
Submitted:
10 April 2024
Posted:
12 April 2024
You are already at the latest version
Abstract
(1) Background: The aim of the research was to present and emphasize the importance of magnetic resonance imaging (MRI) in diagnosing Achilles tendon (AT) ruptures by presenting case reports. (2) Materials and Methods: The sample of respondents included 7 patients (4 males and 3 females, 2 athletes and 5 non-athletes), aged 25 to 58 years, with AT injuries, who were examined and treated at the Institute for Treatment and Rehabilitation "Niška Banja", Niš, Serbia. Ankle examinations with MRI were conducted using the Esaote O-scan 0.3 T machine. The examinations were performed without the application of a paramagnetic contrast agent and without the use of anesthesia. Results: The MRI method's sensitivity and overall diagnostic accuracy were excellent, with 100% true positives. In our study, the method accurately detected the presence, location, and severity of AT injuries in all cases. MRI is an important and reliable method for detecting AT injuries, classifying them, monitoring the course of recovery, and assessing the effects of therapy. Conclusions: An unrecognized or delayed diagnosis of an AT injury can lead to chronic changes. Timely diagnosis (clinical examination, ultrasonography, magnetic resonance imaging) and appropriate treatment (conservative or operative) enable patients to return to normal activities, including sports. Unfortunately, the use of MRI is limited by restricted access and the cost of the examination.
Keywords:
Achilles Tendon Injuries
; Screening Techniques
; Interesting Images
; athletes and non-athletes
; case reports
1. Introduction
The calcaneal or Achilles tendon (AT), the strongest and largest human body tendon, is frequently injured due to high biomechanical stress, up to 10 times body weight [1], and limited vascularization [2]. Its earliest known reference dates to 1693 in Philip Verheien's "Corporis Humani Anatomia," using the eponym "chorda Achillis" [3,4]. In 1717, Lorenz Heister introduced the Latin term "Tendo Achillis" [5]. The AT, about 15 cm long, connects the gastrocnemius, soleus, and plantaris muscles to the calcaneus' posterosuperior aspect. It lacks a synovial membrane but has a paratenon covering, receiving blood supply from the Musculo-tendon joint and innervation from the sural and tibial nerves [6]. It aids walking, running, and jumping through strong contractions [2].
Triceps surae muscle action generates translational force via the AT for plantar foot flexion (about 93% of the force) [2], essential for mobility, walking, running, and jumping [7,8]. AT is susceptible to damage from repeated loads, predominantly in athletes involved in sports and exercise [1]. Injuries include Achilles tendinopathy (55-65%), insertion issues (25-35%), and partial lesions or undiagnosed ruptures [10]. Rupture rates are estimated at 5.5-9.9 per 100,000 people in North America and 6-18 per 100,000 in Europe, with 60-75% occurring in sports, particularly basketball and football [11].
Detailed history and physical examination are crucial for diagnosing AT rupture, although 20-25% are initially missed [12]. Signs include sudden pain, inability to bear weight, weakness, stiffness, diffuse swelling, and bruising, with the rupture site typically 2-6 cm proximal to the tendon insertion [13]. Diagnosis employs diagnostic tests such as Simmonds or Thompson Calf Squeeze Test, Matles Test, O’Brien Test, Copeland Test, standard radiography, ultrasound, and magnetic resonance imaging [14]. The research aims to underscore the significance of MRI in diagnosing AT rupture through case reports.
The aim of the research was to present and emphasize the importance of MRI in diagnosing AT ruptures by presenting case reports.
2. Materials and Methods
2.1. Sample of Images
We reported images of 7 patients (5 males and 2 females, 2 athletes and 5 non-athletes), aged 25 to 58 years, with AT injuries, examined and treated at the Institute for Treatment and Rehabilitation "Niška Banja", Niš, Serbia, with the current research approved by its Ethics Committee (Approval Code: 3516/1). All participants provided consent and underwent screening by a physician.
2.2. Procedures
Ankle examinations with MRI were conducted using the Esaote O-scan 0.3 T. These examinations are performed without the application of a paramagnetic contrast agent and without the use of anesthesia.
Based on our extensive experience, we have identified several characteristic cases of AT injuries.
2.3. Screening Techniques
The following screening techniques are commonly used:
• Spin-Echo: basic pulse sequence T1W and T2W in which the cortical, trabeculated bone and fibrocartilaginous structures (ligaments, tendons) have a low signal intensity;
• Short Tau Inversion Recovery: a sequence that saturates the adipose tissue signal (the most sensitive sequence for detecting changes in bone marrow and muscles);
• Proton Density: a sequence that displays tissues with a higher concentration or density of hydrogen protons.
The examinations are conducted in all three planes: sagittal (SP), coronal (CP), and axial (AP). Among these, sagittal and axial sections provide the most informative data for assessing the morphology of AT injuries.
Patients who undergo an MRI scan usually receive a standard ankle radiograph following a clinical examination to rule out acute bone structure discontinuation. Some patients underwent echo sonography as part of their treatment, while others came directly for an MRI examination, either with or without a suspected AT lesion.
In the interpretation of AT injuries, we employed the Kuwada classification [15], proposed in 1990. It is the most widely used system for describing AT rupture.
2.4. Classification of AT Lesions
AT lesions can be grouped (according to the severity of the injury and the degree of withdrawal) into four types:
• type I: partial rupture ≤50% (usually treated with conservative treatment);
• type II: complete rupture with tendinous spacing ≤3 cm (typically treated with end-to-end anastomosis);
• type III: complete rupture with tendinous spacing of 3 to 6 cm (often requires tendon / synthetic graft);
• type IV: complete rupture with a defect >6 cm (neglected rupture, often requires tendon / synthetic graft and resection of gastrocnemius) [16,17,18].
MRI offers excellent contrast resolution for assessing AT morphology [19]. Normally, the tendon appears homogeneously hypointense in all imaging sequences. In some asymptomatic cases, a mild intrasubstantial hypo intensity in the distal segment of the tendon may be the result of an artifact associated with the magic angle phenomenon. This is not because the tendon itself changes its axis, but rather because the inner fibers have a spiral bend near the calcaneal attachment [2]. The contour of a normal tendon should be smooth and well-defined in different orthogonal planes. The AT has no sheath but is covered by a thin, intermediate-signaling peritenon. Tendon integrity can be easily assessed on sagittal sections, which should show the myotendinous joint and the distal aspect of the muscle. The application of paramagnetic contrast usually does not provide additional information, so the native MRI image is sufficient for assessment. Neighboring structures, such as muscle, calcaneus, retrocalcaneal bursa, Kager's fat pad, and flat subcutaneous adipose tissue, should also be evaluated for associated changes [20,21,22,23].
3. Results
The screening method demonstrated a high rate of success in identifying and characterizing AT injuries. In our study, the method accurately detected the presence, location, and severity of AT injuries in the all cases.
The method's sensitivity and overall diagnostic accuracy were found to be excellent. Sensitivity refers to the method's ability to correctly identify positive cases (i.e., the presence of an injury), and it showed a 100% of true positives.
Figure 1.
The first MRI examination at the "Niška Banja" institution, three months after the operative treatment (plastic surgery) for patient (an athlete) O.Đ. (1988). The following are MRI scans taken after injuries in various patients. MRI finding: Condition after surgical treatment for a complete rupture of the AT; image A - T1W sagittal section - inhomogeneity in the AT sheath - postoperative sequelae; image B - T2W axial section - condition after surgical treatment of complete AT rupture.
Figure 1.
The first MRI examination at the "Niška Banja" institution, three months after the operative treatment (plastic surgery) for patient (an athlete) O.Đ. (1988). The following are MRI scans taken after injuries in various patients. MRI finding: Condition after surgical treatment for a complete rupture of the AT; image A - T1W sagittal section - inhomogeneity in the AT sheath - postoperative sequelae; image B - T2W axial section - condition after surgical treatment of complete AT rupture.
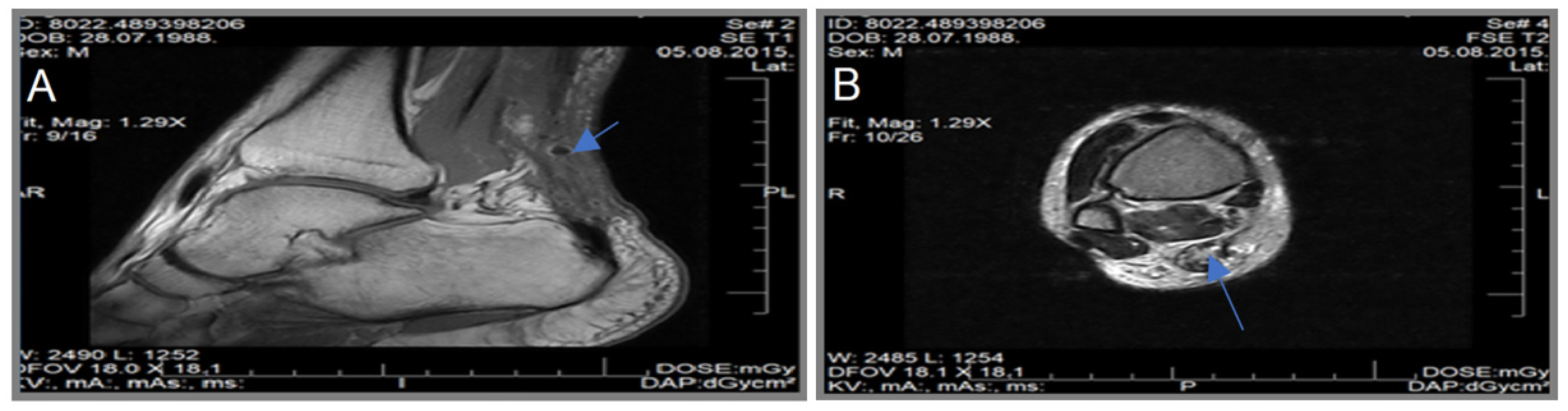
Figure 2.
The first MRI examination after a bowling injury for patient (recreative athlete) G.Š. (1958). MRI finding: Partial rupture in the field of tendinosis (upper images from left to right); AT tendinosis (lower images from left to right); image A - T1W sagittal section - AT with a normal course, voluminous, convex anterior margins, hypersignal in the non-insertional part; image B - T2W axial section - voluminous AT, with hypersignal fibers, predominantly in the posterolateral and anteromedial aspects; image C - T1W sagittal section - voluminous AT, convex anterior margins, heterosignal; image D - T2W sagittal section - heterosignal, voluminous.
Figure 2.
The first MRI examination after a bowling injury for patient (recreative athlete) G.Š. (1958). MRI finding: Partial rupture in the field of tendinosis (upper images from left to right); AT tendinosis (lower images from left to right); image A - T1W sagittal section - AT with a normal course, voluminous, convex anterior margins, hypersignal in the non-insertional part; image B - T2W axial section - voluminous AT, with hypersignal fibers, predominantly in the posterolateral and anteromedial aspects; image C - T1W sagittal section - voluminous AT, convex anterior margins, heterosignal; image D - T2W sagittal section - heterosignal, voluminous.
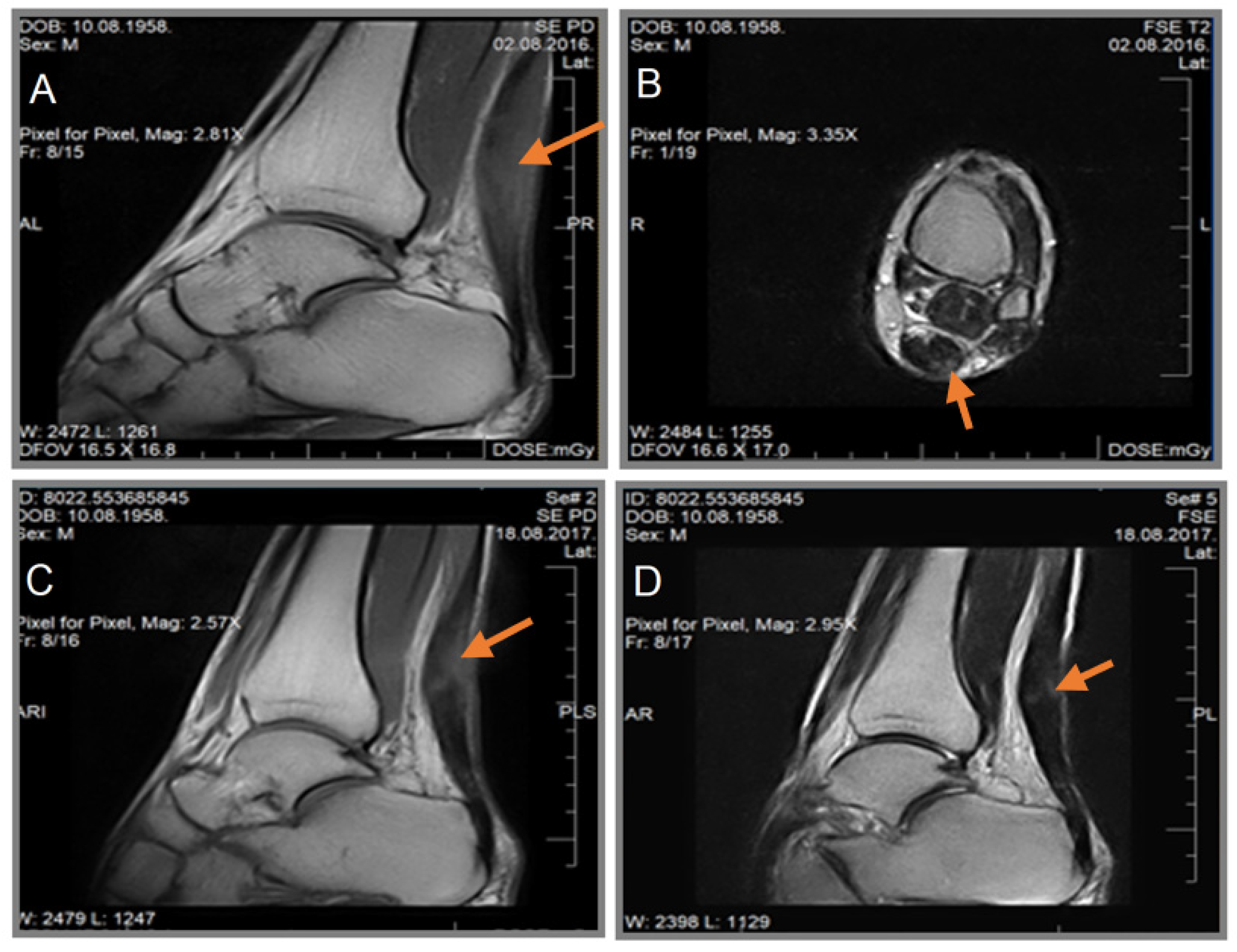
Figure 3.
The first MRI examination after an injury in patient, D.P. (1996). MRI finding: intrasubstantial hypersignal in the AT, anterior contour irregularity from 4 mm to 10 mm from the insertion; image A - T2W axial section, T2W sagittal section: intrasubstance hypersignal in the longitudinal orientation localized in the non-insertional part - partial lesion (single arrow). Hypersignal characteristic of Kager's fat pad edema and fluid (double arrow); image B - T1W sagittal section: Inhomogeneous hypersignal of the AT with a central portion of high signal (single arrow). Linear zones of hyposignal in Kager's fat pad (double arrow).
Figure 3.
The first MRI examination after an injury in patient, D.P. (1996). MRI finding: intrasubstantial hypersignal in the AT, anterior contour irregularity from 4 mm to 10 mm from the insertion; image A - T2W axial section, T2W sagittal section: intrasubstance hypersignal in the longitudinal orientation localized in the non-insertional part - partial lesion (single arrow). Hypersignal characteristic of Kager's fat pad edema and fluid (double arrow); image B - T1W sagittal section: Inhomogeneous hypersignal of the AT with a central portion of high signal (single arrow). Linear zones of hyposignal in Kager's fat pad (double arrow).

Figure 4.
The first MRI examination after an injury in the patient Ž.L. (1969). MRI finding: AT rupture in the area of tendinosis; severe paratendinitis; tenosynovitis; image A - T1W sagittal section: AT voluminous with hyperintensity (IS fluid) immediately above the insertion; image B - T2 axial section: increased transverse diameter of the AT with a central zone of fluid signal intensity. Tenosynovitis of the peroneal muscle tendons.
Figure 4.
The first MRI examination after an injury in the patient Ž.L. (1969). MRI finding: AT rupture in the area of tendinosis; severe paratendinitis; tenosynovitis; image A - T1W sagittal section: AT voluminous with hyperintensity (IS fluid) immediately above the insertion; image B - T2 axial section: increased transverse diameter of the AT with a central zone of fluid signal intensity. Tenosynovitis of the peroneal muscle tendons.
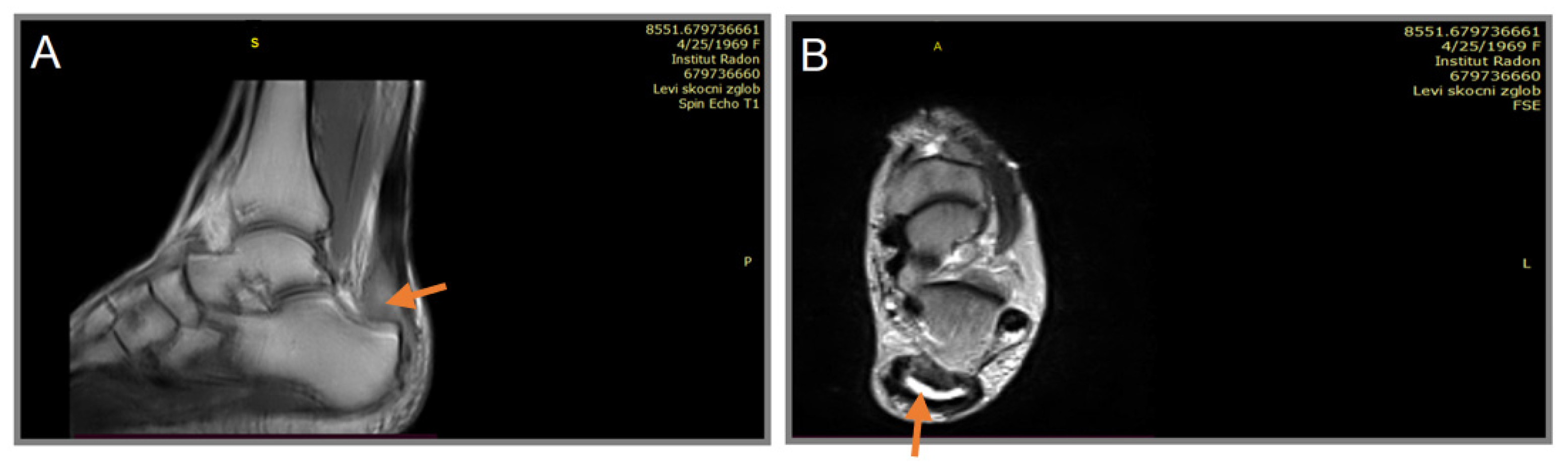
Figure 5.
First MRI examination after acute trauma in patient P.B. (1961). MRI finding: Complete rupture of the AT with a 6 mm diameter KK defect, 40 mm from insertion, with fiber retraction; image A - T1W sagittal section: state after complete rupture of the AT with a defect of increased signal intensity (characteristic of blood) and fiber retraction; image B - T2W axial section: enlarged diameter AT, heterosignal, predominantly fluid signal intensity, unclear contours predominantly posteriorly; image C - T2W sagittal section: defect of the AT with fluid signal intensity and fiber retraction; image D - T2W axial section: voluminous AT with preserved fiber signal intensity distal to the injury. Synovial proliferation in the anterior groove.
Figure 5.
First MRI examination after acute trauma in patient P.B. (1961). MRI finding: Complete rupture of the AT with a 6 mm diameter KK defect, 40 mm from insertion, with fiber retraction; image A - T1W sagittal section: state after complete rupture of the AT with a defect of increased signal intensity (characteristic of blood) and fiber retraction; image B - T2W axial section: enlarged diameter AT, heterosignal, predominantly fluid signal intensity, unclear contours predominantly posteriorly; image C - T2W sagittal section: defect of the AT with fluid signal intensity and fiber retraction; image D - T2W axial section: voluminous AT with preserved fiber signal intensity distal to the injury. Synovial proliferation in the anterior groove.
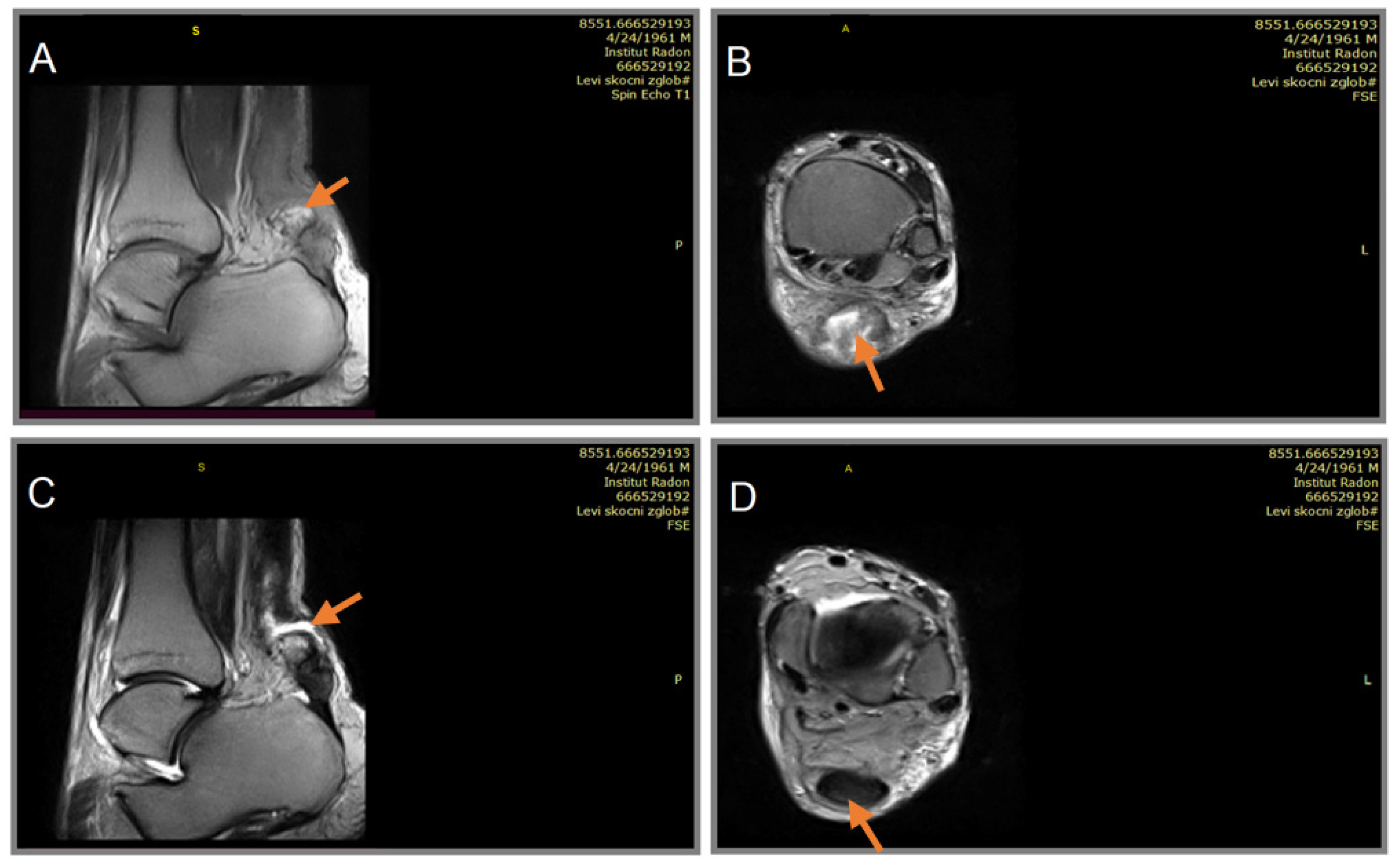
Figure 6.
First MRI examination of rheumatoid arthritis patient C.V. (1971). MRI finding: AT rupture with fiber retraction and a 20 mm diameter defect; image A - T1W sagittal section (2016) - defect with fiber retraction of the AT; image B - T1W sagittal section (2017) - follow-up examination; image C - T2W axial section - AT fiber defect of signal intensity edema and fluid.
Figure 6.
First MRI examination of rheumatoid arthritis patient C.V. (1971). MRI finding: AT rupture with fiber retraction and a 20 mm diameter defect; image A - T1W sagittal section (2016) - defect with fiber retraction of the AT; image B - T1W sagittal section (2017) - follow-up examination; image C - T2W axial section - AT fiber defect of signal intensity edema and fluid.
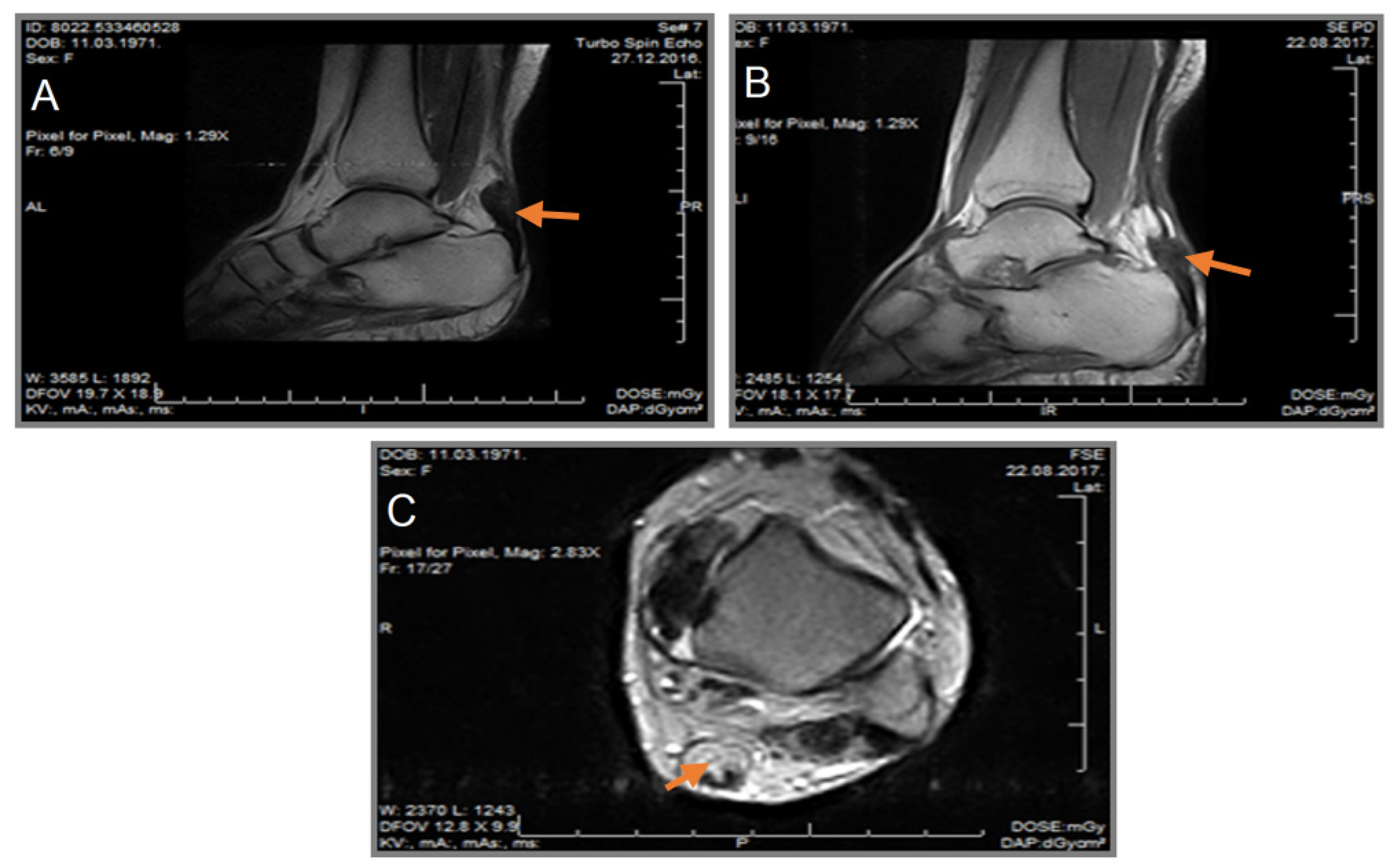
The first examination of patient C.V. (1971) was conducted in December 2016, followed by conservative treatment. The control examination was conducted in August 2017.
Figure 7.
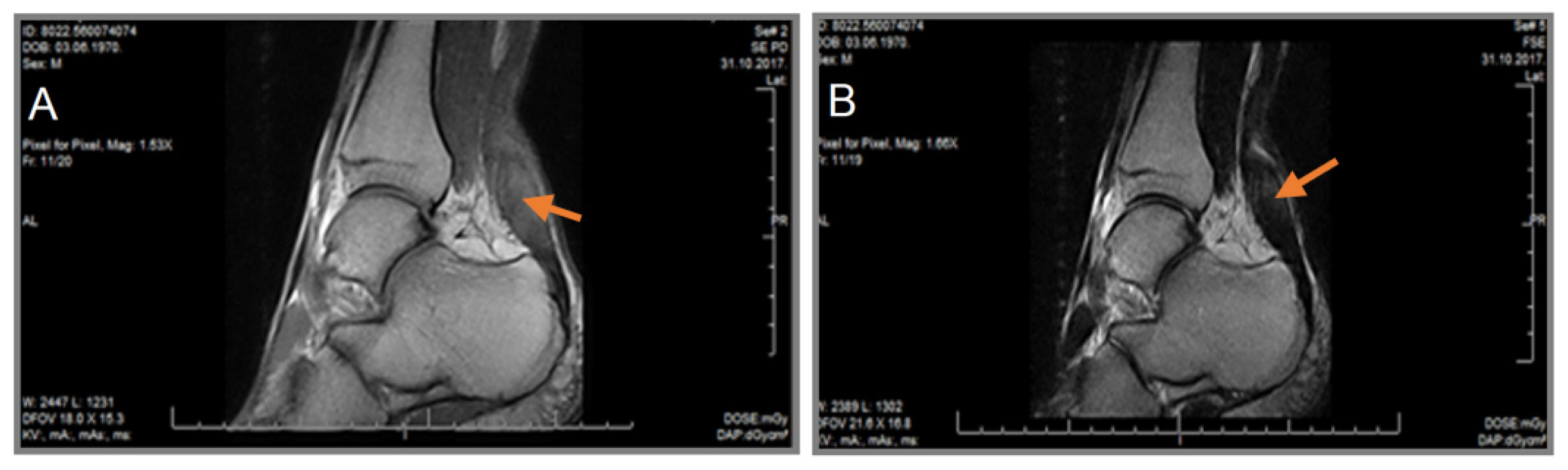
The first MRI examination after a work-related injury (police officer) for patient D.A. (1970). The first examination was conducted in August 2017, followed by conservative treatment. The control examination was conducted in October 2017; MRI finding: Partial rupture of the non-insertion part of the AT; image A - T1W sagittal section - AT voluminous, fusiformly shaped, homogeneously hyperintense; image B - T2W sagittal section - AT voluminous, fusiformly shaped, moderately hyperintense.
Figure 7.
The first MRI examination after a work-related injury (police officer) for patient D.A. (1970). The first examination was conducted in August 2017, followed by conservative treatment. The control examination was conducted in October 2017; MRI finding: Partial rupture of the non-insertion part of the AT; image A - T1W sagittal section - AT voluminous, fusiformly shaped, homogeneously hyperintense; image B - T2W sagittal section - AT voluminous, fusiformly shaped, moderately hyperintense.
4. Discussion
The screening method conducted at the Institute for Treatment and Rehabilitation "Niška Banja" has provided valuable information regarding the extent of AT injuries, assisting clinicians in tailoring appropriate treatment plans. This high level of accuracy in injury diagnosis is crucial for guiding healthcare providers in making informed decisions and optimizing patient care.
There are only a few epidemiological studies on the frequency of AT ruptures. These studies have shown an increase in incidence in the West over the last few decades, which is likely due to the increased popularity of recreational sports among middle-aged individuals. Ball games account for over 60% of AT ruptures in many series. The two most commonly discussed pathophysiological theories include chronic tendon degeneration and the failure of the inhibitory mechanism of the musculotendinous unit. Reports of AT ruptures associated with corticosteroid use, whether systemic or local, have been made, but the role of corticosteroids in large patient populations is marginal. Furthermore, recent studies do not confirm previous findings of blood group “O” dominance in patients with AT rupture.
Comparative series with surgical and non-surgical treatments and postoperative plaster immobilization in relation to early functional treatment have been published [24]. Although conservative treatment has its supporters, such as plaster immobilization for 8 weeks, surgical treatment appears to have been the method of choice in the late 1980s and 1990s for athletes, young individuals, and cases of delayed rupture [25]. Early ruptures in non-athletes can also be treated conservatively. In small well-motivated patient groups, functional postoperative treatment is well-tolerated, safe, and effective. The lack of a universal and consistent protocol for subjective and objective assessment of AT ruptures has prevented any direct comparison of results [26]. There is also no single, universally accepted surgical technique. Although early ruptures have been successfully treated with percutaneous sutures (simple end-to-end sutures), many authors combine simple tendon sutures with plastic procedures of various types [24]. The main objection to surgical treatment is the high rate of complications. Most complications are minor and related to the wound, which may delay recovery but do not affect the final outcome. Major complications are rare but can be severe (major postoperative skin and soft tissue defects in the Achilles region). Complications of conservative treatment mainly include re-rupture and residual tendon elongation, which can result in significant muscle weakness.
After six months of physical treatment, the patient can return to the activities they were engaged in before the injury, including sports.
It is assumed that a physically inactive lifestyle leads to a decrease in tendon vascularization, while maintaining a continuous level of activity prevents structural changes within the musculotendinous unit caused by inactivity and aging. Proper warm-up and stretching are necessary to prevent muscle-tendon injuries, but improper or excessive stretching or warming can predispose to these injuries.
5. Conclusions
An unrecognized or delayed diagnosis of an AT injury can lead to chronic changes. Timely diagnosis (clinical examination, ultrasonography, magnetic resonance imaging) and appropriate treatment (conservative or operative) enable patients to return to normal activities, including sports.
MRI is an important and reliable method for detecting AT injuries, classifying them, monitoring the recovery process, and evaluating the effects of therapy. Its success in detecting and characterizing injuries can significantly contribute to improved patient outcomes and the overall quality of healthcare in this context. Unfortunately, the use of MRI is limited by restricted access and the cost of examination.
Author Contributions
“Conceptualization, S.S.; V.Ž.; S.B.; B.B.; and E.B.; methodology, D.S.; S.B.; Š.S; and T.D.; investigation, S.S.; and V.Ž.; resources, N.A.; writing—original draft preparation, S.S.; S.B; Š.S.; B.B.; and N.A. writing—review and editing, S.S.; V.Ž.; D.S.; S.B.; B.T.; T.D.; and A-C.Ş. supervision, Š.S.; B.B.; N.A.; E.B.; T.D.; and A-C.Ş. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research was supported by a grant from the Ministry of Education and Science of the Republic of Serbia within a project OI179024.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethic Committee (Approval Code: 3516/1).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Järvinen, T. A.; Kannus, P.; Paavola, M.; Järvinen, T. L.; Józsa, L.; Järvinen, M. Achilles tendon injuries. Curr. Opin. Rheumatol., 2001, 13, 150-155. [CrossRef]
- Schweitzer, M. E.; Karasick, D. MR imaging of disorders of the Achilles tendon. Am. J. Roentgenol., 2000, 175, 613-625. [CrossRef]
- Klenerman, L. The early history of tendo Achillis and its rupture. J. Bone JT. Surg., Br. Vol., 2007, 89, 545-547. [CrossRef]
- Suy, R. Philip Verheyen (1648–1710) and his Corporis Humani Anatomiae. Acta Chir. Belg., 2007, 107, 343-354. [CrossRef]
- Hyrtl, J. Onomatologia anatomica. Wien: W. Braumüller; p. 531-32. 1880.
- Standring, S. (Ed.). Gray's anatomy e-book: The anatomical basis of clinical practice. Elsevier Health Sciences. 2021.
- Moore, K. L.; Agur, A. M.; Dalley, A. F. Essential clinical anatomy. 2015.
- Wong, M.; Jardaly, A. H.; Kiel, J. Anatomy, bony pelvis and lower limb, Achilles tendon. 2018.
- Williams, S. K.; Brage, M. Heel pain-plantar fasciitis and Achilles enthesopathy. Clin. Sports Med., 2004, 23, 123-144. [CrossRef]
- Chiodo, C. P.; Glazebrook, M.; Bluman, E. M.; Cohen, B. E.; Femino, J. E.; Giza, E.; Sluka, P. Diagnosis and treatment of acute Achilles tendon rupture. J. Am. Acad. Orthop. Surg., 2010, 18, 503-510. [CrossRef]
- Litin, S. C. Mayo Clinic family health book, 5th Edition: Completely revised and updated. Rochester, MN: Mayo Clinic Press. p. 1392. 2018.
- O'Brien, T. The needle test for complete rupture of the Achilles tendon. J. Bone JT. Surg., 1984, 66, 1099-1101.
- DiStefano, V. J.; Nixon, J. E. Achilles tendon rupture: Pathogenesis, diagnosis, and treatment by a modified pullout wire technique. J. Trauma, 1972, 12, 671-677.
- Kader, D.; Mosconi, M.; Benazzo, F.; Maffulli, N. Achilles tendon rupture. In Tendon injuries: Basic science and clinical medicine (pp. 187-200). London: Springer London. 2005.
- Kuwada, G. T. Classification of tendo Achillis rupture with consideration of surgical repair techniques. J. Foot Surg., 1990, 29, 361-365.
- Nickisch, F. Anatomy of the Achilles tendon. The Achilles tendon: Treatment and rehabilitation (pp. 2-16), London: Springer London. 2009.
- Chiodo, C. P.; Wilson, M. G. Current concepts review: Acute ruptures of the Achilles tendon. Foot Ankle Int., 2006, 27, 305-315. [CrossRef]
- Popović, N.; Lemaire, R. Diagnosis and treatment of acute ruptures of the Achilles tendon. Current concepts review. Acta Orthop. Belg., 1999, 65, 458-471.
- Recht, M. P.; Donley, B. G. Magnetic resonance imaging of the foot and ankle. J. Am. Acad. Orthop. Surg., 2001, 9, 187-199. [CrossRef]
- Möller, M.; Movin, T.; Granhed, H.; Lind, K.; Faxen, E.; Karlsson, J. Acute rupture of tendo Achillis: A prospective, randomised study of comparison between surgical and non-surgical treatment. J. Bone JT. Surg., Br. Vol., 2001, 83, 843-848. [CrossRef]
- Fox, J. M.; Blazina, M. E.; Jobe, F. W.; Kerlan, R. K.; Carter, V. S.; Shields Jr, C. L.; Carlson, G. J. Degeneration and rupture of the Achilles tendon. Clin. Orthop. and Relat. Res., 1975, 107, 221-224. [CrossRef]
- Sharma, P.; Maffulli, N. Tendon injury and tendinopathy: Healing and repair. J. Bone Joint Surg., 2005, 87, 187-202. [CrossRef]
- Resnick, D.; Kang, H. S.; Pretterklieber, M. L. Internal derangements of joints, Volume 2, pp. 1589-1598. Philadelphia (PA): Saunders Elsevier. 2007.
- Arriaza, R.; Arriaza, Á.; López-Vidriero, E.; Gayoso, R.; Agrasar, C.; Saavedra-Garcia, M. A. Quadriceps tendon autograft and platelet rich plasma injection to treat chronic Achilles tears—A minimum two-year follow-up. Ann. Transl. Med., 2017, 7. [CrossRef]
- Leppilahti, J.; Orava, S. Total Achilles tendon rupture: A review. Sports Med., 1998, 25, 79-100. [CrossRef]
- Alrabaa, R. G.; Freibott, C.; Vosseller, J. T. Patient perception of Achilles tendon rupture treatment. Injury, 2020, 51, 2710-2716. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



