-94. [CrossRef]
- Chen, Y.; Michalak, M.; Agellon, L.B. Importance of Nutrients and Nutrient Metabolism on Human Health. Yale J Biol Med. 2018, 91(2):95-103.
- Choi, S.W.; Friso, S. Epigenetics: A New Bridge between Nutrition and Health. Adv Nutr. 2010, 1(1):8-16. [CrossRef]
- Kanehisa, M.; Araki, M.; Goto, S.; Hattori, M.; Hirakawa, M.; Itoh, M.; Katayama, T.; Kawashima, S.; Okuda, S.; Tokimatsu, T.; Yamanishi, Y. KEGG for linking genomes to life and the environment. Nucleic Acids Res. 2008, 36(Database issue):D480-4. [CrossRef]
- Slavin, J.L.; Lloyd, B. Health benefits of fruits and vegetables. Adv Nutr. 2012, 3(4):506-16. [CrossRef]
- Song, W.; Derito, C.M.; Liu, M.K.; He, X.; Dong, M.; Liu, R.H. Cellular antioxidant activity of common vegetables. J Agric Food Chem. 2010, 58(11):6621-9. [CrossRef]
- Hamidi, M.; Boucher, B.A.; Cheung, A.M.; Beyene, J.; Shah, P.S. Fruit and vegetable intake and bone health in women aged 45 years and over: a systematic review. Osteoporos Int. 2011, 22(6):1681-93. [CrossRef]
- Ioniță-Mîndrican, C.-B.; Ziani, K.; Mititelu, M.; Oprea, E.; Neacșu, S.M.; Moroșan, E.; Dumitrescu, D.-E.; Roșca, A.C.; Drăgănescu, D.; Negrei, C. Therapeutic Benefits and Dietary Restrictions of Fiber Intake: A State of the Art Review. Nutrients, 2022, 14, 2641; [CrossRef]
- Lee, S.; Choi, Y.; Jeong, H.S.; Lee, J.; Sung, J. Effect of different cooking methods on the content of vitamins and true retention in selected vegetables. Food Sci Biotechnol. 2017, 27(2):333-342. [CrossRef]
- Tian, J.; Chen, J.; Lv, F.; Chen, S.; Chen, J.; Liu, D.; Ye, X. Domestic cooking methods affect the phytochemical composition and antioxidant activity of purple-fleshed potatoes. Food Chem. 2016, 197 Pt B:1264-70. [CrossRef]
- Knecht, K.; Sandfuchs, K.; Kulling, S.E.; Bunzel, D. Tocopherol and tocotrienol analysis in raw and cooked vegetables: a validated method with emphasis on sample preparation. Food Chem. 2015, 169:20-7. [CrossRef]
- https://www.who.int/news-room/fact-sheets/detail/healthy-diet; accesed on 14.09.2022.
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: the EAT–Lancet Commission on healthy diets from sustainable food systems. The Lancet, 2019, 393(10170):447-492; [CrossRef]
- Cena, H.; Calder, P.C. Defining a Healthy Diet: Evidence for The Role of Contemporary Dietary Patterns in Health and Disease. Nutrients. 2020, 12(2):334. [CrossRef]
- Probst, Y.C.; Guan, V.X.; Kent, K. Dietary phytochemical intake from foods and health outcomes: A systematic review protocol and preliminary scoping. BMJ Open. 2017; 7:e013337. [CrossRef]
- Ionita, A.C.; Mititelu, M.; Moroşan, E. Analysis of heavy metals and organic pollutants from some Danube river fishes, Farmacia, 2014, 62(2):299-305.
- Mititelu, M.; Moroşan, E.; Neacsu, S.M.; Ioniţă, E.I. Research regarding the pollution degree from romanian Black Sea coast. Farmacia, 2018, 66, 1059–1063. http://doi.org/10.31925/farmacia.2018.6.20.
- Mititelu, M.; Nicolescu, T.O.; Ioniţă, C.A.; Nicolescu, F. Study of Heavy Metals and Organic Polluants From Some Fisches of Danube River, Journal of Enviromental Protection and Ecology, 2012, 13(2A):869-874.
- Mititelu, M.; Nicolescu, T.O.; Ioniţă, C.A.; Nicolescu, F. Heavy Metals Analisys in Some Wild Edible Mushrooms. J. Environmental Prot. Ecol. 2012, 13, 875–879.
- Mititelu, M.; Ioniţă, A.C.; Moroşan, E. Research regarding integral processing of mussels from Black Sea. Farmacia 2014, 62, 625–632.
- Mititelu, M.; Neacsu, S.M.; Oprea, E.; Dumitrescu, D.-E.; Nedelescu, M.; Drăgănescu, D.; Nicolescu, T.O.; Rosca, A.C.; Ghica, M. Black Sea Mussels Qualitative and Quantitative Chemical Analysis: Nutritional Benefits and Possible Risks through Consumption. Nutrients, 2022, 14, 964. [CrossRef]
- Ioniţă, A.C.; Ghica, M.; Moroşan, E.; Nicolescu, F.; Mititelu, M. In vitro effects of some synthesized aminoacetanilide n’-substituted on human leukocytes separated from peripheral blood, Farmacia, 2019, 67(4), 684-690. [CrossRef]
- Johnston, A.; Holt, D.W. Substandard drugs: a potential crisis for public health. Br J Clin Pharmacol. 2014, 78(2):218-43. [CrossRef]
- Dunton, G.F. Sustaining Health-Protective Behaviors Such as Physical Activity and Healthy Eating. JAMA. 2018, 320(7):639-640. [CrossRef]
- Jakicic, J.M.; Rogers, R.J.; Davis, K.K.; Collins, K.A. Role of physical activity and exercise in treating patients with overweight and obesity. Clin. Chem. 2018, 64, 99–107. [CrossRef]
- Park, J.H.; Moon, J.H.; Kim, H.J.; Kong, M.H.; Oh, Y.H. Sedentary Lifestyle: Overview of Updated Evidence of Potential Health Risks. Korean J Fam Med. 2020, 41(6):365-373. [CrossRef]
- Rees-Punia, E.; Evans, E.M.; Schmidt, M.D.; Gay, J.L.; Matthews, C.E.; Gapstur, S.M.; Patel, A.V. Mortality Risk Reductions for Replacing Sedentary Time With Physical Activities. Am J Prev Med. 2019; 56(5):736-741. [CrossRef]
- Mullane, S.L.; Buman, M.P.; Zeigler, Z.S.; Crespo, N.C.; Gaesser, G.A. Acute effects on cognitive performance following bouts of standing and light-intensity physical activity in a simulated workplace environment. J Sci Med Sport. 2017, 20(5):489-493. [CrossRef]
- Magnon, V.; Vallet, G.T.; Auxiette, C. Sedentary Behavior at Work and Cognitive Functioning: A Systematic Review. Front Public Health. 2018, 31;6:239. [CrossRef]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2010. 7th Edition, Washington, DC: U.S. Government Printing Office, December 2010. https://health.gov/sites/default/files/2020-01/DietaryGuidelines2010.pdf, accesed on 14.09.2022.
- Jequier, E.; Constant, F. Water as an essential nutrient: The physiological basis of hydration. Eur. J. Nutr. 2010, 64:115–123. [CrossRef]
- Lorenzo, I.; Serra-Prat, M.; Yébenes, J.C. The Role of Water Homeostasis in Muscle Function and Frailty: A Review. Nutrients. 2019; 11(8):1857. [CrossRef]
- Nakamura, Y.; Watanabe, H.; Tanaka, A.; Yasui, M.; Nishihira, J.; Murayama, N. Effect of Increased Daily Water Intake and Hydration on Health in Japanese Adults. Nutrients. 2020, 12(4):1191. [CrossRef]
- Armstrong, L.E.; Ganio, M.S.; Casa, D.J.; Lee, E.C.; MacDermott, B.P.; Klau, J.F.; Jimenez, L.; Lieberman, H.R. Mild dehydration affects mood in healthy young women. J. Nutr. 2012, 142:328–388. [CrossRef]
- Benton, D.; Burgess, N. The effect of the consumption of water on the memory and attention of children. Appetite. 2009, 53:143–146. [CrossRef]
- Zhou, Y.; Zhu, X.; Qin, Y.; Li, Y.; Zhang, M.; Liu, W.; Huang, H.; Xu, Y. Association between total water intake and dietary intake of pregnant and breastfeeding women in China: a cross-sectional survey. BMC Pregnancy Childbirth. 2019, 19(1):172. [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S. M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E. S.; Kheirandish-Gozal, L.; Neubauer, D. N.; O'Donnell, A. E.; Ohayon, M.; Peever, J.; Rawding, R.; Sachdeva, R. C.; Setters, B.; Vitiello, M. V.; Ware, J. C.; Adams Hillard, P. J. National Sleep Foundation's sleep time duration recommendations: methodology and results summary. Sleep health, 2015, 1(1), 40–43. [CrossRef]
- Vyazovskiy, V.V. Sleep, recovery, and metaregulation: explaining the benefits of sleep. Nat Sci Sleep. 2015, 7:171-84. [CrossRef]
- Cirelli, C.; Tononi, G. Is sleep essential? PLoS Biol. 2008, 6(8):e216. [CrossRef]
- Vassalli, A.; Dijk, D.J. Sleep function: current questions and new approaches. Eur J Neurosci. 2009, 29(9):1830-41. [CrossRef]
- Passarino, G.; De Rango, F.; Montesanto, A. Human longevity: Genetics or Lifestyle? It takes two to tango. Immun Ageing. 2016, 13:12. [CrossRef]
- Limpens, M.A.M.; Asllanaj, E.; Dommershuijsen, L.J.; Boersma, E.; Ikram, M.A.; Kavousi, M.; Voortman, T. Healthy lifestyle in older adults and life expectancy with and without heart failure. Eur J Epidemiol, 2022, 37, 205–214; [CrossRef]
- Chudasama, Y.V.; Khunti, K.; Gillies, C.L.; Dhalwani, N.N.; Davies, M.J.; Yates, T.; Zaccardi, F. Healthy lifestyle and life expectancy in people with multimorbidity in the UK Biobank: A longitudinal cohort study. PLoS Med, 2020, 17(9): e1003332. [CrossRef]
- Reichenberger, J.; Schnepper, R.; Arend, A.K.; Blechert, J. Emotional eating in healthy individuals and patients with an eating disorder: evidence from psychometric, experimental and naturalistic studies. Proc Nutr Soc. 2020, 79(3):290-299. [CrossRef]
- European Commission - State of Health in the EU · România · Profilul de țară din 2021 în ceea ce privește sănătatea; https://health.ec.europa.eu/system/files/2022-01/2021_chp_romania_romanian.pdf; accessed on 10.05.2023.
- Lawshe, C.H. A quantitative approach to content validity. Pers. Psychol., 1975, 28 (4): 563-575.
- Yusoff, M.S.B. ABC of Content Validation and Content Validity Index Calculation, Educ. Med. J., 2019, 11, 49-54.
- Connelly, L. M. Pilot studies. Medsurg Nursing, 2008, 17(6):411-2.
- Viechtbauer, W.; Smits, L.; Kotz, D.; Budé, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simpleformula for the calculation of sample size in pilot studies. Journal of Clinical Epidemiology, 2015, 68(11):1375-1379. [CrossRef]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika, 1974, 39(1):31-36. [CrossRef]
- Bartlett, M.S. A note on the multiplying factors for various χ2 approximations. Journal of the Royal Statistical Society, 1954, 16(2):296-298.
- Bonkat, G.; Bartoletti, R.; Bruyére, F.; Cai, T.; Geerlings, S.E.; Köves, B.; Schubert, S.; Wagenlehner, F. EAU Guidelines on Urological Infections 2020. In European Association of Urology Guidelines. 2020 Edition. (Vol. presented at the EAU Annual Congress Amsterdam 2020). European Association of Urology Guidelines Office. http://uroweb.org/guideline/urological-infections/ accessed on 05.05.2023.
- Ioniță-Mîndrican, C.-B.; Mititelu, M.; Musuc, A.M.; Oprea, E.; Ziani, K.; Neacșu, S.M.; Grigore, N.D.; Negrei, C.; Dumitrescu, D.-E.; Mireșan, H.; Roncea, F.N.; Ozon, E.A.; Măru, N.; Drăgănescu, D.; Ghica, M. Honey and Other Beekeeping Products Intake among the Romanian Population and Their Therapeutic Use. Appl. Sci. 2022, 12, 9649. [CrossRef]
- Năstăsescu, V.; Mititelu, M.; Stanciu, T.I.; Drăgănescu, D.; Grigore, N.D.; Udeanu, D.I.; Stanciu, G.; Neacșu, S.M.; Dinu-Pîrvu, C.E.; Oprea, E.; Ghica, M. Food Habits and Lifestyle of Romanians in the Context of the COVID-19 Pandemic. Nutrients 2022, 14, 504. [CrossRef]
- IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.
- Addinsoft (2020) XLSTAT Statistical and Data Analysis Solution. New York. https://www.xlstat.com.
- Venables, W.N.; Ripley, B.D. Modern Applied Statistics with S. Fourth Edition. Springer, New York., 2002, ISBN 0-387-95457-0.
- Branca, F.; Nikogosian, H.; Lobstein, T. World Health Organization. Regional Office for Europe. In The Challenge of Obesity in the WHO European Region and the Strategies for Response; WHO Regional Office for Europe: Copenhagen, Denmark, 2007; ISBN 9789289014083.
- Ashwell, M.; Gibson, S. Waist-to-height ratio as an indicator of early health risk: Simpler and more predictive than using a matrix based on BMI and waist circumference. BMJ Open, 2016, 6, e010159. [CrossRef]
- Frank, S.M.; Webster, J.; McKenzie, B.; Geldsetzer, P.; Manne-Goehler, J.; Andall-Brereton, G.; Houehanou, C.; Houinato, D.; Gurung, M.S.; Bicaba, B.W.; McClure, R.W.; Supiyev, A.; Zhumadilov, Z.; Stokes, A.; Labadarios, D.; Sibai, A.M.; Norov, B.; Aryal, K.K.; Karki, K.B.; Kagaruki, G.B.; Mayige, M.T.; Martins, J.S.; Atun, R.; Bärnighausen, T.; Vollmer, S.; Jaacks, L.M. Consumption of Fruits and Vegetables Among Individuals 15 Years and Older in 28 Low- and Middle-Income Countries. J Nutr. 2019; 149(7):1252-1259. [CrossRef]
- Menozzi, D.; Sogari, G.; Mora, C. Explaining Vegetable Consumption among Young Adults: An Application of the Theory of Planned Behaviour. Nutrients. 2015; 7(9):7633-50. [CrossRef]
- https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Nutritional_habits_statistics&oldid=572524; accesed on 14.06.2023.
- Mititelu, M; Stanciu, T.I.; Udeanu, D.I.; Popa, D.E.; Drăgănescu, D.; Cobelschi, C.; Grigore, N.D.; Pop, A.L.; Ghica, M. The impact of covid-19 lockdown on the lifestyle and dietary patterns among romanian population, Farmacia, 2021, (69)1, 1-11. [CrossRef]
- Nitu, I.; Rus, V.A.; Sipos, R.S.; Nyulas, T.; Cherhat, M.P.; Ruta, F.; Nitu, C.C. Assessment of Eating Behavior During the COVID-19 Pandemic Period. A Pilot Study. Journal of Interdisciplinary Medicine, June 2021, Volume 6/Issue 2/ ISSN: 2501 – 8132.
- Nsiah-Asamoah, C.N.A.; Buxton, D.N.B. Hydration and water intake practices of commercial long-distance drivers in Ghana: what do they know and why does it matter? Heliyon. 2021; 7(3):e06512. [CrossRef]
- Haghighatdoost, F.; Feizi, A.; Esmaillzadeh, A.; Rashidi-Pourfard, N.; Keshteli, A. H.; Roohafza, H.; Adibi, P. Drinking plain water is associated with decreased risk of depression and anxiety in adults: Results from a large cross-sectional study. World Journal of Psychiatry, 2018, 8(3), 88–96. [CrossRef]
- Lotrean, L.M.; Ionut, C.; de Vries, H. Tobacco use among Romanian youth. Salud Publica Mex. 2006; 48 Suppl 1:S107-12. [CrossRef]
- Mota, M.; Popa, S.G.; Mota, E.; Mitrea, A.; Catrinoiu, D.; Cheta, D.M.; Guja, C.; Hancu, N.; Ionescu-Tirgoviste, C.; Lichiardopol, R.; Mihai, B.M.; Popa, A.R.; Zetu, C.; Bala, C.G.; Roman, G.; Serafinceanu C.; Serban, V.; Timar, R.; Veresiu, I.A.; Vlad, A.R. Prevalence of diabetes mellitus and prediabetes in the adult Romanian population: PREDATORR study. J Diabetes. 2016; 8(3):336-44. [CrossRef]
- Popa, S.; Mota, M.; Popa, A.; Mota, E.; Timar, R.; Serafinceanu, C.; Cheta, D.; Graur, M.; Hancu N. Prevalence of dyslipidemia and its association with cardiometabolic factors and kidney function in the adult Romanian population: The PREDATORR study. Diabetes Metab Syndr. 2019; 13(1):596-602. [CrossRef]
- Moţa, E.; Popa, S.G.; Mota, M.; Mitrea, A.; Penescu, M.; Tuţă, L.; Serafinceanu, C.; Hâncu, N.; Gârneaţă, L.; Verzan, C.; Lichiardopol, R.; Zetu, C.; Căpuşă, C.; Vlăduţiu, D.; Guja, C.; Catrinoiu, D.; Bala, C.; Roman, G.; Radulian, G.; Timar, R.; Mihai, B. Prevalence of chronic kidney disease and its association with cardio-metabolic risk factors in the adult Romanian population: the PREDATORR study. Int Urol Nephrol. 2015; 47(11):1831-8. [CrossRef]
- Searchinger, T.; Hanson, C.; Ranganathan, J.; Lipinski, B.; Waite, R.; Winterbottom, R.; et al. World Resources Report 2013–14: Interim Findings. Creating a Sustainable Food Future: Interim Findings. A menu of solutions to sustainably feed more than 9 billion people by 2050, World Resources Institute (WRI), 2014. https://www.wri.org/research/creating-sustainable-food-future-interim-findings.
Figure 1.
The influence of food quality on health. Created with BioRender (accessed on November 25, 2023).
Figure 1.
The influence of food quality on health. Created with BioRender (accessed on November 25, 2023).
Figure 2.
The multinomial logistic regression results with categories of adherence to a healthy diet as a dependent variable (bold values: p<0.05).
Figure 2.
The multinomial logistic regression results with categories of adherence to a healthy diet as a dependent variable (bold values: p<0.05).
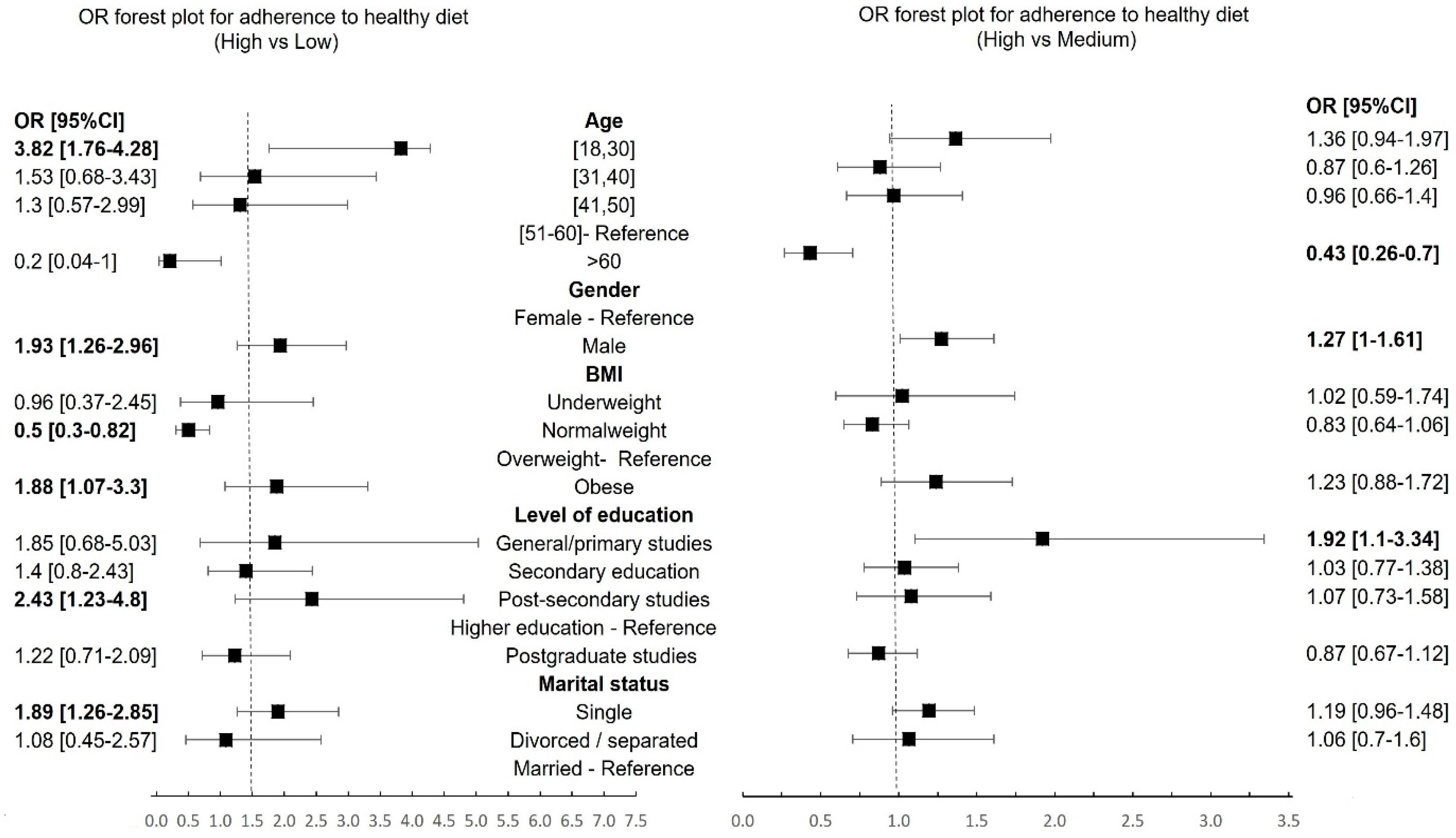
Figure 3.
Frequency of consumption of various categories of food products among young people (18-30 years): 1- very rarely or not at all; 2- once a week; 3- twice a week; 4- more than 2 times a week; 5-daily.
Figure 3.
Frequency of consumption of various categories of food products among young people (18-30 years): 1- very rarely or not at all; 2- once a week; 3- twice a week; 4- more than 2 times a week; 5-daily.
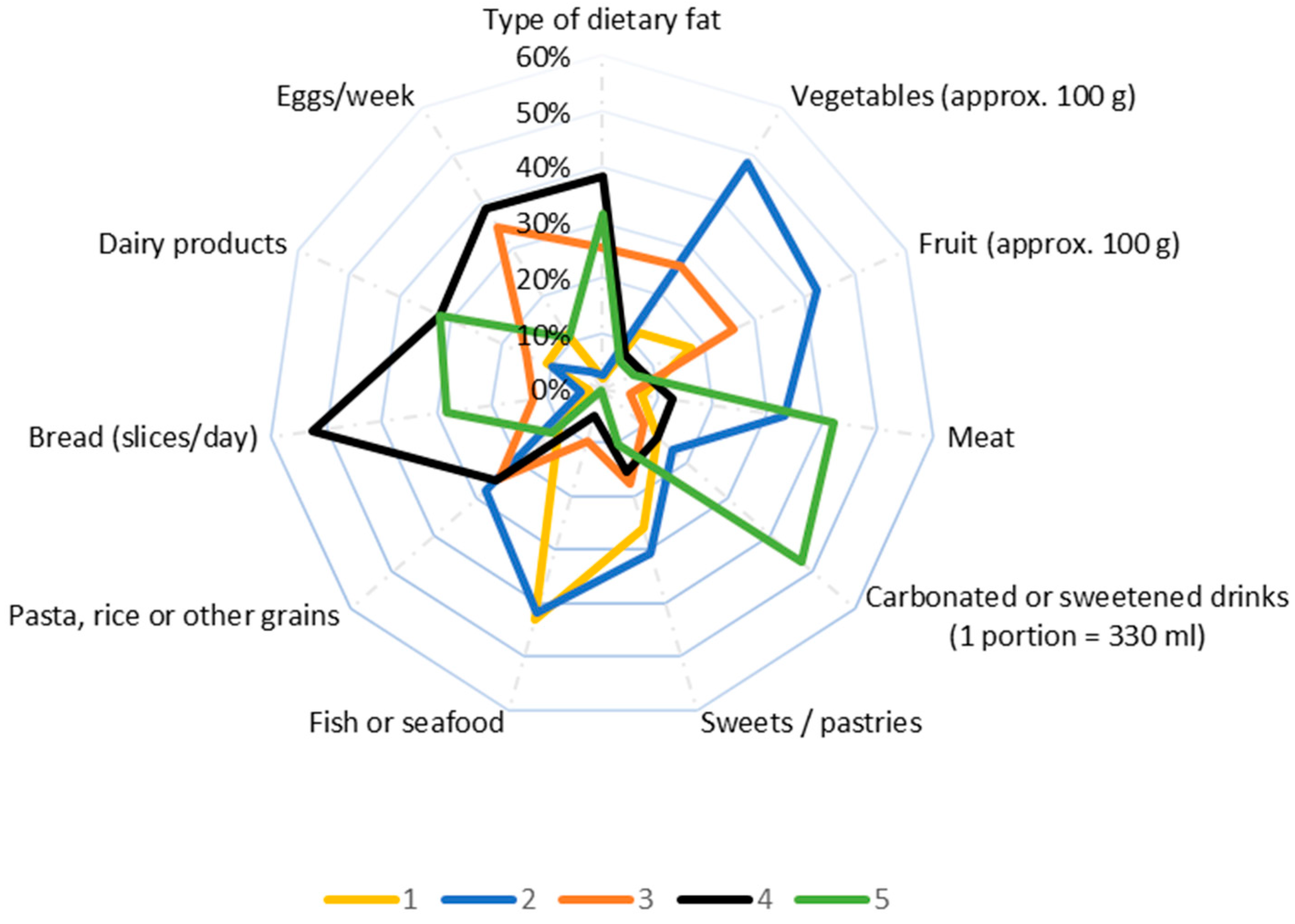
Figure 4.
The bi-plot with BMI categories and most consumed food products.
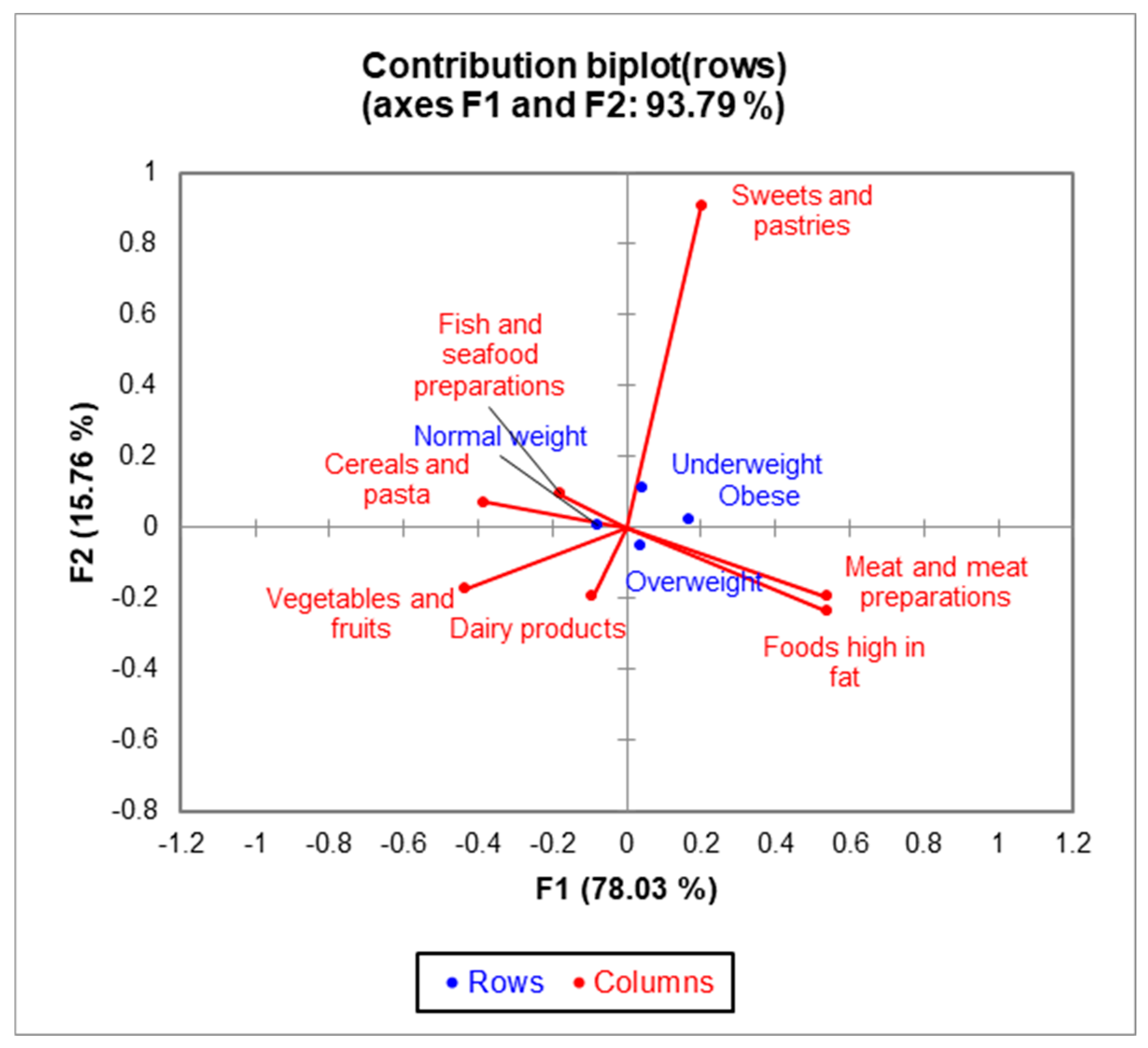
Figure 5.
The bi-plot with age categories and most consumed food products.
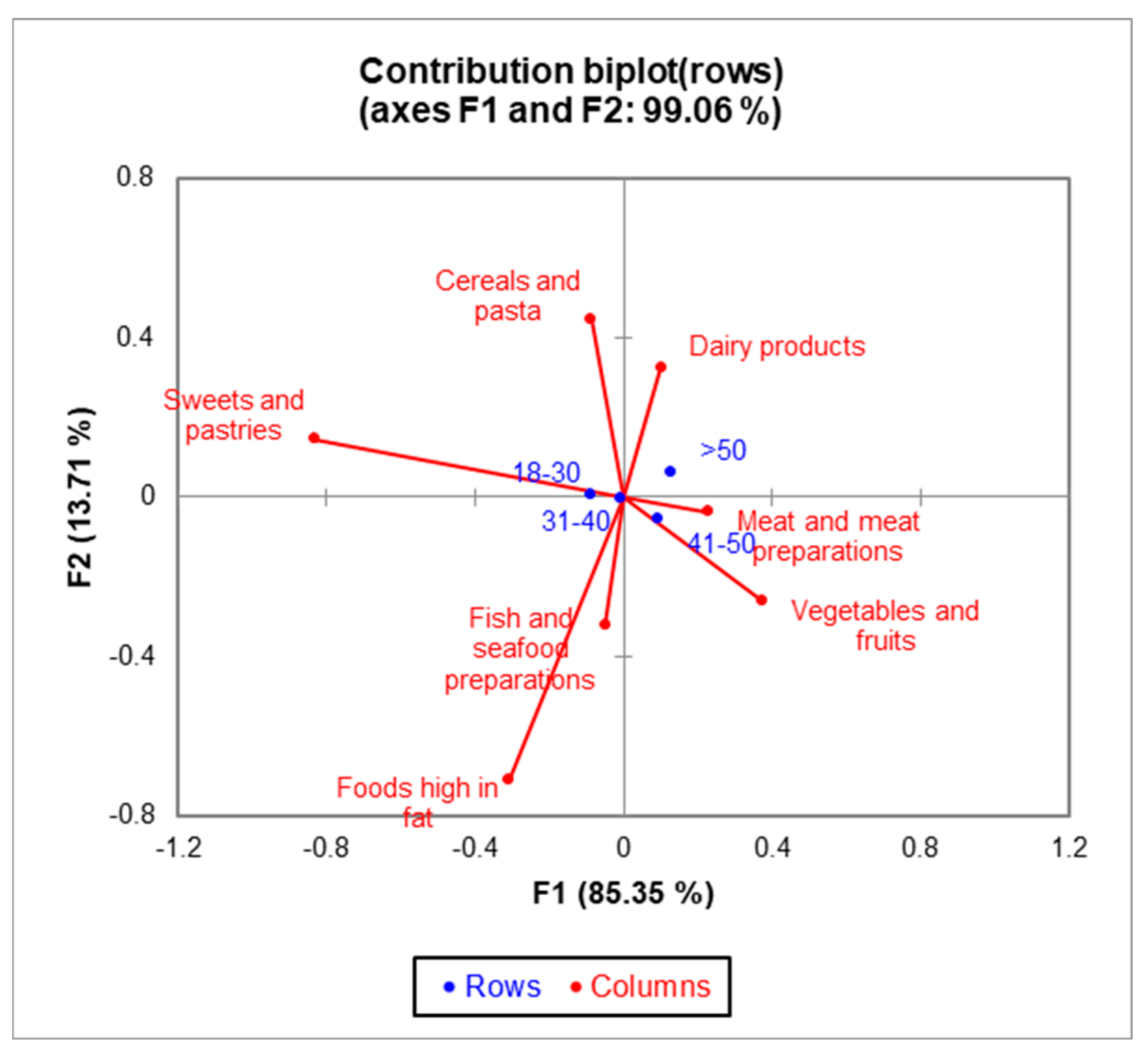
Figure 6.
Adherence to a healthy diet by gender and BMI.
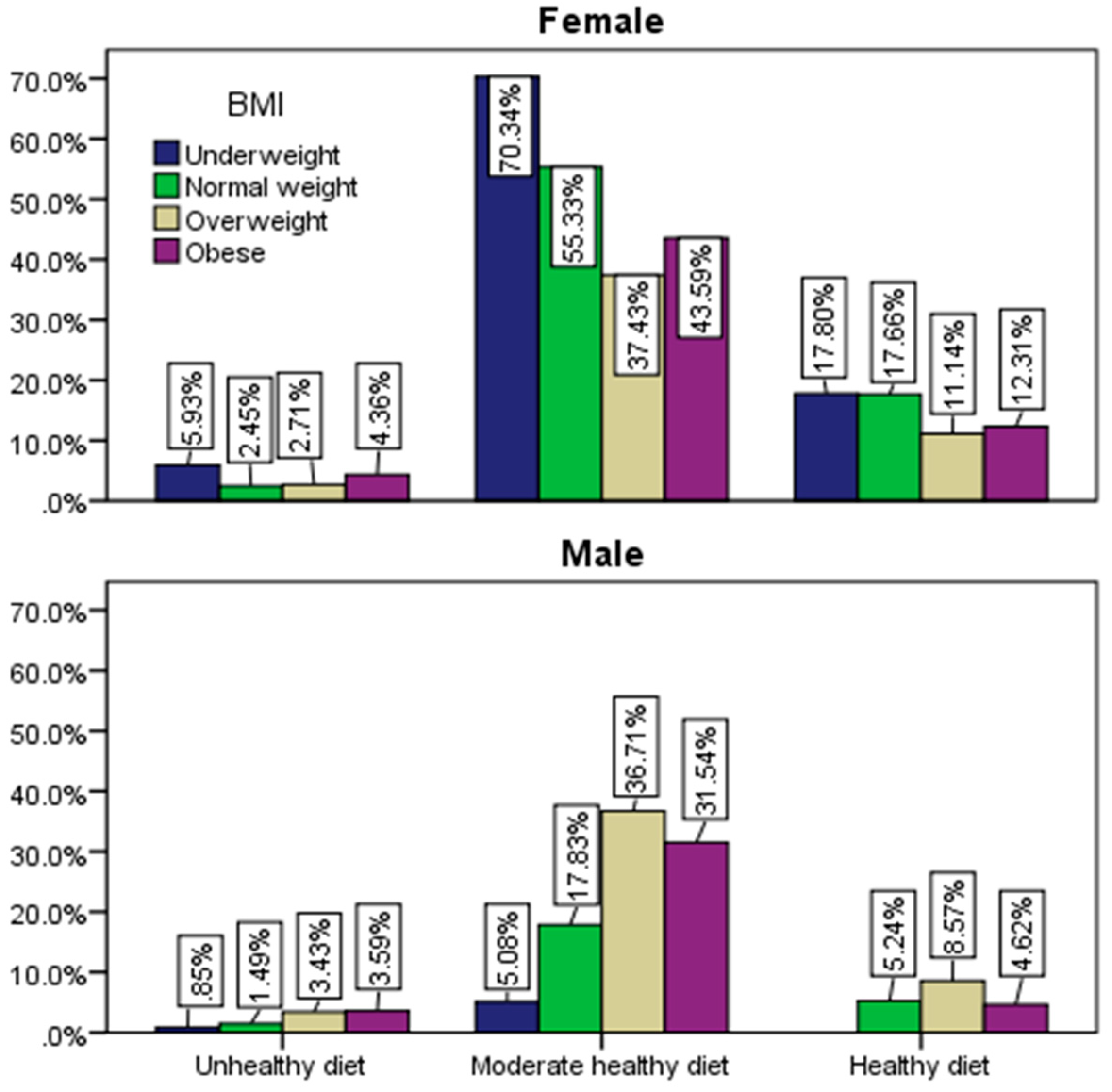
Figure 7.
The multinomial logistic regression results with categories of adherence to a healthy diet as a dependent variable (bold values: p<0.05).
Figure 7.
The multinomial logistic regression results with categories of adherence to a healthy diet as a dependent variable (bold values: p<0.05).
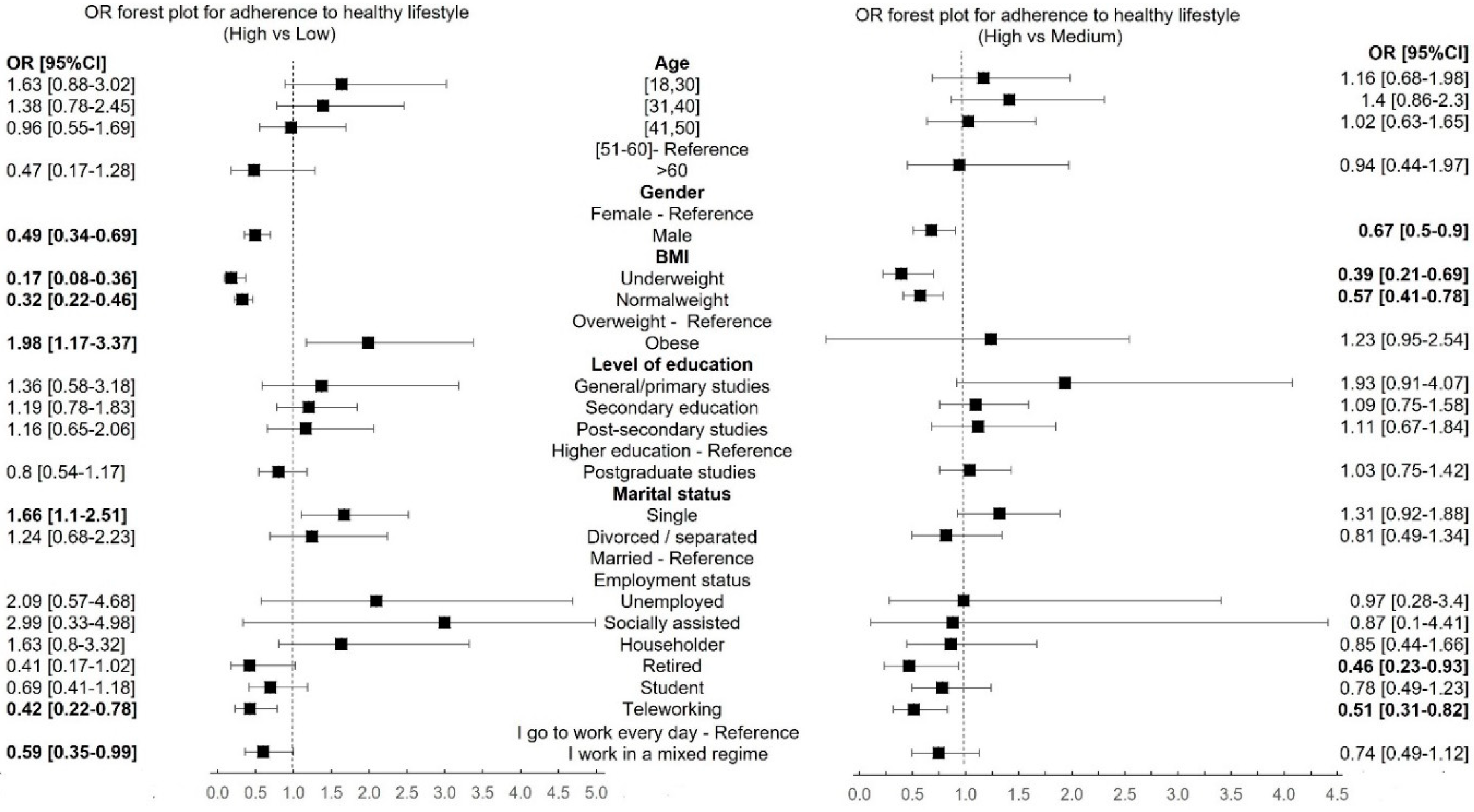
Figure 8.
Adherence to a healthy lifestyle by gender and BMI.
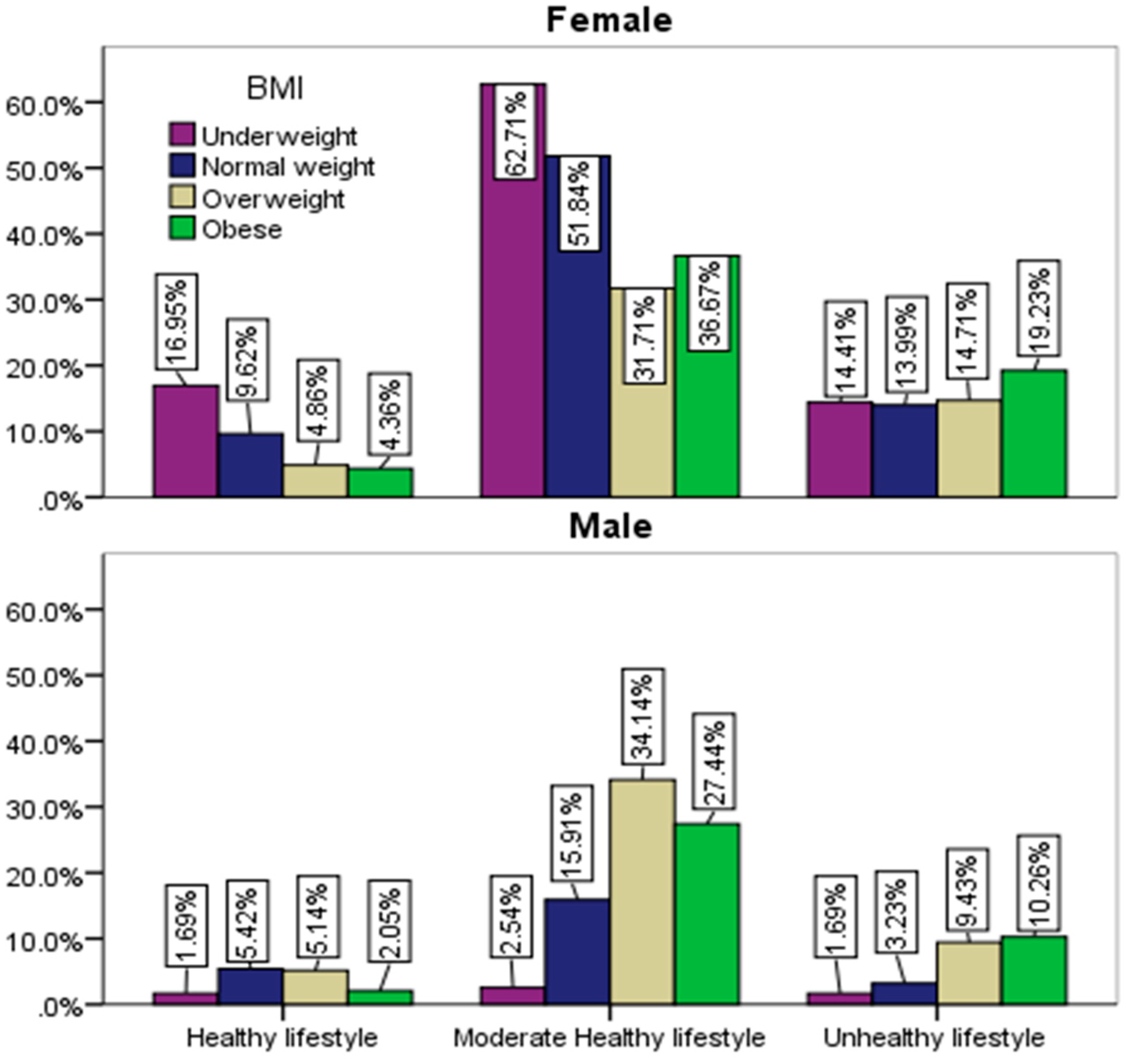
Figure 9.
Distribution of gender and sleep duration by BMI.
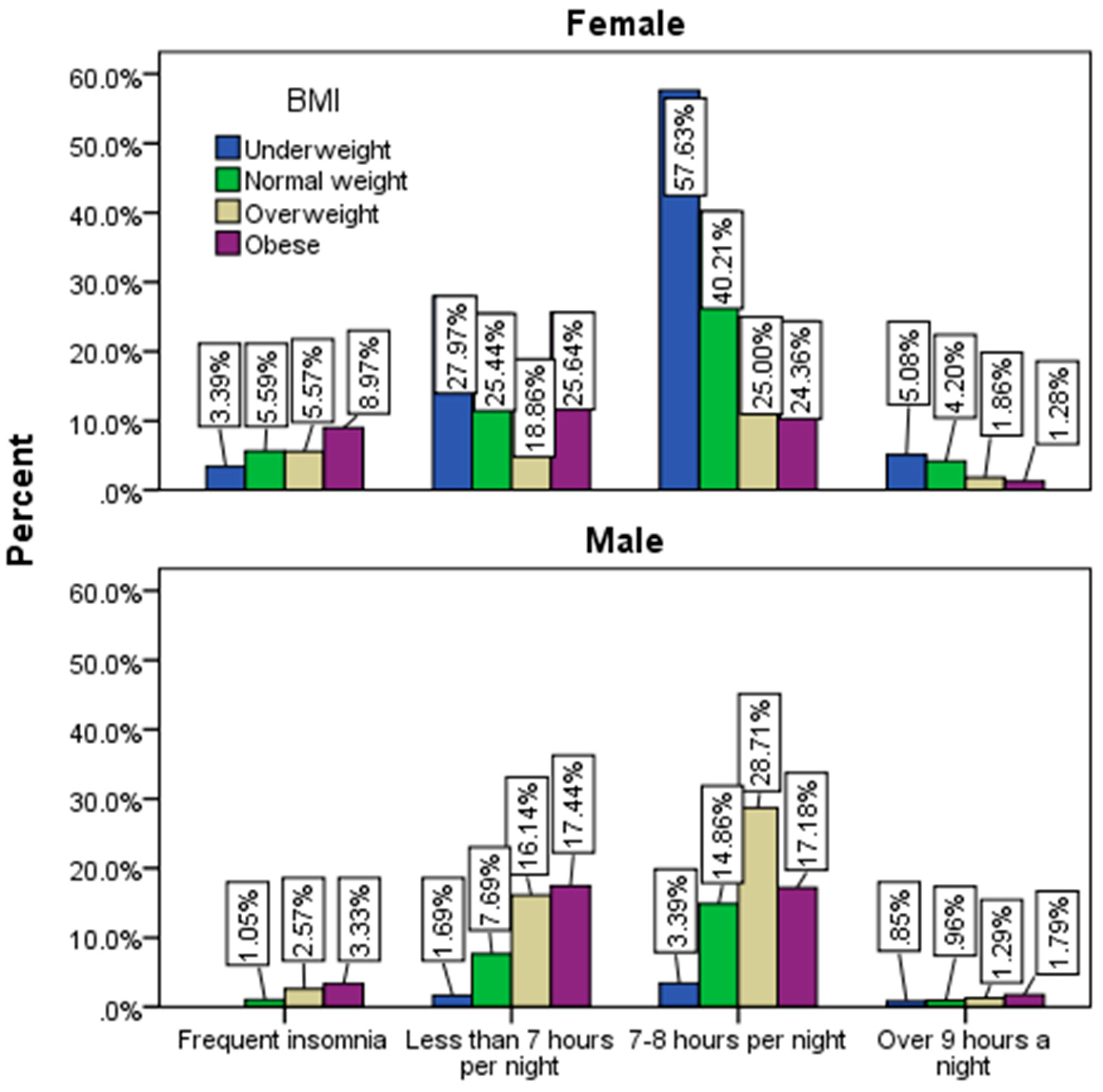
Figure 10.
Adherence to a healthy lifestyle and a heathy diet by BMI.
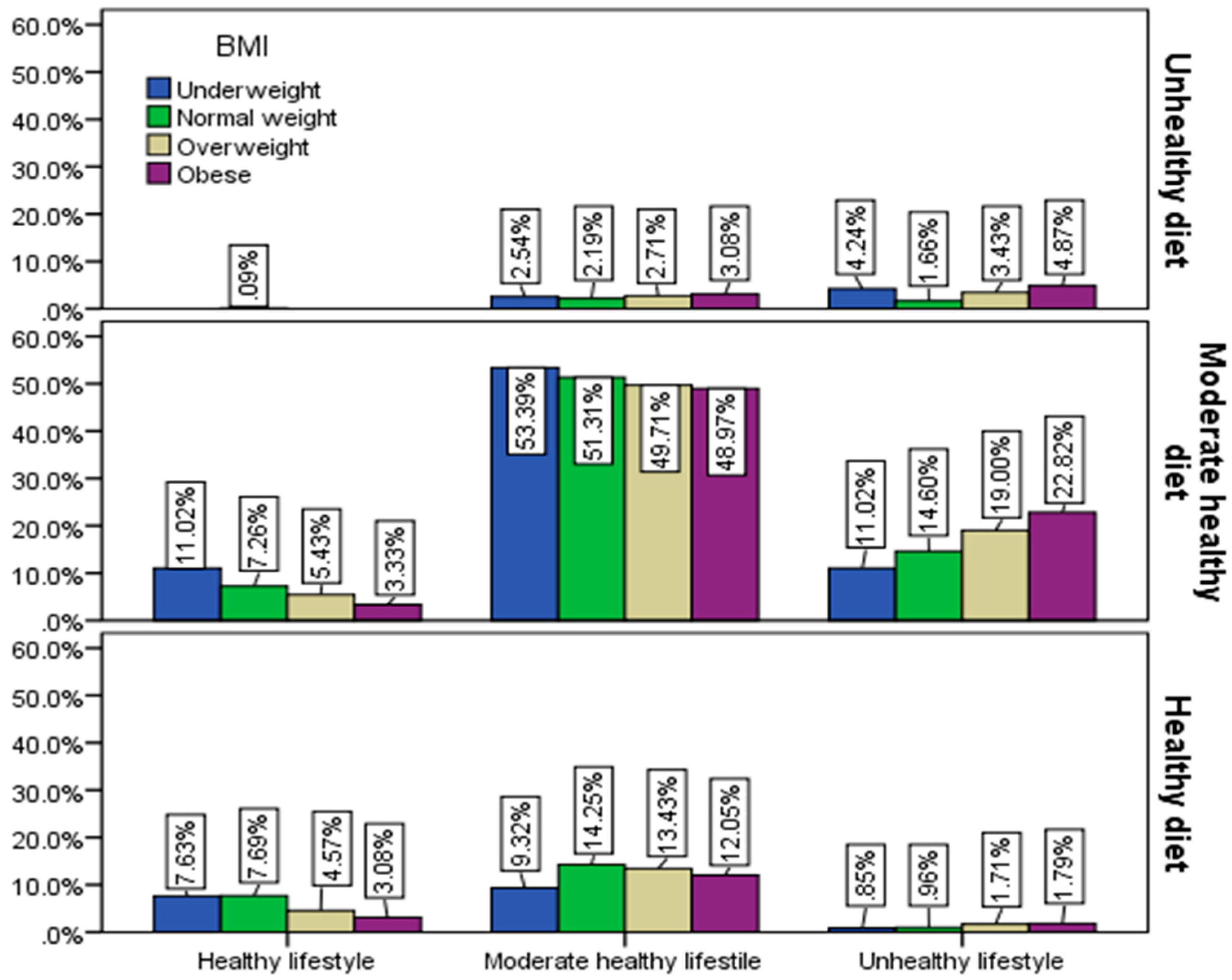
Figure 11.
Application of a restrictive diet by gender and BMI.
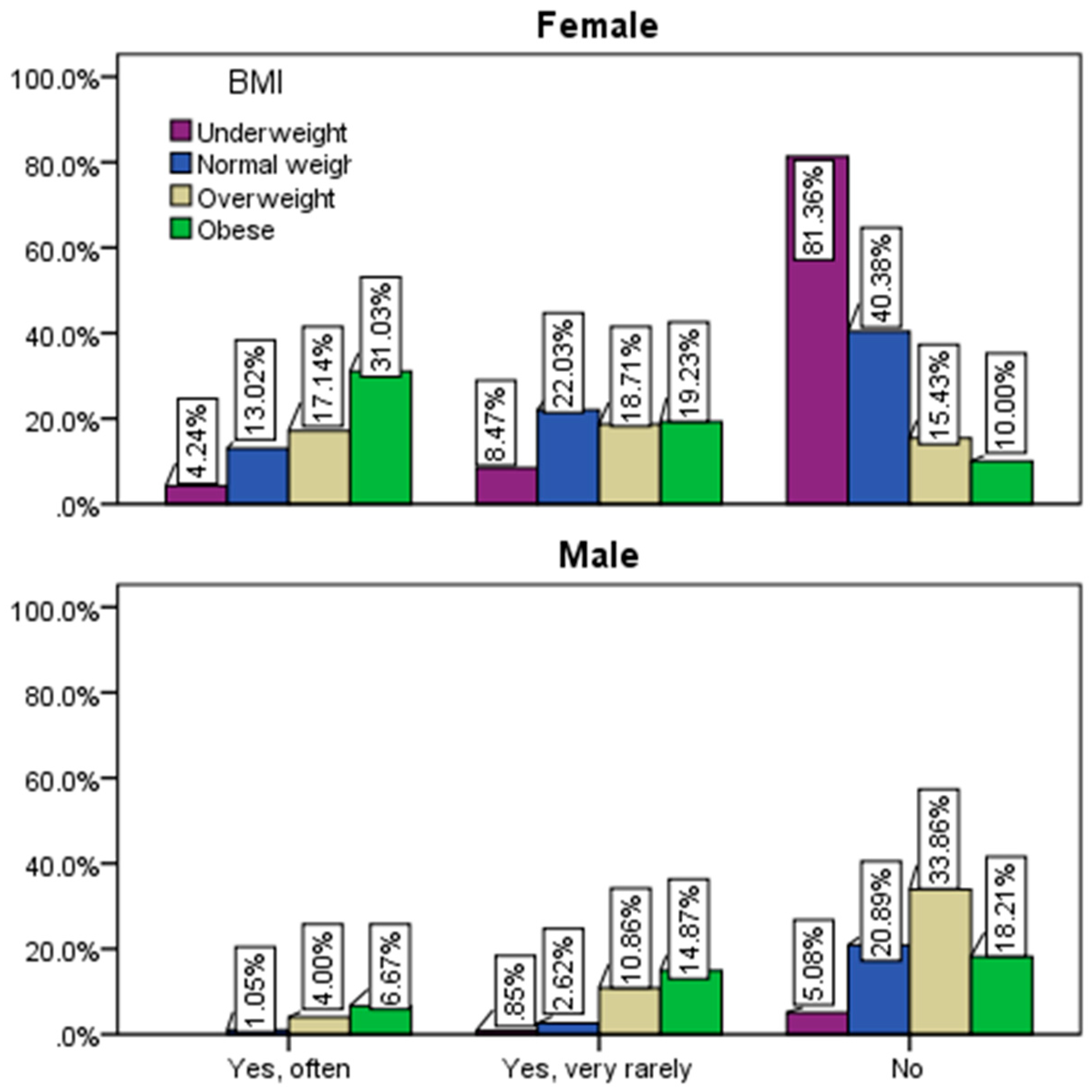
Figure 12.
The need for competent advice from nutritionists.
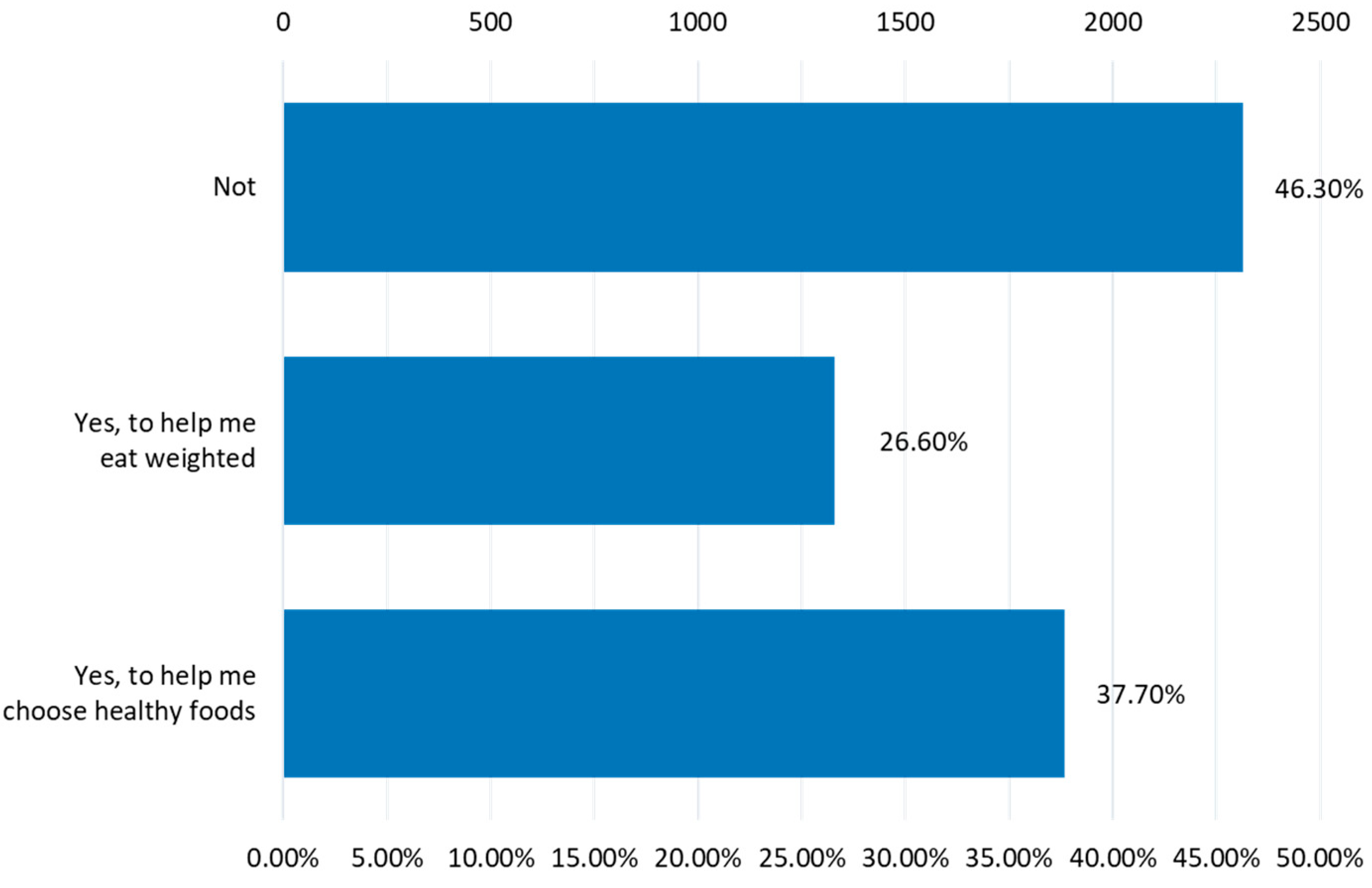
Figure 13.
Health risk factors.
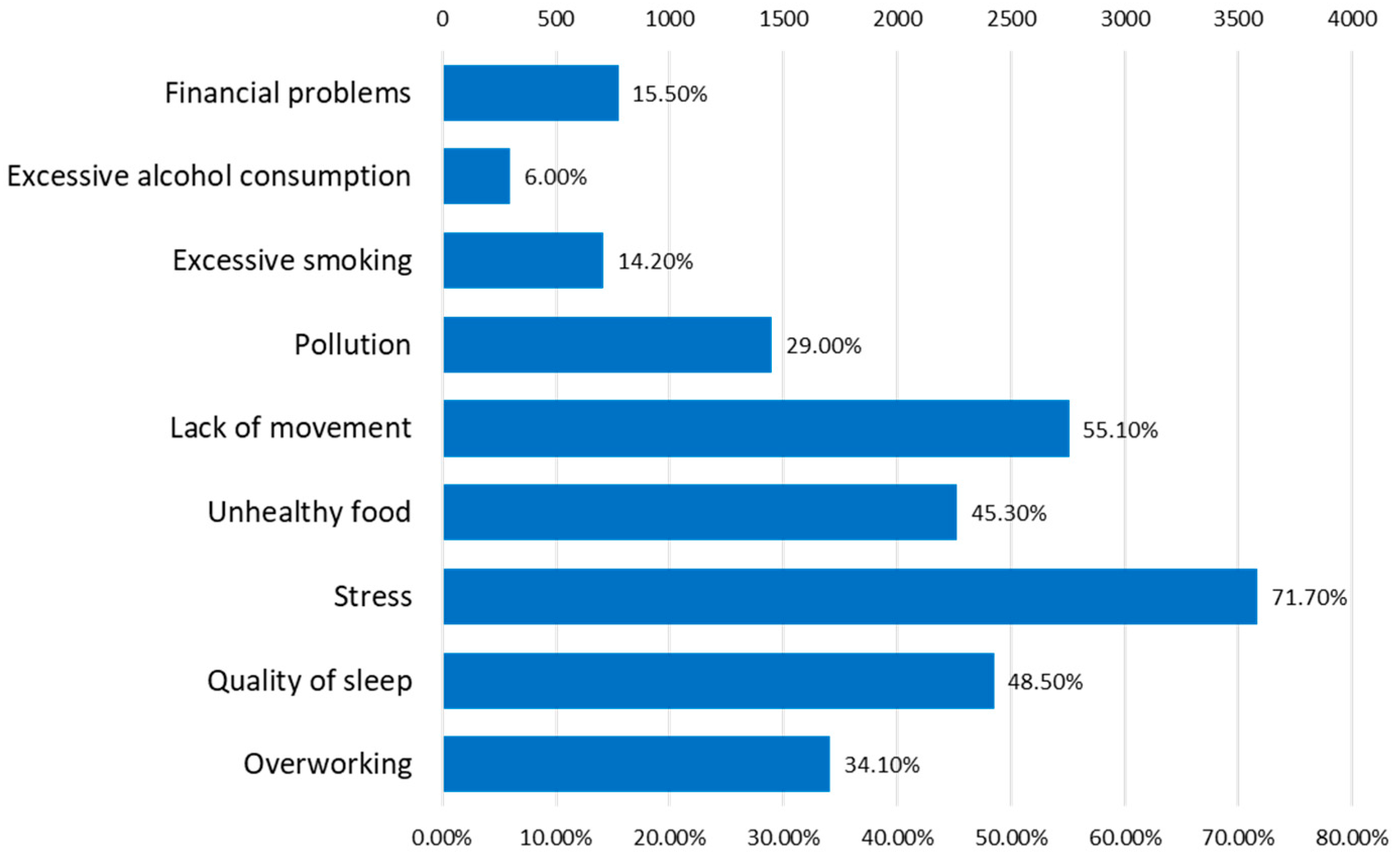
Figure 14.
Risk factors for the mental state.
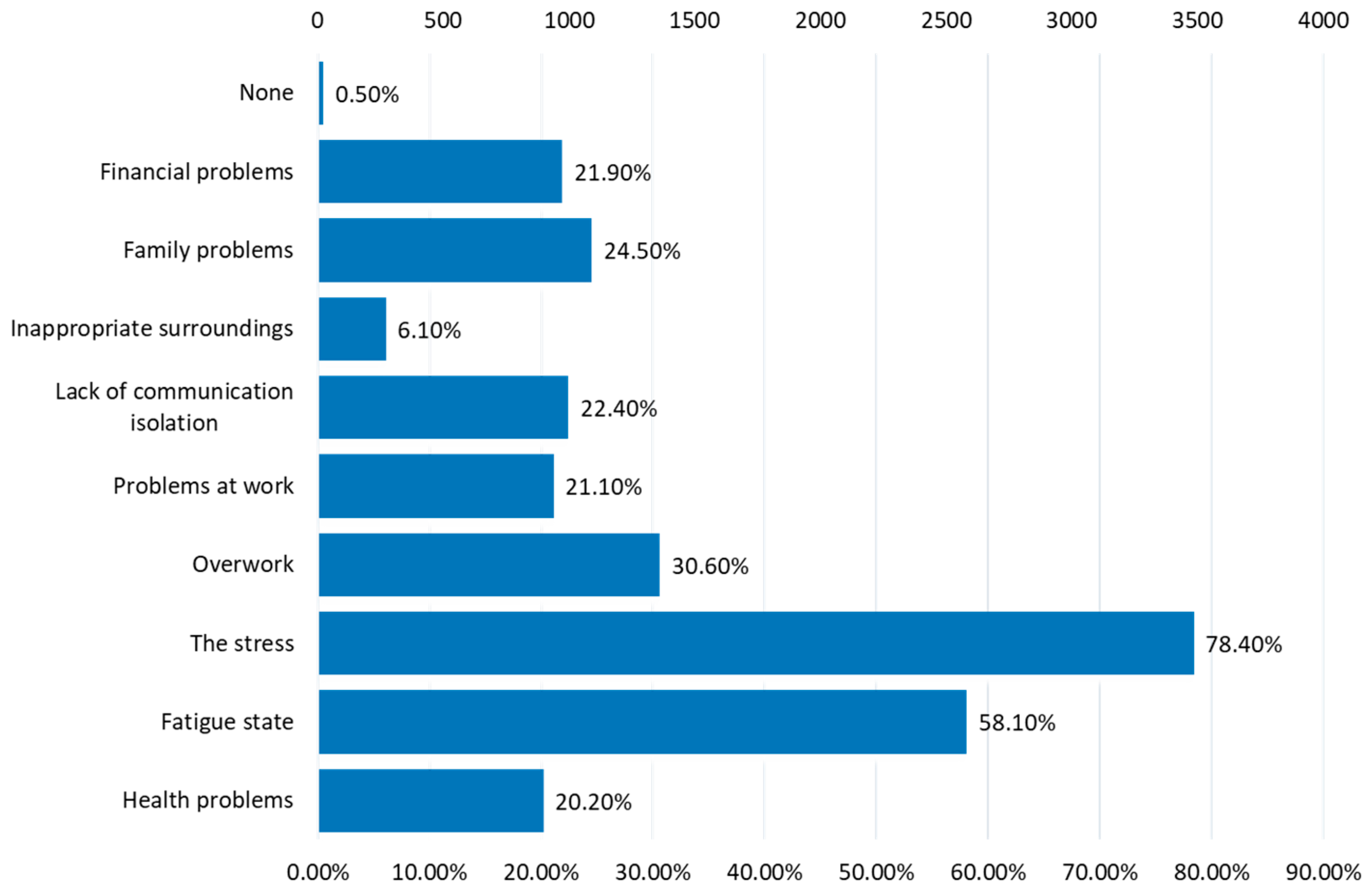
Figure 15.
Psycho-emotional problems.
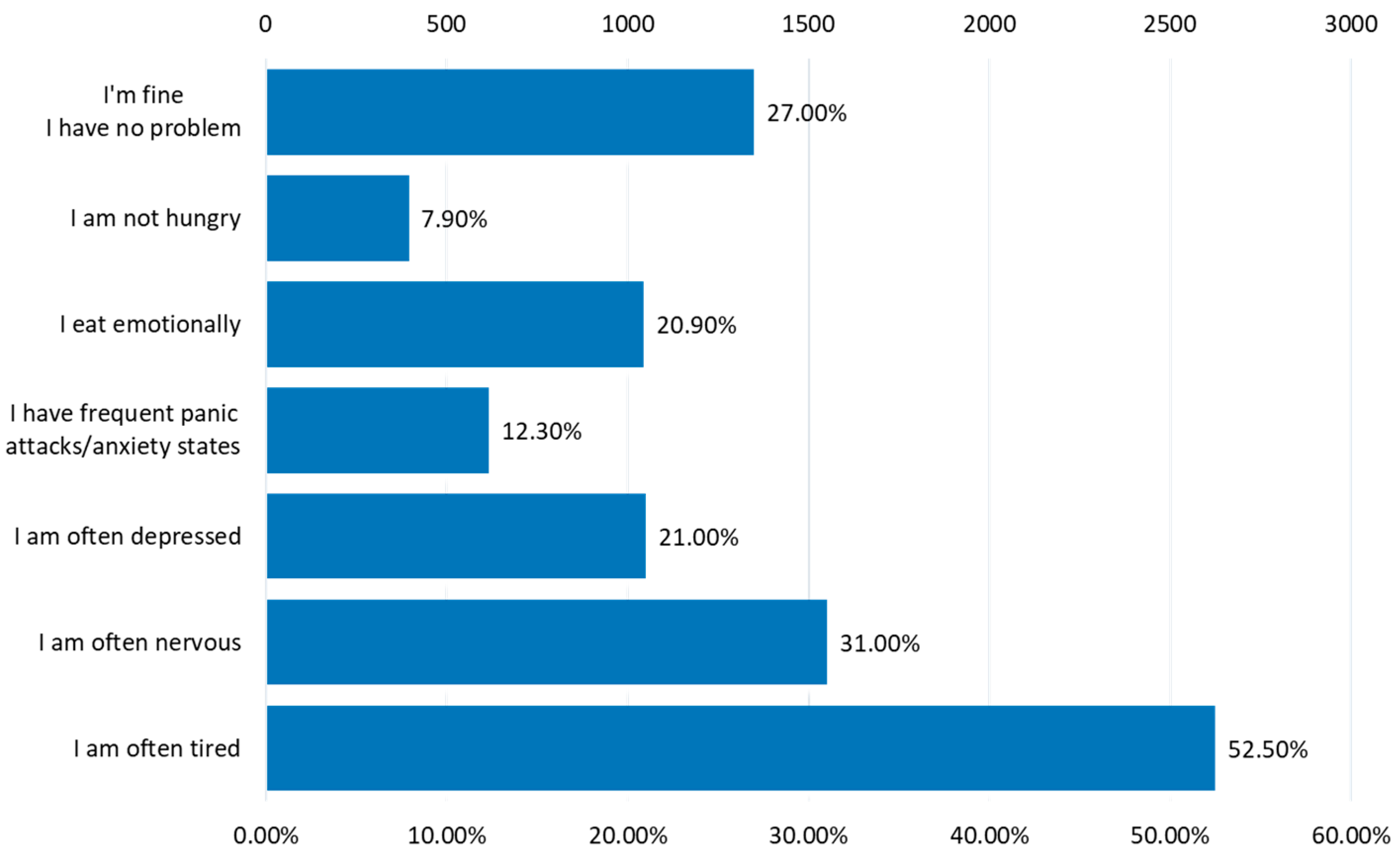
Figure 16.
Associated chronic diseases.
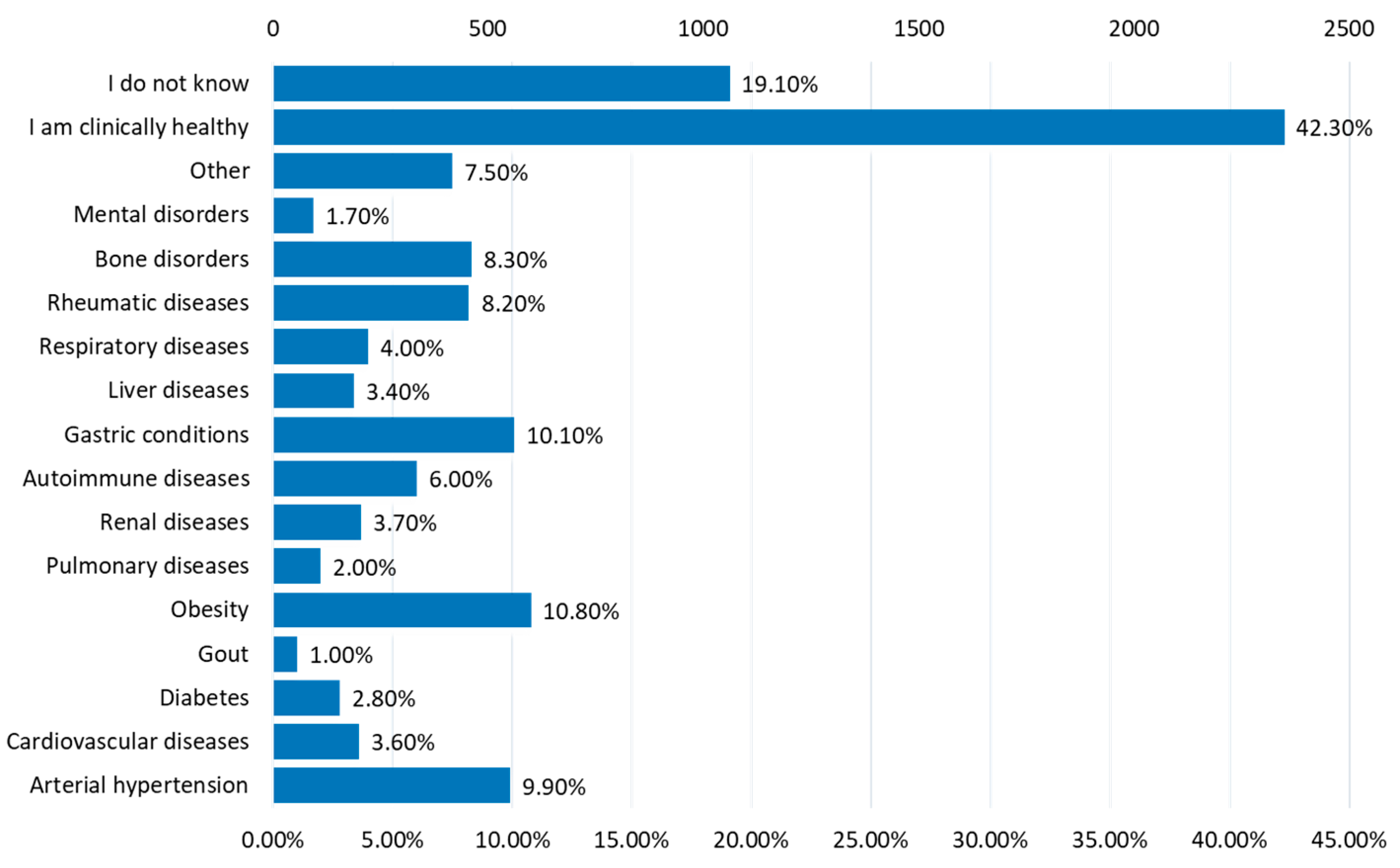
Figure 17.
Factors that depreciate lifestyle.
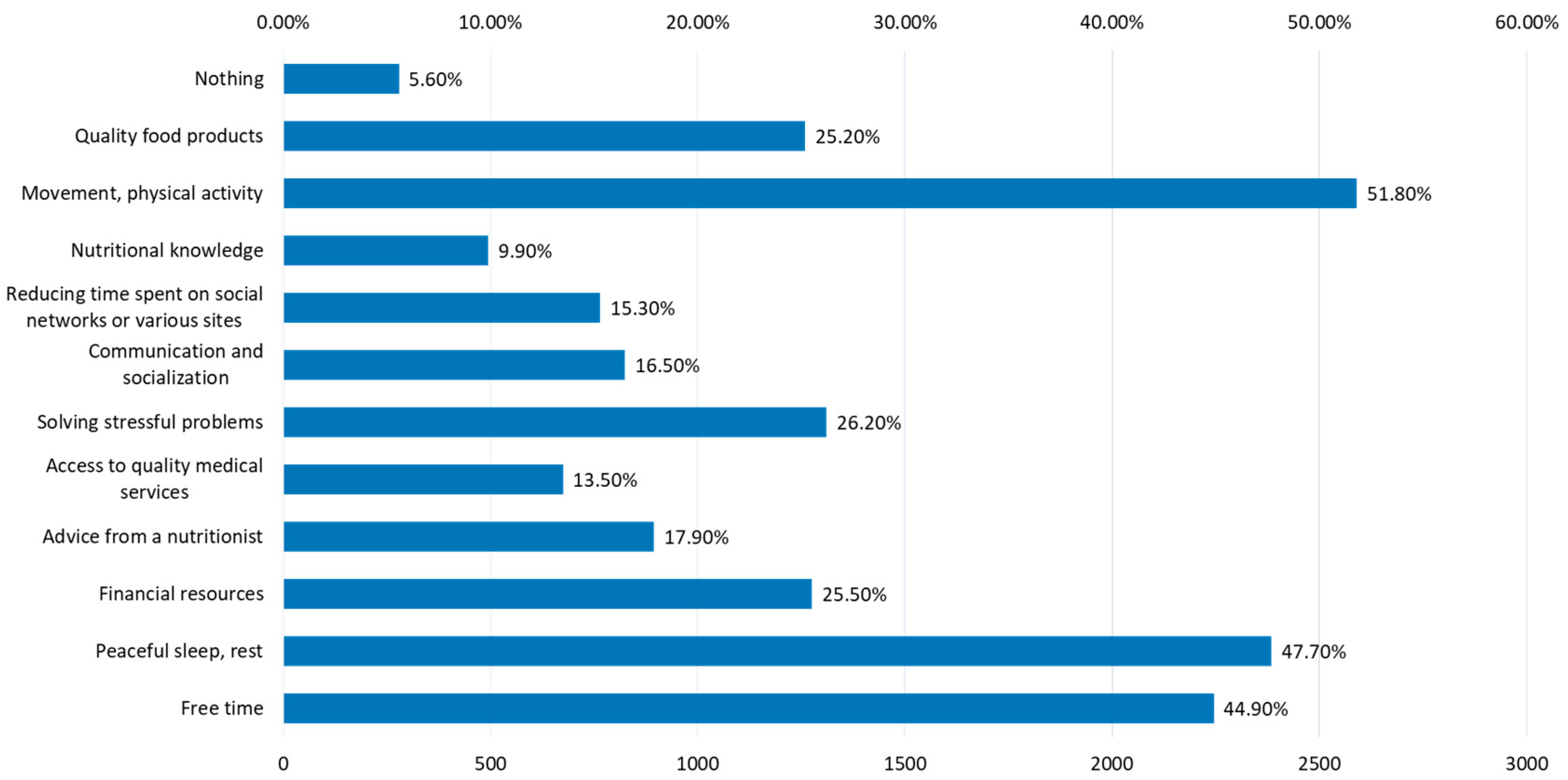
Figure 18.
Ways of recreation.
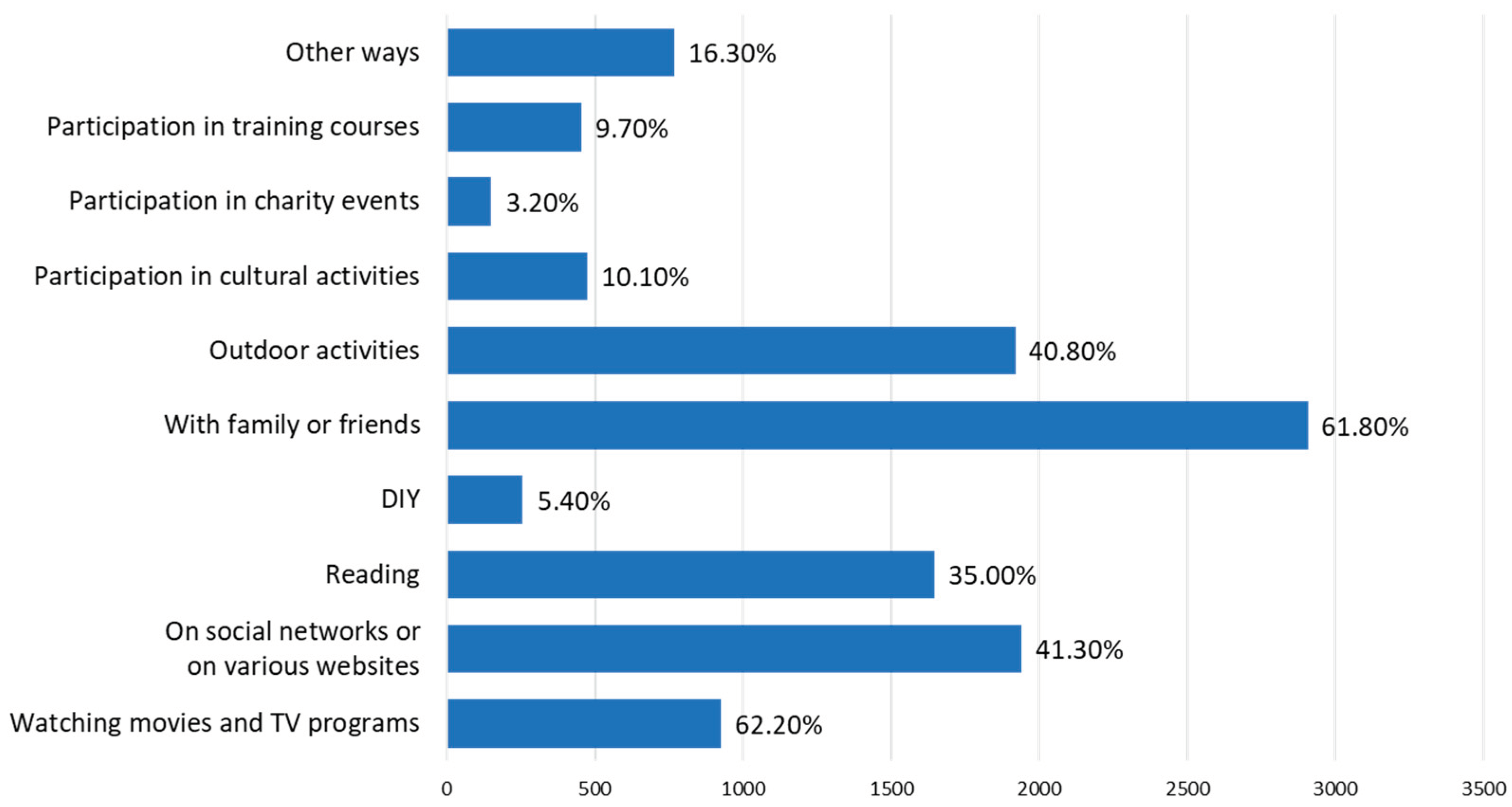

Table 1.
Socio-demographic and Anthropometric characteristics of respondents.
| Characteristics | Total population - n (%) | Male - n (%) | Female - n (%) |
|---|---|---|---|
| 4704 (100) | 1568 (33.3) | 3136 (66.7) | |
| Age (years); p<0.0001 | |||
| 18-30 | 1756 (37.3) | 528 (33.7) | 1228 (39.2) |
| 31-40 | 1136 (24.2) | 354 (22.6) | 782 (24.9) |
| 41-50 | 1034 (22) | 344 (21.9) | 690 (22) |
| 51-60 | 534 (11.3) | 204 (13) | 324 (10.5) |
| >60 | 246 (5.2) | 138 (8.8) | 1008 (3.4) |
| Residence areas; p=0.0002 | |||
| Urban areas | 3648 (77.6) | 1144 (72.9) | 2504 (79.8) |
| Rural areas | 1056 (22.4) | 424 (23.1) | 632 (20.2) |
| Level of education; p<0.0001 | |||
| General/primary studies | 298 (6.3) | 154 (9.8) | 144 (4.6) |
| Secondary education | 1090 (23.2) | 392 (25.0) | 698 (22.3) |
| Post-secondary studies | 420 (8.9) | 132 (8.4) | 288 (9.2) |
| Higher education | 1616 (34.4) | 528 (33.7) | 1088 (34.7) |
| Postgraduate studies | 1280 (27.2) | 362 (23.1) | 918 (29.3) |
| Marital status; p=0.0049 | |||
| Single | 1688 (35.9) | 634 (53.7) | 1054 (59.6) |
| Divorced/separated | 306 (6.5) | 92 (5.9) | 214 (6.8) |
| Married | 2710 (57.6) | 842 (40.4) | 1868 (33.6) |
| Employment status; p<0.0001 | |||
| Unemployed | 78 (1.7) | 34 (2.2) | 44 (1.4) |
| Socially assisted | 26 (0.6) | 10 (0.6) | 16 (0.5) |
| Householder | 312 (6.6) | 36 (2.3) | 276 (8.8) |
| Retired | 270 (5.7) | 140 (8.9) | 130 (4.1) |
| Student | 838 (17.8) | 210 (13.4) | 628 (20) |
| Teleworking | 274 (5.8) | 92 (5.9) | 182 (5.8) |
| Going to work every day | 2406 (51.1) | 848 (54.1) | 1558 (49.7) |
| Mixed working regime | 500 (10.6) | 198 (12.6) | 302 (9.6) |
| Body mass index (BMI); p<0.0001 | |||
| Normal (18.5-24.9) | 2288 | 562 (35.8) | 1726 (55.0) |
| Overweight (25-29.9) | 1400 | 682 (43.5) | 718 (22.9) |
| Underweight (<18.5) | 236 | 14 (0.9) | 222 (7.1) |
| Obese (≥30) | 780 | 310 (19.8) | 470 (15.0) |
Secondary education—baccalaureate degree; Higher education—bachelor's degree; Postgraduate studies—master's degree, residency, doctorate, other specializations; Mixed working regime—teleworking and commuting.
Table 2.
Adherence to a healthy diet of age-group, gender, BMI group, Residence areas, Education level, Marital status, and Employment status.
Table 2.
Adherence to a healthy diet of age-group, gender, BMI group, Residence areas, Education level, Marital status, and Employment status.
|
Variable |
Healthy diet |
Moderate healthy diet |
Unhealthy diet |
p-value Chi-squared test |
|||
| n | % | n | % | n | % | ||
| Total | 974 | 20.7 | 3476 | 73.9 | 234 | 5.4 | |
| Age | |||||||
| 18-30 | 292 | 30 | 1334 | 38.4 | 130 | 51.2 | <0.0001 |
| 31-40 | 270 | 27.7 | 810 | 23.3 | 56 | 22 | |
| 41-50 | 222 | 22.8 | 766 | 22 | 44 | 17.3 | |
| 51-60 | 106 | 10.9 | 408 | 11.7 | 20 | 7.9 | |
| >60 | 84 | 8.6 | 158 | 4.6 | 4 | 1.6 | |
| Gender | |||||||
| F | 698 | 71.7 | 2296 | 66.1 | 142 | 55.9 | 0.0020 |
| M | 276 | 28.3 | 1180 | 33.9 | 112 | 44.1 | |
| BMI | |||||||
| Underweight | 42 | 4.3 | 178 | 5.1 | 16 | 6.2 | 0.0102 |
| Normal weight | 524 | 53.8 | 1674 | 48.1 | 90 | 35.4 | |
| Overweight | 276 | 28.3 | 1038 | 29.8 | 86 | 33.8 | |
| Obese | 132 | 13.6 | 586 | 16.8 | 62 | 24.4 | |
| Residence areas | |||||||
| Urban | 788 | 80.9 | 2668 | 76.8 | 96 | 75.6 | 0.1315 |
| Rural | 186 | 19.1 | 808 | 23.2 | 62 | 24.4 | |
| Level of education | |||||||
| General/primary studies | 36 | 3.7 | 248 | 7.2 | 14 | 5.5 | 0.0087 |
| Secondary education |
202 | 20.7 | 818 | 23.5 | 70 | 27.5 | |
| Post-secondary studies | 84 | 8.6 | 300 | 8.6 | 36 | 14.2 | |
| Higher education |
344 | 35.3 | 1204 | 34.6 | 68 | 26.9 | |
| Postgraduate studies | 308 | 31.6 | 906 | 26.1 | 66 | 25.9 | |
| Marital status | |||||||
| Single | 314 | 32.2 | 1254 | 36.1 | 120 | 47.2 | 0.0394 |
| Divorced/separated | 64 | 6.6 | 228 | 6.5 | 14 | 5.6 | |
| Married | 596 | 61.2 | 1994 | 57.4 | 120 | 47.2 | |
| Employment status | |||||||
| Unemployed | 8 | 0.8 | 64 | 1.8 | 6 | 2.4 | 0.0038 |
| Socially assisted | 10 | 1 | 16 | 0.5 | 0 | 0 | |
| Householder | 68 | 6.9 | 222 | 6.4 | 22 | 8.7 | |
| Retired | 84 | 8.6 | 182 | 5.2 | 4 | 1.6 | |
| Student | 140 | 14.4 | 632 | 18.2 | 66 | 25.9 | |
| Teleworking | 66 | 6.7 | 204 | 5.9 | 4 | 1.6 | |
| Going to work every day | 486 | 49.8 | 1796 | 51.7 | 124 | 48.8 | |
| Mixed regime | 112 | 11.5 | 360 | 10.3 | 28 | 11 | |
Secondary education—baccalaureate degree; Higher education—bachelor's degree; Postgraduate studies—master's degree, residency, doctorate, other specializations; Mixed working regime—teleworking and commuting.
Table 3.
Adherence to a healthy lifestyle of age-group, gender, BMI group, Residence areas, Education level, Marital status, and Employment status.
Table 3.
Adherence to a healthy lifestyle of age-group, gender, BMI group, Residence areas, Education level, Marital status, and Employment status.
| Variable |
Healthy lifestyle |
Moderate healthy lifestyle |
Unhealthy lifestyle |
p-value Chi-squared test |
|||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Total | 578 | 12.28 | 3126 | 66.45 | 1000 | 21.25 | |
| Age | |||||||
| 18-30 | 208 | 35.99 | 1118 | 35.76 | 430 | 43.00 | 0.0038 |
| 31-40 | 120 | 20.76 | 790 | 25.27 | 226 | 22.60 | |
| 41-50 | 134 | 23.18 | 698 | 22.33 | 200 | 20.00 | |
| 51-60 | 66 | 11.42 | 350 | 11.20 | 118 | 11.80 | |
| >60 | 50 | 8.65 | 170 | 5.44 | 26 | 2.60 | |
| Gender | |||||||
| F | 362 | 62.63 | 2064 | 66.03 | 710 | 71.00 | 0.0363 |
| M | 216 | 37.37 | 1062 | 33.97 | 290 | 29.00 | |
| BMI | |||||||
| Underweight | 44 | 7.61 | 154 | 4.93 | 38 | 3.80 | 0.0001 |
| Normal weight | 344 | 59.52 | 1550 | 49.58 | 394 | 39.40 | |
| Overweight | 140 | 24.22 | 922 | 29.49 | 338 | 33.80 | |
| Obese | 50 | 8.65 | 500 | 15.99 | 230 | 23.00 | |
| Residence areas | |||||||
| Urban areas | 484 | 83.74 | 2384 | 76.26 | 80 | 78.00 | 0.0193 |
| Rural areas | 94 | 16.26 | 742 | 23.74 | 220 | 22.00 | |
| Level of education | |||||||
| General/primary studies | 20 | 3.46 | 218 | 6.97 | 60 | 6.00 | 0.0167 |
| Secondary education | 124 | 21.45 | 692 | 22.14 | 274 | 27.40 | |
| Post-secondary studies | 46 | 7.96 | 268 | 8.77 | 100 | 10.00 | |
| Higher education | 212 | 36.68 | 1056 | 33.78 | 348 | 34.80 | |
| Postgraduate studies | 176 | 30.45 | 886 | 28.34 | 218 | 21.80 | |
| Marital status | |||||||
| Single | 190 | 32.87 | 1104 | 35.32 | 394 | 39.40 | 0.1682 |
| Divorced/separated | 46 | 7.96 | 188 | 6.01 | 72 | 7.20 | |
| Married | 342 | 59.17 | 1834 | 58.67 | 534 | 53.40 | |
| Employment status | |||||||
| Unemployed | 6 | 1.04 | 42 | 1.34 | 10 | 3.00 | p<0.0001 |
| Socially assisted | 2 | 0.35 | 14 | 0.45 | 10 | 1.00 | |
| Householder | 24 | 4.15 | 182 | 5.82 | 106 | 10.60 | |
| Retired | 58 | 10.03 | 178 | 5.69 | 34 | 3.40 | |
| Student | 12 | 17.65 | 542 | 17.34 | 194 | 19.40 | |
| Teleworking | 54 | 9.34 | 178 | 5.57 | 46 | 4.60 | |
| Going to work every day | 258 | 44.64 | 1648 | 52.72 | 500 | 50.00 | |
| Mixed working regime | 74 | 12.48 | 346 | 10.7 | 80 | 8.00 | |
Secondary education—baccalaureate degree; Higher education—bachelor's degree; Postgraduate studies—master's degree, residency, doctorate, other specializations; Mixed working regime—teleworking and commuting.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



