
Submitted:
11 April 2024
Posted:
15 April 2024
You are already at the latest version
Abstract
Background: Schistosome egg deposition in pregnant women may affect the placenta of infected mothers and cause Placental Schistosomiasis (PS). Histopathological examination of placental tissue is an inadequate detection method due to low sensitivity. So far, there has not been any sys-tematic review on PS. Methods: We conducted a systematic literature search on PubMed and in-cluded relevant secondary literature found in the citations of the primarily included publications. Results: We found a total of 8 publications describing PS with a total of 92 cases, describing egg deposition of dead and/or viable eggs and worms of S. haematobium and S. mansoni in placental tissue. One cross-sectional study investigating the prevalence of PS and its association to adverse birth outcomes, found 22% of placentas to be infested using a maceration technique but only < 1% using histologic examination. Additionally, no direct link to deleterious pregnancy outcomes could be shown. Conclusions: PS is a highly unattended and underdiagnosed condition in en-demic populations, due to a lack of awareness as well as low sensitivity of histopathological examinations. However, PS may play an important role in mediating or reinforcing adverse birth outcomes (ABO) such as fetal growth restriction (FGR) in maternal schistosomiasis, possibly by placental inflammation.
Keywords:
Schistosomiasis
; Placenta
; Adverse Birth Outcomes
; Pregnancy
; Praziquantel
1. Introduction
Schistosomiasis is a parasitic disease affecting around 220 million people worldwide [1], among which there is an estimated number of 40 million women of reproductive age [2]. After infecting humans, Schistosoma spp. excrete eggs that become trapped in various tissues –depending on the causative species. In women, if trapped within the genital organs, they can cause female genital schistosomiasis (FGS). [3] Pregnant women may also be affected from egg deposition in the placenta. Previous research describes the placental villi, the intervillous space and the decidua, to be the most common places of detection [4]. Pregnant women are a particular vulnerable population for schistosomiasis, as it contributes to maternal anemia [5] and may be linked to adverse birth outcomes (ABO) in their newborns, such as low birth weight, small for gestational age (SGA), fetal growth restriction (FGR) and stillbirth [6,7]. Exact mechanisms of the pathophysiological link between maternal schistosomiasis and ABO have not yet been fully understood and might be multi-causal. Suggested contributors include maternal anemia, a known risk factor for ABO [8], which is associated with schistosomiasis [5] as well as other parasitic diseases. Furthermore, inflammation at the feto-maternal interface due to placental egg deposition and the trans-placental transfer of schistosomal antigens may play an important role [6]. Since the beginning of the 20th century there have only been few case reports and clinical trials investigating placental schistosomiasis (PS). This may be due to neglected attendance to the topic, but also methodologic difficulties to identify infested placentas with sufficient sensitivity, because standard histopathological methods can only investigate a little part of the placenta. Sutherland et al. have already called in 1965 for studies using tissue dissolution techniques – and investigated a series of placentas with a maceration technique using 10% sodium hydroxide [9]. Renaud et al. then later used in 1972 a maceration technique using potassium hydroxide (KOH) [10]. Recently, a description for an improved maceration technique has been described by our study group, using ethanol fixation and maceration with 4% KOH over 24 hours, which allowed a complete dissolution of placental tissue while maintaining well preserved the morphological features of the observed schistosomal eggs [11]. Because of the important role of PS as a possible mechanistic link between maternal schistosomiasis and ABO and its highly underestimation and underdiagnosing, we aimed to review the current literature and give an overview of the cases that have been described in the past century.
2. Materials and Methods
PubMed was used as the search tool. The key words used to gather information on PS in general were ‘placental’, and ‘schistosomiasis’. A total of 47 PubMed listed publications were screened for information on PS published in the years 1975 to 2024. Furthermore, we included literature that was published between 1914 and 1994 that was not accessible with PubMed but cited in the reviewed literature. Only publications concerning anatomopathological aspects of PS were selected and are displayed in the table and flow chart, respectively. Of the 47 publications screened, one investigated the presence of schistosomiasis in the placenta by polymerase chain reaction (PCR), three were case reports on schistosomiasis in pregnancy without confirmation of PS, six were trials on schistosomiasis without aspects of PS, 20 addressed immune responses and inflammation associated with schistosomiasis in humans, eight were animal models, five were reviews and one a study without aspects of schistosomiasis. Those 45 publications were excluded. The remaining two publications identified in PubMed were case reports that referred directly on placental involvement in schistosomiasis. In addition, six publications reporting on PS were identified in the references of the PubMed listed literature. For completeness, it is worth mentioning that an additional conference abstract from 1968 was identified that addressed PS, but did not provide clear information about additional cases. Overall, eight scientific full-text publications on placental involvement of schistosomiasis were identified and considered for this review (Figure 1).
3. Results
In eight publications that were considered relevant for this review we found 92 documented cases of PS, which are summarized in Table 1. Among these 92 cases, four cases reported adult worms and all cases schistosome eggs in placental tissue, respectively. In 84 cases the causative species was S. haematobium, in seven cases S. mansoni and one case showed placental infestation of both species. None of the cases described a direct detection of S. japonicum eggs or worms in the placenta.
The first mention of intrauterine infection with Schistosoma spp. dates to Fujinami and Namakura in 1911, who detected S. japonicum in the fetus of a infected pregnant dog [18]. The experimental intrauterine infestation of animals with Schistosoma spp. was later confirmed by Narabayashi et al. in 1914 [19]. Narabayashi also first described egg deposition in the placenta of two guinea pigs. He then described a case series of 22 human newborns, whose mothers were exposed to S. japonicum during pregnancy, of which three infants were infected with S. japonicum despite never having had contact with fresh water [19]. Some concluded that this could be seen as a proof that vertical transmission of the parasite could also happen in humans [20]. However, transplacental invasion of Schistosoma spp. has never been confirmed in humans since then. About 30 years later Prates (1948) first mentioned placental involvement of schistosomiasis in humans in a case series of 5 women due to an infection with S. haematobium [12].
The first detailed histopathological description of human PS was later provided by Sutherland et al. in 1965, who described a case with placental egg infestation of S. haematobium in a pregnant woman with epileptiform seizures [9]. The authors realized the need for a maceration technique as method of choice for the investigation of placental tissue because random sectioning of the placental tissue would give false negative results. After their observation of the initial case, the authors further investigated another 22 placentas (using a 10% sodium hydroxide maceration) of which they found additional seven to be infected with either S. haematobium or S. mansoni. In 1968, Rodrigues presented several cases of PS at the Congress of the International Academy of Pathology in Milano, Italy [21]. However, the conference abstract leaves it unclear whether the cases mentioned were newly described cases from Mozambique or references to the existence of such cases from the scientific literature.
In 1969 Bittencourt et al. published one case of PS due to S. mansoni describing both egg deposition as well as adult worms in the examined placental tissue [13]. In 1980 the same author published another case series of four cases – including the previous case from 1965 – and reported additional three cases of stillbirths with granulomatous placentitis that might have been caused by placental infestation with S. mansoni [15]. Two years earlier in 1978, Viggiano et al. had reported another case of PS due to S. mansoni [14], but neither Viggiano nor Bittencourt performed a maceration technique to examine placentas.
The most extensive investigation on PS until present was done by Renaud et al. in 1972, who were the first to carry out a systematic investigation of placentas on an extensive scale in Ivory Coast using a maceration technique with caustic potash. From the examined 322 placentas, 72 (22.3%) were positive for schistosome eggs (S. haematobium) by maceration technique whereas histopathologic sectioning revealed only one positive result showing eggs in the intervillous space [10]. None of the women was prior known to be infected with S. haematobium.
In 1994, Peres et al. published another case report in which he described a woman with a prolapsed umbilical cord who subsequently gave birth to an otherwise healthy premature baby via cesarean section. Routine examination of the placenta by histological examination revealed both dead and viable eggs of S. mansoni in the villous vessels without surrounding inflammatory reaction [16]. The most recent description is from 2014 by Schleenvoigt et al. who first described PS in a German traveler returning from Malawi. The woman had presented with painless macrohematuria and was diagnosed and treated for schistosomiasis during pregnancy. The histopathological examination of the placenta 18 weeks post treatment revealed egg deposition of S. haematobium inside the villi.
4. Discussion
4.1. Underestimated Prevalence of Placental Schistosomiasis?
Placental schistosomiasis has recently been reaffirmed to be underestimated and underdiagnosed, mainly due to the lack of attention towards this issue [11]. This seems to be confirmed by the latest findings from Franz et al., who examined 268 placentas of women from Ivory Coast and Ghana with PCR for the presence of Schistosoma spp. and found positive signals in 19% (n=51) of the samples [22]. The latter is in accordance with the earlier reported prevalence of PS of 20% in an endemic population of Ivory Coast by Renaud et al. [10] detected by maceration.
4.2. Contribution to Adverse Birth Outcomes (ABO)
The growing importance of PS is not only due to its unacknowledged occurrence but also due to its possible role as a mechanistic link between maternal schistosomiasis and adverse birth outcomes (ABO), such as prematurity, low birth weight (LBW), fetal growth restriction (FGR) and stillbirth or miscarriage [6]. Of the 92 cases summarized in Table 1, 22 were associated with prematurity, 22 with LBW and 13 with fetal death (miscarriage or stillbirth). However, there was most likely a strong selection bias, as the examination of the placenta in most case reports was due to pregnancy complications. Only the cross-sectional study of Renaud et al. in 1972 investigated independently a possible association between PS and ABO. The analysis of newborn weight and length revealed no association with PS. Furthermore, these authors observed that placental infestation generally appeared to take place after the 3rd month of gestation – probably due to circulatory changes in the pelvic blood system throughout the pregnancy – and concluded that PS seems not to contribute to fetal death, at least before this time point in pregnancy [10]. Nevertheless, there remains evidence, albeit contradictory, that maternal schistosomiasis contributes to adverse birth outcomes, particularly the occurrence of LBW [23,24,25,26]. The underlying pathophysiologic mechanisms are not yet fully understood. Maternal anemia which is strongly associated with schistosomiasis [5] is a known risk factor for ABO [8], but cannot explain sufficiently all contributions [7]. Placental egg deposition and trans-placental transfer of schistosomal antigens to the fetal bloodstream – both closely related to PS – may play an important role as well [6].
4.3. Discussed Pathophysiologic Mechanisms
The transfer of schistosome soluble egg antigen (SEA) across the placenta has been well documented [27,28,29], and appears to happen frequently (up to 86%) in maternal schistosomiasis [29]. McDonald et al. investigated the effects of SEA on placental trophoblast cells in vitro and found a dose-depending upregulation of proinflammatory and chemotactic cytokines [30]. Kurtis et al. have shown that maternal schistosomiasis due to S. japonica was directly associated with both elevated proinflammatory signals in the placenta (TNF-α, IL-6, IL, IL-1β and TNF-IIR) and fetal cord blood (TNF-IIR and IFN-y), respectively [31]. Considering that the upregulation of fetal proinflammatory signals seems to be dose-depending, one can assume that direct deposition of eggs in the placenta might elicit a much stronger proinflammatory response. Increased levels of endotoxins circulating in the maternal blood stream due to schistosomiasis derived microbial translocation may also contribute to placental inflammation [32]. Elevated levels of endotoxins have been found in both non-pregnant [33] and pregnant adults, and were associated with placental inflammation [32].
The immune milieu at the fetal-maternal interface plays a crucial role in various aspects of healthy pregnancies, and is physiologically delineated by a cytokine profile linked to TH-2 cells [34,35]. However, its disbalance through maternal infections can lead to pregnancy complications [36]. For example, shifts towards a more proinflammatory cytokine imprint of the placenta due to maternal malaria infection have been linked to intrauterine growth restriction (IUGR) [37]. Also, in the aforementioned study of Kurtis et al. elevated levels of placental TNF-α and IL-1β were associated with decreased birth weight [31]. Similar findings were reported by Abioye et al., indicating that increased levels of proinflammatory cytokines were linked to a higher risk of prematurity and small-for-gestational-age (SGA) infants [38].
4.4. Treatment Strategies
The question remains whether maternal schistosomiasis or PS specifically should be treated during pregnancy. Praziquantel, the drug of choice for schistosomiasis, has been withheld from pregnant women for decades, due to safety concerns. This practice changed with an updated risk-benefit analysis of the WHO in 2002 [39]. The most recent WHO treatment guidelines for schistosomiasis in 2022 recommend the treatment of pregnant women in second and third trimester both on an individual and mass drug administration level [40]. Still, the use of praziquantel in pregnancy remains a neglected field of research [2]. Two major randomized controlled studies have addressed the safety and efficacy of praziquantel in pregnant women infected with S. mansoni [41] and S. japonicum [42], respectively. Both trials showed that praziquantel can be safely used during second or third trimester. A more recent trial carried out in Gabon addressed the same question in pregnant women infected with S. haematobium (clinicaltrials.gov NCT03779347) [43]. So far, no trials have investigated treatment effects of praziquantel stratified among women who were suffering from PS.
5. Conclusion
We have reviewed and summarized the available literature concerning PS and its contribution to ABO as well as possible underlying mechanisms. The determination of the frequency of PS among pregnant women in endemic regions remains a challenge, and further research using improved maceration techniques [11] are required. Further investigation on the association of PS on ABO and possible advantages of treatment are also urgently needed to prevent morbidity in both mothers and their offspring. Future research on ABO should not be restricted to crude birthweight and prevalence of LBW, but include the assessment of being small for gestational age and calculate the latter with sonographic confirmed gestational age and standard international growth curves [44].
Author Contributions
Conceptualization, BTS; literature search, JG, SM and BTS; writing—original draft preparation, JG and BTS; writing—review and editing, JG, SM, MH, SDD, DGO, JR, JM and BTS; supervision, JM and BTS; All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Data Availability Statement
No new data were created in this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hotez, P.J.; Alvarado, M.; Basáñez, M.G.; Bolliger, I.; Bourne, R.; Boussinesq, M.; Brooker, S.J.; Brown, A.S.; Buckle, G.; Budke, C.M.; u.c. The Global Burden of Disease Study 2010: Interpretation and Implications for the Neglected Tropical Diseases. PLoS Negl. Trop. Dis. 2014, 8, 17. [CrossRef]
- Friedman, J.F.; Olveda, R.M.; Mirochnick, M.H.; Bustinduy, A.L.; Elliott, A.M. Praziquantel for the Treatment of Schistosomiasis during Human Pregnancy. Bull. World Health Organ. 2018, 96, 59–65. [CrossRef]
- World Health Organization Female genital schistosomiasis: A pocket atlas for clinical health-care professionals. Who/Htm/Ntd/2015.4 2015, 2015, 49.
- Bittencourt, A.L.; Gomes Pinto Garcia, A. The Placenta in Hematogenous Infections. Pediatr. Pathol. Mol. Med. 2002, 21, 401–432. [CrossRef]
- Adam, I.; ALhabardi, N.A.; Al-Wutayd, O.; Khamis, A.H. Prevalence of schistosomiasis and its association with anemia among pregnant women: a systematic review and meta-analysis. Parasites and Vectors 2021, 14.
- Freer, J.B.; Bourke, C.D.; Durhuus, G.H.; Kjetland, E.F.; Prendergast, A.J. Schistosomiasis in the first 1000 days. Lancet Infect. Dis. 2018, 18, e193–e203. [CrossRef]
- Friedman, J.F.; Mital, P.; Kanzaria, H.K.; Olds, G.R.; Kurtis, J.D. Schistosomiasis and Pregnancy. Trends Parasitol. 2007, 23, 159–164. [CrossRef]
- Haider, B.A.; Olofin, I.; Wang, M.; Spiegelman, D.; Ezzati, M.; Fawzi, W.W. Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 2013, 347.
- Sutherland, J.C.; Berry, A.; Hynd, M.; Proctor, N.S.. Placental Bilharziasis. South African J. Obstet. amd Gynaecol. 1965, 76–80. [CrossRef]
- Renaud, R.; Brettes, P.; Castanier, C.; Loubiere, R. Placental Bilharziasis. Int. J. Gynecol. Obstet. 1972, 10, 24–30. [CrossRef]
- Holtfreter, M.C.; Neubauer, H.; Groten, T.; El-Adawy, H.; Pastuschek, J.; Richter, J.; Häussinger, D.; Pletz, M.W.; Schleenvoigt, B.T. Improvement of a tissue maceration technique for the determination of placental involvement in schistosomiasis. PLoS Negl. Trop. Dis. 2017, 11. [CrossRef]
- Prates, M.M.; Tropical, M.; Tropical, M. A bilharziose na Africa oriental portuguesa e sua importancia na etiología dos carcinomas primitivos do fígado dos indígenas. An. Inst. Med. Trop. (Lisb). 1948, 5, 149.
- Bittencourt, A.L.; Mott, K. Placental Schistosomiasis. Gaz. Médica da Bahia 1969, 3, 113–117.
- Viggiano, M.G.; Leite, M.S. Placentite esquistosomótica. J. Bras. Ginecol. 1978, 85, 273–278.
- Bittencourt, A.L.; De Almeida, M.A.C.; Iunes, M.A.F.; Casulari Da Motta, L.D.; Bittencourt, L.; Antonio, M.; Almeida, C.D.E.; Amelia, M.; Iunes, F. Placental Involvement in Schistosomiasis Mansoni - Report of Four Cases. Am. J. Trop. Med. Hyg. 1980, 29, 571–575. [CrossRef]
- Peres, L. Schistosoma mansoni eggs in the placenta: an unusual finding. Rev. Hosp. Säo Paulo Esc. Paul. Med 1994, 5, 788–789.
- Schleenvoigt, B.T.; Gajda, M.; Baier, M.; Groten, T.; Oppel-Heuchel, H.; Grimm, M.O.; Pfister, W.; Richter, J.; Pletz, M.W. Placental Schistosoma haematobium infection in a German returnee from Malawi. Infection 2014, 42, 1061–1064. [CrossRef]
- Fujinami, A.; Nakamura, H. On the prophylaxis of schistosomiasis and some investigations on infection with this disease. Chugi- Iji Shimpo 1911, 753.
- Narabayashi, H. Beiträge zur Frage der kongenitalen Invasion von Schistosoma japonicum. Verhandl. Jap. path. Gesellsch. 1914, 4.
- Augustine, D.L. Development in Prenatal Infestation of Belascaris. J. Parasitol. 1927, 13, 256–259. [CrossRef]
- Rodrigues, M. ari. A. Placental bilharziasis - a preliminary report. In Proceedings of the Abstracts of the 7th International Congress of International Academy of Pathology; Milano, Italy, 1968.
- Franz, R.; Hahn, A.; Hagen, R.M.; Rohde, H.; Eberhardt, K.A.; Ehrhardt, S.; Baum, J.; Claussen, L.; Feldt, T.; Hinz, R.; u.c. Screening for Resistant Bacteria, Antimicrobial Resistance Genes, Sexually Transmitted Infections and Schistosoma spp. in Tissue Samples from Predominantly Vaginally Delivered Placentae in Ivory Coast and Ghana. Pathogens 2023, 12. [CrossRef]
- Siegrist, D.; Siegrist-Obimpeh, P. Schistosoma Haematobium Infection in Pregnancy. Acta Trop. 1992, 50, 317–321. [CrossRef]
- Qunhua, L.; Jiawen, Z.; Bozhao, L.; Zhilan, P.; Huijie, Z.; Shaoying, W.; Deln, M.; Hsu, L.-N. Investigation of association between female genital tract diseases and Schistosomiasis japonica infection. Acta Trop. 2000, 77, 179–183.
- Mombo-Ngoma, G.; Honkpehedji, J.; Basra, A.; Mackanga, J.R.; Zoleko, R.M.; Zinsou, J.; Agobe, J.C.D.; Lell, B.; Matsiegui, P.B.; Gonzales, R.; u.c. Urogenital schistosomiasis during pregnancy is associated with low birth weight delivery: analysis of a prospective cohort of pregnant women and their offspring in Gabon. Int. J. Parasitol. 2017, 47, 69–74. [CrossRef]
- Honkpéhèdji, Y.J.; Adegbite, B.R.; Zinsou, J.F.; Dejon-Agobé, J.C.; Edoa, J.R.; Zoleko Manego, R.; McCall, M.; Mbong Ngwese, M.; Lotola Mougeni, F.; Mombo-Ngoma, G.; u.c. Association of low birth weight and polyparasitic infection during pregnancy in Lambaréné, Gabon. Trop. Med. Int. Heal. 2021, 26, 973–981. [CrossRef]
- Romia, S.A.; Handoussa, A.E.; Youseff, S.A.; el Zayat, M.M. Transplacental Transfer of Schistosomal Antigens and Antibodies. J. Egypt. Soc. Parasitol. 1992, 22, 575–582.
- Hassan, M.M.; Hassounah, O.A.; Hegab, M.; Salah, K.; El-Mahrouky, L.; Galal, N. Transmission of Circulating Schistosomal Antigens from Infected Mothers to Their Newborns. J. Egypt. Soc. Parasitol. 1997, 27, 773–780.
- Attallah, A.M.; Ghanem, G.E.; Ismail, H.; El Waseef, A.M. Placental and oral delivery of Schistosoma mansoni antigen from infected mothers to their newborns and children. Am. J. Trop. Med. Hyg. 2003, 68, 647–651. [CrossRef]
- McDonald, E.A.; Kurtis, J.D.; Acosta, L.; Gundogan, F.; Sharma, S.; Pond-Tor, S.; Wu, H.W.; Friedman, J.F. Schistosome egg antigens elicit a proinflammatory response by trophoblast cells of the human placenta. Infect. Immun. 2013, 81, 704–712. [CrossRef]
- Kurtis, J.D.; Higashi, A.; Wu, H.W.; Gundogan, F.; McDonald, E.A.; Sharma, S.; PondTor, S.; Jarilla, B.; Sagliba, M.J.; Gonzal, A.; u.c. Maternal schistosomiasis japonica is associated with maternal, placental, and fetal inflammation. Infect. Immun. 2011, 79, 1254–1261. [CrossRef]
- McDonald, E.A.; Pond-Tor, S.; Jarilla, B.; Sagliba, M.J.; Gonzal, A.; Amoylen, A.J.; Olveda, R.; Acosta, L.; Gundogan, F.; Ganley-Leal, L.M.; u.c. Schistosomiasis japonica during pregnancy is associated with elevated endotoxin levels in maternal and placental compartments. J. Infect. Dis. 2014, 209, 468–472. [CrossRef]
- Onguru, D.; Liang, Y.M.; Griffith, Q.; Nikolajczyk, B.; Mwinzi, P.; Ganley-Leal, L. Short report: Human schistosomiasis is associated with endotoxemia and toll-like receptor 2- and 4-bearing B cells. Am. J. Trop. Med. Hyg. 2011, 84, 321–324. [CrossRef]
- Hanna, N.; Hanna, I.; Hleb, M.; Wagner, E.; Dougherty, J.; Balkundi, D.; Padbury, J.; Sharma, S. Gestational Age-Dependent Expression of IL-10 and Its Receptor in Human Placental Tissues and Isolated Cytotrophoblasts. J. Immunol. 2000, 164, 5721–5728. [CrossRef]
- Ekerfelt, C.; Lidström, C.; Matthiesen, L.; Berg, G.; Sharma, S.; Ernerudh, J. Spontaneous secretion of interleukin-4, interleukin-10 and interferon-γ by first trimester decidual mononuclear cells. Am. J. Reprod. Immunol. 2002, 47, 159–166. [CrossRef]
- PrabhuDas, M.; Bonney, E.; Caron, K.; Dey, S.; Erlebacher, A.; Fazleabas, A.; Fisher, S.; Golos, T.; Matzuk, M.; McCune, J.M.; u.c. Immune mechanisms at the maternal-fetal interface: Perspectives and challenges. Nat. Immunol. 2015, 16, 328–334.
- Moormann, A.M.; Sullivan, A.D.; Rochford, R.A.; Chensue, S.W.; Bock, P.J.; Nyirenda, T.; Meshnick, S.R. Malaria and pregnancy: Placental cytokine expression and its relationship to intrauterine growth retardation. J. Infect. Dis. 1999, 180, 1987–1993. [CrossRef]
- Abioye, A.I.; McDonald, E.A.; Park, S.; Joshi, A.; Kurtis, J.D.; Wu, H.; Pond-Tor, S.; Sharma, S.; Ernerudh, J.; Baltazar, P.; u.c. Maternal, placental and cord blood cytokines and the risk of adverse birth outcomes among pregnant women infected with schistosoma japonicum in the Philippines. PLoS Negl. Trop. Dis. 2019, 13. [CrossRef]
- 2002; 39. World Health Organization Report of the WHO Informal Consultation on the use of Praziquantel during Pregnancy/Lactation and Albendazole/Mebendazole in Children under 24 months; 2002;
- World Health Organization WHO Guideline on control and elimination of human Schistosomiasis; 2022; ISBN 978 92 4 004160 8.
- Ndibazza, J.; Muhangi, L.; Akishule, D.; Kiggundu, M.; Ameke, C.; Oweka, J.; Kizindo, R.; Duong, T.; Kleinschmidt, I.; Muwanga, M.; u.c. Effects of deworming during pregnancy on maternal and perinatal outcomes in entebbe, Uganda: A randomized controlled Trial. Clin. Infect. Dis. 2010, 50, 531–540. [CrossRef]
- Olveda, R.M.; Acosta, L.P.; Tallo, V.; Baltazar, P.I. A randomized double blind placebo controlled trial assessing the efficacy and safety of praziquantel for the treatment of human schistosomiasis during pregnancy. Lancet Infect. Dis. 2016, 16, 199–208. [CrossRef]
- Honkpehedji, Y.J.; Adegnika, A.A.; Dejon-Agobe, J.C.; Zinsou, J.F.; Mba, R.B.; Gerstenberg, J.; Rakotozandrindrainy, R.; Rakotoarivelo, R.A.; Rasamoelina, T.; Sicuri, E.; u.c. Prospective, observational study to assess the performance of CAA measurement as a diagnostic tool for the detection of Schistosoma haematobium infections in pregnant women and their child in Lambaréné, Gabon: Study protocol of the freeBILy clinical trial. BMC Infect. Dis. 2020, 20. [CrossRef]
- Holtfreter, M.C.; Mischlinger, J.; Davi, S.D.; Schleenvoigt, B.T. Investigation on birth weight outcomes in schistosomiasis and praziquantel research: a correspondence. Eur. J. Med. Res. 2023, 28, 231. [CrossRef]
Figure 1.
Flowchart of the systematic literature search with search criteria and selected publications.
Figure 1.
Flowchart of the systematic literature search with search criteria and selected publications.
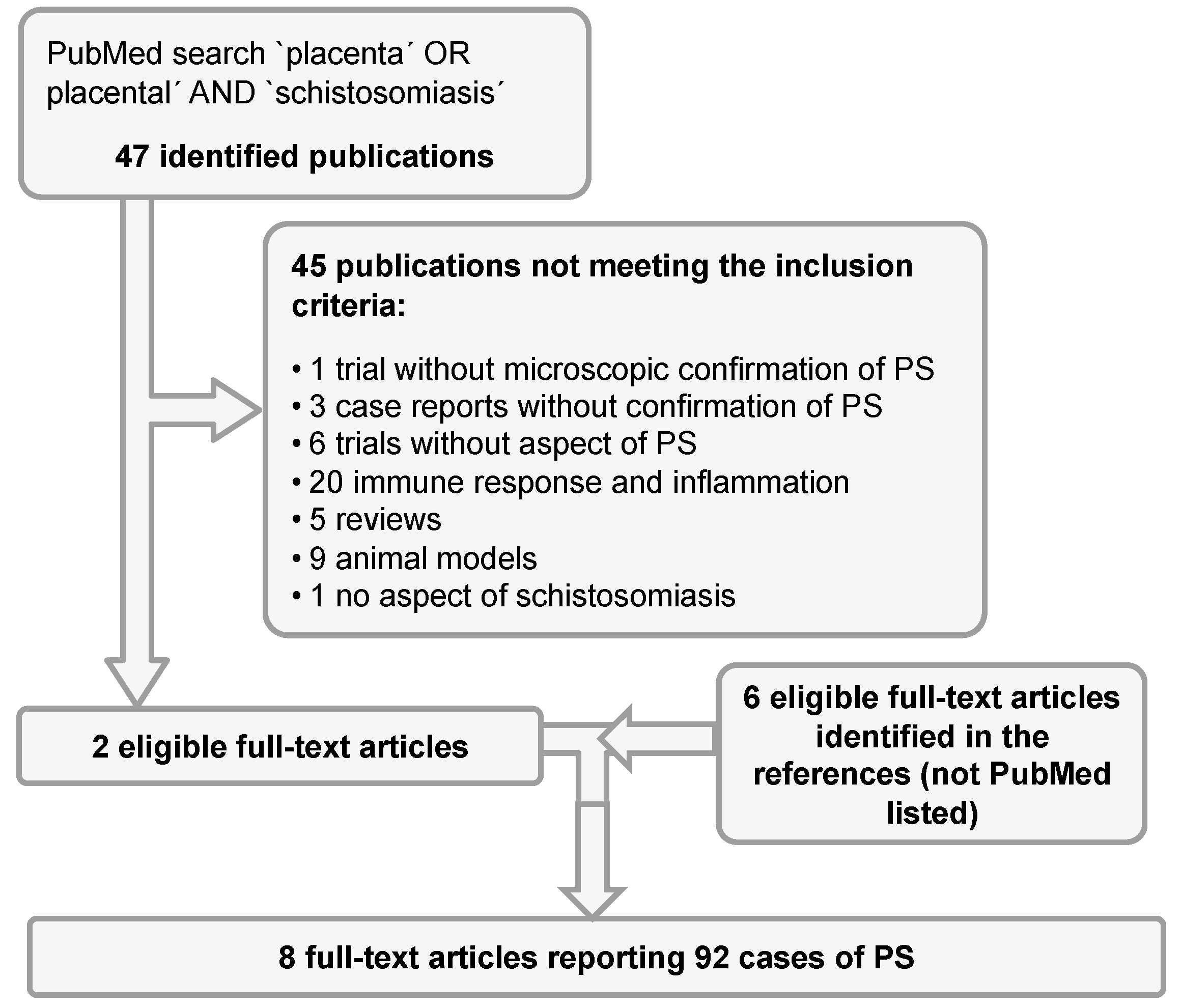

Table 1.
Overview of the cases of Placental Schistosomiasis found in the selected literature.
| Year | Author | Genre | No. of cases | Country of origin | Age | Schistosoma spp. | Adult helminth |
Pregnancy complications |
Applied technique |
|---|---|---|---|---|---|---|---|---|---|
| 1948 | Prates [12] | Case series |
5 | Mozambique | - | S. haematobium | no | NA | Histology |
| 1965 | Sutherland [9] | Case series |
8 | South Africa |
19, NA |
S. haematobium (6) S. mansoni (1) both species (1) |
no | Seizures (1) Preeclampsia (1) | Histology (1), Maceration (7) |
| 1969 | Bittencourt [13] | Case report |
1 | Brazil | 34 | S. mansoni | yes | No | Histology |
| 1971 | Renaud [10] | Clinical study | 72 | Ivory coast |
- | S. haematobium | no | LBW (21) Fetal death (10) Prematurity (21) |
Histology and Maceration |
| 1978 | Viggiano [14] | Case report |
1 | Brazil | 19 | S. mansoni | yes | Fetal death | Histology |
| 1980 | Bittencourt [15] | Case series |
4 (3)Ψ | Brazil | 34, 23, 18, NA | S. mansoni | yes (2) | Fetal death (2) EUG (1) | Histology |
| 1994 | Peres [16] | Case report |
1 | Brazil | 31 | S. mansoni | no | Prematurity, LBW | Histology |
| 2014 | Schleenvoigt [17] | Case report |
1 | Malawi | 28 | S. haematobium | no | no | Histology |
ΨOne of the four cases was the previous described case report from 1969 by the same author. EUG = extrauterine gravidity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



