
Submitted:
09 April 2024
Posted:
09 April 2024
You are already at the latest version
Abstract
With an increase in proportion of elderly patients, the global burden of spinal disease is on the rise. Likewise, there has been an increasing trend in the number of spine surgeries being performed worldwide. As we know, rehabilitation following spine surgery is critical for optimal recovery. However, current literature lacks consensus regarding the appropriate post operative rehabilitation protocol. The goals of rehabilitation after lumbar spine surgery are to improve physical and psychosocial function and may include multiple modalities such as physical therapy, cognitive behavioral therapy, specialized instruments, and instruction to be followed during activities of daily living. In recent years, not only are a greater number of spine surgeries being performed, various different techniques of lumbar spine surgery and spinal fusion have emerged. Physical therapy programs need to be curated after assessing the functional status of the patient by using various patient reported outcome measures and taking into consideration the technique of spinal fusion used and the muscle groups involved in these surgeries. By doing so it is possible to assess the level of functional impairment and then specifically target strengthening of those muscle groups affected by surgery whilst also improving impaired balance and allowing return to activities of daily living. We reviewed available literature pertaining to the history of spinal rehabilitation, the popular patient reported outcome measures used and different rehabilitation methods with the purpose of summarizing the current guidelines for postoperative rehabilitation after spine surgery and to introduce the rehabilitation after lumbar surgeries that we provide at our hospital.
Keywords:
Rehabilitation
; Lumbar surgery
; Physiotherapy
; Muscle exercise
1. Introduction
Low back pain is a major cause of morbidity among middle aged and elderly individuals due to a number of possible etiologies. Even though most of the episodes of low back pain are often self-limiting, incidence of lifetime recurrence is as high as 85% [1]. Chronic low back pain not only impairs physical and psychological health but also leads to decline in social responsibilities including work performance , family life and is a major cause of increasing health care costs [2]. With advancements in medical care and increased life expectancy of the aging population, the global burden of spinal disease has increased [3].With the availability of advanced techniques such as minimally invasive spine surgery, percutaneous pedicle screw fixation, imaging and navigation, larger number of spinal surgeries are being performed nowadays with some studies documenting the number of spine surgeries to be 2.4 times of those performed 15 years ago [4,5].
Following lumbar spinal surgery, postoperative rehabilitation is crucial. It is recommended by spine surgeons for improvement of post operative functional outcome so that patients can perform their activities of daily living (ADL) at the earliest and return to work, sports, and leisure activities in the long term [6,7]. Rehabilitation programs may consist of individual training, group training, home exercises, patient education, or a combination of these, all led by a physical therapist. Furthermore, active rehabilitation is effective and important for improving short-term and long-term functional status [8]. Rehabilitation includes multiple different modalities based on the requirements of the patients such as providing instructions, exercise therapy such as stretching and muscle strengthening, manipulation techniques, mobilization techniques and use of assistive equipment such as walking aids [9]. When assessing the progress of post-operative patients undergoing rehabilitation, physical therapists and surgeons often have to use disease specific patient reported outcome measures and standard physical performance tests. These assessments may provide useful information regarding progress made by the patients following surgery. With different techniques of lumbar spine surgery and spinal fusion being performed, the physical therapy prescribed should be curated taking into the account the technique used and should aim to target strengthening of muscle groups violated during the surgical procedure.
The benefits of physical therapy as per literature in the past have been limited to weak evidence, and the mechanisms of these benefits remain uncertain [10,11] . This article aims to summarize the historical review of rehabilitation, popular patient reported outcome assessment methods, contemporary views on postoperative spinal rehabilitation and ways to introduce rehabilitation after lumbar spine surgery.
2. Historical Review of Rehabilitation (Table 1)
The Roman army probably provided the first rehabilitation services to return wounded soldiers to work. The word “Rehabilitation” was firstly used in the Oxford English dictionary in 1533. However, rehabilitation was used extensively in healthcare by 1918. After World War I, the society recognized rehabilitation was a crucial addition to services for injured or disabled patients [12]. Rehabilitation can be considered a planned and systematic societal support process offered to patients after injury or illness. Initially, orthopedic surgeons were mainly involved. The rehabilitation services that did develop in the twentieth century were initially focused on men of working age, who were injured in war. Because of the increase motor cycle accidents and sports injuries, attention moved to people with spinal cord injuries. Spinal cord injury rehabilitation developed 1940s as evidence of rehabilitation’s revolutionary effectiveness [13]. After World Health Organization (WHO) was established in 1948, they used the biopsychosocial model as a rehabilitation frame work in 1980 [14].
For low back pain rehabilitation, lumbar stabilization exercises became popular over last 40 years. These exercises prioritize the conscious and progressive training of stabilizing muscles of the trunk [15]. Wiliams reported specific exercises known as Williams lumbar flexion exercises in 1937 [16] (Figure 1). These exercises are a series of therapeutic movements and stretches designed to activate the abdominal muscles and relax the paraspinal lumbar muscles. In 1955, Kelly addressed the importance of lumbar muscle relaxation with hanging, which is effective for lumbar foraminal enlargement, reduce muscle spasms, and facet joint release [17]. Pleasant developed and mixed Wiliams and Kelly exercises [18]. His methods consisted three concepts, which are joint mobilization, soft tissue stretching, and muscle building. Calliet reported exercise therapy positively enhanced joint capsules, ligaments, and tendons, and increased blood flow, thereby aiding in the recovery of injured regions [19]. Moreover, he emphasized resistance exercise improved muscle function by increasing the cross-sectional areas of muscles, thereby providing great benefits in prevention and treatment of pain.

Table 1.
History of important lumbar exercises.
| Year | Author | Rehabilitation method |
|---|---|---|
| 1937 | Williams [16] | Lumbar flexion exercises |
| 1955 | Kelly [17] | Hanging exercises |
| 1962 | Pheasant [18] | Posture building |
| 1968 | Calliet [19] | Lumbar lateral flexion exercises |
| 1971 | Böhler [20] | Lumbar extension exercises |
| 1979 | McKenzie [21] | Lumbar extension exercises |
Compared with Williams lumbar flexion exercises, Böhler emphasized the importance of lumbar extensor muscle exercises in 1971 [20]. Then McKenzie recommended that extending the spine could provide significant pain relief to certain patients [21]. McKenzie exercises improve spinal mobility and promote good posture (Figure 2). The long-term goal of the McKenzie exercises is to teach patients suffering from back pain how to manage pain using exercise. Recently, motor control stabilization exercises are becoming popular for the patients with chronic nonspecific low back pain [22]. These exercises intended to retrain coordinated recruitment of the deep abdominal and back muscles through a submaximal voluntary isometric contraction performed in a neutral spine position. WHO has released its first-ever guidelines on managing chronic low back pain in 2023 [23]. According to this guideline, a structured exercise therapy or program and spinal manipulative therapy may be offered as part of care to adults, including older people, with chronic primary low back pain.
3. Various Kinds of Rehabilitation
Postsurgical rehabilitation interventions include therapy, which aims to improve function through the diagnosis and treatment of health conditions, reducing impairments, preventing, or treating complications. Furthermore, rehabilitations restore and compensate for loss of functioning, and prevent or slow deterioration in functioning in every area of a person’s life [24]. Rehabilitation may also include assistive technology, which refers to equipment, or product used to increase, maintain, or improve functional capabilities [24]. Postsurgical rehabilitation can be provided by different healthcare providers including, but not limited to, general practitioners, orthopedic surgeons, physiotherapists, chiropractors, and occupational therapists. Examples of postsurgical rehabilitation interventions are showed in Table 2.
4. Patients Reported Outcome (PRO) Measures Used after Lumbar Surgery
PRO is useful to evaluate the various symptoms of spinal disease separately, it is possible to accurately assess the disability caused by the disease by including the impact of the spinal disease on daily life. It is necessary to use PRO to assess the impact on physical function, ADL, and quality of life. (QOL) These patients reported outcome questionnaires are frequently used by spine surgeons and physical therapists to assess the functional outcome of patients following spinal surgery. Jaeschke et al proposed the term minimal clinically important difference (MCID) (Figure 3) [28]. The minimal detectable change (MDC) was estimated by means of the standard error of measurement in patients who self-assess as unchanged. The MCID describes the smallest clinical difference a patient can perceive in a specific questionnaire of data study.
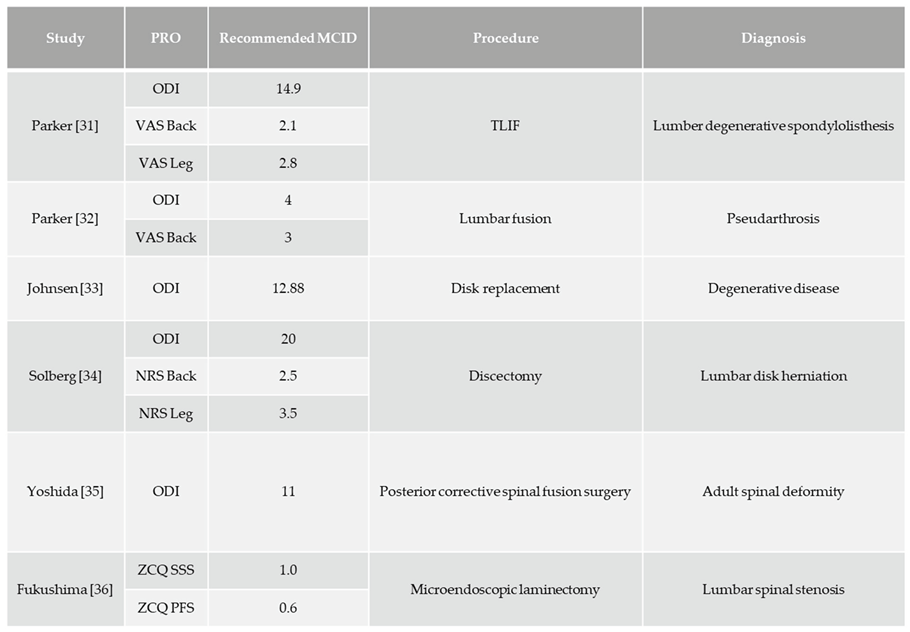
Acknowledging the relevance of such an approach, additional clinically oriented concepts have been introduced which can be used to better interpret PRO measures data. The MCID is relative to the initial symptomatic state before treatment. A helpful concept to rate a cohort’s condition in absolute terms is the patient-acceptable symptom state, defined as the value on a PRO scale beyond which patients with a specific condition consider themselves well or in a satisfactory state [29]. Using all these parameters in the interpretation of evaluation outcomes, a better and patient-oriented description of obtained success rates in therapeutic approaches can be provided. A systematic review of postoperative MCID for lumbar spine disease has been reported by Issa et al.[30] The reported MCID after surgery for lumbar spine disease is shown (Table 2).
Table 3.
MCID in PRO after surgery for lumbar spine disease.
2.1. Roland-Morris Disability Questionnaire (RMDQ) (Figure 4)
The RMDQ is the most commonly used lumber spine-specific assessment method [37].
Problems with the RMDQ include the lack of questions related to mental health and the fact that it is difficult for patients with only leg pain to answer [38].
2.2. Oswestry Disability Index (ODI) (Figure 5)
The ODI was initially published by Fairbank to measure disability in daily living associated with low back pain [39,40]. Score 0-4; No disability, 5-14; Mild disability, 15-24; Moderate disability, 25-34; Severe disability, 35-50; Complete disability. ODI can evaluate ADL impairment due to low back pain and the influence of lower limb pain and is correlated with lower limb pain before and after surgery [41]. ODI is more sensitive to change than more general health measures, when tracking the effectiveness of treatments [42].
2.2. Zurich Claudication Questionnaire (ZCQ)
The ZCQ is a disease-specific assessment of lumbar spinal stenosis (LSS) and is assessed in three domains: symptom severity, functional impairment, and treatment satisfaction [43]. The ZCQ demonstrates good validity and reliability in patients with LSS and is recommended as one of the appropriate methods for evaluating LSS treatment outcomes [44].
2.3. Scoliosis Research Society 22-Item Questionnaire (SRS-22)
The SRS-22 is used to assess QOL and surgical outcomes in an array of different spinal deformities [45,46]. It consists of 22 questions covering four domains: pain, functioning, self-image, and satisfaction with the surgery [47]. The SRS-22 is a valid and reliable tool that has been extensively studied [48]. Markers of sagittal balance, such as the sagittal vertical axis, have a significant correlation with all SRS domains, and pelvic tilt, which describes the orientation of the pelvis in relation to the body, has demonstrated correlation with SRS-22 in function and self-image domains [49,50].
2.4. Lumbar Stiffness Disability Index (LSDI)
The LSDI was designed and validated as a tool to assess functional impacts of lumbar spine stiffness and diminished spinal flexibility [51,52,53]. It is particularly used to evaluate patients after spinal fusion surgery, and it has been shown that LSDI worsens and postoperative satisfaction decreases in surgeries that involve a long fusion [54,55].
5. Physical Performance Tests
The prevalence of lumbar canal stenosis increases with age and is the most common diagnosis in patients over age 65 undergoing spinal surgery [56–58]. Older patients with lumbar spine disease have locomotive syndrome and reduced physical function [59–61]. Therefore, it is important, especially in the rehabilitation field, to assess physical function to aid in the planning of a program of therapeutic interventions. Minimal clinically important difference (MCID) has been reported in physical function assessment as well as in PRO. In general, the following assessments of physical function are used.
5.1. Walk Velocity (Figure 6)
Walk velocity is a performance measure used to assess walking speed in meters per second over a short distance [62]. A decrease in walking speed is defined as walking velocity of 0.8 m/s or less [63]. Changes in postoperative pain after lumbar spine surgery are associated with gait speed. Gait speed is therefore a necessary assessment for the management of pain and disability in patients after lumbar spine surgery [64]. MCID of walk velocity after ASD surgery is 0.1m/S [65].
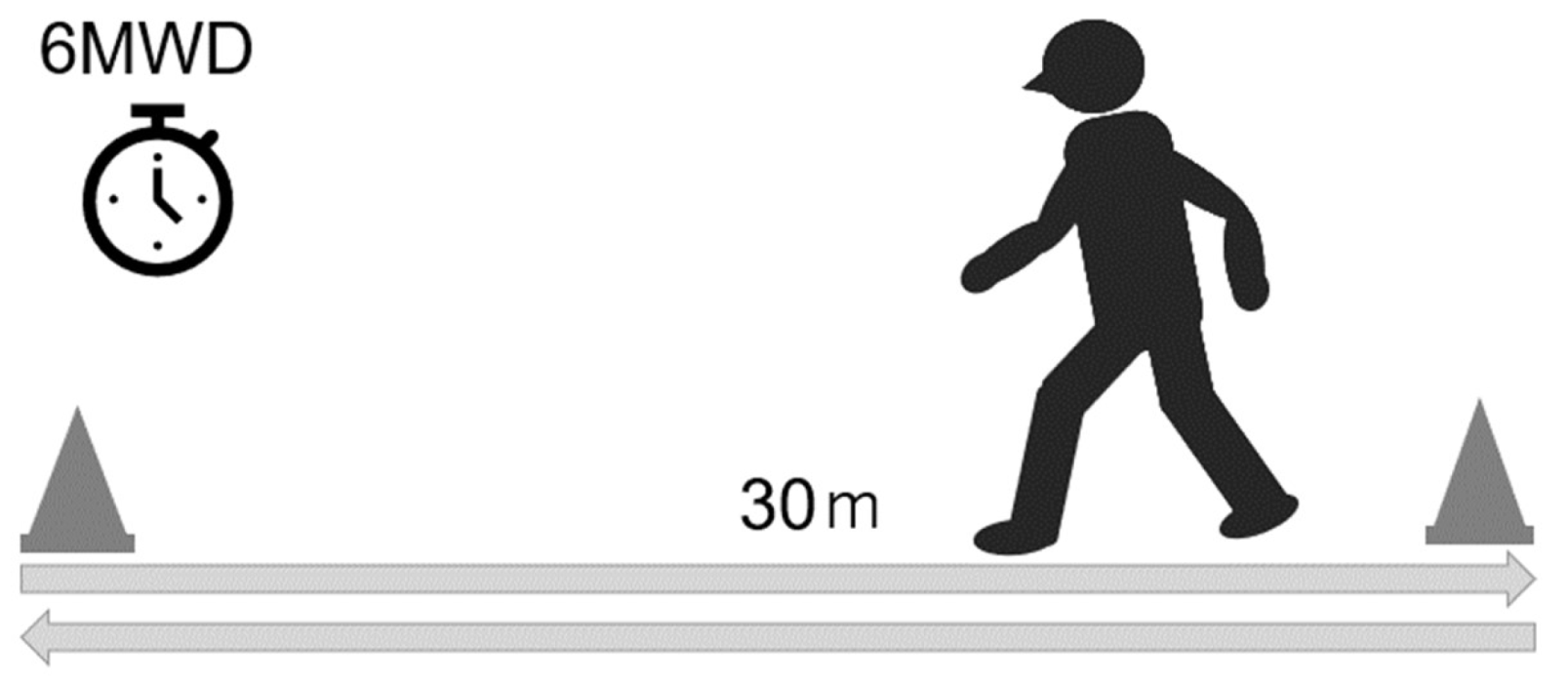
5.2 6-Minute Walk Test (Figure 6)
6-minute walk test involves walking for 6 minutes on a 30m walking path and measuring the distance [66]. Six-minute walking distance is used to evaluate walking efficiency in patients with neurogenic claudication in LSS and ASD [67,68]. Self-reported walking distance in LSS patients underestimates measured walking distance by 31% and has low validity [69]. Therefore, when comparing the improvement of intermittent claudication after treatment, it is desirable to evaluate the actual walking distance using the 6-minute walk test. MCID of 6-minute walk distance after LSS surgery is 57.5m [70].
Figure 7.
6-Minute walk test.
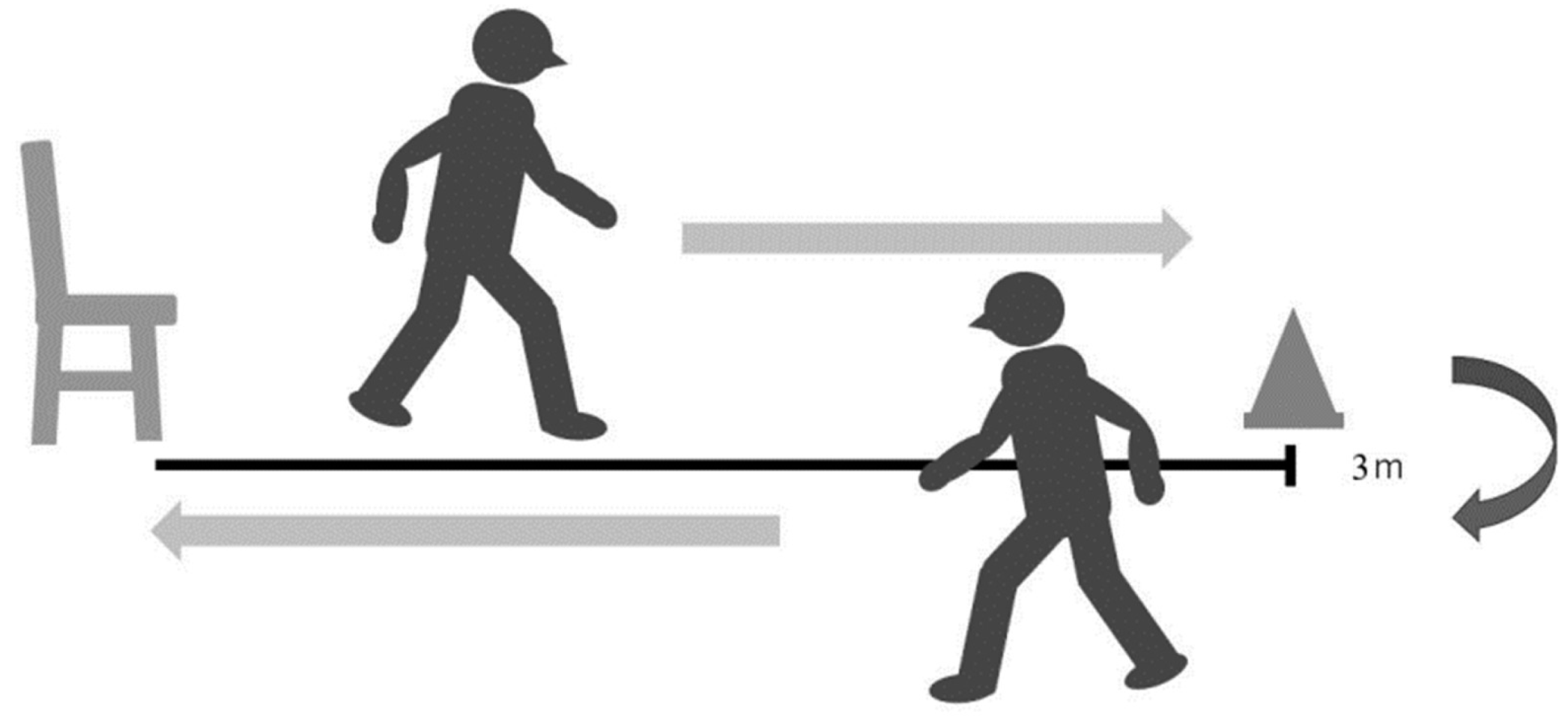
5.3. Timed Up and Go Test (TUG) (Figure 7)
The timed up and go test (TUG) is an objective measure of functional disability that can be used to evaluate various activities such as standing, accelerating, walking, decelerating, and turning, which are often limited in patients with lumbar degenerative diseases [71]. TUG can be easily done with a chair and a 3-m walking space and does not require special equipment [72]. A previous study used TUG to measure motor impairment in patients with lumbar degenerative diseases, with < 11.5 s classified as no impairment, 11.5 to 13.4 s as mild impairment, 13.4 to 18.4 s as moderate impairment, and > 18.4 s as severe impairment [71]. TUG is not easily affected by the patient's mental state, lifestyle, or physique [73,74] and is highly related to factors of daily life functions such as lower limb muscle strength, sense of balance, walking ability, and risk of falling [66]. Furthermore, the TUG is used to evaluate motor function in a wide range of subjects, from healthy patients to those with lumbar degenerative diseases [74,75]. Therefore, TUG is useful for evaluating dynamic balance in lumbar spine diseases. The MCID of TUG after ASD surgery and lumbar degenerative disease surgery is reported to be 2.0 sec [65] and 2.1 sec [76], respectively.
Figure 7.
Timed up and go test.
5.5. Functional Reach Test (FRT) (Figure 8)
The FRT quantifies participants' dynamic in-place standing balance control as reach distance. The distance between the starting and maximal forward reach distance beyond the participant's arm length represents the reach distance and is recorded in centimeters [77]. Spinal mobility has been shown to significantly impact distance reached [78]. Performance of the FRT involves trunk control and depends on back muscle endurance and strength [79,80]. Injury to paraspinal muscles and changes in proprioception of paraspinal muscles due to lumbar spine surgery affect trunk muscle strength, leading to decreased trunk control and postural instability [81], so balance assessment using FRT is necessary.
5.6. The Balance Evaluation Systems Test (BESTest) (Table 4)
The BESTest is a functionality scale developed to assess balance and risk of falls in the elderly [82]. It consists of 36 items and is grouped into six subsections, which represent different systems that may constrain balance, namely A: biomechanical constraints, B: stability limits/verticality, C: anticipatory postural adjustments, D: postural responses, E: sensory orientation, and F: stability in gait. Each item is scored on a four-point ordinal scale from 0 (worst performance) to 3 (best performance). Total and subscale scores are translated to a percentage score. The BESTest influences QOL in ASD [83], and the reliability of the BESTest has been reported [84]. BESTest is difficult to use in clinical practice due to its complexity, so a shortened version called Mini-BESTest [85] has been developed (Table 5).
5.73. D Motion Analyzers and Force Plate
Usually, gait analysis is generally performed with 3D motion analyzers [86,87] and force plates [88,89]. These devices can be used to analyze gait patterns, detailed joint movements, and gravity lines [90,90]. However, the disadvantages of these methods are cost-effectiveness, complexity of equipment operation and analysis process.
5.8. Triaxial Accelerometer (Figure 9)
Gait sway evaluation using an accelerometer (wearable sensor) has become a popular gait evaluation method due to its cost-effectiveness [92,93,94]. Accelerometers are easy to wear and have no limitations on measurement location, making them simple and practical tools in clinical practice [95]. Root mean square (RMS) of trunk acceleration has been used as one of the indicators of gait sway using accelerometers [96]. RMS represents the degree of amplitude of the waveform, and a larger trunk acceleration RMS during gait indicates a greater gait sway.
6. Physical Therapy after Lumbar Spine Surgery
We believe that postoperative physical therapy after lumbar spine surgery is important to strengthen the affected muscles, improve balance, and facilitate return to ADL. Spinal surgery mainly includes decompression and fusion, with good postoperative results regardless of the surgical technique, and in recent years, multi-level fusion has become increasingly common [58,97]. A comparison of surgical techniques, fixation is more invasive than decompression in terms of blood loss, operative time, and length of hospital stay [98,99].
In recent years, lateral lumbar interbody fusion (LLIF) has become more popular, with extreme lateral interbody fusion (XLIF) and oblique lumbar interbody fusion (OLIF) being the most common LLIF techniques. These techniques are less invasive than the conventional posterior lumbar interbody fusion (PLIF) [100] and transforaminal lumber interbody fusion (TLIF) [101] and allows for the insertion of a larger cage, which allows for a greater restoration of lumbar lordosis [102,103].
In physical therapy, it is necessary to identify the path of entry for spinal fusion and to understand the muscles involved [104] (Figure 10). Muscle atrophy results from denervation due to surgical invasion of the multifidus and erector spinae muscles for posterior approach (PLIF and TLIF) [105,106]. LLIF incises the external oblique, internal oblique, and transversus abdominis muscles, resulting in postoperative muscle weakness (Figure 11). Hence rehabilitation should be focused according to the procedure performed as trunk extension and trunk flexion strength strongly correlate with ODI [107].
6.1. Trunk Muscle Strengthening (Figure 12)
After lumbar spine fusion, motion at the level adjacent to the fusion may be altered to compensate for changes caused by the fusion, an occurrence that must also be taken into account when planning postoperative rehabilitation programs. During the early postoperative phase, strengthening exercises should be performed while keeping the lumbar spine in a neutral position to minimize strain on the fused/adjacent segment and thereafter to avoid breakage or pull out of the implants. In functional neutral spine control exercises (NSCE, Figure 3), a destabilizing force acts on the trunk through loading of the extremities, and therefore proper recruitment of the trunk muscles is required to stabilize the lumbo-pelvic complex [108].
Functional NSCE mimic the trunk muscle activity patterns that occur during activities of daily life, such as lifting, pushing, or pulling movements [111,112]. The NSCE program has two main aims: (i) to improve control of the neutral lumbar spine position and (ii) to increase trunk and hip muscle coordination, strength, and endurance [113]. Figure 3 shows the NSCE we have been using since the acute phase.
6.2. Psoas Muscle Strengthening
In XLIF, the disc space is approached through the psoas muscle. XLIF splits the psoas major muscle, resulting in muscle weakness at a rate of 9% to 31% [114]. OLIF avoids splitting of the psoas major muscle, but is still associated with a 1.2% incidence of psoas muscle weakness [115]. Corrective spinal fusion for ASD with OLIF has also been shown to decrease psoas major muscle strength [116]. Strength of the psoas major muscle is related to postoperative gait sway after ASD correction [86] and to the rate of bony fusion [117] making postoperative strengthening of the psoas major muscle an important part of physical therapy programs.
There are some points to keep in mind when strengthening the psoas major muscle after lumbar fusion surgery. The psoas major muscle has a lumbar extension function in lumbar lordosis and a lumbar flexion function in lumbar kyphosis (Figure 13) [118]. Lumbar kyphosis is a factor in impairment of ADL and adjacent segment diseases [119,120]. Hence, it is necessary to strengthen the psoas major muscles in a posture that can maintain the physiological lordotic position of the lumbar spine. The exercises we perform at our clinic to strengthen the psoas major muscles are shown in Figure 14.
6.3. Exercises to Improve Balance after Spinal Fusion Surgery
Balance dysfunction can occur after spinal surgery, increasing the risk of falls and hip fractures. Patients with long-segment thoracolumbar spine fusions had a significantly higher risk of hip fracture than those with only discectomies [121]. After a spinal fusion, ASD patients exhibit altered proprioception, sensorimotor integration failure, and postural reflex dysfunction [122]. In ASD patients after corrective spinal fusion, dynamic balance capacity improves after 6 months postoperatively [123] and is related to achieving the patient-acceptable symptom state in ODI [124]. In recent years, BESTest has been used to evaluate balance ability in ASD [83,84].
It has been reported that patients with ASD have poorer BESTest results and reduced dynamic balance than healthy elderly people [83]. Halvarsson's program includes five of the six domains of this model [125] (Figure 15). Training balance during dual-task conditions appears to be necessary to improve balance control under situations with divided attention, as balance training with single-task exercises have shown to not transfer to dual-task performance [126].
6.4. Guidance on ADL after Spinal Fusion Surgery
Patients who underwent a multilevel fusion, especially more than 4 levels, reported more limitations because of postoperative lumbar stiffness [127]. Patients with ASD after spinal corrective fusion surgery have difficulty with activities such as picking up objects from the floor, cutting toenails, maintaining personal hygiene, and putting on pants, even 2 years after surgery [128]. Lumbar spinal fusion patients with a fixed pelvis should be taught the use of self-help devices and ADL to prevent implant failure (Figure 16).
Rohlmann et al. reported movements and exercise therapy that place stress on the spine in patients undergoing lumbar corpectomy [129,130]. Movements that place stress on the spine include lifting a weight from the ground, forward elevation of straight arms with a weight in hands, tying shoes, and forward bending [129]. After lumbar spinal fusion, it is necessary to teach patients to avoid these behaviors. The exercise therapy that places stress on the spine should be avoided until bony fusion. These exercises include lifting both legs in the supine position, lifting the pelvis in the supine position, outstretching one arm with or without simultaneously outstretching the contralateral leg in the all-fours position, and arching the back in the all-fours position (Figure 17) [130].
5. Conclusions
The purpose of rehabilitation after lumbar spine surgery is to improve physical and psychosocial function, prevent and treat complications, and mitigate residual symptoms. Physical therapy, cognitive-behavioral therapy, and ADL are used to assess lumbar spine disease using PROs and physical performance tests.
The evaluation of lumbar spine disease requires a detailed understanding of the patient's problems using PROs and physical performance tests. In particular, in rehabilitation after lumbar fusion surgery, it is important to strengthen the abdominal muscles, back muscles, and psoas muscles to improve muscle strength that has decreased due to the surgical invasion, and to perform functional neutral spine control exercises to reduce the risk of falling. In addition, compensatory movements involving trunk strengthening exercises and the use of self-help devices should be taught to reduce the burden on the implants and adjacent vertebrae.
Author Contributions
Tomoyoshi Sakaguchi – writing draft preparation; Sharvari Gunjotikar – writing and editing; Masato Tanaka – conceptualization; Tadashi Komatsubara writing and editing; Kajetan Latka – data collection; Shashank J Ekade – writing and editing; Shrinivas P Prabhu – data collection; Kazuhiko Takamatsu – data collection; Yosuke Yasuda – data collection; Masami Nakagawa – data collection. All authors have read and agreed to the submitted version of the manuscript.
Funding
This research was supported by research funds to promote the hospital functions of Japan Organization of Occupational Health and Safe.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the institutional review boards at Okayama Rosai Hospital (approval No. 484, April 8th, 2024).
Informed Consent Statement
No need.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Woolf, A.D. and Pfleger, B., 2003. Burden of major musculoskeletal conditions. Bulletin of the world healthorganization, 81(9), pp.646-656.
- Manchikanti, L., Singh, V., Falco, F.J., Benyamin, R.M. and Hirsch, J.A., 2014. Epidemiology of low back pain in adults. Neuromodulation: Technology at the Neural Interface, 17, pp.3-10.
- Fehlings, M.G., Tetreault, L., Nater, A., Choma, T., Harrop, J., Mroz, T., Santaguida, C. and Smith, J.S., 2015. The aging of the global population: the changing epidemiology of disease and spinal disorders. Neurosurgery, 77, pp.S1-S5.
- Sivasubramaniam, V., Patel, H.C., Ozdemir, B.A. and Papadopoulos, M.C., 2015. Trends in hospital admissions and surgical procedures for degenerative lumbar spine disease in England: a 15-year time-series study. BMJ open, 5(12), p.e009011.
- Kobayashi, K., Sato, K., Kato, F., Kanemura, T., Yoshihara, H., Sakai, Y., Shinjo, R., Ohara, T., Yagi, H., Matsubara, Y. and Ando, K., 2022. Trends in the numbers of spine surgeries and spine surgeons over the past 15 years. Nagoya Journal of Medical Science, 84(1), p.1.
- Cancelliere C, Wong JJ, Yu H, Nordin M, Mior S, Pereira P, Brunton G, Shearer H, Connell G, Verville L, Taylor-Vaisey A, Côté P. Postsurgical rehabilitation for adults with low back pain with or without radiculopathy who were treated surgically: protocol for a mixed studies systematic review. BMJ Open. 2020 Mar 29;10(3):e036817. [CrossRef] [PubMed] [PubMed Central]
- Ebenbichler GR, Inschlag S, Pflüger V, Stemberger R, Wiesinger G, Novak K, Christoph K, Resch KL. Twelve-year follow-up of a randomized controlled trial of comprehensive physiotherapy following disc herniation operation. Clin Rehabil. 2015 Jun;29(6):548-60. Epub 2014 Oct 6. Erratum in: Clin Rehabil. 2016 Jun;30(6):623. [CrossRef] [PubMed]
- Archer KR, Devin CJ, Vanston SW, Koyama T, Phillips SE, Mathis SL, George SZ, McGirt MJ, Spengler DM, Aaronson OS, Cheng JS, Wegener ST. Cognitive-Behavioral-Based Physical Therapy for Patients With Chronic Pain Undergoing Lumbar Spine Surgery: A Randomized Controlled Trial. J Pain. 2016 Jan;17(1):76-89. Epub 2015 Oct 23. Erratum in: J Pain. 2017 Apr;18(4):477. [CrossRef] [PubMed] [PubMed Central]
- Lindgreen P, Rolving N, Nielsen CV, Lomborg K. Interdisciplinary Cognitive-Behavioral Therapy as Part of Lumbar Spinal Fusion Surgery Rehabilitation: Experience of Patients With Chronic Low Back Pain. Orthop Nurs. 2016 Jul.
- Rushton, A., Eveleigh, G., Petherick, E. J., Heneghan, N., Bennett, R., James, G., & Wright, C. (2012). Physiotherapy rehabilitation following lumbar spinal fusion: a systematic review and meta-analysis of randomised controlled trials. BMJ open, 2(4), e000829.
- Wibault, J., Öberg, B., Dedering, Å., Löfgren, H., Zsigmond, P., & Peolsson, A. (2017). Structured postoperative physiotherapy in patients with cervical radiculopathy: 6-month outcomes of a randomized clinical trial. Journal of Neurosurgery: Spine, 28(1), 1-9.
- Ditunno, J. F. (2017). Linking spinal cord injury rehabilitation between the World Wars: The R. Tait McKenzie legacy. The Journal of Spinal Cord Medicine, 40(6), 641–648. [CrossRef]
- Shrosbree RD. Spinal cord injuries as a result of motorcycle accidents. Paraplegia. 1978 May;16(1):102-12. [CrossRef] [PubMed]
- Bolton D. Looking forward to a decade of the biopsychosocial model. BJPsych Bulletin. 2022;46(4):228-232. [CrossRef]
- Vásquez-Ríos JR, Nava-Bringas TI. Lumbar stabilization exercises. Cir Cir. 2014;82:306–313.
- Dydyk AM, Sapra A. Williams Back Exercises. Treasure Island, FL: Stat Pearls Publishing; 2020. https://www.ncbi.nlm.nih.gov/books/NBK551558/.
- Kelly RP, Johnson JT. Acute low back pain. J Am Med Assoc. 1955 Aug 27;158(17):1520-1.
- Pheasant HC. Practical posture building. Clin Orthop. 1962;25:83-91. PMID: 13943115.
- Cailliet R: Low back pain syndrome. Philadelphia: Daves Company, 1998, pp 156–178.
- Böhler L. Ubungsbehandlung von Wirbelbrüchen [Exercise therapy in vertebral fractures]. Hefte Unfallheilkd. 1971;108:60-3.
- McKenzie R. Acute low back ache and exercises. N Z Med J. 1994 Aug 10;107(983):318. [PubMed]
- Niederer D, Mueller J. Sustainability effects of motor control stabilisation exercises on pain and function in chronic nonspecific low back pain patients: A systematic review with meta-analysis and meta-regression. PLoS One. 2020 Jan 15;15(1):e0227423. [CrossRef] [PubMed] [PubMed Central]
- WHO guideline for non-surgical management of chronic primary low back pain in adults. https://www.who.int/publications/i/item/9789240081789.
- The World Health Organization World report on disability: chapter 4 rehabilitation. Available: https://www.spine.org/Documents/ResearchClinicalCare/Guidelines/LumbarDiscHerniation.pdf [Accessed 4 Apr 2024].
- Snowdon M, Peiris CL. Physiotherapy Commenced Within the First Four Weeks Post-Spinal Surgery Is Safe and Effective: A Systematic Review and Meta-Analysis. Arch Phys Med Rehabil. 2016 Feb;97(2):292-301. Epub 2015 Sep 25. [CrossRef] [PubMed]
- Elsayyad MM, Abdel-Aal NM, Helal ME. Effect of Adding Neural Mobilization Versus Myofascial Release to Stabilization Exercises after Lumbar Spine Fusion: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2021 Feb;102(2):251-260. Epub 2020 Aug 19. [CrossRef] [PubMed]
- Daniels CJ, Cupler ZA, Gliedt JA, Walters S, Schielke AL, Hinkeldey NA, Golley DJ, Hawk C. Manipulative and manual therapies in the management of patients with prior lumbar surgery: A systematic review. Complement Ther Clin Pract. 2021 Feb;42:101261. Epub 2020 Nov 17. [CrossRef] [PubMed]
- Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989 Dec;10(4):407-15. [CrossRef] [PubMed]
- van Hooff ML, Mannion AF, Staub LP, Ostelo RW, Fairbank JC. Determination of the Oswestry Disability Index score equivalent to a "satisfactory symptom state" in patients undergoing surgery for degenerative disorders of the lumbar spine-a Spine Tango registry-based study. Spine J. 2016 Oct;16(10):1221-1230. Epub 2016 Jun 22. [CrossRef] [PubMed]
- Issa TZ, Lee Y, Henry TW, Trenchfield D, Schroeder GD, Vaccaro AR, Kepler CK. Values derived from patient reported outcomes in spine surgery: a systematic review of the minimal clinically important difference, substantial clinical benefit, and patient acceptable symptom state. Eur Spine J. 2023 Oct;32(10):3333-3351. Epub 2023 Aug 29. [CrossRef] [PubMed]
- Parker SL, Adogwa O, Paul AR, Anderson WN, Aaronson O, Cheng JS, McGirt MJ. Utility of minimum clinically important difference in assessing pain, disability, and health state after transforaminal lumbar interbody fusion for degenerative lumbar spondylolisthesis. J Neurosurg Spine. 2011 May;14(5):598-604. Epub 2011 Feb 18. [CrossRef] [PubMed]
- Parker SL, Adogwa O, Mendenhall SK, Shau DN, Anderson WN, Cheng JS, Devin CJ, McGirt MJ. Determination of minimum clinically important difference (MCID) in pain, disability, and quality of life after revision fusion for symptomatic pseudoarthrosis. Spine J. 2012 Dec;12(12):1122-8. Epub 2012 Nov 14. [CrossRef] [PubMed]
- Johnsen LG, Hellum C, Nygaard OP, Storheim K, Brox JI, Rossvoll I, Leivseth G, Grotle M. Comparison of the SF6D, the EQ5D, and the oswestry disability index in patients with chronic low back pain and degenerative disc disease. BMC Musculoskelet Disord. 2013 Apr 26;14:148. [CrossRef] [PubMed] [PubMed Central]
- Solberg T, Johnsen LG, Nygaard ØP, Grotle M. Can we define success criteria for lumbar disc surgery? : estimates for a substantial amount of improvement in core outcome measures. Acta Orthop. 2013 Apr;84(2):196-201. Epub 2013 Mar 19. [CrossRef] [PubMed] [PubMed Central]
- Yoshida G, Hasegawa T, Yamato Y, Kobayashi S, Shin O, Banno T, Mihara Y, Arima H, Ushirozako H, Yasuda T, Togawa D, Matsuyama Y. Minimum Clinically Important Differences in Oswestry Disability Index Domains and Their Impact on Adult Spinal Deformity Surgery. Asian Spine J. 2019 Feb;13(1):35-44. Epub 2018 Oct 18. [CrossRef] [PubMed] [PubMed Central]
- Fukushima M, Oka H, Oshima Y, Yuzawa Y, Matsudaira K, Tanaka S, Inanami H. Evaluation of the Minimum Clinically Important Differences of the Zurich Claudication Questionnaire in Patients With Lumbar Spinal Stenosis. Clin Spine Surg. 2020 Dec;33(10):E499-E503. [CrossRef] [PubMed]
- Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine (Phila Pa 1976). 1983 Mar;8(2):141-4. [CrossRef] [PubMed]
- Fujiwara A, Kobayashi N, Saiki K, Kitagawa T, Tamai K, Saotome K. Association of the Japanese Orthopaedic Association score with the Oswestry Disability Index, Roland-Morris Disability Questionnaire, and short-form 36. Spine (Phila Pa 1976). 2003 Jul 15;28(14):1601-7. [PubMed]
- Fairbank JC, Pynsent PB. The Oswestry Disability Index. Spine (Phila Pa 1976). 2000 Nov 15;25(22):2940-52; discussion 2952. [CrossRef] [PubMed]
- Vianin M. Psychometric properties and clinical usefulness of the Oswestry Disability Index. J Chiropr Med. 2008 Dec;7(4):161-3. [CrossRef] [PubMed] [PubMed Central]
- Haro H, Maekawa S, Hamada Y. Prospective analysis of clinical evaluation and self-assessment by patients after decompression surgery for degenerative lumbar canal stenosis. Spine J. 2008 Mar-Apr;8(2):380-4. Epub 2007 Mar 13. [CrossRef] [PubMed]
- Carreon LY, Berven SH, Djurasovic M, Bratcher KR, Glassman SD. The discriminative properties of the SF-6D compared with the SF-36 and ODI. Spine (Phila Pa 1976). 2013 Jan 1;38(1):60-4. [CrossRef] [PubMed]
- Stucki G, Daltroy L, Liang MH, Lipson SJ, Fossel AH, Katz JN. Measurement properties of a self-administered outcome measure in lumbar spinal stenosis. Spine (Phila Pa 1976). 1996 Apr 1;21(7):796-803. [CrossRef] [PubMed]
- North American Spine Society (NASS). Clinical Guidelines for Multidisciplinary Spine Care Diagnosis and Treatment of Degenerative Lumbar Spinal Stenosis. Burr Ridge (IL): North American Spine Society (NASS); 2007.
- Bae J, Theologis AA, Strom R, Tay B, Burch S, Berven S, Mummaneni PV, Chou D, Ames CP, Deviren V. Comparative analysis of 3 surgical strategies for adult spinal deformity with mild to moderate sagittal imbalance. J Neurosurg Spine. 2018 Jan;28(1):40-49. Epub 2017 Nov 3. [CrossRef] [PubMed]
- Lonner B, Yoo A, Terran JS, Sponseller P, Samdani A, Betz R, Shuffelbarger H, Shah SA, Newton P. Effect of spinal deformity on adolescent quality of life: comparison of operative scheuermann kyphosis, adolescent idiopathic scoliosis, and normal controls. Spine (Phila Pa 1976). 2013 May 20;38(12):1049-55. [CrossRef] [PubMed]
- Haher TR, Gorup JM, Shin TM, Homel P, Merola AA, Grogan DP, Pugh L, Lowe TG, Murray M. Results of the Scoliosis Research Society instrument for evaluation of surgical outcome in adolescent idiopathic scoliosis. A multicenter study of 244 patients. Spine (Phila Pa 1976). 1999 Jul 15;24(14):1435-40. [CrossRef] [PubMed]
- Berven S, Deviren V, Demir-Deviren S, Hu SS, Bradford DS. Studies in the modified Scoliosis Research Society Outcomes Instrument in adults: validation, reliability, and discriminatory capacity. Spine (Phila Pa 1976). 2003 Sep 15;28(18):2164-9; discussion 2169. [CrossRef] [PubMed]
- Yoshihara H, Hasegawa K, Okamoto M, Hatsushikano S, Watanabe K. Relationship between sagittal radiographic parameters and disability in patients with spinal disease using 3D standing analysis. Orthop Traumatol Surg Res. 2018 Nov;104(7):1017-1023. Epub 2018 Aug 11. [CrossRef] [PubMed]
- Smith JS, Klineberg E, Schwab F, Shaffrey CI, Moal B, Ames CP, Hostin R, Fu KM, Burton D, Akbarnia B, Gupta M, Hart R, Bess S, Lafage V; International Spine Study Group. Change in classification grade by the SRS-Schwab Adult Spinal Deformity Classification predicts impact on health-related quality of life measures: prospective analysis of operative and nonoperative treatment. Spine (Phila Pa 1976). 2013 Sep 1;38(19):1663-71. [CrossRef] [PubMed]
- Hart RA, Pro SL, Gundle KR, Marshall LM. Lumbar stiffness as a collateral outcome of spinal arthrodesis: a preliminary clinical study. Spine J. 2013 Feb;13(2):150-6. Epub 2012 Dec 6. [CrossRef] [PubMed]
- Hart RA, Gundle KR, Pro SL, Marshall LM. Lumbar Stiffness Disability Index: pilot testing of consistency, reliability, and validity. Spine J. 2013 Feb;13(2):157-61. Epub 2013 Jan 19. [CrossRef] [PubMed]
- Furuya H, Ito T, Hirohata K, Mitomo S, Yamasaki K, Igarashi H, Omori K, Hoshino M, Hart RA. Construct Validity and Reliability of the Japanese Version of the Lumbar Stiffness Disability Index. Spine (Phila Pa 1976). 2021 Mar 1;46(5):E333-E337. [CrossRef] [PubMed]
- Durand WM, Daniels AH, Hamilton DK, Passias PG, Kim HJ, Protopsaltis T, Lafage V, Smith JS, Shaffrey C, Gupta M, Kelly MP, Klineberg E, Schwab F, Burton D, Bess S, Ames C, Hart R; International Spine Study Group. Younger Patients Are Differentially Affected by Stiffness-Related Disability Following Adult Spinal Deformity Surgery. World Neurosurg. 2019 Dec;132:e297-e304. Epub 2019 Aug 31. [CrossRef] [PubMed]
- Daniels AH, Reid D, Durand W, Disilvestro K, Hamilton DK, Passias P, Kim HJ, Protopsaltis T, LaFage V, Smith JS, Shaffrey C, Gupta M, Klineberg E, Schwab F, Burton D, Bess S, Ames C, Hart R; International Spine Study Group. Sexual Dysfunction Secondary to Lumbar Stiffness in Adult Spinal Deformity Patients Before and After Long-Segment Spinal Fusion. World Neurosurg. 2020 Jul;139:e474-e479. Epub 2020 Apr 18. [CrossRef] [PubMed]
- Watters WC 3rd, Baisden J, Gilbert TJ, Kreiner S, Resnick DK, Bono CM, Ghiselli G, Heggeness MH, Mazanec DJ, O'Neill C, Reitman CA, Shaffer WO, Summers JT, Toton JF; North American Spine Society. Degenerative lumbar spinal stenosis: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis. Spine J. 2008 Mar-Apr;8(2):305-10. Epub 2007 Dec 21. [CrossRef] [PubMed]
- Ishimoto Y, Yoshimura N, Muraki S, Yamada H, Nagata K, Hashizume H, Takiguchi N, Minamide A, Oka H, Kawaguchi H, Nakamura K, Akune T, Yoshida M. Prevalence of symptomatic lumbar spinal stenosis and its association with physical performance in a population-based cohort in Japan: the Wakayama Spine Study. Osteoarthritis Cartilage. 2012 Oct;20(10):1103-8. Epub 2012 Jul 10. [CrossRef] [PubMed]
- Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010 Apr 7;303(13):1259-65. [CrossRef] [PubMed] [PubMed Central]
- Nagai S, Kawabata S, Michikawa T, Ito K, Takeda H, Ikeda D, Kaneko S, Fujita N. Association between frailty and locomotive syndrome in elderly patients with lumbar spinal stenosis: A retrospective longitudinal analysis. Geriatr Gerontol Int. 2024 Jan;24(1):116-122. Epub 2023 Dec 23. [CrossRef] [PubMed]
- Kato S, Demura S, Kabata T, Matsubara H, Kurokawa Y, Okamoto Y, Kuroda K, Kajino Y, Yokogawa N, Inoue D, Tsuchiya H. Risk factors that hinder locomotive syndrome improvement following surgery for musculoskeletal diseases in older patients: A multicentre prospective study. Mod Rheumatol. 2023 Jul 4;33(4):836-842. [CrossRef] [PubMed]
- Kobayashi T, Morimoto T, Otani K, Mawatari M. Locomotive Syndrome and Lumbar Spine Disease: A Systematic Review. J Clin Med. 2022 Feb 27;11(5):1304. [CrossRef] [PubMed] [PubMed Central]
- Studenski S, Perera S, Patel K, Rosano C, Faulkner K, Inzitari M, Brach J, Chandler J, Cawthon P, Connor EB, Nevitt M, Visser M, Kritchevsky S, Badinelli S, Harris T, Newman AB, Cauley J, Ferrucci L, Guralnik J. Gait speed and survival in older adults. JAMA. 2011 Jan 5;305(1):50-8. [CrossRef] [PubMed] [PubMed Central]
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1;48(1):16-31. Erratum in: Age Ageing. 2019 Jul 1;48(4):601. [CrossRef] [PubMed] [PubMed Central]
- Wada T, Tanishima S, Kitsuda Y, Osaki M, Nagashima H, Noma H, Hagino H. Walking speed is associated with postoperative pain catastrophizing in patients with lumbar spinal stenosis: a prospective observational study. BMC Musculoskelet Disord. 2022 Dec 20;23(1):1108. [CrossRef] [PubMed] [PubMed Central]
- Sakaguchi T, Meena U, Tanaka M, Xiang H, Fujiwara Y, Arataki S, Taoka T, Takamatsu K, Yasuda Y, Nakagawa M, Utsunomiya K. Minimal Clinically Important Differences in Gait and Balance Ability in Patients Who Underwent Corrective Long Spinal Fusion for Adult Spinal Deformity. J Clin Med. 2023 Oct 12;12(20):6500. [CrossRef] [PubMed] [PubMed Central]
- Singh SJ, Puhan MA, Andrianopoulos V, Hernandes NA, Mitchell KE, Hill CJ, Lee AL, Camillo CA, Troosters T, Spruit MA, Carlin BW, Wanger J, Pepin V, Saey D, Pitta F, Kaminsky DA, McCormack MC, MacIntyre N, Culver BH, Sciurba FC, Revill SM, Delafosse V, Holland AE. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Eur Respir J. 2014 Dec;44(6):1447-78. Epub 2014 Oct 30. [CrossRef] [PubMed]
- Takenaka H, Kamiya M, Sugiura H, Nishihama K, Ito A, Suzuki J, Hanamura S. Responsiveness and Minimal Clinically Important Difference of the 6-minute Walk Distance in Patients Undergoing Lumbar Spinal Canal Stenosis Surgery. Clin Spine Surg. 2022 Apr 1;35(3):E345-E350. [CrossRef] [PubMed]
- Kondo R, Yamato Y, Nagafusa T, Mizushima T, Hasegawa T, Kobayashi S, Togawa D, Oe S, Kurosu K, Matsuyama Y. Effect of corrective long spinal fusion to the ilium on physical function in patients with adult spinal deformity. Eur Spine J. 2017 Aug;26(8):2138-2145. Epub 2017 Feb 11. [CrossRef] [PubMed]
- Tomkins-Lane CC, Battié MC. Validity and reproducibility of self-report measures of walking capacity in lumbar spinal stenosis. Spine (Phila Pa 1976). 2010 Nov 1;35(23):2097-102. [CrossRef] [PubMed]
- Takenaka H, Kamiya M, Sugiura H, Nishihama K, Suzuki J, Hanamura S. Minimal Clinically Important Difference of the 6-Minute Walk Distance in Patients Undergoing Lumbar Spinal Canal Stenosis Surgery: 12 Months Follow-Up. Spine (Phila Pa 1976). 2023 Apr 15;48(8):559-566. Epub 2022 Dec 28. [CrossRef] [PubMed]
- Gautschi OP, Smoll NR, Corniola MV, Joswig H, Chau I, Hildebrandt G, Schaller K, Stienen MN. Validity and Reliability of a Measurement of Objective Functional Impairment in Lumbar Degenerative Disc Disease: The Timed Up and Go (TUG) Test. Neurosurgery. 2016 Aug;79(2):270-8. [CrossRef] [PubMed]
- Lin SI, Lin RM. Disability and walking capacity in patients with lumbar spinal stenosis: association with sensorimotor function, balance, and functional performance. J Orthop Sports Phys Ther. 2005 Apr;35(4):220-6. [CrossRef] [PubMed]
- Joswig H, Stienen MN, Smoll NR, Corniola MV, Chau I, Schaller K, Hildebrandt G, Gautschi OP. Effects of Smoking on Subjective and Objective Measures of Pain Intensity, Functional Impairment, and Health-Related Quality of Life in Lumbar Degenerative Disk Disease. World Neurosurg. 2017 Mar;99:6-13. Epub 2016 Nov 22. [CrossRef] [PubMed]
- Stienen MN, Joswig H, Smoll NR, Corniola MV, Schaller K, Hildebrandt G, Gautschi OP. Influence of Body Mass Index on Subjective and Objective Measures of Pain, Functional Impairment, and Health-Related Quality of Life in Lumbar Degenerative Disc Disease. World Neurosurg. 2016 Dec;96:570-577.e1. Epub 2016 Sep 28. [CrossRef] [PubMed]
- Podsiadlo D, Richardson S. The timed "Up & Go": a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991 Feb;39(2):142-8. [CrossRef] [PubMed]
- Maldaner N, Sosnova M, Ziga M, Zeitlberger AM, Bozinov O, Gautschi OP, Weyerbrock A, Regli L, Stienen MN. External Validation of the Minimum Clinically Important Difference in the Timed-up-and-go Test After Surgery for Lumbar Degenerative Disc Disease. Spine (Phila Pa 1976). 2022 Feb 15;47(4):337-342. [CrossRef] [PubMed]
- Duncan PW, Weiner DK, Chandler J, Studenski S. Functional reach: a new clinical measure of balance. J Gerontol. 1990 Nov;45(6):M192-7. [CrossRef] [PubMed]
- Schenkman M, Morey M, Kuchibhatla M. Spinal flexibility and balance control among community-dwelling adults with and without Parkinson's disease. J Gerontol A Biol Sci Med Sci. 2000 Aug;55(8):M441-5. [CrossRef] [PubMed]
- de Waroquier-Leroy L, Bleuse S, Serafi R, Watelain E, Pardessus V, Tiffreau AV, Thevenon A. The Functional Reach Test: strategies, performance and the influence of age. Ann Phys Rehabil Med. 2014 Aug-Sep;57(6-7):452-64. Epub 2014 May 29. [CrossRef] [PubMed]
- Biering-Sørensen F. Physical measurements as risk indicators for low-back trouble over a one-year period. Spine (Phila Pa 1976). 1984 Mar;9(2):106-19. [CrossRef] [PubMed]
- Song J, Araghi K, Dupont MM, Shahi P, Bovonratwet P, Shinn D, Dalal SS, Melissaridou D, Virk SS, Iyer S, Dowdell JE, Sheha ED, Qureshi SA. Association between muscle health and patient-reported outcomes after lumbar microdiscectomy: early results. Spine J. 2022 Oct;22(10):1677-1686. Epub 2022 Jun 6. [CrossRef] [PubMed]
- Horak FB, Wrisley DM, Frank J. The Balance Evaluation Systems Test (BESTest) to differentiate balance deficits. Phys Ther. 2009 May;89(5):484-98. Epub 2009 Mar 27. [CrossRef] [PubMed] [PubMed Central]
- Moke L, Severijns P, Schelfaut S, Van de Loock K, Hermans L, Molenaers G, Jonkers I, Scheys L. Performance on Balance Evaluation Systems Test (BESTest) Impacts Health-Related Quality of Life in Adult Spinal Deformity Patients. Spine (Phila Pa 1976). 2018 May 1;43(9):637-646. [CrossRef] [PubMed]
- Severijns P, Overbergh T, Scheys L, Moke L, Desloovere K. Reliability of the balance evaluation systems test and trunk control measurement scale in adult spinal deformity. PLoS One. 2019 Aug 26;14(8):e0221489. [CrossRef] [PubMed] [PubMed Central]
- Franchignoni F, Horak F, Godi M, Nardone A, Giordano A. Using psychometric techniques to improve the Balance Evaluation Systems Test: the mini-BESTest. J Rehabil Med. 2010 Apr;42(4):323-31. [CrossRef] [PubMed] [PubMed Central]
- Miura K, Kadone H, Koda M, Abe T, Funayama T, Noguchi H, Mataki K, Nagashima K, Kumagai H, Shibao Y, Suzuki K, Yamazaki M. Thoracic kyphosis and pelvic anteversion in patients with adult spinal deformity increase while walking: analyses of dynamic alignment change using a three-dimensional gait motion analysis system. Eur Spine J. 2020 Apr;29(4):840-848. Epub 2020 Jan 31. [CrossRef] [PubMed]
- Asada T, Miura K, Koda M, Kadone H, Funayama T, Takahashi H, Noguchi H, Shibao Y, Sato K, Eto F, Mataki K, Yamazaki M. Can Proximal Junctional Kyphosis after Surgery for Adult Spinal Deformity Be Predicted by Preoperative Dynamic Sagittal Alignment Change with 3D Gait Analysis? A Case-Control Study. J Clin Med. 2022 Oct 4;11(19):5871. [CrossRef] [PubMed] [PubMed Central]
- Haddas R, Wood A, Lieberman I, Derman PB. Assessing the cone of economy in patients with spinal disease using only a force plate: an observational retrospective cohort study. Eur Spine J. 2021 Sep;30(9):2504-2513. Epub 2021 Apr 20. [CrossRef] [PubMed]
- Godzik J, Frames CW, Smith Hussain V, Olson MC, Kakarla UK, Uribe JS, Lockhart TE, Turner JD. Postural Stability and Dynamic Balance in Adult Spinal Deformity: Prospective Pilot Study. World Neurosurg. 2020 Sep;141:e783-e791. Epub 2020 Jun 12. [CrossRef]
- Yagi M, Ohne H, Konomi T, Fujiyoshi K, Kaneko S, Takemitsu M, Machida M, Yato Y, Asazuma T. Walking balance and compensatory gait mechanisms in surgically treated patients with adult spinal deformity. Spine J. 2017 Mar;17(3):409-417. Epub 2016 Oct 17. [CrossRef] [PubMed]
- Huysmans SMD, Senden R, Jacobs E, Willems PJB, Marcellis RGJ, Boogaart MVD, Meijer K, Willems PC. Gait alterations in patients with adult spinal deformity. N Am Spine Soc J. 2023 Dec 30;17:100306. [CrossRef] [PubMed] [PubMed Central]
- Zhong R, Rau PP. Are cost-effective technologies feasible to measure gait in older adults? A systematic review of evidence-based literature. Arch Gerontol Geriatr. 2020 Mar-Apr;87:103970. Epub 2019 Nov 2. [CrossRef] [PubMed]
- Sekine M, Tamura T, Yoshida M, Suda Y, Kimura Y, Miyoshi H, Kijima Y, Higashi Y, Fujimoto T. A gait abnormality measure based on root mean square of trunk acceleration. J Neuroeng Rehabil. 2013 Dec 26;10:118. [CrossRef] [PubMed] [PubMed Central]
- Sakaguchi, T.; Sake, N.; Tanaka, M.; Fujiwara, Y.; Arataki, S.; Taoka, T.; Kodama, Y.; Takamatsu, K.; Yasuda, Y.; Nakagawa, M.; et al. Use of a Triaxial Accelerometer to Measure Changes in Gait Sway and Related Motor Function after Corrective Spinal Fusion Surgery for Adult Spinal Deformity. J. Clin. Med. 2024, 13, 1923. [CrossRef]
- Hulleck AA, Menoth Mohan D, Abdallah N, El Rich M, Khalaf K. Present and future of gait assessment in clinical practice: Towards the application of novel trends and technologies. Front Med Technol. 2022 Dec 16;4:901331. [CrossRef] [PubMed] [PubMed Central]
- Menz HB, Lord SR, Fitzpatrick RC. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture. 2003 Aug;18(1):35-46. [CrossRef] [PubMed]
- Amundsen T, Weber H, Nordal HJ, Magnaes B, Abdelnoor M, Lilleâs F. Lumbar spinal stenosis: conservative or surgical management?: A prospective 10-year study. Spine (Phila Pa 1976). 2000 Jun 1;25(11):1424-35; discussion 1435-6. [CrossRef] [PubMed]
- Liang HF, Liu SH, Chen ZX, Fei QM. Decompression plus fusion versus decompression alone for degenerative lumbar spondylolisthesis: a systematic review and meta-analysis. Eur Spine J. 2017 Dec;26(12):3084-3095. Epub 2017 Jun 24. [CrossRef] [PubMed]
- Chen Z, Xie P, Feng F, Chhantyal K, Yang Y, Rong L. Decompression Alone Versus Decompression and Fusion for Lumbar Degenerative Spondylolisthesis: A Meta-Analysis. World Neurosurg. 2018 Mar;111:e165-e177. Epub 2017 Dec 14. [CrossRef] [PubMed]
- Briggs H, Milligan PR: Chip fusion of the low back following exploration of the spinal canal. J Bone Joint Surg 26:125- 130,1944.
- Hammad A, Wirries A, Ardeshiri A, Nikiforov O, Geiger F. Open versus minimally invasive TLIF: literature review and meta-analysis. J Orthop Surg Res. 2019 Jul 22;14(1):229. [CrossRef] [PubMed] [PubMed Central]
- Tan MWP, Sayampanathan AA, Jiang L, Guo CM. Comparison of Outcomes Between Single-level Lateral Lumbar Interbody Fusion and Transforaminal Lumbar Interbody Fusion: A Meta-analysis and Systematic Review. Clin Spine Surg. 2021 Dec 1;34(10):395-405. [CrossRef] [PubMed]
- Hsieh PC, Koski TR, O'Shaughnessy BA, Sugrue P, Salehi S, Ondra S, Liu JC. Anterior lumbar interbody fusion in comparison with transforaminal lumbar interbody fusion: implications for the restoration of foraminal height, local disc angle, lumbar lordosis, and sagittal balance. J Neurosurg Spine. 2007 Oct;7(4):379-86. [CrossRef] [PubMed]
- Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015 Dec;1(1):2-18. [CrossRef] [PubMed] [PubMed Central]
- Waschke A, Hartmann C, Walter J, Dünisch P, Wahnschaff F, Kalff R, Ewald C. Denervation and atrophy of paraspinal muscles after open lumbar interbody fusion is associated with clinical outcome--electromyographic and CT-volumetric investigation of 30 patients. Acta Neurochir (Wien). 2014 Feb;156(2):235-44. Epub 2014 Jan 3. [CrossRef] [PubMed]
- Cho SM, Kim SH, Ha SK, Kim SD, Lim DJ, Cha J, Kim BJ. Paraspinal muscle changes after single-level posterior lumbar fusion: volumetric analyses and literature review. BMC Musculoskelet Disord. 2020 Feb 5;21(1):73. [CrossRef] [PubMed] [PubMed Central]
- Tarnanen S, Neva MH, Kautiainen H, Ylinen J, Pekkanen L, Kaistila T, Vuorenmaa M, Häkkinen A. The early changes in trunk muscle strength and disability following lumbar spine fusion. Disabil Rehabil. 2013 Jan;35(2):134-9. Epub 2012 Jun 7. [CrossRef] [PubMed]
- Tarnanen SP, Neva MH, Häkkinen K, Kankaanpää M, Ylinen J, Kraemer WJ, Newton RU, Häkkinen A. Neutral spine control exercises in rehabilitation after lumbar spine fusion. J Strength Cond Res. 2014 Jul;28(7):2018-25. [CrossRef] [PubMed]
- Hagins M, Adler K, Cash M, Daugherty J, Mitrani G. Effects of practice on the ability to perform lumbar stabilization exercises. J Orthop Sports Phys Ther. 1999 Sep;29(9):546-55. [CrossRef] [PubMed]
- Grooms DR, Grindstaff TL, Croy T, Hart JM, Saliba SA. Clinimetric analysis of pressure biofeedback and transversus abdominis function in individuals with stabilization classification low back pain. J Orthop Sports Phys Ther. 2013 Mar;43(3):184-93. Epub 2012 Nov 16. [CrossRef] [PubMed]
- McGill SM, Karpowicz A, Fenwick CM, Brown SH. Exercises for the torso performed in a standing posture: spine and hip motion and motor patterns and spine load. J Strength Cond Res. 2009 Mar;23(2):455-64. [CrossRef] [PubMed]
- Voight ML, Hoogenboom BJ, Cook G. The chop and lift reconsidered: integrating neuromuscular principles into orthopedic and sports rehabilitation. N Am J Sports Phys Ther. 2008 Aug;3(3):151-9. [PubMed] [PubMed Central]
- Tarnanen S, Neva MH, Dekker J, Häkkinen K, Vihtonen K, Pekkanen L, Häkkinen A. Randomized controlled trial of postoperative exercise rehabilitation program after lumbar spine fusion: study protocol. BMC Musculoskelet Disord. 2012 Jul 20;13:123. [CrossRef] [PubMed] [PubMed Central]
- Epstein NE. Review of Risks and Complications of Extreme Lateral Interbody Fusion (XLIF). Surg Neurol Int. 2019 Dec 6;10:237. [CrossRef] [PubMed] [PubMed Central]
- Li JX, Phan K, Mobbs R. Oblique Lumbar Interbody Fusion: Technical Aspects, Operative Outcomes, and Complications. World Neurosurg. 2017 Feb;98:113-123. Epub 2016 Oct 21. [CrossRef] [PubMed]
- Yagi M, Fujita N, Hasegawa T, Inoue G, Kotani Y, Ohtori S, Orita S, Oshima Y, Sakai D, Sakai T, Taneichi H, Togawa D, Nakanishi K, Nakashima H, Yoshii T, Nakamura M, Iwasaki M, Watanabe M, Haro H, Kanemura T, Hosogane N; New Technology Assessment Committee of The Japanese Society for Spine Surgery and Related Research. Nationwide Survey of the Surgical Complications Associated with Lateral Lumbar Interbody Fusion in 2015-2020. Spine Surg Relat Res. 2022 Dec 12;7(3):249-256. [CrossRef] [PubMed] [PubMed Central]
- Choi MK, Kim SB, Park CK, Malla HP, Kim SM. Cross-Sectional Area of the Lumbar Spine Trunk Muscle and Posterior Lumbar Interbody Fusion Rate: A Retrospective Study. Clin Spine Surg. 2017 Jul;30(6):E798-E803. [CrossRef] [PubMed]
- Santaguida PL, McGill SM. The psoas major muscle: a three-dimensional geometric study. J Biomech. 1995 Mar;28(3):339-45. [CrossRef] [PubMed]
- Blondel B, Schwab F, Ungar B, Smith J, Bridwell K, Glassman S, Shaffrey C, Farcy JP, Lafage V. Impact of magnitude and percentage of global sagittal plane correction on health-related quality of life at 2-years follow-up. Neurosurgery. 2012 Aug;71(2):341-8; discussion 348. [CrossRef] [PubMed]
- Phan K, Nazareth A, Hussain AK, Dmytriw AA, Nambiar M, Nguyen D, Kerferd J, Phan S, Sutterlin C 3rd, Cho SK, Mobbs RJ. Relationship between sagittal balance and adjacent segment disease in surgical treatment of degenerative lumbar spine disease: meta-analysis and implications for choice of fusion technique. Eur Spine J. 2018 Aug;27(8):1981-1991. Epub 2018 May 28. Erratum in: Eur Spine J. 2021 Dec;30(12):3774. [CrossRef] [PubMed]
- Li CY, Chang CL, Tai TW. Incidence and risk factors for hip fracture in elderly patients undergoing lumbar spine surgery: a nationwide database study with 11-year follow-up. Osteoporos Int. 2018 Dec;29(12):2717-2723. Epub 2018 Oct 15. [CrossRef] [PubMed]
- Yagi M, Ohne H, Kaneko S, Machida M, Yato Y, Asazuma T. Does corrective spine surgery improve the standing balance in patients with adult spinal deformity? Spine J. 2018 Jan;18(1):36-43. Epub 2017 May 23. [CrossRef] [PubMed]
- Sakaguchi, T.; Tanaka, M.; Suthar, H.; Fujiwara, Y.; Uotani, K.; Arataki, S.; Yamauchi, T.; Sugyo, A.; Takamatsu, K.; Yasuda, Y.; et al. Chronological Evaluation of Gait Ability and Posture Balance after Adult Spinal Deformity Surgery. Appl. Sci. 2022, 12, 4285. [CrossRef]
- Sakaguchi T, Tanaka M, Sake N, Latka K, Fujiwara Y, Arataki S, Yamauchi T, Takamatsu K, Yasuda Y, Nakagawa M, Takahashi N, Kishimoto T. The Most Significant Factor Affecting Gait and Postural Balance in Patients' Activities of Daily Living Following Corrective Surgery for Deformity of the Adult Spine. Medicina (Kaunas). 2022 Aug 18;58(8):1118. [CrossRef] [PubMed] [PubMed Central]
- Halvarsson A, Dohrn IM, Ståhle A. Taking balance training for older adults one step further: the rationale for and a description of a proven balance training programme. Clin Rehabil. 2015 May;29(5):417-25. Epub 2014 Sep 8. [CrossRef] [PubMed] [PubMed Central]
- Agmon M, Belza B, Nguyen HQ, Logsdon RG, Kelly VE. A systematic review of interventions conducted in clinical or community settings to improve dual-task postural control in older adults. Clin Interv Aging. 2014 Mar 25;9:477-92. [CrossRef] [PubMed] [PubMed Central]
- Kimura H, Fujibayashi S, Otsuki B, Takahashi Y, Nakayama T, Matsuda S. Effects of Lumbar Stiffness After Lumbar Fusion Surgery on Activities of Daily Living. Spine (Phila Pa 1976). 2016 Apr;41(8):719-27. [CrossRef] [PubMed]
- Togawa D, Hasegawa T, Yamato Y, Yoshida G, Kobayashi S, Yasuda T, Oe S, Banno T, Arima H, Mihara Y, Ushirozako H, Matsuyama Y. Postoperative Disability After Long Corrective Fusion to the Pelvis in Elderly Patients With Spinal Deformity. Spine (Phila Pa 1976). 2018 Jul 15;43(14):E804-E812. [CrossRef] [PubMed]
- Rohlmann A, Pohl D, Bender A, Graichen F, Dymke J, Schmidt H, Bergmann G. Activities of everyday life with high spinal loads. PLoS One. 2014 May 27;9(5):e98510. [CrossRef] [PubMed] [PubMed Central]
- Rohlmann A, Schwachmeyer V, Graichen F, Bergmann G. Spinal loads during post-operative physiotherapeutic exercises. PLoS One. 2014 Jul 7;9(7):e102005. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Williams lumbar flexion exercises, A: Pelvic tilt B: Sit-up in knee flexion C: Double knees to chest to stretch the elector spine, D: Seated reach to toes stretches the hamstrings and elector spine, E: Forward crouch to stretch iliofemoral ligament F: Seated flexion G, H: Strengthening of quadriceps muscles, and stretching of gluteus maximus and elector spine.
Figure 1.
Williams lumbar flexion exercises, A: Pelvic tilt B: Sit-up in knee flexion C: Double knees to chest to stretch the elector spine, D: Seated reach to toes stretches the hamstrings and elector spine, E: Forward crouch to stretch iliofemoral ligament F: Seated flexion G, H: Strengthening of quadriceps muscles, and stretching of gluteus maximus and elector spine.
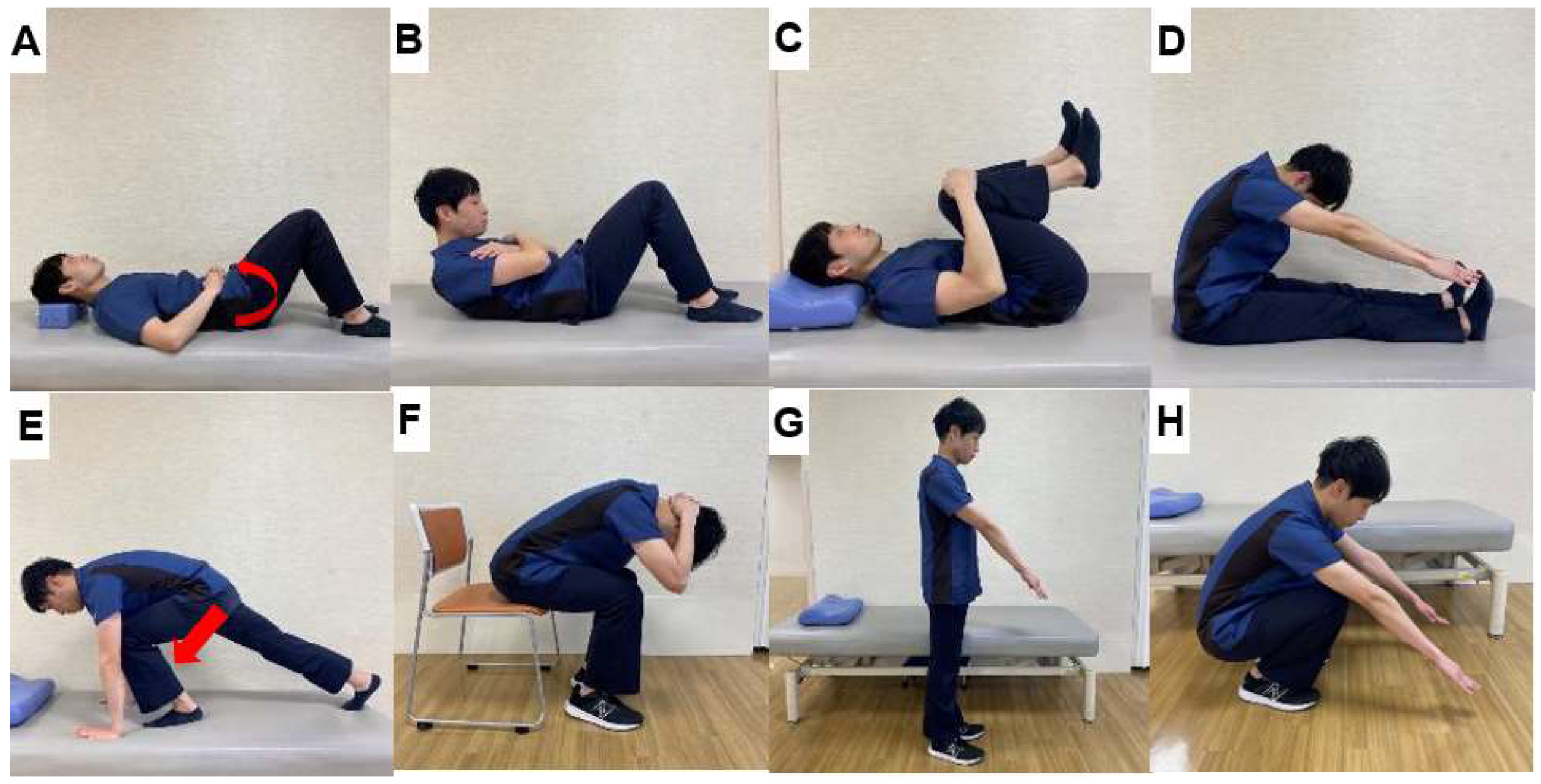
Figure 2.
McKenzie exercises, A: Flexion in standing B: Extension in standing C: Flexion in lying, D: Therapist assisted side glide in standing E: Side glide in standing F: Extension in lying.
Figure 2.
McKenzie exercises, A: Flexion in standing B: Extension in standing C: Flexion in lying, D: Therapist assisted side glide in standing E: Side glide in standing F: Extension in lying.
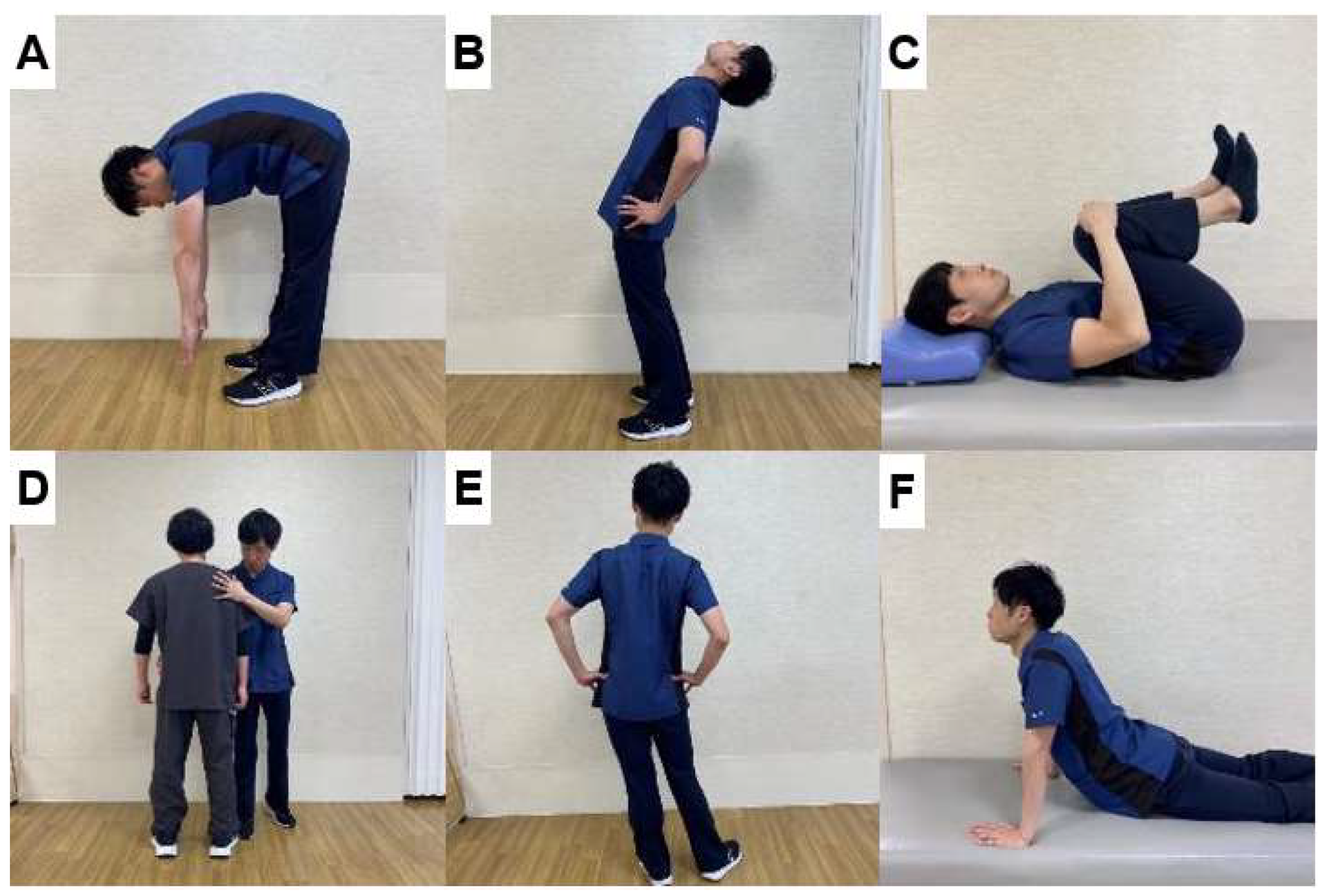
Figure 3.
Interpretation of changes in post-treatment evaluation results, A: Post-treatment evaluation results are measurement error and clinically not important., B: The post-treatment assessment results showed changes beyond the measurement error, but not clinically important changes., C: The results of the post-treatment evaluation show clinically important changes.
Figure 3.
Interpretation of changes in post-treatment evaluation results, A: Post-treatment evaluation results are measurement error and clinically not important., B: The post-treatment assessment results showed changes beyond the measurement error, but not clinically important changes., C: The results of the post-treatment evaluation show clinically important changes.
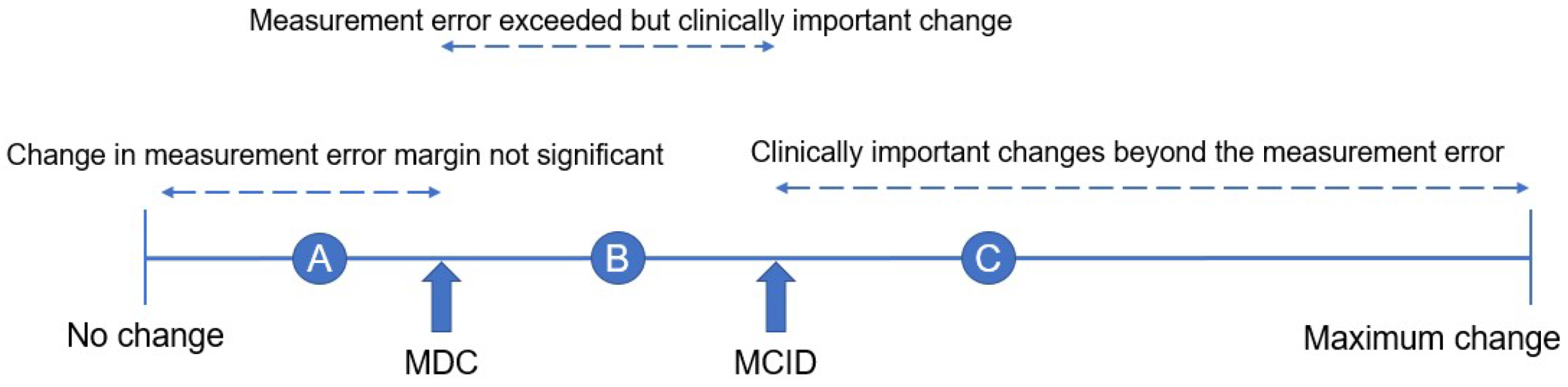
Figure 4.
Roland-Morris Low back pain and Disability Questionnaire (RMDQ).
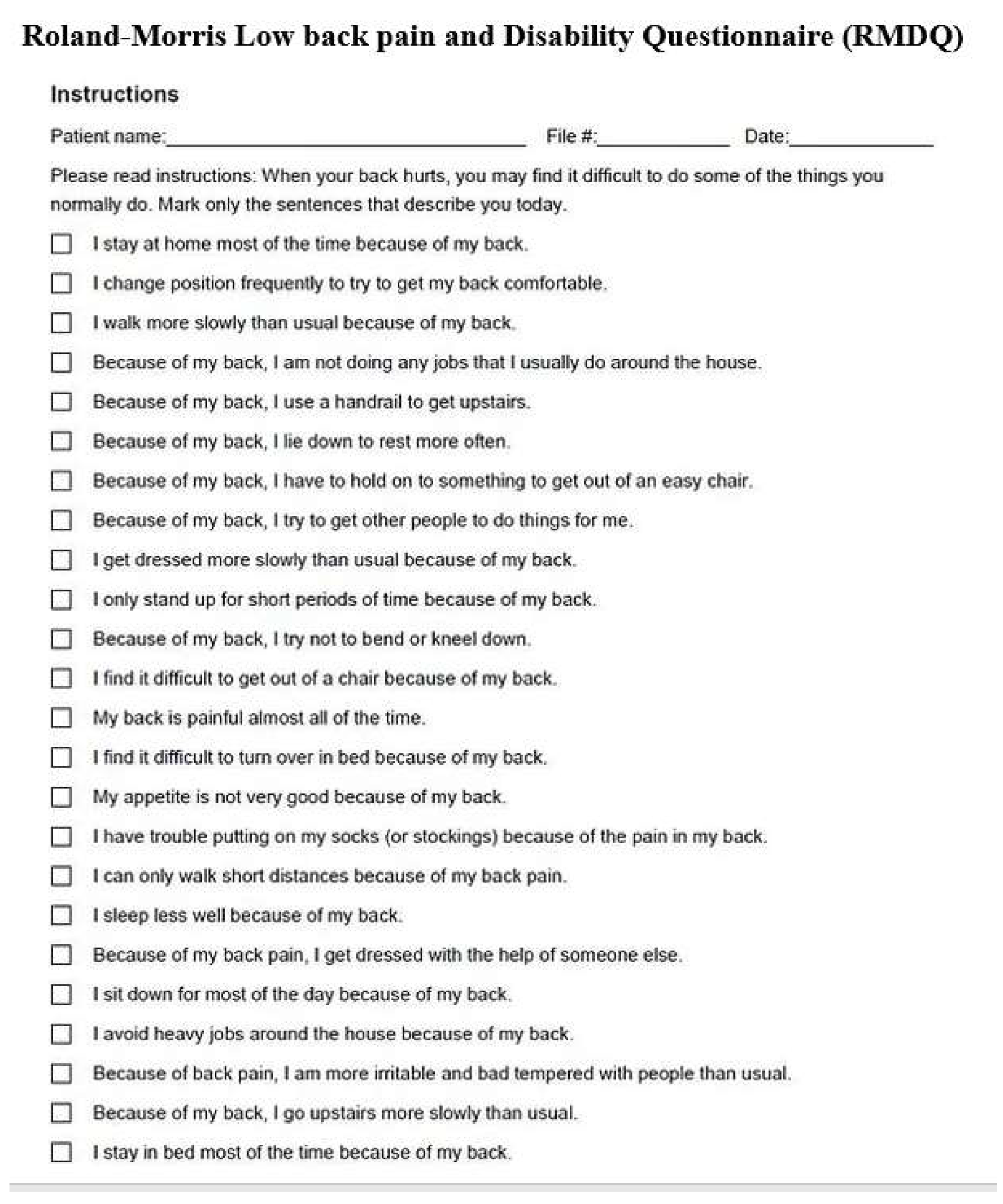
Figure 5.
Oswestry Disability Index.

Figure 6.
Walk velocity.
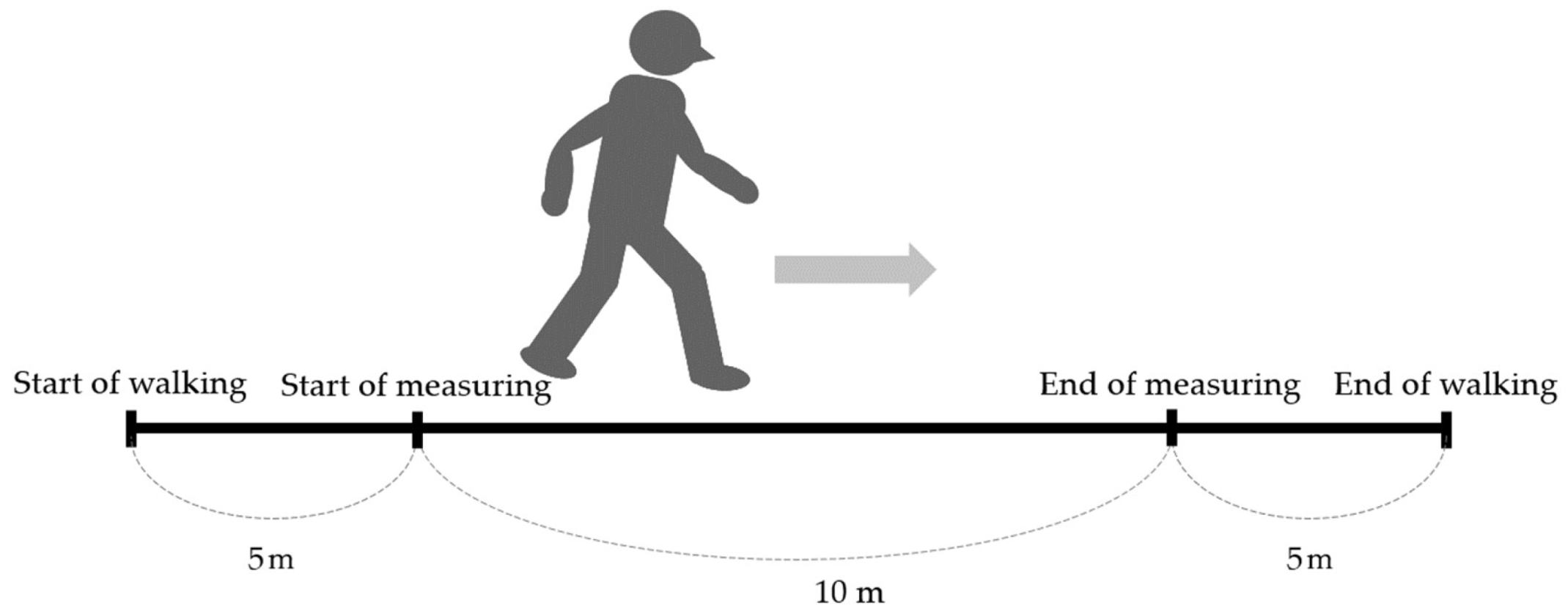
Figure 8.
Functional Reach Test.
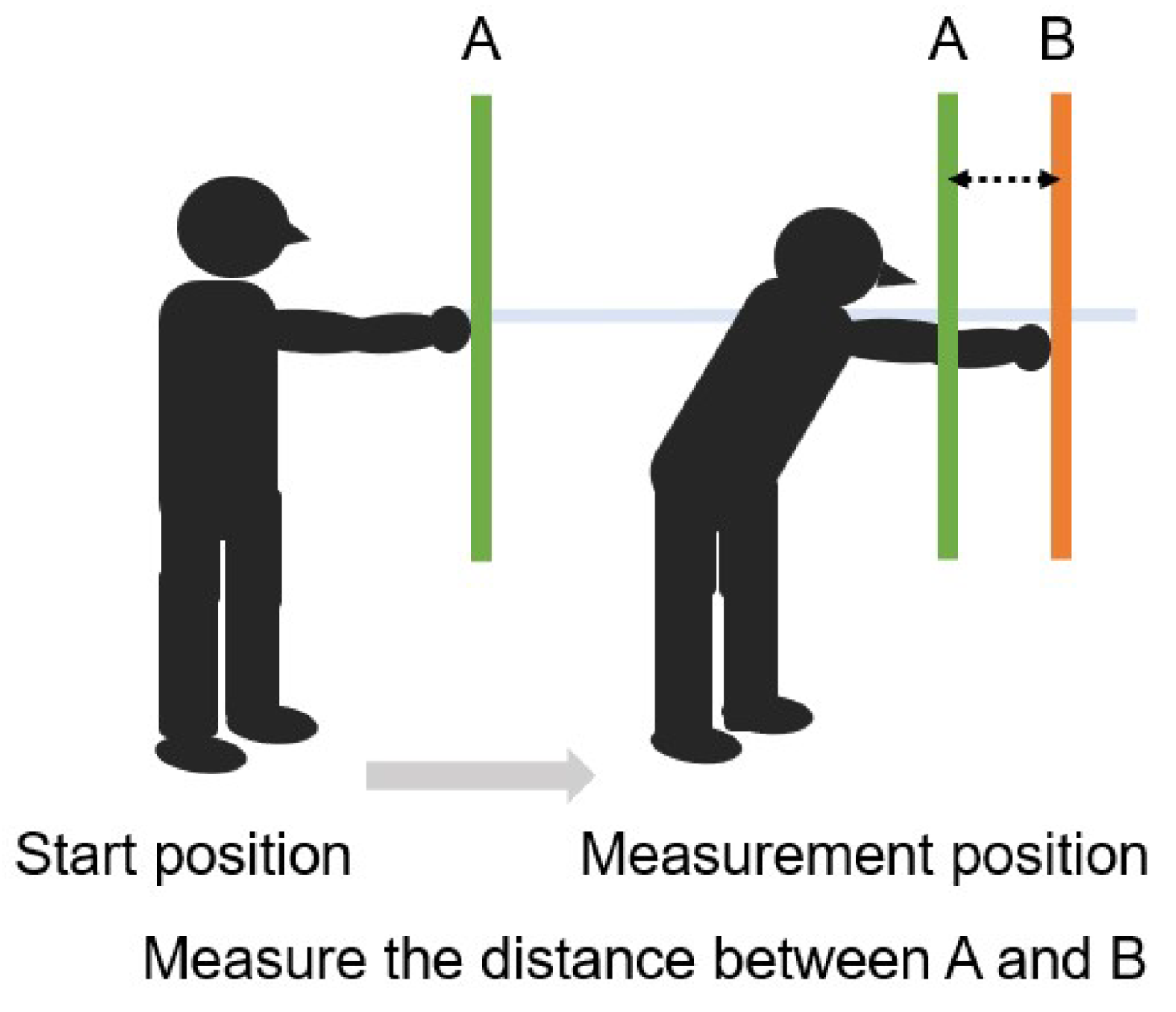
Figure 9.
The principle of accelerometer.
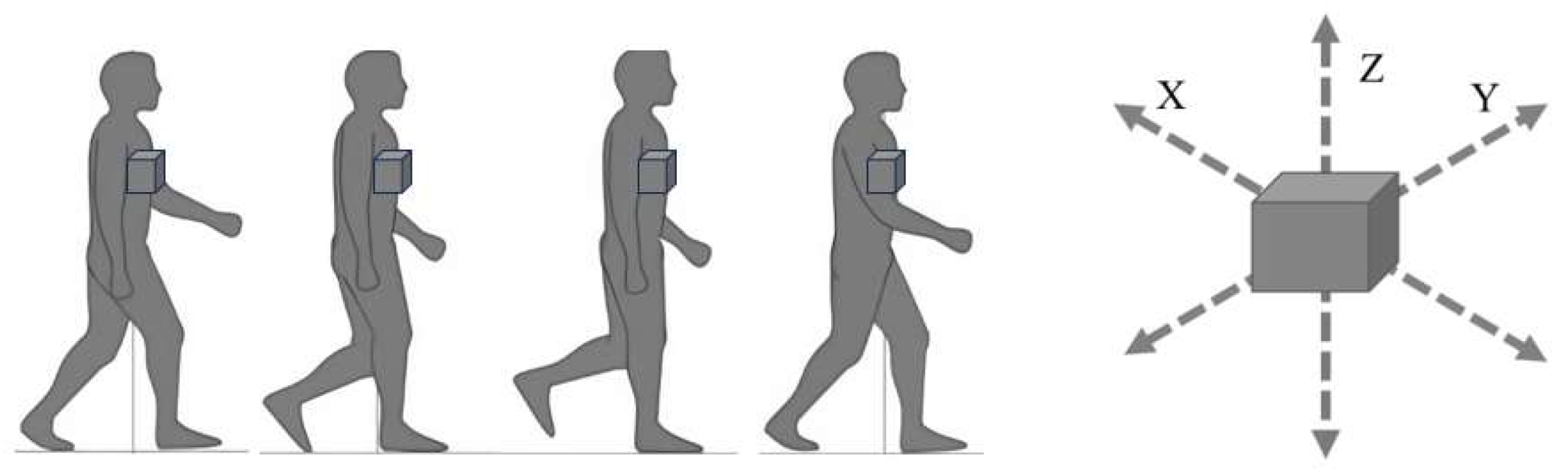
Figure 10.
The path of entry for different spinal fusion techniques.
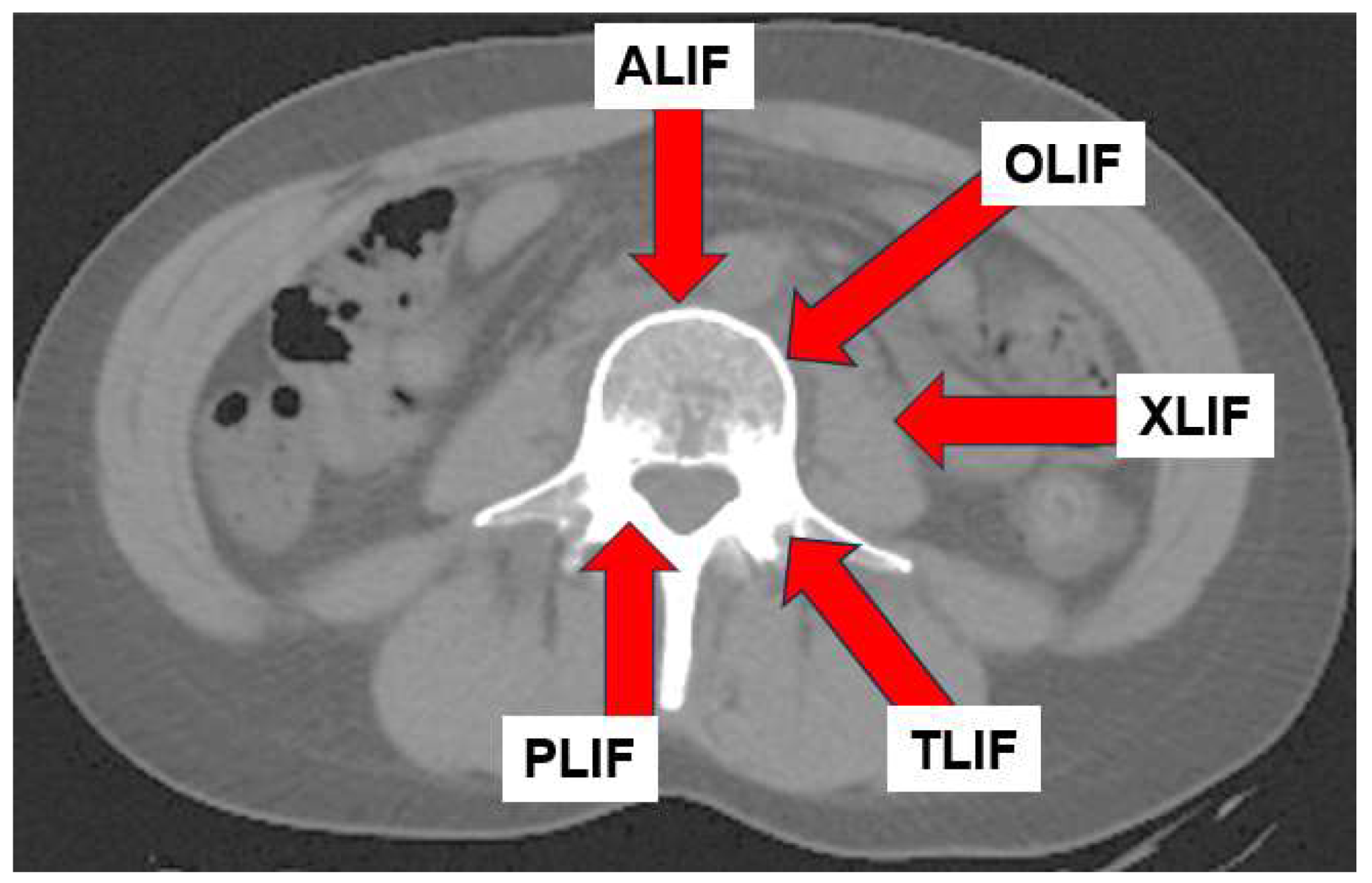
Figure 11.
Oblique lumbar interbody fusion (OLIF) approach.
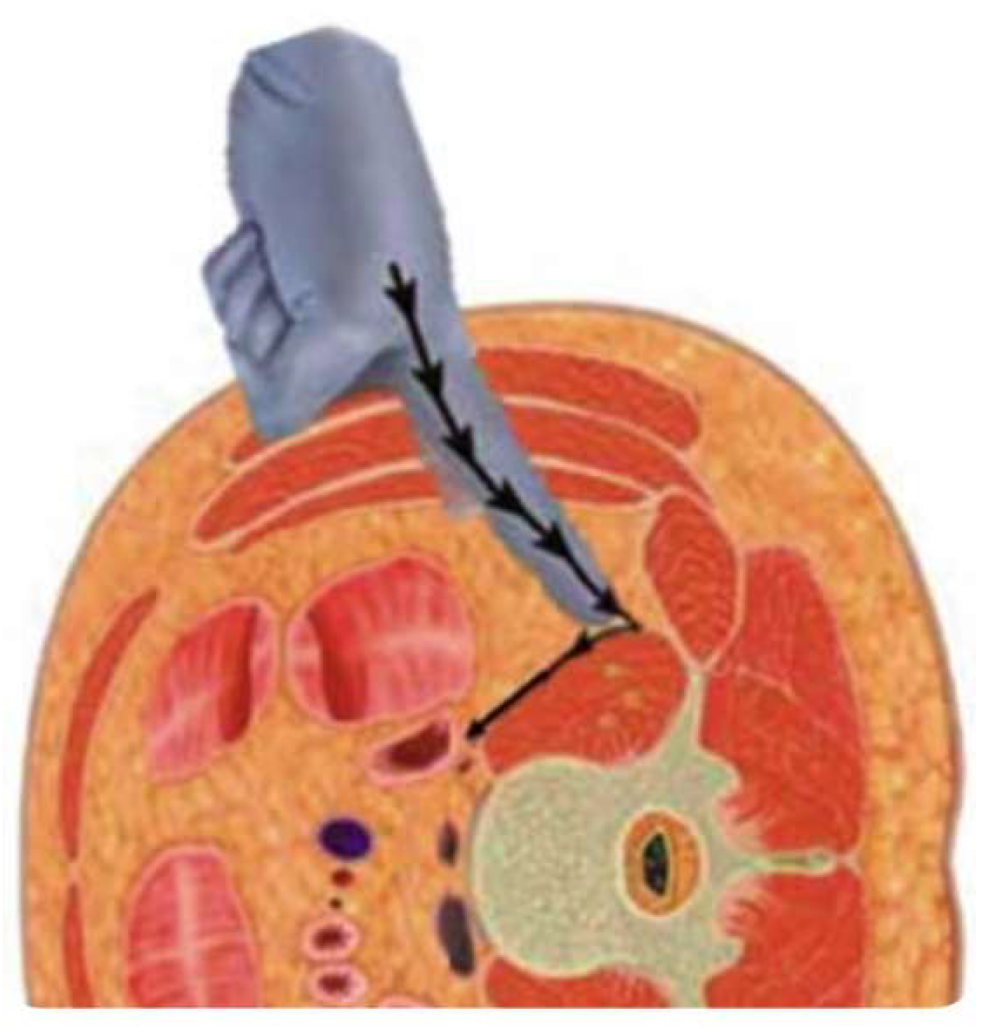
Figure 12.
Functional neutral spine control exercises, A: Drow-in [109,110], B: Bird dog exercise, C: Clam shell exercise, D: Bilateral shoulder extension, E: Bilateral shoulder flexion, F: Hip abduction.
Figure 12.
Functional neutral spine control exercises, A: Drow-in [109,110], B: Bird dog exercise, C: Clam shell exercise, D: Bilateral shoulder extension, E: Bilateral shoulder flexion, F: Hip abduction.
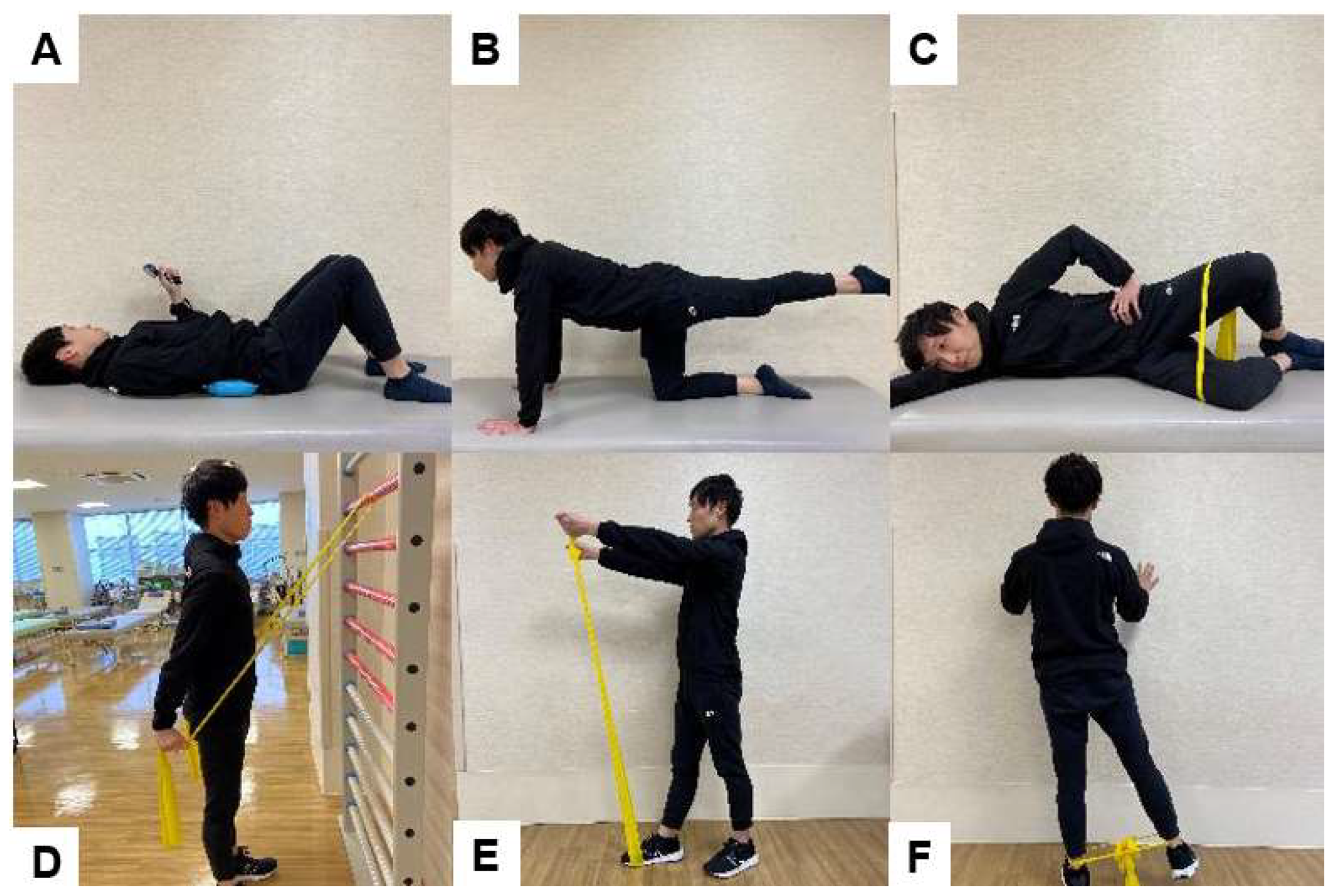
Figure 13.
Effect of iliopsoas muscle in three positions.
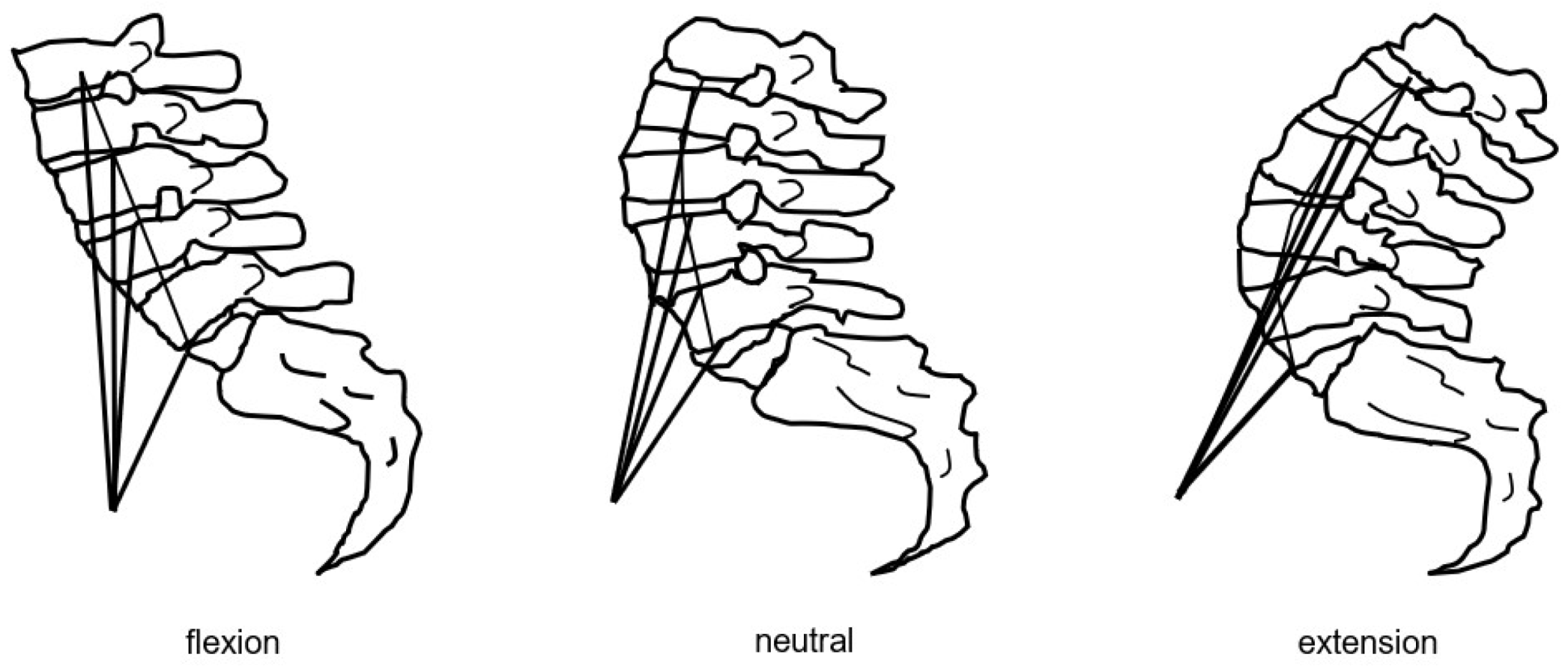
Figure 14.
Iliopsoas muscle exercise, A: Hip flexion exercise in sitting position , B: Wall Standing exercise.
Figure 14.
Iliopsoas muscle exercise, A: Hip flexion exercise in sitting position , B: Wall Standing exercise.
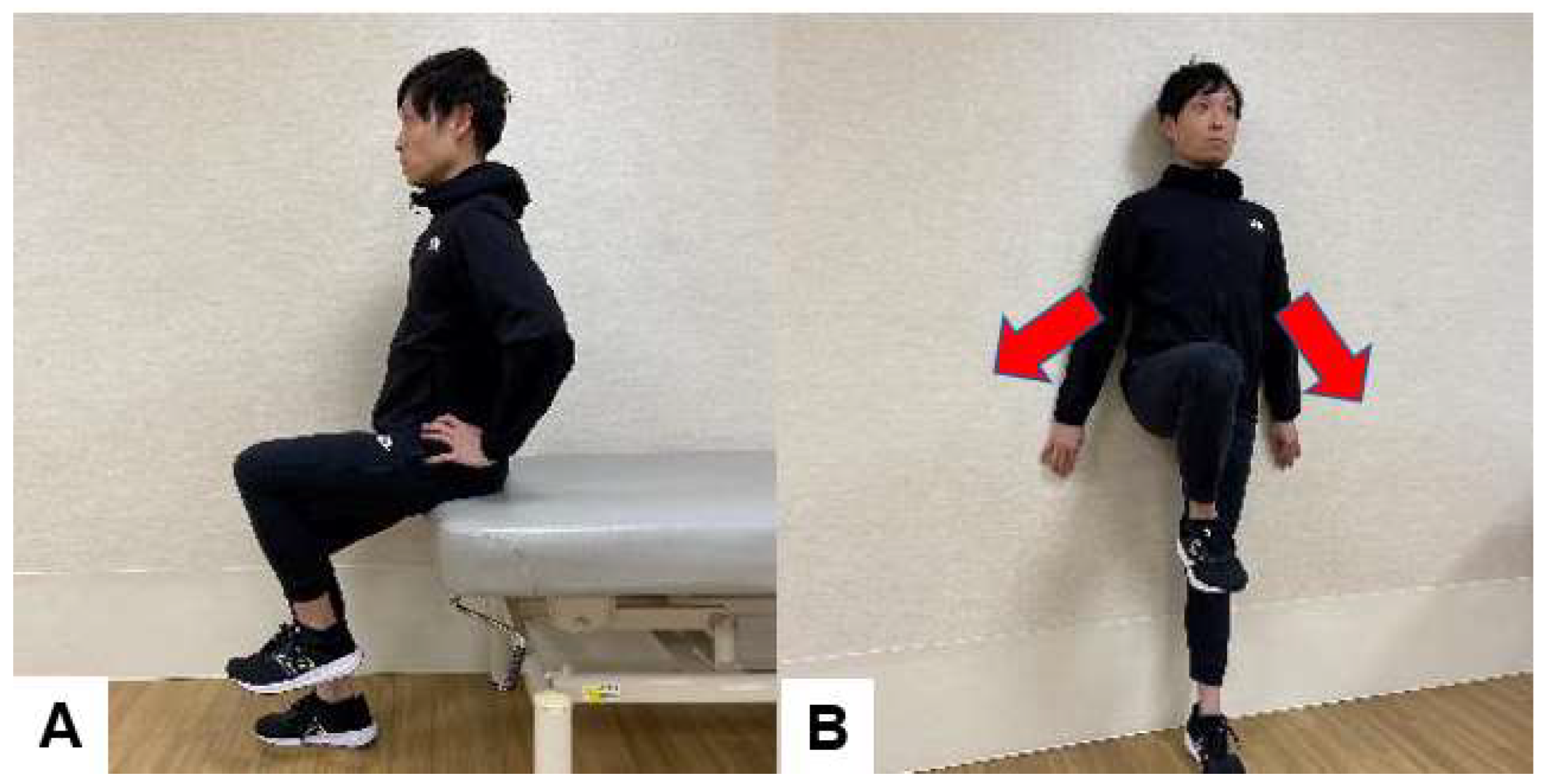
Figure 15.
Dual and multitask balance exercise, A: Walk while trying not to drop the ball on the tray B: Stand on balance cushions with eyes closed, C: Catch the ball while standing on the balance cushion, D: Slalom walking with additional cognitive tasks.
Figure 15.
Dual and multitask balance exercise, A: Walk while trying not to drop the ball on the tray B: Stand on balance cushions with eyes closed, C: Catch the ball while standing on the balance cushion, D: Slalom walking with additional cognitive tasks.
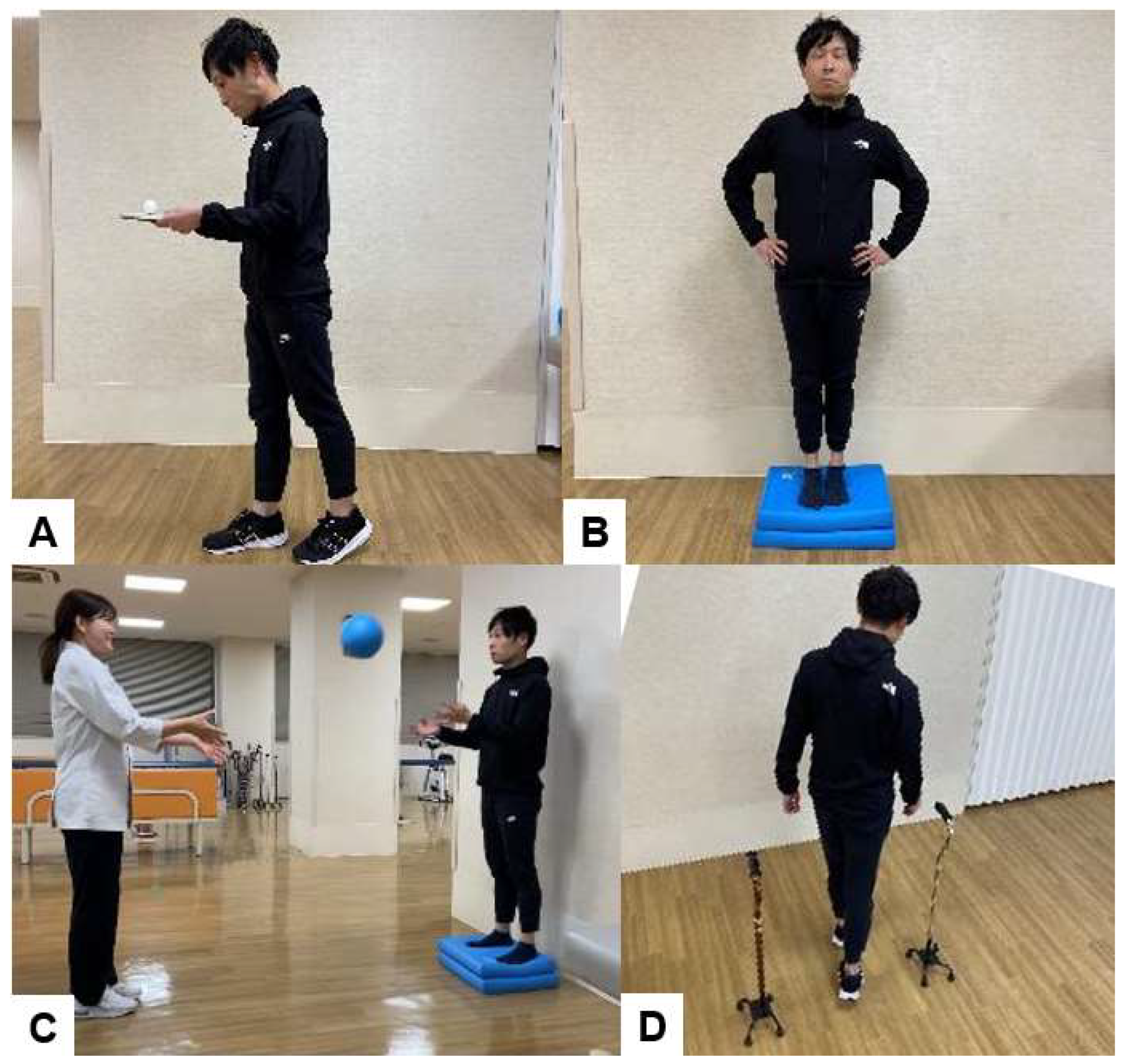
Figure 16.
Self-help devices and coaching of ADL, A: Getting up from lateral position, B: Pick up things from the floor , C: How to pick up objects from the floor using self-help tools, D: How to put on pants using a trouser aid, E: How to put on pants using a trouser aid, F: How to put on shoes using a shoehorn.
Figure 16.
Self-help devices and coaching of ADL, A: Getting up from lateral position, B: Pick up things from the floor , C: How to pick up objects from the floor using self-help tools, D: How to put on pants using a trouser aid, E: How to put on pants using a trouser aid, F: How to put on shoes using a shoehorn.
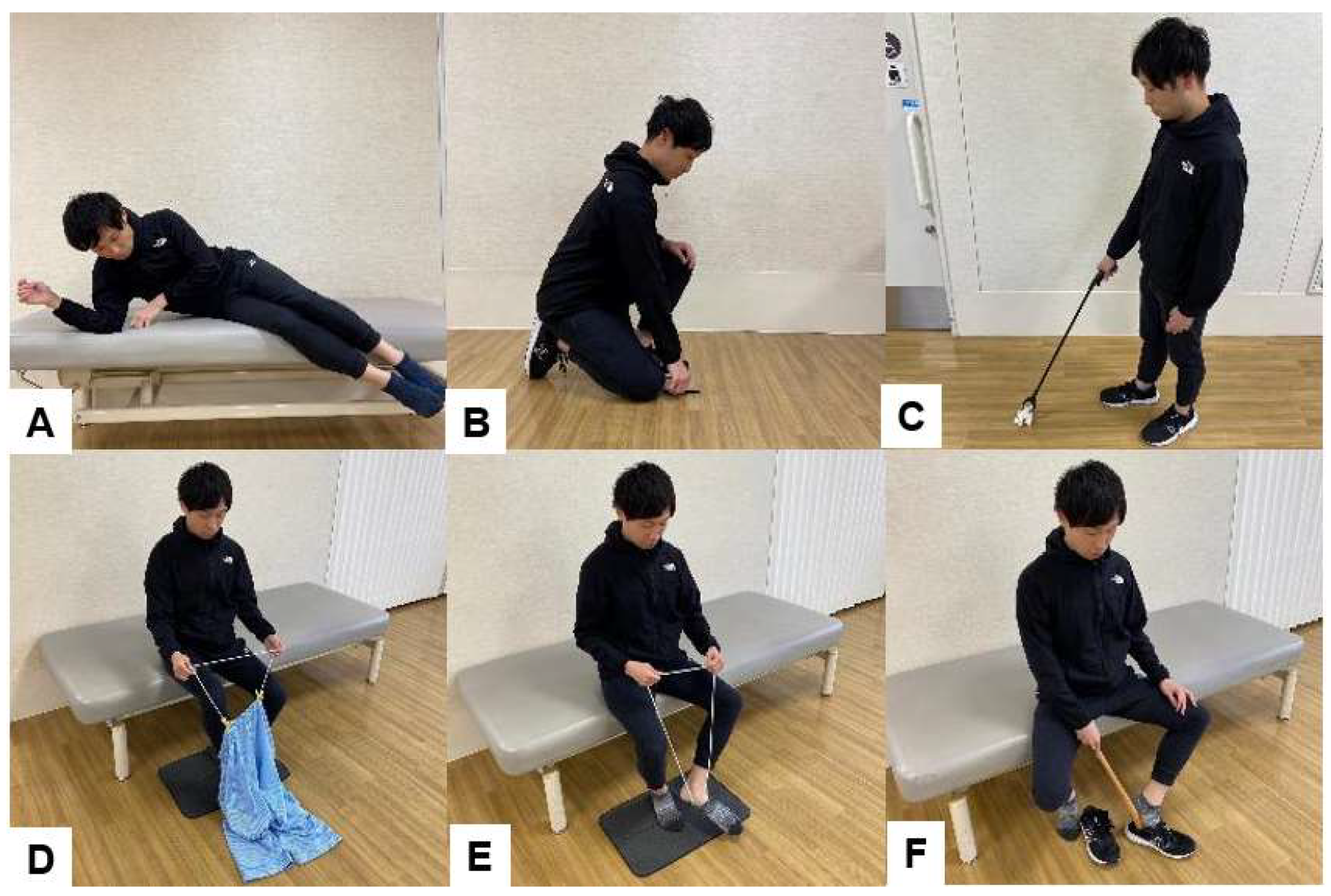
Figure 17.
The restricted exercise, A: Lifting both legs in the supine position ,B: Lifting the pelvis in the supine position, C: Outstretching one arm with or without simultaneously outstretching the contralateral leg in the all-fours position, D: Arching the back in the all-fours position.
Figure 17.
The restricted exercise, A: Lifting both legs in the supine position ,B: Lifting the pelvis in the supine position, C: Outstretching one arm with or without simultaneously outstretching the contralateral leg in the all-fours position, D: Arching the back in the all-fours position.
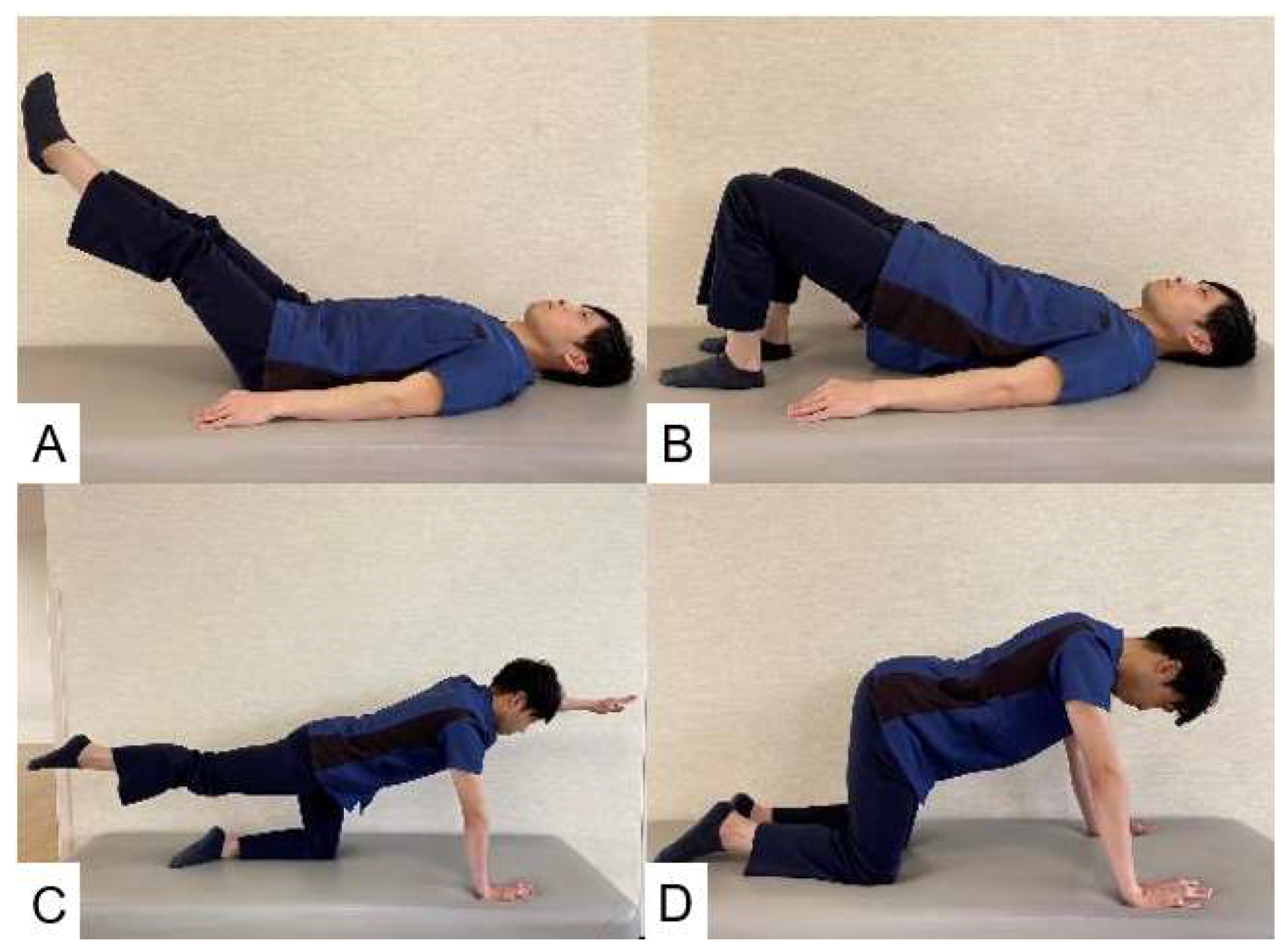
Table 2.
Example of selected interventions for rehabilitation after lumbar surgery.
| Intervention | Definition | Example |
| Patient education and self-management [9] | Teaching patient’s skills that they can use to manage their health condition | How to deal with pain The importance of physical activity in pain reduction Restrictions and working posture postoperatively (ergonomics) Coping with pain flare-ups How to return to work and cope with physical, social, and other barriers |
| Early Exercise [25] | A subcategory of physical activity that is planned, structured, repetitive, and purposeful; can be supervised (eg, by a healthcare professional) or unsupervised | Stretching, Muscle strengthening Endurance exercises Neuromuscular closed chain exercises Range of motion exercise |
| Manual therapies [26,27] | Myofascial release: Technique that applies low-impact, prolonged stretching to the fascial complex to restore optimal length of fascial tissue, decrease pain, and improve functionality. Neural mobilization: A technique that stretches damaged nerves and improves their glide and extensibility. Manipulation: techniques incorporating a high-velocity low-amplitude impulse or thrust applied at or near the end of a joint’s passive range of motion Mobilization: techniques incorporating a low-velocity and small or large amplitude oscillatory movement, within a joint’s passive range of motion |
Myofascial release Neural mobilization Massage Lumbar manipulation, mobilization |
| Assistive technologies | Any item, piece of equipment or product system, used to increase, maintain, or improve the functional capabilities of people with disabilities | Walking aids Socks aids Pants aids Shoehorn Reacher |
Table 4.
BESTest.
| Ⅰ. Biomechanical constraints | Ⅱ. Stability limits | Ⅲ. Anticipatory Postural Adjustments | Ⅳ. Postural Responses | Ⅴ. Sensory orientation | Ⅵ. Stability in gait |
|---|---|---|---|---|---|
| 1. Base of support | 6. Sitting verticality (left and right) and lateral lean | 9. Sit to stand | 14.In-place response, forward | 19. Sensory integration for balance, Stance on firm surface, | 21. Gait level surface |
| 2. CoM alignment | 7. Functional reach forward | 10.Rise to toes | 15. In-place response, backward | 20. Incline, EC | 22. Change in gait speed |
| 3. Ankle strength and ROM | 8. Functional reach lateral | 11. Stand on one leg | 16. Compensatory stepping correction, forward | 23. Walk with head turns, horizontal | |
| 4. Hip/trunk lateral strength | 12. Alternate stair touching | 17. Compensatory stepping correction, backward | 24. Walk with pivot turns | ||
| 5. Sit on floor and stand up | 13. Standing arm raise | 18. Compensatory stepping correction, lateral | 25. Step over obstacles | ||
| 26. Timed “Get Up & Go” Test | |||||
| 27. Timed “Get Up & Go” Test with dual task |
CoM=center of mass, ROM=range of motion, CTSIB=Clinical Test of Sensory Integration for Balance, EO=eyes open, EC=eyes closed.
Table 5.
Mini Balance Evaluation Systems Test (Mini BESTest).
| Anticipatory Postural Adjustments | Postural Responses | Sensory Orientation | Dynamic Gait |
|---|---|---|---|
| 1. Sit to stand | 4. Compensatory stepping correction, forward | 7. Stance on firm surface, EO | 11. Change in gait speed |
| 2.Rise to toes | 5. Compensatory stepping correction, backward | 9. Stance on foam, EC | 12. Walk with head turns, horizontal |
| 3. Stand on one leg (left and right) | 6. Compensatory stepping correction, lateral (left and right) | 10. Incline, EC | 13. Walk with pivot turns |
| 12. Step over obstacles | |||
| 14. Cognitive Get up and Go |
EO= Eyes Open; EC= Eyes Closed.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



