
Submitted:
09 April 2024
Posted:
10 April 2024
You are already at the latest version
Abstract
Although migraine belongs to the main causes of disability worldwide the mechanisms of its pathogenesis are poorly known, which is among the reasons that this disease is underdiagnosed and undertreated. As migraine diagnosis is based on the subjective assessment of symptoms, there is a need to establish objective markers of its occurrence and severity. Tryptophan (TRP) metabolism has been associated with the pathogenesis of neurological and psychiatric disorders. In the present work, we investigated an association between migraine and the urine concentration of TRP and its metabolites 5-hydroxyindoleacetic acid (5-HIAA), kynurenine (KYN), kynurenic acid (KYNA) and quinolinic acid (QA) in 21 low-frequency episodic migraine patients and 32 controls. Migraine patients displayed lower urinary levels of 5-HIAA and KYNA, but KYN and QA were enhanced as compared with the controls. Consequently, the patients were characterized by different values of the 5-HIAA/TRP, KYN/TRP, KYNA/KYN, and KYNA/QA ratios. Furthermore, urinary concentration of 5-HIAA was negatively correlated with Migraine Disability Assessment score, monthly migraine, and monthly headache days. A negative correlation between Patient Health Questionnaire 9 scores assessing depression. In conclusion, the urinary 5-HIAA level may be an easy-to-determine marker of migraine occurrence and severity and may contribute to the identification of migraine patients with depression.
Keywords:
migraine
; tryptophan metabolism
; serotonin
; 5-hydroxyindoleacetic acid
; migraine-related anxiety
1. Introduction
Migraine is the fifth (second in young women) cause of disability worldwide, but despite its high prevalence, it is undiagnosed and untreated [1]. This may result from poor knowledge of the mechanisms of migraine pathogenesis, which, in turn, may be a consequence of the restricted availability of the disease target tissue and limited value of animal models of human migraine as they reflect some aspects of the migraine syndrome and not the entire spectrum of symptoms [2]. Therefore, there is still a need for studies to expand current knowledge on the molecular mechanisms of migraine pathogenesis.
Migraine is a complex disease with many symptoms and many factors playing a role in its pathogenesis and these issues have been addressed in several excellent reviews, e.g., [3]. In general, the activation and sensitization of the trigeminal system may be crucial for migraine headache induction (reviewed in [4]).
Tryptophan (TRP) metabolism can be implicated in the pathogenesis of neurological and psychiatric disorders (reviewed in [5]). Tryptophan was reported to be associated with migraine in several studies, but their results are inconsistent as they were performed in different types and phases of migraine (reviewed in [6]). A negative correlation between dietary intake of TRP and migraine risk was observed [7]. However, TRP is a precursor of several biologically active substances that may be responsible for the observed associations of migraine with TRP.
After intake, the majority of TRP is metabolized in the digestive tract in the kynurenine (KYN), serotonin (5-HT), and indole pathways that are competitively initiated by indoleamine 2,3-dioxygenase (IDO-1), TRP hydroxylase and bacterial TRPase (TNA), respectively [8]. 5-Hydroxyindoleacetic acid (5-HIAA) is the main metabolite of serotonin produced by the action of monoamine oxidase and aldehyde dehydrogenase and excreted in the urine [9]. Consequently, 5-HIAA is employed to determine serotonin levels in the body.
The KYN pathway of TRP metabolism gains an emerging role in migraine pathogenesis which is supported by its involvement in the pathogenesis of functional gastrointestinal diseases and the functioning of the gut-brain-microbiota axis [6,10,11,12].
Although most of the ingested TRP is metabolized in the KYN pathway, 5-HT has an established role as a neurotransmitter and consequently is a natural candidate to play a role in migraine pathogenesis. This is supported by the identification of 5-HT as a blood vasoconstrictor, fitting the role of neurovascular incidence in the causative role of the trigeminal system in migraine pathogenesis [13]. Moreover, 5-HT receptors are widely distributed in the brain, including areas that are important in migraine [14]. The agonists of the 5-HT1 serotonin receptor have a long history of anti-migraine drugs [15]. Furthermore, serotonin is the precursor for the synthesis of melatonin in the pineal gland and melatonin may exert beneficial effects in migraine preventive and abortive treatment [16].
In this work, we investigated the urinary levels of TRP and its main metabolites: 5-HIAA, KYN, kynurenic acid (KYNA), and quinolinic acid (QA) in the 5-HT and KYN pathways in migraine patients and controls. Our working hypothesis was that the serotonin pathway of TRP metabolism evaluated by the urinary level of 5-HIAA might play a role in migraine pathogenesis. To verify this hypothesis, we associated some migraine characteristics related to the severity of the disease and its timing with the urinary concentration of 5-HIAA in migraine patients.
Migraine is frequently reported to be associated with mood disorders, symptoms of anxiety, and depression [17,18]. On the other hand, tryptophan metabolism may be implicated in mental health [19]. It was postulated that migraine patients with 3 or more headache days per month should be screened for anxiety symptoms [20]. Therefore, we looked for a correlation between the concentration of TRP metabolites and some indicators of anxiety and depression.
2. Results
2.1. Characteristics of Migraine Patients
All subjects enrolled in this study displayed normal results of routine laboratory tests (results not shown).
All migraine patients suffered from low-frequency episodic migraine and 8 of them experienced aura, mostly visual (Table 1). Non-steroidal anti-inflammatory drugs, triptans (sumatriptan, zolmitriptan, or almotriptan), and a gepant (rimegepant) were used as abortive drugs. Botulinum neurotoxin type A (BoNT/A) and monoclonal antibodies to calcitonin gene-related peptide (CGRP): erenumab, fremanezumab, and galkanezumab were administrated in the preventive treatment. Most of the patients showed mild syndromes of mood disorders, anxiety, and depression.
2.2. Tryptophan and Its Metabolites in Migraine Patients and Controls
Figure 1 presents the results of the determination of the urinary levels of TRP and products of its metabolism in migraine patients and controls. There were no differences between the urine levels of TRP in migraine patients and controls. Migraine patients had a lower level of 5-HIAA and KYNA than controls (p < 0.01 and p < 0.05, respectively), but they had higher levels of KYN and QA than controls (p < 0.05 and p < 0.001, respectively). The first interpretation of these results would be that migraine may be associated with a bias of tryptophan metabolism towards the kynurenine pathway, but such an immediate conclusion is not directly supported by a decrease in KYNA level.
To explore further changes in TRP metabolism associated with migraine, some ratios of the concentrations of the metabolites were analyzed (Figure 2).
The 5-HIAA/TRP ratio was higher in migraine patients group than controls. That ratio indicates the activity of the indoleamine 2,3-dioxygenase (IDO), playing a major role in the control of the kynurenine pathway of degradative TRP metabolism and therefore can be considered as a measure of the ratio of the TRP metabolism in the kynurenine pathway [21]. This was confirmed by an increased KYN/TRP ratio in migraine patients. The median of the KYN/KYNA ratio in the control individuals was about 6, but the median for migraine patients was lower by about half. These results suggest that KYNA was further metabolized in both groups.
2.3. Associations of Migraine Severity and Timing with Tryptophan Metabolites
We looked for a correlation between the clinical characteristics of migraine and parameters of TRP metabolism in migraine patients group. First, we analyzed the correlation between the scor es of the MIDAS (Migraine Disability Assessment Scale) questionnaire and the urinary levels of TRP, 5-HIAA, KYN, KYNA, and QA as well as some of their ratios (Table 2).
The analysis of the MIDAS score with TRP, its metabolites, and their ratios showed a negative correlation between 5-HIAA and the 5-HIAA/TRP ratio.
To visualize an interindividual variability of the correlated parameters we presented them along with a line adjusted by linear regression (Figure 3). Linear regression does not fit the data well, especially in the case of 5-HIAA. However, adjustments with nonlinear regression did not produce significantly better fits (data not shown).
Next, we looked for a correlation between number of migraine days per month (MMD) and tryptophan metabolism (Table 3).
Similarly to MIDAS, MMD was negatively correlated with the urinary concentration of 5-HIAA and the 5-HIAA/TRP ratio. To visualize these correlations, we presented the variability of the data along with the corresponding regression lines (Figure 4).
Figure 4 shows a high interindividual variability of data and linear regression does not model well the dependence between variables. Moreover, there was not a functional relationship between MMD and 5-HIAA or 5-HIAA/TRP ratio as some single values of the former corresponded to more than one value of the latter. This problem will be presented in the Discussion section.
Next, we checked a correlation between the number of monthly headache days (MHD) and TRP metabolism (Table 4).
The number of headaches per month was correlated only with the urinary 5-HIAA concentration in migraine patients.
Figure 5 presents interindividual variability of MHD and urinary levels of 5-HIAA along with a regression line. In general, data displayed a decreasing tendency up to 10 MHD and an abrupt increase in urinary 5-HIAA concentration at 13 MHD may be occasional.
Other parameters characterizing migraine: pain intensity evaluated by numeric rating scale (NRS), the number of headache attacks per month or quarter, duration of migraine, occurrence of aura, number of attacks per month, the use of gepants, triptans, onabotulinumtoxinA and non-steroidal anti-inflammatory drugs in the abortive treatment and the use of anti-VEGF drugs, and other drugs in preventive treatment were not correlated with TRP metabolism.
2.4. Association of Anxiety/Depression with Tryptophan Metabolites in Migraine Patients
As most of the migraine patients enrolled in this study showed mild symptoms of anxiety and depression, the next clinical characteristic we looked for a correlation with TRP metabolism was the Patient Health Questionnaire 9 (PHQ-9) score (Table 5). The PHQ-9 scale is a nine-item test that assesses the occurrence and severity of depression during the last two weeks before investigation [22].
We observed a negative correlation between PHQ-9 scores and urine concentration of 5-HIAA. We visualized the obtained results by a plot presenting the interindividual distribution of PHQ-9 scores and urinary 5-HIAA concentration (Figure 6)
That significant correlation between PHQ-9 and 5-HIAA prompted us to search for a correlation between Generalized Anxiety Disorder 7-item (GAD-7) scores and TRP metabolites, but we did not observe any significant association between them (data not shown). To continue exploring the idea of association of mood disorders/depression in migraine patients, we looked for a correlation between all characteristics of migraine we explored, i.e. MIDAS score, MMD, MHD, duration of migraine, number of migraine headache attacks per month/quarter, PHQ-9 and GAD with vanillylmandelic acid (VMA), homovanillic acid (HVA) and xanthurenic acid (XA). All these substances can be related to tryptophan metabolism and the functioning of the brain [23,24,25,26]. Moreover, it was shown that 5-HIAA correlated positively with HVA in cerebrospinal fluid of migraine patients [27]. However, calculations did not result in any significant correlation between migraine characteristics and VMA, HVA, or XA (data not shown).
Finally, we looked for a correlation between gastrointestinal symptom score (GIS) and TRP metabolism as we previously suggested that the kynurenine pathway of tryptophan metabolism may play a role in the pathogeneses of migraine and functional gastrointestinal disorders [11]. We did not obtain any correlation between GIS scale scores and tryptophan metabolism (data not shown).
3. Discussion
In the present work, we showed that patients with episodic migraine displayed different urinary levels of the TRP metabolites 5-HIAA, KYN, KYNA, and QA as compared with the controls. Consequently, the patients were characterized by different values of the KYN/TRP, KYNA/KYN, and KYNA/QA ratios. No differences were observed for the urinary levels of TRP and the 5-HIAA/TRP ratio. On the other hand, urinary concentration of 5-HIAA was negatively correlated with MIDAS score, MMD, MHD, and MIDAS score and MMD were also negatively correlated with the 5-HIAA/TRP ratio. Furthermore, a negative correlation of PHQ-9 with urinary 5-HIAA was observed.
The routine diagnosis of migraine is based on the reporting of symptoms by patients asked by a physician and the allocation of their answers on the scale(s) used by the physician. Therefore, such a diagnosis is subjective and so it is difficult to standardize the criteria for migraine diagnosis. Several indicators are postulated to be associated with migraine and so they can support the disease diagnosis. In general, migraine is considered a complex disease with its pathogenesis underlined by the interaction of genetic and environmental factors. Genetic markers are proposed in monogenic migraines, including familial hemiplegic migraine and migraine with aura associated with hereditary small-vessel disorders [28]. Despite significant progress in genome analysis, the association of genetic factors with common migraine is still a big challenge [29]. Moreover, these markers are more useful in migraine therapy than diagnosis. At present, neuroimaging cannot be considered a routine method in common migraine diagnosis and is recommended in migraine with specific, rare symptoms (reviewed in [30]). Therefore, there is a need to establish migraine markers that could support the routine diagnosis of the disease.
In our work, we pointed out a non-invasive, easy-to-determine parameter, 5-HIAA, which correlated with certain characteristics of migraine. Surely, it cannot be considered an independent marker of migraine, but its informative potential may be high as this TRP metabolite is excreted with urine. Our results suggest that 5-HIAA is strongly associated with migraine as it was correlated, either singly or in combination with TRP with several migraine attributes, including MIDAS score MMD, MHD, and additionally with PHQ-9 scores.
Other studies associating migraine with 5-HIAA produced various results. However, we have not found any recent study on this subject. 5-HIAA is a representative of 5-hydroxyindoles (5-HIs), which were reported to fall during headache attacks in the blood of 17 out of 20 migraine patients [31]. However, another study performed on 14 migraine patients showed that urine concentrations of 5-HT and 5-HIAA fluctuated during and after migraine attacks [32]. The results of 5-HIAA variation were confirmed in a subsequent study performed in cerebrospinal fluid [33]. However, a 1976 study showed a significant increase in urine excretion of 5-HIAA during the early headache stage and the lack of correlation between some migraine characteristics and the levels of 5-HIAA in cerebrospinal fluids of migraine patients and a positive correlation with others [27]. A study with 9 migraine patients and 4 controls did not show any significant changes in the urine 5-HIAA in migraine patients relative to control individuals [34]. It was shown that migraine patients displayed lower plasma 5-HT and higher 5-HIAA levels than controls and patients with tension headaches [35]. However, during migraine attacks, plasma 5-HIAA concentrations were lower than in controls. A study performed on 8 migraine patients and 10 tension-type headache sufferers showed significantly decreased levels of 5-HIAA in the urine of both groups as compared with controls [36]. Another study showed increased concentrations of serum 5-HIAA between attacks of migraine with aura and at the beginning of attacks of both migraine with and without aura [37]. Urinary level of 5-HIAA was observed not to change in young men but it decreased in female migraine patients when compared with their sex-matched controls [38]. No association was observed between 5-HIAA excretion and the characteristics of migraine. In summary, there are few studies investigating the urine level of 5-HIAA in migraine patients and the results of these studies are inconsistent and the most likely reasons for this inconsistency may be fluctuations of 5-HIAA levels during the disease course of different types of migraine and weak statistical power of those studies.
We observed a high interindividual variability among migraine patients in their responses to questions of questionnaires and no functional dependence was observed between scores following the answers and the levels of 5-HIAA, i.e., a single 5-HIAA concentration was measured in a few patients, but they differently responded to the questionnaire questions. This was especially striking when a regression line was drawn along with individual results. This underlines a need for more objective criteria for migraine characteristics.
Migraine is frequently associated with symptoms of anxiety and/or depression (reviewed in [39,40]). This association is reported as bidirectional, i.e., migraine headaches may increase the risk of anxiety/depression and vice versa [41,42]. Therefore, there is a need to identify these migraine patients who require special psychiatric care. Our study showed that PHQ-9 scores were correlated with urinary 5-HIAA levels and therefore its determination may help to identify such patients. However, our results based on a single self-reported questionnaire cannot determine any role of 5-HIAA in migraine-associated mental disorders as it would require performing special psychological examinations by specialized personnel. However, several studies showed fluctuations in 5-HIAA levels in neurological and psychiatric disorders (reviewed in [43]). Therefore, the result we obtained may be considered a small contribution to the link between migraine and mental disorders suggesting that TRP metabolism in general, and 5-HIAA in particular, may contribute to the mechanism underlying that association. However, it is not justified to widely discuss our results in a comparison with other studies performed with specialized methods.
In our previous works, we considered tryptophan metabolism in the context of the gut-brain-microbiota axis [44,45,46,47]. However, those studies were performed on hospital patients, but this study enrolled patients of an outpatient clinic and most of them were not willing to donate blood or undergo the examination of the gut and the microbiota.
The two most important limitations of our study are the small number of enrolled individuals and the lack of standardization of TRP intake. The small number of individuals in our study resulted in a moderate statistical power of the tests we employed to analyze our data. However, we employed the resampling bootstrap technique to lower the chance of accepting a false hypothesis. We want to underline that many studies we cited in our discussion, published in highly impacted journals, enrolled even fewer patients than we did. Moreover, it could be considered that the determination of the sample size before research may not be the best solution, as it depends on the test that is to be used, which, in turn, depends on the distribution of data. We could not increase the number of patients due to limited financial and human resources, but the number of individuals in our cohort was in the typical range for 5’-HIAA/headache/migraine studies published so far.We did not interfere with the diet of enrolled individuals, but we did not observe any difference between the urine concentration of TRP in the patients and the control groups and also the 5’-HIAA/TRP ratio was the same in both groups. Another limitation of our study is not to measure the level of 3-hydroxykynurenine, a product of the KYN pathway of TRP metabolism, especially since this molecule is reported to exert a dual, pro- or anti-oxidative action in the central nervous system [48]. Moreover, increased conversion of TRP to KYN with a decrease of KYNA/QA ratio suggests that the level of 3-hydroxykynurenine might change [49].
Although we did not observe changes in the KYN, KYNA, and QA levels, we cannot exclude alterations in the kynurenine pathway of TRP metabolism in our patients, as we did not measure the level of all metabolites of that pathway. In particular, 3-hydroxykynurenine levels were not measured. More evidence on the role of the KYN pathway of TRP metabolism in migraine and headaches can be found in other works, e.g., [50,51,52,53].
Although our study was conducted in the interictal phase of migraine, there is emerging evidence that symptoms associated with the headache phase may persist between migraine attacks [54]. These symptoms include allodynia, hypersensitivity, photophobia, phonophobia, osmophobia, visual/vestibular disturbances, and motion sickness. Therefore, the interictal phase of migraine should be further investigated to identify all migraine-related factors that may lower the quality of patients life.
In summary, the urinary concentration of 5-HIAA may be considered a marker of episodic migraine in the interictal period and may serve to identify these migraine patients who are at increased risk of migraine-associated mental disorders.
4. Materials and Methods
4.1. Patients and Ethics
A total of 21 patients with migraine and 32 age- and gender-matched migraine-free individuals (controls) were enrolled in this study and everyone signed an informed consent to participate in this study. The participants were recruited from patients of the Department of Developmental Neurology and Epileptology, Polish Mother’s Memorial Hospital Research Institute in Lodz, and the Department of Neurology and Neurology Outpatient Clinic of the Regional County Hospital in Sieradz, Poland. The study was approved by the Bioethical Committee of Polish Mother Memorial Hospital Research Institute, Lodz, Poland (permit no. 51/2020) and the Bioethical Committee of Medical University of Lodz, Lodz, Poland (permit no. RNN/176/18/KE).
4.2. Diagnosis
Migraine was diagnosed according to the criteria of the International Classification of Headache Disorders 3-beta (ICHD-3 beta) [21]. Only patients with episodic migraine cases were included in this study. The exclusion criteria for both groups included organic diseases of the central or peripheral nervous system, any form of functional neurological disorder, except for episodic migraine as per inclusion criteria for the patient group, advanced and/or decompensated, eventually exacerbated comorbidities, genetic diseases, mental disorders and diseases, congenital physical and/or intellectual disability, a history of significant multiple traumas.
Mood disorder was assessed with a non-standard questionnaire based on the self-reported presence of 5 out of the 8 symptoms of sad mood, - hipo- or insomnia, feelings of guilt, decreased energy levels, decreased concentration, decreased appetite, decrease in pleasurable activities (anhedonia), and increased or decreased psychomotor activity [55]. Also, GAD-7, Generalized Anxiety Disorder 7-item and PHQ-9, Patient Health Questionnaire 9, were used to assess patients’ mental health.
The characteristics of migraine patients, including the disease duration, aura, frequency of attacks, treatment, and others were presented in Table 1.
4.3. Determination of TRP Metabolites
All patients were informed to adhere to the dietary recommendations before donating urine samples, including refraining from eating fish and seafood 48 hrs. and other tryptophan-rich foods 24 h before urine donation. Fasting urine samples for the analysis of TRP metabolites were collected into containers with a solution of 0.1% hydrochloric acid as a stabilizer. The urine samples were taken in the interictal period 10-30 days after the last migraine attack, which corresponded to the last administration of headache abortive drugs. L-tryptophan and its following metabolites: 5-HIAA, KYN, KYNA, and QA were determined in urine with liquid chromatography–tandem mass spectrometry (LC–MS/MS—Ganzimmun Diagnostics AG, Mainz, Germany; D-ML-13147–01-01) as described elsewhere [56] with some modifications [57]. The concentration of TRP and its metabolites were expressed in mg/g creatinine (mg/gCr). The concentration ratios 5-HIAA/TRP, KYN/TRP, KYNA/KYN, and KYNA/QA were calculated and presented in plots.
4.4. Data Analysis
Shapiro-Wilk W test was used to check the normality of data distribution for each measured parameter in the control and patient groups. If both controls and patients followed a normal distribution, the unpaired Student t-test was used to assess the significance of differences between groups, otherwise Mann-Whitney U test was used. The statistical power of the tests with a given sample size was calculated with G*Power software [58]. Using that software, we calculated that the power of our studies ranged from 0.72 to 0.82 for a given sample size of 21 for migraine patients and 32 for controls with a significance level (alpha) of 0.05. To decrease the chance that the differences we observed resulted from pure chance, we employed the resampling bootstrap technique (10,000 iterations). The correlation between concentrations of TRP and its metabolites and characteristics of migraine were analyzed by Spearman’s rank test. All analyses were performed with STATISTICA 13.3 software (TIBCO Software INC., Palo Alto, CA, USA) and Resampling Stats Add-In for Excel v.4 (The Institute for Statistics Education, An Elder Research Company, Arlington, VA, USA).
Author Contributions
Conceptualization, J.B., J.C. and MF.; methodology, C.C., M.D., and E.P.; software, J.B.; validation, X.X., Y.Y. and Z.Z.; formal analysis, J.B.; investigation, M.F., C.C., J.C, M.D., and E.P.; writing—original draft preparation, J.B.; writing—review and editing, J.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted by the Declaration of Helsinki, and approved by the Bioethical Committee of Polish Mother Memorial Hospital Research Institute, Lodz, Poland (permit no. 51/2020) and the Bioethical Committee of Medical University of Lodz, Lodz, Poland (permit no. RNN/176/18/KE).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Anonymized data may be obtained from the corresponding author upon a reasonable request.
Acknowledgments
The authors thank the lab technicians from ALAB Laboratories for participating in diagnostic procedures.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Eigenbrodt, A.K.; Ashina, H.; Khan, S.; Diener, H.C.; Mitsikostas, D.D.; Sinclair, A.J.; Pozo-Rosich, P.; Martelletti, P.; Ducros, A.; Lantéri-Minet, M.; et al. Diagnosis and management of migraine in ten steps. Nat Rev Neurol 2021, 17, 501–514. [Google Scholar] [CrossRef]
- Demartini, C.; Greco, R.; Francavilla, M.; Zanaboni, A.M.; Tassorelli, C. Modelling migraine-related features in the nitroglycerin animal model: Trigeminal hyperalgesia is associated with affective status and motor behavior. Physiology & Behavior 2022, 256, 113956. [Google Scholar] [CrossRef]
- Ferrari, M.D.; Goadsby, P.J.; Burstein, R.; Kurth, T.; Ayata, C.; Charles, A.; Ashina, M.; van den Maagdenberg, A.M.J.M.; Dodick, D.W. Migraine. Nature Reviews Disease Primers 2022, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Ashina, M.; Hansen, J.M.; Do, T.P.; Melo-Carrillo, A.; Burstein, R.; Moskowitz, M.A. Migraine and the trigeminovascular system-40 years and counting. Lancet Neurol 2019, 18, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Yu, S.; Long, Y.; Shi, A.; Deng, J.; Ma, Y.; Wen, J.; Li, X.; Liu, S.; Zhang, Y.; et al. Tryptophan metabolism: Mechanism-oriented therapy for neurological and psychiatric disorders. Front Immunol 2022, 13, 985378. [Google Scholar] [CrossRef] [PubMed]
- Körtési, T.; Spekker, E.; Vécsei, L. Exploring the Tryptophan Metabolic Pathways in Migraine-Related Mechanisms. Cells 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Razeghi Jahromi, S.; Togha, M.; Ghorbani, Z.; Hekmatdoost, A.; Khorsha, F.; Rafiee, P.; Shirani, P.; Nourmohammadi, M.; Ansari, H. The association between dietary tryptophan intake and migraine. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology 2019, 40, 2349–2355. [Google Scholar] [CrossRef] [PubMed]
- Xue, C.; Li, G.; Zheng, Q.; Gu, X.; Shi, Q.; Su, Y.; Chu, Q.; Yuan, X.; Bao, Z.; Lu, J.; et al. Tryptophan metabolism in health and disease. Cell Metab 2023, 35, 1304–1326. [Google Scholar] [CrossRef] [PubMed]
- Lenchner, J.R.; Santos, C. Biochemistry, 5 Hydroxyindoleacetic Acid. In StatPearls; StatPearls PublishingCopyright © 2024, StatPearls Publishing LLC.: Treasure Island (FL), 2024.
- Fila, M.; Chojnacki, C.; Chojnacki, J.; Blasiak, J. The kynurenine pathway of tryptophan metabolism in abdominal migraine in children - A therapeutic potential? Eur J Paediatr Neurol 2023, 48, 1–12. [Google Scholar] [CrossRef]
- Fila, M.; Chojnacki, J.; Pawlowska, E.; Szczepanska, J.; Chojnacki, C.; Blasiak, J. Kynurenine Pathway of Tryptophan Metabolism in Migraine and Functional Gastrointestinal Disorders. International journal of molecular sciences 2021, 22. [Google Scholar] [CrossRef]
- Spekker, E.; Nagy-Grócz, G.; Vécsei, L. Ion Channel Disturbances in Migraine Headache: Exploring the Potential Role of the Kynurenine System in the Context of the Trigeminovascular System. International journal of molecular sciences 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Villalón, C.M.; VanDenBrink, A.M. The Role of 5-Hydroxytryptamine in the Pathophysiology of Migraine and its Relevance to the Design of Novel Treatments. Mini Rev Med Chem 2017, 17, 928–938. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Altamirano, J.L.; Olmos-Hernandez, A.; Jaime, H.B.; Carrillo-Mora, P.; Bandala, C.; Reyes-Long, S.; Alfaro-Rodríguez, A. Review: 5-HT1, 5-HT2, 5-HT3 and 5-HT7 Receptors and their Role in the Modulation of Pain Response in the Central Nervous System. Curr Neuropharmacol 2018, 16, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Török, N.; Vécsei, L. Are 5-HT(1) receptor agonists effective anti-migraine drugs? Expert Opin Pharmacother 2021, 22, 1221–1225. [Google Scholar] [CrossRef] [PubMed]
- Andre Leite, G.; Adriana Martini, F.; Reinaldo Teixeira, R.; Eliova, Z.; José, C.-N.; Mario Fernando Prieto, P. Randomised clinical trial comparing melatonin 3 mg, amitriptyline 25 mg and placebo for migraine prevention. Journal of Neurology, Neurosurgery & Psychiatry 2016, 87, 1127. [Google Scholar] [CrossRef]
- Duan, S.; Ren, Z.; Xia, H.; Wang, Z.; Zheng, T.; Li, G.; Liu, L.; Liu, Z. Associations between anxiety, depression with migraine, and migraine-related burdens. Front Neurol 2023, 14, 1090878. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.F.P.; Mercante, J.P.P.; Tobo, P.R.; Kamei, H.; Bigal, M.E. Anxiety and depression symptoms and migraine: a symptom-based approach research. J Headache Pain 2017, 18, 37. [Google Scholar] [CrossRef] [PubMed]
- Cervenka, I.; Agudelo, L.Z.; Ruas, J.L. Kynurenines: Tryptophan’s metabolites in exercise, inflammation, and mental health. Science (New York, N.Y.) 2017, 357. [Google Scholar] [CrossRef] [PubMed]
- Irimia, P.; Garrido-Cumbrera, M.; Santos-Lasaosa, S.; Aguirre-Vazquez, M.; Correa-Fernández, J.; Colomina, I.; Pozo-Rosich, P. Impact of monthly headache days on anxiety, depression and disability in migraine patients: results from the Spanish Atlas. Scientific reports 2021, 11, 8286. [Google Scholar] [CrossRef]
- The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia : an international journal of headache 2013, 33, 629–808. [CrossRef]
- Al Ghadeer, H.A.; Al Salman, S.A.; Alshakhs, Z.M.; Alghanim, J.H.; Alneamah, A.A.; Almazyadi, H.S.; Alalawi, H.H.; AlHassan, M.I.; Alsuwailem, B.S.; Albonasser, A.A.; et al. Migraine Headache and the Risk of Depression. Cureus 2022, 14, e31081. [Google Scholar] [CrossRef] [PubMed]
- Andreou, D.; Saetre, P.; Werge, T.; Andreassen, O.A.; Agartz, I.; Sedvall, G.C.; Hall, H.; Terenius, L.; Jönsson, E.G. Tryptophan hydroxylase gene 1 (TPH1) variants associated with cerebrospinal fluid 5-hydroxyindole acetic acid and homovanillic acid concentrations in healthy volunteers. Psychiatry Res 2010, 180, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Bonifačić, D.; Aralica, M.; Sotošek Tokmadžić, V.; Rački, V.; Tuškan-Mohar, L.; Kučić, N. Values of vanillylmandelic acid and homovanillic acid in the urine as potential prognostic biomarkers in ischaemic stroke patients. Biomarkers 2017, 22, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, S.I.; Schapiro, M.B.; May, C. Reduced Brain Delivery of Homovanillic Acid to Cerebrospinal Fluid During Human Aging. Archives of Neurology 2004, 61, 1721–1724. [Google Scholar] [CrossRef] [PubMed]
- Sathyasaikumar, K.V.; Tararina, M.; Wu, H.Q.; Neale, S.A.; Weisz, F.; Salt, T.E.; Schwarcz, R. Xanthurenic Acid Formation from 3-Hydroxykynurenine in the Mammalian Brain: Neurochemical Characterization and Physiological Effects. Neuroscience 2017, 367, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Kangasniemi, P.J. Changes in serotonin metabolism during migraine attacks. Monogr Neural Sci 1976, 3, 60–66. [Google Scholar] [CrossRef]
- Grangeon, L.; Lange, K.S.; Waliszewska-Prosół, M.; Onan, D.; Marschollek, K.; Wiels, W.; Mikulenka, P.; Farham, F.; Gollion, C.; Ducros, A.; et al. Genetics of migraine: where are we now? The Journal of Headache and Pain 2023, 24, 12. [Google Scholar] [CrossRef]
- Cader, M.Z. The genetics of migraine and the path to precision medicine. Prog Brain Res 2020, 255, 403–418. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.W.; Burch, R.C.; Frishberg, B.M.; Marmura, M.J.; Mechtler, L.L.; Silberstein, S.D.; Turner, D.P. Neuroimaging for Migraine: The American Headache Society Systematic Review and Evidence-Based Guideline. Headache 2020, 60, 318–336. [Google Scholar] [CrossRef]
- Berstad, J.R. Total 5-hydroxyindoles in blood related to migraine attacks. Acta Neurol Scand 1976, 54, 293–300. [Google Scholar] [CrossRef]
- Deanović, Z.; Iskrić, S.; Dupelj, M. Fluctuation of 5-hydroxy-indole compounds in the urine of migrainous patients. Biomedicine 1975, 23, 346–349. [Google Scholar] [PubMed]
- Hyypp, M.T.; Kangasniemi, P. Variation of plasma free tryptophan and CSF 5-HIAA during migraine. Headache 1977, 17, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Curzon, G.; Theaker, P.; Phillips, B. Excretion of 5-hydroxyindolyl acetic acid (5HIAA) in migraine. J Neurol Neurosurg Psychiatry 1966, 29, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.D.; Odink, J.; Tapparelli, C.; Van Kempen, G.M.; Pennings, E.J.; Bruyn, G.W. Serotonin metabolism in migraine. Neurology 1989, 39, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Milovanović, D.D.; Majkić-Sing, N.; Mirković, D.; Pavlović, J. Plasma and urinary serotonin and 5-hydroxyindol-3-acetic acid in adults with migraine and tension-type headache. Advances in experimental medicine and biology 1999, 467, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.A.; Cotrim, M.D.; Morgadinho, M.T.; Ramos, M.I.; Santos, E.S.; de Macedo Tdos, R. Migraine, serum serotonin and platelet 5-HT2 receptors. Cephalalgia : an international journal of headache 1990, 10, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Bousser, M.G.; Elghozi, J.L.; Laude, D.; Soisson, T. Urinary 5-HIAA in migraine: evidence of lowered excretion in young adult females. Cephalalgia: an international journal of headache 1986, 6, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Antonaci, F.; Nappi, G.; Galli, F.; Manzoni, G.C.; Calabresi, P.; Costa, A. Migraine and psychiatric comorbidity: a review of clinical findings. J Headache Pain 2011, 12, 115–125. [Google Scholar] [CrossRef]
- Dresler, T.; Caratozzolo, S.; Guldolf, K.; Huhn, J.I.; Loiacono, C.; Niiberg-Pikksööt, T.; Puma, M.; Sforza, G.; Tobia, A.; Ornello, R.; et al. Understanding the nature of psychiatric comorbidity in migraine: a systematic review focused on interactions and treatment implications. J Headache Pain 2019, 20, 51. [Google Scholar] [CrossRef]
- Hommer, R.; Lateef, T.; He, J.P.; Merikangas, K. Headache and mental disorders in a nationally representative sample of American youth. Eur Child Adolesc Psychiatry 2022, 31, 39–49. [Google Scholar] [CrossRef]
- Kim, B.S.; Chung, P.W.; Kim, B.K.; Lee, M.J.; Park, J.W.; Chu, M.K.; Ahn, J.Y.; Bae, D.W.; Song, T.J.; Sohn, J.H.; et al. The impact of remission and coexisting migraine on anxiety and depression in cluster headache. J Headache Pain 2020, 21, 58. [Google Scholar] [CrossRef] [PubMed]
- Jayamohananan, H.; Manoj Kumar, M.K. T, P.A. 5-HIAA as a potential biological marker for neurological and psychiatric disorders. Adv Pharm Bull 2019, 9, 374–381. [Google Scholar] [CrossRef]
- Chojnacki, C.; Gąsiorowska, A.; Popławski, T.; Błońska, A.; Konrad, P.; Zajdler, R.; Chojnacki, J.; Blasiak, J. Reduced Intake of Dietary Tryptophan Improves Beneficial Action of Budesonide in Patients with Lymphocytic Colitis and Mood Disorders. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Chojnacki, C.; Popławski, T.; Chojnacki, J.; Fila, M.; Konrad, P.; Blasiak, J. Tryptophan Intake and Metabolism in Older Adults with Mood Disorders. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Chojnacki, C.; Popławski, T.; Konrad, P.; Fila, M.; Błasiak, J.; Chojnacki, J. Antimicrobial treatment improves tryptophan metabolism and mood of patients with small intestinal bacterial overgrowth. Nutr Metab (Lond) 2022, 19, 66. [Google Scholar] [CrossRef] [PubMed]
- Chojnacki, C.; Popławski, T.; Konrad, P.; Fila, M.; Chojnacki, J.; Błasiak, J. Serotonin Pathway of Tryptophan Metabolism in Small Intestinal Bacterial Overgrowth-A Pilot Study with Patients Diagnosed with Lactulose Hydrogen Breath Test and Treated with Rifaximin. Journal of clinical medicine 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Colín-González, A.L.; Maldonado, P.D.; Santamaría, A. 3-Hydroxykynurenine: An intriguing molecule exerting dual actions in the Central Nervous System. NeuroToxicology 2013, 34, 189–204. [Google Scholar] [CrossRef]
- Fathi, M.; Vakili, K.; Yaghoobpoor, S.; Tavasol, A.; Jazi, K.; Hajibeygi, R.; Shool, S.; Sodeifian, F.; Klegeris, A.; McElhinney, A.; et al. Dynamic changes in metabolites of the kynurenine pathway in Alzheimer’s disease, Parkinson’s disease, and Huntington’s disease: A systematic Review and meta-analysis. Front Immunol 2022, 13, 997240. [Google Scholar] [CrossRef]
- Curto, M.; Lionetto, L.; Negro, A.; Capi, M.; Perugino, F.; Fazio, F.; Giamberardino, M.A.; Simmaco, M.; Nicoletti, F.; Martelletti, P. Altered serum levels of kynurenine metabolites in patients affected by cluster headache. J Headache Pain 2015, 17, 27. [Google Scholar] [CrossRef] [PubMed]
- Fila, M.; Chojnacki, C.; Chojnacki, J.; Blasiak, J. The kynurenine pathway of tryptophan metabolism in abdominal migraine in children - A therapeutic potential? Eur J Paediatr Neurol 2024, 48, 1–12. [Google Scholar] [CrossRef]
- Fila, M.; Chojnacki, J.; Pawlowska, E.; Szczepanska, J.; Chojnacki, C.; Blasiak, J. Kynurenine Pathway of Tryptophan Metabolism in Migraine and Functional Gastrointestinal Disorders. International journal of molecular sciences 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Tuka, B.; Nyári, A.; Cseh, E.K.; Körtési, T.; Veréb, D.; Tömösi, F.; Kecskeméti, G.; Janáky, T.; Tajti, J.; Vécsei, L. Clinical relevance of depressed kynurenine pathway in episodic migraine patients: potential prognostic markers in the peripheral plasma during the interictal period. J Headache Pain 2021, 22, 60. [Google Scholar] [CrossRef] [PubMed]
- Vincent, M.; Viktrup, L.; Nicholson, R.A.; Ossipov, M.H.; Vargas, B.B. The not so hidden impact of interictal burden in migraine: A narrative review. Front Neurol 2022, 13, 1032103. [Google Scholar] [CrossRef] [PubMed]
- Sekhon, S.; Gupta, V. Mood Disorder. In StatPearls; StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.: Treasure Island (FL), 2024.
- Zhu, W.; Stevens, A.P.; Dettmer, K.; Gottfried, E.; Hoves, S.; Kreutz, M.; Holler, E.; Canelas, A.B.; Kema, I.; Oefner, P.J. Quantitative profiling of tryptophan metabolites in serum, urine, and cell culture supernatants by liquid chromatography-tandem mass spectrometry. Anal Bioanal Chem 2011, 401, 3249–3261. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.H.; Yoo, D.; Ahn, T.B.; Lee, W.; Hong, J. Profiling Analysis of Tryptophan Metabolites in the Urine of Patients with Parkinson’s Disease Using LC-MS/MS. Pharmaceuticals (Basel) 2023, 16. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*power 3.1: Tests for correlation and regression analyses. Behav Res Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
Figure 1.
Tryptophan (TRP) and its main metabolites in migraine patients and controls. Urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), kynurenic acid (KYNA), and quinolinic acid (QA) were expressed in milligrams per gram of creatinine (mg/gCr). The results are presented as median with boxes representing I and III quartiles and whiskers representing Min to Max values. Differences between migraine patients and controls were analyzed by U Mann–Whitney test; n = 21 in migraine patients group and n = 32 in controls; *—p < 0.05; **—p < 0.01; ***—p < 0.001 as compared with controls.
Figure 1.
Tryptophan (TRP) and its main metabolites in migraine patients and controls. Urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), kynurenic acid (KYNA), and quinolinic acid (QA) were expressed in milligrams per gram of creatinine (mg/gCr). The results are presented as median with boxes representing I and III quartiles and whiskers representing Min to Max values. Differences between migraine patients and controls were analyzed by U Mann–Whitney test; n = 21 in migraine patients group and n = 32 in controls; *—p < 0.05; **—p < 0.01; ***—p < 0.001 as compared with controls.
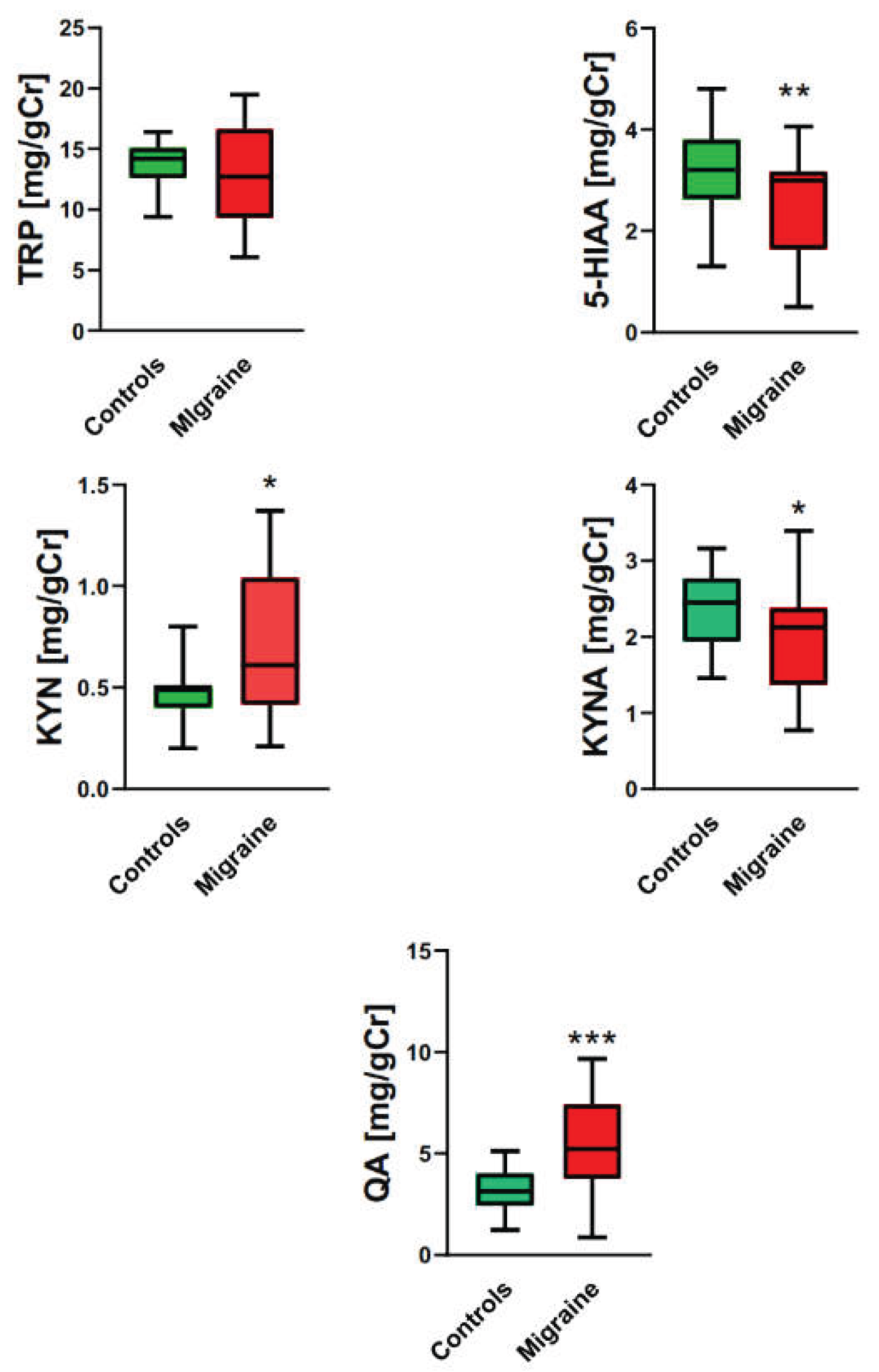
Figure 2.
Ratios of urinary levels of 5-hydroxyaminoacetic acid (5-HIAA) and kynurenine (KYN) to tryptophan (TRP), KYN to kynurenic acid (KYNA), and KYNA to quinolinic acid (QA) in migraine patients and controls. Results are presented as the median with boxes representing I and III quartiles and whiskers representing Min to Max values. Differences between migraine patients and controls were analyzed by U Mann–Whitney test; n = 21 in migraine patients group and n = 32 in controls; ***—p < 0.001 as compared with controls.
Figure 2.
Ratios of urinary levels of 5-hydroxyaminoacetic acid (5-HIAA) and kynurenine (KYN) to tryptophan (TRP), KYN to kynurenic acid (KYNA), and KYNA to quinolinic acid (QA) in migraine patients and controls. Results are presented as the median with boxes representing I and III quartiles and whiskers representing Min to Max values. Differences between migraine patients and controls were analyzed by U Mann–Whitney test; n = 21 in migraine patients group and n = 32 in controls; ***—p < 0.001 as compared with controls.
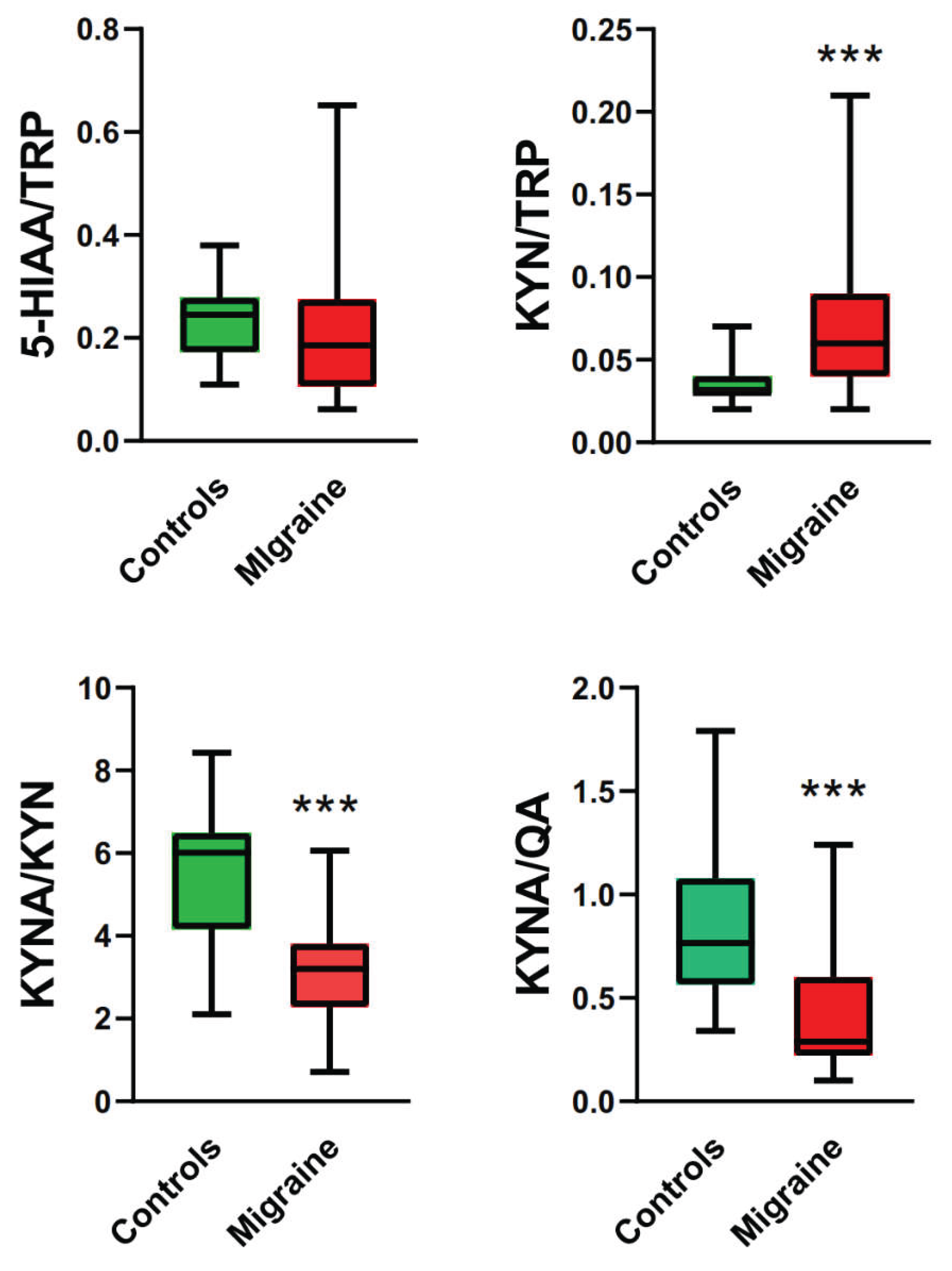
Figure 3.
Correlation between the severity of migraine evaluated by Migraine Disability Assessment Scale (MIDAS) score and urine concentration of 5- hydroxyaminoacetic acid (5-HIAA) measured in mg per g of creatinine (gCr) (upper panel) or the ratio of 5-HIAA to tryptophan (TRP) (lower panel) in migraine patients. The correlation was assessed by the Spearman rank test with the rho rank coefficient (r). A linear regression line was drawn by the least square method with the equations Y = –0.126X + 4.150 (R2 = 0.312, upper panel) and Y = –0.012X + 0.390 (R2 = 0.226, lower panel). .
Figure 3.
Correlation between the severity of migraine evaluated by Migraine Disability Assessment Scale (MIDAS) score and urine concentration of 5- hydroxyaminoacetic acid (5-HIAA) measured in mg per g of creatinine (gCr) (upper panel) or the ratio of 5-HIAA to tryptophan (TRP) (lower panel) in migraine patients. The correlation was assessed by the Spearman rank test with the rho rank coefficient (r). A linear regression line was drawn by the least square method with the equations Y = –0.126X + 4.150 (R2 = 0.312, upper panel) and Y = –0.012X + 0.390 (R2 = 0.226, lower panel). .
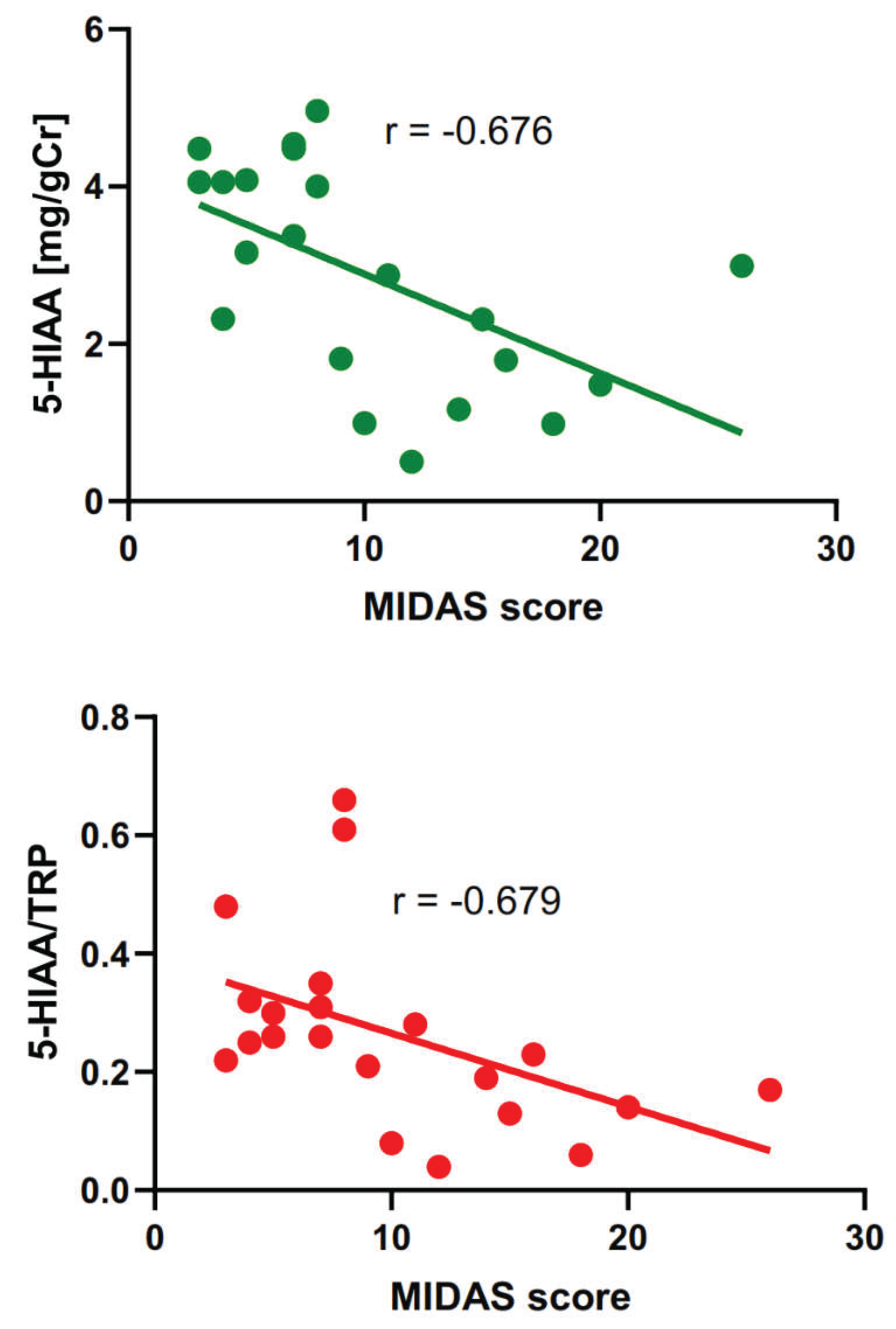
Figure 4.
Correlation between monthly migraine days (MMD) and urine concentration of 5- hydroxyaminoacetic acid (5-HIAA) measured in mg per g of creatinine (gCr) (upper panel) or the ratio of 5-HIAA to tryptophan (TRP) (lower panel) in migraine patients. The correlation was assessed by the Spearman rank test with the rho rank coefficient (r). The linear regression line was drawn by the least square method with the equations Y = –0.283X + 3.780 (R2 = 0.234, upper panel) and Y = –0.032X + 0.365 (R2 = 0.219, lower panel).
Figure 4.
Correlation between monthly migraine days (MMD) and urine concentration of 5- hydroxyaminoacetic acid (5-HIAA) measured in mg per g of creatinine (gCr) (upper panel) or the ratio of 5-HIAA to tryptophan (TRP) (lower panel) in migraine patients. The correlation was assessed by the Spearman rank test with the rho rank coefficient (r). The linear regression line was drawn by the least square method with the equations Y = –0.283X + 3.780 (R2 = 0.234, upper panel) and Y = –0.032X + 0.365 (R2 = 0.219, lower panel).
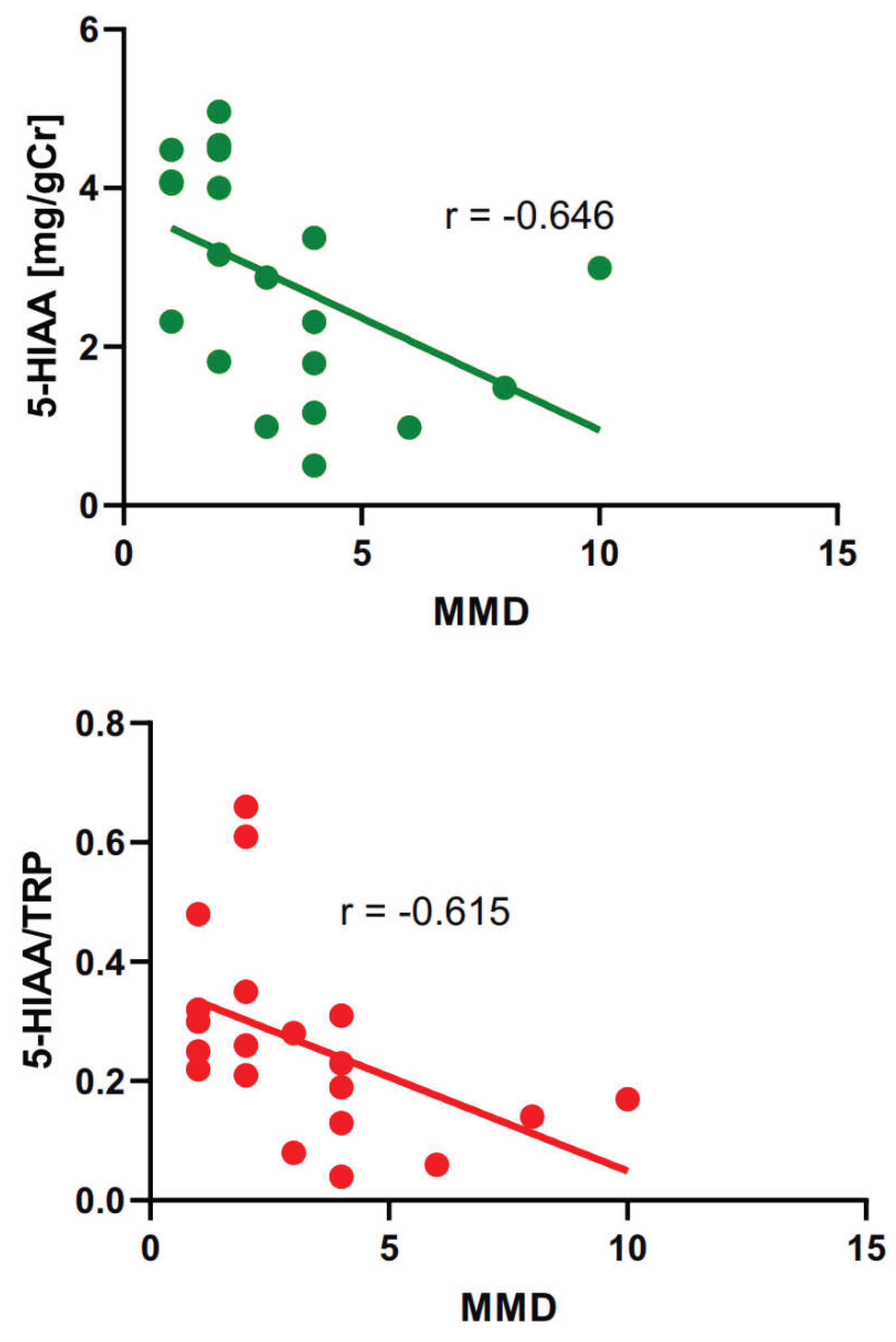
Figure 5.
Correlation between monthly headache days (MHD) and the urine concentration of 5- hydroxyaminoacetic acid (5-HIAA) measured in mg per g of creatinine (gCr) in migraine patients. The correlation was assessed by the Spearman rank test with the rho rank coefficient (r). The linear regression line was drawn by the least square method with the equation Y = –0.222X + 3.976 (R2 = 0.251).
Figure 5.
Correlation between monthly headache days (MHD) and the urine concentration of 5- hydroxyaminoacetic acid (5-HIAA) measured in mg per g of creatinine (gCr) in migraine patients. The correlation was assessed by the Spearman rank test with the rho rank coefficient (r). The linear regression line was drawn by the least square method with the equation Y = –0.222X + 3.976 (R2 = 0.251).
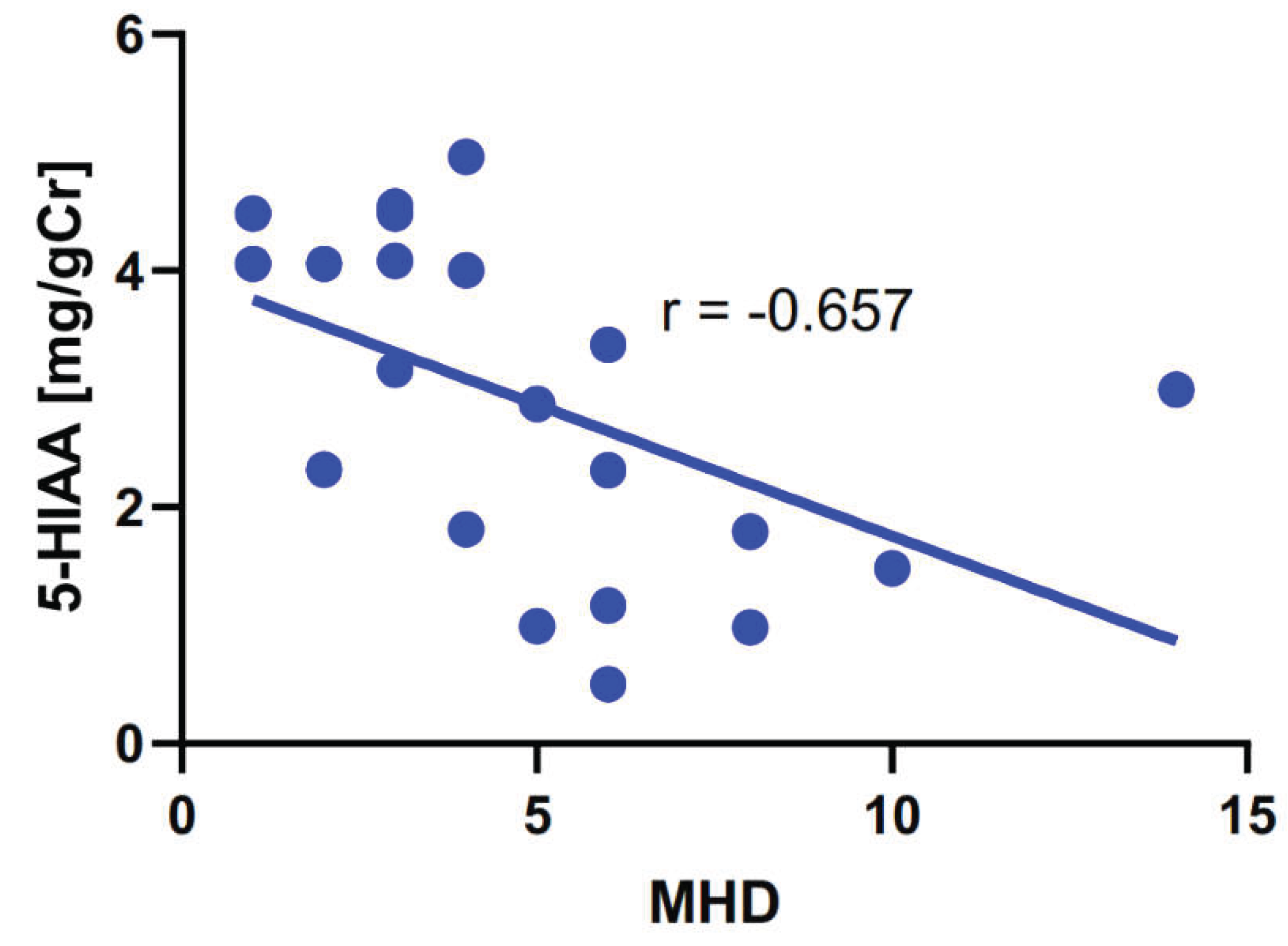
Figure 6.
Correlation between monthly headache days (MHD) and urine concentration of 5- hydroxyaminoacetic acid (5-HIAA) measured in mg per g of creatinine (gCr) in migraine patients. The correlation was assessed by the Spearman rank test with the rho rank coefficient (r). The linear regression line was drawn by the least square method with the equation Y = –0.122X + 3.601 (R2 = 0.080). .
Figure 6.
Correlation between monthly headache days (MHD) and urine concentration of 5- hydroxyaminoacetic acid (5-HIAA) measured in mg per g of creatinine (gCr) in migraine patients. The correlation was assessed by the Spearman rank test with the rho rank coefficient (r). The linear regression line was drawn by the least square method with the equation Y = –0.122X + 3.601 (R2 = 0.080). .
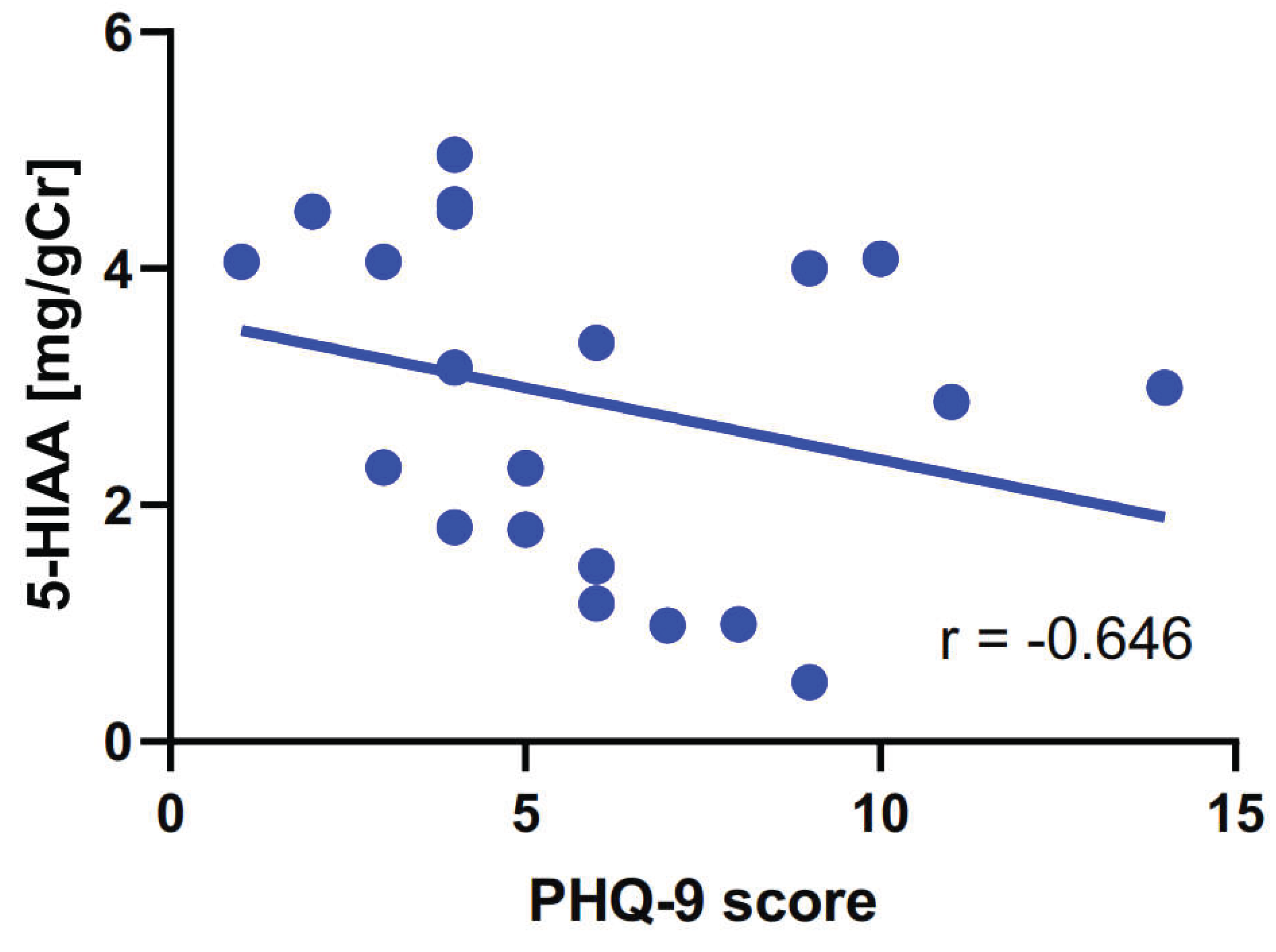

Table 1.
Characteristics of migraine patients enrolled in this study (n = 21).
| Characteristic | Specification (Mean ± SD (range) or type and number) |
|---|---|
| Age | 39 ± 13 (26-65) |
| Sex | 14 F, 7 M |
| Migraine type | Episodic, 21 |
| Aura | 8 |
| Frequency of attacks (per month) | 1.2 ± 1.1 (0.3-4.0) |
| Frequency of attacks (per quarter) | 3.5 ± 2.9 (1-12) |
| Time since diagnosis (years) | 18 ± 12 (3-40) |
| Treatment | Abortive 16, prophylactic 5, both 3 |
| Pain intensity (NRS 1) | 7.0 ± 1.5 (5-10) |
| MIDAS | 10.0 ± 5.9 (3-26) |
| Monthly migraine days Monthly headache days |
3.2 ± 2.4 (1-10) 5.0 ± 3.1 (1-14) |
| Mood disorders | 8 |
| Anxiety (GAD-7 score) | 4.4 ± 3.1 (0-12) |
| Depression (PHQ-9 score) | 6.0 ± 3.2 (1-14) |
1 NRS, Numeric Rating Scale; MIDAS, Migraine Disability Assessment; GAD-7, Generalized Anxiety Disorder 7-item; PHQ-9, Patient Health Questionnaire 9.
Table 2.
Correlation between the intensity of migraine headache evaluated by the MIDAS 1) questionnaire scores and the urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), KYNA, and quinolinic acid QA as well as their ratios in migraine patients. The correlations were analyzed with the Spearman rank test with the rho rank correlation coefficient.
Table 2.
Correlation between the intensity of migraine headache evaluated by the MIDAS 1) questionnaire scores and the urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), KYNA, and quinolinic acid QA as well as their ratios in migraine patients. The correlations were analyzed with the Spearman rank test with the rho rank correlation coefficient.
| MIDAS score and | rho-Spearman | p |
|---|---|---|
| TRP | 0.163 | 0.309 |
| 5-HIAA | – 0.676 | 0.001 |
| KYN | 0.242 | 0.304 |
| KYNA | – 0.050 | 0.835 |
| QA | 0.145 | 0.543 |
| 5-HIAA/TRP | – 0.679 | 0.001 |
| KYN/TRP | – 0.184 | 0.437 |
| KYNA/KYN | 0.077 | 0.748 |
| KYNA/QA | – 0.158 | 0.506 |
1) MIDAS, Migraine Disability Assessment Scale.
Table 3.
Correlation between monthly migraine days (MMD) and the urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), KYNA, and quinolinic acid QA as well as their ratios in migraine patients. The correlations were analyzed with the Spearman rank test with the rho rank correlation coefficient.
Table 3.
Correlation between monthly migraine days (MMD) and the urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), KYNA, and quinolinic acid QA as well as their ratios in migraine patients. The correlations were analyzed with the Spearman rank test with the rho rank correlation coefficient.
| MMD and | rho-Spearman | p |
|---|---|---|
| TRP | 0.195 | 0.410 |
| 5-HIAA | -0.646 | 0.002 |
| KYN | -0.188 | 0.427 |
| KYNA | 0.002 | 0.995 |
| QA | 0.143 | 0.548 |
| 5-HIAA/TRP | -0.615 | 0.003 |
| KYN/TRP | -0.116 | 0.627 |
| KYNA/KYN | 0.042 | 0.862 |
| KYNA/QA | -0.108 | 0.651 |
1) MMD, Monthly Migraine Days; TRP – tryptophan, 5-HIAA – 5-hydroxyaminoacetic acid; KYN – kynurenine KYNA – kynurenic acid; QA – quinolinic acid.
Table 4.
Correlation between monthly headache days (MHD) and the urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), KYNA, and quinolinic acid (QA) as well as their ratios in migraine patients. The correlations were analyzed with the Spearman rank test with the rho rank correlation coefficient.
Table 4.
Correlation between monthly headache days (MHD) and the urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), KYNA, and quinolinic acid (QA) as well as their ratios in migraine patients. The correlations were analyzed with the Spearman rank test with the rho rank correlation coefficient.
| MHD and | rho-Spearman | p |
|---|---|---|
| TRP | 0.149 | 0.518 |
| 5-HIAA | -0.657 | 0.001 |
| KYN | -0.206 | 0.369 |
| KYNA | -0.051 | 0.826 |
| QA | 0.159 | 0.491 |
| 5-HIAA/TRP | -0.418 | 0.060 |
| KYN/TRP | -0.152 | 0.510 |
| KYNA/KYN | 0.032 | 0.890 |
| KYNA/QA | -0.136 | 0.556 |
Table 5.
Correlation between the intensity of migraine headache evaluated by the PHQ-9 1) questionnaire and the urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), KYNA, and quinolinic acid (QA) as well as their ratios in migraine patients. The correlations were analyzed with the Spearman rank test with the rho rank correlation coefficient.
Table 5.
Correlation between the intensity of migraine headache evaluated by the PHQ-9 1) questionnaire and the urinary levels of tryptophan (TRP), 5-hydroxyaminoacetic acid (5-HIAA), kynurenine (KYN), KYNA, and quinolinic acid (QA) as well as their ratios in migraine patients. The correlations were analyzed with the Spearman rank test with the rho rank correlation coefficient.
| PHQ-9 score and | rho-Spearman | p |
|---|---|---|
| TRP | 0.004 | 0.987 |
| 5-HIAA | -0.427 | 0.048 |
| KYN | -0.334 | 0.139 |
| KYNA | -0.160 | 0.489 |
| QA | 0.216 | 0.347 |
| 5-HIAA/TRP | -0.307 | 0.176 |
| KYN/TRP | 0.042 | 0.862 |
| KYNA/KYN | 0.238 | 0.299 |
| KYNA/QA | -0.198 | 0.390 |
1) PHQ-9, Patient Health Questionnaire 9
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



